© 2017 Haneke. This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms. php and incorporate the Creative Commons Attribution – Non Commercial (unported, v3.0) License (http://creativecommons.org/licenses/by-nc/3.0/). By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms (https://www.dovepress.com/terms.php). Psoriasis: Targets and Therapy 2017:7 51–63 Psoriasis: Targets and erapy Dovepress submit your manuscript | www.dovepress.com Dovepress 51 REVIEW open access to scientific and medical research Open Access Full Text Article http://dx.doi.org/10.2147/PTT.S126281 Nail psoriasis: clinical features, pathogenesis, differential diagnoses, and management Eckart Haneke 1–4 1 Department of Dermatology, Inselspital, University of Bern, Bern, Switzerland; 2 Dermatology Practice Dermaticum, Freiburg, Germany; 3 Centro de Dermatología Epidermis, Instituto CUF, Porto, Portugal; 4 Department of Dermatology, University Hospital, Gent, Belgium Abstract: Psoriasis is the skin disease that most frequently affects the nails. Depending on the very nail structure involved, different clinical nail alterations can be observed. Irritation of the apical matrix results in psoriatic pits, mid-matrix involvement may cause leukonychia, whole matrix affection may lead to red lunulae or severe nail dystrophy, nail bed involvement may cause salmon spots, subungual hyperkeratosis, and splinter hemorrhages, and psoriasis of the distal nail bed and hyponychium causes onycholysis whereas that of the proximal nail fold causes psoriatic paronychia. The more extensive the involvement, the more severe is the nail destruction. Pustular psoriasis may be seen as yellow spots under the nail or, in case of acroder- matitis continua suppurativa, as an insidious progressive loss of the nail organ. Nail psoriasis has a severe impact on quality of life and may interfere with professional and other activities. Management includes patient counseling, avoidance of stress and strain to the nail apparatus, and different types of treatment. Topical therapy may be tried but is rarely sufficiently efficient. Perilesional injections with corticosteroids and methotrexate are often beneficial but may be painful and cannot be applied to many nails. All systemic treatments clearing widespread skin lesions usually also clear the nail lesions. Recently, biologicals were introduced into nail psoriasis treatment and found to be very effective. However, their use is restricted to severe cases due to high cost and potential systemic adverse effects. Keywords: nail psoriasis, etiology, pathology, quality of life, impact, treatment Introduction Psoriasis is a chronic inflammatory disease with a strong genetic background but highly influenced by environmental factors. Its prevalence is ~1–2% of the world population with considerable differences among regions and individuals with different skin types. It is the skin disease that most frequently affects the nail. At the time of consultation, roughly one half of the patients suffer from nail changes. Over lifetime, up to 90% of all psoriatics will have had nail alterations. The prevalence of nail psoriasis is even higher in psoriatic arthritis. 1 Nail lesions often appear around 10 years later than skin lesions, which may in part be the reason for nail psoriasis being observed less frequently in children. In general, cutaneous psoriasis is more severe in individuals with nail involvement. Etiology and pathogenesis Neither gender nor race predilection appears to exist. There is no association of HLA- C0602 with nail and joint involvement, but nail psoriasis is often associated with an inflammation at the insertion points of tendons and ligaments giving rise to enthesitis. Correspondence: Eckart Haneke Schlippehof 5, 79110 Freiburg, Germany Tel +49 761 897 8368 Fax +49 761 383 7401 Email [email protected] Psoriasis: Targets and Therapy downloaded from https://www.dovepress.com/ by 161.62.252.40 on 26-Jan-2018 For personal use only. 1 / 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

© 2017 Haneke. This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms. php and incorporate the Creative Commons Attribution – Non Commercial (unported, v3.0) License (http://creativecommons.org/licenses/by-nc/3.0/). By accessing the work
you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms (https://www.dovepress.com/terms.php).
Psoriasis: Targets and Therapy 2017:7 51–63
Psoriasis: Targets and Therapy Dovepress
submit your manuscript | www.dovepress.com
Dovepress 51
R E V I E W
open access to scientific and medical research
Open Access Full Text Article
http://dx.doi.org/10.2147/PTT.S126281
Nail psoriasis: clinical features, pathogenesis, differential diagnoses, and management
Eckart Haneke1–4
1Department of Dermatology, Inselspital, University of Bern, Bern, Switzerland; 2Dermatology Practice Dermaticum, Freiburg, Germany; 3Centro de Dermatología Epidermis, Instituto CUF, Porto, Portugal; 4Department of Dermatology, University Hospital, Gent, Belgium
Abstract: Psoriasis is the skin disease that most frequently affects the nails. Depending on
the very nail structure involved, different clinical nail alterations can be observed. Irritation
of the apical matrix results in psoriatic pits, mid-matrix involvement may cause leukonychia,
whole matrix affection may lead to red lunulae or severe nail dystrophy, nail bed involvement
may cause salmon spots, subungual hyperkeratosis, and splinter hemorrhages, and psoriasis of
the distal nail bed and hyponychium causes onycholysis whereas that of the proximal nail fold
causes psoriatic paronychia. The more extensive the involvement, the more severe is the nail
destruction. Pustular psoriasis may be seen as yellow spots under the nail or, in case of acroder-
matitis continua suppurativa, as an insidious progressive loss of the nail organ. Nail psoriasis
has a severe impact on quality of life and may interfere with professional and other activities.
Management includes patient counseling, avoidance of stress and strain to the nail apparatus,
and different types of treatment. Topical therapy may be tried but is rarely sufficiently efficient.
Perilesional injections with corticosteroids and methotrexate are often beneficial but may be
painful and cannot be applied to many nails. All systemic treatments clearing widespread skin
lesions usually also clear the nail lesions. Recently, biologicals were introduced into nail psoriasis
treatment and found to be very effective. However, their use is restricted to severe cases due to
high cost and potential systemic adverse effects.
Keywords: nail psoriasis, etiology, pathology, quality of life, impact, treatment
IntroductionPsoriasis is a chronic inflammatory disease with a strong genetic background but highly
influenced by environmental factors. Its prevalence is ~1–2% of the world population
with considerable differences among regions and individuals with different skin types.
It is the skin disease that most frequently affects the nail. At the time of consultation,
roughly one half of the patients suffer from nail changes. Over lifetime, up to 90% of
all psoriatics will have had nail alterations. The prevalence of nail psoriasis is even
higher in psoriatic arthritis.1 Nail lesions often appear around 10 years later than
skin lesions, which may in part be the reason for nail psoriasis being observed less
frequently in children. In general, cutaneous psoriasis is more severe in individuals
with nail involvement.
Etiology and pathogenesisNeither gender nor race predilection appears to exist. There is no association of HLA-
C0602 with nail and joint involvement, but nail psoriasis is often associated with an
inflammation at the insertion points of tendons and ligaments giving rise to enthesitis.
Correspondence: Eckart Haneke Schlippehof 5, 79110 Freiburg, Germany Tel +49 761 897 8368 Fax +49 761 383 7401 Email [email protected]
Journal name: Psoriasis: Targets and TherapyArticle Designation: REVIEWYear: 2017Volume: 7Running head verso: HanekeRunning head recto: Nail psoriasisDOI: http://dx.doi.org/10.2147/PTT.S126281
P
soria
sis:
Tar
gets
and
The
rapy
dow
nloa
ded
from
http
s://w
ww
.dov
epre
ss.c
om/ b
y 16
1.62
.252
.40
on 2
6-Ja
n-20
18F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

Psoriasis: Targets and Therapy 2017:7submit your manuscript | www.dovepress.com
Dovepress
Dovepress
52
Haneke
Thus, the nail lesions were believed to represent an abnormal
response to tissue stressing of the integrated nail-joint appara-
tus, rather than being due to autoimmunity. The nail and joint
disease may be linked to tissue-specific factors, including
tissue biomechanical stressing and microtrauma, that lead to
activation of aberrant innate immune responses.2 However, a
case of skin and nail psoriasis definitely disappearing after
allogeneic bone marrow transplantation is more in favor of
predominant immunogenetic factors.3
Clinical characteristics of nail psoriasisPsoriasis causes a variety of both specific as well as ambigu-
ous nail lesions. Fingernails are more frequently affected than
toe nails, probably because they grow faster. Particularly, for
scientific purposes, nail psoriasis is often divided into matrix
and nail bed involvement or both, which is also reflected in
many trials differentiating the response into general, more on
matrix or nail bed psoriasis. Pits are the most characteristic
and most frequent signs and are seen as small, sharply delim-
ited depressions in the nail surface. They are of remarkably
even size and depth. Their distribution may be haphazard or
they may sometimes be arranged in parallel transverse or
short longitudinal lines. They are the result of tiny psoriatic
foci in the apical matrix producing parakeratosis, which
breaks off when it grows out from under the proximal nail
fold then leaving these depressions. Sometimes, the para-
keratosis remains and is seen as an ivory-colored spot in the
proximal half of the nail plate. Pits may be single, which is
not yet psoriasis specific, or multiple. Ten pits in one nail or
>50 pits on all nails are regarded as proof of psoriasis. Red
spots in the lunula usually represent a very active psoriasis
lesion with dilatation of the capillaries and thinning of the
suprapapillary plate. Red or mottled lunulae are due to the
dilatation of matrix blood vessels.4
Total matrix affection results in complete nail destruction
with crumbling of the plate, whereas leukonychia is seen
when the mid- to distal matrix is affected and parakeratotic
cells are incorporated into the nail plate making it optically
opaque. In most cases, psoriatic leukonychia is an ill-defined
white transverse band. Splinter hemorrhages are very narrow,
some millimeters long reddish-darkbrown to black streaks.
