1 Washington Hilton Washington, DC October 9—10, 2015 CPNP Annual Symposium Program Book 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Washington Hilton Washington, DC
October 9—10, 2015 CPNP Annual Symposium
Program Book
1

NOTES

Table of Contents
President’s Welcome 2
Support 3
Program at a Glance 4
The gut balance revolution 9 Gerard Mullin, MD, The Johns Hopkins University School of Medicine
Childhood obesity: Fighting a battle of epic proportions 23 Shikha Sundaram MD and Helen Seagle RD, Children’s Hospital of Colorado
“Nutrition ROCKs HCT”: Nutrition Research for Optimizing Care in Kids 29 undergoing hematopoietic cell transplantation Lori Bechard PhD, Med, RD, LDN, Boston Children’s Hospital
Nutrition for the child with cystic fibrosis 41 Tami Miller RD, Children’s Hospital of Wisconsin
Nutritional issues in cholestatic disease 48Binita Kamath MBBChir, MRCP, MTR, The Hospital for Sick Children
Iron deficiency and the developing brain 57 Michael K. Georgieff, MD, University of Minnesota
Nutrition and diet in the management of inflammatory bowel disease 68 Athos Bousvaros MD, MPH and Karen Warman RD, Boston Children’s Hospital
Case study breakouts 83
The Elimination Diet: Practical Tips and Assessing nutritional needs in the hypometabolic child Nutrition care for children undergoing hematopoietic cell transplantation Troubleshooting pancreatic enzyme therapy (PERT) in cystic fibrosis Nutritional Issues in Alagille Syndrome Inflammatory Bowel Disease
Blenderized Tube Feedings: Managing a New Frontier 101 Margaret Girten RD, CSP, LDN and Julia Driggers RD, LDN, CNSC, Children’s Hospital of Philadelphia
1

President’s Welcome
I would like to welcome you all to the third annual NASPGHAN/CPNP Nutrition Symposium. I believe this year’s program is our best ever. We listened to your feedback from last year and made some significant changes. We expanded the nutrition content available on Friday to allow participants to take full advantage of their included registration to the NASPGHAN annual meeting. We shortened most of the talks during our Saturday symposium to allow for a greater number and variety of speakers. We changed our breakout sessions to a roundtable format to allow for more interaction with the presenters and your peers. Let us know what you think about these changes so we can continue to provide a high quality experience.
We have also experienced great growth in our Council for Pediatric Nutrition Professionals (CPNP) over this past year. I am delighted to share that we have 130 members as part of our council from throughout North America and we have made great strides towards our council goals. We launched the listserv, developed our website and obtained status as an official provider of continuing professional education (CPE) through the Commission of Dietetic Registration (CDR). We will once again have a brief council meeting during the lunch hour on Saturday. I encourage everyone to attend to learn about what we are currently doing and what we have planned next!
We hope you enjoy this year’s symposium. Next year, in lieu of our regular annual meeting will be the World Congress in Montreal, Canada (October 4-10, 2016), including a full day of nutrition content with presenters from around the world. There will be many more details to come regarding this exciting event. We hope to see many of you there!
Thank you so much for being here.
Sincerely,
Jenny Crouse, MS, RD, CD, CDE President, Council for Pediatric Nutrition Professionals
2

NASPGHAN Nutrition Symposium CPNP Founders
Thanks to the following companies for their support of this event and the establishment of the Council of Pediatric Nutrition Professionals
Abbott Nutrition
Dr. Schar
Mead Johnson Nutrition
Nestlé Nutrition
QOL Medical
Support for this year’s symposium has been generously provided by:
Abbott Nutrition
Mead Johnson Nutrition
Nestlé Nutrition
3

NASPGHAN/CPNP ANNUAL SYMPOSIUM
Friday, October 9, 2015
7:00AM - 8:00AM Meet the professor breakfast (extra fee – ticket required) Fairchild West
EoE and Elimination Diets Amir Kagalwalla MD and Sally Schwartz RD 8:15AM – 10:00AM Plenary Session I International Ballroom Center
Basic Science Year in Review Nicola Jones MD, PhD, The Hospital for Sick Children Business Meeting
Clinical Science Year in Review William Balistreri MD, Cincinnati Children’s Hospital Medical Center
10:30AM – 12:00PM Concurrent Session I
Nutrition Lincoln Room Moderators: Russell Merritt MD and Ala Shaikhkhalil MD
LONG TERM COMPLICATIONS OF TPN: NOW THAT MY INTESTINAL FAILURE PATIENTS ARE NOT DYING OF LIVER DISEASE, WHAT ELSE SHOULD I WORRY ABOUT? Jane Balint MD, Nationwide Children’s Hospital
Learning objectives: 1. Identify potential complications of lipid minimization strategies 2. Describe an approach to micronutrient monitoring in long term parenteral nutrition 3. Discuss renal and bone complications of parenteral nutrition
Oral Abstract Presentation COMBATING CLABSIS-PREVENTING CENTRAL LINE INFECTIONS AND OTHER CENTRAL LINE
CHALLENGES John Kerner MD, Lucile Packard Children’s Hospital
Learning objectives: 1. Identify evidence based practices for CLABSI prevention 2. Describe at least one modality for the prevention of catheter-related venous thrombosis 3. Discuss the approach to the patient with central line occlusion
Oral Abstract Presentation
4

Malabsorption Georgetown Room Moderators: Michelle Pietzak MD and Maria Mascarenhas MBBS
ADVANCES IN CF THERAPIES AND THEIR EFFECT ON GASTROINTESTINAL MANIFESTATIONS Daniel Gelfond MD, WNY Pediatric Gastroenterology
Learning objectives: 1. Outline pathophysiology of CF and impact of CFTR on clinical manifestations 2. Recognize gastrointestinal manifestations of the Cystic fibrosis and discuss therapeutic
interventions 3. Outline recent development and advances in CF therapy targeting specific genetic
mutations 4. Discuss role of wireless motility capsule as gastrointestinal biomarker of CFTR activity Oral Abstract Presentation
DISCORDANT SEROLOGIES AND BIOPSIES: WHAT TO DO? Dascha C. Weir MD, Boston Children's Hospital
Learning objectives: 1. Recognize the potential complexities in the use of celiac serologic markers and small
intestinal biopsies in clinical practice. 2. Discuss a clinical approach to the treatment and monitoring of patients with discordant
serology and biopsies.
Oral Abstract Presentation 2:30PM – 4:00PM Concurrent Session II
Virtual NAFLD (No Fee Registration required - See ticket for room assignments) Moderators: Stephanie Abrams, Amal Aqul, Sarah Barlow, Molly Bozic, Nirav Desai, Rima Fawaz, Ariel Feldstein, Regy Gonzales-Peralta, Nitika Gupta, Evelyn Hsu, Rohit Kohli, Jean Molleston, Karen Murray, Nadia Ovchinsky, Emily Perito, Jeff Schwimmer, Dellys Soler-Rodriguez, and Shikha Sundaram
Speaker: Miriam Vos MD, MSPH, FAHA, Emory School of Medicine Learning objectives: 1. To address when to biopsy and when to re-biopsy in pediatric NAFLD 2. To understand dyslipidemia in the setting of NAFLD– how to assess and when to start medications 3. To discuss treatment with Vitamin E (and other medications)
5
Nutrition Lincoln Room Moderators: Ruba Abdelhadi MD and Timothy Sentongo MD
BACTERIAL OVERGROWTH IN PEDIATRIC SHORT BOWEL SYNDROME Conrad Cole MD, Cincinnati Children’s Hospital Medical Center
Learning Objectives: 1. Learn risk factors for developing bacterial overgrowth 2. Discuss diagnostic challenges 3. Understand the differential diagnosis 4. Review therapeutic options
Oral Abstract Presentation
STATE OF THE ART RESEARCH LECTURE - CUTTING EDGE OR CRAZY: IS SURGERY THE MOST EFFECTIVE TREATMENT FOR NASH? Stavra Xanthakos MD, Cincinnati Children’s Hospital Medical Center
Learning objectives: 1. Review the current guidelines for when to consider bariatric surgery in youth 2. Describe the types of bariatric surgeries performed in adolescents, including risks and
benefits 3. Review the evidence and gaps in knowledge re: bariatric surgery as a specific treatment
for NASH
Oral Abstract Presentation
5:00PM - 7:00PM CPNP Reception Holmead Room, Lobby Level
Saturday, October 10, 2015
All sessions will take place in the Georgetown Room on the Concourse Level 7:30AM – 8:00AM Breakfast Concourse Foyer 8:00AM - 8:05PM INTRODUCTIONS
Praveen Goday MBBS, CNSC, Chair, NAPGHAN Nutrition Committee 8:05AM - 8:35AM THE GUT BALANCE REVOLUTION
Gerard Mullin MD, The Johns Hopkins University School of Medicine 8:35AM – 9:15AM CHILDHOOD OBESITY: FIGHTING A BATTLE OF EPIC PROPORTIONS
Shikha Sundaram MD and Helen Seagle RD, Children’s Hospital of Colorado 9:15AM - 9:45AM “NUTRITION ROCKS HCT”: NUTRITION RESEARCH FOR OPTIMIZING CARE IN KIDS
UNDERGOING HEMATOPOIETIC CELL TRANSPLANTATION Lori Bechard PhD, Med, RD, LDN, Boston Children’s Hospital
9:45AM - 10:15AM NUTRITION FOR THE CHILD WITH CYSTIC FIBROSIS
Tami Miller RD, Children’s Hospital of Wisconsin
6

10:15AM – 10:30AM Break Concourse Foyer 10:30AM - 11:00AM NUTRITIONAL ISSUES IN CHOLESTATIC DISEASE
Binita Kamath MBBChir, MRCP, MTR, The Hospital for Sick Children 11:00AM - 11:30AM NUTRITIONAL CHALLENGES IN CHILDREN WITH AUTISM
Cade Nylund MD, MS, FAAP, Walter Reed National Military Medical Center 11:30AM – 12:00PM IRON DEFICIENCY AND THE DEVELOPING BRAIN
Michael K. Georgieff MD, University of Minnesota 12:00PM – 1:00PM Lunch/Poster Session
1:00PM - 1:35PM NUTRITION AND DIET IN THE MANAGEMENT OF INFLAMMATORY BOWEL DISEASE
Athos Bousvaros MD, MPH and Karen Warman RD, Boston Children’s Hospital
1:40PM - 3:10PM Case study breakouts [3 consecutive sessions, 30 minutes each] Dupont, Embassy, Cardozo – Terrace Level
THE ELIMINATION DIET: PRACTICAL TIPS AND PITFALLS - Wendy Elverson RD, LDN, Boston Children’s Hospital
ASSESSING NUTRITIONAL NEEDS IN THE HYPOMETABOLIC CHILD- Monica Cicchini MS,RD, CSP, LD Georgetown University Hospital
NUTRITION CARE FOR CHILDREN UNDERGOING HEMATOPOIETIC CELL TRANSPLANTATION, NOW AND LATER - Lori Bechard PhD, Med, RD, LDN, Boston Children’s Hospital
TROUBLESHOOTING PANCREATIC ENZYME THERAPY (PERT) IN CYSTIC FIBROSIS– Tami Miller RD, CSP, CD, Children’s Hospital of Wisconsin
NUTRITIONAL ISSUES IN ALAGILLE SYNDROME – Binita Kamath MBBChir, MRCP, MTR, The Hospital for Sick Children
INFLAMMATORY BOWEL DISEASE – Karen Warman RD, Boston Children’s Hospital
3:15PM - 4:15PM BLENDERIZED TUBE FEEDINGS: MANAGING A NEW FRONTIER Margaret Girten RD, CSP, LDN and Julia Driggers RD, LDN, CNSC, Children’s Hospital of Philadelphia
7

3:45PM – 5:15PM Psychology II - Psychology and Gastroenterology:
Keys to Effective Integration Monroe Room, Concourse Level Moderator: Anthony Alioto PhD, BCB
ABDOMINAL PAIN: INTEGRATING PSYCHOLOGICAL TREATMENTS INTO MEDICAL CARE Miranda vanTilburg PhD, University of North Carolina, Center for Functional GI and Motility Disorders Learning objectives: 1. Describe the role of psychosocial factors in functional abdominal pain disorders 2. Identify evidence-based psychological/behavioral treatments for functional abdominal pain
disorders and how to integrate with medical care 3. Identify patients most likely to benefit from integrated care
CONSTIPATION AND SOILING: INTEGRATED MODELS OF CARE Rose Schroedl PhD, Nationwide Children’s Hospital
Learning objectives: 1. Summarize integrated models of care for constipation and fecal incontinence 2. Discuss the evidence-base for integrated models of care 3. Describe an algorithm for treatment decision making INTERDISCIPLINARY INPATIENT APPROACHES TO WEANING TUBE DEPENDENT CHILDREN FROM ENTERAL FEEDING Alan Silverman PhD, Medical College of Wisconsin Learning objectives: 1. Describe existing interdisciplinary care models for weaning tube dependent children 2. Summarize the current state of empirical support for interdisciplinary treatment approaches
to weaning tube dependent children from enteral feeding 3. List methods for medical oversight that can help to ensure the safety of patients undergoing
treatment
8

TheGutBalanceRevolution
GerardE.MullinMDAssociateProfessorofMedicine
www.thefoodmd.comJohnsHopkinsUniversitySchoolofMedicine
NASPGHANCPNPNutritionSymposiumOctober10th,2015
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
LearningObjectives
• Knowtheroleofthegutmicrobiotainhumanhealthanddisease
• Becomefamiliarwiththepathophysiologyofobesityandhowalterationsinthegutmicrofloraleadtoobesity
• Tounderstandhowprebioticsandprobioticscanpromotealeanmetabolismbyfosteringahealthygutmicrobiome
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Introductiontothegutmicrobiome
Wearecompositeofspecies:a‘supra‐organism’ Ourmicrobialcensusexceedsthetotalnumberofourownhumancellsby~10fold
Ourlargestcollectionofmicrobesresidesintheintestine(~10‐100trillionorganisms)
Theaggregategenomesofthesegutspecies(microbiome)maycontain>100foldmoregenesthanour‘own’genome
Themicrobiomeisanintegralpartofourgeneticlandscape(‘humanmetagenome’)andofourgeneticevolution
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
9

