Dr/Ahmed Bahnassy Consultant Radiologist MBCHB-MSc-FRCR Former: Senior consultant Radiologist Riyadh Military hospital AP Radiology -Qassim Univeristy-KSA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dr/Ahmed BahnassyConsultant RadiologistMBCHB-MSc-FRCR
Former:Senior consultant Radiologist Riyadh Military hospital
AP Radiology -Qassim Univeristy-KSA



• Safe
• Bedside- compatible
• Reliable
• Early imaging
• Serial imaging:
Brain maturation
Evolution of lesions
• Inexpensive
• Suitable for screening



Embryology• At the end of the 4th week after conception,
the cranial end of the neural tube differentiates into 3 primary brain vesicles
– Prosencephalon (Forebrain)• Diencephalon
– Thalmus– Hypothalmus– Posterior Pituitary
• Telencephalon– Cerebral hemispheres– Cortex & Medullary Center– Corpus Striatum– Olfactory System
– Mesencephalon (midbrain)• Cerebral Aqueduct• Superior and inferior colliculi
(quadrigeminal body)
– Rhombencephalon (hindbrain)• Myelencephalon
– Closed part of medulla oblongata
• Metencephalon– Pons– Cerebellum– 3rd, 4th, and lateral ventricles– Choroid Plexus

Anatomy of the Neonatal Brain
Cerebrum• 2 Hemispheres (Gray and White Matter)
• Lobes of the Brain– Frontal– Parietal– Occipital– Temporal
• Gyrus and Sulcus– Gyrus: convulutions of the brain surface causing
infolding of the cortex
– Sulcus: Groove or depression separating gyri.

Anatomy of the Neonatal Brain
Cerebrum• Fissures– Interhemispheric
• Area of Falx Cerebri
– Sylvian • Most lateral aspect of brain• Location of middle cerebral artery
– Quadrigeminal • Posterior and inferior from the cavum
vergae• Vein of Galen posterior to fissure
• Falx Cerebri– Fibrous structure separating the 2
cerebral hemispheres• Tentorium Cerebelli
– “V” shaped echogenic extension of the falx cerebri separating the cerebrum and the cerebellum

Cerebrum• Basal Ganglia
• collection of gray matter
– Caudate Nucleus & Lentiform Nucleus
• Largest basal ganglia• Relay station between the
thalmus and cerebral cortex
• Germinal Matrix includes periventricular tissue and caudate nucleus
– Thalmus• 2 ovoid brain structures • Located on either side of the 3rd
ventricle superior to the brainstem
• Connects through middle of the 3rd ventricle through massa intermedia
– Hypothalmus• “Floor” of 3rd Ventricle• Pituitary Gland is connected to
the hypothalmus by the infundibulum

Anatomy of the Neonatal Brain
• Meninges– Dura Mater– Arachnoid– Pia Mater
• Cerebral Spinal Fluid (CSF)– Surrounds and protects brain and spinal
cord.
– 40% formed by ventricles, 60% extracellular fluid from circulation.

Ventricular System• Lateral Ventricles: Largest of
the CSF cavities.– Frontal Horn– Body– Occipital Horn– Temporal Horn
• Trigone “Atrium”• Foramen of Monro
• 3rd Ventricle• Aqueduct of Sylvius
• 4th Ventricle• Foramen of Luschka• Foramen of Megendie
• Cisterns– Cisterna Magna
• Spaces at the base of the skull where the arachnoid is widely separated from the pia mater.

Anatomy of the Neonatal Brain
• Corpus Callosum– Broad band of connective fibers between cerebral hemispheres.– The “roof” of the lateral ventricles.
• Cavum Septum Pellucidum– Thin, triangular space filled with CSF– Lies between the anterior horn of the lateral ventricles.– “Floor” of the corpus callosum
• Choroid Plexus– Mass of specialized cells that regulate IV pressure by secretion/absorption of CSF– Within atrium of the lateral ventricles
Choroid Plexus
Cavum Septum Pellucidum

Anatomy of the Neonatal Brain
Brain Stem
• Midbrain
• Pons
• Medulla Oblongata

Anatomy of the Neonatal Brain
Cerebellum• Posterior cranial
fossa
• 2 Hemispheres connected by Vermis
• 3 Pairs of Nerve Tracts
– Superior Cerebellar Peduncles– Middle Cerebellar Peduncles– Inferior Cerebellar Peduncles

Cerebrovascular System
• Internal Cerebral Arteries
• Vertebral Arteries• Circle of Willis
– Middle Cerebral Artery
• Longest branch in Circle of Willis that provides 80% of blood to the cerebral hemispheres

Anatomy of the Neonatal Skull
• Fontanelles (“Soft Spots”)– Spaces between bones of the skull

