Neonatal Intensive Care and Premature Babies By: Holley Dobransky, Maria Gosz, and Jennifer Zabinski

Neonatal Intensive Care and Premature Babies By: Holley Dobransky, Maria Gosz, and Jennifer Zabinski.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Neonatal Intensive Care and Premature
Babies
By: Holley Dobransky, Maria Gosz, and Jennifer
Zabinski

Prematurity A baby delivered at less than 37 weeks
(more than 3 weeks early) The earlier the baby is born the more
severe the health problems will likely be If the baby needs extra help they will be
admitted to the NICU

Ethical Issues Relating to Age Viability
Before 22 weeks Providing care at this stage is experimental.
Attempts to resuscitate should only take place if the outcome looks promising and if the parents choose.
Between 22 weeks, 0 days and 22 weeks, 6 days Standard practice should be not to resuscitate the
baby. Resuscitation should only be attempted if parents request it and they know the risks and potential outcomes.

Ethical Issues Relating to Age Viability
Between 23 weeks, 0 days and 23 weeks, 6 days It is hard to predict the outcome. Parents should
get the final decision but doctors need to inform the parents of there opinion and recommendation.
Between 24 weeks, 0 days and 24 weeks, 6 days Baby will be offered full invasive intensive care and
support unless the parents and doctors feel that for the babies best interest care should not be given.
At 25 weeks and above Intensive care should be given unless he or she is
known to be affected by a severe abnormality that will significantly affect chance of survival.
Risk Factors for Premature Birth Multiple births (twins, triplets, etc.) Infections during pregnancy Chronic health problems in the mother
(diabetes, high blood pressure, heart disease, and kidney disease)
Previous preterm birth Premature rupture of membranes Smoking, drinking, or drug use during
pregnancy
Babies born prematurely are more likely to have problems with…
Feedings Jaundice Breathing Infections Regulating body temperature Anemia Hypoglycemia (low blood sugar)

Breathing Problems Many premature babies will need help
breathing
Respiratory Support Ventilator CPAP Nasal cannula

Ventilator Mechanical ventilation through an
endotracheal tube A tube is placed in the baby’s mouth into the
trachea Oxygen is blown in and out of the lungs
under pressure This is used when the baby cannot breath on
his/her own The machine does most, if not all, of the
breathing for the baby

Baby on a Ventilator

Respiratory Distress Syndrome (RDS) Occurs in premature babies due to the
lack of surfactant in the lungs Surfactant keeps the airways in the
lungs from collapsing Surfactant Therapy allows the baby’s
lungs to further develop rather than putting more effort into fully breathing
Use either a ventilator or CPAP machine

CPAP CPAP- Continuous positive airway pressure Prongs or a mask are positioned over the
baby's face or nostrils Oxygen is given at a constant pressure This is used when a baby can breath on
his/her own The machine helps keep the lungs open
between breaths 5-6 LPM
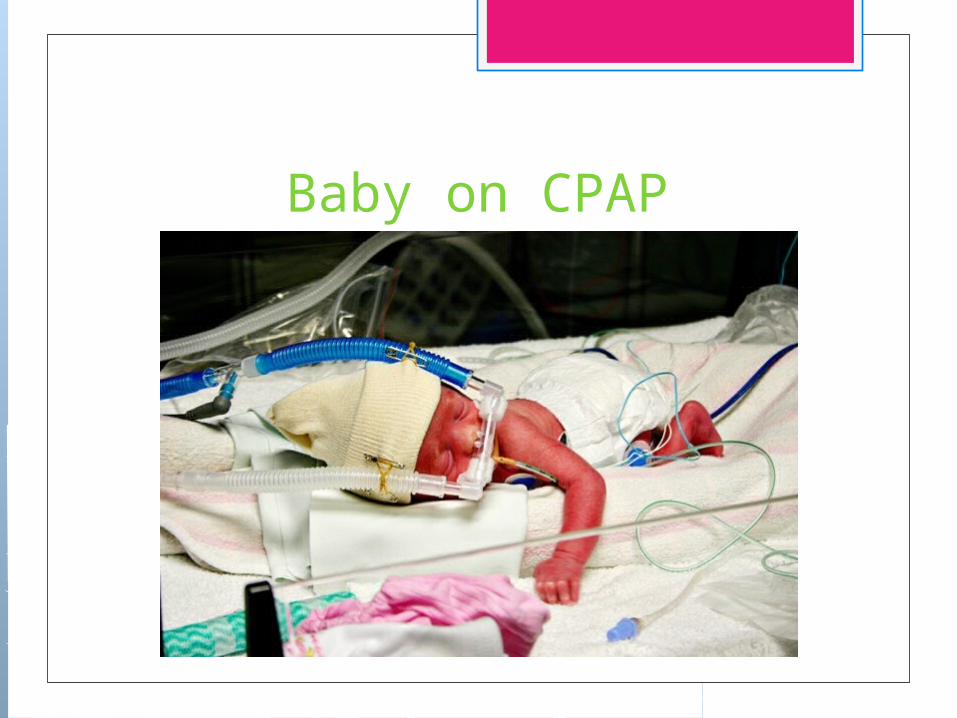
Baby on CPAP
Nasal Cannula Small prongs deliver oxygen to the baby
through the nostrils This is used when the baby does not
need CPAP to keep the lungs open, but still needs extra oxygen
1-3 LPM

