Neurocognitive Function in Clinically Stable Men with Bipolar I Disorder or Schizophrenia and Normal Control Subjects Lori L. Altshuler, Joseph Ventura, Wilfred G. van Gorp, Michael F. Green, David C. Theberge, and Jim Mintz Background: Patients with bipolar disorder and schizophrenia have been shown to have neurocognitive deficits when compared with control subjects. The degree and pattern of impairment between psychiatric groups have rarely been compared, especially when subjects are psychiatrically stable. Methods: Using a standard neurocognitive battery, we compared euthymic outpatients with bipolar disorder (n 40), stable patients with schizophrenia (n 20), and subjects with no psychiatric disorder (n 22). The neurocognitive domains assessed included executive functioning, verbal memory, visual memory, procedural learning, visuoconstructive ability, and language functions. Effect sizes were calculated for each cognitive domain across groups. Results: Stable schizophrenic subjects demonstrated a generalized cognitive impairment across most domains compared with control subjects, with average effect sizes of .9. Euthymic bipolar subjects were significantly impaired compared with control subjects only in executive functioning (Wisconsin Card Sorting Task) and verbal memory (California Verbal Learning Test) domains (effect sizes in the .8 –.9 range). Performance on the executive function measures was bimodal among bipolar subjects, suggesting two subgroups: one with relatively normal and one with impaired executive functioning. No significant differences between the bipolar patient group and control subjects were observed in visuoconstructive ability, procedural learning, or language function. Conclusions: Both euthymic bipolar subjects and relatively stable schizophrenic subjects differed from control subjects in neurocognitive function. Among schizophrenic subjects, a generalized cognitive impairment was observed, and the degree of impairment was greater in the schizophrenic compared with the bipolar subjects. Subjects with bipolar disorder were impaired in two specific domains (verbal memory and executive function). Furthermore, within the bipolar group there was a subset with relatively normal executive functioning and a subset with significant impairment. Possible reasons for the persistence of these neurocognitive deficits in some subjects with bipolar disorder during periods of euthymia are reviewed. Key Words: Bipolar illness, schizophrenia, neurocognition, func- tion, neuropsychology I n recent years, research on schizophrenia has undergone several fundamental shifts in focus that include consideration of neurocognitive deficits not only as a core feature of the disorder (Keefe 1995) but also as a potent predictor of functional outcome (Green 1996; Green et al 2000; Harvey et al 1998). Cognitive deficits in executive control, attention, working mem- ory, and declarative memory can be severe, generally ranging from 1 to 2 standard deviations below healthy comparison groups (Bilder et al 2000). These deficits have been shown to be present in first-episode patients who are antipsychotic naïve (Bilder et al 2000; Heaton et al 1994; Hoff et al 1992; Saykin et al 1991, 1994) and in patients in clinical remission as well as in the active symptomatic state (Braff 1992; Gold and Green, in press; Nuechterlein and Danson 1984; Nuechterlein et al 1998). Fur- thermore, consistent and highly significant relationships have been detected between key cognitive domains (e.g., episodic memory, immediate/working memory, vigilance, and executive functioning) and functional outcome in schizophrenia (Green 1996; Green et al 2000). The diagnostic specificity of the neurocognitive deficits for schizophrenia and their predictive potential for functional out- come needs further clarification. Studies of subjects with bipolar disorder have demonstrated neurocognitive deficits in many of the same cognitive domains that have previously been reported to be abnormal in patients with schizophrenia (Coffman et al 1990; Ferrier et al 1999; Gard et al 1999; Hawkins et al 1997; Kessing 1998; Martinez-Aran et al 2002; McKay et al 1995; Morice 1990; Paradiso et al 1997; Rossi et al 2000; Sapin et al 1987; Tham et al 1997; van Gorp et al 1998, 1999; Zubieta et al 2001); however, it is difficult to draw conclusions from most of these studies due to methodologic problems, such as grouping bipolar subjects with those with major depression (Gruzelier et al 1988; Kessing 1998; McKay et al 1995), not controlling for the effects of current mood state (mania or depression) (Dupont et al 1990; Seidman et al 2002), or using a limited battery consisting of only one or two neurocognitive tests (Waddington et al 1989; Wolfe et al 1987). In recent studies, investigators have improved methods by including structured diagnostic assessments (Gard et al 1999; van Gorp et al 1998, 1999), studying subjects who were clearly euthymic (Dickerson et al 2001; Gard et al 1999; Rossi et al 2000; van Gorp et al 1998, 1999), and controlling for other confounding variables (Gard et al 1999; Paradiso et al 1997; Zubieta et al 2001). Very few studies involving assessments of bipolar subjects in the euthymic state have been reported. Such studies are critical because they might identify trait-related persistent deficits asso- ciated with the illness. In the few studies reported to date, euthymic subjects with bipolar illness have demonstrated resid- ual neurocognitive impairments despite improvement in clinical state. Friedman et al (1977) found that euthymic bipolar patients From the Department of Psychiatry and Biobehavioral Sciences (LLA, JV, MG, DCT, JM), University of California-Los Angeles; The Department of Veter- ans Affairs Greater Los Angeles Healthcare System (LLA, JV, MFG, JM), Los Angeles, California; and Department of Psychiatry (WGvG), Columbia University, New York, New York. Address reprint requests to Lori Altshuler, M.D., University of California- Los Angeles, Department of Psychiatry, Mood Disorders Research Pro- gram, 300 Medical Plaza, Room 1544, Los Angeles, CA 90095–7057; E-mail: [email protected]. Received March 3, 2004; revised July 26, 2004; accepted August 4, 2004. BIOL PSYCHIATRY 2004;56:560 –569 0006-3223/04/$30.00 doi:10.1016/j.biopsych.2004.08.002 © 2004 Society of Biological Psychiatry

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
NBCLJ
BcsMwesRsetwcCnisnd
Kt
IdoCofgp(1aNtbm
F
A
R
0d
eurocognitive Function in Clinically Stable Men withipolar I Disorder or Schizophrenia and Normalontrol Subjects
ori L. Altshuler, Joseph Ventura, Wilfred G. van Gorp, Michael F. Green, David C. Theberge, andim Mintz
ackground: Patients with bipolar disorder and schizophrenia have been shown to have neurocognitive deficits when compared withontrol subjects. The degree and pattern of impairment between psychiatric groups have rarely been compared, especially whenubjects are psychiatrically stable.ethods: Using a standard neurocognitive battery, we compared euthymic outpatients with bipolar disorder (n � 40), stable patientsith schizophrenia (n � 20), and subjects with no psychiatric disorder (n � 22). The neurocognitive domains assessed included
xecutive functioning, verbal memory, visual memory, procedural learning, visuoconstructive ability, and language functions. Effectizes were calculated for each cognitive domain across groups.esults: Stable schizophrenic subjects demonstrated a generalized cognitive impairment across most domains compared with control
ubjects, with average effect sizes of .9. Euthymic bipolar subjects were significantly impaired compared with control subjects only inxecutive functioning (Wisconsin Card Sorting Task) and verbal memory (California Verbal Learning Test) domains (effect sizes inhe .8–.9 range). Performance on the executive function measures was bimodal among bipolar subjects, suggesting two subgroups: oneith relatively normal and one with impaired executive functioning. No significant differences between the bipolar patient group andontrol subjects were observed in visuoconstructive ability, procedural learning, or language function.onclusions: Both euthymic bipolar subjects and relatively stable schizophrenic subjects differed from control subjects ineurocognitive function. Among schizophrenic subjects, a generalized cognitive impairment was observed, and the degree of
mpairment was greater in the schizophrenic compared with the bipolar subjects. Subjects with bipolar disorder were impaired in twopecific domains (verbal memory and executive function). Furthermore, within the bipolar group there was a subset with relativelyormal executive functioning and a subset with significant impairment. Possible reasons for the persistence of these neurocognitive
eficits in some subjects with bipolar disorder during periods of euthymia are reviewed.ey Words: Bipolar illness, schizophrenia, neurocognition, func-ion, neuropsychology
n recent years, research on schizophrenia has undergoneseveral fundamental shifts in focus that include considerationof neurocognitive deficits not only as a core feature of the
isorder (Keefe 1995) but also as a potent predictor of functionalutcome (Green 1996; Green et al 2000; Harvey et al 1998).ognitive deficits in executive control, attention, working mem-ry, and declarative memory can be severe, generally rangingrom 1 to 2 standard deviations below healthy comparisonroups (Bilder et al 2000). These deficits have been shown to beresent in first-episode patients who are antipsychotic naïveBilder et al 2000; Heaton et al 1994; Hoff et al 1992; Saykin et al991, 1994) and in patients in clinical remission as well as in thective symptomatic state (Braff 1992; Gold and Green, in press;uechterlein and Danson 1984; Nuechterlein et al 1998). Fur-
hermore, consistent and highly significant relationships haveeen detected between key cognitive domains (e.g., episodicemory, immediate/working memory, vigilance, and executive
rom the Department of Psychiatry and Biobehavioral Sciences (LLA, JV, MG,DCT, JM), University of California-Los Angeles; The Department of Veter-ans Affairs Greater Los Angeles Healthcare System (LLA, JV, MFG, JM), LosAngeles, California; and Department of Psychiatry (WGvG), ColumbiaUniversity, New York, New York.
ddress reprint requests to Lori Altshuler, M.D., University of California-Los Angeles, Department of Psychiatry, Mood Disorders Research Pro-gram, 300 Medical Plaza, Room 1544, Los Angeles, CA 90095–7057;E-mail: [email protected].
eceived March 3, 2004; revised July 26, 2004; accepted August 4, 2004.
006-3223/04/$30.00oi:10.1016/j.biopsych.2004.08.002
functioning) and functional outcome in schizophrenia (Green1996; Green et al 2000).