Indications for Sonographic Exam
• Cranial abnormality found on pre-natal sonogram• Increasing head circumference with or without
increasing intracranial pressure• Acquired or Congenital inflammatory disease• Prematurity
• Diagnosis of hypoxia, hypertension, hypercapnia, hypernaturemia, acidosis, pneumothorax, asphyxia, apnea, seizures, coagulation defects, patent ductus arteriosus, or elevated blood pressure
• History of birth trauma or surgery• Suctioning of infant• Genetic syndromes and malformations

Sonographic Technique• What anatomy do you scan?
– Supratentorial Compartment• Both cerebral hemispheres• Basal Ganglia• Lateral & 3rd Ventricle• Interhemispheric fissure• Subarachnoid space
– Views» Coronal» Modified Coronal (anterior fontanelle)» Sagittal (anterior fontanelle)» Parasagittal (anterior fontanelle)
– Infratentorial Compartment• Cerebellum• Brain Stem• 4th Ventricle• Basal Cisterns
– Views» Coronal (mastoid fontanelle and occipitotemporal area)» Modified Coronal » Sagittal» Parasagittal (with increased focal depth & decreased frequency)

• Transucers : 5–7.5–10 MHz
• Appropriately sized
• Standard examination: use 7.5–8 MHz
• Tiny infant and/or superficial structures: use additional higher frequency (10 MHz)
• Large infant, thick hair, and/or deep structures: use additional lower frequency (5 MHz)


Anterior FontanelThe Standard view window
Posterior FontanelSupplementary view window
Mastoid FontanelSupplementary view window
TemporalSupplementary view window

• Coronal Views (at least 6 standard planes)








• Sagittal Views (at least 5 standard planes)











23. Tentorium24. Mesencephalon25. Occipital lobe26. Parieto-occipital fissure27. Calcarine fissure28. Pons29. Medulla oblongata30. Fourth ventricle31. Cisterna magna32. Cisterna quadrigemina33. Interpeduncular fossa34. Fornix35. Internal capsule36. Occipital horn of lateralventricle37. Insula38. Falx39. Straight sinus (sinus rectus)40. Temporal horn of lateralventricle41. Circle of Willis42. Prepontine cistern
1. Interhemispheric fissure2. Frontal lobe3. Skull4. Orbit5. Frontal horn of lateral ventricle6. Caudate nucleus7. Basal ganglia8. Temporal lobe9. Sylvian fissure10. Corpus callosum11. Cavum septum pellucidum12. Third ventricle13. Cingulate sulcus14. Body of lateral ventricle15. Choroid plexus(*: plexus in third ventricle)16. Thalamus17. Hippocampal fissure18. Aqueduct of Sylvius19. Brain stem20. Parietal lobe21. Trigone of lateral ventricle22. Cerebellum(a: hemispheres; b: vermis)



Doppler uses
• Typical transcranial Doppler with imaging scan and recording from middle cerebral artery (MCA).
• Doppler image shows circle of Willis. – A = anterior cerebral artery – M = middle cerebral artery– P = posterior cerebral artery– RI = resistive index
• Demonstrates– Decreased blood
flow/ischemia/infarction– Vascular abnormalities– Cerebral Edema– Hydrocephalus– Intracranial Tumors– Near-field structures


Middle Cerebral Artery

Carotid Siphon - Genu

Anterior Cerebral Artery

Posterior Cerebral Artery – P1

Ophthalmic Artery

Basilar Artery

BLOOD FLOW VELOCITY
• Changes in flow velocity occur when:
• There is a change in vessel caliber• There is a change in volume flow

should we do doppler study
cyst=doppler
vein of galen aneurysm


Chiari Malformation
• Downward displacement of the cerebellar tonsils and
the medulla through the foramen magnum. • Arnold-Chiari malformation shows a small displaced
cerebellum, absence of the cisterna magna, malposition of the fourth ventricle, absence of the septum pellucidum, and widening of the third ventricle – Commonly related
to meningomyelocele

Chiari Malformation• Sonographic Features
– Small posterior fossa– Small, displaced
Cerebellum– Possible
Myelomeningocele– Widened 3rd Ventricle– Cerebellum herniated
through enlarged foramen magnum
– 4th ventricle elongated– Posterior horns enlarged– Cavum Septum
pellucidum absent– Interhemispheric Fissure
widened– Tentorium low and
hypoplastic

Holoprosencephaly• Common large central ventricle because prosencephalon
failed to cleave into separate cerebral hemispheres.
– Alobar Holoprosencephaly (Most Severe)• Fused thalami anteriorly to a fused choroid plexus• Single midline ventricle• No falx cerebrum, corpus callosum, interhemispheric
fissure, or 3rd ventricle
– Semilobar Holoprosencephaly• Single ventricle• Presents with portions of the falx and interhemispheric
fissure• Thalmi partially separated• 3rd Ventricle is rudimentary• Mild facial anomalies
– Lobar Holoprosencephaly (Least Severe)• Near complete separation of hemipsheres; only anterior
horns fused• Full development of falx and interhemispheric fissure

