Nadia Mujahid, MD Co-Director Geriatric Fracture Program Rhode Island Hospital August 4th, 2016

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Nadia Mujahid, MD Co-Director Geriatric Fracture Program Rhode Island Hospital August 4th, 2016

Grant through the Donald W. Reynolds Foundation to disseminate Geriatric Education among sub specialists
Serve as a Geriatric Consultant with Depuy Synthes

Why is this topic worth discussing? Preoperative evaluation guidelines Important consideration on beta blockers and
anticoagulation in the perioperative period Strategies to reduce perioperative risk in
geriatric patients

US: ~ 330,000 hip fractures / year. Expected to increase to 550,000 by 2040. 1-year mortality = 20% to 24% Many patients will lose their independence after
hip fracture. The cost of caring for hip fractures was reported
to be $17 billion in 1997, and it is estimated to grow to $62 billion by 2040.
US Department of Health and Human Services. The 2004Surgeon General’s report on bone health and osteoporosis. http://www.surgeongeneral.gov/library/bonehealth/docs/Osteo Agency for Healthcare Research and Quality. 2005 HCUP Nationwide Inpatient Sample (NIS) Comparison Report.
Rockville, MD:US Department of Health and Human Services; 2008. Youm T, Koval KJ, Zuckerman JD. The economic impact of geriatric hip fractures. Am J Orthop. 1999;28(7):423-428.

Cooper. Am J Med. 1997; 103(2A):12s-19s
40%
Unable to walk independently
30%
Permanent disability
20%
Death within one year
80%
Unable to carry out at least one activity of daily living
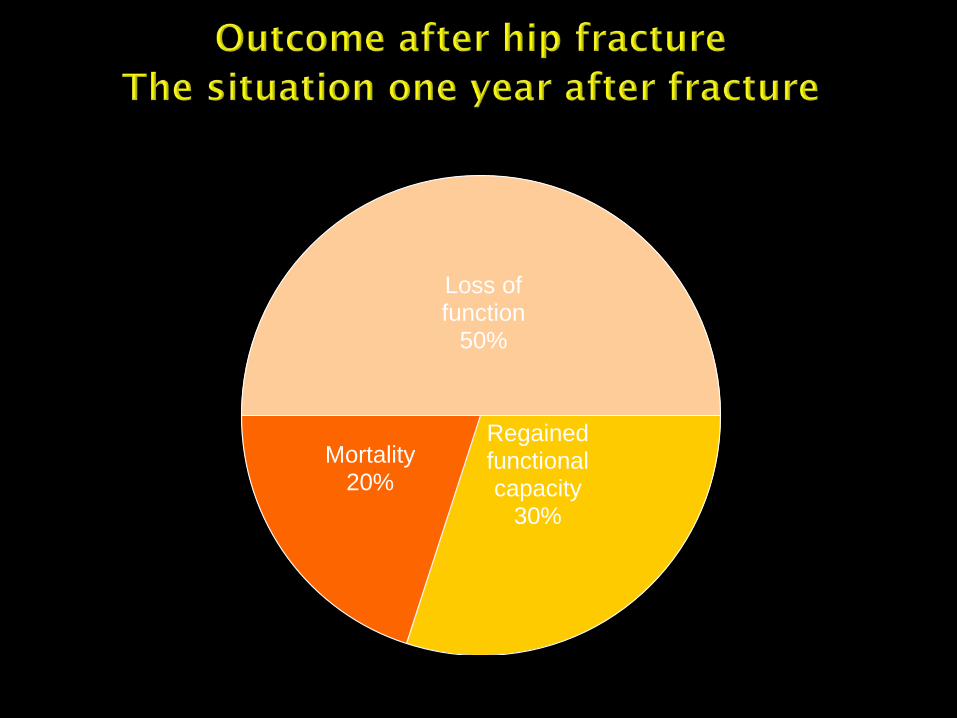
Loss of function
50%
Regained functional capacity
30%
Mortality 20%

Most patients benefit from surgical stabilization of their fractures
The sooner patients have surgery, the less time they have to develop iatrogenic illness
Goal is to have surgery ideally within 24 hours - less decubitii ( 1)
- reduce major medical complications ( 2) - decreased preoperative pain ( 3)
- decreased average LOS by 2 days ( 3)
- earlier ambulation - reduced delirium (4) a. Grimes JP, Am J Med. 2002; 112:702-9 b. Hoenig H, Arch Int Med. 1997; 157:513-20.. c. Orosz GM, JAMA. 2004;291: 1738-43 d. Parker MJ, J Bone Joint 5urg [Br]. 1992:74:203-5.

93 yr old female admitted s/p trip and fall accident at home around 2pm yesterday. She was seen at a local hospital and transported to RIH for a right peri-prosthetic femur fracture.
Available labs: Hb: 9.8mgdl, Cr: 0.98mg/dl EKG: NSR, rate of 85 bpm No prior labs/EKG in lifechart, pt is a resident
of Fall River, MA Per pt she recently had “cardiac surgery” and
had angina 3 weeks ago

You are consulted by the Ortho trauma team to evaluate the patient for a possible second case this morning.

