Neural mechanisms of emotion regulation in childhood anxiety Kathryn M. Hum, 1 Katharina Manassis, 2 and Marc D. Lewis 3 1 Department of Human Development and Applied Psychology, University of Toronto, Toronto, ON, Canada; 2 Department of Psychiatry, The Hospital for Sick Children, University of Toronto, Toronto, ON, Canada; 3 Behavioral Science Institute, Radboud University, Nijmegen, The Netherlands Background: The present study was designed to examine the cortical processes that mediate cognitive regulation in response to emotion-eliciting stimuli in anxious children. Methods: Electroencephalo- graphic (EEG) activity was recorded from clinically anxious children (n = 29) and typically developing children (n = 34). Event-related potential components were recorded while children performed a go/ no-go task using facial stimuli depicting angry, calm, and happy expressions. Results: Anxious children had significantly greater posterior P1 and frontal N2 amplitudes, components associated with attention/arousal and cognitive control, respectively, than typically developing children. Anxious children also had significantly greater error-related negativities and correct-response negativities rel- ative to typically developing children. For the anxious group only, there were no differences in neural activation between face (emotion) types or trial (Go vs. No-go) types. A regression analysis revealed that No-go N2 amplitudes for calm faces predicted self-reported anxiety levels. Conclusions: Anxious children appeared to show increased cortical activation regardless of the emotional content of the stimuli. Anxious children also showed greater medial-frontal activity regardless of task demands and response accuracy. Taken together, these findings suggest indiscriminate cortical processes that may underlie the hypervigilant regulatory style seen in clinically anxious individuals. Keywords: Childhood anxiety, event-related potentials, emotion faces, emotion regulation. Introduction Anxiety disorders are the most prevalent form of psychopathology in childhood and adolescence, with approximately 2.5–5% of children and adolescents meeting criteria for an anxiety disorder (Breton et al., 1999; Canino et al., 2004; Ford, Goodman, & Melt- zer, 2003; Lewinsohn, Hops, Roberts, Seeley, & An- drews, 1993). Anxiety disorders may negatively influence peer interactions, impair children’s func- tioning at school, hinder participation in social activities, and have a significant impact on family processes. Constitutional risk factors (e.g., inhibited temperament) and environmental risks (e.g., par- enting style) are thought to interact in the genesis of childhood anxiety disorders, but numerous devel- opmental pathways have been proposed. These pathways are thought to result in less effective styles of emotion regulation, rendering the child vulnerable to anxious coping responses in the face of environ- mental stress (De Pauw & Mervielde, 2010; Hirsh- feld-Becker, Micco, Simoes, & Henin, 2008). Regulatory tendencies correspond with distinct neural processes in anxious adults. However, little is known about the neural mechanisms of emotion processing that distinguish anxious children from their peers. The present study was designed to examine the cortical activation patterns in anxious children that may mediate self-regulatory processes in the presence of emotional stimuli. Emotion regulation may be conceptualized as the cognitive processes involved in monitoring, evaluat- ing, and modifying emotional reactions to achieve a particular goal (Thompson, 1994). Individuals who are able to successfully regulate their emotions rec- ognize when their emotions diverge from a reference point, and attempt to shift their emotional state to- ward that point by recruiting effective coping strat- egies (e.g., response inhibition, attention shifting, and reappraisal) (Hoeksma, Oosterlaan, & Schipper, 2004). Children who have less effective styles of emotion regulation often develop serious behavior problems that can result in a variety of clinical diagnoses (reviewed in Hum & Lewis, in press). Anxious children tend to focus their attention on potential signs of danger, and interpret ambiguous or novel stimuli negatively (Bishop, 2007; Pine, Helfinstein, Bar-Haim, Nelson, & Fox, 2009). Biases during initial or perceptual stages of information processing often lead to subsequent biases in cog- nitive processing, which may contribute to ineffective coping responses (e.g., hypervigilance) that render anxious children susceptible to social inhibition and/or avoidance behaviors in the presence of emotion-inducing stimuli (Perez-Edgar et al., 2010; White, Suway, Pine, Bar-Haim, & Fox, 2011). Human faces are emotionally provocative stimuli that effectively capture attention. Humans efficiently and automatically decode facial expressions that Conflict of interest statement: No conflicts declared. Journal of Child Psychology and Psychiatry 54:5 (2013), pp 552–564 doi:10.1111/j.1469-7610.2012.02609.x ȑ 2012 The Authors. Journal of Child Psychology and Psychiatry ȑ 2012 Association for Child and Adolescent Mental Health. Published by Blackwell Publishing, 9600 Garsington Road, Oxford OX4 2DQ, UK and 350 Main St, Malden, MA 02148, USA

Neural Mechanisms of Emotion Regulation in Childhood Anxiety
Jan 15, 2016
Neural mechanisms underlying emotion regulation in childhood anxiety. Neuropsychology.
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Neural mechanisms of emotion regulationin childhood anxiety
Kathryn M. Hum,1 Katharina Manassis,2 and Marc D. Lewis31Department of Human Development and Applied Psychology, University of Toronto, Toronto, ON, Canada;2Department of Psychiatry, The Hospital for Sick Children, University of Toronto, Toronto, ON, Canada;
3Behavioral Science Institute, Radboud University, Nijmegen, The Netherlands
Background: The present study was designed to examine the cortical processes that mediate cognitiveregulation in response to emotion-eliciting stimuli in anxious children. Methods: Electroencephalo-graphic (EEG) activity was recorded from clinically anxious children (n = 29) and typically developingchildren (n = 34). Event-related potential components were recorded while children performed a go/no-go task using facial stimuli depicting angry, calm, and happy expressions. Results: Anxiouschildren had significantly greater posterior P1 and frontal N2 amplitudes, components associated withattention/arousal and cognitive control, respectively, than typically developing children. Anxiouschildren also had significantly greater error-related negativities and correct-response negativities rel-ative to typically developing children. For the anxious group only, there were no differences in neuralactivation between face (emotion) types or trial (Go vs. No-go) types. A regression analysis revealed thatNo-go N2 amplitudes for calm faces predicted self-reported anxiety levels. Conclusions: Anxiouschildren appeared to show increased cortical activation regardless of the emotional content of thestimuli. Anxious children also showed greater medial-frontal activity regardless of task demands andresponse accuracy. Taken together, these findings suggest indiscriminate cortical processes that mayunderlie the hypervigilant regulatory style seen in clinically anxious individuals. Keywords: Childhoodanxiety, event-related potentials, emotion faces, emotion regulation.
IntroductionAnxiety disorders are the most prevalent form ofpsychopathology in childhood and adolescence, withapproximately 2.5–5% of children and adolescentsmeeting criteria for an anxiety disorder (Breton et al.,1999; Canino et al., 2004; Ford, Goodman, & Melt-zer, 2003; Lewinsohn, Hops, Roberts, Seeley, & An-drews, 1993). Anxiety disorders may negativelyinfluence peer interactions, impair children’s func-tioning at school, hinder participation in socialactivities, and have a significant impact on familyprocesses. Constitutional risk factors (e.g., inhibitedtemperament) and environmental risks (e.g., par-enting style) are thought to interact in the genesis ofchildhood anxiety disorders, but numerous devel-opmental pathways have been proposed. Thesepathways are thought to result in less effective stylesof emotion regulation, rendering the child vulnerableto anxious coping responses in the face of environ-mental stress (De Pauw & Mervielde, 2010; Hirsh-feld-Becker, Micco, Simoes, & Henin, 2008).Regulatory tendencies correspond with distinctneural processes in anxious adults. However, little isknown about the neural mechanisms of emotionprocessing that distinguish anxious children fromtheir peers. The present study was designed toexamine the cortical activation patterns in anxious
children that may mediate self-regulatory processesin the presence of emotional stimuli.
Emotion regulation may be conceptualized as thecognitive processes involved in monitoring, evaluat-ing, and modifying emotional reactions to achieve aparticular goal (Thompson, 1994). Individuals whoare able to successfully regulate their emotions rec-ognize when their emotions diverge from a referencepoint, and attempt to shift their emotional state to-ward that point by recruiting effective coping strat-egies (e.g., response inhibition, attention shifting,and reappraisal) (Hoeksma, Oosterlaan, & Schipper,2004). Children who have less effective styles ofemotion regulation often develop serious behaviorproblems that can result in a variety of clinicaldiagnoses (reviewed in Hum & Lewis, in press).Anxious children tend to focus their attention onpotential signs of danger, and interpret ambiguousor novel stimuli negatively (Bishop, 2007; Pine,Helfinstein, Bar-Haim, Nelson, & Fox, 2009). Biasesduring initial or perceptual stages of informationprocessing often lead to subsequent biases in cog-nitive processing, which may contribute to ineffectivecoping responses (e.g., hypervigilance) that renderanxious children susceptible to social inhibitionand/or avoidance behaviors in the presence ofemotion-inducing stimuli (Perez-Edgar et al., 2010;White, Suway, Pine, Bar-Haim, & Fox, 2011).