Holoprosencephaly
Alobar Holoprosencephaly Semilobar Holoprosencephaly

Dandy-Walker Malformation
• Congenital anomaly of the roof of the 4th ventricle with occlusion of the aqueduct of Sylvius and foramina of Magendie and Luschka
• A huge 4th ventricle cyst occupies the area where the cerebellum usually lies with secondary dilation of the 3rd ventricle; absent cerebellar vermis

Dandy-Walker Malformation

Agenesis of the Corpus Callosum
• Complete or partial absence of the connection tissue between cerebral hemispheres– Narrow frontal horns– Marked separation of lateral ventricles– Widening of occipital horns and 3rd Ventricle
• “Vampire Wings”

Agenesis of the Corpus Callosum

Ventriculmegaly• Enlargement of the ventricles
without increased head circumference– Communicating– Non-communicating– Resut of cerebral atrophy
• Sonographic Findings– Ventricles greater than
normal size first noted in the trigone and occipital horn areas
– Visualization of the 3rd and possibly 4th ventricles
– Choroid plexus appears to “dangle” within the ventricular trium
– Thinned brain mantle in case of cerebral atrophy

Hydrocephalus• Enlargement of ventricles with increased
head circumference– Communicating– Non-communicating
• Sonographic Findings– Blunted lateral angles of enlarged lateral
ventricles– Possible intrahemispheric fissure
rupture– Thinned brain mantle
• Aqueductal Stenosis– Most common cause of congenital
hydrocephalus– Aqueduct of Sylvius is narrowed or is a
small channel with blind ends; occasionally caused by extrinsic lesions posterior to the brain stem
– Sonographic Findings• Widening of lateral and 3rd ventricles• Normal 4th ventricle

Hydrancephaly
• Occlusion of internal carotid arteries resulting in necrosis of cerebral hemispheres– Absence of both cerebral
hemispheres with presence of the falx, thalmus, cerebellum, brain stem, and postions of the occipital and temporal lobes
– Sonographic findings• Fluid filled cranial vault• Intact cerebellum and
midbrain

Cephalocele
• Herniation of a portion of the neural tube through a defect in the skull
• Sonographic Findings– Sac/pouch containing brain tissue and/or CSF and
meninges– Lateral Ventricle Enlargement

Subarachnoid Cysts
• Cysts lined with arachnoid tissue and containing CSF• Causes
– Entrapment during embryogenesis
– Residual subdural hematoma
– Fluid extravasation sectondary to meningeal tear or ventricular rupture

Hemorrhagic Pathology
• Subependymal-Intraventricular Hemorrhage (SEH-IVH)– Caused by capillary bleeding in the germinal matrix– Most frequent location is the thalamic-caudate groove– Continued subependymal (SEH) bleeding pushes into the
ventricular cavity (IVH) & continues to follow CSF pathways causing obstruction
– Treatment: Ventriculoperitoneal Shunt– Since 70% of hemorrhages are asymptomatic, it is necessary
to scan babies routinely– Small IVH’s may not be seen from the anterior fontanelle
because blood tends to settle out in the posterior horns
• Risk Factors– Pre term infants– Less than 1500 grams birth weight

