Volume 134 No. 2 Pp. 139–358 A NESTHESIOLOGY FEBRUARY 2021 Downloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Volume 134
No. 2 Pp. 139–358
An
esthesio
log
yFebruary 2021
ALNV134N2_Cover.indb 2ALNV134N2_Cover.indb 2 29-Dec-20 21:26:3829-Dec-20 21:26:38
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Liposomal Bupivacaine Is Not Superior to
Standard Local Anesthetics
February2021
Volume 134 Number 2anesthesiology.org The Journal of the American Society of Anesthesiologists, Inc.
ALNV134N2_Cover.indb 3ALNV134N2_Cover.indb 3 29-Dec-20 21:26:3829-Dec-20 21:26:38
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

CAUTION: Federal (United States) law restricts this device to sale by or on the order of a physician. See instructions for use for full prescribing information, including indications, contraindications, warnings, precautions, and adverse events.
Edwards, Edwards Lifesciences, the stylized E logo, Acumen, Acumen IQ, ClearSight, ForeSight, ForeSight Elite, HemoSphere, HPI, Hypotension Prediction Index, and Swan-Ganz are trademarks of Edwards Lifesciences Corporation or its affiliates. All other trademarks are the property of their respective owners.
© 2020 Edwards Lifesciences Corporation. All rights reserved. PP--US-5676 v1.0
Edwards Lifesciences • One Edwards Way, Irvine CA 92614 USA • edwards.com
The monitoring platform of the futureSmart. Innovation.
HemoSphere advanced monitoring platform enables proactive, individualized patient management.Full-range compatibility with noninvasive, minimally-invasive and invasive solutions
Learn more at Edwards.com/HemoSphere
Acumen Hypotension Prediction Index software and Acumen IQ sensor
ForeSight Elite tissue oximetry sensor
ClearSight finger cuff Swan-Ganz pulmonary artery catheter
ALNV134N2_Cover.indb 2ALNV134N2_Cover.indb 2 29-Dec-20 21:26:4129-Dec-20 21:26:41
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

21-102
Develop your leadership talents with expert support
Some leadership comes naturally, but true leaders recognize the need to hone those skills. Knowing how to motivate teams, infl uence the public and build successful practices is more science than art. Yet few of us learn how to lead in medical school.
That’s why ASA has created Lead the Leader: Leadership Development Suite.
Developed in partnership with American College of Healthcare Executives and the Kello School of Management at Northwestern University, this targeted program is designed to help high-performing clinicians become more effective leaders—on your time and your terms.
Your goals, your program.Choose how, when and what you want to learn. Watch videos, listen to podcasts, read articles and connect with the online community over the topics you fi nd most relevant.
Discover your leadership pathasahq.org/leadership
Achieve your full potential within the specialty
02_2021 LeadtheLeader Ad.indd 102_2021 LeadtheLeader Ad.indd 1 12/18/20 10:08 AM12/18/20 10:08 AMALNV134N2_Cover.indb 3ALNV134N2_Cover.indb 3 29-Dec-20 21:26:4129-Dec-20 21:26:41
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
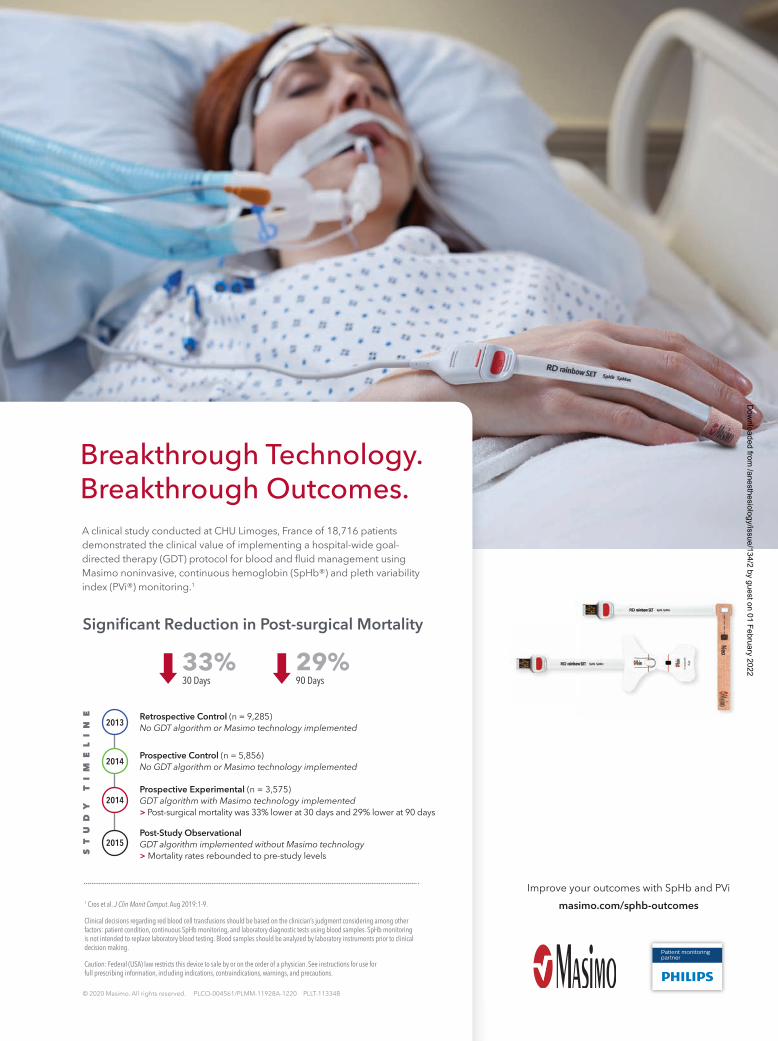
Breakthrough Technology. Breakthrough Outcomes.A clinical study conducted at CHU Limoges, France of 18,716 patients demonstrated the clinical value of implementing a hospital-wide goal-directed therapy (GDT) protocol for blood and fluid management using Masimo noninvasive, continuous hemoglobin (SpHb®) and pleth variability index (PVi®) monitoring.1
1 Cros et al. J Clin Monit Comput. Aug 2019:1-9.
Clinical decisions regarding red blood cell transfusions should be based on the clinician’s judgment considering among other factors: patient condition, continuous SpHb monitoring, and laboratory diagnostic tests using blood samples. SpHb monitoring is not intended to replace laboratory blood testing. Blood samples should be analyzed by laboratory instruments prior to clinical decision making.
Caution: Federal (USA) law restricts this device to sale by or on the order of a physician. See instructions for use for full prescribing information, including indications, contraindications, warnings, and precautions.
Improve your outcomes with SpHb and PVimasimo.com/sphb-outcomes
© 2020 Masimo. All rights reserved. PLCO-004561/PLMM-11928A-1220 PLLT-11334B
Retrospective Control (n = 9,285) No GDT algorithm or Masimo technology implemented
Prospective Control (n = 5,856) No GDT algorithm or Masimo technology implemented
Prospective Experimental (n = 3,575) GDT algorithm with Masimo technology implemented> Post-surgical mortality was 33% lower at 30 days and 29% lower at 90 days
Post-Study Observational GDT algorithm implemented without Masimo technology > Mortality rates rebounded to pre-study levels
2013
2014
2014
2015
ST
UD
Y
TI
ME
LI
NE
Significant Reduction in Post-surgical Mortality
33%30 Days
29%90 Days
Patient monitoring partner
PLMM-11928A Ad, SpHb + PVi, Limoges Study Outcomes, 8.125 x 10.875, Jan 2021, Global.indd 1PLMM-11928A Ad, SpHb + PVi, Limoges Study Outcomes, 8.125 x 10.875, Jan 2021, Global.indd 1 12/9/20 9:23 AM12/9/20 9:23 AMALNV134N2_Cover.indb 4ALNV134N2_Cover.indb 4 29-Dec-20 21:26:4229-Dec-20 21:26:42
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

147 Perineural Liposomal Bupivacaine Is Not Superior to Nonliposomal Bupivacaine for Peripheral Nerve Block Analgesia: A Systematic Review and Meta-analysis
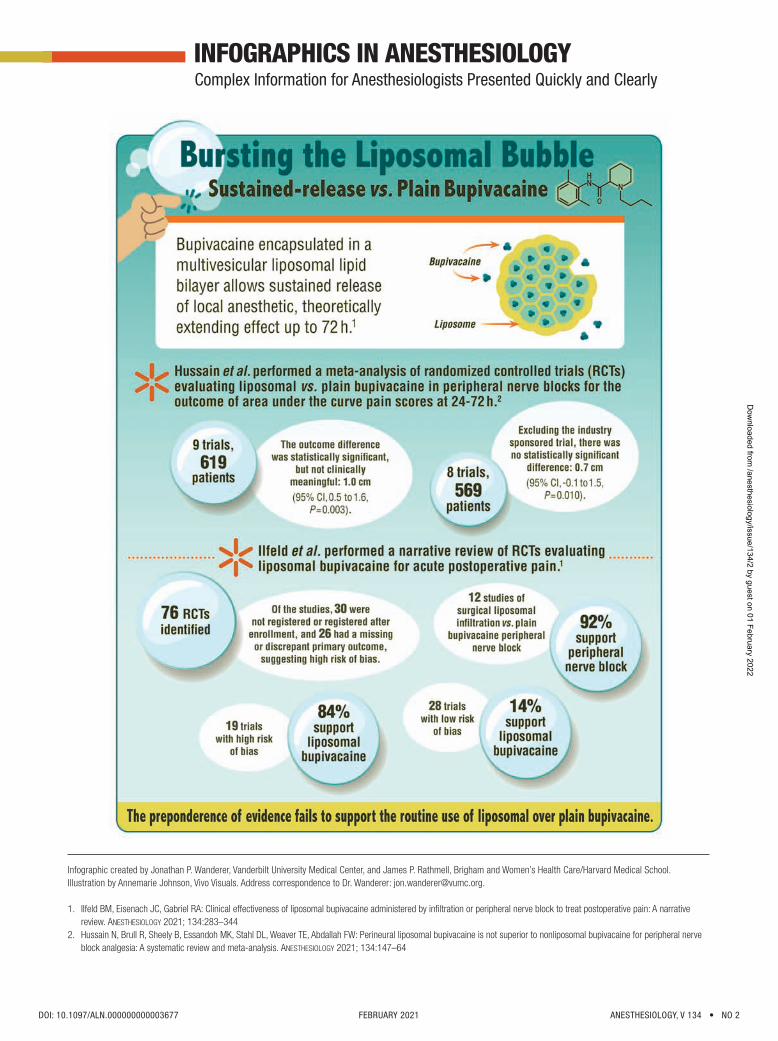
The effectiveness of perineural liposomal bupivacaine in improving peripheral nerve block analgesia across various surgical proce-dures compared to that of nonliposomal local anesthetics was evaluated in this systematic review and meta-analysis of nine ran-domized controlled trials involving 619 patients. The primary outcome was the difference in weighted mean area under the curve of the pooled 24- to 72-h rest pain scores, evaluated on a 0- to 10-cm scale, between patients receiving perineural analgesia including liposomal bupivacaine and those receiving nonliposomal local anesthetics. Across 24 to 72 h, the mean difference (95%
CI) in area under the curve of rest pain was found to be 1.0 (0.5 to 1.6) cm · h in favor of liposomal bupivacaine but this difference failed to meet the threshold for clinical significance (2.0 cm · h). Excluding an industry-sponsored trial rendered the difference between the groups nonsignificant (0.7 [–0.1 to 1.5] cm · h). See the accompanying Editorial on page 139. (Summary: M. J. Avram. Image: A. Johnson, Vivo Visuals.)
165 Exposure–Response Relationship of Tranexamic Acid in Cardiac Surgery: A Model-based Meta-analysis
Tranexamic acid is an antifibrinolytic agent that reduces postoperative blood loss and rates of erythrocyte transfusion and reoper-ation in cardiopulmonary bypass surgery. There also appears to be a dose-response relationship between tranexamic acid and the risk of postoperative seizure. The present study quantified the effect of tranexamic acid exposure on postoperative bleeding events and seizure using model-based meta-analysis, an extension of traditional meta-analysis that includes parametric models to describe the effect of dose. A total of 82 clinical trials (49,817 patients) were selected, including 64 randomized controlled trials (12,378 patients) for the effectiveness analysis and 18 observational studies (37,439 patients) for the analysis of seizure. This analysis found
that low-dose tranexamic acid (total dose approximately 20 mg/kg) was sufficient to reduce postoperative blood loss and erythrocyte transfusion in cardiopulmonary bypass surgery. Although higher tranexamic acid doses were found to achieve a marginal gain in effectiveness, they increased the risk of postoperative seizure, particularly in procedures involving a high risk of bleeding. See the accompanying Editorial on page 143. (Summary: M. J. Avram. Image: J. P. Rathmell.)
189 Intraoperative Oxygen Concentration and Neurocognition after Cardiac Surgery: A Randomized Clinical Trial
Excessive oxygen use leading to hyperoxia may be injurious, especially in the context of ischemia-reperfusion injury. Although cardiac surgery with cardiopulmonary bypass is associated with exposure to ischemia-reperfusion, patients undergoing such surgery are often treated with higher oxygen concentrations to protect against myocardial and cerebral hypoxia. The hypothesis that titration of intraoperative oxygenation to achieve normoxia reduces postoperative cognitive dysfunction on the second postoperative day com-pared to standard practice hyperoxia was tested in a randomized doubled blind trial of 100 patients 65 yr or older having coronary artery bypass graft surgery requiring cardiopulmonary bypass. Normoxic patients received a minimum fraction of inspired oxygen
of 0.35 to maintain an arterial partial pressure of oxygen above 70 mmHg before and after cardiopulmonary bypass and between 100 and 150 mmHg during it. Hyperoxic patients received a fraction of inspired oxygen of 1.0 throughout surgery. The median (interquartile range) Telephonic Montreal Cognitive Assessment score of the hyperoxia and normoxia groups on postoperative day 2 were not different (18 [16 to 20] vs. 18 [14 to 20]). (Summary: M. J. Avram. Image: J. P. Rathmell.)
179 Intraoperative Blood Pressure Monitoring in Obese Patients: Arterial Catheter, Finger Cuff, and Oscillometry
Perioperative blood pressure monitoring in obese patients can be a challenge because of the limitations of both continuous intraarterial and intermittent noninvasive oscillometric blood pressure monitoring in these patients. The hypothesis that the agree-ment between continuous noninvasive finger cuff blood pressure measurements and continuous intraarterial measurements is better than that between oscillometric blood pressure measurements at the upper arm, forearm, and lower leg and intraarterial measurements was tested in a prospective method comparison study in 90 patients with a body mass index of 40 kg/m2 or more having bariatric surgery. The absolute and trending agreement of finger cuff blood pressure measurements with intraarterial blood
pressure measurements were only moderate but for mean arterial pressure and diastolic blood pressure they were better than between oscillometric (at each of the three measurement sites) and intraarterial blood pressure measurements. The absolute and trending agreement of forearm oscillometric measurements with intraarterial blood pressure measurements was better than the agreement of upper arm oscillometric measurements with intraarterial blood pressure measure-ments. (Summary: M. J. Avram. Image: A. Johnson, Vivo Visuals.)
TMA
THIS MONTH IN
DOI: 10.1097/ALN.0000000000003672 FEBRUARY 2021 ANESTHESIOLOGY, V 134 • NO 2
ALNV134N2_Text.indb 4ALNV134N2_Text.indb 4 29-Dec-20 19:42:5729-Dec-20 19:42:57
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

202 An Electroencephalogram Metric of Temporal Complexity Tracks Psychometric Impairment Caused by Low-dose Nitrous Oxide
Nitrous oxide, an N-methyl-d-aspartate receptor antagonist, has analgesic and hypnotic properties as well as strong dissociative effects. It can be used to understand mechanisms of progressive cognitive impairment by non-γ-aminobutyric acid (GABA) drug sedation. The temporal complexity of the electroencephalogram (EEG), the evolution in time of EEG motifs, indicates the dynamics of cortical transitions between metastable states and has been shown to correlate with cognitive task performance. The hypothesis that nitrous oxide would reduce temporal complexity was tested in a multidose, single-blind, crossover trial of twelve participants breathing nitrous oxide (end-tidal concentration of 20%, 30%, or 40%, in a random order), while a 32-channel EEG and psychometric function were recorded. At
baseline, regional temporal complexity was greater in the midline than in channels overlying lateral temporal brain regions. Increasing nitrous oxide exposure decreased brain complexity in the midline and prefrontal regions, while it did not change in the lateral temporal region. A quantitative EEG default-mode-network complexity metric based on temporal complexity was sensitive to psychometric impairment caused by low-dose nitrous oxide. (Summary: M. J. Avram. Image: From original article.)
219 Fast-spiking Interneurons Contribute to Propofol-induced Facilitation of Firing Synchrony in Pyramidal Neurons of the Rat Insular Cortex
Propofol primarily potentiates γ-aminobutyric acid–mediated (GABAergic) inhibitory synaptic transmission in the cerebral cortex. The propofol-induced alpha rhythm in an electroencephalogram is correlated with propofol-induced loss of conscious-ness. Fast-spiking GABAergic neurons are the principal inhibitory neurons in the cerebral cortex. The hypothesis that propo-fol-induced facilitation of unitary inhibitory postsynaptic currents results in firing synchrony among postsynaptic pyramidal neurons that receive inhibitory input from the same presynaptic fast-spiking neuron was tested using whole-cell patch-clamp recordings simultaneously from one fast-spiking neuron and two or three pyramidal neurons in rat insular cortical slice prepa-
rations. Propofol facilitated spike synchrony among pyramidal neurons by enhancing inhibitory input from fast-spiking neurons. Bath application of 1 and 10 µM propofol promoted postsynaptic pyramidal neuron firing synchrony when a presynaptic fast-spiking neuron was activated with 100- and 100/150- ms interburst intervals (in the alpha range), respectively. Propofol failed to synchronize pyramidal neuron firing when the presynaptic fast-spiking neuron was activated with 1050-, 250-, or 75-ms interburst intervals. (Summary: M. J. Avram. Image: From original article.)
262 “Silent” Presentation of Hypoxemia and Cardiorespiratory Compensation in COVID-19 (Clinical Focus Review)
A lack of dyspnea in response to hypoxemia (silent hypoxia) is commonly observed. COVID-19 is bringing large numbers of severely hypoxemic patients to medical care and highlighting the phenomenon of silent hypoxia. COVID-19 patients may not present with marked dyspnea because their main gas exchange abnormality involves intrapulmonary shunt and even mild hyperventilation is capable of significantly reducing arterial carbon dioxide and decreasing respiratory drive mediated by both the carotid and central chemoreceptors. Hypoxemia is well tolerated when compensated by cardiovascular responses normally involving increased cardiac output, mediated predominately by tachycardia, with only moderate augmentation of blood pres-
sure. Deterioration in oxygen saturation and cardiovascular compensation can occur rapidly in hypoxemic patients, particularly in patients with profound shunt physiology. Deterioration in oxygenation is caused most often by a combination of factors, including increasing shunt, reduced cardiac output, decreased ventilation, and gas exchange on the steep portion of the oxyhemoglobin dissociation curve. (Summary: M. J. Avram. Image: J. P. Rathmell.)
283 Clinical Effectiveness of Liposomal Bupivacaine Administered by Infiltration or Peripheral Nerve Block to Treat Postoperative Pain: A Narrative Review (Review Article)
Bupivacaine hydrochloride is the longest acting local anesthetic approved by the U.S. Food and Drug Administration. Sustained local anesthetic release that may extend the analgesic duration can be achieved by encasing the local anesthetic within various carriers. Liposomal bupivacaine is a sustained release bupivacaine preparation that has been approved for clinical use by the U.S. Food and Drug Administration. The present article provides a comprehensive summary of the 76 published randomized controlled trials involving the clinical use of liposomal bupivacaine when administered to control acute postsurgical pain. The overwhelming
majority of the randomized controlled trials comparing liposomal bupivacaine with unencapsulated bupivacaine or ropivacaine failed to demonstrate the superiority of liposomal bupivacaine even though the dose of liposomal bupivacaine was almost always maximized, while that of the comparator was rarely optimized. Even when compared to a placebo, infiltration with liposomal bupivacaine provided greater analgesia in only a minority of randomized controlled trials. The review concludes by identifying knowledge gaps for future research. (Summary: M. J. Avram. Image: A. Johnson, Vivo Visuals.)