Techniquesusedtocharacterizethegutmicrobiome
NIH HUMAN MICROBIOME
PROJECT
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Energy
Transport
Defense and Repair
Structural Integrity
Communication
Detoxification & Biotransformation
Assimilation
Properly Functioning
GastrointestinalMicroBiome
BioFilm & Permeability
Mast Cell Degranulation
Phase IIIDetoxification
n-ButyrateSCFA
Production
Oral Tolerance, NF-κB, IL-10, IL-17
ObesityNutrition
&Metabolis
m
GI MotilityEntero-HepaticReCirculaton
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
EcosystemsandBiodiversity
• Increasedspeciesdiversityincreasestheefficiencyandproductivityofanecosystem
• Morediversecommunitiesarefunctionallylesssusceptibletoexternalstressors
• Inrelativeterms,increasingstresshasastrongernegativeeffectonlow‐diversecommunities
Global Ecosystem Changes
Natural Processes
Biodiversity
Stability
Ecosystem Functioning
Ecosystem Services
Human Wellbeing
Khanna S and Tosh PK. (2014).. Mayo Clin Proc. 89(1): 107‐114.Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
10
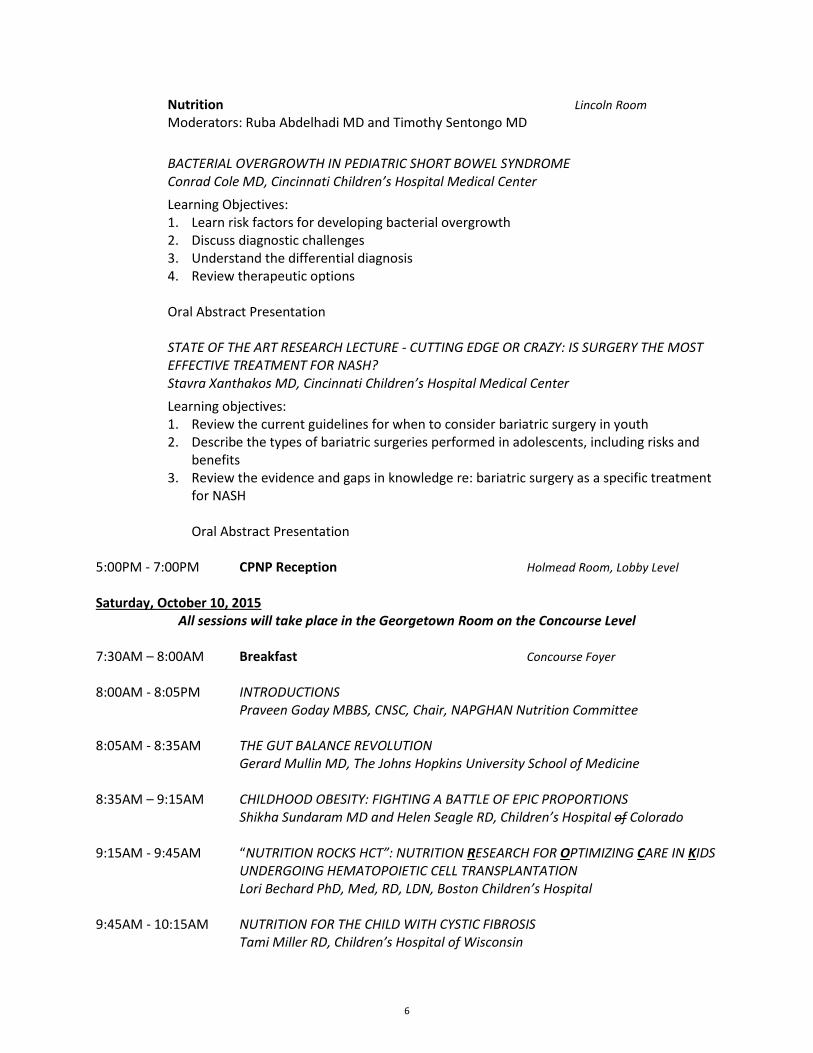
J. Physiol Biochem DOI 10.1007/s13105-0390-3 In Press 2/2015. Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
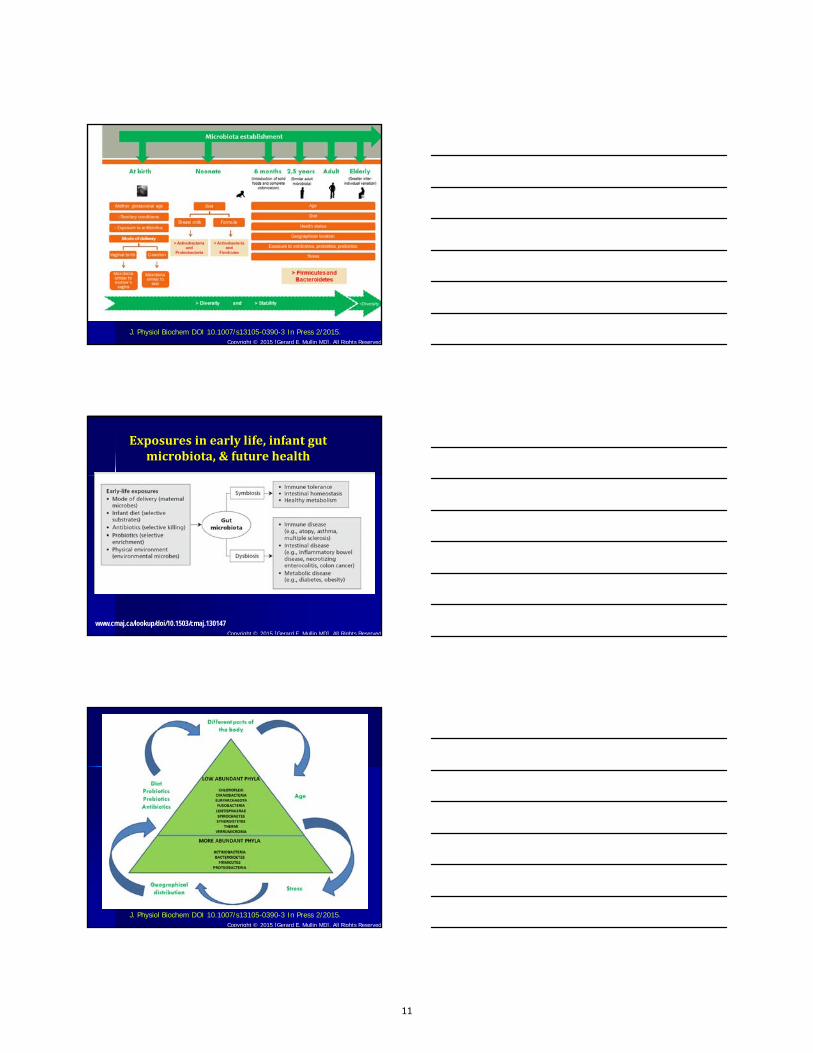
Exposuresinearlylife,infantgutmicrobiota,&futurehealth
www.cmaj.ca/lookup/doi/10.1503/cmaj.130147Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
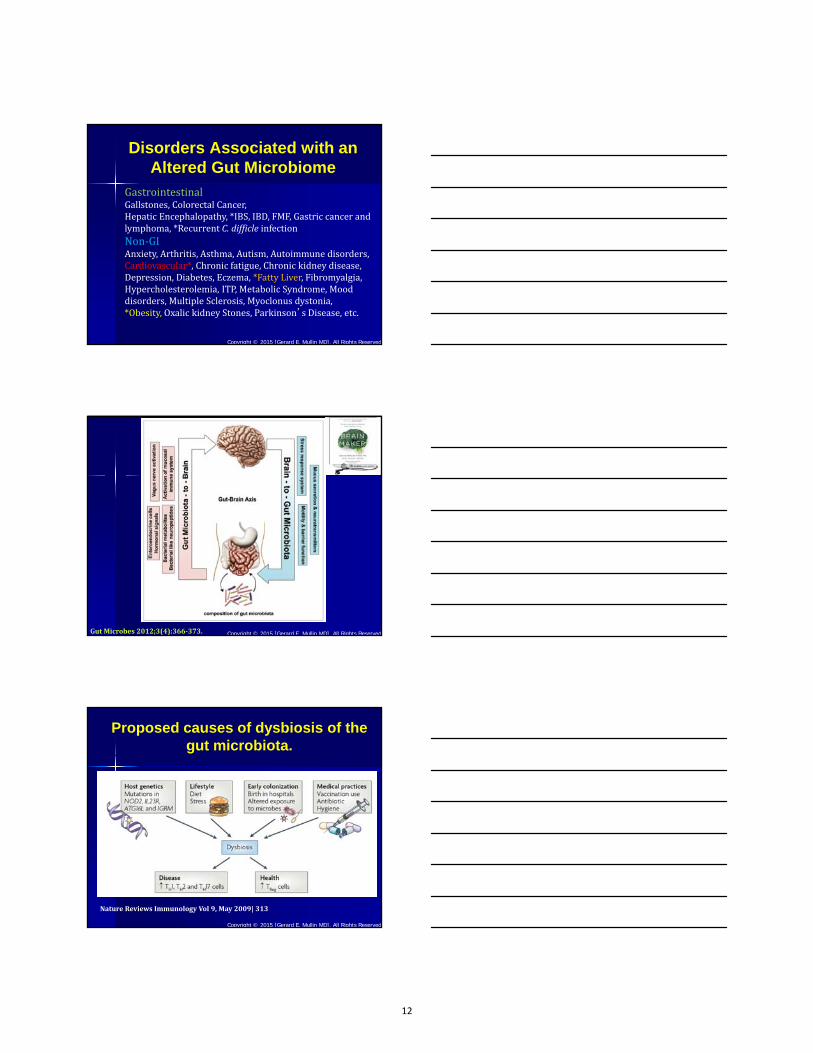
J. Physiol Biochem DOI 10.1007/s13105-0390-3 In Press 2/2015. Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
11
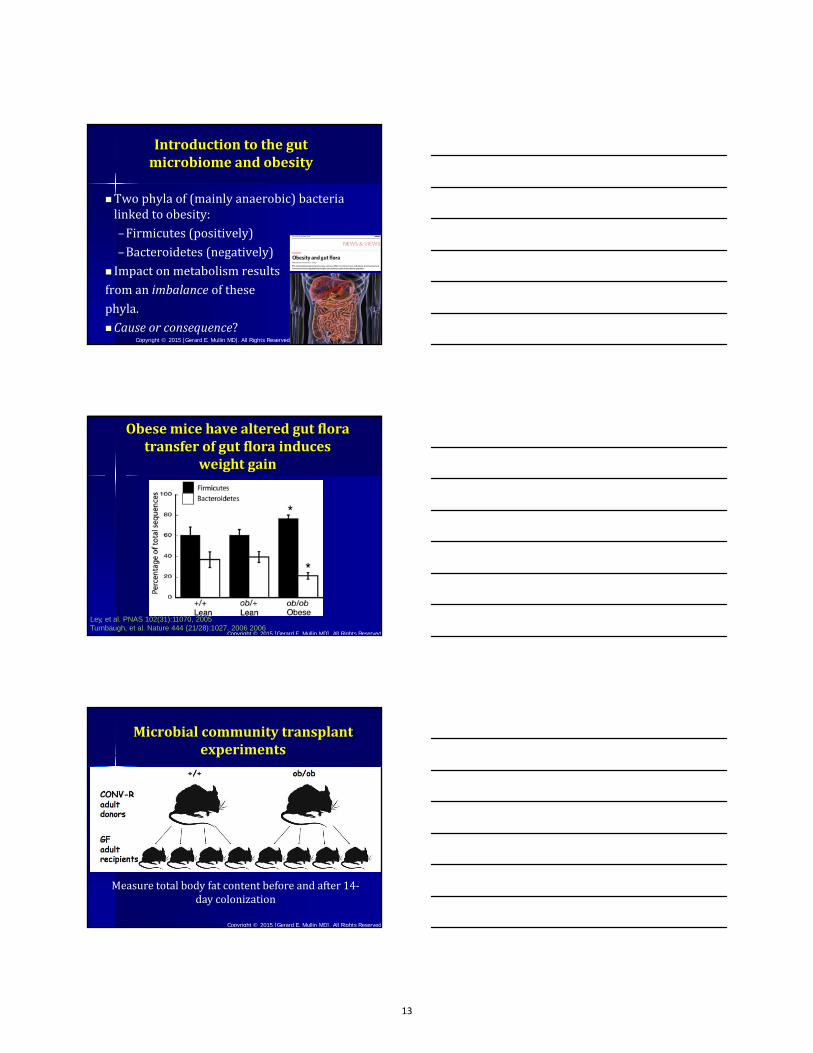
Disorders Associated with an Altered Gut Microbiome
GastrointestinalGallstones,ColorectalCancer,HepaticEncephalopathy,*IBS,IBD,FMF,Gastriccancerandlymphoma,*RecurrentC.difficle infectionNon‐GIAnxiety,Arthritis,Asthma,Autism,Autoimmunedisorders,Cardiovascular*,Chronicfatigue,Chronickidneydisease,Depression,Diabetes,Eczema,*FattyLiver,Fibromyalgia,Hypercholesterolemia,ITP,MetabolicSyndrome,Mooddisorders,MultipleSclerosis,Myoclonusdystonia,*Obesity,OxalickidneyStones,Parkinson’sDisease,etc.
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
GutMicrobes2012;3(4):366‐373. Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Proposed causes of dysbiosis of the gut microbiota.
NatureReviewsImmunologyVol 9,May2009|313
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
12
Introductiontothegutmicrobiomeandobesity
Twophylaof(mainlyanaerobic)bacterialinkedtoobesity:–Firmicutes (positively)–Bacteroidetes (negatively)
Impactonmetabolismresultsfromanimbalance ofthesephyla.Causeorconsequence?
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Obesemice have altered gut floratransfer of gut flora induces
weight gain
Ley, et al. PNAS 102(31):11070, 2005Turnbaugh, et al. Nature 444 (21/28):1027. 2006 2006
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Microbialcommunitytransplantexperiments
Measuretotalbodyfatcontentbeforeandafter14‐daycolonization
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
13

Comparisonofenergyextractionbetweenobeseandleanmice
Turnbaugh,etal.Nature 444:1027,2006
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Functionalinteractionsbetweenthegutmicrobiotaandhost
metabolism
Nature 489, 242–249 (13 September 2012) doi:10.1038/nature11552 Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Host remodeling of the gut microbiomeandmetabolic changes in pregnancy
Cell, 150:470‐480,2012
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
14
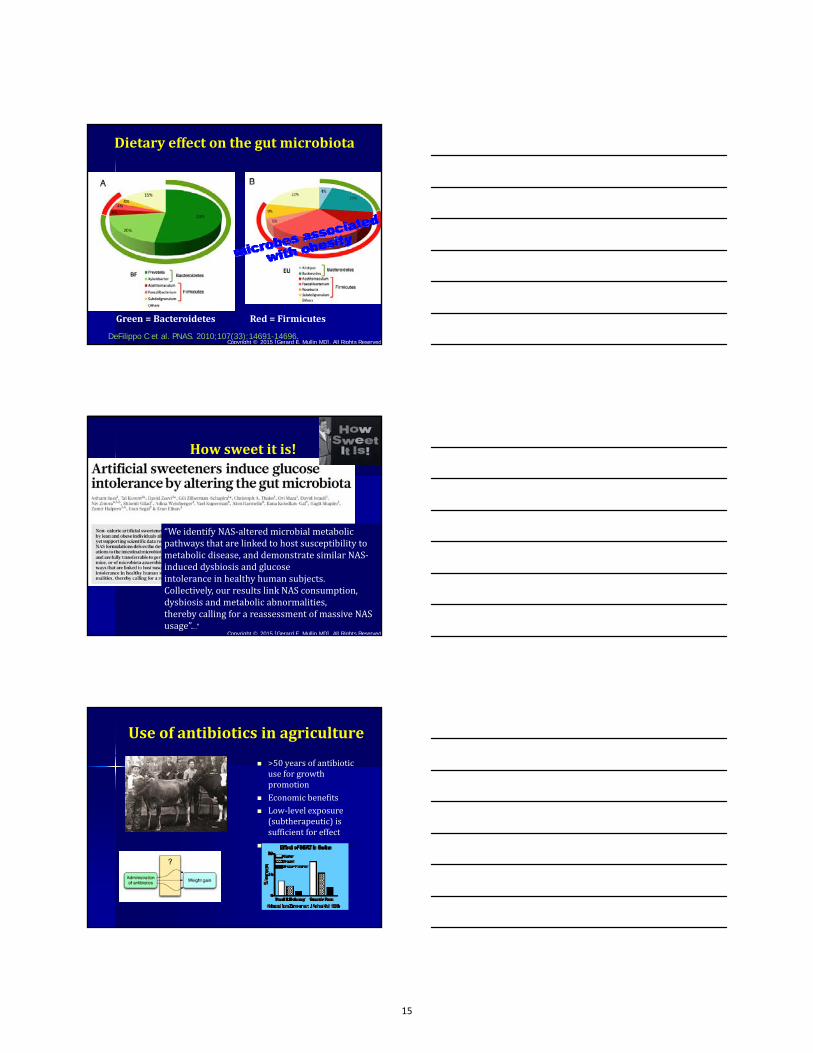
Dietaryeffectonthegutmicrobiota
DeFilippo C et al. PNAS. 2010;107(33):14691-14696.
Green=BacteroidetesRed=Firmicutes
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
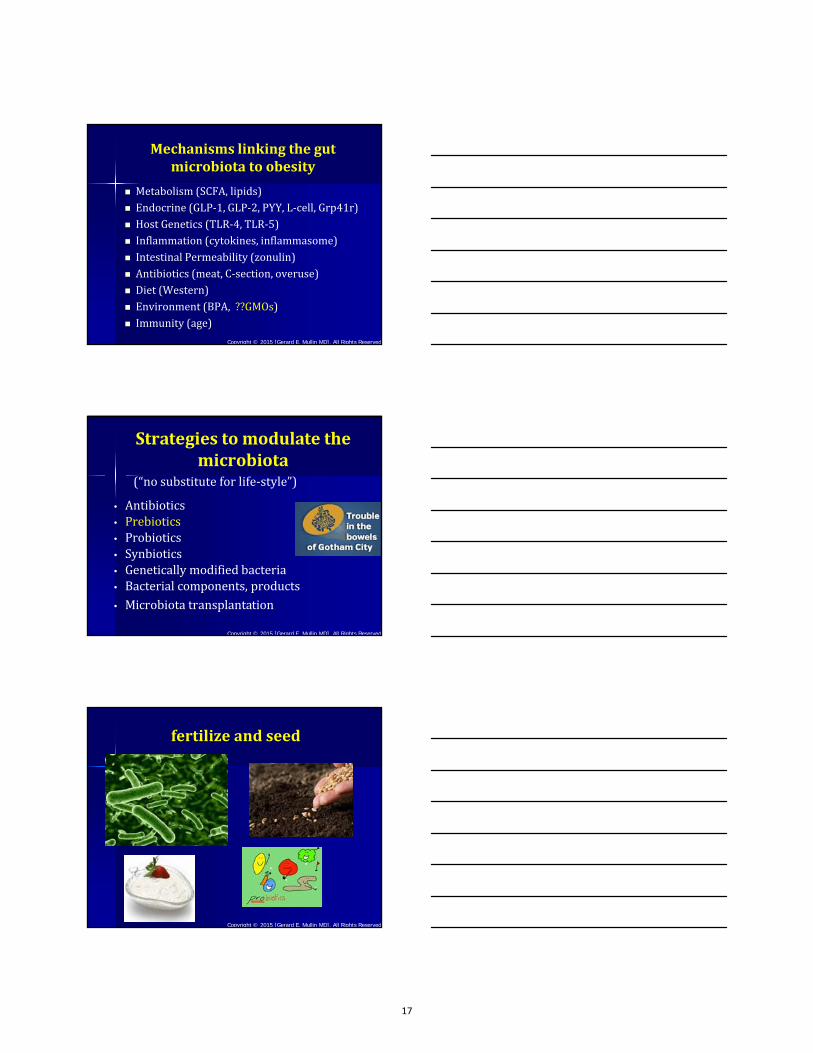
Howsweetitis!
“WeidentifyNAS‐alteredmicrobialmetabolicpathwaysthatarelinkedtohostsusceptibilitytometabolicdisease,anddemonstratesimilarNAS‐induceddysbiosisandglucoseintoleranceinhealthyhumansubjects.Collectively,ourresultslinkNASconsumption,dysbiosisandmetabolicabnormalities,therebycallingforareassessmentofmassiveNASusage”...”
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Useofantibioticsinagriculture
>50yearsofantibioticuseforgrowthpromotion
Economicbenefits Low‐levelexposure(subtherapeutic)issufficientforeffect
Differentclasseswork
15

Repeatedexposuretobroad‐spectrumantibioticsatages0‐23monthsisassociatedwithearlychildhoodobesity.Becausecommonchildhoodinfectionswerethemostfrequentdiagnosesco‐occurringwithbroad‐spectrumantibioticprescription,narrowingantibioticselectionispotentiallyamodifiableriskfactorforchildhoodobesity.
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Diet BacteriaAltered EffectonBacteria References
Carbohydrate‐reduced Bacteroidetes Increased Walker etal.BMCMicrobiol.2011;11:7.]
Calorie‐restrictedClostridiumcoccoides,Lactobacillus spp.andBifidobacteria spp.
Decreased(growthprevented)
Obesity2009;17:1906–1915.
Complexcarbohydrates
Mycobacteriumaviumsubspecies
paratuberculosisandEnterobacteriaceae
DecreasedWalkeretal.BMC
Microbiol.2011;11:7.
RefinedsugarsC.difficile andC.perfringens
IncreasedBergetal.Inflamm.BowelDis.2012
High‐fat Bifidobacteria spp. Decreased(absent)Zhangetal.ISMEJ.2010;4:232–241.
Highn‐6PUFAfromsaffloweroil Bacteroidetes Decreased
DelaSerre etal.Am.J.Physiol.2010;299:
High‐fatandhigh‐sugar
Clostridiuminnocuum,Catenibacteriummitsuokai and
Enterococcus spp.
IncreasedTurnbaughetal.Sci.Transl.Med.2009;1
DietCanInfluenceMicrobialPopulationsBrownetal.(2012)Nutrients.4(8):1095–1119.
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Diet‐induceddysbiosisanddiseases.
Chan Y et al. Clinical Consequences of Diet-Induced Dysbiosis Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
16
Mechanismslinkingthegutmicrobiotatoobesity
Metabolism(SCFA,lipids) Endocrine(GLP‐1,GLP‐2,PYY,L‐cell,Grp41r) HostGenetics(TLR‐4,TLR‐5) Inflammation(cytokines,inflammasome) IntestinalPermeability(zonulin) Antibiotics(meat,C‐section,overuse) Diet(Western) Environment(BPA,??GMOs) Immunity(age)
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Strategies tomodulate themicrobiota
(“no substitute for life‐style”)
• Antibiotics• Prebiotics• Probiotics• Synbiotics• Genetically modified bacteria• Bacterial components, products• Microbiota transplantation
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
fertilizeandseed
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
17

EOPertof etalBenefMicrobes. 2013Mar1;4(1):53‐652013Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
PrebioticRichFoods
JerusalemartichokesOnionsChicoryGarlicLeeksBananasFruitSoybeansBurdockrootAsparagus
SugarmapleChinesechivesPeasLegumesEggplantHoneyGreenTeaYogurt,cottagecheese,kefir
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Delzenne, Neyrinck, Bäckhed , Cani Targeting gut microbiota in obesity: effects ofprebiotics and probiotics Nature Reviews | Endocrinology Volume 7 | November 2011
PROBIOTICS PREBIOTICS
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
18
World J Gastroenterol 2014;21;20 (43): 16079-16094Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Strategies tomodulate themicrobiota
(“no substitute for life‐style”)
• Antibiotics• Prebiotics• Probiotics• Synbiotics• Genetically modified bacteria• Bacterial components, products• Microbiota transplantation
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
ProbableMechanismsofActionoftheAnti‐obesityEffectsof
Probiotics
Arora T, et al., Probiotics: Interaction with gut microbiome and antiobesity potential, Nutrition Volume 29, Issue 4, April 2013, Pages 591–596
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
19

Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Anti‐obesityEffectsofBifidobacteriaProbioticSupplementationofAnimalStudies
World J Gastroenterol 2014;21;20 (43): 16079-16094
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Anti‐obesityEffectsofProbioticLactobacillusSupplementationofAnimalStudies
World J Gastroenterol 2014;21;20 (43): 16079 16094
20

Anti‐obesityEffectsofProbioticSupplementation:HumanStudies
World J Gastroenterol 2014;21;20 (43): 16079-16094
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Strategies tomodulate themicrobiota
(“no substitute for life‐style”)
• Antibiotics• Probiotics• Prebiotics• Synbiotics• Genetically modified bacteria• Bacterial components, products• Microbiota transplantation
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
21

Questions?
Copyright © 2015 [Gerard E. Mullin MD]. All Rights Reserved
22
Childhood Obesity: Fighting a Battle of Epic Proportions
Shikha S. Sundaram, MD MSCIAssociate Professor of Pediatrics
Children’s Hospital Colorado
Helen Seagle, MS RDNClinical Dietitian in Lifestyle Medicine
Children’s Hospital Colorado
Disclosures
• We have no financial relationships with acommercial entity to disclose.
Objectives
• To understand the epidemiology of pediatricobesity in the United States
• To understand the myriad of complications ofpediatric obesity
• To understand the complex pathogenesis ofobesity
• To understand the dietitian skillset necessaryto combat childhood obesity
23
Definitions
• Body mass index (BMI) is a measure used todetermine childhood overweight and obesity.
• Overweight is defined as a BMI at or abovethe 85th percentile and below the 95th
percentile for children and teens of the sameage and sex.
• Obesity is defined as a BMI at or above the95th percentile for children and teens of thesame age and sex.
15%–<20% 20%–<25% 25%–<30% 30%–<35% ≥35%
Prevalence* of Self-Reported Obesity Among U.S. Adults by State and Territory, BRFSS, 2013
*Prevalence estimates reflect BRFSS methodological changes started in 2011. These estimates should not becompared to prevalence estimates before 2011.
CA
MT
ID
NVUT
AZNM
WY
WA
OR
CO
NE
ND
SD
TX
OK
KS
IA
MN
AR
MO
LA
MI
IN
KY
IL OH
TN
MS AL
WI
PA
WV
SC
VA
NC
GA
FL
NY
VT
ME
HI
AK
NHMARICTNJDEMDDC
PRGUAM
24

