Neil Ferguson Dept. of Infectious Disease Epidemiology Faculty of Medicine Imperial College Antiviral use in a pandemic: predicting impact and the risk of resistance

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Neil Ferguson
Dept. of Infectious Disease EpidemiologyFaculty of Medicine
Imperial College
Antiviral use in a pandemic:predicting impact and the risk of resistance

Introduction
• Modelling antiviral use in a pandemic
• Effect of treatment on transmission
• Post-exposure prophylaxis
• Use in containment at source
• Uncertainties
• Antiviral resistance:
Seeded resistance
Evolution of resistance

Modelling approach
workplace
household
elementary school
secondary school
workplace
• State-of-the-art large scale simulation (up to 300 million pop.)
• Individuals reside in households, but go to school or a workplace during the day.
• Transmission probabilities are specified separately for households and different place types.
• Local movement/travel : random contact between strangers, at a rate which depends on distance.
• Air travel incorporated.

Influenza natural history
• New analysis of best available data on pandemic and inter-pandemic flu.
• Short incubation period – 1-2 days.
• People most infectious very soon after symptoms.
0
2
4
6
8
10
12
14
16
0
0.5 1
1.5 2
2.5 3
3.5 4
4.5 5
Days
Fre
qu
enc
y
0
0.5
1
1.5
2
0 2 4 6 8 10
Days post infection
Infe
cti
ou
sn
es
s
.
0
1000
2000
3000
4000
5000
Vir
al l
oa
d (
da
ta)
.

Assumptions about antiviral effect
• Values initially used estimated by Longini et al from analysis of Roche data.
Treatment (or PEP) assumed to reduce infectiousness by 60%, from time treatment starts.
Uninfected individual on prophylaxis has 30% drop in susceptibility (=risk of infection per exposure event).
Prophylaxis reduces chance of becoming a ‘case’ by 65%.
• Now using updated values, but results v. similar.

Clinical influenza
• Previous work assumed 50% of infections become ‘clinical cases’ – i.e. have ILI, independent of age.
• Have also looked at 67% (value used by Longini and others).
• More important quantity is proportion of infections seeking healthcare – here Longini and Ferguson assumptions more similar (Ferguson assumed 90% cases sought healthcare, Germann assumed 60%).
• Cases assumed to be 2-fold more infectious than non-ILI-generating infections (assumption based on data from Hayden et al. & Cauchemez et al.).
• Aetiology of disease complex and variable, even for pandemics. No clear basis to predict age-specific clinical attack rates.

• Large urban centres affected first, followed by spread to less densely populated areas. Epidemic only a little slower than GB.
A US pandemic
0
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
0 30 60 90 120 150 180Day of global outbreak
Da
ily
cas
es
First UScase
Up to 12% absenteeism at peak
R0=2.0/1.7

Mitigation: case treatment
• Main effect is to reduce severity of cases, but treatment within 24h of onset can also reduce transmission (reduction the proportion ill from 34% to 28%).
• 25% stockpile is then just enough, assuming 90% of ‘cases’ receive drug – but demand may be higher.
• Effect relies on very early treatment – within 24h – since infectiousness peaks soon after symptoms start.
• 48h delay gives no reduction in transmission and much poorer clinical benefit.
• So 25% stockpile is bare minimum – could well lead to rationing.
0
0.5
1
1.5
2
0 2 4 6 8 10
Days post infection
Infe
cti
ou
sn
es
s
.0
1000
2000
3000
4000
5000
Vir
al l
oa
d (
da
ta)
.
No treatment
2 day delay
1 day delay
0 day delay
0%
10%
20%
30%
40%
Att
ack
rate
R0

Household prophylaxis (PEP)
• Household prophylaxis+ treatment of everyone in house of case, not just case herself.
• 2006 Nature paper results: Combined with school closure and rapid case treatment, PEP can reduce clinical case numbers by ~1/3 for R0=2– but needs antiviral stockpile of 50% of population.
• UK now increasing stockpile to >50%, considering role for household PEP.

