Resistant hypertension M3 renal ambulatory teaching session

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 1/41
Resistant hypertensionM3 renal ambulatory teaching session

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 2/41
Clinical case
A 70 yo woman with a long-standing h/o HTN comes forfollowup. Her medications include atenolol 100 mgdaily, HCTZ 12.5 mg daily, lisinopril 40 mg daily and
ibuprofen 400 mg bid for osteoarthritis. She doe notsmoke or drink alcohol. Range of systolic and diastolicBPs (measured 3 x while she is seated) range from 164-170 mmHg/92-96 mm Hg and her pulse is 72 bpm. Her
BMI is 32.Fundoscopic exam reveals arteriolarnarrowing. Cardovascular exam is normal. She has noabdominal bruites. Lab data: K 3.8 mq/L, cr 1.2 mg/dL.No microalbuminuria.
Adapted from Moser et al, Resistant or Difficult-to-Control HTN, NEngJMed 354 (4), 2006, pp385-392.

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 3/41
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 4/41
How common is resistance?
More common than we think
Prevalence ?
Best estimates from HTN outcomes studies Medications provided free of charge
Adherence is monitored
Titration of BP dictated by protocols
ALLHAT (Antihypertensive and Lipid LoweringTreatment to Prevent Heart Attack Trial) 5 yr f/u 34% uncontrolled on average 2 medications
23% on 3 or more medications
8% prescribed 4 or more medications
More conservatively perhaps15%

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 5/41
Queries……
1. Common clinical characteristics of patients withresistant hypertension include all of the following except:
a. Obesity
b. DM
c. CKD
d. Black race
e. Male sex

