Neural correlates of working memory dysfunction in first-episode schizophrenia patients: An fMRI multi-center study Frank Schneider a,b, ⁎ , Ute Habel a , Martina Reske a , Thilo Kellermann a , Tony Stöcker c , N. Jon Shah b,c , Karl Zilles b,c , Dieter F. Braus d,1 , Andrea Schmitt d,2 , Ralf Schlösser e,f , Michael Wagner g , Ingo Frommann g , Tilo Kircher a,h , Alexander Rapp h , Eva Meisenzahl i , Sandra Ufer i , Stephan Ruhrmann j , Renate Thienel a,k , Heinrich Sauer f , Fritz A. Henn d,3 , Wolfgang Gaebel l a Department of Psychiatry and Psychotherapy, RWTH Aachen University, Pauwelsstr. 30, 52074 Aachen, Germany b Brain Imaging Center West (BICW), Research Center Jülich, Germany c Institute of Neuroscience and Biophysics 3 - Medicine, Research Center Jülich, Germany d Central Institute of Mental Health, Mannheim, Germany e Department of Psychiatry and Psychotherapy, University of Mainz, Germany f Department of Psychiatry and Psychotherapy, University of Jena, Germany g Department of Psychiatry and Psychotherapy, University of Bonn, Germany h Department of Psychiatry and Psychotherapy, University of Tübingen, Germany i Department of Psychiatry and Psychotherapy, University of Munich, Germany j Department of Psychiatry and Psychotherapy, University of Cologne, Germany k Department of Psychiatry and Psychotherapy, University of Essen, Germany l Department of Psychiatry and Psychotherapy, University of Düsseldorf, Germany Received 2 August 2005; received in revised form 16 July 2006; accepted 23 July 2006 Available online 28 September 2006 Abstract Working memory dysfunction is a prominent impairment in patients with schizophrenia. Our aim was to determine cerebral dysfunctions by means of functional magnetic resonance imaging (fMRI) in a large sample of first-episode schizophrenia patients during a working memory task. 75 first-episode schizophrenia patients and 81 control subjects, recruited within a multi-center study, performed 2- and 0-back tasks while brain activation was measured with fMRI. In order to guarantee comparability between data quality from different scanners, we developed and adopted a standardized, fully automated quality assurance of scanner hard- and software as well as a measure for in vivo data quality. After these quality-control measures had been implemented, 48 patients and 57 controls were included in the final analysis. During attention-related processes, even when the performance between patients and controls was comparable, there was a recognizable emergence of cerebral dysfunctions with hypoactivations in the ventrolateral prefrontal cortex (VLPFC), in the Schizophrenia Research 89 (2007) 198 – 210 www.elsevier.com/locate/schres ⁎ Corresponding author. Department of Psychiatry and Psychotherapy, RWTH Aachen University, Pauwelsstr. 30, 52074 Aachen, Germany. Tel.: +49 241 80 89632; fax: +49 241 80 82401. E-mail address: [email protected] (F. Schneider). 1 Present address: Dr. Horst Schmidt Klinik, Hospital for Psychiatry and Psychotherapy, Wiesbaden. 2 Present address: Department of Psychiatry, University of Göttingen. 3 Present address: Brookhaven National Laboratory, New York, USA. 0920-9964/$ - see front matter © 2006 Elsevier B.V. All rights reserved. doi:10.1016/j.schres.2006.07.021

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

89 (2007) 198–210www.elsevier.com/locate/schres
Schizophrenia Research
Neural correlates of working memory dysfunction in first-episodeschizophrenia patients: An fMRI multi-center study
Frank Schneider a,b,⁎, Ute Habel a, Martina Reske a, Thilo Kellermann a, Tony Stöcker c,N. Jon Shah b,c, Karl Zilles b,c, Dieter F. Braus d,1, Andrea Schmitt d,2, Ralf Schlösser e,f,
Michael Wagner g, Ingo Frommann g, Tilo Kircher a,h, Alexander Rapp h,Eva Meisenzahl i, Sandra Ufer i, Stephan Ruhrmann j, Renate Thienel a,k,
Heinrich Sauer f, Fritz A. Henn d,3, Wolfgang Gaebel l
a Department of Psychiatry and Psychotherapy, RWTH Aachen University, Pauwelsstr. 30, 52074 Aachen, Germanyb Brain Imaging Center West (BICW), Research Center Jülich, Germany
c Institute of Neuroscience and Biophysics 3 - Medicine, Research Center Jülich, Germanyd Central Institute of Mental Health, Mannheim, Germany
e Department of Psychiatry and Psychotherapy, University of Mainz, Germanyf Department of Psychiatry and Psychotherapy, University of Jena, Germanyg Department of Psychiatry and Psychotherapy, University of Bonn, Germany
h Department of Psychiatry and Psychotherapy, University of Tübingen, Germanyi Department of Psychiatry and Psychotherapy, University of Munich, Germanyj Department of Psychiatry and Psychotherapy, University of Cologne, Germanyk Department of Psychiatry and Psychotherapy, University of Essen, Germany
l Department of Psychiatry and Psychotherapy, University of Düsseldorf, Germany
Received 2 August 2005; received in revised form 16 July 2006; accepted 23 July 2006Available online 28 September 2006
Abstract
Working memory dysfunction is a prominent impairment in patients with schizophrenia. Our aim was to determine cerebraldysfunctions by means of functional magnetic resonance imaging (fMRI) in a large sample of first-episode schizophrenia patientsduring a working memory task.
75 first-episode schizophrenia patients and 81 control subjects, recruited within a multi-center study, performed 2- and 0-backtasks while brain activation was measured with fMRI. In order to guarantee comparability between data quality from differentscanners, we developed and adopted a standardized, fully automated quality assurance of scanner hard- and software as well as ameasure for in vivo data quality. After these quality-control measures had been implemented, 48 patients and 57 controls wereincluded in the final analysis.
During attention-related processes, even when the performance between patients and controls was comparable, there was arecognizable emergence of cerebral dysfunctions with hypoactivations in the ventrolateral prefrontal cortex (VLPFC), in the
⁎ Corresponding author. Department of Psychiatry and Psychotherapy, RWTH Aachen University, Pauwelsstr. 30, 52074 Aachen, Germany. Tel.:+49 241 80 89632; fax: +49 241 80 82401.
E-mail address: [email protected] (F. Schneider).1 Present address: Dr. Horst Schmidt Klinik, Hospital for Psychiatry and Psychotherapy, Wiesbaden.2 Present address: Department of Psychiatry, University of Göttingen.3 Present address: Brookhaven National Laboratory, New York, USA.
0920-9964/$ - see front matter © 2006 Elsevier B.V. All rights reserved.doi:10.1016/j.schres.2006.07.021

199F. Schneider et al. / Schizophrenia Research 89 (2007) 198–210
superior temporal cortex and in the thalamus. During working memory performance, parietal hypoactivations, especially in theprecuneus, were prominent and were accompanied by poorer performance in patients. A hyperfrontality emerged in the ventro-lateral prefrontal cortex. Hence, results point to a dysfunctional ventrolateral prefrontal–parietal network during working memoryin patients, suggesting impairments in basic functions such as retrieval, storage and maintenance.
The brain activation pattern of this large and significant sample of first-episode schizophrenia patients indicates an imbalancedsystem failing to adjust the amount of brain activity required in the cerebral network involved in attention and working memory.© 2006 Elsevier B.V. All rights reserved.
Keywords: Schizophrenia; First-episode; Working memory; Multi-center study; fMRI; n-back
1. Introduction
Working memory, comprising of the short-term stor-age of information and executive processes, is essentialfor sustaining adequate reactions and adaptations tochanging requirements of the environment. Several stud-ies have demonstrated working memory impairments inchronic (Honey et al., 2002) and first-episode (Lenczet al., 2003) schizophrenia patients.
