ORIGINAL STUDIES Natural History of Plasma Leakage in Dengue Hemorrhagic Fever A Serial Ultrasonographic Study Anon Srikiatkhachorn, MD,* Anchalee Krautrachue, MD,† Warangkana Ratanaprakarn, MD,† Lawan Wongtapradit, MD,† Narong Nithipanya, MD,† Siripen Kalayanarooj, MD,† Ananda Nisalak, MD,‡ Stephen J. Thomas, MD,‡ Robert V. Gibbons, MD,‡ Mammen P. Mammen, Jr., MD,‡ Daniel H. Libraty, MD,* Francis A. Ennis, MD,* Alan L. Rothman, MD,* and Sharone Green, MD* Background: Although plasma leakage is the major cause of mortality and morbidity in patients with dengue hemorrhagic fever (DHF), a detailed assessment of the natural course of this process is still lacking. We employed serial ultrasound examination to delin- eate the locations and the timing of plasma leakage and to evaluate the usefulness of ultrasound in detecting plasma leakage in DHF. Method: Daily ultrasound examinations of the abdomen and right thorax were performed in 158 suspected dengue cases to detect ascites, thickened gall bladder wall and pleural effusions. Cases were classified into dengue fever (DF), DHF or other febrile illness (OFI) based on serology and evidence of plasma leakage including hemoconcentration and pleural effusion detected by chest radio- graph. Results: Ultrasonographic evidence of plasma leakage was detected in DHF cases starting from 2 days before defervescence and was detected in some cases within 3 days after fever onset. Pleural effusion was the most common ultrasonographic sign of plasma leakage (62% of DHF cases one day after defervescence). Thicken- ing of the gallbladder wall and ascites were detected less frequently (43% and 52% of DHF cases respectively) and resolved more rapidly than pleural effusions. The size of pleural effusions, ascites and gall bladder wall thickness in DHF grade I and II were smaller than those of grade III patients. Ultrasound detected plasma leakage in 12 of 17 DHF cases who did not meet the criteria for significant hemoconcentration. Conclusions: Ultrasound examinations detected plasma leakage in multiple body compartments around the time of defervescence. Ultrasonographic signs of plasma leakage were detectable before changes in hematocrits. Ultrasound is a useful tool for detecting plasma leakage in dengue infection. Key Words: dengue hemorrhagic fever, pleural effusion, ascites, gall bladder wall thickening (Pediatr Infect Dis J 2007;26: 283–290) D engue virus (DV) infections are a significant health threat to populations living in tropical and subtropical regions. 1 Infection with any of the 4 serotypes of DV can produce a broad spectrum of illness, ranging from asymp- tomatic infection to severe life-threatening illness. 2 Symp- tomatic dengue illness is typically classified into dengue fever (DF), a self limited febrile illness, or a more severe form, dengue hemorrhagic fever (DHF), which is characterized by plasma leakage into the chest and abdominal cavities and bleeding diathesis. Although it has been well established that hypotension secondary to plasma leakage typically occurs during the 48 hours period after defervescence, the onset, the course and the anatomic pattern of plasma leakage leading to compromised circulation have not been delineated in detail. Studies have suggested that ultrasonogram of the chest and abdomen might be useful for detecting signs of plasma leakage in DHF patients. Several sonographic findings have been reported including fluid in the chest and the abdomen, thickening of the gallbladder wall and pericardial effusion. 3–9 In most studies ultrasound examinations were performed only once and therefore these studies failed to yield important information on the kinetics of plasma leakage. In addition, due to the retrospective nature and the lack of nondengue cases in most previous studies, the sensitivity and the speci- ficity of various ultrasound findings in differentiating DHF cases from DF or other febrile illnesses (OFI) remain un- known. To study the course of plasma leakage in DHF, we performed daily chest and abdominal ultrasonographic stud- ies in children prospectively recruited for suspected DV infection. Patients with DF and OFI were included in the study. The ability to objectively follow evidence of plasma leakage in these patients provides significant insights into the pattern of plasma leakage in this disease. Accepted for publication January 4, 2007. From the *University of Massachusetts Medical School, Worcester, Massa- chusetts; †Queen Sirikit National Institute of Child Health, Bangkok, Thailand; and ‡Armed Forces Research Institute of Medical Sciences, Bangkok, Thailand. Address for correspondence: Center for Infectious Disease and Vaccine Research, University of Massachusetts Medical School, 55 Lake Avenue North, Room S5-326, Worcester, MA 01655. E-mail: anon. [email protected]. Copyright © 2007 by Lippincott Williams & Wilkins ISSN: 0891-3668/07/2604-0283 DOI: 10.1097/01. inf.0000258612.26743.10 The Pediatric Infectious Disease Journal • Volume 26, Number 4, April 2007 283

Natural History of Plasma Leakage in Dengue.2
Nov 27, 2015
nnjjjnnnjnnkmmmmmmmmmmmmmmmmmmmmmmmmmmmmm
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ORIGINAL STUDIES
Natural History of Plasma Leakage in DengueHemorrhagic Fever
A Serial Ultrasonographic StudyAnon Srikiatkhachorn, MD,* Anchalee Krautrachue, MD,† Warangkana Ratanaprakarn, MD,†
Lawan Wongtapradit, MD,† Narong Nithipanya, MD,† Siripen Kalayanarooj, MD,†Ananda Nisalak, MD,‡ Stephen J. Thomas, MD,‡ Robert V. Gibbons, MD,‡
Mammen P. Mammen, Jr., MD,‡ Daniel H. Libraty, MD,* Francis A. Ennis, MD,*Alan L. Rothman, MD,* and Sharone Green, MD*
Background: Although plasma leakage is the major cause ofmortality and morbidity in patients with dengue hemorrhagic fever(DHF), a detailed assessment of the natural course of this process isstill lacking. We employed serial ultrasound examination to delin-eate the locations and the timing of plasma leakage and to evaluatethe usefulness of ultrasound in detecting plasma leakage in DHF.Method: Daily ultrasound examinations of the abdomen and rightthorax were performed in 158 suspected dengue cases to detectascites, thickened gall bladder wall and pleural effusions. Caseswere classified into dengue fever (DF), DHF or other febrile illness(OFI) based on serology and evidence of plasma leakage includinghemoconcentration and pleural effusion detected by chest radio-graph.Results: Ultrasonographic evidence of plasma leakage was detectedin DHF cases starting from 2 days before defervescence and wasdetected in some cases within 3 days after fever onset. Pleuraleffusion was the most common ultrasonographic sign of plasmaleakage (62% of DHF cases one day after defervescence). Thicken-ing of the gallbladder wall and ascites were detected less frequently(43% and 52% of DHF cases respectively) and resolved morerapidly than pleural effusions. The size of pleural effusions, ascitesand gall bladder wall thickness in DHF grade I and II were smallerthan those of grade III patients. Ultrasound detected plasma leakagein 12 of 17 DHF cases who did not meet the criteria for significanthemoconcentration.Conclusions: Ultrasound examinations detected plasma leakage inmultiple body compartments around the time of defervescence.Ultrasonographic signs of plasma leakage were detectable beforechanges in hematocrits. Ultrasound is a useful tool for detectingplasma leakage in dengue infection.
