Nephrostomy Dr Christopher Watts Consultant Radiologist Salisbury District Hospital

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Nephrostomy
Dr Christopher Watts
Consultant Radiologist
Salisbury District Hospital
Talk Overview
Indications & Contraindications
Patient preparation
Consent
Kit
Techniques – dilated and non dilated kidney
Complications
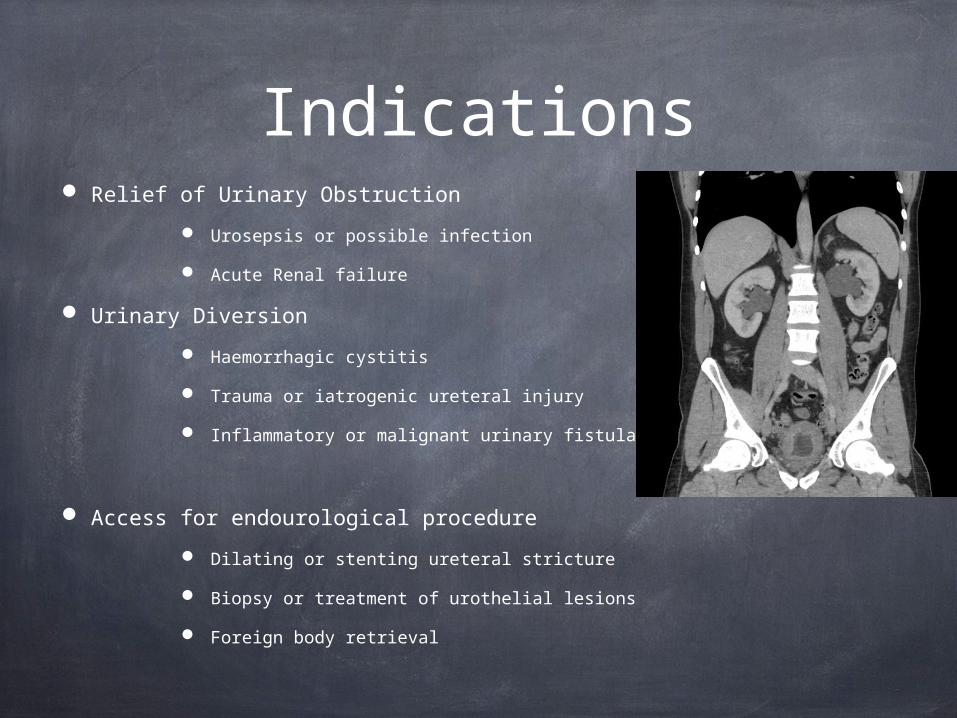
Indications Relief of Urinary Obstruction
Urosepsis or possible infection
Acute Renal failure
Urinary Diversion
Haemorrhagic cystitis
Trauma or iatrogenic ureteral injury
Inflammatory or malignant urinary fistula
Access for endourological procedure
Dilating or stenting ureteral stricture
Biopsy or treatment of urothelial lesions
Foreign body retrieval
QuickTime™ and aJVT/AVC Coding decompressorare needed to see this picture.


ContraindicationsAbsolute
? None…
RelativeDying patient
Uncorrectable severe coagulopathy / bleeding diathesis
Severe hyperkalaemia and/or metabolic acidosis
Pregnancy
Who should do it?
When should it be done?
IR or Urologists?
Part of RCR specialty IR training
Not just a drainage….
During the day
Possibly during the night Single kidney Sepsis
The referral
Speak to your urologist
Get a detailed overview of the problem and the patient’s current state of health
Discuss the urgency of the case
Review relevant imaging
Is there another way?
Patient Preparation
Bloods…..
Bleeding Risk Assessment
Evidence of coagulopathy
Is the patient on warfarin
FBC – plts >50 x 109
INR - <1.5
Hyperkalaemia
K >6.5 – call your medic / anesthetist. Can the patient be dialysed?