The diagnostic specificity of the neurocognitive deficits forschizophrenia and their predictive potential for functional out-come needs further clarification. Studies of subjects with bipolardisorder have demonstrated neurocognitive deficits in many ofthe same cognitive domains that have previously been reportedto be abnormal in patients with schizophrenia (Coffman et al1990; Ferrier et al 1999; Gard et al 1999; Hawkins et al 1997;Kessing 1998; Martinez-Aran et al 2002; McKay et al 1995; Morice1990; Paradiso et al 1997; Rossi et al 2000; Sapin et al 1987; Thamet al 1997; van Gorp et al 1998, 1999; Zubieta et al 2001);however, it is difficult to draw conclusions from most of thesestudies due to methodologic problems, such as grouping bipolarsubjects with those with major depression (Gruzelier et al 1988;Kessing 1998; McKay et al 1995), not controlling for the effects ofcurrent mood state (mania or depression) (Dupont et al 1990;Seidman et al 2002), or using a limited battery consisting of onlyone or two neurocognitive tests (Waddington et al 1989; Wolfe etal 1987). In recent studies, investigators have improved methodsby including structured diagnostic assessments (Gard et al 1999;van Gorp et al 1998, 1999), studying subjects who were clearlyeuthymic (Dickerson et al 2001; Gard et al 1999; Rossi et al 2000;van Gorp et al 1998, 1999), and controlling for other confoundingvariables (Gard et al 1999; Paradiso et al 1997; Zubieta et al 2001).
Very few studies involving assessments of bipolar subjects inthe euthymic state have been reported. Such studies are criticalbecause they might identify trait-related persistent deficits asso-ciated with the illness. In the few studies reported to date,euthymic subjects with bipolar illness have demonstrated resid-ual neurocognitive impairments despite improvement in clinical
state. Friedman et al (1977) found that euthymic bipolar patientsBIOL PSYCHIATRY 2004;56:560–569© 2004 Society of Biological Psychiatry

mcS(s(safiGhcblcra(W
cAndfpnpcDtaso
cmp
T
M
H
T
G
R
sN tionS sler A
L.L. Altshuler et al BIOL PSYCHIATRY 2004;56:560–569 561
anifested cognitive impairment that was greater than age aloneould explain. Similarly, using the Halstead Reitan battery,avard et al (1980) found that 87% of the older bipolar patientsage �40 years) continued to score in the abnormal range whenymptomatically recovered. Only a single measure on this batteryCategory Test) was reported, making it difficult to tease out thepecific cognitive domains that might have been differentiallyffected. Sapin et al (1987) found that 20 euthymic medication-ree bipolar patients demonstrated significant differences innformation processing compared with control subjects. vanorp et al (1999) found that bipolar patients in the euthymic statead declarative but not procedural memory impairment. Using aomprehensive battery, Zubieta et al (2001) found that euthymicipolar patients had poorer performance on measures of verbalearning, executive functioning, and motor coordination thanontrol subjects. Several more recent studies have similarlyeported executive function deficits, impaired verbal fluency,nd impaired sustained attention in euthymic bipolar subjectsClark et al 2002; El Badri et al 2001; van Gorp et al 1998;ilder-Willis et al 2001).All of these studies compared euthymic subjects with normal
ontrol subjects rather than with another psychiatric population.n earlier study (Dickerson et al 1991) found overlappingeuropsychological abnormalities in patients with bipolar disor-er and schizophrenia, but it did not have a normal control groupor comparison. To our knowledge, only five studies have beenublished in which the investigators directly compared theeuropsychological function of stable outpatients with schizo-hrenia, stable outpatients with bipolar illness, and a normalontrol group while also using a structured instrument to makeSM-IV diagnoses and a standardized neuropsychological bat-
ery (Gard et al 1999; Hawkins et al 1997; Morice 1990; Rossi etl 2000; Tam et al 1998) (Table 1); however, in these studies,ymptom state at the time of the study was not always carefullyperationalized.
The purpose of the study reported here was to furtherompare neurocognitive functioning in carefully defined euthy-ic bipolar subjects with that of stable outpatients with schizo-
able 1. Neuropsychological Functioning in “Remitted” Bipolar Disorder P
Reference N, Diagnosis, State Neurocognitive Tests
orice 1990 20 BP, 60 SZ, 34 NCremitted manicpatients
WAIS-R, WCST
awkins et al 1997 22 BP, 46 SZ, 26 NCoutpatientsreceivingtreatment
WAIS-R, DS, DSym,Arith, Sim, TMTA/B, FAS, BNT,Lang tests
am et al 1998 23 BP, 26 SZ, 10 NCOutpatient status
implied
WCST, RT, BM, CPT orSPAN, Size Est
ard et al 1999 20 BP, 20 SZ, 20 NCOutpatient status
implied
WAIS-R NI, SentenceArrangement, FAS
ossi et al 2000 40 BP, 66 SZ, 64 NC“euthymic” BP,stable SZ
WCST
BP, bipolar disorder; SZ, schizophrenia; NC, normal control; WAIS-R, Wechpan; DSym, digit symbol; Arith, arithmetic; Sim, similarities; TMT A/B, Traiaming Task; Lang. Tests, language tests; NP, neuropsychological; RT, reacPAN, span of apprehension; Size Est, size estimation task; WAIS-R NI, Wech
hrenia. In this study, we examined similarities and differences
in the pattern and severity of neurocognitive deficits in subjectswith one of these two disorders and in normal control subjects.
Methods and Materials
SubjectsThis study was reviewed and approved by the institutional
review board of the Greater Los Angeles Veterans AdministrationMedical Center (GLAVAMC), and informed consent was obtainedfrom all subjects. Patients with bipolar I disorder or schizophre-nia were recruited from consecutive admissions to the outpatientmental health clinics of the GLAVAMC. All subjects underwentthe Structured Clinical Interview for DSM-III-R (SCID). A trainedinterviewer administered the SCID to confirm a diagnosis ofeither bipolar disorder or schizophrenia. This interviewer wasrequired to achieve a minimum overall � of .75 (minimum �sensitivity � .75 and specificity � .75) on symptom agreementand 90% accuracy of agreement on diagnosis (Ventura et al1998). Exclusion criteria included a history of head injury withloss of consciousness exceeding 1 hour, learning disability,migraine headache, liver function abnormalities, alcoholic de-mentia, abuse of alcohol within the past 6 months, prior historyof cocaine abuse or dependence, diabetes, hypertension, historyof seizure disorder, any other neurologic illness, left-handedness,or treatment with electroconvulsive therapy within 2 years of theneuropsychological testing.
Patients were followed prospectively monthly for up to 6months until 3 consecutive months of euthymia or stability, asdefined below, were documented. Subjects with bipolar illnesswere excluded if they met criteria for any other current SCID-obtained DSM-III-R Axis I disorder, including current substanceuse or anxiety disorder. Bipolar subjects were required to have 3months of euthymia, operationalized as having a Young ManiaRating Scale (Young et al 1978) score of �7 and a HamiltonDepression Rating Scale (Hamilton 1960) score of �6 on once-monthly assessments for 3 consecutive months before neuropsy-chological testing. Subjects were taking a range of mood stabi-
s, Schizophrenia Patients, and Normal Control Subjects
Findings Conclusions Limitations
and SZ showedoor WCSTerformance
Cognitive inflexibility notspecific to SZ
Symptom state at time oftesting was not welldefined
BP � NCnly on DSym,MT A/B
NP impairment in BP isintermediate, SZimpairment is globalcompared with NC
Depression was assessedwith self-reportinstrument, but maniawas not
BP � NC onCST
NP functioning candifferentiate betweenSZ, BP, NC
Symptom state at time oftesting was notdefined
erformedorse than BP
nd NC
Frontal lobe deficits notfound in all disorders
Symptom state at time oftesting might not havebeen assessed
BP, NC onCST
BP can be differentiatedfrom SZ on WCST
Symptom state not welldefined, single NP test
dult Intelligence Scale-Revised; WCST, Wisconsin Card Sorting Test; DS, digiting Test A and B; FAS, Controlled Oral Word Association Test; BNT, Bostontime task; BM, backward masking task; CPT, continuous performance test;dult Intelligence Scale Revised as a neuropsychological instrument.
atient
BPpp
SZ �oT
SZ �W
SZ pwa
SZ �W
sler Al Mak
lizing medications, including lithium (63%), anticonvulsants
www.elsevier.com/locate/biopsych
((
iRttomwal
mresSd
2tDasav
562 BIOL PSYCHIATRY 2004;56:560–569 L.L. Altshuler et al
w
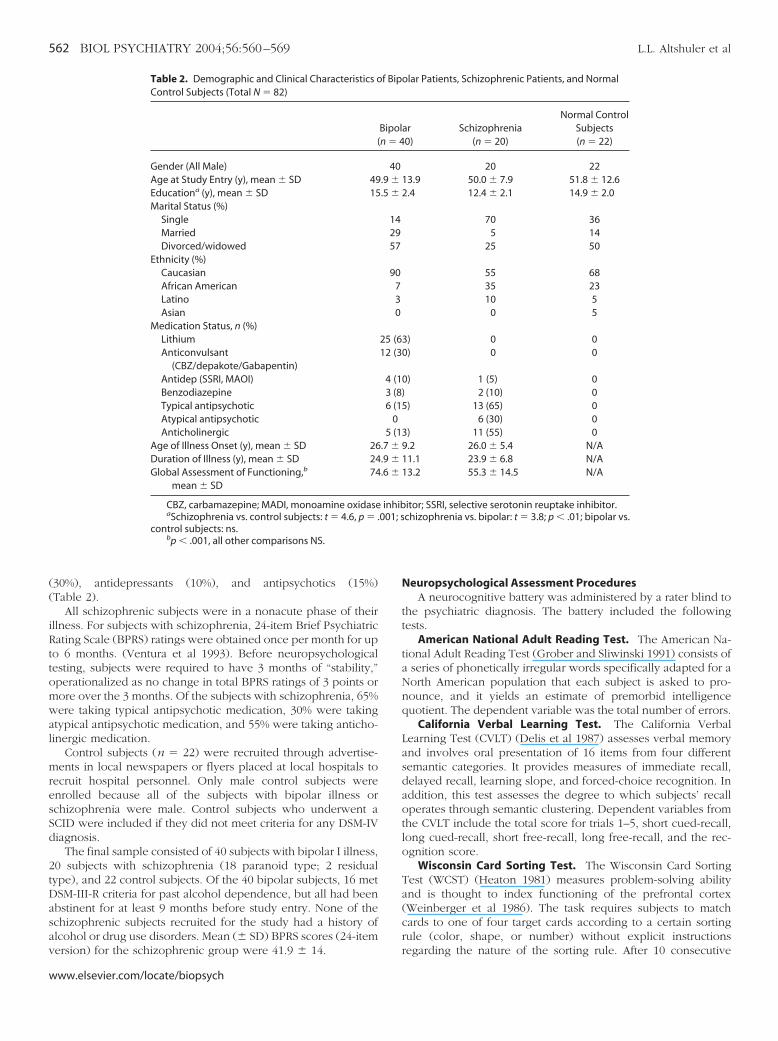
30%), antidepressants (10%), and antipsychotics (15%)Table 2).