Human faces are emotionally provocative stimulithat effectively capture attention. Humans efficientlyand automatically decode facial expressions thatConflict of interest statement: No conflicts declared.
Journal of Child Psychology and Psychiatry 54:5 (2013), pp 552–564 doi:10.1111/j.1469-7610.2012.02609.x
� 2012 The Authors. Journal of Child Psychology and Psychiatry � 2012 Association for Child and Adolescent Mental Health.Published by Blackwell Publishing, 9600 Garsington Road, Oxford OX4 2DQ, UK and 350 Main St, Malden, MA 02148, USA

convey information about an individual’s emotionalstate (Ohman, 2009). Nonconscious perception offacial expressions may elicit emotional responsesthat activate learned associations and/or modulatecognitive processing and behavioral responding(Ohman, 2002; Tottenham, Hare, & Casey, 2011).For instance, an angry facial expression initiallycaptures one’s attention to signal a change in cur-rent behavior (e.g., trigger response inhibition).Response inhibition, a core executive function involvedin emotion regulation, enabling self-control and goaldirected behavior, is mediated by activity in prefrontalareas such as the orbital frontal cortex (OFC) and theanterior cingulate cortex (ACC) (Blair, 2003).
Neural mechanisms underlying emotion regula-tion may be examined using electroencephalography(EEG). EEG is an appealing method for clinical re-search, particularly with anxious children, as it isnoninvasive and offers high temporal resolution(Banaschewski & Brandeis, 2007). Electrical brainactivity is recorded at the scalp using an array ofelectrodes and averaged over many trials on a giventask, generating an event-related potential (ERP).Various ERP components are thought to tap differentphases of emotion regulation (Dennis, 2010). Early,automatic stimulus-related processes may be in-dexed by the posterior P1 component. The P1, aneural indicator of visual perception, attention, andarousal, peaks at about 100–130 ms post-stimulusat occipital electrode sites (Hillyard, Vogel, & Luck,1998). Behavioral studies indicate an attentionalbias toward angry relative to neutral faces in anxiouschildren (Roy et al., 2008; Waters, Henry, Mogg,Bradley, & Pine, 2010). Some studies indicate,however, that severely anxious children demonstratean attentional bias toward both angry and happyfaces (Waters, Mogg, Bradley, & Pine, 2008). Paral-leling these behavioral findings, ERP studies revealdifferential modulation of early ERP componentsacross emotion face types among anxious adults(Bar-Haim, Lamy, & Glickman, 2005; Holmes, Niel-sen, & Green, 2008; Kolassa & Miltner, 2006;Mueller et al., 2009). Yet, some studies indicate thatthese early ERP components are unaffected by facialexpression (e.g., Eimer & Holmes, 2002), withgreater amplitudes seen in anxious than nonanxiousadults regardless of the type of emotional face stim-uli (Eldar, Yankelevitch, Lamy, & Bar-Haim, 2010;Muhlberger et al., 2009). Thus it remains unclearhow anxiety influences early perceptual responses inrelation to the valence of emotional faces, althoughgreater responsiveness to emotionality is oftenrevealed.
As mentioned above, cognitive processes ofresponse inhibition and response monitoring areoften involved in emotion regulation. Later ERPcomponents that reflect these more cognitive pro-cesses may be indexed by the stimulus-locked N2and response-locked ERP components. The frontalN2 component, a neural indicator of conflict
monitoring or response inhibition, is thought to re-flect control processing and is observed 200–300 mspost-stimulus at medial-frontal electrode sites inadults (Donkers & van Boxtel, 2004; Folstein & VanPetten, 2008), but later in children (Lewis, Lamm,Segalowitz, Zelazo, & Stieben, 2006). Source modelssuggest the OFC and the ACC as neural generators ofthe N2 (Bekker, Kenemans, & Verbaten, 2005; Bok-ura, Yamaguchi, & Kobayashi, 2001). Using anemotional go/no-go task requiring response inhibi-tion, anxious children had slower Go responses toneutral faces when embedded in angry face No-gotrials (Ladouceur, Dahl, Williamson, et al., 2006;Waters & Valvoi, 2009). The authors of these studiessuggest that early perceptual processing of emo-tional facial expressions influences later cognitivecontrol processes. Similar to these behavioral stud-ies, ERP studies have revealed that N2 amplitudesare influenced by anxiety levels (Righi, Mecacci, &Viggiano, 2009; Sehlmeyer et al., 2010), withreduced N2 amplitudes elicited in response to fearfulfaces seen in high trait anxious adults (Dennis &Chen, 2009). Few studies if any, however, haveexamined stimulus-locked ERP components inresponse to emotional faces in anxious children.
The response-locked error-related negativity (ERN)and the correct-response negativity (CRN), believedto reflect response monitoring processes, are ob-served at medial-frontal electrode sites 50–150 msfollowing incorrect and correct responses, respec-tively (Falkenstein, Hohnsbein, Hoormann, &Blanke, 1991; Gehring, Goss, Coles, Meyer, & Don-chin, 1993). Source models point to the ACC as thegenerator of the ERN (van Veen & Carter, 2002).Anxiety is often associated with personality traits(e.g., perfectionism) that may lead to hypervigilanceand sensitivity to error (Hewitt et al., 2002; Weems,Costa, Watts, Taylor, & Cannon, 2007). EnhancedERN amplitudes have been seen for high-anxiousadults (Aarts & Pourtois, 2010; Hajcak, McDonald, &Simons, 2003a; Olvet & Hajcak, 2008). Similarly,greater ERN amplitudes have been seen in childrenwith anxiety (Ladouceur, Dahl, Birmaher, Axelson, &Ryan, 2006; McDermott et al., 2009; Meyer, Wein-berg, Klein, & Hajcak, 2012; Santesso, Segalowitz, &Schmidt, 2006). In one study, young adults withhigh-state anxiety displayed smaller ERNs for angryfaces and larger ERNs for happy faces (Comptonet al., 2007). Very few studies if any, however, haveexamined the ERN/CRN in response to emotionalface stimuli in anxious children.
In sum, stimulus- and response-locked ERPssuggest increased cortical activity when anxiousindividuals attempt to regulate their attention, ap-praisal, and response to stimuli, and this effect isamplified by emotion-inducing cues. However, to ourknowledge, no study has yet investigated anxiouschildren’s ERP responses to positive versus negativeemotion faces. To investigate anxious children’sneural responses to different emotions, we developed
doi:10.1111/j.1469-7610.2012.02609.x Neural mechanisms underlying childhood anxiety 553
� 2012 The Authors. Journal of Child Psychology and Psychiatry � 2012 Association for Child and Adolescent Mental Health.

a modified go/no-go task using emotionally evoca-tive facial expressions while recording neural acti-vation with dense-array EEG. Anxious versuscomparison group differences were evaluated for thestimulus-locked P1 and frontal N2 components andthe response-locked CRN and ERN components. Itwas hypothesized that ERP amplitudes would begreater for anxious children, particularly in responseto angry faces. We also compared ERP amplitudesacross No-go versus Go conditions and correct ver-sus incorrect trials, to determine whether and howmuch anxious children discriminate between task-and performance-related demands.
MethodsEthical approval of the present study was obtainedfrom the University of Toronto and the Hospital forSick Children in Toronto, Canada.
Participants
Forty-seven children, 8–12 years of age, were referred toparticipate in the study from the Anxiety DisordersClinic at the Hospital for Sick Children in Toronto, priorto the start of treatment. Diagnostic assessments werecompleted with parents confirming a primary (mostimpairing) diagnosis of an Axis 1 anxiety disorder(Generalized Anxiety Disorder, Social Anxiety Disorderor Separation Anxiety Disorder) using a semi-struc-tured parent interview (Anxiety Disorders InterviewSchedule) (Silverman & Albano, 1996) (Table 1). Forty-one age-matched children, free of any psychiatric dis-orders, were recruited from the community using adepartmental research participant database or throughlocal advertisements. Table 2 presents the child andfamily characteristics of the final sample of clinical andcomparison groups (see Appendix for further exclusioncriteria and medication details).