They are analogous to Auspitz’s phenomenon of the skin
and either due to hemorrhage from the dilated capillaries
in the nail bed or due to blood clots in these longitudinally
arranged small vessels. Salmon or oil spots are very frequent
and represent psoriatic plaques in the most distal matrix and
the nail bed. This area looks like paper on which a drop of oil
has fallen: a yellowish-brownish spot with a red margin shines
through the plate because the psoriatic squames compressed
under the nail are imbibed with serum. When a salmon spot
reaches the hyponychium, the parakeratosis breaks out and
psoriatic onycholysis develops. This typically has a reddish
proximal margin differentiating it from most other causes of
onycholysis, such as onychomycosis. Subungual hyperpara-
keratosis may be thick and then no oil drop phenomenon is
seen. The hyperkeratosis may be very marked and at times
so extreme as to resemble pachyonychia congenita. Psoriasis
affecting the dorsal as well as the ventral surface of the proxi-
mal nail fold results in swelling and rounding of its free edge.
This leads to a spontaneous loss of the cuticle characterizing
the pattern of chronic paronychia.
As mentioned earlier, psoriatic arthritis is very frequently
associated with severe nail involvement and psoriatic paro-
nychia, complete nail destruction, and swelling of the distal
interphalangeal joint. This has a serious negative influence
on the quality of life.
In contrast, psoriatic pachydermoperiostosis is closely
related to psoriatic arthritis but usually without obvious nail
changes. Mainly the big toe is considerably swollen and
often painful.
Three different forms of pustular psoriasis are differenti-
ated. Nail changes are seen in all of them. The nail changes in
the palmar plantar pustular psoriasis of Barber–Königsbeck
are similar to the common type of psoriasis, but the surface
defects may be larger and are called elkonyxis. Yellow sub-
ungual spots represent large Munro’s abscesses. Subungual
abscesses are frequent in the generalized pustular psoriasis
of von Zumbusch. Acrodermatitis continua suppurativa of
Hallopeau is the most notorious form of pustular psoriasis of
the nails. It often begins with one single digit where the skin
of the distal phalanx turns red and develops some pustules
migrating under the nail and causing nail dystrophy. With
time, the entire nail unit may disappear leaving a red smooth
digit tip until the disease slowly wanes off. Less frequently,
acrodermatitis continua suppurativa may initially involve
several fingers and toes and run a rapid and severe course.
Recently, a mutation in the interleukin 36 receptor antagonist
gene leading to a defect in interleukin 36 antagonist was
identified in generalized pustular psoriasis and acrodermatitis
continua suppurativa supporting the view that it belongs to
the autoinflammatory diseases group.5,6 Pustulosis palmo-
plantaris is histopathologically and genetically different and
rarely affects the periungual skin.7
Reiter’s disease is also known as reactive arthritis. It is
a systemic condition with characteristic joint, mucosal, eye,
P
soria
sis:
Tar
gets
and
The
rapy
dow
nloa
ded
from
http
s://w
ww
.dov
epre
ss.c
om/ b
y 16
1.62
.252
.40
on 2
6-Ja
n-20
18F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

Psoriasis: Targets and Therapy 2017:7 submit your manuscript | www.dovepress.com
Dovepress
Dovepress
53
Nail psoriasis
genito-urinary, skin, and nail changes. The latter are very
similar to pustular psoriasis. However, they often have a more
brownish tint due to a higher content of erythrocytes in the
pustules. Histopathology with extensive spongiform pustules
is virtually identical to pustular psoriasis.8
Nail psoriasis in childrenPsoriasis may occur at any age. Although rare, it was also
observed in the newborn. Erythrodermic psoriasis in children
usually shows ungual involvement with nail dystrophy and
marked subungual hyperkeratosis similar to pityriasis rubra
pilaris. Even pustular psoriasis and psoriatic arthritis were
observed in children.6
Diagnosis of nail psoriasisIn most cases, nail psoriasis follows cutaneous psoriasis and
is therefore easy to diagnose. However, ~5% of nail pso-
riasis occurs isolated and may pose diagnostic challenges.
This is particularly the case when even the nail alterations
are atypical such as a single nail in a child or of a toe,
isolated nail bed psoriasis without pits and salmon spots.
Histopathology is usually diagnostic, provided the biopsy is
sufficient, which is, unfortunately, often not the case. It has
to be remembered that matrix lesions cause changes of the
nail plate and those of the nail bed are seen under the nail
plate. The biopsy has to be taken slightly more proximal
than anticipated and must include enough subungual soft
tissue. In contrast, nail clippings are diagnostic for the most
important differential diagnosis, the various onychomycosis
forms, and sometimes give a strong hint at nail psoriasis.
Furthermore, nail psoriasis exhibits some features not com-
monly seen in cutaneous lesions.1 Dermatoscopy makes
the clinical signs more obvious and helps in the diagnosis.
Videodermatoscopy allows higher magnifications than the
usual hand-held dermatoscopes. Capillaroscopy shows the
dilated tortuous capillaries of the proximal nail fold. This
is even better visible in laser confocal microscopy. The
features of high-frequency ultrasound are less reliable but
may be of help for the very experienced. Optical coherence
microscopy uses a similar principle but has a much higher
resolution.
Differential diagnosisIn most cases, nail psoriasis is diagnosed on clinical grounds.8
Skin lesions elsewhere with one or several psoriatic nail
features suggest the correct diagnosis. With a good biopsy,
histopathology is usually pathognomonic and helps to delin-
eate nail psoriasis from other conditions, particularly onycho-
mycosis. The clinical diagnosis of pustular psoriasis is made
on the basis of red skin areas with a rim of small pustules.
Reiter’s disease requires additional laboratory examinations.1
Onychomycosis is said to be the most frequent nail dis-
ease. It has many features in common with nail psoriasis,
both clinically and histopathologically (Table 1).1
Another important differential diagnosis is the asym-
metric gait nail unit syndrome seen mainly in the big toenail
as an onycholysis without further criteria of nail psoriasis or
onychomycosis.9 Furthermore, nonspecific nail dystrophy,
particularly of toenails, is very common in the elderly, in
subjects with peripheral arterial disease, chronic venous
stasis, after trauma to the leg, in peripheral neuropathy, and
in some dermatoses such as eczema, nail lichen planus,
Darier’s disease, Hailey-Hailey disease, alopecia areata, and
many drugs.1,8
Table 1 Differential diagnosis of nail psoriasis and onychomycosis
Psoriasis Onychomycosis
Frequency High, commonest dermatosis with nail involvement Very high: up to 30–40% of all nail disordersCourse Chronic, often recurrent Chronic, often progressiveSymptoms Usually cosmetically and functionally embarrassing Embarrassing, sometimes painSigns Variable depending on nail structure involved Variable, depending on severity and type of onychomycosis as
well as pathogenic agentPits Very common, regular in size and shape Rare, irregularOnycholysis Common CommonDiscoloration None to yellow Yellow to brownSpores and hyphae Rarely spores Very frequentTransverse furrows Rare RareSkin lesions elsewhere Very common Often tinea pedum/manuumTrauma May be induced by Köbner phenomenon Important predisposing factorHeredity Strong hereditary component, particularly in juvenile
onset psoriasisAutosomal dominant susceptibility to develop onychomycosis
Note: Copyright © 2009. Haneke E. Adapted from Haneke E. Non infectious inflammatory disorders of the nail apparatus. J Dtsch Dermatol Ges. 2009;7:787–797.10 Data from Haneke E.1
P
soria
sis:
Tar
gets
and
The
rapy
dow
nloa
ded
from
http
s://w
ww
.dov
epre
ss.c
om/ b
y 16
1.62
.252
.40
on 2
6-Ja
n-20
18F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

Psoriasis: Targets and Therapy 2017:7submit your manuscript | www.dovepress.com
Dovepress
Dovepress
54
Haneke
Grading and assessment of nail psoriasisReliable repeatable specific validated severity and outcome
measures are necessary to evaluate a disease and its response
to a specific treatment.11 This was missing in nail psoriasis
until the nail psoriasis severity index (NAPSI), target NAPSI,
and its many variants were established.12 NAPSI is calculated
by dividing each nail into four quadrants. Each quadrant is
evaluated for the presence of psoriasis manifestations of
the nail matrix, such as pitting, leukonychia, red spots in
the lunula, and nail plate crumbling, as well as of the nail
bed, such as oil-drop phenomenon, onycholysis, subungual
hyperkeratosis, and splinter hemorrhages. If any of these
signs is present in all four quadrants, a score of 4 is given.
A score of 0 represents no signs in any quadrant. Each nail
is evaluated for a matrix and a nail bed score of 0–4. They
are combined to yield a maximal score of 0–8 for each nail.
All nails may be evaluated, with the total NAPSI score being
the sum of the scores, up to 80 if only fingers are considered,
or up to 160 if fingers plus toes are included.12 If only the
most seriously affected nail is evaluated, it is called target
NAPSI; this is often done to assess the effects of a therapeutic
regimen.11 Many therapeutic studies use (target) NAPSI-50,
NAPSI-75, and NAPSI-90 to indicate the percentage of
patients that reach a (target) NAPSI improvement of 50, 75,
or 90%, respectively. The NAPSI has some disadvantages,
such as being too time-consuming to be used in clinical
practice, and that the NAPSI scores often do not correspond
with the clinical severity of nail psoriasis.13 A new scoring
system, the N-NAIL, overcomes many of these limitations,
but it has yet to prove its clinical practicability.13 The use of
many different scoring systems, major differences in study
design, inclusion criteria, and follow-up make it difficult if
not impossible to compare the results of most nail psoriasis
trials.11 In addition, subjective and objective patient factors
such as quality of life, satisfaction with treatment ease and
outcome, adverse effects and not the least practicability, and
cost of treatment are important factors.11 Such an evalua-
tion and assessment tool for nail psoriasis has recently been
published under the term of nail assessment in psoriasis and
psoriatic arthritis.14
AssociationsPsoriasis is a frequent skin disease. In the last decades, a
metabolic syndrome associated with psoriasis has been
described; however, this is not of particular importance for
ungual psoriasis except in psoriatic arthritis. Associations
and co-occurrence with other skin disorders involving the
nail are rather common. The most important differential
diagnosis is onychomycosis. Both conditions may look very
similar. A psoriatic nail may be colonized with pathogenic
fungi, and a true infection of the psoriatic nail is not infre-
quent (Table 1).1,15
Impact on quality of lifeNail psoriasis has a profound negative influence on all aspects
of quality of life as well as on daily, sports, and professional
activities.16–20 Women try to hide their nails and cover them
with nail lacquer; although common nail varnishes are not
harmful, artificial nails, particularly when long, increase
the mechanical stress and strain to the nail plate – nail bed
attachment acting as a Köbner phenomenon and worsening
nail psoriasis. Similarly, professional activities with particu-
lar use of the fingers may have a deteriorating effect on the
disease. Matrix involvement scores higher than pure nail bed
affection as it results in more obvious nail plate damage.19
CourseNail psoriasis is chronic but often improves and worsens
without known reasons (Figures 1–4). Trauma may play an
important role in the exacerbation of nail psoriasis. There
may be periods without any nail alterations.1,8,10
Management of nail psoriasisManagement of the disease includes patient education,
avoidance of trauma to the nails, and different therapeutic
approaches with physical and pharmaceutical procedures
and agents.