Baby on Nasal Cannula

ThermoregulationIsolette Warmer
Brain Cooling Program Babies must be at least 36 weeks old Used on babies who had the potential of
asphyxiation in the womb The lack of oxygen can lead to lack of
blood to the brain which later affects the rest of the body
Reduction in the babies core temp to allow it to recover from the lack of oxygen
Hyperbilirubinemia Also called jaundice Refers to a yellowing of the skin and/or eyes Caused by a buildup of bilirubin in the blood Bilirubin is produced by the normal
breakdown of red blood cells Usually the liver breaks down the bilirubin
and passes it through the body When the bilirubin builds up faster than the
liver can break it down, jaundice occurs

Hyperbilirubinemia All babies are born with red blood cells
that they don’t need As their body breaks down the cells, an
orange color (bilirubin) is released into the blood
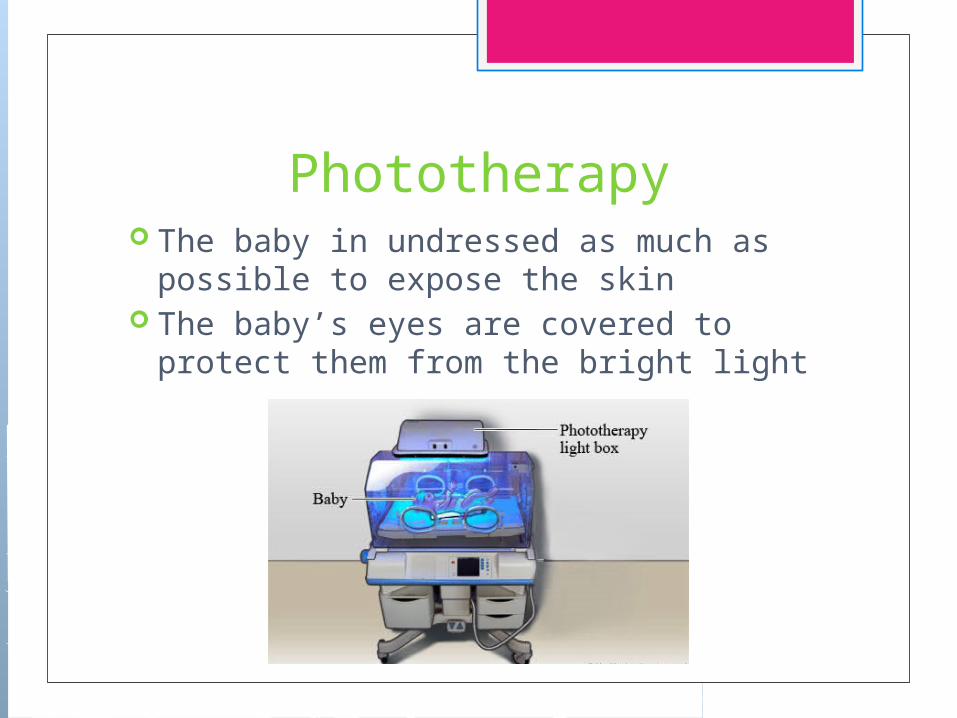
Phototherapy The baby in undressed as much as
possible to expose the skin The baby’s eyes are covered to protect
them from the bright light

Phototherapy

Total Parenteral Nutrition (TPN) TPN is IV nutrition given to babies who
cannot yet handle food Infants who are very premature have
immature digestive systems that cannot handle milk or formula
It is also given to babies who are unable to absorb enough nutrients through regular feedings
TPN

Breast Milk Breast milk has an advantage over formula
because it contains proteins that help fight infection and promote growth
Can be given by bottle or by gavage (tube) feeding
Fortifiers may be added to the milk to give the baby more vitamins and minerals
20 calories per ounce Calories can be added to the milk to make it 22
or 24 calories if the baby needs to grow faster
Formula There are special formulas designed for
premature babies Can be given to the baby by bottle or
gavage feeding

NG Tube Feedings NG- Nasogastric A small tube is placed into the baby’s
stomach through the nose Breast milk or formula is given through
the tube directly into the stomach, giving the baby extra calories
The tube is replaced frequently