Best done by the Revised Goldman Cardiac
Risk Index (RCRI) Most studied and Validated Predictive value for cardiac complications and
mortality significant in All types of non-cardiac surgery except AAA
Does Not Capture all-cause Mortality

1 point for each risk factor 1. High risk surgery (peritoneal, thoracic, supra
inguinal, vascular) 2. Hx of CAD 3. Hx of CHF 4. Hx of CVA 5. Hx of DM insulin dependent 6. Pre op Cr >2.0mg/dl Lee et all, circulation 1999; Auerbach circulation 2006

Risk Factors Rate 95% CI
No Risk Factors 0.4% 0.1 – 0.8%
One Risk Factor 1.0% 0.5 – 1.4%
Two Risk Factors 2.4% 1.3 – 3.5%
Three Risk Factors 5.4% 2.8 – 7.9%
Devereaux, PJ, Goldman, L, Cook, DJ, et al. CMAJ 2005; 173:627

Risk Factors Rate Rate with Beta Blockers
None 0.4 – 1.0% < 1%
One to Two 2.2 – 6.6% 0.8 – 1.6%
Three or More > 9% > 3%
Auerbach, A, Goldman, L. Circulation 2006; 113:1361
# of risk factors determine the risk of major cardiac complication.
A major cardiac complication is described as cardiac death and nonfatal MI, cardiac arrest or ventricular fibrillation, pulmonary edema and or complete heart block.
Risk reduces with the use of BB

DELAY SURGERY
Unstable Coronary
syndrome Decompensated heart
failure Significant arrhythmia Severe valvular heart
disease Sepsis
NO NEED TO DELAY SURGERY
Stable CAD Ch. Compensated left
ventricular failure Ch. Kidney disease UTI without sepsis Delirium

Pre operative cardiac testing (echo, stress testing) is unlikely to improve outcomes or change management for almost all geriatric fracture patients
Preoperative subspecialty consultation (e.g. cardiology) is rarely needed
Timely surgery and avoidance should be the primary goals

Relevant class 1 recommendation Emergent surgery should proceed to OR; focus
on risk reduction, perioperative surveillance and treatment
Active cardiac conditions should be treated and surgery still considered when stable
-ACS, decompensated heart failure, severe valvular disease and arrhythmias

Relevant class IIb guidelines: Noninvasive testing might be considered “if it will
change management” in patients with poor functional capacity (<4 METs) and multiple risk factors undergoing intermediate risk surgery
Remember: Many frail geriatric fracture patients fall in this
category Echocardiography and or stress testing or
angiography is very unlikely to change management. This will only delay surgery and pt recovery.

Continue if on BB at home Start if pt is high risk (3 or more risk factors) No need to start if pt is low risk (<2 risk
factors) as they may cause more harm then benefit
Use with holding parameters.
AHA guidelines revised (2009)

Perioperative beta blockers reduced cardiovascular events but caused more strokes and higher mortality (POISE trail -2008)
Very high doses of BB were started in the pts, not titrated up, stopped only if systolic BP <100 mm HG or HR <50 bpm
Less aggressive, titrated beta blockade may
help reduce MI (DECREASE trial -2009) Bisoprolol 2.5 mgs started 30 days prior to surgery Non fatal MI decreased in BB group No difference in strokes and overall mortality


Aggressive intravascular volume restoration Avoid medications that promote hypotension Pain control Rapid identification of any acute medical
problems that may require pre operative treatment

Intra operative hypotension is common -anesthesia, blood loss, poor cardiovascular
reserve Intra operative hypotension is dangerous for
elderly patients -Can result in stroke, MI, AKI

-Keep preoperative Hb >10mg/dl {>8.5mg/dl} -IV hydration with isotonic fluids (saline, ringer
lactate) -Fractures bleed a lot so assess vascular status -Too much is better than too little

Avoid most medications that promote hypotension Routinely stop all blood pressure meds like ACE-
I/ ARBS and diuretics Stop oral hypoglycemic agents, use ISS If pt on insulin, reduce dose to 1/3rd to prevent
hypoglycemia* Stop clopidogrel/warfarin Continue BP meds that are important for heart rate
control like BB and CCB. Continue aspirin

Pre operative pain control is essential Pain causes tremendous adrenergic stress on
elderly patients and can promote arrhythmias, delirium and drain energy reserves
Strategies for optimization: IV acetaminophen (three doses can be ordered) IV opiates (morphine 2-4 mgs IV or
hydromorphone 0.5 mg IV)

68 yr old male admitted directly from the airport after a trip and fall accident on a road in St. Martin where he was vacationing.
Past Hx: DCM, AFIB now s/p cardio version, severe MR s/p St. Jude valve replacement, HTN, HLD, PTSD, GERD, neuropathy.
PAST SURGICAL HX: MVR in 1995, Biventricular ICD placement 2012