Patient counseling includes education on the nature of
psoriasis, how life may be influenced by nail involvement,
about the specific problems of treatment, that nail psoriasis
is not due to an allergy or an “unhealthy” diet and thus is not
treatable with particular foods. However, smoking increases
the risk of psoriasis and obesity and alcohol use are associated
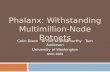
Figure 1 The thumbs of the patient mainly show nail bed involvement with subungual hyperkeratosis, salmon spot, and onycholysis.Notes: (A) Before treatment (September 2011). (B) After 3 months of topical treatment with calcipotriol plus betamethoasone dipropionate ointment and clobetasol solution under the nails: the right thumb shows some improvement and the left thum nail has worsened (December 2011).
P
soria
sis:
Tar
gets
and
The
rapy
dow
nloa
ded
from
http
s://w
ww
.dov
epre
ss.c
om/ b
y 16
1.62
.252
.40
on 2
6-Ja
n-20
18F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

Psoriasis: Targets and Therapy 2017:7 submit your manuscript | www.dovepress.com
Dovepress
Dovepress
55
Nail psoriasis
with a higher risk for psoriasis. It is important to avoid trauma
to the nail unit that will inevitably exacerbate the condition
or induce recurrences. Manicure and nail cleaning have to
be performed cautiously without further traumatizing the
hyponychium and attachment of the nail to the nail bed. It is
helpful to explain that genes are the most important etiologi-
cal factors and that the skin and nail lesions are amenable to
treatment but that the genes cannot be corrected. Many genes
contribute to the psoriatic personality, which may explain the
enormous variability of the clinical features including the
response to treatment. Particularly, chronic repeated trauma
is thought to be an aggravating factor. The development of
pits may be the result of microtraumata to the enthesis of the
extensor tendon and the dorsal aponeurosis of the distal inter-
phalangeal joint.2 They may be masked using nail varnish.
All nail psoriasis treatments require a long time, as the
nail is a slow-growing cutaneous appendage. The effect of any
treatment can usually not be evaluated before 3–6 months,
and it may take a year or longer to reach the maximum
improvement achievable with a given therapy. Pretreatment
photographs are highly recommended and should be repeated
at all follow-up visits to show the therapeutic result to the
patients. Concomitant onychomycosis may prevent clinical
cure, and it is a must to exclude fungal infection when start-
ing nail psoriasis therapy; a single remaining altered nail
during an otherwise efficacious therapy may be a hint at a
concomitant mycotic infection.1,21
Many different therapeutic measures are available. Their
choice depends on various factors such as severity of nail
involvement and its impact on quality of life, associated skin
lesions, psoriatic arthritis, comorbidities, profession, age,
patient preferences, potential risks, and not the least costs
and their reimbursement.
Nail psoriasis is very recalcitrant to almost all topical
treatments, whereas systemic therapies clearing the skin
are usually effective also in nail psoriasis.22 The problem of
all topical drugs is their limited penetration to the diseased
tissue: through all layers of the proximal nail fold with the
underlying nail in matrix lesions, through the nail plate, and
subungual hyperkeratosis in nail bed psoriasis. Hence, pits,
though often being rather inconspicuous, are the most resis-
tant to treatment. Nevertheless, a 3-month trial of a potent
antipsoriatic topical preparation is warranted (Figure 1). The
less nail is left the easier the penetration of the drug to the
very psoriatic lesion is. Clipping the onycholytic nail over
the nail bed is essential to reach nail bed psoriasis. Thinning
the nail by filing or grinding, or drilling holes into the nail
plate with mechanical burrs23 or with ablative lasers, is often
used to enhance nail penetration.24
Corticosteroids are often used in nail psoriasis. They have
to be class IV (high potency) and applied once or twice a day
on the proximal nail fold in case of matrix and on the nail
plate in nail bed affection. Although probably still the most
commonly used drugs, corticosteroids were rarely tested
in controlled studies. Both clobetasol and betamethasone
dipropionate were tested in clinical trials and showed compa-
rable results11 concerning pitting, salmon patches, subungual
hyperkeratosis, and onycholysis.25,26 All high-potency steroids
carry the risk of skin atrophy when used on the proximal nail
fold, often associated with hypopigmentation. Whether or
not using them for 4–5 days a week as a “pulse” treatment is
Figure 2 Further development of the nail psoriasis.Notes: (A) After continued topical treatment (March 2012). (B) After repeated perilesional injections of triamcinolone acetonide crystal suspension (10 mg/mL), a marked improvement is seen (June 2012).
Figure 3 As topical and injection treatments are insufficient and inconvenient, systemic methotrexate is instituted.Notes: (A) Further improvement of the left thumb nail after 2 months of methotrexate (September 2012). (B) Despite continuous methotrexate therapy, the left thumb nail worsened again (July 2013).
Figure 4 There is residual nail bed psoriasis under methotrexate therapy. Finally, a biological treatment is instituted.Notes: (A) Slight distal onycholysis and subungual hyperkeratosis (November 2013). (B) Six weeks after the beginning of adalimumab therapy, the patient has 20 clear nails for the first time since >25 years.
P
soria
sis:
Tar
gets
and
The
rapy
dow
nloa
ded
from
http
s://w
ww
.dov
epre
ss.c
om/ b
y 16
1.62
.252
.40
on 2
6-Ja
n-20
18F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

Psoriasis: Targets and Therapy 2017:7submit your manuscript | www.dovepress.com
Dovepress
Dovepress
56
Haneke
equally effective and reduces this risk remains to be proven.
Clobetasol 8% was tested as a nail lacquer with good results
depending of the duration of the treatment.27
Perilesional injections are another type of local treat-
ment. This increases the concentration of the drug at the
site of disease while minimizing the dose for the whole
organism. Perilesional injection of corticosteroids is by far
the most often performed (Figure 2), either by injection with
a needle or by high air-pressure devices.28 Injection with a
30 G needle and using some distraction techniques such as
vibration and pressure around the area to be injected make
the procedure tolerable although some patients prefer the
needle-less technique. Apparently, the efficacy of different
high-pressure injectors varies considerably (O Correia, Inst
CUF, personal communication, 2014). We inject 0.1 mL of
a triamcinolone acetonide suspension (10 mg/mL) into both
sides of the proximal nail fold; injection into or under the nail
bed is extremely painful and requires prior anesthesia.29,30 The
injections are repeated on a monthly basis for 6 months and,
then, followed by every 6 weeks and later every other months.
However, not all patients tolerate the injections. Matrix and
nail bed signs of psoriasis respond slightly differently with
salmon spots and subungual hyperkeratosis usually show-
ing the best effect. Adverse effects are not uncommon with
subungual hematoma and temporary nail deformation being
relatively frequent29,30 and the disappearing digit, atrophy of
the terminal phalanx bone, and rupture of the extensor tendon
being the most serious ones.31–34 Epidermoid inclusion cysts
were observed after jet injections necessitating amputation.35
The combination of the vitamin D3 derivate calcipotriol
and a potent corticosteroid, such as betamethasone dipro-
pionate, has shown good results;26,27 personal experience
has shown that twice or even thrice daily application may be
worth trying. Another vitamin D derivative, such as tacalcitol,
was used alternatively with 8% clobetasol nail lacquer.33
Vitamin D3 (calcitriol) and its analogs calcipotriol and
tacalcitol are well established in the therapy of psoriasis
vulgaris due to their effects on epidermal differentiation
and proliferation and regulation of production and release of
proinflammatory cytokines.11 Most studies were done with
calcipotriol and tacalcitol.36,37 Apparently, their effect on nail
bed lesions is more marked than on matrix signs.
Calcineurin inhibitors have a profound inhibitory effect
on T-cell functions that are implicated in the pathogenesis of
psoriasis. Used systemically, cyclosporin A (CyA) is highly
active against psoriasis, but topical application of CyA
showed ambiguous results.11 The new calcineurin inhibitor
tacrolimus shows much better skin and nail penetration. It
demonstrated good activity on nail bed and matrix psoriasis
in a controlled study.38 No studies with pimecrolimus were
published until now.11
Tazarotene is a synthetic retinoid with antiinflammatory
and antiproliferative actions on keratinocytes. Tazarotene
0.1% was used for the treatment of nail psoriasis. The results
were variable, but one study compared it with clobetasol
showing equal results.25 It was also used in childhood nail
psoriasis.39 Side effects are mainly skin irritation with redness
and desquamation.11
5-Fluorouracil (5-FU) is an antimitotic and antiprolif-
erative agent, which is active against disorders with a high
proliferative activity, such as psoriasis. Only one study of
topical 5-FU with 20% urea as a penetration enhancer showed
good effects on nail psoriasis, but inflammation, infection,
onycholysis, and discoloration were observed as adverse
effects.40 Other investigators did not see a beneficial response.
This does not make 5-FU a favorite nail psoriasis agent.11
Dithranol was once the most commonly used antipso-
riatic topical, but because of its unpleasant cosmesis, it is
rarely used nowadays. One study reported some improve-
ment of nail bed lesions, but the staining of the nails made
it unacceptable.41
Indigo naturalis extract regulates proliferation and differ-
entiation of epidermal keratinocytes, restores the epidermal
barrier function, and inhibits inflammatory reactions. Twice
daily application of an oily extract reduced nail bed lesions
such as hyperkeratosis and onycholysis by about one half; it
was thus more effective than calcipotriol solution.42,43 Studies
are in progress to make it colorless and cosmetically more
acceptable (CH Yang, Chang Gung Memorial Hospital, per-
sonal communication, May 8, 2017).
