h National Health and Hospitals Reform Commission Submission response: Governance, accountability and coordination – the keys to person-centred health care 30 May 2008

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

h
National Health and HospitalsReform Commission
Submission response:
Governance, accountability
and coordination – the keys
to person-centred health care
30 May 2008


National Health and Hospitals Reform Commission PricewaterhouseCoopers | iii
PricewaterhouseCoopersABN 52 780 433 757Darling Park Tower 2
201 Sussex StreetGPO BOX 2650SYDNEY NSW 1171
DX 77 SydneyAustraliawww.pwc.com/au
Telephone +61 2 8266 0000Facsimile +61 2 8266 9999
National Health and Hospitals Reform CommissionPO Box 685Woden ACT 2606
30 May 2008
Dear Commission members
About this submission
Health care is a critical and challenging issue for all Australians. We are honoured to be giventhe opportunity to offer our views as a contribution to the debate.
In our submission, we seek to provide insights into how to achieve person-centred, evidence-based modelsof coordinated care with the aim of improving health outcomes for all people.
We propose a concept which has at its core strong governance at all levels of the system.In preparing our submission, we have drawn on our knowledge and experience of the Australian andinternational health systems, and our understanding of their complexities. To contribute to the transitionfrom knowledge to action, we highlight practical examples of innovation which can make a difference in thereal world, as well providing a structure for making it happen.
Appendix A sets out where we have addressed the Commission’s Terms of Referencein this document.
Yours faithfully
John WalshPartner – Health Actuarial andAdvisory Practice
Mark JohnsonSenior Partner – ChiefExecutive Officer (CEO)

National Health and Hospitals Reform Commission PricewaterhouseCoopers | ii
Authorship
This submission was produced by a team of consultants in the Health Actuarial and Advisory practiceof PricewaterhouseCoopers Australia. The following individuals compose the core team: John Walsh,Anne-Marie Feyer, Caitlin Francis, Kirsten Armstrong, Lorraine Acheson, Rebecca Jessop, andMonica Iglesias.
We would also like to acknowledge the contributions made to this submission by the following individuals:Bianca Jordaan, Carrie Schulman, Craig Gear, Jan Muysken, Kim Smith, Laura Applebee, Mary Mitchelhill,Nathan Schlesinger, Noreen Dowd, Richard Baldwin, Richard Stewart, Roger McComiskie,Susan McKerihan, and Tony Peake.

Executive summary
National Health and Hospitals Reform Commission PricewaterhouseCoopers | iii
Executive summary
Achieving person-centred and evidence-based models of care operating seamlessly across the full carecontinuum, with the aim of improving health outcomes for individuals, is an ambition for most developedcountries. The extent to which this has been achieved, in Australia and elsewhere, has been highlyvariable. As a consequence of the number of complex interactions involved, most health systems haveevolved somewhat organically, with changes, even quite dramatic ones, happening in relative isolation.
However, Australia is now poised to make real change to deliver on the ambition. The question is notwhether this should happen, but how.
Governance: the answer to person-centred health care
This submission takes up the proposition that strong governance is key if we want accountable andperson-centred health care. Specifically, structured and multi-layered governance is the essentialprerequisite to achieving a coordinated and holistic system, in which all elements are aligned, andwhich thus maximises patient value (ie cost-effective, optimal quality care).
To implement such a vision will require: Figure 1: Governance cycle
funding governance and clarity to ensurethere is an agreed position on the fundingflows within the system, and how thesefunding flows affect health careexpenditure and delivery
strategic oversight to secure the right,needs-based, high quality, value formoney and sustainable services acrossthe care continuum
market oversight to ensure fair andappropriate market management with thegoals of improved quality and value formoney
monitoring and comparative oversight toensure effective performancemanagement of the system
robust and evidence-based data whichunderpins all of the above.
1
2
3
Data
1
2
3
1
2
3
DataSource: PricewaterhouseCoopers, May 2008 © copyright
In order to achieve this governance imperative, and for reasons highlighted throughout our submission,we recommend the establishment of an Australian Health Commission with a charter to facilitate:
central planning and oversight, with cascading responsibility and accountability for deliveryand outcomes
service planning and delivery across the continuum of care for individual Australians

Executive summary
iv | PricewaterhouseCoopers National Health and Hospitals Reform Commission
The diagram below, while lacking in fine detail at this stage, presents an idea of how the future healthsystem may be structured to achieve the level of accountability and coordination – facilitated by stronggovernance – that is required.
Figure 2: System management structure
The Australian Department ofHealth and Ageing (DoHA) setsthe overall system policydirection to support States andTerritories and the fundholder todevelop and improve health carepurchasing and delivery.
DoHA
State andTerritories
The proposed Australian HealthCommission will be the financialand quality regulator for thepublic Australian health system,acting as a link between theCommonwealth and States andTerritories.
State and Territory health departmentswill be the system managers at ajurisdictional level and must:• ensure that all patients have access
to sustainable, high quality primary,secondary and specialist care
• ensure there is equity of access forthe patient
• ensure that patients’ interests areprotected and promoted
• support and performance managefundholders.
eg AreaHealthServices
eg PrivateHealthFunds
Fundholders are responsible forunderstanding the needs,experiences and expectationsof all their population, and willdevelop and implement strategies(based on intelligence and data) toensure that appropriate servicesand pathways of care areavailable to their populations.
Fundholders
AustralianHealth
Commission
The Australian Department ofHealth and Ageing (DoHA) setsthe overall system policydirection to support States andTerritories and the fundholder todevelop and improve health carepurchasing and delivery.
DoHA
State andTerritories
The proposed Australian HealthCommission will be the financialand quality regulator for thepublic Australian health system,acting as a link between theCommonwealth and States andTerritories.
State and Territory health departmentswill be the system managers at ajurisdictional level and must:• ensure that all patients have access
to sustainable, high quality primary,secondary and specialist care
• ensure there is equity of access forthe patient
• ensure that patients’ interests areprotected and promoted
• support and performance managefundholders.
eg AreaHealthServices
eg PrivateHealthFunds
Fundholders are responsible forunderstanding the needs,experiences and expectationsof all their population, and willdevelop and implement strategies(based on intelligence and data) toensure that appropriate servicesand pathways of care areavailable to their populations.
Fundholders
AustralianHealth
Commission
Source: PricewaterhouseCoopers, May 2008 © copyright
Key trends in Australia: the imperative
On many health indicators, such as life expectancy, Australia performs well when compared with otherOrganisation for Economic Co-operation and Development (OECD) countries. However, these key healthindicators are lag indicators: they do not say how we will meet the health needs of today and, critically, oftomorrow. Specifically, emerging trends in population health, health expenditure, system evolution andquality and safety provide more timely indicators of our system’s readiness – or more correctly, lack ofreadiness – for change. In particular:
increasing demand as a result of the ageing of the baby-boom generation, rising prevalence ofchronic disease and changing community expectations
rising costs as a consequence of these demographic issues and the growing expenditure onspecialised medicine and technology aimed at (for the most part) prolonging life
the inability of the present system – given its complexity and fragmentation – to appropriately fundand implement the shift from an acute and episodic approach to health care to one which encouragesboth prevention and coordinated management
limited capacity to deliver person-centred health care as a consequence of substantial access, data,workforce and infrastructure issues
uneven quality as a result of fragmented quality and safety governance mechanisms, poor accessand the episodic approach to care
embedded inequity in the system as illustrated by the difference in adult life expectancy betweenIndigenous and non-Indigenous people in Australia, which is estimated to be approximately 17 years.
Ultimately, these issues are reflected in an inability of our hospital system to meet demand for inpatientservices, and sub-optimal system and patient outcomes.

Executive summary
National Health and Hospitals Reform Commission PricewaterhouseCoopers | v
Priorities for action
If the Australian health system is to achieve its ambition, change – both incremental and revolutionary – isrequired on a number of fronts. To help prioritise the actions that will need to be taken, we provide views onfuture directions in the following key areas of governance. Our views are based on evidence andexperience both from Australia and abroad.
Funding governance: aligning funding allocation models with incentives
Consider introducing an integrated funding approach for specific sub-populations/membership that isbased on a robust resource-allocation methodology across the continuum of care, and includes boththe public and private sectors.
Strategic oversight: understanding health need to align service delivery with quality
Introduce a systematic and comprehensive approach to needs assessment to ensure the right healthcare is delivered at the right time and place for all Australians.
Use the lessons learnt from major chronic disease prevention and management studies to inform anationwide application of proven approaches
Encourage strong, coordinated governance and multi-stakeholder cooperation to introduce bestpractice models of care and improve safety and quality through improved collection, reporting andsharing of information and successes
Market oversight: addressing key capacity issues – access, workforce and infrastructure
Constantly monitor access and efficiency at both primary and secondary levels – and address keypressure points in the system.
Introduce evidence-based approaches to workforce management and planning (such as role andincentive redesign, original approaches to training) to help ensure the ongoing viability of the newapproach.
Implement infrastructure developments based on innovative organisation design, incentive structuresand team-working to maximise the productivity and efficiency of hospitals and other facilities
Monitoring and comparative oversight: fit-for-purpose information management, data andbenchmarking
Match the performance management of the system to performance expectations by introducing aperson-centred approach to information, including personal health records and a central longitudinaldatabase.
Produce and use data in a timely manner to achieve a system of monitoring and benchmarking whichspans the continuum of care, to support other objectives of access, efficiency, and outcomes
Find a balance between privacy management and the imperative of health planning whichencourages research and information-based innovation.
Conclusion
In presenting our submission, we are fully aware of and acknowledge the magnitude of not only the issuesfacing the Australian health system, but also the changes required. This is a challenging and critical task forAustralia and we do not take the issue lightly. We have therefore attempted to tackle these matters from themindset of an evidence-based approach within a practical framework.

Governance: the answer to person-centred health care
National Health and Hospitals Reform Commissionvi PricewaterhouseCoopers
Contents
Authorship ii
Executive summary iii
1 Governance: the answer to person-centred health care 1
1.1 The role of governance 3
1.2 What the system might look like 10
2 Key trends in Australia: the imperative for change 13
2.1 Population health trends 15
2.2 Rising costs and expenditure: emergingtrends 21
2.3 Trends in system evolution 24
2.4 Limited capacity to deliver person-centredhealth care 34
2.5 Threats to quality and safety 41
3 Priorities for action 47
3.2 Funding governance: Aligning fundingallocation models with incentives 50
3.3 Strategic oversight: understanding healthneed to align service delivery with quality 56
3.4 Market oversight: addressing key capacityissues – access, workforce andinfrastructure 65
3.5 Monitoring and comparative oversight: fit-for-purpose information management, dataand benchmarking 75
Appendix A Addressing the terms of reference 80
Appendix B Checklist for action 81
B.1 Plan 82
B.2 Execute 85
B.3 Manage 87
Appendix C Acronyms 89
Appendix D References 90
PwC contacts 95

National Health and Hospitals Reform Commission PricewaterhouseCoopers | 1
1Governance: the answer to person-
centred health care

1 Governance: the answer to person-centred health care
2 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Key points of this chapter
An essential pre-requisite to an accountable and coordinated health system is that it isunderpinned by a clear governance structure which aligns funding, strategy and delivery
Our vision of strong governance includes funding, strategic, market and monitoringoversight.
To implement such a vision effectively will require the development of and adherence toclear functional roles for the key participants in the health system.
This will include setting up an Australian Health Commission to provide oversight to ensurethat services are aligned to needs across the continuum of care for all Australians.
Introduction to this chapter
Achieving person-centred, evidence-based models of coordinated care across the full continuumof care, with the aim of improving health outcomes for all people, is an ambition of most developedcountries. However, the extent to which seamless health systems have been achieved, inAustralia and elsewhere, is highly variable given the complex interactions involved. Most systemshave evolved organically, with changes, even quite dramatic ones, happening in relative isolation.Such evolution is necessarily plagued by lack of alignment between system parts. Nevertheless,Australia is now poised to make real change to deliver this ambition. The question is not whetherthis should happen, but how.
In this chapter we discuss what we believe are the key building blocks to implementing such achange and what this vision could look like in functional terms. In subsequent chapters weconsider in more detail why the Australian health system needs to change (Chapter 2) and howthis could be achieved (Chapter 3).

1 Governance: the answer to person-centred health care
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 3
1.1 The role of governance
An essential pre-requisite to an accountable and coordinated health system is that it isunderpinned by a multi-layered governance structure which aims to achieve alignmentbetween all components of funding, strategy and delivery.
Strong governance in the health system helps to ensure:
the need for health care and prevention services is determined by robust and evidence-based data
strategies for and the implementation of service delivery are directly related to the need thathas been identified
performance is monitored and managed (underpinned by sound data) to achieve optimalhealth and economic outcomes.
To implement such a vision requires:
funding governance to ensure there is an agreed position on and understanding of thefunding flows within the system and how these funding flows affect health care expenditureand delivery
strategic oversight to secure the right, needs-based, high quality, value for money andsustainable services across the continuum of care
1
market oversight to ensure fair and appropriate market management with the goals ofimproved quality and value for money
monitoring and comparative oversight to ensure effective performance management of thesystem
robust and evidence-based data which underpins all of the above.
We have summarised these functions and associated activities in the following ‘Governance cycle’(Figure 3), which has been developed by drawing from Australian and international experience,including expert contributions, academic reviews and experience from health and other sectors. Ithas been designed to describe the requirements for delivering the desired outputs and outcomesof appropriate care and value for money – ie patient value.

1 Governance: the answer to person-centred health care
4 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Figure 3: Governance cycle
1
2
3
Data
1
2
3
1
2
3
DataSource: PricewaterhouseCoopers, May 2008 © copyright
Key features of our recommended approach are described below.
Funding governance
To ensure there is an agreed position on and understanding of the funding flows within thesystem and how these affect health care expenditure and delivery
A necessary first step towards achieving a sustainable health system is an agreed position andplan for responding to ongoing cost escalation, while recognising the public perception that systemresponse and access blocks are worse than ever. In other words: ‘How can the system’s ‘image’be improved without spending even more money in a cost-spiral?’
In a nation like Australia, where the health funding structure is multi-layered, such a positionrequires a level of agreement between the various tiers of government (Commonwealth, State,Territories, and Area Health Services) and major private funders (health insurers and injuryinsurers). This has been unobtainable to date.
Consensus is critical
Such consensus regarding funding governance is required not only at a government level but alsoat a program and/or regional level. One of the major findings of the Second Round of Coordinated

1 Governance: the answer to person-centred health care
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 5
Care Trials (CCT2)2
was the importance of governance and management across levels of bothfunder and service provider levels, the lack of which contributed to many of the difficulties of thetrials. At the same time, two of the more successful trials (TeamCare II and the IndigenousSunrise trial) demonstrated the power of what could be achieved within the Australian system in acoordinated health system with strong and cohesive funding governance.
Alternative: a single fundholder
An alternative to consensus may be the integration of funding. In this approach a single entity orfundholder is able to purchase appropriate services across the care continuum on behalf of itsallocated ‘memberships’ or constituencies. There are many examples of such an approach, andthese are discussed in more detail in the Funding section of Chapter 3. In the context ofgovernance, the appeal of this approach is in allowing meaningful control and planning of a ‘mini-health system’. Ideally, this planning would be congruent with a national plan of action. Forexample, an Australian Health Commission is a possibility, as suggested in a recent report to theVictorian Government.
3
One of the first roles of such a body might be the realistic projection of trends, needs and costs inthe Australian health system and a plan for funding them, as set out in the Wanless
4Report in the
UK.
Funding structure options
While the nature of the health system should not be determined by its funding structure, thefunding structure can either support and enhance its broader objectives or actually inhibit andnarrow them.
To support the drive for greater person-centred and coordinated care, in Chapter 3 we suggestoptions for changes in the funding structure in Australia.
However, in the first instance we need to consider what steps are required to bring about a moreperson-centred approach and in particular what other governance structures are needed tomanage the process. The pace and effectiveness of such changes will be influenced in part (butnot completely) by the funding structure in place.
Strategic oversight
To secure the right, needs-based, high quality, value for money and sustainable servicesacross the continuum of care (ie patient value)1
In keeping with the governance cycle presented above, a strategic oversight of the health systemwould prescribe strategic options that are supported by the planning components of (a) needsassessment mapped to current service delivery, (b) development of service models agreed asappropriate for achieving best outcomes, (c) priority setting, and (d) development of a riskmanagement framework.
a. Needs assessment
Health service development in Australia (both funding and service models) has followed atrajectory that responds to incremental demand; that is, services change slowly and are heavilybased on ‘what happened last year’. In turn, these services are heavily influenced by the capabilityof the provider to deliver.
We believe that the available information should be used to assess and project need across thecare continuum at a level that credibly identifies and describes major segments of the population.
1 Governance: the answer to person-centred health care
6 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
In this context, need should be considered in terms of volume of service, which translates tofunding, and also in terms of the service mix most appropriate to achieve best outcomes based onevidence.
Such an assessment will require a major rethink of the format and content of data held within thehealth system, and how such data is used and accessed. Where required data is not available itwill need to be defined and captured.
Finally, the extent to which the identified need can and will be matched by demand and supply(both formal and informal) should be the subject of an informed debate at the highest politicallevel.
b. Service delivery: determining priorities and assessing strategic options
The development of service models and the very concept of a ‘health service’ should span acrossthe continuum of care to encompass health promotion and prevention, the range of treatmentsavailable and disease maintenance, and palliative care. Planning, coordination and delivery ofservices should be centred on each individual Australian (ie not only each ‘patient’) and theirhealth needs.
As with the above discussion on funding governance, this implies the need for a servicecoordination function on a sub-population basis. This would be a person or organisation (ie a‘fundholder’) who has the trust of the individuals in the group, as successfully trialled in CCT2.
2
In terms of service coordination and delivery with respect to funding and resource allocation,relevant sub-populations should be considered as units. These may be geographical or based onother attributes such as membership of a Registered Health Organisation (health insurer).Resources should be allocated or directed to such units according to robust allocation protocolswhich are risk adjusted and further modified to allow for co-contributions and health fundmembership.
Actual service provision should be evidence-based and supplied by approved providers ofappropriate health care specialties and organised by the chosen service coordinator. Fundholderswould manage the providers’ service delivery through contracts to encourage effectiveperformance management.
Incentives should exist for safe and efficient service delivery, and penalties for over-servicing orinefficiency. But at the same time there needs to be opportunity for innovative business modelswhich will encourage the growth and diversification of the workforce and infrastructure. The role ofincentives is discussed in more detail in Chapter 3
c. Risk management
A comprehensive risk analysis and mitigation strategy is needed for the key risks of quality andsafety, political and social, and financial. The strategy would identify dimensions such as:
risk of service being unavailable (ie under-supply or inefficient throughput)
risk of adverse events
risk of funds being expended (eg through inefficient or inappropriate use, unplannedtechnological change etc).
Both the funding and service delivery models and their respective governance structures need torecognise these risks. They need to be built around minimising risk through elements such as

1 Governance: the answer to person-centred health care
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 7
quality assurance, pay-for-performance, efficient and effective workforce, infrastructuredeployment, and equalisation strategies for financial over-runs.
This strategic approach to health care planning and delivery implies a strong monitoring andfeedback function which should capitalise on enhanced data availability and usage.
Market oversight
To ensure fair and appropriate market management with the goals of improved quality andvalue for money
Health services can only be delivered if the appropriate workforce and infrastructure (bricks andmortar, equipment, etc) – ie the ‘market’ – are in place. Planning, engagement and appropriatereward are the key components of ensuring the viability of this market.
Provider and infrastructure development
The current availability and appropriateness of the workforce, infrastructure, and alternativesources of supply (including more diversified private participation and informal/volunteer capacity)to meet the projected needs of the population should be the subject of a major investigation.
Where shortages are identified, the price elasticity and other impediments to workforce andinfrastructure growth (eg training, competing labour opportunities, private investmentinfrastructure) should be modelled to estimate the impact on demand of establishing the requiredsupply. In particular, service availability and delivery should continue to be based on evidence andneed rather than on demand-induced supply.
At the same time, however, real unmet need and inequity – both volume and service type – mustbe identified and addressed. Where workforce shortages cannot be remedied, alternative modelsof care and innovative technology must be used.
The expected impact on required funding for market development should then be fed back into thefunding discussions.
The use of contracts
Methods of implementation need to be considered as part of this impact assessment andassociated strategy. Options are likely to cover a wide range of components and methodologies,including:
performance-based contracts, with ‘performance’ defined across a range of outcomedimensions, including health outcomes
engagements in infrastructure maintenance and development through budget commitmentsand private-public-partnership schemes with performance-based metrics
development and mentoring of the leaders in our health system to equip them for changeand innovation
engagement in a feasible workforce strategy which recognises and incorporatesdemographic changes, labour market pressures and economics across the healthworkforce.

1 Governance: the answer to person-centred health care
8 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Monitoring and comparative oversight
To ensure effective performance management of the system
A person-centred system across the continuum of health care also requires a person-centredapproach to monitoring and oversight. However, currently, the Australian system can currently becharacterised as the aggregate of:
a small number of discrete public hospital systems with largely independent monitoring andoversight
episode reporting and surveillance on medical and pharmaceutical use and providers,through Medicare Australia
self-monitoring and governance, largely driven by prudential considerations, by privatehospital providers and health insurers
very little coordinated monitoring of community and alternative health care
centralised data collection and aggregate reporting, to the extent possible given data qualityissues, by the AIHW.
In a recent report for the Victorian Department of Human Services5
the following outcomedimensions were identified as critical to appropriate performance management oversight:
clinically appropriate
operational excellence
patient experience
sustainability.
The report recommended a hierarchical governance structure to achieve these performancemeasure outcomes, characterised by (1) a central governing body with ultimate ownership andstrategic oversight, (2) coordinating agencies, and (3) operational health services. This structure isreflected in the model that we present in Section 1.2.
Robust and evidence-based data
Data and information must underpin and drive the entire governance structure
Achieving the above governance goals will require a comprehensive and effective system of datacollection and storage, information management and reporting, and benchmarking to measure forefficiency and effectiveness of actions and outcomes. This will call for:
personal health records, developed and coded with a unique identifier and fed into a centraldatabase (secured and protected by digital certification and encryption), which is linked orlinkable to other recognised databases across the continuum of care (prevention andscreening, primary care, secondary care, emergency care, tertiary care, ambulatory care,rehabilitation and outcomes, community care, residential aged care, mortality)
information that is captured and made available across diagnoses, services and outcomes
information that is made available and reported at an aggregate level using performanceindicators and benchmarks across the continuum of care
personal information which is owned by each individual and shared as consideredappropriate by that person with, for example, treating service providers

1 Governance: the answer to person-centred health care
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 9
database(s) that are made available in agreed and hierarchical formats to accreditedresearchers and bodies/representatives of approved institutions (including governmentdepartments)
privacy concerns surrounding these developments being carefully considered and balancedagainst the potential benefits
health data that is held and managed by an independent authority with an independentgovernance structure and charter for operation; eg an Australian Health Commission.