Hemorrhagic Pathology
• Grades– Based on the extension of the hemorrhage– Ventricular measurement
• Mild dilation: 3-10 mm• Moderate dilation: 11-14 mm• Large dilation: greater than 14mm
• Grade I– Without ventricular enlargement
• Grade II– Minimal ventricular enlargement
• Grade III– Moderate or large ventricular enlargement
• Grade IV– Intraparenchymal hemorrhage
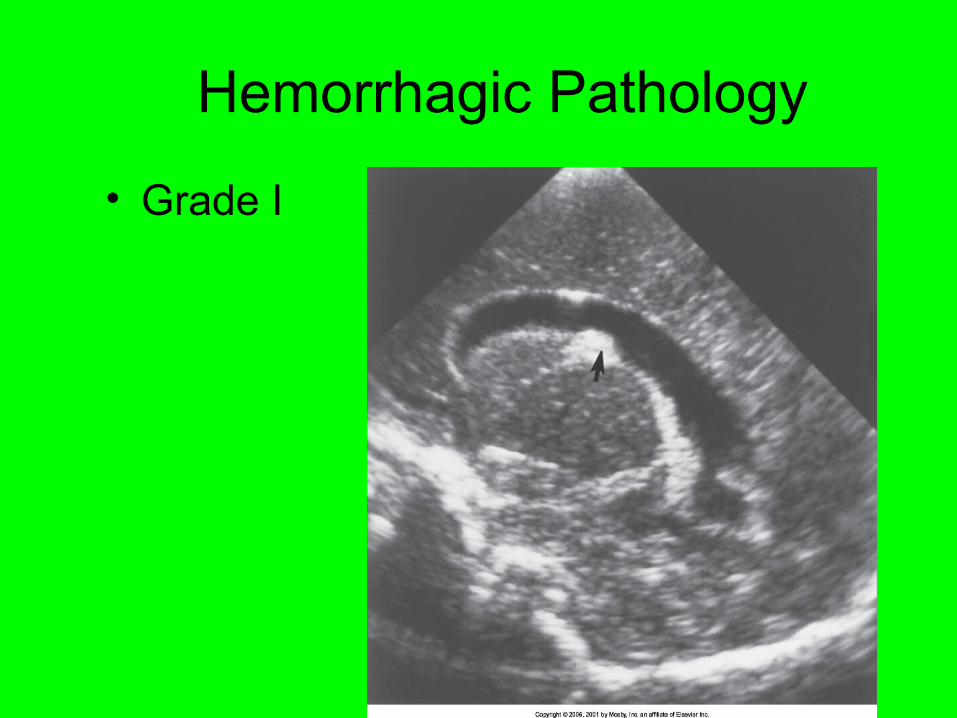
Hemorrhagic Pathology
• Grade I

Hemorrhagic Pathology
• Grade II

Hemorrhagic Pathology• Grade III

Hemorrhagic Pathology
• Grade IV

Intraparenchymal Hemorrhage
• Brain parenchyma destroyed
• Originally considered an extension of IVH, but may actually be a primary infarction of the periventricular and subcortical white matter with destruction of the lateral wall of the ventricle.
• Sonographic Finding– Zones of increased
echogenicity in white matter adjacent to lateral ventricles

Intracerebellar Hemorrhage• Types
– Primary – Venous Infarction– Traumatic Laceration– Extension from IVH
• Sonographic Findings– Areas of increased
echogenicity within cerebellar parenchyma
• Coronal views through mastoid fontanelle may be essential to differentiate from large IVH in the cisterna magna

Epidural Hemorrhages and Subdural Collections
• Best diagnosed with CT because the lesions are located peripherally along the surface of the brain.

Ischemic-Hypoxic Lesions
• Hypoxia: Lack of adequate oxygen to the brain• Ischemia: lack of adequate blood flow to the brain
– Types• Selective neuronal necrosis• Status marmoratus• Parasagittal cerebral injury• Periventricular leukomalacia (PVL), white matter
necrosis (WMN), or cerebral edema• Focal brain lesions (occurs when lesions are distributed
within large arteries)
– Sonographic Findings• Areas of increased echogenicity in subcortical and deep
white matter in the basal ganglia

Ischemic-Hypoxic LesionsPeriventricular Leukomalacia (PVL) or White
Matter Necrosis (WMN)• Most important cause of abnormal neurodevelopment
in preterm infants• Early chronic stage
– Multiple cavities develop in necrotic white matter adjacent to frontal horns
• Middle chronic Stage– Cavities resolve and leave gliotic scars and diffuse
cerebral atrophy – Increased Echogenicity
• Late chronic stage– Echolucencies develop in the echolucent lesions
corresponding to the cavitary lesions in the white matter (cysts)

PVL or WMN1 2
3
4

Brain Infections
• Common infections referred to by TORCH– T: Toxoplasma Gondii
– O: Other (Syphilis)
– R: Rubella Virus
– C: Cytomegalovirus
– H: Herpes Simplex Type 2
• Consequences– Mortality
– Mental Retardation
– Developmental Delay

Ependymitis and Ventriculitis
• Ependymitis– Irritation from hemorrhage within
the ventricle
– Occurs earlier than ventriculitis• Sonographic Features
– Thickened, hypoechoic ependyma (epithelial lining of the ventricles)
• Ventriculitis– Common complication of purulent
meningitis• Sonographic Findings
– Thin septations extending from the walls of the lateral ventricles.

Questions to be answered during exam




Why US spines ?
Spinal ultrasound (SUS) is becoming increasingly accepted as a first line screening test in neonates suspected of spinal dysraphism .


Challenging MRI
The advantages of SUS are not only a diagnostic sensitivity equal to MRI but that, unlike MRI, SUS can be performed portably, without the need for sedation or general anaesthesia.
In addition, MRI is highly dependent on factors affecting resolution, including patient movement, physiological motion from cerebral spinal fluid (CSF) pulsation and vascular flow, factors that do not affect SUS . New generation high frequency ultrasound machines
with extended field of view capability now permit imaging of high diagnostic quality in young babies.