Has childhood obesity plateaued?
Certain populations are disproportionately affected by obesity
Complications of Childhood Obesity
25
Childhood Obesity Increases Risk of Adult Obesity
AJCN 70S:145S,1999
Is Obesity Really all aboutENERGY BALANCE?
Etiopathogenesis of obesity: Obesogenic environment
26

Appetite Regulation• Leptin: Mediator of long term
energy balance, suppressing the urge to eat when caloric intake maintains ideal fat stores.
• Ghrelin: a fast acting hormone that may play a role in meal initiation
Fat Patterning in Obesity
• Adipocytes from some locations (gluteal & femoral) efficientlycapture excess nutrients from the blood‐stream for storage, while others accumulate TGs but readily release them for use by other tissues.
Fat Cell Development:Number and Size
• During growth periods in childhood: fat cells increase in number• During periods of excess intake: fat cells increase in size• Fat cells reach maximum size: fat cell numbers increase again• Fat loss: cell size may shrink but not the number
27

What can we do?
Refining the RD role
Services
Self‐awareness
Cultural‐awareness
Diet assessment
Document
Behavior change
Health literacy
28

Nutrition ROCKs HCT:
Nutrition Research for Optimizing Care in Kids during
hematopoietic cell transplantation
Lori J. Bechard, PhD, MEd, RD, LDN
Disclosures
• Currently employed by Nestle Nutrition– No products or services produced by this
company are relevant to my presentation.
• Previously employed by Boston Children’sHospital
Outline
• Changes over the course of HCT– Energy expenditure– Body composition– Bone health
• Feeding modalities during HCT• Other nutrition interventions
– Vitamin D– Lipids– Exercise
29

http://www.stanfordchildrens.org/content‐public/topic/images/22/125422.gif
HCT – a unique nutritional situation
• History
• Inflammation
• Infection
• Treatment
• Toxicity
• Survivorship
Metabolic impact of HCT
• Changes in energy expenditure
• Changes in body composition
• Changes in bone health
What are the energy requirements of children
undergoing HCT?
• Prospective cohort study of 37 childrenundergoing HCT enrolled in a supportive careregimen including PN provided at 100% ofmeasured REE (as opposed to standard of care)
• REE measured weekly by indirect calorimetry
30

Indirect CalorimetryMeasured at bedside weekly while hospitalized
Decreased (NS)
Significantly decreased
31
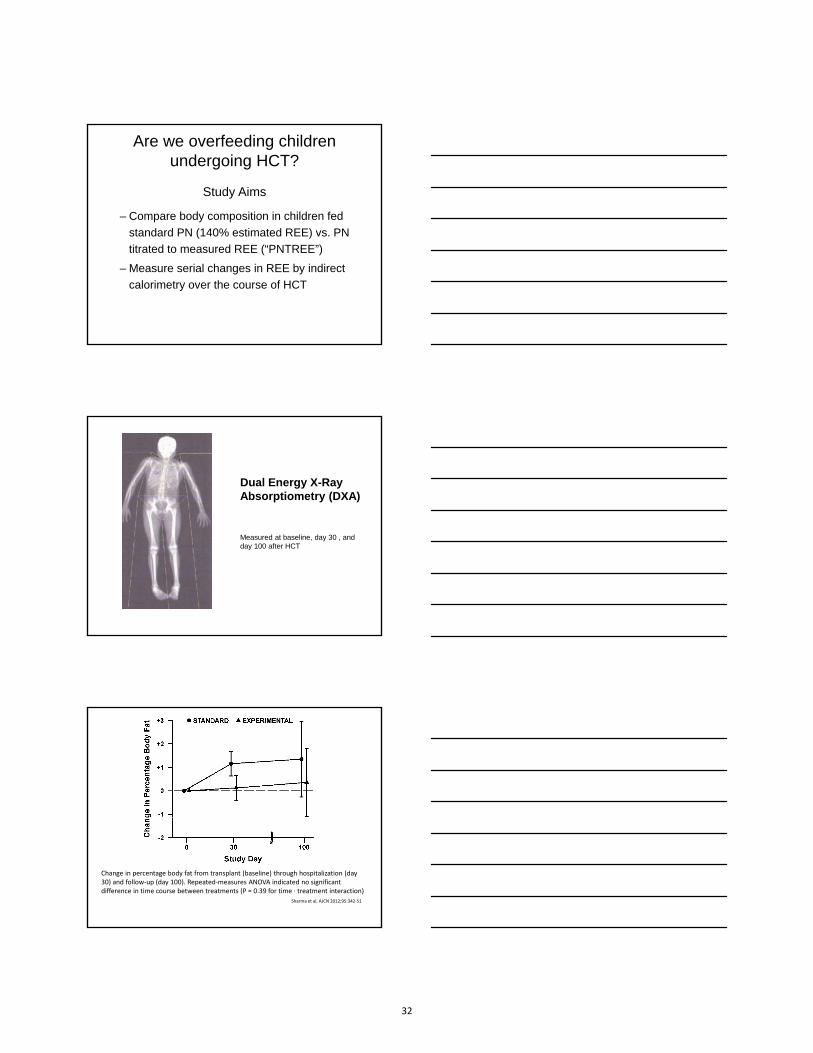
Are we overfeeding children undergoing HCT?
Study Aims
– Compare body composition in children fed
standard PN (140% estimated REE) vs. PN
titrated to measured REE (“PNTREE”)
– Measure serial changes in REE by indirect
calorimetry over the course of HCT
Dual Energy X-RayAbsorptiometry (DXA)
Measured at baseline, day 30 , and day 100 after HCT
Change in percentage body fat from transplant (baseline) through hospitalization (day 30) and follow‐up (day 100). Repeated‐measures ANOVA indicated no significantdifference in time course between treatments (P = 0.39 for time ∙ treatment interaction)
Sharma et al, AJCN 2012;95:342‐51
32

REE changes over time despite different energy intakes
Bechard, et al. Bone Marrow Transplant 2012 47(10);1301‐6
PNTREEDiscussion
• Total % body fat increased significantly in the standard group by 1.2 +0.5 kg from baseline to 30 days; the increase persisted to 100 days, but wasnot statistically significant– Clinically significant??
• Lean body mass decreased dramatically in both groups, persisted to 100 days, not influenced by increased intake with standard regimen– Suggests need for alternative and adjunctive therapies aimed at preserving
lean mass
• Weight and BMI z-score decrease significantly in both groups over study period– Likely influenced by loss of lean body mass– Is standard regimen simply contributing to increase in body fat?
Clinical outcomes of PNTREE participants
Sharma et al, AJCN 2012;95:342‐51
33
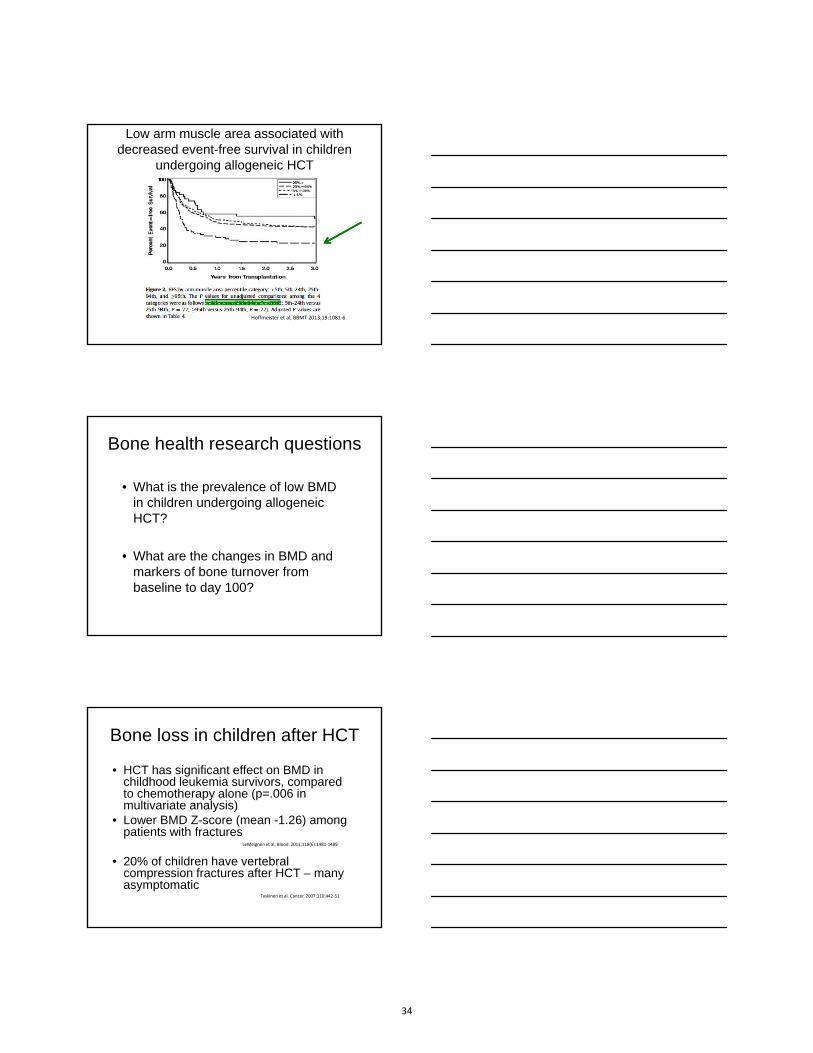
Low arm muscle area associated with decreased event-free survival in children
undergoing allogeneic HCT
16
Hoffmeister et al, BBMT 2013;19:1081‐6
Bone health research questions
• What is the prevalence of low BMDin children undergoing allogeneicHCT?
• What are the changes in BMD andmarkers of bone turnover frombaseline to day 100?
17
Bone loss in children after HCT
• HCT has significant effect on BMD inchildhood leukemia survivors, comparedto chemotherapy alone (p=.006 inmultivariate analysis)
• Lower BMD Z-score (mean -1.26) amongpatients with fractures
• 20% of children have vertebralcompression fractures after HCT – manyasymptomatic
LeMeignen et al. Blood. 2011;118(6):1481‐1489
Taskinen et al. Cancer. 2007;110:442‐51
18
34

Bone changes following HCT in children
from Petryk et al J Clin Endocrinol Metab 2006;291: 899–905
Change in BMC & BMD Z-score during HCT
Adjusted for age, sex, Tanner stage, lean mass, fat mass, REE, energy intake, insulin
sensitivity, inpatient steroid intake, and serum phosphorus.
*significant decline from baseline; timetrend significant at p<0.0001 for BMD Z‐
score, p=0.007 for BMC Z‐score.
Error bars = + 1 standard error
20Bechard et al, Ped Blood Cancer 2015;62(4):687‐92
Challenges to feeding children during HCT
• Many children require PN– Mucositis
– Enteritis
• Enteral feeding– Access
– Tolerance
• Volume management
35
Enteral feeding in pediatric HCT
• Retrospective analysis of 49 pts.,autologous and allogeneic transplants
• NG-tube placed during conditioning or within1st week
• 86% maintained exclusively on EN• No significant weight loss• Engraftment comparable to historical
controls
Langdana, Bone Marrow Transplant, 2001
Feasibility of enteral feeding (EN) in children during allogeneic HCT
• 65 children prospectively enrolled• EN via nasogastric tube on day +1• 50 pts. (77%) received EN only
– Faster platelet recovery (23 vs. 29 days, p=0.01)– Shorter length of stay (29 vs. 40 days, p<0.001)
• 15 pts. (23%) required PN• PN group - more frequent and severe acute
GVHD• No difference in weight or BMI outcomes
Azarnoush et al., Bone Marrow Transplant, 2012;47:1191-5
Vitamin D
• Deficiency and insufficiency common inHCT patients
(Duncan et al, BBMT 2011;17:749-53)
36

Serum vitamin D levels in patients and controls
25
From Campos et al, Nutrition 2014; 30:654‐9
Change in vitamin D status during HCT
Adjusted for age, sex, Tanner stage, lean mass, fat mass, REE, energy intake, insulin sensitivity, serum phosphorus, inpatient steroid intake, and vitamin D intake
*significant decline from baseline; time trend significant, p=0.001
26Bechard et al, Ped Blood Cancer 2015;62(4):687‐92
Baseline vitamin D sufficiency associated with improved outcomes
27
From Hansson et al, BBMT 2014;20:1537‐43.
37

Physical exercise
• Systematic review of RCTs(van Haren, Phys Ther 2013;93:514-28)
– Endurance exercise
– Resistance exercise
– Other types
• Positive impact– Quality of life
– Fatigue• Link with body composition changes?
28
Lipids in HCT
• Energy and essential fatty acids
• Problems with parenteral lipids
• Omega-3 benefits?
29
Alternatives to soybean lipids in pediatric HCT?
• Olive oil– 28 children randomized to olive oil vs MCT based lipid
emulsion– Favorable lipid biomarkers
Hartman et al, Clin Nutr 2009;28:631-5
• Blend of oils– 14 children randomized to soybean based vs.
MCT/soybean/fish lipid emulsion– Similar lipid biomarkers
Baena-Gomez et al, Ann Nutr Metab 2013;63:103-110
• Fish oil– Exclusive fish oil used to treat EFAD in case report of
HCT patient with soy allergyGura et al, Clin Nutr 2005; 24:839-47
30
38

Conclusions
• HCT is associated with…– Decline in lean body mass
– Changes in energy expenditure
– Bone loss
– Low vitamin D status
• PN is not required for all
• Research gaps remain
31
Future directions
• Bone health
• Body composition– Physical activity
– Energy balance
• Modular nutrients– Vitamin D
– Omega 3 fatty acids
• Long term outcomes
AcknowledgementsBoston Children’s Hospital
– Chris Duggan, MD, MPH
– Sharon Collier, MEd, RD, LDN
– Kathy Gura, PharmD, RPh
– Henry Feldman, PhD
– Catherine Gordon, MD, MS
– Christy Duncan, MD
– Clinical Dietitians - Tara McCarthy, MS, RD, Sarah Larson, MS, RD,Katie Galvin, MS, RD
Dana Farber Cancer Institute– Eva Guinan, MD
– Melissa O’Connor, MS, RN, PNP
Patients of the Dana-Farber Boston Children’s Cancer and Blood Disorders Center Stem Cell Transplant Program
33
39

I have no financial relationships with a commercial entity to disclose.
41

The Changing Face of CF
Learning Objectives:
• Apply current consensus guidelines andresearch findings for the care of infantswith CF
• Gain further knowledge to managepancreatic insufficiency
• Discuss co-morbid complications whichsignificantly impact the nutrition status ofchildren with CF
Early InterventionNewborn Screening Comprehensive Care
Visit Frequency:
• Monthly ‐ 0‐6 months• Every other month – 6‐12 months• Weight checks with PMD prn
Care Coordination:
• Education• Genetic Counseling• Community Resources (WIC, SNAP,
Enzyme rebate programs)
Clinical Intervention:
Sweat testingLab MonitoringChest x‐rays
42

CF Growth Standards
Age Chart Weight/length BMI
0‐12Months WHO > 50%12‐24
Months WHO > 75%
2‐20 Years CDC
> 50% for age
Nutritional strategies
• Optimize calorie intake
• Salt
• Fat-soluble vitamins
• Pancreatic enzymes
Increase Calorie Intake
• Breast milk or milk based formula– Offer Lactation support
• > 60% of infants need high calorie breastmilk or formula
• Choose high calorie foods
• Fortify complementary foods with fat
43

Salt Supplementation
0‐6 Months 6‐12 Months >12 MonthsEating table
foods
1/8 teaspoon 1/4 teaspoon Salt foods liberally
• Add to applesauce with enzymes
• Divide into 3‐4 bottlefeedings
• Add to complimentaryfoods
• Avoid water as beverage
• Counsel for extremeconditions
Fat-soluble Vitamins
• Vitamin deficiencies at newbornscreening
• Monitor levels and adjust doses
• Supplement vitamin D
When to Start PERT• 2 CFTR mutations associated with
Pancreatic Insufficiency (PI)
• Fecal elastase
– Unequivocal signs/symptomsof malabsorption pending lab results• Lack of weight gain since birth• Visibly greasy or oily stools
44

PERT Dosing Guidelines
• 3,000‐5,000 total lipase units at eachfeeding initially
• May exceed 10,000 units lipase/day ininfancy
• 1750-2000 units lipase/kg = optimalgrowth
• Frequent adjustments during infancy
Optimizing Enzyme Efficacy
• Synchronize food and enzymes• Dose at beginning or middle of meal• Do not crush or dissolve enzymes taken
orally• Give divided doses for extended meal
times• PPIs do not increase enzyme
effectiveness
Enteral Nutrition and PERT
• No universal strategy to dose enzymeswith tube feedings– Intact enzymes
• PO enzymes before, middle and end of feeding• Suspend beads in nectar and flush into tube
– Mechanical and chemical dissolution• Dissolve beads in bicarbonate solution• Crush beads or non-enteric coated enzymes
– Add to formula + time = predigested formula
45
Troubleshooting Enzymes and Enteral Nutrition
• Anecdotal evidence to use formulaswith more LCT (Two Cal HN™ vs Nutren 2.0™ )
• Dose enzymes based on fat content offormula– 2000 units lipase/gm fat
• Closed tube feeding systems
CF-Related Diabetes
• Occurs in ~ 20% Teens with CF– Start screening with OGTT age 10
• Requires insulin and few diet restrictionswith carb counting– Dose insulin with overnight tube feedings
• Greatly worsens clinical outcomes
Constipation• Very common in CF: Sticky intestinal mucous
• Leads to poor appetite, abdominal pain, symptomsof malabsorption from overflow diarrhea
• Polyethylene Glycol (PEG) is common treatment– Daily dosing– Purge clean-outs
• Chronic treatment often required
46

47

Nutritional Issues in Cholestatic Disease
NASPGHAN-CPNP Joint Session
Binita M. Kamath, MBBChir MRCP MTRAssociate Professor
Division of Gastroenterology, Hepatology and NutritionThe Hospital for Sick Children
University of Toronto
October 2015
THE HOSPITAL FOR SICK CHILDREN
I have no financial relationships with a commercial entity to disclose.
OUTLINE
• Overview of cholestatic diseases
• Mechanisms of nutritional impairment in cholestasis
• Impact of poor nutrition in cholestasis
• Optimizing nutrition in cholestasis
48
Cholestatic Diseases
Cholestatic Diseases
• Cholestasis = interruption in bile flow
• Bile: bilirubin, bile salts, cholesterol
• Hallmark disease: biliary atresia (BA)
• Other diseases
– Alagille syndrome
– Progressive familial intrahepatic cholestasis
– Alpha-1-antitrypsin deficiency
Mechanisms of Nutritional
Impairment in Cholestasis
49

Mechanisms of Malnutrition in Cholestasis
1. Severe depletion of intraluminal bile acids andsecondary fat malabsorption
2. Poor intake due to
a. organomegaly and/or ascites (reduced gastric capacity)
b. anorexia (toxins?)
3. Portal hypertension exacerbates malabsorption
4. Pruritus
Mechanisms of Malnutrition in Cholestasis
5. Increased energy expenditure
• Measured REE almost 30% higher than expected in BA
• Normal infants retain 50% energy intake for growth, but only 35% in BA
6. Hepatic IGF-1
7. Recurrent infections
Assessment of Malnutrition in Cholestasis
1. Weight – affected by ascites
2. Anthropometricsa. mid-arm circumference b. TSFc. Head circumference
50