Key Words: dengue hemorrhagic fever, pleural effusion, ascites,gall bladder wall thickening(Pediatr Infect Dis J 2007;26: 283–290)
Dengue virus (DV) infections are a significant healththreat to populations living in tropical and subtropical
regions.1 Infection with any of the 4 serotypes of DV canproduce a broad spectrum of illness, ranging from asymp-tomatic infection to severe life-threatening illness.2 Symp-tomatic dengue illness is typically classified into dengue fever(DF), a self limited febrile illness, or a more severe form,dengue hemorrhagic fever (DHF), which is characterized byplasma leakage into the chest and abdominal cavities andbleeding diathesis. Although it has been well established thathypotension secondary to plasma leakage typically occursduring the 48 hours period after defervescence, the onset, thecourse and the anatomic pattern of plasma leakage leading tocompromised circulation have not been delineated in detail.
Studies have suggested that ultrasonogram of the chestand abdomen might be useful for detecting signs of plasmaleakage in DHF patients. Several sonographic findings havebeen reported including fluid in the chest and the abdomen,thickening of the gallbladder wall and pericardial effusion.3–9
In most studies ultrasound examinations were performed onlyonce and therefore these studies failed to yield importantinformation on the kinetics of plasma leakage. In addition,due to the retrospective nature and the lack of nondenguecases in most previous studies, the sensitivity and the speci-ficity of various ultrasound findings in differentiating DHFcases from DF or other febrile illnesses (OFI) remain un-known.
To study the course of plasma leakage in DHF, weperformed daily chest and abdominal ultrasonographic stud-ies in children prospectively recruited for suspected DVinfection. Patients with DF and OFI were included in thestudy. The ability to objectively follow evidence of plasmaleakage in these patients provides significant insights into thepattern of plasma leakage in this disease.
Accepted for publication January 4, 2007.From the *University of Massachusetts Medical School, Worcester, Massa-
chusetts; †Queen Sirikit National Institute of Child Health, Bangkok,Thailand; and ‡Armed Forces Research Institute of Medical Sciences,Bangkok, Thailand.
Address for correspondence: Center for Infectious Disease and VaccineResearch, University of Massachusetts Medical School, 55 LakeAvenue North, Room S5-326, Worcester, MA 01655. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0891-3668/07/2604-0283DOI: 10.1097/01. inf.0000258612.26743.10
The Pediatric Infectious Disease Journal • Volume 26, Number 4, April 2007 283

MATERIALS AND METHODSPatients. Children less than 15 years of age who had fever(38°C) for less than 72 hours without an obvious focus ofinfection were recruited from June 2004 to November 2005.Patients were admitted for observation and treatment accord-ing to World Health Organization guidelines.2 DV infectionswere confirmed by RT-PCR to detect dengue genome inplasma obtained on the day of admission, and by serology ofpaired acute and convalescence plasma.10–12 Patients withpositive dengue RT-PCR were observed until one day afterdefervescence or longer depending on their clinical course.Daily complete blood count, plasma albumin and AST levelswere obtained. Ultrasonograms and a right lateral decubituschest radiogram were obtained as described below. Clinicalclassification of dengue cases was assigned according to theWorld Health Organization criteria by 2 reviewers who wereblinded to the ultrasound results. Percent hemoconcentrationwas calculated according to the formula: % Hemoconcentra-tion � �(peak hematocrit surrounding defervescence) – (ad-mission hematocrit or minimum hematocrit before deferves-cence)�/(admission hematocrit or minimum hematocrit beforedefervescence) � 100. A diagnosis of DHF was assigned if apatient fulfilled all of the following clinical criteria: (1) fever,(2) liver enlargement, (3) hemorrhagic manifestations includ-ing positive tourniquet test or skin or mucosal bleeding, (4)evidence of plasma leakage including shock and/or ascites orpleural effusion detected by clinical examination or rightlateral decubitus chest radiogram, or hemoconcentration.Laboratory criteria include (1) thrombocytopenia (plateletcount below 100,000/mm3) and (2) hemoconcentration de-fined as a 20% or more increase in hematocrit from base-linevalue.2 DHF cases were classified according to their severityas follows: DHF grade I, patients with DHF without sponta-neous bleeding or hypotension; DHF grade II, DHF patientswith spontaneous bleeding; DHF grade III, DHF cases withhypotension with pulse pressure of 20 mm Hg or less; DHFgrade IV, DHF cases with profound shock and unobtainableblood pressure.2
The day of defervescence (temperature less than 38°C)was defined as fever day 0. Days before defervescence weredefined as fever day –1, �2, etc and those after defervescencewere defined as fever day �1, �2 respectively. The studywas approved by the Institutional Review Boards of theQueen Sirikit National Institute of Child Health, the ThaiMinistry of Public Health, the US Army Surgeon General andthe University of Massachusetts Medical School. Writteninformed consent was obtained from the legal guardian ofeach participant.Ultrasonogram. Ultrasound examinations were performeddaily with a portable ultrasound scanner (GE Logiq Book)using a 2.5 MHz convex transducer. The studies were per-formed by a team of 4 radiologists who were blinded to thelaboratory results of the study participants. Ultrasound pro-cedures were carried out according to a predetermined pro-tocol and the results recorded on a standardized form. Todetect pleural effusion, longitudinal scans of the right hemi-thorax at the midclaivular and the midaxillary line and atransverse scan of the right upper abdominal quadrant were
performed in the supine position. A longitudinal scan at theright midaxillary line in an upright position was performedafter subjects were in an upright position for at least 3minutes. The vertical dimensions of the fluid collection weredetermined by measuring the distance between the top of thedome of the diaphragm and the base of the lung (Fig. 1 A, Bavailable online only).