1 Governance: the answer to person-centred health care
10 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
1.2 What the system might look like
To implement this vision of strong governance requires the development of andadherence to clear functional roles for key participants in the health system
The above discussion, and the body of our submission, envisage quite a different structure for ourhealth system from that which currently exists. In particular, we will seek to establish the need fora governance body (such as an ‘Australian Health Commission’) independent of both theCommonwealth and States/Territories, but acting as a link between the two, and with two keythemes in mind:
central planning and oversight, with cascading responsibility and accountability for deliveryand outcomes
service planning and delivery across the continuum of care for individual Australians.
The following diagram (Figure 4), while lacking in fine detail at this stage, presents an idea of howthe future health system could be structured to achieve the level of accountability and coordination– facilitated by strong governance – that is required.
Figure 4: System management structure
The Australian Department ofHealth and Ageing (DoHA) setsthe overall system policydirection to support States andTerritories and the fundholder todevelop and improve health carepurchasing and delivery.
DoHA
State andTerritories
The proposed Australian HealthCommission will be the financialand quality regulator for thepublic Australian health system,acting as a link between theCommonwealth and States andTerritories.
State and Territory health departmentswill be the system managers at ajurisdictional level and must:• ensure that all patients have access
to sustainable, high quality primary,secondary and specialist care
• ensure there is equity of access forthe patient
• ensure that patients’ interests areprotected and promoted
• support and performance managefundholders.
eg AreaHealthServices
eg PrivateHealthFunds
Fundholders are responsible forunderstanding the needs,experiences and expectationsof all their population, and willdevelop and implement strategies(based on intelligence and data) toensure that appropriate servicesand pathways of care areavailable to their populations.
Fundholders
AustralianHealth
Commission
The Australian Department ofHealth and Ageing (DoHA) setsthe overall system policydirection to support States andTerritories and the fundholder todevelop and improve health carepurchasing and delivery.
DoHA
State andTerritories
The proposed Australian HealthCommission will be the financialand quality regulator for thepublic Australian health system,acting as a link between theCommonwealth and States andTerritories.
State and Territory health departmentswill be the system managers at ajurisdictional level and must:• ensure that all patients have access
to sustainable, high quality primary,secondary and specialist care
• ensure there is equity of access forthe patient
• ensure that patients’ interests areprotected and promoted
• support and performance managefundholders.
eg AreaHealthServices
eg PrivateHealthFunds
Fundholders are responsible forunderstanding the needs,experiences and expectationsof all their population, and willdevelop and implement strategies(based on intelligence and data) toensure that appropriate servicesand pathways of care areavailable to their populations.
Fundholders
AustralianHealth
Commission
Source: PricewaterhouseCoopers, May 2008 © copyright
Sitting below these high level roles are specific functions, which are set out in Table 1.

1 Governance: the answer to person-centred health care
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 11
Table 1: Functional roles
Functions DoHA Australian Health Commission States/TerritoriesFundholders: Area HealthServices and private health funds
Funding governance – To ensure there is an agreed position on and understanding of the funding flows within the system and how these affect health care expenditure and delivery
Establish a frameworkwhich aligns funding andincentive structures tomeet need and provideevidence-based person-centred care
Determine national policyfor the management ofhealth system
Provide clear budgetaryframework
Develop relationships withstakeholders and providedata to inform theframework
Project future health needs and costs anddevelop appropriate financing framework(alignment between funding/incentives/need)
Provide overall financial and quality regulationfor health system including: ACSQHC, MSACand PBAC
Provide clear budgetary framework forjurisdictional activity
Develop relationships with key stakeholdersand provide data to inform the framework
Develop relationships with keystakeholders and provide data toinform the framework
Strategic oversight – To secure the right, needs-based, high quality, value for money and sustainable services across the continuum of care (ie patient value)1
Assess need andunderstand currentservices
Describe gaps anddefine services
Decide priorities andassess risks
Decide strategic priorities
Develop principles ofnational ethical framework
Develop funding allocation method based onneed
Set principles and rules on competition andsupply structure
Set pricing guidelines
Set and lead regional strategic direction andtranslate policy into action
Strategic regional oversight to help definelocal health economy needs and supportdesirable changes
Ensure partnershipdevelopment/stakeholder engagement
Assess regional supply structure andoversee change and transformation
Asses local health economy needand prioritise
Undertake stakeholderengagement
Undertake investment/divestment in services
Determine supply structure
Market oversight – To ensure fair and appropriate market management with the goals of improved quality and value for money
Implement contracts(incl. entry)
Develop providers
Develop principles ofmarket management andprovider development
Design incentives to encourage appropriateparticipation
Develop national contract for services
Appoint national arbiter on competition
Appoint regional arbiter on competition,reconfiguration and contract issues
Establish and implementprocurement strategy includingfair and transparent procurement,provider challenge and ongoingmarket assessment/making
Monitoring and comparative oversight – To ensure effective performance management of the system
Manage performance(ongoing)
Set principles and rules forintervention and failuremanagement
Provide national oversight for quality, safety,value for money and sustainability
Develop information infrastructurerequirements
Develop nationwide KPIs and benchmarkingsystem
Monitor national performance based onagreed benchmarks and KPIs
Provide regional oversight for quality,safety, value for money and sustainability
Oversee funder development
Implement region-wide KPIs
Conduct regional benchmarking
Provide regional intervention and failuremanagement
Establish contracts with providers
Monitor KPIs (incl national dataset)
Ensure continuity of service
Provide local intervention andfailure management

1 Governance: the answer to person-centred health care
12 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Summary
In this chapter we have set out our vision of a governance structure that would beready to meet the numerous challenges facing the Australian health system, includingincreasing demand, rising costs, uneven quality and misaligned incentives. If ignored,these challenges will overwhelm the health system, creating a massive financialburden and devastating health problems for the many individuals concerned.
6
Next we consider these issues in more detail and how they are threatening thesustainability of the current system.

National Health and Hospitals Reform Commission PricewaterhouseCoopers | 13
2Key trends in Australia: the imperative
for change

2 Key trends in Australia: the imperative for change
14 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Key points of this chapter
Emerging trends in population health, health expenditure, system evolution and quality and safetyprovide timely indicators of our system’s readiness – or more correctly, lack of readiness – forchange. Those trends are:
increasing demand as a result of the ageing of the baby-boom generation, rising prevalenceof chronic disease and changing community expectations
rising costs as a consequence of those demographic issues and the growing expenditure onspecialised medicine and technology aimed (for the most part) at prolonging life
the inability of the present system – given its complexity and fragmentation – toappropriately fund and implement the shift from an acute and episodic approach to healthcare to one which encourages both prevention and coordinated management
limited capacity to deliver person-centred health care as a consequence of substantialaccess, data, workforce and infrastructure issues
uneven quality as a result of fragmented quality and safety governance mechanisms, pooraccess and an episodic approach to care
embedded inequity in the system, as illustrated by the difference in adult life expectancybetween Indigenous and non-Indigenous people in Australia, which is estimated to beapproximately 17 years.
Introduction to this chapter
On many health indicators, Australia performs well when compared with other OECD countries.Australia has, for example, one of the highest life expectancies in the world
7. However, the
existing record of health gains in Australia reflects how well we have met past population healthneeds, not how we will meet the population health needs of today and, critically, of tomorrow.
The inherent lag in the majority of population health indicators means that a review of other data isessential when assessing the system’s fitness for purpose. In this chapter we have thereforeconsidered the following key trends and issues for Australia:
1 Population health trends
2 Rising costs and expenditure: emerging trends
3 Trends in system evolution
4 Limited capacity to deliver person-centred health care
5 Threats to quality and safety

2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 15
2.1 Population health trends
The ageing of the baby-boom generation and the rising prevalence of chronic disease areputting great pressure on the health system. Also, the long embedded inequity in healthcare for Indigenous Australians has had a huge negative impact on their health.
Ageing
Australia’s population is ageing due to lower fertility rates and longer life expectancy. Internationalcomparisons place Australia sixth highest in life expectancy at birth, only 2 years lower thanJapan, the country with the highest life expectancy. Newborn Australians can expect to live longerthan children in Spain, France, New Zealand and Germany. Since the mid 1970s our fertility ratehas declined, reaching a low of 1.73 babies per woman in 2001.
8Despite recent increases (1.81
babies per woman in 2006), it remains well under the replacement level of 2.1 births per woman,and contributes to the overall ageing of Australia’s population.
9
In 2006, approximately 2.7 million Australians were aged 65 years and over, and 333,000Australians were aged 85 years and over. This represents a doubling of the number of peopleaged over 85 in the past 20 years, growth which is projected to continue to 4.2% of the totalpopulation over the next 30 years, or 1.1 million in 2036.
10
Long life is a sign of good health, and so the ageing of Australia’s population is an indicator ofsignificant health gain. However, along with this positive trend, ageing will also affect:
the length of time people live with disability and chronic disease, and the consequentimpacts on designing sustainable policies for long-term care and developing age-appropriate services and settings
11
health care expenditure not only in terms of the anticipated high rate of growth, but also inrelation to the shift in health resources from the young and working age to older people
12
Australia’s overall dependency ratio (or the ratio of the economically dependent part of thepopulation to the economically productive part), which will increase over time
12
the rate of injury amongst the elderly, eg motor vehicle accidents and falls13
.
The changing health landscape: the rise in chronic disease
Health systems must be sufficiently responsive to deal with changing health trends. One of the keyhealth trends facing Australia is the growth in chronic conditions, which, when combined with anageing population, is having a significant impact on the cost of health care.
14
Chronic health conditions requiring ongoing, long-term care are increasingly common and areexpected to account for about 80% of the overall disease burden in Australia by 2020.
15In
contrast, just 7% of the burden of disease and injury in Australia was attributed to injuries in 2003,with suicide and self-inflicted injuries, road traffic accidents and falls accounting for the bulk of thisburden.
16
Over the past two decades chronic disease has grown to a level that has surpassed infectiousdisease and injuries.
17This rise in the prevalence of chronic conditions is relatively recent and can
be attributed to:
improvements in the management of previously acute conditions
demographic changes
2 Key trends in Australia: the imperative for change
16 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
lifestyle changes (ie increased risk behaviours such as smoking, alcohol consumption,physical inactivity).
17
Chronic diseases are also the leading cause of disability in the community and are associated withhigh use of disability and community support services.
17
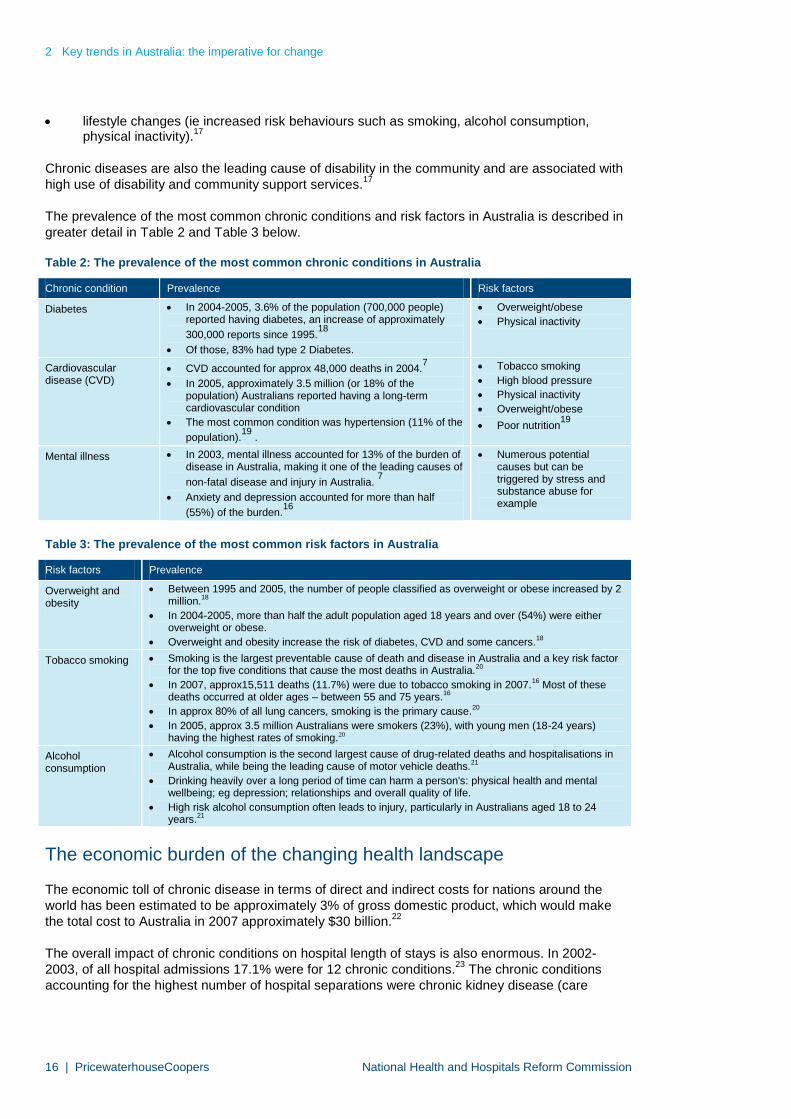
The prevalence of the most common chronic conditions and risk factors in Australia is described ingreater detail in Table 2 and Table 3 below.
Table 2: The prevalence of the most common chronic conditions in Australia
Chronic condition Prevalence Risk factors
Diabetes In 2004-2005, 3.6% of the population (700,000 people)reported having diabetes, an increase of approximately
300,000 reports since 1995.18
Of those, 83% had type 2 Diabetes.
Overweight/obese
Physical inactivity
Cardiovasculardisease (CVD)
CVD accounted for approx 48,000 deaths in 2004.7
In 2005, approximately 3.5 million (or 18% of thepopulation) Australians reported having a long-termcardiovascular condition
The most common condition was hypertension (11% of the
population).19
.
Tobacco smoking
High blood pressure
Physical inactivity
Overweight/obese
Poor nutrition19
Mental illness In 2003, mental illness accounted for 13% of the burden ofdisease in Australia, making it one of the leading causes of
non-fatal disease and injury in Australia.7
Anxiety and depression accounted for more than half
(55%) of the burden.16
Numerous potentialcauses but can betriggered by stress andsubstance abuse forexample
Table 3: The prevalence of the most common risk factors in Australia
Risk factors Prevalence
Overweight andobesity
Between 1995 and 2005, the number of people classified as overweight or obese increased by 2million.18
In 2004-2005, more than half the adult population aged 18 years and over (54%) were eitheroverweight or obese.
Overweight and obesity increase the risk of diabetes, CVD and some cancers.18
Tobacco smoking Smoking is the largest preventable cause of death and disease in Australia and a key risk factorfor the top five conditions that cause the most deaths in Australia.20
In 2007, approx15,511 deaths (11.7%) were due to tobacco smoking in 2007.16 Most of thesedeaths occurred at older ages – between 55 and 75 years.16
In approx 80% of all lung cancers, smoking is the primary cause.20
In 2005, approx 3.5 million Australians were smokers (23%), with young men (18-24 years)having the highest rates of smoking.20
Alcoholconsumption
Alcohol consumption is the second largest cause of drug-related deaths and hospitalisations inAustralia, while being the leading cause of motor vehicle deaths.21
Drinking heavily over a long period of time can harm a person's: physical health and mentalwellbeing; eg depression; relationships and overall quality of life.
High risk alcohol consumption often leads to injury, particularly in Australians aged 18 to 24years.21
The economic burden of the changing health landscape
The economic toll of chronic disease in terms of direct and indirect costs for nations around theworld has been estimated to be approximately 3% of gross domestic product, which would makethe total cost to Australia in 2007 approximately $30 billion.
22
The overall impact of chronic conditions on hospital length of stays is also enormous. In 2002-2003, of all hospital admissions 17.1% were for 12 chronic conditions.
23The chronic conditions
accounting for the highest number of hospital separations were chronic kidney disease (care

2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 17
involving dialysis), coronary heart disease, oral disease, depression and arthritis. However, thechronic conditions responsible for the longest mean length of stay were stroke, colorectal cancer,lung cancer, COPD and osteoporosis, with the average length of stay more than seven days.
23
Depression has one of the highest rates of hospital admission as well as a relatively high averagelength of stay (approximately six days),
23suggesting that it would be a significant contributor to the
increasing cost of chronic disease. In addition to the financial costs associated with extendedlength of stay, the human cost cannot be underestimated.
We consider that the exponential growth of chronic disease over a relatively short time has been,and will continue to be, a significant influence on financial and system trends in the Australianhealth system.
Indigenous health
The significant health gains experienced by many Australians have not been shared byIndigenous Australians, who continue to suffer a greater burden of ill health than the rest of thepopulation. Indigenous Australians experience lower levels of access to health services, greaterhealth risks, poorer health and a shorter life expectancy than non-Indigenous people.
24
Indigenous life expectancy and mortality
The adult life expectancy of Indigenous people is estimated to be on average 17 years less thanthat of non-Indigenous Australians – in other words, 59 years for males and 65 years forfemales.
25
A comparison of Indigenous populations in Australia, New Zealand, Canada and the United Statesof America reveals that Australia has the greatest disparity in life expectancy between Indigenousand non-Indigenous people.
26
Indigenous burden of disease
Indigenous Australians suffer a burden of disease that is two-and-a-half times greater than that ofthe total Australian population. Chronic conditions were responsible for 70% of this difference.
In terms of health service use, Indigenous people are:1
five times more likely than non-Indigenous Australians to be hospitalised for conditions thatcould be avoided through prevention and early management
twice as likely to be hospitalised for circulatory system diseases
three times more likely to be hospitalised for endocrine, nutritional and metabolic diseases,including diabetes
three times more likely to be hospitalised for chronic respiratory disease.
When combined, these findings reveal a situation that needs immediate attention and support inorder to improve the quality of life, satisfaction and health status of many Indigenous communities.
1Data are for NSW, Vic, Qld, WA, SA and NT combined based on State/Territory of usual residence.

2 Key trends in Australia: the imperative for change
18 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Drivers of Indigenous health outcomes
Research confirms that many of the poor health outcomes described above are related to thecontinued socio-economic disadvantages experienced by Indigenous people
27. These include:
poor access to education
low incomes
poor access to medical care
overcrowded housing
poor nutrition.26
Access to appropriate health services is perhaps the most immediate contributory factor to poorhealth. The following case study outlines some of the key issues Indigenous people face inaccessing health services. This information is taken from a recent project undertaken byPricewaterhouseCoopers for NSW Health (Case study 1).

2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 19
Case study 1: Issues identified in accessing health services for indigenous people
Geography – Limited service availability in rural and remote areas and limited outreach servicesresult in individuals being unable to get to appointments and can take people away from theirhomes for extended periods, sometimes on a permanent basis. ‘When we are forced to leave ourcountry and our homes we lose touch with our culture and identity. I haven’t been back home tomy country for 18 years because of my health condition”.
Prevention – Indigenous people are provided with limited education on the lifestyle choices thathave an impact on their chronic conditions (eg smoking); self-management projects are notstandardised, resulting in limited care and action planning; and systems do not support thecollection of standardised population health information in order to understand the unmet healthneed. ‘I didn’t know much about cancer, heart disease and other health issues until I got sick. Weneed more young people to understand that they need to take care of their health from a veryearly age”.
Affordability – Indigenous people experience higher costs when accessing and receiving care,including medication, transport, child care, limited bulk billing, and patient and family membercosts for extended stays or for relocation to larger centres for services. “If we can’t afford it wedon’t go to the appointments and we don’t buy healthy food or the tablets we need”.
Workforce – There are limited Indigenous health workers (especially males), particularly in theprison system. Indigenous employee programs are not considered flexible enough and there islack of training and up-skilling of the Indigenous workforce with limited skills transfer betweenmainstream and Indigenous health staff. “The AMS health staff don’t know what the mainstreamhealth staff do and they don’t know what we do”.
Cultural sensitivity – Many issues were raised highlighting the need for cultural sensitivity fromthose providing Indigenous health services. This particularly related to history and pastexperiences of family and friends, community education on how to access mainstream services,the building of trust by providers, and the lack of identifiers that indicate Indigenous people arewelcome at a service (eg artwork, flag out front).“I make the doctors feel comfortable when theylook scared about me being Aboriginal”.
Infrastructure/accountability – The Commonwealth/state funding split results in a lack ofintegration (ie silos) of funding and does not promote continuity of care.
Communication – Indigenous patients/community do not know what services are being provided,what the roles/responsibilities of staff are, what are the waiting times, etc and carers are not beingmade aware of support available to them. “I don’t understand what the doctors and nurses aresaying to me when they explain the operation and tests I need to have and what I need to do.They don’t write it down for me so I can ask other doctors at the AMS and my family memberswhat it is all about”.
Provision of care – Health care providers (including General Practitioner’s (GPs)) are not askingdirect questions regarding Aboriginality. In addition, there are limited standardised tools for thescreening and assessment of Indigenous patients; mainstream providers do not know the bestmodel of care for their Indigenous patients, nor how to refer patients to the appropriate services;and the discharge process does not facilitate links between services to share information. “When Iget the courage to actually go to another appointment they tell me the referral hasn’t come throughand I have to wait another few weeks”.
It is obvious that a complex network of factors contributes to the significant disparities in healthstatus between Indigenous peoples and other Australians; socio-economic disadvantage cannotfully explain the disparities in health status.
The high prevalence of chronic health conditions experienced by Indigenous people is of particularnote. Many of the issues affecting health outcomes for Indigenous Australians emerge from poor

2 Key trends in Australia: the imperative for change
20 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
care coordination, which is consistent with the experience of many other Australians. This, in turn,leads to significantly higher rates of complications and death.
For Indigenous Australians, these issues are compounded and exacerbated by the culturalappropriateness of services and geographic distance to services. Substantive progress will rely oninvestments across the continuum of care for Indigenous communities – primary, secondary andtertiary care.
26