All schizophrenic subjects were in a nonacute phase of theirllness. For subjects with schizophrenia, 24-item Brief Psychiatricating Scale (BPRS) ratings were obtained once per month for upo 6 months. (Ventura et al 1993). Before neuropsychologicalesting, subjects were required to have 3 months of “stability,”perationalized as no change in total BPRS ratings of 3 points orore over the 3 months. Of the subjects with schizophrenia, 65%ere taking typical antipsychotic medication, 30% were takingtypical antipsychotic medication, and 55% were taking anticho-inergic medication.
Control subjects (n � 22) were recruited through advertise-ents in local newspapers or flyers placed at local hospitals to
ecruit hospital personnel. Only male control subjects werenrolled because all of the subjects with bipolar illness orchizophrenia were male. Control subjects who underwent aCID were included if they did not meet criteria for any DSM-IViagnosis.
The final sample consisted of 40 subjects with bipolar I illness,0 subjects with schizophrenia (18 paranoid type; 2 residualype), and 22 control subjects. Of the 40 bipolar subjects, 16 metSM-III-R criteria for past alcohol dependence, but all had beenbstinent for at least 9 months before study entry. None of thechizophrenic subjects recruited for the study had a history oflcohol or drug use disorders. Mean (� SD) BPRS scores (24-item
Table 2. Demographic and Clinical Characteristics oControl Subjects (Total N � 82)
(
Gender (All Male)Age at Study Entry (y), mean � SD 49Educationa (y), mean � SD 15Marital Status (%)
SingleMarriedDivorced/widowed
Ethnicity (%)CaucasianAfrican AmericanLatinoAsian
Medication Status, n (%)LithiumAnticonvulsant
(CBZ/depakote/Gabapentin)Antidep (SSRI, MAOI)BenzodiazepineTypical antipsychoticAtypical antipsychoticAnticholinergic
Age of Illness Onset (y), mean � SD 26Duration of Illness (y), mean � SD 24Global Assessment of Functioning,b
mean � SD74
CBZ, carbamazepine; MADI, monoamine oxidaseaSchizophrenia vs. control subjects: t � 4.6, p � .
control subjects: ns.bp � .001, all other comparisons NS.
ersion) for the schizophrenic group were 41.9 � 14.
ww.elsevier.com/locate/biopsych
Neuropsychological Assessment ProceduresA neurocognitive battery was administered by a rater blind to
the psychiatric diagnosis. The battery included the followingtests.
American National Adult Reading Test. The American Na-tional Adult Reading Test (Grober and Sliwinski 1991) consists ofa series of phonetically irregular words specifically adapted for aNorth American population that each subject is asked to pro-nounce, and it yields an estimate of premorbid intelligencequotient. The dependent variable was the total number of errors.
California Verbal Learning Test. The California VerbalLearning Test (CVLT) (Delis et al 1987) assesses verbal memoryand involves oral presentation of 16 items from four differentsemantic categories. It provides measures of immediate recall,delayed recall, learning slope, and forced-choice recognition. Inaddition, this test assesses the degree to which subjects’ recalloperates through semantic clustering. Dependent variables fromthe CVLT include the total score for trials 1–5, short cued-recall,long cued-recall, short free-recall, long free-recall, and the rec-ognition score.
Wisconsin Card Sorting Test. The Wisconsin Card SortingTest (WCST) (Heaton 1981) measures problem-solving abilityand is thought to index functioning of the prefrontal cortex(Weinberger et al 1986). The task requires subjects to matchcards to one of four target cards according to a certain sortingrule (color, shape, or number) without explicit instructions
olar Patients, Schizophrenic Patients, and Normal
ar SchizophreniaNormal Control
Subjects0) (n � 20) (n � 22)
20 2213.9 50.0 � 7.9 51.8 � 12.62.4 12.4 � 2.1 14.9 � 2.0
70 365 14
25 50
55 6835 2310 5
0 5
3) 0 00) 0 0
0) 1 (5) 0) 2 (10) 05) 13 (65) 0
6 (30) 03) 11 (55) 09.2 26.0 � 5.4 N/A11.1 23.9 � 6.8 N/A13.2 55.3 � 14.5 N/A
itor; SSRI, selective serotonin reuptake inhibitor.chizophrenia vs. bipolar: t � 3.8; p � .01; bipolar vs.
f Bip
Bipoln � 4
40.9 �.5 �
142957
90730
25 (612 (3
4 (13 (86 (1
05 (1
.7 �
.9 �
.6 �
inhib001; s
regarding the nature of the sorting rule. After 10 consecutive

msed
Mwlbdw
CsFsfcff
(mnavt
AmcPdd
wvsds
ecaTibrftr
Icsptfst
ap
L.L. Altshuler et al BIOL PSYCHIATRY 2004;56:560–569 563
atches, the sorting rule changes without warning, and theubject needs to determine the new principle. Perseverativerrors and number of categories achieved were used as depen-ent measures.
Verbal Fluency Test. A verbal fluency test, drawn from theultilingual Aphasia Examination (Benton and Hamsher 1978),as used to assess speed of lexical search, and indirectly, frontal
obe functioning. This test assesses the quantity of words thategin with a certain letter and are produced within 60 sec. Theependent variable was the total number of correctly namedords.
Rey-Osterreith Complex Figure Test. The Rey-Osterreithomplex Figure Test (Osterreith 1944; Rey 1941) assesses visuo-patial constructional ability and visual memory. The Complexigure assesses planning and organizational skills and problem-olving strategies, as well as perceptual, motor, and memoryunctions (Waber and Holmes 1986). On this test, the subjectopies a complex figure and then, after a delay, reproduces theigure from memory. The dependent variable was the total scoreor the delay condition.
Trail Making Test (Trails A and B). The Trail Making TestReitan and Wolfson 1985) is a test of rapid visual search andental flexibility. The task requires subjects to 1) connectumbers that are arranged randomly on a page in proper order;nd 2) alternate between numbers and letters. The dependentariable was the total time needed to successfully complete theask.
Block Design. The Block Design subtest from the Wechslerdult Intelligence Scale-Revised (WAIS-R; Wechsler 1981) is aeasure of visuospatial organization and visuomotor function,
onsisting of 12 1-inch blocks that are colored in red and white.articipants are asked to arrange the blocks to match the patternisplayed in the model provided by the examiner. The depen-ent variable was the raw score total for the block design subtest.
Vocabulary Subtest from the WAIS-R. This test consists of 35ords of increasing difficulty that are presented orally andisually. The subject is required to define the words that are thencored (0–2) according to how well the words are defined. Theependent variable was the raw score total for the vocabularyubtest.
Stroop Color Word Association Test. The Stroop test (Comallit al 1962) measures the relative speeds of reading the names ofolors, naming colors, and naming color names that are printed innother color (e.g., the color red is used to print the word “blue”).he score is the amount of time needed by the subject to correctly
dentify items per page. The last task has an interference componentecause it requires the subject to override or inhibit a readingesponse. The Stroop test is viewed as a measure of executiveunctioning and cognitive flexibility. The dependent variable washe time to completion in seconds for naming the colored squares,eading words, and naming all word-colors (interference).
Star Mirror Tracing Task. The Star Mirror Task (Lafayettensurance Company, Lafayette, Indiana) is an apparatus thatonsists of a metal plate attached to a base platform, with aecond polished metal “mirror” hinged vertically. A black, six-ointed star figure is painted on the base platform. Subjectsraced the star with their dominant hand, which was obstructedrom direct view by a shield positioned between them and thetar’s pathway. The dependent variable was the percent of timehat the subject was off-target.
The Pursuit Rotor Test. The Pursuit Rotor (Lafayette Insur-nce Company, photoelectric model) requires subjects to hold a
hotosensitive wand and to pursue and maintain contact with a2-cm light disk rotating on a variable speed turntable. For adetailed description of the Pursuit Rotor, see van Gorp et al(1998). The dependent variable was the on-target time in sec-onds per trial.
Statistical ProceduresThe distributions of scores for each variable were examined to
ensure that they approximated a normal distribution. Variableswith a skewed distribution were normalized with log transfor-mations. Analysis of variance (ANOVA) was performed on keydemographic variables to determine whether there were anysignificant differences across groups. One-way ANOVA was thenperformed on the neurocognitive variables to compare means inthe three diagnostic groups. If the overall ANOVA main effect(with df � 2) was significant, pairwise t tests (Fisher’s leastsignificant difference) were performed on the neurocognitivevariables. With only three groups, this stepdown method givesexperimentwise protection at the nominal � level against type Ierrors. All results at p � .05 were judged to be significant. Effectsizes were calculated for each of the three pairwise comparisons(in Table 3, large effect sizes are indicate with a superscript letter“a”).