Methotrexate was also used for perimatrical and nail bed
injections with acceptable results. The dose was 0.1 mL of a
25 mg/mL solution. Good results were seen after 6 months
and 15 weeks, respectively.44,45
Systemic treatments are indicated in widespread psoria-
sis. Those therapies proven successful for skin lesions usu-
ally also improve nail psoriasis. However, many physicians
and patients are reluctant to treat isolated ungual psoriasis
systemically. A European Consensus Paper on the treatment
of psoriasis defines the involvement of particularly sensi-
tive areas such as the head and neck, genito-anal area, and
nails as moderate to severe. The selection of the mode of
treatment then depends on the severity of the nail disease,
its impact on quality of life, on professional, sports, and
social activities, and in particular on potential associated
psoriatic arthritis.
Systemic corticosteroids are not a good option for pso-
riasis vulgaris and in particular for nail psoriasis. High doses
P
soria
sis:
Tar
gets
and
The
rapy
dow
nloa
ded
from
http
s://w
ww
.dov
epre
ss.c
om/ b
y 16
1.62
.252
.40
on 2
6-Ja
n-20
18F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

Psoriasis: Targets and Therapy 2017:7 submit your manuscript | www.dovepress.com
Dovepress
Dovepress
57
Nail psoriasis
are necessary with a considerable risk of serious side effects,
break-through phenomena, and development of pustulation
of hitherto not pustular psoriasis.
Methotrexate has been introduced into the treatment of
cutaneous psoriasis and psoriatic arthritis in the 1960s. It is an
inexpensive drug with good efficacy in skin lesions; however,
as an antimetabolite, it slows down the nail growth rate and
improvement in nail lesions is therefore often slow and seen
very late (Figure 3). Furthermore, there is a risk of severe side
effects such as hepatotoxicity, lymphopenia, lekopenia, nau-
sea, and erosive stomatitis. Long-term toxicity includes liver,
lung, and heart fibrosis. The dose is usually slowly increased
to reach ~10–20 mg/week. Both oral and injection therapies
are possible with virtually equal doses as the bioavailability
of methotrexate is very good.46–48 NAPSI improvement is
between 25 and maximally 50%. Methotrexate has also been
injected intralesionally with a good result.44,45
Ciclosporin A is another established systemic antipsori-
atic drug. It is a calcineurin inhibitor with strong immunosup-
pressive action. Its positive effect on cutaneous and ungual
psoriasis is well established, both in single-drug studies as
well as in comparative ones.49,50 The dose is usually 3–5 mg/
kg daily, but half the dose is often given in Japan after initial
improvement.51 Although ciclosporin is probably the most
active “classical” systemic antipsoriatic drug, it is limited
to a treatment period of 6–12 months because of potentially
serious adverse effects such as disturbance of renal function,
arterial hypertension, diabetes mellitus, nausea, hypertricho-
sis, gingival hyperplasia, paresthesia, fatigue, and headache.
Synthetic retinoids have been used to treat extensive skin
psoriasis. The first of these drugs was etretinate. Although it
had a good effect on nail changes in some cases,52,53 etretinate
is no longer used and substituted by its derivative acitretin.
Acitretin is the follower product of etretinate with a shorter
half-life in the body. It is usually given in a dose of 0.5–1 mg/
kg/day.54,55 Its action is slow and, in most cases, does not reach
>50% improvement of nail psoriasis.56 All retinoids have a
number of side effects, particularly when given in a dose
>0.5 mg/kg/day, such as dry and cracking lips, dry mouth,
hair loss, and in children ossification disturbances. High-dose
retinoids can have an onychodestructive effect and are no
longer recommended as the first-line nail psoriasis treatment;57
however, good results were seen in generalized pustular pso-
riasis and acrodermatitis continua suppurativa.57 Acitretin is
occasionally used in combination with photochemotherapy
with ultraviolet (UV) A and narrow band UV B.
Fumaric acid esters are used for psoriasis treatment in
some countries, mainly in Europe, but their use was somewhat
controversial. A case report described a good effect on nail
psoriasis.58 Side effects are mainly gastrointestinal, flushing,
lymphopenia, and rarely renal dysfunction.
Leflunomide is a disease-modifying antirheumatic agent
with an effect on psoriatic arthritis and also a modest action
on nail psoriasis.59 Sulfasalazine was used in one patient
with a beneficial effect.60 Silicic acid was given orally and
topically on skin lesions. Ten of the 12 patients treated had
nail lesions, and five of them cleared completely, although
the nails were not treated with the silicic acid gel; thus, a
systemic effect was postulated.61
Apremilast is a new small-molecule oral phosphodies-
terase 4 inhibitor reducing the expression of several proin-
flammatory mediators; it is more an antiinflammatory than
immunosuppressive agent distinguishing it from most other
systemic antipsoriatic compounds. It has an excellent safety
profile with no known organ toxicity, thus obviating the need
for laboratory controls.62 It is approved for the treatment of
cutaneous psoriasis and psoriatic arthritis and has shown a
good effect in nail psoriasis, although only after 32 weeks.
Its cost may, however, limit its widespread use.63,64 A nail
lacquer containing apremilast is being developed;65 however,
human studies on nail psoriasis have not yet been published.
Tofacitinib is a small-molecule oral Janus kinase inhibitor
interfering in the JAK–STAT pathway. It is active against pso-
riasis and alopecia areata including their nail manifestations.
In four Phase III randomized controlled studies and compared
to etanercept, a twice daily dose of 5 or 10 mg was shown to
be noninferior to etanercept injected subcutaneously twice
weekly with sustained effects up to 52 weeks.66–69
Biologicals are a new development in the treatment of
many, mainly immunologically mediated diseases, among
them also psoriasis. There are several classes, both concern-
ing the nature of the antibody as well as their target, such
as humanized and fully human antibodies and antibodies
to tumor necrosis factor-a, various interleukins, and T-cell
inhibitors, respectively. They all have profound immunosup-
pressive actions and are thus not without risk, particularly
concerning infections and re-activation of tuberculosis, to
mention but a few.11 Biologicals are usually considered sec-
ond- or third-line treatments when other established topical
and systemic antipsoriatic drugs were not or not sufficiently
active in suppressing nail lesions.70 In contrast, nail psoriasis
was found to be an indicator of poor prognosis for the treat-
ment of psoriasis with biologicals independent of the specific
substance used.71 In most cases, nail psoriasis responses lag
behind those of cutaneous psoriasis, which can in part be
explained by the slow growth of nails as nail plate changes
P
soria
sis:
Tar
gets
and
The
rapy
dow
nloa
ded
from
http
s://w
ww
.dov
epre
ss.c
om/ b
y 16
1.62
.252
.40
on 2
6-Ja
n-20
18F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

Psoriasis: Targets and Therapy 2017:7submit your manuscript | www.dovepress.com
Dovepress
Dovepress
58
Haneke
have to grow out, whereas nail bed changes may be seen
earlier. In comparison with “classical” systemic drugs, eg,
methotrexate and cyclosporin, biologicals often show a dra-
matic and more rapid improvement. However, only 20–57%
of the patients reach a 90% improvement of their NAPSI
score with biologicals and the effect is lost after 47 months
in average.72,73 The most likely mechanism is the formation
of antidrug antibodies, but compensatory production of
other proinflammatory cytokines and a particular individual
reaction may be the cause that many patients stop this treat-
ment.74 In many countries, biologicals are not automatically
reimbursed by the social health insurance and patients and
physicians have to give evidence that previous, less expensive
treatments were not sufficiently efficacious.
TNF-a inhibitors were the first biologicals developed
for psoriasis treatment. TNF-a is a cytokine with proinflam-
matory action that induces keratinocyte proliferation and
prevents apoptosis. Most experience was gained with inflix-
imab, the first of this group, but in general, the efficacy of all
TNF-a inhibitors currently available for psoriasis treatment
is virtually comparable. Also their side effects and limita-
tions are the same. Activation of opportunistic infections,
congestive heart failure, demyelinating disorder, antibodies
against TNF-a inhibitors, and rarely lupus erythematosus
may occur.11
Infliximab is a chimeric human-mouse IgG1 antibody
binding membrane-bound and soluble TNF-a. This reduces
epidermal T-lymphocyte infiltration. It exhibits certain anti-
genicity and may thus induce autoantibodies that may reduce
its effectiveness thus requiring higher doses with time. It has
to be given intravenously, and ~16% of the patients develop
infusion reactions such as fever, chills, flush, urticaria,
myalgia, arthralgia, nausea, hypotension, and dyspnea.75
Infliximab was associated with a higher rate of onychomy-
cosis compared to the other TNF-a inhibitors.76 Patients
with a high psoriasis area severity index (PASI) response
also show a good NAPSI response. Almost one half of the
patients demonstrated complete nail clearance after 50 weeks.
NAPSI reduction by 50% was achieved by almost all patients,
80% reached NAPSI-75, 30% reached NAPSI-90, and 10%
cleared completely.77 Infliximab appears to be the fastest
acting TNF-a inhibitor. Its dosage is usually 5 mg/kg given
on weeks 0, 2, and 6 and if necessary 8.