Measurements of anterior gallbladder wall thicknesswere carried out without fasting (Fig. 1C, D available online).We examined the hepatorenal pouch and retrovesicular areain a supine position for ascites. Fluid present in the hepato-renal pouch was recorded as present or absent (Fig. 1E, Favailable online). Quantitative measurements of the fluidcollected behind the urinary bladder were taken by measuringthe anteroposterior and transverse diameter of the fluid in atransverse scan of the retrovesicular space (Fig. 1G, H avail-able online).
To evaluate the interoperator variability in interpretingthe ultrasonogram, unmarked ultrasound records were readby a different ultrasonographer at the end of the recruitmentseason and the 2 readings were compared. The concordancerate for the presence or absence of an ultrasound finding wasabove 90%.Chest Radiogram. A right lateral decubitus chest radiogramwas obtained one day after defervescence (fever day �1).The magnitude of a pleural effusion was determined semi-quantitatively as pleural effusion index (PEI) using the fol-lowing formula: PEI � (vertical dimension of the fluid/widthof the right pleural cavity) � 100.10 The chest radiogramswere read blinded after the completion of the recruitmentseason.Statistical Analysis. Variables are reported as mean (SE) ornumber (%) as appropriate. Analysis of categorical variableswas performed using �2. Continuous variables were analyzedusing multivariate analysis. Correlations were analyzed usingSpearman analysis for nonparametric test and Pearson anal-ysis for parametric test. A P value �0.05 was consideredsignificant. All analyses were performed using SPSS (version12) statistical program.
RESULTSCharacteristics of Study Subjects. Table 1 shows the baselinecharacteristics of the study patients. There were 82 patientswith DV infection with 61 and 21 cases classified as DF andDHF, respectively. All the DHF cases met all 4 clinicalcriteria including fever, hepatomegaly, hemorrhagic tendencyand clinical and/or radiologic evidence of plasma leakage. Allhad platelet counts below 100,000/mm3. There were 27, 10, 7and 36 cases with dengue serotypes 1, 2, 3 and 4, respectively(Table 2). The PCR was negative in 2 cases with positiveserology. Eleven dengue-infected patients had primary infec-tions based on the serologic response; all had DF. Theremainder of the dengue cases had secondary DV infections.Among the DHF cases, there were 2, 14 and 5 cases of DHFgrade I, II and III, respectively. Seventy-six participants werecategorized as OFI. There were no differences in hematocritsor plasma albumin levels between groups at admission, but
Srikiatkhachorn et al The Pediatric Infectious Disease Journal • Volume 26, Number 4, April 2007
© 2007 Lippincott Williams & Wilkins284
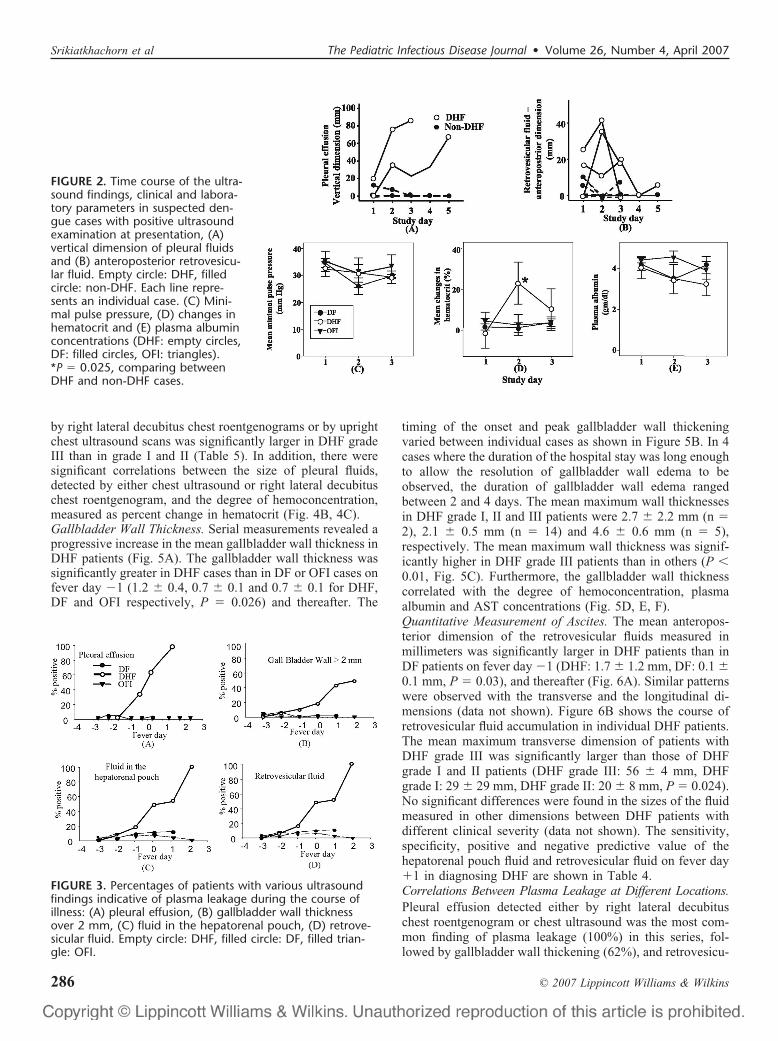
DV infected patients had higher AST levels but lower plateletcounts than the patients with OFI (Table 1).Temporal Sequence of Ultrasonographic Signs During DVInfection. To study the development of plasma leakage earlyin the course of the disease, we analyzed the ultrasoundfindings on the day of presentation when the duration of feverwas less than 72 hours. Although few patients in any diag-nostic group had positive ultrasound findings at that time,retrovesicular fluid and pleural effusion were detected in ahigher proportion of DHF patients compared with DF andOFI patients (Table 3). Of the 3 DHF cases with ascitesdetected by ultrasound examinations, only one had ascitesdetected by physical examination. The initial ultrasound find-ings detected in non-DHF patients were absent on subsequentexaminations while the findings in DHF were persistent
(Fig. 2A, B). No differences in plasma albumin levels, pulsepressure and changes in hematocrit between DHF cases andDF and OFI cases were detected during the initial 24 hours ofhospitalization (Fig. 2C, D, E). However, hemoconcentrationbecame significantly greater in DHF cases compared withnon-DHF cases during the subsequent 24 hours (Fig. 2D).
