1 Nausea and Vomiting in Pregnancy Tekoa L. King CNM, MPH June 7, 2016 Disclaimer • I do not have any financial relationships with any of the products mentioned in this presentation Objectives • Review of epidemiology of NVP • Discuss efficacy and safety of pharmacologic treatments • Algorithm for diagnosis and treatment of NVP A modern day presentation…… • Sarah is G1 P0 now7 weeks after her LMP presenting for her first prenatal visit • c/o “nausea all day” vomits once or twice and retches when she brushes her teeth. Sensitive to smells. Sx present x 2 weeks • Wearing sea bands her sister gave her but they are not helping • Urinating less frequently than usual and urine sp gr is 1030

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Nausea and Vomiting in Pregnancy
Tekoa L. King CNM, MPHJune 7, 2016
Disclaimer• I do not have any financial relationships with any of
the products mentioned in this presentation
Objectives• Review of epidemiology of NVP
• Discuss efficacy and safety of pharmacologic treatments
• Algorithm for diagnosis and treatment of NVP
A modern day presentation……• Sarah is G1 P0 now7 weeks after her LMP presenting for her
first prenatal visit
• c/o “nausea all day” vomits once or twice and retches when she brushes her teeth. Sensitive to smells. Sx present x 2 weeks
• Wearing sea bands her sister gave her but they are not helping
• Urinating less frequently than usual and urine sp gr is 1030

2
How Would You Treat Her?A. Review non-pharmacologic
treatments and schedule a return visit in a week
B. Prescribe Diclegis, metoclopramide, or another anti-emetic and offer IV hydration
C. Admit for IV hydration, NPO, start ondansetron
D. Other
R e vi e w
n o n- p h
a r ma c o
l o g ..
P r es c r i
b e Di c l e
g i s , m e
t o c .. .
A d mi t f o
r I V h y d
r a t io n ,
. . . O t he r
48%
2%9%
41%
Nausea and Vomiting of Pregnancy (NVP)
Niebyl JR 2010 NEJM, Lacroix R 2000, Matthews A et al Cochrane review 2014
• 50-80% of all pregnant women experience NVP– 50% experience retching– 25% have nausea only– 25% unaffected
• Mean onset is ~ 5th wk s/p LMP, peaks at 9th wk– 60% resolve by 12-14 weeks– 90% resolve by 20 weeks– 5% will have symptoms throughout pregnancy
• Second most common reason for prenatal hospitalizations in US (11.4% of all non-delivery antenatal admissions)
Women’s Reports of NVP• Effect of NVP
– 50% say NVP affects their ability to work– 25% require time off from work– 50% say it affects their relationship– 55% report being depressed
• Effect of severe NVP or hyperemesis:– 76% changed plans for future children– 15% terminated pregnancy secondary to hyperemesis– 7% with long-term psychologic sequelae
• Yet, 75% of women with NVP are worried that drugs to treat NVP are teratogenic
Miller F 2002, O’Brien B 1992, Poursharif B 2007, Baggley 2004
Modified “PUQE” INDEX
Score: MILD: < 6; MODERATE: 7-12; SEVERE: ≥ 13
1. On an average day, for how long do you feel nauseated or sick to your stomach?
> 6 hrs(5 pts.)
4-6 hrs(4 pts)
2-3 hrs(3 pts)
≤1 hr(2 pts)
Not at all(1 pt)
2. On an average day how many times do you vomit or throw up?
7 or more(5 pts)
5-6 (4 pts)
3-4 (3 pts)
1-2 (2 pts)
None (1 pt)