Impact of Poor Nutrition in
Cholestasis
Outcomes of Malnutrition in Cholestasis
• Growth failure is an important factor associated with
death or moving to ICU in a multi-center cohort
(mostly BA)
– height or weight <2 s.d., associated with increased morbidity
and mortality PELD
• Growth failure was an independent risk factor for pre-
transplant mortality, post-transplant mortality, and
even graft failure in 755 listed BA patients (SPLIT)
McDiarmid et al, Transplantation 2002 & Utterson et al, J Ped 2005
Outcomes of Malnutrition in Cholestasis
• BA Research Consortium
• N=100
• Infants with BA who ultimately
required LT or died had poorer
growth after HPE compared to
those who survived with their
native liver at 24 months of age
DeRusso et al, Hepatology 2007
51

Outcomes of Malnutrition in Cholestasis
• Severity of malnutrition and poor growth in children
with BA before LT is predictive of cognitive
performance years after transplantation
Wayman KI et al, J Ped 1997
Optimizing Nutrition in Cholestasis
Lipid
‐MCTs carried in PV system
‐ 30‐50% of total lipids as MCT
Lipid
‐MCTs carried in PV system
‐ 30‐50% of total lipids as MCT
Protein
‐ 2‐3g/kg/d
‐BCAA?
Protein
‐ 2‐3g/kg/d
‐BCAA?
CHO &Energy
‐ 120‐150%
‐ 2/3 as CHO polymer
CHO &Energy
‐ 120‐150%
‐ 2/3 as CHO polymer
Vitamin EVitamin E
Vitamin DVitamin D
Vitamin KVitamin K
H2O & Electrolytes
‐rarely restrict H2O
‐restrict Na to 2‐3mmol/kg/d
H2O & Electrolytes
‐rarely restrict H2O
‐restrict Na to 2‐3mmol/kg/d
52
MCTs: The Data?
• Difficult to specify the ideal dietary fat content and ratio of MCT to LCT
– Limited data point to better fat solubilization and growth ofcholestatic infants fed with 30% or 70% MCT against a 50/50% mixture of MCT/LCT
– Very high (>80%) MCT to total lipid risks of essential fatty acid deficiency
– Recent study shows effectiveness of enteral MCT formula (140% DRI) as compared to ad lib oral intake of same formula
Macias-Rosales, JPGN 2015
PUFA / EFA
• Intraluminal bile salt depletion
• Levels difficult to measure and interpret.
• Most centres lack access to clinical measurement
Branch chain amino acids (BCAA)
– Randomized study in children with ESLD demonstrated improved nutritional status and body composition in those with BCAA-enriched formula
– MCT-containing complete BCAA formulas are expensive and not readily available
Chin SE et al, 1992
53

Water and Electrolytes
• Typically normal fluid – rarely restricted
• Sodium restricted to 1-2 mmol/kg/day
– Do not correct the hyponatraemia of ESLD
– Severe hyponatraemia may require fluid restriction
• Potassium 2mmol/kg/day
Nutritional Requirements in Cholestasis
Nutritional element Daily Requirement Source
Lipid 30‐50% of total energy30‐70% MCT
PUFA/LCP >10% of total energy rapeseed, walnut,fish, sunflower, soybean oils
Protein 3‐4g/kg Whey protein
BCAA 10% total AAs
Energy 120‐150% requirement for age 2/3 as CHO, 1/3 as lipid
CHO CHO polymer
Na Minimum
K 2‐3 mmol/kg
Fat Soluble Vitamins
Shneider, Pediatrics 2012
54

Parenteral Nutrition
• Indications
– diarrhea, vomiting*
– repeated episodes of gastrointestinal hemorrhage
• Risk of worsening decompensated liver disease with PN
is low
– mild biochemical deterioration
• Can typically achieve mixed enteral and PN
Parenteral Nutrition
• 20 year retrospective review, single centre
• BA listed for LTx, <36 months
• PN=25, Non-PN=22
• From the start of PN administration to the clinical endpoint, mean
TSF z‐score increased from ‐2.5 ± 0.2 to ‐1.8 ± 0.2 (p=0.003), and
mean MAC z‐score increased from ‐2.2 ± 0.2 to ‐1.4 ± 0.2 (p<0.0001).
• Of the 22 patients in the non‐PN group, 6 (27%) received NG feeds
Sullivan J, Liver Transp 2012
Parenteral Nutrition
55

Gaps in Knowledge
Summary
56
Iron Deficiency and the Developing Brain
Michael K. Georgieff, M.D.Professor, Pediatrics and Child Development
Head, Section of NeonatologyDirector Center for Neurobehavioral Development
University of Minnesota Masonic Children’s HospitalUniversity of Minnesota
Minneapolis, MN
I have received a research grant from Mead Johnson
Nutritionals.I have no conflict of interest for
this presentation
Learning Objectives
Define the common causes of iron deficiency in newborn infants and toddlers
Identify the regions of the brain that are particularly vulnerable to early childhood iron deficiency
Characterize the behaviors that are affected by early life iron deficiency
57

OverviewWhy worry about iron?
Nutrient-brain interactions- why the brain needs iron
Iron needs in infancy– Sequelae of iron deficiency
Fetal and neonatal iron– Term and preterm infants– Sequelae of iron deficiency
Why Worry About Iron Deficiency?
2 billion people world-wide are iron deficient (WHO)– 30-50% of pregnant women
Every cell/organ system needs iron for proper development and subsequent function
Iron deficiency anemia is associated with clinical symptoms– Due to tissue level ID
– Symptoms occur prior to anemia
Main reason to worry is the effect on the developing brain– Cognitive and motor effects
– Some temporary (while ID), others long-term (after iron repletion)
– The long-term effects are the real cost to society
• Increased depression, anxiety, risk of schizophrenia, autism
• Loss of job and educational potential
Early Nutrition and Brain Development:General Principles
Positive or negative nutrient effects
on brain development
Based on…
Timing, Dose and Duration of Exposure
Kretchmer, Beard, Carlson, 1996
58
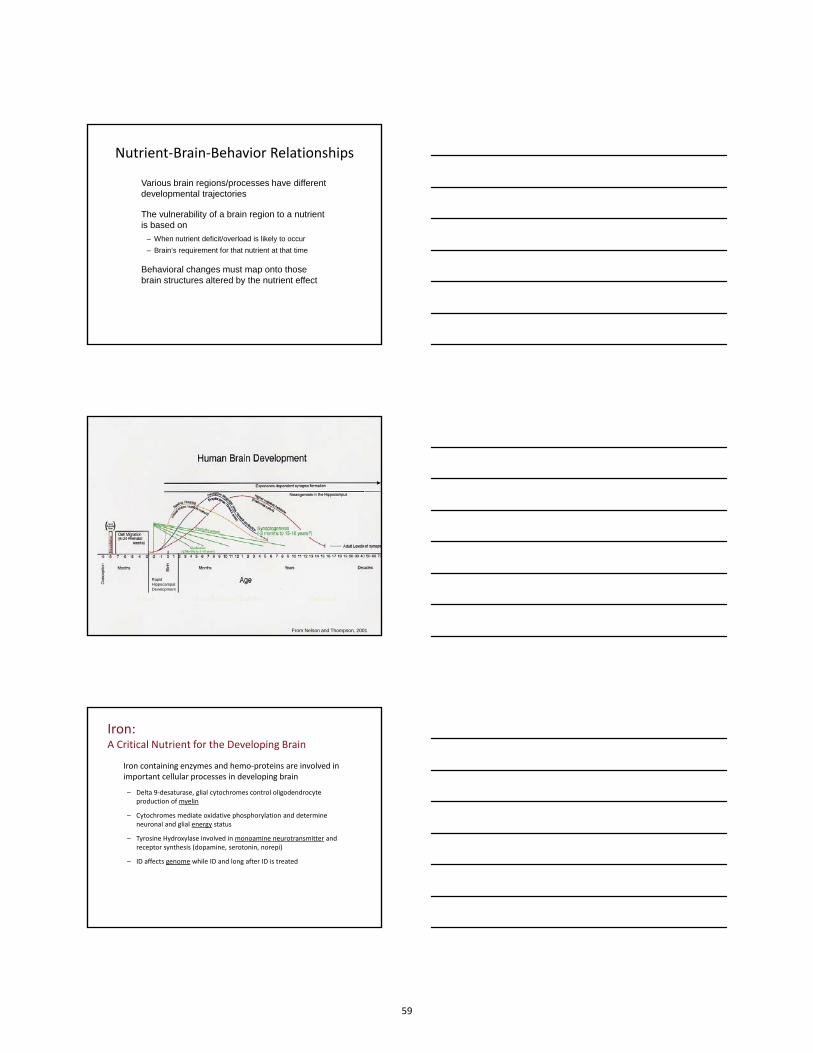
Nutrient‐Brain‐Behavior Relationships
Various brain regions/processes have different developmental trajectories
The vulnerability of a brain region to a nutrient is based on
– When nutrient deficit/overload is likely to occur
– Brain’s requirement for that nutrient at that time
Behavioral changes must map onto those brain structures altered by the nutrient effect
Fetus Late Infancy/Toddler Pubertal
RapidHippocampalDevelopment
From Nelson and Thompson, 2001
Iron:A Critical Nutrient for the Developing Brain
Iron containing enzymes and hemo‐proteins are involved in important cellular processes in developing brain
– Delta 9‐desaturase, glial cytochromes control oligodendrocyteproduction of myelin
– Cytochromes mediate oxidative phosphorylation and determineneuronal and glial energy status
– Tyrosine Hydroxylase involved in monoamine neurotransmitter and receptor synthesis (dopamine, serotonin, norepi)
– ID affects genome while ID and long after ID is treated
59

Fetus Late Infancy/Toddler
The Differential Effect of Timing of ID on Brain Development
RapidHippocampalDevelopment
Iron Deficiency in the Infant or Toddler (6-24 months)
Lozoff et al, Nutr Rev, 2006
Factors Determining Infant Iron Status
Courtesy of B. Lozoff, MD
60
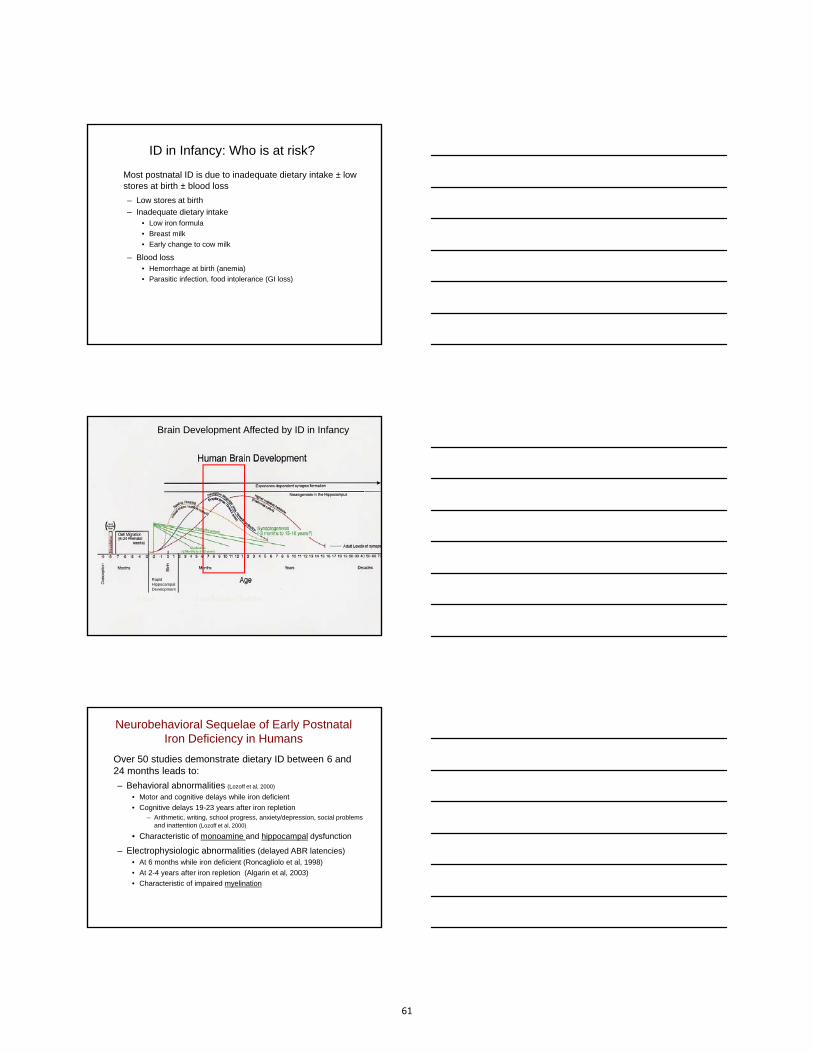
ID in Infancy: Who is at risk?
Most postnatal ID is due to inadequate dietary intake ± low stores at birth ± blood loss
– Low stores at birth
– Inadequate dietary intake• Low iron formula
• Breast milk
• Early change to cow milk
– Blood loss• Hemorrhage at birth (anemia)
• Parasitic infection, food intolerance (GI loss)
Fetus Late Infancy/Toddler
Brain Development Affected by ID in Infancy
RapidHippocampalDevelopment
Neurobehavioral Sequelae of Early Postnatal Iron Deficiency in Humans
Over 50 studies demonstrate dietary ID between 6 and 24 months leads to:
– Behavioral abnormalities (Lozoff et al, 2000)
• Motor and cognitive delays while iron deficient
• Cognitive delays 19-23 years after iron repletion– Arithmetic, writing, school progress, anxiety/depression, social problems
and inattention (Lozoff et al, 2000)
• Characteristic of monoamine and hippocampal dysfunction
– Electrophysiologic abnormalities (delayed ABR latencies)• At 6 months while iron deficient (Roncagliolo et al, 1998)
• At 2-4 years after iron repletion (Algarin et al, 2003)
• Characteristic of impaired myelination
61

85
90
95
100
105
110
115
1 5 12 17Age (years)
Cognitive Composite Score
Good Iron Status *
Chronic Iron Deficiency **
Effect of Iron Deficiency in Infancy on General Cognitive Performance
*initial difference, t = 10.1, p < 0.001*slope = 7.03, p = 0.001
**initial difference, t = 3.7, p = 0.04**slope NS
(B Lozoff et al)
Courtesy of B. Lozoff
Effect of Iron Deficiency in Infancy on Affect and Engagement
Courtesy of B. Lozoff
Effect of Iron Deficiency in Infancy on Affect and Engagement
62

Motor Coordination and Affect in Human Toddlers: a Dose Response Effect (Lozoff et al, 2008)
IDA NA ID
IS
p=0.05
0
0.1
0.2
0.3
0.4
0.5
Prob
abili
ty o
f per
form
ing
with
poo
rco
ordi
natio
n
Scor
e p < 0.05
03738394041424344
IDA NA ID IS
Orientation/Engagement (BRS)
Shyness (EAS)
p < 0.01
0
1.9
2.1
2.3
2.5
2.7
IDA NA ID IS
Scor
e
NigrostriatalPathway
Tuberohypophyseal Pathway
Mesocorticolimbic Pathway
Major Dopamine Pathways
Courtesy of B. Lozoff
Neurotransmitter Effects in the Rat
Effects on monoamines, esp dopamine, known since late 1970’s(studies by Yehuda, Youdim, Beard)
While ID: Decreased DAT, D1R, D2R and increased SERT– Regional differences- Large effects in striatum, ventral midbrain
– Changes related to timing and severity (E Unger et al, 2012)
63

Slower Nerve Conduction Velocity: Evoked Potential Latencies 3 Years after Iron Rx
*** p < 0.001
Algarin et al. (2003). Pediatric Research 53:217‐223
4.1
4.0
3.9
3.8
ABR Central Conduction Time(Wave I-V Interval, ms)
90
100
80
VEP Wave P100 Latency (ms)
***
110
***
Former Iron Deficient Anemic
Control
Myelin Effects in the Rat
Altered fatty acid profile in myelin fraction
Decreased myelin proteins, including myelin basic protein
Decreased oligodendrocyte proliferation
Transcripts for myelin basic protein affected
– short term (while ID)
– long term (at P180 after iron repletion)
(Studies by Connor, Clardy, Rao)
Fetus Late Infancy/Toddler
Brain Development Affected by Fetal/Neonatal ID
RapidHippocampalDevelopment
64

Fetal Iron: Endowment and Distribution
Fetuses have 75mg of elemental iron per kilogram body weight during 3rd trimester
– Term infant: 250mg
– 24 weeker (500g): 37.5 mg
Majority is in the RBCs (55mg/kg)
Liver storage pools are relatively large at term (12 mg/kg); serum ferritin >40 mcg/L
Non-storage tissues, including brain, heart, skeletal muscle account for the rest (8 mg/kg)
What Can Negatively Affect Neonatal Iron Status?
Decreased maternal iron supply– Fetus with very iron deficient mother (Hgb<8.5)– Common (>30%) in developing countries– No studies of newborn brain iron status
Decreased placental iron transfer during gestation– Prematurity
• Iron accreted during third trimester• Generally negative iron balance during NICU stay
– IUGR due to maternal hypertension during pregnancy• 50% affected• 75,000 infants per year in US• 32% decrease in brain iron concentration (Georgieff et al, 1995)
– Early cord clamping
Term Infants:What Can Negatively Affect Neonatal Iron Status?
Diabetes Mellitus during pregnancy
– Chronically hypoxic fetus (IDM)=> Increased erythropoeisis
– 65% affected
– 150,000 infants per year in US
– 40% decrease in brain iron concentration (Petry et al, 1992)
Basic principle:
Iron prioritized to RBCs over brain &
other organs when Fe demand> Fe supply
65

Factors that Determine Preterm Infant Iron Status in the NICU
Negative Iron Balance• Low Endowment (IUGR)
• Phlebotomy Losses
• Iron Rx at 2 months
• Iron Rx < 2mg/kg/d
• rhEpo Rx
• Rapid Postnatal Growth
Positive Iron Balance• Older gestation & AGA
• RBC Transfusion
• Iron Rx at 2 weeks
• Iron Rx @ 2-4 mg/kg/d
• Iron Rx @ 6mg/kd/d c rhEpo
• Parenteral Iron
• Slow Postnatal Growth Rate
Preterm infants have elevated ZnPP at 34 weeks PCA (Winzerling &Kling)
Neurobehavioral Sequelae of Fetal and Neonatal IDFewer studies than in postnatal ID
– Decreased maternal iron status• increased risk of schizophrenia in offspring (Insel et al, 2008)• increased risk of autism in offspring (Schmidt et al, 2014)
– Term infants with low neonatal iron stores have• impaired auditory recognition memory processing (Siddappa et al, 2004)
• poorer school age neurodevelopment (Tamura et al, 2002)
• worse immediate and delayed recall at 3.5 y (Riggins et al, 2009)
– Preterm infants with now iron stores at 36 weeks PCA• more abnormal reflexes (Armany-Sivan, 2006)
• longer conduction times on BAER (Amin et al, 2010)
– Early iron supplementation in preterms => higher mental processing composite score at 5.3 years (Steinmacher et al, 2007)
SUGGESTS SIGNIFICANT HIPPOCAMPAL AND MYELIN IMPAIRMENTS
Hippocampal Effects: Rodent ModelsShort and long-term genomic changes (ES Carlson et al, 2007)
– Dendritic structure, synaptic efficacy, oxidative metabolism
Reduced energy status (M deUngria et al, 2000)
Glutamate and GABA sequestration (R Rao et al, 2003)
Altered dendritic morphology (ES Carlson et al, 2009)*
Long-term suppression of BDNF and its receptor (P Tran et al, 2009)
Reduced LTP (long-term potentiation) (Pisasnsky et al, 2013)
Reduced learning and memory– Morris Water Maze (B Felt and B Lozoff, 1996)
– Radial Arm Maze (AT Schmidt et al, 2007)
66