ANESTHESIOLOGY, V 134 • NO 2 FEBRUARY 2021 DOI: 10.1097/ALN.0000000000003672
ALNV134N2_Text.indb 5ALNV134N2_Text.indb 5 29-Dec-20 19:42:5829-Dec-20 19:42:58
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
TABLE OF CONTENTS Volume 134
Issue 2
February 2021
This Month in A NESTHESIOLOGY ......................................1A
Science, Medicine, and the Anesthesiologist ...........13A
Infographics in Anesthesiology ................................17A
Editorials Liposomal Bupivacaine : Effective, Cost-effective, or (Just) Costly?
M. E. McCann ...............................................................................139
Optimal Tranexamic Acid Dosing Regimen in Cardiac Surgery: What Are the Missing Pieces?
D. Faraoni , J. H. Levy .....................................................................143
Perioperative Medicine
CLINICAL SCIENCE
Perineural Liposomal Bupivacaine Is Not Superior to Nonliposomal Bupivacaine for Peripheral Nerve Block Analgesia : A Systematic Review and Meta-analysis
N. Hussain , R. Brull , B. Sheehy , M. K. Essandoh , D. L. Stahl , T. E. Weaver , F. W. Abdallah ............................................................147
Nine trials were included in a meta-analysis examining the difference in 24- to 72-h rest pain severity scores for liposomal and nonliposomal bupivacaine. The area under the curve pain scores for the 24- to 72-h period were statistically but probably not clinically significant. Secondary outcome analysis likewise failed to uncover benefits for liposomal bupivacaine regarding analgesic consumption, length of stay, and functional recovery.
Exposure – Response Relationship of Tranexamic Acid in Cardiac Surgery : A Model-based Meta-analysis
P. J. Zufferey , J. Lanoisel é e , B. Graouch , B. Vieille , X. Delavenne , E. Ollier ...................................................................165
This model-based meta-analysis found that low-dose tranexamic acid (total dose, approximately 20 mg/kg) was sufficient to reduce postoperative blood loss and erythrocyte transfusion in cardiopulmonary bypass surgery. Although higher tranexamic acid doses were found to achieve a marginal gain in effectiveness, they increased the risk of postoperative seizure, particularly in procedures involving a high risk of bleeding.
Intraoperative Blood Pressure Monitoring in Obese Patients : Arterial Catheter, Finger Cuff, and Oscillometry
R. Schumann , A. S. Meidert , I. Bonney , C. Koutentis , W. Wesselink , K. Kouz , B. Saugel .........................................................................179
In a study of 90 obese patients having bariatric surgery, the agreement between finger cuff and intraarterial measurements was better than the agreement between oscillometric and intraarterial measurements for mean arterial and diastolic blood pressure, but not systolic blood pressure. Forearm oscillometry demonstrated better measurement performance than upper arm or lower leg oscillometry.
•
•
ON THE COVER: Liposomal bupivacaine is purported to extend analgesia associated with wound in ltration and peripheral nerve blocks. However, evidence of the clinical e ectiveness of liposomal bupivacaine is mixed. In this issue of Anesthesiology, Hussain et al. present a meta-analysis to evaluate the e ectiveness of perineural liposomal bupivacaine in improving peripheral nerve block analgesia as compared to nonliposomal local anesthetics. In the same issue, Ilfeld et al. provide a comprehensive summary of all currently published randomized controlled trials involving the clinical administration of liposomal bupivacaine to control postoperative pain. In an accompanying editorial, McCann reviews the history of clinical trial data and approval of liposomal bupivacaine by the U. S. Food and Drug Administration. Cover Illustration: A. Johnson, Vivo Visuals.
• Hussain et al.: Perineural Liposomal Bupivacaine Is Not Superior to Nonliposomal Bupivacaine for Peripheral Nerve Block Analgesia: A Systematic Review and Meta-analysis, p. 147
• Ilfeld et al.: Clinical E ectiveness of Liposomal Bupivacaine Administered by In ltration or Peripheral Nerve Block to Treat Postoperative Pain: A Narrative Review, p. 283
• McCann: Liposomal Bupivacaine: E ective, Cost-e ective, or (Just) Costly? p. 139
Refers to This Month in ANESTHESIOLOGY
Refers to EditorialThis article has an Audio Podcast
See Supplemental Digital ContentCME ArticleThis article has a Video Abstract
Part of the Letheon writing competitionThis article has a Visual AbstractThis article is Open Access
•
Anesthesiology (ISSN 0003-3022) is published monthly by Wolters Kluwer Health, Inc., 14700 Citicorp Drive, Bldg 3, Hagerstown, MD 21742. Periodicals postage paid at Hagerstown, MD, and at additional mailing offi ces.Postmaster: Send address changes to Anesthesiology, P.O. BOX 1610, Hagerstown, MD 21740.
ALNV134N2_Text.indb 3ALNV134N2_Text.indb 3 29-Dec-20 19:42:5929-Dec-20 19:42:59
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

*Urban sites also available*
I feel valued and appreciated as an important member of the team.
The hospital work is varied and interesting and the culture here is second to none!
With world class recreational pursuits at our doorstep, there are endless opportunities to go play outside!
It has been a wonderful place to live, practice, raise my children, and enjoy life.
www.betterhere.caLive where others only vacation
APPLYNOW
ANESTHESIOLOGISTOPPORTUNITIES
Trail, British Columbia, Canada
ALNV134N2_Text.indb 4ALNV134N2_Text.indb 4 29-Dec-20 19:43:0029-Dec-20 19:43:00
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
The Journal of the American Society of Anesthesiologists, Inc. • anesthesiology.org
Intraoperative Oxygen Concentration and Neurocognition after Cardiac Surgery: A Randomized Clinical Trial
S. Shaefi, P. Shankar, A. L. Mueller, B. P. O’Gara, K. Spear, K. R. Khabbaz, A. Bagchi, L. M. Chu, V. Banner-Goodspeed, D. E. Leaf, D. S. Talmor, E. R. Marcantonio, B. Subramaniam ...........189
A total of 100 cardiac surgical patients were randomly assigned to 35 or 100% inspired oxygen before and after cardiopulmonary bypass. Neurocognitive function 2 days, 1 month, 3 months, and 6 months after surgery was similar in each group. Supplemental intraoperative oxygen does not worsen postoperative neurocognitive function. Inspired oxygen fraction should be chosen on the basis of other considerations.
An Electroencephalogram Metric of Temporal Complexity Tracks Psychometric Impairment Caused by Low-dose Nitrous Oxide
X. C. E. Vrijdag, H. van Waart, S. J. Mitchell, J. W. Sleigh .................202
A quantitative electroencephalogram analysis can identify associations between treatment with low-dose nitrous oxide and performance on psychometric tests. Temporal complexity decreases in the medial cortical regions during nitrous oxide administration and is correlated with psychometric performance.
BASIC SCIENCE
Fast-spiking Interneurons Contribute to Propofol-induced Facilitation of Firing Synchrony in Pyramidal Neurons of the Rat Insular Cortex
Y. Koyanagi, Y. Oi, M. Kobayashi .....................................................219
Multiple whole cell patch clamp recordings in rat cortical slices reveal that propofol facilitates firing synchrony among pyramidal neurons. Propofol-induced activation of presynaptic fast-spiking interneurons was necessary to achieve firing synchrony of postsynaptic pyramidal neurons. These observations suggest that propofol facilitates pyramidal neuron firing synchrony in the cerebral cortex by enhancing inhibitory inputs from fast-spiking interneurons.
Molecular Modification of Transient Receptor Potential Canonical 6 Channels Modulates Calcium Dyshomeostasis in a Mouse Model Relevant to Malignant Hyperthermia
J. R. Lopez, A. Uryash, J. Adams, P. M. Hopkins, P. D. Allen ..............234
Muscle-specific overexpression of the nonconducting transient receptor potential canonical 6 channel both reduced intracellular Ca2+ concentration in RYR1-p.R163C mice at rest and reduced the absolute maximum levels of intracellular Ca2+ concentration reached during exposure to halothane. Despite this, its overexpression did not restore intracellular Ca2+ concentration to wild-type levels, and although its overexpression increased the length of survival after halothane exposure, it was unable to rescue the lethal phenotype.
Education
IMAGES IN ANESTHESIOLOGY
Using Left Ventricular Assist Device Doppler Assessment to Understand Pump–Patient Interactions during a Venous Arterial–Extracorporeal Membrane Oxygenation Weaning Trial
S. P. De Ridder, S. Jacobs, D. F. Dauwe...........................................248
CLINICAL FOCUS REVIEW
Perioperative Blood Pressure ManagementB. Saugel, D. I. Sessler ..................................................................250
Intraoperative hypotension is common during noncardiac surgery and associated with myocardial injury, acute kidney injury, and death. Postoperative hypotension is also common and associated with myocardial injury and death, and largely missed by conventional monitoring.
“Silent” Presentation of Hypoxemia and Cardiorespiratory Compensation in COVID-19
P. E. Bickler, J. R. Feiner, M. S. Lipnick, W. McKleroy ........................262
Severe hypoxemia presents variably, and sometimes silently, without subjective complaints of dyspnea. The adequacy of cardiovascular compensation for oxygen delivery to tissues should be a focus in all hypoxemic patients.
Acute Respiratory Distress Syndrome: Contemporary Management and Novel Approaches during COVID-19
G. W. Williams, N. K. Berg, A. Reskallah, X. Yuan, H. K. Eltzschig .......270
Acute respiratory distress syndrome remains a condition that carries a high mortality. Evidence-based clinical management and emerging concepts for new therapies for COVID-19 are reviewed.
REVIEW ARTICLE
Clinical Effectiveness of Liposomal Bupivacaine Administered by Infiltration or Peripheral Nerve Block to Treat Postoperative Pain: A Narrative Review
B. M. Ilfeld, J. C. Eisenach, R. A. Gabriel .........................................283
This review summarizes the evidence from randomized, controlled trials for the use of liposomal bupivacaine in providing postoperative analgesia. The preponderance of evidence fails to support the routine use of liposomal bupivacaine over standard local anesthetics.
MIND TO MIND
Dying AloneK. L. Goff ......................................................................................345
Behind the MaskA. E. Holman, V. T. Gauger ..............................................................346
•
•
•
•
ALNV134N2_Text.indb 5ALNV134N2_Text.indb 5 29-Dec-20 19:43:0029-Dec-20 19:43:00
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
The Journal of the American Society of Anesthesiologists, Inc. • anesthesiology.org
Correspondence Perioperative Management of Glucose-lowering Drugs: Comment
S. H. Gregory ................................................................................349
Perioperative Management of Glucose-lowering Drugs: Comment V. Thiruvenkatarajan , D. Jesudason , N. Nanjappa , E. J. Meyer , R. M. Van Wijk ...............................................................................349
Perioperative Management of Glucose-lowering Drugs: Reply J.-C. Preiser , M. Cnop ...................................................................350
Burst-suppression and Postoperative Delirium: Comment H. P. Grocott ..................................................................................351
Burst-suppression and Postoperative Delirium: Reply J. C. Pedemonte , J. J. Locascio , T. Houle , O. Akeju ..........................352
Balanced Crystalloid versus 0.9% Sodium Chloride: What We Overlook in Our Research
A. Kasatkin , A. Urakov , A. Nigmatullina , M. Kopytov .........................353
A Contemporary Reading List A. J. Schwartz ...............................................................................354
Podcasts from ANESTHESIOLOGY Promoting Medical English Learning in Non – English-speaking Countries
C. Liang , X. Zhang , F. Fang , J. Cang , C. Miao ..................................355
Erratum ....................................................................... 357
Careers & Events ........................................................19A
ANESTHESIOLOGY (ISSN 0003–3022) is published monthly by Wolters Kluwer Health, Inc., 14700 Citicorp Drive, Bldg 3, Hagerstown, MD 21742. Business offi ce: Two Commerce Square, 2001 Market Street, Philadelphia, PA 19103. Periodicals postage paid at Hagerstown, MD, and at additional mailing offi ces. Copyright © 2021, the American Society of Anesthesiologists, Inc. All Rights Reserved.
Annual Subscription Rates: United States—$1077 Individual, $2671 Institution, $434 In-training. Rest of World—$1136 Individual, $2965 Institution, $434 In-training. Single copy rate $266. Subscriptions outside of North America must add $58 for airfreight delivery. Add state sales tax, where applicable. The GST tax of 7% must be added to all orders shipped to Canada (Wolters Kluwer Health, Inc.’s GST Identifi cation # 895524239, Publications Mail Agreement # 1119672). Indicate in-training status and name of institution. Institution rates apply to libraries, hospitals, corporations, and partnerships of three or more individuals. Subscription prices outside the United States must be prepaid. Prices subject to change without notice. Subscriptions will begin with currently available issue unless otherwise requested. Visit us online at www.lww.com.
Individual and in-training subscription rates include print and access to the online version. Online-only subscrip-tions for individuals ($356) and persons in training ($356) are available to nonmembers and may be ordered by downloading a copy of the Online Subscription FAXback Form from the Web site, completing the information requested, and faxing the completed form to 301-223-2400. Institutional rates are for print only; online sub-scriptions are available via Ovid. Institutions can choose to purchase a print and online subscription together for a discounted rate. Institutions that wish to purchase a print subscription, please contact Wolters Kluwer Health, Inc.,
14700 Citicorp Drive, Bldg 3, Hagerstown, MD 21742; phone: 800-638-3030; fax: 301-223-2400. Institutions that wish to purchase an online subscription or online with print, please contact the Ovid Regional Sales Offi ce near you or visit www.ovid.com/site/index.jsp and select Contact and Locations.
Address for non-member subscription information, orders, or change of address: Wolters Kluwer Health, Inc., 14700 Citicorp Drive, Bldg 3, Hagerstown, MD 21742; phone: 800-638-3030; fax: 301-223-2400.
Address for member subscription information, orders, or change of address: Members of the American Society of Anesthesiologists receive the print and online journal with their membership. To become a member or provide a change of address, please contact the American Society of Anesthesiologists, 1061 American Lane, Schaumburg, Illinois 60173-4973; phone: 847-825-5586; fax: 847-825-1692; e-mail: [email protected]. For all other membership inquiries, contact Wolters Kluwer Health, Inc., Customer Service Department, P.O. Box 1610, Hagerstown, MD 21740; phone: 800-638-3030; fax: 301-223-2400.
Postmaster: Send address changes to Anesthesiology, P.O. BOX 1610, Hagerstown, MD 21740.
Advertising: Please contact Hilary Druker, National Account Manager, Health Learning, Research & Practice, Medical Journals, Wolters Kluwer Health, Inc.; phone: 609-304-9187; e-mail: [email protected]. For classifi ed advertising: Dave Wiegand, Recruitment Advertising Representative, Wolters Kluwer Health, Inc.; phone: 847-361-6128; e-mail: [email protected].
INSTRUCTIONS FOR AUTHORS
The most recently updated version of the Instructions for Authors is available at www.anesthesiology.org. Please refer to the Instructions for the preparation of any material for submission to ANESTHESIOLOGY.
Manuscripts submitted for consideration for publication must be submitted in electronic format via Editorial Manager (https://www.editorialmanager.com/aln). Detailed directions for submission and the most recent ver-sion of the Instructions for Authors can be found on the Journal’s Web site (http://www.anesthesiology.org). Books and educational materials for review should be sent to Alan Jay Schwartz, M.D., M.S.Ed., Director of Education, Department of Anesthesiology and Critical Care Medicine, The Children’s Hospital of Philadelphia,
34th Street and Civic Center Blvd., Room 9327, Philadelphia, Pennsylvania 19104-4399. Article-specifi c permission requests are managed with Copyright Clearance Center’s Rightslink service. Information can be accessed directly from articles on the journal Web site. More information is available at http://anesthesi-ology.pubs.asahq.org/public/rightsandpermissions.aspx. For questions about the Rightslink service, e-mail [email protected] or call 877-622-5543 (U.S. only) or 978-777-9929. Advertising and related correspondence should be addressed to Advertising Manager, Anesthesiology, Wolters Kluwer Health, Inc., Two Commerce Square, 2001 Market Street, Philadelphia, Pennsylvania 19103 (Web site: http://www.wkadcenter.com/). Publication of an advertisement in Anesthesiology does not constitute endorsement by the Society or Wolters Kluwer Health, Inc. of the product or service described therein or of any representations made by the advertiser with respect to the product or service.
ALNV134N2_Text.indb 6ALNV134N2_Text.indb 6 29-Dec-20 19:43:0029-Dec-20 19:43:00
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
The Journal of the American Society of Anesthesiologists, Inc. anesthesiology.org
Trusted Evidence: Discovery to Practice
Mission: Promoting scientific discovery and knowledge in perioperative, critical care, and pain medicine to advance patient care.
®
EDITOR-IN-CHIEF
Evan D. Kharasch, M.D., Ph.D. Editor-in-Chief, Anesthesiology
Department of Anesthesiology Duke University Durham, North Carolina Tel: 1-800-260-5631 E-mail: [email protected]
PAST EDITORS-IN-CHIEF
Henry S. Ruth, M.D., 1940–1955Ralph M. Tovell, M.D., 1956–1958James E. Eckenhoff, M.D., 1959–1962Leroy D. Vandam, M.D., 1963–1970Arthur S. Keats, M.D., 1971–1973Nicholas M. Greene, M.D., 1974–1976C. Philip Larson, Jr., M.D., 1977–1979John D. Michenfelder, M.D., 1980–1985Lawrence J. Saidman, M.D., 1986–1996Michael M. Todd, M.D., 1997–2006James C. Eisenach, M.D., 2007–2016
COVER ART
James P. Rathmell, M.D., Boston, MassachusettsAnnemarie B. Johnson, C.M.I. Medical Illustrator, Winston-Salem, North Carolina
CME EDITORS
Leslie C. Jameson, M.D. Dan J. Kopacz, M.D.
EDITORIAL OFFICE
Ryan Walther, Managing Editor E-mail: [email protected] Tedeschi, Digital Communications Director E-mail: [email protected] Workman, Peer Review SupervisorPhilip JacksonCaitlin Washburn Anesthesiology Journal 1061 American Lane Schaumburg, IL 60173-4973 Tel: 1-800-260-5631 E-mail: [email protected]
WOLTERS KLUWER HEALTH PUBLICATION STAFF
Miranda Walker, Senior PublisherSara Cleary, Senior Journal Production Editor/Team LeaderEmily Moore, Journal Production EditorColette Lind, Journal Production AssociateHilary Druker, National Account Manager
For reprint inquiries and purchases, please contact [email protected] in North America, and [email protected] for rest of world.
Anesthesiology is abstracted or indexed in Index Medicus/MEDLINE, Science Citation Index/SciSearch, Current Contents/Clinical Medicine, Current Contents/Life Sciences, Reference Update, EMBASE/Excerpta Medica, Biological Abstracts (BIOSIS), Chemical Abstracts, Hospital Literature Index, and Comprehensive Index to Nursing and Allied Health Literature (CINAHL).
The affiliations, areas of expertise, and conflict-of-interest disclosure statements for each Editor and Associate Editor can be found on the Journal’s Web site (www.anesthesiology.org).
All articles accepted for publication are done so with the understanding that they are contributed exclusively to this Journal and become the property of the American Society of Anesthesiologists, Inc. Statements or opinions expressed in the Journal reflect the views of the author(s) and do not represent official policy of the American Society of Anesthesiologists unless so stated.