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 6/41
Common characteristics of
patients with resistant HTN
Older age
Obesity Presence of sleep apnea
Excessive dietary Na ingestion
DM
CKD Female
African American
Left ventricular hypertrophy
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 7/41
What compels us to recognizepatients with resistant hypertension
and treat more aggressively?
Identify patients with reversible causes of HTN
Disproportionately high risk cardiovascular events
The higher the degree of BP elevation the more likelythe patient will have
CHF
Stroke
MI
Renal failure
Higher healthcare cost and use of resources
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 8/41
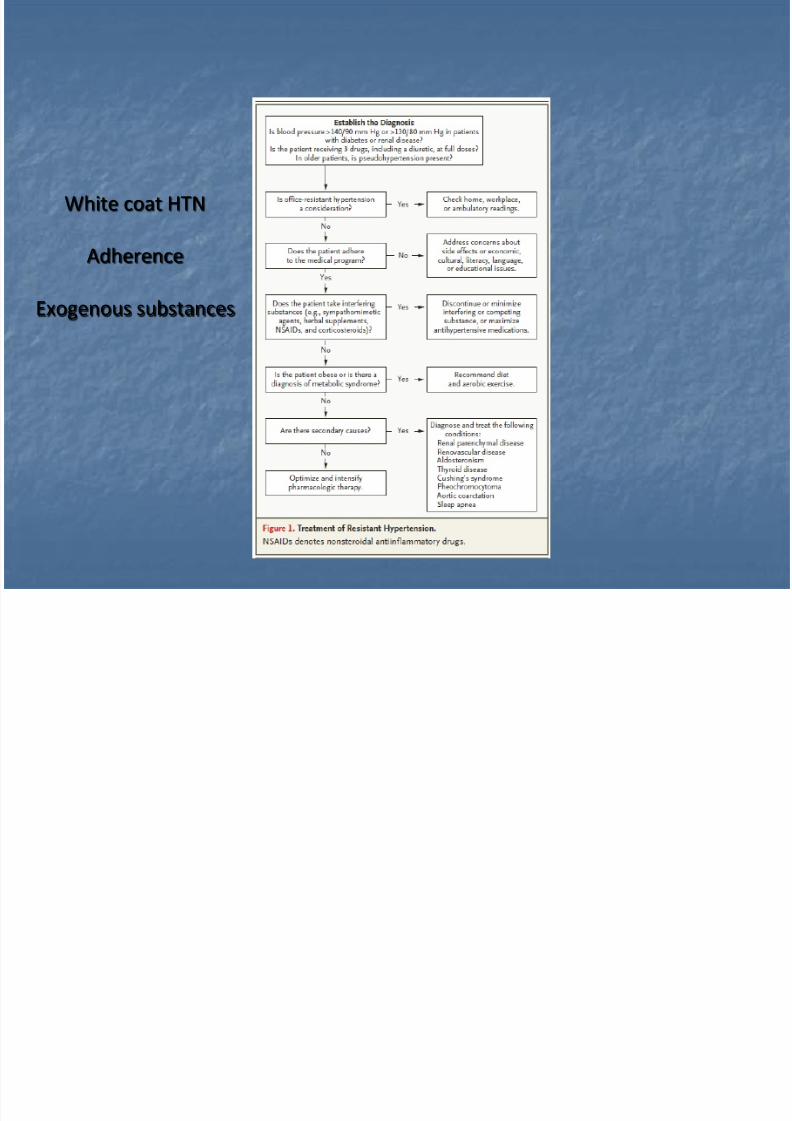
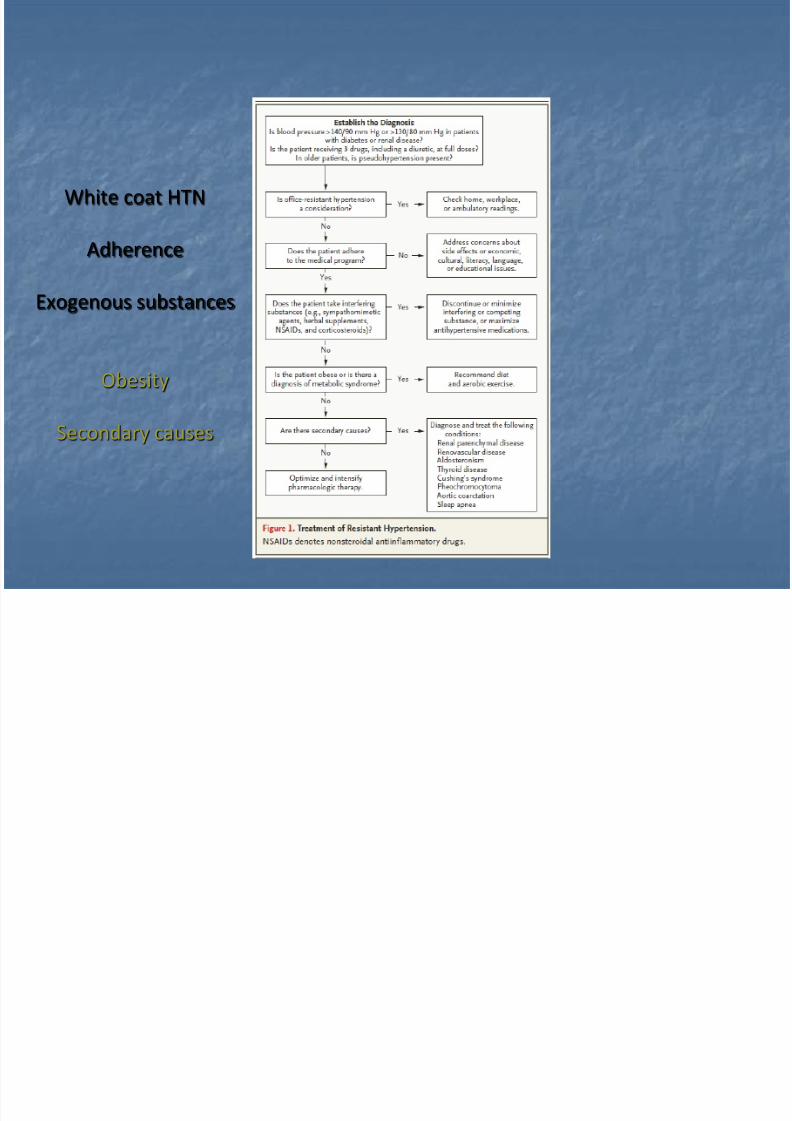
White coat HTN
Adherence
Exogenous substances

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 9/41
Drugs that can raise BP
• Cyclosporine, tacrolimus, corticosteroids
• Ibuprofen, piroxicam
• Celecoxib, rofecoxib
• 30-35 mcg estrogen oral contraceptives
• Sibutramine (meridia), phentermine(adipex), ma huang (ephedra)
• Nicotene, amphetamines
• Fludrocortisone
• Bromocriptine
• Phenelzine
• Testosterone
• Pseudoephedrine
Immunosuppressive
NSAIDs
COX-2 inhibitors
Estrogens
Weight loss agents
Stimulants
Mineralocorticoids
Anti-parkinsonian
MAO inhbitiors
Anabolic steroids
Sympathomimetics
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 10/41
White coat HTN
Adherence
Exogenous substances
Obesity
Secondary causes

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 11/41
Obesity
Associated with
Increasing severity of HTN
Use of increasing number of antihypertensive medications
Increased likelihood of never achieving goal BP
“On a population basis, the probability of lack of BP controlin obese patients is about 50% higher than hypertensivepatients who are at normal weight.”
Mechanisms:
Increased Na and fluid retention
Greater sympathetic activation
Increased stimulation of the renin-angiotensin-aldosterone
system
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 12/41
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 13/41
OSATreatment
Treatment with CPAP likely benefits BP control
Reduction in daytime and nighttime SBP and DBPs by10 mm Hg in recent study
Other studies variable results
http://www.smart-kit.com/wp-content/uploads/2006/12/cpap%20mayo.jpg
http://www.medgadget.com/archives/img/398792dij.jpg