Procedure
All children were accompanied to the laboratory by aparent. After a brief introduction to the testing envi-ronment and procedures, parental consent and childassent were obtained. Children were first asked tocomplete two questionnaires: the MultidimensionalAnxiety Scale for Children (MASC) (March, 1998) and
the Child Depression Index (CDI) (Kovacs, 1992). Uponcompletion of the questionnaires, children were showna bin with a wide selection of desirable toys such aslarge action figures, stuffed animals, and gift certifi-cates from an electronic gaming or clothing store. Toensure high motivation, children were offered a toy fromthe prize bin contingent on successful completion of thetask. Next, the EEG net application procedures weredescribed, and children were asked to complete theState-Trait Anxiety Inventory for Children (STAIC-S)(Spielberger, 1973). All children were then fitted with a128-channel Geodesic Sensor Net (Electrical GeodesicsInc., Eugene, OR, USA) and seated with the distanceand alignment to the monitor controlled by the use of achin rest. Children were then asked to perform the go/no-go task (see below). While the children completed thequestionnaires and before they performed the task,parents were escorted to an adjacent room where theywere asked to provide basic demographic informationand complete the Child Behavior Checklist (CBCL)(Achenbach, 1991). All families were paid $30 CDN plustwo toys or gift certificates for their participation.
Questionnaires
The MASC (March, 1998) measures trait anxiety in chil-dren and adolescents, asking children to report how theyhavebeen thinking, feeling, andacting recently.Childrenindicate, using a 4-point Likert scale, how often eachstatement is trueabout themselves . In thepresent study,the MASC Total and Anxiety Disorder Index subscales
Table 1 Distribution of clinical participants who met diag-nostic criteria for (a) specific anxiety disorder(s)
Clinical group (n = 29)
Anxiety disorder diagnosis (n)GAD only 14SOC only 3SEP only 2SOC & SEP 2GAD & SOC 4GAD & SEP 3GAD, SOC & SEP 1
GAD, generalized anxiety disorder; SOC, social anxiety disor-der; SEP, separation anxiety disorder.
Table 2 Child and family characteristics for the final sample ofclinical and comparison participants
Clinical group(n = 29)
Comparisongroup (n = 34)
Age (years) 10.31 (1.22) 10.14 (1.39)Gender (M:F) 10:19 13:21Handedness (right:left) 25:4 30:4Ethnicity, n (%)European 23 (79.3) 17 (50.0)East Asian 1 (3.4) 3 (8.8)South Asian 2 (6.9) 5 (14.7)African/Caribbean 0 (0) 1 (2.9)Latin American 0 (0) 2 (5.9)Others/Unknown 3 (10.3) 6 (17.6)
Mother’s education, n (%)Some high school 1 (3.4) 1 (2.9)High school graduate 1 (3.4) 1 (2.9)College graduate 7 (24.1) 9 (26.5)University graduate 15 (51.7) 17 (50.0)Post-graduate/Professional 4 (13.8) 6 (17.6)Unknown 1 (3.4) 0 (0)
Father’s education, n (%)Grade 8 or less 0 (0) 2 (5.9)Some high school 3 (10.3) 1 (2.9)High school graduate 5 (17.2) 4 (11.8)College graduate 3 (10.3) 8 (23.5)University graduate 11 (37.9) 12 (35.3)Post-graduate/Professional 7 (24.1) 6 (17.6)Unknown 0 (0) 1 (2.9)
Family income, n (%)$10,000–$69,999 10 (34.5) 9 (26.4)$70,000–$149,999 13 (44.7) 13 (38.2)Greater than $150,000 6 (20.7) 10 (29.4)Declined to report 0 (0) 2 (5.9)
554 Kathryn M. Hum, Katharina Manassis, and Marc D. Lewis J Child Psychol Psychiatry 2013; 54(5): 552–64
� 2012 The Authors. Journal of Child Psychology and Psychiatry � 2012 Association for Child and Adolescent Mental Health.

were used. The STAIC-S (Spielberger, 1973) measuresstate anxiety by asking children to evaluate how they feelat the moment and to assess feelings of apprehension,tension, and worry. The CDI (Kovacs, 1992) was admin-istered to evaluate the presence and severity of comorbiddepressive symptomatology. For each item, the child isasked to endorse the statement that best describes his orher feelings. For this study, the CDI Total subscale wasused. The CBCL (Achenbach, 1991) assesses a variety ofchildren’s emotional and behavioral problems. Parentsare asked to indicate whether, and to what degree, theirchild exhibits a list of symptoms. For this study, only theinternalizing (anxious, depressed, withdrawn, and so-matic complaints) and externalizing (rule-breaking andaggressive behaviors) subscales were used. For allquestionnaires, standardized T-scores were calculated,with higher scores representing greater impairment ordysfunction.
EEG task
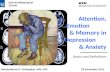
An emotional go/no-go task was presented usingE-Prime software (Psychological Software Tools, Pitts-burgh, PA, USA). Children were instructed to press abutton as quickly as possible in response to a facedepicting an emotional expression, using gender as thego/no-go cue (Figure 1). Gender was considered anarbitrary cue, not requiring additional processing of theemotion expression, and was switched across trialblocks and counterbalanced.
The task consisted of 288 trials using stimuli fromthe NimStim set of facial expressions (Tottenham et al.,2009). Eight male and eight female models depictingangry, calm, and happy emotions (open and closedmouth conditions) were used. Previous studies haveshown that anxious individuals (particularly those withsocial anxiety) perceive neutral faces as threatening(Mohlman, Carmin, & Price, 2007; Yoon & Zinbarg,2008). As we did not want to conflate the negativeemotion condition (i.e., angry faces) with the nonemo-tional condition, calm (rather than neutral) faces wereincluded in the set of facial stimuli.
To establish a ratio of two Go trials to every No-gotrial, each face was used three times, and presented inpseudorandom order. The task consisted of four blockswith a break between each block. To ensure that dif-ferences in neural activation were not due to age- orskill-related differences in performance level, the taskwas dynamically adjusted with a response-duration
algorithm that ensured successful inhibition on 75% ofthe No-go trials. The initial Go response window was setat 550 ms and decreased by 50 ms or increased by150 ms when the participant succeeded or failed toinhibit No-go trial responses, respectively (see Appendixfor further EEG task and stimuli details).
EEG data analysis
Electroencephalographic was recorded and sampled at250 Hz (Electrical Geodesics Inc.). Impedances for allEEG channels were below 50 kX (as recommended byEGI). Standard EEG filtering and artifacting procedureswere used to process the data (see Appendix for details).
The P1was scored as themeanactivation 125–175 mspost-stimulus onset, averaged across six occipital elec-trode sites (Figure 2). The N2 was scored as the meanactivation 250–400 ms post-stimulus onset (a windowappropriate for children of this age), averaged acrossthree medial frontal electrode sites. For the ERN, themost negative peak in a time window from 50 ms pre-response to 100 ms postresponse was detected on errorNo-go trials. The ERN was scored as the mean activation50 ms around this peak (i.e., 25 ms on either side of thepeak), averaged across three medial frontal electrodesites. Given the task design, a target No-go error rate of25% led to insufficient trial counts to examine ERN val-ues for each emotion. Hence, ERN analyses were col-lapsed across emotion conditions. The CRN wasevaluated using the same approach for correct Go trials.
Statistical analysis
The effects of age, gender, CBCL externalizing scores,and trial count (ERP analyses only) were entered ascovariates for all analyses of variance (ANOVAs).Externalizing scores were included as a covariate aschildren with comorbid internalizing and externalizingproblems often have distinct neural activation profiles(Stieben, Lewis, Granic, Zelazo, & Segalowitz, 2007).
Figure 1 Go/No-go taskFigure 2 Montages used to examine posterior P1, frontal N2, ERNand CRN activation levels
doi:10.1111/j.1469-7610.2012.02609.x Neural mechanisms underlying childhood anxiety 555
� 2012 The Authors. Journal of Child Psychology and Psychiatry � 2012 Association for Child and Adolescent Mental Health.

SPSS Statistics version 19.0 (IBM, Armonk, NY, USA)was used for all statistical analyses. Unless indicatedotherwise, all results are expressed as means ± stan-dard deviations. An alpha level of .05 was used for allstatistical tests, and the Bonferroni correction was usedto adjust for multiple comparisons.
ResultsQuestionnaire results
Table 3 presents the questionnaire data for bothclinical and comparison groups. An independentsamples t-test revealed no significant depressionlevel (CDI) differences between groups. As expected,however, independent samples t-tests revealed sig-nificant differences between groups for the CBCLinternalizing scale, MASC total, and STAIC-S scores.These data confirm that our clinical sample of chil-dren had significantly elevated levels of anxiety rel-ative to comparison children, both in their daily lives(CBCL Internalizing, MASC) and in the experimentalsituation (STAIC-S).