Subjects with schizophrenia had significantly less educationthan did subjects with bipolar disorder [t (67) � 4.5, p � .001] andcontrol subjects [t (67) � �3.4, p � .002], with no significantdifference between the latter two groups. Statistically controllingfor education is a complex matter because poorer educationalperformance in schizophrenic patients might result from the veryabilities that are the object of interest for this study. If this is so,controlling for differences in education might attenuate other-wise valid associations. In all comparisons tested below, how-ever, the data were analyzed with and without controlling forsubject education, and all of the significant findings involvingneurocognitive functioning in the former analysis (reportedbelow) remained significant even when education was statisti-cally controlled.
Results
Demographic DataDemographic information is shown in Table 2. There were no
statistically significant differences in age among the three groupsat study entry. The subjects with schizophrenia were found to befunctioning at a significantly lower level compared with subjectswith bipolar disorder, as measured by the Global Assessment ofFunctioning (American Psychiatric Association 1994) [t (46) �4.76, p � .001].
Patterns of Neurocognitive Functioning Across DomainsNeurocognitive data for subjects with bipolar disorder, sub-
jects with schizophrenia, and control subjects are shown in Table3. (Some of these domains have been previously reported on ina subset of the current sample [van Gorp et al 1998, 1999].)Schizophrenic subjects consistently performed more poorly thanbipolar and control subjects across a range of tests, even withBonferroni adjustment for 21 variables. For schizophrenic sub-jects there was a shift in the distributions, with an average effectsize across tests of .9 (median effect size � .94). Among bipolarsubjects, large effects (�.8) were seen in only two cognitivedomains, executive functioning (specifically, set shifting on theWCST) and declarative memory (Table 3).
Executive Functioning. On the executive functioning tests,subjects with bipolar illness and schizophrenia showed signifi-
cant impairment compared with control subjects on the WCSTwww.elsevier.com/locate/biopsych
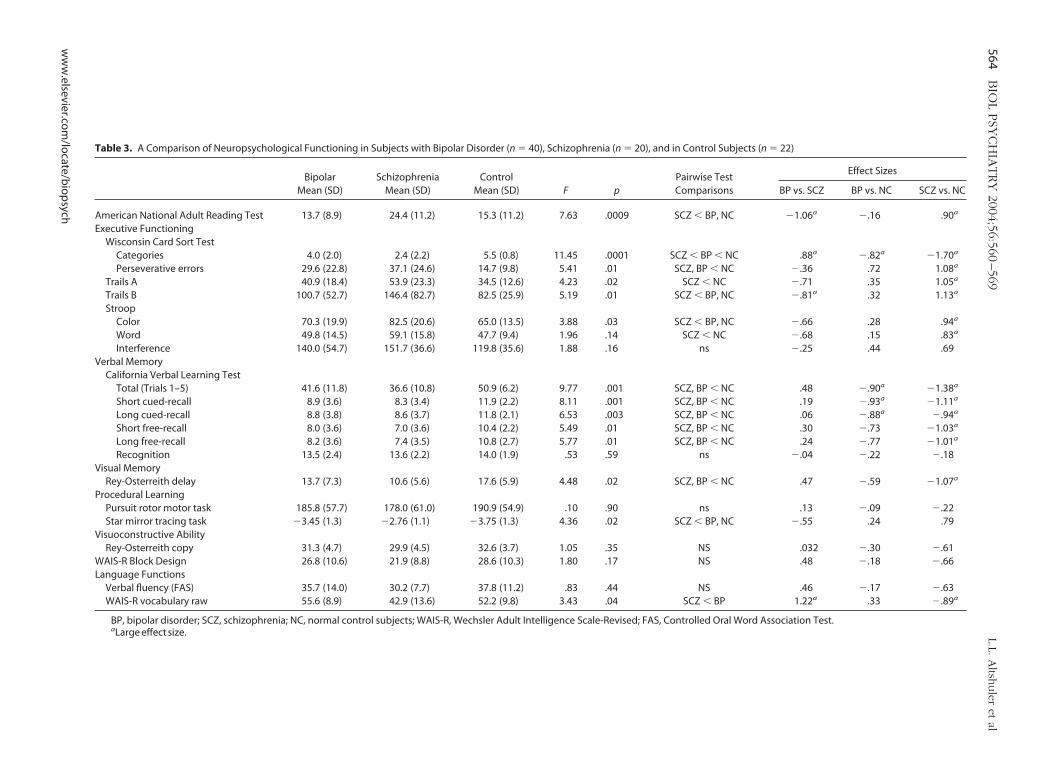
Table 3. A Comparison of Neuropsychological Functioning in Subjects with Bipolar Disorder (n � 40), Schizophrenia (n � 20), and in Control Subjects (n � 22)
BipolarMean (SD)
SchizophreniaMean (SD)
ControlMean (SD) F p
Pairwise TestComparisons
Effect Sizes
BP vs. SCZ BP vs. NC SCZ vs. NC
American National Adult Reading Test 13.7 (8.9) 24.4 (11.2) 15.3 (11.2) 7.63 .0009 SCZ � BP, NC �1.06a �.16 .90a
Executive FunctioningWisconsin Card Sort Test
Categories 4.0 (2.0) 2.4 (2.2) 5.5 (0.8) 11.45 .0001 SCZ � BP � NC .88a �.82a �1.70a
Perseverative errors 29.6 (22.8) 37.1 (24.6) 14.7 (9.8) 5.41 .01 SCZ, BP � NC �.36 .72 1.08a
Trails A 40.9 (18.4) 53.9 (23.3) 34.5 (12.6) 4.23 .02 SCZ � NC �.71 .35 1.05a
Trails B 100.7 (52.7) 146.4 (82.7) 82.5 (25.9) 5.19 .01 SCZ � BP, NC �.81a .32 1.13a
StroopColor 70.3 (19.9) 82.5 (20.6) 65.0 (13.5) 3.88 .03 SCZ � BP, NC �.66 .28 .94a
Word 49.8 (14.5) 59.1 (15.8) 47.7 (9.4) 1.96 .14 SCZ � NC �.68 .15 .83a
Interference 140.0 (54.7) 151.7 (36.6) 119.8 (35.6) 1.88 .16 ns �.25 .44 .69Verbal Memory
California Verbal Learning TestTotal (Trials 1–5) 41.6 (11.8) 36.6 (10.8) 50.9 (6.2) 9.77 .001 SCZ, BP � NC .48 �.90a �1.38a
Short cued-recall 8.9 (3.6) 8.3 (3.4) 11.9 (2.2) 8.11 .001 SCZ, BP � NC .19 �.93a �1.11a
Long cued-recall 8.8 (3.8) 8.6 (3.7) 11.8 (2.1) 6.53 .003 SCZ, BP � NC .06 �.88a �.94a
Short free-recall 8.0 (3.6) 7.0 (3.6) 10.4 (2.2) 5.49 .01 SCZ, BP � NC .30 �.73 �1.03a
Long free-recall 8.2 (3.6) 7.4 (3.5) 10.8 (2.7) 5.77 .01 SCZ, BP � NC .24 �.77 �1.01a
Recognition 13.5 (2.4) 13.6 (2.2) 14.0 (1.9) .53 .59 ns �.04 �.22 �.18Visual Memory
Rey-Osterreith delay 13.7 (7.3) 10.6 (5.6) 17.6 (5.9) 4.48 .02 SCZ, BP � NC .47 �.59 �1.07a
Procedural LearningPursuit rotor motor task 185.8 (57.7) 178.0 (61.0) 190.9 (54.9) .10 .90 ns .13 �.09 �.22Star mirror tracing task �3.45 (1.3) �2.76 (1.1) �3.75 (1.3) 4.36 .02 SCZ � BP, NC �.55 .24 .79
Visuoconstructive AbilityRey-Osterreith copy 31.3 (4.7) 29.9 (4.5) 32.6 (3.7) 1.05 .35 NS .032 �.30 �.61
WAIS-R Block Design 26.8 (10.6) 21.9 (8.8) 28.6 (10.3) 1.80 .17 NS .48 �.18 �.66Language Functions
Verbal fluency (FAS) 35.7 (14.0) 30.2 (7.7) 37.8 (11.2) .83 .44 NS .46 �.17 �.63WAIS-R vocabulary raw 55.6 (8.9) 42.9 (13.6) 52.2 (9.8) 3.43 .04 SCZ � BP 1.22a .33 �.89a
BP, bipolar disorder; SCZ, schizophrenia; NC, normal control subjects; WAIS-R, Wechsler Adult Intelligence Scale-Revised; FAS, Controlled Oral Word Association Test.aLarge effect size.