When to perform ?
SUS is possible in the neonate owing to a lackof ossification of the predominantly cartilaginousposterior arch of the spine . The quality ofultrasound assessment decreases after the first3–4 months of life as posterior spinous elementsossify, and in most children SUS is not possiblebeyond 6 months of age. However, the persistingacoustic window in children with posterior spinaldefects of SD enables ultrasound to be performedat any age

When to request US spines ?Current RCR guidelines are thatall neonates with a hairy patch or sacral dimple should undergo SUS . However, while more than 90% of patients with occult SD have a cutaneous abnormality over the lower spine , a cutaneous marker may have a low yield in predicting the presence of a clinically significant abnormality. In a recent review of 200 SUS examinations performed over an 11-year period, SD was found in less than 1% of cases when a cutaneous marker was the only clinically detectedabnormality .

Gastrulation stage

Neurulation stage

Retrogressive differentiation and relative cord ascent
Formation of the ventriculus terminalis, the
caudal portion of the conus medullaris, and the filum terminale through the processes of canalization and retrogressive
differentiation.


Sonographic examination of the neonatal spine is performed with the infant in a warm room lying in a prone, lateral decubitus, or semi-erect position.
Feeding the infant before examination helps him
or her to relax. Placing a towel under the infant’s pelvis will flex
the spine enough to separate the midline posterior arches .
.


A high frequency (7- to 15-MHz) linear-array transducer should be used .. higher frequency transducers are beneficial for optimization of superficial structures such as skin lesions and sinus tracts.
Extended field-of-view (EFOV) imaging is
an additional feature that can demonstrate the whole neonatal spine from T12 to the coccyx

• Mark T 12 in transverse plane (presence of ribs witnessing)
• Then count downwards to end of cord.

Alternatively by
Locating the last lumbar vertebra, L5, byevaluating the lumbosacral junction. Thencount cephalad to the conus medullaris.
Locating the last ossified vertebral body,the first coccygeal segment. Then count thefive sacral segments cephalad into thelumbar vertebra.

The spinal cord lies in the spinal canal within anechoic CSF of the subarachnoid space. Surrounding
the canal is the dura mater, which is shown by anechogenic line dorsal and ventral to the canal. The
cord is lined with the arachnoid sheet, which exhibits an echogenic line parallel to the cord’s surface.
Caudally, the lumbar enlargement tapers, forming the conus medullaris, which extends and becomes the filum terminale.

Filum teminale
The filum terminale images as an echogenic cordlike structure that is surrounded by echogenic nerve roots of the cauda
equina. For that reason, separation of the two is difficult.
However, the filum terminale is commonly more echogenic than the surrounding cauda equina.
The filum terminale normally measure less than or equal to 2 mm.

Cord
On a sagittal image, the spinal cord appears asa hypoechoic cylindrical structure with two echogeniccomplexes centrally. These represent thecentral echo complex. The normal cord lies onethird to one half of the way between the dorsal andventral walls of the spinal canal On a transverse image, the cervical spinal cordappears as an oval shape, whereas the thoracic andlumbar portions are more circular.

Conus level
The level of the conus usually ends between T12 and L1 or L2 .If it ends at the L2-L3 disk space or
lower, it is abnormal, and one should explore for any tethering masses. However, it must be noted that a normal cord may lie around L3, mainly in preterm infants.
The normal position of the cord should be centralin the spinal canal. The spinal cord is held in placeby echogenic dentate ligaments passing laterallyfrom each side of the cord.
The normal spinal cord produces a rhythmic movement

• Standard views


Cystic ventriculus terminalis (normal variant)

Cystic distension of distal spinal canal (normal variant )
Size smaller than
5 mm and stability over time
distinguish this normal variant
from small syrinx.

Filar cyst (normal variant)
criteria for filar cyst:
location just below
conus medullaris, fusiform shape, well defined, thin walled, and hypoechoic.

Pseudo-masses
• Clumped nerve roots..
• Use 2 planes..to see the whole length of nerve root.

Dysmorphic coccyx
• Cartilagenous angulated lesion.
• Not dermal sinus track.

Three processes can lead to congenital anomalies:
First, premature separation of the skin ectoderm from the neural tube can lead to entrapment of mesodermal elements, such as fat.
Second, failed neurulation leads to dysraphisms,
such as myelomeningocele(overt or closed )

Last ,anomalies of the filum terminale, such as fibrolipomas and caudal regression syndrome caused by disembryogenesis of the caudal cell mass

Classification
Congenital spinal dysraphisms can be classified on the basis of the presence or absence
of a soft-tissue mass and skin covering .
Those without a mass include tethered cord,
diastematomyelia, anterior sacral meningocele,
and spinal lipoma.
Those with a skin covered soft-tissue mass include lipomyelomeningocele and myelocystocele.
And those with a back mass but without skin covering include myelomeningocele and myelocele



Lipoma

Dorsal dermal sinus track

Tethered cord
Sonographically, tethered cord is diagnosedin neonates by the presence of a low-lyingconus (below the L2–L3 disk space) andlack of normal nerve root motion during realtimesonography
Search for cause

Intradural lipoma
• Hyperechoic dural mass..
• Tethered cord.