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 14/41
Queries……..
3. You would suspect a secondary cause of HTN in allof the following patients with HTN except a patient
a. with previously well controlled and nowuncontrolled HTN
b. who develops hypokalemia on a diuretic
c. with snoring and daytime somnolenced. who develops HTN at the age of 75
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 15/41
When to suspect secondary HTN
• Severe HTN at a young age (age of onset <20-30 yrsin absence of family hx) or older (onset > 50 yrs)
• HTN refractory to medical management or onceresponsive now difficult to control
• Episode of hypertensive crisis or paroxysmal BPelevations
• Symptoms related to the underlying diagnosis (muscle weakness, episodes of tachycardia, sweating,tremor, thinning of skin, flank pain)
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 16/41
When to suspect secondary HTN
• Loud snoring, awaken with H/A, sleep inappropriatelythroughout day
• Ingestion of medications that affect BP (decongestants, estrogens, appetite suppressants,NSAIDS, exogenous thyroid hormone, recent EtOH,illicit stimulants, adrenal steroids)
• A patient with significant HTN and unprovokedhypokalemia and metabolic alkalosis

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 17/41
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 18/41
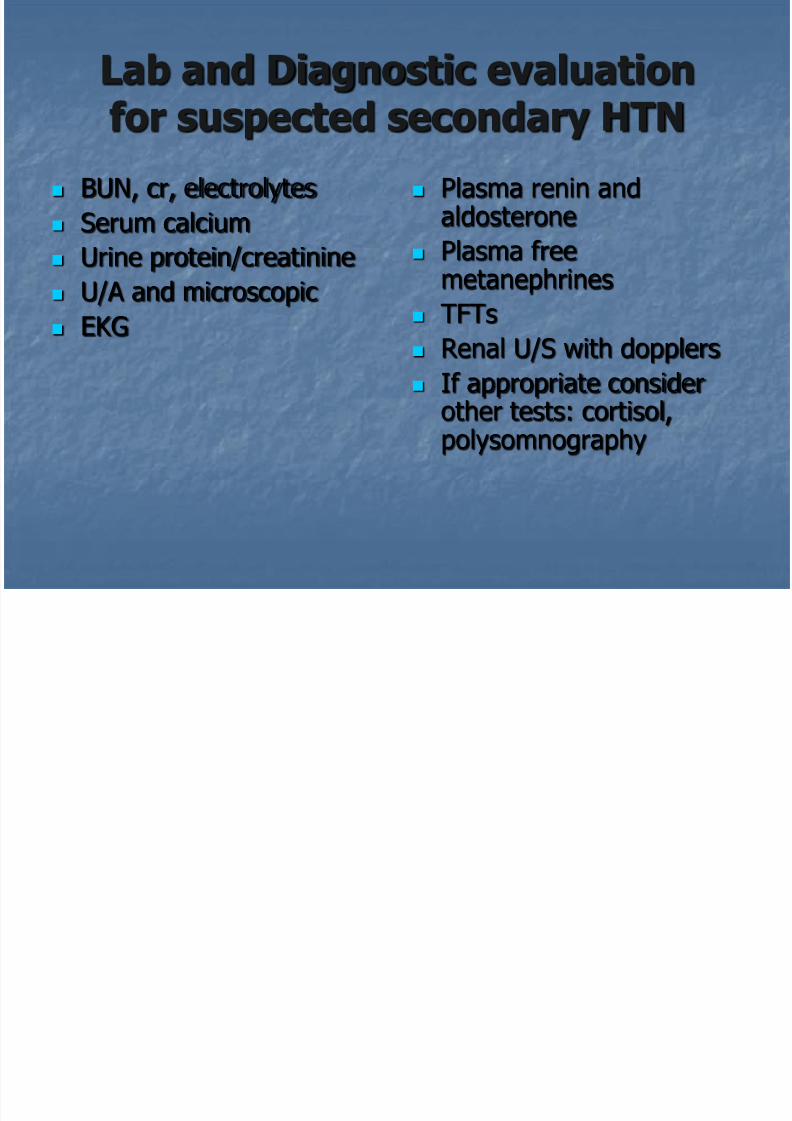
Lab and Diagnostic evaluationfor suspected secondary HTN
BUN, cr, electrolytes
Serum calcium
Urine protein/creatinine
U/A and microscopic
EKG
Plasma renin andaldosterone
Plasma free
metanephrines TFTs
Renal U/S with dopplers
If appropriate consider
other tests: cortisol,polysomnography

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 19/41
Back to our case……
A 70 yo woman with a long-standing h/o HTN comes forfollowup. Her medications include atenolol 100 mgdaily, HCTZ 12.5 mg daily, lisinopril 40 mg daily and
ibuprofen 400 mg bid for osteoarthritis. She doe notsmoke or drink alcohol. Range of systolic and diastolicBPs (measured 3 x while she is seated) range from 164-170 mmHg/92-96 mm Hg and her pulse is 72 bpm. Her
BMI is 32.Fundoscopic exam reveals arteriolarnarrowing. Cardovascular exam is normal. She has noabdominal bruites. Lab data: K 3.8 mq/L, cr 1.2 mg/dL.No microalbuminuria.
Adapted from Moser et al, Resistant or Difficult-to-Control HTN, NEngJMed 354 (4), 2006, pp385-392.