Behavioral results
Table 4 presents the go/no-go behavioral data forclinical and comparison children. Multiple univari-ate ANOVAs revealed no significant group differencesin accuracy, response duration (i.e., response timeallotment), Go response times, or error No-goresponse times. These data confirm that group dif-ferences in neural activation patterns are probablynot due to variations in task performance.
ERP results
P1:Figure 3A and B present the topography maps andgrand-averaged waveforms for the P1 component,respectively. For correct No-go trials, clinical childrenhad greater P1 amplitudes across all emotion facesrelative to comparison children (Figure 3C). A 2
(Group) · 3 (Emotion type) mixed-model ANOVA re-vealed a significant effect of group F(1,57) = 5.56,p = .022 but no effect of emotion type. These datasuggest heightened attention and/or arousal in re-sponse to the facial stimuli, irrespective of emotionalvalence, for the clinical group.
Frontal N2
Figure 4A and B present the topography maps andgrand-averaged waveforms for the correct No-go N2component. A 2 (Group) · 3 (Emotion type) mixed-model ANOVA revealed a significant effect of emotiontype F(1,57) = 7.27, p = .009, a significant effect ofgroup F(1,57) = 9.48, p = .003, and a significantinteraction effect F(1,57) = 5.47, p = .023 (Figure 4C).Between-group comparisons revealed significantdifferences for the calm (p = .006) and happy(p < .001) face types. Within the comparison group,butnot the clinical group, significantdifferences inN2amplitudeswere seen for angry versus calm (p = .010)and angry versus happy face types (p = .002). Insummary, for correct No-go trials, clinical childrenhad greater (more negative) N2 amplitudes relative tocomparison children. Differences in activation levelswere not seen across emotion types within the clinicalgroup. However, comparison children recruitedgreater N2 activation in response to angry faces thanboth calm and happy faces. These data suggest thatclinical children failed to discriminate between theemotionfaces,whereascomparisonchildrenallocatedcortical resourcesdifferentially according to face type.
Figure 4D presents the correct Go N2 amplitudesand the correct No-go N2 amplitudes, collapsedacross emotion conditions. A 2 (Group) · 2 (Trialtype) mixed-model ANOVA revealed a significantmain effect for trial type F(1,57) = 4.94, p = .030, asignificant effect of group F(1,56) = 14.67, p £ .001,and a significant interaction effect F(1,56) = 5.56,p = .022. Within-group comparisons revealed a dif-ference between trial types for comparison children(p = .004), but not for clinical children (p = .537).
Table 3 Questionnaire measures for clinical and comparison children
Clinical group (n = 29) Comparison group (n = 34) p-value
CBCL Internalizing Scale T-score 71.62 (4.63) 46.68 (7.81) .000*MASC Total Scale T-score 55.52 (7.94) 49.88 (8.93) .011*MASC Anxiety Disorders Index T-score 54.72 (9.10) 48.94 (9.80) .019*STAIC S-Anxiety Scale T-Score 50.17 (9.97) 43.74 (9.09) .009*CDI Total T-Score 46.75 (8.01) 44.09 (6.42) .152
CBCL, Child Behavior Checklist; MASC, Multidimensional Anxiety Scale for Children; STAIC-S, State-Trait Anxiety Inventory forChildren; CDI, Child Depression Index; *p < .05.
Table 4 EEG task behavioral data for clinical and comparison children
Clinical group (n = 29) Comparison group (n = 34) p-value
Accuracy (%) 78.42 (3.99) 77.34 (4.50) .103Response duration (ms) 734.73 (137.21) 794.25 (153.42) .255Go response time (ms) 427.32 (40.97) 439.68 (61.53) .360Error No-go response time (ms) 381.56 (47.94) 376.65 (58.02) .993
556 Kathryn M. Hum, Katharina Manassis, and Marc D. Lewis J Child Psychol Psychiatry 2013; 54(5): 552–64
� 2012 The Authors. Journal of Child Psychology and Psychiatry � 2012 Association for Child and Adolescent Mental Health.

These data reveal that anxious children recruitedsimilar levels of activation on correct Go and No-gotrials, while comparison children recruited greateractivation on No-go trials. These findings suggestthat anxious children recruited the same amount ofneural activation despite differences in the need forresponse inhibition.
Response-locked ERP components
As noted previously, ERN values were aggregatedacross emotion conditions due to the low frequencyof No-go errors per condition. To allow for compari-sons between components, we similarly averagedacross emotion conditions for the CRN (see Appendixfor CRN analyses by emotion type). Figure 5A and Bpresent the topography maps and grand-averagedwaveforms for the ERN and CRN components. Toanalyze ERN and CRN amplitudes, a 2 (group) · 2(trial type) mixed-model ANOVA revealed a signifi-cant main effect for trial type F(1,56) = 5.77,
(A)
(B)
(C)
Figure 3 P1 data. (A) Topography maps for comparison andclinical groups at 170 ms post-stimulus onset. (B) Grand-averagedwaveforms at electrode O1. (C) Mean P1 activation ± standarderrors, 125–175 ms post-stimulus onset, averaged across the sixelectrodes in the occipital montage
(A)
(B)
(C)
(D)
Figure 4 N2 data. (A) Topography maps by emotion for com-parison and clinical groups at 325 ms post-stimulus onset. (B)Grand-averaged waveforms at electrode Fz. (C) Mean No-go N2activation ± standard errors, 250–400 post-stimulus onset, aver-aged across the three electrodes in the medial-frontal montage.(D) Mean Go N2 versus No-go N2 activation ± standard errors
doi:10.1111/j.1469-7610.2012.02609.x Neural mechanisms underlying childhood anxiety 557
� 2012 The Authors. Journal of Child Psychology and Psychiatry � 2012 Association for Child and Adolescent Mental Health.

p = .020, a significant main effect for groupF(1,56) = 6.67, p = .012, but no significant interac-tion effect F(1,56) = .020, p = .887 (Figure 5C).These data indicate that greater activation was seenfor error No-go responses relative to correct Go re-sponses, and clinical children showed greater acti-vation for both components compared with controlchildren.
Regression analyses
A regression analysis was performed to evaluate howwell ERP amplitudes predicted anxiety levels. Theassociation between correct No-go N2 amplitudes forcalm faces and Anxiety Disorder Index scores was).28, F(1,61) = 5.16, p = .027. Thus, approximately8% of the variance in anxiety levels was accountedfor by its relationship with calm N2 amplitudes. Theregression equation for predicting self-reportedanxiety from calm N2 amplitudes was found to beY¢ = 48.56–0.53x. The 95% CI for the slope predict-ing anxiety levels from calm N2 amplitudes rangedfrom )0.06 to )1.0. Thus, for each microvolt increasein No-go N2 amplitude for calm faces, the predictedAnxiety Disorder Index T-score decreased by about.06 to 1 point.
DiscussionAdvances in neuroimaging can provide importantinsights into the neural circuitry that underliesdysfunctional emotion regulation in children whodevelop behavior problems. The present studyexamined cortical activation patterns associatedwith self-regulation elicited in response to emotion-ally evocative facial expressions in a sample of clin-ically anxious children.
Heightened neural activation in response to allemotional expressions
As hypothesized, anxious children had greater P1amplitudes in response to all emotion faces, relativeto comparison children, suggesting heightenedattention and/or arousal in response to the stimuli.Similarly, anxious children had greater frontal N2amplitudes than their age-matched peers, suggest-ing greater neural resources dedicated to responsemonitoring or inhibitory control. These findingssuggest that anxious children devoted moreresources to emotion regulation.
Activation differences for the P1 component werenot seen across emotion types for either group. Forthe comparison group, these findings are consistentwith previous findings that early perceptual compo-nents do not discriminate facial emotion among typ-ically developing children (Batty & Taylor, 2006;Todd, Lewis, Meusel, & Zelazo, 2008). However,counter to our hypotheses, N2 amplitudes differed byemotion type for the comparison group (greater
amplitudes in response to angry faces), but not forthe anxious group. These findings suggest that angryfaces induced greater neural activation in normalchildren to support cognitive control processes pre-sumed to regulate fear or anxiety. However, clinicallyanxious children appeared to sustain heightenedneural activation, as though they were engaged inprocesses of emotion regulation, regardless of stim-ulus valence (or objective threat). This may have been
(A)
(B)
(C)
Figure 5 ERN and CRN data. (A) Topography maps for compari-son and clinical groups 25 ms post-response. (B) Grand-averagedwaveforms at electrode Fz. (C) Mean ERN versus CRN activa-tion ± standard errors
558 Kathryn M. Hum, Katharina Manassis, and Marc D. Lewis J Child Psychol Psychiatry 2013; 54(5): 552–64
� 2012 The Authors. Journal of Child Psychology and Psychiatry � 2012 Association for Child and Adolescent Mental Health.