Working memory has primarily been associated withactivation in the prefrontal and parietal cortex. Neuroi-maging studies in healthy humans have indicated that thedorsolateral prefrontal cortex (DLPFC) subsides over theprocesses of manipulative functions in working memorywhilst the ventrolateral prefrontal cortex is involved inencoding, maintenance and inhibition (Postle et al., 2000;D'Esposito et al., 1999). The implicated network issomewhat broader, as a recent meta-analysis of 24imaging studies identified further robust activation in thelateral premotor cortex, the dorsal cingulate and medialpremotor cortex, the frontal poles and medial and lateralposterior parietal cortex (Owen et al., 2005). Clearly, theDLPFC is of major relevance in this functional network,and it has been shown that its activity is load dependent,seemingly increasing with load; however, when workingmemory capacity is exceeded, both increases anddecreases in activation have been reported (Johnson etal., 2006; Jaeggi et al., 2003; Callicott et al., 1999). Theinterpretation of these discrepant findings is complicatedby the fact that less activation may be linked to betterperformance as a consequence of practice or worseperformance due to working memory demands aboveperformance capacity. Several models have thereforesuggested an inverted U-shape function to reflect therelationship between performance and DLPFC activa-tion. The increase in activation at higher loads is reversedto a decrease when cognitive load goes beyond workingmemory capacity (Manoach, 2003; Callicott et al., 2003;Johnson et al., 2006).
In schizophrenia, prefrontal cortex dysfunctions arewell known and have been reported as frontal hypo-
activation during rest as well as during tasks tapping thefrontal cortex (Weinberger and Berman, 1996). Examplesof such tasks include theWisconsin Card Sorting Test, butalso the Tower of London (Andreasen et al., 1992), verbalfluency (Fu et al., 2005), the Sternberg (Veltman et al.,2003) and the n-back task. However, hypofrontality is notalways present in schizophrenia; its presence depends onthe symptomatology, the task (Callicott et al., 1998; Carteret al., 1998; Curtis et al., 1999; Weinberger and Berman,1996) and the cognitive load.
During working memory, a prefrontal dysfunctionhas often been observed in schizophrenia patients; thishas varied in nature from hypofrontality (Barch et al.,2001; Jacobsen et al., 1997; Keshavan et al., 2002;Perlstein et al., 2003; Volz et al., 1999) to hyperfron-tality (Manoach et al., 1999, 2000). Furthermore, pa-tients sometimes exhibited no differences in frontalinvolvement (Honey et al., 2002; Kindermann et al.,2004), leaving the question of the exact nature andsignificance of the prefrontal dysfunction unanswered.Correspondingly, a review of fMRI findings on pre-frontal function in schizophrenia found evidence ofhypofrontality in only 60% of studies (Walter and Wolf,2002; Wolf et al., 2006). Although a number of in-fluencingmethodological factors have been identified anddiscussed (such as different tasks addressing divergentcognitive processes, differential motivational effects andperformance levels, illness parameters, etc.; Manoach,2003), a differential characterization of cerebral dysfunc-tions during working memory is still lacking. One hy-pothesis states that performance or cognitive load is thecrucial factor, as it was repeatedly found, that the invertedU-shape function may be shifted to the left (Manoach,2003) and may also be somewhat flatter (Johnson et al.,2006) indicating reduced load sensitivity in patients. Fur-thermore, decomposing the elements of working memoryretrieval may be more affected compared to encoding(Johnson et al., 2006).
Moreover, results mainly relied on small samples, sothat findings could not reliably be generalized. Althoughrandom effect modeling was mostly used, greater

200 F. Schneider et al. / Schizophrenia Research 89 (2007) 198–210
samples are more representative of the population andless influenced by outliers; statistically, sensitivity maybe increased by higher degrees of freedom. Glahn et al.(2005) concluded from their meta-analysis of 12 n-backstudies in schizophrenia patients two main points.Firstly, given the heterogeneity of schizophrenia patientsrelatively large well-characterized samples should beinvestigated. Secondly, although DLPFC hypoactiva-tion is a relatively consistent finding, dysfunctions arenot restricted to it, and there is a complex pattern ofhypo- and hyperactivations that should be considered inthe context of the larger network supporting the task,when making inferences on the neurobiological mech-anisms of schizophrenia.
Most likely, findings related to the hypo- or hyper-function of the prefrontal cortex in schizophrenia are botha valid demonstration of dysfunctions reflecting ineffi-cient processes and/or compensatory strategies in schizo-phrenia, which may be the result of an imbalanced systemattempting to cope differentially with task requirements.
For these reasons, we aimed to clarify thedysfunctional activation pattern during working mem-ory in schizophrenia by pursuing two objectives.Firstly, we focused on first-episode schizophreniapatients; hence, a relatively homogeneous samplewhere secondary effects due to the consequences ofa chronic illness course, such as social maladaptationand long-term medication, are minimal. Secondly, weused a multi-center approach with the uniquepossibility of pooling the data of a large number ofthese patients which would be virtually impossible inonly one center. Hence, results permit more general-ized conclusions based on the size and breadth of thesample as well as a conservative uniform dataanalysis. Although this methodological procedureholds its own risks and concerns, we believe theadvantages outweigh the problems. We attempted toaccount for the additional variance resulting fromincluding data from multiple centers with the devel-opment and use of rigorous quality control measures.Validity and significance of results benefit consider-ably from more homogeneous and sufficiently largeclinical samples where the same inclusion anddiagnostic criteria, measurements, tasks and analyseswere applied in a similar time frame. Patients andcontrols performed a 2-back and 0-back task duringfMRI measurements. This task was chosen since it isrelevant for the pathophysiology of the disease andhas been shown to discriminate reliably betweenpatients and controls. Furthermore, responses can beassessed most accurately during fMRI measurements.Our hypothesis was that indications of an imbalanced
system would be most prominent during higher taskdemands, i.e., the 2-back task. We further hypothe-sized that these indications would take the form of notonly frontal hypoactivations but also hyperactivationsin the underlying fronto-parieto-basal ganglia–cerebel-lar network relevant to working memory. However,since findings here are still relatively inconsistent, wedid not specify the direction of dysfunctions in theseregions.
2. Methods
2.1. Participants
Patients were recruited from the Psychiatry Depart-ments at the Universities of Düsseldorf, Bonn,Cologne, Essen, Jena, Mainz, Munich, Tübingen, aswell as from the Central Institute of Mental Health inMannheim where patients associated with the GermanResearch Network of Schizophrenia participated indifferent studies including the present fMRI study.FMRI measurements took place at the end of the firsthospitalization of each patient (6–8 weeks). Data from75 patients and 81 controls were collected. 48 patients(26 male, 22 female with a mean age of 31.0±9.9 years(range 18–55), mean education of 12.6±3.2 years (7–18) and mean parental education of 12.2±2.9 years (9–18)) and 57 controls (31 male, 26 female, mean age30.9±8.3 years (17–57), mean education 13.9±3.4 (8–18) and mean parental education 12.5±3.2 years (7.5–18)) fulfilled quality control criteria for further analysis(see below for procedure of quality control). Therewere no significant differences in age or educationbetween groups.
Patients were diagnosed with schizophrenia by ex-perienced clinical psychiatrists using a standardizedclinical interview (SCID; German Version, Wittchen etal., 1997; DSM IV; n=42 paranoid, n=2 disorganized,n=3 undifferentiated, n=1 schizophreniform disorder).Diagnoses were followed up over a period of 2 years,and as such, a possible change in the diagnosis of schi-zophrenia could be ruled out. Patients were medicated for66±53 days on average; mean age of onset was 29.1±9.8 years. Additional psychopathological ratings revealedslightly more negative (PANSS (Kay et al., 1987); 13.5±5.8 (7–30)) than positive symptoms (9.2±3.3 (7–21)) andmoderate general psychopathology (25.3±9.6 (16–61),inter-rater reliability r=0.74, PANSS positive score).Mean clinical global impression score was 3.2±1.2, meanglobal assessment of functioning (GAS) was 65.5±14.4and depressive symptoms were minimal (HAMD), 5.1±6.0. Since this study is part of the longitudinal studies

Fig. 1. (a) Quality control I. Top left: total percentage signal change(PSC) and its standard deviation. PSC describes the total amount ofrandom noise corrupting the data of that particular measurement. Bottomleft: Correlation coefficient R of the data quantiles and standard normalquantiles. R is a measure of coherent noise (artifacts). The differentcolours in the scatterplot mark the different centers. (b) Quality control II.Scatterplot of PSC distribution for patients and controls separately. Athreshold of 3.4 was empirically defined for exclusion of subjects withunacceptable data quality (non-task-related variance).