2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 21
2.2 Rising costs and expenditure: emerging trends
Costs are rising in an unsustainable way as a consequence of demographic issues andthe growing expenditure on specialised medicine and technology aimed (for the mostpart) at prolonging life. In addition, there is a mismatch of expenditure to actual needwhich is an inefficient use of resources.
Cost escalation
In Australia, as in all developed countries, health spending is expected to increase at a muchfaster rate than in the past. By 2020, health care spending globally is projected to triple in realdollar terms, consuming 21% of GDP in the US and 16% of GDP in other OECD countries.
6
In the ten years to 2005-2006, Australia’s total health expenditure increased from $39.0 billion to$86.7 billion – a growth rate of 8.3% of a year. This represents an increase from 7.5% to 9.0% ofGDP in a period of strong economic growth, and an average ‘real growth’ (ie in excess of thehealth constant price deflator) over the period of 5.1% a year.
28
On this basis, the ominous predictions of the Intergenerational Report (IGR)29
seem well within therealms of possibility, with health spending projected to nearly double as a proportion of GDP overthe next 40 years. Indeed, the IGR notes the need to manage fiscal pressure, including the growthin government spending. The IGR further reports that Commonwealth health spending is projectedto continue to rise strongly and is the main spending pressure, with spending on pharmaceuticalbenefits projected to grow the fastest. For example, expenditure on medications grew in real termsat an average rate of 8.6% a year from 1995–1996 to 2005–2006.
30
Much of this fiscal pressure stems not only from the rapid rise of chronic diseases and populationageing, but also from the development of high-cost more specialised medicine and technology.This is aimed for the most part at prolonging life. PwC’s work with the pharmaceutical industry hashighlighted technological advances (such as biological and other niche products) resulting fromthe growth of the genetic and biotechnology industries. The impact of this will be:
increasing research and development costs to manufacturers
changes in the regulatory model for specialty product listing and pricing. These innovationscost more to develop and therefore increase the cost to the government
market price expectations for specialty products which might not be met by governmentreimbursement. At PwC we are currently looking at this very issue to establish alternativefunding sources for high-cost specialised drugs that are not being funded by a cost-constrained and technology assessment-driven PBS
the need to prove better and more cost-effective patient outcomes for specialty products
more severe pricing pressure exerted by F2 drugs on F1 drugs, causing the cost of F1drugs to the government to rise.
Other drivers of health system costs include:
an increase in public expectation; namely, expectations that state-of-the-art health servicewill be available at all times and at any cost
31
a rise in consumerism in health, partly driven by increased wealth of the baby boomers andtheir ability and desire to pay for high cost interventions to keep them well
32
an increase in litigation, which has been shown to lead to over-servicing particularly in thefield of diagnostic medicine.
33

2 Key trends in Australia: the imperative for change
22 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Mismatch of health expenditure to health need
Appropriate targeting of health resources to health needs is critical if Australia is to continue to seethe improvements in mortality and life expectancy that we have enjoyed over the past century.
The current challenges facing the Australian health system point to the need to move towards asystem that is able to manage the growing burden of chronic disease resulting from the changingdemographics and consequent health trends.
This will require a proactive and supportive approach to health care across the continuum, thatencourages prevention, early detection and ongoing management, rather than the traditional acutecare model that has focused on episodic care. Yet the main areas of health expenditure are stillhospital, medical, dental, medicines, and capital. Together these areas comprise 82% of totalhealth expenditure (Table 4).
The corollary is that only 18% of our health expenditure is applied to the other areas, of which1.7% and 4.5% is spent on public health and community health respectively. These issues areclearly demonstrated in Figure 5, where we map the allocation of funding along the whole carecontinuum.
It would seem at first glance that this distribution of funds falls considerably short of a systemmoving to manage the key risk drivers (ie ageing and chronic disease). It is also evident that totalexpenditure is not, by itself, a necessary and sufficient lever for structural change in the healthsystem. Spending more without structural reform may simply continue the pattern of supportinghealth system structures, models of care and funding models, which promote an acute-care-focused and episodic approach to health care.

2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 23
Figure 5: The model of care and health expenditure
Person in thecommunity
Person enterssystem
EmergencyDepartment
Inpatientcare
Discharge Person in the community
Health
pro
motion
Prim
ary
pre
vention
Secondary
pre
vention
Tert
iary
pre
vention
Com
munity
care
packages
Genera
lpra
ctitioners
Identification
ofpatients
Case
findin
g
Triage
Em
erg
ency
care
Protocols, policies and procedures
Framework of cultural respect
Ongoing data collection and managementS
cre
enin
gand
ass
essm
ent
Acute
care
Care
pla
nnin
g
Refe
rral
Dis
charg
epla
nnin
g
Refe
rral
Tra
nsitio
nalcare
Patientfo
llow
-up
and
recall
Com
munity
care
pack
ages
Self
managem
ent
Ongoin
gcare
Genera
lpra
ctitioners
Self
managem
ent
Refe
rralto
altern
ative
care
Com
munity
health
serv
ices
Com
munity
health
serv
ices
Aged Care
Chronic Care
Mental Health
Community Care
Emergency Care
Surgery
Healthpromotion and
preventionCare and service provision Ongoing care and
follow-up
82% of total health expenditure is on hospital,medical, dental, medicines and capital
4.5% of health expenditure is oncommunity health
1.7% of health expenditure is onpublic health
Person in thecommunity
Person enterssystem
EmergencyDepartment
Inpatientcare
Discharge Person in the community
Health
pro
motion
Prim
ary
pre
vention
Secondary
pre
vention
Tert
iary
pre
vention
Com
munity
care
packages
Genera
lpra
ctitioners
Identification
ofpatients
Case
findin
g
Triage
Em
erg
ency
care
Protocols, policies and procedures
Framework of cultural respect
Ongoing data collection and managementS
cre
enin
gand
ass
essm
ent
Acute
care
Care
pla
nnin
g
Refe
rral
Dis
charg
epla
nnin
g
Refe
rral
Tra
nsitio
nalcare
Patientfo
llow
-up
and
recall
Com
munity
care
pack
ages
Self
managem
ent
Ongoin
gcare
Genera
lpra
ctitioners
Self
managem
ent
Refe
rralto
altern
ative
care
Com
munity
health
serv
ices
Com
munity
health
serv
ices
Aged Care
Chronic Care
Mental Health
Community Care
Emergency Care
Surgery
Healthpromotion and
preventionCare and service provision Ongoing care and
follow-up
Person in thecommunity
Person enterssystem
EmergencyDepartment
Inpatientcare
Discharge Person in the community
Health
pro
motion
Prim
ary
pre
vention
Secondary
pre
vention
Tert
iary
pre
vention
Com
munity
care
packages
Genera
lpra
ctitioners
Identification
ofpatients
Case
findin
g
Triage
Em
erg
ency
care
Protocols, policies and procedures
Framework of cultural respect
Ongoing data collection and managementS
cre
enin
gand
ass
essm
ent
Acute
care
Care
pla
nnin
g
Refe
rral
Dis
charg
epla
nnin
g
Refe
rral
Tra
nsitio
nalcare
Patientfo
llow
-up
and
recall
Com
munity
care
pack
ages
Self
managem
ent
Ongoin
gcare
Genera
lpra
ctitioners
Self
managem
ent
Refe
rralto
altern
ative
care
Com
munity
health
serv
ices
Com
munity
health
serv
ices
Aged Care
Chronic Care
Mental Health
Community Care
Emergency Care
Surgery
Healthpromotion and
preventionCare and service provision Ongoing care and
follow-up
82% of total health expenditure is on hospital,medical, dental, medicines and capital
4.5% of health expenditure is oncommunity health
1.7% of health expenditure is onpublic health
Source: PricewaterhouseCoopers, May 2008 © copyright

2 Key trends in Australia: the imperative for change
24 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
2.3 Trends in system evolution
The present system is unable to appropriately fund and implement a shift from an acuteand episodic approach to one which encourages both prevention and coordinatedmanagement. This is because of the system’s complexity and fragmentation, including apoor incentive structure which is not aligned to need or outcomes.
The significant changes in health needs in Australia have, of course, not gone unnoticed in thepolicy arena. For example, in 2002-2003, a national strategic approach was developed to addressthe increasing burden of chronic disease through the development of policy guidelines for theprevention and management of chronic disease.
17This strategy – the National Chronic Disease
Strategy – informs the health system about the most effective care for asthma, cancer, diabetes,osteoarthritis, rheumatoid arthritis and osteoporosis and heart, stroke and vascular disease.
However, while this policy represents best practice principles for person-centred management ofchronic disease, the current operation of our health system is ill-equipped to deal with the changesthe policy requires. The reasons for this are considered below.
Complexity and fragmentation
There is growing evidence that, in Australia, as elsewhere around the world, our health system willnot be sustainable if it is left unchanged over the next 15 years. In particular, the system isundermined by complexity and fragmentation and insufficient capacity for delivery of person-centred health care. Ultimately, these limitations are reflected in what can be considered a sub-optimal system outcome (in terms of poor accountability), as well as sub-optimal patientoutcomes; namely, threats to quality and safety.
The Australian health system involves many stakeholders working across different levels ofgovernment and in the public and private sectors. However, optimal health care delivery requirescareful coordination of services and resources to deliver a safe and high quality system supportedby integrated information.
The fragmented nature of the current health system is typified by different and often uncoordinatedfunding sources required to deliver care, which is most clearly demonstrated by the split in fundingresponsibilities between federal (primary care) and state health (acute, community and non-residential aged care). Figure 6 below clearly illustrates the extent of this issue across all fundingsources.

2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 25
Figure 6: Sources of health care funding in Australia
Australian Government
State and territorygovernments
Injury compensation funds
Private health insurers
Person
Australian Government
State and territorygovernments
Injury compensation funds
Private health insurers
Person
Funding Sources
Pathology
DiagnosticsC
omm
unity
HealthG
Ps
Age
dCar
e
Allied Health
Publichospitals
Specialists
Priva
teH
ospital
Pha
rmac
eutic
als
Pathology
DiagnosticsC
omm
unity
HealthG
Ps
Age
dCar
e
Allied Health
Publichospitals
Specialists
Priva
teH
ospital
Pha
rmac
eutic
als
Source: PricewaterhouseCoopers, May 2008 © copyright
To see how the scenario described in Figure 6 is reflected in the actual distribution of health careexpenditure across the health care sector for 2005-2006, we have highlighted in Table 4 belowwhere blocks of expenditure (shaded in blue) exceed $200 million a year from a particular source.From this we can see that many funders are significantly involved in a number of areas and thathospitals (public and private) and medical services receive their funding from the most variednumber of sources.

2 Key trends in Australia: the imperative for change
26 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Table 4: Australia’s health spending by area of expenditure and source of funds, 2005-2006
Government Non-government
Australian Government
Area of expenditureDirect
outlaysPremium
rebates TotalState and
local Total
Healthinsurance
funds Individuals Other TotalTotal healthexpenditure
Total hospitals 10,862 1,750 12,612 12,618 25,230 3,462 667 1,642 5,772 31,003
Public hospital services 9,898 207 10,105 12,374 22,479 409 386 1,046 1,840 24,319
Private hospitals 963 1,544 2,507 244 2,751 3,054 282 597 3,932 6,683
Patient transport services 118 47 165 899 1,064 92 209 74 375 1,439
Total institutional 10,080 1,797 12,777 13,518 26,295 3,555 876 1,716 6,147 32,441
Medical services 11,918 321 12,239 - 12,239 636 1,745 879 3,261 15,499
Dental services 96 384 480 515 995 760 3,573 10 4,342 5,337
State/territory provider .. .. .. 515 515 .. 19 .. 19 534
Private provider 96 384 480 .. 480 760 3,554 10 4,323 4,804
Other health practitioners 517 194 711 - 711 384 1,653 288 2,324 3,035
Community health and other 419 - 419 3,167 3,588 - 173 139 313 3,899
Public health 798 - 798 632 1,429 - 47 - 47 1,476
Medications 6,093 24 6,117 - 6,117 47 5,276 62 5,384 11,501
Benefit-paidpharmaceuticals 6,046 - 6,046 - 6,046 - 1,240 - 1,240 7,286
All other medications 48 24 71 - 71 47 4,036 62 4,144 4,216
Aids on appliances 276 133 409 - 409 264 2,072 42 2,378 2,787
Administration 1,080 323 1,403 455 1,858 639 - - 639 2,497
Research 1,275 - 1,275 229 1,504 - - 412 412 1,915
Total non-institutional 22,472 1,380 23,852 4,997 28,848 2,729 14,539 1,831 19,100 47,948
Total recurrent expenditure 33,452 3,177 36,629 18,514 55,143 6,284 15,415 3,547 25,246 80,389
Capital expenditure 183 .. 183 1,898 2,080 n.a. n.a. 3,087 3,087 5,167
Capital consumption 88 .. 88 1,234 1,323 .. .. .. .. 1,323
Total health expenditure 33,723 3,177 36,900 21,646 58,546 6,284 15,415 6,634 28,333 89,879
Non-specific tax expenditure 329 .. 329 .. 329 .. -329 .. -329 ..
Total health expenditure 34,052 3,177 37,229 21,646 58,875 6,284 15,086 6,634 28,004 86,879
Source: AIHW Health Expenditure Australia. Table A3: total health expenditure, current prices by area of expenditure and source of funds(a), 2005-2006 ($ million)

2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 27
To compound the issue of fragmentation in funding sources, there is also little evidence ofattempts to provide funding in a way that actually facilitates a ‘continuum of care’. For example, insome cases certain payers have more influence over the overall service delivery model than otherand this puts pressure on the service provider to supply more (or less) services of a particular typeregardless of their appropriateness in the continuum and for any individual.
Fragmentation in the public system
The split in funding between federal (primary care) and state health (acute, community and non-residential aged care) makes effective coordination hard to achieve. Funding boundaries are alsoblurred within the state systems, for example, mental health and aged care, which compounds theissue. In the context of a growing and ageing population with chronic and complex conditions –requiring best practice clinical treatment regimes, with access to multiple service providersworking together collaboratively – this situation is not sustainable.
At present the overriding theme from the available evidence is that neither funding nor processsupports integration at any point of the overall patient experience, as illustrated in the followingcase study (Case study 2).
Case study 2: Fragmentation in chronic and complex care34
PwC has worked closely with a number of NSW Area Health Services (AHS) toimprove the assessment and management of people with chronic conditions. Ourwork identified a range of challenges in delivering appropriate and timely care tosuch people which resulted from a lack of integration between services:
complexity and a lack of standardisation in making referrals to particularservices, including out-of-hours referrals and transfers between residential agedcare facilities and hospitals
no systematic process for the transfer of patient information between servicesand poor information management between service providers, resulting inpotential inefficiencies such as clients being on multiple waiting lists for services
limited opportunities to network and exchange information between serviceproviders
a focus on acute episodic care as opposed to a model of care designed to meetthe ongoing needs of people with chronic conditions
a longer length of stay in the emergency department for people with agedand/or chronic and complex conditions
limited contact between AHS staff and general practitioners in the managementof patients who were admitted to hospital
a lack of case management to coordinate care.
A number of Medicare items have been introduced to promote the delivery ofpackages of care by general practitioners; eg the practice incentives program fordiabetes, and enhanced primary care chronic disease management items.However, restrictions exist, and they hinder the effectiveness of those items inappropriately managing people with chronic disease. For example, under theenhanced primary care items, a maximum of five referrals for allied health servicesare allowable in a calendar year. This cap prevents a person-centred approach tocare since management is not based on the individual’s needs but on a definednumber of referrals.

2 Key trends in Australia: the imperative for change
28 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Limited interface between public and private systems
As illustrated in Figure 6 private health insurance predominantly covers hospital and in-hospitalmedical/pharmaceutical costs. It therefore does not provide an integrated service on behalf of itsmembers. The following impediments have contributed to this:
There is little incentive for private health insurers to implement preventative interventions,as they can only benefit financially if they see a payback in terms of reduced hospital costsfor members. Moreover, the risk equalisation arrangements significantly limit any benefithealth insurers would gain from such a reduction.
There is also an impediment to health insurers’ capacity to take advantage of out-of-hospitaltreatment, which was encouraged in recent legislation after many years of lobbying. This isa result of a ‘Catch-22’ situation, where private hospital providers are only likely to deliverthese out-of-hospital packages if they can be confident health insurers will sponsor them.However, health insurers need the packages to be in place before they can be properlyevaluated and benefits assessed.
And finally, due to privacy issues, private health insurers have experienced difficulty gettingrelevant information (eg asking members for information about their health, analysing theirown data, and particularly in identifying members to whom they could target interventions).Some private health insurers point out they have opted for broader campaigns, for example,diabetes management, with offers taken up by those who do not actually have the disease.
Despite this, a number of private health insurers have been able to implement successfulprevention programs, which have resulted in an overall reduction in private hospitalisations. Theseprograms have been targeted at cardiovascular disease management, diabetes management andweight loss programs (prior to knee reconstruction surgery, for example).
As a result, there appears to be increasing interest from the private health insurance industry inextending their role in health service provision. This is fuelled by the recognition that their currentrole is unlikely to be viable in a changing structural landscape in the long term. These issues areconsidered in more detail in Chapter 3.
Mismatch of funding to need
As described above, there is evidence in the Australian health system that the distribution ofexpenditure does not match the underlying need for care. One of the main reasons for this is thatresources are generally not allocated based on evidence. For example, funding for publichospitals is inconsistent between the different Australian states, with inconclusive outcomes (egpopulation-based funding in NSW, case-mix-based funding in Victoria).
Within service types too, there is anecdotal evidence that resources are not being allocatedequitably to different types of underlying need. While there is no appropriate data to test this in themainstream health system, the following case study illustrates this effect in the related area ofdisability services (Case study 3).

2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 29
Case study 3: Estimating the unmet need for disability services in NSW35
In 2005, the NSW Department of Ageing, Disability and Home Care engaged PwC to develop abaseline dataset and modelling tool to help estimate the unmet need for disability services inNSW.
The project involved building a model of disability ‘prevalence’ and a model of service levelprovision in order to compare the extent to which services matched prevalence, at present andinto the future. A variety of service level scenarios were developed to analyse the way in which thesupply-demand balance was likely to change over the next 25 years.
The project identified significant unmet need for disability services, which resulted in a largeincrease in disability funding in NSW. Importantly, the analysis identified that this funding neededto be targeted to certain disability types – people with physical disability were receivingsignificantly less support services than people with an intellectual disability.
In addition, the fee-for-service approach encourages an uneven and inequitable distribution of thehealth workforce. Funds follow where the doctor is attracted by rational economic decisions, whichmay not be where patients’ need lies.
Operators in the health system are free to set their own prices; for doctors this means choosingwhether or not to bulk bill and choosing the gap fee that patients pay. As a result, higher socio-economic areas are generally more attractive, leaving many lower socio-economic areasunderserviced. From an equity-of-access viewpoint, there should be higher bulk-billing levels inlower socio-economic areas than is currently the case. The following case study (Case study 4)highlights these challenges and how the funding model contributes to the issues.

2 Key trends in Australia: the imperative for change
30 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Case study 4: GP workforce supply and demand modelling36
In 2004 PwC undertook significant work for the Australian Medical Workforce Advisory Committee(AMWAC) to estimate the shortage of GPs in Australia and to project the supply and appropriatedistribution of GPs across Australia for 2004 to 2014.
We estimated that, overall, there was a shortage of 800 to 1,300 GPs in Australia and projectedthat in order to achieve balance by 2013, the number of new entrants to the workforce would needto increase from current levels of 700 a year to 1200 or 1300 a year.
Significantly, we identified that shortages were experienced predominantly in outer metropolitan,regional and rural areas, with remote and very remote areas receiving 10% to 20% less GPservices per person than other areas. Regions with lower socio-economic indicators also havesignificantly lower access to GP services than other regions and significantly higher throughput,measured as the number of GP services provided per hour worked. Substantially more GPs wouldbe required in low socio-economic areas and the rural and remote regions for patients to receiveservices equivalent to those in the higher income urban areas.
A contributing factor to the under-supply in these areas is the existing funding model, where thefunding follows the doctor, thereby allocating resources to where the doctor wants to work ratherthan where the need for services is greatest. Although the government has introduced incentivesto encourage doctors to work in non-metropolitan areas, the funding approach provides a perverseincentive in that it encourages an over-supply of practitioners in some areas and an under-supplyin others. NSW, for example, had higher GP service utilisation compared to all other states.
Unsurprisingly, the price of services was also a substantial factor to patients, with serviceutilisation per person significantly lower in areas with higher patient co-payments. The analysisalso highlighted the interaction of various parts of the health system. For example, GP serviceutilisation was 5% lower in areas which contained a hospital than those which did not.
Misaligned incentives
The fee-for-service funding mechanism also gives providers the wrong type of incentive,encouraging more services but not necessarily better health as illustrated in the following casestudy (Case study 5).
Case study 5: Fee-for-service funding, an example of inefficient service provision
There is much anecdotal evidence of fee-for-service funding leading to inappropriate serviceprovision. PwC’s work as national evaluator for CCT2 highlighted an example of difficulties inproviding influenza vaccinations.
2
One trial doctor operating in a rural area explained that his approach during a patient consultation(one service) was to write a prescription for the vaccination to be collected from a pharmacist (aseparate service) and to offer a home visit (another service) to administer the vaccination once thepatient had advised they had collected the vaccine.
The doctor did not have the infrastructure to store the vaccine on his premises, and while co-location of pharmacy and medical services would have led to a better outcome at a significantlyreduced overall cost, there were no incentives for this to take place.

2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 31
Even hospital case-mix (AMWAC-based) funding may not provide the right incentives, as hospitalsare paid each time a patient presents and departs. As a result, the funding system encouragesmore presentations (attendances), not fewer.
Obstacles to care coordination
The issues described above provide the evidence for why it has been difficult to embed effectivecoordinated care on a day-to-day basis in the Australian health system. In addition, the nationalevaluation of CCT2 exposed the magnitude of the change required to move from conceptualmodels to implementation of care coordination.
Specifically, the evidence highlights the fact that one of the core impediments to change isunderestimating the scale of the task that would be required. This is manifest in many differentways: the skills required for delivery, the time required for delivery, the coordination required fordelivery, and the technology required for delivery (see Case study 6).
Case study 6: Structural impediments to effective care coordination
Five CCT2 trials were operational between 2002 and 2005, for which PwC was the nationalevaluator. They consisted of two mainstream and three Indigenous trials, each with a uniquedesign plan for the funding and delivery of coordinated care.
The challenges associated with achieving care coordination within the trials included:
underestimation of the complexity involved in moving from conceptual models to a carecoordination model; eg developing, negotiating and implementing a new clinical servicedelivery model
constraints on GPs’ time, which meant it was difficult for them to be in a position to fullydrive care coordination within the primary care setting
lack of coordination between mainstream and Indigenous community health workers andthe AMSs
at all points in the continuum of care, trained health professionals appropriate to theircommunity environment are needed; where training lagged, delivery of care coordinationwas undermined
the arbitrary nature of allocating a set number of participants to service coordinators, eg 200clients for one FTE, without appreciating the fact that varying demands of different casesplaced different workload pressures on coordinators
turnover of staff at a number of levels of the project, including the department, the trials andthe local evaluators; this was a particular problem for trials located in rural and remote areas
a generic approach to managing the trials through a variety of project officers and contractmanagers appointed by each funding body
successful IT implementation
instances of limited community engagement and capacity building, which hampered theeffective introduction of care coordination frameworks for the Indigenous trials.

