الرحمن بسم ال الرحيمCNS EXAMINATION Dr. M.H.F. Neurosurgeon

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

بسم ال الرحمن الرحيم
CNS EXAMINATIONDr. M.H.F.Neurosurgeon

2
Consciousness: 1.State(awakefullness): RAS (lower pons to thalamus).2.Content(awareness): cerebral cortex &thalamus.
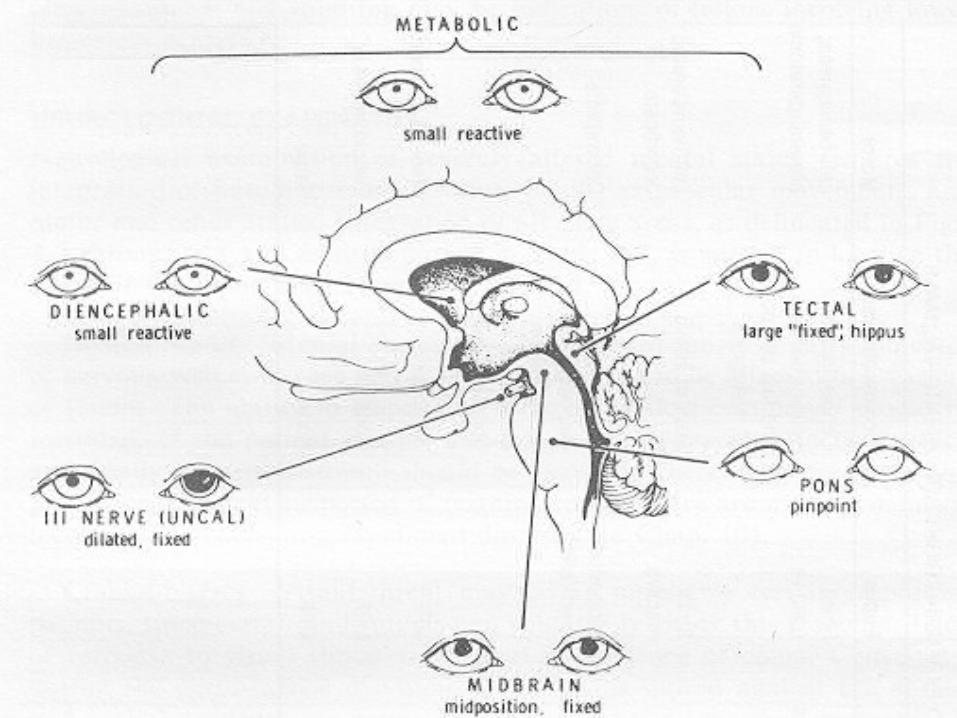
•Evaluation of comatose pt.: a.GCS. b.pupils, fundi & ocular movements c.FND d.resp.pattern.
3
4
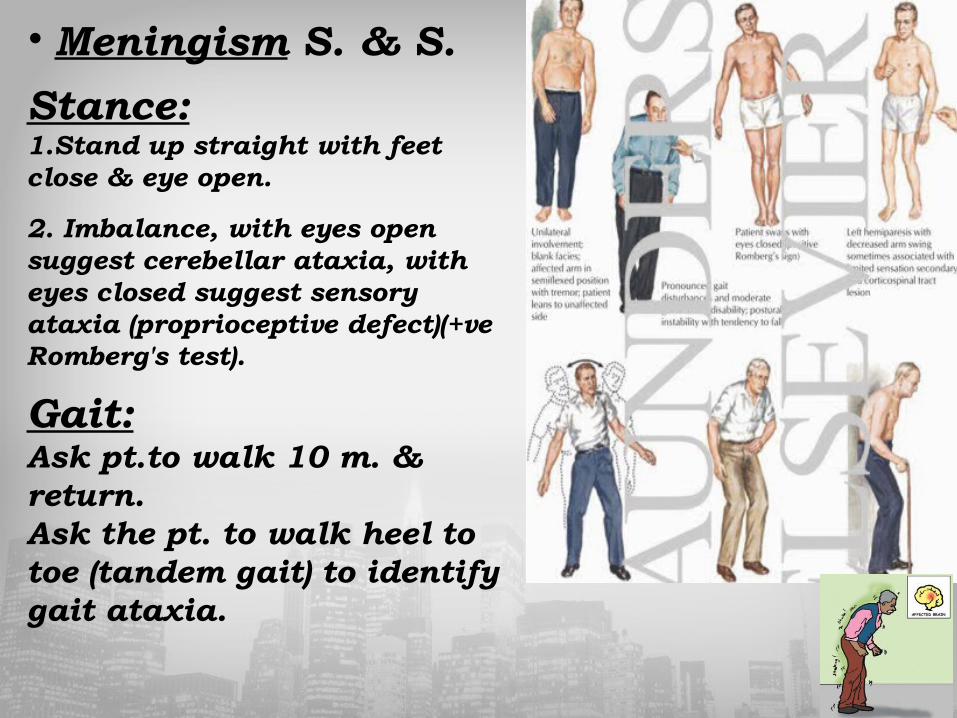
• Meningism S. & S.
Stance:1.Stand up straight with feet close & eye open.
2. Imbalance, with eyes open suggest cerebellar ataxia, with eyes closed suggest sensory ataxia (proprioceptive defect)(+ve Romberg's test).
Gait:Ask pt.to walk 10 m. & return.Ask the pt. to walk heel to toe (tandem gait) to identify gait ataxia.
5
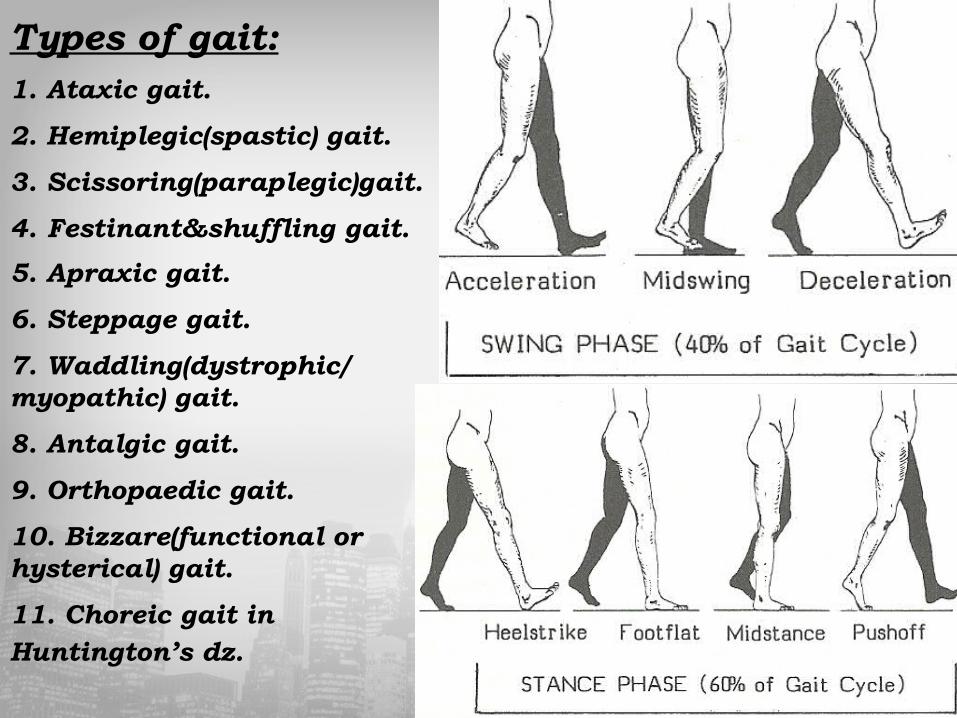
Types of gait:1. Ataxic gait.
2. Hemiplegic(spastic) gait.
3. Scissoring(paraplegic)gait.
4. Festinant&shuffling gait.
5. Apraxic gait.
6. Steppage gait.
7. Waddling(dystrophic/myopathic) gait.
8. Antalgic gait.
9. Orthopaedic gait.
10. Bizzare(functional or hysterical) gait.
11. Choreic gait in Huntington’s dz.

6
Speech difficulties:Speech difficulties:
1. Mutism: bilateral medial frontal lobe lesion→no attempt to speak.
2. Dysphonia: impairment of voice production from vocal cord &/or larynx dz.
3. Dysarthria: disarticulation.
4. Dysphasia: disturb of understand &/or expression of words.

7
Examination for Speech disorder: Dysarthria & Dysphonia:
1. Listen to pt. volume, rhythm & clarity of speech.
2. Ask pt. to repeat: (yellow lorry) for lingual sounds & (baby hippopotamus) for lip (labial) sounds. Then a tongue twister (e.g. the Leith Police dismisseth us).
3. Ask pt.to count steadly to 30to asses ms. Fatique.
4. Ask the pt. to cough & say Aaah to test dysphonia.

• Causes of Dysarthria & Dysphonia:1. Spastic (pseudobulbar) dysarth: bilat.UMNL. (+ve jaw jerk)
2. Bulbar dysarthria: LMNL, pt. has ligual sounds/nasal speech.
3. Extrapyramidal dysarthria: d.to parkinsonism, monotonous speech.
4. Cerebellar (ataxic) dysarthria:slow,slurred speech.
5. Myasthenia gravis speech (fatiguable speech).
6. Dysphonia c.by laryngitis/vagus n. damage, cough bovine.
9
Dysphasia:
assess fluency, comprehension, repetition, naming, dyslexia & agraphia.
1. Listen for fluency, paraphasia (incorrect words) & neologisms (nonsense words).
2. naming.
3. asses comprehention: give simple 3 command e.g. pick up the piece of paper, fold it in half & place it under the book (without visual clues).
4. Repeat a simple sentence (repetition).
5. Ask the pt. to read passage (lyxia).
6. Ask the pt. to write a sentence(graphia).

10
naming repetition comprehention
Fluency
+/-ve -ve +ve -ve Broca's Aphasia
-ve -ve -ve +ve Wernicke's Aphasia:
+ve -ve +ve +ve Conduction Aphasia
-ve +ve +ve +ve Anomic Aphasia
-ve -ve -ve -ve Global Aphasia
-ve +ve -ve +ve Transcorticalsensory
-/+ve +ve +ve -ve Transcortical motor
-ve +ve -ve -ve Mixed transcortical
11
Mental function:
1. Appearance & behaviour: self neglect, Depression, Dementia, Drinking & Drug abuse. Behavior (frontalism), flat affect, emotional liability & hysteria.
2. Mood: Depression, Schizophrenia blunting affect.
3.Vegetative symptoms: (wt.loss, sleep disturb, appetite, constipation & libido).
4. Delusion, Illusion & hallucination: Delusion: firmly held belief not altered by rational argument.
Illusion: Miss interpretation of external stimuli.
Hallucination: Perception without external stimuli,

12
Mental assessement:1. Attention & Orientation:
2. Memory:
3. Calculation:
4. Abstract:
5. Spatial orientation: constructional apraxia.
6. Visual & body perception (Agnosia)
Prosopagnosia: Failure to recognize faces Hemineglect: One side ignorance Asomatognosia: Failure to recognize left hand. Anosagnosia: Unawareness of affected side weakness. Asteriognosis: Sensory agnosia. Agraphaesthesia: Failure to recognize shape. Gerstman's syndrome = Acalculia, finger agnosia, Rt.-Lt.disorientation & agraphesthesia.
7. Apraxia: a.Ideational apraxia b.Ideomotor apraxia c. Dressing apraxia d.Constructional apraxia
13

