1 Presented by Tracey Anderson, MSN, CNRN, FNP-BC, ACNP-BC Neurosurgery Nurse Practitioner UCHealth Medical Group – Brain & Spine Complete advanced assessment of patients with neurologic complaint Identify appropriate diagnostic tests based on presenting symptoms Identify those presentations requiring emergent referral Review NPH & Back Pain as seen in Primary Care

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Presented by
Tracey Anderson, MSN, CNRN, FNP-BC, ACNP-BCNeurosurgery Nurse Practitioner
UCHealth Medical Group – Brain & Spine
� Complete advanced assessment of patients
with neurologic complaint
� Identify appropriate diagnostic tests based
on presenting symptoms
� Identify those presentations requiring
emergent referral
� Review NPH & Back Pain as seen in Primary
Care
2
� Onset
� Progression� Previous similar events
� Aggravated/Relieved by…
� Others with similar symptoms� General medical problems
� Recent surgeries/illnesses
� Medications
� Level of Consciousness
� Memory/Cognition � Cranial Nerves
� Motor Exam
� Sensory Exam� Vital Signs
� Orientation� Memory – Short Term� Judgment� Attention Span� Concentration� Memory – Long Term� Current Events
� Assesses frontal lobe

3
Area How To Hints
Orientation Person: First, Last
Place: Location, City, State
Time: Year, month, day
of week, date
Reason for visit?
Avoid yes/no questions
and don’t give hints
Memory
Short Term
3 Items – repeat in 3-5 minutes
Always use same 3
things
Area How To
Judgment “What would you do if you were in a crowded theater and saw a
fire?”
Attention Span
Concentration
Note if you must frequently regain their attention
Area How To Hints
Memory
Long Term
Who is current president and who were the last 3 before him?
Know them yourself!
Current Events
Ask what significant event/holiday has
recently happened
4
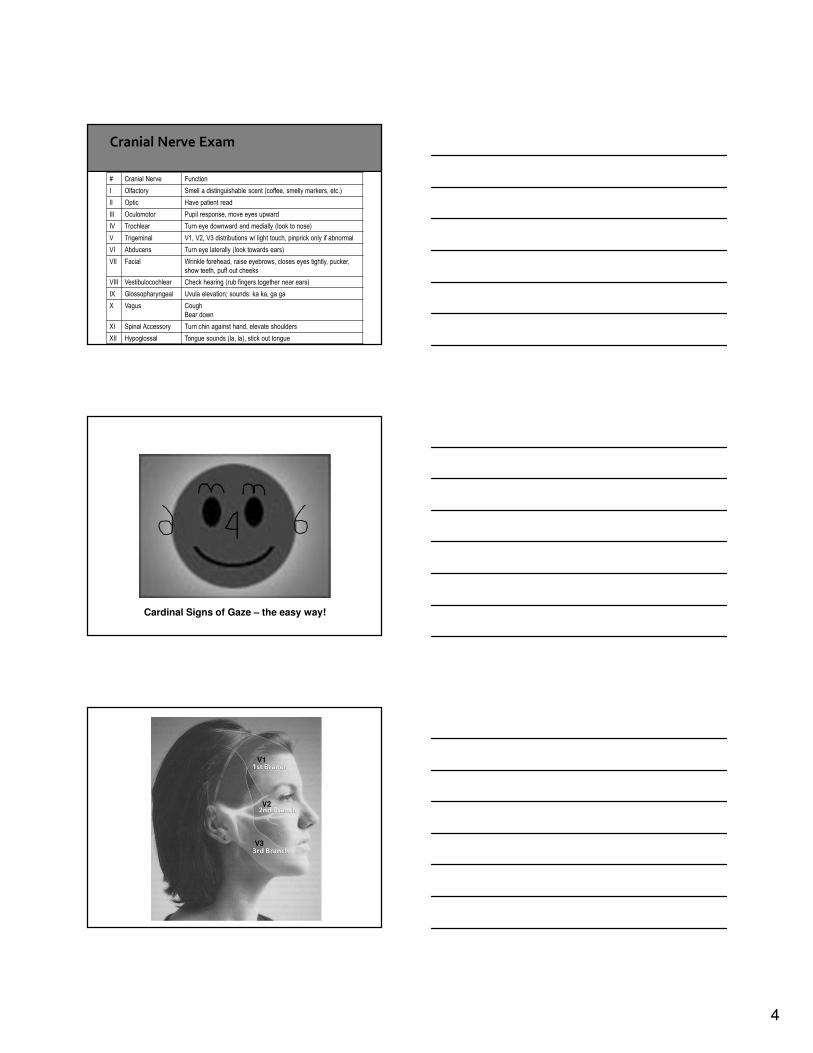
# Cranial Nerve Function
I Olfactory Smell a distinguishable scent (coffee, smelly markers, etc.)
II Optic Have patient read
III Oculomotor Pupil response, move eyes upward
IV Trochlear Turn eye downward and medially (look to nose)
V Trigeminal V1, V2, V3 distributions w/ light touch, pinprick only if abnormal
VI Abducens Turn eye laterally (look towards ears)
VII Facial Wrinkle forehead, raise eyebrows, closes eyes tightly, pucker,
show teeth, puff out cheeks
VIII Vestibulocochlear Check hearing (rub fingers together near ears)
IX Glossopharyngeal Uvula elevation; sounds: ka ka, ga ga
X Vagus Cough
Bear down
XI Spinal Accessory Turn chin against hand, elevate shoulders
XII Hypoglossal Tongue sounds (la, la), stick out tongue
Cardinal Signs of Gaze – the easy way!