Adalimumab is a human monoclonal IgG1 antibody
against TNF-a. It binds to cell surface proteins of the TNF-a
receptor preventing its action. Its mechanism of action is
similar to that of infliximab. Roughly 50–60% of NAPSI
improvement are achieved.11,78
The combination with cyclosporin was shown to be
particularly effective reaching a reduction of the NAPSI
score of 100%.79 Adalimumab did not increase the rate of
onychomycoses.76 The dose is 80 mg at baseline, then 40 mg
every 2 weeks, but some authors gave 40 mg from the begin-
ning (Figure 4).11
Certolizumab pegol is a PEGylated TNF-a inhibitor
that is Fc free. It is effective in the treatment of rheumatoid
arthritis and psoriasis with efficacy in nail psoriasis, enthesi-
tis, and dactylitis.80,81
Being a fusion of the TNF receptor with the Fc part of the
IgG1 antibody etanercept blocks the action of TNF-a. Thus,
its mechanism of action is similar to that of infliximab and
adalimumab. Several reports on its use in nail psoriasis dem-
onstrated good results.82 There was no statistically different
outcome with 50 mg once or twice weekly after 12 weeks and
target NAPSI improvement between 71 and 76%.83 It was also
effective in refractory acrodermatitis continua suppurativa.84
Golimumab is another TNF-a inhibitor approved for
psoriatic arthritis with an effect on nail psoriasis. Target
NAPSI improvement was over 40% after 24 weeks and 52%
after 52 weeks of treatment with 50 mg every 4 weeks.85,86
All TNF-a inhibitors have the potential to paradoxically
worsen psoriasis or even induce it.87,88 In many cases, this
regresses despite continuation of the therapy or when another
biological is used. This is apparently independent from the
condition for which TNF-a inhibitors were administered.88–91
The mechanism of action may be an unabated interferon-a
production by plasmacytoid dendritic cells, which might result
in psoriasis flares and induction of psoriasiform lesions.91,92
T-cell inhibitors such as alefacept and efalizumab are
not widely used because of their considerable adverse effect
profile.93 Efalizumab is a monoclonal CD11a antibody and
was withdrawn from the market because of cases of leuken-
cephalopathy observed under treatment with this molecule.
Alefacept is a fusion protein binding at the CD2 portion of
the leukocyte function antigen-3 linked to the Fc portion of
human IgG1 and targets T lymphocytes. No studies to evalu-
ate the efficacy of these drugs in nail psoriasis were published.
Rituximab causes B-cell depletion. Its role in the treat-
ment of nail psoriasis is not yet examined.93,94
New biologicals focus on the inhibition of interleukins
involved in the propagation of the psoriatic process. Their
nonspecific immunosuppressive action is less pronounced
compared with the TNF-a inhibitors. The targets are mainly
IL-12/IL-23 and IL-17. However, it was shown that anti-IL-12
action might be proinflammatory under certain circumstances
and thus counterproductive for the therapy of psoriasis.95
P
soria
sis:
Tar
gets
and
The
rapy
dow
nloa
ded
from
http
s://w
ww
.dov
epre
ss.c
om/ b
y 16
1.62
.252
.40
on 2
6-Ja
n-20
18F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

Psoriasis: Targets and Therapy 2017:7 submit your manuscript | www.dovepress.com
Dovepress
Dovepress
59
Nail psoriasis
Anti-interleukin 17 therapy is based on the fact that IL-17
plays a central role in the development of psoriatic lesions,
but IL-17 is also important for the defense against extracel-
lular pathogens and recruits neutrophils.
IL-17 inhibitors are secukinumab, ixekizumab, and bro-
dalimumab, but there are no ongoing studies with the last one.
Secukinumab is a human monoclonal IL-17A antibody
approved for plaque psoriasis and psoriatic arthritis that has
also shown good efficacy in nail psoriasis. It has an early
onset action and a sustained effect. Its safety profile is accept-
able. It is administered subcutaneously with a 300 mg dose
at weeks 0, 1, 2, 3, 4, and then every 4 weeks. At 16 weeks,
both 150 and 300 mg secukinumab were superior to placebo
with further improvement with longer treatment periods.96,97
Ixekizumab is another humanized monoclonal antibody
directed against IL-17A recently approved for psoriasis. It
demonstrated significant improvement of the NAPSI score as
early as 2 weeks after start of the treatment, which sustained
to week 20 when given in a dose of 75 mg at weeks 0, 2,
4, 8, and 12 and then 120 mg every 4 weeks from week 20
onward.98,99
Brodalumab is a human monoclonal IL-17A antibody
active against plaque psoriasis. It was more active than
ustekinumab in a head-to-head comparison. Although
approved in the US and Japan, the clinical development was
terminated as suicidal ideation and behavior were observed.100
IL-23 is another important proinflammatory cytokine
involved in the pathogenesis of psoriasis.
Antibodies targeting the p40 subunit of IL-23 also have an
action against IL-12 as they both share this subunit. Antibod-
ies directed against the p19 subunit are selective for IL-23.
Ustekinumab is a monoclonal antibody directed against
the p40 subunit of IL-12/23. It is active against psoriasis and
psoriatic arthritis and was also shown to have a good action
on nail psoriasis. Nail improvement was observed from week
4 onward with significant improvement of 90% at week 40.
NAPSI and PASI improvement ran parallel. The dose is 45
and 90 mg if the weight is over 100 kg, usually at weeks 0,
4, 16, and 28.101–103 Efficacy and side effects are comparable
to the other IL inhibitors.
Briakinumab was another monoclonal antibody directed
at p40. After showing good clinical results, its development
was stopped because of severe infections and a higher inci-
dence of other severe side effects.104
Guselkumab is a fully human IgG1k monoclonal IL-23
antagonist directed against the unique p19 subunit of IL-23;
it has no anti-IL-12 component. It has a profound action
on moderate-to-severe plaque psoriasis and was superior to
adalimumab.105 The dose given was 100 mg at weeks 0, 4,
12, 16, and 20 and then every 8 weeks.
Tildrakizumab and BI-655066 are also targeting the p19
subunit of IL-23. They are currently being studied for vari-
ous indications including psoriasis.106,107 No results are yet
available concerning nail psoriasis.
In summary, most new biological drugs have a good and
reliable action on nail psoriasis with an acceptable adverse
effect profile. They are more active than most of the classical
systemic antipsoriatic drugs.
Radiotherapy is an “old“ treatment modality, which has
come out of time not only because of potential long-term
adverse effects but also because most dermatologists no
longer operate X-ray machines because of the difficulties to
comply with the bureaucratic challenges associated with the
use of therapeutic ionizing rays. However, some studies report
favorable results with Grenz rays,108 superficial X-rays,109,110
and electron beam therapy.111
Light has been used for a long time, but as nails are
virtually impermeable for UV B and allow <2% of UV A to
penetrate, the effect is rather limited.112 Potentiation of UV
by specific photosensitizers, called photochemotherapy, was
beneficial in some studies48,113 but is often associated with
multiple melanonychias.114
Intense pulsed light (IPL) is a broad-spectrum light
source with a high-energy intensity. With a 550 nm filter, it
has been used for the treatment of plaque psoriasis. A trial
on 20 patients with finger and toenail psoriasis using IPL
with a cutoff filter of 550 nm and a median of 8.6 sessions
resulted in significant improvement in the NAPSI with
nail bed lesions showing a reduction of 71% and matrix
lesions of 32%. A relapse was seen in three patients after
6 months.115
Lasers have also been used to treat nail psoriasis. The
pulsed dye laser (PDL) is the device of choice as it targets
the dilated capillaries in the matrix and nail bed. In many
studies, 1.5–6 ms pulses were used with a good effect on
matrix and nail bed lesions.116,117 A comparative study using
6 ms pulse length and 9 J/cm2 and 0.45 ms and 6 J/cm2
gave almost the same improvement of matrix and nail bed
lesions with significantly less pain with the shorter pulse.118
Side effects are mainly pain, hemorrhage, and pigmentation.
These results were confirmed in another trial.119 PDL with
tazarotene was significantly more effective than tazarotene
alone.120 A comparison of the PDL with the excimer laser
gave significantly better improvement with the PDL.121 In
another comparative study, PDL was compared with the
Nd:YAG laser. Both groups were treated with calcipotriol
P
soria
sis:
Tar
gets
and
The
rapy
dow
nloa
ded
from
http
s://w
ww
.dov
epre
ss.c
om/ b
y 16
1.62
.252
.40
on 2
6-Ja
n-20
18F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

Psoriasis: Targets and Therapy 2017:7submit your manuscript | www.dovepress.com
Dovepress
Dovepress
60
Haneke
betamethasone in addition. Whereas the results were com-
parably good, the Nd–YAG was significantly more painful.122
Photodynamic therapy (PDT) uses light and a photoactive
substance that both generate reactive oxygen species able
to kill those cells that accumulated the photosensitizer. In a
comparative study, no difference was found between PDL
and PDT.117 However, there is considerable heat develop-
ment during the illumination of the target and this is often
not tolerated by the patients.
ConclusionNail involvement in psoriasis is common. It is an indicator of
poor prognosis and of a higher risk to develop psoriatic arthritis.
Surprisingly, nail psoriasis is only briefly mentioned in most
national and European guidelines on the diagnosis and treat-
ment of psoriasis; however, the European Nail Society is now
working on recommendations for the treatment of nail psoriasis.
The many treatments available give evidence that hitherto
none is the ideal therapy. Topicals have to fight with the dif-
ficulties to get through the nail and nail fold to the diseased
structures. Injections that bring the remedy to the site of the
disease process and greatly avoid systemic effects are pain-
ful and carry the risk of local side effects. Systemic drugs
are often not used for isolated nail psoriasis, although this is
accepted as a severe psoriasis considerably impairing quality
of life. However, it is known that virtually all systemic treat-
ments that improve the skin lesions are also beneficial for
the nails, although often with a delayed and less pronounced
response. The potential systemic adverse effects have to be
kept in mind before and during such a therapy. The develop-
ment of new biologicals has revolutionized psoriasis treat-
ment and thus also that of ungual psoriasis. Finally, there
are some physical modalities such as ionizing rays, various
light qualities including photodynamic treatment, and lasers.
Many treatment possibilities may make it delicate to
choose the right approach. It is certainly wise to begin with
a topical antipsoriatic preparation (Table 2). This has to be
used for a minimum of 4–6 months before its efficacy can
be evaluated. If this does not help sufficiently, a classical
antipsoriatic drug such as methotrexate, fumaric acid ester,
and cyclosporine would be the second choice while keep-
ing in mind all potential contraindications. If the results are
not satisfying a biological may be chosen. Again, there are
many contraindications that have to be carefully looked for
before starting such a treatment. The choice is huge now, and
the treating physician has to select among TNF-a blockers,
agents interfering with T-lymphocyte functions, and IL-23
and IL-17 inhibitors.