14
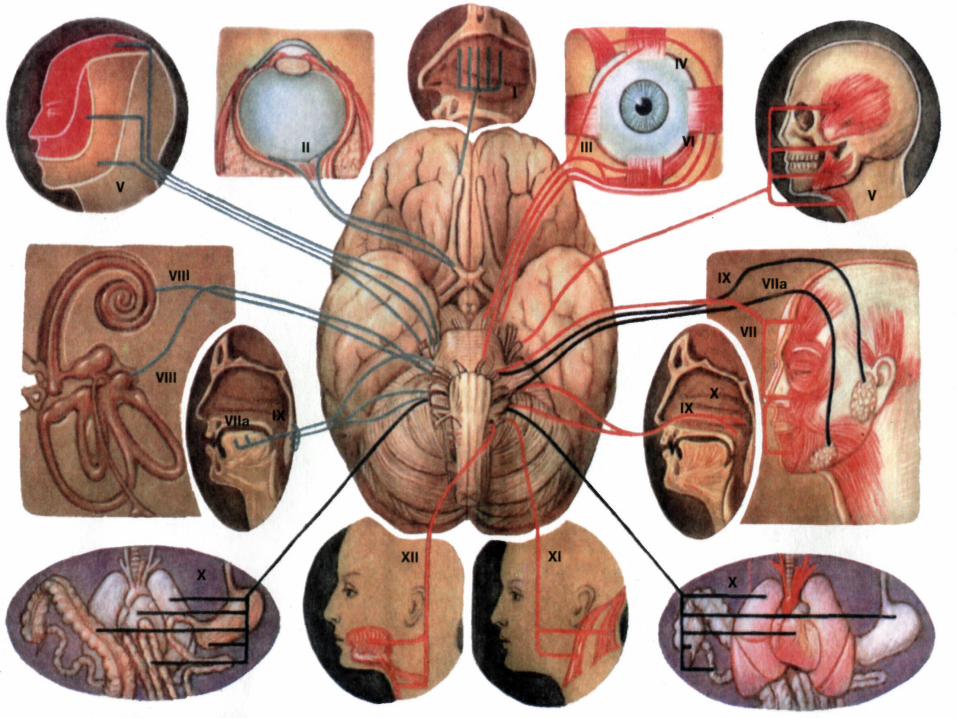
Cranial nerves examination:I. Olfactory nerve: Close eye & shut one nostril & use coffee, chocolate, soap, & ask pt. to sniff.
Causes of Anosmia:Bilateral anosmia caused by common cold.Unilateral anosmia caused by HI & basal skull #, or brain tumour. Parkinson & Huntington dz.
Paraosmia is perceiving of pleasant odour as unpleasant & may occur in HI, sinus infection or drug.

15
Optic nerve: a. Inspection: ptosis, proptosis, enophthalamus & lid retraction.
b. Pupil: size, shape, symmetry, light/accomodation Rx.
c.Visual acuity:Snellen chart.
d.Visual field: perimetry & confrontation test.
e.Colour vision: Ishihara test plates.
f.Fundoscopy:1.optic disc: papilloedema, papillitis & colloid bodies (drusen).
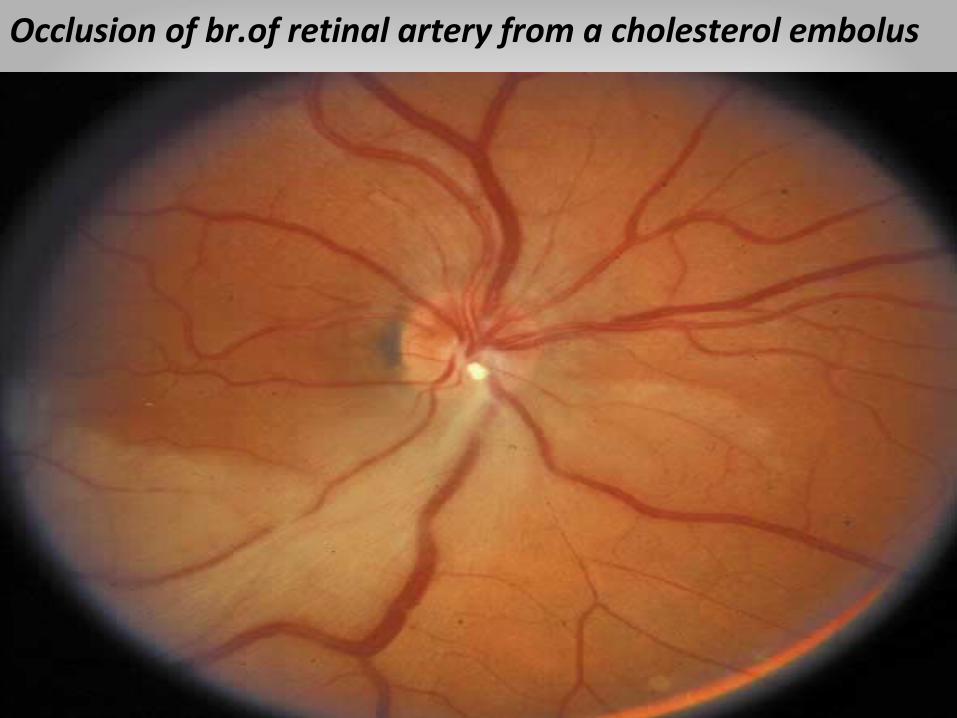
2. bld vess: A-V nipping, neovascularization & cholesterol embolous.
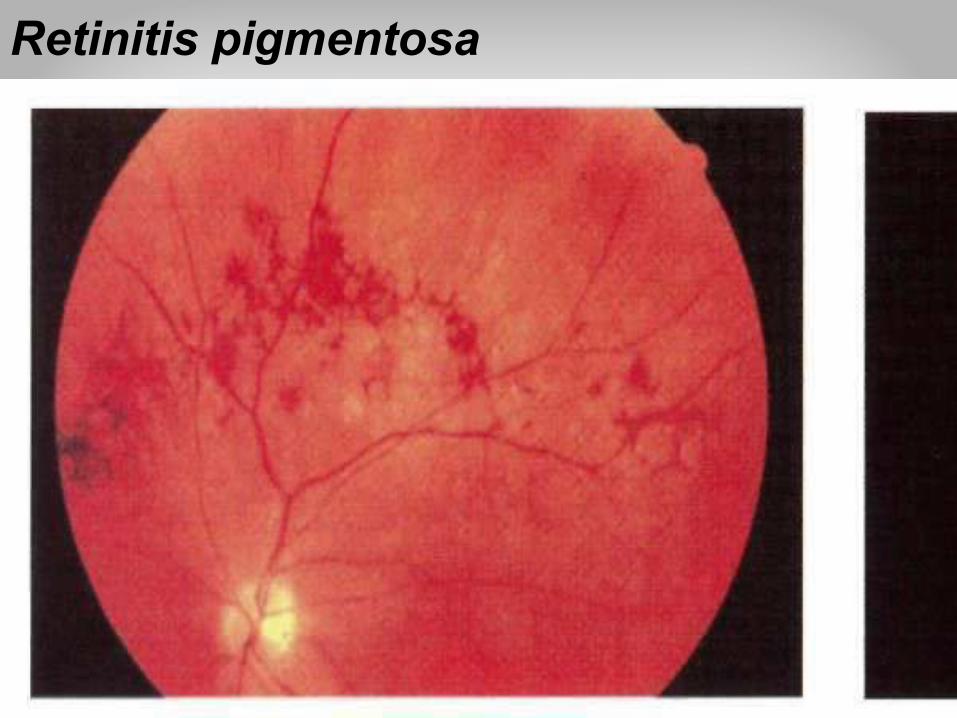
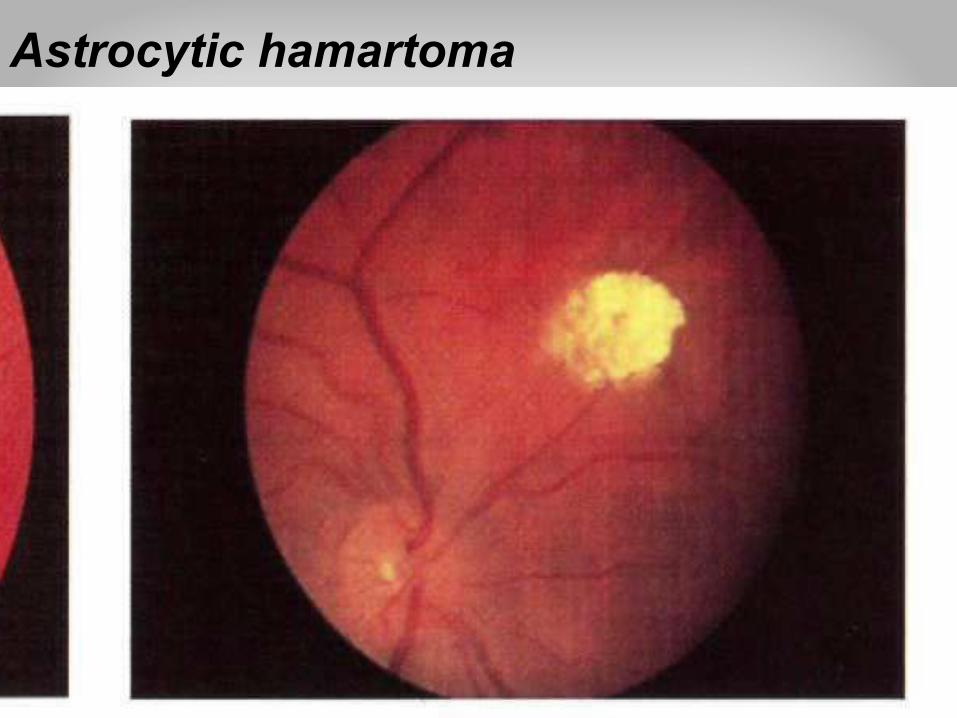
3. Retina: Red lesion: dot & blot hrg, flame hrg., sub hyaloid hrg. White lesion: hard exudates, cotton wall (soft) exudates. Black lesion: moles/melanoma, laser burn, Retinitis pigmentosa.