ASA OFFICERS
Beverly K. Philip, M.D., PresidentRandall Clark, M.D., President-ElectMary Dale Peterson, M.D., Immediate Past PresidentMichael Champeau, M.D., First Vice-President
ALNV134N2_Text.indb 8ALNV134N2_Text.indb 8 29-Dec-20 19:43:0029-Dec-20 19:43:00
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
The Journal of the American Society of Anesthesiologists, Inc. anesthesiology.org
Trusted Evidence: Discovery to Practice
Mission: Promoting scientific discovery and knowledge in perioperative, critical care, and pain medicine to advance patient care.
®
EDITOR-IN-CHIEF
Evan D. Kharasch, M.D., Ph.D., Durham, North Carolina
ASSISTANT EDITOR-IN-CHIEF
Michael J. Avram, Ph.D., Chicago, Illinois
EXECUTIVE EDITORS
Deborah J. Culley, M.D., Boston, MassachusettsAndrew Davidson, M.B.B.S., M.D., F.A.N.Z.C.A., Victoria, AustraliaJerrold H. Levy, M.D., F.A.H.A., F.C.C.M., Durham, North CarolinaJames P. Rathmell, M.D., Boston, Massachusetts
EDITORS
Brian Thomas Bateman, M.D., Boston, MassachusettsJ. David Clark, M.D., Ph.D., Palo Alto, CaliforniaAmanda A. Fox, M.D., M.P.H., Dallas, TexasYandong Jiang, M.D., Ph.D., Houston, TexasSachin Kheterpal, M.D., M.B.A., Ann Arbor, MichiganMartin J. London, M.D., San Francisco, CaliforniaJamie W. Sleigh, M.D., Hamilton, New ZealandLaszlo Vutskits, M.D., Geneva, Switzerland
STATISTICAL EDITOR
Timothy T. Houle, Ph.D., Boston, Massachusetts
ASSOCIATE EDITORS
Takashi Asai, M.D., Ph.D., Osaka, JapanBeatrice Beck-Schimmer, M.D., Zurich, SwitzerlandJames M. Blum, M.D., F.C.C.M., Atlanta, GeorgiaChad Michael Brummett, M.D., Ann Arbor, MichiganJohn Butterworth, M.D., Richmond, VirginiaMaxime Cannesson, M.D., Ph.D., Los Angeles, CaliforniaMaurizio Cereda, M.D., Philadelphia, Pennsylvania
Vincent W. S. Chan, M.D., F.R.C.P.C., F.R.C.A., Toronto, CanadaSteven P. Cohen, M.D., Baltimore, MarylandMelissa L. Coleman, M.D., Hershey, PennsylvaniaAlbert Dahan, M.D., Ph.D., Leiden, The NetherlandsDouglas Eleveld, M.D., Groningen, The NetherlandsHolger K. Eltzschig, M.D., Ph.D., Houston, TexasCharles W. Emala, Sr., M.D., M.S., New York, New YorkDavid Faraoni, M.D., Ph.D., F.C.C.P., F.A.H.A., Toronto, CanadaJorge A. Galvez, M.D., M.B.I., Philadelphia, PennsylvaniaLaurent Glance, M.D., Rochester, New YorkStephen T. Harvey, M.D., Nashville, TennesseeHarriet W. Hopf, M.D., Salt Lake City, UtahVesna Jevtovic-Todorovic, M.D., Ph.D., M.B.A., Aurora, ColoradoRu-Rong Ji, Ph.D., Durham, North CarolinaCor J. Kalkman, M.D., Utrecht, The NetherlandsMeghan Lane-Fall, M.D., M.H.S.P., Philadelphia, PennsylvaniaAdam B. Lerner, M.D., Boston, MassachusettsKate Leslie, M.B.B.S., M.D., M.Epi., F.A.N.Z.C.A., Parkville, AustraliaGeorge A. Mashour, M.D., Ph.D., Ann Arbor, MichiganDaniel McIsaac, M.D., M.P.H., Ottawa, CanadaJane S. Moon, M.D., Los Angeles, CaliforniaJochen D. Muehlschlegel, M.D., M.M.Sc., Boston, MassachusettsPaul S. Myles, M.B., B.S., M.P.H., M.D., F.F.A.R.C.S.I., F.A.N.Z.C.A., Melbourne, AustraliaPeter Nagele, M.D., M.Sc., Chicago, IllinoisMark D. Neuman, M.D., M.Sc., Philadelphia, PennsylvaniaCraig Palmer, M.D., Tucson, ArizonaCyril Rivat, M.D., Montpellier, FranceJeffrey Sall, M.D., Ph.D., San Francisco, CaliforniaWarren S. Sandberg, M.D., Ph.D., Nashville, TennesseeAlan Jay Schwartz, M.D., M.S.Ed., Philadelphia, PennsylvaniaDaniel I. Sessler, M.D., Cleveland, OhioAllan F. Simpao, M.D., M.B.I., Philadelphia, PennsylvaniaNikolaos J. Skubas, M.D., Cleveland, OhioKen Solt, M.D., Boston, MassachusettsDavid A. Story, M.B.B.S., B.Med.Sci., M.D., Parkville, AustraliaMichel Struys, M.D., Groningen, The Netherlands
ALNV134N2_Text.indb 9ALNV134N2_Text.indb 9 29-Dec-20 19:43:0029-Dec-20 19:43:00
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
The Journal of the American Society of Anesthesiologists, Inc. anesthesiology.org
Trusted Evidence: Discovery to Practice
Mission: Promoting scientific discovery and knowledge in perioperative, critical care, and pain medicine to advance patient care.
®
Eric Sun, M.D., Ph.D., Palo Alto, CaliforniaBobbieJean Sweitzer, M.D., F.A.C.P., Chicago, IllinoisMarcos F. Vidal Melo, M.D., Ph.D., Boston, MassachusettsJonathan P. Wanderer, M.D., M.Phil., Nashville, TennesseeDavid S. Warner, M.D., Durham, North CarolinaDuminda N. Wijeysundera, M.D., Ph.D., F.R.C.P.C., Toronto, CanadaHannah Wunsch, M.D., M.Sc., Toronto, CanadaMichael Zaugg, M.D., M.B.A., Edmonton, Canada
VISUAL TEAM
Christina Boncyk, M.D., Nashville, TennesseeJorge A. Galvez, M.D., M.B.I., Philadelphia, PennsylvaniaMeghan Lane-Fall, M.D., M.S.H.P., Philadelphia,
PennsylvaniaDaniel Larach, M.D., Los Angeles, CaliforniaOlivia Nelson, M.D., Philadelphia, PennsylvaniaJames P. Rathmell, M.D., Boston, MassachusettsAllan F. Simpao, M.D., M.B.I., Philadelphia, PennsylvaniaNaveen Vanga, M.D., Houston, TexasAnnemarie B. Johnson, C.M.I., Medical Illustrator,
Winston-Salem, North CarolinaTerri Navarette, Graphic Artist, Schaumburg, Illinois
AUDIO TEAM
Jorge A. Galvez, M.D., M.B.I., Philadelphia, PennsylvaniaYoung-Tae Jeon, M.D., Seoul, KoreaYandong Jiang, M.D., Ph.D., Houston, TexasRie Kato, M.D., D. Phil., Kanagawa, JapanJames P. Rathmell, M.D., Boston, MassachusettsCyril Rivat, M.D., Montpelier, FranceBobbieJean Sweitzer, M.D., Chicago, IllinoisHenrique F. Vale, M.D., Jackson, Mississippi
SOCIAL MEDIA TEAM
Rita Agarwal, M.D., Palo Alto, CaliforniaSean Barnes, M.B.A., M.D., Baltimore, MarylandNabil Elkassabany, M.D., Philadelphia, PennsylvaniaAlana Flexman, M.D., F.R.C.P.C., Vancouver, CanadaJorge A. Galvez, M.D., M.B.I., Philadelphia, PennsylvaniaHarriet W. Hopf, M.D., Salt Lake City, UtahRuth Landau, M.D., New York City, New YorkEdward R. Mariano, M.D., M.A.S., Palo Alto, CaliforniaEmily Sharpe, M.D., Rochester, MinnesotaSasha Shillcutt, M.D., M.S., F.A.S.E., Lincoln, NebraskaCaitlin Sutton, M.D., Houston, TexasAllan F. Simpao, M.D., M.B.I., Philadelphia, PennsylvaniaAnkeet Udani, M.D., M.S.Ed., Durham, North Carolina
ALNV134N2_Text.indb 10ALNV134N2_Text.indb 10 29-Dec-20 19:43:0029-Dec-20 19:43:00
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
You are preparing for an open abdominal procedure in an obese patient (body mass index, 39 kg/m2). In addition to tidal volume ventilation of 7 mL/kg of predicted body weight, you decide to use high positive end-expiratory pressure (PEEP) to minimize postoperative pulmonary complications. Based on a recent randomized clinical trial that compared high PEEP (12 cm H2O) and hourly recruitment maneuvers with low PEEP (4 cm H2O) and no recruitment maneuvers, which of the following outcomes is MOST likely in this patient?
A. Similar risk of postoperative respiratory complications
B. Lower risk of hypotensive episodes intraoperatively
C. Higher risk of postoperative respiratory complications because this patient’s body mass index is less than 40
ASA YOUR EDUCATION
SEE if you answered correctlyasahq.org/SEE2021A-Question
21-100
You are preparing for an open abdominal procedure in an obese patient (body mass index, 39 kg/mventilation of 7 mL/kg of predicted body weight, you decide to use high positive end-expiratory pressure (PEEP) to minimize postoperative pulmonary complications. Based on a recent randomized clinical trial that compared high PEEP (12 cm Hhourly recruitment maneuvers with low PEEP (4 cm Hwhich of the following outcomes is MOST likely in this patient?
A. complications
B. intraoperatively
C. complications because this patient’s body mass index is less than 40
SEE if you answered correctlyasahq.org/SEE2021A-Question
Stay plu ed into the most important advances in the specialty with Summaries of Emerging Evidence (SEE) 2021—now available!
Challenge your thinking
02_2021 ASA+Your Edu_SEE Ad.indd 102_2021 ASA+Your Edu_SEE Ad.indd 1 12/18/20 9:41 AM12/18/20 9:41 AMALNV134N2_Text.indb 10ALNV134N2_Text.indb 10 29-Dec-20 19:43:0029-Dec-20 19:43:00
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
ANESTHESIOLOGY CME PROGRAMANESTHESIOLOGY CME PROGRAM
Instructions for Obtaining ANESTHESIOLOGY Continuing Medical Education (CME) CreditCME Editors: Leslie C. Jameson, M.D., and Dan J. Kopacz, M.D.
ANESTHESIOLOGY’S Journal CME is open to all readers. To take part in ANESTHESIOLOGY Journal-based CME, complete the following steps:
1. Read the accreditation information presented on this page.2. Read this month’s articles designated for credit (listed below) in
either the print or online edition.3. Register at http://www.asahq.org/shop-asa. In the category, search for
Journal CME. Nonmembers will need to provide payment.4. Achieve a score of at least 50% correct on the six-question online
journal quiz and complete the evaluation.5. Claim credit in 15-minute increments, for a maximum of 1 AMA
PRA Category 1 Credits™ per journal article.
Accreditation InformationPurpose: The focus of Anesthesiology Journal-based CME is to educate readers on current developments in the science and clinical practice of anesthesiology.
Target Audience: Anesthesiology Journal-based CME is intended for anesthesiologists. Researchers and other healthcare professionals with an interest in anesthesiology may also participate.
Accreditation and Designation Statements: The American Society of Anesthesiologists is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
The American Society of Anesthesiologists designates this journal-based activity for a maximum of 1 AMA PRA Category 1 CreditsTM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Maintenance of Certi cation in AnesthesiologyTM pro-gram and MOCA® are registered trademarks of the American Board of Anesthesiology®. MOCA 2.0® is a trademark of the American Board of Anesthesiology®.
This activity contributes to the CME component of the American Board of Anesthesiology’s redesigned Maintenance of Certi cation in AnesthesiologyTM (MOCA®) program, known as MOCA 2.0®. Please consult the ABA website, http://www.theABA.org, for a list of all MOCA 2.0 requirements.
RatesTwo options are available: ASA Member Non-memberAnnual Fee $0 $120Payment may be made using Visa or MasterCard.Please direct any questions about Journal-based CME to: [email protected] of Release: January 2021Expiration Date: January 2024
This Month’s ANESTHESIOLOGY Journal-based CME ArticlesRead the article by Ilfeld et al. entitled “Clinical E ectiveness of Liposomal Bupivacaine Administered by In ltration or Peripheral Nerve Block to Treat Postoperative Pain: A Narrative Review” on page 283 and the article by Hussain et al. entitled “Perineural Liposomal Bupivacaine Is Not Superior to Nonliposomal Bupivacaine for Peripheral Nerve Block Analgesia: A Systematic Review and Meta-analysis” on page 147.
Learning ObjectivesAfter successfully completing this activity, the learner will be able to describe the clinical e ects of liposomal bupivacaine used for in ltration at the surgical site and in comparison with aqueous local anesthetics; describe the clinical e ects of liposomal bupivacaine used for peripheral nerve blockade and in comparison with aqueous bupivacaine; and describe the cost–bene t relationship of liposomal bupivacaine in comparison with aqueous bupivacaine.
DisclosuresThese journal articles have been selected for and planned as a journal CME activity, which is designated for AMA PRA Category 1 CreditTM. The authors disclosed relationships in keeping with Anesthesiology’s requirements for all journal submissions. All relationships journal authors disclosed to Anesthesiology are disclosed to learners, even those rela-tionships that are not relevant nancial relationships, per the ACCME’s requirements for CME activities.
Editor-in-Chief: Evan D. Kharasch, M.D., Ph.D., has disclosed no relevant nancial relationships with commer-cial interests.
CME Editors: Leslie C. Jameson, M.D., has disclosed no relevant nancial relationships with commercial interests. Dan J. Kopacz, M.D., has disclosed holding an equity posi-tion with Solo-Dex, Inc.
ASA Sta : Kari Lee and Anne Farace have disclosed no relevant nancial relationships with commercial interests.
DisclaimerThe information provided in this activity is for continuing education purposes only and is not meant to substitute for the independent medical judgment of a healthcare provider relative to diagnostic and treatment options of a speci c patient’s medical condition.
DOI: 10.1097/ALN.0000000000003675
ALNV134N2_Text.indb 11ALNV134N2_Text.indb 11 29-Dec-20 19:43:0129-Dec-20 19:43:01
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
CALL FOR SUBMISSIONS
Problem-based Learning DiscussionsDue February 8 at 11:59 p.m. CT
Scientifi c AbstractsScientifi c and Educational Exhibits Due April 5 at 11:59 p.m. CT
Medically Challenging Cases/Quality Improvement ProjectsDue May 24 at 11:59 p.m. CT
Submit your work at asahq.org/AnnualMeetingSubmissions
OCTOBER 9-13, 2021
Be a part of
21-101
Be recognized as an anesthesia physician leader!
Apply for the Fellow of the American Society of Anesthesiologists® (FASA®) designation and demonstrate your infl uence in areas of professionalism, leadership, advocacy, education, and scholarly activities.
19-089
Stand out from the crowd asahq.org/fasa
ANES21 Submissions Ad.indd 1ANES21 Submissions Ad.indd 1 12/18/20 9:52 AM12/18/20 9:52 AMALNV134N2_Text.indb 12ALNV134N2_Text.indb 12 29-Dec-20 19:43:0129-Dec-20 19:43:01
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Key Papers from the Most Recent Literature Relevant to Anesthesiologists
SCIENCE, MEDICINE, AND THE ANESTHESIOLOGIST
ANESTHESIOLOGY, V 134 • NO 2 FEBRUARY 2021 DOI: 10.1097/ALN.0000000000003676
Martin J. London, M.D., Editor
Antenatal dexamethasone for early preterm birth in low-resource countries. N Engl J Med 2020 Oct 23 [Epub ahead of print]. PMID: 33095526.Antenatal glucocorticoids have been shown to reduce preterm infant mortality and morbidity in women in developed coun-tries, but their use in low-resource countries is controversial. The authors conducted a placebo-controlled randomized trial of intramuscular dexamethasone (6 mg every 12 h to a maximum of 4 doses) in pregnant women between 26 and 33 weeks gestation at risk for preterm birth in 29 South Asian and African hospitals. The primary outcomes were neonatal death alone, stillbirth or neonatal death, and possible maternal bacterial infection. A total of 2,852 women (with 3,070 fetuses) underwent randomization. The trial was stopped for benefit at the second interim analysis. Comparing the dexamethasone group versus
placebo, neonatal death occurred in 20% versus 24% of infants (relative risk 0.84 [95% CI, 0.72 to 0.97], P = 0.03), stillbirth or neonatal death occurred in 26% versus 29% of infants or fetuses (relative risk 0.88 [95% CI, 0.78 to 0.99], P = 0.04), and the incidence of possible maternal bacterial infection was 5% versus 6% (relative risk 0.76 [95% CI, 0.56 to 1.03]) with no significant between-group difference in the incidence of adverse events. (Article Selection: Laszlo Vutskits, M.D. Image: Adobe Stock.)Take home message: Antenatal dexamethasone significantly reduces risks of neonatal death alone and stillbirth or neonatal death, without a greater inci-dence in possible maternal bacterial infection, compared to placebo among women in low-resource countries at risk for preterm birth.
Association of lumbar puncture with spinal hematoma in patients with and without coagulopathy. JAMA 2020; 324:1419–28. PMID: 33048155.Coagulopathy is considered a risk factor for spinal hematoma in lumbar puncture. The authors report a nationwide (Den-mark), population-based cohort study (2008 to 2018) using medical registries to detect subjects undergoing lumbar puncture (83,711 lumbar punctures among 64,730 patients) with cerebrospinal fluid analysis stratifying subjects with coagulopathy (platelets lower than 150 × 109/l, international normalized ratio (INR) greater than 1.4, or activated partial thromboplastin time longer than 39 s). The primary outcome was 30-day risk of spinal hematoma. A secondary outcome was risk of traumatic lumbar puncture (greater than 300 × 106 erythrocytes/l). Thrombocytopenia was present in 9% of patients, elevated INR in 2%,
and prolonged activated partial thromboplastin time in 3%. Comparing patients without coagulopathy versus patients with coagulopathy, spinal hematoma occurred within 30 days for 0.20% (95% CI, 0.16 to 0.24%) versus 0.23% (95% CI, 0.15 to 0.34%). Independent risk factors included male sex (adjusted hazard ratio 1.72 [95% CI, 1.15 to 2.56]), age 41 through 60 yr (adjusted hazard ratio 1.96 [95% CI, 1.01 to 3.81]) and age 61 through 80 yr (adjusted hazard ratio 2.20 [95% CI, 1.12 to 4.33]). Risk did not increase significantly with the severity of coagulopathy, by pediatric specialty or medical indication, nor by the cumulative number of procedures. Traumatic lumbar punctures occurred more frequently among patients with elevated INR levels or elevated activated partial thromboplastin time. (Article Selection: Martin J. London, M.D. Image: Adobe Stock.)Take home message: In a retrospective nationwide cohort study the risk of spinal hematoma after lumbar puncture was low and not different between those with and without coagulopathy, although the observed rates may be confounded by preferential selection of lower-risk patients.
Life expectancy after bariatric surgery in the Swedish Obese Subjects study. N Engl J Med 2020; 383:1535–43. PMID: 33053284.Obesity lowers life expectancy, and bariatric surgery may improve life expectancy in obese subjects. This long-term follow-up analysis from the prospective intervention Swedish Obese Subjects study examined mortality after bariatric surgery in a cohort of 2,007 patients receiving bariatric surgery between 1987 and 2001, compared with a control group of 2,040 patients receiving usual obesity care and 1,135 patients without obesity. At 20 to 24 yr follow-up, 23% in the bariatric surgery group, 26% in the usual obesity care group, and 11% in the reference cohort had died. The hazard ratio for death in the bariatric surgery group compared with the usual care group was 0.77 (95% CI, 0.68 to 0.87; P < 0.001), and the hazard ratio for
death between the reference cohort and the usual obesity care group was 0.44 (95% CI, 0.31 to 0.48; P < 0.001). Life expectancy in the usual obesity care group was 3 yr shorter than in the surgery group (95% CI, 1.8 to 4.2; P < 0.001), and 9 yr shorter in the usual obesity care group than the reference cohort (95% CI, 6.4 to 10.5; P < 0.001). In subgroup analysis, the mortality benefit of bariatric surgery was similar in high- and low-risk patients. (Article Selection: Marilyn D. Michelow, M.D. Image: Adobe Stock.)Take home message: Bariatric surgery improved long-term life expectancy in patients with obesity compared to usual obesity care, but mortality remained higher relative to the general population.