Summary
• Iron plays a critical role in early neurodevelopment
• Early iron deficiency without anemia affects brainfunction
• ID brain/behavior alterations persist after resolution ofID
• Early detection of at-risk infants is crucial for brainhealth
• Need new tools to detect pre-anemic iron deficiency
References 1. Lozoff B, Beard J, Connor J, Felt B, Georgieff M, Schallert T. Long‐lasting nueral and behavioral effects of early iron deficiency in infancy. Nutr Rev
64:S34‐S43, 2006.
2. Kretchmer, N., Beard, J.L., Carlson, S. (1996). The role of nutrition in the development of normal cognition. American Journal of Clinical Nutrition, 63, 997S‐1001S.
3. Thompson RA & Nelson CA, (2001) Developmental science and the media. Early brain development. American Psychologist 56(1), 5‐15.
4. Lozoff et al, 2008 Dose‐response relationships between iron deficiency with or without anemia and infant social‐emotional behavior. J Pediatr. 2008;152(5):696‐702.
5. Roncagliolo M, Garrido M, Walter T, Peirano P, Lozoff B. Evidence of altered central nervous system development in infants with iron deficiency anemia at 6 mo: delayed maturation of auditory brainstem responses. Am J Clin Nutr. 1998;68(3):683‐90.
6. Algarín C, Peirano P, Garrido M, Pizarro F, Lozoff B. (2003). Iron deficiency anemia in infancy: long‐lasting effects on auditory and visual system functioning. Pediatric Research. 53, 217‐23
7. Unger EL, Hurst AR, Georgieff MK, Schallert T, Rao R, Connor JR, Kaciroti N, Lozoff B, Felt B. Behavior and monoamine deficits in pre‐ and peri‐natal iron deficiency are not corrected by early postnatal moderate or high iron diet in rats. J Nutrition. 142: 2040‐9, 2012.
8. Clardy SL, Wang X, Zhao W, et al. Acute and chronic effects of developmental iron deficiency on mRNA expression patterns in the brain. J Neural Transm Suppl. 2006;71:173‐96.
9. Petry CD, Eaton MA, Wobken JD, Mills MM, Johnson DE, Georgieff MK. Iron deficiency of liver, heart, and brain in newborn infants of diabetic mothers. J Pediatr 121:109‐114, 1992.
10. Siddappa AM, Georgieff MK, Wewerka S, Worwa C, Nelson CA, deRegnier R‐A. Auditory recognition memory in iron‐deficient infants of diabetic mothers. Pediatric Research 55: 1034‐1041, 2004.
11. Tamura T, Goldenberg RL, Hou J, et al: Cord serum ferritin concentrations and mental and psychomotor development of children at five years of age, J Pediatr 2002; 140:165.
12. Amin SB, Orlando M, Eddins A, MacDonald M, Monczynski C, Wang H. J Pediatr 2010; 156:377‐81.
13. Insel, B.J., Schaefer, C.A., McKeague, I.W., Susser, E.S., Brown, A.S. (2008) Maternal iron deficiency and the risk of schizophrenia in offspring.Archives of General Psychiatry, 65, 1136‐44.
14. Riggins T, Miller NC, Bauer PB, Georgieff MK, Nelson CA. Consequences of Low Neonatal Iron Status due to Maternal Diabetes Mellitus on ExplicitMemory Performance in Childhood. Developmental Neuropsychology, 34:762‐79, 2009.
15. Carlson ES, Tkac I, Magid R, O’Connor MB, Andrews NC, Schallert T, Gunshin H, Georgieff MK, Petryk A. Iron is essential for neuron developmentand memory function in mouse hippocampus. J Nutrition,139(4):672‐9, 2009.
16. Tran PV, Fretham SJB, Carlson ES, Georgieff MK. Long‐term reduction of hippocampal BDNF activity following fetal‐neonatal iron deficiency in adult rats.
17. Pisansky MT, Wickham RJ, Su J, Fretham S, Yuan L‐L, Sun M, Gewirtz JC, Georgieff MK. Iron deficiency with or without anemia impairs prepulseinhibition of the startle reflex. Hippocampus. 23(10):952‐62; 2013.
18. Fretham SJB, Carlson ES, Georgieff MK. The role of iron in learning and memory. Advances in Nutrition, 2: 1‐10, 2011.
Conceptual Model of Neurodevelopmental Effects of Early Iron Deficiency
PoorerOutcome
Infant Iron
Deficiency
LearningExperiences
DisadvantagedBrain Iron
FunctionalIsolation
Limited Support forChild Dev.
Parenting
Poor feeding
Neurochemistry‐dopamine, striatum
Neuroanatomy‐myelin,dendrites
Neurometabolism
Cognitive,Motor
Affective‐Social
MaternalDepression
practices Environment
Maternal IronDeficiency
‐hippocampus
LanguageSensory,
Courtesy of B. Lozoff
From Lozoff et al, 2006
67

Individualized Nutrition Plans for Patients with IBD
Karen Warman, RDAthos Bousvaros, MD, MPH
Inflammatory Bowel Disease CenterCPNP, October 2015
Dr. Bousvaros has the following financial relationships to disclose:
Prometheus – research supportDyax ‐ consultantShire – data safety monitoring boardJanssen – research supportTakeda – consultantPeabody Arnold ‐ medicolegal
No products or services produced by any of these companies are relevant to my presentation.
• Can involve any partof the intestine.
• Transmuralinflammation
• Abscesses and fistulae
• Recurs after surgery
• Nutritional therapies are effective
• High colon cancer risk
• Colon only
• Inner lining only
• Abscesses very rare
• Surgery “cures”
• Nutritional therapies usually ineffective
• High colon cancer risk
Crohn’s disease vs. Ulcerative Colitis
68

Ulcerative colitis – continuous Crohn’s colitis - discontinuous
Theory of pathogenesis
Exposure of a genetically predisposed host to an environmental trigger, resulting in immunologically mediated damage against the bowel.
Variable phenotypes of enterocolitis in IL‐10 deficient mice
(Kim and Sartor, Gastroenterology 2005;128:891‐906)
IL-10 knockout mouse
Escherichiacoli
Enterococcusfaecalis
Cecal(Crohn-like)inflammation
Distal colitis (UC-like)
69

Inflammatory Bowel Disease Diagnostic Approach
• Suspect the diagnosis– History, Exam, CBC, ESR, Albumin– Possible role for serologic testing
• Exclude other etiologies– Stool culture, C. difficile, TB skin test
• Classify disease as CD or UC• Determine disease location
– Upper endoscopy, colonoscopy, UGI/SBFT• Identify extraintestinal manifestations
– Liver function tests, Joint, Skin, Eye exams
Crohn’s – Oral ulcers
Crohn’s disease – Small Bowel Imaging
• Options– Upper
GI/SBFT– Abdominal
CT– Abdominal
MRI
ileum
Ascending colon
70

Normal colon
Smooth and shinyNormal vascularityTortuousNormal folds
Perianal CD
Ulcerative colitis
Loss of vascularpattern
GranularityExudateDiffuse continuous
diseaseNo ileal involvement
71
IBD ‐management
• Medical• Surgical• Nutritional• Supportive (psychosocial)• Surveillance
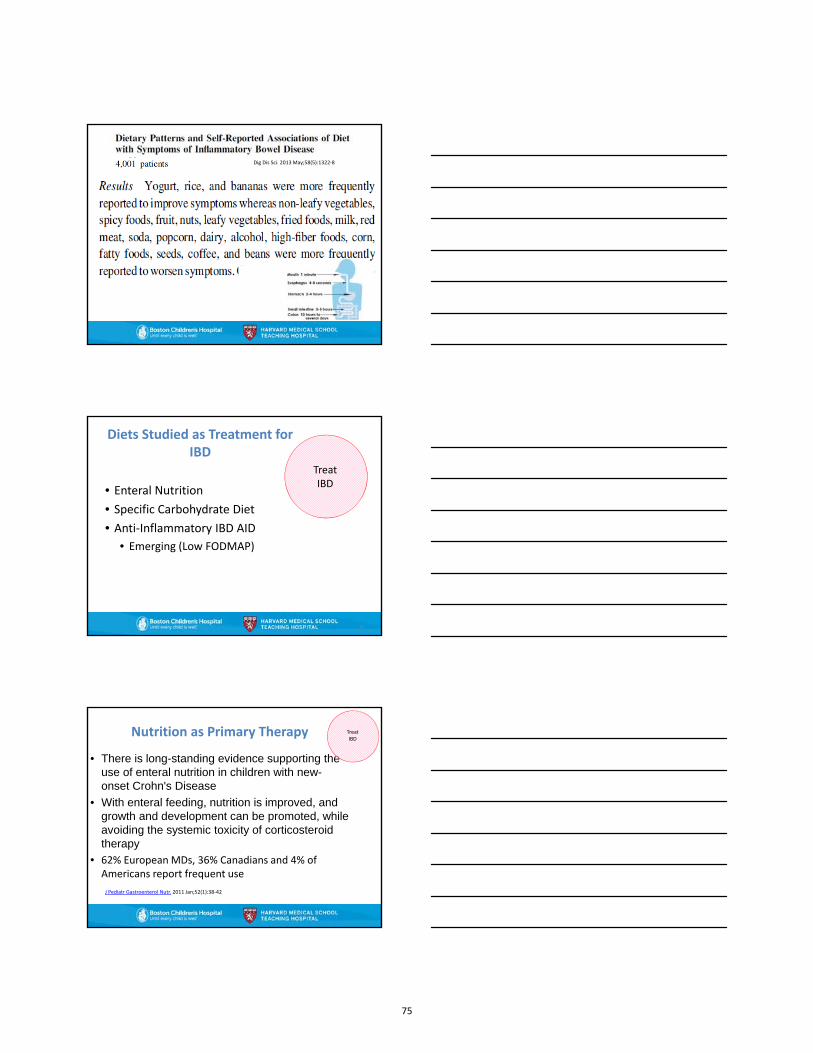
Crohn’s colitis
Deep fissuresSegmental
distributionRectal sparingIleal involvementGranulomas
on biopsy
The “Balancing Act”
72

Treatment options for UC and Crohn’s diseaseUlcerative colitis Crohn’s disease
Aminosalicylates
Corticosteroids
Infliximab
Calcineurin inhibitors
Enteral nutrition
Corticosteroids
Infliximab
Adalimumab
Aminosalicylates
6MP/azathioprine
Infliximab
Aminosalicylates?
Antibiotics?
6MP/azathioprine
Methotrexate
Anti-TNF agents
Induction
Main-tenance
Goals For Nutritional Intervention
Meet Nutrient Needs
Symptom Control
TreatIBD
Nutrition and Diet
• Nutrition is what our body needs on a daily basisto stay healthy
• Diet (food) is the choice of what we eat.
• and overall wellness
73

Nutrients At Risk
Meet Nutrient Needs
Meet Nutrient Needs
• Protein• Calories• Vitamin D• Iron• Zinc• Folic Acid• B12• Magnesium• Calcium
19
Dietary Components Targeted
1. Animal Fat2. High sugar intake3. Gliadin4. Emulsifiers5. Maltodextrins6. Low Fiber Intake
20
IngredientsCream, Skim Milk, Sugar, Vanilla Extract, Guar Gum, Salt, Mono & Diglycerides, Dextrose, Polysorbate 80, Carrageenan, Cellulose Gum.
What do they hear?
– Raw vegetables– Cruciferous
vegetables– Citrus fruits– Red meat– Carbonated
beverages– Coffee– Tea
Avoid– Alcohol– Fatty and fried foods– Spicy Foods– Sugars– Seeds – Popcorn
21
Clinical Gastroenterology and Hepatology 2014;12:1592‐1600
74
Dig Dis Sci. 2013 May;58(5):1322‐8
Diets Studied as Treatment for IBD
• Enteral Nutrition• Specific Carbohydrate Diet• Anti‐Inflammatory IBD AID
• Emerging (Low FODMAP)
23
TreatIBD
Nutrition as Primary Therapy
• There is long-standing evidence supporting theuse of enteral nutrition in children with new-onset Crohn's Disease
• With enteral feeding, nutrition is improved, andgrowth and development can be promoted, whileavoiding the systemic toxicity of corticosteroidtherapy
• 62% European MDs, 36% Canadians and 4% ofAmericans report frequent use
J Pediatr Gastroenterol Nutr. 2011 Jan;52(1):38‐42
TreatIBD
75
Enteral Nutrition
• For a period of 6 to 8 weeks the diet is abeverage that will support nutrient needs
• These beverages replace standard meals
• No solid foods are included
• Either take by mouth or given by tube
TreatIBD
Theories as to why it works
• Providing calories and nutrients• Removal of dietary components which
– Affect microbial composition– Decrease pro‐inflammatory responses– Promote restitution of the epithelial barrier
26
TreatIBD
How well does exclusive enteral nutrition work?
• Response rates:– In adults: 55%– In children: 50% to 75%
• Effective for Crohn’s disease but not Ulcerative Colitis– May be more effective in small bowel Crohn’s
• Elemental (hypoallergenic) and Polymeric (wholeprotein) formulas both seem to work
• Probably not a good long term treatment• Partial enteral nutrition has shown a 50% reduction in
relapse in CD compared to a regular diet.
J Hum Nutr Diet.2013 27(suppl. 2) 28‐35,
TreatIBD
Inflamm Bowel Dis. 2013 Jun;19(7):1374‐8Gut 2006:;55:356‐361Aliment Pharmacol Ther 2006 24,1333‐1340
76

28
Specific Carbohydrate Diet
• Includes– Meat, fish, eggs, vegetables, nuts, low‐sugar fruits
• Avoids– Sugar– Diary, except homemade fermented yogurt and
lactose reduced milk– All grains (no wheat, rye, barley, corn, millet,
quinoa, rice• No pasta, bread, baked goods
29
TreatIBD
Specific Carbohydrate Diet • JPGN 2014;58:87‐91
– Retrospective 7 children with Crohn’s– No Immunosuppressive meds– On diet 5 to 30 months– Symptoms ,Serum albumin, C‐reactive protein, hematocrit, stool calprotectin either
normalized or improved by 3 months.
• JPGN 2014;59:516‐521– Prospective study of 9 children with Crohn’s– All saw clinical and mucosal improvement on 12 to 52 weeks of SCD
• J Acad Nutr Diet 2015;115:1226‐1232– Descriptive study of 50 Patients on SCD (9 had UC) remainder CD– 42 % were on no medication– Quality of Life questionnaire average: 60.0 on a scale of 35 to 70– Mean time on diet 34 months– 16 of the patients reported eating forbidden foods (7 on no drugs)– Meal preparation estimation of 10‐11 hours a week
30
77
31
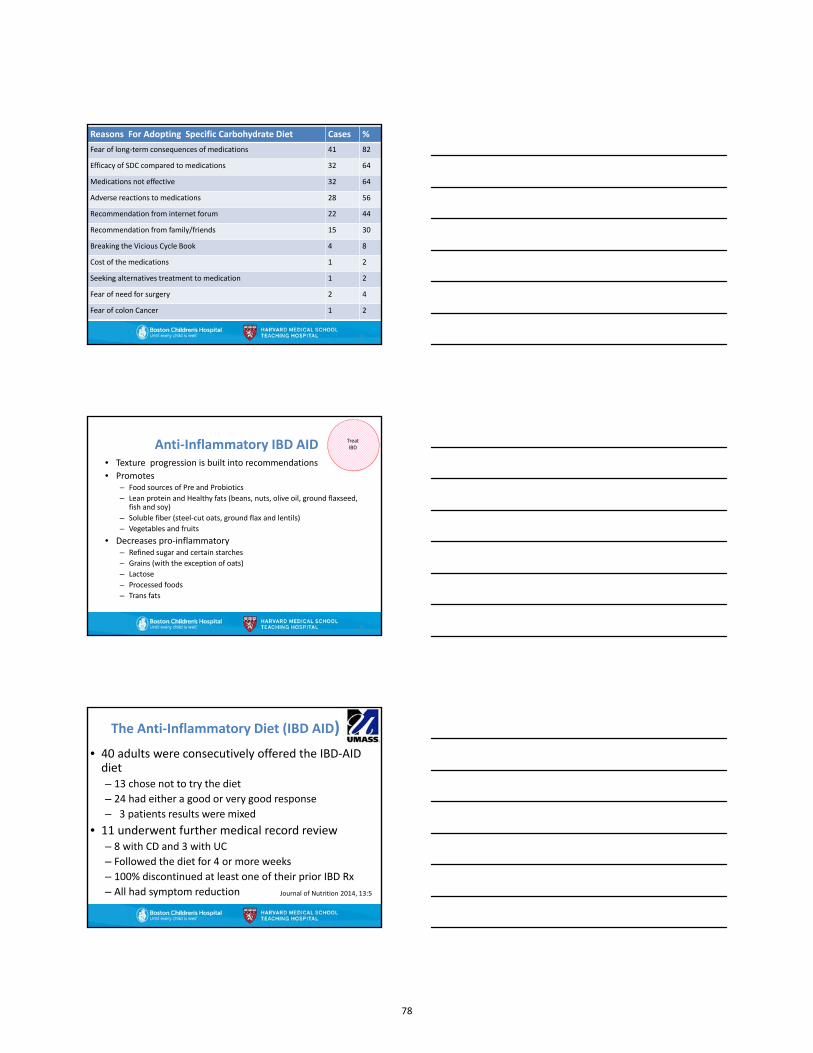
Reasons For Adopting Specific Carbohydrate Diet Cases %
Fear of long‐term consequences of medications 41 82
Efficacy of SDC compared to medications 32 64
Medications not effective 32 64
Adverse reactions to medications 28 56
Recommendation from internet forum 22 44
Recommendation from family/friends 15 30
Breaking the Vicious Cycle Book 4 8
Cost of the medications 1 2
Seeking alternatives treatment to medication 1 2
Fear of need for surgery 2 4
Fear of colon Cancer 1 2
Anti‐Inflammatory IBD AID• Texture progression is built into recommendations• Promotes
– Food sources of Pre and Probiotics– Lean protein and Healthy fats (beans, nuts, olive oil, ground flaxseed,
fish and soy)– Soluble fiber (steel‐cut oats, ground flax and lentils)– Vegetables and fruits
• Decreases pro‐inflammatory– Refined sugar and certain starches – Grains (with the exception of oats)– Lactose – Processed foods– Trans fats
32
TreatIBD
The Anti‐Inflammatory Diet (IBD AID)
• 40 adults were consecutively offered the IBD‐AIDdiet– 13 chose not to try the diet– 24 had either a good or very good response– 3 patients results were mixed
• 11 underwent further medical record review– 8 with CD and 3 with UC– Followed the diet for 4 or more weeks– 100% discontinued at least one of their prior IBD Rx– All had symptom reduction Journal of Nutrition 2014, 13:5
78

Diets Targeting Symptom Control
• Low Residue/Fiber• Low Lactose• Low FODMAP
34
Symptom Control
Low Fiber/residue diet• Indications
– To prevent bowel obstructions in patients withCrohn’s disease and narrowed segments of intestine.
• (Gut 1985:26: 989‐93) 71 patients following low fiber were randomized to reintroduce fiber, showing no difference in outcome
– To reduce (not eliminate) the residue in the colonpre‐ and postoperatively.
– Definition is usually < 10 grams fiber per day. Thediet is intended for short‐term use.
Symptom control
Nutrition in Clinical Practice 2015 30:462‐73
Why not continue on low fiber?
• High red meat protein intake• High fat • Trend towards highly refined foods with food
additives and preservatives with added soybeanoil (sources of Omega‐6)
• Fiber offers pro and prebiotics that change thebalance of beneficial bacteria.
• Lignans, flavonoids and anti‐oxidants from fruits and vegetables
• Higher sodium intake especially problematic withuse of steroids
79

Primary sources of FODMAPS
Low FODMAP• 52 patient with Crohn’s• 20 patients with UC• Instructed on Low FODMAP
70% followed the diet• 50% responded favorable
to the diet defined as• Improvement in 5 out of 10 of the
following symptoms• Abdominal pain• Bloating• Passing gas (wind)• Diarrhea
38
Journal of Crohn’s and Colitis:2009; 3, 8‐14
SymptomControl
Emulsifiers• CMC or polysorbate ‐80 given in
drinking water or chow• Significant increase in colitis• Amount consistent human
consumption • Polysorbate 80
– Ice cream, whipped cream, mayonnaise, salad dressings, rotisserie chicken
• Carboxymethylcellulose– CMC, cellulose gum or cellulose
and sodium carboxymethylcellulose
– Ice cream, dressing, cheese, icing, toppings, cottage cheese, creamcheese spread
39
2013:J Crohn’s and Colitis 7,338‐341
2015:Nature 7, 92‐96
80

