167 March 2006 Volume 32 Number 3 B reakdowns in verbal and written communica- tion between health care providers are a major concern in the delivery of care. Suboptimal com- munication is not only a common occurrence but is also associated with untoward events. The Joint Commission on the Accreditation of Healthcare Organizations notes that 65% of sentinel events, 1 and 90% of root cause analyses conducted at OSF St. Joseph Medical Center (Bloomington, Illinois) include communication as a con- tributing factor. On January 1, 2006, a new requirement went into effect, associated with the Joint Commission’s National Patient Safety Goal 2, which strives to improve the effectiveness of communication among caregivers. 2 This new requirement (2E) states that facilities must implement a standardized approach to hand-off commu- nications, including an opportunity to ask and respond to questions. Communication handoffs are critically important in creating a shared mental model around the patient’s condition. Without a good shared model, we lose situ- ational awareness. This loss of situational awareness has led to well-known tragedies. 3 Daily experience in health care has taught us that there are many opportu- nities for improving the passage of information during handoffs. Many barriers can potentially contribute to commu- nication difficulties between clinicians. A lack of structure and standardization for communications, uncertainty about who is responsible for the patient’s SBAR: A Shared Mental Model for Improving Communication Between Clinicians National Patient Safety Goals Background: The importance of sharing a common mental model in communication prompted efforts to spread the use of the SBAR (Situation, Background, Assessment, and Recommendation) tool at OSF St. Joseph Medical Center, Bloomington, Illinois. Case Study: An elderly patient was on warfarin sodi- um (Coumadin) 2.5 mg daily. The nurse received a call from the lab regarding an elevated international nor- malized ratio (INR) but did not write down the results (she was providing care to another patient). On the basis of the previous lab cumulative summary, the physician increased the warfarin dose for the patient; a dangerously high INR resulted. Actions Taken: The medical center initiated a col- laborative to implement the use of the SBAR communi- cation tool. Education was incorporated into team resource management training and general orientation. Tools included SBAR pocket cards for clinicians and laminated SBAR “cheat sheets” posted at each phone. SBAR became the communication methodology from leadership to the microsystem in all forms of reporting. Discussion: Staff adapted quickly to the use of SBAR, although hesitancy was noted in providing the “recom- mendation” to physicians. Medical staff were encouraged to listen for the SBAR components and encourage staff to share their recommendation if not initially provided. Article-at-a-Glance Kathleen M. Haig, R.N. Staci Sutton, R.N. John Whittington, M.D. Department Editors: Marcia M. Piotrowski, R.N., M.S., Peter Angood, M.D., Paula Griswold, M.S., Gina Pugliese, R.N., M.S., Sanjay Saint, M.D., M.P.H., Susan E. Sheridan, M.I.M., M.B.A., Kaveh G. Shojania, M.D. Readers may submit National Patient Safety Goals inquiries and submissions to Steven Berman ([email protected]) and Marcia Piotrowski ([email protected]). Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

167March 2006 Volume 32 Number 3
Breakdowns in verbal and written communica-tion between health care providers are a majorconcern in the delivery of care Suboptimal com-
munication is not only a common occurrence but is alsoassociated with untoward events The Joint Commissionon the Accreditation of Healthcare Organizations notesthat 65 of sentinel events1 and 90 of root cause analyses conducted at OSF St Joseph Medical Center(Bloomington Illinois) include communication as a con-tributing factor On January 1 2006 a new requirementwent into effect associated with the Joint CommissionrsquosNational Patient Safety Goal 2 which strives to improvethe effectiveness of communication among caregivers2
This new requirement (2E) states that facilities mustimplement a standardized approach to hand-off commu-nications including an opportunity to ask and respondto questions
Communication handoffs are critically important increating a shared mental model around the patientrsquoscondition Without a good shared model we lose situ-ational awareness This loss of situational awarenesshas led to well-known tragedies3 Daily experience inhealth care has taught us that there are many opportu-nities for improving the passage of information duringhandoffs
Many barriers can potentially contribute to commu-nication difficulties between clinicians A lack of structure and standardization for communicationsuncertainty about who is responsible for the patientrsquos
SBAR A Shared Mental Model forImproving CommunicationBetween Clinicians
National Patient Safety Goals
Background The importance of sharing a commonmental model in communication prompted efforts tospread the use of the SBAR (Situation BackgroundAssessment and Recommendation) tool at OSF StJoseph Medical Center Bloomington Illinois
Case Study An elderly patient was on warfarin sodi-um (Coumadin) 25 mg daily The nurse received a callfrom the lab regarding an elevated international nor-malized ratio (INR) but did not write down the results(she was providing care to another patient) On thebasis of the previous lab cumulative summary thephysician increased the warfarin dose for the patient adangerously high INR resulted
Actions Taken The medical center initiated a col-laborative to implement the use of the SBAR communi-cation tool Education was incorporated into teamresource management training and general orientationTools included SBAR pocket cards for clinicians andlaminated SBAR ldquocheat sheetsrdquo posted at each phoneSBAR became the communication methodology fromleadership to the microsystem in all forms of reporting
Discussion Staff adapted quickly to the use of SBARalthough hesitancy was noted in providing the ldquorecom-mendationrdquo to physicians Medical staff were encouragedto listen for the SBAR components and encourage staff toshare their recommendation if not initially provided
Article-at-a-Glance
Kathleen M Haig RNStaci Sutton RN
John Whittington MD
Department Editors Marcia M Piotrowski RN MS Peter Angood MD Paula Griswold MS Gina
Pugliese RN MS Sanjay Saint MD MPH Susan E Sheridan MIM MBA Kaveh G Shojania MD
Readers may submit National Patient Safety Goals inquiries and submissions to Steven Berman (sbermanjcahoorg) and Marcia Piotrowski (marciapiotrowskimedvagov)
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
168March 2006 Volume 32 Number 3
care management (quarterback of the team) hierar-chy sex and ethnic background may all be contribut-ing factors4 Differences in communication stylesbetween nurses and physicians are also a major con-tributing factor5 Because of varied training approach-es nurses tend to be very descriptive and detailed in their communications whereas physicians tend touse brief statements summarizing salient patient infor-mation sometimes called ldquobullet pointsrdquo or ldquohead-linesrdquo Variations in communication style can causefrustration
In Fall 2002 OSF St Joseph Medical Center recog-nized that some of the communication problemsbetween clinicians could be linked to variations incommunication styles We started looking for ideas toimprove communication Michael Leonard MDphysician leader for patient safety at KaiserPermanente (Denver) introduced us to a model ofstructured communication that would help clinicianshave a shared mental model for the patientrsquos clinicalcondition He called this structured communicationSBARmdashndashSituation Background Assessment andRecommendation67
Implementing Use of SBAR at theMedical CenterInvestigation of near-miss occurrences and results of root cause analyses resulted in identification of aneed to develop a standardized approach to hand-offcommunications among caregivers Stories of actualcases demonstrated the impact of misinterpreted com-munication from nurse-to-nurse nurse-to-physicianand physician-to-physician One such story involved an elderly patient who was on warfarin sodium(Coumadin) 25 mg daily The nurse received a callfrom the lab regarding an elevated international normalized ratio (INR) for this patient but did notwrite down the results as she was in the process of providing care to another patient Later when shesaw the physician she asked him if he saw thepatientrsquos INR results to which he responded ldquoYesrdquoHowever he was looking at a cumulative summaryfrom the lab which did not include the most recent ele-vated INR results On the basis of the information onthe lab cumulative summary the physician increased
the warfarin sodium dose for the patient resulting in adangerously elevated INR
In 2003 to promote a culture of safety OSF StJoseph Medical Center selected SBAR as a mechanismto support open honest communication for sharinginformation asking questions and providing sugges-tions However SBAR was not aggressively implement-ed at that time
The framework for spread of SBAR entailed leader-ship better ideas set-up and the social system8 Asleadership support has been found to be key to the suc-cess in previous projects this topic was selected in2004 as a key project in the system strategic map forfiscal year (FY) 2005 Goals were aligned with incen-tives by naming the chief nurse officer (CNO) as theexecutive leader of the team with a portion of hercompensation being based on achieving the goal TheCNO asked staff questions regarding SBAR during herrounding and requested that requests andor reportingof issues be forwarded using the SBAR format In addi-tion the medical director was named as an executivesponsor to champion the use of SBAR among medicalstaff peers The medical director not only promotedthe use of SBAR among staff when reporting a patientcondition to him but also encouraged his peers to lis-ten for the use of SBAR and to encourage the staff toprovide the ldquoRrdquo or recommendation The patient safetyofficer [KH] was delegated as the projectrsquos day-to-dayleader
The interdisciplinary Spread Team representingmultiple nursing units pharmacy rehab medical imag-ing education staff and media relations was estab-lished It met biweekly for one hour for a period of oneyear (September 2004ndashSeptember 2005) The teamrsquosaims as stated in its charter were as follows Improve communication among clinical caregivers Provide timely and accurate information throughspread of the use of the SBAR communication tool Extend education relative to team resource manage-ment concepts9ndash13 to improve the efficiency timelinessand effectiveness of team interventions throughout themedical center
In September 2004 the spread team was assignedthe task of developing ldquobetter ideasrdquo to describe thecase for use of SBAR to reduce communication deficits
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
169March 2006 Volume 32 Number 3
as a contributing factor to potential adverse eventsThe first better idea was development of an ldquoelevatorspeechrdquomdasha description of SBAR in a few short sen-tencesmdashto explain the projectrsquos intent
The set-up targeted the clinical caregivers includingnurses lab personnel medical imaging personnel rehabpersonnel dieticians social services personnel pharma-cists and physicians for the initial spread plan Initialkey messengers to spread the Better Ideas included teammembers and Nursing Practice Council members Thesemembers were asked to select one peer who was anearly adopter to create a Social System for the spread ofSBAR Technical support aided knowledge managementby providing measurement and feedback to the adopter audiences
Addressing the Spread of SBAR Efforts to promote the use of SBAR began in April 2004 approximately five months before the formal team formation through introduction of theconcept in clinical educational settings Baseline infor-mation was obtained in August 2004 during the pro-jectrsquos pre-implementation phase through a ldquosecretshoppersrdquo survey Ten staff members were called atrandom by either the corporate or the internal patientsafety officer They were asked to describe what SBARstood for and then provide an example of how this con-cept is used in their daily communications Results ofthe monthly survey were displayed on a run chart andshared throughout the organization for feedback Thebaseline data demonstrated that on average staffwere able to respond correctly 60 of the time
In September 2004 the team set an aim to increasethe use of the SBAR communication tool to 90 bySeptember 2005 Starting in November 2004 teamresource management on the SBAR concept was con-ducted in multiple areas specifically the intensive careunitpost-intensive care unit (ICUPICU) respiratorycardiac rehabilitation cardiac catheterization lab inter-ventional radiology medical surgical floatregistrypediatrics transitional care unit and supervision staffThis training was selected as an organizational goal tosupport the improvement efforts
Using the Plan Do Study Act (PDSA) performanceimprovement methodology efforts to incorporate SBAR
began on a general medical nursing unit in October2004 Tests of change were conducted with tools creat-ed by the team and revisions were made on the basis ofinput from the front-line staff members who piloted thetool Tests were small using one person for one day andgradually increasing those involved in the test until aworkable tool was obtained Once this was achievedthe SBAR trigger tool was spread to the surgical unit inJanuary 2005 and to the critical care unit in March 2005Finally SBAR was spread housewide in April 2005 fol-lowing meetings with managers of nonclinical areassuch as social services rehabilitation medical imagingand pharmacy