SMAMARTIN J. LONDON, M.D., EDITOR
ALNV134N2_Text.indb 12ALNV134N2_Text.indb 12 29-Dec-20 19:43:0129-Dec-20 19:43:01
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

SCIENCE, MEDICINE, AND THE ANESTHESIOLOGIST
Key Papers from the Most Recent Literature Relevant to Anesthesiologists
DOI: 10.1097/ALN.0000000000003676 FEBRUARY 2021 ANESTHESIOLOGY, V 134 • NO 2
Decoding the mystery of American pain reveals a warning for the future. Proc Natl Acad Sci USA 2020; 117:24785–9. PMID: 32958666.With an accumulating burden of disease and degenerative changes with aging, the prevalence of self-reported (Gallup polls, U.S. and European governmental polls) pain has been hypothesized to increase with advancing age, a trend observed in most developed countries. However, pain prevalence in the United States assessed using large cross-sectional surveys appears to peak in middle age followed by a decline. The authors analyzed statistically a group of such surveys over dif-ferent time periods to demonstrate that successive birth cohorts (covering 1930 to 1990) have been reporting more pain throughout their lives than preceding cohorts. They demonstrate that it is not that pain declines among the elderly, but
rather that later birth cohorts are more likely to report more pain. This pattern of increased pain is mostly attributable to subjects without college educa-tions, although changes in occupation (from more physical to more sedentary) or ranges of obesity were not significant risk factors. (Article Selection: J. David Clark, M.D, Ph.D. Image: M. Lane-Fall/Adobe Stock.)Take home message: The increasing prevalence of self-reported pain over successive birth cohorts appears to be primarily related to deterioration in social and economic conditions experienced by less well-educated Americans born after 1950. These observations are likely to have significant implica-tions for healthcare utilization in the future.
Developing and validating subjective and objective risk-assessment measures for predicting mortality after major surgery: An international prospective cohort study. PLoS Med 2020; 17:e1003253. PMID: 33057333.With increasing availability of large datasets, preoperative risk stratification has become an important tool to guide clin-ical decisions and resource allocation. In this prospective cohort study, the authors compared the accuracy of available objective surgical risk tools with subjective clinical judgment (e.g., American Society of Anesthesiologists Physical Status) in predicting 30-day mortality after major surgery. For 1 week in 2017, prospective risk, surgical, and outcome data were collected in 22,631 adult patients who underwent surgery requiring at least one overnight stay in 274 hospitals in the
United Kingdom, Australia, and New Zealand. The authors compared subjective assessment with three objective tools for predicting 30-day mortality: the Portsmouth-Physiology and Operative Severity Score for the Enumeration of Mortality, the Surgical Risk Scale, and the Surgical Outcome Risk Tool. Logistic regression models combining subjective assessment and the best objective tool were evaluated. The Surgical Outcome Risk Tool demonstrated the best discrimination of the objective tools (area under receiver operating characteristic curve [AUC] = 0.90 [95% CI, 0.88 to 0.92]), but subjective assessment demonstrated equally good discrimination (AUC = 0.89 [95% CI, 0.86 to 0.91]) compared to the Surgical Outcome Risk Tool (P = 0.309). Combining subjective assessment and the Surgical Outcome Risk Tool improved discrimination (AUC = 0.92 [95% CI, 0.90 to 0.94]). (Article Selection: David Faraoni, M.D., Ph.D. Image: Adobe Stock.)Take home message: A combination of subjective clinical judgment with objective risk models improved perioperative risk prediction relative to either method alone.
Gabapentin for chronic pelvic pain in women (GaPP2): A multicentre, randomised, double-blind, placebo-controlled trial. Lancet 2020; 396:909–17. PMID: 32979978.Chronic pelvic pain is a condition affecting 20% or more of females causing both suffering and disability. Effective treatment options remain limited. Off-label use of gabapentin has been suggested, but data from clinical trials are lacking. To address this gap, the gabapentin for chronic pelvic pain (GaPP2) collaborative conducted a 39-center randomized double-blind trial in the United Kingdom. Entry criteria included: female sex 18 to 50 yr of age, chronic pelvic pain of at least 3 months dura-tion, and no obvious pelvic pathology at laparoscopy. A total of 306 participants were randomized to gabapentin, titrated up
to 2,700 mg/day or matched placebo, for 16 weeks. The study’s two primary outcome measures were worst and average pain scores (assessed using a 0 to 10 numeric rating scale) at weeks 13 to 16 of therapy. Gabapentin had no significant effect on pain scores; the mean change in the worst pain score from baseline was mean ± SD, –1.4 ± 2.3 in the gabapentin group and –1.2 ± 2.1 in the placebo group (adjusted mean difference –0.20 [97.5% CI, –0.81 to 0.42], P = 0.47). Gabapentin was associated with a higher incidence of self-reported adverse effects (dizziness, drowsiness, and visual distur-bances) compared to placebo (7% vs. 2%, P = 0.04). (Article Selection: J. David Clark, M.D, Ph.D. Image: Adobe Stock.)Take home message: Off-label use of gabapentin for females with chronic pelvic pain and no evidence of pelvic pathology was ineffective in reducing average or worst pain scores and was associated with a higher incidence of adverse effects.
ALNV134N2_Text.indb 13ALNV134N2_Text.indb 13 29-Dec-20 19:43:0229-Dec-20 19:43:02
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

SCIENCE, MEDICINE, AND THE ANESTHESIOLOGIST
Key Papers from the Most Recent Literature Relevant to Anesthesiologists
ANESTHESIOLOGY, V 134 • NO 2 FEBRUARY 2021 DOI: 10.1097/ALN.0000000000003676
Delivering transformative action in paediatric pain: A Lancet Child & Adolescent Health Commission. Lancet Child Adolesc Health 2021; 5:47–87. PMID: 33064998.Appropriate management of pediatric pain remains a challenge. The Lancet Child and Adolescent Health Commission puts into perspective four transformative goals which, if implemented, will improve the lives of children and adolescents with pain and their families over the next decade. First, the Commission outlines a strategy to make children’s pain matter to others. They advocate for the importance of understanding the social science of pain and discuss how the absence of voice can lead to an assumption that there is an absence of need. Second, they argue that development of safe and effective
treatments will only emerge if they are informed by an in-depth understanding of the developmental aspects of nociception and pain systems. Third, they recommend that pain can and should be assessed, no matter the age or clinical status of the child. Finally, they emphasize that every child should have access to evidence-based pain assessment and subsequent treatment using the most effective methods and means available. A detailed list of priorities for research, clinical practice, and political actions are articulated around these four transformative goals. The ensemble of these goals should be conducted in parallel to achieve a meaningful change in pediatric pain management. (Article Selection: Laszlo Vutskits, M.D. Image: Adobe Stock.)Take home message: A multidisciplinary Commission of Pediatric Pain experts has published in review article format a multipronged approach to improving detection and treatment of pain in infants, children, and adolescents.
Frequency and outcomes of preoperative stress testing in total hip and knee arthroplasty from 2004 to 2017. JAMA Cardiol 2020 Sep 30 [Epub ahead of print]. PMID: 32997100.While the American College of Cardiology and the American Heart Association advocate for evidence-based preoperative cardiac assessments based on patient functional status, risk factors, and the urgency and nature of surgery, temporal trends and outcomes of preoperative testing in specific noncardiac surgery populations have not been rigorously described. This retrospective, cross-sectional study included 801,396 elective total hip (27.9%) and total knee arthroplasty (72.1%) patient records (2003 to 2017), from the IBM MarketScan Commercial and Medicare Supplemental Databases (median age
62 yr, 58.1% female). The study aimed to describe temporal trends in preoperative cardiac stress testing within 60 days before surgery, characteristics associated with testing, and cardiac events during the total joint arthroplasty hospitalization. Over the study period, the rate of preoperative cardiac stress testing was 10%, with a decline in testing from 2006 through 2017 at an annual rate ranging from –0.71% to –0.40%. Patient factors associated with preoperative cardiac stress testing included age, male sex, and at least one Revised Cardiac Risk Index condition. The overall rate of myocardial infarction or cardiac arrest was 0.24%, which was not associated with patient risk factors or preoperative testing. (Article Selection: Meghan Prin, M.D., M.S. Image: M. Lane-Fall/Adobe Stock.)Take home message: In a retrospective cohort analysis using national administrative databases, preoperative stress testing decreased from 2006 to 2017 while the rate of coded cardiac complications was unchanged between those tested or not.
Lung ultrasound and pulmonary congestion during stress echocardiography. JACC Cardiovasc Imaging 2020; 13:2085–95. PMID: 32682714.The “B-profile” detected by lung ultrasound is considered a sign of pulmonary congestion. To assess the significance of this pattern during stress echocardiography, the authors prospectively performed transthoracic echocardiography and lung ultrasound (before, at, or immediately after peak stress) in 2,145 patients undergoing this procedure at 11 centers. B-lines were scored 0 to 10 in each of four locations. New regional wall motion abnormalities, reduced left ventricular contractile reserve, abnormal coronary flow velocity reserve, and abnormal heart rate reserve were also assessed. Subjects were grouped by absence of stress B-lines (score: 0 to 1, 64.7%), mild B-lines (score: 2 to 4, 20%), moderate B-lines (score: 5
to 9, 9.7%) and severe B-lines (score: great than 10, 5.4%). During a median follow-up of 15.2 months, 38 deaths and 28 nonfatal myocardial infarctions occurred in 64 patients. Independent predictors of death and nonfatal myocardial infarction included severe B-lines (hazard ratio 3.54 [95% CI, 1.47 to 8.69], P = 0.006), abnormal heart rate reserve (hazard ratio 2.28 [95% CI, 1.22 to 4.26], P = 0.010), abnormal coronary flow velocity reserve (hazard ratio 2.18 [95% CI, 1.06 to 4.48], P = 0.034), and age (hazard ratio 1.03 [95% CI, 1.00 to 1.06], P = 0.037). (Article Selection: Martin J. London, M.D. Image: M. Lane-Fall/Adobe Stock.)Take home message: Severe B-lines on lung ultrasound during peak stress predict death and nonfatal myocardial infarction and may assist in risk stratification.
ALNV134N2_Text.indb 14ALNV134N2_Text.indb 14 29-Dec-20 19:43:0229-Dec-20 19:43:02
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

SCIENCE, MEDICINE, AND THE ANESTHESIOLOGIST
Key Papers from the Most Recent Literature Relevant to Anesthesiologists
DOI: 10.1097/ALN.0000000000003676 FEBRUARY 2021 ANESTHESIOLOGY, V 134 • NO 2
Multiplexed plasma immune mediator signatures can differentiate sepsis from noninfective SIRS: American Surgical Association 2020 annual meeting paper. Ann Surg 2020; 272:604–10. PMID: 32932316.The systemic inflammatory response syndrome (SIRS) is commonly triggered by sepsis, but it can also be triggered in the absence of sepsis leading to inappropriate antibiotic usage. Cytokine inflammatory responses can be initiated by microbial “pathogen-associated molecular patterns,” and/or from injured tissue displaying “damage-associated molecular patterns.” The authors used a multiplexed assay of 31 different cytokines from plasma of patients with: sepsis of varying severity (n = 29); trauma-induced SIRS (n = 11); and healthy controls (n = 11) incorporating decision trees and machine learning
statistical techniques to identify significant intergroup differences. Septic patients had high concentrations of interleukin-6, interleukin-1α, and triggering receptor expressed on myeloid cells-1 (TREM-1). In contrast, sterile injury was associated with widespread mediator suppression. Application of a two-group multivariate random-forest model (evaluating combinations of cytokines) correctly classified 11 of 11 injury patients and 28 of 29 infection patients. (Article Selection: Jamie Sleigh, M.D. Image: M. Lane-Fall/Adobe Stock.)Take home message: Machine learning based on multiplexed plasma cytokine assays may eventually allow distinction between sepsis-related and injury-related SIRS with the potential to reduce inappropriate antibiotic usage.
Part 1: Executive summary: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2020; 142:S337–S357. PMID: 33081530.The American Heart Association has updated the 2015 recommendations for cardiopulmonary resuscitation (CPR) and emergency cardiovascular care. A series of publications presents reports from writing groups evaluating literature on basic and advanced life support for adults, pediatric patients, and neonates as well as resuscitation education science and systems of care. New clinical recommendations, updated algorithms, and areas of focus for adult resuscitation include CPR during transport, CPR before calling for help, feedback for CPR quality, analysis of rhythm during chest compressions,
vasopressor use during cardiac arrest, modes of defibrillation, point of care echocardiography during CPR, targeted temperature management, and resuscitation for opioid-associated emergencies. Pediatric care topics include initial and interval doses of epinephrine for cardiac arrest, ventilation rate during CPR, and traumatic shock management. Neonatal topics include epinephrine for resuscitation, oxygen concentration for preterm infants at birth, and tracheal intubation and suction of nonvigorous newborns with meconium staining. Recommendations for first aid include control of life-threatening external bleeding, stroke recognition, cooling for heatstroke and dental avulsion. In total, the 2020 American Heart Association Guidelines include 491 recommendations of which 51% are based on limited evidence and 17% on expert opinion and thus persistent knowledge gaps that require additional research are also emphasized. (Article Selection: BobbieJean Sweitzer, M.D., F.A.C.P. Image: M. Lane-Fall/Adobe Stock.)Take home message: New and updated recommendations for resuscitation and cardiovascular care based on recommendations of individual American Heart Association writing groups have been published as summarized in this executive summary.
Small airway loss in the physiologically ageing lung: A cross-sectional study in unused donor lungs. Lancet Respir Med 2020 Oct 5 [Epub ahead of print]. PMID: 33031747.The decline in lung function due to aging has been attributed to mechanisms including loss of alveolar tissue, increased chest wall rigidity, reduced elastic lung recoil, and lower dynamic lung volumes. However, data regarding the effect of aging on airways of small diameter (less than 2.0 mm) remain scarce. In this cross-sectional study, lungs retrieved from donors were analyzed using ex vivo computed tomography and whole-lung high-resolution computed tomography (micro-com-puted tomography). The aim was to determine total airway numbers stratified by airway diameter. Micro-computed tomog-
raphy in particular allowed for the measurement of number, length, and diameter of terminal bronchioles. Lungs from 32 nonsmoking donors (aged 16 to 83 yr) were included in the study. Between 30 and 80 yr, an age-dependent reduction in number of small airways with a diameter of 2 to 2.5 mm and with a diameter of less than 2 mm was found, with a β coefficient per decade of −0.119 (95% CI, −0.193 to −0.045; R2 = 0.29) and of −0.158 (−0.233 to −0.084; R2 = 0.47), respectively. No age-dependent reduction in number of airways greater than 2.5 mm in diameter was shown. The micro-computed tomography analysis demonstrated that after 30 yr of age, the number of terminal bronchioles steadily decreased (β coefficient per decade −2035; 95% CI, −2818 to −1252; R2 = 0.55). (Article Selection: Beatrice Beck-Schimmer, M.D. Image: M. Lane-Fall/Adobe Stock.)Take home message: This study reveals an important component of physiological lung aging by showing an age-dependent reduction in number of small airways and terminal bronchioles.
ALNV134N2_Text.indb 15ALNV134N2_Text.indb 15 29-Dec-20 19:43:0229-Dec-20 19:43:02
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
DOI: 10.1097/ALN.000000000003677 FEBRUARY 2021 ANESTHESIOLOGY, V 134 • NO 2
Infographic created by Jonathan P. Wanderer, Vanderbilt University Medical Center, and James P. Rathmell, Brigham and Women’s Health Care/Harvard Medical School. Illustration by Annemarie Johnson, Vivo Visuals. Address correspondence to Dr. Wanderer: [email protected].
1. Ilfeld BM, Eisenach JC, Gabriel RA: Clinical effectiveness of liposomal bupivacaine administered by infiltration or peripheral nerve block to treat postoperative pain: A narrative review. Anesthesiology 2021; 134:283–344
2. Hussain N, Brull R, Sheely B, Essandoh MK, Stahl DL, Weaver TE, Abdallah FW: Perineural liposomal bupivacaine is not superior to nonliposomal bupivacaine for peripheral nerve block analgesia: A systematic review and meta-analysis. Anesthesiology 2021; 134:147–64
Copyright © 2018, the American Society of Anesthesiologists, Inc. Wolters Kluwer Health, Inc. All Rights Reserved. <journal-title> <ppub_year>; <volume>:<fpage>–<lpage>
Complex Information for Anesthesiologists Presented Quickly and ClearlyINFOGRAPHICS IN ANESTHESIOLOGY
Infographic
References
ALNV134N2_Text.indb 16ALNV134N2_Text.indb 16 29-Dec-20 19:43:0329-Dec-20 19:43:03
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
AQI:Where DataBecomesValueHELPING ADVANCE THE SPECIALTY HELPS YOUAnesthesiologists are proud to hold themselves to a higher standard than required — and AQI registries demonstrate that to the industry and consumers. Your participation makes the specialty stronger and helps you optimize treatment, compete more effectively and contain costs.
Get started now asahq.org/registries
19-079
10_2019 AQI_Registries .indd 1 8/28/19 3:39 PMALNV134N2_Text.indb 18ALNV134N2_Text.indb 18 29-Dec-20 19:43:0329-Dec-20 19:43:03
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

EDITORIAL
ANESTHESIOLOGY, V 134 • NO 2 FEBRUARY 2021 139
Image: A. Johnson, Vivo Visuals.
This editorial accompanies the articles on pp. 147 and 283.
Accepted for publication December 1, 2020. From Harvard Medical School, Cambridge, Massachusetts, and Boston Children’s Hospital, Boston, Massachusetts.
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved. Anesthesiology 2021 ; 134 : 139 – 42 . DOI: 10.1097/ALN.0000000000003658
Liposomal Bupivacaine Effective, Cost-effective, or (Just) Costly? Mary Ellen McCann, M.D.
One of the missions of the Food and Drug Administration
(Silver Spring, Maryland) is to pro-tect the public health by assuring the safety, e cacy, and security of human drugs. 1 According to Food and Drug Administration guid-ance, new drugs can be approved as long as they show e cacy com-pared to placebo, even if there are already drugs approved and avail-able that have been deemed e ec-tive. 2 Exparel (Pacira Biosciences, Inc., USA), an extended release liposomal formulation of bupiva-caine, rst approved by the Food and Drug Administration in 2011 for surgical site in ltration, was approved under these circum-stances. In this issue, two articles review 10 yr of research on the clinical e ectiveness of liposomal bupivacaine. Ilfeld et al . 3 provide an extensive narrative review of pub-lished randomized controlled tri-als, and Hussain et al . 4 conducted a systemic review and meta-analysis of the clinical e ectiveness of liposomal versus nonliposomal bupivacaine for peripheral nerve blocks.
The narrative review by Ilfeld et al . included 76 ran-domized controlled trials. Importantly, they were evaluated using the Cochrane Risk of Bias Version 2 tool. This tool consists of ve domains: bias from the randomizing pro-cess, bias due to deviations from intended intervention, bias due to missing outcome data, bias in measurement of out-come, and bias in selection of reported results. It does not measure the conduct of a trial. A summary bias judgment can be either “ low ” or “ high ” risk of bias, or can express “ some concerns, ” and a high risk summary judgment gen-erally indicates a nding of high risk in at least one of the domains. 5 The authors found that 35 to 40% of random-ized controlled trials reviewed had evidence of high risk or
some concerns for bias. The chief sources of bias included lack of trial registration, registration after enrollment, failure to de ne the primary outcome measure, and problems with de nition ( e.g. , discrepancy between registry and published article). Minimization of bias in randomized controlled tri-als is important to prevent data dis-tortion and erroneous conclusions. The Cochrane Risk of Bias tool does not measure con icts of inter-est by industry funding. Almost half of the studies in this review reported either direct funding or nancial support for the authors by the manufacturer of liposomal bupivacaine. Not surprisingly, lipo-somal bupivacaine was found to be superior to comparators in 46% of these con icted trials but was found to be superior in only 11% of the noncon icted trials.