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 20/41
What would you suggest for this patient?
Adherence to medication
Discontinue NSAID
Exercise, weight loss Dietary Na restriction
Increase dose of HCTZ or change to furosemide
Add another agent like a CCB
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 21/41
Clinical case #2
A 49 yo AA man returns for f/u to your clinic. He is currently onmetoprolol XL 100 mg qd, lisinopril 40 mg qd, losartan 100 mgqd, and clonidine 0.2 mg tid. He has a strong FH of HTN. Hefollows a strict low Na diet. Previous evaluation for secondarycauses of HTN, including evaluation for OSA, was unrevealing.
BP today is 150/100, pulse 65. His urinalysis has trace proteinand is blood chemistries are normal. What would be the nextdrug of choice for this patient?
a. Amlodipine 10 mg qd
b. Minoxidil 5 mg qdc. Furosemide 40 mg qdd. Chlorthalidone 25 mg qde. Spironolactone 25 mg qd
Modified from The Journal of Clinical Hypertension, suppl 1, vol 9, no 1, Jan 2007, p 31.

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 22/41
Algorithm for treatment of HTN
http://www.nhlbi.nih.gov/guidelines/hypertension/express.pdf
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 23/41
Which is the ideal drugcombination
I don’t know
Combination of CCB, ACE-inhibitor/ARB, diuretic oftenrecommended
A different approach based on PE physiology
High systemic vascular resistance Increased catecholamine secretion
Volume excess
Hirsch, Cleveland Clinic Journal of Medicine: Vol 74, N 6, June 2007, pp449-456.

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 24/41
http://www.nhlbi.nih.gov/guidelines/hypertension/express.pdf
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 25/41
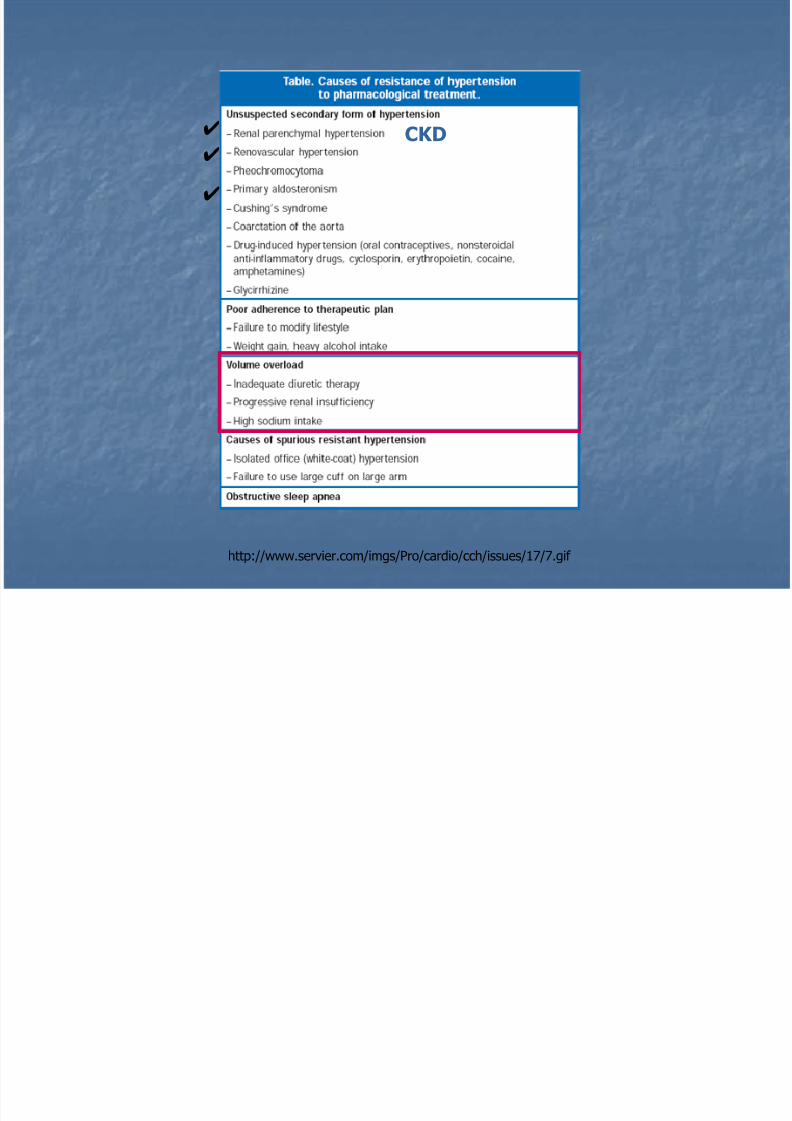
✔✔✔
http://www.servier.com/imgs/Pro/cardio/cch/issues/17/7.gif
CKD✔
✔
✔