16
Papilloedema
17
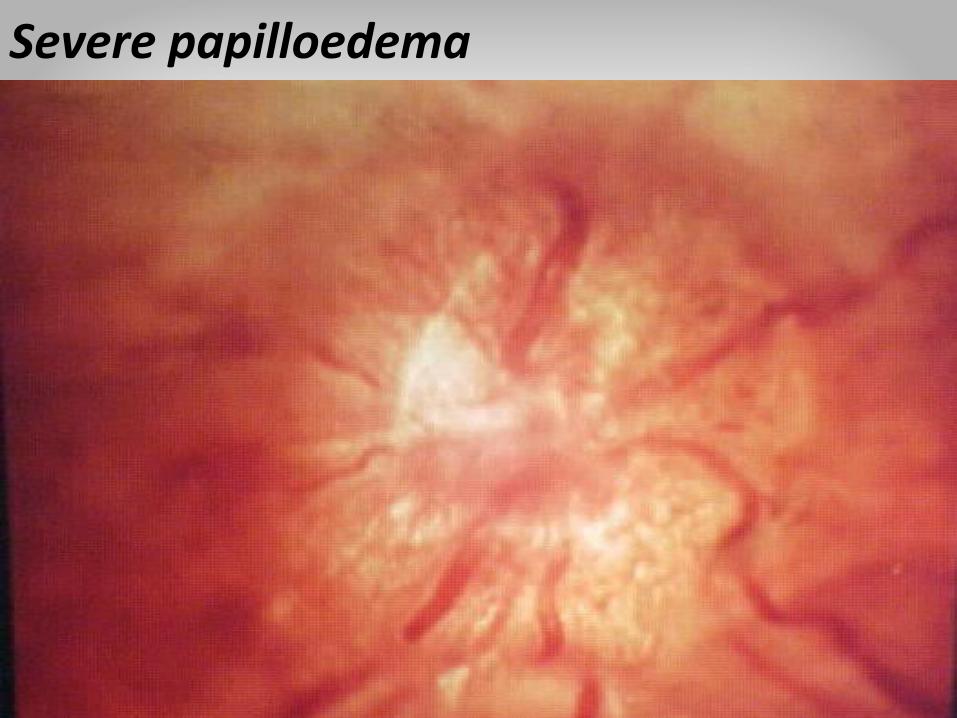
Severe papilloedema
18
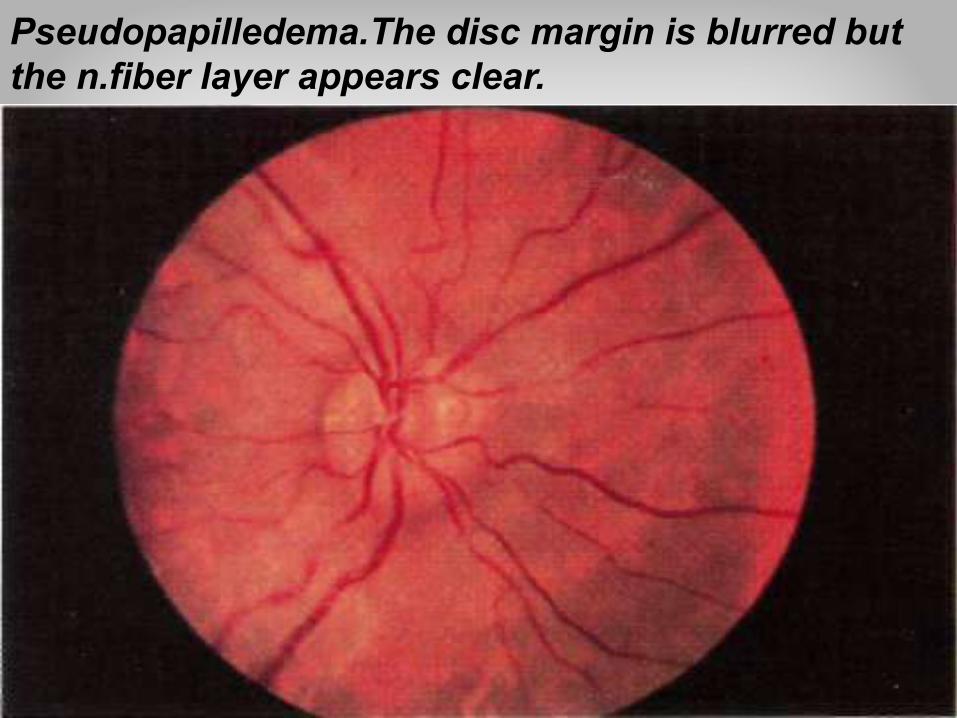
Pseudopapilledema.The disc margin is blurred but the n.fiber layer appears clear.

19
Optic disc drusen

20
Anterior optic neuritis in right eye

21
Anterior ischaemic optic neuropathy in right eye
22
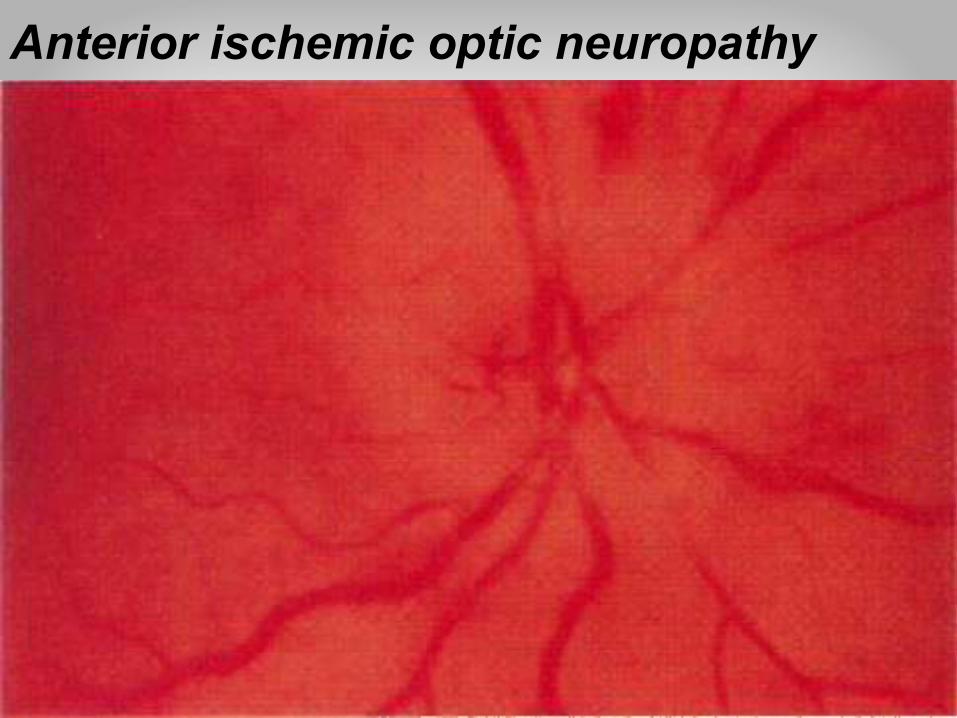
Anterior ischemic optic neuropathy

23
Neuroretinitis

24
Optic disc swelling&optociliary shunt vessels
25
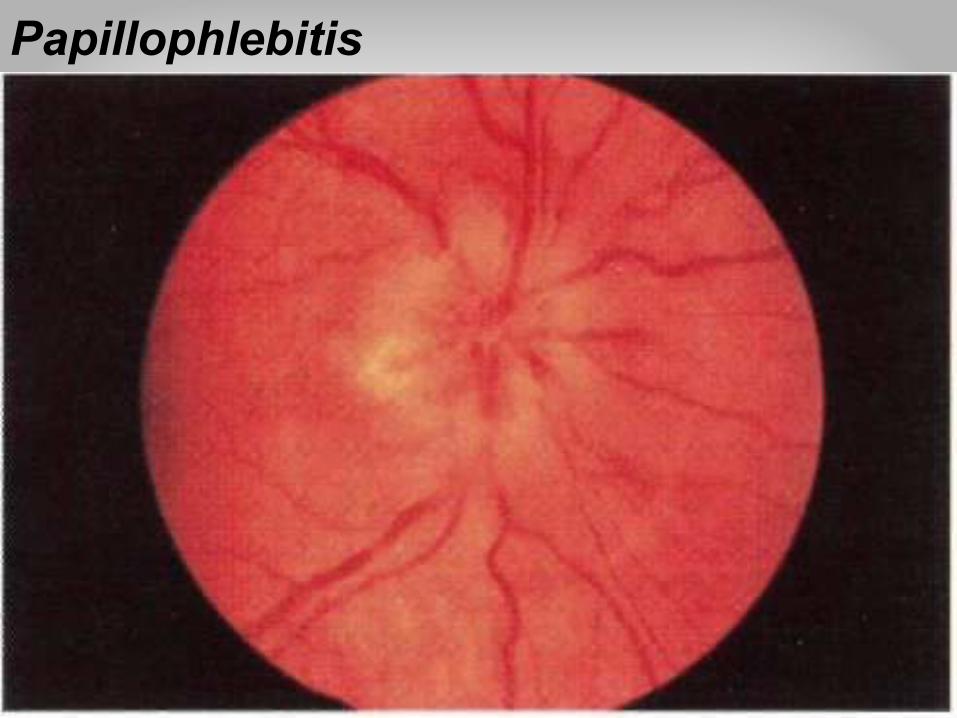
Papillophlebitis

26
Optic disc edema&hyperemia(central retinal v.occlusion)
27
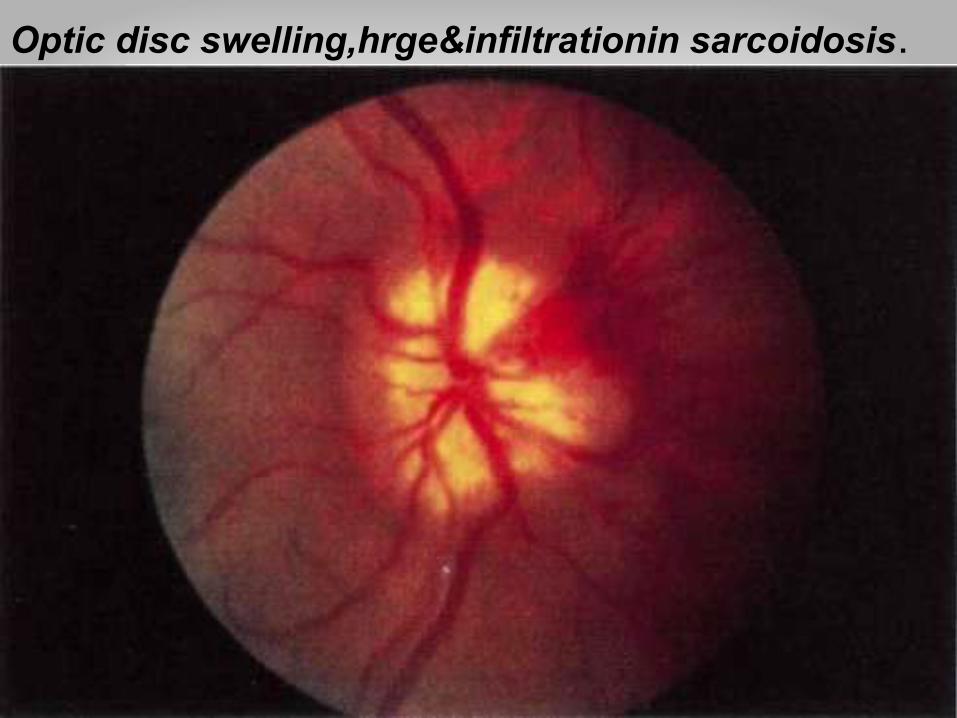
Optic disc swelling,hrge&infiltrationin sarcoidosis.