3. On an average day how many times do you have retching or dry heaves without bringing anything up?
7 or more(5 pts)
5-6 (4 pts)
3-4 (3 pts)
1-2 (2 pts)
None (1 pt)
Lacasse A et al 2008, Koren G 2005, Ebrahimi N 2009

3
Pathways that Mediate Nausea and Vomiting Offer Several Targets for Pharmacologic Treatments
Vomiting Center(H1, Achm, 5HT3)
Cortex (anxiety)
Vestibular system(H1)
Chemoreceptor trigger zone(D2, 5HT3, H1)
GI tract(5HT3)
Ondansetron, Phenothiazines,AntihistaminesMetoclopramide
Metoclopramide
Antihistamines
LorazepamPharmacologic Therapies
1. Antihistamines (H1 antagonists)– Diphenhydramine
(Benadryl)– Doxylamine (Unisom)
2. Anticholinergics– Dicyclomine (Bentyl)
3. Dopamine antagonistsa. Phenothiazines (Central D2
antagonists)• Promethazine (Phenergan)• Prochlorpemazine (Compazine)
b. Benzamides (Central and peripheral D2 antagonist)
• Metoclopramide (Reglan)
c. Butyrophenones (tranquilizers with anti-emetic profile similar to the phenothiazines)
• - Droperidol (Inapsine)
Pharmacologic Therapies cont.
4. Serotonin antagonist– Ondansetron (Zofran)
5. Corticosteroids– Methylprednisolone (Medrol)
6. Cannabinoids
Prescribing Practices for NVP
Koren G 2014

4
Therapies for NVP and HG
SafetyEfficacy
vs
The treatment of NVP is largely supportive
Vitamin B6 (Pyridoxine)• Efficacy:
– 2 RCTs found pyridoxine (10 mg to 25 mg TID) more effective than placebo in � NVP
– Cochrane Review • Non-significant effect on emesis
– OR, 0.75; 95% CI, 0.35-1.66• Modest effect on nausea score
– OR, 0.92; 95% CI, 0.40-1.44• Safety:
– No teratogenic risks• ACOG recommends first line therapy with or without doxylamine
Shakian V et al 1991, McKeigue PM et al 1994 Vutyavanich T et al 1995, Kutcher JS et al 2003
The Bendectin Story• 10 mg doxylamine/10 mg pyridoxine/10 mg dicyclomine qd
to qid• Approved by FDA for NVP in 1956• Dicyclomine removed from product in 1970’s• 1980: lawsuits and media coverage resulted in Bendectin
being discontinued in 1983• Remained in use in Europe and Canada
• Efficacy: in treating NVP in 2 RCTs – RR 0.53 (95% CI 0.41-0.68)
• Safety: Pooled RR for fetal malformation in multiple studies– RR 0.98 (95% CI 0.93-1.02)
Magee LA et al 2002, Koren G 2015, Jewel Cochrane 2003
Time-Trend of NVP Hospitalization RateLimb Reduction Deformities, and Bendectin Usage
(1974-1994)
NVP-18McKeigue PM et al 1994
NVP Hospitalizations*
Limb Reduction Deformities
Bendectin Sales
*NVP hospitalizations per 10,000 live births

5
2013: FDA Approves Diclegis Diclegis• 10 mg doxylamine and 10 mg pyridoxine in a delayed release