The primary outcome in these 76 trials varied and was not always designated. There were
two types of primary outcome measures used: postopera-tive pain scales such as the visual analogue scale scores and numeric rating scales scores, or the mean morphine equiv-alents administered postoperatively to “ rescue ” the patient from pain. Some studies reported mean values, and others reported area under the curve values.
The rst 12 studies reviewed compared liposomal bupi-vacaine surgical site in ltration to placebo. Seven found no statistical di erence between liposomal bupivacaine and placebo, and of these, 88% were deemed at low risk for bias. The ve that did show statistical di erences were all rated with high risk for bias. Thirty-six of the randomized con-trolled trials compared surgical site in ltration of liposomal bupivacaine to surgical site in ltration of bupivacaine, rop-ivacaine, or lidocaine. Twenty-seven of these comparisons
“ … liposomal bupivacaine was found to be superior to comparators in 46% of … con icted [pharma-sponsored] trials but was found to be superior in only 11% of the noncon icted trials. ”
ALNV134N2_Text.indb 139ALNV134N2_Text.indb 139 29-Dec-20 19:43:0329-Dec-20 19:43:03
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

140 Anesthesiology 2021; 134:139–42 Mary Ellen McCann
EDITORIAL
used a maximum dose of liposomal bupivacaine of 266 mg but used a smaller dose of regular bupivacaine or ropiva-caine, possibly biasing the studies toward results favoring liposomal bupivacaine. Only six of the 36 studies of com-paring surgical site in ltration with liposomal bupivacaine with nonliposomal local anesthetic in ltration found the liposomal preparation to be superior. Five of these six stud-ies were judged to have high or concerning risk for bias. In ve of the six studies, the active comparator dose of bupi-vacaine was much lower than the liposomal bupivacaine dose, demonstrating that more bupivacaine works better than less bupivacaine. Twelve studies compared liposomal bupivacaine for surgical in ltration with a peripheral nerve block administered with either nonliposomal bupivacaine or ropivacaine. The nal group of 16 studies evaluated lipo-somal bupivacaine for a nerve block or epidural injection compared to placebo or active comparators, nonliposomal bupivacaine, or intrathecal hydromorphone, using the sim-ilar outcome measures to all the previous trials. Of these last 28 trials reviewed, 43% showed superiority of liposo-mal bupivacaine; 82% showed high risk or some concerns for bias. The authors concluded, “ Whether introduced by surgical in ltration or as part of a peripheral nerve block, the preponderance of current evidence fails to support the routine use of liposomal bupivacaine over standard local anesthetics when treating postoperative pain. ”
The systematic review and meta-analysis by Hussain et al . of the clinical e ectiveness of liposomal versus non-liposomal bupivacaine for peripheral nerve blocks evalu-ated the primary outcome of the 24- to 72-h di erence in the weighted mean area under the curve rest pain scores between patients receiving perineural analgesia inclusive of liposomal bupivacaine versus nonliposomal local anesthetics. The authors chose this time frame for the primary out-come measure because liposomal bupivacaine is promoted to improve the duration and quality of analgesia beyond the rst 24 h. 4 A variety of secondary outcomes relating to postoperative pain rating scores and opioid rescues were also evaluated during the postoperative period of 0 to 72 h. Nine trials were included in this meta-analysis. The authors found that the mean di erence (95% CI) in area under the curve of rest pain was found to be 1.0 cm/h (0.5 to 1.6; P = 0.003) in favor of liposomal bupivacaine, but this di er-ence failed to meet the prede ned threshold for clinical sig-ni cance ( i.e. , 2.0 cm/h; P < 0.001). Liposomal bupivacaine was similar to nonliposomal bupivacaine for all other anal-gesic and functional outcomes. The authors concluded that liposomal bupivacaine used perineurally in peripheral nerve blocks provides a clinically unimportant improvement in the area under the curve of postoperative pain scores com-pared to nonliposomal bupivacaine.
The results of these two articles should not come as a surprise in light of the early studies performed for the regulatory approval of liposomal bupivacaine. In 2006, SkyePharma, later known as Pacira Pharmaceuticals and
then Pacira Biosciences, collectively referred to here as Pacira Biosciences, submitted an New Drug Application application to the Food and Drug Administration for Exparel brand liposomal bupivacaine for an indication of relief of postoperative surgical pain, administered as wound in ltration. 6 For this indication, Pacira submitted ve phase 2 active comparator-controlled studies and three phase 3 active comparator-controlled studies using nonliposomal bupivacaine as the comparator. 6 None of these eight stud-ies showed clinical or statistical di erence between the two formulations.
Unable to demonstrate a bene t over nonliposomal bupivacaine, in 2009, the sponsor submitted two phase 3 placebo-controlled clinical trials showing e cacy of lipo-somal bupivacaine against placebo. 6 As allowed by regula-tion, despite no greater e cacy of liposomal bupivacaine than nonliposomal bupivacaine, the Food and Drug Administration in 2011 approved liposomal bupivacaine for surgical site in ltration to relieve postoperative pain for hemorrhoidectomy and bunionectomy. For this initial approval, the Food and Drug Administration deemed it not necessary for an advisory committee to meet. 7
In 2014, Pacira submitted a supplemental New Drug Application application for approval of liposomal bupiva-caine for an additional indication of postsurgical analgesia via nerve block, for which they submitted data from two new studies. The rst investigated intercostal nerve blocks and found that liposomal bupivacaine was not superior to placebo, based on no di erences in area under the curve analysis for pain intensity at rest using a numerical rating scale-R over 72 h. The second investigated femoral nerve blocks and found that liposomal bupivacaine at a dose of 266 mg was superior to placebo for pain relief, based on a primary outcome measure of area under the curve analysis of Numeric Rating Scale-Rest through 72 h but not superior on its secondary outcome measure of time to rst opioid rescue. This supplemental New Drug Application was not approved in the rst review cycle. In 2017, Pacira submitted two new multicenter, randomized, double-blind, and placebo-controlled nerve block studies. 8 , 9 The rst evaluated the e cacy of lipo-somal bupivacaine for postsurgical analgesia via femoral nerve block in patients undergoing total knee arthro-plasty. The second evaluated liposomal bupivacaine for postsurgical analgesia via ultrasound-guided brachial plexus nerve blocks by either supraclavicular or intersca-lene approach in patients undergoing shoulder surgery. Out of these four studies, both the two in 2014 and the two in 2017, the brachial plexus nerve block study was the only one that met both the primary e cacy end-point of improved area under the curve estimates of pain relief for the rst 48 to 72 h after surgery and decreased opioid rescues.
The Food and Drug Administration Anesthetic and Drug Products Advisory Committee met in 2018
ALNV134N2_Text.indb 140ALNV134N2_Text.indb 140 29-Dec-20 19:43:0329-Dec-20 19:43:03
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Editorial
Anesthesiology 2021; 134:139–42 141 Mary Ellen McCann
to review the supplemental New Drug Application request to approve liposomal bupivacaine for the new indication of regional nerve blocks. 10 , 11 This advisory committee consisted of 10 members with expertise in anesthesiology, pain medicine, pharmacology, or biosta-tistics, as well as a consumer and industry representative. Concerns raised by this committee included the lack of active comparator groups in the submitted studies, a lack of safety studies, and the lack of evidence for opioid sparing. Most of the voting advisory commit-tee members voted six to four against expanding the indication for liposomal bupivacaine. In 2018, the Food and Drug Administration approved Exparel for “ … use as an interscalene brachial plexus nerve block to produce post-surgical regional analgesia following shoulder sur-gery in adults. ” 12
To summarize, both the review by Ilfeld et al . and the meta-analysis by Hussain et al . concluded that liposomal bupivacaine did not show clinical superiority over exist-ing, active comparators, nonliposomal bupivacaine or ropivacaine. For the indication for in ltration, the stud-ies submitted by Pacira Biosciences did not demonstrate superiority of liposomal bupivacaine compared to these same active comparators. For the indication of periph-eral nerve block, they submitted only placebo studies. Although demonstrating e cacy of a new agent is sim-plest using a randomized placebo-controlled trial design, this design gives no information about the e cacy of a new agent compared to existing agents. Trials that have an active comparator arm as well as a placebo arm can deter-mine e cacy as well as give information about e cacy vis- à -vis existing, e ective drugs.
Why is all of this important? New drugs can be very nancially rewarding for pharmaceutical companies. 13
Once Exparel was approved, Pacira Biosciences began an aggressive and powerful marketing strategy. Between 2013 and 2019, they paid $ 25.8 million to more than 27,000 physicians for a variety of services including compensa-tion for being a speaker or faculty at nonaccredited edu-cational events. 14 Sales of liposomal bupivacaine increased during this time with the company reporting a 25% growth in 2019 over 2018 with full-year revenues of $ 421 million in 2019. 15 The cost of a single dose of 266 mg of Exparel brand liposomal bupivacaine is about $ 334. 16 Nonliposomal bupivacaine costs about $ 3 per dose. In this era of medical austerity, when the bene ts and costs of expensive drugs are being considered, one would hope that newly approved expensive drugs would at least be an improvement over existing, inexpensive drugs.
Competing Interests
The author declares no competing interests. The author was the acting Chair for the Food and Drug Administration Anesthetic and Analgesic Drug Products Advisory Committee February 14 and 15, 2018, which advised on
Pacira ’ s (Pacira Biosciences, Parsippany, New Jersey) sNDA application for expanded indication for Exparel for nerve blocks.
Correspondence
Address correspondence to Dr. McCann: [email protected]
References
1. Food and Drug Administration : What we do . 2018 . Available at: https://www.fda.gov/about-fda/what-we-do . Accessed November 5, 2020.
2. US Food and Drug Adnimistration : CFR - Code of Federal Regulations Title 21. April 1 , 2019 . Available at: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/cfrsearch.cfm?fr=314.126 . Accessed November 11, 2020.
3. Ilfeld BM , Eisenach JC , Gabriel RA : Clinical e ec-tiveness of liposomal bupivacaine administered by in ltration or peripheral nerve block to treat postop-erative pain: A narrative review. A nesthesiology 2020 ; 134 : 283 – 344
4. Hussain N , Brull R , Sheehy B , Essandoh MK , Stahl DL , Weaver TE , Abdallah FW : Perineural liposomal bupiv-acaine is not superior to nonliposomal bupivacaine for peripheral nerve block analgesia: A systematic review and meta-analysis. A nesthesiology 2020 ; 134 : 147 – 64
5. Sterne JAC , Savovic J , Page MJ , Elbers RG , Blencowe NS , Boutron I , Cates CJ , Cheng HY , Corbett MS , Eldridge SM , Emberson JR , Hernan MA , Hopewell S , Hrobjartsson A , Junqueira DR , Juni P , Kirkham JJ , Lasserson T , Li T , McAleenan A , Reeves BC , Shepperd S , Shrier I , Stewart LA , Tilling K , White IR , Whiting PF , Higgins JPT : RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019 ; 366 : l4898
6. Food and Drug Administration : NDA 022496, S009, EXPAREL assessment of e cacy data of studies submitted in support of sNDA. February 15 , 2017 . Available at: https://www.fda.gov/media/111376/download . Accessed November 20, 2020.
7. Center for Drug Evaluation and Research : Application number: 022496 Orig1s000, Cross Discipline Team Leader Review. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2011/022496Orig-1s000MedR.pdf . Accessed November 5, 2020.
8. Food and Drug Administration : Brie ng document anesthesia and analgesia drug products advisory meet-ing February 14 and February 15, 2018. Available at: https://www.fda.gov/media/110968/download . Accessed November 4, 2020.
9. Food and Drug Administration : Advisory Committee Meeting brie ng document, EXPAREL ® (bupi-vacaine liposome injectable suspension). Meeting of the Anesthetic and Analgesic Drug Products
ALNV134N2_Text.indb 141ALNV134N2_Text.indb 141 29-Dec-20 19:43:0429-Dec-20 19:43:04
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

142 Anesthesiology 2021; 134:139–42 Mary Ellen McCann
EDITORIAL
Advisory Committee. Available at: https://www.fda.gov/files/advisory%20committees/published/Pacira-Briefing-Information-for-the-February-14-15--2018-Meeting-of-the-Anesthetic-and-Analgesic-Drug-Products-Advisory-Committee.pdf . Accessed November 5, 2020.
10. Litman RS : Anesthetic and Analgesic Drug Products Advisory Committee activity and decisions in the opi-oid-crisis era. A nesthesiology 2020 ; 133 : 740 – 9
11. Food and Drug Administration : Center for Drug Evaluation and Research, summary minutes of the Anesthetic and Analgesic Drug Products Advisory Committee meeting, February 14-15, 2018. Available at: https://www.fda.gov/media/112187/download . Accessed November 4, 2020.
12. Food and Drug Administration : In brief: FDA approves new use of Exparel for nerve block pain relief following shoulder surgeries. April 16 , 2018 . Available at: https://www.fda.gov/news-events/fda-brief/fda-brief-fda-approves-new-use-exparel-nerve-block-pain-relief-
following-shoulder-surgeries . Accessed November 5, 2020.
13. Van Zee A : The promotion and marketing of oxycon-tin: Commercial triumph, public health tragedy. Am J Public Health 2009 ; 99 : 221 – 7
14. OpenPaymentsData.CMS.gov : Pacira Pharmaceuticals Incorporated. 2020 . Available at: https://open-paymentsdata.cms.gov/company/100000000135 . Accessed November 5, 2020.
15. Pacira Biosciences, Inc. : News release Pacira reports record fourth quarter and full-year revenues . 2020 . Available at: https://investor.pacira.com/news-re-leases/news-release-details/pacira-reports-record-fourth-quarter-and-full-year-revenues-0 . Accessed November 5, 2020.
16. Exparel : EXPAREL is a cost-e ective option for post-surgical pain management in the hospital and ambu-latory (outpatient) settings . 2020 . Available at: https://www.exparel.com/hcp/value/total-hip-arthroplasty . Accessed November 6, 2020.
ALNV134N2_Text.indb 142ALNV134N2_Text.indb 142 29-Dec-20 19:43:0429-Dec-20 19:43:04
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
EDITORIAL
ANESTHESIOLOGY, V 134 • NO 2 FEBRUARY 2021 143
Image: J. P. Rathmell.
This editorial accompanies the article on p. 165.
Accepted for publication November 6, 2020. Published online fi rst on December 17, 2020. From the Division of Cardiac Anesthesia, Department of Anesthesia and Pain Medicine, The Hospital for Sick Children, Toronto, Canada (D.F.); the Department of Anesthesiology and Pain Medicine, University of Toronto, Toronto, Canada (D.F.): and the Department of Anesthesiology and Critical Care, Duke University School of Medicine, Durham, North Carolina (J.H.L.).
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved. Anesthesiology 2021 ; 134 : 143 – 6 . DOI: 10.1097/ALN.0000000000003637
Optimal Tranexamic Acid Dosing Regimen in Cardiac Surgery: What Are the Missing Pieces? David Faraoni , M.D., Ph.D., F.A.H.A. , Jerrold H. Levy , M.D., F.A .H.A., F.C.C.M.
Multiple randomized clinical trials evaluating prophylac-
tic tranexamic acid administration consistently demonstrate a reduc-tion of bleeding and allogeneic blood product transfusion require-ments. 1 , 2 International guidelines recommend prophylactic admin-istration of anti brinolytic agents in patients undergoing high-risk cardiac surgical procedures. 3 , 4 In the most recent large trial, patients scheduled to undergo coronary artery bypass surgery and at risk for perioperative complications were randomized to receive either tranexamic acid (50 to 100 mg/kg of actual body weight) or pla-cebo. 5 Tranexamic acid was associ-ated with a lower risk of bleeding than placebo without increase in mortality or thrombotic compli-cations within 30 days of surgery. However, tranexamic acid was also associated with a higher risk of postoperative seizures (0.1% vs . 0.7%, P = 0.002). In a 1-yr fol-low-up study, there was no di erence in death or severe dis-ability between patients exposed to tranexamic acid or the placebo. 6 Despite the favorable safety pro le of tranexamic acid, several questions remain unanswered ( g. 1 ), and the optimal dose needed to reduce bleeding without increas-ing the risk of side e ects, especially seizures, is still not established.
In this issue of Anesthesiology , Zu erey et al . per-formed a model-based meta-analysis to describe the e ect of di erent tranexamic acid doses on postoperative bleed-ing and clinical seizures. 7 Their meta-analysis objectives were to estimate the dose-response relationship and identify the optimal dosing regimen to be used in adults undergoing
cardiac surgery with cardiopulmo-nary bypass. The authors included 64 randomized controlled tri-als and 18 observational studies of intravenous tranexamic acid administration in adult cardiac surgical patients. They found that the plasma concentration required to achieve 50% of maximum e ect was 5.6 mg/l (95% credible inter-val, 0.7 to 11.1 mg/l) or 22.4 mg/l to achieve 80% inhibition of bri-nolytic activation. The authors also reported an increased risk of postoperative clinical seizure incidence of 1.07 (95% credible interval, 1.06 to 1.09) per 10 mg/l increase in tranexamic acid plasma concentration. Compared to no exposure to tranexamic acid, a plasma concentration of 100 mg/l doubled the risk of clinical sei-zures (2.1; 95% credible interval, 1.9 to 2.4). Among other risk fac-tors, open-chamber procedures and prolonged cardiopulmonary bypass duration both signi cantly
increased the risk of clinical seizures. Using their mod-el-based meta-analysis, the authors conclude that low-dose tranexamic acid (total dose of 20 mg/kg of actual body weight) provides the best balance between reduction in postoperative blood loss and red blood cell transfusion and the risk of clinical seizure. The use of higher doses would only marginally improve the clinical e ect at the cost of an increased risk of seizure.
The results reported in this model-based meta-analy-sis are relevant and an important step toward de ning the optimal tranexamic acid dosing regimen in adult cardiac surgical patients. This analysis rst integrates the results obtained from large clinical trials with our knowledge of
“ … low-dose tranexamic acid (total dose of 20 mg/kg of actual body weight) provides the best balance between reduction in postoperative blood loss and red blood cell transfusion and the risk of clinical seizure. ”
ALNV134N2_Text.indb 143ALNV134N2_Text.indb 143 29-Dec-20 19:43:0429-Dec-20 19:43:04
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
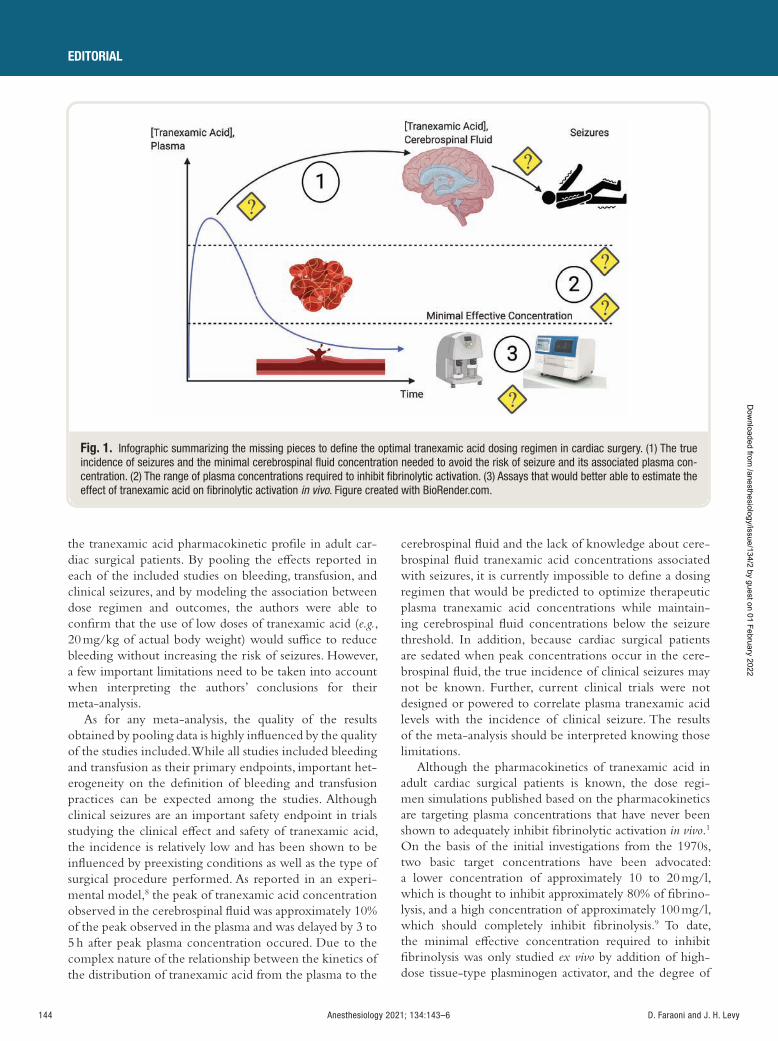
144 Anesthesiology 2021; 134:143–6 D. Faraoni and J. H. Levy
EDITORIAL
the tranexamic acid pharmacokinetic pro le in adult car-diac surgical patients. By pooling the e ects reported in each of the included studies on bleeding, transfusion, and clinical seizures, and by modeling the association between dose regimen and outcomes, the authors were able to con rm that the use of low doses of tranexamic acid ( e.g. , 20 mg/kg of actual body weight) would su ce to reduce bleeding without increasing the risk of seizures. However, a few important limitations need to be taken into account when interpreting the authors ’ conclusions for their meta-analysis.