Diet Restriction At Risk Nutrients
Low‐Residue/Fiber < 10 gm fiber/day ; generally insoluble fiber such as raw fruits and vegetables and whole grains
Folate, Vitamins A & C, PotassiumHigh fat
Enteral Only formula used None, complete nutrition
Specific Carbohydrate Diet All grains, lactose, processed meats and legumes
Folate, thamin, B6, riboflavin, niacin, calcium and Vitamin D
Low‐FODMAP Fermentable Oligo‐, Di and Mono Saccharides and PolyolsNo wheat, barley and rye,Defines vegetables and fruitsNo sugar alcohols
Folate, thiamin, B6 , riboflavin, niacin, calcium and Vitamin D,Vitamins A and C without guidance
Anti‐Inflammatory IBD AID All grains except Oatmeal Lactose, processed meats, trans fats.
Folate, thiamin, B6 , riboflavin, niacin, calcium and Vitamin D,
40
Meet Nutrient Needs
Symptom Control
TreatIBD
Summary
• Enteral nutrition is the only diet approach toinduction at this time
• 80% enteral nutrition is the 2nd best option• Maintenance is likely to be a hybrid of the diets
based on– Functional symptoms– Ability to follow a restrictive diet– Degree of motivation from both the family and the
child– Nutritional status
42
81
43
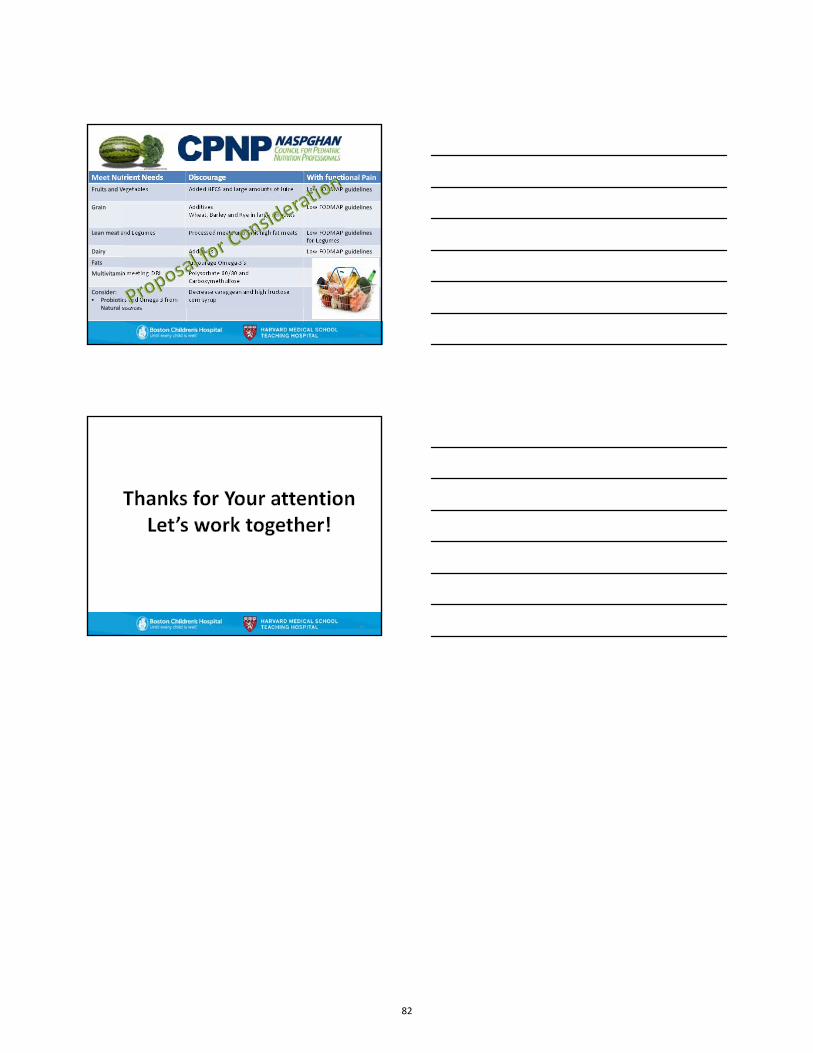
Meet Nutrient Needs Discourage With functional Pain
Fruits and Vegetables Added HFCS and large amounts of Juice Low FODMAP guidelines
Grain AdditivesWheat, Barley and Rye in large amounts
Low FODMAP guidelines
Lean meat and Legumes Processed meats and limit high fat meats Low FODMAP guidelinesfor Legumes
Dairy Additives Low FODMAP guidelines
Fats Encourage Omega‐3’s
Multivitamin meeting DRI Polysorbate 60/80 and Carboxymethullose
Consider:• Probiotics and Omega 3 from
Natural sources
Decrease caraggean and high fructose corn syrup
44
82

CPNP Symposium, Saturday 10/9/15
Case Study Breakout: The Elimination Diet: Practical Tips and Pitfalls
Wendy Elverson, RD, LDN, Boston Children’s Hospital, Center for Nutrition
CASE: Baby Girl Jane with FPIES (Food Protein Induced Enterocolitis Syndrome)
History:
Full term, breast fed, @ 2 weeks fussiness, abdominal distension, mucous in stool Milkfree/soy free diet for mother and Ranitidine followed by Omeprazole Rx for baby.
2 months ↑ Omeprazole. 3 months nursing refused, EBM (expressed breast milk) via bottle refused→ Nutramigen
vomiting, diarrhea, irritability→ Alimentum vomiting, diarrhea, irritability→ Elecare infant (permother “Like a New Baby”).
6 months oat cereal introduced,? fussiness solids stopped. 6 ½ months retry oat and sweet potato introduced around the same time→ Day 9 classic FPIES
symptoms (2‐3 hours after ingestion repetitive vomiting, pallor, retching) presumably to oat. 6 ½‐11 months symptoms with multiple other foods. Not classic FPIES symptoms. Symptoms
included diarrhea, mucous in stool, irritability, night waking, single episode vomiting. Foodscausing one or more symptoms mentioned above: apple, pear, carrot, cauliflower, NeocateNutra (contains corn syrup solids and rice starch), white potato, egg and watermelon).
11 months lamb introduction day 3 resulted in FPIES symptoms.
Dietitian Visit One: Age 12 months Foods tolerating: Banana, avocado, Elecare infant (intake of 65 calories per Kg per day) Growth: Weigh: 49th%ile, Length: 71st%ile. Growth history looks good. Recommendations:
o Avoid: milk, soy, oat, rice, lamb, carrot, sweet potato, cauliflowero Foods to trial: Quinoa, flounder or tilapia or sole, white potato, canola oil, blueberry,
peach, plum, prune, broccoli, spinach, pea, corno Recommendations: Continue Elecare infant. Solids 3 times per day. Separate all
feeding by 2‐3 hours. Food before formula at meal time. Try sippy cup, Finger foodideas given.
Dietitian Visit Two: Age 17 months Foods tolerating: Banana, avocado, tilapia, quinoa (flakes and puffs), potato (pieces and
Cheecha puffs), corn (cereal and quinoa corn pasta), Elecare infant 20‐24 fl. Oz. per day Foods questioned: Baked egg Growth and Nutrition: Weight: 41st %ile, Length: 65th%ile. Food processor nutrient analysis of a
typical day meeting greater than 80% DV for vitamins and minerals except vitamin D (290 IU).Adequate protein intake. Calorie intake 85 calories per Kg per day.
83

Recommendations: o Avoid: Milk, soy, oat, rice, lamb, carrot, sweet potato, cauliflower o Foods to trial: Canned coconut milk in cooking and cereal, homemade potato pancakes
(quinoa or corn flour and corn oil), canola oil, chicken, beef or turkey, red or orange fruit or vegetable such as tomato or clementine), ground flaxseed, legumes other than soy, peanut (Bamba or peanut flour as skin test negative)
o Other recommendations: Continue Elecare infant (20‐24 fl. Oz. per day). Introduce one new food every 3‐5 days. 3 meals and 2 snacks per day separated by 2‐3 hours. Solids before formula at meal and snack time. Start 400 IU vitamin D daily.
Dietitian Visit Three: Age 21 months Foods Tolerating: Banana, avocado, tilapia, quinoa (flakes and puffs), potato (pieces and
Cheecha puffs), corn (cereal and quinoa corn pasta), canola oil, grapes, pollock, chicken, garlic, shredded coconut, peanut butter, wheat, cucumber, watermelon, cinnamon, lemon, Elecare infant 18‐20 fl. Oz. per day.
Food Questioned: Baked egg (not tried since visit two), Strawberry day 3 of introduction (few bites) → 2 hours post ingestion vomited 3 times, lethargic and pale.
Growth and Nutrition: Weight 41st%le, Length 70th%ile. Recommendations:
o Avoid: milk (fresh), soy, oat, rice, lamb, carrot, sweet potato, cauliflower, strawberry o Foods to trial: Kidney bean turkey or pork, retry baked egg, baked milk, calcium fortified
coconut milk as a beverage once a day. o Other recommendations: Continue Elecare infant ~20 fl. Oz. per day until age 2 years
(then transition to whole milk or coconut milk depending on tolerance to dairy), continue vitamin D 400 IU per day.
Discussion Points:
1. FPIES: What is it? 2. What are the most common foods that trigger FPIES? 3. Which food group should be introduced first? 4. At what pace should new foods be introduced? 5. Should volume of food on first few days of introduction be limited? 6. What are your favorite FPIES friendly finger foods? 7. How do you advance texture for the infant with FPIES who is only taking a few foods? 8. If a baby with FPIES is breast feeding and refusing all formula what nutrients should you be
concerned about after 6 months of age?
84

CPNP Symposium, Saturday 10/9/15
Case Study Breakout: Nutrition for the Hypometabolic Child
Monica Cicchini, MS, RD, CSP, LD, MedStar Georgetown University Hospital
Case Presentation:
Past medical history significant for: Down Syndrome, severely neurologically impaired due to Hypoxic Ischemic Encephalopathy. He has seizures, hydrocephalus, dysphagia, global developmental delays, and diabnois of cerebral palsy.
Fed Solely through G‐J tube. Currently on Elecare because of history of "vomiting." Vomiting may be secondary to
congestion/respiratory status. No change in vomiting when transitioned from Similac Advance to Elecare at 6 months of age.
Dietitian Visit One: 22 months old Anthropometrics: 10.8 kg (10%ile, wt/age z‐score ‐1.28), 75 cm (0%ile, length/age z‐score ‐3.15),
wt/length 92%ile, z‐score 1.39) Diet: 24 ounces Elecare 20 kcal/oz daily. 45 kcal/kg, 1.3 gm/kg, 67 mL/kg Labs: CBC/CMP Normal Supplement: poly‐vi‐sol Recommendations:
o Decrease to 22 ounces/day Elecare (decrease by 10% total kcal) o Increase water to 100 mL/kg/day
Dietitian Visit Two: 28 months old
Anthropometrics: 11.25 kg (6%ile, wt/age z‐score ‐1.52), 78 cm (0%ile, length/age z‐score ‐3.77), wt/length 91%ile, z‐score 1.33)
Diet: 22 ounces Elecare 20 kcal/oz daily plus 4.5 ounces water. (39 kcal/kg, 1.1y gm/kg, 89 mL/kg)
Labs: CBC/CMP Normal Supplement: poly‐vi‐sol Recommendations:
o Change to Complete Pediatric Reduced Calorie 660 mL/day (35 kcal/kg, 1.76 gm/kg) o Add 400 mL free water o Add Centrum Complete (crushed) o Check Vitamin D levels and replace if low o Add Morton Lite Salt with a goal of 1‐3 mEq/day Na and K o Evaluate meds for any additional kcal
85

Dietitian Visit Two: 36 months old
Anthropometrics: 14 kg (42%ile, wt/age z‐score ‐.2), 81 cm (0%ile, length/age z‐score 4.36), wt/length 100%ile, z‐score 2.84)
Diet: Complete Pediatric Reduced Calorie 660 mL/day plus 400 mL free water (28 kcal/kg, 1.41 gm/kg)
Labs: CBC/CMP Normal Supplement: Centrum Complete Recommendations:
o Decrease to to Complete Pediatric Reduced Calorie 600 mL/day (26 kcal/kg, 1.28 gm/kg) o Add 600 mL free water o Continue Centrum Complete (crushed) o May benefit from calcium supplement o Check Vitamin D levels and replace if low o Continue Morton Lite Salt with a goal of 1‐3 mEq/day Na and K o Evaluate meds for any additional kcal
Discussion Points: 1. What are nutritional areas to consider in an initial visit with a hypometabolic child? 2. What are appropriate minimum calorie and protein goals? If protein is low are their modulars
that you can use? 3. What are some formulas you can use if you are managing a hypometabolic child? Can you use a
blenderized diet? If so, how would it be managed? 4. What are some supplements you can use to meet micronutrient needs? 5. When giving large fluid flushes should distilled (electrolyte free) water be used or can that lead
to hyponatremia and possible seizure activity? 6. What are the pros and cons for using morton lite salt versus pedialyte to achieve
sodium/potassium goals 7. How would your recommendations change if the patient was a po feeder but required thickened
feedings 8. What lab values and testing would you consider besides CBC, CMP and Vitamin D level? 9. What would you manage from 3 years to beyond? What are your growth expectations and
based on which growth chart
86

Nutrition care for children undergoing hematopoietic cell transplantation - now and later Lori J. Bechard, PhD, RD, LDN Case presentation • 17 yo female with CML, presents for HCT from unrelated donor • Well nourished at presentation • High dose cyclophosphamide & TBI for conditioning --> Anorexia, nausea, emesis
Inpatient course
• PN initiated to provide 140% estimated requirements • Minimal oral intake for 3 weeks • Engraftment at 24 days post transplant • Slow resumption of oral intake
Outpatient course
• Discharged from hospital • Oral intake continues to improve with resolution of mucositis • Readmitted 2 weeks later with abdominal pain, diarrhea, anorexia • Colonoscopy and biopsy revealed graft-versus-host disease
Acute GI GVHD
• Treated with prednisone, mycophenylate, cyclosporine • Kept NPO for large amounts of bloody stool • Diet SLOWLY liberalized with decreasing stool output • Poor oral intake persists with accompanying weight loss
Enteral feedings initiated
• G tube placed • Supplemental feedings with polymeric formula • Oral intake somewhat improved • Discharged with overnight G tube feedings
Case update
• Oral intake up and down • Uses G tube for medications, occasional feedings • Weight gain remains problematic • Persistent chronic oral GVHD; at risk for osteoporosis with long term steroids Questions for discussion 1. How should energy needs be assessed in children undergoing HCT? 2. What is the best route for feeding children undergoing HCT? 3. How do complications of HCT impact nutritional status, both short term and long term?
87
Nutrition challenges in a medically and socially complex child with Cystic Fibrosis Tami Miller, RD, CSP, CD
Initial Presentation: 4 yr old male with CF (F508del/621+1G‐‐>T) and pancreatic insufficiency arrived in ER with respiratory distress, worsening cough, poor weight gain and growth. He previously received care out of state and moved to Wisconsin 9 months earlier; interim care was managed by his PMD. Child received G‐tube feedings beginning at age two, but the move resulted in a lapse of supplies, formula and medication refills. The child lived in a chaotic household which resulted in foster placement within a few months of receiving care at our institution.
Growth July, 2013
Height (z‐score) 91.4 cm (‐3.5)Weight (z‐score) 11.5 kg (‐ 4.4)BMI (z‐score) 4% (‐1.8)
Physical assessment: Extremity wasting, thin hair, barrel chest, clubbing, distended abdomen. He appeared 1‐2 years younger than reported age. Lung function (FEV1) was 50% of predicted value.
Nutrition Prescription: Estimated energy needs based on DRI: 1500+ calories (130 Cal/kg); 26+ grams protein (2.2 gm/kg);
Nutrition Intervention: High calorie oral diet; peptide based 1 cal/ml formula: 3 cans over night; 1 can in AM & PM (1200 cals / 38 gm pro = 80% enteral support).
Zenpep 10,000 3/meal & before daytime tube feedings; 2/snack; 3 crushed in overnight tube feeding. CF vitamins + vit. D
Interval History: In the next year of care at CF Center, child had intermittent CF exacerbations with 3 courses of IV antibiotics. FEV1 = 80% predicted. He was in foster care and received consistent respiratory and nutrition therapies. Foster parents note slow eating; refusal to sit at table; poor appetite; distracted at meals. Foster parents want G‐tube removed.
Revised Nutrition Intervention: High calorie diet; peptide based 1.5 cal/ml formula: 3 cans overnight with 5 crushed Zenpep 10,000. Estimated energy needs increased to 1770 Calories/day (105 Cal/kg) to support increased weight, activity, lung function, growth. Enteral nutrition supplied 66% of energy needs.
Cyproheptadine prescribed. Behavioral strategies implemented: Limit meals to 20 minutes, no grazing, positive behaviors rewarded; negative behaviors ignored.
Growth July, 2013 August, 2014
Height (z‐score) 91.4 cm (‐3.5) 104 cm (‐ 2.1)Weight (z‐score) 11.5 kg (‐ 4.4) 16.8 kg (‐1.6)BMI (z‐score) 4% (‐1.8) 55% (0.12)
Recent Updates: FEV1 improved to 85% predicted with one hospitalization in last year. Child attends school which requires “healthy” foods at snack and lunch, and limited time to eat. Poor appetite continues. Weight did not increase in 6 months.
Updated Nutrition Interventions: PM tube feeding was restarted for additional support. Energy needs increased to 1700‐1940 Calories/day (90‐102 Cal/kg). Enteral nutrition now supplies 77‐88% of estimated needs.
Growth July, 2013 August, 2014 June, 2015
Height (z‐score) 91.4 cm (‐3.5) 104 cm (‐ 2.1) 111 cm (‐1.8) Weight (z‐score) 11.5 kg (‐ 4.4) 16.8 kg (‐1.6) 19 kg (‐1.3) BMI (z‐score) 4% (‐1.8) 55% (0.12) 50% (0)
Discussion: What are some approaches to pancreatic enzyme therapy with tube feeding support?
What approaches can be considered to work towards “normal” eating schedule by increasing the number of meals while balancing enteral feedings to meet the need for adequate nutrition?
How much recovery of growth could be expected over time?
88
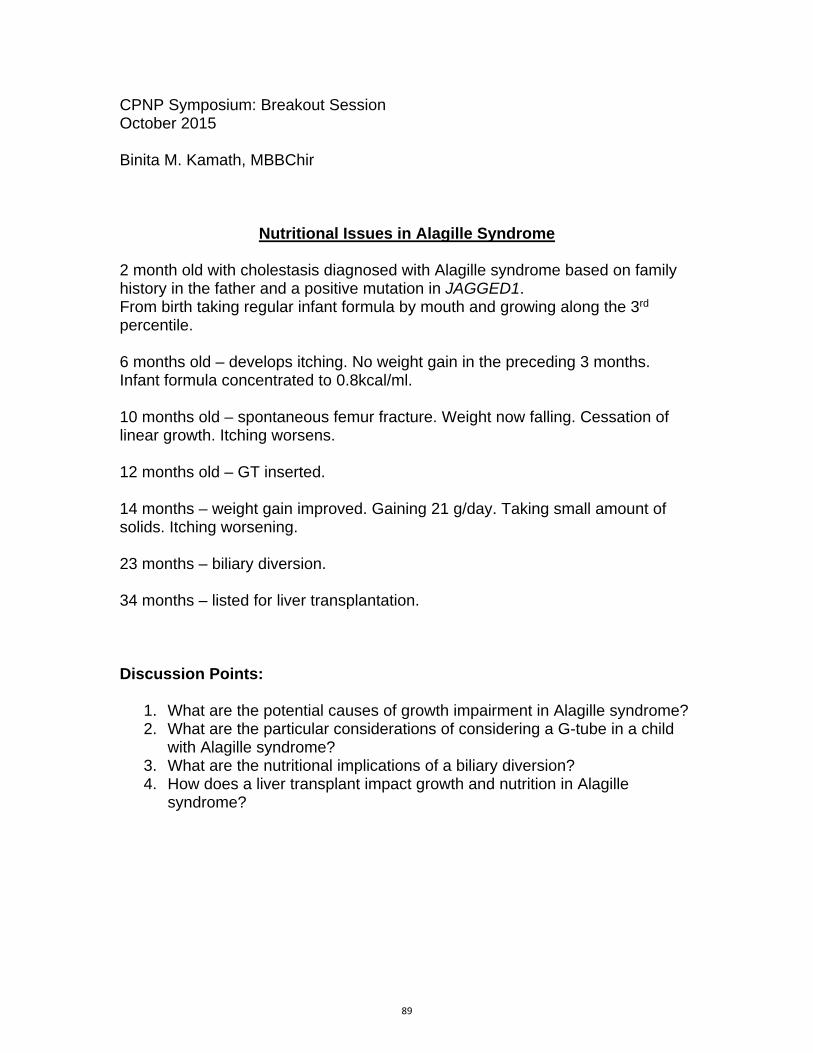
CPNP Symposium: Breakout Session October 2015 Binita M. Kamath, MBBChir
Nutritional Issues in Alagille Syndrome
2 month old with cholestasis diagnosed with Alagille syndrome based on family history in the father and a positive mutation in JAGGED1. From birth taking regular infant formula by mouth and growing along the 3rd percentile. 6 months old – develops itching. No weight gain in the preceding 3 months. Infant formula concentrated to 0.8kcal/ml. 10 months old – spontaneous femur fracture. Weight now falling. Cessation of linear growth. Itching worsens. 12 months old – GT inserted. 14 months – weight gain improved. Gaining 21 g/day. Taking small amount of solids. Itching worsening. 23 months – biliary diversion. 34 months – listed for liver transplantation. Discussion Points:
1. What are the potential causes of growth impairment in Alagille syndrome? 2. What are the particular considerations of considering a G-tube in a child
with Alagille syndrome? 3. What are the nutritional implications of a biliary diversion? 4. How does a liver transplant impact growth and nutrition in Alagille
syndrome?
89