tablet– Usual dose is 2 tablets at night– If insufficient response add 1 tablet taken in the morning– Max dose is qid: 1 in morning, 1 in afternoon and 2 tabs at
night• Instructions
– Take on an empty stomach as some foods inhibit absorption
– Needs to be taken regularly and not prn because the delayed release is a critical component of effectiveness
Diclegis• Contraindications
– Known hypersensitivity to doxylamine or ethanolamine derivative antihistamines, or pyridoxine
– MAO inhibitors intensify and prolong anticholinergic and CNS effects
• Warnings– Classified as an antihistamine: may cause somnolence– Not recommended if drinking alcohol or taking sedatives– Anticholinergic effects: persons with asthma, narrow angle
glaucoma, stenosing peptic ulcer, or urinary bladder neck obstruction should use it with caution
Diclegis• Few interesting notes:
– Mechanism of action is not known
– Pharmacokinetics are interesting:• Peak concentration is 5-7 hours• No pregnancy induced changes in pharmacokinetics• Doxylamine accumulates but pyridoxine does not• Terminal half life is 12.5 hr and 0.5 hr respectively
– Has not been studied in adolescents or women with hyperemesis
– Breastfeeding women should not take Diclegis– Fatalities reported following pediatric overdose
Matok et al 2014, Duschesney Prescribing information for Diclegis

6
Studies of Diclegis• Efficacy:
– Significant reduction of nausea and vomiting and improvement in quality of life
– Koren G 2010: Double blind RCT, N = 261• Mean change in PUQE score from before treatment to
after 3 days of treatment– 4.8 ± 2.7 in Diclegis group vs 3.9 ± 2.6 in Placebo
group (P = .006)– Similar differences in global assessment of
wellbeing– No difference in reports of adverse effects between groups
• Overall in older studies this drug combination results in an average of 70% reduction in NVP
Koren G 2010, Magee LA 2002, ACOG 2015
Studies of Diclegis• Safety:
– More than 170,000 women in case control and cohort studies found no increase in adverse fetal/newborn effects
Punchline:• Initiation before symptoms is more effective than waiting for
symptoms to appear• Diclegis is more effective than homemade combinations because
the extended release formulation appears to work better than short-acting over-the-counter formulations
• ACOG recommends this combination of doxylamine/pyridoxine as the first-line drug if non-pharmacologic measures are not effective
Koren G 2010, Magee LA 2002, ACOG 2015, McKeigue KM 1994
Antihistamines: H1 BlockersDoxylamine (Unisom), Diphenhydramine (Benadryl),
Dimenhydrinate (Dramamine), Hydroxyzine (Atarax, Vistaril), Meclizine (Antivert)