As for any meta-analysis, the quality of the results obtained by pooling data is highly in uenced by the quality of the studies included. While all studies included bleeding and transfusion as their primary endpoints, important het-erogeneity on the de nition of bleeding and transfusion practices can be expected among the studies. Although clinical seizures are an important safety endpoint in trials studying the clinical e ect and safety of tranexamic acid, the incidence is relatively low and has been shown to be in uenced by preexisting conditions as well as the type of surgical procedure performed. As reported in an experi-mental model, 8 the peak of tranexamic acid concentration observed in the cerebrospinal uid was approximately 10% of the peak observed in the plasma and was delayed by 3 to 5 h after peak plasma concentration occured. Due to the complex nature of the relationship between the kinetics of the distribution of tranexamic acid from the plasma to the
cerebrospinal uid and the lack of knowledge about cere-brospinal uid tranexamic acid concentrations associated with seizures, it is currently impossible to de ne a dosing regimen that would be predicted to optimize therapeutic plasma tranexamic acid concentrations while maintain-ing cerebrospinal uid concentrations below the seizure threshold. In addition, because cardiac surgical patients are sedated when peak concentrations occur in the cere-brospinal uid, the true incidence of clinical seizures may not be known. Further, current clinical trials were not designed or powered to correlate plasma tranexamic acid levels with the incidence of clinical seizure. The results of the meta-analysis should be interpreted knowing those limitations.
Although the pharmacokinetics of tranexamic acid in adult cardiac surgical patients is known, the dose regi-men simulations published based on the pharmacokinetics are targeting plasma concentrations that have never been shown to adequately inhibit brinolytic activation in vivo . 1
On the basis of the initial investigations from the 1970s, two basic target concentrations have been advocated: a lower concentration of approximately 10 to 20 mg/l, which is thought to inhibit approximately 80% of brino-lysis, and a high concentration of approximately 100 mg/l, which should completely inhibit brinolysis. 9 To date, the minimal e ective concentration required to inhibit brinolysis was only studied ex vivo by addition of high-dose tissue-type plasminogen activator, and the degree of
Fig. 1. Infographic summarizing the missing pieces to defi ne the optimal tranexamic acid dosing regimen in cardiac surgery. (1) The true incidence of seizures and the minimal cerebrospinal fl uid concentration needed to avoid the risk of seizure and its associated plasma con-centration. (2) The range of plasma concentrations required to inhibit fi brinolytic activation. (3) Assays that would better able to estimate the effect of tranexamic acid on fi brinolytic activation in vivo . Figure created with BioRender.com.
ALNV134N2_Text.indb 144ALNV134N2_Text.indb 144 29-Dec-20 19:43:0529-Dec-20 19:43:05
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Editorial
Anesthesiology 2021; 134:143–6 145 D. Faraoni and J. H. Levy
brinolysis was measured with viscoelastic testing, either thromboelastography or thromboelastometry. 10 , 11 From those studies, the tranexamic acid concentration to e ec-tively inhibit brinolysis was in the range of 6 to 15 mg/l. Two important limitations need to be noted. Experiments were performed ex vivo in the absence of endothelium and other plasma components that could in uence brino-lytic activation. Further, viscoelastic hemostatic tests have poor sensitivity to detect brinolytic activation. 12 Plasmin generation assays have recently been used to measure the impact of intravenous tranexamic acid administration on plasmin generation and brinolytic activation. In a cohort of healthy women undergoing cesarean delivery, the abil-ity of the plasmin generation assay to detect the e ect of tranexamic acid on brinolytic activation was found supe-rior to what could be detected using thromboelastome-try. 13 Although such an assay could be seen as a promising tool to estimate the e ect of tranexamic acid on brino-lytic activation in cardiac surgical patients, further in vivoclinical studies are needed before the minimal e ective concentration of tranexamic acid can be used to de ne the optimal dosing scheme.
In summary, the model-based meta-analysis published by Zu erey et al . in this issue of Anesthesiology con rms the safety and the clinical e ect of low-dose tranexamic acid in adult cardiac surgical patients. In order to further re ne the optimal dosing scheme, more studies will be needed to complete the missing information required to determine the minimal e ective concentration of tranexamic acid to be targeted to inhibit brinolytic activation and reduce bleeding, while minimizing the risk of seizures.
Competing Interests
The authors are not supported by, nor maintain any nan-cial interest in, any commercial activity that may be associ-ated with the topic of this article.
Correspondence
Address correspondence to Dr. Faraoni: [email protected]
References
1. Koster A , Faraoni D , Levy JH : Anti brinolytic therapy for cardiac surgery: An update. A nesthesiology 2015 ; 123 : 214 – 21
2. Levy JH , Koster A , Quinones QJ , Milling TJ , Key NS : Anti brinolytic therapy and perioperative consider-ations. A nesthesiology 2018 ; 128 : 657 – 70
3. Task Force on Patient Blood Management for Adult Cardiac Surgery of the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Cardiothoracic Anaesthesiology (EACTA), Boer C , Meesters MI , Milojevic M , Benedetto U , Bolliger D , von Heymann C , Jeppsson
A , Koster A , Osnabrugge RL , Ranucci M , Ravn HB , Vonk ABA , Wahba A , Pagano D : 2017 EACTS/EACTA guidelines on patient blood management for adult cardiac surgery. J Cardiothorac Vasc Anesth 2018 ; 32 : 88 – 120
4. Raphael J , Mazer CD , Subramani S , Schroeder A , Abdalla M , Ferreira R , Roman PE , Patel N , Welsby I , Greilich PE , Harvey R , Ranucci M , Heller LB , Boer C , Wilkey A , Hill SE , Nuttall GA , Palvadi RR , Patel PA , Wilkey B , Gaitan B , Hill SS , Kwak J , Klick J , Bollen BA , Shore-Lesserson L , Abernathy J , Schwann N , Lau WT : Society of Cardiovascular Anesthesiologists clini-cal practice improvement advisory for management of perioperative bleeding and hemostasis in cardiac sur-gery patients. Anesth Analg 2019 ; 129 : 1209 – 21
5. Myles PS , Smith JA , Forbes A , Silbert B , Jayarajah M , Painter T , Cooper DJ , Marasco S , McNeil J , Bussi è res JS , McGuinness S , Byrne K , Chan MT , Landoni G , Wallace S ; ATACAS Investigators of the ANZCA Clinical Trials Network : Tranexamic acid in patients undergoing coronary-artery surgery. N Engl J Med 2017 ; 376 : 136 – 48
6. Myles PS , Smith JA , Kasza J , Silbert B , Jayarajah M , Painter T , Cooper DJ , Marasco S , McNeil J , Bussi è res JS , McGuinness S , Byrne K , Chan MTV , Landoni G , Wallace S , Forbes A ; ATACAS Investigators and the ANZCA Clinical Trials Network : Tranexamic acid in coronary artery surgery: One-year results of the Aspirin and Tranexamic Acid for Coronary Artery Surgery (ATACAS) trial. J Thorac Cardiovasc Surg 2019 ; 157 : 644 – 652.e9
7. Zu erey PJ , Lanoiselée J , Graouch B , Vieille B , Delavenne X , Ollier E : Exposure-response relationship of tranexamic acid in cardiac surgery: A model-based meta-analysis. A nesthesiology 2020 ; 134 : 165 – 78
8. Lecker I , Wang DS , Romaschin AD , Peterson M , Mazer CD , Orser BA : Tranexamic acid concentrations associ-ated with human seizures inhibit glycine receptors. J Clin Invest 2012 ; 122 : 4654 – 66
9. Andersson L , Nilsoon IM , Colleen S , Granstrand B , Melander B : Role of urokinase and tissue activator in sustaining bleeding and the management thereof with EACA and AMCA. Ann N Y Acad Sci 1968 ; 146 : 642 – 58
10. Yee BE , Wissler RN , Zanghi CN , Feng C , Eaton MP : The e ective concentration of tranexamic acid for inhibition of brinolysis in neonatal plasma in vitro . Anesth Analg 2013 ; 117 : 767 – 72
11. Rozen L , Faraoni D , Sanchez Torres C , Willems A , Noubouossie DC , Barglazan D , Van der Linden P , Demulder A : E ective tranexamic acid concentration for 95% inhibition of tissue-type plasminogen activator induced hyper brinolysis in children with congenital heart disease: A prospective, controlled, in-vitro study. Eur J Anaesthesiol 2015 ; 32 : 844 – 50
ALNV134N2_Text.indb 145ALNV134N2_Text.indb 145 29-Dec-20 19:43:0529-Dec-20 19:43:05
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

146 Anesthesiology 2021; 134:143–6 D. Faraoni and J. H. Levy
EDITORIAL
12. Raza I , Davenport R , Rourke C , Platton S , Manson J , Spoors C , Khan S , De ’ Ath HD , Allard S , Hart DP , Pasi KJ , Hunt BJ , Stanworth S , MacCallum PK , Brohi K : The incidence and magnitude of brinolytic acti-vation in trauma patients. J Thromb Haemost 2013 ; 11 : 307 – 14
13. Miszta A , Ahmadzia HK , Luban NLC , Li S , Guo D , Holle LA , Berger JS , James AH , Gobburu JVS , van den Anker J , de Laat B , Wolberg AS : Application of a plasmin generation assay to de ne pharmacodynamic e ects of tranexamic acid in women undergoing cesarean deliv-ery. J Thromb Haemost 2020 [Epub ahead of print]
ALNV134N2_Text.indb 146ALNV134N2_Text.indb 146 29-Dec-20 19:43:0529-Dec-20 19:43:05
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
PERIOPERATIVE MEDICINE
ANESTHESIOLOGY, V 134 • NO 2 FEBRUARY 2021 147
Liposomal bupivacaine used for in ltration 1 – 18 and eld blocks 19 – 25 is proposed to provide extended postoper-
ative analgesia up to 72 h 26 , 27 after various surgical proce-dures. Recently, the U.S. Food and Drug Administration
(Silver Spring, Maryland) approved liposomal bupivacaine for perineural use in interscalene block of the brachial plexus. 28 However, evidence of the clinical e ectiveness of perineurally applied liposomal bupivacaine in extending
ABSTRACT Background: Liposomal bupivacaine is purported to extend analgesia of peripheral nerve blocks when administered perineurally. However, evidence of the clinical effectiveness of perineural liposomal bupivacaine is mixed. This meta-analysis seeks to evaluate the effectiveness of perineural liposomal bupivacaine in improving peripheral nerve block analgesia as compared with nonliposomal local anesthetics.
Methods: The authors identifi ed randomized trials evaluating the effec-tiveness of peripheral nerve block analgesic that compared liposomal bupi-vacaine with nonliposomal local anesthetics. The primary outcome was the difference in area under the receiver operating characteristics curve (AUC) of the pooled 24- to 72-h rest pain severity scores. Secondary outcomes included postoperative analgesic consumption, time to fi rst analgesic request, incidence of opioid-related side effects, patient satisfaction, length of hospital stay, liposomal bupivacaine side effects, and functional recovery. AUC pain scores were interpreted in light of a minimal clinically important difference of 2.0 cm · h.
Results: Nine trials (619 patients) were analyzed. When all trials were pooled, AUC pain scores ± SD at 24 to 72 h were 7.6 ± 4.9 cm · h and 6.6 ± 4.6 cm · h for nonliposomal and liposomal bupivacaine, respectively. As such, perineural liposomal bupivacaine provided a clinically unimportant benefi t by improving the AUC (95% CI) of 24- to 72-h pain scores by 1.0 cm · h (0.5 to 1.6; P = 0.003) compared with nonliposomal bupivacaine. Excluding an industry-sponsored trial rendered the difference between the groups nonsig-nifi cant (0.7 cm · h [ − 0.1 to 1.5]; P = 0.100). Secondary outcome analysis did not uncover any additional benefi ts to liposomal bupivacaine in pain sever-ity at individual timepoints up to 72 h, analgesic consumption, time to fi rst analgesic request, opioid-related side effects, patient satisfaction, length of hospital stay, and functional recovery. No liposomal bupivacaine side effects were reported.
Conclusions: Perineural liposomal bupivacaine provided a statistically signifi cant but clinically unimportant improvement in the AUC of postop-erative pain scores compared with plain local anesthetic. Furthermore, this benefi t was rendered nonsignifi cant after excluding an industry-sponsored trial, and liposomal bupivacaine was found to be not different from plain local anesthetics for postoperative pain and all other analgesic and func-tional outcomes. High-quality evidence does not support the use of peri-neural liposomal bupivacaine over nonliposomal bupivacaine for peripheral nerve blocks.
(ANESTHESIOLOGY 2021 ; 134 : 147 – 64 )
Perineural Liposomal Bupivacaine Is Not Superior to Nonliposomal Bupivacaine for Peripheral Nerve Block Analgesia A Systematic Review and Meta-analysis Nasir Hussain , M.D., M.Sc. , Richard Brull , M.D. , Brendan Sheehy , M.D. , Michael K. Essandoh , M.D. , David L. Stahl , M.D. , Tristan E. Weaver , M.D. , Faraj W. Abdallah , M.D., M.Sc.
ANESTHESIOLOGY 2021 ; 134 : 147 – 64
This article has been selected for the Anesthesiology CME Program. Learning objectives and disclosure and ordering information can be found in the CME section at the front of this issue. This article is featured in “This Month in Anesthesiology,” page 1A. This article is accompanied by an editorial on p. 139 and a review article on p. 283. This article has a related Infographic on p. 17A. This article has an audio podcast. This article has a visual abstract available in the online version.
Submitted for publication July 27, 2020. Accepted for publication November 19, 2020. From the Department of Anesthesiology, The Ohio State University, Wexner Medical Center, Columbus, Ohio (N.H., B.S., M.K.E., D.L.S., T.E.W.); Department of Anesthesiology and Pain Medicine, University of Toronto, Canada (R.B., F.W.A.); Women ’ s College Research Institute, Toronto, Canada (R.B., F.W.A.); and the Department of Anesthesiology and Pain Medicine, Ottawa Hospital Research Institute, University of Ottawa, Ottawa, Canada (F.W.A.).
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved. Anesthesiology 2021 ; 134 : 147 – 64 . DOI: 10.1097/ALN.0000000000003651
EDITOR ’ S PERSPECTIVE
What We Already Know about This Topic
• Liposomal bupivacaine was developed in an effort to extend the duration of local analgesia
• Despite the availability of many studies, it remains unclear whether and when liposomal bupivacaine offers significant advantages over the standard formulation
What This Article Tells Us That Is New
• Nine trials were included in a meta-analysis examining the difference in 24- to 72-h rest pain severity scores for liposomal and nonliposomal bupivacaine
• The area under the curve pain scores for the 24- to 72-h period were statistically but probably not clinically signifi cant
• Secondary outcome analysis likewise failed to uncover benefi ts for lipo-somal bupivacaine regarding analgesic consumption, length of stay, and functional recovery
ALNV134N2_Text.indb 147ALNV134N2_Text.indb 147 29-Dec-20 19:43:0529-Dec-20 19:43:05
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

148 Anesthesiology 2021; 134:147–64
PERIOPERATIVE MEDICINE
Hussain et al .
the duration of postoperative analgesia of peripheral nerve blocks is not de nitive. 29 Indeed, a recent Cochrane review 30
of seven trials could not con rm the claim that liposomal bupivacaine improved analgesic outcomes.
This systematic review and meta-analysis aims to evalu-ate the e ectiveness of perineural liposomal bupivacaine in improving peripheral nerve block analgesia, in comparison with nonliposomal local anesthetics, across various surgical procedures. We designated the di erence in postoperative pain severity over the 24- to 72-h interval as a primary outcome. We also assessed the potential bene ts of liposomal bupiva-caine on short-term analgesic outcomes, as well as long-term outcomes, such as persistent postsurgical pain, opioid depen-dence, and health-related quality of life. Industry-sponsored trials were a priori considered a potential source of bias to be identi ed in the literature search and subsequent analysis.
Materials and Methods The authors adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement guidelines in preparation of this study. 31 We searched for randomized trials that compared the e ect of perineural liposomal bupivacaine with nonliposomal local anesthetics on short-term analgesic outcomes and other long-term outcomes in patients having surgery with peripheral regional anesthesia techniques. The created study protocol was not registered with the International prospective register of systematic reviews (PROSPERO).
Eligibility Criteria
Randomized trials of adult patients (18 yr or older) under-going any type of surgery with peripheral nerve blocks that compared perineural liposomal bupivacaine with non-liposomal local anesthetics were considered. All types of single-injection peripheral nerve blocks were considered, regardless of dose or volume of liposomal bupivacaine used. Only nonliposomal local anesthetic ( i.e. , not combined with liposomal bupivacaine) was considered as a comparator. Studies involving perineural adjuvants other than epineph-rine were excluded. Studies of eld blocks ( i.e. , transversus abdominal block) and in ltration techniques ( i.e. , port site in ltration or local in ltration analgesia) were not included to preserve homogeneity between studies. Studies of healthy volunteers were not eligible. Abstracts were not considered unless the full-text studies were available, and any foreign language studies were translated using an online translator.
Literature Search
A systematic search strategy was created by an evidence-based medicine librarian (L.B.) for the U.S. National Library of Medicine (Bethesda, Maryland) database (MEDLINE), Cochrane Database of Systematic Reviews, and Excerpta Medica database from inception to May 1, 2020. The search strategy was based on an initial search generated for MEDLINE (appendix 1). The strategy contained key words
related to liposomal bupivacaine, pain, analgesic consumption, and postoperative analgesia. The reference lists of potentially eligible citations were also manually searched to identify addi-tional trials that ful lled inclusion criteria. We also reviewed the U.S. clinical trials registry ( http://www.clinicaltrials.gov ) for in-progress or completed clinical trials that satis ed our inclusion criteria. Finally, conference proceedings for the American Society of Anesthesiologists (Schaumburg, Illinois) 2011 to 2020 and American Society of Regional Anesthesia and Pain Medicine (Pittsburgh, Pennsylvania) 2013 to 2020 were electronically searched for potentially eligible citations.
Selection of Included Studies
Two reviewers (N.H. and B.S.) independently screened the titles and abstracts yielded by the literature search. The full texts of potentially eligible citations were then retrieved and evaluated for inclusion by the same independent reviewers. Any disagreement between the two reviewers was discussed until a consensus was reached. If consensus could not be reached between the two independent reviewers, a third reviewer (F.A.) made the nal decision.