V1
V2
V3

5
# Cranial Nerve Function
I Olfactory Smell a distinguishable scent (coffee, smelly markers, etc.)
II Optic Have patient read
III Oculomotor Pupil response, move eyes upward
IV Trochlear Turn eye downward and medially (look to nose)
V Trigeminal V1, V2, V3 distributions w/ light touch, pinprick only if abnormal
VI Abducens Turn eye laterally (look towards ears)
VII Facial Wrinkle forehead, raise eyebrows, closes eyes tightly, pucker,
show teeth, puff out cheeks
VIII Vestibulocochlear Check hearing (rub fingers together near ears)
IX Glossopharyngeal Uvula elevation; sounds: ka ka, ga ga
X Vagus Cough
Bear down
XI Spinal Accessory Turn chin against hand, elevate shoulders
XII Hypoglossal Tongue sounds (la, la), stick out tongue
Facing Cranial Nerve Assessment, Barbara Bolek, American Nurse Today, November 2006.
© American Association of Neuroscience Nurses 2006 15
Alzheimer’s stage 4
(not able to place 2
hands)
Alzheimer’s stage 5
(lose both hands)
Alzheimer’s stage 6
OR
Ischemic Vascular Dementia-note the paucity of hands
Micrographia
Frontal Lobe Dementia
Lewy Body Dementia
CLOCK DRAWING*
6
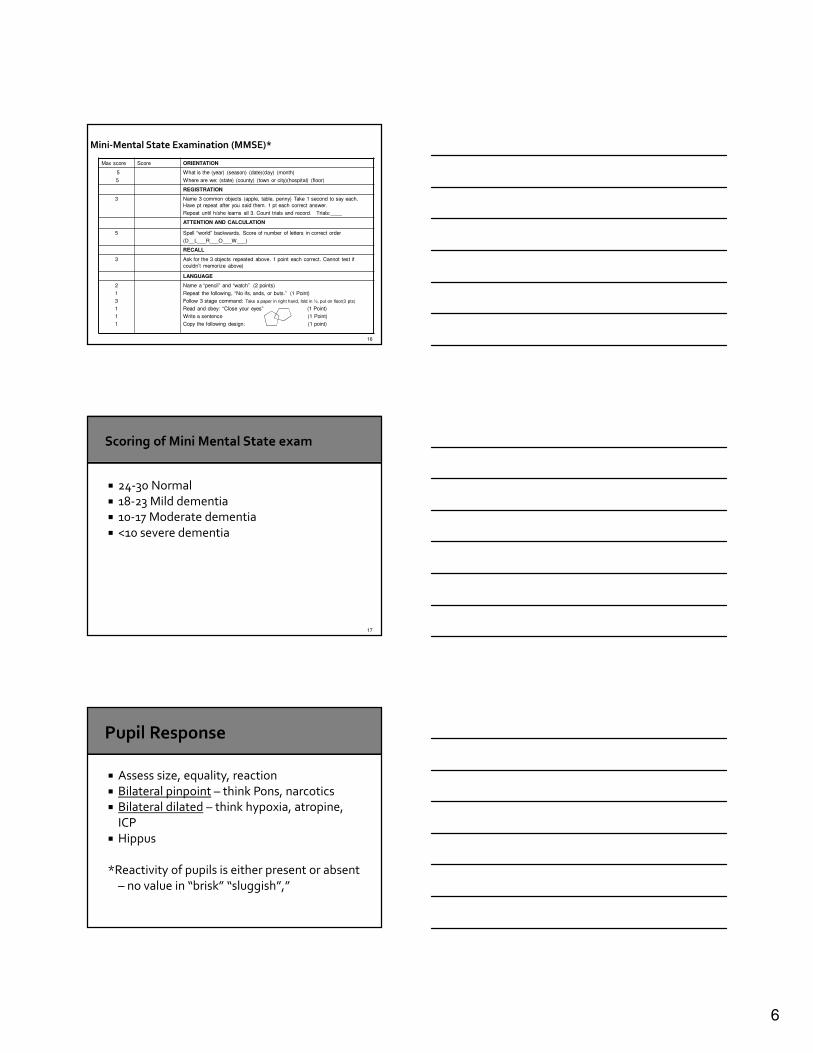
16
Max score Score ORIENTATION
5
5
What is the (year) (season) (date)(day) (month)
Where are we: (state) (county) (town or city)(hospital) (floor)
REGISTRATION
3 Name 3 common objects (apple, table, penny) Take 1 second to say each.
Have pt repeat after you said them. 1 pt each correct answer.
