NEUROMUSCULAR JUNCTION AND INFECTIOUS DISORDERS Dayna Ryan, PT, DPT Winter 2012

N EUROMUSCULAR J UNCTION AND I NFECTIOUS D ISORDERS Dayna Ryan, PT, DPT Winter 2012.
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

NEUROMUSCULAR JUNCTION AND INFECTIOUS DISORDERS
Dayna Ryan, PT, DPT
Winter 2012

NEUROMUSCULAR JUNCTION DISEASES
• Botulism• Myasthenia Gravis• Lambert-Eaton Syndrome

Latin: “botulus,” meaning sausage
• Etiology- Neurotoxin produced by Clostridium Botulinum- Anaerobic, Gram-positive rods- Found in improperly preserved or canned foods
& contaminated wounds
• Classification (mode of acquisition)- Food-borne (ingested)- Wound- Unclassified
BOTULISM

• Lesion- Pre-synatic terminals
• Mechanism1.Botulinum toxin enters presynaptic terminals2.Blocks the fusion of ACh vesicles with
presynaptic membrane 3.Inhibit ACh release into neuromuscular junction4.Nerve impulse fails to transmit across the
neuromuscular junction5.Muscle paralysis
• Progression- Typically get full recovery in both adult & infant

MECHANISM OF ACTION OF BOTULINUM TOXIN

INCIDENCE
10 adult & 100 infant cases in US each year
Infant botulismAge 3 wk - 9 month
Signs and symptomsDevelop within 12-36 hours following ingestion of contaminated
food
Mortality rate from 1990 – 1996 in US Type A (6.7%), type E (6.5%), type B (0%)
Gradual recovery over weeks - 12 months

SIGNS & SYMPTOMS Develops within 12-36 hours following
ingestion of contaminated foodFlaccid symmetrical paralysisBlurred & double vision, photophobiaDry mouth, nausea, & vomitingDifficulty in swallowing & speechRespiratory failure can occur in 6-8
hours

TREATMENT
ABE serum antitoxin (antibodies of type A, B, E toxin)
Debridement & antibiotics for wound Removal of toxin from GI (gastric
lavage)Supportive measures, e.g. IV,
mechanical vent

MYASTHENIA GRAVIS
• Fluctuating weakness & fatigability
• Autoimmune disorder– Abnormal Thymus function in 75% of
cases
• Classifications of MG– Ocular myasthenia (~10-15%) – Generalized weakness (~85%)– Myasthenic crisis: respiratory failure

MECHANISM OF MG
ACh receptors # reduced; Decreased efficiency of neuromuscular transmission
Nerve impulse fails to pass across the neuromuscular junction to cause muscle contraction
Antibodies block & damage ACh receptors

MYASTHENIA GRAVIS Prevalence: 14/100,000 Ratio of women-to-men= 3:2
Factors that exacerbate MG: hyper- or hypothyroidism, menstrual cycle
Disease Progression:Slowly, progressive weakness (maximal
weakness occurs in first year in 2/3 of all cases)
After 15-20 years, weakness becomes fixed Remissions occur in about 25% of
cases

SIGNS & SYMPTOMS
Generalized weakness: proximal muscles more affected
Fatigability of skeletal musclesprogressive muscular weakness on exertion, followed by recovery of strength after rest
Respiratory impairments

SIGNS & SYMPTOMS
Muscle weakness varies day to day and over long periods of time
Cranial muscles are the first to show weakness
Patients compensate for weak muscles (e.g. use of thumb to close jaw)

Eyelids fatigue with sustained upward gaze

DIAGNOSISTest anti-Ach receptor antibodies
if +, then MG
Tensilon test Repetitive movements or holding a position Compare performance following giving Tensilon
(anticholinesterase) vs. Placebo (saline) If strength/endurance is improved, then MG
EMG Reduced amplitudes over repetitive stimulation

TreatmentAnticholinesterase drugsThymectomy ImmunosuppressantsPlasmaphoresis
Blood is routed to a machine that separates the plasma & cells
Plasma, which contains antibodies, dissolved proteins, glucose, clotting factors, etc., is discarded while cells are returned to the body
Temporarily (4-6 weeks) reducing anti-ACh receptors antibodies
Used to get a patient more stable for surgery or to get them out of crisis
Intravenous immunoglobulin (IVIG)

LAMBERT-EATON SYNDROME
Rare but still the most frequent presynaptic neuromuscular transmission disorders in adults
Etiology~50% of cases associated with cancer,
especially small cell carcinoma of the lungOthers primarily from autoimmune disorders
e.g. RA, thyroid disease, MS