28
Hypcremic disc with telangiectatic vess(Leber's optic npathy)

29
Swollen optic disc in early papilledema
30
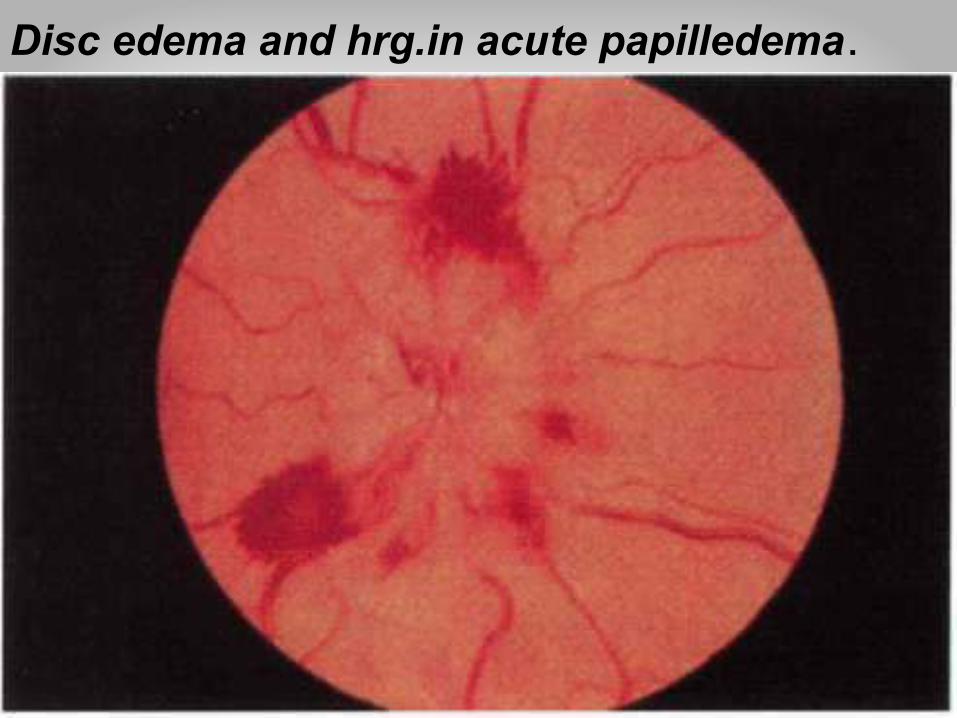
Disc edema and hrg.in acute papilledema.
31
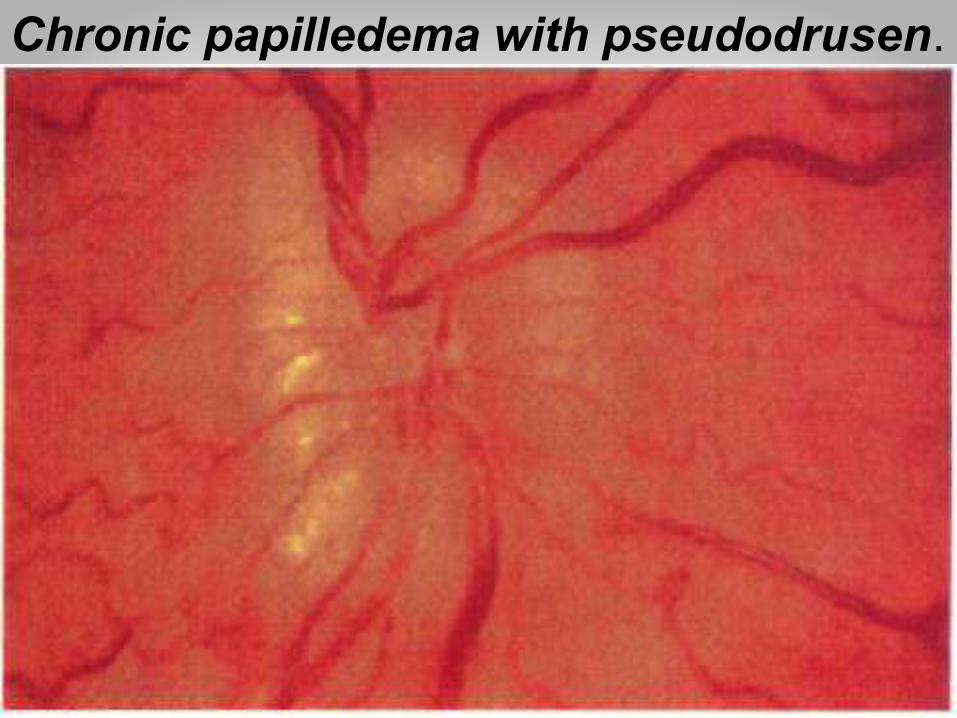
Chronic papilledema with pseudodrusen.
32
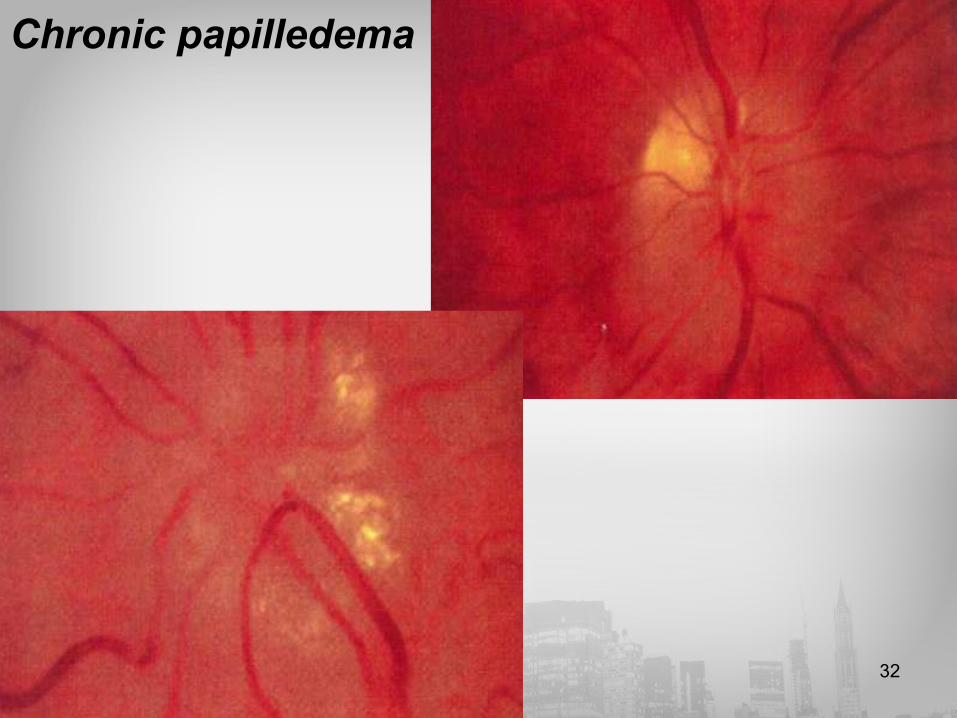
Chronic papilledema

33
Swollen optic disc in malignant hypertension.

34
Diabetic papillopathy
35
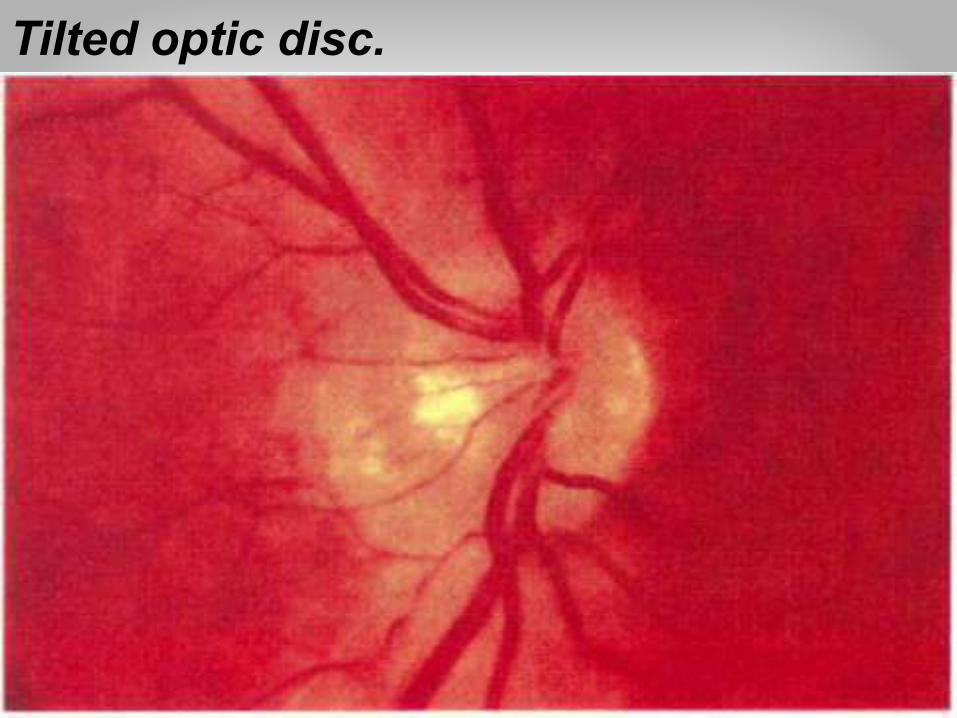
Tilted optic disc.
36
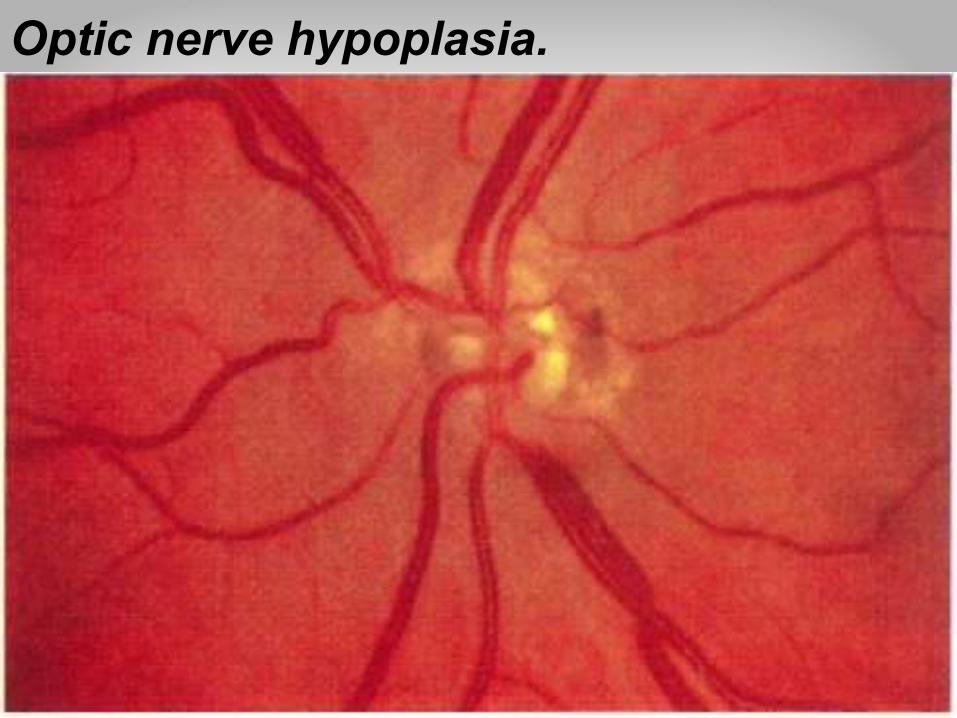
Optic nerve hypoplasia.
37
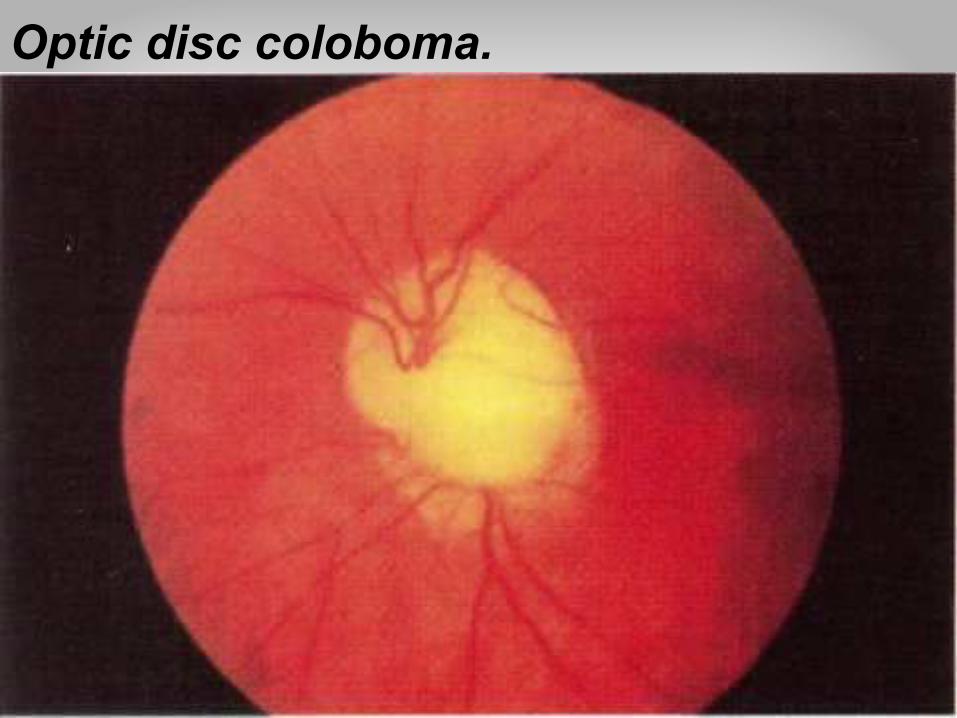
Optic disc coloboma.