Repeat until h/she learns all 3. Count trials and record. Trials:____
ATTENTION AND CALCULATION
5 Spell “world” backwards. Score of number of letters in correct order
(D__L___R___O___W___)
RECALL
3 Ask for the 3 objects repeated above. 1 point each correct. Cannot test if
couldn’t memorize above)
LANGUAGE
2
1
3
1
1
1
Name a “pencil” and “watch” (2 points)
Repeat the following, “No ifs, ands, or buts.” (1 Point)
Follow 3 stage command: Take a paper in right hand, fold in ½, put on floor(3 pts)
Read and obey: “Close your eyes” (1 Point)
Write a sentence (1 Point)
Copy the following design: (1 point)
17
� 24-30 Normal
� 18-23 Mild dementia� 10-17 Moderate dementia
� <10 severe dementia
� Assess size, equality, reaction
� Bilateral pinpoint – think Pons, narcotics� Bilateral dilated – think hypoxia, atropine,
ICP
� Hippus
*Reactivity of pupils is either present or absent
– no value in “brisk” “sluggish”,”
7
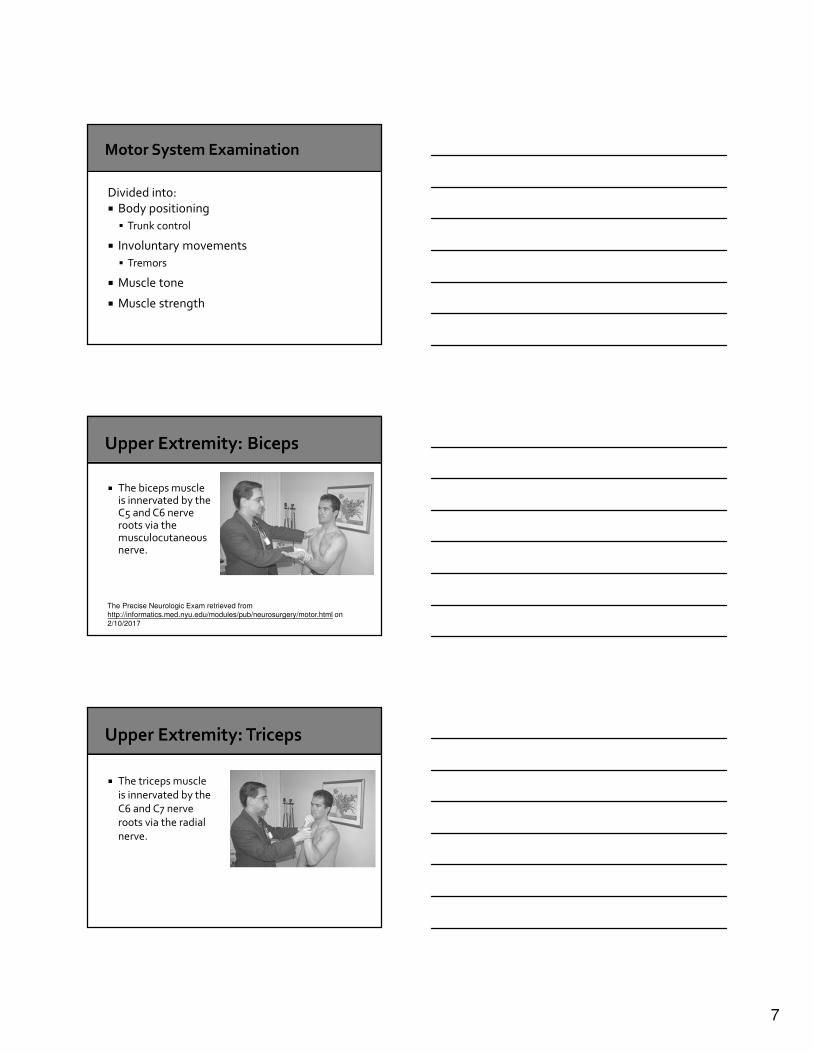
Divided into:
� Body positioning
� Trunk control
� Involuntary movements
� Tremors
� Muscle tone
� Muscle strength
� The biceps muscle is innervated by the C5 and C6 nerve roots via the musculocutaneous nerve.
The Precise Neurologic Exam retrieved from http://informatics.med.nyu.edu/modules/pub/neurosurgery/motor.html on
2/10/2017
� The triceps muscle
is innervated by the C6 and C7 nerve roots via the radial
nerve.

8
� The deltoid muscle
is innervated by the C5 nerve root via the axillary nerve.
� Indicates an upper motor neuron lesion
� May be first indicator of pending change
� The wrist extensors are innervated by C6 and C7 nerve roots via the radial nerve.
� The radial nerve is the "great extensor" of the arm: it innervates all the extensor muscles in the upper and lower arm.

9
� Finger flexion is
innervated by the C8 nerve root via the median nerve.
� Tests forearm flexors and the
intrinsic hand muscles.
� Finger abduction or
"fanning" is innervated by the T1 nerve root via
the ulnar nerve.
� Thumb opposition
is innervated by the C8 and T1 nerve roots via the
median nerve.