Data Extraction
A data extraction form was created using a Microsoft Excel (USA) spreadsheet and piloted by an independent reviewer (N.H). Data extraction was subsequently carried out inde-pendently by two reviewers (N.H. and B.S.). Any discrepancies in data extraction were discussed until a consensus was reached. If consensus could not be reached between the two indepen-dent reviewers, a third reviewer (F.A.) made the nal decision.
The data extraction form collected information regard-ing the following variables: year of publication; participant age; publication year; type of surgery; surgical anesthetic; type of regional anesthetic technique; dose and volume of nonli-posomal local anesthetic used; dose of volume of liposomal bupivacaine used; adjuvant used in local anesthetic solution; preoperative, intraoperative, and postoperative analgesic regi-mens; rest and dynamic pain scores at all reported times; anal-gesic consumption at all reported times; time to rst analgesic request (duration of analgesia); opioid-related side e ects; satisfaction with pain relief; hospital length of stay; liposo-mal bupivacaine – related side e ects; functional recovery; and long-term outcomes including incidence of persistent post-surgical pain, health-related quality of life, opioid dependence, and pain-related disability. The primary source of data was numerical data presented in tables and gures. Data reported in graphical form were extracted with the assistance of graph digitizing software (GraphClick, Arizona Software, USA).
Assessment of Methodologic Quality and Risk of Bias
The methodologic quality of included trials was evaluated independently by two reviewers (N.H. and B.S.) using the Cochrane Collaboration tool for risk of bias assessment. 32 We conservatively assigned an “ unclear risk of bias ” to blinding of
ALNV134N2_Text.indb 148ALNV134N2_Text.indb 148 29-Dec-20 19:43:0529-Dec-20 19:43:05
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:147–64 149
Analgesia after Perineural Liposomal Bupivacaine
Hussain et al .
personnel and outcome assessors ’ domain for those studies in which the methods did not provide su cient details.
In addition, the methodologic quality for each out-come pooled across trials was assessed using the Grades of Recommendation, Assessment, Development, and Evaluation 33 , 34 guidelines. The strength of evidence was then rated as being of high quality ( ⊕ ⊕ ⊕ ⊕ ), moderate quality ( ⊕ ⊕ ⊕ ⊝ ), low quality ( ⊕ ⊕ ⊝ ⊝ ), or very low qual-ity ( ⊕ ⊝ ⊝ ⊝ ) evidence.
All quality assessments were done in duplicate by two inde-pendent reviewers (N.H. and B.S.). Any discrepancies in qual-ity assessment were discussed until a consensus was reached. If consensus could not be reached between the two independent reviewers, a third reviewer (F.A.) made the nal decision.
Primary and Secondary Outcomes
Because liposomal bupivacaine is promoted to improve dura-tion and quality of analgesia beyond the rst 24 h, 26 , 27 , 35 we selected analgesic outcomes that emphasized the 24- to 72-h time interval to evaluate the comparative clinical e ective-ness of liposomal bupivacaine and nonliposomal local anes-thetic. To that end, the primary outcome of this meta-analysis was designated as the 24- to 72-h di erence in the weighted mean area under the curve (AUC) rest pain scores between patients receiving perineural analgesia inclusive of liposomal bupivacaine versus nonliposomal local anesthetics.
The secondary analgesic outcomes examined included cumulative oral milligram morphine equivalent consumption on days one (0 to 24 h), two (25 to 48 h), and three (49 to 72 h) postoperatively; postoperative rest pain severity (visual analog scale) scores at 1, 6, 12, 24, 48, and 72 h postopera-tively; time to rst analgesic request (hours); opioid-related side e ects (nausea and vomiting, sedation/respiratory depres-sion, pruritus, hypotension, urinary retention, or constipation); patient satisfaction; and hospital length of stay (hours). We also evaluated incidence of liposomal bupivacaine adverse e ects ( i.e. , hypesthesia, pyrexia, pruritus) 36 ; postoperative functional recovery; and long-term outcomes, including the risk of per-sistent postsurgical pain, health-related quality of life, opioid dependence, and pain-related disability.
Measurement of Outcome Data
All measures of postoperative pain severity that were expressed as units of a 10-unit scale were converted to an equivalent score on the 0- to 10-cm visual analog scale score (0, no pain; and 10, worst pain possible). 37 , 38 Similarly, all measures of patient satisfaction were also converted to a 0- to 10-cm score (0, least satis ed; and 10, most satis ed). 38 All opioid consump-tion data were converted to cumulative oral morphine equiv-alents for the speci c time interval ( i.e. , 0 to 24 h, 25 to 48 h, 49 to 72 h). 39 Time-to-event data were presented in hours.
Statistical Analysis
The mean ± SD were sought for all continuous outcomes. When these were not available, statistical conversions 40 – 43
were made using the presented data to approximate these values. Speci cally, the median and interquartile range were used to approximate the mean and SD when its value was not provided. 40 In situations where a mean and 95% CI was provided, conversions were made to a mean and SD using the methods described by the Cochrane Collaboration. 41
The median was used to approximate the mean in situa-tions where it was the only value provided. If no measure of variance was provided, the value of the SD was imputed as a last resort. 42 This was done by calculating the pooled SD from all other studies included in the same outcome analyzed. 42 Finally, when needed for statistical pooling, cat-egorical/ordinal data were converted to continuous form with corresponding mean ± SD using the natural units of the most familiar instrument. 38 In all circumstances, authors were contacted for additional results data, if needed.
For AUC analysis, the weighted mean di erence (95% CI) in AUC of acute rest pain between liposomal bupiva-caine and plain local anesthetic over the rst 24- to 72-h postoperative period was calculated using the weighted means of the pooled rest pain scores during the 24-, 48-, and 72-h timepoints. The weighted means were then used to calculate the AUC for a speci c time interval ( i.e. , 24 to 48 h and 48 to 72 h). The results of individual studies were weighted by their overall sample size. This analysis was only conducted if (1) data were available for all three timepoints and (2) data for a speci c timepoint was available from three or more studies.
For evaluation of the e ect of liposomal bupivacaine on postoperative functional recovery, we a priori planned to report (1) the mean di erence if all studies used the same continuous scale, (2) the log (odds ratio) if trials reported continuous data and used di erent tools measuring the same theme to assess postoperative function, or (3) an odds ratio if all trials reported binary outcomes. If scenario 2 was applicable, the conversion to log (odds ratio) from a standardized mean di erence was done using the formula log (odds ratio) = standardized mean di erence ( π / √ 3), 44 , 45
under the assumption that the mean scores for each group followed a logistic distribution and that variances were equal between the two groups.
Meta-analysis
For continuous outcomes, pooling was performed using the inverse variance method because we anticipated clinical heterogeneity between studies. For dichotomous outcomes, pooling was performed using the Mantel – Haenszel ran-dom-e ects model. 46 For our primary outcome, a weighted mean di erence with 95% CI was calculated, and a two-tailed P value of < 0.05 was designated as the threshold of statistical signi cance.
For the continuous secondary outcomes of this review, a mean di erence with 99% CI was calculated. For the dichot-omous secondary outcomes, an odds ratio with 99% CI was calculated. Finally, for postoperative functional recovery, reporting depended on the nature of data (as described above).
ALNV134N2_Text.indb 149ALNV134N2_Text.indb 149 29-Dec-20 19:43:0529-Dec-20 19:43:05
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

150 Anesthesiology 2021; 134:147–64
PERIOPERATIVE MEDICINE
Hussain et al .
The 99% CI was used for all secondary outcomes to decrease the risk of type I error associated with multiple testing, and a two-tailed P value of < 0.01 was designated as the threshold of statistical signi cance. To that end, we also used a threshold for statistical signi cance adjusted by the Bonferroni – Holm cor-rection for comparisons in the secondary outcome analysis. 47
Statistical pooling was only performed for those out-comes that had data from three or more studies. A quali-tative evaluation was performed for those outcomes with fewer than three studies.
Interpretation of Outcome Results
For rest pain scores during the 24- to 72-h time interval, the results were interpreted in light of the minimal clinically important di erence in pain scores for acute postoperative pain. This has been de ned to be a 1.0-cm change on a 0- to 10-cm scale at an individual timepoint across a variety of surgeries. 48
For an AUC encompassing three measurements (24, 48, and 72 h), a threshold equivalent to 2.0 cm · h is calculated using the trapezoid method 49 and a minimum clinically important di erence of 1.0 cm 48 for each of the three measurements.
Although not rigorously established, for cumulative opi-oid consumption during the 0- to 72-h interval, we con-sidered a 30-mg di erence in oral morphine consumption 50
(or 10 mg intravenous morphine) to be clinically important.
Assessment of Heterogeneity
For the primary outcome of this review ( i.e. , 24- to 72-h di er-ence in the AUC of rest pain scores), a priori sensitivity analysis was carried out by sequential exclusion of data from trials (1) published in nonindexed journals, (2) available as abstracts only, (3) published only in only U.S. Clinical Trials Registry, (4) with high-risk of bias in one or more domains of the Cochrane risk of bias tool, (5) that used other long-acting local anesthetics ( i.e. , levobupivacaine or ropivacaine), and (6) supported by or declared con ict of interest with industry, speci cally compa-nies involved in manufacturing liposomal bupivacaine.
The extent of statistical heterogeneity in our second-ary outcomes was assessed by calculating a percentage of variation ( I2 ) statistic, with values greater than 50% indi-cating signi cant heterogeneity. For instances of signi cant heterogeneity, the Grades of Recommendation, Assessment, Development, and Evaluation quality of evidence for an outcome were downgraded.
Assessment of Publication Bias
The risk of publication bias was assessed using the Egger ’ s regression test when data from at least three trials were available for an estimate of e ect. 51
Data Management
Forest and funnel plots were generated using Review Manager Software (RevMan version 5.2; Nordic Cochrane
Center, Denmark; Cochrane Collaboration). Sensitivity analysis and tests for publication bias were performed using Comprehensive Meta-Analysis 3.0 (Engelwood, USA).
Results The literature search identi ed a total of 439 unique citations, and an additional 31 were identi ed after searching the U.S. Clinical Trials Registry. Thus, a total of 470 citations underwent screening based on title and abstract alone. Of these, 418 were excluded for many reasons, including incorrect comparison (n = 298), incorrect study design (n = 95), and incomplete study data (n = 26). The remaining 52 citations had their full-text ver-sions retrieved or protocols reviewed for additional eligibility. After full-text screening, a total of 43 citations were excluded because of incorrect comparator (n = 42) 1 – 25 , 52 – 68 or lack of available data (n = 1). 69 As a result, a total of nine randomized trials were included in this review, 70 – 78 of which four 73 – 76 were from the U.S. Clinical Trials Registry and ve 70 – 72 , 77 ,78 were published as full text. The ow diagram for study inclusion can be viewed in gure 1 . Of these trials, the authors of one study declared con icts of interest related to industry sponsorship. 71
Study Characteristics
The study characteristics and outcomes included in this review are presented in table 1 . The nine trials 70 – 78 involved 619 patients, of whom 316 received peripheral nerve blocks using perineural liposomal bupivacaine, and 303 received blocks with nonliposomal local anesthetics. Rest pain scores from 24 to 72 h postoperatively were assessed by all nine trials. 70 – 78 Eight of the trials reported opioid consumption beyond 24 h. 70 – 77
Speci c details regarding the measures of pain assessed by the included trials can be viewed in appendix 2. The risk of bias assessment for all included studies can be viewed in gure 2 .
The types of surgeries performed included major shoulder surgery, 71 rotator cu surgery, 73 arthroscopic shoulder surgery, 76
hip arthroscopy, 70 total knee arthroplasty, 74 video-assisted tho-racoscopic surgery, 75 minimally invasive lung resection, 77
in atable penile prosthesis placement, 78 and total mastectomy. 72
The details of the peripheral nerve blocks techniques used are summarized in table 2 . The blocks included interscalene nerve block, 71 , 73 , 76 adductor canal block, 74 intercostal nerve block, 75 , 77
dorsal penile block, 78 fascia iliaca block, 70 and pectoralis myo-fascial plane block. 72 The volume and dose of perineural lipo-somal bupivacaine ranged from 10 to 40 ml and 88 to 266 mg, respectively; one trial did not specify the dose used. 77 All stud-ies compared the use of perineural liposomal bupivacaine to plain long-acting local anesthetic bupivacaine 70 – 77 or ropiva-caine 78 ; three studies 70 , 71 , 73 had additional study arms that mixed liposomal bupivacaine with plain bupivacaine.
Primary Outcome
AUC of Rest Pain over 24 to 72 h . Across 24 to 72 h, 70 – 74 , 76 –
78 the mean di erence (95% CI) in AUC of rest pain was found to be 1.0 cm · h (0.5 to 1.6; P = 0.003) in favor of
ALNV134N2_Text.indb 150ALNV134N2_Text.indb 150 29-Dec-20 19:43:0529-Dec-20 19:43:05
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
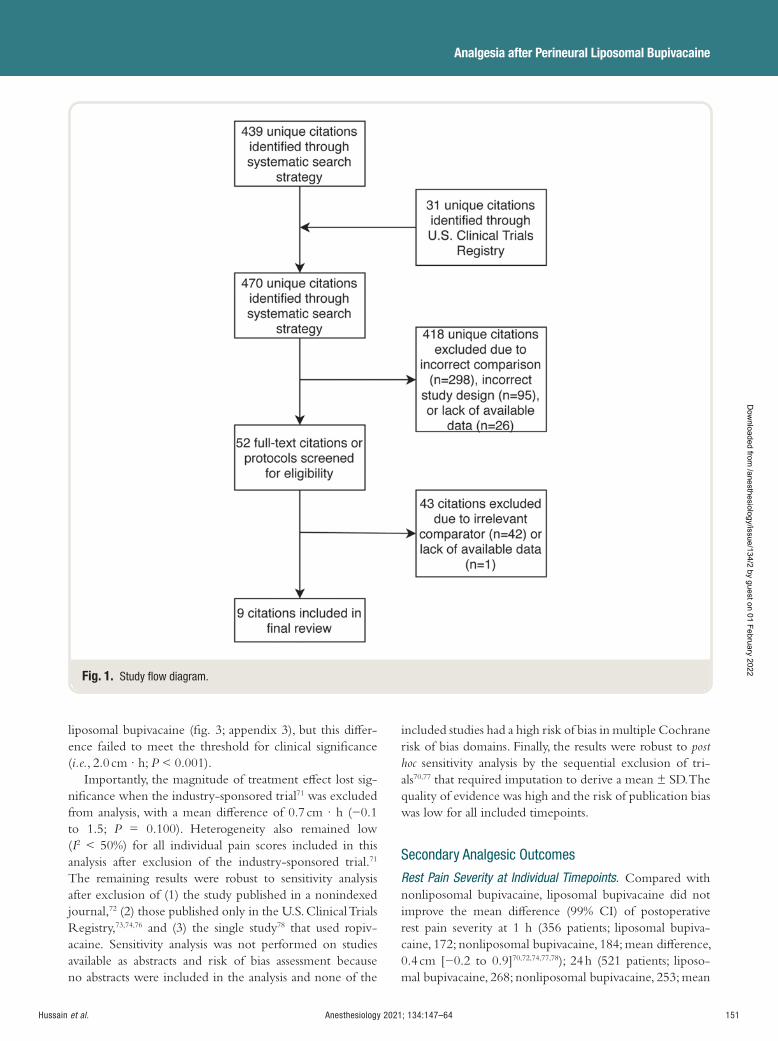
Anesthesiology 2021; 134:147–64 151
Analgesia after Perineural Liposomal Bupivacaine
Hussain et al .
liposomal bupivacaine ( g. 3 ; appendix 3), but this di er-ence failed to meet the threshold for clinical signi cance ( i.e. , 2.0 cm · h; P < 0.001).
Importantly, the magnitude of treatment e ect lost sig-ni cance when the industry-sponsored trial 71 was excluded from analysis, with a mean di erence of 0.7 cm · h ( − 0.1 to 1.5; P = 0.100). Heterogeneity also remained low ( I 2 < 50%) for all individual pain scores included in this analysis after exclusion of the industry-sponsored trial. 71
The remaining results were robust to sensitivity analysis after exclusion of (1) the study published in a nonindexed journal, 72 (2) those published only in the U.S. Clinical Trials Registry, 73 , 74 , 76 and (3) the single study 78 that used ropiv-acaine. Sensitivity analysis was not performed on studies available as abstracts and risk of bias assessment because no abstracts were included in the analysis and none of the
included studies had a high risk of bias in multiple Cochrane risk of bias domains. Finally, the results were robust to post hoc sensitivity analysis by the sequential exclusion of tri-als 70,77 that required imputation to derive a mean ± SD. The quality of evidence was high and the risk of publication bias was low for all included timepoints.
Secondary Analgesic Outcomes
Rest Pain Severity at Individual Timepoints . Compared with nonliposomal bupivacaine, liposomal bupivacaine did not improve the mean di erence (99% CI) of postoperative rest pain severity at 1 h (356 patients; liposomal bupiva-caine, 172; nonliposomal bupivacaine, 184; mean di erence, 0.4 cm [ − 0.2 to 0.9] 70 , 72 , 74 , 77 , 78 ); 24 h (521 patients; liposo-mal bupivacaine, 268; nonliposomal bupivacaine, 253; mean
Fig. 1. Study fl ow diagram.
ALNV134N2_Text.indb 151ALNV134N2_Text.indb 151 29-Dec-20 19:43:0529-Dec-20 19:43:05
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
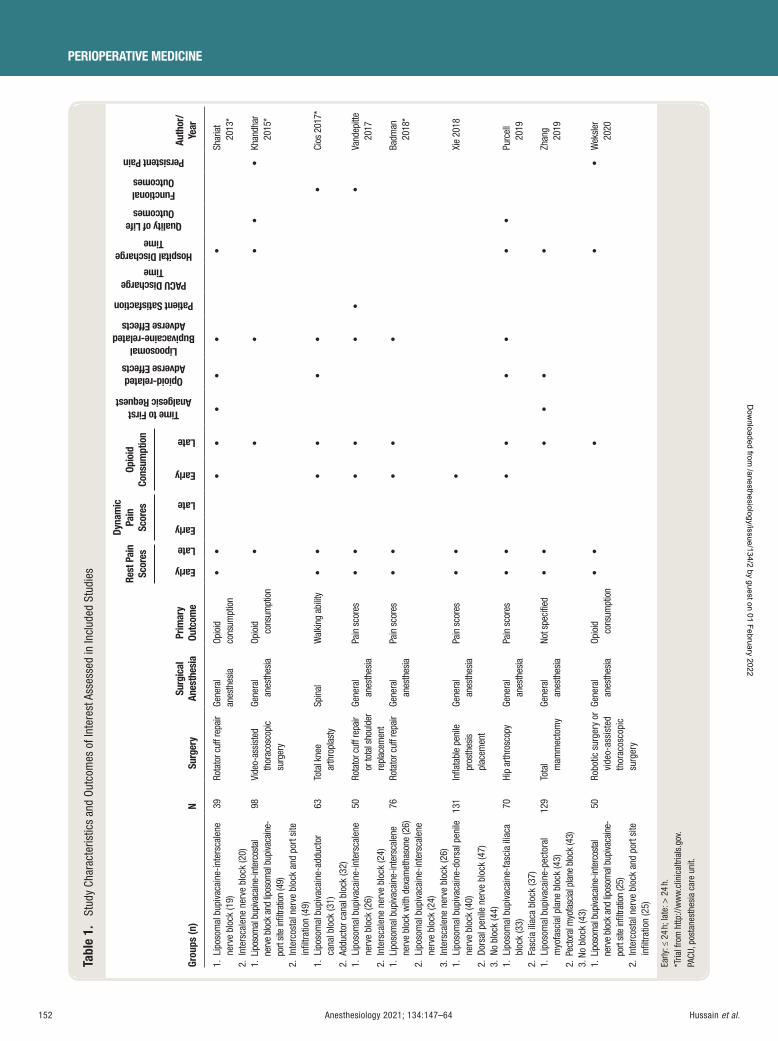
152 Anesthesiology 2021; 134:147–64
PERIOPERATIVE MEDICINE
Hussain et al .