In summary, nail psoriasis is still an underestimated part
of psoriasis, but the outlook is bright with many new treat-
ments available.
DisclosureThe author reports no conflicts of interest in this work.
References 1. Haneke E. Nail disorders. In: Goldsmith LA, Katz SI, Gilchrest BA,
Paller AS, Leffel DJ, Wolff K, editors. Fitzpatrick’s Dermatology in General Medicine. 9th ed. New York: McGraw-Hill; In press 2017.
2. McGonagle D, Tan AL, Benjamin M. The nail as a musculoskeletal appendage-implications for an improved understanding of the link between psoriasis and arthritis. Dermatology. 2009;218:97–102.
3. Yokota A, Hukazawa M, Nakaseko C, et al. Resolution of psoriasis vulgaris following allogeneic bone marrow transplantation for aplastic anemia. Rinsho Ketsueki. 1996;37(1):35–39.
4. Peña-Romero A, Toussaint-Caire S, Domínguez-Cherit J. Mottled lunulae in nail psoriasis: report of three cases. Skin Appendage Disord. 2016;2(1–2):70–71.
5. Marrakchi S, Guigue P, Renshaw BR, et al. Interleukin-36-receptor antagonist deficiency and generalized pustular psoriasis. N Engl J Med. 2011;365(7):620–628.
6. Kelati A, Baybay H, Najdi A, Zinoune S, Mernissi FZ. Pediatric pso-riasis: should we be concerned with comorbidities? A cross sectional study. Pediatr Int. 2017;59(8):923–928.
7. Misiak-Galazka M, Wolska H, Rudnicka L. What do we know about palmoplantar pustulosis? J Eur Acad Dermatol Venereol. 2017;31(1):38–44.
8. Jiaravuthisan MM, Sasseville D, Vender RB, Murphy F, Muhn CY. Psoriasis of the nail: anatomy, pathology, clinical presentation, and a review of the literature on therapy. J Am Acad Dermatol. 2007;57(1):1–27.
Table 2 Treatment algorithm for nail psoriasis
Hitherto untreated mild NP (three nails, NAPSI <16)
Topical steroid class III–IVSteroid plus calcipotriol
No improvement Injections (steroids, methotrexate)
No improvement Systemic antipsoriatics (MTX, CyA [FAE])
More than three nails, NAPSI >16. Unsuccessfully pretreated
Systemic antipsoriatics (MTX, CyA [FAE])
No improvement Biologicals: TNF-a inhibitor No improvement Biologicals: TNF-a inhibitorIf TNF-a inhibitors no longer active or show a paradox worsening
IL-12/23 or IL-17 inhibitor
If IL-12/23 or IL-17 inhibitors no longer active Selective p19 inhibitor (IL-23)
Abbreviations: CyA, cyclosporin A; FAE, fumaric acid ester; MTX, methotrexate; NP, nail psoriasis; NAPSI, nail psoriasis severity index.
P
soria
sis:
Tar
gets
and
The
rapy
dow
nloa
ded
from
http
s://w
ww
.dov
epre
ss.c
om/ b
y 16
1.62
.252
.40
on 2
6-Ja
n-20
18F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

Psoriasis: Targets and Therapy 2017:7 submit your manuscript | www.dovepress.com
Dovepress
Dovepress
61
Nail psoriasis
9. Zaias N, Rebell G, Escovar S. Asymmetric gait nail unit syndrome: the most common worldwide toenail abnormality and onychomycosis. Skinmed. 2014;12(4):217–223.
10. Haneke E. Non infectious inflammatory disorders of the nail apparatus. J Dtsch Dermatol Ges. 2009;7:787–797.
11. Pasch MC. Nail psoriasis: a review of treatment options. Drugs. 2016;76(6):675–705.
12. Rich P, Scher RK. Nail psoriasis severity index: a useful tool for evalu-ation of nail psoriasis. J Am Acad Dermatol. 2003;49(2):206–212.
13. Klaassen KM, van de Kerkhof PC, Bastiaens MT, Plusje LG, Baran RL, Pasch MC. Scoring nail psoriasis. J Am Acad Dermatol. 2014;70(6): 1061–1066.
14. Augustin M, Blome C, Costanzo A, et al. Nail assessment in psoriasis and psoriatic arthritis (NAPPA): development and validation of a tool for assessment of nail psoriasis outcomes. Br J Dermatol. 2014;170(3): 591–598.
15. Klaassen KM, Dulak MG, van de Kerkhof PC, Pasch MC. The preva-lence of onychomycosis in psoriatic patients: a systematic review. J Eur Acad Dermatol Venereol. 2014;28(5):533–541.
16. Alpsoy E, Polat M, Fettahlıoğlu-Karaman B, et al. Internalized stigma in psoriasis: a multicenter study. J Dermatol. 2017;44(8):885–891.
17. Malakouti M, Brown GE, Leon A, et al. The dermatologic intimacy scale: quantitatively measuring the impact of skin disease on intimacy. J Dermatolog Treat. 2017;28(4):347–352.
18. Paek SY, Thompson JM, Qureshi AA, Merola JF, Husni ME. Compre-hensive assessment of the psoriasis patient (CAPP): a report from the GRAPPA 2015 annual meeting. J Rheumatol. 2016;43(5):961–964.
19. de Jong EM, Seegers BA, Gulinck MK, Boezeman JB, van de Kerkhof PC. Psoriasis of the nails associated with disability in a large number of patients: results of a recent interview with 1728 patients. Dermatol-ogy. 1996;193(4):300–303.
20. van der Velden HM, Klaassen KM, van de Kerkhof PC, Pasch MC. The impact of fingernail psoriasis on patients’ health-related and disease-specific quality of life. Dermatology. 2014;229(2):76–82.
21. de Vries AC, Bogaards NA, Hooft L, et al. Interventions for nail psoriasis. Cochrane Database Syst Rev. 2013;(1):CD007633.
22. Haneke E. Histopathology of the Nail – Onychopathology. Boca Raton: CRC Press; 2017.
23. Brem J. Effective topical method of therapy for onychomycosis. Cutis. 1981;27(1):69–76.
24. Tsai MT, Tsai TY, Shen SC, et al. Evaluation of laser-assisted trans-nail drug delivery with optical coherence tomography. Sensors (Basel). 2016;16(12):iiE2111.
25. Rigopoulos D, Gregoriou S, Katsambas A. Treatment of psoriatic nails with tazarotene cream 0.1% vs. clobetasol propionate 0.05% cream: a double-blind study. Acta Derm Venereol. 2007;87(2):167–168.
26. Tosti A, Piraccini BM, Cameli N, et al. Calcipotriol ointment in nail psoriasis: a controlled double-blind comparison with betamethasone dipropionate and salicylic acid. Br J Dermatol. 1998;139(4):655–659.
27. Baran R, Tosti A. Topical treatment of nail psoriasis with a new corticoid-containing nail lacquer formulation. J Dermatol Treat. 1999;10:201–204.
28. Nantel-Battista M, Richer V, Marcil I, Benohanian A. Treatment of nail psoriasis with intralesional triamcinolone acetonide using a needle-free jet injector: a prospective trial. J Cutan Med Surg. 2014;18(1):38–42.
29. de Berker DA, Lawrence CM. A simplified protocol of steroid injection for psoriatic nail dystrophy. Br J Dermatol. 1998;138(1):90–95.
30. Saleem K, Azim W. Treatment of nail psoriasis with a modified regi-men of steroid injections. J Coll Physicians Surg Pak. 2008;18(2): 78–81.
31. Wolf R, Tur E, Brenner S. Corticosteroid-induced ‘disappearing digit’. J Am Acad Dermatol. 1990;23(4 pt 1):755–756.
32. Deffer TA, Goette DK. Distal phalangeal atrophy secondary to topical steroid therapy. Arch Dermatol. 1987;123(5):571–572.
33. Bjorkman A, Jorgsholm P. Rupture of the extensor pollicis longus tendon: a study of aetiological factors. Scand J Plast Reconstr Surg Hand Surg. 2004;38(1):32–35.
34. Jakubik J. Finger tendon rupture following local application of triamcinolone-acetonide (Kenalog A-40). Acta Chir Plast. 1981;23(3): 180–188.
35. Mascaró JM. Epidermoid cyst formation after jet injection of tri-amcinolone for nail psoriasis. In: 29th Conf Coll Ibero Latino Am Dermatol CILAD; Sevilla; September 16–19, 2012.
36. Sanchez Regaña M, Martin Ezquerra G, Umbert Millet P. Nail psoria-sis: a combined treatment with 8% clobetasol nail lacquer and tacalcitol ointment. J Eur Acad Dermatol Venereol. 2008;22(8):963–969.
37. Tzung TY, Chen CY, Yang CY, Lo PY, Chen YH. Calcipotriol used as monotherapy or combination therapy with betamethasone dipropionate in the treatment of nail psoriasis. Acta Derm Venereol. 2008;88(3): 279–280.
38. De Simone C, Maiorino A, Tassone F, D’Agostino M, Caldarola G. Tacrolimus 0.1% ointment in nail psoriasis: a randomized controlled open-label study. J Eur Acad Dermatol Venereol. 2013; 27(8):1003–1006.
39. Diluvio L, Campione E, Paternò EJ, Mordenti C, El Hachem M, Chi-menti S. Childhood nail psoriasis: a useful treatment with tazarotene 0.05%. Pediatr Dermatol. 2007;24(3):332–333.
40. Fritz K. Successful local treatment of nail psoriasis with 5-fluorouracil [in German]. Z Hautkr. 1989;64(12):1083–1088.
41. Yamamoto T, Katayama I, Nishioka K. Topical anthralin therapy for refractory nail psoriasis. J Dermatol. 1998;25(4):231–233.
42. Lin YK, Chang YC, Hui RC, et al. A Chinese herb, Indigo naturalis, extracted in oil (Lindioil) used topically to treat psoriatic nails: a randomized clinical trial. JAMA Dermatol. 2015;151(6):672–674.
43. Lin YK, See LC, Huang YH, et al. Efficacy and safety of Indigo natu-ralis extract in oil (Lindioil) in treating nail psoriasis: a randomized, observer-blind, vehicle-controlled trial. Phytomedicine. 2014;21(7): 1015–1020.