• Effectiveness: – Effective in � vomiting– RR 0.34 (95% CI 0.27-0.43)– OR for drowsiness 2.19 (95% CI 1.1-4.4)
• Safety: – 24 RCTs of various antihistamines– First trimester exposure to antihistamines is associated with a
slightly lower risk of major/minor malformations • OR 0.76 (95% CI 0.60-0.94)
Magee AL et al 2002, Seto A et al 1997 Jewell DA 2003
AnticholinergicsDicyclomine (Bentyl) and Scopolamine (Transderm)
• Dicyclomine – No evidence of effectiveness – No evidence of risk in Bendectin studies
• Scopolamine– Used in non-pregnant persons for N&V– Transdermal patch– Effectiveness: No studies on effectiveness in NVP– Safety: Two observational studies of ~336 women with 1st
trimester exposure found no evidence of � risk to fetus
Mazzotta & Magee 2000, Magee LA 2002
7
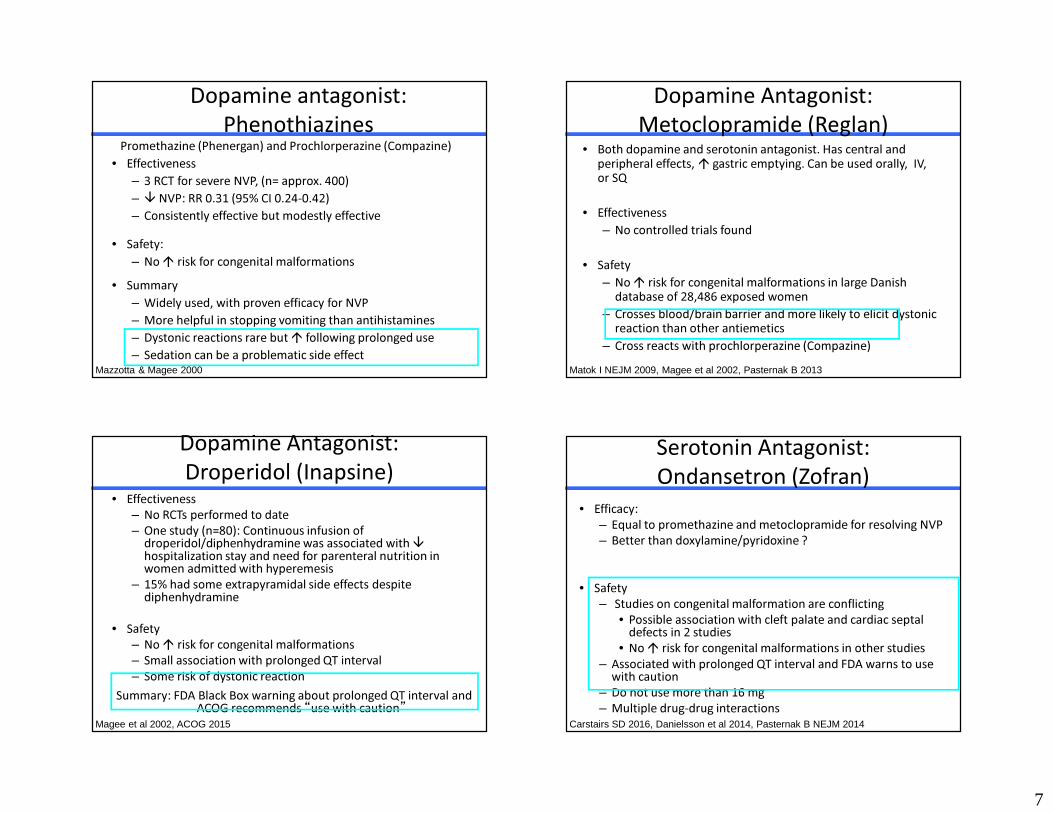
Dopamine antagonist: Phenothiazines
Promethazine (Phenergan) and Prochlorperazine (Compazine)• Effectiveness
– 3 RCT for severe NVP, (n= approx. 400)– � NVP: RR 0.31 (95% CI 0.24-0.42)– Consistently effective but modestly effective
• Safety:– No � risk for congenital malformations
• Summary– Widely used, with proven efficacy for NVP – More helpful in stopping vomiting than antihistamines– Dystonic reactions rare but � following prolonged use– Sedation can be a problematic side effect
Mazzotta & Magee 2000
Dopamine Antagonist: Metoclopramide (Reglan)
• Both dopamine and serotonin antagonist. Has central and peripheral effects, � gastric emptying. Can be used orally, IV, or SQ
• Effectiveness– No controlled trials found
• Safety– No � risk for congenital malformations in large Danish
database of 28,486 exposed women– Crosses blood/brain barrier and more likely to elicit dystonic
reaction than other antiemetics– Cross reacts with prochlorperazine (Compazine)
Matok I NEJM 2009, Magee et al 2002, Pasternak B 2013
Dopamine Antagonist:Droperidol (Inapsine)
• Effectiveness– No RCTs performed to date– One study (n=80): Continuous infusion of
droperidol/diphenhydramine was associated with �hospitalization stay and need for parenteral nutrition in women admitted with hyperemesis
– 15% had some extrapyramidal side effects despite diphenhydramine
• Safety– No � risk for congenital malformations– Small association with prolonged QT interval– Some risk of dystonic reaction
Summary: FDA Black Box warning about prolonged QT interval and ACOG recommends “use with caution”
Nageotte M 1996, ACOG 2004, Magee et al 2002Magee et al 2002, ACOG 2015
Serotonin Antagonist:Ondansetron (Zofran)
• Efficacy: – Equal to promethazine and metoclopramide for resolving NVP– Better than doxylamine/pyridoxine ?