because all emotion faces were appraised as threat-ening or simply because they felt anxious throughoutthe experiment and were less sensitive to differencesin incoming perceptual information than non-anx-ious children. In either case, anxious children mayhave recruited cortical resources underpinningemotion regulation at high – perhaps maximal – lev-els, across all emotion face conditions. The findingthat medial prefrontal cortical activation is appar-ently indiscriminant during emotion regulation con-trasts with pediatric behavioral studies that reportthreat-related attention biases and adult ERP studiesthat report greater amplitudes in response tothreatening than non-threatening stimuli for anxiousindividuals (Aarts & Pourtois, 2010; Bar-Haim et al.,2005; Dennis & Chen, 2009; Kolassa & Miltner,2006; Mueller et al., 2009; Roy et al., 2008; Waterset al., 2010). This discrepancy may be attributed totask differences and/or age-related differences.Anxious adults may have developed more effectivecoping mechanisms and strategies than anxiouschildren, resulting in greater differences in neuralresponse patterns in relation to different emotionalstimuli. Anxious children may also have been moresensitive to the demands of the task, leading them toexperience heightened arousal (as evidenced by theP1) when withholding the Go response (as evidencedby the No-go N2). These findings are consistent withprevious pediatric behavioral and adult ERP studiesthat reveal an attentional bias and greater ERPamplitudes regardless of the emotional face type(Eldar et al., 2010; Muhlberger et al., 2009; Waterset al., 2008).
Heightened neural activation irrespective of trial orresponse type
No-go N2 amplitudes are often greater than Go N2amplitudes, as heightened neural activation is typi-cally shown when inhibiting the pre-potent (Go)motor response (Nieuwenhuis, Yeung, van den Wil-denberg, & Ridderinkhof, 2003). Comparison chil-dren exhibited this differential pattern of neuralactivation, but the anxious children did not. Simi-larly, ERN amplitudes are often greater than CRNamplitudes, as a heightened neural response fol-lowing error responses typically signals the need forgreater control over subsequent responses (Coles,Scheffers, & Holroyd, 2001; Falkenstein, Hoormann,Christ, & Hohnsbein, 2000). In the present study,the difference in ERN relative to CRN amplitudes wassimilar for both groups. However, clinical childrenhad greater CRN and ERN amplitudes relative tocomparison children. These data reveal that anxiouschildren engaged in heightened response monitoringprocesses following correct and incorrect responses.These findings are consistent with previous researchshowing greater ERN and CRN amplitudes in anx-ious than non-anxious individuals, perhaps becauseanxious individuals often experience pathological
levels of worry related to error sensitivity (Endrass,Klawohn, Schuster, & Kathmann, 2008; Hajcak,McDonald, & Simons, 2003b).
Neural activation predicting anxiety levels
The regression analyses revealed that for correct No-go trials, N2 amplitudes elicited in response to calmfaces were predictive of self-reported anxiety, withmore negative activation predicting increased anxi-ety. These findings suggest that neural responses tocalm, nonemotional faces (as opposed to negativelyor positively valenced faces) predicted anxiety levelsin children. These findings are consistent with pre-vious studies that report neutral faces perceived asbeing threatening (Mohlman et al., 2007; Yoon &Zinbarg, 2008). In summary, the neural activationpatterns of clinical children were indistinguishablebetween trial types and response types. Consistentwith the heightened neural activation and lack ofdiscrimination in response to all emotion types, itappears that low- as well as high-level situationaldemands required heightened levels of neural acti-vation in anxious children. These results suggest,once again, a style of emotion regulation character-ized by indiscriminate, over-generalized, and exces-sive efforts at self-monitoring or self-control, withlittle sensitivity to the actual features of stimuli andsituations.
LimitationsA primary limitation of this research was the rela-tively small sample size. Our clinical group was alsocomprised of children with different anxiety disor-ders, as well as children with comorbid types ofanxiety, which prevented us from isolating neuralmechanisms specific to a particular disorder. Hence,to increase confidence in our interpretations of thedata, replication with a larger sample and a morehomogeneous clinical group will be needed. Fur-thermore, neither puberty nor IQ was formally as-sessed. Next, the P1 has been shown to be influencedby stimulus characteristics such as luminance andcontrast (Rousselet, Husk, Bennett, & Sekuler, 2008;Vlamings, Goffaux, & Kemner, 2009). Although wecontrolled for luminance and hue between emotionconditions, it is possible that clinical and comparisongroups differed in light sensitivity (and therefore re-sponded differently to luminance characteristics)rather than attention and arousal. Future studiesmight examine this possibility. Next, the ERP com-ponents that we analyzed were selected carefully, butother components may also be relevant (e.g., thefrontal P3). We also acknowledge that competingtheories exist regarding what specific cognitive pro-cesses these ERP components represent (particularlyin regard to emotion regulation). Lastly, modelsdepicting the most convincing emotion expressionswere selected for inclusion in our go/no-go task.
doi:10.1111/j.1469-7610.2012.02609.x Neural mechanisms underlying childhood anxiety 559
� 2012 The Authors. Journal of Child Psychology and Psychiatry � 2012 Association for Child and Adolescent Mental Health.

However, some models were better at posing theemotional expressions than others. Further studiesare required using different sets of facial stimuli.
ConclusionsIn the present study, anxious children demonstratedheightened cortical activation patterns, elicited by allemotion face types, upon execution of Go and No-gotrial responses, and following both correct andincorrect responses. These findings suggest indis-criminately enhanced cortical activation patterns,which may underlie a rigid and ineffective style ofemotion regulation. To the best of our knowledge,this study is the first to examine cortical activationelicited in response to emotional facial stimuli in asample of clinically anxious children. Indiscriminateand heightened emotion regulation tendencies maypromote maladaptive behavior patterns that main-tain anxiety across development. For example,hypervigilance might affect anxious children’s abilityto learn and apply cognitive behavioral strategies,thus affecting treatment outcome. Future studies are
required to investigate changes in neural activationpatterns in response to treatment intervention and totest whether neural activation patterns can predicttreatment outcomes.
AcknowledgementsThe authors thank Dr. Maryanne Shaw for her hardwork and dedication in recruiting clinical families toparticipate in the study, and Alex Lamey for hisprogramming assistance. The present study wasfunded by grants from the Ontario Mental HealthFoundation (MDL) and the Natural Sciences andEngineering Research Council of Canada (KMH). Theauthors have declared that they have no competingor potential conflicts of interest.
Correspondence toKathryn M. Hum, University of Toronto, HumanDevelopment and Applied Psychology, 252 BloorStreet West, Toronto, ON M5S 1V6, Canada; Tel:+1 416 978-1003; Email: [email protected]
Key points
• Anxiety may influence early perceptual responses to emotional faces as well as later cognitive control pro-cesses. The present study examined the neural activation patterns tapping both perceptual and cognitiveprocessing in response to emotional faces in anxious children.
• Anxious children showed increased neural activation regardless of the emotional valence of the facial stimuli,and greater medial-frontal activity irrespective of task demands and response accuracy.
• These patterns of heightened neural activation may underlie the hypervigilant and indiscriminant regulatorystyle seen in clinically anxious children, providing further insights into the neurobiological mechanisms thatpromote and maintain childhood anxiety.
• Future studies might investigate the changes in neural activation patterns that occur in response to treatmentintervention and whether neural activation patterns can predict treatment outcomes.
ReferencesAarts, K., & Pourtois, G. (2010). Anxiety not only increases, but
also alters early error-monitoring functions. Cognitive, Affec-tive & Behavioral Neuroscience, 10, 479–492.
Achenbach, T. M. (1991). Manual for the child behaviorchecklist/4–18 and 1991 profile. Burlington, VT: Universityof Vermont, Department of Psychiatry.
Banaschewski, T., & Brandeis, D. (2007). Annotation: whatelectrical brain activity tells us about brain function thatother techniques cannot tell us – A child psychiatricperspective. Journal of Child Psychology and Psychiatry,48, 415–435.
Bar-Haim, Y., Lamy, D., & Glickman, S. (2005). Attentionalbias in anxiety: A behavioral and ERP study. Brain andCognition, 59, 11–22.
Batty, M., & Taylor, M. J. (2006). The development of emotionalface processing during childhood. Developmental Science, 9,207–220.
Bekker, E. M., Kenemans, J. L., & Verbaten, M. N. (2005).Source analysis of the N2 in a cued Go/NoGo task. BrainResearch. Cognitive Brain Research, 22, 221–231.
Bishop, S. J. (2007). Neurocognitive mechanisms of anxiety:An integrative account. Trends in Cognitive Sciences, 11,307–316.