Chest ultrasonograms revealed pleural effusion in 16%,33% and 62% of DHF patients on fever day �1, 0 and �1respectively (Fig. 3A). The percentage of DHF cases with athickened gallbladder wall (defined as more than 2 mm) was11%, 19% and 43% on fever day �1, 0 and �1 respectively(Fig. 3B). Some DF and OFI cases had a thickened gallblad-der wall which was not found on subsequent examinations.The temporal pattern of ascites was similar to the pattern ofpleural effusion with fluid detected in the hepatorenal pouchin 6%, 29%, 42% of DHF cases, and in the retrovesicularspace in 17%, 47%, 52% of DHF cases on fever day �1, 0and �1 respectively (Fig. 3D, E). The sensitivity, specificity,positive and negative predictive value of ultrasound scans indiagnosing DHF are shown in Table 4.Detection of Pleural Fluid by Chest Ultrasound and ChestRoentgenogram. Pleural effusions detected by chest roent-genograms are generally considered a sign of plasma leakagein DHF. To compare chest roentgenograms and chest ultra-sound scans in detecting plasma leakage, we performed rightlateral decubitus chest roentgenograms and upright chestultrasound scans on all patients with confirmed DV infectionsand forty-two OFI patients (as controls) on fever day �1.Right lateral decubitus chest roentgenogram detected pleuraleffusions in 100% of DHF cases, but also in 9% of DF casesand 19% of OFI cases (Table 5). The sizes of the pleuraleffusions, expressed as PEI, were significantly larger in DHFcases than in DF and OFI cases (DHF: 15.5% � 3.1%, DF:0.2% � 0.1%, OFI: 0.4% � 0.1%, P � 0.001, Table 5). Thesizes of pleural effusions detected in DF and OFI cases werenot different (P � 0.97). Chest ultrasound scans detectedfluid in 62%, 1.6% and 0% of DHF, DF and OFI casesrespectively. The vertical dimension of pleural fluid detectedby ultrasound showed a good correlation with the size of theeffusion determined by right lateral decubitus chest roentgen-ogram (r2 � 0.49, P � 0.001 Fig. 4A). The sensitivity andspecificity of the right lateral decubitus chest roentgenogramand upright chest ultrasound in diagnosing DHF one day afterdefervescence are shown in Table 4.
We analyzed the relationship between the sizes ofpleural effusions and the severity of illness in patients withDHF. The magnitude of pleural effusions determined either
TABLE 1. Baseline Characteristic of Patients
Clinical Diagnosis DF DHF OFI
Number of cases 61 21 76Age, y (mean � SE) 9.58 (0.34) 10.31 (0.53) 9.16 (1.1)Sex (M/F) 37/24 10/11 43/33Albumin (g/dL) (mean � SE) 4.2 (0.1) 4.2 (0.1) 4.2 (0.1)Hematocrit (%) (mean � SE) 37.5 (0.4) 38.4 (0.8) 37.1 (0.3)Platelet ( 103 count/mm3) 186 (8.5)* 165 (22)* 259 (8)AST (mean � SE) 59 (11)† 85 (11)† 36 (2)Fever duration at
presentation (mean � SE)1.9 (0.1) 2.4 (0.1)‡ 1.6 (0.1)
Fever day (mean � SE) �2.5 (0.2) �2.2 (0.3) �1.8 (0.2)
*Average platelet count was lower in DF and DHF groups than OFI group (P � 0.01).†AST was elevated in DF and DHF patients compared with patients with other febrile
illness (P � 0.002).‡Mean durations of fever at presentation were greater in DHF group compared with
DF and OFI groups (P � 0.045).There were no differences in hematocrits or plasma albumin concentrations at the
time of presentation in any of these groups.DF, dengue fever; DHF, dengue hemorrhagic fever; OFI, other febrile illness.