• Safety– Studies on congenital malformation are conflicting
• Possible association with cleft palate and cardiac septal defects in 2 studies
• No � risk for congenital malformations in other studies– Associated with prolonged QT interval and FDA warns to use
with caution– Do not use more than 16 mg– Multiple drug-drug interactions
Carstairs SD 2016, Danielsson et al 2014, Pasternak B NEJM 2014
8
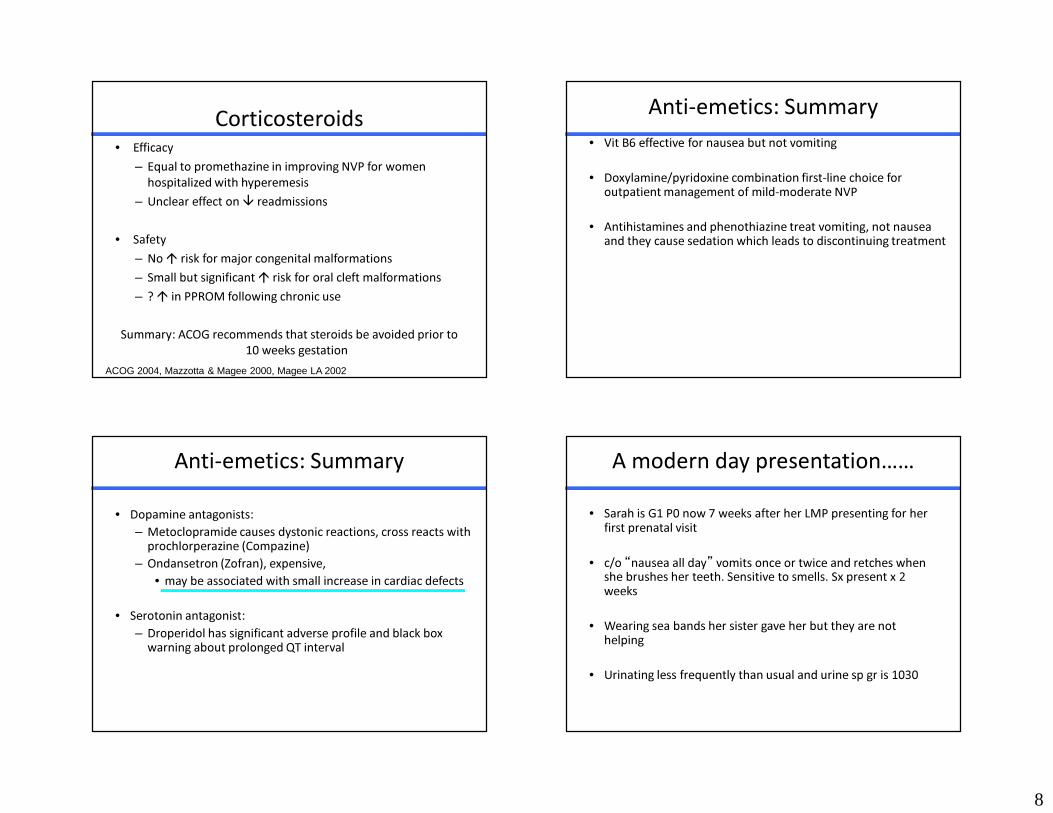
Corticosteroids• Efficacy
– Equal to promethazine in improving NVP for women hospitalized with hyperemesis
– Unclear effect on � readmissions
• Safety – No � risk for major congenital malformations– Small but significant � risk for oral cleft malformations– ? � in PPROM following chronic use
Summary: ACOG recommends that steroids be avoided prior to 10 weeks gestation
ACOG 2004, Mazzotta & Magee 2000, Magee LA 2002
Anti-emetics: Summary• Vit B6 effective for nausea but not vomiting
• Doxylamine/pyridoxine combination first-line choice for outpatient management of mild-moderate NVP
• Antihistamines and phenothiazine treat vomiting, not nausea and they cause sedation which leads to discontinuing treatment
Anti-emetics: Summary• Dopamine antagonists:
– Metoclopramide causes dystonic reactions, cross reacts with prochlorperazine (Compazine)
– Ondansetron (Zofran), expensive, • may be associated with small increase in cardiac defects
• Serotonin antagonist: – Droperidol has significant adverse profile and black box
warning about prolonged QT interval
A modern day presentation……• Sarah is G1 P0 now 7 weeks after her LMP presenting for her
first prenatal visit
• c/o “nausea all day” vomits once or twice and retches when she brushes her teeth. Sensitive to smells. Sx present x 2 weeks
• Wearing sea bands her sister gave her but they are not helping
• Urinating less frequently than usual and urine sp gr is 1030

9
How Would You Treat Her?A. Review non-pharmacologic treatments
and schedule a return visit in a weekB. Prescribe Diclegis, metoclopramide, or
another anti-emetic and offer IV hydration
C. Admit for IV hydration, NPO, start ondansetron
D. Other
R e vi e w
n o n- p h
a r ma c o
l o g ..