Baby with NG Tube

NICU Around the World 800 women die a day from
preventable causes related to pregnancy and childbirth
2.9 million newborns die within the first month, and 2.6 million are still born
Main causes are preventable and treatable, such as complications due to premature birth, complications during delivery and infection.
Equivalent to the population of Minnesota dying every year
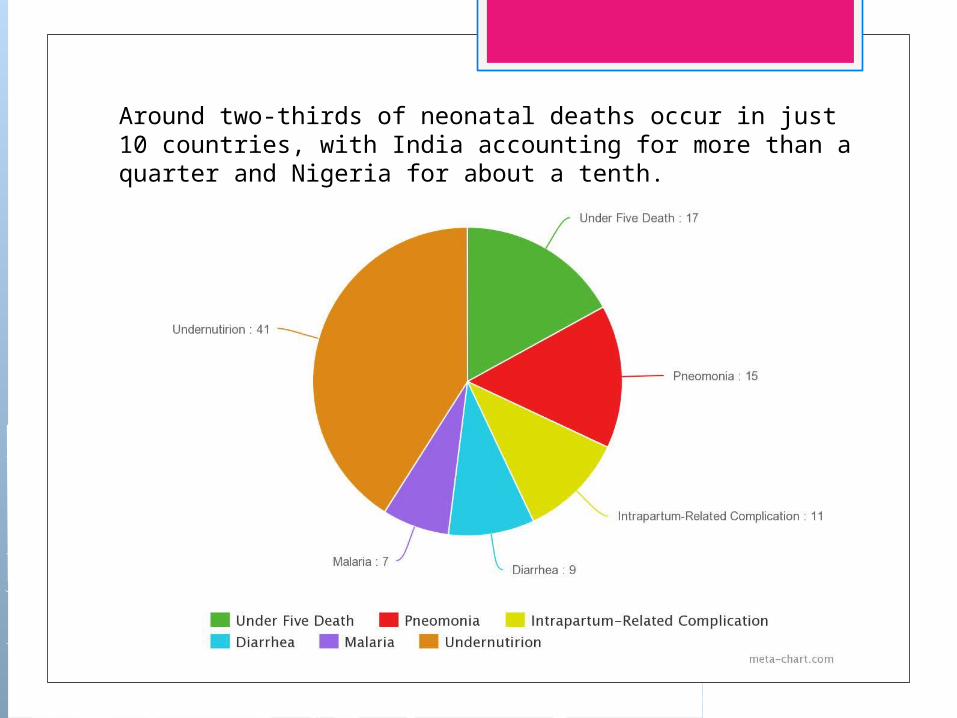
Around two-thirds of neonatal deaths occur in just 10 countries, with India accounting for more than a quarter and Nigeria for about a tenth.

Mortality Rates in 1,000 Highest Rates
Afghanistan 117 Mali 104 Somalia 100 Central African
Republic 92 Guinea-Bissau 90 Chad 90 Niger 86 Angola 79
Lowest RatesJapan 2Norway 2.5Singapore 2.5Italy 3.3Canada 4.7United States
6

44% of child deaths under the age of five take place during the neonatal period.
Prevention measureVaccinesGood NutritionBreast feedingAntibioticsZinc Supplements Low-osmolality oral rehydration

Sources http://www.ncbi.nlm.nih.gov/books/NBK11389/ http://nuffieldbioethics.org/wp-content/uploads/2014/07/CCD-Short-Version-FINAL.pdf http://www.tommys.org/prem/hospital/breathing http://www.nlm.nih.gov/medlineplus/ency/article/001562.htm http://www.nlm.nih.gov/medlineplus/ency/article/007302.htm http://www.marchofdimes.org/baby/newborn-jaundice.aspx# http://www.med.umich.edu/1libr/pa/umphototherapy.htm http://kidshealth.org/parent/growth/growing/preemies.htm http://www.healthline.com/health/pregnancy/premature-baby-infections http://
www.mayoclinic.org/diseases-conditions/premature-birth/basics/risk-factors/con-20020050
http://www.mayoclinic.org/diseases-conditions/premature-birth/basics/definition/con-20020050
http://www.gatesfoundation.org/What-We-Do/Global-Development/Maternal-Newborn-and-Child-Health
http://www.who.int/mediacentre/factsheets/fs178/en/ https://www.cia.gov/library/publications/the-world-factbook/rankorder/2091rank.html http://
www.childmortality.org/files_v19/download/unicef-2013-child-mortality-report-LR-10_31_14_195.pdf
http://www.gatesfoundation.org/What-We-Do/Global-Development/Maternal-Newborn-and-Child-Health
http://www.saintpetershcs.com/Advanced-Technologies-NICU/ http://www.saintpetershcs.com/Advanced-Technologies-NICU/ http://www.saintpetershcs.com/Advanced-Technologies-NICU/
Related Documents