Mechanism
1. Antibodies destroy voltage-gated Ca++ channel
2. Block of Ca++ into presynaptic terminal
3. Reduced release of presynaptic ACh vesicles
4. Reduced probability of reaching depolarization threshold of a muscle fiber

SIGNS & SYMPTOMS– Muscle weakness and fatigue
• At proximal limbs & torso (LE > UE)
• Difficulties climbing stairs, lifting objects
– Early symptoms: aching of thighs and difficulty walking
– Decreased or absent DTRs– Cranial nerves usually spared

Lambert-Eaton Syndrome
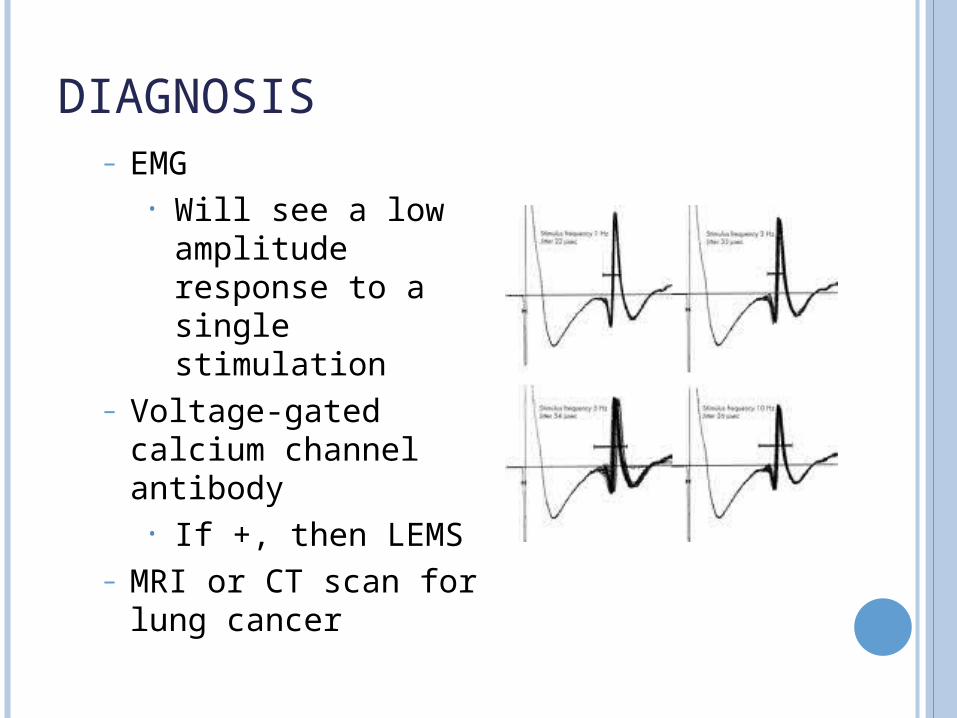
DIAGNOSIS– EMG
• Will see a low amplitude response to a single stimulation
– Voltage-gated calcium channel antibody
• If +, then LEMS– MRI or CT scan for
lung cancer

INFECTIOUS DISORDERS OF THE NS
• Meningitis • Encephalitis • Lyme Disease • West Nile Virus

MENINGITIS
= meninges of the brain and SC become inflamed
All 3 layers can be involved, but usually pia and arachnoid
Etiology: bacterial or viral infection Viral (Aseptic) – most common Tuberculous – enter by inhalation Bacterial – EMERGENCY!!
Incidence: 2-6/1,000,000 adults

MENINGITIS

• SIGNS & SYMPTOMS Fever & chills Severe headache Stiff & painful neck!
(cardinal sign) Mental status changes Sensitivity to light
(photophobia) Confusion Vomiting
Pain in lumbar area and posterior thigh Positive Kernig sign

SIGNS & SYMPTOMS - PROGRESSION Positive Brudzinski
sign as it progresses when neck is flexed,
patient flexes leg to decreased stretch on meninges
Seizures or coma if untreated
Focal neurologic signs, e.g. CN palsies or deafness
Edema, which causes increased ICP and can lead to lethargy and confusion

BACTERIAL MENINGITIS IN A BABY Fever Poor feeding Vomiting Bulging Fontanels
Soft spots Seizures High-pitched cry