Andy is a 15 year old young man with Crohn’s disease January 27, 2012 (age 11 y 4 months) presented to GI in 2012 at the age of 11 years with h/o oral inflammation initially thought to be secondary to an orthodontic appliance RX: antibiotics as well as 2 courses of prednisolone, improving with therapy, but would return. No fevers, abdominal complaints, joint pains, rashes, redness of the eyes, blood in the stool or vomiting. Appetite: excellent Energy Level: Good, but not playing sports Physical Findings: Bowel movement 1 formed daily Multiple anal skin tags. April 03, 2012 (11 years 7 months) Endoscopy was reported as normal, but oral biopsies showed evidence of "squamous mucosa with reactive epithelial changes . The findings are reflective of a chronic inflammatory process. There was a single non necrotizing granuloma in the colon Some worsening of a mouth sore over the last several days; Medications: Ferrous sulfate 45 mg by mouth daily. Vitamin D supplement 50,000 IU 30 days Started: Flagyl (antibiotic) possible side effects metallic taste and risk of neurological symptoms for long term use Mesalamine (Asacol) (5 ASA) risk of reversible low sperm count, nausea and vomiting June 05, 2012 1 (11 years 9 months) Symptoms: resolution of oral ulcers and some improvement in anal tags No abdominal pain, nocturnal stools, fever, joint pain, rashes, redness of the eyes Appetite: Improved Energy level Improved Bowel Movements 3 -4 without blood or mucus Noted high Liver function tests MEDICATIONS:
Flagyl ( metronidazole) 250 mg p.o. t.i.d. Antibiotic Long-term use often limited by nerve damage, dose reduction may decrease risk
Asacol 1200 mg p.o. b.i.d. 5 ASA 3-7% have increase in colitis Iron sulfate 45 mg extended release once daily.
Supplement
. July 17, 2012 11 years 10 months Family consulted a homeopathic practitioner who recommended started supplements instead of standard therapy. Family elected to keep therapy and start supplements Added
Moducare 1 tablet PO BID Plant sterol Liver fraction iron supplement2 tablets pol daily 1300 mg
Acetyl glutathione 200 mg po daily Lyop-spheric Vitamin C 1 packet daily Fish oil 1 teaspoon daily Lauricidin or monolauric acid (from coconut oil) 1.5 grams Po BID
Symptoms: No abdominal pain, no new mouth sores. Bowel Movement 1-2 /day without blood or mucus Appetite: somewhat poor Energy: good
90

Stopped the Flagyl at this visit September 18, 2012 12 years Family expressed desire to avoid all medications if possible , very concerned about the elevated Liver enzymes Symptoms: Denies, however mother does most of the talking. Bowel Movements 1/day No nausea, abdominal pain Energy level: good Appetite: good Medications: None. MD discussed concern of no medical management in light of increase in inflammatory markers Started Pentasa
February 19, 2013 12 years 5 months Appetite: good Energy level: good Bowel Movement 1/day Anemia worsened Increased Fe to 2 daily May 21, 2013 15:30 12 years 8 months Bowel movements one formed stool per day without blood or mucus. Appetite/Diet struggle with eating red meat and green leafy vegetables concerned about Iron intake August 20, 2013 No change , except significant concern with swallowing multiple capsules. Referred to psychology June 16, 2015 14 years 9 months Symptoms Abdominal pain as often as 5-6 times per week. His pain is often in the periumbilical region. The pain lasts typically 5-6 minutes and is described as a constant pain. Bowel movements: Increased, but no blood or mucus on stools No fevers, joint pains, rashes, mouth sores or inflammation of the oral or perianal area. Meds unchanged MD recommended nutritional supplements due to suboptimal weight gain July 07, 2015 (1st RD visit) REASON FOR VISIT : Inflammatory Bowel Disease, induction therapy with Enteral nutrition Mother asking about use of several supplements including Kids DHA, Rainbow Light D3 200 IU/day, Smarty Pants Multivitamin, Intesti Flor Probiotic and Digestive Aide, in addition to taking Vitamin C 125 mg and Iron 65 mg daily. He has tried Ensure in the past, reporting that it was not well tolerated, both in flavor and resulting in stomach ache. He reports bloating and urgency to move his bowels. 24 hour recall Bagel with cream cheese and 1 cup milk Sandwich with mozzarella cheese, tomato and basil Oatmeal Raisin Cookies Meat loaf with soup, yogurt and corn Grilled cheese Sandwich with sweet biscuits. Growth Chart (Based on CDC growth charts)
14yr 10m (178.0 Months), male
Pentasa 1500 mg po q am and 2000 mg nightly
5-ASA Headaches, diarrhea and abdominal pain Difficulty swallowing tabs (requires 7 daily)
3-7% worsening of colitis
Vitron-C 65 mg elemental 1 per day daily
Lactobacillus GG 1 capsure
91
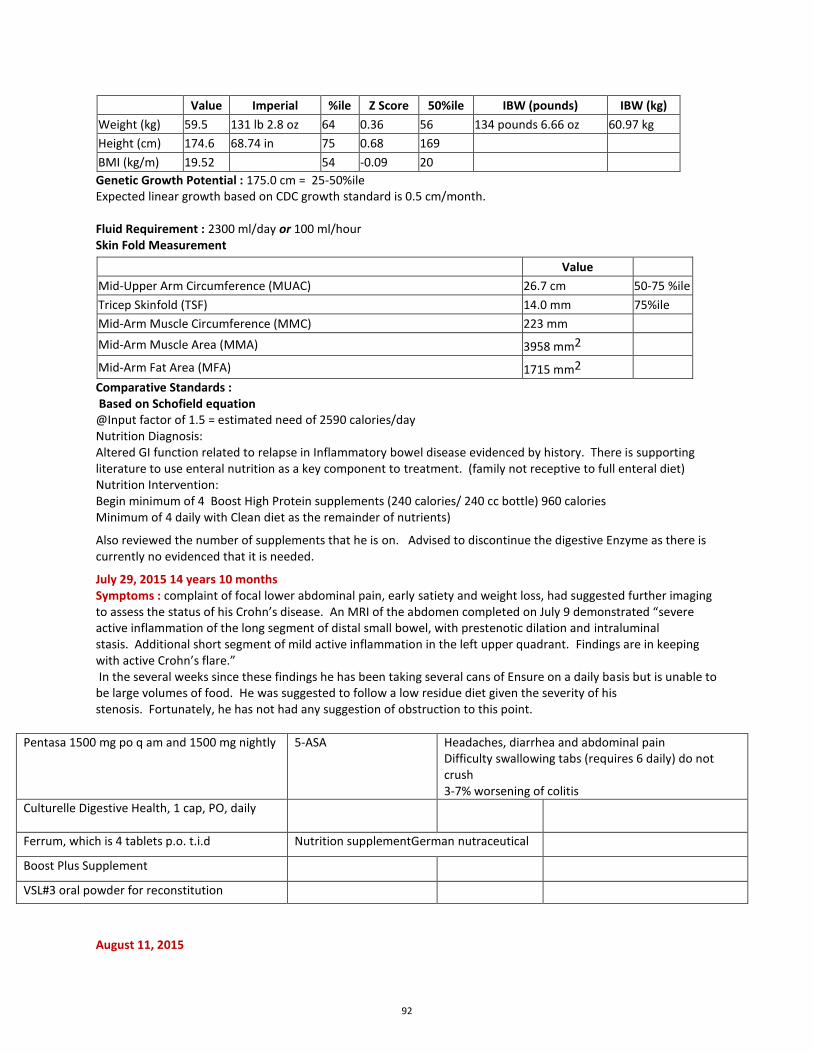
Value Imperial %ile Z Score 50%ile IBW (pounds) IBW (kg)
Weight (kg) 59.5 131 lb 2.8 oz 64 0.36 56 134 pounds 6.66 oz 60.97 kg Height (cm) 174.6 68.74 in 75 0.68 169 BMI (kg/m) 19.52 54 -0.09 20 Genetic Growth Potential : 175.0 cm = 25-50%ile Expected linear growth based on CDC growth standard is 0.5 cm/month. Fluid Requirement : 2300 ml/day or 100 ml/hour Skin Fold Measurement
Value
Mid-Upper Arm Circumference (MUAC) 26.7 cm 50-75 %ile Tricep Skinfold (TSF) 14.0 mm 75%ile Mid-Arm Muscle Circumference (MMC) 223 mm
Mid-Arm Muscle Area (MMA) 3958 mm2
Mid-Arm Fat Area (MFA) 1715 mm2
Comparative Standards : Based on Schofield equation @Input factor of 1.5 = estimated need of 2590 calories/day Nutrition Diagnosis: Altered GI function related to relapse in Inflammatory bowel disease evidenced by history. There is supporting literature to use enteral nutrition as a key component to treatment. (family not receptive to full enteral diet) Nutrition Intervention: Begin minimum of 4 Boost High Protein supplements (240 calories/ 240 cc bottle) 960 calories Minimum of 4 daily with Clean diet as the remainder of nutrients)
Also reviewed the number of supplements that he is on. Advised to discontinue the digestive Enzyme as there is currently no evidenced that it is needed.
July 29, 2015 14 years 10 months Symptoms : complaint of focal lower abdominal pain, early satiety and weight loss, had suggested further imaging to assess the status of his Crohn’s disease. An MRI of the abdomen completed on July 9 demonstrated “severe active inflammation of the long segment of distal small bowel, with prestenotic dilation and intraluminal stasis. Additional short segment of mild active inflammation in the left upper quadrant. Findings are in keeping with active Crohn’s flare.” In the several weeks since these findings he has been taking several cans of Ensure on a daily basis but is unable to be large volumes of food. He was suggested to follow a low residue diet given the severity of his stenosis. Fortunately, he has not had any suggestion of obstruction to this point.
Pentasa 1500 mg po q am and 1500 mg nightly
5-ASA Headaches, diarrhea and abdominal pain Difficulty swallowing tabs (requires 6 daily) do not crush 3-7% worsening of colitis
Culturelle Digestive Health, 1 cap, PO, daily
Ferrum, which is 4 tablets p.o. t.i.d Nutrition supplementGerman nutraceutical
Boost Plus Supplement
VSL#3 oral powder for reconstitution
August 11, 2015
92

Has been taking Boost plus , adopting many gluten free grains (decreasing but not eliminating gluten) with focus on Clean diet. 24 hour recall 11 am 1 boost plus and Udi’s GF bagel with egg, cheese and ham 3 pm 1 Boost Plus 7 pm GF macaroni with two large meatballs made with GF breadcrumbs 8 pm 2 gf cookies and 1 boost Plus 10 pm 2 cookies (that contained wheat) By history this is approximately 2000 calories/day Growth Chart
14yr 11m (179.0 Months), male, (CDC growth chart) Value Imperial %ile Z Score 50%ile IBW (pounds) IBW (kg)
Weight (kg) 59.7 131.0 lb 9.86 oz 63 0.34 56.0 135 lb 12.89 oz 61.6 kg Height (cm) 175.5 69.09 in 77 0.75 170.0
BMI (kg/m2) 19.38 44 -0.16 20.0 Fluid Requirement : 2294.0 ml/day or 100.0 ml/hour Comparative Standards : Based on Schofield equation @Input factor of 1.5 = estimated need of 2590 calories/day Nutrition Diagnosis:
Altered GI function related to Crohn’s disease evidenced by MRI. There are strictures that may require surgery. The only known nutrition based therapy to decrease inflammation is 100% enteral nutrition.
Nutrition Intervention: Discussed what is known about use of nutrition as a primary treatment for Crohn’s disease.
Encouraged the use of 5 to 6 Boost plus (or provide samples of Ensure plus , Pedisure Peptide or Peptamen (all 1.5 calories/cc) for the next 6 to 8 weeks as a primary therapy for Crohn’s .
AM agreed to this therapy in hopes of avoiding surgery. It was made clear that this therapy will be part of a medical plan that should maximize the changes of avoiding surgery, but will not guarantee.
August 31, 2015 15 years REASON FOR VISIT : Crohns disease, Using Enteral nutrition to assist with induction therapy. Currently taking Boost Plus (360 calories/8 fl. ounces bottle) seven daily ( 2500 calories) plus 1 tablespoon of applesauce with VSL #3 and 1 cup of clear juice daily. He reports that he feels well. His mother believes that his "color" has improved. They are not eating in front of him. They report that although it has been hard, they find that they are finding other activities to do as a family. His energy level is good, although he needed to rest a bit more than his 18 year old brother while on vacation. Mother was unsure of whether this was due to the heat and sun that he did not tolerate. His bowel movement are reported as normal, soft, without any abdominal pain. Mother questions whether to encourage him to go out for cross country while on the enteral formula He reports that the current amount of formula his keeping him satisfied, he would not like to drink more. He is currently drinking 8 fl. ounces every 2 to 3 hours of the waking day. They are concerned about whether he will need permission to do this at school.
8/15 Humira
Biologic Anti-TNF
Injection site reactions
Increased risk of TB including immune suppression, the rare risk of hepatosplenic T-cell lymphoma, infection, hepatitis, psoriasis, infusion reactions in the more likely risk of possible response due to antibody formation.
93

Interval between visits : 20 days Actual weight gain annualized : 20.0 grams/day or 7.3 kg/year Expected Weight Gain (based on CDC) : 5.3 kg/year Actual linear growth annualized : 0.0 cm/month or 0.0 cm/year. Expected Linear Growth (based on CDC) : 6 cm/year. Growth Chart 15yr (180.0 Months), male, (CDC growth chart) Value Imperial %ile Z Score 50%ile IBW (pounds) IBW (kg) Weight (kg) 60.1 132.0 lb 8 oz 63 0.33 56.0 135 lb 12.89 oz 61.6 kg Height (cm) 175.5 69.09 in 76 0.7 170.0 BMI (kg/m2) 19.51 45 -0.13 20.0 Fluid Requirement : 2302.0 ml/day or 100.0 ml/hour Comparative Standards : Based on Schofield equation @Input factor of 1.5 = estimated need of 2599 calories/day Nutrition Diagnosis Altered GI function related to Crohns evidenced by history. He is doing well on the enteral formula, gaining weight well. Nutrition Intervention Continue enteral formula (exclusive) for the next 4 weeks, then we will discuss transition back to "clean diet" September 01, 2015 MD note: Improving on enteral nutrition and Humira. Re-evaluate for surgery after 3 months Medications
Boost Nutritional Supplement (8 oz bottle), 6 refills Humira 40 mg/0.8 mL subcutaneous kit, 40 mg, Subcutaneous, Q14day, 11 refills Pentasa 500 mg oral capsule, extended release, 5 refills VSL#3 oral powder for reconstitution
94
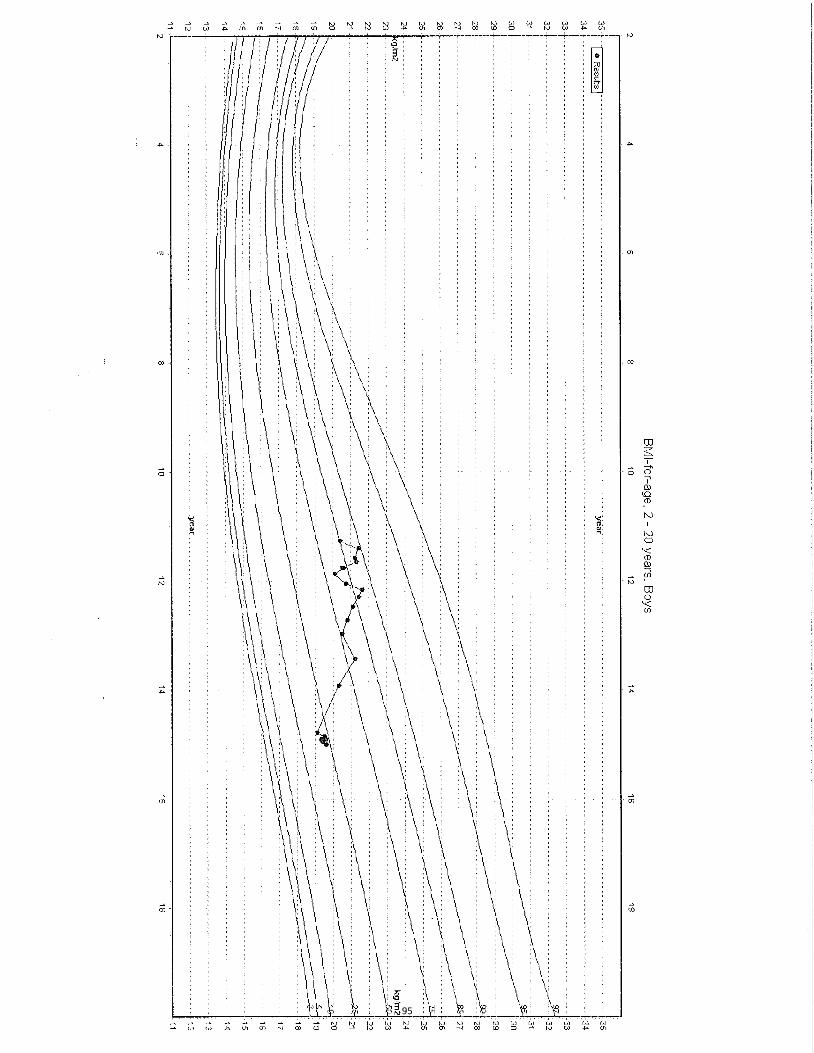
95
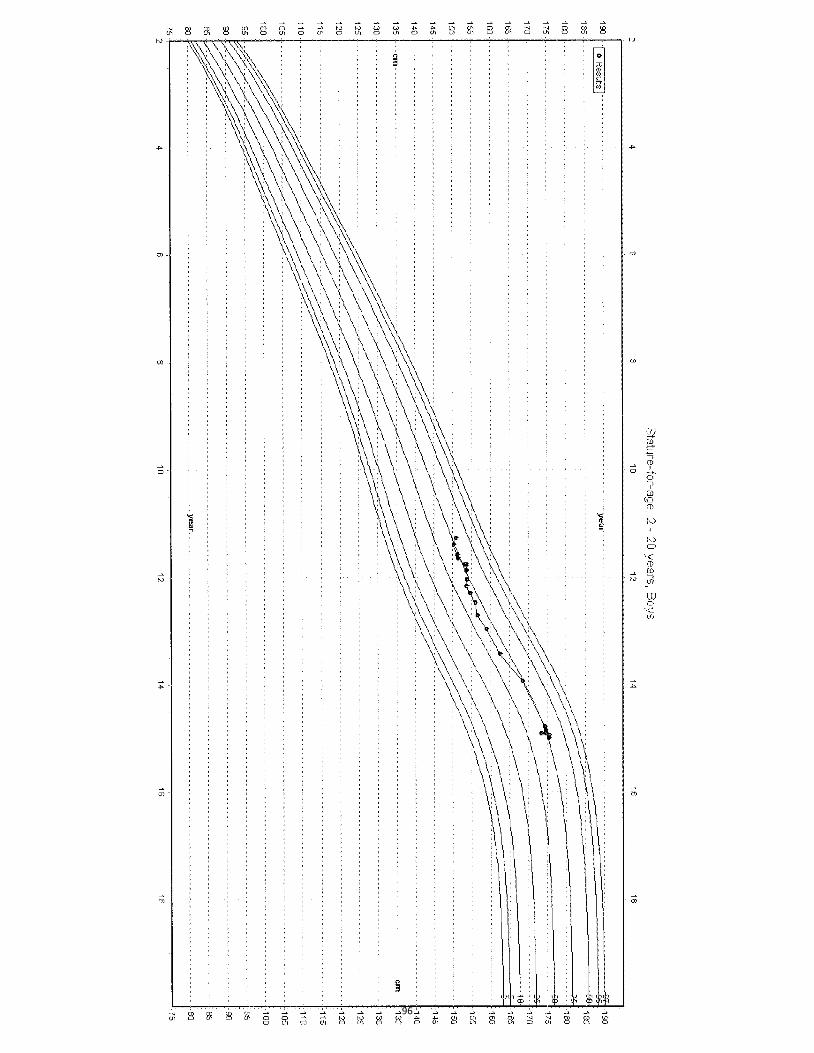
96