564B
IOL
PSY
CH
IATRY
2004;56:560–569
L.L.A
ltshuler
etal
ww
w.elsevier.co
m/lo
cate/bio
psych
(of1rwwasst
brft11wpdpcpo
FTsj
L.L. Altshuler et al BIOL PSYCHIATRY 2004;56:560–569 565
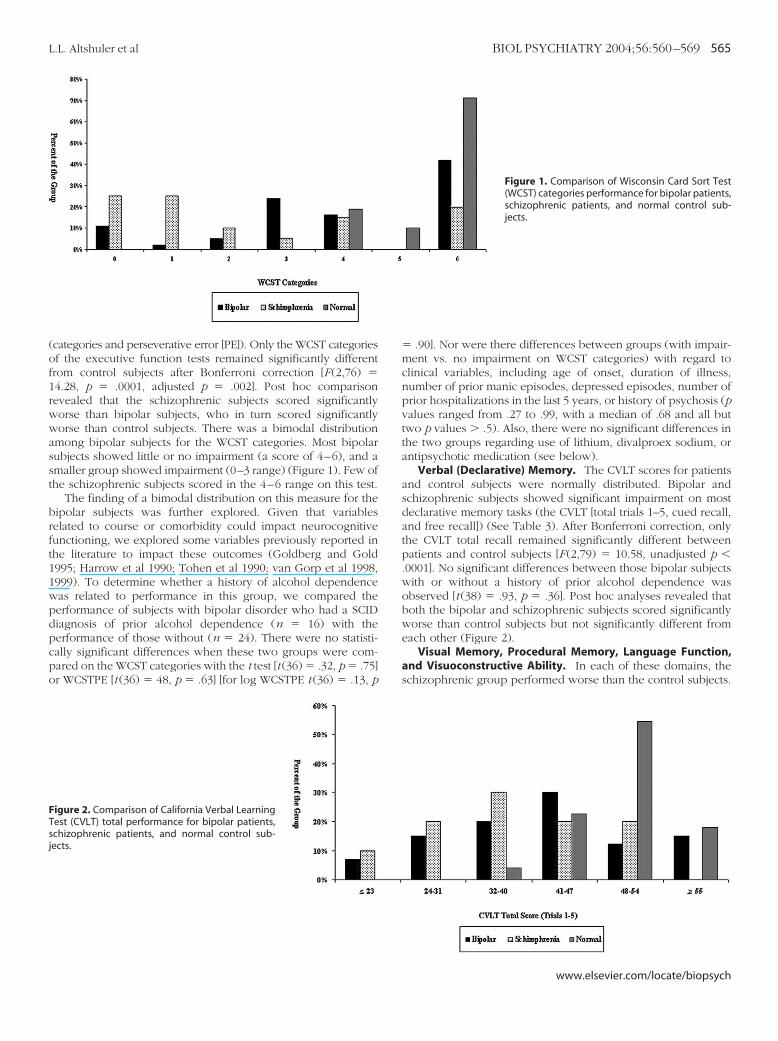
categories and perseverative error [PE]). Only the WCST categoriesf the executive function tests remained significantly differentrom control subjects after Bonferroni correction [F (2,76) �4.28, p � .0001, adjusted p � .002]. Post hoc comparisonevealed that the schizophrenic subjects scored significantlyorse than bipolar subjects, who in turn scored significantlyorse than control subjects. There was a bimodal distributionmong bipolar subjects for the WCST categories. Most bipolarubjects showed little or no impairment (a score of 4–6), and amaller group showed impairment (0–3 range) (Figure 1). Few ofhe schizophrenic subjects scored in the 4–6 range on this test.
The finding of a bimodal distribution on this measure for theipolar subjects was further explored. Given that variableselated to course or comorbidity could impact neurocognitiveunctioning, we explored some variables previously reported inhe literature to impact these outcomes (Goldberg and Gold995; Harrow et al 1990; Tohen et al 1990; van Gorp et al 1998,999). To determine whether a history of alcohol dependenceas related to performance in this group, we compared theerformance of subjects with bipolar disorder who had a SCIDiagnosis of prior alcohol dependence (n � 16) with theerformance of those without (n � 24). There were no statisti-ally significant differences when these two groups were com-ared on the WCST categories with the t test [t (36) � .32, p � .75]r WCSTPE [t (36) � 48, p � .63] [for log WCSTPE t (36) � .13, p
igure 2. Comparison of California Verbal Learningest (CVLT) total performance for bipolar patients,chizophrenic patients, and normal control sub-ects.
� .90]. Nor were there differences between groups (with impair-ment vs. no impairment on WCST categories) with regard toclinical variables, including age of onset, duration of illness,number of prior manic episodes, depressed episodes, number ofprior hospitalizations in the last 5 years, or history of psychosis (pvalues ranged from .27 to .99, with a median of .68 and all buttwo p values � .5). Also, there were no significant differences inthe two groups regarding use of lithium, divalproex sodium, orantipsychotic medication (see below).
Verbal (Declarative) Memory. The CVLT scores for patientsand control subjects were normally distributed. Bipolar andschizophrenic subjects showed significant impairment on mostdeclarative memory tasks (the CVLT [total trials 1–5, cued recall,and free recall]) (See Table 3). After Bonferroni correction, onlythe CVLT total recall remained significantly different betweenpatients and control subjects [F (2,79) � 10.58, unadjusted p �.0001]. No significant differences between those bipolar subjectswith or without a history of prior alcohol dependence wasobserved [t (38) � .93, p � .36]. Post hoc analyses revealed thatboth the bipolar and schizophrenic subjects scored significantlyworse than control subjects but not significantly different fromeach other (Figure 2).
Visual Memory, Procedural Memory, Language Function,and Visuoconstructive Ability. In each of these domains, theschizophrenic group performed worse than the control subjects.
Figure 1. Comparison of Wisconsin Card Sort Test(WCST) categories performance for bipolar patients,schizophrenic patients, and normal control sub-jects.
www.elsevier.com/locate/biopsych

TdcoDf
I
nlto(thwmpceat[mt
pmspcCtcnawdts
D
otSpThaamwaofmfmMob
566 BIOL PSYCHIATRY 2004;56:560–569 L.L. Altshuler et al
w
he bipolar group was generally intermediate, but none of theseifferences were significant after Bonferroni correction. Specifi-ally, no significant differences were observed between groupsn Pursuit Rotor Test, Star Mirror Tracing Task, Rey-Osterreithelay, WAIS-R Block Design and Vocabulary tests, and verbal
luency (Table 3).
mpact of Medication Status on Neurocognitive FunctioningMedication Status in Bipolar Disorder. There were no sig-
ificant differences between subjects with bipolar illness takingithium (n � 25) and those not taking lithium (n � 15) for any ofhe neurocognitive tests administered in this study. The numbersf subjects with bipolar illness taking antipsychotic medicationsn � 6) or anticholinergic medication (n � 5) were too small andhe number of comparisons too large for definitive conclusions;owever, the use of antipsychotic medication in bipolar patientsas not related to CVLT total scores. The use of antipsychoticedication in bipolar subjects was significantly associated withoorer performance on WCST categories [t (26) � 2.81, p � .01]ompared with bipolar subjects not using antipsychotics; how-ver, in the larger subgroup of bipolar patients not takingntipsychotic medication, performance on the WCST categoryest was still significantly lower than for the control subjectst (41) � 2.16, p � � .04]. Thus, the use of antipsychoticedication per se did not explain the executive function cogni-
ive disturbance in the bipolar subjects.Medication Status in Schizophrenic Subjects. For schizo-
hrenic patients, the number of patients taking anticholinergicedication (n �11) or not taking anticholinergics (n � 9) was
mall, so the results should be viewed as tentative. Schizophrenicatients taking anticholinergic medication performed signifi-antly worse than those not taking an anticholinergic on theVLT (p � .02); however, schizophrenic patients who were not
aking any anticholinergic medications still performed signifi-antly worse than control subjects on the CVLT (p � .05). Theumber of schizophrenic patients who were taking typicalntipsychotic medication (n � 13) compared with those whoere taking atypical antipsychotics (n � 7) was also too small forefinitive conclusions; however, schizophrenic patients takingypical versus atypical antipsychotic medications did not differignificantly on the neurocognitive tests.
iscussion
The present study has several limitations. First, it involvesnly male veteran subjects, and the generalization of the findingso women or a nonveteran population remains to be explored.econd, the subject sample size is small, which results in limitedower for estimating effect sizes or for examining subgroups.hird, all subjects were taking medication. In the present study,owever, patients were assessed at a time of relative stability,nd both a structured clinical instrument for psychiatric diagnosisnd structured rating scales were included to assess the degree ofanic, depressive, and psychotic symptoms. These assessmentsere used to verify that bipolar patients were in fact euthymicnd that schizophrenic patients were relatively stable at the timef neuropsychological testing. Although many prior studies haveound cognitive impairments that are similar across many do-ains in schizophrenia and bipolar illness, these were often
ound when bipolar subjects were inpatients and most likelyanic (Albus et al 1996; Goldberg et al 1993; Gruzelier et al 1988;cGrath et al 1997; Zihl et al 1998). Other studies failed to reportr reported very limited information on the symptom status of
ipolar subjects during neuropsychological testing (Bellini et alww.elsevier.com/locate/biopsych
1988; Gard et al 1999; Hobart et al 1999; Tam et al 1998). Wewere not able to find any other studies of stable schizophrenicoutpatients, euthymic bipolar outpatients, and normal controlsubjects in which these groups were evaluated with both acomprehensive neurocognitive battery and structured assess-ment criteria for defining euthymia and stability.
We observed a more diffuse pattern of neurocognitive impair-ment in the schizophrenic subjects compared with the bipolarpatients, who performed in a way that was comparable to thecontrol subjects. That is, euthymic bipolar patients as a group didnot show as extensive or broad neurocognitive dysfunction asseen in the schizophrenic subjects here and as previouslyreported (Gold and Green, in press; Goldberg et al 1993; Green2001). Although bipolar patients performed more poorly as agroup than control subjects on tests of executive function, theyperformed significantly better than the schizophrenic patients.Similarly, for verbal memory, bipolar patients’ performance wasagain intermediate between schizophrenic patients and controlsubjects. These findings suggest deficits in these cognitive do-mains for bipolar patients that are distinct and are not solely staterelated.