Patient Preparation Sedation
I like it BUT the patient may become agitated.
If giving conscious sedation the patient needs to be appropriately starved
6 hours solids
2 hours clear fluids
Combination of an opiate and benzodiazepine
E.g. morphine & Midazolam
Check local policy or guidelines
Monitoring and Oxygen
Patient Preparation
Antibiotics – evidence is weak
Potentially infected, obstructed system
Very easy to make the patient worse when trying to make them better
Septicaemia
Antibiotics to consider
Gentamycin 160-240mg IV
Cefuroxime 1.5gm iv
CHECK HOSPITAL GUIDELINES
Consent and Complications
Major (<5%)Septic Shock
1-3% ( <10% if
pyonephrosis)
Haemorrhage 1-4%
Bowel Transgression <1%
Pleural Complications <1%
SIR classification
MINOR
A no therapy or consequence
B nominal therapy, no consequence, overnight admission for observation only
MAJOR
C therapy , minor hospitalisation <48 hrs
D major therapy, increased care, prolonged hospitalisation >48hours
E permanent adverse sequelae
F death
Success RatesObstructed Dilated system without stones 95-98%
Non-dilated collecting system 80-85%
Where to Puncture?
Considerations:
•Anatomy – Where am I least likely to cause significant complications
•Bleeding
•Perforation
•Pneumothorax
•Next intervention
•Simple nephrostomy
•Ureteral intervention
•Patient comfort
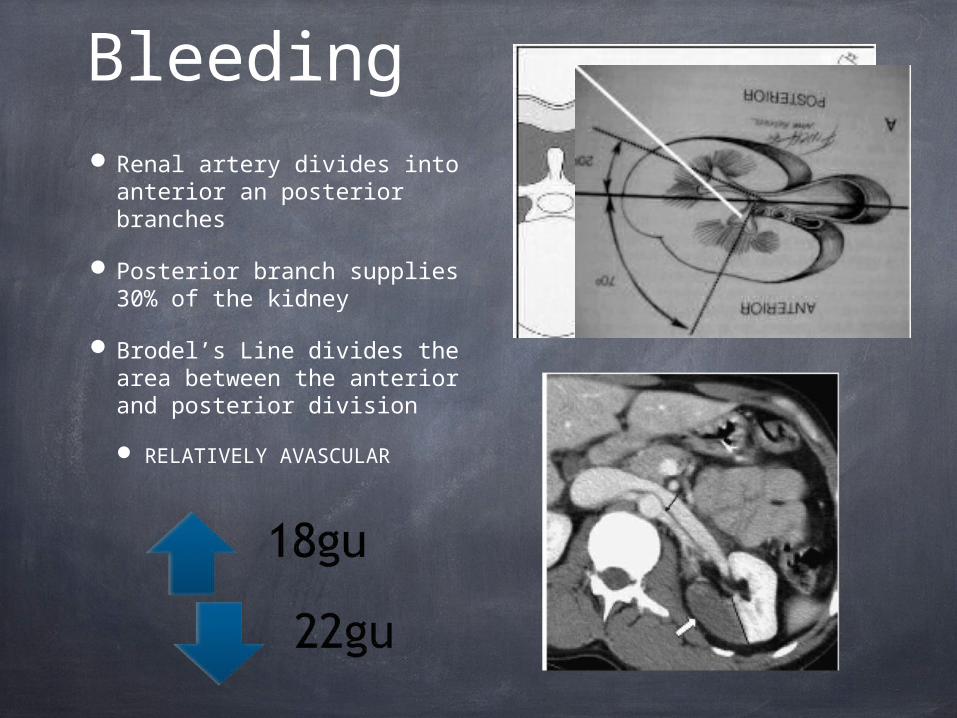
Bleeding Renal artery divides into
anterior an posterior branches
Posterior branch supplies 30% of the kidney
Brodel’s Line divides the area between the anterior and posterior division
RELATIVELY AVASCULAR

Other anatomical considerations
BOWEL
LUNG
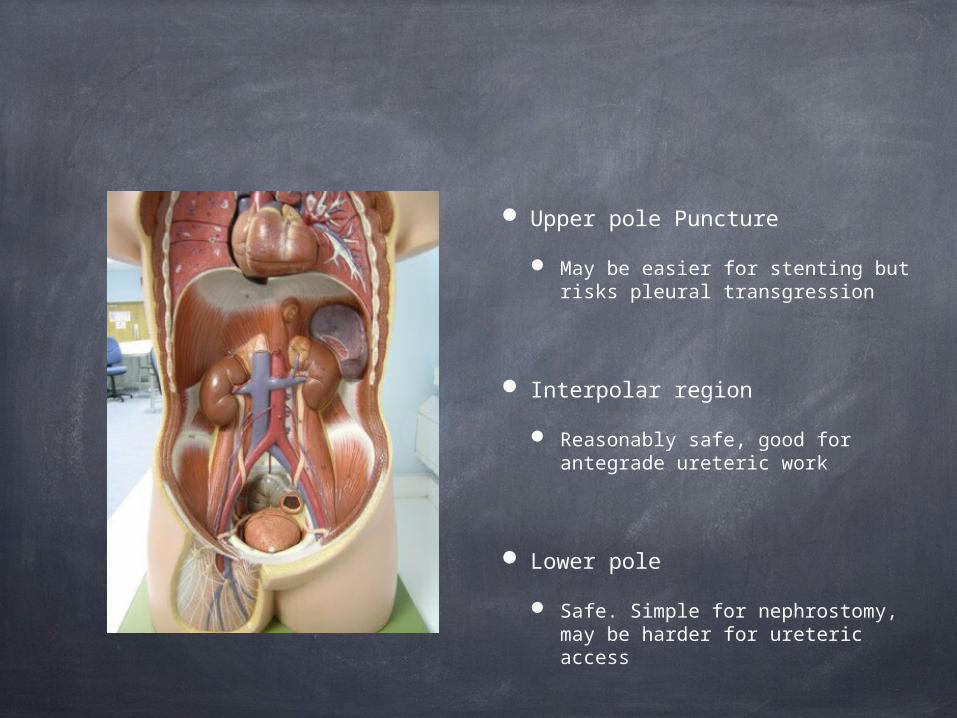
Upper pole Puncture