10
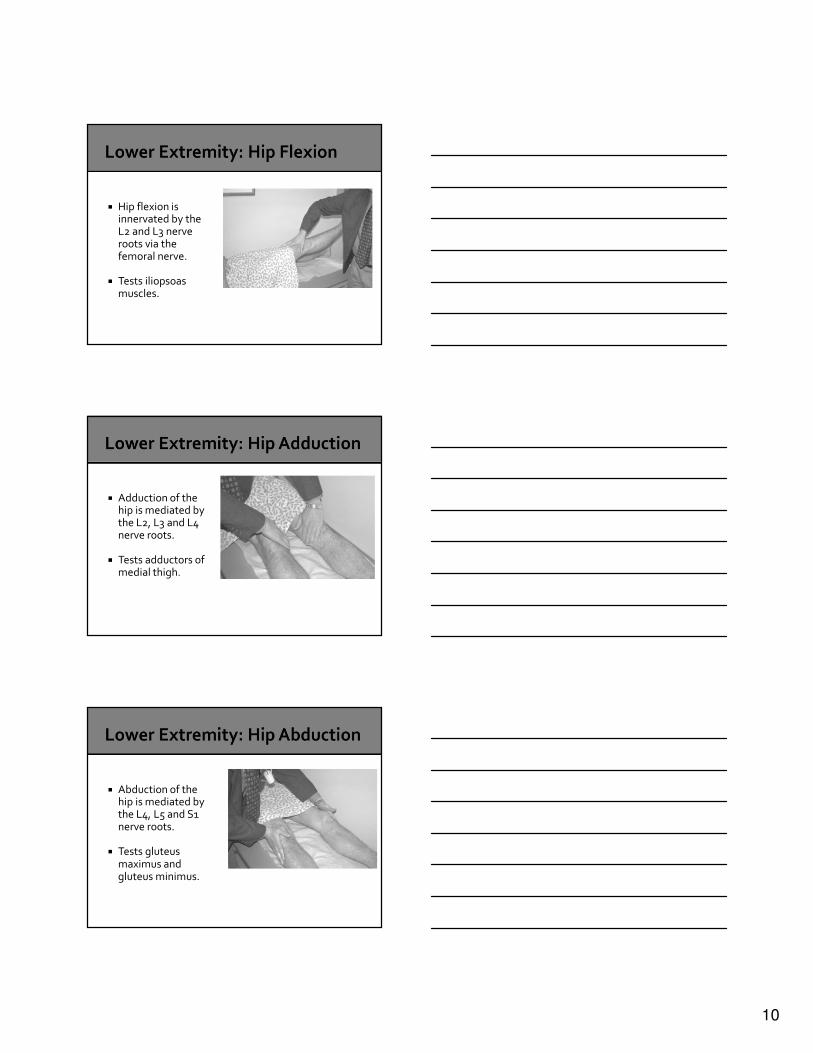
� Hip flexion is innervated by the L2 and L3 nerve roots via the femoral nerve.
� Tests iliopsoas muscles.
� Adduction of the hip is mediated by the L2, L3 and L4 nerve roots.
� Tests adductors of medial thigh.
� Abduction of the hip is mediated by the L4, L5 and S1 nerve roots.
� Tests gluteus maximus and gluteus minimus.
11
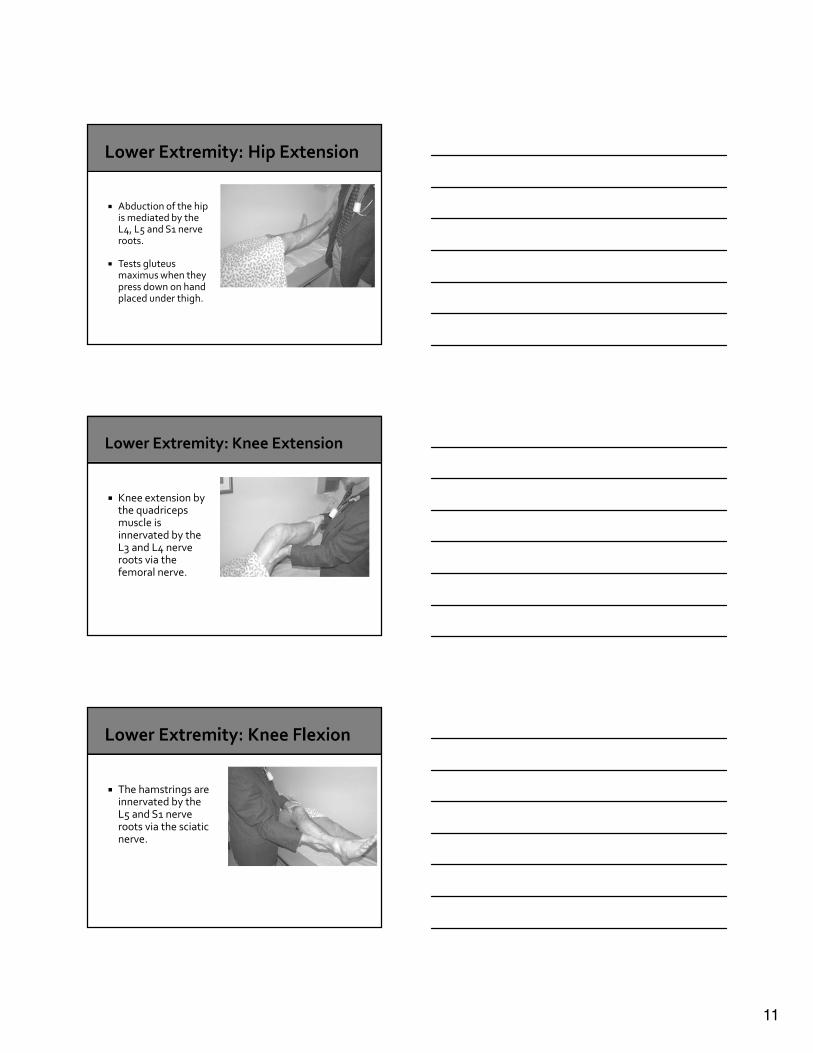
� Abduction of the hip is mediated by the L4, L5 and S1 nerve roots.
� Tests gluteus maximus when they press down on hand placed under thigh.