201F. Schneider et al. / Schizophrenia Research 89 (2007) 198–210
carried out by the ResearchNetwork, patients' medicationis double blind and presently unknown (risperidone vs.haloperidol). Exclusion criteria for patients were anypsychiatric comorbidity (DSM IV) and left-handedness,in addition to the usual exclusion criteria for MRI (metalimplants, neurological diseases, disorders which affectcerebral metabolism). Healthy controls were recruited viaadvertisements and were chosen for their similarity topatients with respect to age and parental education (so thatno significant differences emerged between groups). Theywere screened by comprehensive assessment proceduresand had no medical, neurological, or psychiatric history(DSM IV). They had no first-degree relatives withpsychiatric diseases. Urine drug screening (for opioids,methadone, amphetamines, or cannabinoids) before fMRImeasurements guaranteed inclusion with negative drugscreening only. After a complete description of the study,written informed consent was obtained. The local IRBsapproved the protocol, which is in accordance with theDeclaration of Helsinki.
2.2. Stimuli
The working memory task consisted of an n-backtask with a randomized sequence of 0-back and 2-backconditions arranged in a block design. Subjects viewedsingle letters (A–Z, red on a black background) inrandom order. Each letter appeared for 500 ms to whichsubjects had to react within 900 ms by pressing theresponse button (LUMItouch) for the target letter withtheir right index finger. The target probability for bothconditions was .37 with a ratio of 48 non-targets to 28targets. Baseline phases required the patient to simplyconcentrate on and fixate the sequence of letters (with-out any response required). During the 0-back task,subjects also saw a sequence of letters and had to respondto a target letter (X). The 2-back task required the patientto press the button when a letter occurred which matchedthe one presented two letters back. Stimulus presenta-tions were computerized (PRESENTATION or Experi-mental Run Time System, ERTS). Subjects wereinstructed in detail with task examples on a computerbefore the experiment started and again during the ex-periment with a single slide displaying the instructions(concentrate on the letters, press the button for each Xobserved, press the button if the letter presented twoletters back is the same). The paradigm was applied intwo runs with 99 whole brain acquisitions in each run, inwhich baseline (fixation) and activation blocks (0-backor 2-back) alternated. Each run included the same num-ber of 0-back (n=4) and 2-back (n=4) blocks and8 baselines of fixation, and had a duration of 8.25 min.
Each block lasted for 30 s and comprised of 6 wholebrain acquisitions.
2.3. Data acquisition
Cerebral activation was measured using fMRI, basedon Echo Planar Imaging (EPI) using BOLD contrast.FMRI brain images were acquired using Siemens andPhillips 1.5T MR scanners. The acquisition comprised ofa 3D data set (256×256×128 sagittal, FOV 230 mm,TE=4.4 ms, TR=11.4 ms, α=15°) and transaxial func-tional images (EPI, 64×64, 32 slices, FOV200×200mm2,voxel size: 3.125×3.125×3 mm3, TE=66 ms, TR=5 s,α=90°), covering the whole brain and positioned parallelto the intercomissural line (AC-PC).
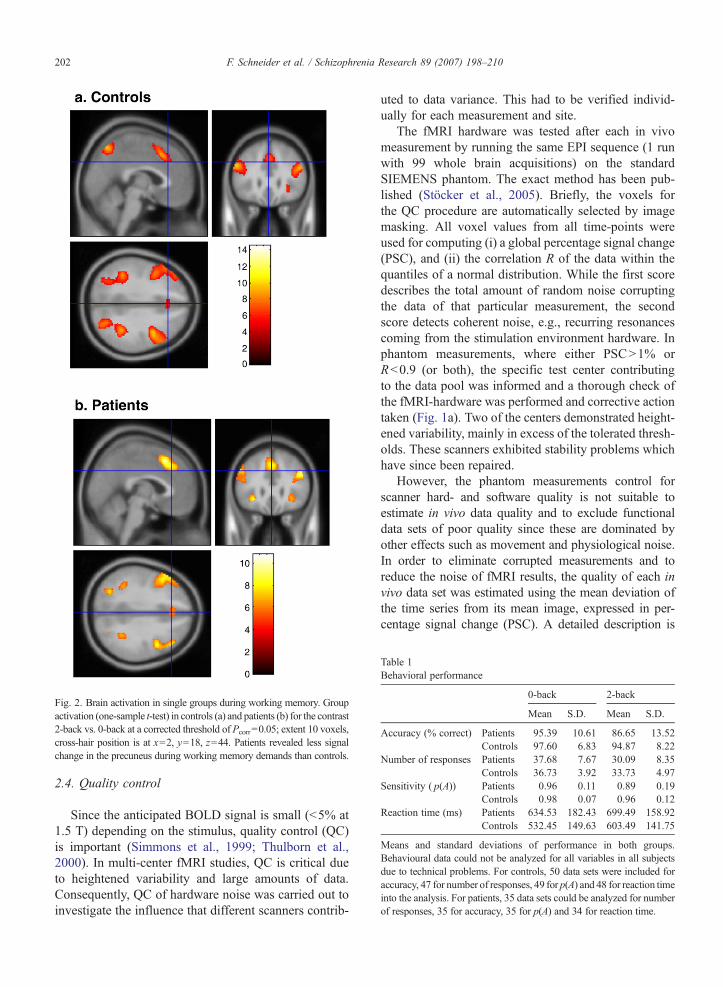
Fig. 2. Brain activation in single groups during working memory. Groupactivation (one-sample t-test) in controls (a) and patients (b) for the contrast2-back vs. 0-back at a corrected threshold of Pcorr=0.05; extent 10 voxels,cross-hair position is at x=2, y=18, z=44. Patients revealed less signalchange in the precuneus during working memory demands than controls.
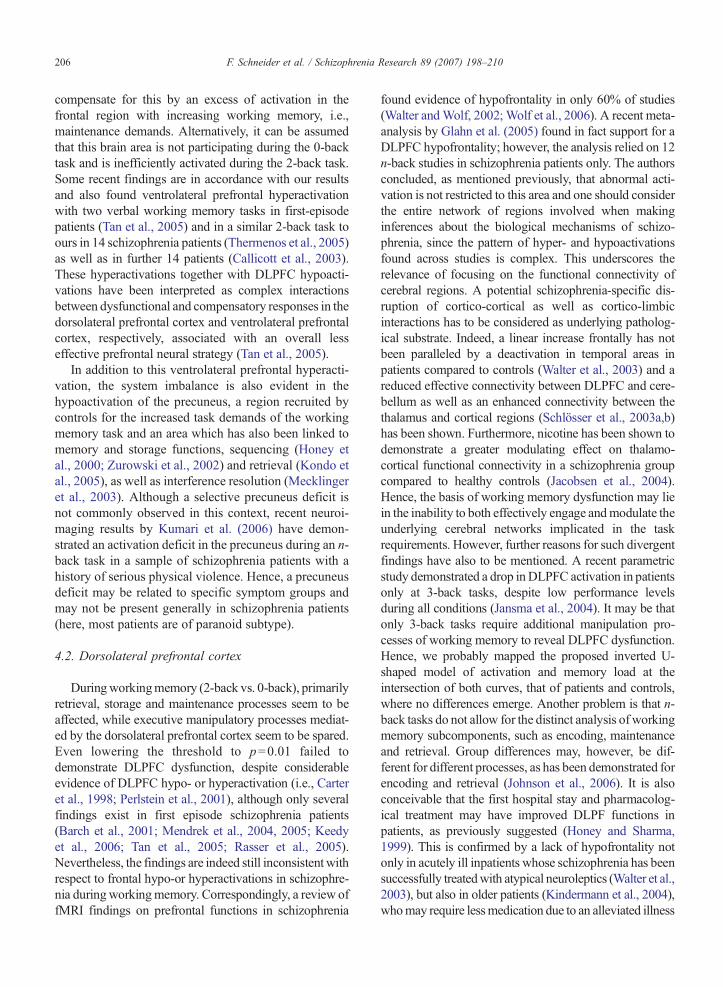
Table 1Behavioral performance
0-back 2-back
Mean S.D. Mean S.D.