Identifying and Implementing Solutions Better ideas included incorporation of SBAR into a vari-ety of reporting documents as listed in Table 1 (above)Multiple mechanisms were used to spread the use ofSBAR including those listed in Table 2 (page 170) Thelaminated poster is shown in Figure 1 (page 171) thenursersquos report to a physician in Figure 2 (page 172) andthe hand-off form in Figure 3 (page 173)
Shift report hand-off tools specific to specialtynursing units (labor postpartum nursery)
Strategic goal-reporting Emergency medical services run reports SBAR briefings for emergency department cardiac
arrests andor trauma patients Charge nurse to charge nurse briefing tool Incident reports Shift hand-off reports including certified nursing
assistants Case review descriptions Hospital forms (including administrative staff
meeting minutes the ethics committee issue formand the inpatient and outpatient satisfactionreporting tools)
A service excellence report to report patient andorstaff opportunities for improvement to managers ofall hospital departments
Table 1 Reporting Documents IncorporatingSituation Background Assessment and
Recommendation (SBAR)
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
170March 2006 Volume 32 Number 3
Feasibility and Implementation Issues Implementation approaches included the followingstrategies
Leadership key strategic initiative goals andincentives are aligned and an executive sponsor wasdelegated Better ideas develop the case and describe the ideas Set-upmdashtarget population early adopters Social system and communication key messengerscommunication strategies and technical support Measurement and feedback
Stories were shared that demonstrated missed oppor-tunities and the resulting impact as well as success sto-ries in which SBAR facilitated a shared mental modelDecision aids standardization redundancy of SBAR inhospital forms and forcing functions in reporting toolsled to early successes
Educational training was provided for current andnew staff Constant reminders by leadership in requiringdocumentation to be in the SBAR format assisted inearly adoption Spread efforts were advanced to alldepartments including nonclinical areas for use in com-munication and documentation
The spread team found it difficult to identify outcomemeasures and sought advice from behavior experts Theteam then arrived at the following two outcome meas-ures Consistent use of the medication reconciliation
process Timely and accurate communication betweennurses pharmacists and physicians is critical to accom-plish medication reconciliation This communicationmust occur at multiple points during the inpatient stayincluding admission transfer between units and dis-charge14ndash17 Variances in medication lists can result induplication omission wrong doses and so on poten-tially resulting in patient harm Using SBAR communica-tion techniques should result in improved use of themedication reconciliation process Number of adverse patient events Improvedcommunication should improve the efficiency and effec-tiveness of teamwork and thus result in a reduction of alltypes of adverse events to patients
ResultsProcess Measure Use of SBARSt Joseph Medical Center realized a mean of 96 use of SBAR in FY 2005 (Figure 4 page 174) Teamresource management training was conducted with
Laminated posters displayed on the units Stickers placed on each phone at the nursing units Middle managers shared stories of staffrsquos SBAR use
and these staff members were recruited as spreadagents to their peers
Examples developed for nonclinical areas Staff on the obstetrics unit conducted peer obser-
vation for the use of SBAR in nurse-physician com-munication and shift hand-off reports
Input from the patient services practice councilwas obtained in development of a user-friendlytool for shift hand-off reports
Staff ldquopracticedrdquo their SBAR hand-off reports to physicians with peers before making the call
Monthly gamesquizzes with rewards Good examples of SBAR were recognized by being
published on Web sites on hospital bulletin boardsin hospital publications and so on
Peer assist meetings were held to brainstorm ideasfor use of SBAR among different departments
A shared drive was developed to share data andteam activities
The medical director asked physicians to listen foruse of SBAR in communication from nursing staffand encourage nursing staff to give the ldquoRrdquo part ofSBAR (recommendation)
SBAR training and a follow-up quiz were added toall new employeesrsquo orientation
SBAR was incorporated into annual safety educa-tion for all employees
SBAR was included in team resource managementtraining
Screensavers were used to promote knowledge anduse of SBAR
A safety hotline using SBAR was created
Dixon NM Does your organization have an asking problemKnowledge Management Review 718ndash23 MayndashJun 2004
Table 2 Mechanisms to Spread Use ofSituation Background Assessment and
Recommendation (SBAR)
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
171March 2006 Volume 32 Number 3
983 of targeted staff exceeding a goal of 90Retraining was completed with 87 of targeted staffAbbreviated versions of team resource managementtraining was provided to 39 of physicians and midlev-el practitioners exceeding the goal of 25
Outcome Measures Medication Reconciliation andAdverse Events
The spread team considered medication reconcilia-tion and adverse events as separate processes not direct-ly dependent on SBAR However the teamrsquos thinkingwas that better communication reflecting SBAR usewould improve reconciliation and the incidence ofadverse events
The frequency of medication reconciliation demon-strated notable gains from October 2002ndashAugust 2004 to September 2004ndashDecember 2005mdashadmissionreconciliation improved from a mean of 72 to a meanof 88 (Figure 5 page 174) and discharge reconcilia-tion improved from a mean of 53 to a mean of 89(Figure 6 page 175)
The rate of adverse events was measured using theGlobal Trigger Tool which contains a list of multipletriggers appropriate for general care surgical careintensive care emergency department medicationlaboratory and perinatal care that prompt the reviewerto look further for evidence of an adverse event18ndash20
The rate of events per 1000 patient days is measured
Figure 1 The information on the laminated poster also reproduced on the pocket cards for clinicians describes the
Situation Background Assessment and Recommendation (SBAR) steps with an example for each
Laminated Poster
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
172March 2006 Volume 32 Number 3
Figure 2 The Situation Background Assessment and Recommendation (SBAR) Report to a Physician is intended
for a nurse making a report to a physician
Nursersquos Report to a Physician
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
173March 2006 Volume 32 Number 3
Figure 3 The hand-off form can be used by nurses at shift change
Hand-off Form
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
174March 2006 Volume 32 Number 3
by calculating the total number ofevents dividing by the total of lengthof stay for all charts reviewed andmultiplying by 1000 Each month 20charts were chosen at random to bereviewed The rate of events wasreduced from a baseline of 899 per1000 patient days in October 2004 to3996 per 1000 patient days overall inFY 2005
Adverse drug events identifiedthrough use of the Global Trigger Tooldecreased from a baseline of 2997 per1000 patient days to 1764 per 1000patient days
ReflectionsThe power of top managementrsquosinvolvement in performance improve-ment projects was realized Selectleaders from the top managementteam were not only involved in imple-menting SBAR but also providedhuman technological and financialresources
Flattening of the hierarchy amongnursing staff and physicians led to a cooperative effort to improve communication and improved satis-faction for each of those populationsIt was helpful to start with a smallgroup which included a few key members and early adopters and then spread the change to peers Use of story-telling promoted the benefits of goodcommunication and the potential hazards of poor communication Selecting team members from areas in which SBAR plays a crucial role led to early adoption and buy-in of the concept The addition of a media relations staff member and the incorpora-tion of information technology assisted the team infeedback
Next steps include integration of SBAR into the elec-tronic medical record for documentation by all clinicalcaregivers
Summary and ConclusionsFor OSF St Joseph Medical Center use of SBAR in bothoral and written communication has improved patientsafety by providing clear accurate feedback of informa-tion between caregivers There are fewer incidents ofmissed information during handoffs since SBAR wasimplemented because concise facts are shared in anorganized format
Staff members are encouraged to ldquorecommendrdquo on the basis of their observations and this assistsphysicians with situational awareness through the
Figure 4 Use of Situation Background Assessment and Recommendation
(SBAR) reached a mean of 96 in fiscal year 2005
SBAR Use 2004ndash2005
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at admission improved from a mean
of 72 to a mean of 88
Use of SBAR in Admission Reconciliation2004ndash2005
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
175March 2006 Volume 32 Number 3
eyes of the bedside caregiver Staffmembers feel empowered and haveinfluence over decisions that affectwork life using SBAR thus improvingjob satisfaction Currently SBAR tools are being tested in communica-tion handoffs between shifts fortransfers to other departments (forexample radiology operating room)and with patients admitted from theemergency department SBAR pro-motes the six aims of the Institute of Medicine in providing safe effi-cient effective equitable timely andpatient-centered lines of communica-tion21 J
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at discharge improved from a mean of
53 to a mean of 89
Use of SBAR in Discharge Reconciliation2004ndash2005
Kathleen M Haig RN is Director Quality ResourceManagementRisk ManagerPatient Safety Officer andStaci Sutton RN is Emergency Services Manager OSF StJoseph Medical Center Bloomington Illinois JohnWhittington MD is Patient Safety OfficerDirector of Knowledge Management OSF Healthcare SystemPeoria Illinois Please address correspondence to JohnWhittington johnwwhittingtonosfhealthcareorg
1 Joint Commission on Accreditation of Healthcare OrganizationsSentinel Event Statistics-June 30 2005 httpwwwjcahoorgaccred-ited+organizationssentinel+eventsentinel+event+statisticshtm (lastaccessed Jan 24 2006)2 Joint Commission on Accreditation of Healthcare Organizations2006 Critical Access Hospital and Hospital National Patient
Safety Goals httpwwwjcahoorgaccredited+organizationspatient+safety06_npsg06_npsg_cah_haphtm (last accessed Jan 24 2006)3 Wachter RM Shojania KG Internal Bleeding The Truth Behind
Americas Terrifying Epidemic of Medical Mistakes New YorkRugged Land 2004 4 Thomas EJ Sexton JB Helmreich RL Discrepant attitudes aboutteamwork among critical care nurses and physicians Crit Care Med
31956ndash959 Mar 20035 Greenfield LJ Doctors and nurses A troubled partnership Ann
Surg 230279-288 Sep 19996 Leonard M Graham S Bonacum D The human factor The crit-ical importance of effective teamwork and communication in pro-viding safe care Qual Saf Health Care 13 (suppl 1)i85ndashi90 Oct20047 McFerran SC et al Perinatal patient safety project A multicenterapproach to improve performance reliability at Kaiser Permanente JPerinat Neonatal Nurs 1937ndash45 JanndashMar 2005
References
8 Institute for Healthcare Improvement Framework for SpreadhttpwwwihiorgIHITopicsImprovementSpreadingChangesChanges (last accessed Jan 24 2006)9 Helmreich RL Merritt AC Culture at Work in Aviation and
Medicine National Organizational and Professional Influences
Aldershot UK Ashgate 200110 Helmreich RL On error management Lessons from aviation BMJ
320(7237)781ndash785 Mar 2000 11 Kosnik LK The new paradigm of crew resource management justwhat is needed to re-engage the stalled collaborative movement Jt
Comm J Qual Improv 28235ndash241 May 200212 Risser DT et al The potential for improved teamwork to reducemedical errors in the emergency department The MedTeams ResearchConsortium Ann Emerg Med 34373-383 Sep 1994 13 Wiener EL Kanki BG Helmreich RL Cockpit Resource
Management San Diego Harcourt Brace 199314 Gleason KM et al Reconciliation of discrepancies in medicationhistories and admission orders of newly hospitalized patients Am J
Health Syst Pharm 611689ndash1695 Aug 15 2004 15 Pronovost P et al Medication reconciliation tool A practical tool toreduce medication errors during patient transfer from an intensive careunit Journal of Clinical Outcomes Management 1126ndash33 Jan 200416 Rozich JD et al Medication safety One organizations approachto the challenge Journal of Clinical Outcomes Management 827ndash34Oct 2001 17 Whittington J Cohen H OSF healthcares journey in patient safe-ty Qual Manag Health Care 1353-59 JanndashMar 2004 18 Resar RK Rozich JD Classen D Methodology and rationale forthe measurement of harm with trigger tools Qual Saf Health Care 12(suppl 2)ii39ndashii45 Dec 2003 19 Rozich JD Haraden CR Resar RK Adverse drug event triggertool A practical methodology for measuring medication related harmQual Saf Health Care 12194ndash200 Jun 2003 20 Institute for Healthcare Improvement Global Trigger Tool for
Measuring Adverse Events (IHI Tool) httpwwwihiorgIHITopicsPatientSafetySafetyGeneralToolsGlobalTriggerToolforMeasuringAEshtm (last accessed Jan 24 2006)21 Institute of Medicine Crossing the Quality Chasm WashingtonDC National Academy Press 2001
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations

168March 2006 Volume 32 Number 3
care management (quarterback of the team) hierar-chy sex and ethnic background may all be contribut-ing factors4 Differences in communication stylesbetween nurses and physicians are also a major con-tributing factor5 Because of varied training approach-es nurses tend to be very descriptive and detailed in their communications whereas physicians tend touse brief statements summarizing salient patient infor-mation sometimes called ldquobullet pointsrdquo or ldquohead-linesrdquo Variations in communication style can causefrustration