2 Key trends in Australia: the imperative for change
32 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Governance structures
There are significant differences in the role and scope of the various health authorities acrossAustralia as reflected in Table 5 below. This situation therefore only reinforces the significantissues highlighted above in relation to system fragmentation ie opaque accountabilities and limitedservice integration/coordination.

2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 33
Table 5: Management of health and human services by jurisdiction – the state of play in 2004-200537
Jurisdiction Scope Organisational divisions Regions
Australian
Government
Separate authorities for Family and Community Servicesand Veterans' Affair
Acute Care, Ageing and Aged Care, Health ServicesImprovement, Medical and Pharmaceutical Services, Office ofAboriginal and Torres Strait Islander Health, Population Health,Portfolio Strategies, Primary Care
Each state and territory is a region
ACT Separate authorities for Disability, Housing andCommunity Services, Australian Capital Territory (ACT)Emergency Services Authority provides the ambulanceservice, Separate Health and Community ServicesComplaints Commission (HCSCC) established late 2004
Allied Health Adviser, Clinical operations, Financial and Risk,Management, Government Relations and Planning, HumanResource Management, Information Services, Nursing andMidwifery, Office Policy, Population Health
None. All services directly managed by theDepartment
NT Separate authorities for Community Development, Sportand Cultural Affairs, Separate HCSCC
Aboriginal Health, Family and Social Policy, Acute Care,Community Services, Corporate Management Services, HealthServices, Information Strategy and Quality
None. All services directly managed by theDepartment
St John Ambulance Service is separately incorporated
NSW Separate authorities for Ageing, Disability and HomeCare, Housing, Community Services and MedicalResearch, Separate HCSCC
Health System, Performance, Health System Support, PopulationHealth, Strategic Development
8 AHSs, plus: Ambulance Service of NSW, Children’sHospital Westmead, Justice Health, ClinicalExcellence Commission, NSW Cancer Institute
QLD Separate authorities for Child Safety, Communities,Emergency Services, Housing, Disability Services,Separate Health Rights Commission of Queensland(QLD)
Health Services Information, Innovation and Workforce Reform,Resource Management, Strategic Policy and Government Liaison
3 Zones
37 Districts within zones
All services directly managed by the Department
SA Department of Families and Communities, SeparateHCSCC announced in 2004, Separate bodies deliverambulance services, Separate Veterans RepatriationHospital, Separate Hospitals and Domestic Care
Population and Environmental Healthy, Service Planning, StateDental, Mental Health, and Drug and Alcohol – all managed in aregion, South Australia (SA) Health Reform
2 metropolitan health regions and Children, Youth andWomen's Health Service with own boards.
4 country regional health services
TAS Separate HCSCC Children and Families, Community, Population and Rural Health,Corporate Services, Hospitals and Ambulance, HousingTasmania
None. All services directly managed by theDepartment
VIC Separate Office of the Health Services Commissioner,Office for Children reporting to Minister for Children
Disability Services, Financial and Corporate Services, Housing &Community Building, Metropolitan Health & Aged Care Services,Operations, Policy & Strategic Projects, Rural & Regional Health& Aged Care Services
8 Regions, 12 networks with own boards within metroregions, 71 agencies with own boards in rural regions,Victorian Ambulance Service
WA Separate authorities for Community Development,Disability Services and Housing, Office of Health Review,Separate Office of Safety and Quality
Clinical Policy Division, Statewide Health Support, PopulationHealth Division, Country Health Services, Central Wait ListBureau
3 AHSs, 1 Country Health Service and Women's andChildren's Health Service, all directly managed by theDepartment
St John Ambulance Service is separately incorporated
Source: Rix M, Owen A, Eagar K. (Re)form with Substance? Restructuring and Governance in the Australia Health System 2004/05. Australian and New Zealand Health Policy 2005;2(19), Table 2
In addition, there is no evidence to suggest whether any of these structures produce more effective policy than others. Nor is there evidence to indicate whichstructure is best able to manage the health system and its reform.37. Hence, our recommended new approach to governance as set out in Chapter 1.

2 Key trends in Australia: the imperative for change
34 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
2.4 Limited capacity to deliver person-centred health care
There is limited capacity within the health system to deliver person-centred health care.This is a consequence of substantial access, data, workforce and infrastructure issues.
The ideal health landscape requires person-centred health care that allows for a seamlessinterface across the entire continuum of care, targeted to each patient’s health need and itsvariations over time. In an ideal world, this results in the timely management of health, withconditions that can be managed within the community being managed there, and conditionsrequiring acute care being managed in hospitals.
However, timely access to health care is not universal in Australia. This reflects the fact that, inaddition to the structural impediments identified above, the Australian health system has limitedcapacity to deliver person-centred health care in terms of the necessary supporting data,workforce and infrastructure requirements. These issues are discussed in more detail below,under the topics Access, Data, Workforce and Infrastructure.
Access
Many people experience difficulty accessing services due to factors such as gender, age, limitedproficiency in English , disability, ethnicity or geography. However, these socio-economic factorsnotwithstanding, data on the Australian hospital system indicates that all states and territories facechallenges in providing timely access to elective surgery and emergency department care.
For example, in 2005–2006, the median waiting time for elective surgery in public hospitals was32 days. Almost 5% of people admitted for elective surgery from the elective surgery waiting listshad waited more than 365 days.
38Within emergency care, delays occur while patients wait to be
seen by a practitioner. In 2005–2006, for all triage categories the proportion of patients receivingemergency department care within the required time was 69%, ranging from 52% in the AustralianCapital Territory to 77% in Victoria.
Common issues in accessing primary health care include the cost of health care and the limitedavailability of bulk billing, along with the impact of geography. Geography, in particular, is an issuein relation to a person’s access to GPs, since a patient’s inability to access GP services caninfluence demand for other health services; for example, a lack of GP services in a particular areacan be related to high use of emergency departments.
39Also, compared with metropolitan GPs,
those in rural or remote areas spend more of their time working in local hospitals.
Geography also affects the type of services that are available. For example, expenditure onIndigenous primary health care services, other community health services, and services deliveredthrough hospital accident and emergency departments is more prevalent in rural and remoteareas, which has an impact on the availability of primary care services in those areas.
The widespread existence of waiting and delays for health care inevitably has an impact on thequality of care provided. NSW Health Clinical Services Redesign Program is one example of astate’s approach to, among other things, improving patient flow and removing system constraints.These in turn improve patient and staff satisfaction through reduced waiting times. WA has alsorecently commenced a clinical service redesign initiative through WA Health aimed at reducingdelays to the patient’s journey and improving access across key areas of the health service.

2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 35
Data
There are considerable issues concerning the quality of available data in Australia, which limitsour capacity to plan and deliver coordinated health services for people across their life-cycle, withthe aim of achieving optimal health outcomes within existing resource constraints.
Per person vs per episode
The most logical method for estimating the health needs and planning services for any sub-population is to describe the characteristics of the sub-population in terms of the individuals itcomprises (eg through a unique patient identifier). However, there are very few ‘per person’datasets available in Australia that contain longitudinal records of personal health care use (oneexception is the WA linked dataset).
Currently, our major unit-record datasets record information on a ‘per episode’ or ‘per service’basis, as follows:
state inpatient statistical collections, which record extensive details of every episode ofinpatient hospitalisation within its jurisdiction
MBS medical episodes of care
pharmaceutical benefits under PBS
various minimum datasets of community care.
So although it is possible to internally link an individual’s records using a unique identifier (eg theMedicare number for MBS), it is not possible to link records across these datasets in a practicalway. For example, while aggregate summaries of use can be derived using various statisticallinkage keys and probabilistic matching of records, our experience is that these linkages areunreliable and unwieldy in a day-to-day care coordination setting.
Other issues include privacy and the complex nature of Australia’s health data ownership.
Health data content
The content of the currently available data is not sufficient to address the needs of a modernhealth system based on an integrated continuum of care. Other than purpose-specific researchcollections (eg Bettering the Evaluation and Care of Health (BEACH)),
40there is little information
available about primary and community care delivered or its outcomes for patients.
For example, as part of the national evaluation of CCT2, we compiled a major purpose-specificnational data collection with impressive commitment from the full range of federal and state dataowners. Quality issues aside, it was clear that the data could not provide the information neededto properly understand the (sub-acute) experience and determinants of outcome for patients withchronic and complex conditions.
2
In our view, there are many areas for improvement in Australian health data quality and access.Taking into account the political and financial realities, Table 9 in Chapter 3 comments on each ofwhat we define as ‘features of an ideal data system’.

2 Key trends in Australia: the imperative for change
36 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Collection, storage and use of data: our information management system
In addition to the nature and form of our health data, the processes involved in collecting,retrieving and reporting on this information also impede good health service delivery. Ourexperience in compiling information and performance reports in a wide range of health settingsindicates that datasets are poorly planned, disorganised, and dependent on an individual’sfamiliarity and ‘corporate history’ to achieve productive reports. Some common themes haveemerged, which affect data integrity:
Processes are not reviewed to ensure efficiencies of new systems are realised andaccurate data is captured at the point of entry.
Training is inadequate and usually underestimated, affecting the accuracy of informationcaptured and the use of that information.
Clinician engagement is not always seen as critical, resulting in systems not being used anddata being incomplete.
New systems often require additional information beyond what is used for patient care,resulting in users spending more time at the computer or having to find workarounds.
The case study below (Case study 7) highlights many of the information management issues thatneed to be addressed if greater care and service integration is going to be achieved.
Case study 7: The importance of effective and efficient information management processes2
For the national evaluation of CCT2 our dataset sought to include personal characteristics foreach participant, as well as their health status at several measurement points, and all records ofhealth service use (hospital, medical, pharmaceutical, community health). As a result we were wellplaced to observe the following systemic information management issues:
major confusion about privacy protocols when accessing the data, even with full support ofboth levels of government
delays (of 18 months) in the Health Insurance Commission (now Medicare Australia) settingup a website to supply MBS and PBS utilisation on trial participants – this meant that trialswere effectively flying blind in their attempts to monitor expenditure against their allocatedrisk-based fund pool
state and territory health departments being unable to supply hospital inpatient data on trialparticipants easily and quickly, and the need for multiple re-runs where errors were detected
a total inability to gather data linked to community-based services.
This position has arisen despite awareness and investment by states and the Commonwealth invarious data and information management systems (eg eHealth strategies), yet their full potentialhas yet to be realised. For example, each state has their own eHealth project and associateddeadlines, addressing similar needs but all are taking different approaches and are notcoordinated.
A further point is that, unlike the public health systems who have been key members of theNational eHealth Transition Authority, the private health sector has not been involved in agreeingor developing the technology building blocks and standards of the broader health system. This willfurther impede effective information sharing across the health system if not appropriatelyaddressed.

2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 37
Workforce
Having the right workforce is critical to the effecftive delivery of services in the health sector. Over10% of Australia’s workforce is employed in the community services and health sectors and thisgroup is growing 3 to 4 times faster than the total Australian workforce.
41
Australia’s health workforce is currently subject to a range of challenges. Three key challengesare:
workforce size and composition, which is particularly difficult to change given thatoccupational roles and tasks that have been in place for many decades and remain in ‘silos’
poor workforce distribution, in part reflecting the predominantly sole-practice nature ofemployment for many doctors and allied health professionals, which makes optimalworkforce distribution difficult to achieve
education and training that is lengthy and resource intensive.
Together, these issues mean that there is limited flexibility and capacity to achieve greaterproductivity. This lack of flexibility adds to the difficulty of developing models of person-centredhealth care, raising the critical issue of how to staff these ideal models of care.
Workforce shortage and mix
A series of research projects commissioned by the Australian Medical Workforce AdvisoryCommittee (AMWAC) and the National Health Workforce Taskforce (NHWT) have highlighted thefact that key health professions and skill groups are experiencing real shortages to an extentwhich may not be remedied by simply allocating more training places. Work recently undertakenby PwC for the NHWT indicates that significant shortages could arise in the nursing and medicalworkforces, while strong growth in demand for physiotherapists and podiatrists may also lead toshortages.
42
Role design
Role redesign is a national and international trend aimed at better use of resources andappropriately meeting demand. It involves the development and extension of existing clinical rolesto meet workforce demands; for example, clinical assistants, physician assistants, nursepractitioners and nurse prescribing. Funding and structural governance models must also adapt torecognise these trends.
Technology and policy changes
Changes in health technology and public policy can have an immediate impact on workforce need,and the way in which new initiatives are introduced must be considered in concert with theworkforce and infrastructure available to meet them. Without the right workforce, recent initiativessuch as the National Bowel Cancer Screening Program (Example 1) and the Teen Dental Planmay fail.

2 Key trends in Australia: the imperative for change
38 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Example 1
The National Bowel Cancer Screening Program began screening with the Faecal Occult BloodTest (FOBT) from May 2006 by targeting those aged 55 to 65 years of age, and is beingintroduced progressively to June 2008. It is estimated that, as a result of positive FOBT tests,there may be up to 11,500 more colonoscopy examinations required in the first year of theprogram
43. However, a debate is needed on how these additional examinations will be conducted
given current workforce pressures. Issues for discussion include the respective roles andresponsibilities of (1) nurses and medical specialists and (2) between medical specialists inconducting colonoscopies. Without resolution, the future effectiveness of this program may be indoubt.
Workforce composition
Growth in the health workforce has been far from even, suggesting that the industry is alreadyexperiencing dramatic changes in the model of staffing, with roles and responsibilities for heathcare professionals evolving. Between 2000 and 2005 the health workforce reportedly experienceddramatic changes in composition. The AIHW
44found that over this period the number of
pharmacists shrank by 2.8%, and of general practitioners by 1%. In contrast, medical specialistsgrew by 47%. The mix of skills within the nursing sphere also changed. Registered nurses grew by13%, enrolled nurses by 30% and personal care and nursing assistants grew by 90%.
Ample research evidence shows that maintaining the right skill mix is critical to providing qualityhealth care (Example 2).
Example 2
In 2005 the NSW Department of Health commissioned a major study by the University ofTechnology, Sydney, into the workload of nurses in NSW public hospitals
45. This study found that:
patient acuity and the mix of AR-DRGs has increased from 2001 to 2006
skill mix (the proportion of registered nurses compared with other categories of nurses) ismore critical to patient outcomes than hours of nursing provided
the additional hours of nursing care that have been added by the NSW health system areprimarily in categories of nurses other than registered nurses
work environmental factors such as nurses’ autonomy, control over their practice and goodnursing leadership on the ward were statistically significant predictors of job satisfaction.
As well as clinical staff, the health management workforce appears to be severely limited. TheAIHW reports that there are 8,600 health services managers, the number growing by 107% in the5 years to 2005.
44With a total health workforce of 722,000 this suggests a staff-to-manager ratio
of one manager to every 84 staff. In most complex organisations such a span of control ofmanagers would seem inappropriate, and these figures suggest that not all health employees witha management role are captured by these surveys.
The recent history of major health system failures indicates a number of examples of poormanagement decision-making. Despite the importance of management in a large and complexsystem such as health, the health management workforce has not been the subject of anysignificant study recently.
2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 39
Workforce distribution
Rural and remote areas continue to experience shortages in health workers. Long hours, difficultyin obtaining locum replacement, no guarantee of income for doctors funded through fee-for-service, limited professional development opportunities, and lower incomes for the more specialistprofessions all make rural and remote placements less desirable. This is compounded by the factthat most training of health professionals occurs in metropolitan areas, where many will settle andremain. Outer metropolitan areas are also experiencing significant workforce shortages as theirpopulations continue to grow.
Analysis of work output data illustrates the differences in models of care which already existbetween different regions of Australia. Our study of GP supply and demand, reported earlier inSection 2.3 (Case study 4), showed that, after adjusting for other factors, the hours worked per GPwas 6% to 14% higher in rural and remote areas, and higher again for low socio-economic areas.Throughput – measured as services per hour worked – was highest in outer-metropolitan regionsand substantially lower in the higher socio-economic areas.
36
Unequal remuneration leads to the distribution of workers between the public and private sectorsalso being less than optimal, but it does not always imply an overall workforce shortage. Hospitalpharmacy, for example, is experiencing shortages, while in contrast, community pharmacy isgenerally well staffed and exploring ways to develop its role in the provision of primary care.
Training
Training times of up to 10 years for some health professionals and the need for significant on-the-job training means workforce planning is essential. Despite shortages in workforce, a majorimpediment to workforce growth is the lack of clinical capacity to train new staff. The recent studyby the NHWT – conducted in conjunction with PwC – highlighted that substantial additional nursetraining places were required in most states, but clinical capacity to train new nurses issignificantly less than the number of trainees required. Across the industry there is a need forincreased middle management, mentoring, supervision and coaching skills.
46
Infrastructure
Another major challenge limiting the effective delivery of Australia’s health care system is theabsence of appropriate infrastructure at both the hospital and community level.
Hospital design and quality
Many hospitals are working with infrastructure that was not designed to maximise patient flow andcare, and as such they are trying to retro-fit their service offerings with minimal control over facilitydesign and space. The implications of this are wide-ranging and have a major impact on their abilityto deliver patient care in an efficient and safe way.
Issues typically fall under two main categories:
1 The location of departments, wards and facilities; eg proximity of the emergency departmentto support services, location and alignment of surgical and medical wards, movement ofinpatients across facilities.
2 The design of wards and facilities; eg the scalability and flexibility of bed numbers to matchpatient mix to nursing specialty, design and layout of discharge wards, waiting rooms andrecovery rooms.
In addition, the design and layout of a hospital must be supported by efficient processes,technologies, equipment, and effective management and allocation of staff.

2 Key trends in Australia: the imperative for change
40 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Community-based care
From a community health perspective, there is a basic lack of the infrastructure necessary tosupport a system of integrated community networks, backed up by specialist hospital or otherservices as required. Such infrastructure is particularly relevant to mental health services atpresent, but will increasingly be relevant to a wider spectrum of chronic disease and disabilityrequiring care and support. It would need to include:
47
appropriate housing
supported accommodation
rehabilitation facilities
upgraded hospital and clinical services
appropriate networks of support services.
2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 41
2.5 Threats to quality and safety
The quality of health care in Australia is very uneven as a result of fragmented qualityand safety governance mechanisms, poor access and an episodic approach to care.
Australia is considered to have a high quality health care system, rating well internationally, andserving the bulk of the population well. Recent analysis of mortality from causes that werepotentially avoidable through timely and effective health care (amenable mortality), which is a keyindicator of potential weaknesses in health care, indicates that Australia performed strongly whencompared to other countries.
48For instance, between 1997–1998 and 2002–2003, Australia
experienced improvements in amenable mortality even though it was already starting from arelatively strong base. In contrast, the US experienced a small improvement despite its relativelypoor base levels.
49
Australia can take some comfort from this finding. However, the health system’s growing lack of fitwith population health need, as described in Section 2.1, will put greater strain on the system. Theimpact of a system under strain is already evident. A review of the medical records of over 14,000admissions to 28 hospitals in NSW and South Australia revealed that 16.6% of these admissionswere associated with an adverse event, caused by health care management, which resulted indisability or a longer hospital stay for the patient. Of those adverse events, 51% were consideredpreventable.
50
Impact of poor quality and safety
The human, social and economic costs of poor quality health care are enormous. If we includepoor access to health care and medication non-compliance, the calculated costs are even greaterand represent a drain of precious resources.
51For example, our research suggests that the impact
of medication non-compliance on health care costs in the US alone is between $77 billion and$300 billion a year. Although no comparable financial data is available for other countries, theproblem seems equally widespread.
52 53 54
Medication non-compliance means that patients are not controlling their disease and are thereforemore likely to re-enter the health system. This contributes to the financial impact, due to additionaldirect costs such as wasted medications and unnecessary re-testing. The following case studyhighlights the extent and cost of widespread non-compliance (Case study 8).

2 Key trends in Australia: the imperative for change
42 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Case study 8: The extent and cost of medication non compliance
PwC’s research report Pharma 202054
reported the widespread nature of medication non-compliance:
Non-compliance to long-term therapies for chronic illnesses in developed countriesaverages 50%.
55
Non-compliance rates for short-term medicines such as antibiotics is just as poor. In onerecent survey, 22% of respondents said they had omitted doses or failed to complete theirlast course of antibiotics, and the non-compliance rate exceeded 30% in some countries.
56
In the US the cost of non-compliance has been estimated at between $77 billion and $300 billion ayear. While the estimate spans a wide range, the minimum level of estimated cost is significant.
52
53
Attention therefore needs to be given to maintaining and improving quality and safety in thefollowing areas:
public accountability, through public reporting and open disclosure of health careperformance
workforce quality, through clinical supervision, credentialing of staff and appropriate staffmix
embedded evidenced-based and best practice health care delivery across the whole system
integrated health care across the continuum of care (rather than professional silos), tominimise the risk of communication failures and adverse events, as described in Example 3below.
Example 3
A teenager (Mr J) died from meningococcal disease following a brief history of intermittentheadaches, fever, vomiting, stiff neck and, in the later stages, sensitivity to light and dizziness.Although examined by 10 doctors in three hospitals, Mr J’s illness was identified only after a post-mortem examination.
On investigation, it could not be determined whether a correct diagnosis could have been madeearlier had the correct procedures been followed. The following breakdowns in communicationwere identified:
Hospital 1 emergency department did not identify, review and communicate informationfrom Dr A who initially examined Mr J.
Hospital 1 did not follow triage procedures to ensure appropriately trained and experienceddoctors examined Mr J.
Junior Medical Officer (JMO) did not seek a second opinion.
JMO did not provide adequate discharge information to Mr J or his regular GP.
Mr J’s GP did not seek pathology results from hospital 1.
Mr J’s GP referred Mr J to hospital 2 without communicating the full history of treatment.
Hospital 2 initially assessed and treated Mr J on the basis of the GP’s diagnosis without afull clinical assessment to confirm it.
Source: Health Care Complaints Commission (2003) Case studies: Volume 1.