44. Sarıcaoglu H, Oz A, Turan H. Nail psoriasis successfully treated with intralesional methotrexate: case report. Dermatology. 2011;222(1):5–7.
45. Daulatabad D, Grover C, Singal A. Role of nail bed methotrexate injec-tions in isolated nail psoriasis: conventional drug via an unconventional route. Clin Exp Dermatol. Epub 2017 Apr 10:doi: 10.1111/ced.13087.
46. Bauzá A, Redondo P, Aquerreta D. Psoriatic onycho-pachydermo periostitis: treatment with methotrexate. Br J Dermatol. 2000;143(4): 901–902.
47. Gümüşel M, Özdemir M, Mevlitoğlu I, Bodur S. Evaluation of the efficacy of methotrexate and cyclosporine therapies on psoriatic nails: a one-blind, randomized study. J Eur Acad Dermatol Venereol. 2011;25(9):1080–1084.
48. Sanchez-Regana M, Sola-Ortigosa J, Alsina-Gibert M, Vidal-Fernan-dez M, Umbert-Millet P. Nail psoriasis: a retrospective study on the effectiveness of systemic treatments (classical and biological therapy). J Eur Acad Dermatol Venereol. 2011;25(5):579–586.
49. Arnold WP, Gerritsen MJ, van de Kerkhof PC. Response of nail pso-riasis to cyclosporin. Br J Dermatol. 1993;129(6):750–751.
50. Mahrle G, Schulze HJ, Farber L, Weidinger G, Steigleder GK. Low-dose short-term cyclosporine versus etretinate in psoriasis: improvement of skin, nail, and joint involvement. J Am Acad Dermatol. 1995;32(1):78–88.
51. Syuto T, Abe M, Ishibuchi H, Ishikawa O. Successful treatment of psoriatic nails with low-dose cyclosporine administration. Eur J Dermatol. 2007;17(3):248–249.
52. Rabinovitz HS, Scher RK, Shupack JL. Response of psoriatic nails to the aromatic retinoid etretinate. Arch Dermatol. 1983;119(8):627–628.
53. Gajardo J. Experiencia clinica con etretinato (Tigason) en 26 paci-entes portadores de psoriasis. [Clinical experience with etretinate (Tigason) in 26 patients with psoriasis] [Spanish]. Rev Med Chil. 1989;117(5):516–522.
54. Murray HE, Anhalt AW, Lessard R, et al. A 12-month treatment of severe psoriasis with acitretin: results of a Canadian open multicenter study. J Am Acad Dermatol. 1991;24(4):598–602.
55. Brazzelli V, Martinoli S, Prestinari F, Borroni G. An impressive therapeutic result of nail psoriasis to acitretin. J Eur Acad Dermatol Venereol. 2004;18(2):229–230.
P
soria
sis:
Tar
gets
and
The
rapy
dow
nloa
ded
from
http
s://w
ww
.dov
epre
ss.c
om/ b
y 16
1.62
.252
.40
on 2
6-Ja
n-20
18F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

Psoriasis: Targets and Therapy 2017:7submit your manuscript | www.dovepress.com
Dovepress
Dovepress
62
Haneke
56. Tosti A, Ricotti C, Romanelli P, Cameli N, Piraccini BM. Evaluation of the efficacy of acitretin therapy for nail psoriasis. Arch Dermatol. 2009;145(3):269–271.
57. Baran R. Therapeutic assessment and side-effects of the aromatic retinoid on the nail apparatus (French). Ann Dermatol Venereol. 1982;109(4):367–371.
58. Vlachou C, Berth-Jones J. Nail psoriasis improvement in a patient treated with fumaric acid esters. J Dermatolog Treat. 2007;18(3):175–177.
59. Behrens F, Finkenwirth C, Pavelka K, et al. Leflunomide in psoriatic arthritis: results from a large European prospective observational study. Arthritis Care Res (Hoboken). 2013;65(3):464–470.
60. Gerster JC, Hohl D. Nail lesions in psoriatic arthritis: recovery with sulfasalazine treatment. Ann Rheum Dis. 2002;61(3):277.
61. Lassus A. Colloidal silicic acid for the treatment of psoriatic skin lesions, arthropathy and onychopathy. A pilot study. J Int Med Res. 1997;25(4):206–209.
62. Torres T, Puig L. Apremilast: a novel oral treatment for psoriasis and psoriatic arthritis. Am J Clin Dermatol. Epub 2017 Jun 8:doi: 10.1007/s40257-017-0302-0.
63. Papp K, Reich K, Leonardi CL, et al. Apremilast, an oral phospho-diesterase 4 (PDE4) inhibitor, in patients with moderate to severe plaque psoriasis: results of a phase III, randomized, controlled trial (efficacy and safety trial evaluating the effects of apremilast in psoriasis [ESTEEM] 1). J Am Acad Dermatol. 2015;73(1):37–49.
64. Paul C, Cather J, Gooderham M, et al. Efficacy and safety of apremilast, an oral phosphodiesterase 4 inhibitor, in patients with moderate-to-severe plaque psoriasis over 52 weeks: a phase III, ran-domized controlled trial (ESTEEM 2). Br J Dermatol. 2015;173(6): 1387–1399.
65. Kushwaha AS, Repka MA, Narasimha Murthy S. A novel apremilast nail lacquer formulation for the treatment of nail psoriasis. AAPS PharmSciTech. Epub 2017 Apr 28:doi: 10.1208/s12249-017-0776-3.
66. Di Lernia V, Bardazzi F. Profile of tofacitinib citrate and its potential in the treatment of moderate-to-severe chronic plaque psoriasis. Drug Des Devel Ther. 2016;10:533–539.
67. Papp KA, Menter MA, Abe M, et al. Tofacitinib, an oral Janus kinase inhibitor, for the treatment of chronic plaque psoriasis: results from two, randomised, placebo-controlled, phase 3 trials. Br J Dermatol. 2015;173:949–961.
68. Bachelez H, van de Kerkhof PC, Strohal R, et al. Tofacitinib versus etanercept or placebo in moderate-to-severe chronic plaque psoriasis: a phase 3 randomised non-inferiority trial. Lancet. 2015;386(9993): 552–561.
69. Merola JF, Elewski B, Tatulych S, Lan S, Tallman A, Kaur M. Efficacy of tofacitinib for the treatment of nail psoriasis: two 52-week, random-ized, controlled phase 3 studies in patients with moderate-to-severe plaque psoriasis. J Am Acad Dermatol. 2017;77(1):79.e–87.e.
70. Langley RG, Saurat JH, Reich K; on behalf of the Nail Psoriasis Delphi Expert Panel. Recommendations for the treatment of nail psoriasis in patients with moderate to severe psoriasis: a dermatology expert group consensus. J Eur Acad Dermatol Venereol. 2012;26(3):373–381.
71. Bardazzi F, Lambertini M, Chessa MA, Magnano M, Patrizi A, Pirac-cini BM. Nail involvement as a negative prognostic facor in biological therapy for psoriasis: a retrospective study. J Eur Acad Dermatol Venereol. 2017;31:843–846.
72. Gniadecki R, Kragballe K, Dam TN, Skov L. Comparison of drug survival rates for adalimumab, etanercept and infliximab in patients with psoriasis vulgaris. Br J Dermatol. 2011;164(5):1091–1096.
73. Gniadecki R, Bang B, Bryld LE, Iversen L, Lasthein S, Skov L. Com-parison of long-term drug survival and safety of biologic agents in patients with psoriasis vulgaris. Br J Dermatol. 2015;172(1):244–252.
74. Arnold T, Schaarschmidt ML, Herr R, Fischer JE, Goerdt S, Peitsch WK. Drug survival rates and reasons for drug discontinuation in psoriasis. J Dtsch Dermatol Ges. 2016;14(11):1089–1099.
75. Callen JP. Complications and adverse reactions in the use of newer biologic agents. Semin Cutan Med Surg. 2007;26(1):6–14.
76. Al-Mutairi N, Nour T, Al-Rqobah D. Onychomycosis in patients of nail psoriasis on biologic therapy: a randomized, prospective open label study comparing etanercept, infliximab and adalimumab. Expert Opin Biol Ther. 2013;13(5):625–629.
77. Fabroni C, Gori A, Troiano M, Prignano F, Lotti T. Infliximab efficacy in nail psoriasis. A retrospective study in 48 patients. J Eur Acad Dermatol Venereol. 2011;25(5):549–553.
78. Irla N, Yawalkar N. Marked improvement in nail psoriasis during treatment with adalimumab. Dermatology. 2009;219(4):353–356.
79. Karanikolas GN, Koukli EM, Katsalira A, et al. Adalimumab or cyclo-sporine as monotherapy and in combination in severe psoriatic arthritis: results from a prospective 12-month nonrandomized unblinded clinical trial. J Rheumatol. 2011;38(11):2466–2474.
80. Reich K, Ortonne JP, Gottlieb AB, et al. Successful treatment of moder-ate to severe plaque psoriasis with the PEGylated Fab0 certolizumab pegol: results of a phase II randomized, placebo-controlled trial with a re-treatment extension. Br J Dermatol. 2012;167:180–190.
81. Mease PJ, Fleischmann R, Deodhar AA, et al. Effect of certolizumab pegol on signs and symptoms in patients with psoriatic arthritis: 24-week results of a Phase 3 double-blind randomised placebo-controlled study (RAPID-PsA). Ann Rheum Dis. 2014;73(1):48–55.
82. Rallis E, Stavropoulou E, Rigopoulos D, Verros C. Rapid response of nail psoriasis to etanercept. J Rheumatol. 2008;35(3):544–545.
83. Ortonne JP, Paul C, Berardesca E, et al. A 24-week randomized clinical trial investigating the efficacy and safety of two doses of etanercept in nail psoriasis. Br J Dermatol. 2013;168(5):1080–1087.
84. Weisshaar E, Diepgen TL. Successful etanercept therapy in therapy-refractory acrodermatitis continua suppurativa Hallopeau. J Dtsch Dermatol Ges. 2007;5(6):489–492.