May be easier for stenting but risks pleural transgression
Interpolar region
Reasonably safe, good for antegrade ureteric work
Lower pole
Safe. Simple for nephrostomy, may be harder for ureteric access
The Procedure
For dilated collecting systems
US puncture
For Non Dilated collecting systems
Not straightforward.
‘Hybrid IVU’
Frusemide
CT
Kit
Angiocath 16gu
Kellet Needle -19gu

Access Kits
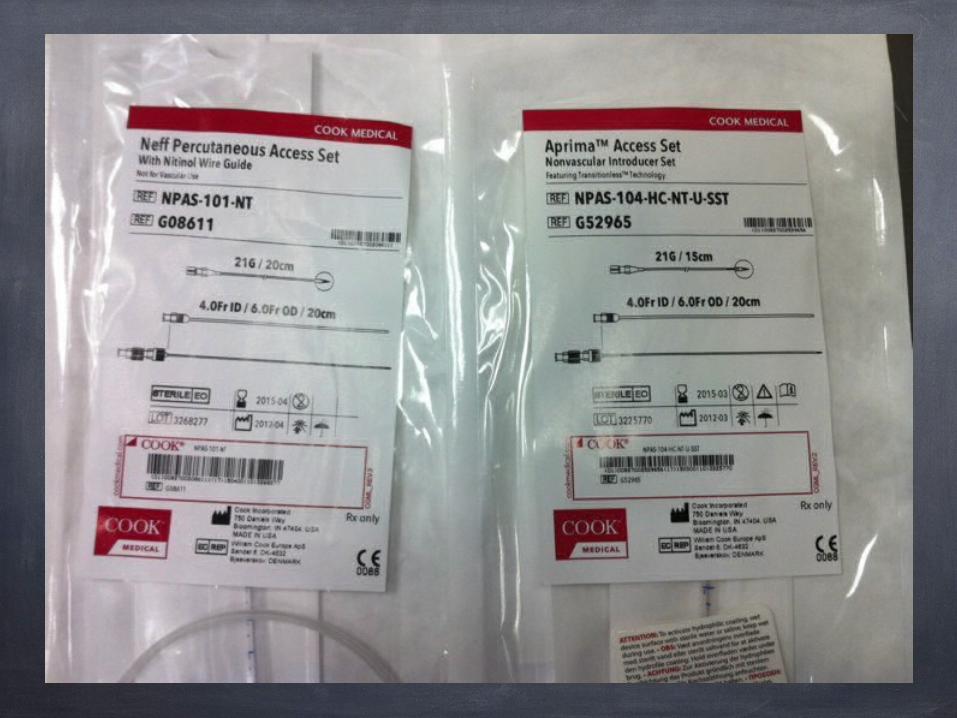
Access Kits
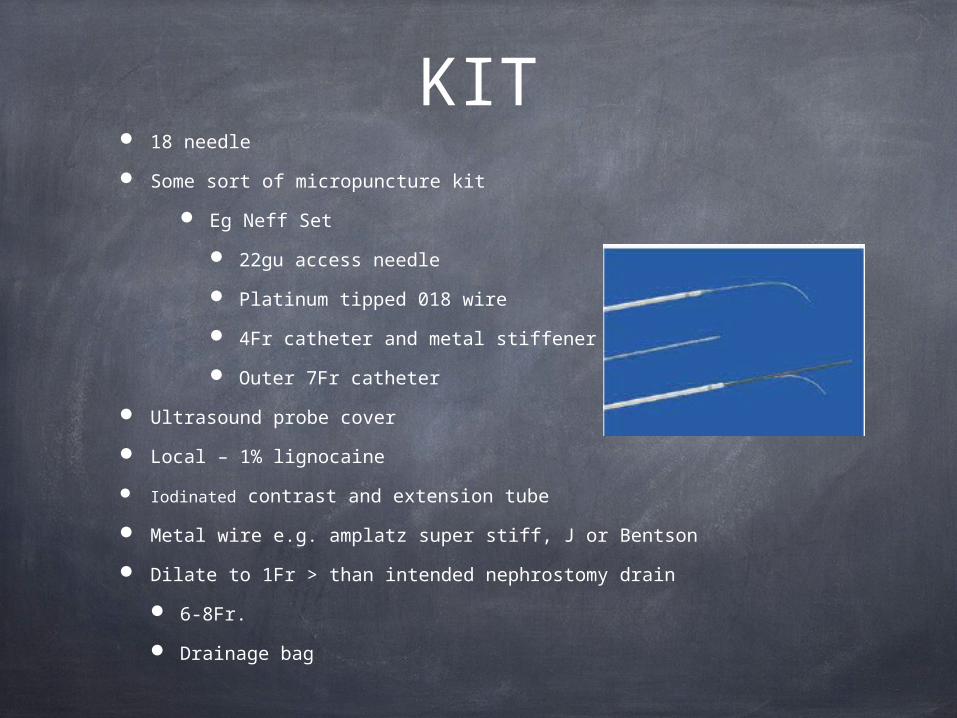
KIT 18 needle
Some sort of micropuncture kit
Eg Neff Set
22gu access needle
Platinum tipped 018 wire
4Fr catheter and metal stiffener
Outer 7Fr catheter
Ultrasound probe cover
Local – 1% lignocaine
Iodinated contrast and extension tube
Metal wire e.g. amplatz super stiff, J or Bentson
Dilate to 1Fr > than intended nephrostomy drain
6-8Fr.