Thick filum terminale

Fatty filum

Lipoma of filum terminale
Tethered cord
L3

Diastematomyelia
• Echogenic spur between two hemicords in transverse image.

Caudal regression syndrome
• Blunted conus medullaris.
• Fatty filum
• Absence of sacral vertebrae and coccyx .

Myelomeningocele
• Cystic mass (CSF)
• +tethered cord
• +neural elements.
• +soft tissue mass

Unilocular meningocele

Lipomyelomenimgeocyle

Trauma evaluation
haematoma

Spinal cord compression
craniocervical narrowing in bone dysplasia


Neuroblastoma

Sacrococcygeal teratoma





Conclusion• Spinal ultrasound (SUS) is becoming
accepted as a first line screening test in neonates with high sensitivity and specificity.
• Recognizing normal anatomy ,variants and congenital anomalies early in life help in futur planning of management .


• Echostructure.
• Size.
• Variations.
• Congenital anomalies.
• Renal abnormality.

RENAL ANATOMY
RENAL CORTEX
MEDULLA
MAJORCALYCES
RENALPELVIS
RENALMEDULLARYPYRAMID
RENALCAPSULEURETER
MINORCALYX
RENAL COLUMN

NORMAL RENAL SONOGRAPHY
• Paired retroperitoneal organs
• Renal sinus- dense central echoes due to renal fat– Contains:
• Collecting system: calyces, infundibula, & part of renal pelvis
– bifid system seen as two separate lobulations
• Renal vessels: renal hilium• Lymphatics
• Fat
• Fibrous tissues

RENAL SINUS
• Central area of the kidney from the medial border
• Bounded by fat– anteriorly and posteriorly by
fibrous sheath known as Gerota’s fascia
– laterally by the laterocoronal fascia which becomes continuous with peritoneum & abdominal wall

RENAL SONOGRAPHY• Renal parenchyma - 2 parts cortex & medulla
– thickest at the renal poles
• Cortex located between capsule & medulla
– low level uniform echoes
– less echogenic than liver & spleen
– Columns of Bertin = columns of cortical tissue located between
pyramids
» can enlarge & mimic a mass
» normal variant
• medulla
– renal volume is estimated by water displacement
• V = 0.49 x length x width x anterior posterior dimension
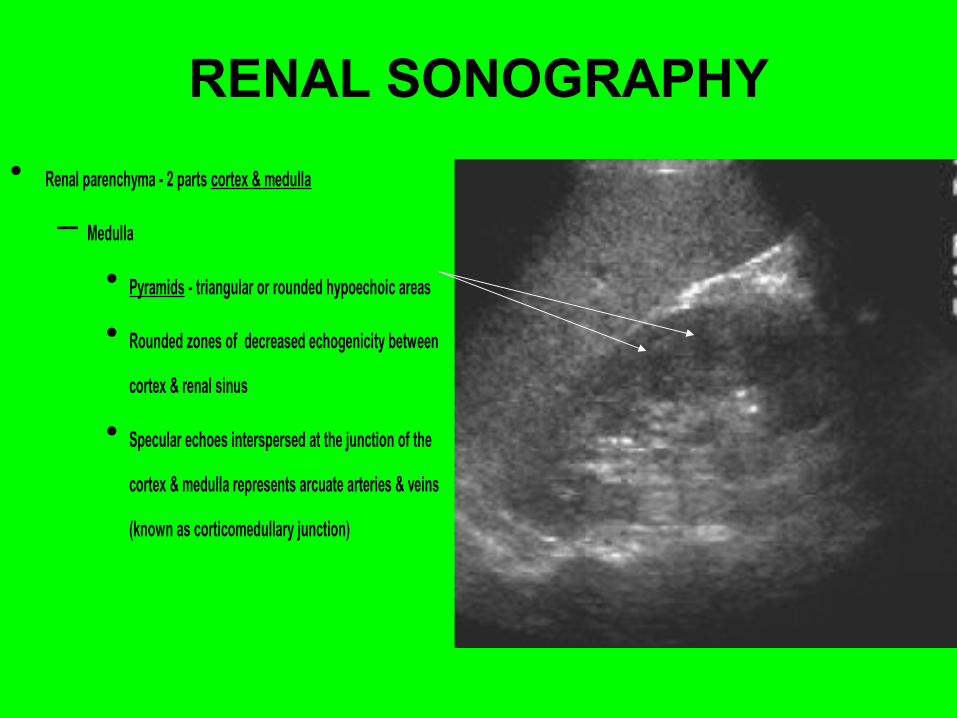
RENAL SONOGRAPHY
• Renal parenchyma - 2 parts cortex & medulla
– Medulla
• Pyramids - triangular or rounded hypoechoic areas
• Rounded zones of decreased echogenicity between
cortex & renal sinus
• Specular echoes interspersed at the junction of the
cortex & medulla represents arcuate arteries & veins
(known as corticomedullary junction)