85. Kavanaugh A, McInnes I, Mease P, et al. Golimumab, a new human tumor necrosis factor alpha antibody, administered every four weeks as a sub-cutaneous injection in psoriatic arthritis: twenty-four-week efficacy and safety results of a randomized, placebo-controlled study. Arthritis Rheum. 2009;60(4):976–986.
86. Kavanaugh A, van der Heijde D, McInnes IB, et al. Golimumab in psoriatic arthritis: one-year clinical efficacy, radiographic, and safety results from a phase III, randomized, placebo-controlled trial. Arthritis Rheum. 2012;64(8):2504–2517.
87. Sfikakis PP, Iliopoulos A, Elezoglou A, Kittas C, Stratigos A. Psoriasis induced by antitumor necrosis factor therapy: a paradoxical adverse reaction. Arthritis Rheum. 2005;52:2513–2518.
88. Wollina U, Hansel G, Koch A, Schönlebe J, Köstler E, Haroske G. Tumor necrosis factor-a inhibitor-induced psoriasis or psoriasiform exanthemata. First 120 cases from the literature including a series of 6 new cases. Am J Clin Dermatol. 2008;9:1–14.
89. Pink AE, Foni A, Smith CH, Barker JNWN. The development of sarcoidosis on antitumour necrosis factor therapy: a paradox. Br J Dermatol. 2010;163:641–666.
90. Pirard D, Arco D, Debrouckere V, Heenem M. Anti-tumor necrosis factor alpha-induced psoriasiform eruptions: three further cases and current overview. Dermatology current overview. Dermatology. 2006;213:182–186.
91. Conrad C, Lapointe AK, Gilliet M. Paradoxic psoriasis induced by anti-TNF treatment – a report of 8 cases and evidence for a new patho-genic mechanism. In: 93rd Ann Meet Swiss Soc Dermatol Venereol; Geneva; 2011; FC 11, Dermatol Helv 2011;6:30
92. Haneke E. Nail psoriasis. In: Soung J, Koo B, editors. Psoriasis. Rijeka: Intech; 2011:141–186.
93. Menter A. The status of biologic therapies in the treatment of moderate to severe psoriasis. Cutis. 2009;84(suppl 4):14–24.
94. Wcisło-Dziadecka D, Zbiciak M, Brzezińska-Wcisło M, Mazurek U. Anti-cytokine therapy for psoriasis – not only TNF-a blockers. Overview of reports on the effectiveness of therapy with IL-12/IL-23 and T and B lymphocyte inhibitors. Postepy Hig Med Dosw (online). 2016;70:1198–1205.
95. Puig L. The role of IL 23 in the treatment of psoriasis. Expert Rev Clin Immunol. 2017;13(6):525–534.
P
soria
sis:
Tar
gets
and
The
rapy
dow
nloa
ded
from
http
s://w
ww
.dov
epre
ss.c
om/ b
y 16
1.62
.252
.40
on 2
6-Ja
n-20
18F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1

Psoriasis: Targets and Therapy 2017:7 submit your manuscript | www.dovepress.com
Dovepress
Dovepress
Psoriasis: Targets and Therapy
Publish your work in this journal
Submit your manuscript here: https://www.dovepress.com/psoriasis-targets-and-therapy-journal
Psoriasis: Targets and Therapy is international, peer-reviewed, open access journal focusing on psoriasis, nail psoriasis, psoriatic arthritis and related conditions, identification of therapeutic targets and the optimal use of integrated treatment interventions to achieve improved outcomes
and quality of life. Visit http://www.dovepress.com/testimonials.php to read real quotes from published authors.
Dovepress
63
Nail psoriasis
96. Reich K, Sullivan J, Arenberger P, et al. Secukinumab is effective in subjects with moderate to severe plaque psoriasis with significant nail involvement: 16 week results from the TRANSFIGURE study. Presented at: 23rd World Congress of Dermatology; Vancouver, Canada; June 8–15, 2015
97. Paul C, Reich K, Gottlieb AB, et al; CAIN457A2211 Study Group. Secukinumab improves hand, foot and nail lesions in moderate-to-severe plaque psoriasis: subanalysis of a randomized, double-blind, placebo-controlled, regimen-finding phase 2 trial. J Eur Acad Dermatol Venereol. 2014;28(12):1670–1675.
98. Leonardi C, Matheson R, Zachariae C, et al. Anti-interleukin-17 monoclonal antibody ixekizumab in chronic plaque psoriasis. N Engl J Med. 2012;366(13):1190–1199.
99. Langley RG, Rich P, Menter A, et al. Improvement of scalp and nail lesions with ixekizumab in a phase 2 trial in patients with chronic plaque psoriasis. J Eur Acad Dermatol Venereol. 2015;29(9):1763–1770.
100. Puig L. Brodalumab: the first anti-IL-17 receptor agent for psoriasis. Drugs Today (Barc). 2017;53(5):283–297.
101. Rallis E, Kintzoglou S, Verros C. Ustekinumab for rapid treatment of nail psoriasis. Arch Dermatol. 2010;146(11):1315–1316.
102. Vitiello M, Tosti A, Abuchar A, Zaiac M, Kerdel FA. Ustekinumab for the treatment of nail psoriasis in heavily treated psoriatic patients. Int J Dermatol. 2013;52(3):358–362.
103. Rich P, Bourcier M, Sofen H, et al; PHOENIX 1 Investigators. Ustekinumab improves nail disease in patients with moderate-to-severe psoriasis: results from PHOENIX 1. Br J Dermatol. 2014;170(2):398–407.
104. Gordon KB, Langley RG, Gottlieb AB, et al. A phase III, randomized, controlled trial of the fully human IL-12/23 mAb briakinumab in mod-erate-to-severe psoriasis. J Invest Dermatol. 2012;132(2):304–314.
105. Blauvelt A, Papp KA, Griffiths CE, et al. Efficacy and safety of gusel-kumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: results from the phase III, double-blinded, pla-cebo- and active comparator-controlled VOYAGE 1 trial. J Am Acad Dermatol. 2017;76(3):405–417.
106. Reich K, Papp KA, Blauvelt A, et al. Tildrakizumab versus placebo or etanercept for chronic plaque psoriasis (reSURFACE 1 and reSUR-FACE 2): results from two randomised controlled, phase 3 trials. Lancet. 2017;390(10091):276–288.
107. Krueger JG, Ferris LK, Menter A, et al. Anti-IL-23A mAb BI 655066 for treatment of moderate-to-severe psoriasis: safety, efficacy, phar-macokinetics, and biomarker results of a single-rising-dose, random-ized, double-blind, placebo-controlled trial. J Allergy Clin Immunol. 2015;136(1):116.e–124.e.
108. Lindelof B. Radiotherapy is rarely used in daily clinical care of patients suffering from nail psoriasis. Acta Derm Venereol. 1989;69(1):80–82.
109. Finnerty EF. Successful treatment of psoriasis of the nails. Cutis. 1979;23(1):43–44.
110. Yu RC, King CM. A double-blind study of superficial radiotherapy in psoriatic nail dystrophy. Acta Derm Venereol. 1992;72(2):134–136.
111. Kwang TY, Nee TS, Seng KT. A therapeutic study of nail psoriasis using electron beams. Acta Derm Venereol. 1995;75(1):90.
112. Stern DK, Creasey AA, Quijije J, Lebwohl MG. UV-A and UV- B pen-etration of normal human cadaveric fingernail plate. Arch Dermatol. 2011;147(4):439–441.
113. Marx JL, Scher RK. Response of psoriatic nails to oral photochemo-therapy. Arch Dermatol. 1980;116(9):1023–1024.
114. MacDonald KJ, Hargreaves GK, Ead RD. Longitudinal melanonychia during photochemotherapy. Br J Dermatol. 1986;114(3):395–396.
115. Tawfik AA. Novel treatment of nail psoriasis using the intense pulsed light: a one-year follow-up study. Dermatol Surg. 2014;40(7): 763–768.
116. Oram Y, Karincaoglu Y, Koyuncu E, Kaharaman F. Pulsed dye laser in the treatment of nail psoriasis. Dermatol Surg. 2010;36(3):377–381.
117. Fernández-Guarino M, Harto A, Sánchez-Ronco M, García-Morales I, Jaén P. Pulsed dye laser vs. photodynamic therapy in the treatment of refractory nail psoriasis: a comparative pilot study. J Eur Acad Dermatol Venereol. 2009;23(8):891–895.
118. Treewittayapoom C, Singvahanont P, Chanprapaph K, Haneke E. The effect of different pulse durations in the treatment of nail psoriasis with 595-nm pulsed dye laser: a randomized, double- blind, intrapatient left-to-right study. J Am Acad Dermatol. 2012;66(5):807–812.
119. Goldust M, Raghifar R. Clinical trial study in the treatment of nail pso-riasis with pulsed dye laser. J Cosmet Laser Ther. Epub 2013 Oct 16.
120. Huang YC, Chou CL, Chiang YY. Efficacy of pulsed dye laser plus topical tazarotene versus topical tazarotene alone in psoriatic nail disease: a single-blind, intrapatient left-to-right controlled study. Lasers Surg Med. 2013;45(2):102–107.
121. Al-Mutairi N, Noor T, Al-Haddad A. Single blinded left-to-right com-parison study of excimer laser versus pulsed dye laser for the treatment of nail psoriasis. Dermatol Ther (Heidelb). 2014;4(2):197–205.
122. Arango-Duque LC, Roncero-Riesco M, Usero Bárcena T, Palacios Álvarez I, Fernández López E. Treatment of nail psoriasis with pulse dye laser plus calcipotriol betametasona gel vs. Nd:YAG plus calcipot-riol betamethasone gel: an intrapatient left-to-right controlled study. Actas Dermosifiliogr. 2017;108(2):140–144.
P
soria
sis:
Tar
gets
and
The
rapy
dow
nloa
ded
from
http
s://w
ww
.dov
epre
ss.c
om/ b
y 16
1.62
.252
.40
on 2
6-Ja
n-20
18F
or p
erso
nal u
se o
nly.
Powered by TCPDF (www.tcpdf.org)
1 / 1
Related Documents