Drainage bag
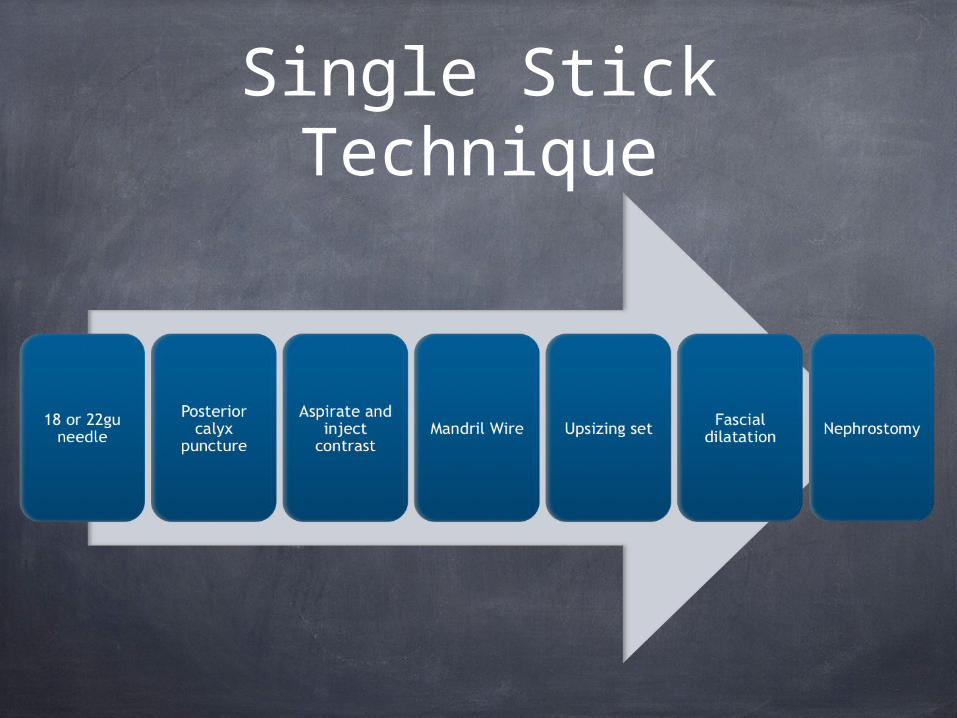
Single Stick Technique
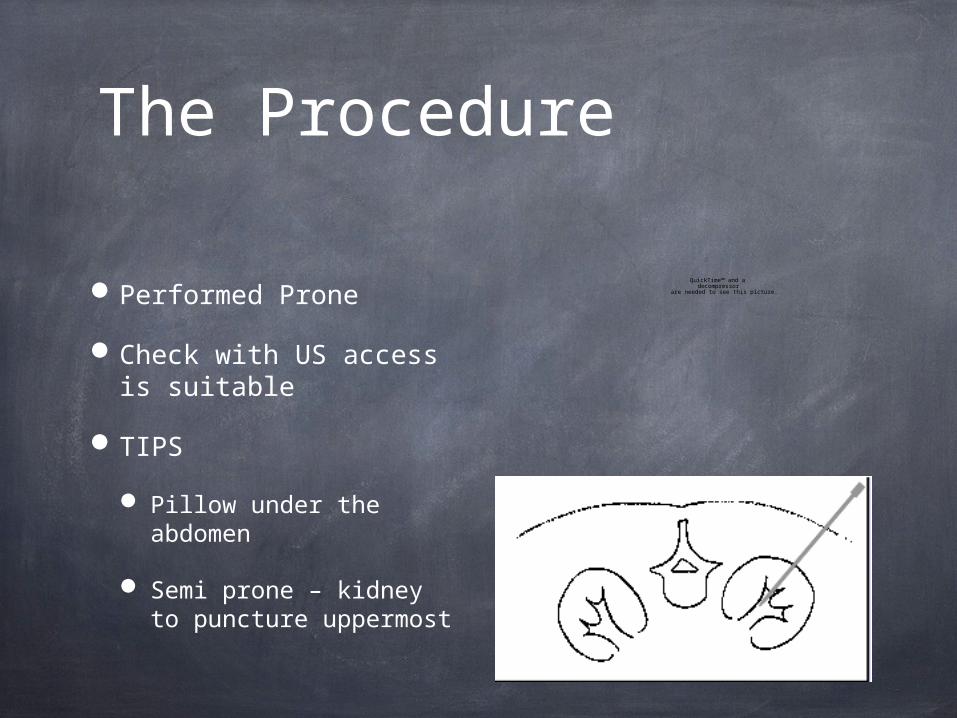
The Procedure
Performed Prone
Check with US access is suitable
TIPS
Pillow under the abdomen
Semi prone – kidney to puncture uppermost
QuickTime™ and a decompressor
are needed to see this picture.