In Fall 2002 OSF St Joseph Medical Center recog-nized that some of the communication problemsbetween clinicians could be linked to variations incommunication styles We started looking for ideas toimprove communication Michael Leonard MDphysician leader for patient safety at KaiserPermanente (Denver) introduced us to a model ofstructured communication that would help clinicianshave a shared mental model for the patientrsquos clinicalcondition He called this structured communicationSBARmdashndashSituation Background Assessment andRecommendation67
Implementing Use of SBAR at theMedical CenterInvestigation of near-miss occurrences and results of root cause analyses resulted in identification of aneed to develop a standardized approach to hand-offcommunications among caregivers Stories of actualcases demonstrated the impact of misinterpreted com-munication from nurse-to-nurse nurse-to-physicianand physician-to-physician One such story involved an elderly patient who was on warfarin sodium(Coumadin) 25 mg daily The nurse received a callfrom the lab regarding an elevated international normalized ratio (INR) for this patient but did notwrite down the results as she was in the process of providing care to another patient Later when shesaw the physician she asked him if he saw thepatientrsquos INR results to which he responded ldquoYesrdquoHowever he was looking at a cumulative summaryfrom the lab which did not include the most recent ele-vated INR results On the basis of the information onthe lab cumulative summary the physician increased
the warfarin sodium dose for the patient resulting in adangerously elevated INR
In 2003 to promote a culture of safety OSF StJoseph Medical Center selected SBAR as a mechanismto support open honest communication for sharinginformation asking questions and providing sugges-tions However SBAR was not aggressively implement-ed at that time
The framework for spread of SBAR entailed leader-ship better ideas set-up and the social system8 Asleadership support has been found to be key to the suc-cess in previous projects this topic was selected in2004 as a key project in the system strategic map forfiscal year (FY) 2005 Goals were aligned with incen-tives by naming the chief nurse officer (CNO) as theexecutive leader of the team with a portion of hercompensation being based on achieving the goal TheCNO asked staff questions regarding SBAR during herrounding and requested that requests andor reportingof issues be forwarded using the SBAR format In addi-tion the medical director was named as an executivesponsor to champion the use of SBAR among medicalstaff peers The medical director not only promotedthe use of SBAR among staff when reporting a patientcondition to him but also encouraged his peers to lis-ten for the use of SBAR and to encourage the staff toprovide the ldquoRrdquo or recommendation The patient safetyofficer [KH] was delegated as the projectrsquos day-to-dayleader
The interdisciplinary Spread Team representingmultiple nursing units pharmacy rehab medical imag-ing education staff and media relations was estab-lished It met biweekly for one hour for a period of oneyear (September 2004ndashSeptember 2005) The teamrsquosaims as stated in its charter were as follows Improve communication among clinical caregivers Provide timely and accurate information throughspread of the use of the SBAR communication tool Extend education relative to team resource manage-ment concepts9ndash13 to improve the efficiency timelinessand effectiveness of team interventions throughout themedical center
In September 2004 the spread team was assignedthe task of developing ldquobetter ideasrdquo to describe thecase for use of SBAR to reduce communication deficits
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
169March 2006 Volume 32 Number 3
as a contributing factor to potential adverse eventsThe first better idea was development of an ldquoelevatorspeechrdquomdasha description of SBAR in a few short sen-tencesmdashto explain the projectrsquos intent
The set-up targeted the clinical caregivers includingnurses lab personnel medical imaging personnel rehabpersonnel dieticians social services personnel pharma-cists and physicians for the initial spread plan Initialkey messengers to spread the Better Ideas included teammembers and Nursing Practice Council members Thesemembers were asked to select one peer who was anearly adopter to create a Social System for the spread ofSBAR Technical support aided knowledge managementby providing measurement and feedback to the adopter audiences
Addressing the Spread of SBAR Efforts to promote the use of SBAR began in April 2004 approximately five months before the formal team formation through introduction of theconcept in clinical educational settings Baseline infor-mation was obtained in August 2004 during the pro-jectrsquos pre-implementation phase through a ldquosecretshoppersrdquo survey Ten staff members were called atrandom by either the corporate or the internal patientsafety officer They were asked to describe what SBARstood for and then provide an example of how this con-cept is used in their daily communications Results ofthe monthly survey were displayed on a run chart andshared throughout the organization for feedback Thebaseline data demonstrated that on average staffwere able to respond correctly 60 of the time
In September 2004 the team set an aim to increasethe use of the SBAR communication tool to 90 bySeptember 2005 Starting in November 2004 teamresource management on the SBAR concept was con-ducted in multiple areas specifically the intensive careunitpost-intensive care unit (ICUPICU) respiratorycardiac rehabilitation cardiac catheterization lab inter-ventional radiology medical surgical floatregistrypediatrics transitional care unit and supervision staffThis training was selected as an organizational goal tosupport the improvement efforts
Using the Plan Do Study Act (PDSA) performanceimprovement methodology efforts to incorporate SBAR
began on a general medical nursing unit in October2004 Tests of change were conducted with tools creat-ed by the team and revisions were made on the basis ofinput from the front-line staff members who piloted thetool Tests were small using one person for one day andgradually increasing those involved in the test until aworkable tool was obtained Once this was achievedthe SBAR trigger tool was spread to the surgical unit inJanuary 2005 and to the critical care unit in March 2005Finally SBAR was spread housewide in April 2005 fol-lowing meetings with managers of nonclinical areassuch as social services rehabilitation medical imagingand pharmacy
Identifying and Implementing Solutions Better ideas included incorporation of SBAR into a vari-ety of reporting documents as listed in Table 1 (above)Multiple mechanisms were used to spread the use ofSBAR including those listed in Table 2 (page 170) Thelaminated poster is shown in Figure 1 (page 171) thenursersquos report to a physician in Figure 2 (page 172) andthe hand-off form in Figure 3 (page 173)
Shift report hand-off tools specific to specialtynursing units (labor postpartum nursery)
Strategic goal-reporting Emergency medical services run reports SBAR briefings for emergency department cardiac
arrests andor trauma patients Charge nurse to charge nurse briefing tool Incident reports Shift hand-off reports including certified nursing
assistants Case review descriptions Hospital forms (including administrative staff
meeting minutes the ethics committee issue formand the inpatient and outpatient satisfactionreporting tools)
A service excellence report to report patient andorstaff opportunities for improvement to managers ofall hospital departments
Table 1 Reporting Documents IncorporatingSituation Background Assessment and
Recommendation (SBAR)
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
170March 2006 Volume 32 Number 3
Feasibility and Implementation Issues Implementation approaches included the followingstrategies
Leadership key strategic initiative goals andincentives are aligned and an executive sponsor wasdelegated Better ideas develop the case and describe the ideas Set-upmdashtarget population early adopters Social system and communication key messengerscommunication strategies and technical support Measurement and feedback
Stories were shared that demonstrated missed oppor-tunities and the resulting impact as well as success sto-ries in which SBAR facilitated a shared mental modelDecision aids standardization redundancy of SBAR inhospital forms and forcing functions in reporting toolsled to early successes
Educational training was provided for current andnew staff Constant reminders by leadership in requiringdocumentation to be in the SBAR format assisted inearly adoption Spread efforts were advanced to alldepartments including nonclinical areas for use in com-munication and documentation
The spread team found it difficult to identify outcomemeasures and sought advice from behavior experts Theteam then arrived at the following two outcome meas-ures Consistent use of the medication reconciliation
process Timely and accurate communication betweennurses pharmacists and physicians is critical to accom-plish medication reconciliation This communicationmust occur at multiple points during the inpatient stayincluding admission transfer between units and dis-charge14ndash17 Variances in medication lists can result induplication omission wrong doses and so on poten-tially resulting in patient harm Using SBAR communica-tion techniques should result in improved use of themedication reconciliation process Number of adverse patient events Improvedcommunication should improve the efficiency and effec-tiveness of teamwork and thus result in a reduction of alltypes of adverse events to patients
ResultsProcess Measure Use of SBARSt Joseph Medical Center realized a mean of 96 use of SBAR in FY 2005 (Figure 4 page 174) Teamresource management training was conducted with
Laminated posters displayed on the units Stickers placed on each phone at the nursing units Middle managers shared stories of staffrsquos SBAR use
and these staff members were recruited as spreadagents to their peers
Examples developed for nonclinical areas Staff on the obstetrics unit conducted peer obser-
vation for the use of SBAR in nurse-physician com-munication and shift hand-off reports
Input from the patient services practice councilwas obtained in development of a user-friendlytool for shift hand-off reports
Staff ldquopracticedrdquo their SBAR hand-off reports to physicians with peers before making the call
Monthly gamesquizzes with rewards Good examples of SBAR were recognized by being
published on Web sites on hospital bulletin boardsin hospital publications and so on
Peer assist meetings were held to brainstorm ideasfor use of SBAR among different departments
A shared drive was developed to share data andteam activities
The medical director asked physicians to listen foruse of SBAR in communication from nursing staffand encourage nursing staff to give the ldquoRrdquo part ofSBAR (recommendation)
SBAR training and a follow-up quiz were added toall new employeesrsquo orientation
SBAR was incorporated into annual safety educa-tion for all employees
SBAR was included in team resource managementtraining
Screensavers were used to promote knowledge anduse of SBAR
A safety hotline using SBAR was created
Dixon NM Does your organization have an asking problemKnowledge Management Review 718ndash23 MayndashJun 2004
Table 2 Mechanisms to Spread Use ofSituation Background Assessment and
Recommendation (SBAR)
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
171March 2006 Volume 32 Number 3
983 of targeted staff exceeding a goal of 90Retraining was completed with 87 of targeted staffAbbreviated versions of team resource managementtraining was provided to 39 of physicians and midlev-el practitioners exceeding the goal of 25
Outcome Measures Medication Reconciliation andAdverse Events
The spread team considered medication reconcilia-tion and adverse events as separate processes not direct-ly dependent on SBAR However the teamrsquos thinkingwas that better communication reflecting SBAR usewould improve reconciliation and the incidence ofadverse events
The frequency of medication reconciliation demon-strated notable gains from October 2002ndashAugust 2004 to September 2004ndashDecember 2005mdashadmissionreconciliation improved from a mean of 72 to a meanof 88 (Figure 5 page 174) and discharge reconcilia-tion improved from a mean of 53 to a mean of 89(Figure 6 page 175)
The rate of adverse events was measured using theGlobal Trigger Tool which contains a list of multipletriggers appropriate for general care surgical careintensive care emergency department medicationlaboratory and perinatal care that prompt the reviewerto look further for evidence of an adverse event18ndash20
The rate of events per 1000 patient days is measured
Figure 1 The information on the laminated poster also reproduced on the pocket cards for clinicians describes the
Situation Background Assessment and Recommendation (SBAR) steps with an example for each
Laminated Poster
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
172March 2006 Volume 32 Number 3
Figure 2 The Situation Background Assessment and Recommendation (SBAR) Report to a Physician is intended
for a nurse making a report to a physician
Nursersquos Report to a Physician
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
173March 2006 Volume 32 Number 3
Figure 3 The hand-off form can be used by nurses at shift change
Hand-off Form
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
174March 2006 Volume 32 Number 3
by calculating the total number ofevents dividing by the total of lengthof stay for all charts reviewed andmultiplying by 1000 Each month 20charts were chosen at random to bereviewed The rate of events wasreduced from a baseline of 899 per1000 patient days in October 2004 to3996 per 1000 patient days overall inFY 2005