Whereas the CVLT scores were normally distributed in thebipolar, schizophrenic, and control subjects, a bimodal patternfor executive function as assessed by the WCST was seen in thebipolar cohort, with many in the group indistinguishable fromnormal and many indistinguishable from the group with schizo-phrenia. These findings suggest that studies reporting meandifferences between bipolar disorder and schizophrenic patientsmight be failing to recognize that a subgroup of bipolar patientsis demonstrating most of the impairment. The reason for thisdifference between subgroups remains to be clarified. Prelimi-nary explorations did not reveal an association of executiveimpairment with an alcohol history, as it did in a smaller priorstudy (van Gorp et al 1998). Furthermore, medication status andprior course of illness did not explain differences in thesevariables. Very few studies of executive functioning in bipolarsubjects compared with both a control and a schizophrenicsample have been done. Morice (1990) found that both schizo-phrenic and bipolar subjects performed poorly on WCST cate-gories and perseverative errors, which were not distinguishablefrom each other even after controlling for intelligence quotient.In another study, schizophrenic subjects performed significantlyworse than control subjects on WCST categories and total errors,and bipolar patients showed an intermediate performance (Rossiet al 2000). Similarly, Martinez-Aran et al (2002) found a patternof deficits in executive function in both groups, but the WCSTdeficits were worse in schizophrenia. Findings from the presentstudy seem consistent with those of previous studies that foundthat deficits in executive neurocognitive functioning exist in bothpsychiatric groups but are more pronounced in the schizo-phrenic cohort when compared with subjects with bipolardisorder. Although previously reported executive deficits inbipolar subjects seem to be intermediate between control sub-jects and schizophrenic subjects, previous studies did not reportthe percentage of bipolar subjects who actually scored in theimpaired range, but rather mean scores. Thus, it is not possible toassess whether a bimodal pattern existed in those studies as it did inours. In our study, those bipolar subjects taking antipsychoticmedication performed significantly more poorly on the WCSTcategory test, suggesting that either antipsychotic medication or ahistory of psychosis (leading to the prescribing of antipsychoticmedication) might contribute to executive functioning deficits;
however, this association is not completely explanatory because the
lav
es(c1bhfAcaTedrt(uwfar(sbdsageHbdrAwiiioAcctAd(b
rcdritncfa
L.L. Altshuler et al BIOL PSYCHIATRY 2004;56:560–569 567
arger bipolar patient subgroup who were not taking antipsychoticslso performed significantly worse than control subjects on thisariable.
One possibility for our findings of bimodality could be thexistence of another comorbidity in this cohort of the bipolarubjects, such as attention-deficit/hyperactivity disorderADHD). High rates of comorbid ADHD have been reported inhildren with bipolar disorder (Sachs et al 2000; Wozniak et al995), but the continuing comorbidity in adults has only recentlyegun to be explored (Sachs et al 2000). Attention-deficit/yperactivity disorder has been associated with executive dys-unction in children (Seidman et al 2001). It is well known thatDHD persists into adulthood in many affected children. Be-ause the SCID for adults does not have an ADHD module, ourdults were not systematically assessed for this comorbidity.hus, whether the subjects of the cohort in our current study whoxhibit abnormal frontal (executive) functioning represent aistinct group with ADHD comorbidity is unclear. Recent neu-opsychological studies of persons with adult ADHD have iden-ified deficits in performing a range of working memory tasksBarkley 1997; Barkley et al 1996; Schweitzer et al 2000) and lessse of frontal regions on positron emission tomography scanshile performing these tasks (Schweitzer et al 2000). Executive
unction impairment has been observed in some bipolar subjectss early as the first episode of bipolar illness and mightepresent a vulnerability marker for developing bipolar disorderYurgelun-Todd et al, unpublished data). One recent prospectivetudy (Meyer et al, in press) of adolescents at risk of developingipolar disorder revealed that 67% of the adults with bipolarisorder had shown impairment on neuropsychological mea-ures sensitive to frontal lobe function in adolescence, beforend therefore preceding the diagnosis of bipolar disorder, sug-esting either a neurodevelopmental vulnerability that is initiallyxpressed as attentional deficits or a comorbidity of ADHD.armer et al (2002) have recently proposed that what seems toe a working memory deficit in euthymic subjects with bipolarisorder might in fact represent a sustained attentional deficitepresenting a reduced inherent capacity (Clark et al 2002).gain, this might be present in only a subpopulation of subjectsith the illness and might account for our current findings. This
nherent attentional deficit might be independent from course ofllness variables and thus explain our inability to find course-of-llness variables associated with the group with executive mem-ry impairment. This is an area that requires further study. If anDHD comorbidity is responsible for executive dysfunction in aohort of bipolar subjects, then bipolar subjects without thisomorbidity have relatively little executive cognitive deficits inhe euthymic state. If persons with bipolar disorder and withoutDHD comorbidity also have executive dysfunction, then thisysfunction might represent, as suggested by Harmer et al2002), a sustained attentional deficit as a core trait marker ofipolar illness.
The reason for the impairment in declarative memory alsoemains to be further elucidated. The degree to which specificlasses of medication contribute to this neuropsychologicaleficit seen in patients with bipolar disorder and schizophreniaequires further study. Medications used to treat both bipolarllness and schizophrenia can impact neuropsychological func-ion and confound results. The issue of medication effects oneurocognitive functioning in bipolar patients is complex andan probably only be definitively addressed in studies designedor that purpose. Lithium in particular has been demonstrated to
ffect tests of memory and speed of information processing(Ananth et al 1987; Gold et al 1991; Honig et al 1999; Kocsis et al1993; Prohaska et al 1996). The effects on neurocognitiveperformance with typical antipsychotic medication have beenmixed (Epstein et al 1996; Goldberg and Gold 1995; Verdoux etal 1995). Although some studies reported that neurocognitivefunctioning might have been impaired by the use of typicalantipsychotics, most conclude that the impact on cognition islimited and point out that cognitive deficits existed in schizo-phrenic patients during the preantipsychotic era (Goldberg andGold 1995). In contrast, most studies of the effects of anticholin-ergic medication in schizophrenia have found an associationwith impaired neurocognitive functioning (Gold et al 1991;Sweeney et al 1991). Consistent with the previous literature, theschizophrenic patients in our sample who were not takinganticholinergic medication also had significantly poorer verballearning performance than control subjects. Thus, the use anti-cholinergic medication did not alone explain the poor neurocog-nitive performance found in the schizophrenic patients com-pared with control subjects. Our analysis suggests thatmedication effects alone cannot account for the patterns ofneurocognitive performance differences among groups; how-ever, the results from the medication analyses must be consid-ered speculative because of the small number of subjects in-volved in the subgroups. Another possibility is that both theexecutive functioning and memory problems could relate toduration of illness, severity of prior illness, or other comorbidmedical conditions, although such clinical variables explored inthe current study were not significantly associated with theneurocognitive impairments seen. Alternatively, it is also possiblethat, independent of medication, the neuropsychological deficitsrepresent, as mentioned above, a core feature of each illness.
The current findings suggest enduring neurocognitive impair-ment on a range of domains in stable schizophrenic subjects, andan enduring neurocognitive impairment in a subset of bipolarsubjects in two specific cognitive domains (executive functioningand declarative memory) in the euthymic state. This discrete butenduring impairment in specific neurocognitive domains mightgive clues to the underlying brain regions either involved in theprimary pathology of the disorder or impacted by the presence ofthe disorder. Knowledge of the brain regions known to beinvolved in the specific affected cognitive processes might guideneuroimaging studies that selectively target examination of thesebrain regions. Frontal lobe abnormalities have been reported inbipolar subjects in several structural and functional imagingstudies (Altshuler et al, in press; Beyer and Krishnan 2002;Blumberg et al 2000, 2003; Strakowski et al 1999; Doris et al 2004;Lopez-Larson et al 2002; Sharma et al 2003). Studies have notgenerally reported structural volumetric hippocampal abnormal-ities (Altshuler et al 1998, 2000; Brambilla et al 2002; Hauser et al1989) that would help to explain the declarative memory deficitsseen in this study; however, in a recent study, reduced hip-pocampal volume in bipolar subjects was reported (Blumberg etal 2003).
The relationship between the presence of these neurocogni-tive deficits and functional impairment in subjects with bipolardisorder has only recently begun to be explored. Preliminarydata from our group (Altshuler et al, unpublished data) suggestthat low performance on neurocognitive measures of verbalmemory and executive function might be associated with lowcurrent role functioning and are an area of current exploration inour laboratory. These data might have implications for understand-
ing the varied functional outcome in the bipolar population.www.elsevier.com/locate/biopsych
DIaApeA
A
A
A
A
A
A
B
B
B
B
B
B
B
B
B
B
C
C
C
D
D
D
D
568 BIOL PSYCHIATRY 2004;56:560–569 L.L. Altshuler et al
w
This research was supported by a Merit Review Award,epartment of Veteran Affairs, and a Stanley Medical Research
nstitute research grant (both to LLA). Lori L. Altshuler serves asconsultant or is on the advisory board and speakers’ bureau forbbott Laboratories, Bristol-Meyers Squibb, Eli Lilly and Com-any, Forrest Laboratories, Janssen Pharmaceuticals, AstraZen-ca, and Pfizer Inc. Additionally, she has research support frombbott Laboratories, Eli Lilly, and Pfizer.
lbus M, Hubmann W, Wahlheim C, Sobizack N, Franz U, Mohr F (1996):Contrasts in neuropsychological test profile between patients with first-episode schizophrenia and first-episode affective disorders. Acta Psychi-atr Scand 94:87–93.
ltshuler LL, Bartzokis G, Grieder T, Curran J, Jimenez T, Leight K, et al (2000):An MRI study of temporal lobe structures in men with bipolar disorder orschizophrenia. Biol Psychiatry 48:147–162.
ltshuler LL, Bartzokis G, Grieder T, Curran J, Mintz J (1998): Amygdalaenlargement in bipolar disorder and hippocampal reduction in schizo-phrenia: An MRI study demonstrating neuroanatomic specificity. ArchGen Psychiatry 55:663– 664.