Accuracy (% correct) Patients 95.39 10.61 86.65 13.52Controls 97.60 6.83 94.87 8.22
Number of responses Patients 37.68 7.67 30.09 8.35Controls 36.73 3.92 33.73 4.97
Sensitivity ( p(A)) Patients 0.96 0.11 0.89 0.19Controls 0.98 0.07 0.96 0.12
Reaction time (ms) Patients 634.53 182.43 699.49 158.92Controls 532.45 149.63 603.49 141.75
Means and standard deviations of performance in both groups.Behavioural data could not be analyzed for all variables in all subjectsdue to technical problems. For controls, 50 data sets were included foraccuracy, 47 for number of responses, 49 for p(A) and 48 for reaction timeinto the analysis. For patients, 35 data sets could be analyzed for numberof responses, 35 for accuracy, 35 for p(A) and 34 for reaction time.
202 F. Schneider et al. / Schizophrenia Research 89 (2007) 198–210
2.4. Quality control
Since the anticipated BOLD signal is small (b5% at1.5 T) depending on the stimulus, quality control (QC)is important (Simmons et al., 1999; Thulborn et al.,2000). In multi-center fMRI studies, QC is critical dueto heightened variability and large amounts of data.Consequently, QC of hardware noise was carried out toinvestigate the influence that different scanners contrib-
uted to data variance. This had to be verified individ-ually for each measurement and site.
The fMRI hardware was tested after each in vivomeasurement by running the same EPI sequence (1 runwith 99 whole brain acquisitions) on the standardSIEMENS phantom. The exact method has been pub-lished (Stöcker et al., 2005). Briefly, the voxels forthe QC procedure are automatically selected by imagemasking. All voxel values from all time-points wereused for computing (i) a global percentage signal change(PSC), and (ii) the correlation R of the data within thequantiles of a normal distribution. While the first scoredescribes the total amount of random noise corruptingthe data of that particular measurement, the secondscore detects coherent noise, e.g., recurring resonancescoming from the stimulation environment hardware. Inphantom measurements, where either PSCN1% orRb0.9 (or both), the specific test center contributingto the data pool was informed and a thorough check ofthe fMRI-hardware was performed and corrective actiontaken (Fig. 1a). Two of the centers demonstrated height-ened variability, mainly in excess of the tolerated thresh-olds. These scanners exhibited stability problems whichhave since been repaired.
However, the phantom measurements control forscanner hard- and software quality is not suitable toestimate in vivo data quality and to exclude functionaldata sets of poor quality since these are dominated byother effects such as movement and physiological noise.In order to eliminate corrupted measurements and toreduce the noise of fMRI results, the quality of each invivo data set was estimated using the mean deviation ofthe time series from its mean image, expressed in per-centage signal change (PSC). A detailed description is

Table 2SPM results for 0-back vs. baseline of fixation
Controls–patients Patients–controls
Side x y z k Maximum SPM{T}
Anatomical region Side x y z k Maximum SPM{T}
Anatomical region
R 26 6 −8 327 4.33 Ventrolateral prefrontalcortex
R 42 −26 48 114 4.32 Postcentral gyrus
L −28 20 −12 249 4.35 Ventrolateral prefrontalcortex
L −30 −42 66 92 3.81 Postcentral gyrus
R 50 −36 8 41 3.59 Superior temporal gyrus R 34 −34 68 26 3.47 Postcentral gyrusL −28 −34 0 45 3.85 Hippocampus R 50 −6 34 22 3.63 Precentral gyrusL −6 −4 −6 48 3.65 Thalamus R 6 −32 56 634 4.75 Paracentral
lobuleL −16 2 12 19 3.53 Caudate
MNI coordinates (x, y, z) of activation maxima (SPM{T} value) and extent of activated clusters (k) representing significant group differences (two-sample t-tests) between patients and controls during 0-back at p=0.001 with a cluster extent of at least 17 voxels. Results were masked to includeonly regions showing activations in both groups. The left side presents hypoactivations of patients (controls–patients), and the right side presentshyperactivations (patients–controls).
203F. Schneider et al. / Schizophrenia Research 89 (2007) 198–210
given by Stöcker et al. (2005). A threshold of PSCb3.4has been adopted as a tolerable degree of signal variation(Fig. 1b). The boundary for data exclusion was foundempirically and is strongly study-dependent. This wasiteratively determined by consecutively excluding sub-jects with high PSC values in their time series in order tomaximize the statistical power of group differences (asdetermined by the maximum F-statistic of the respectivetwo-sample t-tests) within a voxel-based analysis. At thesame time, data quality across groups has been kept equalto avoid serious misinterpretation of results. Thisprocedure led to the exclusion of 27 patients and 24controls due to values above the given threshold.
2.5. Data analysis
2.5.1. Behavioral dataAccuracy (percent correct) was the main dependent
measure in this study. Number of responses, reactiontime and p(A) were also assessed. p(A), a performance
Table 3SPM results for 2-back vs. 0-back
Controls–patients Patie
Side x y z k Maximum SPM{T} Anatomical region Side
L −8 −70 54 729 4.90 Precuneus R
R 42 −28 46 94 4.30 Postcentral gyrus RR
MNI coordinates (x,y,z) of activation maxima (SPM{T} value) and extent ofsample t-tests) between patients and controls during the contrast 2-back vs. 0-bmasked to include only regions showing activations in both groups. The lefright side presents hyperactivations (patients–controls).
variable derived from signal detection theory andwithout parametric assumptions, was calculatedaccording to Grier's formula (Grier, 1971). p(A) issuperior to the usual measure of sensitivity (d′) whenonly a few trials are available. p(A) is related to therate of correct responses and similar to the betterknown d′ in that it measures discrimination ratherthan bias. The d′ index is calculated under theassumption of normal distributions with equal vari-ance. However, the p(A) index avoids makingdistributional assumptions. It is based on an estimateof the “average” area of possible receiver operatingcharacteristic (ROC). p(A) ranges from 0 to 1, with 1reflecting perfect detection and chance level at 0.5.Group differences were analyzed with separate two-way repeated-measure ANOVAs with between-subjectfactor group (patients, controls) and within-subjectfactor task (2-back, 0-back) for each variable. Post hoct-tests with adjusted p-values were performed todecompose significant effects.
nts–controls
x y z k Maximum SPM{T} Anatomical region
40 14 −12 55 3.71 Ventrolateral prefrontalcortex
36 −24 10 46 3.74 Insula44 −72 8 33 3.53 Middle occipital gyrus
activated clusters (k) representing significant group differences (two-ack at p=0.001 with a cluster extent of at least 17 voxels. Results weret side presents hypoactivations of patients (controls–patients), and the

204 F. Schneider et al. / Schizophrenia Research 89 (2007) 198–210
2.5.2. FMRIData analysis was performed using SPM2 (http://
www.fil.ion.ucl.ac.uk/spm). The first three images werediscarded. After realignment, co-registration, stereotaxicnormalization and smoothing (10 mm isotropic Gaussianfilter), statistical parametric maps were calculated sepa-rately for each subject using a delayed boxcar convolvedwith a hemodynamic response function. Contrast imagesfor each subject were created contrasting the 0-back andthe fixation baseline (attention processes) and the 2-backwith the 0-back condition (working memory). The groupanalysis was based on a random effect model, applyingone-sample t-test per group per contrast (Fig. 2, correctedthreshold at p=0.05). Between-group comparisons wereperformed on these contrasts with two-sample t-tests.