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 26/41
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 27/41
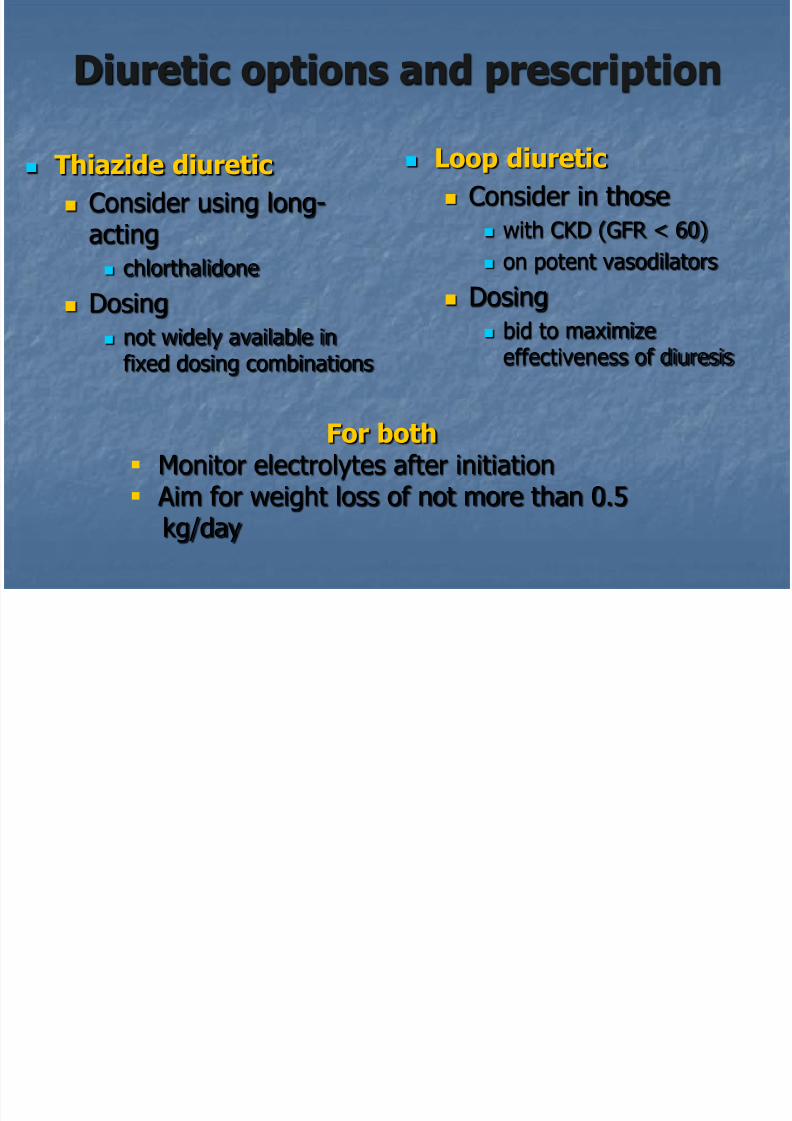
Diuretic options and prescription
Thiazide diuretic
Consider using long-acting
chlorthalidone
Dosing
not widely available infixed dosing combinations
Loop diuretic
Consider in those
with CKD (GFR < 60)
on potent vasodilators
Dosing
bid to maximizeeffectiveness of diuresis
For both Monitor electrolytes after initiation Aim for weight loss of not more than 0.5
kg/day
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 28/41
Na excess and BP control
“Increasing the dose of antihypertensive agents
in the presence of an expanded extracellular
fluid volume has no effect on the arterialpressure.” Finnerty 1971
http://www.healthcarevox.com/uploads/US.jpg