Blair, R. J. (2003). Facial expressions, their communicatoryfunctions and neuro-cognitive substrates. PhilosophicalTransactions of the Royal Society of London. Series B,Biological Sciences, 358, 561–572.
Bokura, H., Yamaguchi, S., & Kobayashi, S. (2001). Electro-physiological correlates for response inhibition in a Go/NoGo task. Clinical Neurophysiology, 112, 2224–2232.
Breton, J. J., Bergeron, L., Valla, J. P., Berthiaume, C., Gaudet,N., Lambert, J., ... & Lepine, S. (1999). Quebec child mentalhealth survey: Prevalence of DSM-III-R mental health disor-ders. Journal of Child Psychology and Psychiatry, 40, 375–384.
Canino, G., Shrout, P. E., Rubio-Stipec, M., Bird, H. R., Bravo,M., Ramirez, R., ... & Martinez-Taboas, A. (2004). The DSM-IV rates of child and adolescent disorders in Puerto Rico:Prevalence, correlates, service use, and the effects of impair-ment. Archives of General Psychiatry, 61, 85–93.
Coles, M. G., Scheffers, M. K., & Holroyd, C. B. (2001). Why isthere an ERN/Ne on correct trials? Response representa-tions, stimulus-related components, and the theory of error-processing Biological Psychology, 56, 173–189.
Compton, R. J., Carp, J., Chaddock, L., Fineman, S. L.,Quandt, L. C., & Ratliff, J. B. (2007). Anxiety and errormonitoring: Increased error sensitivity or altered expecta-tions? Brain and Cognition, 64, 247–256.
560 Kathryn M. Hum, Katharina Manassis, and Marc D. Lewis J Child Psychol Psychiatry 2013; 54(5): 552–64
� 2012 The Authors. Journal of Child Psychology and Psychiatry � 2012 Association for Child and Adolescent Mental Health.

De Pauw, S. S., & Mervielde, I. (2010). Temperament, person-ality and developmental psychopathology: A review based onthe conceptual dimensions underlying childhood traits.Child Psychiatry and Human Development, 41, 313–329.
Dennis, T. A. (2010). Neurophysiological markers for childemotion regulation from the perspective of emotion-cogni-tion integration: Current directions and future challenges.Developmental Neuropsychology, 35, 212–230.
Dennis, T. A., & Chen, C. C. (2009). Trait anxiety and conflictmonitoring following threat: An ERP study. Psychophysiol-ogy, 46, 122–131.
Donkers, F. C., & van Boxtel, G. J. (2004). The N2 in go/no-gotasks reflects conflict monitoring not response inhibition.Brain and Cognition, 56, 165–176.
Eimer, M., & Holmes, A. (2002). An ERP study on the timecourse of emotional face processing. Neuroreport, 13, 427–431.
Eldar, S., Yankelevitch, R., Lamy, D., & Bar-Haim, Y. (2010).Enhanced neural reactivity and selective attention to threatin anxiety. Biological Psychology, 85, 252–257.
Endrass, T., Klawohn, J., Schuster, F., & Kathmann, N.(2008). Overactive performance monitoring in obsessive-compulsive disorder: ERP evidence from correct and erro-neous reactions. Neuropsychologia, 46, 1877–1887.
Falkenstein, M., Hohnsbein, J., Hoormann, J., & Blanke, L.(1991). Effects of crossmodal divided attention on late ERPcomponents. II. Error processing in choice reaction tasks.Electroencephalography and Clinical Neurophysiology, 78,447–455.
Falkenstein, M., Hoormann, J., Christ, S., & Hohnsbein, J.(2000). ERP components on reaction errors and their func-tional significance: A tutorial. Biological Psychology, 51, 87–107.
Folstein, J. R., & Van Petten, C. (2008). Influence of cognitivecontrol and mismatch on the N2 component of the ERP: Areview. Psychophysiology, 45, 152–170.
Ford, T., Goodman, R., & Meltzer, H. (2003). The British Childand Adolescent Mental Health Survey 1999: The prevalenceof DSM-IV disorders. Journal of the American Academy ofChild and Adolescent Psychiatry, 42, 1203–1211.
Gehring, W. J., Goss, B., Coles, M. G. H., Meyer, D. E., &Donchin, E. (1993). A neural system for error detection andcompensation. Psychological Science, 4, 385–390.
Hajcak, G., McDonald, N., & Simons, R. F. (2003a). Anxietyand error-related brain activity. Biological Psychology, 64,77–90.
Hajcak, G., McDonald, N., & Simons, R. F. (2003b). To err isautonomic: Error-related brain potentials, ANS activity, andpost-error compensatory behavior. Psychophysiology, 40,895–903.
Hewitt, P. L., Caelian, C. F., Flett, G. L., Sherry, S. B., Collins,L., & Flynn, C. A. (2002). Perfectionism in children: Associ-ations with depression, anxiety, and anger. Personality andIndividual Differences, 32, 1049–1061.
Hillyard, S. A., Vogel, E. K., & Luck, S. J. (1998). Sensory gaincontrol (amplification) as a mechanism of selective attention:electrophysiological and neuroimaging evidence. Philosoph-ical Transactions of the Royal Society of London. Series B,Biological sciences, 353, 1257–1270.
Hirshfeld-Becker, D. R., Micco, J. A., Simoes, N. A., & Henin, A.(2008). High risk studies and developmental antecedents ofanxiety disorders. American Journal of Medical Genetics.Part C, Seminars in Medical Genetics, 148C, 99–117.
Hoeksma, J. B., Oosterlaan, J., & Schipper, E. M. (2004).Emotion regulation and the dynamics of feelings: A concep-tual and methodological framework. Child Development, 75,354–360.
Holmes, A., Nielsen, M. K., & Green, S. (2008). Effects ofanxiety on the processing of fearful and happy faces: Anevent-related potential study. Biological Psychology, 77,159–173.
Hum, K. M., & Lewis, M. D. (in press). Neural mechanisms ofemotion regulation in children: Implications for normativedevelopment and emotion-related disorders. In K. C. Barrett,N. A. Fox, G. A. Morgan, D. Fidler, & L. Daunhauer (Eds.),Handbook of self-regulatory processes in development: Newdirections and international perspectives. Taylor & Francis,Inc.
Kolassa, I. T., & Miltner, W. H. (2006). Psychophysiologicalcorrelates of face processing in social phobia. Brain Re-search, 1118, 130–141.
Kovacs, M. (1992). Children’s depression inventory (CDI). NewYork: Multi-health Systems, Inc.
Ladouceur, C. D., Dahl, R. E., Birmaher, B., Axelson, D. A., &Ryan, N. D. (2006). Increased error-related negativity(ERN) in childhood anxiety disorders: ERP and sourcelocalization. Journal of Child Psychology and Psychiatry,47, 1073–1082.
Ladouceur, C. D., Dahl, R. E., Williamson, D. E., Birmaher, B.,Axelson, D. A., Ryan, N. D., & Casey, B. J. (2006). Processingemotional facial expressions influences performance on aGo/NoGo task in pediatric anxiety and depression. Journalof Child Psychology and Psychiatry, 47, 1107–1115.
Lewinsohn, P. M., Hops, H., Roberts, R. E., Seeley, J. R., &Andrews, J. A. (1993). Adolescent psychopathology: I. Prev-alence and incidence of depression and other DSM-III-Rdisorders in high school students. Journal of AbnormalPsychology, 102, 133–144.
Lewis, M. D., Lamm, C., Segalowitz, S. J., Zelazo, P. D., &Stieben, J. (2006). Neurophysiological correlates of emotionregulation in children and adolescents. Journal of CognitiveNeuroscience, 18, 430–443.
March, J. (1998). Multidimensional anxiety scale for children(MASC). Toronto, Canada: Multi-Health Systems, Inc.
McDermott, J. M., Perez-Edgar, K., Henderson, H. A., Chronis-Tuscano, A., Pine, D. S., & Fox, N. A. (2009). A history ofchildhood behavioral inhibition and enhanced responsemonitoring in adolescence are linked to clinical anxiety.Biological Psychiatry, 65, 445–448.
Meyer, A., Weinberg, A., Klein, D. N., & Hajcak, G. (2012). Thedevelopment of the error-related negativity (ERN) and itsrelationship with anxiety: Evidence from 8 to 13 year-olds.Developmental Cognitive Neuroscience, 2, 152–161.
Mohlman, J., Carmin, C. N., & Price, R. B. (2007). Jumping tointerpretations: Social anxiety disorder and the identifica-tion of emotional facial expressions. Behaviour Research andTherapy, 45, 591–599.