2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 43
Safety and quality policy: from concept to implementation
Again, the needs of the safety and quality agenda have not gone unnoticed in the policy arena.Nine priority programs
57have been identified by the Australian Commission on Safety and Quality
in HealthCare and approved by health ministers for action. These are:
patient charter of rights
open disclosure
hygiene – a national approach to reducing health care-associated infections
patient identification
a national clinical handover initiative
medication safety
accreditation
quantification and benchmarking
using information technology and communication to support implementation strategies.
Jurisdictional support is available to support these quality and safety initiatives, with monitoringsystems in place to continually assess the performance of our health systems. The challenge is toapproach these priority programs from a truly national perspective and to use an all-of-Australiaapproach to ensure widespread and consistent improvements rather than the pockets ofexcellence that we have previously seen.
However, key issues remain concerning measurement of performance, inconsistent datareporting, and governance within a federation of states and a mix of private and public providers.These are discussed below.
Challenges in measuring performance
In 2004, all states and territories agreed to contribute to a national report on sentinel events.58
Inaddition, most states and territories in Australia are now publishing reports on sentinel events andstatewide incidents, and statistics related to the safety and quality of health care in eachstate.
59,60,61The availability of these reports will enable Australia to compare itself with quality and
safety data of other countries62
and review the provision of health care in Australia from aninternational perspective.
While national reporting on sentinel events is an important first step, it does not fully address theissue of measuring performance at a national level. For example, other performance measuresare not available for all states and territories despite the knowledge from international experiencethat reporting of this type is a key driver of quality improvement in individual hospitals.
63Australia’s
health ministers must decide whether all jurisdictions should commit to a level of transparency andaccountability for individual hospitals.
Inconsistent data reporting
While sentinel events are reported on a national basis, states and territories have developed oradopted different incident reporting systems locally. As a consequence, it is not possible to makecomparative data analysis to asses the causes of clinical incidents and use the information todrive national safety and quality programs. The collection of clinical incident data would thereforebe enhanced by the setting up of a national data collection system.

2 Key trends in Australia: the imperative for change
44 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
A national data collection system, assisted by the recently announced national workforce register,could also help with monitoring clinical workforce movements between states and the public andprivate sector.
Quality and safety governance
The fragmentation of the funding structure is replicated in the quality and safety governancemechanisms in Australia. Public and private health care providers work in a range of communityand institutional settings in eight jurisdictions, each with its own governance responsibilities andeach responding to local circumstances and conditions in which health care is delivered. Inaddition, a number of national and state safety and quality bodies exist, all working towardsimproving the Australian health system.
With this combination of resources and the national focus on quality and safety, it is possible thatAustralia already has the capacity to implement effectively the proposed improvement initiatives.However, these bodies have yet to work in a coordinated and collaborative way to ensuresystematic improvements in the health system are made. Indeed, a review of the previous Councilfor Safety and Quality in Health Care in 2004-2005 observed that there was ineffectivedissemination of national safety and quality initiatives due to lack of appropriate relationships withjurisdictions and stakeholders.
64
This situation needs to change and therefore a stronger over-arching governance structure isrequired. For example, an Australian Health Commission, as suggested in Chapter 1, could takeon the role of overall health system governance oversight.

2 Key trends in Australia: the imperative for change
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 45
Summary
There are many challenges in the Australian health system, largely arising as a consequence ofsystem complexity and fragmentation and inadequate incentives. This means that our system ispoorly prepared to deal with demand and cost escalation and changing models of care. Thefollowing require urgent action:
access
quality and safety
data
workforce
infrastructure.
In Chapter 3 we present a plan for action – based on existing good practice in Australia andoverseas – for addressing these issues in both the short and longer term.


National Health and Hospitals Reform Commission PricewaterhouseCoopers | 47
3Priorities for action
3 Priorities for action
48 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Key points of this chapter
In this chapter we provide our views on the future priorities for the health system and how theycould be achieved given existing good practice. Areas for consideration include:
developing an integrated funding approach for specific sub-populations/membership, basedon a robust resource-allocation methodology across the continuum of care
developing a systematic and comprehensive approach to needs assessment to ensure theright health care is delivered at the right time and place for all Australians
building on the lessons learned from major chronic disease prevention and managementstudies to inform a nationwide application of proven approaches
establishing strong, coordinated governance and multi-stakeholder co-operation tointroduce best practice models of care to improve safety and quality
using an evidence-based approaches to workforce management and planning to helpensure the ongoing viability of the system
establishing infrastructure developments which are based on innovative organisationdesign, incentive structures and team-working to maximise the productivity and efficiency ofhospitals and other facilities
encourage an approach to performance management which meets performanceexpectations through a person-centred approach to information, facilitated by personalhealth records and a central longitudinal database, managed by an Australian HealthCommission
Introduction to this chapter
Change – both incremental and revolutionary – is required on a number of fronts, if the Australianhealth system is to achieve its ambition of improving health outcomes by having person-centred,evidence-based models of care operating seamlessly across the full care continuum. In thischapter we provide our views – based on evidence and experience from both Australia andabroad – on the future priorities for the health system and how they could be achieved givenexisting good practice.
We have structured our discussion around each of the layers of governance outlined in Chapter 1and Figure 7 below, as follows:
1 Funding governance: Aligning funding allocation models with incentives
2 Strategic oversight: Understanding need and improving service delivery and quality
3 Market oversight: Addressing key capacity issues – access, workforce and infrastructure
4 Monitoring and comparative oversight: Obtaining fit-for-purpose information management,data and benchmarking

3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 49
Figure 7: Governance cycle
1
2
3
Data
1
2
3
1
2
3
DataSource: PricewaterhouseCoopers, May 2008 © copyright
Appendix B contains more detail concerning the specific steps that are required to deliver keyactivities of this approach from first principles. It can be considered a useful checklist whenimplementing change.
3 Priorities for action
50 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
3.2 Funding governance: Aligning funding allocation models withincentives
Consider introducing an integrated funding approach for specific sub-populations that isbased on a robust resource-allocation methodology across the continuum of care, andincludes both the public and private sectors and aligned incentives.
Australia needs a clear position acknowledging the future demands of the health system, and aplan to fund those demands through an efficient alignment of financial incentives. This implieseither a far more productive partnership between funders than has ever been the case or, morepragmatically, an integration of the funding function in respect of defined population segments tocover the continuum of care.
In developing an overall funding structure it will be important to achieve a set of objectives and toalign those objectives with incentives for all participants in the system. The major participants andthe related objectives are:
payers (including government at all tiers and other fundholders) to achieve a sustainablehealth system, which implies appropriate access and outcomes while achieving value formoney and thus containing costs to a level acceptable to the community
providers (at an organisational and individual clinician level) to be able to deliver care andsupport which enables reasonable and necessary clinical freedom and appropriate rewards,within affordable parameters and which optimises quality
investors to achieve a reasonable return on invested capital, while at the same timecontributing to the necessary outcomes of other stakeholders
individual Australians to enjoy a health system which encourages healthy living, preventsdisease and provides access to necessary care at a cost appropriate to the individual
In recognition of these objectives, we discuss how the overall funding model could be developedmatters in detail below, under the following inter-related topics:
Funding for prevention and continuum of care
Allocating resources
The imperative of efficiency
Role of private health insurance.
Funding for prevention and continuum of care
As discussed in Chapter 2, health system costs are increasing at a rate demanding a higher andhigher proportion of GDP. Clearly, controlling costs while at the same time meeting expectationsand maintaining quality are paramount objectives. Two obvious ways of addressing this ‘costproblem’ are:
investing in cost-effective prevention activities to either curb the onset of disease or mitigatethe development of disease to more severe proportions
harnessing the benefits of care coordination to substitute less costly treatments (egcommunity care) for more costly ones (eg inpatient care).
Both these initiatives deliver the added benefit of not only reducing the overall burden of diseasebut also enhancing people’s quality of life.

3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 51
Prevention and mitigation
There are many examples of funding directed at public health initiatives with a view to preventionor mitigation of disease. Some have been very successful, through a combination of incentives toproviders and public awareness programs through schools, workplaces and the community (forexample, early childhood immunisation of a range of viruses, and workplace sponsorship of fluvaccination). Others have successfully used legislative compulsion, manufacturing andinfrastructure improvements and public awareness, such as the very effective road trafficinitiatives (safer cars and roads, mandatory seat belts, speed restrictions and random breathtesting) and workplace initiatives (occupational health and safety).
Looking forward, there seems to be a strong case for a dedicated funding initiative directed atpublic health and chronic disease management, with a view to reducing the burden of inpatientcare integrated with primary care at a population level. Examples of where this has been eitherrolled out or trialled are:
the Sharing Health Care Initiative65
in Australia, which found impressive results in a range ofchronic disease self-management initiatives
the incorporation of a population health funding component in the allocation of resources toRegional Health Authorities by some Canadian provinces (eg Alberta)
66
the Quality Outcomes Framework, introduced in the UK in 2003, which is the world’s firstpay-for-performance mechanism in primary care and aims to (among other indicators)reward GPs for chronic condition prevention and management activity
the trialling of the Health Benefit Groups and Health Resource Groups concept from the UKin Australian Indigenous populations,
67where populations are considered in terms of their
potential to benefit from certain disease management initiatives.
Care coordination
‘Care coordination’ has been discussed for a decade as an opportunity to achieve better healthoutcomes through substitution and coordination of services across the continuum of care. The firstand second rounds of the Coordinated Care Trials were launched by Australian governments inorder to explore these questions. In particular, the primary objective of CCT2 was:
‘to provide additional benefits to clients and communities through coordination and integration ofcare and effective use of resources for identified populations.’
The ‘effective use of resources’ in this objective was predominantly concerned with the holdingand application of pooled funds by each trial to allow the purchasing of services as appropriatefrom the continuum of care. With respect to this question, the national evaluation of CCT2 foundthat for the mainstream trials, a range of benchmarks were available including Australian norms,fund pooling and control group performance. The key trends to emerge suggested that:
intervention group participants had increased access to primary care services comparedwith the control group participants
had the trials operated for longer, total intervention costs would have fallen below controlcosts, and may have absorbed the costs of care coordination
inpatient utilisation was reduced for intervention participants relative to control groupparticipants.
Throughout this submission we present the other benefits which were delivered to trial participantswithin a broader health outcome framework.
3 Priorities for action
52 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Many other countries and organisations work on the principle of resource allocation across thecontinuum of care, including:
Canada, in which the Federal Government devolves funding responsibilities across thecontinuum of care to the provinces
the NHS system in the UK, where Primary Care Trusts are ultimately fundholders for allservices
the New Zealand system, with its hierarchical allocation from government to District HealthBoards to Primary Health Organisations
the US Health Maintenance Organisations; eg Kaiser Permanente, which has moremembers in the US than the population of any Australian state.
Additionally, much thinking has occurred in the Australian context, including who might be thefundholders and the place of private insurers, in particular in Scotton,
68and the previously
discussed Coordinated Care Trials.
Allocating resources
In the event that sub-populations become funded in this way there is a need to predict theexpected service demand of that group in as much detail as possible. Effectively, given an overallnational health budget across the continuum of care in the tens of billions of dollars, how does onecarve out sub-populations and fund them in a relative sense?
Potential sub-populations
Funded populations could be defined in a number of mutually-inclusive ways, such asgeographically, by disease group, by membership of health insurers or by other special needscategories (eg Indigenous Australians).
In this submission we do not seek to be prescriptive in specifying a vision for funded populations,but offer some ideas as follows:
1 Funding to be allocated as at present from the Commonwealth to the states, including cash-outs of MBS and PBS commitments. A difficulty with this approach is that futureCommonwealth governments could restrict total funding; therefore, a needs-basedapproach is required to replace the current AHCA formulas. Private health insurers couldengage directly with the states in coordinating funding and care for their members, and theCommonwealth private insurance rebate would continue at present purely as a financialtransaction.
2 As for (1), with states identifying sub-populations such as the existing health services toassume responsibility for service delivery across the continuum.
3 As for (1) and (2) but with specific needs-based sub-population groupings for specific healthconditions and/or Indigenous populations. This step, which in some cases may be acrosshealth services, provides the opportunity for enhanced delivery models, the benefits ofwhich are discussed in Section 3.3 below. Further population sub-groupings may comprisethe membership of private health insurers.
4 Alternatively, the Commonwealth could withdraw funding from the states and allocatedirectly to sub-populations. This approach would have the benefit of (a) removing a layer ofbureaucracy, and (b) allowing more flexibility in the formation of sub-populations and theirboundaries or non-boundaries; for example the smaller disease groups, Indigenouspopulations and private health insurers. The disadvantage would be the loss of the localcorporate memory of state health departments, but this could be overcome by giving them

3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 53
an oversight function with respect to public service delivery and budget holders, as inScotton’s Managed Competition model.
68
5 As discussed in Chapter 1, establishing an Australian Health Commission to act as a centralrepository of data and allocation analyses.
Allocation methodologies
There are a range of options regarding how resources might be allocated to defined populationstaking into account their expected service utilisation in an efficient delivery system. These optionsare ideally based on a combination of the population need and prior utilisation, giving anaggregated risk-based expenditure over a period (capitation)
In determining the amount to be allocated to a particular budget holder, there is a variety of‘groupers’ and approaches at a population level as described in a 2003 PricewaterhouseCoopersstudy,
66the main ones being Adjusted Clinical Groups (ACGs) and Diagnostic Cost Groups
(DCGs). There have also been approaches to grouping populations and approaches using theCCT2 national dataset.
69,70Sub-allocations to facilities would continue to use episodic case mix-
based funding as, for example, in the Victorian Health Services allocations.
Broadly speaking, the principal approaches all use the same methodology. This requires a break-down of sub-group populations to a level which is (i) sufficiently granular to allow meaningfuldefinition and differentiation between the groups with respect to their personal characteristics andservice utilisation, while (ii) simultaneously having sufficient volume not to be overwhelmed byvariability. Each sub-group is then given an average ‘capitation’ – that is, expected expenditureover a period, perhaps adjusted for extraneous variables such as age and gender. The sub-population’s resource allocation will then be the sum of each of their members’ capitation amount.
There are many challenges and difficulties that need to be considered in implementing of such asystem, some of which follow:
Significant enhancement of Australia’s health data would be necessary, using linked orlongitudinal unit records.
The ‘groupers’ required to allocate funds on a person or sub-population basis would need tobe comprehensive and thoroughly tested in Australian populations.
Sub-population allocation would need to avoid gaming or cream-skimming to ensure equity.
Sub-populations would need to be large enough to mitigate statistical variability of utilisation(analyses suggest a required sub-population size of perhaps 500,000 for statisticalcredibility and to enable a pragmatic approach to sufficient volume and mix of hospital bedsand service providers).
Even with large sub-populations, some means of equalisation or risk sharing would bedesirable and perhaps inevitable.
71
It would be the role of an Australian Health Commission to develop the allocation method andimplement it accordingly.
The imperative of efficiency
Person-based capitation has the great benefit of allowing sub-populations to be measured interms of financial cost per unit of person-benefit; that is, person-based outcomes can be agreed,measured and compared across providers and populations. Service models can then beconstructed using the accumulated evidence and, eventually, pay-for-performance type contractscan be negotiated with providers, based on person outcomes.

3 Priorities for action
54 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
For some years NSW has used a type of population-based resource distribution formula toallocate funds to Area Health Services, but this approach did not fully achieve its goal of creatingincentives for efficient service delivery. Therefore, at the same time as person-based capitation,the system needs to achieve allocative efficiency of service performance.
In terms of hospital inpatient providers, this implies a continuation of case mix-based episodicmonitoring using AN-DRGs or one of the adaptations; for example, Weighted Inlier EquivalentSeparations (WIES) in Victoria. In terms of other health professionals and ambulatory services,appropriate case mix-adjusted clinical pathways are required; for example, the Australian NationalSub-Acute and Non-Acute Patient Classification System (AN-SNAP).
Role of private health insurance
Australia’s private health insurance system provides faster access to healthcare requiring inpatientmanagement – usually elective surgery, but increasingly more complicated managementinterventions – and usually in private hospitals. It also provides part insurance against ancillaryhealth services, the most significant of which are dental and optical, but which also include arange of ‘lifestyle’ products.
Health insurers satisfy a relatively small, though important, part of the overall funding structure –member contributions comprise about 7% of total health expenditure. However, health insurersplay very little role in the funding and provision of primary care, diagnostics, pharmaceuticals andcommunity care. Moreover, efforts to change the equalisation arrangements so that healthinsurers have greater incentives to manage the health of high cost members have failed.
However, in a reformed funding system as outlined above, consideration must be given to the roleof health insurers.
Potential funding models
One option discussed in recent times is withdrawal of the government subsidy of the industry, andapplication of this rebate funding ($3 billion) to public health funding. In our view this would triggera pernicious membership spiral which would cause the demise of the industry and ultimatelytransfer more demands onto the public system.
However, there is justifiable concern over the ‘value’ purchased by the rebate, considering therelatively narrow role of health insurers across the continuum of care. Therefore, a positiveoutcome for both government and health insurers (and their members) would be to trigger abeneficial membership spiral, whereby the population could identify and see value in an enhancedrole for health insurers to cover more service across the continuum of care. As healthier andyounger members join, the community-rated contribution rate would stabilise, and pressure on thepublic system would be relieved. Private health insurers could engage directly with the states asfundholders in coordinating funding and care for their members.
In the context of this above discussion, it is perhaps also worth considering the relativeattractiveness of some of the key features of health insurance models such as pricing, regulatory,and risk equalisation structure, as set out in Table 6 below.

3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 55
Table 6: Results of health insurance – health care outcomes72
Negative– Neutral Good
––• Ageing reserves/ levelpremium
• Risk equalisation
–––• Community rating
––• Risk sharing
–––• Duplicate
–––• Substitutive
––• Scale
––• Rating / benefit regulation
Incentiveprevention
Care qualityCare costAdministrative
costEquityFeatures of health insurance
Results of health insurance – health care outcomes
Negative– Neutral Good
––• Ageing reserves/ levelpremium
• Risk equalisation
–––• Community rating
––• Risk sharing
–––• Duplicate
–––• Substitutive
––• Scale
––• Rating / benefit regulation
Incentiveprevention
Care qualityCare costAdministrative
costEquityFeatures of health insurance
Results of health insurance – health care outcomes
Source: PricewaterhouseCoopers research. Healthy choices, 2006, p12.
Incentives for private health insurance take-up
If private health insurance were to take a ‘fundholder’ role, their membership would require somefinancial and product support to encourage them to participate.
Integral from a product perspective would be programs and product add-ons (similar to ancillarybenefits) supporting wellness (ie prevention) and chronic disease management (ie carecoordination).
On the financial side, membership engagement in such activities could be supported andsubsidised or rewarded. The government rebate could be more strategically used to influencemembership dynamics, by underpinning community rating and risk equalisation.

3 Priorities for action
56 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
3.3 Strategic oversight: understanding health need to align servicedelivery with quality
Introduce a systematic and comprehensive approach to needs assessment and to qualityand safety, to ensure the right health care is delivered at the right time and place for allAustralians. Apply the lessons learned from major chronic disease prevention andmanagement studies to inform the nationwide implementation of such strategies.
In Australia, the extent to which needs assessments are undertaken in a methodical andcomprehensive way (as set out in Appendix B) is limited. For example, despite the growingincidence of chronic disease, there is limited understanding of the actual prevalence of clinical riskfactors such as obesity. As a result, it is hard to design the appropriate cost-effective serviceswhich also optimise health outcomes.
We therefore consider it ought to be a matter of priority to develop such a systematic approach toneeds assessment. As discussed in Section 3.4, a person-based approach to data andinformation will facilitate this imperative.
Nevertheless, a range of models of care have been developed in Australia to promote bestpractice and facilitate the delivery of the right care, in the right place, at the right time, and ought tobe considered for wider roll-out. These models cross multiple settings and stages in the patientexperience, for example:
chronic disease prevention and management models
improving service integration by implementing best practice models of care
improving safety and quality through better multi-stakeholder co-operation andstandardisation.
Chronic disease prevention and management models
Below we discuss three important contributors to chronic disease prevention and management:
chronic disease self-management
care coordination
workplace wellness.
Self-management
Evidence in Australia and overseas suggests that self management programs can help those withchronic conditions to improve their quality of life by giving them the knowledge, skills andconfidence to better manage condition-related problems. Self-management interventions have thepotential to bring about long-term systemic benefits that could lessen the burden of chronicdisease in Australia.
Activities associated with self-management cover a broad range of areas, including regularphysical activity, healthier eating, and improved social functioning and symptom control. ‘Self-efficacy’ – the belief in one’s own ability to successfully perform health behaviours – is animportant prerequisite for such behaviour change.
The Australian medical profession is increasingly supportive of the concept of self-managementwith its focus on person-centred care. State and territory governments are starting to incorporateself-management programs for consumers into their chronic disease management strategies. In
3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 57
addition, in November 2005, the Commonwealth endorsed the National Chronic Disease Strategyto manage and improve chronic disease prevention and care in the Australian population, whichincluded self-management as a key strategy.
The following case study highlights some of the lessons from the national evaluation of theSharing Health Care Initiative for making self-management work in a sustainable way (Case study9).
Case study 9: Lessons for making self-management work in a sustainable way
An important project in highlighting the effectiveness of self-management in preventing andmanaging chronic disease was the Sharing Health Care Initiative, where demonstration projectsexplored a range of self-management interventions. Most combined a number of chronic care self-management interventions including:
care plans (formal and informal)
training and education on general and more disease-specific aspects of managing chronicdisease as well nutrition and exercise advice
support; eg telephone coaching, buddy systems or regularly scheduled activities to maintainmotivation.
From the national evaluation65
(conducted by PwC), the key features of the programs whichappeared to have the greatest impact on client health outcomes were:
applying flexibility in terms of the intervention itself (ie tailored approaches had the bestresponse) and in the mode of delivery to facilitate ongoing participation
identifying and responding to client needs through the use of appropriate assessment tools
providing appropriate and structured support.
The projects that were best able to meet the challenges of implementing self-management in thecommunity:
were organisationally mature, with good infrastructure and support
had strong relationships with key stakeholders (eg community groups and divisions ofgeneral practice and local GPs)
were very flexible in their approach and design and responsive to client feedback
tailored recruitment and implementation approaches to their target group
built organisational capacity in terms of network partnerships and knowledge transfer.
Care coordination
The evidence base for the value of providing integrated and coordinated services along thecontinuum of care is very strong. A major Australian initiative in this regard was the first andsecond round of Coordinated Care Trials. The key outcomes of CCT2 are described in the casestudy below (Case study 10).