� Knee extension by the quadriceps muscle is innervated by the L3 and L4 nerve roots via the femoral nerve.
� The hamstrings are innervated by the L5 and S1 nerve roots via the sciatic nerve.

12
� Ankle dorsiflexion is innervated by the L4 and L5 nerve roots via the peroneal nerve.
� Tests anterior compartment of lower leg.
� Ankle plantar flexion is innervated by the S1 and S2 nerve roots via the tibial nerve.
� Tests posterior compartment of lower leg.
� Move large toe towards head.
� This tests the extensor halucis longus (EHL) muscle.
� The EHL is almost completely innervated by the L5 nerve root.
13
� 5/5 = normal against gravity & resistance
� 4/5 = full ROM against moderate resistance and gravity
� 3/5 = full ROM against gravity only
� 2/5 = extremity moves but not against gravity
� 1/5 = muscle contracts, extremity doesn’t move
� 0/5 = no visible/palpable contraction/movement
� Stereognosis – size & shape
� Graphesthesia - feel� Discrimination – right vs. left
� Calculation
� Serial 7’s: Subtract 7 from 100 serially
� What is 6 x 7
� How many quarters in $1.75
� Rapid Alternating Movements
� Finger to Nose� Heel-Shin
� Balance
� Romberg
� Gait
14
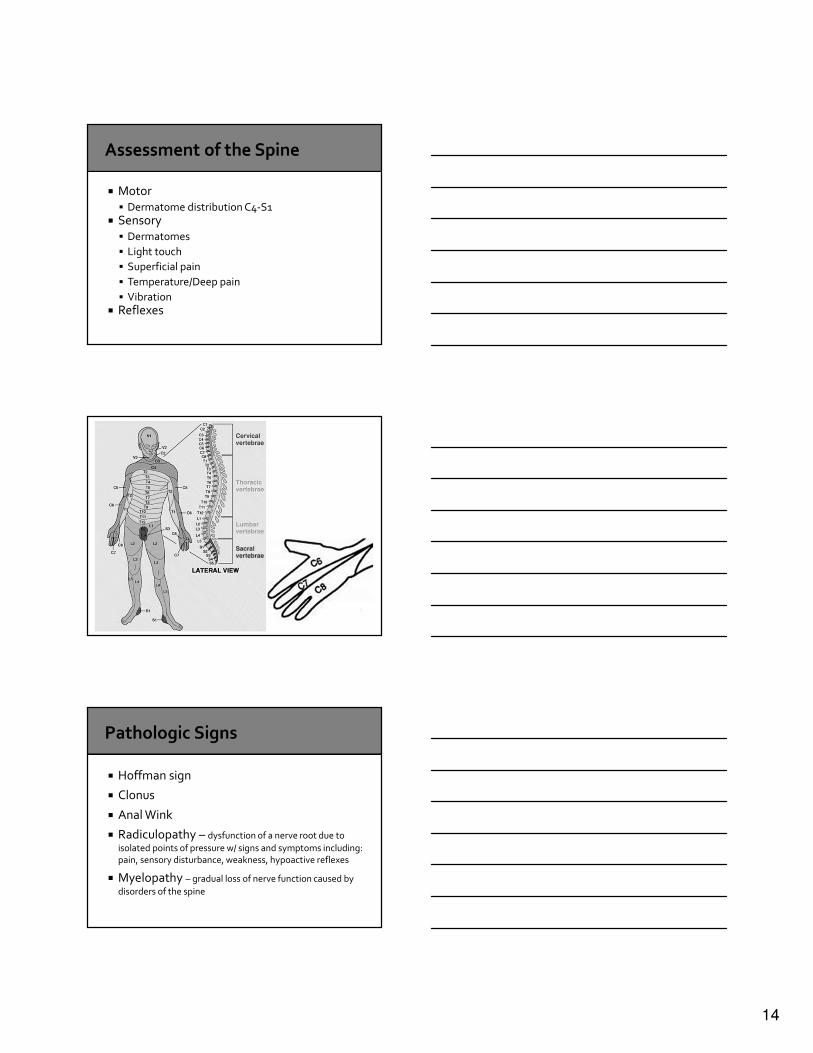
� Motor� Dermatome distribution C4-S1
� Sensory� Dermatomes
� Light touch
� Superficial pain
� Temperature/Deep pain
� Vibration� Reflexes
� Hoffman sign
� Clonus
� Anal Wink
� Radiculopathy – dysfunction of a nerve root due to
isolated points of pressure w/ signs and symptoms including: pain, sensory disturbance, weakness, hypoactive reflexes
� Myelopathy – gradual loss of nerve function caused by
disorders of the spine
15
� Patient supine
� Lift each leg (one at a time) to approx 70 degrees� Positive result
� Sciatic pain
� Radicular pain that goes below knee
▪ Worsened by ankle dorsiflexion
▪ Improved with ankle plantar flexion or lowering leg
� Reproducing back pain or pain in the hamstring area is NOT a positive result
� Level of
Consciousness� Glasgow Coma Score
▪ Motor
▪ Verbal
▪ Eyes
� CNS� II/III pupils (midbrain)
� V/VII corneals (pons)
� IX/X cough/gag (medulla)
� Developmental Progression / Delays
� Reaction to Strangers / Pain� Sick vs. Not Sick
� Emergence of migraines in very young
� Input of parents
� Great website: http://library.med.utah.edu/pedineurologicexam/html/introduction.html

16
� Environment
� Opioids� Fluid & Electrolyte Balance
� Infection
� Fatigue� Pain
Neurologic Assessment of the Older Adult, AANN Clinical Practice Guideline Series 2014
� Wet, Wacky, & Wobbly!