97

98

99

100

BLENDERIZED TUBE FEEDINGS: MANAGING A NEW FRONTIER
Julia Driggers RD, LDN, CNSC
Mimi Girten, RD, CSP, LDN
Children's Hospital of Philadelphia, Department of Gastroenterology and Nutrition
Disclosures
• Nothing to Disclose
Introduction
• Summarize history of enteral nutrition
• Understand reasons for using blenderizedtube feedings (BTF) instead of commercialformula
• Identify & compare components of differentblend types
• Recognize traits of patients who might besuited for BTF
101

Introduction
• Understand challenges for the dietitian.
• Recognize how BTF works for the family.
• Identify bumps in the road when using a BTF.
• Recognize challenges moving forward
So, what’s Blenderized Tube feeding?
Designed By: Amy Dean
In the Beginning…
Designed By: Amy Dean
102

…
And back again…
……
Designed By: Amy Dean
“Typical Diet” + Blender = Done?
What’s in a Blend?
Designed By: Amy Dean
103

Who’s a Good Fit?
How‐To’s of Preparation & Administration of Blenderized
Tube FeedingsPediatric Population
104

Types of BlendThick vs. Thin
Administration
Creating a Recipe
Equipment Preparation
Food Safety
Thick Formulas
Administration – Thick Blends
Use: Treatment of
Gagging
Refluxing
Nissen Fundoplications
Volume Intolerance
105

Administration – Thick Blends
Description:
Thick/Pasty Liquid
High Caloric Density (> 30 kcal/oz)
Minimal Free Water
Administration – Thick Blends
– Require a G-Tube (14-16 French)
– Administered via Plunger Syringe only
– Start 1 oz ‘Bolus’ pushed in slowly over 10 min.
– Increase ‘Bolus’ to 2- 4 oz goal
– Water flush (5-10 ml) proceeds
TIME SAVER: Olive Oil or Oil Spray (PAM) can be used to lubricate the syringe and end of plunger for easier administration
Administration – Thick Blends
106

Recipe 1: w/ Commercial Formula
Recipe 2: w/o Commercial Formula
8 oz Pediatric Formula 1.54 oz Strained sweet potato4 oz Strained peaches 6 oz Plain yogurt2 Tablespoon oil6 Tablespoons sugar or cornstarch ½ Cup dry infant cereal
Estimated Caloric Content:
1100‐ 1200 kcal32% Fat, 55% CHO, 13% Pro65% Free Water
8 oz Whole milk2.5 oz Strained chicken 4 oz Strained pears 4 oz Strained squash 6 oz Greek yogurt1 Tablespoon oil4 Tablespoons sugar or cornstarch ½ Cup dry infant cereal Estimated Caloric Content:
900‐1000 kcal30% Fat, 55% CHO, 15% Pro64% Free Water
Creating a Recipe – Thick Blends 1) Choose a Protein Source • Liquid Protein (Milk/Formula)• 4 – 8 oz Needed Only • Thicker Protein (Meat/Yogurt)• 80-90 % Protein Needs from above
Sources. Additional from Cereals
2) Choose a Carbohydrate Source• Use Stage II Fruits/Vegetables• Choose High Vit. A & Vit. C• Less than 8 – 12 oz (2-3 jars)
3) Thickening Agents/ CHO Source• Grains to add kcals/fiber/thicken• Need up to 8 TBSP Infant Cereal• Adding White Granulated Sugar or
Cornstrach
4) Choose a Fat Source • Omega 3, Omega 6 Blend• 1-2 TBSP
12‐15% Protein, 30‐35% Fat, 55‐60 % CHO
Thin Liquids
Administration – Thin Blends
Use:
Natural / Holistic Option
Formula Intolerance (**Volume Tolerant)
Oral Aversions / Delayed Oro-motor skill
Description:
Medium/Thin Liquid
Moderate Free Water
20-30 kcal/oz Formula
107

Administration – Thin Blends– Require a G-Tube (14-16 French)
– Administered via Infinity® PumpAddendum to Directions for Use: “…DO NOT USE HOMEMADE BLENDERIZED OR LIQUIDIZED FOODS, OR OTHER NON-COMMERCIALLY AVAILABLE FEEDING SOLUTIONS…”
– Thin formula required to flow through pump
– Pump feeds to run < 2 hrs. for food safety
– Possibly keep on ice (< 40 F) if hang time longer than 2 hrs. Use of Chill Bags
Note: Fat can degrade pump tubing
Administration – Thin Blends
– Administered via Plunger Syringe• 60-90 ml syringe with plunger
• Push slowly
• Allows for varying degrees of thickness
– Administered via Gravity Syringe• Syringe without plunger
• Elevated to gravity to flow through
• Formula required to be very thin
Creating a Recipe– Thin Blends
• Marsha Dunn Klein, MEd, OTR/L and
• Suzanne Evans Morris, PhD, CCC‐SLP
• Copyright © 2007 by Mealtime Notions, LLC
• Charts may be reproduced for instructional use and educational purposes. They should not replace the advice of a physician
108

Protein
2 slices Wheat Bread 140 7½ cup Infant Cereal, cooked 80 4½ cup Brown Rice, cooked 100 2.5 6 oz Carrots, BF Stage I 90 06 oz Green Beans, BF Stage III 90 3
4 oz Apple Sauce, pureed 80 02 oz Peaches, pureed 40 0 2 oz Prunes, BF Stage I 50 0
2 cups Soy Milk, original 220 16
1 Egg with Yolk, cooked 70 62.5 oz Chicken, BF Stage I 70 0
2 tsp Flaxseed Oil 80 02 tsp Canola Oil 80 0
1190 38.5
1 tsp 100 % Maple Syrup 20 0
1210 38.5
Cows Milk 8 gm Pro/cupHemp Milk 4‐5 gm Pro/cupCoconut Milk, canned 5 gm Pro/cup
Mono‐ Olive Oil, Canola, Avocado, NutsOmega 3‐ Flax, Canola, Walnut, Hemp, Fish
Molasses, Agave, Table Sugar, Corn Starch, Hemp Protein, Avocado
12‐15% Protein, 30‐35% Fat, 55‐60 % CHO
Getting Started with Blenderized Feeds
• Thick Blend
• Thin Blend
Choose Appropriate Type Blend
• Calorie, Protein, Fluid needs
• 15‐20 % more Calories than formula Calculate Needs
• Start “Single Ingredient” Bolus (1‐2 oz) 1‐4 X day
• Continue Formula ≥ 50% calorie need (Overnight or Bolus)
50 % Calorie Needs from Formula
• Add 1 New Ingredient per Blend
• Note GI Reaction (Vomiting, Diarrhea, etc.)Increase Blenderized Food and Variety
109

Monitoring Tolerance of Blended Foods
Pediasure 1.5 Puree ChickenCarrotsPeas Pears
Prunes Soft, light brown
Child with looser BM without straining
X X X
√
Equipment
Designed by Mimi Girten
Equipment
Designed by Mimi Girten
110
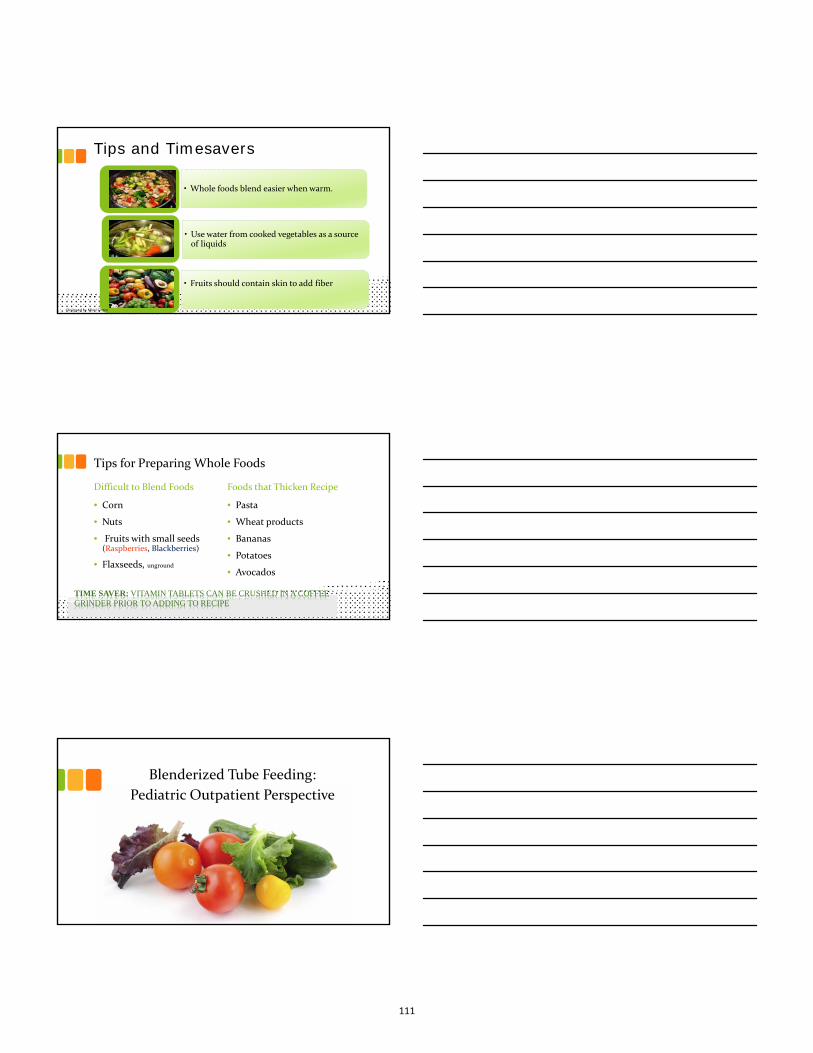
Tips and Timesavers
• Whole foods blend easier when warm.
• Use water from cooked vegetables as a source of liquids
• Fruits should contain skin to add fiber
Designed by Mimi Girten
Tips for Preparing Whole Foods
Difficult to Blend Foods
• Corn
• Nuts
• Fruits with small seeds (Raspberries, Blackberries)
• Flaxseeds, unground
Foods that Thicken Recipe
• Pasta
• Wheat products
• Bananas
• Potatoes
• Avocados
TIME SAVER: VITAMIN TABLETS CAN BE CRUSHED IN A COFFEE GRINDER PRIOR TO ADDING TO RECIPE
Blenderized Tube Feeding:
Pediatric Outpatient Perspective
111

How it works…for the Dietitian
• Nutrition assessment
– Medical history
– Nutritional history
– Lab data
– Growth parameters
– Estimated needs
– Medications
– Bowel habits
– Allergies
Develop Parental Goals
Feed real food
Feel part of the family
Less reflux and constipation
Sit at the table
Improve heath
Improved tolerance (less gagging, retching, vomiting)
Develop Nutritional Goals• Nutritional
• Adequacy • Tolerance• Growth
• Stable lab data• Less reflux and constipation• Improved volume tolerance• Reduction of gagging, retching and vomiting• Communication
112
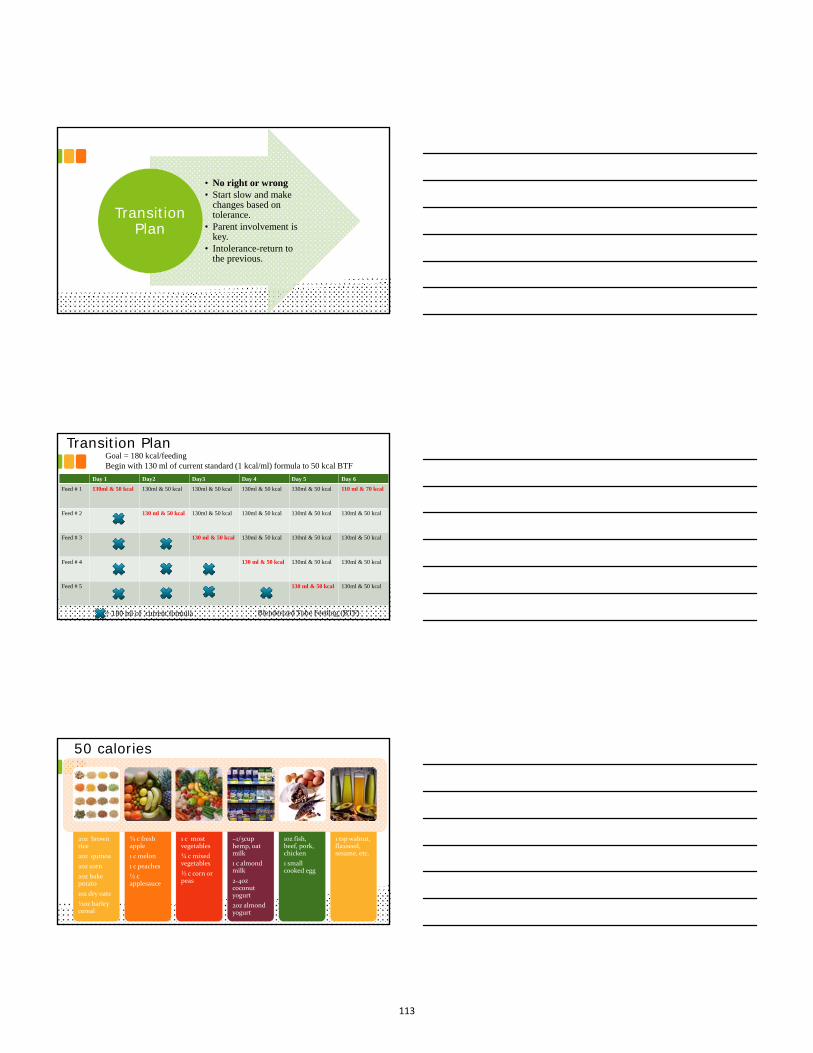
• No right or wrong• Start slow and make
changes based on tolerance.
• Parent involvement is key.
• Intolerance-return to the previous.
Transition Plan
Transition Plan
Day 1 Day2 Day3 Day 4 Day 5 Day 6
Feed # 1 130ml & 50 kcal 130ml & 50 kcal 130ml & 50 kcal 130ml & 50 kcal 130ml & 50 kcal 110 ml & 70 kcal
Feed # 2 130 ml & 50 kcal 130ml & 50 kcal 130ml & 50 kcal 130ml & 50 kcal 130ml & 50 kcal
Feed # 3 130 ml & 50 kcal 130ml & 50 kcal 130ml & 50 kcal 130ml & 50 kcal
Feed # 4 130 ml & 50 kcal 130ml & 50 kcal 130ml & 50 kcal
Feed # 5 130 ml & 50 kcal 130ml & 50 kcal
= 180 ml of current formula
Goal = 180 kcal/feedingBegin with 130 ml of current standard (1 kcal/ml) formula to 50 kcal BTF
Blenderized Tube Feeding (BTF)
50 calories
2oz brown rice
2oz quinoa
2oz corn
2oz bake potato
1oz dry oats
½oz barley cereal
¾ c fresh apple
1 c melon
1 c peaches
½ c applesauce
1 c most vegetables
¾ c mixed vegetables
½ c corn or peas
~1/3cup hemp, oat milk
1 c almond milk
2‐4oz coconut yogurt
2oz almond yogurt
1oz fish, beef, pork, chicken
1 small cooked egg
1 tsp walnut, flaxseed, sesame, etc.
113

Transition Plan1 BTF, 4
CP
2 BTF, 3 CP
3 BTF, 2 CP
4 BTF, 1 CP
ALL BTF
Blenderized Tube Feeding (BTF)Commercial Product (CP)
Food Allergies
114

Food Allergies
Hypoallergenic formula
Begin transition as you would if child was eating orally.
Follow American Academy of
Pediatrics (AAP) and American Academy of Asthma, Allergy and Immunology
(AAAAI)
Introduce 1 food at a time waiting 3-5 days to start a new food.
Be sure to continuously check
for nutritional adequacy.
Fleischer DM, Spergel JM, Assa’ad AH, Pongracic JA. J Allergy Clin Immunol: In Practice 2013;1:29‐36
BTF and Food Allergies
Fortified Soy milk: complete
Fortified Rice milk: (low protein)
Fortified Hemp, Oat, Almond (variable protein)
Soy, Almond, Coconut Yogurt
Meat
Dairy
Egg
Other legumes
AmaranthArrowrootBarleyBuckwheatCornOat
PotatoQuinoaRiceRyeTapioca
Recipe Analysis & Adjustments
115

Be Organized
Safe Food Practices
Right Equipment
KEYS TO SUCCESSFUL PREPARATION
Food Safety
Partnership for Food Safety Education 2010
CLEAN: Wash hands and surfaces often
SEPARATE: Don't cross-contaminate!
COOK: Cook to proper temperature
CHILL: Refrigerate promptly
Communication and Follow Up is Essential
Parent
RD
Medical Team
116

Assessment
Develop
Goals
Plan
&
Transition
Poor growthConstipationVolume limitedRetching
GrowthImprove constipationAll BTF
TeachingWeekly Updates: phone & emailMonthly Visits: Weight and re-assess
Initial Visit
Updates: 1 month follow up• Tolerated addition of
blended food
• Transitioned all feeds
• 1.5 lb. weight gain over the month
Visit:• Re-assess nutritional
goals based on progress
• Reviewed excessivesupplementation
• Started on hypoallergenic MVI
• Re-educated on food allergies
Plan:• Increase by 100 kcal
every 2-3 days.
• Goal: 1800 kcal/day
• Every 6 week follow up till at goal kcal and catch up
• Recipe analysis & adjustment at each visit
Follow Up Visit
How it works…for the family
• Medical team
• Insurance reimbursements
• Supplies
• Ingredient trials / transition
• Recipe development
• Prepare the blend
• Time/Storage/Food Safety
• Administration of feeds
• Monitor & communicate
117
Bumps in the road…
Inpatient admissions
Insurance issues Emergencies Tube clogging/degradation
Reactions/Intolerance Nutrient shortfalls Poor weight gain +/- growth
Vacation and Travel
Resources
Supply List
Support Groups
Books & Websites
Blogs
Journals
Food Safety
Nutrient Analysis
118

Strategies for Success
BF ARE NOT a one
size fits ALL
Every child and family is different
Take it one step at a
time
Start with the basics
Develop your own
resources & strategies
Develop your own ideas &
technique
119

THANK YOU
120
Related Documents