QuickTime™ and aH.264 decompressor
are needed to see this picture.
QuickTime™ and aJVT/AVC Coding decompressorare needed to see this picture.

Post Procedural Care
Bed Rest for 4hours
Obs – Bp/Pulse 30min for 4 hrs
Temperature
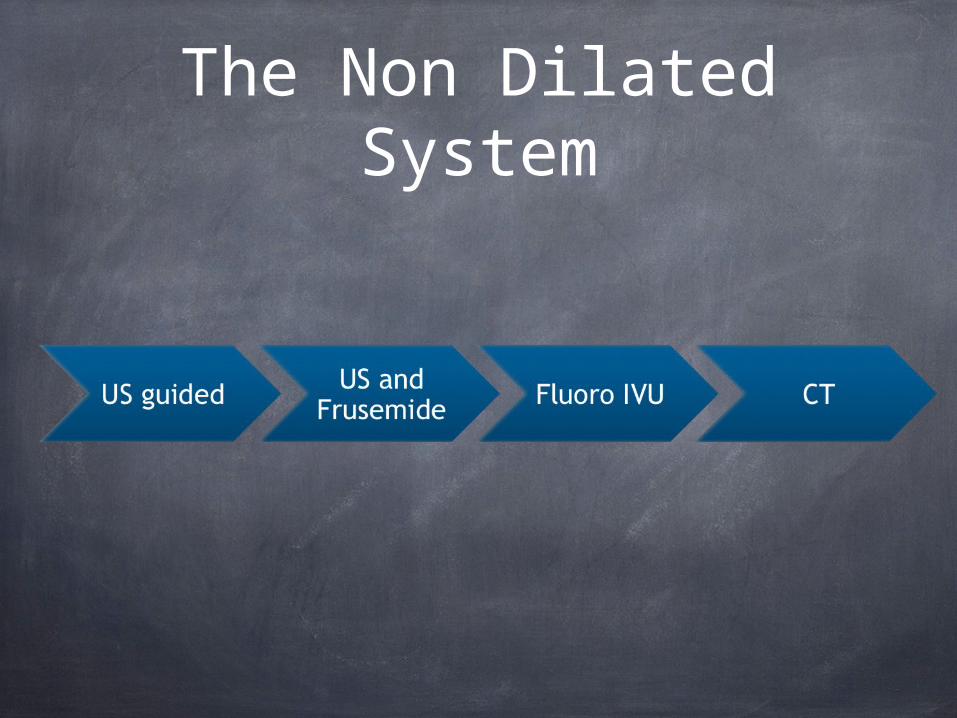
The Non Dilated System

Single stick v Double Stick
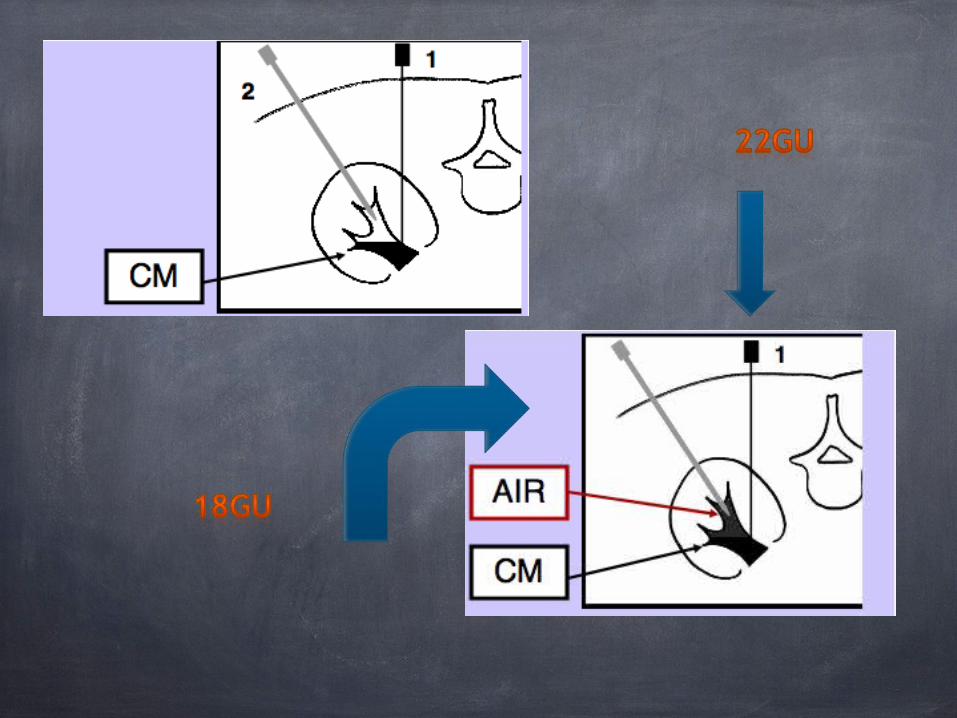

Non Dilated US guided
22gu needle better for single stick
If good views may be successful
Small volumes of contrast
Consider frusemide to plump up the calyces