Adverse drug events identifiedthrough use of the Global Trigger Tooldecreased from a baseline of 2997 per1000 patient days to 1764 per 1000patient days
ReflectionsThe power of top managementrsquosinvolvement in performance improve-ment projects was realized Selectleaders from the top managementteam were not only involved in imple-menting SBAR but also providedhuman technological and financialresources
Flattening of the hierarchy amongnursing staff and physicians led to a cooperative effort to improve communication and improved satis-faction for each of those populationsIt was helpful to start with a smallgroup which included a few key members and early adopters and then spread the change to peers Use of story-telling promoted the benefits of goodcommunication and the potential hazards of poor communication Selecting team members from areas in which SBAR plays a crucial role led to early adoption and buy-in of the concept The addition of a media relations staff member and the incorpora-tion of information technology assisted the team infeedback
Next steps include integration of SBAR into the elec-tronic medical record for documentation by all clinicalcaregivers
Summary and ConclusionsFor OSF St Joseph Medical Center use of SBAR in bothoral and written communication has improved patientsafety by providing clear accurate feedback of informa-tion between caregivers There are fewer incidents ofmissed information during handoffs since SBAR wasimplemented because concise facts are shared in anorganized format
Staff members are encouraged to ldquorecommendrdquo on the basis of their observations and this assistsphysicians with situational awareness through the
Figure 4 Use of Situation Background Assessment and Recommendation
(SBAR) reached a mean of 96 in fiscal year 2005
SBAR Use 2004ndash2005
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at admission improved from a mean
of 72 to a mean of 88
Use of SBAR in Admission Reconciliation2004ndash2005
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
175March 2006 Volume 32 Number 3
eyes of the bedside caregiver Staffmembers feel empowered and haveinfluence over decisions that affectwork life using SBAR thus improvingjob satisfaction Currently SBAR tools are being tested in communica-tion handoffs between shifts fortransfers to other departments (forexample radiology operating room)and with patients admitted from theemergency department SBAR pro-motes the six aims of the Institute of Medicine in providing safe effi-cient effective equitable timely andpatient-centered lines of communica-tion21 J
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at discharge improved from a mean of
53 to a mean of 89
Use of SBAR in Discharge Reconciliation2004ndash2005
Kathleen M Haig RN is Director Quality ResourceManagementRisk ManagerPatient Safety Officer andStaci Sutton RN is Emergency Services Manager OSF StJoseph Medical Center Bloomington Illinois JohnWhittington MD is Patient Safety OfficerDirector of Knowledge Management OSF Healthcare SystemPeoria Illinois Please address correspondence to JohnWhittington johnwwhittingtonosfhealthcareorg
1 Joint Commission on Accreditation of Healthcare OrganizationsSentinel Event Statistics-June 30 2005 httpwwwjcahoorgaccred-ited+organizationssentinel+eventsentinel+event+statisticshtm (lastaccessed Jan 24 2006)2 Joint Commission on Accreditation of Healthcare Organizations2006 Critical Access Hospital and Hospital National Patient
Safety Goals httpwwwjcahoorgaccredited+organizationspatient+safety06_npsg06_npsg_cah_haphtm (last accessed Jan 24 2006)3 Wachter RM Shojania KG Internal Bleeding The Truth Behind
Americas Terrifying Epidemic of Medical Mistakes New YorkRugged Land 2004 4 Thomas EJ Sexton JB Helmreich RL Discrepant attitudes aboutteamwork among critical care nurses and physicians Crit Care Med
31956ndash959 Mar 20035 Greenfield LJ Doctors and nurses A troubled partnership Ann
Surg 230279-288 Sep 19996 Leonard M Graham S Bonacum D The human factor The crit-ical importance of effective teamwork and communication in pro-viding safe care Qual Saf Health Care 13 (suppl 1)i85ndashi90 Oct20047 McFerran SC et al Perinatal patient safety project A multicenterapproach to improve performance reliability at Kaiser Permanente JPerinat Neonatal Nurs 1937ndash45 JanndashMar 2005
References
8 Institute for Healthcare Improvement Framework for SpreadhttpwwwihiorgIHITopicsImprovementSpreadingChangesChanges (last accessed Jan 24 2006)9 Helmreich RL Merritt AC Culture at Work in Aviation and
Medicine National Organizational and Professional Influences
Aldershot UK Ashgate 200110 Helmreich RL On error management Lessons from aviation BMJ
320(7237)781ndash785 Mar 2000 11 Kosnik LK The new paradigm of crew resource management justwhat is needed to re-engage the stalled collaborative movement Jt
Comm J Qual Improv 28235ndash241 May 200212 Risser DT et al The potential for improved teamwork to reducemedical errors in the emergency department The MedTeams ResearchConsortium Ann Emerg Med 34373-383 Sep 1994 13 Wiener EL Kanki BG Helmreich RL Cockpit Resource
Management San Diego Harcourt Brace 199314 Gleason KM et al Reconciliation of discrepancies in medicationhistories and admission orders of newly hospitalized patients Am J
Health Syst Pharm 611689ndash1695 Aug 15 2004 15 Pronovost P et al Medication reconciliation tool A practical tool toreduce medication errors during patient transfer from an intensive careunit Journal of Clinical Outcomes Management 1126ndash33 Jan 200416 Rozich JD et al Medication safety One organizations approachto the challenge Journal of Clinical Outcomes Management 827ndash34Oct 2001 17 Whittington J Cohen H OSF healthcares journey in patient safe-ty Qual Manag Health Care 1353-59 JanndashMar 2004 18 Resar RK Rozich JD Classen D Methodology and rationale forthe measurement of harm with trigger tools Qual Saf Health Care 12(suppl 2)ii39ndashii45 Dec 2003 19 Rozich JD Haraden CR Resar RK Adverse drug event triggertool A practical methodology for measuring medication related harmQual Saf Health Care 12194ndash200 Jun 2003 20 Institute for Healthcare Improvement Global Trigger Tool for
Measuring Adverse Events (IHI Tool) httpwwwihiorgIHITopicsPatientSafetySafetyGeneralToolsGlobalTriggerToolforMeasuringAEshtm (last accessed Jan 24 2006)21 Institute of Medicine Crossing the Quality Chasm WashingtonDC National Academy Press 2001
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations

169March 2006 Volume 32 Number 3
as a contributing factor to potential adverse eventsThe first better idea was development of an ldquoelevatorspeechrdquomdasha description of SBAR in a few short sen-tencesmdashto explain the projectrsquos intent
The set-up targeted the clinical caregivers includingnurses lab personnel medical imaging personnel rehabpersonnel dieticians social services personnel pharma-cists and physicians for the initial spread plan Initialkey messengers to spread the Better Ideas included teammembers and Nursing Practice Council members Thesemembers were asked to select one peer who was anearly adopter to create a Social System for the spread ofSBAR Technical support aided knowledge managementby providing measurement and feedback to the adopter audiences
Addressing the Spread of SBAR Efforts to promote the use of SBAR began in April 2004 approximately five months before the formal team formation through introduction of theconcept in clinical educational settings Baseline infor-mation was obtained in August 2004 during the pro-jectrsquos pre-implementation phase through a ldquosecretshoppersrdquo survey Ten staff members were called atrandom by either the corporate or the internal patientsafety officer They were asked to describe what SBARstood for and then provide an example of how this con-cept is used in their daily communications Results ofthe monthly survey were displayed on a run chart andshared throughout the organization for feedback Thebaseline data demonstrated that on average staffwere able to respond correctly 60 of the time
In September 2004 the team set an aim to increasethe use of the SBAR communication tool to 90 bySeptember 2005 Starting in November 2004 teamresource management on the SBAR concept was con-ducted in multiple areas specifically the intensive careunitpost-intensive care unit (ICUPICU) respiratorycardiac rehabilitation cardiac catheterization lab inter-ventional radiology medical surgical floatregistrypediatrics transitional care unit and supervision staffThis training was selected as an organizational goal tosupport the improvement efforts
Using the Plan Do Study Act (PDSA) performanceimprovement methodology efforts to incorporate SBAR
began on a general medical nursing unit in October2004 Tests of change were conducted with tools creat-ed by the team and revisions were made on the basis ofinput from the front-line staff members who piloted thetool Tests were small using one person for one day andgradually increasing those involved in the test until aworkable tool was obtained Once this was achievedthe SBAR trigger tool was spread to the surgical unit inJanuary 2005 and to the critical care unit in March 2005Finally SBAR was spread housewide in April 2005 fol-lowing meetings with managers of nonclinical areassuch as social services rehabilitation medical imagingand pharmacy
Identifying and Implementing Solutions Better ideas included incorporation of SBAR into a vari-ety of reporting documents as listed in Table 1 (above)Multiple mechanisms were used to spread the use ofSBAR including those listed in Table 2 (page 170) Thelaminated poster is shown in Figure 1 (page 171) thenursersquos report to a physician in Figure 2 (page 172) andthe hand-off form in Figure 3 (page 173)
Shift report hand-off tools specific to specialtynursing units (labor postpartum nursery)
Strategic goal-reporting Emergency medical services run reports SBAR briefings for emergency department cardiac
arrests andor trauma patients Charge nurse to charge nurse briefing tool Incident reports Shift hand-off reports including certified nursing
assistants Case review descriptions Hospital forms (including administrative staff
meeting minutes the ethics committee issue formand the inpatient and outpatient satisfactionreporting tools)
A service excellence report to report patient andorstaff opportunities for improvement to managers ofall hospital departments
Table 1 Reporting Documents IncorporatingSituation Background Assessment and
Recommendation (SBAR)
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
170March 2006 Volume 32 Number 3
Feasibility and Implementation Issues Implementation approaches included the followingstrategies
Leadership key strategic initiative goals andincentives are aligned and an executive sponsor wasdelegated Better ideas develop the case and describe the ideas Set-upmdashtarget population early adopters Social system and communication key messengerscommunication strategies and technical support Measurement and feedback
Stories were shared that demonstrated missed oppor-tunities and the resulting impact as well as success sto-ries in which SBAR facilitated a shared mental modelDecision aids standardization redundancy of SBAR inhospital forms and forcing functions in reporting toolsled to early successes
Educational training was provided for current andnew staff Constant reminders by leadership in requiringdocumentation to be in the SBAR format assisted inearly adoption Spread efforts were advanced to alldepartments including nonclinical areas for use in com-munication and documentation
The spread team found it difficult to identify outcomemeasures and sought advice from behavior experts Theteam then arrived at the following two outcome meas-ures Consistent use of the medication reconciliation
process Timely and accurate communication betweennurses pharmacists and physicians is critical to accom-plish medication reconciliation This communicationmust occur at multiple points during the inpatient stayincluding admission transfer between units and dis-charge14ndash17 Variances in medication lists can result induplication omission wrong doses and so on poten-tially resulting in patient harm Using SBAR communica-tion techniques should result in improved use of themedication reconciliation process Number of adverse patient events Improvedcommunication should improve the efficiency and effec-tiveness of teamwork and thus result in a reduction of alltypes of adverse events to patients
ResultsProcess Measure Use of SBARSt Joseph Medical Center realized a mean of 96 use of SBAR in FY 2005 (Figure 4 page 174) Teamresource management training was conducted with
Laminated posters displayed on the units Stickers placed on each phone at the nursing units Middle managers shared stories of staffrsquos SBAR use
and these staff members were recruited as spreadagents to their peers
Examples developed for nonclinical areas Staff on the obstetrics unit conducted peer obser-
vation for the use of SBAR in nurse-physician com-munication and shift hand-off reports
Input from the patient services practice councilwas obtained in development of a user-friendlytool for shift hand-off reports
Staff ldquopracticedrdquo their SBAR hand-off reports to physicians with peers before making the call
Monthly gamesquizzes with rewards Good examples of SBAR were recognized by being
published on Web sites on hospital bulletin boardsin hospital publications and so on
Peer assist meetings were held to brainstorm ideasfor use of SBAR among different departments
A shared drive was developed to share data andteam activities
The medical director asked physicians to listen foruse of SBAR in communication from nursing staffand encourage nursing staff to give the ldquoRrdquo part ofSBAR (recommendation)
SBAR training and a follow-up quiz were added toall new employeesrsquo orientation
SBAR was incorporated into annual safety educa-tion for all employees
SBAR was included in team resource managementtraining