Varying timing and coverage in PEP
• Table shows cumulative clinical attack rate over pandemic.
• Results assume case treatment and prophylaxis of households of treated cases.
• No NPIs.
• Even with only 75% coverage and a 2 day delay, PEP can reduce attack rates by 25%.
• But effect v limited for >2 day delay.
Delay to treat(days)
% cases detected and treated R0=1.9 R0=2.4
N/A 0 32 39
0 50 23 30
75 20 27
90 18 25
1 50 25 32
75 22 28
90 20 27
2 50 27 34
75 24 32
90 23 30
3 50 28 36
75 26 34
90 26 33

Stockpile sizes required for PEP
• As previous slide, but showing antiviral courses used, as % of population size.
• No allowance for wastage made here (e.g. due to treating non-flu ILI).
• Conservatively, need drug for 75% of population to cover all these scenarios and allow for some wastage.
Delay to treat(days)
% cases detected and treated R0=1.9 R0=2.4
N/A 0 0 0
0 50 39 47
75 48 60
90 52 66
1 50 39 47
75 50 60
90 55 66
2 50 40 48
75 51 61
90 56 67
3 50 40 48
75 52 61
90 58 67

Use of AV incontainment at source
• Need to add geographically targeted mass prophylaxis to treatment and close contact PEP to block transmission enough to achieve control.
• Still also need NPIs (and vaccine also helps).
• Need a maximum of 3m courses of drug – if you need more then outbreak is too large to be contained.
• Need to detect outbreak at <50 cases, react to new cases in 2 days.
• Too intensive to be used except in containment at source.

Uncertainties
• Nature of virus – modelling assumes next pandemic virus will look like past pandemic viruses – but H5N1 might be different, and the duration and dose of NAI required for treatment may differ.
• Transmission rates in different settings.
• (Real-world) effectiveness of drug.
• Adherence.
• Behavioural responses to epidemic and other controls.
• Antiviral resistance.
• …..

Antiviral resistance
• Resistance only a major issue during a pandemic if a resistant strain emerges with close to the transmission fitness of wild-type.
• Current spread of oseltamivir-resistant H1N1 strains demonstrates this is a possibility.
• But we have no idea of the probability (per treated &/or infected person) of such a strain emerging during a pandemic.
• So can only look at plausible illustrative scenarios.
• Two possibilities:
Resistance emerges elsewhere and a mixture of sensitive and resistant strains are seeded into your country.
Resistance emerges for the first time in your country.

Selection of resistance: theoretical worst case
• Amplification of resistance depends on level and promptness of treatment & prophylaxis.
• Reduction in attack rate from antivirals also quantifies selection pressure for resistance.
• If all cases were treated instantaneously, attack rate would be reduced to 24%. Adding 100% prophylaxis would give 16%.
• But if 1% of infections entering country at start of epidemic are resistant, antiviral effect substantially reduced.
• Resistance substantially ampilfied, esp. by PEP.
Worst-case – 100% of cases get instantaneous treatment or treatment+ household PEP from day 1. No NPI.
26.3%28.2%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
Treat only Treat+PEP
Clin
ical
att
ack
rate
21%
72%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Treat only Treat+PEP
Prop
orti
on o
f all
case
s in
fect
ed w
ith
resi
stan
t vir
us
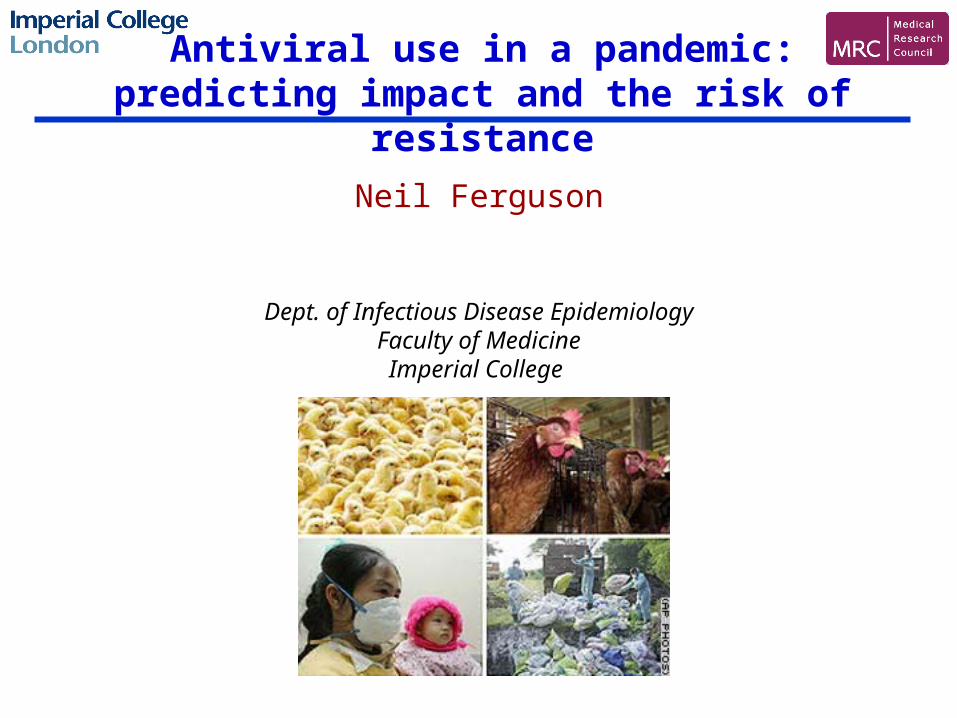
Real-world selection pressurefor resistance
• Delays in real-world treatment mean weaker selection, so much less amplification of resistance.
• Large-scale use of household prophylaxis would amplify resistance more, but effect still v. limited.
• Final level of resistance can be less than seeded proportion, due to ‘head start’ of sensitive epidemic.
Treatment of 60% of cases within 1 day of onset. Treatment starts after 1000 cases in US.
0.9%
1.8%
0.0%0.2%0.4%0.6%0.8%1.0%1.2%1.4%1.6%1.8%2.0%
Treat only Treat+PEP
Prop
orti
on o
f all
case
s in
fect
ed w
ith
resi
stan
t vir
us