� Triad of Symptoms
� Gait disturbance
� Cognitive deficit
� Urinary incontinence
� More prevalent as population ages
� Rule out other causes� High volume LP can be diagnostic (pre/post
LP eval by physical therapy)

17
� Differentials
� Decision on imaging and other work up� Consult with a peer
� Decision to refer to specialist
� Biggest risk is missing a diagnosis that is time
sensitive – never hesitate to refer to ED!
18
� Loss of Consciousness / Unresponsiveness
� Acute Vision Loss
� Prolonged Seizure (Status Epilepticus)
� Acute loss of extremity function (paralysis)
� Loss of Bowel/Bladder control
� Chronic Back Pain without neurologic deficit
� Chronic headaches that have been evaluated for cranial lesions
� Non-hemorrhagic metastatic lesions that are asymptomatic
� Numbness
� Tingling
� Stable deficits that have been present for weeks/months
� Fevers, chills, recent urinary or skin infections� Significant trauma� Unrelenting night pain or pain at rest� Progressive motor or sensory deficit� Saddle anesthesia� Urinary or bowel dysfunction or incontinence� Unexplained weight loss� History of cancer or strong suspicion of cancer� Severe osteoporosis� Immunosuppression� Chronic oral steroid use� Intravenous drug use� Substance abuse

19
� 70% of back pain is musculoskeletal in nature
� One of the most common complaints that
drive people to seek medical care (ED/PCP)
� Almost all MRIs will have some kind of
finding, the majority of which is not surgical
� The natural history is generally favorable
� 30-60% of patients recover within 1 week
� 60-90% of patients recover within 6 weeks
� 95% of patient recover in 12 weeks ( 3 months)
� Relapses and recurrences are common and occur in approximately 40% of patients within a 6 month period
� L3-4 disk herniation:� Affects the L4 nerve root
� Sensory loss in the MEDIAL FOOT
� Motor loss in the KNEE EXTENSION
� Reflex loss in the PATELLA
� L4-5 disk herniation:� Affects the L5 nerve root
� Sensory loss in the DORSAL FOOT (large toe)
� Motor loss in the DORSIFLEXION (anterior tibialis & extensor hallicus longus)
� NO reflex loss
� L5-S1 disk herniation:� Affects the S1 nerve root
� Sensory loss in the LATERAL FOOT (small toe)
� Motor loss in the PLANTAR FLEXION
� Reflex loss in the ACHILLES

20