Screensavers were used to promote knowledge anduse of SBAR
A safety hotline using SBAR was created
Dixon NM Does your organization have an asking problemKnowledge Management Review 718ndash23 MayndashJun 2004
Table 2 Mechanisms to Spread Use ofSituation Background Assessment and
Recommendation (SBAR)
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
171March 2006 Volume 32 Number 3
983 of targeted staff exceeding a goal of 90Retraining was completed with 87 of targeted staffAbbreviated versions of team resource managementtraining was provided to 39 of physicians and midlev-el practitioners exceeding the goal of 25
Outcome Measures Medication Reconciliation andAdverse Events
The spread team considered medication reconcilia-tion and adverse events as separate processes not direct-ly dependent on SBAR However the teamrsquos thinkingwas that better communication reflecting SBAR usewould improve reconciliation and the incidence ofadverse events
The frequency of medication reconciliation demon-strated notable gains from October 2002ndashAugust 2004 to September 2004ndashDecember 2005mdashadmissionreconciliation improved from a mean of 72 to a meanof 88 (Figure 5 page 174) and discharge reconcilia-tion improved from a mean of 53 to a mean of 89(Figure 6 page 175)
The rate of adverse events was measured using theGlobal Trigger Tool which contains a list of multipletriggers appropriate for general care surgical careintensive care emergency department medicationlaboratory and perinatal care that prompt the reviewerto look further for evidence of an adverse event18ndash20
The rate of events per 1000 patient days is measured
Figure 1 The information on the laminated poster also reproduced on the pocket cards for clinicians describes the
Situation Background Assessment and Recommendation (SBAR) steps with an example for each
Laminated Poster
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
172March 2006 Volume 32 Number 3
Figure 2 The Situation Background Assessment and Recommendation (SBAR) Report to a Physician is intended
for a nurse making a report to a physician
Nursersquos Report to a Physician
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
173March 2006 Volume 32 Number 3
Figure 3 The hand-off form can be used by nurses at shift change
Hand-off Form
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
174March 2006 Volume 32 Number 3
by calculating the total number ofevents dividing by the total of lengthof stay for all charts reviewed andmultiplying by 1000 Each month 20charts were chosen at random to bereviewed The rate of events wasreduced from a baseline of 899 per1000 patient days in October 2004 to3996 per 1000 patient days overall inFY 2005
Adverse drug events identifiedthrough use of the Global Trigger Tooldecreased from a baseline of 2997 per1000 patient days to 1764 per 1000patient days
ReflectionsThe power of top managementrsquosinvolvement in performance improve-ment projects was realized Selectleaders from the top managementteam were not only involved in imple-menting SBAR but also providedhuman technological and financialresources
Flattening of the hierarchy amongnursing staff and physicians led to a cooperative effort to improve communication and improved satis-faction for each of those populationsIt was helpful to start with a smallgroup which included a few key members and early adopters and then spread the change to peers Use of story-telling promoted the benefits of goodcommunication and the potential hazards of poor communication Selecting team members from areas in which SBAR plays a crucial role led to early adoption and buy-in of the concept The addition of a media relations staff member and the incorpora-tion of information technology assisted the team infeedback
Next steps include integration of SBAR into the elec-tronic medical record for documentation by all clinicalcaregivers
Summary and ConclusionsFor OSF St Joseph Medical Center use of SBAR in bothoral and written communication has improved patientsafety by providing clear accurate feedback of informa-tion between caregivers There are fewer incidents ofmissed information during handoffs since SBAR wasimplemented because concise facts are shared in anorganized format
Staff members are encouraged to ldquorecommendrdquo on the basis of their observations and this assistsphysicians with situational awareness through the
Figure 4 Use of Situation Background Assessment and Recommendation
(SBAR) reached a mean of 96 in fiscal year 2005
SBAR Use 2004ndash2005
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at admission improved from a mean
of 72 to a mean of 88
Use of SBAR in Admission Reconciliation2004ndash2005
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
175March 2006 Volume 32 Number 3
eyes of the bedside caregiver Staffmembers feel empowered and haveinfluence over decisions that affectwork life using SBAR thus improvingjob satisfaction Currently SBAR tools are being tested in communica-tion handoffs between shifts fortransfers to other departments (forexample radiology operating room)and with patients admitted from theemergency department SBAR pro-motes the six aims of the Institute of Medicine in providing safe effi-cient effective equitable timely andpatient-centered lines of communica-tion21 J
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at discharge improved from a mean of
53 to a mean of 89
Use of SBAR in Discharge Reconciliation2004ndash2005
Kathleen M Haig RN is Director Quality ResourceManagementRisk ManagerPatient Safety Officer andStaci Sutton RN is Emergency Services Manager OSF StJoseph Medical Center Bloomington Illinois JohnWhittington MD is Patient Safety OfficerDirector of Knowledge Management OSF Healthcare SystemPeoria Illinois Please address correspondence to JohnWhittington johnwwhittingtonosfhealthcareorg
1 Joint Commission on Accreditation of Healthcare OrganizationsSentinel Event Statistics-June 30 2005 httpwwwjcahoorgaccred-ited+organizationssentinel+eventsentinel+event+statisticshtm (lastaccessed Jan 24 2006)2 Joint Commission on Accreditation of Healthcare Organizations2006 Critical Access Hospital and Hospital National Patient
Safety Goals httpwwwjcahoorgaccredited+organizationspatient+safety06_npsg06_npsg_cah_haphtm (last accessed Jan 24 2006)3 Wachter RM Shojania KG Internal Bleeding The Truth Behind
Americas Terrifying Epidemic of Medical Mistakes New YorkRugged Land 2004 4 Thomas EJ Sexton JB Helmreich RL Discrepant attitudes aboutteamwork among critical care nurses and physicians Crit Care Med
31956ndash959 Mar 20035 Greenfield LJ Doctors and nurses A troubled partnership Ann
Surg 230279-288 Sep 19996 Leonard M Graham S Bonacum D The human factor The crit-ical importance of effective teamwork and communication in pro-viding safe care Qual Saf Health Care 13 (suppl 1)i85ndashi90 Oct20047 McFerran SC et al Perinatal patient safety project A multicenterapproach to improve performance reliability at Kaiser Permanente JPerinat Neonatal Nurs 1937ndash45 JanndashMar 2005
References
8 Institute for Healthcare Improvement Framework for SpreadhttpwwwihiorgIHITopicsImprovementSpreadingChangesChanges (last accessed Jan 24 2006)9 Helmreich RL Merritt AC Culture at Work in Aviation and
Medicine National Organizational and Professional Influences
Aldershot UK Ashgate 200110 Helmreich RL On error management Lessons from aviation BMJ
320(7237)781ndash785 Mar 2000 11 Kosnik LK The new paradigm of crew resource management justwhat is needed to re-engage the stalled collaborative movement Jt
Comm J Qual Improv 28235ndash241 May 200212 Risser DT et al The potential for improved teamwork to reducemedical errors in the emergency department The MedTeams ResearchConsortium Ann Emerg Med 34373-383 Sep 1994 13 Wiener EL Kanki BG Helmreich RL Cockpit Resource
Management San Diego Harcourt Brace 199314 Gleason KM et al Reconciliation of discrepancies in medicationhistories and admission orders of newly hospitalized patients Am J
Health Syst Pharm 611689ndash1695 Aug 15 2004 15 Pronovost P et al Medication reconciliation tool A practical tool toreduce medication errors during patient transfer from an intensive careunit Journal of Clinical Outcomes Management 1126ndash33 Jan 200416 Rozich JD et al Medication safety One organizations approachto the challenge Journal of Clinical Outcomes Management 827ndash34Oct 2001 17 Whittington J Cohen H OSF healthcares journey in patient safe-ty Qual Manag Health Care 1353-59 JanndashMar 2004 18 Resar RK Rozich JD Classen D Methodology and rationale forthe measurement of harm with trigger tools Qual Saf Health Care 12(suppl 2)ii39ndashii45 Dec 2003 19 Rozich JD Haraden CR Resar RK Adverse drug event triggertool A practical methodology for measuring medication related harmQual Saf Health Care 12194ndash200 Jun 2003 20 Institute for Healthcare Improvement Global Trigger Tool for
Measuring Adverse Events (IHI Tool) httpwwwihiorgIHITopicsPatientSafetySafetyGeneralToolsGlobalTriggerToolforMeasuringAEshtm (last accessed Jan 24 2006)21 Institute of Medicine Crossing the Quality Chasm WashingtonDC National Academy Press 2001
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations

170March 2006 Volume 32 Number 3
Feasibility and Implementation Issues Implementation approaches included the followingstrategies
Leadership key strategic initiative goals andincentives are aligned and an executive sponsor wasdelegated Better ideas develop the case and describe the ideas Set-upmdashtarget population early adopters Social system and communication key messengerscommunication strategies and technical support Measurement and feedback
Stories were shared that demonstrated missed oppor-tunities and the resulting impact as well as success sto-ries in which SBAR facilitated a shared mental modelDecision aids standardization redundancy of SBAR inhospital forms and forcing functions in reporting toolsled to early successes
Educational training was provided for current andnew staff Constant reminders by leadership in requiringdocumentation to be in the SBAR format assisted inearly adoption Spread efforts were advanced to alldepartments including nonclinical areas for use in com-munication and documentation
The spread team found it difficult to identify outcomemeasures and sought advice from behavior experts Theteam then arrived at the following two outcome meas-ures Consistent use of the medication reconciliation
process Timely and accurate communication betweennurses pharmacists and physicians is critical to accom-plish medication reconciliation This communicationmust occur at multiple points during the inpatient stayincluding admission transfer between units and dis-charge14ndash17 Variances in medication lists can result induplication omission wrong doses and so on poten-tially resulting in patient harm Using SBAR communica-tion techniques should result in improved use of themedication reconciliation process Number of adverse patient events Improvedcommunication should improve the efficiency and effec-tiveness of teamwork and thus result in a reduction of alltypes of adverse events to patients
ResultsProcess Measure Use of SBARSt Joseph Medical Center realized a mean of 96 use of SBAR in FY 2005 (Figure 4 page 174) Teamresource management training was conducted with
Laminated posters displayed on the units Stickers placed on each phone at the nursing units Middle managers shared stories of staffrsquos SBAR use
and these staff members were recruited as spreadagents to their peers
Examples developed for nonclinical areas Staff on the obstetrics unit conducted peer obser-
vation for the use of SBAR in nurse-physician com-munication and shift hand-off reports
Input from the patient services practice councilwas obtained in development of a user-friendlytool for shift hand-off reports
Staff ldquopracticedrdquo their SBAR hand-off reports to physicians with peers before making the call
Monthly gamesquizzes with rewards Good examples of SBAR were recognized by being
published on Web sites on hospital bulletin boardsin hospital publications and so on
Peer assist meetings were held to brainstorm ideasfor use of SBAR among different departments
A shared drive was developed to share data andteam activities
The medical director asked physicians to listen foruse of SBAR in communication from nursing staffand encourage nursing staff to give the ldquoRrdquo part ofSBAR (recommendation)
SBAR training and a follow-up quiz were added toall new employeesrsquo orientation
SBAR was incorporated into annual safety educa-tion for all employees
SBAR was included in team resource managementtraining
Screensavers were used to promote knowledge anduse of SBAR
A safety hotline using SBAR was created
Dixon NM Does your organization have an asking problemKnowledge Management Review 718ndash23 MayndashJun 2004
Table 2 Mechanisms to Spread Use ofSituation Background Assessment and
Recommendation (SBAR)
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
171March 2006 Volume 32 Number 3
983 of targeted staff exceeding a goal of 90Retraining was completed with 87 of targeted staffAbbreviated versions of team resource managementtraining was provided to 39 of physicians and midlev-el practitioners exceeding the goal of 25
Outcome Measures Medication Reconciliation andAdverse Events
The spread team considered medication reconcilia-tion and adverse events as separate processes not direct-ly dependent on SBAR However the teamrsquos thinkingwas that better communication reflecting SBAR usewould improve reconciliation and the incidence ofadverse events
The frequency of medication reconciliation demon-strated notable gains from October 2002ndashAugust 2004 to September 2004ndashDecember 2005mdashadmissionreconciliation improved from a mean of 72 to a meanof 88 (Figure 5 page 174) and discharge reconcilia-tion improved from a mean of 53 to a mean of 89(Figure 6 page 175)
The rate of adverse events was measured using theGlobal Trigger Tool which contains a list of multipletriggers appropriate for general care surgical careintensive care emergency department medicationlaboratory and perinatal care that prompt the reviewerto look further for evidence of an adverse event18ndash20