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 29/41
Education
x

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 30/41

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 31/41
Hyperaldosteronism:the link to resistant HTN
Hypothesis is that aldosterone contributes more broadlyto hypertension beyond cases of classical primaryaldosteronism, first described by Conn in 1955
How common is it?
Epstein and Calhoun, Current Hypertension Reports 2007, 9: 98-105
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 32/41
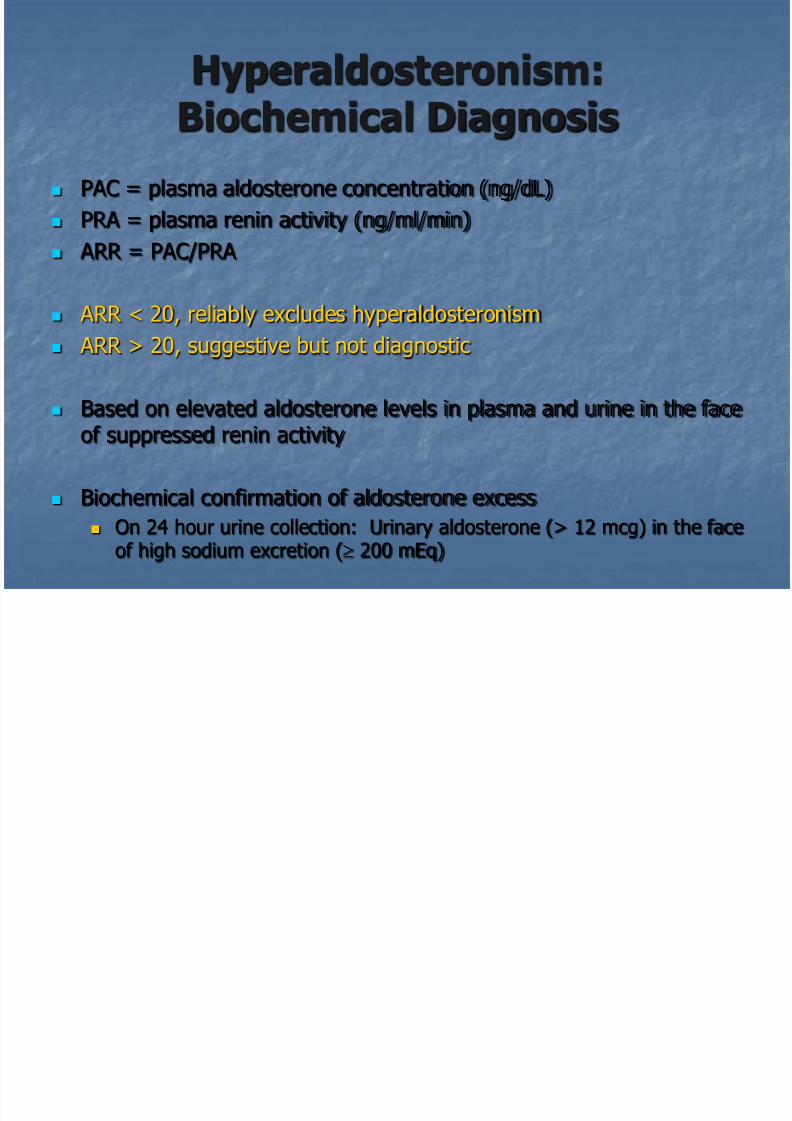
Hyperaldosteronism:Biochemical Diagnosis
PAC = plasma aldosterone concentration (ng/dL)
PRA = plasma renin activity (ng/ml/min)
ARR = PAC/PRA
ARR < 20, reliably excludes hyperaldosteronism
ARR > 20, suggestive but not diagnostic
Based on elevated aldosterone levels in plasma and urine in the faceof suppressed renin activity
Biochemical confirmation of aldosterone excess
On 24 hour urine collection: Urinary aldosterone (> 12 mcg) in the face
of high sodium excretion ( 200 mEq)
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 33/41
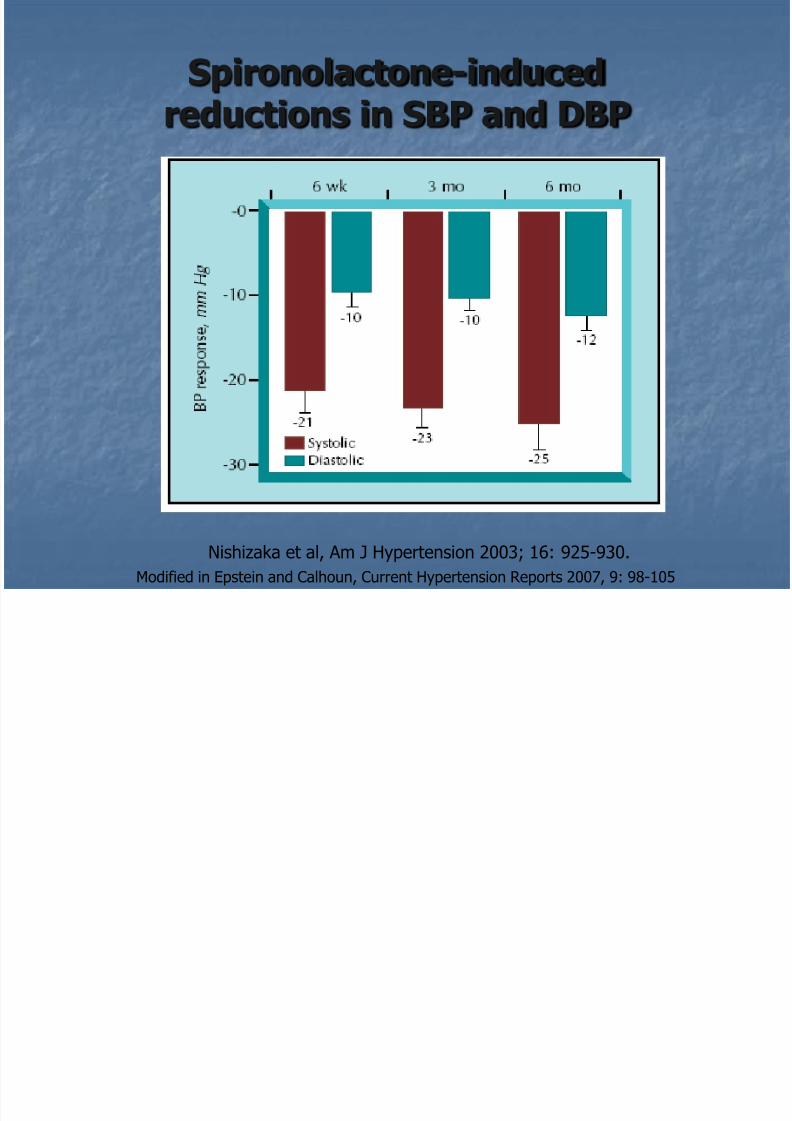
Spironolactone-inducedreductions in SBP and DBP
Nishizaka et al, Am J Hypertension 2003; 16: 925-930.Modified in Epstein and Calhoun, Current Hypertension Reports 2007, 9: 98-105