ltshuler LL, Bookheimer S, Proenza M, Townsend J, Sabb J, Firestine A, et al(in press): Increased amygdala activation during mania: A functionalmagnetic resonance imaging study. Am J Psychiatry.
merican Psychiatric Association (1994): Diagnostic and Statistical Manual ofMental Disorders, 4th ed. Washington, DC: American Psychiatric Press.
nanth J, Ghadirian AM, Engelsmann F. (1987): Lithium and memory: Areview. Can J Psychiatry 32:312–316.
arkley RA (1997): Behavioral inhibition, sustained attention and executivefunctions: Constructing a unifying theory of ADHD. Psychol Bull 121:65–94.
arkley R, Murphy K, Kwasnik D (1996): Psychological adjustment and adap-tive impairments in young adults with ADHD. J Atten Disord 1:41–54.
ellini L, Gambini O, Palladino F, Scarone S (1988): Neuropsychological as-sessment of functional central nervous system disorders. I. Hemisphericfunctioning characteristics in schizophrenia and affective illness. ActaPsychiatr Scand 78:242–246.
enton AL, Hamsher K (1978): Multilingual Aphasia Examination Manual–Revised. Iowa City: University of Iowa.
eyer JL, Krishnan KR (2002): Volumetric brain imaging findings in mooddisorders. Bipolar Disord 4:89 –104.
ilder RM, Goldman RS, Robinson D, Reiter G, Bell L, Bates JA, et al (2000):Neuropsychology of first-episode schizophrenia: Initial characterizationand clinical correlates. Am J Psychiatry 157:549 –559.
lumberg HP, Kaufman J, Martin A, Whiteman R, Zhang JH, Gore JC, et al(2003): Amygdala and hippocampal volumes in adolescents and adultswith bipolar disorder. Arch Gen Psychiatry 60:1201–1208.
lumberg HP, Stern E, Martinez D, Ricketts S, de Asis J, White T, et al (2000):Increased anterior cingulate and caudate activity in bipolar mania. BiolPsychiatry 48:1045–1052.
raff DL (1992): Reply to cognitive therapy and schizophrenia. Schizophr Bull18:37–38.
rambilla P, Barale F, Caverzasi E, Soares JC (2002): Anatomical MRI findingsin mood and anxiety disorders. Epidemiol Psichiatr Soc 11:88 –99.
lark L, Iversen SD, Goodwin GM (1902): Sustained attention deficit in bipo-lar disorder. Br J Psychiatry 180:313–319.
offman JA, Bornstein RA, Olson SC, Schwarzkopf SB, Nasrallah HA (1990):Cognitive impairment and cerebral structure by MRI in bipolar disorder.Biol Psychiatry 27:1188 –1196.
omalli PE, Wapner S, Werner H (1962): Interference effects of Stroop color-word test in childhood, adulthood and aging. J Genet Psychol 100:47–53.
elis DC, Kramer JH, Kaplan E, Ober BA(1987): California Verbal Learning Test:Adult Version Manual. San Antonio: The Psychological Corporation.
ickerson FB, Ringel NB, Boronow JJ (1991): Neuropsychological deficits inchronic schizophrenics. Relationship with symptoms and behavior.J Nerv Ment Dis 179:744 –749.
ickerson FB, Sommerville J, Origoni AE, Ringel NB, Parente F (2001): Outpa-tients with schizophrenia and bipolar I disorder: Do they differ in theircognitive and social functioning? Psychiatry Res 102:21–27.
oris A, Belton E, Ebmeier KP, Glabus MF, Marshall I (2004): Reduction ofcingulate gray matter density in poor outcome bipolar illness. Psychiatry
Res 130:153–159.ww.elsevier.com/locate/biopsych
Dupont RM, Jernigan TL, Butters N, Delis D, Hesselink JR, Heindel W, Gillin JC.(1990): Subcortical abnormalities detected in bipolar affective disorderusing magnetic resonance imaging. Clinical and neuropsychologicalsignificance. Arch Gen Psychiatry 47:55–59.
El Badri SM, Ashton CH, Moore PB, Marsh VR, Ferrier IN (2001): Electrophys-iological and cognitive function in young euthymic patients with bipolaraffective disorder. Bipolar Disord 3:79 – 87.
Epstein JI, Keefe RS, Roitman SL, Harvey PD, Mohs RC (1996): Impact ofneuroleptic medications on continuous performance test measures inschizophrenia. Biol Psychiatry 39:902–905.
Ferrier IN, Stanton BR, Kelly TP, Scott J (1999): Neuropsychological functionin euthymic patients with bipolar disorder. Br J Psychiatry 175:246 –251.
Friedman MJ, Culver CM, Ferrell RB (1977): On the safety of long-term treat-ment with lithium. Am J Psychiatry 134:1123–1126.
Gard D, Harrell EH, Poreh A (1999): Cognitive deficits in schizophrenia on theWAIS-R NI Sentence Arrangement Subtest. Wechsler Adult IntelligenceScale-Revised Neuropsychological Inventory. J Clin Psychol55:1085–1094.
Gold JM, Goldberg TE, Kleinman JE, Weinberger DR (1991): The impact ofsymptomatic state and pharmacological treatment on cognitive func-tioning of patients with schizophrenia and mood disorders. In: Mohr E,Brouwers P, eds. Handbook of Clinical Trials: The Neurobehavioral Ap-proach. Lisse, Netherlands: Swets and Zeitlinger, 185–214.
Gold JM, Green MF (in press): Neurocognition in Schizophrenia. In: Kaplan HI,Sadock BJ, eds. Kaplan and Sadock’s Comprehensive Textbook of Psychia-try. Baltimore: Lippincott, Williams & Wilkins.
Goldberg TE, Gold JM (1995): Neurocognitive functioning in patients withschizophrenia. In: Bloom FE, Kupfer DJ. Psychopharmacology: The FourthGeneration of Progress. New York: Raven Press, 1245–1257.
Goldberg TE, Gold JM, Greenberg R, Griffin S, Schulz SC, Pickar D, et al (1993):Contrasts between patients with affective disorders and patients withschizophrenia on a neuropsychological test battery. Am J Psychiatry150:1355–1362.
Green MF (1996): What are the functional consequences of neurocognitivedeficits in schizophrenia? Am J Psychiatry 153:321–330.
Green MF(1901): Schizophrenia Revealed: From Neurons to Social Interactions.New York: W.W. Norton & Company.
Green MF, Kern RS, Braff DL, Mintz J (1900): Neurocognitive deficits andfunctional outcome in schizophrenia: Are we measuring the “rightstuff”? Schizophr Bull 26:119 –136.
Grober E, Sliwinski M. (1991): Development and validation of a model forestimating premorbid verbal intelligence in the elderly. J Clin Exp Neuro-psychol 13:933–949.
Gruzelier J, Seymour K, Wilson L, Jolley A, Hirsch S (1988): Impairments onneuropsychologic tests of temporohippocampal and frontohippocam-pal functions and word fluency in remitting schizophrenia and affectivedisorders. Arch Gen Psychiatry 45:623– 629.
Hamilton M (1960): A rating scale for depression. J Neurol Neurosurg Psychi-atry 23:56 – 62.
Harmer CJ, Clark L, Grayson L, Goodwin GM (1902): Sustained attentiondeficit in bipolar disorder is not a working memory impairment in dis-guise. Neuropsychologia 40:1586 –1590.
Harrow M, Goldberg JF, Grossman LS, Meltzer HY (1990): Outcome in manicdisorders. A naturalistic follow-up study. Arch Gen Psychiatry 47:665–671.
Harvey PD, Howanitz E, Parrella M, White L, Davidson M, Mohs RC, et al(1998): Symptoms, cognitive functioning and adaptive skills in geriatricpatients with lifelong schizophrenia: A comparison across treatmentsites. Am J Psychiatry 155:1080 –1086.
Hauser P, Altshuler LL, Berrettini W, Dauphinais ID, Gelernter J, Post RM(1989): Temporal lobe measurement in primary affective disorder bymagnetic resonance imaging. J Neuropsychiatry Clin Neurosci 1:128 –134.
Hawkins KA, Hoffman RE, Quinlan DM, Rakfeldt J, Docherty NM, Sledge WH(1997): Cognition, negative symptoms, and diagnosis: A comparison ofschizophrenic, bipolar and control samples. J Neuropsychiatry Clin Neu-rosci 9:81– 89.
Heaton R, Paulsen JS, McAdams LA, Kuck J, Zisook S, Braff D, et al (1994):Neuropsychological deficits in schizophrenics. Relationship to age, chro-nicity and dementia. Arch Gen Psychiatry 51:469 – 476.
Heaton RK (1981): A Manual for the Wisconsin Card Sorting Test. Odessa,Florida: Psychological Assessment Resources.