Fig. 3. Brain activation during working memory. Group differences in fMRp=0.001 (extent 17 voxel) representing (a) hypoactivations of patients cocontrols. (c) Illustration of hypoactivation of patients in the left precuneushyperactivation in the ventrolateral prefrontal cortex (x=40, y=16, z=−12,
Results were then masked with the respective contrast (0-back, 2-back vs. 0-back) to include only regions showingactivations in both groups ( p=0.05 uncorrected). In orderto correct for multiple comparisons within a searchvolume we applied a cluster extent threshold determinedby Monte Carlo simulations (Slotnick et al., 2003). For athreshold at the voxel level at 0.001 and spatial propertiesas present in this study, 10,000 simulations resulted in anextent threshold of 17 resampled voxels. This procedureprevented a false positive rate above 5% due to multipletesting. The analyses supported our hypothesis of theoften-reported frontal dysfunction in patients. Whilstchecking for differential behavioral performance inpatients and controls, we additionally performed anANCOVA with behavioral data as the covariate of no
I activation (two-sample t-test) for the contrast 2-back vs. 0-back atmpared to controls and (b) hyperactivations of patients compared to(x=−8, y=−70, z=54) for 2-back relative to 0-back (left side) andright side).

205F. Schneider et al. / Schizophrenia Research 89 (2007) 198–210
interest. Since results were practically identical to the two-sample t-tests, we relied on the latter for presentation.
3. Results
3.1. Behavioral data
The two-way ANOVA (group, task) for accuracyrevealed a significant main effect for group (F=6.70,df=1, 83, p=0.01), task (F=64.48, df=1, 83, p=0.0001)and a significant group×task interaction (F=17.66,df=1, 83, p=0.0001). For number of responses, a maineffect for task (F=57.53, df=1, 80, p=0.0001) and agroup×task interaction (F=10.82, df=1, 80, p=0.002)emerged. The same applied to p(A): task (F=39.53,df=1, 82, p=0.0001), group×task (F=9.22, df=1, 82,p=0.003). The ANOVA for reaction time demonstratedonly a main effect for group (F=8.26, df=1, 80, p=0.01)and task (F=101.56, df=1, 80, p=0.0001). Post hocanalyses showed that patients and controls differed during2-back only in accuracy ( padj=0.0008) and number ofresponses ( padj=0.02). Responses were faster in controlsthan in patients in 0-back ( padj=0.01) and 2-back( padj=0.01, Table 1).
3.2. FMRI data
Activation in single groups has been visualized inFig. 2. Since we focused on group differences, SPMactivation coordinates are reported for these group dif-ferences only. During low working memory load (0-back vs. baseline), hypoactivations in patients wereobserved in the bilateral VLPFC and the right superiortemporal gyrus as well as in the left thalamus, caudateand hippocampus. Hyperactivations were demonstratedby patients mainly in the bilateral postcentral and pre-central gyrus and the paracentral lobule (Table 2).
Looking at working memory load (2-back vs. 0-back), hypoactivations could be detected in the post-central gyrus and additionally in the precuneus. Hyper-activations were noted in the right VLPFC (inferiorfrontal cortex; Table 3, Figs. 2 and 3), the insula andmiddle occipital gyrus. Because we expected a hypo-frontality in patients, a lower threshold was adopted( p=0.01, uncorrected); however, there was no hypo-frontality observed even at this lower threshold.
4. Discussion
Considering the discrepant findings with respect to afrontal dysfunction in schizophrenia, our results areintriguing. First-episode schizophrenia patients were
characterized by very focal dysfunctions in parietal andventrolateral prefrontal regions during working memorydemands; these working memory demands were accom-panied by poorer performance. However, even the mereattentional demands of the 0-back task revealed ventro-lateral prefrontal, thalamic, caudate, hippocampal andsuperior temporal hypoactivations and hyperactivationsin the paracentral lobule, the postcentral and precentralgyrus, although a comparable behavioral accuracy (butslower response rate) could be observed in patients andcontrols. Interestingly, the crucial impairment in schizo-phrenia during attention and working memory demandsmay lie in the failure to produce an adequate amount ofactivation, especially in the ventrolateral prefrontal cor-tex. This suggests that a dysfunctional ventrolateralprefrontal–parietal network in working memory is al-ready present in the early stages of the illness.
4.1. Ventrolateral prefrontal cortex
During the simpler 0-back task, accuracy is equal inboth groups. However, this task seems to be of greaterdifficulty in schizophrenia patients as suggested byseveral indicators: the higher response times, the reducedactivity in ventrolateral prefrontal areas and an enhancedand hence probably compensatory activity in postcentraland precentral areas. The postcentral hyperactivation isnot characteristic for this task; however, it may be typicalof an aberrant activation pattern of patients as previouslydemonstrated in a similar context (Eyler et al., 2004;Kindermann et al., 2004). Further hypoactivations in thesuperior temporal gyrus (STG) are in accordance withrecent results of dysfunctions in this area during the Towerof London task in first-episode (Rasser et al., 2005) and inolder patients with schizophrenia (Kindermann et al.,2002) as well as after adjustment for performance dif-ferences (Thermenos et al., 2005). Similarly, thalamichypoactivations have also been observed (Andrews et al.,2006) in addition to striatal and hippocampal dysfunctions(Johnson et al., 2006). Interestingly, the ventrolateralprefrontal region which was hypoactivated duringattentional processes is in very close proximity to theventrolateral prefrontal region which was hyperactivatedduring working memory demands. The ventrolateralprefrontal cortex is involved in phonological storageand rehearsal functions as well as maintenance processingof working memory. Following the model of Smith andJonides (1998), the translation into phonological repre-sentations mediated by inferior frontal and superiortemporal regions seems to be dysfunctional in schizo-phrenia. It is conceivable that the system is alreadyinefficient at low task requirements and attempts to
206 F. Schneider et al. / Schizophrenia Research 89 (2007) 198–210
compensate for this by an excess of activation in thefrontal region with increasing working memory, i.e.,maintenance demands. Alternatively, it can be assumedthat this brain area is not participating during the 0-backtask and is inefficiently activated during the 2-back task.Some recent findings are in accordance with our resultsand also found ventrolateral prefrontal hyperactivationwith two verbal working memory tasks in first-episodepatients (Tan et al., 2005) and in a similar 2-back task toours in 14 schizophrenia patients (Thermenos et al., 2005)as well as in further 14 patients (Callicott et al., 2003).These hyperactivations together with DLPFC hypoacti-vations have been interpreted as complex interactionsbetween dysfunctional and compensatory responses in thedorsolateral prefrontal cortex and ventrolateral prefrontalcortex, respectively, associated with an overall lesseffective prefrontal neural strategy (Tan et al., 2005).
In addition to this ventrolateral prefrontal hyperacti-vation, the system imbalance is also evident in thehypoactivation of the precuneus, a region recruited bycontrols for the increased task demands of the workingmemory task and an area which has also been linked tomemory and storage functions, sequencing (Honey etal., 2000; Zurowski et al., 2002) and retrieval (Kondo etal., 2005), as well as interference resolution (Mecklingeret al., 2003). Although a selective precuneus deficit isnot commonly observed in this context, recent neuroi-maging results by Kumari et al. (2006) have demon-strated an activation deficit in the precuneus during an n-back task in a sample of schizophrenia patients with ahistory of serious physical violence. Hence, a precuneusdeficit may be related to specific symptom groups andmay not be present generally in schizophrenia patients(here, most patients are of paranoid subtype).