3 Priorities for action
58 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Case study 10: Making care coordination work
The outcomes of CCT273
were examined within four themes:
Improved outcomes for participants: For the Indigenous trials, benefits focused on a range offeatures that made services more accessible and relevant, and progress was achieved inbuilding momentum around health-related self-determination. For the mainstream trials,benefits in self-reported health were evident among intervention participants, includingimprovements in sense of health and well-being, improved satisfaction with services, and adecreased sense of anxiety about health.
Improved outcomes for communities: A strong focus of the Indigenous trials was thedevelopment of population health initiatives alongside and integrated with care coordinationfor manifest diseases. Mainstream trials connected those with chronic and complex needs tocommunity models rather than to acute models of care, with the results suggesting that, givenknowledge and access to a range of community care options, personal and communityresponsibility for health increases.
Improved access: Most participants confirmed that they experienced improved access to awider variety of services. For Indigenous trials, cultural appropriateness of service improved.For the mainstream trials, only intervention participants reported improved access.
Improved participation in health-related decision-making: Qualitative data demonstrated thatall trials achieved improvements in empowerment for participants but the extent ofachievement varied. For Indigenous trials, enablers of access (eg community involvement,culturally appropriate services) also facilitated exposure to health assessment and theconsideration of health issues. For the mainstream trials in general, improvements inempowerment were greater for intervention clients.
Despite the problems experienced establishing the trials, important indicators of success were:
Involvement of primary care providers: Trials that were well integrated with a healthservice/GP division were characterised by greater capacity to implement care coordination.
Roles and skills: Trained health professionals appropriate to their community environmentare needed; where training lagged, delivery of care coordination was undermined.
Governance and management: There was likely to be greater success in the overalloperation of the trial when trials showed early evidence of having both developed andimplemented policies and procedures.
Information management and technology: The inability to achieve goals of electroniccommunication, networking and data flows was a major impediment to the trials and theirability to effectively engage across the board.
The lessons learned from this initiative form the evidence base for many of the key ingredients forthe implementation of truly integrated services. They must not be lost in the new wave of healthreform.
Workplace wellness
Greater collaboration between the public and private sectors in population health is a growingtheme both in Australia and overseas, as governments realise that regardless of any financialconsiderations, they are not necessarily best placed to bring about behavioural change in thewider working population. At the same time, employers in both the public and private sectors havea strong business motivation to ensure the health of their employees.

3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 59
The following case study (Case study 11) describes the measures business leaders canundertake to accelerate the prevention of chronic disease, as outlined in a report developed byPwC for the World Economic Forum.
Case study 11: Working towards wellness: Accelerating the prevention of chronic disease74
With chronic diseases impairing productivity and leading to associated costs, a number ofmultinational companies have recognised the need to use the workplace to promote long-termbehavioural change which will benefit employers, employees and communities.
Business leaders can act to fight the spread of chronic disease through the following measures:
Take the pulse: Assess the health of employees across the world. The metrics will provide abaseline to measure progress.
Embed a culture of health: Build wellness into the mission, business objectives and policiesof the organisation. Create a supportive environment and culture focussed on wellness.
Manage the change: Commit the appropriate resources to improve the health of employees.Engage with employees to develop wellness programs that will produce long-term resultswhich are consistent with the culture and goals of the organisation.
Collaborate and consolidate: Communicate with employees and collaborate with externalparties through public-private partnerships. Establish evaluation and monitoring programs tomeasure changes, outcomes and financial impact.
Lead by example: Executives can encourage and inspire employees and communities byshowing that they are dedicated to living well.
The opportunities offered by effective public-private partnerships in chronic disease preventionand management have yet to be fully realised in Australia, although the Victorian Government’srecently announced WorkHealth initiative provides an excellent opportunity to address this gap.
Some lessons can also be learned from other countries, for example, the UK, which is beginningto address the issue of workplace wellness in a more systematic way. The UK Department ofWork and Pensions commissioned a wide range of research
75to inform the government’s Health
Work Wellbeing initiative, which is a cross-departmental policy aimed at improving the health ofthose of working age.
Improving service integration through best practice models of care
Given the current structure of the health system, no single health service sector (acute state, statecommunity-based, primary-based Commonwealth services or private providers) can provide thenecessary service requirements across the continuum of care.
On the one hand, this has posed a significant challenge to introducing appropriate models of careacross the continuum of care. However, on the other hand, introducing such models of care hasbeen an important vehicle for greater integration across the system, since the emphasis is onprocess simplification and care standardisation while at the same time tackling cultural barriers tochange and improving communication.
Clinical services redesign program (NSW)
NSW Health has funded and facilitated a clinical services redesign program to increase access topublic hospitals across NSW, which has focused on the patient experience as the primary point ofimprovement. Some innovative examples, across the continuum of care, are included in the casestud below (Case study 12).

3 Priorities for action
60 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Case study 12: Redesigning and improving models of care
Examples, across the continuum of care, of the recent work that PwC has undertaken as part ofthe clinical redesign program:
The GP mental health nurse collaboration model,76
which provides access to mental healthexpertise in the primary care setting in collaboration with the Division of General Practiceand the Area Health Service. The purpose of the model was to integrate private mentalhealth services with community services because the existing fee-for-service fundingarrangements offered no incentives for psychiatrists to be involved in case management orto engage with public sector community services in the management of their patients. Anypre-existing examples of integration were based purely on good relationships and goodwilland, as a result, were not a structural part of the service.
The Acute/Post Acute Care Service (APAC)/GP shared cared initiative77
in which the GPand the Acute/Post Acute Care Service (APAC) team work together to manage the patientin the community. The GP’s role is to establish the clinical diagnosis, prescribe, andadminister the first dose of treatment. The APAC team continues the care under theongoing clinical management of the GP. This model ensures that, where possible, thepatient does not need to go to hospital for initiation of clinical care.
An evidence-based model of care for ongoing and complex care needs which wasconcerned with identifying methods for ‘closing the gaps’ between current practice and thebest practice model for chronic care
78(see Figure 8).

3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 61
Figure 8: Proposed model of Ongoing and Complex Care
Patient / Carer Referred
Single Point of AccessAssessment & Intake
APAC PalliativeCare
Ongoing & Complex Care Team
Low Need Medium Need High Need
Community NursingMonitoring & Review
SELFMANAGEMENT
REHABILITATION COMPLEXCASE
SUPPORT
• Lay led groups
• Individualcoaching
• Centre-based
• Home-based
• Community-based
Generic and Disease-specific Modules
• Support GP
• ComplexClinicalmanagement
MODULES• Lifestyle education
– Self-management
– Diet / Nutrition
– Advance Care planning
– Stress management
– Disease-specific education
– Smoking cessation
• Exercise and Exercise Maintenance
• Monitoring and review / follow-up
• Early intervention
• Complex Case Support
• Discipline specific and Medical Specialistintervention
• Carer support
Exacerbation Stable End of Life
Patient / Carer Referred
Single Point of AccessAssessment & Intake
APAC PalliativeCare
Ongoing & Complex Care Team
Low Need Medium Need High Need
Community NursingMonitoring & Review
SELFMANAGEMENT
REHABILITATION COMPLEXCASE
SUPPORT
• Lay led groups
• Individualcoaching
• Centre-based
• Home-based
• Community-based
Generic and Disease-specific Modules
• Support GP
• ComplexClinicalmanagement
MODULES• Lifestyle education
– Self-management
– Diet / Nutrition
– Advance Care planning
– Stress management
– Disease-specific education
– Smoking cessation
• Exercise and Exercise Maintenance
• Monitoring and review / follow-up
• Early intervention
• Complex Case Support
• Discipline specific and Medical Specialistintervention
• Carer support
Exacerbation Stable End of Life
Source: PricewaterhouseCoopers, Ongoing and Complex Care Report, May 2007
WA initiatives
After recognising the success of this program in NSW, WA Health is currently coordinating anumber of initiatives to deliver a system-wide approach to clinical service redesign. WA Healthfaces similar challenges to NSW in terms of an ageing and growing population, increased demandon emergency care and hospital beds, escalating costs, and projected workforce shortages.Changes that have a direct impact on the timeliness and quality of patient care are WA Health’simmediate priority.
Embedding the models of care
The models of care which are now being developed in Australia across multiple settings andstages in the continuum of care (see Figure 8) will not only help to improve the quality and safetyof the health system but also offer a potential solution to some of the structural challenges facingthe system. Nevertheless, the ability to embed such models in day-to-day practice would begreatly enhanced if incentives and other structural impediments to integration were appropriatelyaligned.

3 Priorities for action
62 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Quality and safety
A culture of quality and safety (including equity of access) needs to underpin the entire allocationparadigm.
However, quality and safety are multi-dimensional issues that affect functional areas across healthorganisations, with repercussions for financial performance, clinical/care management, operations,and technology development and integration. As a consequence, risk, quality and safety becomeessential drivers for improving patient. Key elements of embedding quality and safety are multi-stakeholder co-operation and standardisation.
Multi-stakeholder cooperation
Improving quality requires effort from all stakeholders, as illustrated below (Figure 9).
Figure 9: Quality landscape
Consumers
Fundersand
Employers
Pharmaceuticals
Providers
Rewardquality careand healthybehaviour
Manage the supply chainand beyond
Deliverquality care
anddemonstrate
results
Make informed decisionsdifferently
Consumers
Fundersand
Employers
Pharmaceuticals
Providers
Rewardquality careand healthybehaviour
Manage the supply chainand beyond
Deliverquality care
anddemonstrate
results
Make informed decisionsdifferently
Source: PricewaterhouseCoopers, Quality Conundrum, October 2006
In Australia, the Australian Commission on Safety and Quality in HealthCare (ACSQHC) is anexample of a current aspect of achieving a culture of quality and safety. However, further leversought to be available to facilitate quality and safety, including:
linking the ACSQHC to a national governance authority (eg an Australian HealthCommission), which in turn would have control of the national longitudinal dataset
using the available data to make results and outcomes of health providers and fundedpopulations transparent and comparable
extending funding formulas to include incentives for excellence in outcomes, safety andquality.
The value of payment incentives was highlighted in the PwC report HealthCast 2020: Creating aSustainable Future,
6which identified alignment of payment incentives as one of the key features
of a sustainable health system. A follow-up report79
takes this one step further with a discussionon how to structure payment incentives. It also highlights the following lessons for maintaining thebalance of quality, efficiency, and demand through payment reform:

3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 63
As more care is delivered in outpatient settings, appropriate capital planning and financingflows must also encourage flexibility and innovation; eg inclusion of capital costs for case-mix payments in such settings.
Models that integrate both hospital payment and physician payment create mutually alignedincentives.
In countries whose payers are multiplying, there is more potential for confusion aboutquality improvement and incentives, and, as a result, a single set of improvement metrics ispreferred.
Patients are beginning to shop for care at non-traditional venues and locations. Countriesneed to prepare to develop rational pricing for competing in the global market for healthcare services.
As more data from claims, diagnostic test results, patient surveys and electronic medicalrecords becomes available, providers and payers need to use the results to evaluate theirreimbursement systems.
In recognition of this issue, different strategies are required by government and the relevantstakeholders to improve the overall quality and safety culture (Table 7).
Table 7: Strategies to improve quality and safety in health
Sector Objectives
Consumers Gather information and use it to make different decisions; eg choose providers
who deliver high quality care
Providers Enhance quality reporting and performance in response to increasing
consumer, funder and regulatory demands
Funders Offer financial incentives for providers and consumers to improve quality and
lower costs
Employers Get more value by helping employees make better health care and lifestyle
decisions
Pharmaceuticals Improve reputation and performance by managing pre- and post-market
quality
Experience across the world to date is varied, with some segments making more progress inimproving quality than others. For example, HealthCast 2020
6found that government was viewed
as making the most progress in quality improvement in the Middle East, Australia and Asia. In theUS patient advocacy groups rated first, while in Europe and Canada, physicians ranked highest.
Some broader strategies are beginning to be introduced – for example, Patient Choice in England(See Example 4) – and there is growing awareness of the important role that employers can playin health
74although this is not occurring in any systematic way.
Example 4
The Patient Choice program in England aims to improve the quality of health care throughincreased choice of provider (both public and private); that is, competition for NHS services. Inaddition, the Department of Health is seeking to harmonise the provider performance informationavailable to consumers so that they can make informed decisions about where they wish to betreated. This in itself is a complex, ongoing challenge.

3 Priorities for action
64 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Once again, a strong governance environment, such as would be enhanced by an AustralianHealth Commission in Australia (described in Chapter 1), is necessary to establish and coordinatesuch an approach.
Standardisation
Quality and safety standardisation were identified in Healthcast 20206
as critical for creatingsustainable health systems capable of managing costs and providing equitable access to qualityhealth care. In particular, the review and development of standards and practical tools to supportthose who work in the health system was seen as key to promoting the safe management ofhealth care services.
Often the challenge does not lie in the development of best practice protocols but in theirconsistent implementation. Again, the Clinical Services Redesign Program in NSW has providedthe system with the opportunity to address this issue.

3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 65
3.4 Market oversight: addressing key capacity issues – access,workforce and infrastructure
Constantly monitor access and efficiency across the health system and address keypressure points by introducing evidence-based and innovative approaches to workforceplanning/management and infrastructure design.
Access, workforce and infrastructure limitations are the most immediate challenges facing thehealth system in Australia (as exemplified by unfavourable media coverage). And indeed, theirnegative impact on care quality and staff morale should not be underestimated.
In this section we discuss these three challenges and highlight some of the initiatives that havebeen introduced in Australia and abroad to address the problems, including:
clinical service redesign
importance of role redesign and encouraging workforce distribution
best practice principles for infrastructure design and redevelopment and the role ofmultidisciplinary services.
Access
Access to care refers to the ‘ability of people to obtain health care at the right place and right timeirrespective of income, physical location and cultural background’ (National Health PerformanceCommittee 2001).
Access to public hospitals
Public hospitals have a significant influence on the equity of the overall health care system. Whileaccess to public hospital services is important to the community in general, it is particularly so forpeople of low socio-economic status and others who may have difficulty in accessing alternativeservices, such as those provided by private hospitals. Two important areas of stress in the publichospital system have been the availability of beds for elective surgery and waiting times inemergency departments. These were an important focus of the CSRP (Clinical ServicesRedesign Program) initiatives in NSW (see case study below) and now in WA.
The following case study (Case study 13) describes some of the key strategies identified toimprove access block and the patient experience at a children’s hospital.

3 Priorities for action
66 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Case study 13: Improving the patient experience
PwC conducted a project to understand and improve the journey of children attending a children’shospital, through a quantitative and qualitative analysis of elective, surgical, peri-operative, andemergency cases.
Some of the strategies identified to improve access block were:
weekly validation audits for all long-wait patients
streamlining of patient transfer processes
pre-8am completion of discharge paperwork in the paediatric intensive-care unit
early completion of diagnostics with results available in time to inform X-7.45 am wardround
reorganisation of ward rounds to facilitate early identification and decision regardingpatients who are fit for discharge before the morning bed management meeting
a formal campaign to reduce medical absenteeism through infection control education andpractice, reviewing peer support programs for medical staff, and conducting a formal reviewof the rostering process and the process for finding cover
education for staff on the correct labelling, packaging and transportation of pathologysamples
a formal prioritisation process for urgent samples from the emergency department
piloting of a short-stay unit for isolation patients as per the NSW Health Models ofEmergency Care in an existing isolation-capable ward
development of a sub-specialty-based fact sheet for parents and carers.
The Australian Government is also considering increased use of the private sector for electiveprocedures to augment capacity in the public health system. It has set aside $600 million to workwith the states and territories to cut elective surgery waiting lists. The plan will be delivered inthree stages: (1) delivering an immediate blitz on elective surgery waiting lists; (2) structuralreforms to improve elective surgery performance, and (3) dividend payments that are conditionalupon state and territories meeting elective surgery waiting list reduction targets.
The UK has also attempted to reduce waiting times for elective surgery by formally engaging theprivate sector to increase capacity through the Independent Sector Treatment Centre initiative;this is described in further detail in the case study below (Case study 14)

3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 67
Case study 14: Increasing patient choice in England
The Department of Health in England began the procurement of a series of clinical care contractsfrom Independent Sector providers in December 2002 through its Independent Sector TreatmentCentre program. The intention was to reduce patient waiting times for elective surgery byincreasing patient access to, and choice of, health care providers. For example, the goal of Wave1 of the Independent Sector Treatment Centre initiative was to expand existing NHS capacity by250,000 clinical procedures per year over a five-year period through 15 different clinical serviceprocurements covering a wide range of surgical procedures throughout the UK.
PwC advised the Department of Health on many aspects of this program, some of which may beof relevance to the Australian context in the future eg:
how to create interest from the private health care sector in delivering such a service, egprice and brand protection were potential barriers to participation by the private sector in theUK initiative
identifying and suggesting solutions for addressing the complexities of the program’simplementation, including ongoing performance management and ensuring a level playingfield.
But while the lessons learned are of interest, the private hospital market in Australia is much moremature than the UK’s. It is therefore unlikely that such a formal procurement approach would benecessary here. Nevertheless, strong governance in accordance with the principles outlined inChapter 1 is required to ensure that the $600 million planned for augmenting the elective surgerycapacity of the public system is spent and monitored appropriately.
Access to primary and community care
The primary and community health sector is the part of the health care system most frequentlyused by Australians. It is important in providing preventative care, diagnosis and treatment ofillness, and referral to other health care services. However, many rural and remote communitiesface significant shortfalls in the availability and affordability of primary medical practitioners anddentists. In this respect, those of Indigenous background face considerable access barriers.
A recent project developed a number of solutions to address the barriers Indigenous people facein accessing primary and community care. This is discussed in the case study below (Case study15).

3 Priorities for action
68 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Case study 15: Improving access to mainstream services for Indigenous people in NSW
The following statewide solutions aimed at improving Indigenous people’s access to existinghealth care services are planned for implementation over the coming months:
Models of care for Indigenous people: Embed specific requirements for Indigenous peopleinto existing models of care, initially the chronic disease model then other relevant models,including for emergency department, self-management and single points of access.
Integration of Indigenous health and mainstream chronic care: For Indigenous people toreceive a seamless service from a multidisciplinary integrated chronic care team.
Greater Indigenous cultural awareness and cultural sensitivity of services: Establish a‘cultural audit’ of all chronic disease services, (i) to ensure that all frontline staff in contactwith Indigenous people have sufficient cultural awareness and competence to ensure thatservices are delivered in a culturally sensitive way, and (ii) to enable Area Health Servicesto work with NSW Health and AMSs to develop and deliver tailored programs to staff ofmainstream health services.
Justice health linkages: Link Indigenous patients into both Indigenous and mainstreamhealth care services upon release.
Improved access to primary care: NSW Health has commenced solution development withthe Office for Aboriginal and Torres Strait Islander Health, the Alliance of GPs andaboriginal Health and Medical Research Council of NSW on ways in which this challengecan be addressed.
Improved data quality: Improve the completeness of the current data need, and existingdata collections need to be expanded to understand the extent to which Indigenous peopleaccess services.
The issues and potential solutions which influence access to services in the acute, primary andcommunity (including mental health) sectors are closely related to workforce and infrastructurewhich are discussed next.
Workforce
The workforce challenges affecting the Australian health system include overall shortages withincertain professional groups, uneven distribution of health professionals, particularly in rural andremote areas, and limitations in training capacity. These issues are described in more detailbelow.

3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 69
Reduce shortages through role redesign
Opportunities to reduce workforce shortages exist in the redesigning and extending of existingroles.
The following provides an example (Example 5) of role redesign for ambulance officers andparamedics in NSW.
Example 5
Paramedics in NSW sought to move from the historical focus of ‘taking the patient to health care’to ‘taking health care to the patient’.
80They did this by redesigning their roles as follows:
The roles build on the clinical skills and knowledge of NSW ambulance officers andparamedics and are based on an existing and successful UK model (the Emergency CarePractitioner).
They enable appropriately experienced and trained ambulance officers to “make clinicaldecisions and provide advice and extended care/treatment to patients and where possiblealleviate unnecessary presentation to emergency departments”.
Roles were developed along a continuum with the possibility of future development (see Table 8),which may lead to an independent practitioner-level paramedic. Specifically, the project focuseson improving knowledge of common non-acute presentations, advanced skills, enhancedpharmacology, enhanced clinical risk assessment and clinical decision making protocols.

3 Priorities for action
70 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Table 8: Expanded care continuum – current project and possible future thinking
Current
practice level
ASNSW Project Possible future directions
Ambulance
officer /
paramedic
Expanded decision
making
Extended care
paramedics
Transitional
psition
Emergency care
practitioner
Traditional treat
and transport to
emergency
department
Traditional
vocational
ambulance service
education
Protocol based
Transport to
emergency unless
explicit patient
refusal
Levels 3 (Primary
Care) to 5
(Paramedic)
Provision of advice for
non-transports with
some referral pathways
Mechanism for
improving patient safety
and enhancing clinical
advice for those
patients who are not
transported (approx
12,000/mth)
Provides patient
structured advice
regarding risk of non-
transport
Able to advise patient of
alternate care pathways
but require patient
consent for non-
transport to ED
Not able to discharge
from care
One week additional
ambulance service
education
Extended
assessment,
treatment and
clinical decision
making
Additional referral
pathways and
advanced
assessment
Able to transport to
more appropriate
care pathways (eg
GP, GP collocated
clinic, APAC, X-
Ray, pathology)
Able to treat, re-
visit, and follow up
patient discharge
from care
Eight weeks
additional education
with clinical
placements and
hospital/university
clinical school
Title, position
and scope of
practice to be
determined
Further
expansion of
role and
diagnostic
ability
Postgraduate
education
Regulatory
requirements
determined
Title, position and
scope of practice
to be determined
Autonomous
practitioner
Could be nursing
or paramedic
Qualified in
primary care,
acute care and
pre-hospital care
Education to
Masters level
Self-regulatory
framework in
place
Improving the distribution of health professionals
A number of initiatives have been developed to improve the distribution of health professionals,particularly in rural and remote areas. These include:
minimum income guarantees for private practitioners working in rural and remote areas
an increase in the minimum training, which must be undertaken in rural and remote areas.
Other strategies are likely needed, and ideas proposed by those in the health sector include:
an increase in trainees originally from regional areas and an increase in education andtraining opportunities outside the major capital cities
greater recognition within the medical profession of the value of rural and remoteplacements, to ensure students who undertake these placements are not disadvantaged
stronger financial incentives for health professionals who work in rural and remote areas; egeliminate or reduce HECS debt if they stay for more than five years.