� In the absence of red flag findings, 4 to 6 weeks of conservative therapy is safe and appropriate and imaging is not indicated
� Plain radiographs have a fairly low yield and if the clinical suspicion is sufficiently high then it is generally necessary to proceed directly to MR imaging
� MR imaging in asymptomatic patients has a very high rate of abnormal findings:
� 40% of patients will have herniated disks
� 50% of patients will have a degenerative disk
� 40% of patients will have an annular tear
� X-Rays
� CT / CTA
� MRI / MRA
� Lumbar Puncture
� Angiography
� Mostly a cursory screening
� Helps assess alignment� Dynamic xrays (flexion/extension) can help in
some settings
� Not indicated in acute low back pain unless Red Flag present
� Can be used to monitor fractures
21
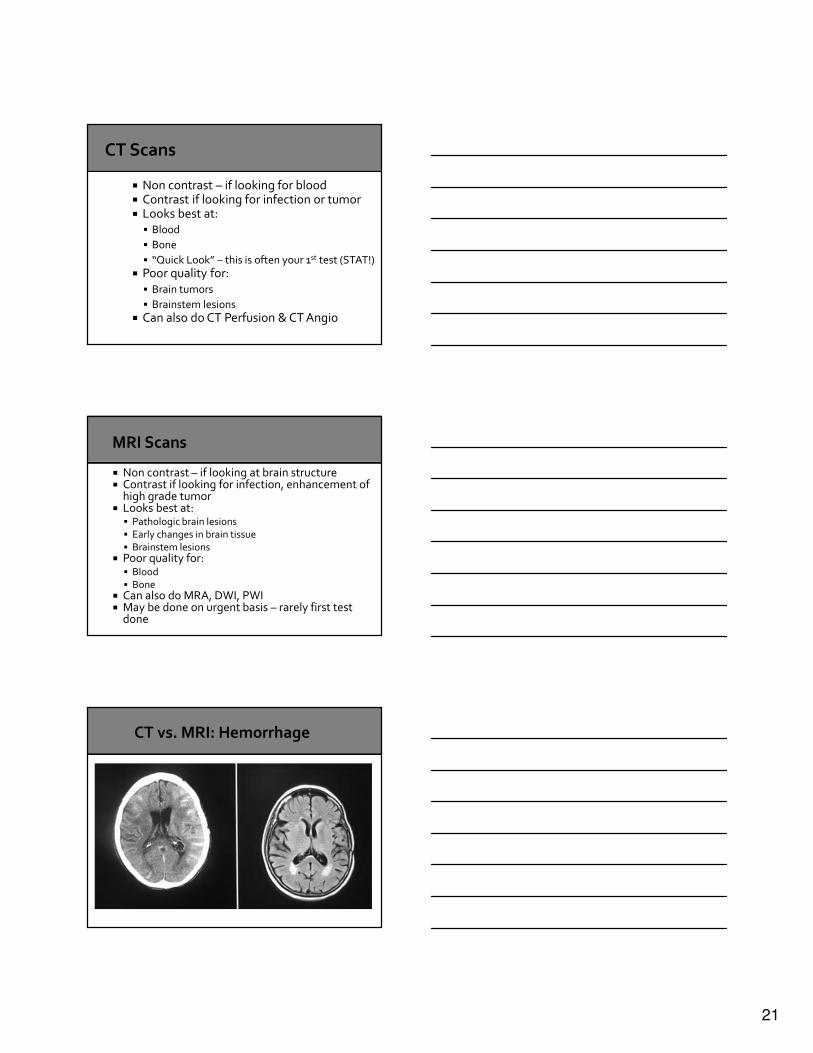
� Non contrast – if looking for blood� Contrast if looking for infection or tumor� Looks best at:
� Blood
� Bone
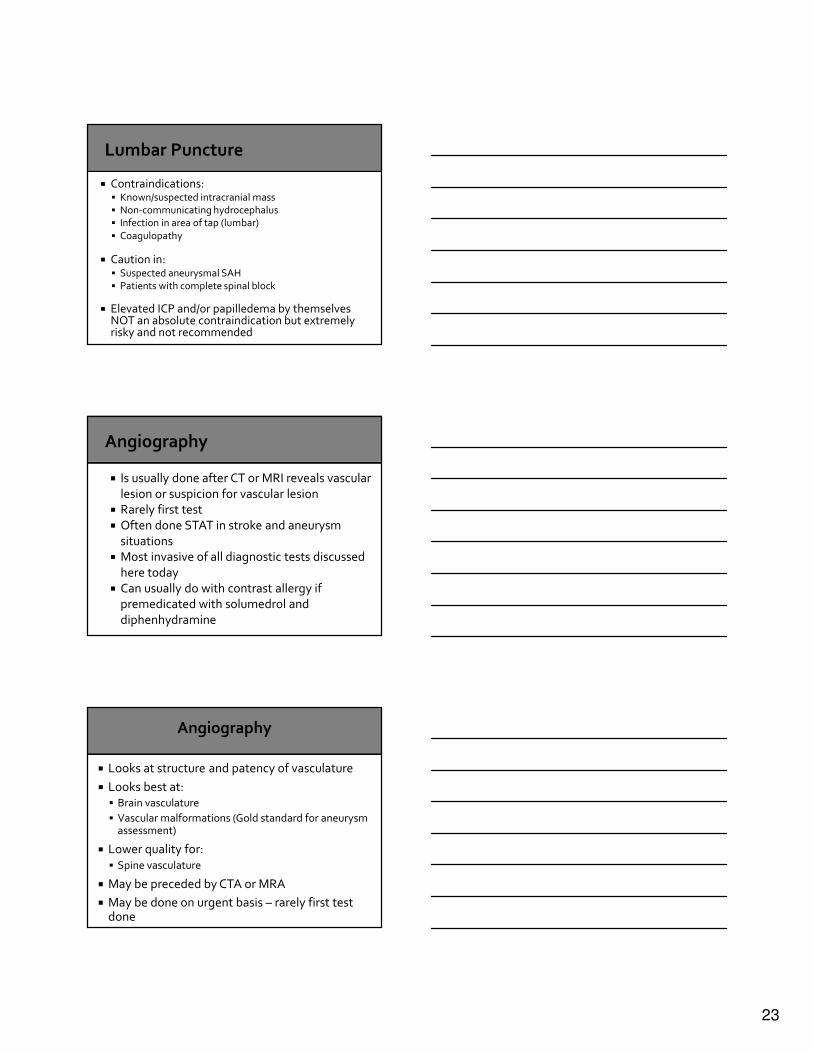
� “Quick Look” – this is often your 1st test (STAT!)� Poor quality for:
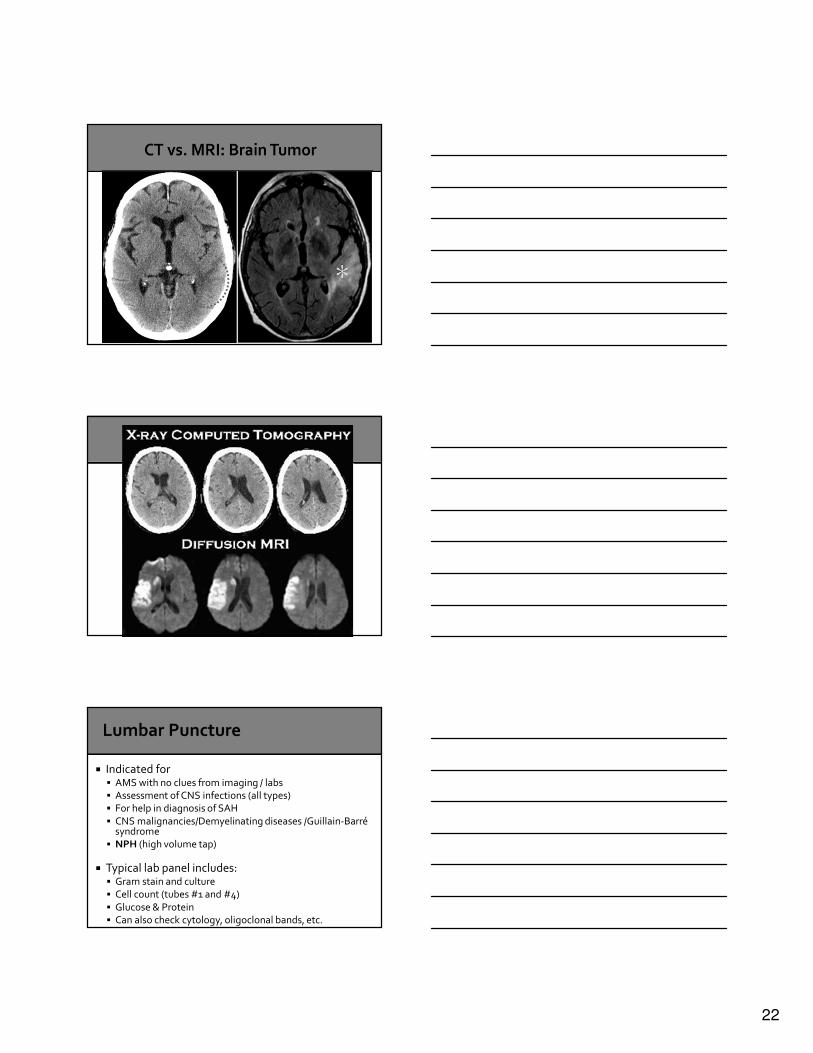
� Brain tumors
� Brainstem lesions� Can also do CT Perfusion & CT Angio
� Non contrast – if looking at brain structure� Contrast if looking for infection, enhancement of
high grade tumor� Looks best at:
� Pathologic brain lesions� Early changes in brain tissue� Brainstem lesions
� Poor quality for:� Blood� Bone
� Can also do MRA, DWI, PWI� May be done on urgent basis – rarely first test
done
22
� Indicated for � AMS with no clues from imaging / labs� Assessment of CNS infections (all types)� For help in diagnosis of SAH
� CNS malignancies/Demyelinating diseases /Guillain-Barrésyndrome
� NPH (high volume tap)
� Typical lab panel includes:� Gram stain and culture� Cell count (tubes #1 and #4)
� Glucose & Protein� Can also check cytology, oligoclonal bands, etc.
23
� Contraindications:� Known/suspected intracranial mass� Non-communicating hydrocephalus� Infection in area of tap (lumbar)
� Coagulopathy
� Caution in:� Suspected aneurysmal SAH� Patients with complete spinal block
� Elevated ICP and/or papilledema by themselves NOT an absolute contraindication but extremely risky and not recommended
� Is usually done after CT or MRI reveals vascular
lesion or suspicion for vascular lesion� Rarely first test
� Often done STAT in stroke and aneurysm