4.2. Dorsolateral prefrontal cortex
Duringworkingmemory (2-back vs. 0-back), primarilyretrieval, storage and maintenance processes seem to beaffected, while executive manipulatory processes mediat-ed by the dorsolateral prefrontal cortex seem to be spared.Even lowering the threshold to p=0.01 failed todemonstrate DLPFC dysfunction, despite considerableevidence of DLPFC hypo- or hyperactivation (i.e., Carteret al., 1998; Perlstein et al., 2001), although only severalfindings exist in first episode schizophrenia patients(Barch et al., 2001; Mendrek et al., 2004, 2005; Keedyet al., 2006; Tan et al., 2005; Rasser et al., 2005).Nevertheless, the findings are indeed still inconsistent withrespect to frontal hypo-or hyperactivations in schizophre-nia duringworkingmemory. Correspondingly, a review offMRI findings on prefrontal functions in schizophrenia
found evidence of hypofrontality in only 60% of studies(Walter andWolf, 2002; Wolf et al., 2006). A recent meta-analysis by Glahn et al. (2005) found in fact support for aDLPFC hypofrontality; however, the analysis relied on 12n-back studies in schizophrenia patients only. The authorsconcluded, as mentioned previously, that abnormal acti-vation is not restricted to this area and one should considerthe entire network of regions involved when makinginferences about the biological mechanisms of schizo-phrenia, since the pattern of hyper- and hypoactivationsfound across studies is complex. This underscores therelevance of focusing on the functional connectivity ofcerebral regions. A potential schizophrenia-specific dis-ruption of cortico-cortical as well as cortico-limbicinteractions has to be considered as underlying patholog-ical substrate. Indeed, a linear increase frontally has notbeen paralleled by a deactivation in temporal areas inpatients compared to controls (Walter et al., 2003) and areduced effective connectivity between DLPFC and cere-bellum as well as an enhanced connectivity between thethalamus and cortical regions (Schlösser et al., 2003a,b)has been shown. Furthermore, nicotine has been shown todemonstrate a greater modulating effect on thalamo-cortical functional connectivity in a schizophrenia groupcompared to healthy controls (Jacobsen et al., 2004).Hence, the basis of working memory dysfunction may liein the inability to both effectively engage andmodulate theunderlying cerebral networks implicated in the taskrequirements. However, further reasons for such divergentfindings have also to be mentioned. A recent parametricstudy demonstrated a drop inDLPFC activation in patientsonly at 3-back tasks, despite low performance levelsduring all conditions (Jansma et al., 2004). It may be thatonly 3-back tasks require additional manipulation pro-cesses of working memory to reveal DLPFC dysfunction.Hence, we probably mapped the proposed inverted U-shaped model of activation and memory load at theintersection of both curves, that of patients and controls,where no differences emerge. Another problem is that n-back tasks do not allow for the distinct analysis of workingmemory subcomponents, such as encoding, maintenanceand retrieval. Group differences may, however, be dif-ferent for different processes, as has been demonstrated forencoding and retrieval (Johnson et al., 2006). It is alsoconceivable that the first hospital stay and pharmacolog-ical treatment may have improved DLPF functions inpatients, as previously suggested (Honey and Sharma,1999). This is confirmed by a lack of hypofrontality notonly in acutely ill inpatients whose schizophrenia has beensuccessfully treatedwith atypical neuroleptics (Walter et al.,2003), but also in older patients (Kindermann et al., 2004),whomay require lessmedication due to an alleviated illness

207F. Schneider et al. / Schizophrenia Research 89 (2007) 198–210
course and a more stable psychopathological status. At thesame time, this suggests that medication may result in anormalized or enhanced brain activation pattern (Honeyet al., 1999; Ramsey et al., 2002), although our data suggestthat not all dysfunctions disappear following medication.Since pharmacological treatment also affects brain activa-tion, the possibility that medication accounts for theseresults cannot definitely be ruled out. It may also bepossible that a DLPFC hypoactivation is associated to aprimarily negative symptomatology, and as the majority ofour patients were diagnosed with paranoid schizophrenia(n=42), this could explain a lack of DLPFC dysfunction.Arguing against this hypothesis is, however, the fact thatpatients exhibited slightly more negative (PANSS) thanpositive symptoms. The data rather suggest that DLPFCdysfunction may not be as characteristic for cognitive dys-functions in schizophrenia and as all-encompassing aspreviously thought, but may rather be a question of im-balanced network interactions (Schlösser et al., 2003a,b),very high working memory load (Jansma et al., 2004) orvery low performance (Perlstein et al., 2001).
4.3. The influence of performance
Correspondingly, another crucial factor probablydetermining frontal hypo- or hyperactivation in patientsseems to be performance. Including performance as acovariate of no interest in the analyses failed to affectgroup differences, but these group differences werealready present at low level attentional demands despiteequal behavioral accuracy. Similar results were observedwith fMRI during emotional processing in schizophrenia(Habel et al., 2004; Schneider et al., 1998) and in a recentfMRI study in older patients (Kindermann et al., 2004).The authors of the latter study (Kindermann et al., 2004)reported reduced activation during spatial workingmemory in medial frontal, superior temporal and basalganglia areas in patients for which the behavioralperformance was not significantly different. Similarly,Carter et al. (1998) observed an attenuated medialprefrontal, precentral gyrus and parietal (postcentralgyrus, precuneus) activation during low workingmemory load in eight schizophrenia patients despite amatched performance, suggesting that behavioral differ-ences cannot fully account for the dysfunctions. Aninvestigation into the existence of a differential perfor-mance between patients revealed predominantly frontalhyperactivation in good n-back performers (althoughreduced performance was observed compared withcontrols) and hypoactivation was observed exclusivelyin poor performers (Perlstein et al., 2001). Recently,during a 2-back task without performance differences,
only a left DLPFC hypoactivation emerged in clinicallystable schizophrenia patients (Mendrek et al., 2005),while several areas were hyperactivated. Even in thecase of matched performance, the system seems to beinefficient or imbalanced, providing either too little ortoo much involvement and failing to adjust the adequatecontribution, as demonstrated by our results.
4.4. Conclusion and methodological considerations
The differing findings in previous studies may beexplained as the result of methodological factors, such assmall samples which were influenced to a greater extentby specific patient or group characteristics and in whichthe activation pattern might also have beenmore affectedby outliers. Our multi-center study provides data from avery large sample of first-episode patients, and withinthis paradigm, data acquisition and analysis werestandardized and identical in all participating centers.Furthermore, a two-step intensive quality control wasapplied in order to reduce the additional variability ofdiverse data sources and different scanners, as well asminimizing the effects of differential data quality (due todifferential non task related variance) in patients andcontrols. Data of controls and patients are maximallyhomogeneous with respect to non-task related variance.Hence, results may be more reliable, valid and generallyapplicable with respect to the early stages of the illness.Our choice of first-episode patients reduces the impact offactors such as illness chronicity, long-term medicationor social withdrawal. However, 42 out of 49 patients areparanoid subtype, which may be a bit atypical, and wecan only infer that this characteristic may be due to thisparticular sample composition, since diagnoses havebeen performed standardized and by experiencedpsychiatrists. A methodological constraint of the studyis the choice of the task contrasting 2-back and 0-backconditions instead of 2-back and 1-back, which showgreater similarities and are comparable with respect totask requirements. On the other hand, using similar tasksmay have concealed differences between the conditionsand our aim was to maximize such dissimilarities inorder to increase sensitivity in detecting groupdifferences.
This multi-center study on a large sample of first-episode schizophrenia patients has demonstrated dys-functions mainly in the ventrolateral prefrontal cortexand the precuneus during working memory. This im-balanced network in schizophrenia patients is evidenteven at low attentional demands. Different quality con-trol measures resulted in conservative data analysis andguaranteed validity of the data. As a methodological

208 F. Schneider et al. / Schizophrenia Research 89 (2007) 198–210
constraint the (differential) influence of medication onbrain activation could not be determined, since themedication of patients is still unknown. However, thedata clearly shows the relative early presence of suchdysfunctions in first-episode patients after their firsthospital stay, where effects of illness chronicity and long-term medication exert less influence on these patients.
Acknowledgements
This study is part of the German Research Networkon Schizophrenia and was funded by the GermanFederal Ministry for Education and Research BMBF(grant 01 GI 9932) and the Federal Ministry of Educa-tion and Research (Brain Imaging Center West, 01 GO0204). The MRI facility in Jülich is supported by theGerman Federal Ministry for Education and Research(BMBF; grant 01 GO 0104).
We thank N. Kathmann for the pre-arrangement ofthe CPT task and P. Engels, H. Greenland, V. Backes,E. Plitzko, J. Reul, N. Seiferth, K. Specht for assistanceand support.
References
Andreasen, N.C., Rezai, K., Alliger, R., Swayze, V.W., Flaum, M.,Kirchner, P., Cohen, G., O'Leary, D.S., 1992. Hypofrontality inneuroleptic-naive patients and in patients with chronic schizo-phrenia. Assessment with xenon 133 single-photon emissioncomputed tomography and the Tower of London. Arch. Gen.Psychiatry 49, 943–958.