TABLE 2. The Serotypes of Virus and the Patterns ofAntibody Response in Dengue Virus Infected Cases
Virus Serotypes
PrimaryAntibodyResponse
SecondaryAntibodyResponse
DF DHF DF DHF
Dengue 1 5 0 10 12Dengue 2 3 0 6 1Dengue 3 1 0 5 1Dengue 4 1 0 29 6Not identified 1 0 0 1
TABLE 3. The Number and the Percentage of Cases With Positive Ultrasound Findings on the Day of Presentation
Clinical Diagnosis TotalCases
Fluid Detected by ChestUltrasound Scan
Gall Bladder Wall Thickness2 mm
RetrovesicularFluid
HepatorenalPouch Fluid
DF 61 1 (1.6) 3 (4.9) 4 (6.5) 1 (1.6)DHF 21 2 (9.5)* 1 (4.2) 3 (14) 1 (4.8)OFI 76 0 (0) 0 (0) 4 (5.2) 0 (0)
*Higher proportion of DHF cases had positive chest ultrasound findings compared to the other 2 groups. P � 0.006 by Pearson �2 test.Values in parentheses indicate % values.DF, dengue fever; DHF, dengue hemorrhagic fever; OFI, other febrile illness.
The Pediatric Infectious Disease Journal • Volume 26, Number 4, April 2007 Serial Ultrasound in Dengue
© 2007 Lippincott Williams & Wilkins 285
by right lateral decubitus chest roentgenograms or by uprightchest ultrasound scans was significantly larger in DHF gradeIII than in grade I and II (Table 5). In addition, there weresignificant correlations between the size of pleural fluids,detected by either chest ultrasound or right lateral decubituschest roentgenogram, and the degree of hemoconcentration,measured as percent change in hematocrit (Fig. 4B, 4C).Gallbladder Wall Thickness. Serial measurements revealed aprogressive increase in the mean gallbladder wall thickness inDHF patients (Fig. 5A). The gallbladder wall thickness wassignificantly greater in DHF cases than in DF or OFI cases onfever day �1 (1.2 � 0.4, 0.7 � 0.1 and 0.7 � 0.1 for DHF,DF and OFI respectively, P � 0.026) and thereafter. The
timing of the onset and peak gallbladder wall thickeningvaried between individual cases as shown in Figure 5B. In 4cases where the duration of the hospital stay was long enoughto allow the resolution of gallbladder wall edema to beobserved, the duration of gallbladder wall edema rangedbetween 2 and 4 days. The mean maximum wall thicknessesin DHF grade I, II and III patients were 2.7 � 2.2 mm (n �2), 2.1 � 0.5 mm (n � 14) and 4.6 � 0.6 mm (n � 5),respectively. The mean maximum wall thickness was signif-icantly higher in DHF grade III patients than in others (P �0.01, Fig. 5C). Furthermore, the gallbladder wall thicknesscorrelated with the degree of hemoconcentration, plasmaalbumin and AST concentrations (Fig. 5D, E, F).Quantitative Measurement of Ascites. The mean anteropos-terior dimension of the retrovesicular fluids measured inmillimeters was significantly larger in DHF patients than inDF patients on fever day �1 (DHF: 1.7 � 1.2 mm, DF: 0.1 �0.1 mm, P � 0.03), and thereafter (Fig. 6A). Similar patternswere observed with the transverse and the longitudinal di-mensions (data not shown). Figure 6B shows the course ofretrovesicular fluid accumulation in individual DHF patients.The mean maximum transverse dimension of patients withDHF grade III was significantly larger than those of DHFgrade I and II patients (DHF grade III: 56 � 4 mm, DHFgrade I: 29 � 29 mm, DHF grade II: 20 � 8 mm, P � 0.024).No significant differences were found in the sizes of the fluidmeasured in other dimensions between DHF patients withdifferent clinical severity (data not shown). The sensitivity,specificity, positive and negative predictive value of thehepatorenal pouch fluid and retrovesicular fluid on fever day�1 in diagnosing DHF are shown in Table 4.Correlations Between Plasma Leakage at Different Locations.Pleural effusion detected either by right lateral decubituschest roentgenogram or chest ultrasound was the most com-mon finding of plasma leakage (100%) in this series, fol-lowed by gallbladder wall thickening (62%), and retrovesicu-
FIGURE 3. Percentages of patients with various ultrasoundfindings indicative of plasma leakage during the course ofillness: (A) pleural effusion, (B) gallbladder wall thicknessover 2 mm, (C) fluid in the hepatorenal pouch, (D) retrove-sicular fluid. Empty circle: DHF, filled circle: DF, filled trian-gle: OFI.
FIGURE 2. Time course of the ultra-sound findings, clinical and labora-tory parameters in suspected den-gue cases with positive ultrasoundexamination at presentation, (A)vertical dimension of pleural fluidsand (B) anteroposterior retrovesicu-lar fluid. Empty circle: DHF, filledcircle: non-DHF. Each line repre-sents an individual case. (C) Mini-mal pulse pressure, (D) changes inhematocrit and (E) plasma albuminconcentrations (DHF: empty circles,DF: filled circles, OFI: triangles).*P � 0.025, comparing betweenDHF and non-DHF cases.
Srikiatkhachorn et al The Pediatric Infectious Disease Journal • Volume 26, Number 4, April 2007
© 2007 Lippincott Williams & Wilkins286

lar fluid (52%). Among the 21 DHF cases, 10 cases had all 3ultrasound findings of plasma leakage, 3 cases had 2 ultra-sound findings and 3 cases had only one ultrasound findings.Five DHF cases (1 DHF grade I and 4 DHF grade II cases)exhibited no ultrasound evidence of plasma leakage and hada small pleural effusion detected only by right lateral decu-bitus chest roentgenograms (mean PEI � 4.7% � 1.02%).There was a significant correlation between the sizes ofpleural effusions (detected either by right lateral decubituschest roentgenograms or ultrasound) and the gallbladder wallthickness (R2 � 0.29, P � 0.01) and the sizes of theretrovesicular fluids (R2 � 0.23, P � 0.03).