38
Central retinal artery occlusion

39
Central retinal artery thrombosis
40
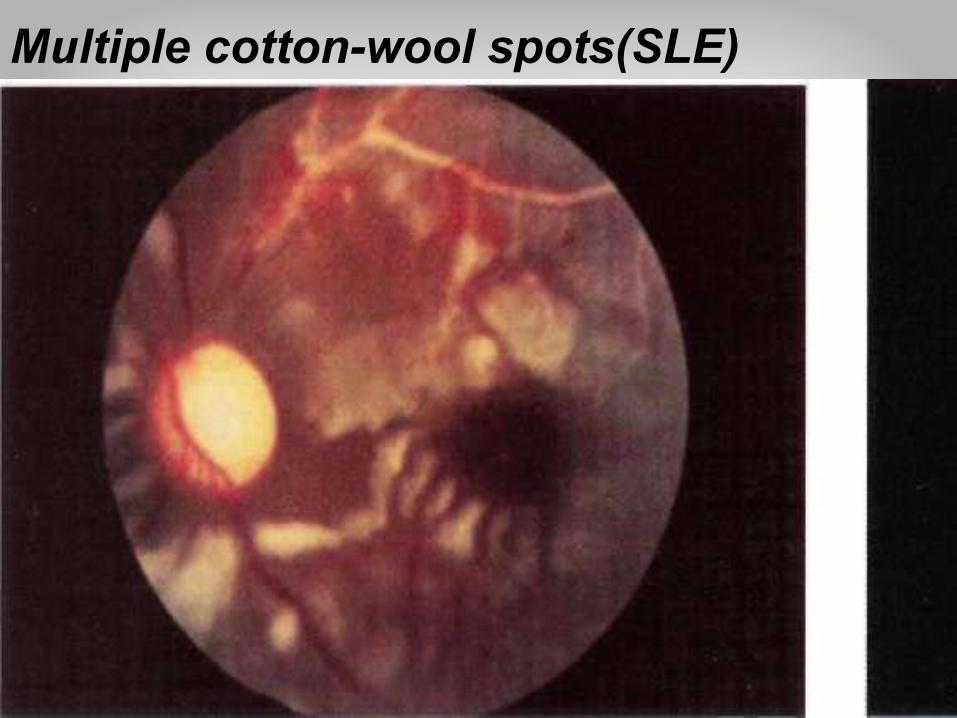
Multiple cotton-wool spots(SLE)

41
Central retinal vein occlt
42
Retinitis pigmentosa

43
Retinitis Pegmentosa
44
Astrocytic hamartoma
45
Occlusion of br.of retinal artery from a cholesterol embolus
46
If severely impaired VA (Snellen chart is unuseful), count fingers. then light percept.
Poor VA with cataracts, ant. optic chamber (glaucoma), retina (macular degen.) or optic neuritis. ↓ VA (central VF defect) c. by cataract.
Macular & Optic n.lesion → central scotoma.
Peripheral retina lesion → ring scotoma.
Optic disc lesion → horizontal or arcuate scotoma.
Optic n. damage from photoreceptors to lat.geniculate body → impaired red-green colour vision.
Congenital red green blindness (X-linked recessive) affect 7% of male.
Papilloedema→enlarged blind spot due to ↑ ICP.
Functional (hysterical) VF loss is bilateral VF constriction (tubular constriction). Bilat. retinal disorder(retinitis pigmentosa)→funnel constriction.

47

48
III,IV&VI Exam:
1.Look for head turn or tilt.
2.pupil, light & accommodation reflux.
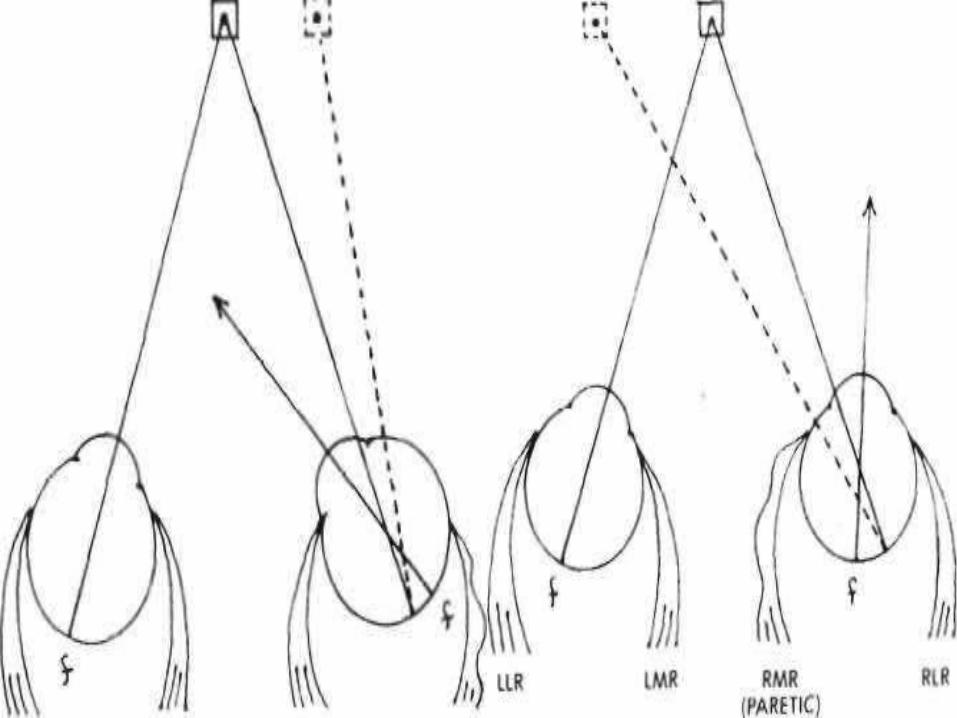
3.Look gaze direction, squint or diplopia.
4. If squint &/or diplopia, do cover test, squint eye; absence of outer image mean covered eye is paralytic.
5. Look for nystagmus direction & position.
4 types of eye movement:1. Saccadic: rapid (frontal lobe).2. Pursuit: slow (occipital lobe).3. Vistibular-positional (vistibulo-ocular): cerebellar & vestibular nuclei.4. Convergence: midbrain.

49Internal and external ophthalmoplegia
50
51
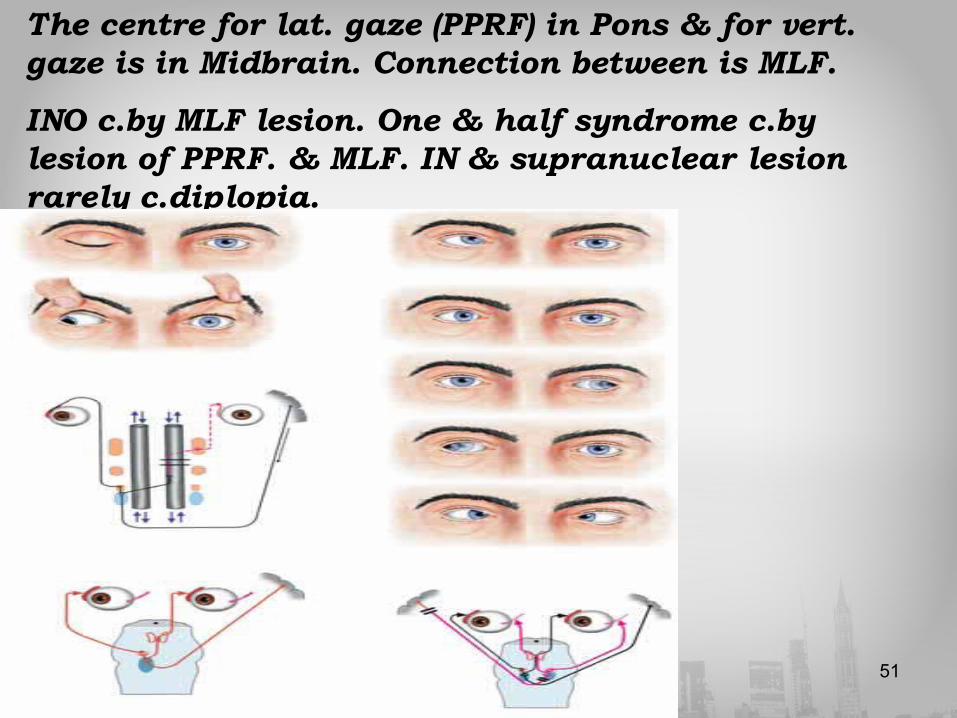
The centre for lat. gaze (PPRF) in Pons & for vert. gaze is in Midbrain. Connection between is MLF.
INO c.by MLF lesion. One & half syndrome c.by lesion of PPRF. & MLF. IN & supranuclear lesion rarely c.diplopia.
52
Squint either Paralytic or incomitant (acquired or congenital) or non paralytic or concomitant squint.
In acquired paralytic squint diplopia is greatest direction of paretic ms., in cong. long standing paralytic squint, the head is tilted to minimize diplopia.
Concomitant squint are same in all direction of gaze, it is not associated with diplopia, because this symptom is suppressed centrally in young child→ amblyopia (lazy eye).

53
Vn.Exam:a. Sensory: ophthalmic, maxillary & mandibular division.Light touch,superficial pain & touch sensation in the ant. 2/3 of tongue.
b. Motor: inspect mastication ms., clench the teeth & feel masseter ms. & open jaw against resistance
c. Corneal reflux & jaw jerk.

54
VII n.Exam:
a. Inspect face asymmetry, blinking, eye closure, spontaneous /involuntary movement. b. wrinkle forehead, bare teeth, shut eye tightly & blow out cheecks. c. Taste from ant. 2/3 of tongue. d. Schirmer’s test. e. corneal reflux.
UMN VII weakness spares frontalis so pt. can wrinkle brow.
LMNVIIweakness involves forehead ms. & pt can’t wrinkle brow & has unilat.
Hyperacusis & loss of taste. Facial diplegia, or bilat. LMN VII weakness is seen in such conditions as GBS or sarcoidosis.
N.B.: Bell’s phenomena: eyes turn upwards on attempts closure which indicates VII n. palsy. Whistle-smile sign (no smile when whistle).