Hobart MP, Goldberg R, Bartko JJ, Gold JM (1999): Repeatable battery for the
assessment of neuropsychological status as a screening test in schizo-
H
H
K
K
K
L
M
M
M
M
M
N
N
O
P
P
R
R
R
S
S
S
S
L.L. Altshuler et al BIOL PSYCHIATRY 2004;56:560–569 569
phrenia, II: Convergent/discriminant validity and diagnostic groupcomparisons. Am J Psychiatry 156:1951–1957.
off AL, Riordan H, O’Donnell DW, Morris L, DeLisi LE (1992): Neuropsycho-logical functioning of first-episode schizophreniform patients. Am J Psy-chiatry 149:898 –903.
onig A, Arts BM, Ponds RW, Riedel WJ (1999): Lithium induced cognitiveside-effects in bipolar disorder: A qualitative analysis and implicationsfor daily practice. Int Clin Psychopharmacol 14:167–171.
eefe RS (1995): The contribution of neuropsychology to psychiatry. Am JPsychiatry 152:6 –15.
essing LV (1998): Cognitive impairment in the euthymic phase of affectivedisorder. Psychol Med 28:1027–1038.
ocsis JH, Shaw ED, Stokes PE, Wilner P, Elliot AS, Sikes C, et al (1993):Neuropsychologic effects of lithium discontinuation. J Clin Psychophar-macol 13:268 –275.
opez-Larson MP, DelBello MP, Zimmerman ME, Schwiers ML, StrakowskiSM (2002): Regional prefrontal gray and white matter abnormalities inbipolar disorder. Biol Psychiatry 52:93–100.
artinez-Aran A, Penades R, Vieta E, Colom F, Reinares M, Benabarre A, et al(2002): Executive function in patients with remitted bipolar disorder andschizophrenia and its relationship with functional outcome. PsychotherPsychosom 71:39 – 46.
cGrath J, Scheldt S, Welham J, Clair A (1997): Performance on tests sensi-tive to impaired executive ability in schizophrenia, mania and well con-trols: Acute and subacute phases. Schizophr Res 26:127–137.
cKay AP, Tarbuck AF, Shapleske J, McKenna PJ (1995): Neuropsychologicalfunction in manic-depressive psychosis. Evidence for persistent deficitsin patients with chronic, severe illness. Br J Psychiatry 167:51–57.
eyer SE, Carlson GA, Wiggs EA, Martinez PE, Ronsaville DS, Klimes-Dougan B, etal (in press): A prospective study of the association among impaired execu-tive functioning, childhood attentional problems and the development ofbipolar disorder. Dev Psychopathol.
orice R (1990): Cognitive inflexibility and pre-frontal dysfunction in schizo-phrenia and mania. Br J Psychiatry 157:50 –54.
uechterlein KH, Asarnow RF, Subotnik KL, Fogelson DL, Ventura J, TorquatoR, Dawson ME (1998): Neurocognitive vulnerability factors for schizo-phrenia: Convergence across genetic risk studies and longitudinal trait-state studies. In: Lenzenweger MF, Dworkin RH, eds. Origins and Devel-opment of Schizophrenia: Advances in Experimental Psychopathology.Washington, D.C.: American Psychological Association, 299 –327.
uechterlein KH, Dawson ME (1984): A heuristic vulnerability/stress modelof schizophrenic episodes. Schizophr Bull 10:300 –312.
sterreith PA (1944): Les test de copie d’une figure complexe; contributionde la perception et de la memoire. (Test of copying a complex figure;contribution to the study of perception and memory.) Archives de Psy-chologie 30:206 –356.
aradiso S, Lamberty GJ, Garvey MJ, Robinson RG (1997): Cognitive impair-ment in the euthymic phase of chronic unipolar depression. J Nerv MentDis 185:748 –754.
rohaska ML, Stern RA, Nevels CT, Mason G, Prange AJ Jr (1996): The rela-tionship between thyroid status and neuropsychological performancein psychiatric outpatients on lithium. Neuropsychiatry Neuropsychol Be-hav Neurol 9:30 –34.
eitan RM, Wolfson D (1985): The Halstead-Reitan Neuropsychological TestBattery. Tucson: Neuropsychology Press.
ey A (1941): L’examen psychologique dans les cas d’encephalopathie trau-matique. (The psychological examination in cases of traumatic enceph-alopathy.) Archives de Psychologie 28:215–285.
ossi A, Arduini L, Daneluzzo E, Bustini M, Prosperini P, Stratta P (1900):Cognitive function in euthymic bipolar patients, stabilized schizo-phrenic patients and healthy controls. J Psychiatr Res 34:333–339.
achs GS, Baldassano CF, Truman CJ, Guille C (1900): Comorbidity of atten-tion deficit hyperactivity disorder with early- and late-onset bipolar dis-order. Am J Psychiatry 157:466 – 468.
apin LR, Berrettini WH, Nurnberger JI Jr, Rothblat LA (1987): Mediationalfactors underlying cognitive changes and laterality in affective illness.Biol Psychiatry 22:979 –986.
avard RJ, Rey AC, Post RM (1980): Halstead-Reitan Category Test in bipolarand unipolar affective disorders. Relationship to age and phase of illness.J Nerv Ment Dis 168:297–304.
aykin AJ, Gur RC, Gur RE, Mozley PD, Mozley LH, Resnick SM, et al (1991):
Neuropsychological function in schizophrenia. Selective impairment inmemory and learning. Arch Gen Psychiatry 48:618 – 624.Saykin AJ, Shtasel DL, Gur RE, Kester DB, Mozley LH, Stafiniak P, Gur RC(1994): Neuropsychological deficits in neuroleptic naive patients withfirst-episode schizophrenia. Arch Gen Psychiatry 51:124 –131.
Schweitzer JB, Faber TL, Grafton ST, Tune LE, Hoffman JM, Kilts CD (2000):Alterations in the functional anatomy of working memory in adult atten-tion deficit hyperactivity disorder. Am J Psychiatry 157:278 –280.
Seidman LJ, Biederman J, Monuteaux MC, Doyle AE, Faraone SV (2001):Learning disabilities and executive dysfunction in boys with attention-deficit/hyperactivity disorder. Neuropsychology 15:544 –556.
Seidman LJ, Kremen WS, Koren D, Faraone SV, Goldstein JM, Tsuang MT(2002): A comparative profile analysis of neuropsychological function-ing in patients with schizophrenia and bipolar psychoses. Schizophr Res53:31– 44.
Sharma V, Menon R, Carr TJ, Densmore M, Mazmanian D, Williamson PC(2003): An MRI study of subgenual prefrontal cortex in patients withfamilial and non-familial bipolar I disorder. J Affect Disord 77:167–171.
Strakowski SM, DelBello MP, Sax KW, Zimmerman ME, Shear PK, Hawkins JM,Larson ER (1999): Brain magnetic resonance imaging of structural abnor-malities in bipolar disorder. Arch Gen Psychiatry 56:254 –260.
Sweeney JA, Keilp JG, Haas GL, Hill J, Weiden PJ (1991): Relationships be-tween medication treatments and neuropsychological test perfor-mance in schizophrenia. Psychiatry Res 37:297–308.
Tam WC, Sewell KW, Deng HC (1998): Information processing in schizophre-nia and bipolar disorder: A discriminant analysis. J Nerv Ment Dis 186:597– 603.
Tham A, Engelbrektson K, Mathe AA, Johnson L, Olsson E, Aberg-Wistedt A(1997): Impaired neuropsychological performance in euthymic patientswith recurring mood disorders. J Clin Psychiatry 58:26 –29.
Tohen M, Waternaux CM, Tsuang MT, Hunt AT (1990): Four-year follow-up oftwenty-four first-episode manic patients. J Affect Disord 19:79 – 86.
van Gorp WG, Altshuler L, Theberge DC, Mintz J (1999): Declarative andprocedural memory in bipolar disorder. Biol Psychiatry 46:525–531.
van Gorp WG, Altshuler L, Theberge DC, Wilkins J, Dixon W (1998): Cognitiveimpairment in euthymic bipolar patients with and without prior alcoholdependence. A preliminary study. Arch Gen Psychiatry 55:41– 46.
Ventura J, Green MF, Shaner A, Liberman RP (1993): Training and qualityassurance on the BPRS: “The Drift Busters”. Int J Methods Psychiatr Res3:221–244.
Ventura J, Liberman RP, Green MF, Shaner A, Mintz J (1998): Training andquality assurance with the Structured Clinical Interview for DSM-IV(SCID-I/P). Psychiatry Res 79:163–173.
Verdoux H, Magnin E, Bourgeois M (1995): Neuroleptic effects on neuro-psychological test performance in schizophrenia. Schizophr Res 14:133–139.
Waber DP, Holmes JM. (1986): Assessing children’s memory productions ofthe Rey-Osterrieth Complex Figure. J Clin Exp Neuropsychol 8:563–580.
Waddington JL, Brown K, O’Neill J, McKeon P, Kinsella A (1989): Cognitiveimpairment, clinical course and treatment history in out-patients withbipolar affective disorder: Relationship to tardive dyskinesia. PsycholMed 19:897–902.
Wechsler D (1981): Manual for the Wechsler Adult Intelligence Scale-Revised.New York: The Psychological Corporation.
Weinberger DR, Berman KF, Zec RF (1986): Physiologic dysfunction of dor-solateral prefrontal cortex in schizophrenia. I. Regional cerebral bloodflow evidence. Arch Gen Psychiatry 43:114 –124.
Wilder-Willis KE, Sax KW, Rosenberg HL, Fleck DE, Shear PK, Strakowski SM(2001): Persistent attentional dysfunction in remitted bipolar disorder.Bipolar Disord 3:58 – 62.
Wolfe J, Granholm E, Butters N, Saunders E, Janowsky D (1987): Verbalmemory deficits associated with major affective disorders: A compari-son of unipolar and bipolar patients. J Affect Disord 13:83–92.
Wozniak J, Biederman J, Mundy E, Mennin D, Faraone SV (1995): A pilotfamily study of childhood-onset mania. J Am Acad Child Adolesc Psychia-try 34:1577–1583.
Young RC, Biggs JT, Ziegler VE, Meyer DA (1978): A rating scale for mania:Reliability, validity and sensitivity. Br J Psychiatry 133:429 – 435.
Zihl J, Gron G, Brunnauer A (1998): Cognitive deficits in schizophrenia andaffective disorders: Evidence for a final common pathway disorder. ActaPsychiatr Scand 97:351–357.
Zubieta JK, Huguelet P, O’Neil RL, Giordani BJ (1901): Cognitive function in
euthymic bipolar I disorder. Psychiatry Res 102:9 –20.www.elsevier.com/locate/biopsych
Related Documents