P r es c r i
b e Di c l e
g i s , m e
t o c. . .
A d mi t f o
r I V h y d
r a t io n ,
. . . O t he r
17%
1%2%
80%
Algorithm for Managing NVP
ACOG 2004, Einarson A et al 2007
PUQE INDEXMILD NVP
Stop prenatal vitamins with iron
Vit B6 10 mg tid-qidand/or
Acustimulation bandsGinger as adjunct
Diet/lifestyle modifications
Algorithm for Managing NVP
ACOG 2004, Einarson A et al 2007
PUQE INDEXMODERATE NVP
No Dehydration Dehydration
IV Fluid replacement with multi-vitamins and
electrolytes
Diclegis 2 tabs at nightor
Metoclopramide 5-10 mg q 6-8 hrs PO
Note: Promethazine 25 mg suppository for breakthrough vomitingDiclegis 2 tabs at night or
Metoclopramide 5-10 mg q 6-8 hrs PO
Algorithm for Managing NVP
ACOG 2004, Einarson A et al 2007
SEVERE
IV fluid replacement with multi-vitamins and electrolytes (Banana Bag)
NPO x 24 hrs then increase as tolerated
Metoclopramide 5-10 mg q 8hr IVor
Ondansetron 1 mg/hr IV x 12-24 hrs or 8 mg over 15 min q 12 hrsor
Droperidol 1 mg/hr with Diphenhydramine 50 mg IV over 30 min q 6 hrsMethylprednisolone 15-20 mg taper dose
orMetoclopramide or Ondansetron PO

10
THANK YOUAdditional Resources
www.motherrisk.org
www.hyperemesis.org
www.otispregnancy.org
ADDITIONAL MATERIALS
Proposed Etiologies of NVP• � Endocrine (hyperthyroid, diabetes)• Placental mass (multiple gestation, mole)
– � placental mass associated with more NVP(multiple gestation, mole)
– � placental mass associated with less NVP (smokers)• Genetic predisposition (HG more frequent in families)• Psychosocial/Psychiatric• Pre-existing vestibular or GI disturbance• Infectious (H. pylori)• Evolutionary biology
Punchline: HG is a diagnosis looking for an etiology
NVP is not a Psychiatric Disorder
• Historical theory: Conversion disorder, Sexual disorder, ambivalence about pregnancy?
• Current studies have not found more psychiatric diagnoses in women with HG compared to women without NVP. However >>
• NVP results in depression and anxiety and the psychological response of “anticipatory vomiting” may be conditioned
• Psychological treatments (e.g. hypnosis) may help ameliorate NVP via their effect on “anticipatory vomiting”
• NVP is more likely in women who experience IPV• NVP may be more likely in women with preexisting eating disorders
Fairweather D 1968, Simptson SW 2001, Buckwalter 2002; Seng J 2007

11
Maternal and Fetal Outcomes of NVPNVP is associated with favorable pregnancy outcomes
Koren G 2014, Flaxman SM 2000
� miscarriages� preterm birth � Congenital malformations
� LBW, and IUGR� stillbirth
And One More…
Yes, women who have severe NVP are more likely to have a girl fetus
Prevention?• In secondary analysis of an RCT on the effects of folic acid it
was noted that women who regularly take a multi-vitamin prior to conception were less likely to need medical attention for NVP (Creizel AZ 1992)
• Prospective descriptive study: Lack of multivitamin supplementation b/4 6 wks gestation significantly associated with � vomiting in pregnancy (Emeliannova S 1999)