Labs on admission: 128 Na, 1.33 Cr, 19 BUN, 11.3/34.2 Hb/HCT, 3.4 INR
EKG: atrial sensed- ventricular paced rhythm You are consulted by Ortho to “clear” the
patient for surgery …


Warfarin is a vitamin K antagonist with a long
half life Common uses: -Cardiac: arrhythmias, valvular heart disease,
thrombus, MI -Cerebrovascular: stroke/ TIA -Thromboembolic disease: DVT/P.E

Goal for surgery: INR <1.5 {1.8} Treatment options: - Vitamin K: oral/IV/Sub Q - Fresh Frozen Plasma: IV - Waiting

Route of administration: % reaching target in 24 hrs:
placebo 20%
Sub Q 31%
IV 77%
PO 82%
Dezze KJ et al: Arch Internal Medicine 2006 166;391

10-15 ml/Kg 1 unit= 190 – 240 ml Lasts only for 6 hours
E.G.; a 70 Kg person needs between 700-1050
ml of FFPs which comes to about 4 units of FFP Use in pts who have active thromboembolism
in which INR reversal is contraindicated

Is not an option

Restart 12- 24 hrs after surgery INR goal (ACCP): 2-3 Takes 3-4 days to reach target levels Bridge based on individual cases

Typical goal INR is between 2.5 and 3.5 High risk of thrombosis with Mitral heart
valves Typically bridge with heparin drip
Preferred over therapeutic LVX Hold drip usually 4-6 hours pre-operatively Recommended to restart heparin drip after
hemostasis achieved (12 – 24 hrs) Can consult cardiology if have additional
questions

68 yr old male admitted directly from the airport after a trip and fall accident on a road in St. Martin where he was vacationing.
Past Hx: DCM, AFIB now s/p cardio version, severe MR s/p St. Jude valve replacement, HTN, HLD, PTSD, GERD, neuropathy.
PAST SURGICAL HX: MVR in 1995, Biventricular ICD placement 2012

Labs on admission: 128 Na, 1.33 Cr, 19 BUN, 11.3/34.2 Hb/HCT, 3.4 INR
EKG: atrial sensed- ventricular paced rhythm You are consulted by Ortho to “clear” the
patient for surgery …

For anticoagulation ? Reversal of AC in this patient

Pt received Vitamin K 10 mg PO x 1. Repeat INR in 8 hours was 3.4 Pt received another dose of Vitamin K 10 mg Repeat INR was 2.2 Started on IV heparin and taken for surgery the
next day with FFPs to help control intra operative bleeding


-Antiplatelet, irreversibly binds to ADP receptors inhibiting platelet activation and aggregation
-No treatment options (no reversal) -Shall we delay surgery? -For how long?
Prasugrel/Effient: -Shall we delay surgery? -For how long?

The ACCP 2012 guidelines, state that LMWH, Coumadin, Fundoparinox, UFH, and Aspirin may be used for VTE prophylaxis.
LMWH is preferred (lovenox) Cr Cl <30 ml/min: Lovenox 30 mg sc daily (instead
of standard dosing (30mg BID) If ASA is used, it should be dosed 325mg twice daily
versus once daily Indications for ASA are contraindications to LVX
and heparin Not just meds: prompt surgery, early weight
bearing, avoiding restraints, delirium prevention and treating pain

Statins reduce perioperative adverse cardiovascular events. NNT 131, 2
Do not stop them abruptly as it increases risk of cardiovascular events 3, 4
i. Schouten (2009) N Engl J Med 361(10) 980-89 ii. Poldermans (2003) Circulation 107:1848-51 iii. Le Manach (2007) Anesth Analg 104(6): 1326-33 iv. Schouten (2007) Am J Cardiol 100(2): 316-20

6.8% across all non cardiac surgeries 14-15% in pts > 65 yrs of age Most common risk factors: Age > 60 yrs, frail pts with + weight loss COPD, OSA, current smokers, ASA class II Functional dependence etc Prevention: Aggressive Intensive Spirometry in
pre & post operative period, OOB status, deep breathing exercises, adequate pain control

Adequate preoperative hydration is essential Rate control and thoughtful beta blockade Review and adjust pre op meds Avoid perioperative hypotension Tolerate a risk for pulmonary edema, more
manageable than hypotension and its consequences
Tolerate preoperative hypertension Avoid over testing and over consultation

ER calls you at 11 pm for evaluation of a 93 yr old female s/p fall at home. She is transferred from an OSH for Rt periprosthetic femur fracture.
Available labs: Hb: 9.8/, Cr: 0.98mg/dl EKG: NSR, rate of 85 bpm AVSS No prior labs/EKG for comparison in lifespan
as pt is from Fall River, MA Per pt she had “cardiac surgery” a few months
ago

You are the on call Ortho resident and have to admit this patient
Which medications from her home meds will you continue?

Atenolol 12.5 mg po bid Furosemide 40 mg po bid Simvastatin 20 mg po qhs Aspirin 81 mgs po daily Plavix 75 mg po daily Quetiaprine 75 mg po qhs


Related Documents