• DIAGNOSIS Lumbar puncture: CSF analysis & culture Blood culture CT, MRI: brain abscess or infarction
Bacterial type Isolation for 3 days Bed rest Antibiotics ASAP Meds for seizure Corticosteroids for cerebral edema
or vasculitis Viral type
Meds to control headache and nausea
• Treatment

ENCEPHALITIS Lesion Site: gray matter of the CNS Etiology: viral or bacterial infection
Most often from viral infection In US, Herpes simplex encephalitis most
common; 1/250,000 – 1/500,000

ENCEPHALITIS Most cases: only mild symptoms or
asymptomatic
Serious cases cause: Fever & chills Headache Nausea & vomiting Mental status changes; irritability Lethargy, fatigue Seizures Stiff neck (if meninges are involved) Bulging fontanels (soft spot in skull) in infants Focal neurological signs, e.g. ataxia,
hemiparesis, aphasia

ENCEPHALITIS Prognosis depends on type
Mortality rate varies from <1% to 50-70% Permanent neural damage is more likely in
infants
Diagnose with spinal tap, EEG, CT scan, or MRI

LYME DISEASELyme disease was first reported in the
US in the town of Old Lyme, Connecticut, in 1975.
Most cases (90%) in mid-Atlantic, northeast, & north central regions.
• Lesion Sites:– CNS and PNS
• Incidence on the rise– 23,763 cases in 2002

EtiologyBitten by an
infected tick carrying the bacterium Borrelia burgdorferi
Risk FactorsHaving a petOutdoor activities Walking in high
grasses

Signs & Symptoms – Early StageThe initial sign is rash
Bull's-eye appearances (i.e. erythema migrans) at the site of tick bite
Present in ~80% of patientsGradually expands to ~ 12” across
Flu-like symptoms: chills, fever, headache, lethargy, muscle pain
Chronic RA is the most commonly recognized symptom
Some neurologic and psychiatric symptoms

LYME DISEASE

PROGRESSION OF LYME DISEASE
Stage 1Flu-like symptoms and rash (7-14 days after
tick bite) Stage 2
Generalized fatigue, loss of appetite, vomiting
Neurologic or cardiac abnormalities develop weeks to months later
Stage 3 (weeks to year later)RA develops in >50% of people who did not
receive earlier treatment Affects knees mostly Often unilateral presentation of joint involved

SIGNS & SYMPTOMS – LATER STAGES
Swollen knee from chronic rheumatoid arthritis is most commonly recognized symptom

TREATMENT OF LYME DISEASE
Oral antibiotics Removal of tick Joint surgeries
**15% of those who received early treatments still get complications involving heart, joints, and nervous system
MOST people have complete recovery within weeks or months of antibiotic treatment

PREVENTION IS KEY
Wear long pants Walk on cleared paths Wear high socks and appropriate shoes Wear light-colored clothing to make ticks
easier to see

WEST NILE VIRUSIt was first discovered in the United States in the summer of 1999 in New York. Since then, the virus has spread throughout the United States
• Lesion: CNS, PNS, Multi-systems
(depends on where bitten)

WEST NILE VIRUS
2009 West Nile Virus Activity in US(Reported to CDC as of December 2009)

WEST NILE VIRUS Etiology:
Single-stranded RNA virus from mosquitos primarily
Flavivirus No treatment available – only supportive care Risk factors: age, hypertension, diabetes,
CAD, immunosuppression

SIGNS & SYMPTOMS ~80% of individuals are asymptomatic
~20% of individuals affected by the virus develop systemic symptoms< 1% develop neurological manifestations
Those that do develop nervous system involvement usually evolve a severe illnessMortality rates 12%-14%

PRESENTING SIGNS AND SYMPTOMS Fever Headache Muscle Ache Joint Pain Fatigue Rash (with
swollen lymph nodes)
Nausea/vomiting Periocular pain
Muscle weakness Altered mental
status Backache Photophobia GI/Respiratory
Symptoms

NEUROLOGIC SIGNS & SYMPTOMS Encephalitis Meningitis Meningoencephalitis Anterior myelitis
Acute flaccid paralysis Proximal muscles
affected more than distal
From damage to anterior horn cells
Painless, asymmetric weakness
No sensory abnormalities

SERIOUS SIGNS & SYMPTOMS
High fever Severe headache Stiff neck Disorientation Coma Tremors Convulsions Muscle weakness Ataxia and
extrapyramidal signs
CN abnormalities Optic neuritis/vision
loss Polyradiculitis Seizures Myelitis Photophobia Numbness Paralysis
Related Documents