The rate of events per 1000 patient days is measured
Figure 1 The information on the laminated poster also reproduced on the pocket cards for clinicians describes the
Situation Background Assessment and Recommendation (SBAR) steps with an example for each
Laminated Poster
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
172March 2006 Volume 32 Number 3
Figure 2 The Situation Background Assessment and Recommendation (SBAR) Report to a Physician is intended
for a nurse making a report to a physician
Nursersquos Report to a Physician
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
173March 2006 Volume 32 Number 3
Figure 3 The hand-off form can be used by nurses at shift change
Hand-off Form
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
174March 2006 Volume 32 Number 3
by calculating the total number ofevents dividing by the total of lengthof stay for all charts reviewed andmultiplying by 1000 Each month 20charts were chosen at random to bereviewed The rate of events wasreduced from a baseline of 899 per1000 patient days in October 2004 to3996 per 1000 patient days overall inFY 2005
Adverse drug events identifiedthrough use of the Global Trigger Tooldecreased from a baseline of 2997 per1000 patient days to 1764 per 1000patient days
ReflectionsThe power of top managementrsquosinvolvement in performance improve-ment projects was realized Selectleaders from the top managementteam were not only involved in imple-menting SBAR but also providedhuman technological and financialresources
Flattening of the hierarchy amongnursing staff and physicians led to a cooperative effort to improve communication and improved satis-faction for each of those populationsIt was helpful to start with a smallgroup which included a few key members and early adopters and then spread the change to peers Use of story-telling promoted the benefits of goodcommunication and the potential hazards of poor communication Selecting team members from areas in which SBAR plays a crucial role led to early adoption and buy-in of the concept The addition of a media relations staff member and the incorpora-tion of information technology assisted the team infeedback
Next steps include integration of SBAR into the elec-tronic medical record for documentation by all clinicalcaregivers
Summary and ConclusionsFor OSF St Joseph Medical Center use of SBAR in bothoral and written communication has improved patientsafety by providing clear accurate feedback of informa-tion between caregivers There are fewer incidents ofmissed information during handoffs since SBAR wasimplemented because concise facts are shared in anorganized format
Staff members are encouraged to ldquorecommendrdquo on the basis of their observations and this assistsphysicians with situational awareness through the
Figure 4 Use of Situation Background Assessment and Recommendation
(SBAR) reached a mean of 96 in fiscal year 2005
SBAR Use 2004ndash2005
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at admission improved from a mean
of 72 to a mean of 88
Use of SBAR in Admission Reconciliation2004ndash2005
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
175March 2006 Volume 32 Number 3
eyes of the bedside caregiver Staffmembers feel empowered and haveinfluence over decisions that affectwork life using SBAR thus improvingjob satisfaction Currently SBAR tools are being tested in communica-tion handoffs between shifts fortransfers to other departments (forexample radiology operating room)and with patients admitted from theemergency department SBAR pro-motes the six aims of the Institute of Medicine in providing safe effi-cient effective equitable timely andpatient-centered lines of communica-tion21 J
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at discharge improved from a mean of
53 to a mean of 89
Use of SBAR in Discharge Reconciliation2004ndash2005
Kathleen M Haig RN is Director Quality ResourceManagementRisk ManagerPatient Safety Officer andStaci Sutton RN is Emergency Services Manager OSF StJoseph Medical Center Bloomington Illinois JohnWhittington MD is Patient Safety OfficerDirector of Knowledge Management OSF Healthcare SystemPeoria Illinois Please address correspondence to JohnWhittington johnwwhittingtonosfhealthcareorg
1 Joint Commission on Accreditation of Healthcare OrganizationsSentinel Event Statistics-June 30 2005 httpwwwjcahoorgaccred-ited+organizationssentinel+eventsentinel+event+statisticshtm (lastaccessed Jan 24 2006)2 Joint Commission on Accreditation of Healthcare Organizations2006 Critical Access Hospital and Hospital National Patient
Safety Goals httpwwwjcahoorgaccredited+organizationspatient+safety06_npsg06_npsg_cah_haphtm (last accessed Jan 24 2006)3 Wachter RM Shojania KG Internal Bleeding The Truth Behind
Americas Terrifying Epidemic of Medical Mistakes New YorkRugged Land 2004 4 Thomas EJ Sexton JB Helmreich RL Discrepant attitudes aboutteamwork among critical care nurses and physicians Crit Care Med
31956ndash959 Mar 20035 Greenfield LJ Doctors and nurses A troubled partnership Ann
Surg 230279-288 Sep 19996 Leonard M Graham S Bonacum D The human factor The crit-ical importance of effective teamwork and communication in pro-viding safe care Qual Saf Health Care 13 (suppl 1)i85ndashi90 Oct20047 McFerran SC et al Perinatal patient safety project A multicenterapproach to improve performance reliability at Kaiser Permanente JPerinat Neonatal Nurs 1937ndash45 JanndashMar 2005
References
8 Institute for Healthcare Improvement Framework for SpreadhttpwwwihiorgIHITopicsImprovementSpreadingChangesChanges (last accessed Jan 24 2006)9 Helmreich RL Merritt AC Culture at Work in Aviation and
Medicine National Organizational and Professional Influences
Aldershot UK Ashgate 200110 Helmreich RL On error management Lessons from aviation BMJ
320(7237)781ndash785 Mar 2000 11 Kosnik LK The new paradigm of crew resource management justwhat is needed to re-engage the stalled collaborative movement Jt
Comm J Qual Improv 28235ndash241 May 200212 Risser DT et al The potential for improved teamwork to reducemedical errors in the emergency department The MedTeams ResearchConsortium Ann Emerg Med 34373-383 Sep 1994 13 Wiener EL Kanki BG Helmreich RL Cockpit Resource
Management San Diego Harcourt Brace 199314 Gleason KM et al Reconciliation of discrepancies in medicationhistories and admission orders of newly hospitalized patients Am J
Health Syst Pharm 611689ndash1695 Aug 15 2004 15 Pronovost P et al Medication reconciliation tool A practical tool toreduce medication errors during patient transfer from an intensive careunit Journal of Clinical Outcomes Management 1126ndash33 Jan 200416 Rozich JD et al Medication safety One organizations approachto the challenge Journal of Clinical Outcomes Management 827ndash34Oct 2001 17 Whittington J Cohen H OSF healthcares journey in patient safe-ty Qual Manag Health Care 1353-59 JanndashMar 2004 18 Resar RK Rozich JD Classen D Methodology and rationale forthe measurement of harm with trigger tools Qual Saf Health Care 12(suppl 2)ii39ndashii45 Dec 2003 19 Rozich JD Haraden CR Resar RK Adverse drug event triggertool A practical methodology for measuring medication related harmQual Saf Health Care 12194ndash200 Jun 2003 20 Institute for Healthcare Improvement Global Trigger Tool for
Measuring Adverse Events (IHI Tool) httpwwwihiorgIHITopicsPatientSafetySafetyGeneralToolsGlobalTriggerToolforMeasuringAEshtm (last accessed Jan 24 2006)21 Institute of Medicine Crossing the Quality Chasm WashingtonDC National Academy Press 2001
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations

171March 2006 Volume 32 Number 3
983 of targeted staff exceeding a goal of 90Retraining was completed with 87 of targeted staffAbbreviated versions of team resource managementtraining was provided to 39 of physicians and midlev-el practitioners exceeding the goal of 25
Outcome Measures Medication Reconciliation andAdverse Events
The spread team considered medication reconcilia-tion and adverse events as separate processes not direct-ly dependent on SBAR However the teamrsquos thinkingwas that better communication reflecting SBAR usewould improve reconciliation and the incidence ofadverse events
The frequency of medication reconciliation demon-strated notable gains from October 2002ndashAugust 2004 to September 2004ndashDecember 2005mdashadmissionreconciliation improved from a mean of 72 to a meanof 88 (Figure 5 page 174) and discharge reconcilia-tion improved from a mean of 53 to a mean of 89(Figure 6 page 175)
The rate of adverse events was measured using theGlobal Trigger Tool which contains a list of multipletriggers appropriate for general care surgical careintensive care emergency department medicationlaboratory and perinatal care that prompt the reviewerto look further for evidence of an adverse event18ndash20
The rate of events per 1000 patient days is measured
Figure 1 The information on the laminated poster also reproduced on the pocket cards for clinicians describes the
Situation Background Assessment and Recommendation (SBAR) steps with an example for each
Laminated Poster
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
172March 2006 Volume 32 Number 3
Figure 2 The Situation Background Assessment and Recommendation (SBAR) Report to a Physician is intended
for a nurse making a report to a physician
Nursersquos Report to a Physician
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
173March 2006 Volume 32 Number 3
Figure 3 The hand-off form can be used by nurses at shift change
Hand-off Form
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
174March 2006 Volume 32 Number 3
by calculating the total number ofevents dividing by the total of lengthof stay for all charts reviewed andmultiplying by 1000 Each month 20charts were chosen at random to bereviewed The rate of events wasreduced from a baseline of 899 per1000 patient days in October 2004 to3996 per 1000 patient days overall inFY 2005
Adverse drug events identifiedthrough use of the Global Trigger Tooldecreased from a baseline of 2997 per1000 patient days to 1764 per 1000patient days
ReflectionsThe power of top managementrsquosinvolvement in performance improve-ment projects was realized Selectleaders from the top managementteam were not only involved in imple-menting SBAR but also providedhuman technological and financialresources
Flattening of the hierarchy amongnursing staff and physicians led to a cooperative effort to improve communication and improved satis-faction for each of those populationsIt was helpful to start with a smallgroup which included a few key members and early adopters and then spread the change to peers Use of story-telling promoted the benefits of goodcommunication and the potential hazards of poor communication Selecting team members from areas in which SBAR plays a crucial role led to early adoption and buy-in of the concept The addition of a media relations staff member and the incorpora-tion of information technology assisted the team infeedback
Next steps include integration of SBAR into the elec-tronic medical record for documentation by all clinicalcaregivers
Summary and ConclusionsFor OSF St Joseph Medical Center use of SBAR in bothoral and written communication has improved patientsafety by providing clear accurate feedback of informa-tion between caregivers There are fewer incidents ofmissed information during handoffs since SBAR wasimplemented because concise facts are shared in anorganized format
Staff members are encouraged to ldquorecommendrdquo on the basis of their observations and this assistsphysicians with situational awareness through the
Figure 4 Use of Situation Background Assessment and Recommendation
(SBAR) reached a mean of 96 in fiscal year 2005
SBAR Use 2004ndash2005
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at admission improved from a mean
of 72 to a mean of 88
Use of SBAR in Admission Reconciliation2004ndash2005
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
175March 2006 Volume 32 Number 3
eyes of the bedside caregiver Staffmembers feel empowered and haveinfluence over decisions that affectwork life using SBAR thus improvingjob satisfaction Currently SBAR tools are being tested in communica-tion handoffs between shifts fortransfers to other departments (forexample radiology operating room)and with patients admitted from theemergency department SBAR pro-motes the six aims of the Institute of Medicine in providing safe effi-cient effective equitable timely andpatient-centered lines of communica-tion21 J
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at discharge improved from a mean of
53 to a mean of 89
Use of SBAR in Discharge Reconciliation2004ndash2005
Kathleen M Haig RN is Director Quality ResourceManagementRisk ManagerPatient Safety Officer andStaci Sutton RN is Emergency Services Manager OSF StJoseph Medical Center Bloomington Illinois JohnWhittington MD is Patient Safety OfficerDirector of Knowledge Management OSF Healthcare SystemPeoria Illinois Please address correspondence to JohnWhittington johnwwhittingtonosfhealthcareorg
1 Joint Commission on Accreditation of Healthcare OrganizationsSentinel Event Statistics-June 30 2005 httpwwwjcahoorgaccred-ited+organizationssentinel+eventsentinel+event+statisticshtm (lastaccessed Jan 24 2006)2 Joint Commission on Accreditation of Healthcare Organizations2006 Critical Access Hospital and Hospital National Patient
Safety Goals httpwwwjcahoorgaccredited+organizationspatient+safety06_npsg06_npsg_cah_haphtm (last accessed Jan 24 2006)3 Wachter RM Shojania KG Internal Bleeding The Truth Behind
Americas Terrifying Epidemic of Medical Mistakes New YorkRugged Land 2004 4 Thomas EJ Sexton JB Helmreich RL Discrepant attitudes aboutteamwork among critical care nurses and physicians Crit Care Med
31956ndash959 Mar 20035 Greenfield LJ Doctors and nurses A troubled partnership Ann