55
Lesions of VII n.:
a.Distal to junction with corda tympani=LMNL.
b.Distal to n.to stapedius=above+ tongue ant.2/3taste loss(ageusia).
c.Distal to lacrimal br.GSPN=above +hyperacusis.
d.Proximal to GSPN.=above+loss of lacrimation.
56
ExamVIIIn.:
Rinne’s & Weber’s test. Check gross hearing in each ear by rubbing fingers about 3 inches from ear, with contralat. ear covered.
If hearing in one ear impaired, perform Rinne & Weber tests.
With conductive hearing loss, from middle ear dz or obstruction of EAM with wax, BC > AC & Weber test will lateralize to the deaf ear.
With SN hearing loss AC better than BC & Weber test will lateralize to good ear.
57
Vistibular nerve Exam:
a. Gait & turning test.
b.Nystagmus (Dix-Hallpikes test) In normal individual, no nystagmus. In peripheral lesion, vertigo & nystagmus after delay of 5-15 second, decline as the position maintained & fatique if the test repeated (fatiquable rotary nystagmus with delay). In central lesion, no latency, no fatique & less prominent vertigo.
c.Oculocephalic test (Doll’s eye reflux).
d.Oculovistibular reflux: In coma, tonic movement occurs towards irrigated ear. In canal paresis, reduced response to cold & warm stimuli.
58
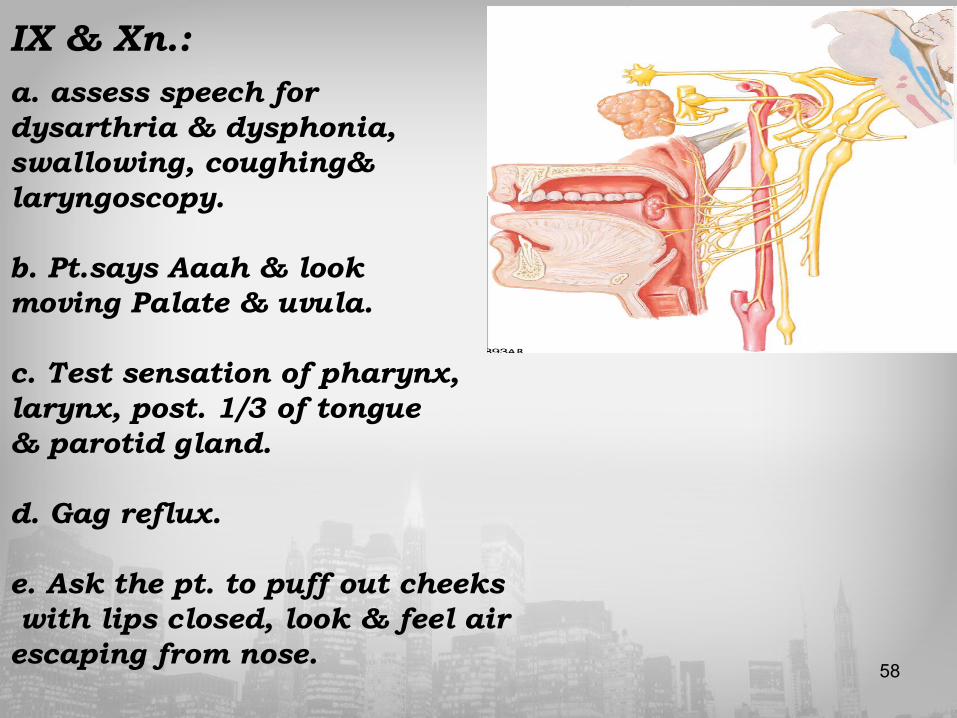
IX & Xn.:
a. assess speech for dysarthria & dysphonia, swallowing, coughing& laryngoscopy. b. Pt.says Aaah & look moving Palate & uvula. c. Test sensation of pharynx, larynx, post. 1/3 of tongue & parotid gland. d. Gag reflux. e. Ask the pt. to puff out cheeks with lips closed, look & feel air escaping from nose.
59
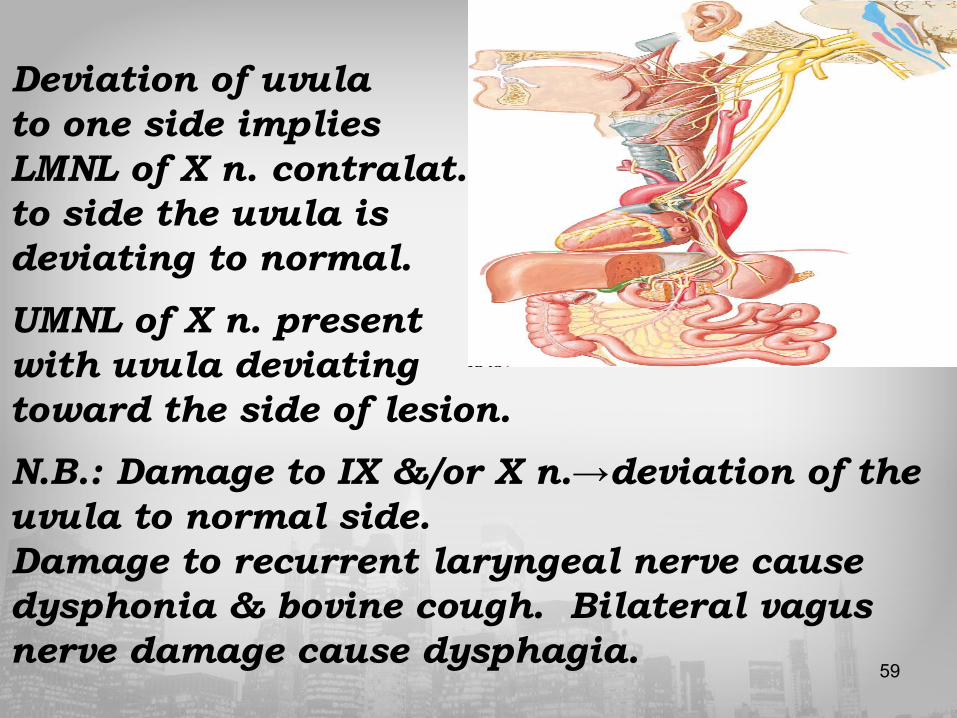
Deviation of uvula to one side implies LMNL of X n. contralat.to side the uvula is deviating to normal.
UMNL of X n. present with uvula deviating toward the side of lesion.
N.B.: Damage to IX &/or X n.→deviation of the uvula to normal side. Damage to recurrent laryngeal nerve cause dysphonia & bovine cough. Bilateral vagus nerve damage cause dysphagia.

60
XI n. Exam: a. Inspect scm & trapezius for wasting & fasciculation.
b. Elevate&turn head against resistance.
c. Shrug shoulder against resistance.
N.B.: ipsilat.cerebral 1/2 supply contralat. Trapezius & ipsilateral scm. ms. Weakness of both ms.on same side means peripheral accessory n. palsy (LMNL.).
Weakness of ipsilateral st.cl.m & contralat. trapezius means UMNL. ipsilateraly. Unilateral delayed shoulder shrug means contralat. UMNL.Bilateral weakness & wasting of scm.ms. means myopathy (dystrophia myotonica & Mgravis). Head tilt means cervical dystonia.

61
XII Exam.:a. Open the mouth & inspect the tongue for wasting, fasciculation & involuntary movement. b. Protrude tongue & look for deviation ipsilateraly.
c. Move tongue & press against cheek to assess power.
d. Assess speech & say yellow lorry.

62
N.B.:LMNL. unilaterally c. deviation of tongue to affected side. LMNL. bilaterally c. wasting & shrunken tongue&in severe weakness there is dysarthria & dysphagia. UMNL. Bilaterally (pseudobulbar palsy) cause spastic conical tongue & result from vascular dz., MND. & MS. Resting tongue tremor=parkinson dz. Orolingual dyskinesia is drug induced (antiparkinson & neuroleptics).
63
Motor system exam: a.Weakness b.Hyperreflexia. c.Hypertonia d.Spasticit
Examination:1. Inspection. 2. Tone. 3. Power & movement.4. coordination. 5. Refluxes.

64
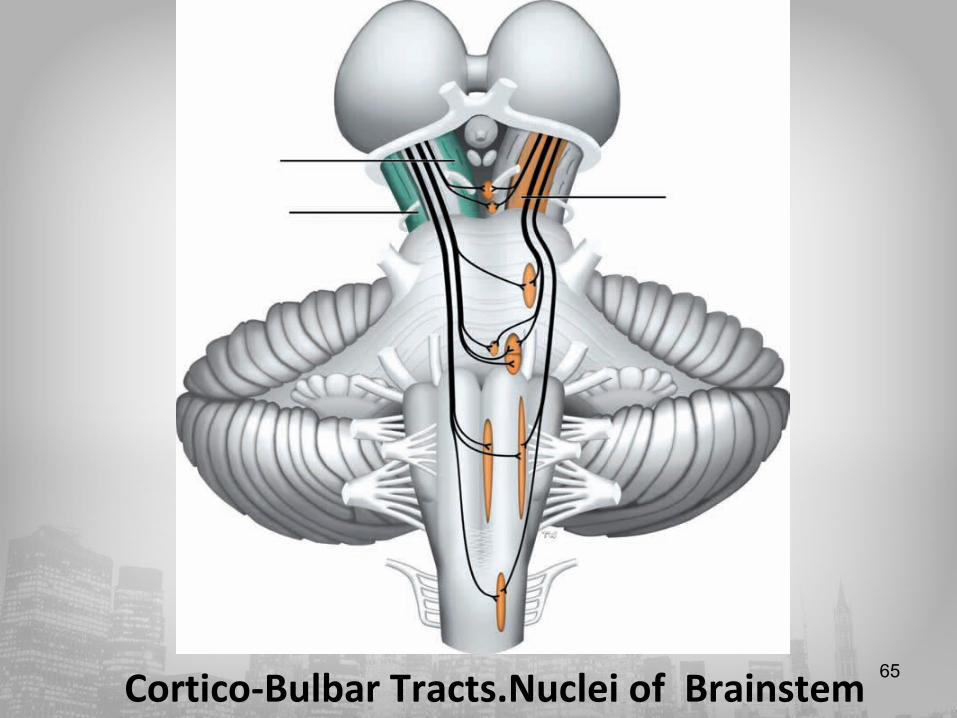
65 Cortico-Bulbar Tracts.Nuclei of Brainstem