3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 71
The following case study (Case study 16) is an example of recent work undertaken to improve thedistribution of health professionals.
Case study 16: Increasing the number of GPs working in outer metropolitan areas
PwC was asked to evaluate the appropriateness, effectiveness and efficiency of programs aimedat relocating, training and retaining doctors from in inner-metropolitan areas to outer-metropolitanareas.
The incentives offered by the programs, which included financial assistance, Medicare rebatesand access to clinical experience and training, were assessed as appropriate, effective andefficient. For example:
total doctors moving to or remaining in outer metropolitan areas was 293, almost double thetarget
15 specialist trainees received training
384 registrar placements were filled.
Our evaluation also found that the following strategies would be effective in increasing the numberof health professionals working in outer metropolitan areas:
increasing the size of the relocation incentive
improving communication, information flow and transparency, particularly regardingeligibility for programs
targeting doctors currently practising in inner-metropolitan areas; recently fellowed doctorsand registrars to work in outer-metropolitan areas.
Training
Expanding training to other care settings (eg private hospitals) provides opportunities to enhancethe capacity to train new health professionals. Case study 17 describes the findings from a recentstudy undertaken by PwC for DoHA on the costs, benefits and potential barriers associated withextending the training approach for medical specialists.

3 Priorities for action
72 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Case study 17: Reviewing the training approach for medical specialists
The vocational training of medical specialists (ie PGY3 and later years leading to collegefellowship) occurs mainly in major metropolitan tertiary teaching hospitals across Australia.
However, over the past generation there has been a significant expansion of medical specialistwork into other settings of care and, in some cases, major migration of specialist treatment out ofpublic hospitals and into these other settings.
Such changes have led to a broad view across health system leaders that the training ofspecialists should be expanded into other care settings to ensure that newly trained specialists aretrained across the full spectrum of presentations. For example, in psychiatry, providing training inother care settings (eg private practice and community settings) ensures access to cognitivebehavioural therapy, psychoanalysis and consultative treatment for high-prevalence low-severityconditions such as depression and anxiety.
Changing the training settings can also result in an increased supply of specialists in the long termby increasing specialist training places now. More specialist training places means more medicaltrainees into the hospital system initially, noting that undergraduate and PGY1 and PGY2 doctorsare an important part of the public hospital workforce.
Overall, therefore, the move to review and extend training opportunities for medical specialists –and other health professionals where appropriate – should be supported.
Infrastructure
It is evident that there are a number of infrastructure issues affecting Australia’s ability to deliverquality person-centred care. These need to be taken into consideration when trying to improve thepatient experience within an acute facility. In recognition of this, the Australian Government hasjust announced the creation of a $10 billion Health and Hospitals Fund in its first budget.
Acute facility design
There are guiding principles that should be adhered to when looking at the design and layout ofacute facilities.
First, the facility and wards should be designed to take into consideration the patient case mix andthe patient requirements. Paediatric facilities, tertiary facilities and individual wards anddepartments can all be designed to enhance the patient experience and to consider the needs andrequirements of a diverse group of patients, carers and families.
Second, the infrastructure should be designed to deliver an effective and efficient patientexperience and reduce the burden and stress on existing hospital resources.
Using LEAN principles will provide a patient-centric focus, eliminate wasteful and unnecessaryactivities, and enable processes to flow. The hospital should be designed so that patients aretaken through services, rather than being pushed and having to wait in queues. Seamless patientexperiences should be designed so that patients move from one area to another with minimaltransportation and motion and with minimal waiting time between services. At the same time, thefacility’s interface with the primary and community care setting ought to be considered.
Much of this thinking has been incorporated into the NSW Health Clinical Service RedesignProgram and is being demonstrated in the $700 million redevelopment of the Royal North ShoreHospital and is planned for the review of the WA hospital system.

3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 73
Multidisciplinary clinics
The Australian Government has set aside $275 million for 31 GP super clinics to be establishedwithin rural, regional and outer-metropolitan communities, with the purpose of providing familieswith more access to a range of health services. The GP super clinics will bring together GPs,nurses, allied health professionals, some specialists and other health care providers to deliver arange of health services tailored to meet local health needs and priorities. It is intended that theclinics will complement and enhance existing health services in their local areas, includingproviding teaching rooms and facilities to enable trainees to undertake on-the-job training andclinical placements.
This move to co-located multidisciplinary working is consistent with developments in New Zealand,the UK and the US, and there are already some examples closer to home; for example, the InalaPrimary Care Centre in Brisbane and the Cessnock Uni-Clinic in NSW.
However, perhaps the most interesting domestic model to consider in this context, from whichsome lessons could be applied to the rest of the Australian population, is the Indigenous medicalservice, as highlighted in the following example (Example 6).
Example 6 Features of Aboriginal Community Controlled Health Services (ACCHS)
An Aboriginal medical service is a primary health care service initiated and operated by the localAboriginal community to deliver holistic, comprehensive and culturally appropriate health care tothe community that controls it.
In keeping with the philosophy of self-determination and the need to provide effective and efficienthealth care to Indigenous people with limited resources, features include:
services forming a network, but each is autonomous and independent, both of one anotherand of government.
community controlled, through a locally elected board of management
large multi-functional services employing several medical practitioners and providing a widerange of services. For example, Townsville Aboriginal and Islanders Health Services(TAIHS) has over 150 employees providing medical and dental care, social and emotionalwellbeing services, a youth shelter, a volatile substance-use service, crisis accommodationand child protection services. The medical unit at TAIHS provides comprehensive primaryhealth care, with a staff of 36, including nine general practitioners, four registered nurses(three Indigenous), six Aboriginal health workers, a dietician and a psychotherapist. Inaddition, they have a number of visiting specialists and allied health professionals
smaller services without medical practitioners, which rely on Aboriginal health workersand/or nurses to provide the bulk of primary care services, often with a preventive, healtheducation focus
GPs who work within these services on a salaried basis.
The integrated primary health care model adopted by ACCHSs is in keeping with the philosophy ofAboriginal community control and the holistic view of health that this entails.
In addition, observations from a recent literature review81
and other research82
are of growingevidence that the more organised physicians are (eg those in large group practices or integrateddelivery systems), the more likely they are to deliver efficient, high quality care. In this context,success factors for improved quality and efficiency include:

3 Priorities for action
74 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Realigned incentives: Streamlined delivery is much less achievable within a fee-for-serviceenvironment which rewards volume over value.
Strong physician leadership: Many of the best-known integrated delivery systems and largemulti-specialty medical groups were founded by strong and charismatic physician leaders.As a minimum, active engagement of GPs and their professional organisations isimportant.
82
Organisational culture: Shared vision, values, and a sense of mission regarding stewardshipfor both individual patients and populations is critical to performance.
Governance: This refers to an organisation’s ability to set goals purposefully, implement aplan, and achieve those goals in an accountable and transparent way. Someone orsomething (eg a board of directors) can cause the organisation to act collectively andintentionally to improve quality or efficiency. Research shows that groups with externalincentives for improving quality – financial or otherwise – tend to score better on qualityindices.
Selection and workforce planning: In organised delivery systems, leaders can selectproviders for participation, excluding those who do not meet standards. Organised systemsalso can be more intentional about the mix of providers they include (eg primary vs specialtycare, physicians vs ancillary providers), targeting them toward the population's healthneeds.
In addition, the need for sufficient and appropriate infrastructural support, including informationtechnology and quality systems, cannot be underestimated (which is considered in more detail inSection 3.4).
82
Public/private interface
Finally, public-private partnerships provide an opportunity for substantial capital redevelopment inthe health sector if they are shown to provide value for money and meet the needs of the relevantpopulation; an example of this is the proposed redevelopment of the Royal North Shore Hospital(see Case study 18).
Case study 18: Proposed redevelopment of the Royal North Shore Hospital #2
Based on a value-for-money assessment, the NSW Government decided to procure the requiredfacilities and associated non-clinical support services for the Royal North Shore Hospitalredevelopment under a public-private partnership (PPP) model, representing the largest healthPPP project in NSW’s history.
In addition to the core hospital, the project also provides for significant commercial opportunities tobe incorporated into the proposed project commercial structure; for example, the operation of acar park with approximately 2,500 spaces, extensive retail facilities, and room for commercialproperty developments.
The project is extremely complex, and the challenge has been to enable NSW Health to deliverthe required high quality health services from the new facilities within the affordability limit. PwChas assisted in this through the development of the benchmark cost model and continues toadvise on the project.

3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 75
3.5 Monitoring and comparative oversight: fit-for-purposeinformation management, data and benchmarking
Match performance management of the system to performance expectations through theefficient and effective collection and use of data including introducing a person-centredapproach to information, facilitated by personal health records and a central longitudinaldatabase.
“From being an early leader in its ability to manage and use health information, Australia is nowincreasingly falling behind comparable countries such as the UK, Canada and USA.” (AHHADiscussion Paper – Information Management, 2008)
In this same paper it is estimated that $10 to $20 billion (probably closer to $20 billion) will berequired over the next 10 to 15 years to deliver a fully planned and implemented system inAustralia.
In the meantime, our health data content requires attention, and its collection, storage andaccessibility present multiple barriers to constructive reporting and system monitoring. All ourmajor systems are set up as provider-payer and/or episodic service repositories, rather than‘person-centred’ information sources. As a result, we are unable to match the performancemanagement of the system to performance expectations.
Making a change will require changes to health care strategy, clinical and business processes,and the culture within health care.
Australia’s data vs the ideal data
Health care is in a state of data overload. It urgently needs to be able to extract, integrate andshare the right information to the right people at the right time. In our view, there are many areasfor improvement in Australian health data quality and access. Taking account of the political andfinancial realities, the table below provides comment for each of what we would define as ‘featuresof an ideal data system’.

3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 76
Table 9: Features of data
Desired feature Explanation Australia’s position (our experience)
Respect and protection ofindividual privacy
Information on the health care system utilisation of individuals isextremely sensitive. Any data system should have securesafeguards to protect the privacy of individuals.
The protection of individual privacy is paramount when considering access to healthinformation. This is often an obstacle to analysis and planning.
Federal and state legislation needs to be aligned to simplify system implementations andwhat individuals need to know. Individuals also need to be educated about the currentrisks to their information and the benefits of being able to share their information with theircarers.
Speed and nature ofaccess to approvedpersons
It is essential that access to data does not impede the nature andextent of investigations necessary to develop health fundingpolicy, and to study the utilisation of health care.
The possible investigations in health planning have been significantly delayed andimpeded by data issues.
Definition and separationof responsibilities (egacute, Home andCommunity Care [HACC]etc)
Components of health data should be defined to correspond withresponsibility of funding and service delivery. There should beclearly defined and described ownership and custodianship ofthese components of health data.
In most cases, we are able to isolate the location and ownership of the more significanthealth datasets, and work with them. However, there are often problems withunderstanding the links and limitations across components.
Consistency of definitionsacross lines ofresponsibility
To facilitate links between components of health data, definitionsof the main parameters should be clearly defined and consistent.
In many instances there are inconsistent definitions across datasets. This requiresmapping, with resultant loss of data and uncertainty of the mapped result.
Coverage andappropriateness ofinformation
The aggregate of health data should be well planned and havecoverage which is consistent with the direction of health policy.
The overall aggregate of health information is overly focused on hospital, medical andpharmaceutical treatments. These do not cover the care continuum.
Completeness ofcoverage of populations
For each component of health care utilisation, there should be auniversal unit record database covering all recipients of care.
The main shortcomings in this area are in respect of pharmaceuticals, which operates ona family and safety net basis, and community care, where government-funded servicesare recorded on a wide variety of databases and summarised through HACC surveys.
Person-based tracking To understand the demand for and use of health services, healthdata should be maintained on a per-person rather than a per-service or per-episode basis.
Almost universally, Australia’s health datasets are maintained on an episodic basis,limiting the analyses available for health funding and service delivery.
Unique linkages To describe clinical pathways and the continuum of care,appropriate data links should be possible on a unique identifierbasis across the component datasets.
While links are being developed in most jurisdictions, we believe successful data linkageis some way off, particularly in view of limitations on access.
Information is shared andable to be used
Information will need to be retrieved from various locations andimported into systems other than the ones that captured theoriginal information.
Some standards and protocols are under development; however these are not alwaysfollowed and implemented by the different states and health systems (both public andprivate).

3 Priorities for action
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 77
A major strategy is needed to approach this ideal situation, and immediate, short-term and long-term solutions are required.
Immediate action
In order to retrieve momentum, immediate steps include:
Acknowledge that past efforts to achieve this end through partial solutions have beenunsuccessful, and that the current initiatives are perceived to be experiencing difficulty, arefragmented, and suffer a lack of buy-in.
Acknowledge that the lack of coordination of efforts, mandating of standards, harmonisingof legislation and involvement of clinicians has impeded progress, wasted efforts andslowed progress.
Accept the national strategy which is to be delivered mid-2008 and start working towardsthe stated goals. eHealth is a long-term initiative – aspects of the strategy may change overtime but some momentum is better than trying to get absolute consensus before taking anyaction.
Identify existing initiatives underway, and do a stocktake of progress, difficulties andprognoses for an outcome which might contribute to a national plan (and how).
Establish standards ensuring that each individual effort by the states and private providerswill inter-operate down the track – it is recognised internationally that lack of standardsmakes interoperability and connectivity nearly impossible.
Determine how best to fund the investment needed in technology, ensuring that those whobenefit most will contribute to the costs.
Begin patient education, helping address privacy concerns and helping patients understandthat they can and do own their health and related information.
Long-term goals
Understanding that ‘the vision’ is currently being developed, the following steps are needed toresume the journey to an integrated health information, data and benchmarking system:
Acknowledge and agree on the need for an Australian central longitudinal health database,with person-based health records.
Develop a strategy to attain the goal of a central database, which is useful and accessible,within privacy requirements, and which may need to be revisited in terms of detail, whileprotecting the overall principles.
Agree on the principle that each person’s longitudinal health record will provide a full andcomprehensive record of health status and health service utilisation across the continuum ofcare.
Develop a plan to merge the major existing health and community care datasets (MedicareAustralia, inpatient statistical collections, emergency department and ambulatory careinformation, HACC Minimum Dataset).
Develop a plan to define the data elements required across the continuum of care, and inparticular in primary care, where diagnosis and health status is totally absent from currentrecording.
Develop protocols for reporting and benchmarking across the continuum of care (ie person-based analysis), and across the continuum of providers (ie provider and service-basedanalysis).
Develop of protocols for access to the central database in such a way as to encourage andfacilitate, rather than impede, research and analysis.

3 Priorities for action
78 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Understand that the private sector (technology organisations) are willing to invest in thissector, however when there is a perceived or real lack of commitment by government tomake the necessary changes, the private sector may be less willing to invest. For example,the fact that NEHTA has funding to develop the Unique Health Identifier, but funding for roll-out has not been agreed, provides uncertain messages to organisations that need to investto develop appropriate interfaces.
To achieve such a vision will require a significant cultural shift within the health system andsubstantial changes in clinical and business processes.
Short-term imperatives
In the meantime, progress is required to help the health system move forward recognising thecurrent limitations on data content and access.
Such progress can take advantage of the deep and rich episodic information which is stored, butnot fully utilised on an episodic basis.
An intermediate plan such as the following could be considered, in parallel with the long-termvision, and capitalising on the immediate actions. In particular, after existing initiatives (includingbarriers) have been identified, and a stocktake of progress has been done (as described above),agreement could be sought to direct these initiatives in a common direction, and with commonobjectives.
Such objectives might include:
Investigate ways in which practical statistical or direct linkage keys could be made morereliable and accessible in linking our major datasets. As with above, privacy requirementsmay need to be revisited in their detail, while protecting the principles.
With linked major datasets (MBS, PBS, hospital inpatient, emergency department,community care) it becomes possible to build a picture of service utilisation on a per-personbasis, which is at least a first approximation to understanding health need.
Provide access to these linked datasets to approved researchers and representatives ofboth Commonwealth and state governments, so as to encourage research and informationreporting.
Develop a more timely and comprehensive set of benchmarking and monitoring reports.
Use the efficacy and acceptance of these reports to feed into the longer-term vision
An immediate action should be the establishment of a Health Commission (eg the AustralianHealth Commission) or body to manage this process within the above pragmatic parameters. TheCommission should be responsible for IT governance, ensuring alignment of regulations, securityand privacy, and clinical process flows.
Summary
We are fully aware of and acknowledge the magnitude of the issues facing the Australian healthsystem and of the changes required. However, we consider it vital to contribute to the debate in aconstructive way.
In this chapter we have provided insights and solutions into how to achieve person-centred,evidence-based models of coordinated care based upon our experience in Australia andinternationally. We hope that the practical examples of innovation and the structure for making ithappen that we have provided can make a difference in the new reform environment.

National Health and Hospitals Reform Commission PricewaterhouseCoopers | 79
Appendices

3 Priorities for action
80 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Appendix A Addressing the terms of reference
In this submission we have carried out a practical assessment of Australia’s health system andrecommended solutions to help address the NHHRC’s terms of reference. The table belowpresents the terms of reference and the relevant section(s) in this submission that address eachone.
Table 10: Addressing the terms of reference
# Terms of reference
Where we have addressed
this in the submission
a Reduce inefficiencies generated by cost-shifting, blame-shifting and
buck-passing.
Sections 1.1, 1.2, 2.2, 2.3,
2.5, 3.2 and 3.5
b Better integrated and coordinated care across all aspects of the
health sector, particularly between primary care and hospital
services around key measurable outputs for health.
Sections 2.3, 2.4, 2.5, 3.2,
3.3, 3.4 and 3.5
c Bring a greater focus on prevention to the health system. Sections 2.1 and 3.2 and 3.3
d Better integrated acute services and aged care services, and
improve the transition between hospital and aged care.
Sections 2.1 and 2.4
e Improve frontline care to better promote healthy lifestyles and
prevent and intervene early in chronic illness.
Sections 2.1 and 3.3
f Improve the provision of health services in rural areas. Sections 2.4 and 3.4
g Improve Indigenous health outcomes. Sections 2.1 and 3.4
h Provide a well qualified and sustainable health workforce into the
future.
Sections 2.4 and 3.4

National Health and Hospitals Reform Commission PricewaterhouseCoopers | 81
Appendix B Checklist for action
In Chapter 1 we introduced the governance cycle which provides a robust strategy forimplementing a person-centred and evidence-based approach to health system reform. PwC hasexperience in helping overseas governments to implement the governance cycle. In this Appendixwe share some of our key learnings from these implementation projects and provide a checklist toassist with implementation in Australia.
A similar governance cycle underpins the reforms to the UK’s National Health Service. In the casestudy below is an example of PwC’s experience in this field (Case study 19).
Case study 19: Developing a world class commissioning capability for the South Central StrategicHealth Authority, UK
PwC was appointed by the South Central SHA to help develop a world-class commissioningcapability, which would help to improve the lives of the four million people living in their catchmentarea.
The five measurable outcomes from this project were to:
1 Help create a strategic commissioning plan for each Primary Care Trust (trust) that setslong-term goals and allows them to measure their success in achieving them.
2 Help create an operating plan for each trust, which develops the Local Delivery Plan in anaffordable manner on a year-by-year basis.
3 Help create a people capability and capacity plan for each trust, which identifies areas forimprovement so that strategic and operating plans can be successfully executed.
4 Segment the commissioning cycle so that the trust can individually and collectively assessbenefits of scale – both within the NHS and working with partners.
5 Specifically identify areas for independent sector involvement – for individual trusts and forthem collectively.
The concept of world-class commissioning and the principles of the governance cycle have beenused to develop a nationwide program of change in the health system in Britain. In addition, arecent development has seen the UK Department of Health engage PwC to develop theoverarching system management framework which builds upon the governance cycle for thewhole of the NHS.

3 Priorities for action
82 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Figure 10: Governance cycle
1
2
3
Data
1
2
3
1
2
3
Data
Source: PricewaterhouseCoopers, May 2008 © copyright
Below is a list of the key actions necessary for the successful implementation of the abovehighlighted activities.
B.1 Plan
Overall, planning requires robust health forecasting tools and methodologies thatunderpin all aspects of the planning cycle.
1 Develop appropriate forecasting models for the health system and review robustness ofexisting forecasting models and data. Show clear, logical assumptions and their subsequentimplications through scenario testing. Describe weaknesses and strengths in forecastingcapability and data and plans for improvement.
2 Investigate the implications of health system forecasts for:
a staff numbers and types: medical and non-medical; clinical and non-clinical
b venues, facilities, equipping implications
c provider effects
d capital build.
3 Use a number of data sources that include Australian and international evidence.

National Health and Hospitals Reform Commission PricewaterhouseCoopers | 83
Assess need and current services
Strategic priorities to inform service provision and funding decisions should be based onappropriate, robust, needs-based assessment rather than on demand or supply
1 Needs assessments should be undertaken at each relevant level of the population,including the entire defined population, appropriate sub-group analysis (condition-based,ethnicity, service utilisation, socio-economic status, geographic location), and at anindividual level in unique and rare circumstances.
2 Needs assessments should test expectation against reality and identify which populationsare accessing services and where unmet need may exist.
3 Establish a comprehensive strategy for future health needs assessment, including plansand reasoning for which assessments may need to be prioritised due to time or financialconstraints.
4 Demonstrate effective communication between public health teams, service planners andfinance in developing needs assessments.
Planned strategic interventions should demonstrate clinical and cost effectiveness,especially considering outcomes that matter to patients (ie outputs rather than inputs)
1 Review applicability of available evidence for proposed services/interventions for relevantpopulation(s).
2 Review appropriate targets/guidelines/protocols/model patient pathways and use models ofbest practice in service options (eg length of stay, outcomes, hospital vs. community vs.social care).
3 Collect data on measures that matter to patients, including patient quality of life measures.
Define services and analyse gaps
Demonstrate thorough understanding of how current services meet otherwise assessedhealth needs
1 Clearly articulate the patient value (eg quality, cost, access, error rate) of services currentlyprovided.
2 Review applicable performance indicators.
3 Review integration of services among different service providers.
4 Identify where current activity may need to be increased or refocused on other populations.Identify areas of misuse.
5 Understand allocation of resources and related activity/outputs.
Undertake a robust and comprehensive gap analysis in the context of eliminating misuse,overuse and under-use
1 Investigate root causes of the gaps in services to compare current performance with itspotential, including:
a process issues – differences in the components of the practice itself
b operational issues – differences in how the policies and procedures are organised
c structural issues – differences in the physical or logistical set-up.
2 Review current activity and services against best practice clinical/public health guidelines.