DISCUSSIONWe performed the first prospective study employing
serial ultrasonography to examine the anatomic and the tem-poral patterns of plasma leakage in DV infected patients. Ourstudies demonstrate that signs of plasma leakage were de-tected in some DHF patients early in the course of the illnessbut in most patients these findings were detected around thetime of defervescence. This is consistent with the clinical
observation that circulatory consequences of plasma leakageare usually observed within 48 hours after defervescence.2
Significantly higher proportion of patients who were eventu-ally diagnosed with DHF exhibited ultrasonographic signs ofleakage at the time of clinical presentation than DF and OFIcases. The ultrasound findings were detected one day beforepeak hemoconcentration and clinical signs of plasma leakagein 20% of DHF cases with at least 10% increase in hemato-crit, indicating that ultrasound studies may be useful in earlydetection of plasma leakage.
Serial hematocrit determination has been routinely usedto detect hemoconcentration as a sign of plasma leakage. A20% increase in hematocrit over baseline is generally ac-cepted as indicative of plasma leakage.2 However, sincebaseline hematocrit values are rarely available at the timepatients present for evaluation, the hematocrit can be used toguide management only by reference to normal values in thepopulation. In previous studies, the hematocrit obtained atconvalescence was used as the baseline hematocrit.13 Sinceour study subjects were enrolled early, preleakage hemat-ocrits were available in most cases. Further, we have ob-
TABLE 5. The Number and the Percentage of Cases With Pleural Effusion, andthe Sizes of the Effusions Detected by Either Right Lateral Decubitus ChestRoentgenogram or Upright Chest Ultrasound Scan on Fever Day �1
Clinical Severity(total cases)
Right Lateral DecubitusChest Roentgenogram Upright Chest Ultrasound
Positive(case (%))
PEI %(mean (SE))
Positive(case (%))
VerticalDimension, mm
(mean (SE))
OFI (42) 8 (19) 0.4 (0�1) 0 (0%) 0DF (61) 5 (9) 0.2 (0.1) 1 (1.6%) 1DHF (21) 21 (100) 15.5 (3.1)* 13 (62%) 23.9 (6.3)DHF I (2) 2 (100) 16.8 (6�8) 1 (50%) 10.3 (10.4)DHF II (14) 14 (100) 10.0 (2.9) 7 (46%) 19.5 (7.7)DHF III (5) 5 (100) 33.7 (4.2)† 5 (100%) 49.4 (12.1)†
*Different from DF and OFI (P � 0.001).†Different from DHF grade I and II (P � 0.05).PEI, pleural effusion index; OFI, other febrile illness; DF, dengue fever; DHF, dengue hemorrhagic fever; DHF I, II, III, dengue
hemorrhagic fever grade 1, 2, 3.
TABLE 4. Sensitivities, Specificities, Positive and Negative Predictive Values of Right Lateral Decubitus ChestRoentgenograms and Various Ultrasound Scans in Diagnosing DHF
Sensitivity(%)
Specificity(%)
PositivePredictive Value
(%)
NegativePredictive Value
(%)
Right lateral decubitus chest roentgenogram (fever day �1) 100 76 61 100Upright chest ultrasound (fever day �1) 62 99 93 94Maximum gallbladder wall thickness 2 mm 62 92 54 94Hepatorenal pouch fluid (fever day �1) 42 100 100 91Retrovesicular fluid (fever day �1) 52 92 55 92
The specificity, sensitivity, positive and negative predictive value of right lateral decubitus chest radiograms, chest ultrasonograms and abdominal ultrasound in diagnosing DHF werecalculated based on fever day �1 findings in 139 study subjects (21, 61, 57 cases of DHF, DF and OFI respectively). Nineteen OFI patients did not stay until defervescence and did nothave chest radiograph performed. Right lateral decubitus chest radiograms were positive in 21 DHF, 5 DF and 8 OFI cases. Upright chest ultrasound detected fluid in 13 DHF, 1 DF,0 OFI cases. Fluid in the hepatorenal pouch was detected in 9 DHF, 0 DF, 0 OFI cases. Retrovesicular fluid was detected in 11 DHF, 7 DF and 2 OFI cases. The specificity, sensitivityand the predictive values of the gall bladder wall thickness over 2 mm at anytime during the course of the hospitalization were calculated based on findings in 21 DHF, 61 DF, 76 OFIcases. Thirteen, 9, and 2 cases of DHF, DF and OFI cases had thickened gall bladder by this criteria. The formula used to calculate these parameters are (1) sensitivity (%) � (numberof DHF cases with positive findings/the number of DHF cases) � 100, (2) specificity (%) � �(number of DF cases with negative findings � number of OFI cases with negative findings)/thenumber of DF � OFI cases� � 100, (3) positive predictive value (%) � (number of DHF cases with positive findings/the number all cases with positive findings) � 100, (4) negativepredictive value � �(number of DF cases with negative findings � number of OFI cases with negative findings)/the number all cases with negative findings� � 100.
The Pediatric Infectious Disease Journal • Volume 26, Number 4, April 2007 Serial Ultrasound in Dengue
© 2007 Lippincott Williams & Wilkins 287

served that in some patients the lowest hematocrit readingswere detected during the illness preceding the rise in hema-tocrits. The percent changes in hematocrits derived fromthese values therefore more closely reflect degrees ofhemoconcentration than values derived using hematocritsobtained at convalescence as baseline values in these cases.Our finding may reflect a significant proportion of DHF caseswith spontaneous hemorrhage in our study. It also under-scores the need to take into consideration, in addition to thenadir and the peak hematocrit readings, the relative timing ofthese readings and associated factors such as blood loss and
fluid therapy, in making clinical classification. In cases wherethe degree of hemoconcentration is difficult to ascertain, adirect demonstration of fluid leakage by ultrasound mighthelp differentiate cases with borderline changes in hemat-ocrits (10–20%), which would not have been correctly clas-sified using hematocrits alone as criteria. In this series, 10 outof 61 cases of DF had an increase in hematocrit between10–20%, but none had pleural effusion detected by chestultrasound. In contrast, among 17 cases of DHF who had lessthan a 20% increase in hematocrit, all but 5 exhibited at least oneultrasonographic finding over the clinical course. Patients who
FIGURE 4. Correlations between the sizes ofpleural effusions determined by upright chestultrasound or right lateral decubitus chestroentgenogram (A), and between these pa-rameters and percent changes in hematocrit(B and C).