66
Ms. weakness in: UMNL., LMNL., ms. dz. (wasting, hypotonia & hyporeflexia), NMJ, fatique weakness (normal/hypotonia & normo refluxia) & functional weakness (normal tone & refluxes & no wasting).
In ms. disorder, ms. Wasting & myopathy u. occure proximaly except in dystonia myotonica myopathy occurs distally. Hyperreflexia = UMNL., Hyporflexia = LMNL. & myopathy. In Holmis Adies syndrome myotonic pupil, there is loss of deep tendon reflexes. In Hypothyroidism, normal refluxes with delayed (slow) relaxation. +ve Hoffman’s = hypertonia & UMNL. In cerebellar damage, pendular reflux. Inverted reflux = tapping biceps tendon → triceps contraction indicate combined spinal cord&root pathology.
67
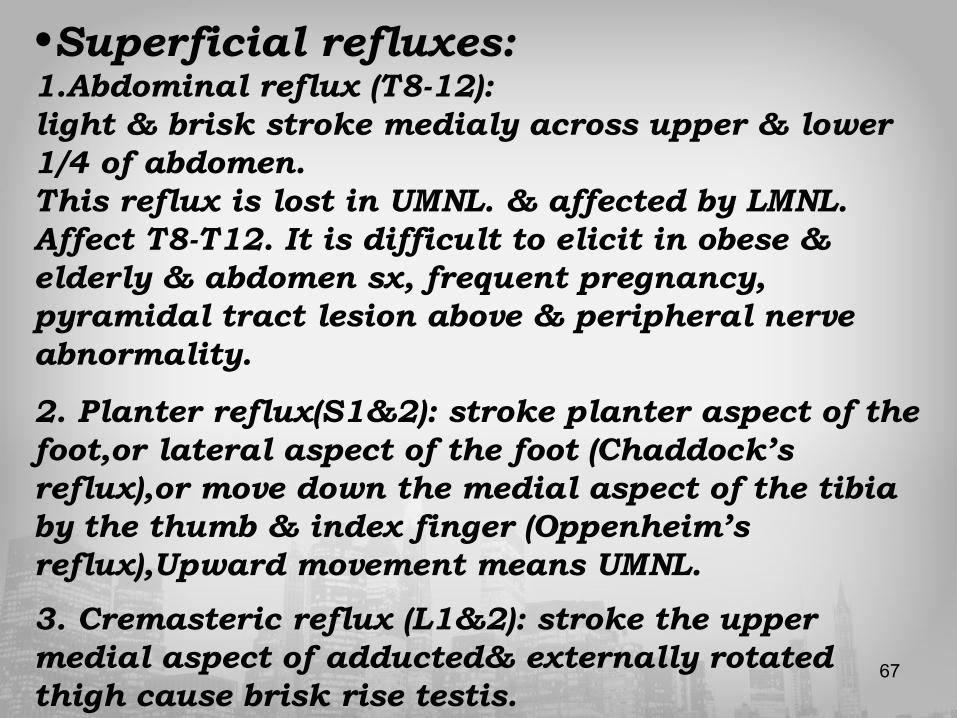
•Superficial refluxes:1.Abdominal reflux (T8-12):light & brisk stroke medialy across upper & lower 1/4 of abdomen.This reflux is lost in UMNL. & affected by LMNL. Affect T8-T12. It is difficult to elicit in obese & elderly & abdomen sx, frequent pregnancy, pyramidal tract lesion above & peripheral nerve abnormality.
2. Planter reflux(S1&2): stroke planter aspect of the foot,or lateral aspect of the foot (Chaddock’s reflux),or move down the medial aspect of the tibia by the thumb & index finger (Oppenheim’s reflux),Upward movement means UMNL.
3. Cremasteric reflux (L1&2): stroke the upper medial aspect of adducted& externally rotated thigh cause brisk rise testis.
68
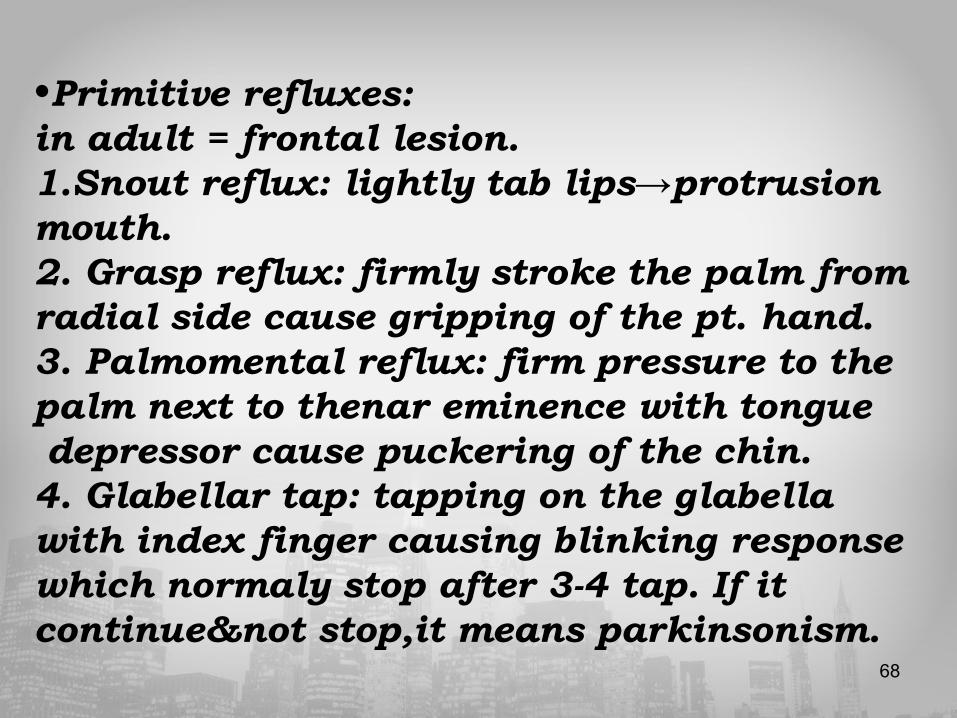
•Primitive refluxes:in adult = frontal lesion. 1.Snout reflux: lightly tab lips→protrusion mouth.2. Grasp reflux: firmly stroke the palm from radial side cause gripping of the pt. hand.3. Palmomental reflux: firm pressure to the palm next to thenar eminence with tongue depressor cause puckering of the chin.4. Glabellar tap: tapping on the glabella with index finger causing blinking response which normaly stop after 3-4 tap. If it continue¬ stop,it means parkinsonism.
69
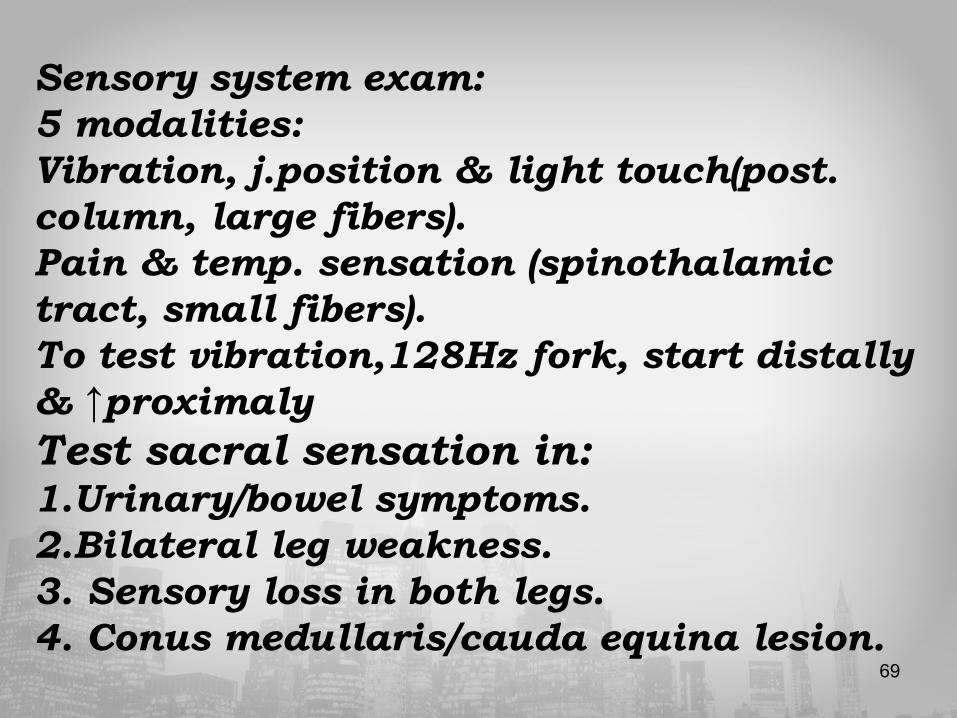
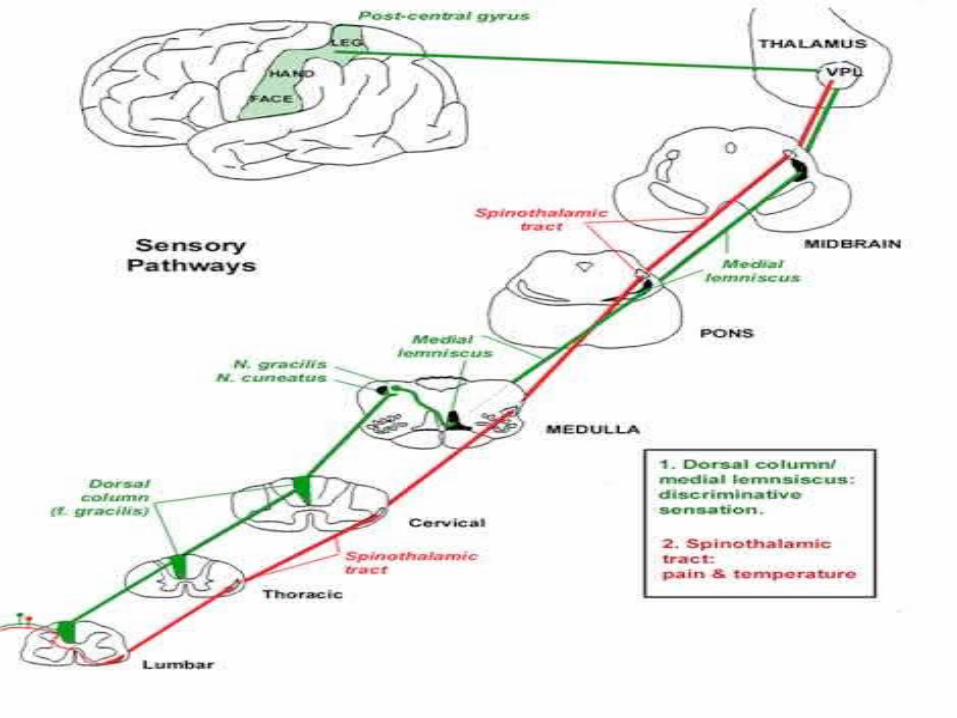
Sensory system exam:5 modalities:Vibration, j.position & light touch(post. column, large fibers). Pain & temp. sensation (spinothalamic tract, small fibers).To test vibration,128Hz fork, start distally & ↑proximalyTest sacral sensation in:1.Urinary/bowel symptoms. 2.Bilateral leg weakness. 3. Sensory loss in both legs. 4. Conus medullaris/cauda equina lesion.
70
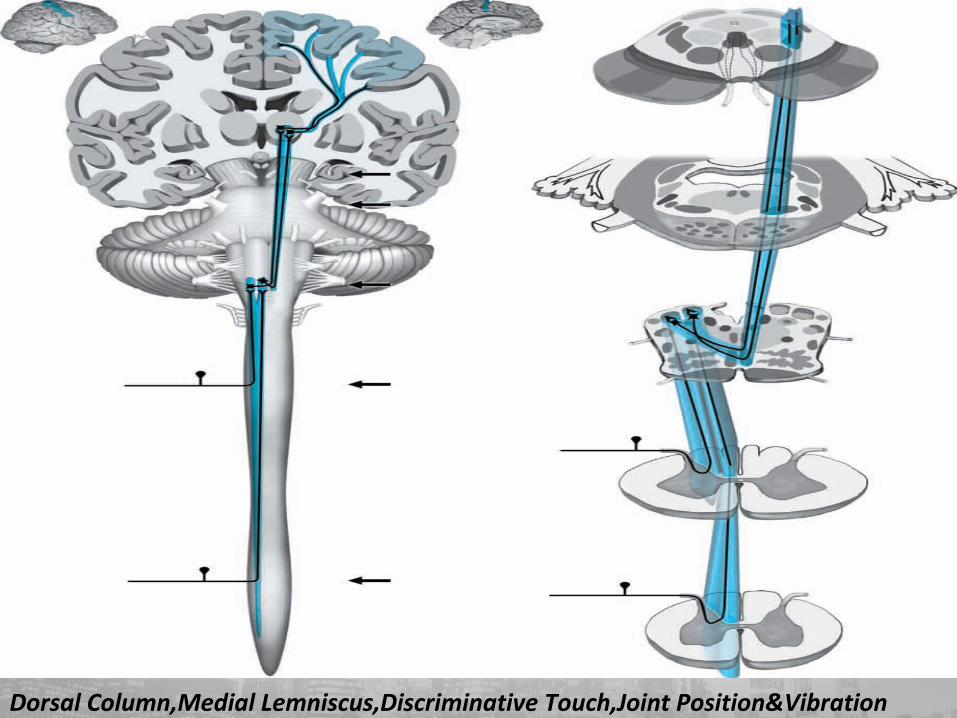
Dorsal Column,Medial Lemniscus,Discriminative Touch,Joint Position&Vibration
71
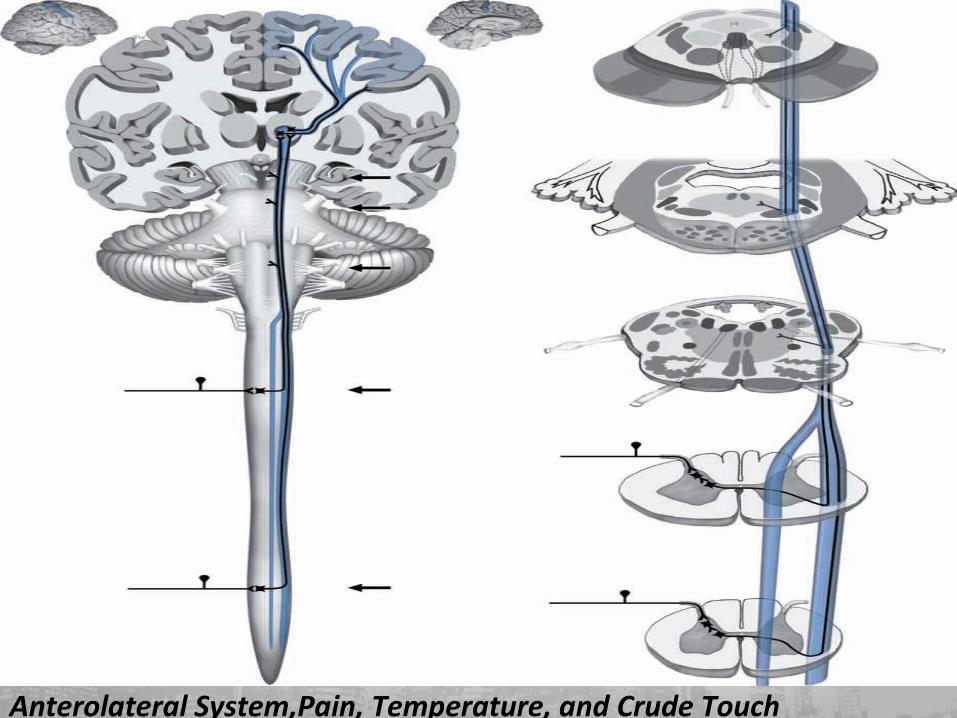
Anterolateral System— Pain, Temperature, and Crude Touch
Anterolateral System,Pain, Temperature, and Crude Touch