Mueller, E. M., Hofmann, S. G., Santesso, D. L., Meuret, A. E.,Bitran, S., & Pizzagalli, D. A. (2009). Electrophysiologicalevidence of attentional biases in social anxiety disorder.Psychological Medicine, 39, 1141–1152.
Muhlberger, A., Wieser, M. J., Herrmann, M. J., Weyers, P.,Troger, C., & Pauli, P. (2009). Early cortical processing ofnatural and artificial emotional faces differs between lowerand higher socially anxious persons. Journal of NeuralTransmission, 116, 735–746.
Nieuwenhuis, S., Yeung, N., van den Wildenberg, W., &Ridderinkhof, K. R. (2003). Electrophysiological correlatesof anterior cingulate function in a go/no-go task: Effects ofresponse conflict and trial type frequency. Cognitive, Affec-tive & Behavioral Neuroscience, 3, 17–26.
Ohman, A. (2002). Automaticity and the amygdala: Noncon-scious responses to emotional faces. Current Directions inPsychological Science, 11, 62–66.
Ohman, A. (2009). Of snakes and faces: An evolutionaryperspective on the psychology of fear. Scandinavian Journalof Psychology, 50, 543–552.
Olvet, D. M., & Hajcak, G. (2008). The error-related negativity(ERN) and psychopathology: Toward an endophenotype. ClinPsychol Rev, 28, 1343–1354.
Perez-Edgar, K., Bar-Haim, Y., McDermott, J. M., Chronis-Tuscano, A., Pine, D. S., & Fox, N. A. (2010). Attention biases
doi:10.1111/j.1469-7610.2012.02609.x Neural mechanisms underlying childhood anxiety 561
� 2012 The Authors. Journal of Child Psychology and Psychiatry � 2012 Association for Child and Adolescent Mental Health.

to threat and behavioral inhibition in early childhood shapeadolescent social withdrawal. Emotion, 10, 349–357.
Pine, D. S., Helfinstein, S. M., Bar-Haim, Y., Nelson, E., & Fox,N. A. (2009). Challenges in developing novel treatments forchildhood disorders: Lessons from research on anxiety.Neuropsychopharmacology, 34, 213–228.
Righi, S., Mecacci, L., & Viggiano, M. P. (2009). Anxiety,cognitive self-evaluation and performance: ERP correlates.Journal of Anxiety Disorders, 23, 1132–1138.
Rousselet, G. A., Husk, J. S., Bennett, P. J., & Sekuler, A. B.(2008). Time course and robustness of ERP object and facedifferences.Journal of Vision, 8, 3 1–18.
Roy, A. K., Vasa, R. A., Bruck, M., Mogg, K., Bradley, B. P.,Sweeney, M., ... & Pine, D. S (2008). Attention bias towardthreat in pediatric anxiety disorders. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 47, 1189–1196.
Santesso, D. L., Segalowitz, S. J., & Schmidt, L. A. (2006).Error-related electrocortical responses are enhanced inchildren with obsessive-compulsive behaviors. Developmen-tal Neuropsychology, 29, 431–445.
Sehlmeyer, C., Konrad, C., Zwitserlood, P., Arolt, V., Falken-stein, M., & Beste, C. (2010). ERP indices for responseinhibition are related to anxiety-related personality traits.Neuropsychologia, 48, 2488–2495.
Silverman, W.K., & Albano, A. M. (1996). The Anxiety disordersinterview schedule for DSM-IV-Child and parent versions.San Antonio, TX: Graywind Publications, A Division of ThePsychological Corporation.
Spielberger, C. D. (1973). The state-trait anxiety inventory forchildren (STAIC). San Antonio, TX: The Psychological Corpo-ration.
Stieben, J., Lewis, M. D., Granic, I., Zelazo, P. D., & Segalowitz,S. J. (2007). Neurophysiological mechanisms of emotionregulation for subtypes of externalizing children. Develop-ment and Psychopathology, 19, 455–480.
Thompson, R. A. (1994). Emotion regulation: A theme insearch of definition. The development of emotion regula-tion: Biological and behavioral considerations. Monographsof the Society for Research in Child Development, 59, 25–52.
Todd, R. M., Lewis, M. D., Meusel, L. A., & Zelazo, P. D. (2008).The time course of social-emotional processing in earlychildhood: ERP responses to facial affect and personalfamiliarity in a Go-Nogo task. Neuropsychologia, 46, 595–613.
Tottenham, N., Hare, T. A., & Casey, B. J. (2011). Behavioralassessment of emotion discrimination, emotion regulation,and cognitive control in childhood, adolescence, and adult-hood. Frontiers in Psychology, 2, 39.
Tottenham, N., Tanaka, J. W., Leon, A. C., McCarry, T., Nurse,M., Hare, T. A., ... & Nelson, C. (2009). The NimStim set offacial expressions: Judgments from untrained researchparticipants. Psychiatry Research, 168, 242–249.
van Veen, V., & Carter, C. S. (2002). The anterior cingulate as aconflict monitor: fMRI and ERP studies. Physiology &Behavior, 77, 477–482.
Vlamings, P. H., Goffaux, V., & Kemner, C. (2009). Is the earlymodulation of brain activity by fearful facial expressionsprimarily mediated by coarse low spatial frequency informa-tion? Journal of Vision, 9, 12 11–13.
Waters, A. M., Henry, J., Mogg, K., Bradley, B. P., & Pine, D. S.(2010). Attentional bias towards angry faces in childhoodanxiety disorders. Journal of Behavior Therapy and Exper-imental Psychiatry, 41, 158–164.
Waters, A. M., Mogg, K., Bradley, B. P., & Pine, D. S. (2008).Attentional bias for emotional faces in children with gener-alized anxiety disorder. Journal of the American Academy ofChild and Adolescent Psychiatry, 47, 435–442.
Waters, A. M., & Valvoi, J. S. (2009). Attentional bias foremotional faces in paediatric anxiety disorders: An investiga-
tion using the emotional Go/No Go task. Journal of BehaviorTherapy and Experimental Psychiatry, 40, 306–316.
Weems, C. F., Costa, N. M., Watts, S. E., Taylor, L. K., &Cannon, M. F. (2007). Cognitive errors, anxiety sensitivity,and anxiety control beliefs: Their unique and specificassociations with childhood anxiety symptoms. BehaviorModification, 31, 174–201.
White, L. K., Suway, J. G., Pine, D. S., Bar-Haim, Y., & Fox, N.A. (2011). Cascading effects: The influence of attention biasto threat on the interpretation of ambiguous information.Behaviour Research and Therapy, 49, 244–251.
Yoon, K. L., & Zinbarg, R. E. (2008). Interpreting neutral facesas threatening is a default mode for socially anxiousindividuals. Journal of Abnormal Psychology, 117, 680–685.
Accepted for publication: 11 July 2012Published online: 10 October 2012
AppendixExclusion criteria
To ensure an updated assessment of the child’sclinical symptomatology, children who were referredfrom the anxiety disorders clinic and who were ratedwithin the clinical range (T-score > 63) of the CBCLinternalizing scale were included in the clinical group(n = 29). Children who were recruited from the com-munity and who were rated within the normal rangeof the CBCL internalizing scale (T-score < 60) wereincluded in the normative comparison group (n = 34).Table A1 presents the child characteristics for allparticipants excluded from the study analyses. Oneclinical participant was excluded due to age (<8 yearsof age). Twelve clinical participants scored below theclinical cutoff on the CBCL internalizing scale, whilefour comparison participants scored above the nor-mal range. These participants were excluded fromfurther analyses. Due to technical difficulties, usableEEG was not available for four (clinical) participants,while insufficient trial counts (i.e., fewer than 10correct No-go trials for each emotion condition) re-sulted in one clinical and three comparison childrenbeing excluded from all analyses. Table A2 presentsthe average trial counts by emotion for each group.
Medication
Three clinical participants were taking medication atthe time of data acquisition (two children were takingmethylphenidate and one child was taking fluoxe-tine). Statistical analyses were conducted with thesethree clinical participants removed, and the sameresults were obtained.
EEG task
Children were given a practice block of 20 trials atthe start of each half to ensure proficiency with thetask. Practice blocks used a different model set withneutral facial expressions only. The task was pro-grammed with a response-duration algorithm that
562 Kathryn M. Hum, Katharina Manassis, and Marc D. Lewis J Child Psychol Psychiatry 2013; 54(5): 552–64
� 2012 The Authors. Journal of Child Psychology and Psychiatry � 2012 Association for Child and Adolescent Mental Health.