Dysplastic kidneyrenal parenchymal thickness
compared to normal
cortico-medullary
ratio
larger volume of medulla in the neonatal kidney results in a ratio of cortex to medulla of 1.64:1 in the neonate as compared with a ratio of 2.59:1 in the adult.

RENAL SONOGRAPHY
• Vascular exchange– renal arteries
• come off of aorta - can be multiple
• right renal artery (RRA) - seen posterior to IVC in sagittal plane
– renal veins• come off of IVC
• left renal vein (LRV) - seen between SMA & aorta in the transverse plane

RENAL ARTERY

RENAL SIZE

Normal renal sizeNormal Liver, Spleen, and KidneyDimensions in Neonates, Infants,and Children: EvaluationwithSonography.. AJR:171,December1998

Development

Anomalies and variations• Congenital variations
– fetal lobulations– dromedary hump.– Fusion anomalies :horseshoe -
isthmus of tissue that connects both kidneys
– Ascent anomalies: pelvic kidney fails to migrate from pelvic area during embryology

Renal pyramids ..The normal and abnormal

principle
Focused sonographic evaluation of the pyramids with high-frequency transducers produces the most detailed images of the
pyramids

This improved resolution is best achieved with lineararray transducers functioning at a high megahertz range (even up to 17 MHz)

warning
Those unfamiliar with this normal neonatal appearance,
the relatively large, normal, hypoechoic
pyramids may be misinterpreted as dilated calices
or renal cystic disease and the relatively thinner
hyperechoic cortex may be misinterpreted as
cortical scarring or even ischemic changes.


normal variant
was beleived due to tamm horsfall protein

Obstruction

Ischaemia

Infection-candidiasis
parenchymal or collecting system
fungus ball

Renal vein thrombosis

ARPKD

Spectrum

Beckwith-Wieldmann syndrome
dysplastictubules

Nephrocalcinosis
early late
hyperechoic cortex and medulla

Linear pattern

Punctate pattern

progress to cyst

lesson of presentation

Lesch Nyhan Syndrome
urate crystaldeposition

Glycogen storage disease

Sickle cell anaemia

• Normal neonatal kidney should be evaluated according to:
• Normal echotexture.• Normal size for age.• Normal development.• Excluding normal variants.• Diagnosing congenital anomalies ..and
lastly evaluating a diseased kidney accordingly .


Importance of the finding
• Most common congenital condition discovered by antenatal US.
• ultrasonography enables us to detect the correctable cause of hydronephrosis, such as ureteropelvic junction obstruction.
• Failure of recognizing those needing surgical intervention will result in permanent loss of the kidney.

Fetal hydronephrosis Detection• Grignon et al developed a grading system for hydronephrosis in
fetuses of 20 weeks gestation or greater in relation to their postnatal findings.
• Grade I dilatations (AP renal pelvic diameter up to 1.0 cm) were described as normal and physiologic because none of the affected patients required surgery after birth.
• Grade II (>1.0–1.5 cm) and grade III (>1.5 cm with slight dilatation of calices) dilatation was termed intermediate hydronephrosis; 50% required postnatal surgical intervention.
• All patients with grade IV dilatation (>1.5-cm pelvis, moderate dilatation of calices, no cortical atrophy) or grade V hydronephrosis (>1.5-cm pelvis, severe caliceal dilatation, atrophic renal cortex) required surgery.
• Their work suggests that one should be concerned with pelvic dilatations greater than 10 mm particularly if there is associated calyceal dilatation and loss of cortex.

• Clinically significant disease is more likely if:
• (1) a grade 3 or 4 hydronephrosis is present;
• (2) the renal pelvis diameter is > 10 mm;
• (3) the renal pelvis/kidney ratio is > 0.5.