Summary: Women with a Hx of severe NVP or hyperemesis can be counseled to take a multi-vitamin prior to subsequent
pregnancy
Creizel AZ et al 1992, Emelianova S 1999
Non-Pharmacologic Treatments for NVP
• Dietary Management
• Complementary/Alternative Therapies: – Acupressure and Acupuncture– Ginger– Vitamin B6
Murphy PA 1998, Hollyer et al 2002 Jewell D 2003

12
Dietary Management • Most common recommendations:
– Small frequent meals– Sip fluids, cold, clear, carbonated, sour– Avoid spicy or strong smelling foods– Eliminate prenatal vitamins with iron– � intake of bland foods– High protein snacks (Jednak MA)
• Avoid triggers (stuffy rooms, strong odors)• Efficacy: no evidence-based research on effectiveness. Few
women report complete relief with diet changes • Safety: no adverse effects
O’Brien B et al 1992, Jednak MA et al 1999
Acupuncture, Acupressure, and Acustimulation “P-6” also called the “Neiguan point”Sea-Bands™
Murphy PA 1998, Steel NM et al 2001, Jewell et al 2003
Relief Bands
Acupuncture/Acupressure
• Cochrane review of 4 RCTs: “Mixed results”:– Acupuncture/Acupressure no more effective than sham therapy
for severity of nausea or frequency of vomiting. Strong placebo effect in patients who received sham therapy
– If assessing presence or absence of NVP• P6 stimulation more effective than no treatment• (OR 0.25, 95% CI 0.14-0.43)• P6 stimulation slightly more effective than sham
treatment• (OR 0.35, 95% CI 0.12-1.06)Summary: Acupressure comparable to effect of anti-emetics in
general
Murphy PA 1998, Smith C et al 2002, Rosen T 2003, Jewell D 2003, Shin HS 2007
Acupressure• Shin HC, 2007
– RCT of 66 women hospitalized for HG– � N&V and � ketonuria over 4 days of following three
acupressure sessions (Rhode score of 12 vs 22)• Summary
– Acupressure and acustimulation have a modest but possibly clinically significant effect on decreasing the severity NVP
– Some of the positive effects may be secondary to attention and placebo effect?
– Safety: No adverse effects
Murphy PA 1998, Roscoe JA 2002, Rosen T 2003, Jewell D 2003, Shin HS 2007

13
Ginger• Efficacy: 6 RCTs with total N = 675 women
– Dose was 1 gm of ginger in extract form– 4 RCTs found ginger to be better than vitamin B6 in � severity
of NVP– 2 RCTs found ginger to be equal to vitamin B6 in � severity of
NVP
• Safety: 5 RCT’s evaluated safety– No adverse effects – Some side effects: headache, diarrhea, GI distress– German Commission E says ginger is contraindicated in
pregnancy– Contraindicated if patient at risk for hemorrhage
Westfall RE 2004, Smith C et al 2004, Bryer E 2005, Borrelli F 2005
Formulations of Ginger
• 1 gm standardized extract equals: – 1 tsp fresh grated rhizome– 2 droppers liquid extract (2 mL)– 4 cups (8 oz) of ginger tea pre-packaged– 4 cups (8 oz) tea made with ½ tsp grated ginger steeped for
5-10 minutes– 8 oz ginger ale, made with real ginger– 2 pieces crystallized ginger (1 inch square, ¼ inch thick)– Capsules come as 100 mg, 400 mg, 500 mg, 1000 mg– Chewable tablets 67.5 mg
Bryer E 2005
What is on the Market?