Andrews, J., Wang, L., Csernansky, J.G., Gado, M.H., Barch, D.M.,2006. Abnormalities of thalamic activation and cognition inschizophrenia. Am. J. Psychiatry 163, 463–469.
Barch, D.M., Carter, C.S., Braver, T.S., Sabb, F.W., MacDonald, A.,Noll, D.C., Cohen, J.D., 2001. Selective deficits in prefrontalcortex function in medication-naive patients with schizophrenia.Arch. Gen. Psychiatry 58, 280–288.
Callicott, J.H., Ramsey, N.F., Tallent, K., Bertolino, A., Knable, M.B.,Coppola, R., Goldberg, T., vanGelderen, P.,Mattay, V.S., Frank, J.A.,Moonen, C.T., Weinberger, D.R., 1998. Functional magneticresonance imaging brain mapping in psychiatry: methodologicalissues illustrated in a study of working memory in schizophrenia.Neuropsychopharmacology 18, 186–196.
Callicott, J.H., Mattay, V.S., Bertolino, A., Finn, K., Coppola, R., Frank,J.A., Goldberg, T.E., Weinberger, D.R., 1999. Physiologicalcharacteristics of capacity constraints inworkingmemory as revealedby functional MRI. Cereb. Cortex 9, 20–26.
Callicott, J.H.,Mattay, V.S., Verchinski, B.A.,Marenco, S., Egan,M.F.,Weinberger, D.R., 2003. Complexity of prefrontal cortical dysfunc-tion in schizophrenia: more than up or down.Am. J. Psychiatry 160,2209–2215.
Carter, C.S., Perlstein,W., Ganguli, R., Brar, J.,Mintun,M., Cohen, J.D.,1998. Functional hypofrontality andworkingmemory dysfunction inschizophrenia. Am. J. Psychiatry 155, 1285–1287.
Curtis, V.A., Bullmore, E.T.,Morris, R.G., Brammer,M.J.,Williams, S.C.,Simmons, A., Sharma, T., Murray, R.M., McGuire, P.K., 1999.
Attenuated frontal activation in schizophrenia may be task dependent.Schizophr. Res. 37, 35–44.
D'Esposito, M., Postle, B.R., Ballare, D., Lease, J., 1999. Maintenanceversus manipulation of information held in working memory: anevent-related fMRI study. Brain Cogn. 41, 66–86.
Eyler, L.T., Olsen, R.K., Jeste, D.V., Brown, G.G., 2004. Abnormal brainresponse of chronic schizophrenia patients despite normal perfor-mance during a visual vigilance task. Psychiatry Res. 30, 245–257.
Fu, C.H, Suckling, J.,Williams, S.C., Andrew, C.M., Vythelingum,G.N.,McGuire, P.K., 2005. Effects of psychotic state and task demand onprefrontal function in schizophrenia: an fMRI study of overt verbalfluency. Am. J. Psychiatry 162, 485–494.
Glahn, D.C., Ragland, J.D., Abramoff, A., Barrett, J., Laird, A.R.,Bearden, C.E., Velligan, D.I., 2005. Beyond hypofrontality: aquantitative meta-analysis of functional neuroimaging studies ofworking memory in schizophrenia. Hum. Brain Mapp. 25, 60–69.
Grier, J.B., 1971. Non-parametric indexes for sensitivity and biascomputing formulas. Psychol. Bull. 75, 424–429.
Habel, U., Klein, M., Shah, N.J., Toni, I., Zilles, K., Falkai, P.,Schneider, F., 2004. Genetic load on amygdala hypofunctionduring sadness in non-affected brothers of schizophrenia patients.Am. J. Psychiatry 161, 1806–1813.
Honey, G.D., Sharma, T., 1999. Functional magnetic resonanceimaging: a window on the brain and the future of schizophreniaresearch. J. Adv. Schizophr. Brain Dis. 1, 106–110.
Honey, G.D., Bullmore, E.T., Soni, W., Varatheesan, M., Williams, S.C.,Sharma, T., 1999. Differences in frontal cortical activation by aworking memory task after substitution of risperidone for typicalantipsychotic drugs in patients with schizophrenia. Proc. Natl. Acad.Sci. U. S. A. 96, 13432–13437.
Honey, G.D., Bullmore, E.T., Sharma, T., 2000. Prolonged reactiontime to a verbal working memory task predicts increased power ofposterior parietal cortical activation. NeuroImage 12, 495–503.
Honey, G.D., Bullmore, E.T., Sharma, T., 2002. Decoupling ofcognitive performance and cerebral functional response duringworking memory in schizophrenia. Schizophr. Res. 53, 45–56.
Jacobsen, L.K., Hamburger, S.D., Van Horn, J.D., Vaituzis, A.C.,McKenna, K., Frazier, J.A., Gordon, C.T., Lenane, M.C.,Rapoport, J.L., Zametkin, A.J., 1997. Cerebral glucose metab-olism in childhood onset schizophrenia. Psychiatry Res. 75,131–144.
Jacobsen, L.K., D'Souza, D.C., Mencl, W.E., Pugh, K.R., Skudlarski,P., Krystal, J.H., 2004. Nicotine effects on brain function andfunctional connectivity in schizophrenia. Biol. Psychiatry 55,850–858.
Jaeggi, S.M., Seewer, R., Nirkko, A.C., Eckstein, D., Schroth, G.,Groner, R., Gutbrod, K., 2003. Does excessive memory loadattenuate activation in the prefrontal cortex? Load-dependentprocessing in single and dual tasks: functional magnetic resonanceimaging study. NeuroImage 19, 210–225.
Jansma, J.M., Ramsey, N.F., van der Wee, N.J., Kahn, R.S., 2004.Working memory capacity in schizophrenia: a parametric fMRIstudy. Schizophr. Res. 68, 159–171.
Johnson, M.R., Morris, N.A., Astur, R.S., Calhoun, V.D., Mathalon, D.H.,Kiehl, K.A., Pearlson, G.D., 2006. A functional magnetic resonanceimaging study of working memory abnormalities in schizophrenia.Biol. Psychiatry 60, 11–21.
Kay, S.R., Fiszbein, A., Opler, L.A., 1987. The Positive and NegativeSyndrome Scale (PANSS) for schizophrenia. Schizophr. Bull. 13,261–276.
Keedy, M.S., Ebens, C.L., Keshavan, M.S., Sweeney, J.A., 2006.Functional magnetic resonance imaging studies of eye movements

209F. Schneider et al. / Schizophrenia Research 89 (2007) 198–210
in first episode schizophrenia: smooth pursuit, visually guidedsaccades and the oculomotor delayed response task. PsychiatryRes. 146, 199–211.
Keshavan, M.S., Diwadkar, V.A., Spencer, S.M., Harenski, K.A.,Luna, B., Sweeney, J.A., 2002. A preliminary functional magneticresonance imaging study in offspring of schizophrenic parents.Prog. Neuro-Psychopharmacol. Biol. Psychiatry 26, 1143–1149.
Kindermann, S.S., Dolder, C.R., Bailey, A., Katz, I.R., Jeste, D.V.,2002. Pharmacological treatment of psychosis and agitation inelderly patients with dementia: four decades of experience. DrugsAging 19, 257–276.
Kindermann, S.S., Brown, G.G., Zorrilla, L.E., Olsen, R.K., Jeste, D.V.,2004. Spatial working memory among middle-aged and olderpatients with schizophrenia and volunteers using fMRI. Schizophr.Res. 68, 203–216.
Kondo, Y., Suzuki, M., Mugikura, S., Abe, N., Takahashi, S., Iijima,T., Fujii, T., 2005. Changes in brain activation associated with useof a memory strategy: a functional MRI study. NeuroImage 24,1154–1163.
Kumari, V., Aasen, I., Taylor, P., Ffytche, D.H., Das, M., Barkataki, I.,Goswami, S., O'Connell, P., Howlett, M., Williams, S.C., Sharma,T., 2006. Neural dysfunction and violence in schizophrenia: anfMRI investigation. Schizophr. Res. 84, 144–164.