Incidence:
• Pre-natal ultrasound
–detects fetal anomaly in 1% of pregnancies, of which 20-30% are genitourinary in origin and 50% manifest as hydronephrosis

Grading of Severity of Hydronephrosis
Grade Central RenalComplex
RenalParenchymalThickness
0 Intact Normal
1 Slight splitting Normal
2 Evident splitting Normal
3 Wide splitting Normal
4 Further dilatation Thin

Pathophysiology:
• Anatomic and functional processes interrupts the flow of urine.
• There is a rise in ureteral pressure causing stretching and dilation; if pressures continue to rise, leads to decline in renal blood flow and GFR.
• When significant obstruction is persistent, it affects nephrogenic tissue and results in varying degrees of cystic dysplasia and renal impairment.


Proper evaluation protocol


I-Mild (Grade II)
• These images shows mild dilatation of the pelvis as well as the calyces of the right kidney

II-Moderate (III)
• The above ultrasound images show cupping of the calyces with moderate dilation (Right kidney) of the pelvis and calyces. Despite the hydronephrosis the renal parenchyma is still preserved.

III-severe (IV)
• The above sonographic images show marked dilatation of the pelvicalyces with sever thinning of the renal parenchyma. note almost total absence of normal renal tissue (cortex).


VU reflux

PUJ obstruction..early

PUJ obstruction ..too late

What is this ?


Posterior urethral valve




choosing the probe

Assesment of DDH
• The technique for performing an infant hip sonogram may vary depending upon one's belief as to pathophysiology.
• Initial focus of hip sonography by Graf was on acetabular morphology, using a single static sonographic view.
• Harcke et al, on the other hand, emphasized assessment of instability in addition to morphology and advocated a dynamic sonographic technique.

• The current recommendation for sonographic examination of the infant hip incorporates assessment of both instability and morphology so the pathophysiology issue is resolved with respect to performance of the sonographic examination .

Hip sonographyTABLE 1 -- HIP SONOGRAPHY FOR DEVELOPMENTAL DYSPLASIA OF THE HIP
View Key Feature Comment
Coronal neutral* A Acetabular morphology Measurement optional
Coronal flexion A Acetabular morphology Measurement optional
Stability (if stressed) Stress optional
Used with Pavlik harness
Transverse flexion A Stability Stress required (except during treatment)
Used with Pavlik harness
Transverse neutral Femoral head position Optional view
Data from Harcke HT, Grissom LE: Performing dynamic sonography of the infant hip. AJR Am J Roentgenol 155:837-844, 1990; with permission.

Correct coronal view

Correct transverse view

I-Morphological assesment
• This system is based upon the appearance of the acetabulum in a coronal neutral position and describes measurement of acetabular slope (alpha angle) and position of the acetabular labrum (beta angle).

How to make good exam
• The proper coronal view, whether the femur is in neutral or in flexion, contains three elements .
• (1) The echoes from the bony ilium should be in a straight line parallel to the surface of the transducer.
• (2) The transition from the os ilium to the triradiate cartilage must be seen definitively.
• (3) Finally, the echogenic tip of the cartilage labrum needs to be present in the same plane that contains the other two elements.

Model view

Take your measurements


• Graf classification of infant hips based on the depth and shape of the acetabulum as seen on coronal ultrasonograms.
• Type I: normal; characterized by a well-formed acetabular cup with the femoral head beneath the acetabular roof.
• Type II: immature in infants less than three months of age and mildly dysplastic in infants older than three months; characterized by a shallow acetabulum with a rounded rim.
• Type III: subluxated; characterized by a very shallow acetabulum with some displacement of the femoral head.
• Type IV: dislocated; characterized by a flat acetabular cup and loss of contact with the femoral head.


II- Stability assesment• The assessment of instability incorporates
dynamic technique in two views that include application of stress.
• Both views are performed with the hip flexed: the transducer orientation is coronal for one view and axial for the other.

Relax your patient
• Assessing the hip when the infant is not relaxed masks the presence of instability.
• To ensure a cooperative infant, it is recommended that a sonogram be performed in a quiet, semidarkened environment with a parent present and visible to the child.
• Bottle feeding the infant during the examination is helpful.

• Examination by ultrasound is modeled after the clinical examination and is based upon the provocative test for dislocation of an unstable hip (Barlow test) or the reduction of a dislocated hip (Ortolani test).

• With subluxation and lesser degrees of instability, the flexed hip tends to seat with abduction.
• Displacement is noted during adduction and stress.

• The key feature of instability is the lateral movement (toward the transducer) of the femoral head along the ischium. This results in increased echogenic soft tissue medially.
• Whereas a normal hip shows slight changes in the appearance of the medial tissues between abduction and adduction, with instability, the thickness more than doubles

Dynamic testing
• At rest :Normal.• With stress
subluxation occurs and B angle increases.




Capsule distension

Compare the 2 sides in difficult cases

Transient synovitis versus septic arthritis




where to scan ?

Obtaining the image

Cervix sign-Hamburger sign

Donut sign

Measurements

Gastric contents effect


Related Documents