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 34/41
Spironolactone-inducedreductions in SBP and DBP
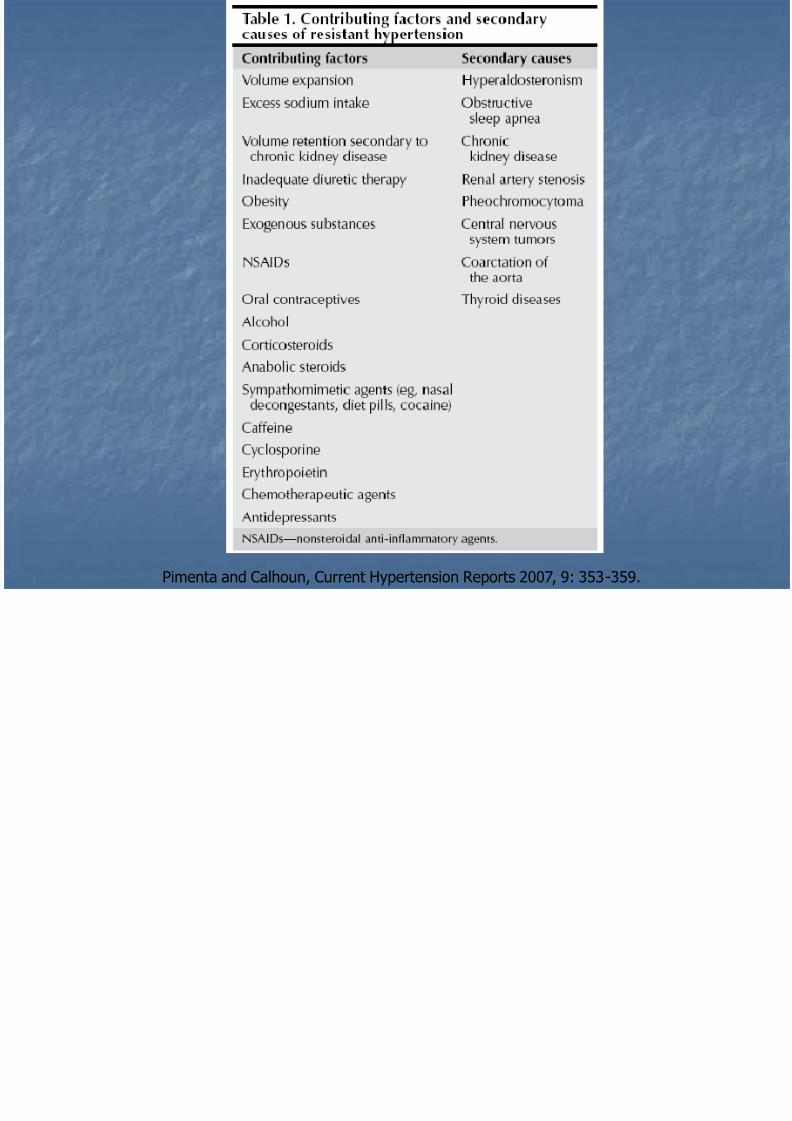
Pimenta and Calhoun, Current Hypertension Reports 2007, 9: 353-359.
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 35/41
Hyperaldosteronism:additional information
Primary aldosteronism
Based on aggregate averages from studies: 40-66%of patients with primary aldosteronism are found to
have aldosterone adenomas
Is there a broader anti-hypertensive benefit of aldosterone antagonists?
The impact of hyperaldosteronism on resistanthypertension may be greater than the typicalparameters of primary hyperaldosteronism wouldindicate.
Low renin HTN as a variant of aldosterone-induced HTN?
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 36/41
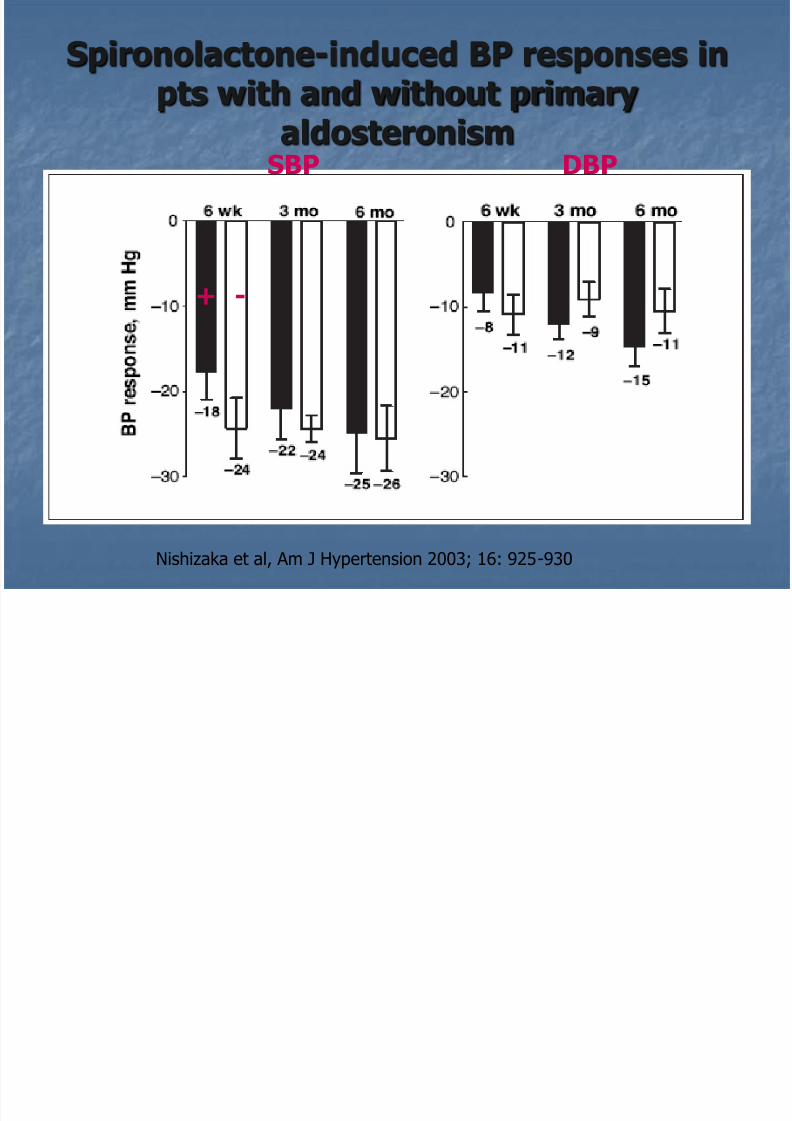
Spironolactone-induced BP responses inpts with and without primary
aldosteronism
Nishizaka et al, Am J Hypertension 2003; 16: 925-930
SBP DBP
+ -