0.0035%
0.0094%
0.000%0.001%0.002%0.003%0.004%0.005%0.006%0.007%0.008%0.009%0.010%
Treat only Treat+PEP
Prop
orti
on o
f all
case
s in
fect
ed w
ith
resi
stan
t vi
rus
1%
30%
0%
5%
10%
15%
20%
25%
30%
35%
Treat only Treat+PEP
Prop
orti
on o
f all
case
s in
fect
ed w
ith
resi
stan
t vi
rus
de novo evolution of resistance
• Assume risk per infected person per day of generating a transmission fit resistant virus of 10-4 and10-5 - pessimistic values.
• In reality evolution of transmissible resistant strain probably requires multiple changes, so this is worst case.
• Treatment of clinical cases never results in substantial resistance overall.
• For very pessimistic assumptions, household PEP can strongly select for resistance.
Instantaneous treatment of all cases from 1st case in US, 10-4 mutation rate.
60% of cases treated in 24h from 1000th case, 10-5 mutation rate.

Conclusions
• Treatment needs to be delivered rapidly to have best direct and indirect effect.
• Household prophylaxis+treatment on its own can reduce attack rates by 1/3, if delivered ‘rapidly’ to >75% of households of cases.
• Large scale prophylaxis (i.e. community rather than household), can achieve near-control, but delivery equally challenging.
• A combination of interventions gives more failsafe policy (e.g. NPIs slow spread of resistance).
• Antiviral resistance only likely to be a larger problem in the first wave if it emerges very early in the pandemic, with virus being fully fit.
• If transmissible resistant strains do emerge early, prophylaxis should be used with caution.

Collaborators
Christophe Fraser Simon Cauchemez
Aronrag Meeyai
Don BurkeDerek Cummings
Steven Riley Sopon Iamsirithaworn
RTI IncNCSA
NIH MIDAS programme

Private stockpiles(bought in advance by households)
• US Govt. initiative to encourage households to stockpile antiviral medkits.
• Modelling predicts impact of 25% private stockpile on attack rates negligible.
• Some reduction in demand for public stockpile (25% public stocks might then be enough).
• Could be huge geographic (income-related) disparities in uptake.
• The same money far better invested in public stocks – if distribution efficient.
0 – 5%5-10%10-15%15-20%20-25%25-30%30-35%35-40%40-45%45-50%50-55%55-60%60%+ (max 67%)
Related Documents