FIGURE 5. Time course of gallblad-der wall thickening. (A) Mean gall-bladder wall thickness in DF, DHFand OFI patients. Empty circle:DHF, filled circle: DF, filled triangle:OFI. *P � .01 for comparison ofDHF and non-DHF patients. (B)Gallbladder wall thickness of indi-vidual DHF patients over the courseof the illness. Dotted, gray, andblack lines indicate patients withDHF grade 1, 2 and 3 respectively.(C) Mean maximum gallbladderwall thickness in patients with OFI,DF and DHF. *P � 0.001 for com-parison of DHF and either DF orOFI cases, **P � 0.01 for compari-son of DHF grade III and eithergrade I or II cases. (D–F) Correlationbetween peak gallbladder wallthickness and percent change inhematocrit (D), plasma albuminlevels (E) or AST levels (F).
Srikiatkhachorn et al The Pediatric Infectious Disease Journal • Volume 26, Number 4, April 2007
© 2007 Lippincott Williams & Wilkins288

had negative ultrasound findings had small pleural effusionsdetected only by right lateral decubitus chest roentgenogram.
Pleural fluid detected by chest roentgenogram has beeninterpreted as evidence of plasma leakage. Our study dem-onstrates that small pleural effusions detected by lateraldecubitus chest roentgenogram are a relatively common find-ing in nondengue febrile patients and in DF patients, con-firming an earlier report.10 This indicates that a small pleuraleffusion in itself is not a reliable marker of plasma leakage asa criterion for clinical classification of dengue cases. Smallpleural effusion, similar to the small and transient ascitic fluidand thickened gall bladder wall observed in non-DHF pa-tients, may reflect mild local serosal inflammation occurringas a nonspecific reaction in febrile illness, distinct fromincreased vascular permeability in DHF. Chest ultrasound hasbeen reported to be more sensitive than upright chest roent-genograms in detecting pleural fluid in DHF cases.7 Wefound that chest ultrasonogram was less sensitive thanright lateral decubitus chest roentgenograms in detectingsmall pleural effusions. However, this lower sensitivitywas associated with a higher specificity for DHF. The sizesof the effusions obtained by ultrasound correlated wellwith those determined by right lateral decubitus chestroentgenogram, and with disease severity and the degree ofhemoconcentration.
Thickening of the gallbladder wall has been reported inconditions with hypoalbuminemia and ascites,14 and in sev-eral viral infections including DHF.6–8,15,16 Although age-adjusted normal values of GBW thickness are not wellestablished, the definition of thickened gallbladder wall hasgenerally been accepted to be above 3 mm.17,18 Based on areceiver operating characteristic curve analysis of our data,we found that a cut-off of 2 mm yielded a better sensitivity indiscriminating DHF cases (data not shown). Consistent withprevious reports, we found a statistically significant differ-ence between maximum gallbladder thickness of patientswith DHF grade III and those of DHF grades I and II.6 Thegallbladder wall thickness also correlated with changes inhematocrits and plasma albumin, and with AST values. Sim-ilar correlations have been reported in hemorrhagic fever withrenal syndrome.19
Ascites is another sign of plasma leakage in DHFpatients. The minimum amount of ascites required for
detection varied according to the location in the abdomenand the examination position.20 –22 We detected fluid inMorrison pouch and the pelvic cavity at comparable fre-quency in DHF cases. The incidence of ascites in DHF inour series is comparable to that previously reported.5–7,23
Fluid was detected in the pelvic cavity in some DF and OFIpatients as well. However, those fluid collections wereminimal in size and were often detected only once duringillness.
Over half of the DHF cases in this series had all 3ultrasonographic signs of plasma leakage; pleural effusion,thickened gallbladder wall and ascites. Pleural effusions oc-curred mostly on fever day �1, in contrast to gallbladder wallthickening and ascites, which were more variable in onset,ranging from fever day �2 to �1. The earlier onset ofgallbladder wall thickening compared with the onset of pleu-ral effusions is consistent with a previous report.8 The rapidresolution of gall bladder wall thickening and ascites suggeststhat the underlying mechanism is a transient increase inpermeability rather than inflammation. This is consistent withthe absence of tissue inflammation at autopsy in DHF and therapid recovery in most DHF patients.24
Because of the lack of clinical or laboratory indices thatwill predict which patients will develop DHF, close monitor-ing of clinical signs and hematocrits are required to detectplasma leakage. Although we have demonstrated that ultra-sound examinations can directly detect plasma leakage beforesignificant hemoconcentration occurs, significant accumula-tion of fluid is still required before it became detectable byultrasound. A parameter capable of detecting plasma leakagein a timely manner is still needed. Because of the relativesmall number of severe DHF cases in this series, the diag-nostic value of various parameters in differentiating DHFcases with cardiovascular compromise cannot be derived. Inaddition, the relatively small number of DHF cases limits thestatistical power to detect differences in ultrasound findingsin patients with different virus serotypes. Additional studieswhich include more severe DHF cases will be required toanswer these questions. Nevertheless, our results indicate thatchest and abdominal ultrasonographic studies are useful indetecting plasma leakage in dengue infected individuals.Among various ultrasound examinations, upright chest ultra-sound appeared to be the most sensitive and yielded superior
FIGURE 6. Time course of retrovesicular fluid.(A) The mean of the fluid size in the antero-posterior dimension in DF, DHF and OFI pa-tients over the course of the illness. Empty cir-cle: DHF, filled circle: DF, filled triangle: OFI.*P � .03, **P � .01 for comparison of DHFand non-DHF patients. (B) Time course of ret-rovesicular fluid in individual DHF cases. Dot-ted, gray, and black lines indicate patients withDHF grade 1, 2 and 3 respectively.