Amount per capsule:Vitamin C (calcium ascorbate) 250 mgVitamin K1 (phytolloquinone) 25 mcgVitamin B6 38 mgGinger Root Extract 50 mgGinger Root 400 mgPeppermint Leaf 25 mgLemon Balm 25 mg
Ondansetron vs Other Drugs• Promethazine
– One RCT ondansetron vs promethazine for women hospitalized for hyperemesis
– No benefit of ondansetron over promethazine for relief of nausea, days of hospitalization but ondansetron was less sedating
– OR 0.29 (95% CI 0.03 – 3.12)
• Metoclopramide– Similar effects in reducing nausea, ondansetron is better at
reducing vomiting– Better adverse outcome profile for ondansetron
Sullivan CA 1996, Abas MN 2014, Oliveira LG 2014
14
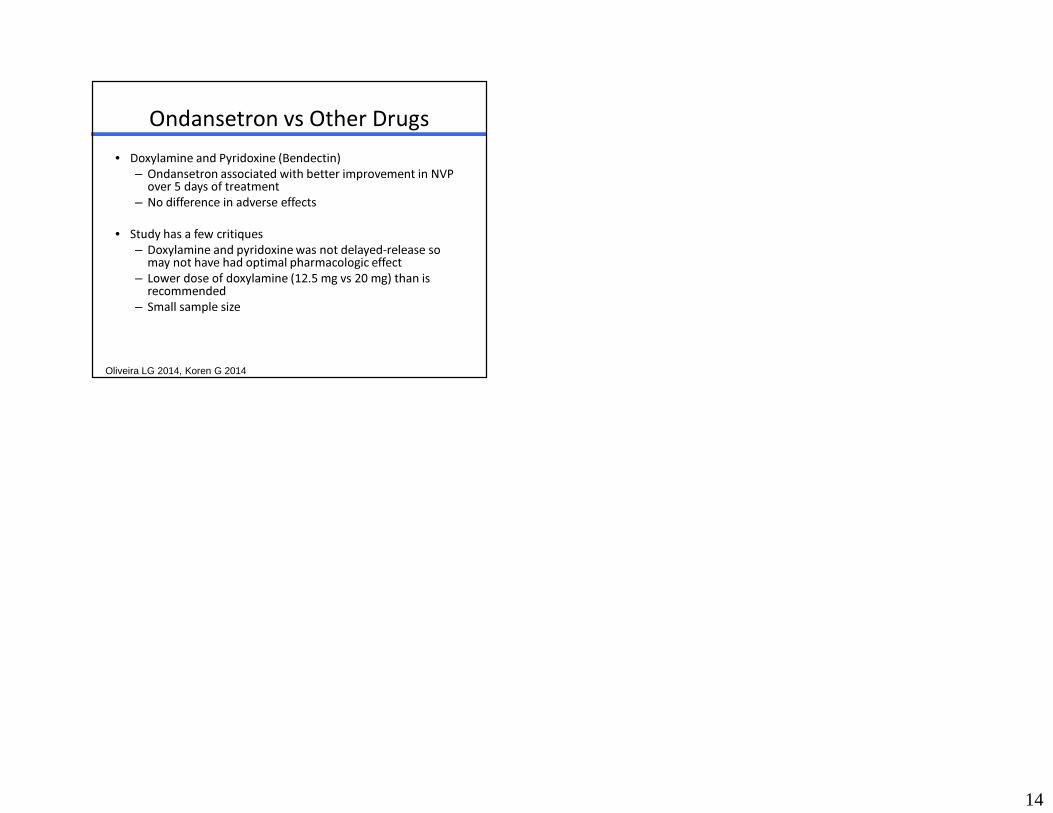
Ondansetron vs Other Drugs• Doxylamine and Pyridoxine (Bendectin)
– Ondansetron associated with better improvement in NVP over 5 days of treatment
– No difference in adverse effects
• Study has a few critiques– Doxylamine and pyridoxine was not delayed-release so
may not have had optimal pharmacologic effect– Lower dose of doxylamine (12.5 mg vs 20 mg) than is
recommended– Small sample size
Oliveira LG 2014, Koren G 2014
Related Documents



![Hyperemesis Gravidarum–A Serious Issue during Pregnancy ...Hyperemesis gravidarum [1] is the medical condition of extreme, persistent nausea and vomiting during pregnancy. It is](https://static.cupdf.com/doc/110x72/5e3e961f88856227b77112e0/hyperemesis-gravidarumaa-serious-issue-during-pregnancy-hyperemesis-gravidarum.jpg)