3 Priorities for action
84 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
3 Pinpoint areas for improvement.
Decide priorities
All decision-making clearly incorporates an ethical framework; decisions are transparentand clearly defensible to all stakeholders
1 Develop and apply an ethical framework to strategic decision making to ensure consistencywith agreed values.
2 The ethical framework should be evidence-based as demonstrated by inclusion ofappropriate study designs; economic evaluations (cost effectiveness, cost utility, costbenefit, cost consequences); and applicable across the continuum of care.
3 Decision-making process and underlying values are clearly stated in a code of practice (toimplement an ethical framework) which:
a is transparent and demonstrates accountability
b provides a clear and consistent framework to inform strategic decisions (helps formbasis and support for investment, disinvestment decisions).
Develop risk management strategy
Develop a formal, systematic and robust approach for corporate risk assessment that isclear and defensible
1 Risk assessment is inclusive and comprehensive where risk is defined, rated and mitigationmethods are established. Risk may be categorised as opportunity, uncertainty, or hazard(eg adverse event).
2 Include qualitative and quantitative analysis of major changes which are likely to affectservice decisions (eg expensive drugs or procedures, rare events such as pandemics,policy changes and global health trends). Quantify impacts through scenario analysis andqualitative frameworks or scorecards.
3 Complete a comprehensive environmental assessment and horizon scan including possiblepolitical, economic, social, and technological developments/risks (Table 11).
Table 11: PEST analysis
Political Economic
Regulatory bodies
Government term and change
Funding, grants and initiatives
Pressure groups
Competitors
Suppliers
Provider changes
Employment rates
Policies
Government funding
Social Technological
Lifestyle and disease trends
Demographic trends
Skills availability
Public attitudes and opinions
Technological development
Research and funding
Information and communications
Innovation potential

National Health and Hospitals Reform Commission PricewaterhouseCoopers | 85
4 Develop a plan for managing identified risks. Options for managing identified risk include:
a changing the distribution of the underlying risk through changes in services (egdisease management programs, shifting care from emergency department to primarycare)
b diversifying the risk (eg increase the number of providers or appropriate services)
c transferring the risk (eg to private health insurance/funder, health care provider)
d sharing the risk (eg with other funders).
Assess strategic options
Develop an innovative, comprehensive, strategic plan for purchasing health care,considering a range of options for provision before devising a final strategy
1 Consider outcomes and outputs, required inputs (relative investment, workforce andinfrastructure) and provider options across entire care value delivery chain for each healthpriority and target.
2 Create an overarching plan for the delivery of health and health care.
3 Evidence consideration of innovative providers (eg local employers), new care pathways,formation of new partnerships, and focus on prevention where applicable.
4 Use a framework covering benefits, costs, investment and risks to assess the range ofoptions under consideration. The framework should cover:
a each option’s attributes, such as short-, medium- and long-term cost implications
b assessment of the how the option serves to move the trust towards its stated strategy
c assessment of the option’s patient value
d assessment of the level of difficulty of implementation, potential timing, barriers(structural, staffing, etc) as well as other assessment criteria.
5 Assess, discuss and agree all options against the chosen criteria in order to establish whichoptions best fit together and are aligned with the stated strategy:
a model the shifting of costs and increased benefits
b demonstrate a ‘car park’ for ideas and programs that may be implemented in thefuture and provide detail on their implementation (eg models of shifting services).
6 Choose a set of programs that is meaningful in light of health needs, current activities,service gaps and expenditures.
7 Consult widely and obtain key stakeholder buy-in (eg local patient groups, media, localgovernment, politicians and clinicians) on chosen strategy.
B.2 Execute
Contract implementation
Contract implementation strategies and processes are comprehensive, robust andensure provider accountability
Contract implementation strategies ought to include:
1 A clear and deliverable timetable for planning, drafting and negotiating the contract(s)including:

3 Priorities for action
86 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
a identification of each of the steps and associated timing in the development of eachcontract through to its execution
b where the procurement is competitive, the timeline should not only comply with goodcommercial practice but also applicable procurement rules
c identification and allocation of sufficient financial and qualified human resources tothe necessary tasks.
2 Sufficient and capable resource allocated to drafting and negotiations.
3 Plans in place to fill potential skills gaps in contract and performance managementexperience.
4 Clearly stated and realistic objectives, preferably prioritised, which are able to guide draftingand negotiation decisions.
5 Realistic and measurable targets for achieving those objectives.
6 Regular reporting mechanisms against the timetables set out.
7 Demonstration of how plans for health needs, budgeting and demand management are tobe reflected in the contract(s), particularly in terms of:
a volumes and pricing
b performance incentives and penalties (including KPIs)
c default and termination thresholds (including KPIs) and provisions
d contract change provisions
e contract management protocols including information requirements, notificationrequirements, and dispute resolution provisions.
8 Ensure KPIs in the contract are aligned with the performance management system toensure that the information is available to monitor the contracted measures.
9 Where new providers (eg from the private sector) are to be invited to tender for a contract,allow for additional time and resources, in addition to the procurement requirements, toresolve possible commercial issues, contract security and level playing field issues.
Provider development
The purchase of health services supports providers (either new or existing) in generatingideas and formulating realistic plans to improve performance or reduce costs, which ismutually beneficial
1 Provider development includes care pathway (re)design and demand management, supportfor provider improvements or introduction of new providers to deliver the services required.This should also include supporting providers in decommissioning of services whereappropriate.
2 The following activities ought to exist for effective provider development:
a complete stakeholder mapping
b understanding the complexity of care pathways including discharge
c working with suppliers
d communities of practice (ie good practice being used).

National Health and Hospitals Reform Commission PricewaterhouseCoopers | 87
B.3 Manage
Managing performance
The purchasing authority has a strategy for regularly monitoring strategic measuresthrough informative, quantitative metrics and outcomes measures and indicators
1 Have clear consensus on KPIs and indicators to be measured and reasons for use iepatient value.
2 Use the best available data sources and try to ensure consistency.
3 Individual indicators (process, clinical, outcomes measures) demonstrate clear input andimpact on greater goals and targets.
4 Agree upon a policy for rewards and remediation.
5 Establish an escalation procedure for when board/executive ought to be informed ofproblems.
6 Have a feedback mechanism to improve provider performance that in turn informs theplanning phase.
Provider performance is managed in a way that encourages providers to deliversustainable best value
1 Have or plan to put in place sufficient financial, technology and human resources to supportcontract and performance management.
2 Implement deliverable, targeted and separate task plans for monthly performancemanagement cycles as well as for quarterly and annual performance management cycles.These plans should indicate responsibility for action.
3 Describe the information systems to be supported and how those information systems areto be used to generate relevant management information for performance managementpurposes, including cost and quality management.
4 Ensure that performance managers receive relevant and timely information.
5 Develop and implement a plan for meaningful engagement with providers, which enablesconstructive challenge and partnership.
6 Establish mechanisms for sharing information and best practice with other purchasers ofhealth care/funders.
7 Ensure information is being passed on to the strategic planning and contract initiationfunctions to inform ongoing improvement.
The overall purpose of effective performance management (ie to increase patient value, in thecontext of health care service delivery) is summarised in Figure 11 below.

3 Priorities for action
88 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Figure 11: Managing performance
Resource
Process
Resource
Output
Ou
tcom
e
Add ValueInput Output
Measure Measure Measure
Measure
Measure
Value demonstrated by:
• Understanding of resources used
• Early warning
• Incremental change
• Continuous improvement
• Achieving excellence
Key Measure = Additional value
Resource
Process
Resource
Output
Ou
tcom
e
Add ValueInput Output
Measure Measure Measure
Measure
Measure
Value demonstrated by:
• Understanding of resources used
• Early warning
• Incremental change
• Continuous improvement
• Achieving excellence
Key Measure = Additional value
Source: PricewaterhouseCoopers, May 2008 © copyright

National Health and Hospitals Reform Commission PricewaterhouseCoopers | 89
Appendix C Acronyms
Table 12: Acronyms table
Acronym Description
ACCHS Aboriginal Community Controlled Health Service
ACSQHC Australian Commission on Safety and Quality in HealthCare
ACT Australian Capital Territory
AHS Area Health Services
AIHW Australian Institute of Health and Welfare
AMWAC Australian Medical Workforce Advisory Committee
APAC Acute/Post Acute Care Service
CCT2 Second Round of Coordinated Care Trials
CSRP Clinical Services Redesign Program
CVD Cardiovascular disease
DADHC Department of Ageing, Disability and Home Care
DoHA Department of Health and Ageing
FOBT Faecal Occult Blood Test
GDP Gross Domestic Product
GP General Practitioner
HACC Home and Community Care
HCSCC Health and Community Services Complaints Commission
IGR Intergenerational Report
IT information technology
KPI Key Performance Indicator
MBS Medical Benefits Scheme
NHS National Health Service
NHWT National Health Workforce Taskforce
NSW New South Wales
NT Northern Territory
OATSIH Office for Aboriginal and Torres Strait Islander Health
OECD Organisation for Economic Co-operation and Development
PBS Pharmaceutical Benefits Scheme
PwC PricewaterhouseCoopers
QLD Queensland
SA South Australia
TAS Tasmania
UK United Kingdom
USA United States of America

90 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
Appendix D References
1. Porter M, Teisberg E. Redefining Health Care. Harvard Business School Press,June 2006.
2. PricewaterhouseCoopers. The National Evaluation of the Second Round of CoordinatedCare Trials. Report to the Australian Department of Health and Ageing, 2007.
3. The Allen Consulting Group. Governments Working Together. Report to the VictorianGoverment, 2004.
4. Wanless D. Securing our Future Health. Taking a Long Term View. Report to the BritishGovernment, 2002.
5. PricewaterhouseCoopers. Development of a Comprehensive Comparative Data SetReport for DHS. Victoria: DHS, 2008.
6. PricewaterhouseCoopers. HealthCast 2020: Creating a Sustainable Future:PricewaterhouseCoopers' Health Research Institute, 2005.
7. Australian Institute of Health and Welfare. Australia's Health 2006. AIHW cat. no. AUS 73.Canberra: AIHW, 2006.
8. Australian Bureau of Statistics. Births Australia. In: ABS cat. no. 3301 Table 1.9, editor.Canberra, 2006.
9. Australian Bureau of Statistics. Births Australia. ABS cat. no. 3301. Canberra: ABS, 2006.
10. Australian Institute of Health and Welfare. Older Australia at a Glance. AIHW cat. no. AGE52. 4th ed. Canberra: AIHW, 2007.
11. World Health Organisation. 10 Facts on Ageing and the Life Course. 28 September ed,2007.
12. Australian Institute of Health and Welfare. Disability and Ageing: Australian PopulationPatterns and Implications. AIHW cat. no. DIS 19. Canberra: AIHW, 2000.
13. Australian Department of Health and Ageing. Injury Prevention, December 2007.
14. Wagner EH, Austin T, Davis C, Hindmarsh M, Schaefer J, Bonomi A. Improving ChronicIllness Care: Translating Evidence into Action. Health Affairs 2001;20(6):64-78.
15. NSW Department of Health. Integrated Primary and Community Health Policy 2007-2012.Sydney: NSW Department of Health, 2006.
16. Begg S, Vos T, Barker B, Stevenson C, Stanley L, Lopez AD. The Burden of Disease andInjury in Australia 2003. PHE 82. Canberra: AIHW, 2007.
17. National Health Priority Action Council. National Chronic Disease Strategy. Canberra:Australian Government Department of Health and Ageing, 2006.
18. Australian Bureau of Statistics. Australian Social Trends 2007. ABS cat. no. 4102.0.Canberra: ABS, 2007.

National Health and Hospitals Reform Commission PricewaterhouseCoopers | 91
19. Australian Bureau of Statistics. Cardiovascular Disease in Australia: A Snapshot 2004-05.ABS cat. no. 4821.0.55.001. Canberra: ABS, 2005.
20. Australian Bureau of Statistics. Tobacco Smoking in Australia: A Snapshot 2004-05. ABScat. no. 4831.0.55.001. Canberra: ABS, 2005.
21. Australian Bureau of Statistics. Alcohol Consumption in Australia: A Snapshot 2004-05.ABS cat. no. 4832.0.55.001. Canberra: ABS, 2005.
22. Australian Bureau of Statistics. Key National Indicators 2007. ABS cat. no. 1345.0Canberra: ABS, 2007.
23. Australian Institute of Health and Welfare. Use of Hospital Services, 2005.
24. Australian Institute of Health and Welfare. Indigenous Australians Health, 2006.
25. Australian Bureau of Statistics and Australian Institue of Health and Welfare. The Healthand Welfare of Australia's Aboriginal and Torres Strait Islander Peoples. ABS cat. no.4704.0, AIHW cat. no. IHW 21. Canberra: ABS and AIHW, 2008.
26. Oxfam Australia. Close the Gap: Solutions to the Indigenous Health Crisis facingAustralia. Victoria: Oxfam Australia, 2007.
27. Blakely T, Hales S, Woodward A. Poverty: Assessing the distribution of health risks bysocioeconomic position at national and local levels. WHO Environmental Burden ofDisease Series no. 10. Geneva: WHO, 2004.
28. Australian Institute of Health and Welfare. Health Expenditure Australia2005-06. Canberra: AIHW, October 2007.
29. Commonwealth of Australia. Intergenerational report 2007. Canberra, 2007.
30. Australian Institute of Health and Welfare. Health Expenditure Australia 2005-06. Healthand Welfare Expenditure Series no. 30 cat. no. HWE 37. Canberra: AIHW, 2007.
31. Victorian Government Department of Human Services. Directions for your health system –Metropolitan Health Strategy. Melbourne: DHS, October 2003.
32. Freund D, Smeeding TM. The Future Costs of Health Care in Aging Societies: Is theGlass Half Full or Half Empty? . Prepared for the Seminar: Ageing Societies: Respondingto the Policy Challenges: UNSW, 8 April 2002.
33. PricewaterhouseCoopers. Accident Compensation Corporation New Zealand SchemeReview. 3.2.3 Special issues for treatment injury, p56: ACC, 2008.
34. PricewaterhouseCoopers. Promoting Integrated and Timely Care in the Community andHospital (PITCCH) Clinical Redesign Project. In collaboration with Sydney West AreaHealth Service, 2007.
35. PricewaterhouseCoopers. Modelling of Service Levels, NSW Disability Service System,2005.
36. PricewaterhouseCoopers. General Practice Workforce Modelling Technical Paper. 2005.

92 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
37. Rix M, Owen A, Eagar K. (Re)form with Substance? Restructuring and Governance in theAustralia Health System 2004/05. Australian and New Zealand Health Policy 2005;2(19).
38. Australian Institute of Health and Welfare. Australian Hospital Statistics2005-06. Health Services series no. 30 cat. no. HSE 50. Canberra: AIHW, 2007.
39. Report on Government Services. 2008.
40. Australian General Practice Statistics and Classification Centre. The BEACH Project:Bettering the Evaluation And Care of Health. A Collaborating Unit of the AustralianInstitute of Health and Welfare, 2008.
41. Australian Bureau of Statistics. Labour Force. Quarterly, February 2008.
42. PricewaterhouseCoopers. Presentation to be presented to the National Health WorkforceForum, 4 July 2008.
43. Macra FA. Providing Colonosopy Services for the Natinal Bowel Cancer ScreeningProgram. Medical Journal of Australia 2007;186(6):280-281.
44. Australian Institute of Health and Welfare. Australia's Health 2006. In: AIHW, editor. Table6.19. Canberra, 2006.
45. Duffield C, Roche M, O'Brien-Pallas L, Diers D, Aisbett C, King M, Aisbett K, Hall J.Glueing it Together: Nurse, their Work Environment and Patient Safety. Final Report:University of Technology, Sydney, 2007.
46. Industry Skills Council. Community Services and Health, Environmental Scan, 2008.
47. Richmond D. Symposium – Out of Darkness into Light. The Richmond Report, speechnotes, May 2003.
48. Newman N. Waiting for Help. Newman Weekly: The New Zealand Centre for PoliticalDebate, 2006.
49. World Health Organisation. Mortality database, 2002.
50. Wilson RM, Runciman WB, Gibberd RW, Harrison BT, Newby L, Hamilton JD. The Qualityin Australian Health Care Study. Medical Journal of Australia 1995;163(9):458-471.
51. Australian Council for Safety and Quality in Healthcare. Charting the Safety and Quality ofHealth Care in Australia. Canberra: Commonwealth of Australia, 2004.
52. Cutting Edge Information. Pharmaceutical Patient Compliance and Disease Management,November 2004.
53. Medco Health Solutions. New Study Finds Lack of Medication Compliance Leads to HighMedical Costs, June 2005.
54. PricewaterhouseCoopers. Pharma 2020: The vision. Which path will you take?:PricewaterhouseCoopers, 2007.
55. World Health Organisation. Adherence to Long-term Therapies: Evidence for Action,2003.
National Health and Hospitals Reform Commission PricewaterhouseCoopers | 93
56. Stein J. Patients Don't Anticipate Consequences of Antibiotic Noncompliance. MedicalNews Today, 21 April 2006.
57. Australian Commission on Safety and Quality in Health Care. Newsletter issue 2July 2007
58. Australian Institute of Health and Welfare. Sentinel Events in Australian public Hospitals2004-05. Safety and Quality Health Care series no. 2. Canberra: AIHW, 2007.
59. NSW Department of Health. Incident Management in the NSW Public Health System2007, 2008.
60. Wakefield J. Patient Safety: From Learning to Action. First Queensland Health Report onClinical Incidents and Sentinel Events: Queensland Health, 2007.
61. Ragg A. Safer Health care: Now and into the Future: Summary of the South AustralianSafety and Quality Program 2007-2011: Department of Health South Australia, 2007.
62. National Patient Safety Agency. Building a Memory: Preventing Harm, Reducing Risksand Improving Patient Safety. The First Report of the National Reporting and LearningSystem and the National Patient Observatory: National Health Service, July 2005.
63. Australian Department of Health and Ageing. State of Our Public Hospitals. June Report:Commonwealth of Australia, 2007.
64. Australian Department of Health and Ageing. The Review of Future GovernanceArrangements for Safety and Quality in Health Care: National Arrangements for Safetyand Quality of Health Care in Australia, 2005.
65. PricewaterhouseCoopers. Sharing Healthcare. Report to the Australian Department ofHealth and Ageing, 2005.
66. PricewaterhouseCoopers. Approaches to Understanding Resource Use and ResourceAllocation. Report to the Australian Department of Health and Ageing, 2003.
67. Commonwealth Department of Health and Aged Care. Development of a StrategicComputer Model for Increasing Allocative Efficiency. Territory Health Services,December 1998.
68. Scotton R. MediCare: Options for the Next 25 years. The Best Long Term Option forHealthcare in Australia would be a System of Managed Competition. Medical Journal ofAustralia 2000;173:41-43.
69. PricewaterhouseCoopers. Coordinated Care Trials Fund Pooling Methodology. Report tothe Australian Department of Health and Ageing, 2000.
70. Duckett SJ, Agius PA. Performance of Diagnosis-Based Risk Adjustment Measures in aPopulation of Sick Australians. ANZ Journal of Public Health 2002;26(6):500-507.
71. PricewaterhouseCoopers. Coordinated Care Trials – Fund Pooling MethodologyExecutive summary Ch 11 Pool risk quantification and management. Report to AustralianDepartment of Health and Ageing, 2000.
72. PricewaterhouseCoopers. Healthy choices: The changing role of the health insurer.PricewaterhouseCoopers, 2006.

94 | PricewaterhouseCoopers National Health and Hospitals Reform Commission
73. PricewaterhouseCoopers. The National Evaluation of the Second Round of CoordinatedCare Trials: Summary of Key Findings. Report for the Department of Health and Ageing,2007:p26.
74. PricewaterhouseCoopers. Working Towards Wellness: Accelerating the Prevention ofChronic Disease. World Economic Forum, January 2007.
75. Department for Work and Pensions. Carol Black’s review. Working for Health, 2008.
76. PricewaterhouseCoopers. Mental Health Clinical Redesign Project. In collaboration withSydney West Area Health Service (SWAHS), 2007.
77. PricewaterhouseCoopers. Improving the Older Person’s Journey and Experience ofHealth Care Across the Care Continuum. In collaboration with North Sydney CentralCoast Area Health Service (NSCCAHS), 2008.
78. Wagner EH. Chronic disease management: What will it take to improve care for chronicillness? Effective Clinical Practice 1998;1:2-4.
79. PricewaterhouseCoopers. You Get What You Pay For: A Global Look at BalancingDemand, Quality, and Efficiency in Healthcare Payment Reform:PricewaterhouseCoopers' Research Institute, 2008.
80. Ambulance Service of NSW. Expanded and Extended Care by Ambulance OfficersCommunication Plan (Draft). Unpublished document, October 2006.
81. Tollen L. Physician Organization in Relation to Quality and Efficiency of Care: A Synthesisof Recent Literature. The Commonwealth Fund, April 2008.
82. McAvoy BR, Coster GD. General Practice and the New Zealand Health Reforms –Lessons for Australia? Australia and New Zealand Health Policy 2005;2.

National Health and Hospitals Reform CommissionPricewaterhouseCoopers 95
PwC contacts
For further information, please contact:
Health Actuarial and Advisory (Sydney)
John Walsh
Partner
+61 (2) 8266 3205
Anne-Marie Feyer
Partner
+61 (2) 8266 3925
Caitlin Francis
Director
+61 (2) 8266 1648
Kirsten Armstrong
Director
+61 (2) 8266 4866
Carrie Schulman
Director
+61 (2) 8266 3170
Christine Callaghan
Director
+61 (2) 8266 1075
Richard Baldwin
Director
+61 (2) 8266 5321
Health Advisory Performance Improvement (National)
Tony Peake
Partner
+61 (3) 8603 6248
Roger McComiskie
Partner
+61 (7) 3257 8616
Bruce McDonald
Partner
+61 (2) 8266 3480
Noreen Dowd
Partner
+61 (3) 8603 2677
Jonathan Lunn
Partner
+61 (2) 8266 4681
Bianca Jordaan
Director
+61 (2) 8266 2892
Stephanie Allen
Director
+61 (8) 9238 3412
Health Insurance
Kim Smith
Partner
+61 (2) 8266 1100
Jan Muysken
Partner
+61 (2) 8266 2714
Health Advisory (Pharmaceuticals)
John Cannings
Partner
+61 (2) 8266 6410
Nathan Schlesinger
Senior Manager
+61 (2) 8266 0990
© 2008 PricewaterhouseCoopers Australia. All rights reserved. "PricewaterhouseCoopers" refers toPricewaterhouseCoopers Australia or, as the context requires, the PricewaterhouseCoopers global network orother member firms of the network, each of which is a separate and independent legal entity.
This submission is protected under the copyright laws of Australia and other countries as an unpublished work.This submission contains information that is proprietary and confidential to PricewaterhouseCoopers and subjectto applicable Federal or State Freedom of Information legislation, and shall not be disclosed outside the recipient'scompany or duplicated, used or disclosed in whole or in part by the recipient for any purpose other than toevaluate this submission. Any other use or disclosure in whole or in part of this information without the expresswritten permission of PricewaterhouseCoopers is prohibited.

pwc.com/au
Related Documents