adjusted to each child’s skill level to provide thesame level of challenge for participants at all ages.The online adaptive algorithm allowed a set errorrate to be maintained for No-go trials. To achieve atarget No-go error rate of approximately 25%, theresponse-duration algorithm was adjusted so thatthe task would slow down if the participant achievedan error rate above this level, or the task would speedup with an error rate below this level. The starting Goresponse window was set at 550 ms for all partici-pants. When participants were easily able to inhibitthe button press response on a No-go trial, the re-sponse time window was decreased by 50 ms forsubsequent Go trials. Alternatively, when childrenfailed to inhibit their response on a No-go trial, theresponse time window was increased by 150 ms forsubsequent Go trials. The response window for No-go trials was set 200 ms longer than the responsewindow for Go trials to ensure that the inhibited Goresponse was deliberate. The stimulus was pro-grammed to offset 200 ms following response exe-cution (for correct Go trials). Error feedback, a redsquare framing the stimulus, indicated an incorrectGo (error or omission) or incorrect No-go (error ofcommission) response. Feedback appeared 200 mspost error-response on No-go trials to avoid onsetwithin the time window of the ERN. A variable cleartime ranging from 400 to 800 ms concluded eachtrial. Responses made within 200 and 1200 ms wereincluded for analysis only as responses outside ofthis range were assumed to reflect nondeliberatebehaviour. It should also be noted that correct Gotrials (used for the correct Go N2 and CRN compo-nents) excluded late Go trials (i.e., responses thatoccurred during error feedback or within the cleartime) and forced Go trials (i.e., Go trials that led eachblock or followed each No-go trial).
EEG task stimuli
Since early, perceptual ERP components are influ-enced by stimulus characteristics, image statisticswere computed using the Image Processing Toolboxpackaged with Matlab 7.0. Luminance statisticswere derived from the average log luminance, whileHue was calculated using Matlab’s rgb2hsv function(Table A3). Multiple univariate ANOVAs failed to re-veal a significant effect between emotion conditions(p > .584).
EEG processing
All channels were referenced to Cz during recording.Data were filtered offline using an FIR band-passfilter with a low-pass frequency of 30 Hz and a high-pass frequency of 0.1 Hz. Filtered data were thensegmented into 800 ms epochs (i.e., 200 ms beforeand 600 ms after stimulus onset) or 600 ms epochs(i.e., 300 ms before and 300 ms after response exe-cution). Trials that contained ocular artefacts (eye-
blink threshold >150 lv and eye-movement thresh-old >100 lv), or non-ocular artefacts (threshold<1 lv or >200 lv) were marked bad using an auto-matic artefact detection tool (Netstation; ElectricalGeodesics Inc.). Next, approximately one-third of alltrials were randomly selected for manual artefactdetection to verify that artefacts were not missed orincorrectly identified. Trials that contained an eyeblink, eye movement or had more than 15 badchannels were removed from further analyses. Of theremaining trials, all bad channels were replaced byvalues interpolated using neighbouring channeldata. Individual participant data were averaged thenre-referenced against the average reference. Finally,stimulus-locked ERP data were baseline-correctedusing the 200-ms time period prior to stimulus on-set. For response-locked ERP components, a 200-mswindow from )300 to )100 ms before the responseonset served as the baseline.
EEG task behavioural data
Multiple mixed-model ANOVAs were conducted toexamine correct Go and incorrect No-go responsetimes. For correct Go response times, a significantlinear interaction effect was seen F(1,58) = 5.27,p = .025. These data suggest that clinical childrenresponded more quickly to happy faces, while con-trol children responded more slowly to happy faces.For error No-go response times, a significant qua-dratic interaction effect was revealed, F(1,58) = 4.35,p = .041. These data suggest that clinical childrenmade slower error responses to calm faces, whilecomparison children made faster error responses tocalm faces (Table A4).
Supplementary ERP analyses
To ensure that ERP differences seen in clinical chil-dren were specific to particular ERP components, theN170 component for correct No-go trials was analy-sed, scored as the maximal negative amplitude 150–300 ms poststimulus onset averaged across fourposterior electrode sites (Figure A1). A 2 (Group) · 3(Emotion type) mixed-model ANOVA failed to reveal asignificant group effect F(1,57) = 2.60, p = .112 (Ta-ble A5).
The parietal P2 component was also analysed forcorrect No-go trials, scored as the mean activation250–350 ms poststimulus onset, averaged acrossfour parietal electrode sites (Figure A1). A 2(Group) · 3 (Emotion type) mixed-model ANOVAfailed to reveal a significant effect of GroupF(1,57) = 1.86, p = .178 (Table A5). Taken together,P2 and N170 activation did not differ betweengroups, suggesting that the anxious group was notsimply more alert or cortically aroused nor were allERP components affected indiscriminately.
For the CRN, A 2 (Group) · 3 (Emotion type)mixed-model ANOVA revealed a significant effect of
doi:10.1111/j.1469-7610.2012.02609.x Neural mechanisms underlying childhood anxiety 563
� 2012 The Authors. Journal of Child Psychology and Psychiatry � 2012 Association for Child and Adolescent Mental Health.

emotion F(1,55) = 6.59, p = .013, a significant effectof group F(1,55) = 10.88, p = .002, but a nonsignifi-cant interaction effect F(1,55) = 0.62, p = .434 (TableA5). These data suggest that greater neural activitywas seen following correct responses to angry faces,and clinical children had greater activation followingexecution of a correct response relative to compari-son children.
Figure A1: Montage used to examine N170 andparietal P2 activation levels
Table A1 Child characteristics for excluded participants
Clinical group(n = 18)
Comparisongroup (n = 7)
Age (years) 10.06 (1.09) 9.63 (1.24)Gender (M:F) 9:9 5:2CBCL internalizingscale T-score
60.28 (11.92) 56.29 (12.18)
MASC total scaleT-score
55.56 (11.49) 53.14 (7.76)
STAIC S-anxietyscale T-Score
50.83 (11.75) 45.86 (15.88)
CDI total T-score 49.72 (12.35) 47.00 (9.09)Anxiety disorderdiagnosis (n)GAD only 6SOC only 1SEP only 0SOC & SEP 1GAD & SOC 2GAD & SEP 5GAD, SOC & SEP 1Unknown 2
GAD, generalized anxiety disorder; SOC, social anxiety disor-der; SEP, separation anxiety disorder.
Table A2 Average trial counts used in the ERP analyses
Clinical group(n = 29)
Comparisongroup (n = 34)
Correct no-go trial countAngry 19.83 (3.35) 19.29 (3.86)Calm 19.59 (3.63) 19.00 (4.04)Happy 20.28 (3.73) 19.32 (4.39)
Correct go trial countAngry 23.55 (3.90) 23.62 (5.02)Calm 22.93 (5.72) 23.97 (6.08)Happy 22.52 (5.12) 22.85 (5.70)
Correct responsenegativity trial count
69.14 (12.15) 69.88 (14.14)
Error related negativitytrial count
21.59 (4.27) 23.85 (4.87)
Table A3 EEG task stimuli characteristics
Angry(n = 32)
Calm(n = 32)
Happy(n = 32) p-value
Image propertiesLuminance 1.76 (0.22) 1.77 (0.23) 1.75 (0.24) .968Hue 6.56 (0.42) 6.55 (0.41) 6.46 (0.41) .584
Table A4 EEG task behavioural data for clinical and compari-son children
Clinical group(n = 29)
Comparison group(n = 34)
Go response time (ms)Angry 431.63 (47.55) 437.12 (62.10)Calm 425.74 (43.22) 436.48 (62.84)Happy 424.58 (42.39) 445.44 (65.88)
Error no-go response time (ms)Angry 378.77 (56.16) 384.90 (80.01)Calm 394.11 (63.70) 367.49 (55.58)Happy 371.80 (51.22) 377.57 (67.82)
Table A5 Supplementary ERP analyses
Clinical group(n = 29)
Comparison group(n = 34)
Parietal P2Angry 2.85 (2.80) 1.84 (2.30)Calm 3.29 (2.75) 2.59 (2.57)Happy 3.08 (2.52) 2.44 (2.40)
N170 amplitudesAngry )0.09 (4.28) )1.46 (3.24)Calm 0.55 (4.47) )0.76 (4.38)Happy 0.51 (4.22) )1.32 (3.42)
Correct response negativityAngry )2.35 (3.18) )0.81 (2.86)Calm )1.95 (3.16) 0.05 (2.63)Happy )1.71 (2.36) 0.08 (3.21)
564 Kathryn M. Hum, Katharina Manassis, and Marc D. Lewis J Child Psychol Psychiatry 2013; 54(5): 552–64
� 2012 The Authors. Journal of Child Psychology and Psychiatry � 2012 Association for Child and Adolescent Mental Health.

Copyright of Journal of Child Psychology & Psychiatry is the property of Wiley-Blackwell and its content may
not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written
permission. However, users may print, download, or email articles for individual use.
Related Documents