Eg 40mg IV -

Fluoro IVU
US FIRST to ensure a safe passage
22Gu spinal needle
50 ml contrast >300mg/dl
5 mins
CENTRED AP
PELVIS PUNCTURE
Aspirate – contrast – air
Opposite 20° AO
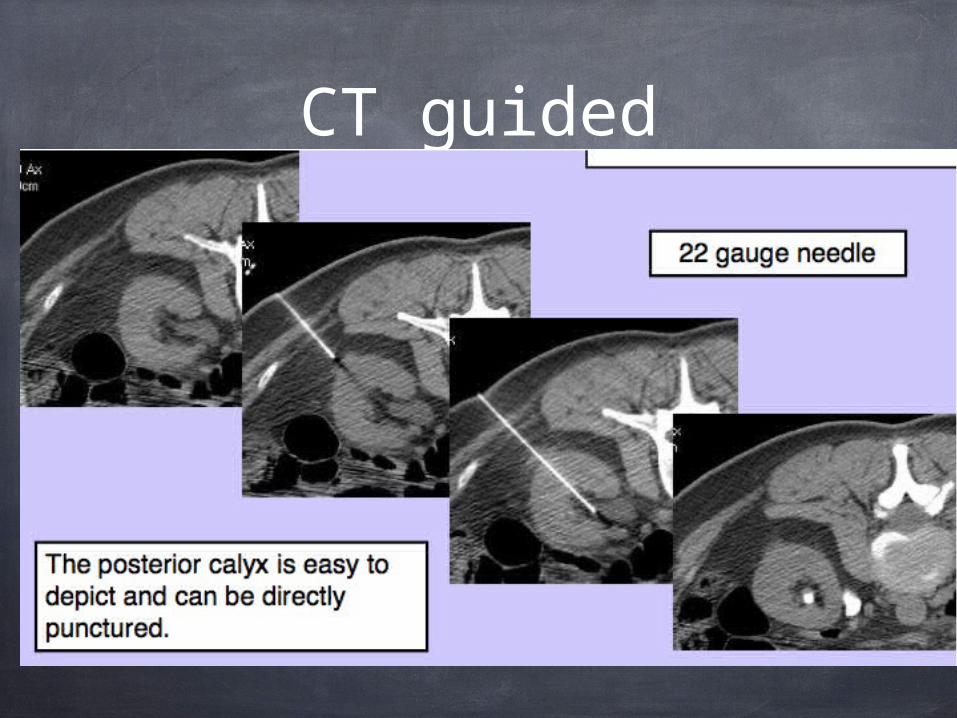
CT guided

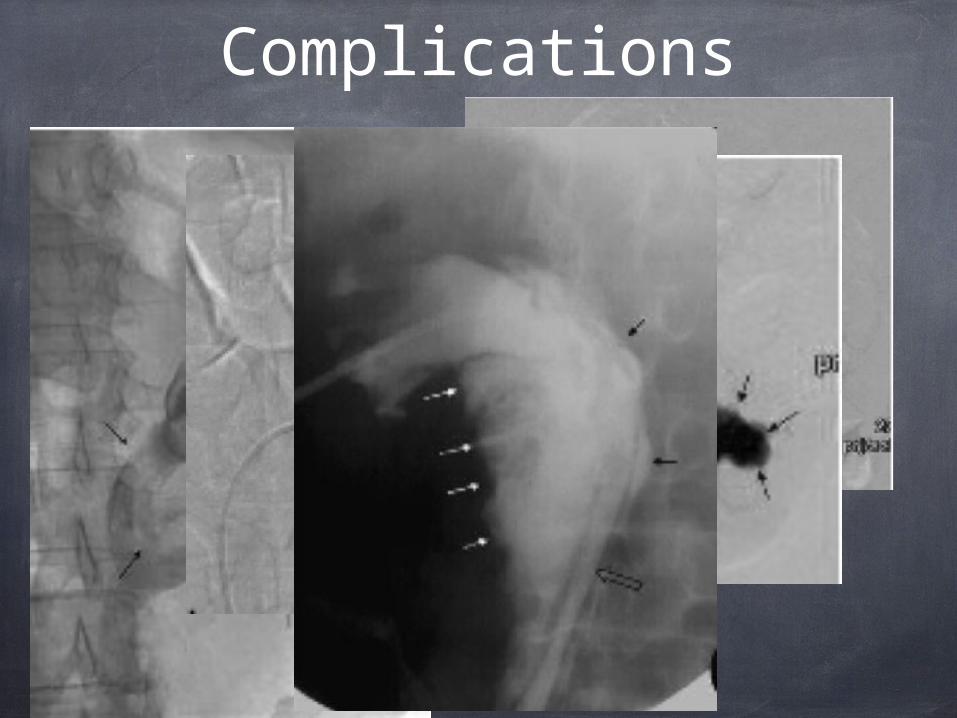
Complications
References Hausegger Percutaneous nephrostomy and antegrade
ureteral stenting: technique— indications—complications.. Eur Radiol (2006) 16: 2016–2030
Patel & Hussain Percutaneous Nephrostomy of non-dilated renal collecting systems with fluoroscopic guidance: Techniques and Results.. Radiology 2004; 233:226-233
Barbaric et al. Percutaneous nephrostomy: placement under CT and fluoroscopic guidance. AJR 1997; 169(1):151-5
Gupta et al Ultrasound-guided percutaneous nephrostomy in non-dilated pelvicaliceal system. J Clin Ultrasound. 1998 Mar-Apr;26(3):177-9.
Quality Improvement Guidelines for Percutaneous Nephrostomy J Vasc Interv Radiol 2003; 14:S277–S281 (SIR website)
Related Documents