Lencz, T., Bilder, R.M., Turkel, E., Goldman, R.S., Robinson, D., Kane,J.M., Lieberman, J.A., 2003. Impairments in perceptual competencyand maintenance on a visual delayed match-to-sample test in first-episode schizophrenia. Arch. Gen. Psychiatry 60, 238–243.
Manoach, D.S., 2003. Prefrontal cortex dysfunction during workingmemory performance in schizophrenia: reconciling discrepantfindings. Schizophr. Res. 60, 285–298.
Manoach, D.S., Press, D.Z., Thangaraj, V., Searl, M.M., Goff, D.C.,Halpern, E., Saper, C.B., Warach, S., 1999. Schizophrenicsubjects activate dorsolateral prefrontal cortex during a workingmemory task, as measured by fMRI. Biol. Psychiatry 45,1128–1137.
Manoach, D.S., Gollub, R.L., Benson, E.S., Searl, M.M., Goff, D.C.,Halpern, E., Saper, C.B., Rauch, S.L., 2000. Schizophrenicsubjects show aberrant fMRI activation of dorsolateral prefrontalcortex and basal ganglia during working memory performance.Biol. Psychiatry 48, 99–109.
Mecklinger, A., Weber, K., Gunter, T.C., Engle, R.W., 2003. Disso-ciable brain mechanisms for inhibitory control: effects of inter-ference content and working memory capacity. Brain Res. Cogn.Brain Res. 18, 26–38.
Mendrek,A., Laurens, K.R.,Kiehl, K.A., Ngan, E.T., Stip, E., Liddle, P.F.,2004. Changes in distributed neural circuitry function in patients withfirst-episode schizophrenia. Br. J. Psychiatry 185, 205–214.
Mendrek, A., Kiehl, K.A., Smith, A.M., Irwin, D., Forster, B.B.,Liddle, P.F., 2005. Dysfunction of a distributed neural circuitry inschizophrenia patients during a working-memory performance.Psychol. Med. 35, 187–196.
Owen, A.M., McMillan, K.M., Laird, A.R., Bullmore, E., 2005. Then-back working memory paradigm: a meta-analysis of normativefMRI studies. Hum. Brain Mapp. 25, 46–59.
Perlstein, W.M., Carter, C.S., Noll, D.C., Cohen, J.D., 2001.Relation of prefrontal cortex dysfunction to working memoryand symptoms in schizophrenia. Am. J. Psychiatry 158,1105–1113.
Perlstein, W.M., Dixit, N.K., Carter, C.S., Noll, D.C., Cohen, J.D.,2003. Prefrontal cortex dysfunction mediates deficits in workingmemory and prepotent responding in schizophrenia. Biol.Psychiatry 53, 25–38.
Postle, B.R., Berger, J.S., Taich, A.M., D'Esposito, M., 2000.Activity in human frontal cortex associated with spatial workingmemory and saccadic behavior. J. Cogn. Neurosci. 12 (Suppl 2),2–14.
Ramsey, N.F., Koning, H.A., Welles, P., Cahn, W., van der Linden, J.A.,Kahn, R.S., 2002. Excessive recruitment of neural systems sub-serving logical reasoning in schizophrenia. Brain 125, 1793–1807.
Rasser, P.E., Johnston, P., Lagopoulos, J., Ward, P.B., Schall, U.,Thienel, R., Bender, S., Toga, A.W., Thompson, P.M., 2005.Functional MRI BOLD response to Tower of London performanceof first-episode schizophrenia patients using cortical patternmatching. NeuroImage 26, 941–951.
Schlösser, R., Gesierich, T., Kaufmann, B., Vucurevic, G., Hunsche, S.,Gawehn, J., Stoeter, P., 2003a. Altered effective connectivity duringworking memory performance in schizophrenia: a study with fMRIand structural equation modeling. NeuroImage 19, 751–763.
Schlösser, R., Gesierich, T., Kaufmann, B., Vucurevic, G., Stoeter, P.,2003b. Altered effective connectivity in drug free schizophrenicpatients. NeuroReport 14, 2233–2237.
Schneider, F., Weiss, U., Kessler, C., Salloum, J.B., Posse, S., Grodd,W., Müller-Gärtner, H.W., 1998. Differential amygdala activationin schizophrenia during sadness. Schizophr. Res. 34, 133–142.
Simmons, A., Moore, E., Williams, S.C., 1999. Quality control forfunctional magnetic resonance imaging using automated dataanalysis and Shewhart charting. Magn. Reson. Med. 41,1274–1278.
Slotnick, S.D., Moo, L.R., Segal, J.B., Hart, J., 2003. Distinctprefrontal cortex activity associated with item memory and sourcememory for visual shapes. Cog. Brain Res. 17, 75–82.
Smith, E.E., Jonides, J., 1998. Neuroimaging analyses of humanworking memory. Proc. Natl. Acad. Sci. U. S. A. 95, 12061–12068.
Stöcker, T., Schneider, F., Klein, M., Habel, U., Kellermann, T., Zilles,K., Shah, N.J., 2005. Automated quality assurance routines forfMRI data applied to a multi-center study. Hum. Brain Mapp. 25,237–246.
Tan, H.Y., Choo, W.C., Fones, C.S., Chee, M.W., 2005. fMRI study ofmaintenance and manipulation processes within working memoryin first-episode schizophrenia. Am. J. Psychiatry 162, 1849–1858.
Thermenos, H.W., Goldstein, J.M., Buka, S.L., Poldrack, R.A., Koch,J.K., Tsuang, M.T., Seidman, L.J., 2005. The effect of workingmemory performance on functional MRI in schizophrenia.Schizophr. Res. 74, 179–194.
Thulborn, K.R., Martin, C., Voyvodic, J.T., 2000. Functional MRimaging using a visually guided saccade paradigm for comparingactivation patterns in patients with probable Alzheimer's diseaseand in cognitively able elderly volunteers. Am. J. Neuroradiol. 21,524–531.
Veltman, D.J., Rombouts, S.A., Dolan, R.J., 2003. Maintenance versusmanipulation in verbal working memory revisited: an fMRI study.NeuroImage 18, 247–256.
Volz, H., Gaser, C., Hager, F., Rzanny, R., Ponisch, J., Mentzel, H.,Kaiser, W.A., Sauer, H., 1999. Decreased frontal activation inschizophrenics during stimulation with the continuous perfor-mance test—a functional magnetic resonance imaging study. Eur.Psychiatr. 14, 17–24.
Walter, H., Wolf, R.C., 2002. Von der Hypofrontalität zurdynamischen Dysfunktion. FMRT Studien bei Patienten mitSchizophrenie [From hypofrontality to dynamic dysfunction:fMRI studies in patients with schizophrenia]. Nervenheilkunde21, 392–399.
Walter, H., Wunderlich, A.P., Blankenhorn, M., Schafer, S., Tomczak,R., Spitzer, M., Gron, G., 2003. No hypofrontality, but absence of

210 F. Schneider et al. / Schizophrenia Research 89 (2007) 198–210
prefrontal lateralization comparing verbal and spatial workingmemory in schizophrenia. Schizophr. Res. 61, 175–184.
Weinberger, D.R., Berman, K.F., 1996. Prefrontal function in schi-zophrenia: confounds and controversies. Philos. Trans. R. Soc.Lond., B Biol. Sci. 351, 1495–1503.
Wittchen, H.U., Zaudig, M., Fydrich, T., 1997. Strukturiertes klini-sches Interview für DSM-IV: SKID [Structured Clinical Interviewfor DSM IV: SCID]. Hogrefe, Göttingen.
Wolf, R.C., Vasic, N., Walter, H., 2006. Das Arbeitsgedächtniskonzeptin der Schizophrenie: Überblick und Ausblick [The concept of
working memory in schizophrenia: current evidence and futureperspectives]. Fortschr Neurol Psychiat. 74, 449–468.
Zurowski, B., Gostomzyk, J., Gron, G., Weller, R., Schirrmeister, H.,Neumeier, B., Spitzer, M., Reske, S.N., Walter, H., 2002. Disso-ciating a common working memory network from different neuralsubstrates of phonological and spatial stimulus processing. Neuro-Image 15, 45–57.
Related Documents