Surg 230279-288 Sep 19996 Leonard M Graham S Bonacum D The human factor The crit-ical importance of effective teamwork and communication in pro-viding safe care Qual Saf Health Care 13 (suppl 1)i85ndashi90 Oct20047 McFerran SC et al Perinatal patient safety project A multicenterapproach to improve performance reliability at Kaiser Permanente JPerinat Neonatal Nurs 1937ndash45 JanndashMar 2005
References
8 Institute for Healthcare Improvement Framework for SpreadhttpwwwihiorgIHITopicsImprovementSpreadingChangesChanges (last accessed Jan 24 2006)9 Helmreich RL Merritt AC Culture at Work in Aviation and
Medicine National Organizational and Professional Influences
Aldershot UK Ashgate 200110 Helmreich RL On error management Lessons from aviation BMJ
320(7237)781ndash785 Mar 2000 11 Kosnik LK The new paradigm of crew resource management justwhat is needed to re-engage the stalled collaborative movement Jt
Comm J Qual Improv 28235ndash241 May 200212 Risser DT et al The potential for improved teamwork to reducemedical errors in the emergency department The MedTeams ResearchConsortium Ann Emerg Med 34373-383 Sep 1994 13 Wiener EL Kanki BG Helmreich RL Cockpit Resource
Management San Diego Harcourt Brace 199314 Gleason KM et al Reconciliation of discrepancies in medicationhistories and admission orders of newly hospitalized patients Am J
Health Syst Pharm 611689ndash1695 Aug 15 2004 15 Pronovost P et al Medication reconciliation tool A practical tool toreduce medication errors during patient transfer from an intensive careunit Journal of Clinical Outcomes Management 1126ndash33 Jan 200416 Rozich JD et al Medication safety One organizations approachto the challenge Journal of Clinical Outcomes Management 827ndash34Oct 2001 17 Whittington J Cohen H OSF healthcares journey in patient safe-ty Qual Manag Health Care 1353-59 JanndashMar 2004 18 Resar RK Rozich JD Classen D Methodology and rationale forthe measurement of harm with trigger tools Qual Saf Health Care 12(suppl 2)ii39ndashii45 Dec 2003 19 Rozich JD Haraden CR Resar RK Adverse drug event triggertool A practical methodology for measuring medication related harmQual Saf Health Care 12194ndash200 Jun 2003 20 Institute for Healthcare Improvement Global Trigger Tool for
Measuring Adverse Events (IHI Tool) httpwwwihiorgIHITopicsPatientSafetySafetyGeneralToolsGlobalTriggerToolforMeasuringAEshtm (last accessed Jan 24 2006)21 Institute of Medicine Crossing the Quality Chasm WashingtonDC National Academy Press 2001
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
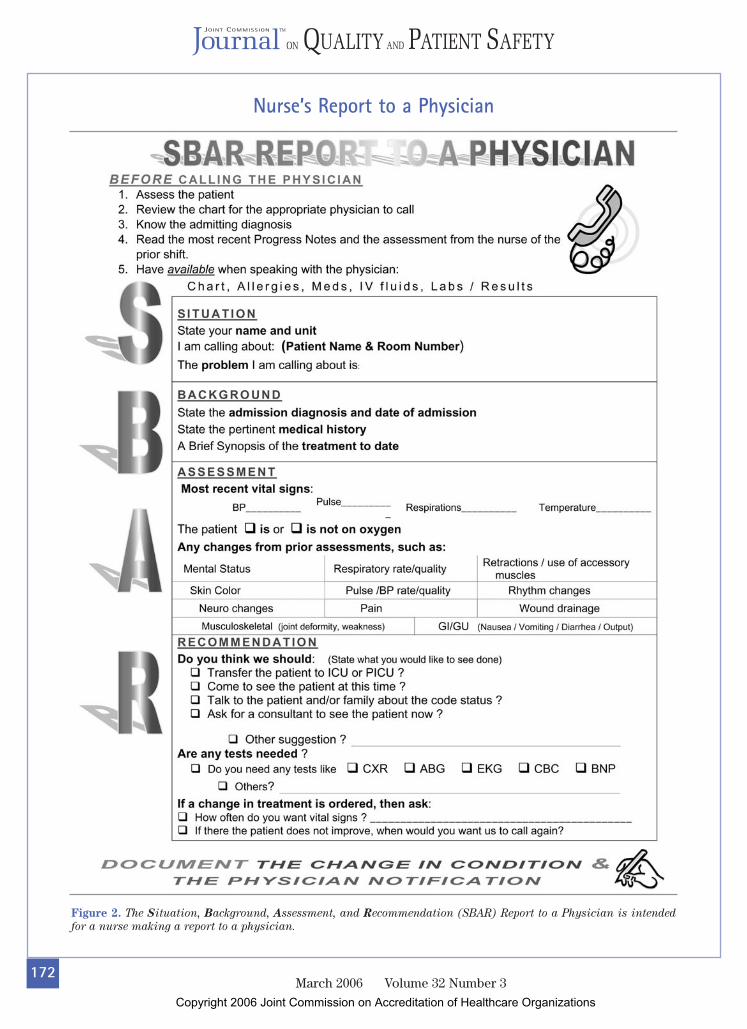
172March 2006 Volume 32 Number 3
Figure 2 The Situation Background Assessment and Recommendation (SBAR) Report to a Physician is intended
for a nurse making a report to a physician
Nursersquos Report to a Physician
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
173March 2006 Volume 32 Number 3
Figure 3 The hand-off form can be used by nurses at shift change
Hand-off Form
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
174March 2006 Volume 32 Number 3
by calculating the total number ofevents dividing by the total of lengthof stay for all charts reviewed andmultiplying by 1000 Each month 20charts were chosen at random to bereviewed The rate of events wasreduced from a baseline of 899 per1000 patient days in October 2004 to3996 per 1000 patient days overall inFY 2005
Adverse drug events identifiedthrough use of the Global Trigger Tooldecreased from a baseline of 2997 per1000 patient days to 1764 per 1000patient days
ReflectionsThe power of top managementrsquosinvolvement in performance improve-ment projects was realized Selectleaders from the top managementteam were not only involved in imple-menting SBAR but also providedhuman technological and financialresources
Flattening of the hierarchy amongnursing staff and physicians led to a cooperative effort to improve communication and improved satis-faction for each of those populationsIt was helpful to start with a smallgroup which included a few key members and early adopters and then spread the change to peers Use of story-telling promoted the benefits of goodcommunication and the potential hazards of poor communication Selecting team members from areas in which SBAR plays a crucial role led to early adoption and buy-in of the concept The addition of a media relations staff member and the incorpora-tion of information technology assisted the team infeedback
Next steps include integration of SBAR into the elec-tronic medical record for documentation by all clinicalcaregivers
Summary and ConclusionsFor OSF St Joseph Medical Center use of SBAR in bothoral and written communication has improved patientsafety by providing clear accurate feedback of informa-tion between caregivers There are fewer incidents ofmissed information during handoffs since SBAR wasimplemented because concise facts are shared in anorganized format
Staff members are encouraged to ldquorecommendrdquo on the basis of their observations and this assistsphysicians with situational awareness through the
Figure 4 Use of Situation Background Assessment and Recommendation
(SBAR) reached a mean of 96 in fiscal year 2005
SBAR Use 2004ndash2005
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at admission improved from a mean
of 72 to a mean of 88
Use of SBAR in Admission Reconciliation2004ndash2005
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
175March 2006 Volume 32 Number 3
eyes of the bedside caregiver Staffmembers feel empowered and haveinfluence over decisions that affectwork life using SBAR thus improvingjob satisfaction Currently SBAR tools are being tested in communica-tion handoffs between shifts fortransfers to other departments (forexample radiology operating room)and with patients admitted from theemergency department SBAR pro-motes the six aims of the Institute of Medicine in providing safe effi-cient effective equitable timely andpatient-centered lines of communica-tion21 J
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at discharge improved from a mean of
53 to a mean of 89
Use of SBAR in Discharge Reconciliation2004ndash2005
Kathleen M Haig RN is Director Quality ResourceManagementRisk ManagerPatient Safety Officer andStaci Sutton RN is Emergency Services Manager OSF StJoseph Medical Center Bloomington Illinois JohnWhittington MD is Patient Safety OfficerDirector of Knowledge Management OSF Healthcare SystemPeoria Illinois Please address correspondence to JohnWhittington johnwwhittingtonosfhealthcareorg
1 Joint Commission on Accreditation of Healthcare OrganizationsSentinel Event Statistics-June 30 2005 httpwwwjcahoorgaccred-ited+organizationssentinel+eventsentinel+event+statisticshtm (lastaccessed Jan 24 2006)2 Joint Commission on Accreditation of Healthcare Organizations2006 Critical Access Hospital and Hospital National Patient
Safety Goals httpwwwjcahoorgaccredited+organizationspatient+safety06_npsg06_npsg_cah_haphtm (last accessed Jan 24 2006)3 Wachter RM Shojania KG Internal Bleeding The Truth Behind
Americas Terrifying Epidemic of Medical Mistakes New YorkRugged Land 2004 4 Thomas EJ Sexton JB Helmreich RL Discrepant attitudes aboutteamwork among critical care nurses and physicians Crit Care Med
31956ndash959 Mar 20035 Greenfield LJ Doctors and nurses A troubled partnership Ann
Surg 230279-288 Sep 19996 Leonard M Graham S Bonacum D The human factor The crit-ical importance of effective teamwork and communication in pro-viding safe care Qual Saf Health Care 13 (suppl 1)i85ndashi90 Oct20047 McFerran SC et al Perinatal patient safety project A multicenterapproach to improve performance reliability at Kaiser Permanente JPerinat Neonatal Nurs 1937ndash45 JanndashMar 2005
References
8 Institute for Healthcare Improvement Framework for SpreadhttpwwwihiorgIHITopicsImprovementSpreadingChangesChanges (last accessed Jan 24 2006)9 Helmreich RL Merritt AC Culture at Work in Aviation and
Medicine National Organizational and Professional Influences
Aldershot UK Ashgate 200110 Helmreich RL On error management Lessons from aviation BMJ
320(7237)781ndash785 Mar 2000 11 Kosnik LK The new paradigm of crew resource management justwhat is needed to re-engage the stalled collaborative movement Jt
Comm J Qual Improv 28235ndash241 May 200212 Risser DT et al The potential for improved teamwork to reducemedical errors in the emergency department The MedTeams ResearchConsortium Ann Emerg Med 34373-383 Sep 1994 13 Wiener EL Kanki BG Helmreich RL Cockpit Resource
Management San Diego Harcourt Brace 199314 Gleason KM et al Reconciliation of discrepancies in medicationhistories and admission orders of newly hospitalized patients Am J
Health Syst Pharm 611689ndash1695 Aug 15 2004 15 Pronovost P et al Medication reconciliation tool A practical tool toreduce medication errors during patient transfer from an intensive careunit Journal of Clinical Outcomes Management 1126ndash33 Jan 200416 Rozich JD et al Medication safety One organizations approachto the challenge Journal of Clinical Outcomes Management 827ndash34Oct 2001 17 Whittington J Cohen H OSF healthcares journey in patient safe-ty Qual Manag Health Care 1353-59 JanndashMar 2004 18 Resar RK Rozich JD Classen D Methodology and rationale forthe measurement of harm with trigger tools Qual Saf Health Care 12(suppl 2)ii39ndashii45 Dec 2003 19 Rozich JD Haraden CR Resar RK Adverse drug event triggertool A practical methodology for measuring medication related harmQual Saf Health Care 12194ndash200 Jun 2003 20 Institute for Healthcare Improvement Global Trigger Tool for
Measuring Adverse Events (IHI Tool) httpwwwihiorgIHITopicsPatientSafetySafetyGeneralToolsGlobalTriggerToolforMeasuringAEshtm (last accessed Jan 24 2006)21 Institute of Medicine Crossing the Quality Chasm WashingtonDC National Academy Press 2001
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations

173March 2006 Volume 32 Number 3
Figure 3 The hand-off form can be used by nurses at shift change
Hand-off Form
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
174March 2006 Volume 32 Number 3
by calculating the total number ofevents dividing by the total of lengthof stay for all charts reviewed andmultiplying by 1000 Each month 20charts were chosen at random to bereviewed The rate of events wasreduced from a baseline of 899 per1000 patient days in October 2004 to3996 per 1000 patient days overall inFY 2005
Adverse drug events identifiedthrough use of the Global Trigger Tooldecreased from a baseline of 2997 per1000 patient days to 1764 per 1000patient days
ReflectionsThe power of top managementrsquosinvolvement in performance improve-ment projects was realized Selectleaders from the top managementteam were not only involved in imple-menting SBAR but also providedhuman technological and financialresources
Flattening of the hierarchy amongnursing staff and physicians led to a cooperative effort to improve communication and improved satis-faction for each of those populationsIt was helpful to start with a smallgroup which included a few key members and early adopters and then spread the change to peers Use of story-telling promoted the benefits of goodcommunication and the potential hazards of poor communication Selecting team members from areas in which SBAR plays a crucial role led to early adoption and buy-in of the concept The addition of a media relations staff member and the incorpora-tion of information technology assisted the team infeedback
Next steps include integration of SBAR into the elec-tronic medical record for documentation by all clinicalcaregivers
Summary and ConclusionsFor OSF St Joseph Medical Center use of SBAR in bothoral and written communication has improved patientsafety by providing clear accurate feedback of informa-tion between caregivers There are fewer incidents ofmissed information during handoffs since SBAR wasimplemented because concise facts are shared in anorganized format
Staff members are encouraged to ldquorecommendrdquo on the basis of their observations and this assistsphysicians with situational awareness through the
Figure 4 Use of Situation Background Assessment and Recommendation
(SBAR) reached a mean of 96 in fiscal year 2005
SBAR Use 2004ndash2005
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at admission improved from a mean
of 72 to a mean of 88
Use of SBAR in Admission Reconciliation2004ndash2005
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
175March 2006 Volume 32 Number 3
eyes of the bedside caregiver Staffmembers feel empowered and haveinfluence over decisions that affectwork life using SBAR thus improvingjob satisfaction Currently SBAR tools are being tested in communica-tion handoffs between shifts fortransfers to other departments (forexample radiology operating room)and with patients admitted from theemergency department SBAR pro-motes the six aims of the Institute of Medicine in providing safe effi-cient effective equitable timely andpatient-centered lines of communica-tion21 J
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at discharge improved from a mean of
53 to a mean of 89
Use of SBAR in Discharge Reconciliation2004ndash2005
Kathleen M Haig RN is Director Quality ResourceManagementRisk ManagerPatient Safety Officer andStaci Sutton RN is Emergency Services Manager OSF StJoseph Medical Center Bloomington Illinois JohnWhittington MD is Patient Safety OfficerDirector of Knowledge Management OSF Healthcare SystemPeoria Illinois Please address correspondence to JohnWhittington johnwwhittingtonosfhealthcareorg
1 Joint Commission on Accreditation of Healthcare OrganizationsSentinel Event Statistics-June 30 2005 httpwwwjcahoorgaccred-ited+organizationssentinel+eventsentinel+event+statisticshtm (lastaccessed Jan 24 2006)2 Joint Commission on Accreditation of Healthcare Organizations2006 Critical Access Hospital and Hospital National Patient
Safety Goals httpwwwjcahoorgaccredited+organizationspatient+safety06_npsg06_npsg_cah_haphtm (last accessed Jan 24 2006)3 Wachter RM Shojania KG Internal Bleeding The Truth Behind
Americas Terrifying Epidemic of Medical Mistakes New YorkRugged Land 2004 4 Thomas EJ Sexton JB Helmreich RL Discrepant attitudes aboutteamwork among critical care nurses and physicians Crit Care Med