72V Pathways,Discriminative Touch,Pain &Temperature
73

74
Examine:1.Light touch. 2.Superficial pain. 3.Deep pain. 4.Temperature. 5.Vibration. 6.Joint position sensation. 7.2point discrimination. 8.Point localization. 9.Steriognosis &graphesthesia. 10. Sensory inattention: recognize one side,u.rt,when both stimulated, parietal lobe lesion.
• Grades of sensory recovery:S0 = Absence of all modalities of sensation.S1 = only deep cutaneous pain.S2 = some superfiscial cutaneous pain.S3 = superfiscial cutaneous pain& tactile sensation with disappear of previous over response.S3+=as S3 with recovery of 2 point discrimination.S4 = normal sensation.
76
Extrapyramidal System Exam:hypokinetic or hyperkinetic.�Hypokinetic disorders are: rigidity, bradykinesia & tremor (Parkinson’s syndrome). There is ↑ flexor tone → stooped posture with head, neck, trunk, arms& legs flexed. Tremor& slowness of movement & cogwheel rigidity. The pt has festinating gait&no motor weakness.� Hyperkinetic disorders are excessive motor activity(chorea,athetosis,dystonia or hemiballismus).
77
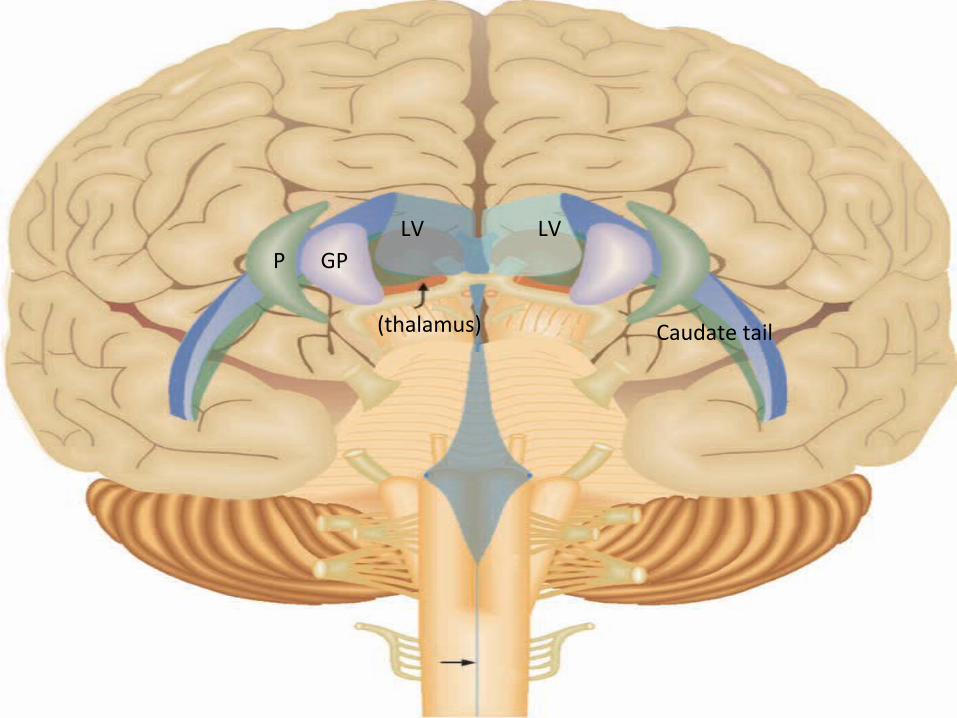
LV LVGP
(thalamus)
P
Caudate tail

78Rubro-Spinal Tract

79Pontine (Medial) Reticulo-Spinal Tract
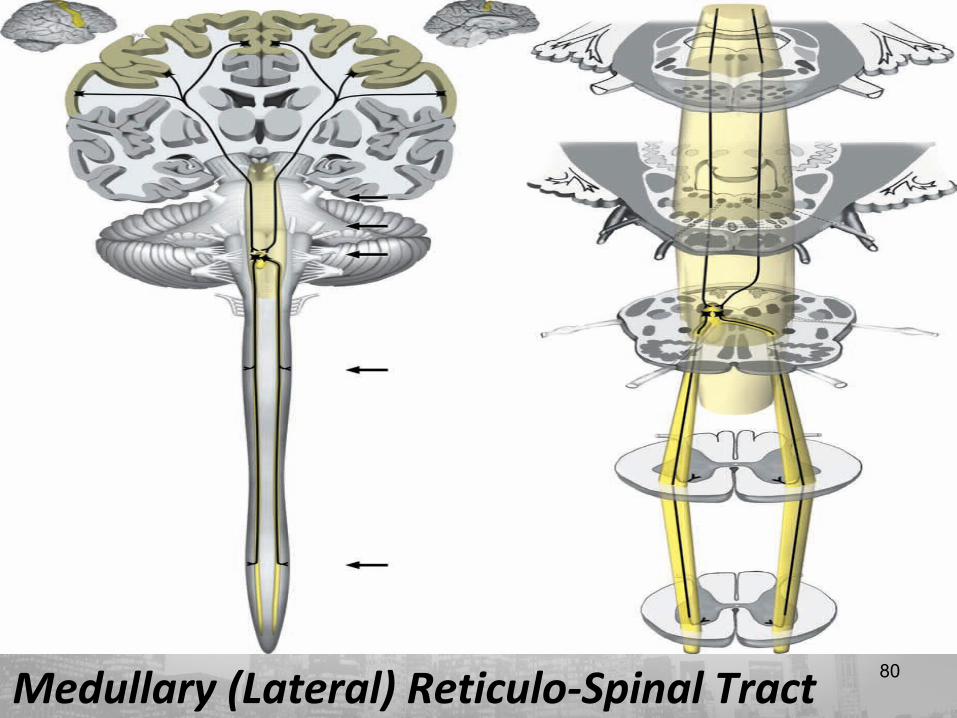
80Medullary (Lateral) Reticulo-Spinal Tract

81Lateral Vestibulo-Spinal Tract
82
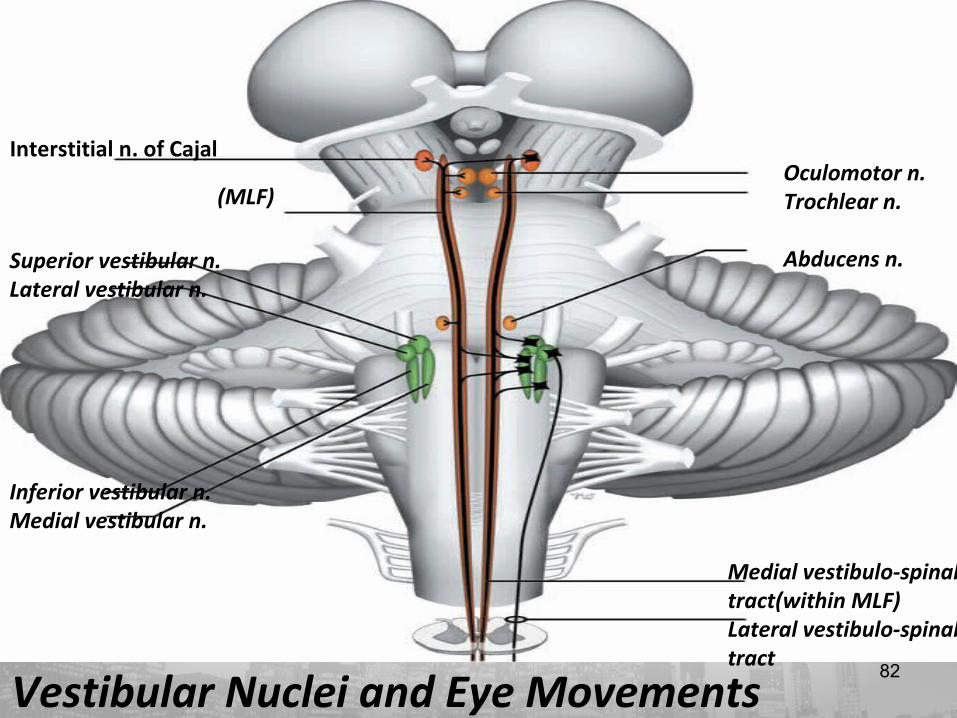
Vestibular Nuclei and Eye Movements
Interstitial n. of Cajal
(MLF)
Superior vestibular n.Lateral vestibular n.
Inferior vestibular n.Medial vestibular n.
Oculomotor n.Trochlear n.
Abducens n.
Medial vestibulo-spinal tract(within MLF)Lateral vestibulo-spinal tract
83
Cerebellar signs: DANISHAssesement of cerebellar function,ms.weakness, proprioceptive loss & extrapyramidal dysfunction. We should test for:1. Stance & Gait. 2. Speech (dysarthria). 3. Nystagmus.4. Tone (hypotonia) & Refluxes(pendular). 5. Rebound phenomina.6. Finger-nose or Heel-Shin test, dysmetria & dyssynergia.7. Intentional tremor. 8. Dysdiadochokinesis.

84
Examination of brain stem death: 1.Confirm cause of irreversible brain stem damage.2. Exclude reversible causes of coma(hypothermia, hypoglycaemia,drug overdose). 3. Confirm ventilator dependency(disconnection cause rise of arterial PCO2 >7kpa with no spontaneous respiration.4. The pupil is fixed&dilated with no light reflux.5. Corneal reflux is absent.6. Oculovestibular reflux absent with no nystagmus.7. Gag reflux is absent.8. The pt.examined by 2 experienced clinician on 2 occasions,24 hrs apart.
Related Documents