The Pediatric Infectious Disease Journal • Volume 26, Number 4, April 2007 Serial Ultrasound in Dengue
© 2007 Lippincott Williams & Wilkins 289
positive and negative predictive value for detecting plasmaleakage in DHF and provides a quantitative measurement thatcorrelates with clinical severity.
ACKNOWLEDGMENTSThe authors thank the arbovirology and molecular
sections of the Armed Forces Research Institute of MedicalSciences for diagnostic testing; Dr. Suchitra Nimmannityafor reviewing the clinical diagnoses; doctors and nurses ofQueen Sirikit National Institute of Child Health and the staffof the Armed Forces Research Institute of Medical Sciencesfor patient care and sample collection.
This work is supported by National Institutes of HealthGrant NIH-P01AI34533 and the Military Infectious DiseaseResearch Program.
The opinions or assertions contained herein are theprivate ones of the authors and are not to be construed asofficial or reflecting the view of the U.S. Government.
REFERENCES1. Dengue/dengue haemorrhagic fever. Wkly Epidemiol Rec. 2000;75:193–
196.2. Nimmannitya S. Clinical manifestations of dengue/dengue haemor-
rhagic fever. In: Monograph on Dengue/Dengue Haemorrhagic Fever.Regional Publication No. 22. WHO Regional office for Southeast Asia.1993:48–61.
3. Gupta S, Singh SK, Taneja V, et al. Gall bladder wall edema in serologyproven pediatric dengue hemorrhagic fever: a useful diagnostic findingwhich may help in prognostication. J Trop Pediatr. 2000;46:179–181.
4. Pelupessy JM, Allo ER, Jota S. Pericardial effusion in dengue haemor-rhagic fever. Paediatr Indones. 1989;29:72–75.
5. Pramuljo HS, Harun SR. Ultrasound findings in dengue haemorrhagicfever. Pediatr Radiol. 1991;21:100–102.
6. Setiawan MW, Samsi TK, Pool TN, Sugianto D, Wulur H. Gallbladderwall thickening in dengue hemorrhagic fever: an ultrasonographic study.J Clin Ultrasound. 1995;23:357–362.
7. Thulkar S, Sharma S, Srivastava DN, et al. Sonographic findings in gradeIII dengue hemorrhagic fever in adults. J Clin Ultrasound. 2000;28:34–37.
8. Venkata Sai PM, Dev B, Krishnan R. Role of ultrasound in denguefever. Br J Radiol. 2005;78:416–418.
9. Wu KL, Changchien CS, Kuo CH, et al. Early abdominal sonographicfindings in patients with dengue fever. J Clin Ultrasound. 2004;32:386–388.
10. Kalayanarooj S, Vaughn DW, Nimmannitya S, et al. Early clinical andlaboratory indicators of acute dengue illness. J Infect Dis. 1997;176:313–321.
11. Innis BL, Nisalak A, Nimmannitya S, et al. An enzyme-linked immu-nosorbent assay to characterize dengue infections where dengue andJapanese encephalitis co-circulate. Am J Trop Med Hyg. 1989;40:418–427.
12. Clarke DH, Casals J. Techniques for hemagglutination and hemagglu-tination-inhibition with arthropod-borne viruses. Am J Trop Med Hyg.1958;7:561–573.
13. Cohen SN, Halstead SB. Shock associated with dengue infection. I.Clinical and physiologic manifestations of dengue hemorrhagic fever inThailand, 1964. J Pediatr. 1966;68:448–456.
14. Kaftori JK, Pery M, Green J, Gaitini D. Thickness of the gallbladderwall in patients with hypoalbuminemia: a sonographic study of patientson peritoneal dialysis. AJR Am J Roentgenol. 1987;148:1117–1118.
15. Yoshie K, Ohta M, Okabe N, Komatsu T, Umemura S. Gallbladder wallthickening associated with infectious mononucleosis. Abdom Imaging.2004;29:694–695.
16. Chateil J, Brun M, Perel Y, et al. Abdominal ultrasound findings inchildren with hemophagocytic lymphohistiocytosis. Eur Radiol. 1999;9:474–477.
17. Patriquin HB, DiPietro M, Barber FE, Teele RL. Sonography of thick-ened gallbladder wall: causes in children. AJR Am J Roentgenol. 1983;141:57–60.
18. McGahan JP, Phillips HE, Cox KL. Sonography of the normal pediatricgallbladder and biliary tract. Radiology. 1982;144:873–875.
19. Kim YO, Chun KA, Choi JY, et al. Sonographic evaluation of gallblad-der-wall thickening in hemorrhagic fever with renal syndrome: predic-tion of disease severity. J Clin Ultrasound. 2001;29:286–289.
20. Dinkel E, Lehnart R, Troger J, Peters H, Dittrich M. Sonographicevidence of intraperitoneal fluid. An experimental study and its clinicalimplications. Pediatr Radiol. 1984;14:299–303.
21. Forsby J, Henriksson L. Detectability of intraperitoneal fluid by ultra-sonography. An experimental investigation. Acta Radiol Diagn (Stockh).1984;25:375–378.
22. Branney SW, Wolfe RE, Moore EE, et al. Quantitative sensitivity ofultrasound in detecting free intraperitoneal fluid. J Trauma. 1995;39:375–380.
23. Setiawan MW, Samsi TK, Wulur H, Sugianto D, Pool TN. Denguehaemorrhagic fever: ultrasound as an aid to predict the severity of thedisease. Pediatr Radiol. 1998;28:1–4.
24. Bhamarapravati N, Tuchinda P, Boonyapaknavik V. Pathology of Thai-land haemorrhagic fever: a study of 100 autopsy cases. Ann Trop MedParasitol. 1967;61:500–510.
Srikiatkhachorn et al The Pediatric Infectious Disease Journal • Volume 26, Number 4, April 2007
© 2007 Lippincott Williams & Wilkins290
Related Documents