31956ndash959 Mar 20035 Greenfield LJ Doctors and nurses A troubled partnership Ann
Surg 230279-288 Sep 19996 Leonard M Graham S Bonacum D The human factor The crit-ical importance of effective teamwork and communication in pro-viding safe care Qual Saf Health Care 13 (suppl 1)i85ndashi90 Oct20047 McFerran SC et al Perinatal patient safety project A multicenterapproach to improve performance reliability at Kaiser Permanente JPerinat Neonatal Nurs 1937ndash45 JanndashMar 2005
References
8 Institute for Healthcare Improvement Framework for SpreadhttpwwwihiorgIHITopicsImprovementSpreadingChangesChanges (last accessed Jan 24 2006)9 Helmreich RL Merritt AC Culture at Work in Aviation and
Medicine National Organizational and Professional Influences
Aldershot UK Ashgate 200110 Helmreich RL On error management Lessons from aviation BMJ
320(7237)781ndash785 Mar 2000 11 Kosnik LK The new paradigm of crew resource management justwhat is needed to re-engage the stalled collaborative movement Jt
Comm J Qual Improv 28235ndash241 May 200212 Risser DT et al The potential for improved teamwork to reducemedical errors in the emergency department The MedTeams ResearchConsortium Ann Emerg Med 34373-383 Sep 1994 13 Wiener EL Kanki BG Helmreich RL Cockpit Resource
Management San Diego Harcourt Brace 199314 Gleason KM et al Reconciliation of discrepancies in medicationhistories and admission orders of newly hospitalized patients Am J
Health Syst Pharm 611689ndash1695 Aug 15 2004 15 Pronovost P et al Medication reconciliation tool A practical tool toreduce medication errors during patient transfer from an intensive careunit Journal of Clinical Outcomes Management 1126ndash33 Jan 200416 Rozich JD et al Medication safety One organizations approachto the challenge Journal of Clinical Outcomes Management 827ndash34Oct 2001 17 Whittington J Cohen H OSF healthcares journey in patient safe-ty Qual Manag Health Care 1353-59 JanndashMar 2004 18 Resar RK Rozich JD Classen D Methodology and rationale forthe measurement of harm with trigger tools Qual Saf Health Care 12(suppl 2)ii39ndashii45 Dec 2003 19 Rozich JD Haraden CR Resar RK Adverse drug event triggertool A practical methodology for measuring medication related harmQual Saf Health Care 12194ndash200 Jun 2003 20 Institute for Healthcare Improvement Global Trigger Tool for
Measuring Adverse Events (IHI Tool) httpwwwihiorgIHITopicsPatientSafetySafetyGeneralToolsGlobalTriggerToolforMeasuringAEshtm (last accessed Jan 24 2006)21 Institute of Medicine Crossing the Quality Chasm WashingtonDC National Academy Press 2001
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
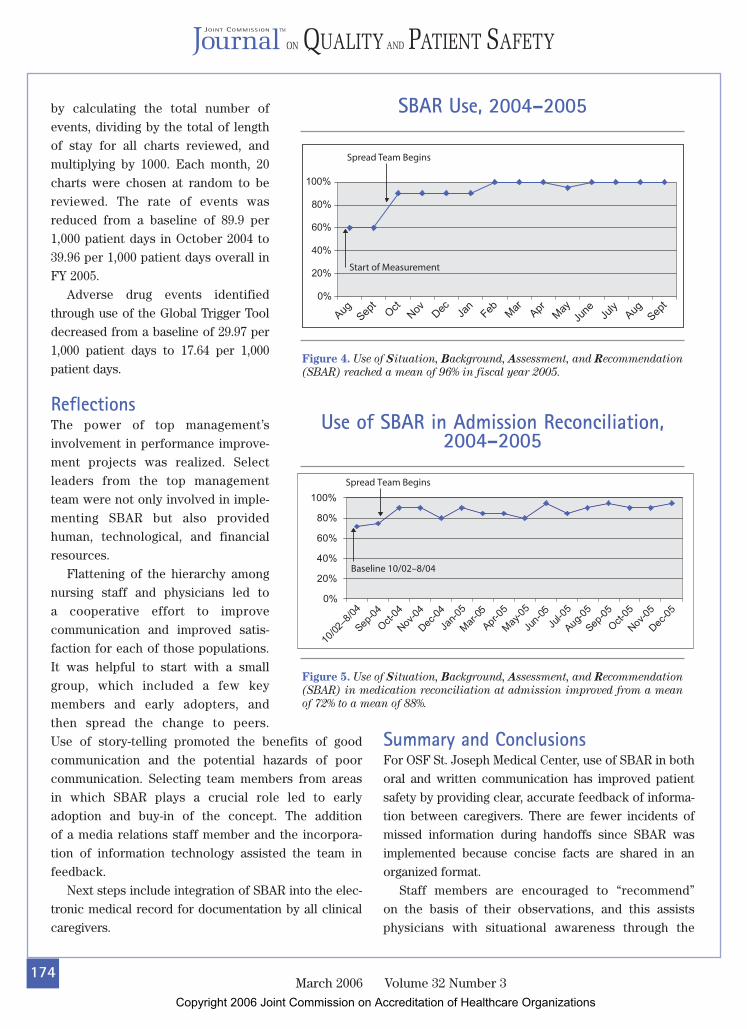
174March 2006 Volume 32 Number 3
by calculating the total number ofevents dividing by the total of lengthof stay for all charts reviewed andmultiplying by 1000 Each month 20charts were chosen at random to bereviewed The rate of events wasreduced from a baseline of 899 per1000 patient days in October 2004 to3996 per 1000 patient days overall inFY 2005
Adverse drug events identifiedthrough use of the Global Trigger Tooldecreased from a baseline of 2997 per1000 patient days to 1764 per 1000patient days
ReflectionsThe power of top managementrsquosinvolvement in performance improve-ment projects was realized Selectleaders from the top managementteam were not only involved in imple-menting SBAR but also providedhuman technological and financialresources
Flattening of the hierarchy amongnursing staff and physicians led to a cooperative effort to improve communication and improved satis-faction for each of those populationsIt was helpful to start with a smallgroup which included a few key members and early adopters and then spread the change to peers Use of story-telling promoted the benefits of goodcommunication and the potential hazards of poor communication Selecting team members from areas in which SBAR plays a crucial role led to early adoption and buy-in of the concept The addition of a media relations staff member and the incorpora-tion of information technology assisted the team infeedback
Next steps include integration of SBAR into the elec-tronic medical record for documentation by all clinicalcaregivers
Summary and ConclusionsFor OSF St Joseph Medical Center use of SBAR in bothoral and written communication has improved patientsafety by providing clear accurate feedback of informa-tion between caregivers There are fewer incidents ofmissed information during handoffs since SBAR wasimplemented because concise facts are shared in anorganized format
Staff members are encouraged to ldquorecommendrdquo on the basis of their observations and this assistsphysicians with situational awareness through the
Figure 4 Use of Situation Background Assessment and Recommendation
(SBAR) reached a mean of 96 in fiscal year 2005
SBAR Use 2004ndash2005
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at admission improved from a mean
of 72 to a mean of 88
Use of SBAR in Admission Reconciliation2004ndash2005
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
175March 2006 Volume 32 Number 3
eyes of the bedside caregiver Staffmembers feel empowered and haveinfluence over decisions that affectwork life using SBAR thus improvingjob satisfaction Currently SBAR tools are being tested in communica-tion handoffs between shifts fortransfers to other departments (forexample radiology operating room)and with patients admitted from theemergency department SBAR pro-motes the six aims of the Institute of Medicine in providing safe effi-cient effective equitable timely andpatient-centered lines of communica-tion21 J
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at discharge improved from a mean of
53 to a mean of 89
Use of SBAR in Discharge Reconciliation2004ndash2005
Kathleen M Haig RN is Director Quality ResourceManagementRisk ManagerPatient Safety Officer andStaci Sutton RN is Emergency Services Manager OSF StJoseph Medical Center Bloomington Illinois JohnWhittington MD is Patient Safety OfficerDirector of Knowledge Management OSF Healthcare SystemPeoria Illinois Please address correspondence to JohnWhittington johnwwhittingtonosfhealthcareorg
1 Joint Commission on Accreditation of Healthcare OrganizationsSentinel Event Statistics-June 30 2005 httpwwwjcahoorgaccred-ited+organizationssentinel+eventsentinel+event+statisticshtm (lastaccessed Jan 24 2006)2 Joint Commission on Accreditation of Healthcare Organizations2006 Critical Access Hospital and Hospital National Patient
Safety Goals httpwwwjcahoorgaccredited+organizationspatient+safety06_npsg06_npsg_cah_haphtm (last accessed Jan 24 2006)3 Wachter RM Shojania KG Internal Bleeding The Truth Behind
Americas Terrifying Epidemic of Medical Mistakes New YorkRugged Land 2004 4 Thomas EJ Sexton JB Helmreich RL Discrepant attitudes aboutteamwork among critical care nurses and physicians Crit Care Med
31956ndash959 Mar 20035 Greenfield LJ Doctors and nurses A troubled partnership Ann
Surg 230279-288 Sep 19996 Leonard M Graham S Bonacum D The human factor The crit-ical importance of effective teamwork and communication in pro-viding safe care Qual Saf Health Care 13 (suppl 1)i85ndashi90 Oct20047 McFerran SC et al Perinatal patient safety project A multicenterapproach to improve performance reliability at Kaiser Permanente JPerinat Neonatal Nurs 1937ndash45 JanndashMar 2005
References
8 Institute for Healthcare Improvement Framework for SpreadhttpwwwihiorgIHITopicsImprovementSpreadingChangesChanges (last accessed Jan 24 2006)9 Helmreich RL Merritt AC Culture at Work in Aviation and
Medicine National Organizational and Professional Influences
Aldershot UK Ashgate 200110 Helmreich RL On error management Lessons from aviation BMJ
320(7237)781ndash785 Mar 2000 11 Kosnik LK The new paradigm of crew resource management justwhat is needed to re-engage the stalled collaborative movement Jt
Comm J Qual Improv 28235ndash241 May 200212 Risser DT et al The potential for improved teamwork to reducemedical errors in the emergency department The MedTeams ResearchConsortium Ann Emerg Med 34373-383 Sep 1994 13 Wiener EL Kanki BG Helmreich RL Cockpit Resource
Management San Diego Harcourt Brace 199314 Gleason KM et al Reconciliation of discrepancies in medicationhistories and admission orders of newly hospitalized patients Am J
Health Syst Pharm 611689ndash1695 Aug 15 2004 15 Pronovost P et al Medication reconciliation tool A practical tool toreduce medication errors during patient transfer from an intensive careunit Journal of Clinical Outcomes Management 1126ndash33 Jan 200416 Rozich JD et al Medication safety One organizations approachto the challenge Journal of Clinical Outcomes Management 827ndash34Oct 2001 17 Whittington J Cohen H OSF healthcares journey in patient safe-ty Qual Manag Health Care 1353-59 JanndashMar 2004 18 Resar RK Rozich JD Classen D Methodology and rationale forthe measurement of harm with trigger tools Qual Saf Health Care 12(suppl 2)ii39ndashii45 Dec 2003 19 Rozich JD Haraden CR Resar RK Adverse drug event triggertool A practical methodology for measuring medication related harmQual Saf Health Care 12194ndash200 Jun 2003 20 Institute for Healthcare Improvement Global Trigger Tool for
Measuring Adverse Events (IHI Tool) httpwwwihiorgIHITopicsPatientSafetySafetyGeneralToolsGlobalTriggerToolforMeasuringAEshtm (last accessed Jan 24 2006)21 Institute of Medicine Crossing the Quality Chasm WashingtonDC National Academy Press 2001
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
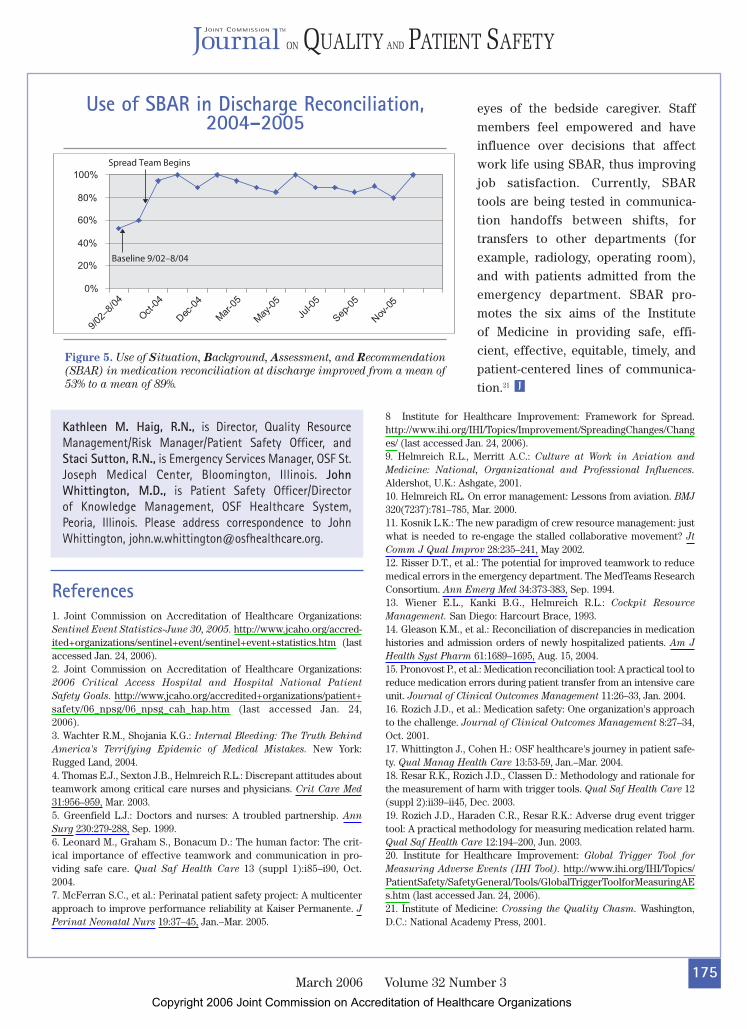
175March 2006 Volume 32 Number 3
eyes of the bedside caregiver Staffmembers feel empowered and haveinfluence over decisions that affectwork life using SBAR thus improvingjob satisfaction Currently SBAR tools are being tested in communica-tion handoffs between shifts fortransfers to other departments (forexample radiology operating room)and with patients admitted from theemergency department SBAR pro-motes the six aims of the Institute of Medicine in providing safe effi-cient effective equitable timely andpatient-centered lines of communica-tion21 J
Figure 5 Use of Situation Background Assessment and Recommendation
(SBAR) in medication reconciliation at discharge improved from a mean of
53 to a mean of 89
Use of SBAR in Discharge Reconciliation2004ndash2005
Kathleen M Haig RN is Director Quality ResourceManagementRisk ManagerPatient Safety Officer andStaci Sutton RN is Emergency Services Manager OSF StJoseph Medical Center Bloomington Illinois JohnWhittington MD is Patient Safety OfficerDirector of Knowledge Management OSF Healthcare SystemPeoria Illinois Please address correspondence to JohnWhittington johnwwhittingtonosfhealthcareorg
1 Joint Commission on Accreditation of Healthcare OrganizationsSentinel Event Statistics-June 30 2005 httpwwwjcahoorgaccred-ited+organizationssentinel+eventsentinel+event+statisticshtm (lastaccessed Jan 24 2006)2 Joint Commission on Accreditation of Healthcare Organizations2006 Critical Access Hospital and Hospital National Patient
Safety Goals httpwwwjcahoorgaccredited+organizationspatient+safety06_npsg06_npsg_cah_haphtm (last accessed Jan 24 2006)3 Wachter RM Shojania KG Internal Bleeding The Truth Behind
Americas Terrifying Epidemic of Medical Mistakes New YorkRugged Land 2004 4 Thomas EJ Sexton JB Helmreich RL Discrepant attitudes aboutteamwork among critical care nurses and physicians Crit Care Med
31956ndash959 Mar 20035 Greenfield LJ Doctors and nurses A troubled partnership Ann
Surg 230279-288 Sep 19996 Leonard M Graham S Bonacum D The human factor The crit-ical importance of effective teamwork and communication in pro-viding safe care Qual Saf Health Care 13 (suppl 1)i85ndashi90 Oct20047 McFerran SC et al Perinatal patient safety project A multicenterapproach to improve performance reliability at Kaiser Permanente JPerinat Neonatal Nurs 1937ndash45 JanndashMar 2005
References
8 Institute for Healthcare Improvement Framework for SpreadhttpwwwihiorgIHITopicsImprovementSpreadingChangesChanges (last accessed Jan 24 2006)9 Helmreich RL Merritt AC Culture at Work in Aviation and
Medicine National Organizational and Professional Influences
Aldershot UK Ashgate 200110 Helmreich RL On error management Lessons from aviation BMJ
320(7237)781ndash785 Mar 2000 11 Kosnik LK The new paradigm of crew resource management justwhat is needed to re-engage the stalled collaborative movement Jt
Comm J Qual Improv 28235ndash241 May 200212 Risser DT et al The potential for improved teamwork to reducemedical errors in the emergency department The MedTeams ResearchConsortium Ann Emerg Med 34373-383 Sep 1994 13 Wiener EL Kanki BG Helmreich RL Cockpit Resource
Management San Diego Harcourt Brace 199314 Gleason KM et al Reconciliation of discrepancies in medicationhistories and admission orders of newly hospitalized patients Am J
Health Syst Pharm 611689ndash1695 Aug 15 2004 15 Pronovost P et al Medication reconciliation tool A practical tool toreduce medication errors during patient transfer from an intensive careunit Journal of Clinical Outcomes Management 1126ndash33 Jan 200416 Rozich JD et al Medication safety One organizations approachto the challenge Journal of Clinical Outcomes Management 827ndash34Oct 2001 17 Whittington J Cohen H OSF healthcares journey in patient safe-ty Qual Manag Health Care 1353-59 JanndashMar 2004 18 Resar RK Rozich JD Classen D Methodology and rationale forthe measurement of harm with trigger tools Qual Saf Health Care 12(suppl 2)ii39ndashii45 Dec 2003 19 Rozich JD Haraden CR Resar RK Adverse drug event triggertool A practical methodology for measuring medication related harmQual Saf Health Care 12194ndash200 Jun 2003 20 Institute for Healthcare Improvement Global Trigger Tool for
Measuring Adverse Events (IHI Tool) httpwwwihiorgIHITopicsPatientSafetySafetyGeneralToolsGlobalTriggerToolforMeasuringAEshtm (last accessed Jan 24 2006)21 Institute of Medicine Crossing the Quality Chasm WashingtonDC National Academy Press 2001
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
Related Documents