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 37/41
Responses toaldosterone blockade
Contribution of hyperaldosteronism to HTN may begreater than indicated by hormone levels alone.
Levels of aldosterone, renin, ARR, urine aldosterone arenot necessarily predictive of BP response to aldosteroneblockade.
It is important to check biochemical parameters toascertain aldosterone excess to ultimately identify thosewith adenomas.

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 38/41
Clinical use of aldosterone blocking agents
Spironolactone
Begin at 12.5-25 mg daily
Maximum dose generally 25-50 mg daily
Monitor K after 1 week in high risk patients, 4 weeksif lower risk
10% breast tenderness

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 39/41
Take Home Points
1. Modifying contributing risk factors can have a favorableimpact on BP control, eg. obesity, exogenous medications.
2. Both the severity of HTN and the number of patients with
hypertension increase with sleep apnea severity, asindicated by the respiratory disturbance index.
3. In general, diuretics are under-prescribed in the treatmentof resistant hypertension and use of diuretics in
appropriate doses may improve the efficacy of other anti-hypertensive agents.

7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 40/41
Take Home Points
4. In patients with resistant hypertension, the prevalenceof hyperaldosteronism is particularly high.
5. Aldosterone antagonists have been shown to providesignificant additional BP benefit in patients with resistanthypertension when added to existing multi-drugregimens, which already include a diuretic and an ACEinhibitor.
7/27/2019 Nephrology - Resistant HTN
http://slidepdf.com/reader/full/nephrology-resistant-htn 41/41
Related Documents