situations� Most invasive of all diagnostic tests discussed
here today
� Can usually do with contrast allergy if premedicated with solumedrol and
diphenhydramine
� Looks at structure and patency of vasculature
� Looks best at:� Brain vasculature
� Vascular malformations (Gold standard for aneurysm assessment)
� Lower quality for:� Spine vasculature
� May be preceded by CTA or MRA
� May be done on urgent basis – rarely first test done

24
� CTV / MRV
� EMG/NCV� High Volume LP
� Triad of NPH: Cognitive Dysfunction, Gait Disturbance, Urinary Incontinence
� Muscle Biopsy
� Most back pain is not surgical
� Correlate symptoms to dermatomes (spine)� Hemiparesis/Unilateral symptoms – think brain
� Always ok to ask what imaging a provider wants
before seeing a patient � If you’re worried, something’s wrong
� Has had intermittently for months
� Always when she has her menstrual cycle� Relieved with ASA and rest and caffeine

25
� Sudden onset severe HA at 10:25am
� Dizzy, very nauseated� Relieved by nothing
� Family feels she’s confused now
� Not able to control her legs to walk
� Worsening HA over 4 hours
� Now with stiff neck� Feels chilled and like he has flu
� Notices a rash on body
26
� 1 month progression of right sided weakness
� Having trouble periodically naming things� Has had low level headache for several
months
� No weight loss� Had an episode that was concerning for
seizure yesterday
� Helping friend move, heard a “POP”
� Severe low back pain� Intermittent pain down right leg
� No bowel or bladder issues
� Better if he lays down
� Neurologic Assessment of the Older Adult, A Guide for Nurses. AANN Clinical
Practice Guideline Series. 2014.� The complete neurological examination: what every nurse practitioner
should know. Murray TA, Kelly NR, Jenkins S. Adv Nurse Pract. 2002
Jul;10(7);24-8.� Haymore, J. A Neuron in a haystack. AACN Clinical issues (1079-0713), 15(4),
568.
� Mechanical Low Back Pain. Retrieved 3/16/2015 from http://emedicine.medscape.com/article/310353-clinical
� Greenberg M. Handbook of Neurosurgery. 8th Edition.
� Acute Low Back Pain: Recognizing the “Red Flags” in the Workup. Della-Giustina, D. Consultant. 2013;53(6):436-440,
27
� Gait Disorders
� http://library.med.utah.edu/neurologicexam/html/
gait_abnormal.html
� Neurologic Exam
� http://www.neuroexam.com/
Related Documents