Tabl
e 1.
St
udy
Char
acte
ristic
s an
d Ou
tcom
es o
f Int
eres
t Ass
esse
d in
Incl
uded
Stu
dies
Grou
ps (n
) N
Surg
ery
Surg
ical
An
esth
esia
Pr
imar
y Ou
tcom
e
Rest
Pai
n Sc
ores
Dyna
mic
Pa
in
Scor
es
Opio
id
Cons
umpt
ion
Time to First Analgesic Request
Opioid-related Adverse Effects
Lipoosomal Bupivacaine-related
Adverse Effects
Patient Satisfaction
PACU Discharge Time
Hospital Discharge Time
Quality of Life Outcomes
Functional Outcomes
Persistent Pain
Auth
or/
Year
Early
Late
Early
Late
Early
Late
1. L
ipos
omal
bup
ivac
aine
-inte
rsca
lene
ne
rve
bloc
k (1
9)
2. I
nter
scal
ene
nerv
e bl
ock
(20)
39
Rota
tor c
uff r
epai
r Ge
nera
l an
esth
esia
Op
ioid
co
nsum
ptio
n •
•
•
• •
• •
•
Shar
iat
2013
*
1. L
ipos
omal
bup
ivaca
ine-
inte
rcos
tal
nerv
e bl
ock
and
lipos
omal
bup
ivaca
ine-
port
site
infi l
tratio
n (4
9)
2. I
nter
cost
al n
erve
blo
ck a
nd p
ort s
ite
infi l
tratio
n (4
9)
98
Vide
o-as
sist
ed
thor
acos
copi
c su
rger
y
Gene
ral
anes
thes
ia
Opio
id
cons
umpt
ion
•
•
•
•
•
• Kh
andh
ar
2015
*
1. L
ipos
omal
bup
ivac
aine
-add
ucto
r ca
nal b
lock
(31)
2.
Add
ucto
r can
al b
lock
(32)
63
Tota
l kne
e ar
thro
plas
ty
Spin
al
Wal
king
abi
lity
• •
• •
•
•
•
Ci
os 2
017 *
1. L
ipos
omal
bup
ivac
aine
-inte
rsca
lene
ne
rve
bloc
k (2
6)
2. I
nter
scal
ene
nerv
e bl
ock
(24)
50
Rota
tor c
uff r
epai
r or
tota
l sho
ulde
r re
plac
emen
t
Gene
ral
anes
thes
ia
Pain
sco
res
• •
• •
• •
•
Va
ndep
itte
2017
1. L
ipos
omal
bup
ivac
aine
-inte
rsca
lene
ne
rve
bloc
k w
ith d
exam
etha
sone
(26)
2.
Lip
osom
al b
upiv
acai
ne-in
ters
cale
ne
nerv
e bl
ock
(24)
3.
Int
ersc
alen
e ne
rve
bloc
k (2
6)
76
Rota
tor c
uff r
epai
r Ge
nera
l an
esth
esia
Pa
in s
core
s •
•
•
•
•
Badm
an
2018
*
1. L
ipos
omal
bup
ivac
aine
-dor
sal p
enile
ne
rve
bloc
k (4
0)
2. D
orsa
l pen
ile n
erve
blo
ck (4
7)
3. N
o bl
ock
(44)
131
Infl a
tabl
e pe
nile
pr
osth
esis
pl
acem
ent
Gene
ral
anes
thes
ia
Pain
sco
res
• •
•
Xi
e 20
18
1. L
ipos
omal
bup
ivac
aine
-fas
cia
iliac
a bl
ock
(33)
2.
Fas
cia
iliac
a bl
ock
(37)
70
Hip
arth
rosc
opy
Gene
ral
anes
thes
ia
Pain
sco
res
• •
• •
•
•
•
•
Pu
rcel
l 20
19
1. L
ipos
omal
bup
ivac
aine
-pec
tora
l m
yofa
scia
l pla
ne b
lock
(43)
2.
Pec
tora
l myo
fasc
ial p
lane
blo
ck (4
3)
3. N
o bl
ock
(43)
129
Tota
l mam
mec
tom
y Ge
nera
l an
esth
esia
No
t spe
cifi e
d •
•
• •
•
•
Zhan
g 20
19
1. L
ipos
omal
bup
ivaca
ine-
inte
rcos
tal
nerv
e bl
ock
and
lipos
omal
bup
ivaca
ine-
port
site
infi l
tratio
n (2
5)
2. I
nter
cost
al n
erve
blo
ck a
nd p
ort s
ite
infi l
tratio
n (2
5)
50
Robo
tic s
urge
ry o
r vi
deo-
assi
sted
th
orac
osco
pic
surg
ery
Gene
ral
anes
thes
ia
Opio
id
cons
umpt
ion
• •
•
•
• W
eksl
er
2020
Early
: ≤ 2
4 h;
late
: > 2
4 h.
* T
rial f
rom
http
://w
ww
.clin
ical
trial
s.go
v . PA
CU, p
osta
nest
hesi
a ca
re u
nit.
ALNV134N2_Text.indb 152ALNV134N2_Text.indb 152 29-Dec-20 19:43:0629-Dec-20 19:43:06
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
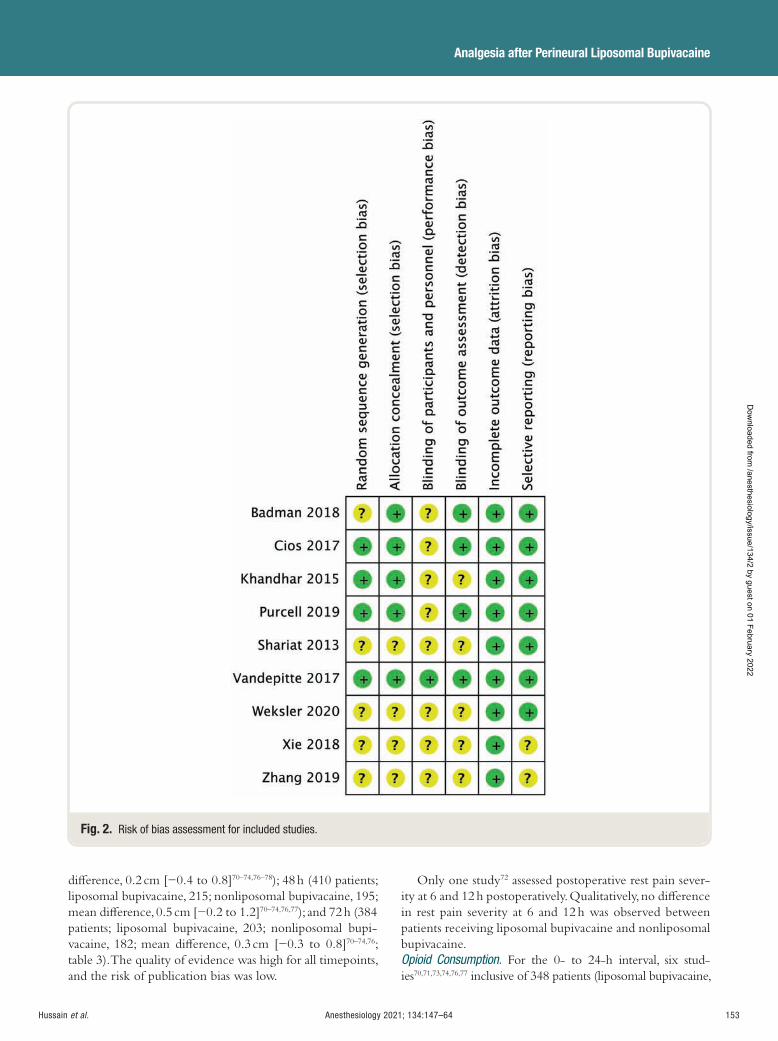
Anesthesiology 2021; 134:147–64 153
Analgesia after Perineural Liposomal Bupivacaine
Hussain et al .
di erence, 0.2 cm [ − 0.4 to 0.8] 70 – 74 , 76 – 78 ); 48 h (410 patients; liposomal bupivacaine, 215; nonliposomal bupivacaine, 195; mean di erence, 0.5 cm [ − 0.2 to 1.2] 70 – 74 , 76 ,77 ); and 72 h (384 patients; liposomal bupivacaine, 203; nonliposomal bupi-vacaine, 182; mean di erence, 0.3 cm [ − 0.3 to 0.8] 70 – 74 , 76 ; table 3 ). The quality of evidence was high for all timepoints, and the risk of publication bias was low.
Only one study 72 assessed postoperative rest pain sever-ity at 6 and 12 h postoperatively. Qualitatively, no di erence in rest pain severity at 6 and 12 h was observed between patients receiving liposomal bupivacaine and nonliposomal bupivacaine. Opioid Consumption . For the 0- to 24-h interval, six stud-ies 70 , 71 , 73 , 74 , 76 , 77 inclusive of 348 patients (liposomal bupivacaine,
Fig. 2. Risk of bias assessment for included studies.
ALNV134N2_Text.indb 153ALNV134N2_Text.indb 153 29-Dec-20 19:43:0629-Dec-20 19:43:06
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
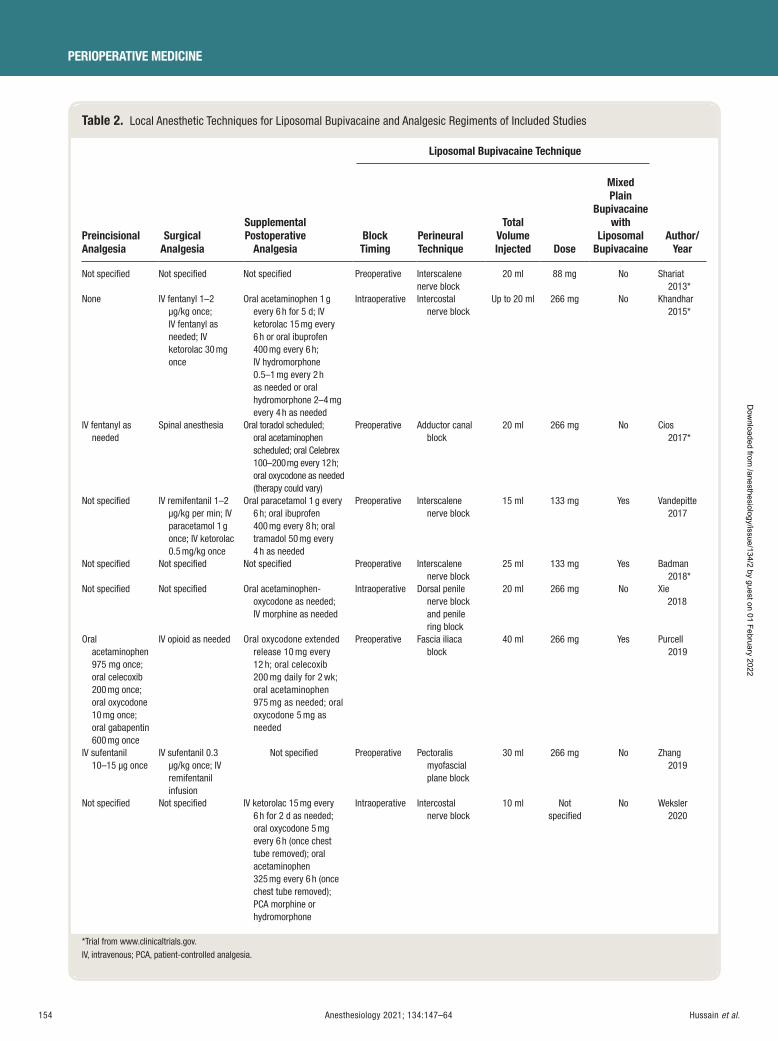
154 Anesthesiology 2021; 134:147–64
PERIOPERATIVE MEDICINE
Hussain et al .
Table 2. Local Anesthetic Techniques for Liposomal Bupivacaine and Analgesic Regiments of Included Studies
Preincisional Analgesia
Surgical Analgesia
Supplemental Postoperative
Analgesia
Liposomal Bupivacaine Technique
Author/Year
Block Timing
Perineural Technique
Total Volume Injected Dose
Mixed Plain
Bupivacaine with
Liposomal Bupivacaine
Not specifi ed Not specifi ed Not specifi ed Preoperative Interscalene nerve block
20 ml 88 mg No Shariat 2013 *
None IV fentanyl 1 – 2 μ g/kg once; IV fentanyl as needed; IV ketorolac 30 mg once
Oral acetaminophen 1 g every 6 h for 5 d; IV ketorolac 15 mg every 6 h or oral ibuprofen 400 mg every 6 h; IV hydromorphone 0.5 – 1 mg every 2 h as needed or oral hydromorphone 2 – 4 mg every 4 h as needed
Intraoperative Intercostal nerve block
Up to 20 ml 266 mg No Khandhar 2015 *
IV fentanyl as needed
Spinal anesthesia Oral toradol scheduled; oral acetaminophen scheduled; oral Celebrex 100 – 200 mg every 12 h; oral oxycodone as needed (therapy could vary)
Preoperative Adductor canal block
20 ml 266 mg No Cios 2017 *
Not specifi ed IV remifentanil 1 – 2 μg/kg per min; IV paracetamol 1 g once; IV ketorolac 0.5 mg/kg once
Oral paracetamol 1 g every 6 h; oral ibuprofen 400 mg every 8 h; oral tramadol 50 mg every 4 h as needed
Preoperative Interscalene nerve block
15 ml 133 mg Yes Vandepitte 2017
Not specifi ed Not specifi ed Not specifi ed Preoperative Interscalene nerve block
25 ml 133 mg Yes Badman 2018 *
Not specifi ed Not specifi ed Oral acetaminophen-oxycodone as needed; IV morphine as needed
Intraoperative Dorsal penile nerve block and penile ring block
20 ml 266 mg No Xie 2018
Oral acetaminophen 975 mg once; oral celecoxib 200 mg once; oral oxycodone 10 mg once; oral gabapentin 600 mg once
IV opioid as needed Oral oxycodone extended release 10 mg every 12 h; oral celecoxib 200 mg daily for 2 wk; oral acetaminophen 975 mg as needed; oral oxycodone 5 mg as needed
Preoperative Fascia iliaca block
40 ml 266 mg Yes Purcell 2019
IV sufentanil 10 – 15 μ g once
IV sufentanil 0.3 μ g/kg once; IV remifentanil infusion
Not specifi ed Preoperative Pectoralis myofascial plane block
30 ml 266 mg No Zhang 2019
Not specifi ed Not specifi ed IV ketorolac 15 mg every 6 h for 2 d as needed; oral oxycodone 5 mg every 6 h (once chest tube removed); oral acetaminophen 325 mg every 6 h (once chest tube removed); PCA morphine or hydromorphone
Intraoperative Intercostal nerve block
10 ml Not specifi ed
No Weksler 2020
* Trial from www.clinicaltrials.gov . IV, intravenous; PCA, patient-controlled analgesia.
ALNV134N2_Text.indb 154ALNV134N2_Text.indb 154 29-Dec-20 19:43:0629-Dec-20 19:43:06
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
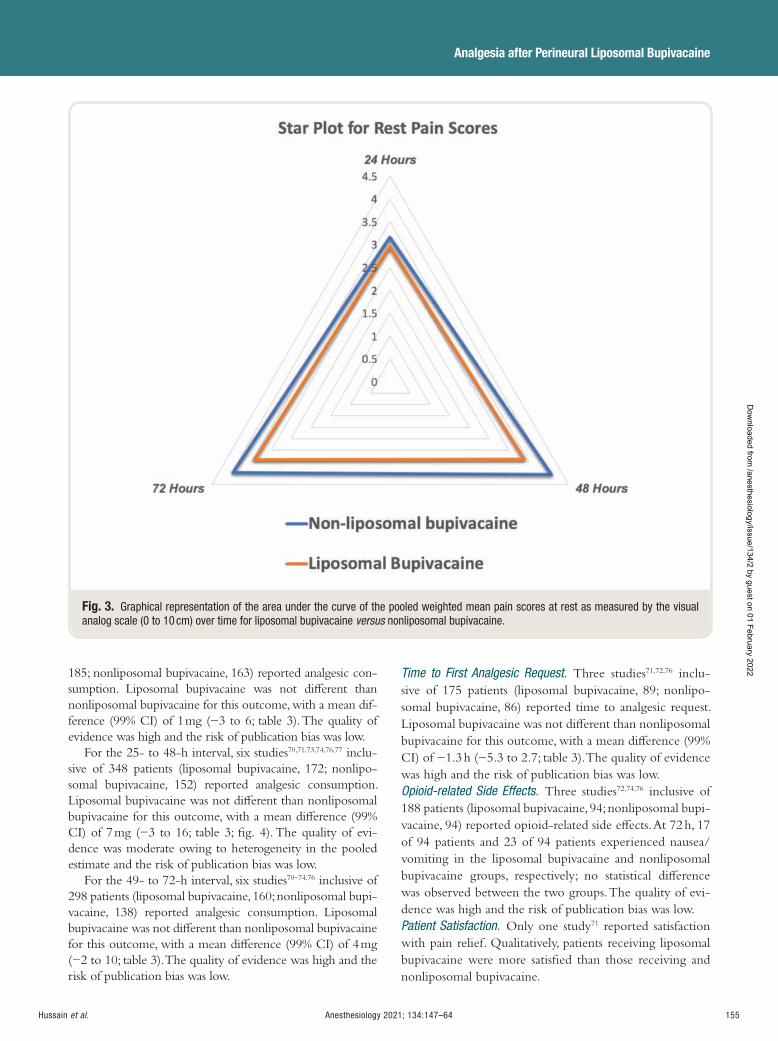
Anesthesiology 2021; 134:147–64 155
Analgesia after Perineural Liposomal Bupivacaine
Hussain et al .
185; nonliposomal bupivacaine, 163) reported analgesic con-sumption. Liposomal bupivacaine was not di erent than nonliposomal bupivacaine for this outcome, with a mean dif-ference (99% CI) of 1 mg ( − 3 to 6; table 3 ). The quality of evidence was high and the risk of publication bias was low.
For the 25- to 48-h interval, six studies 70 , 71 , 73 , 74 , 76 , 77 inclu-sive of 348 patients (liposomal bupivacaine, 172; nonlipo-somal bupivacaine, 152) reported analgesic consumption. Liposomal bupivacaine was not di erent than nonliposomal bupivacaine for this outcome, with a mean di erence (99% CI) of 7 mg ( − 3 to 16; table 3 ; g. 4 ). The quality of evi-dence was moderate owing to heterogeneity in the pooled estimate and the risk of publication bias was low.
For the 49- to 72-h interval, six studies 70 – 74 , 76 inclusive of 298 patients (liposomal bupivacaine, 160; nonliposomal bupi-vacaine, 138) reported analgesic consumption. Liposomal bupivacaine was not di erent than nonliposomal bupivacaine for this outcome, with a mean di erence (99% CI) of 4 mg ( − 2 to 10; table 3 ). The quality of evidence was high and the risk of publication bias was low.
Time to First Analgesic Request . Three studies 71 , 72 , 76 inclu-sive of 175 patients (liposomal bupivacaine, 89; nonlipo-somal bupivacaine, 86) reported time to analgesic request. Liposomal bupivacaine was not di erent than nonliposomal bupivacaine for this outcome, with a mean di erence (99% CI) of − 1.3 h ( − 5.3 to 2.7; table 3 ). The quality of evidence was high and the risk of publication bias was low. Opioid-related Side Effects . Three studies 72 , 74 , 76 inclusive of 188 patients (liposomal bupivacaine, 94; nonliposomal bupi-vacaine, 94) reported opioid-related side e ects. At 72 h, 17 of 94 patients and 23 of 94 patients experienced nausea/vomiting in the liposomal bupivacaine and nonliposomal bupivacaine groups, respectively; no statistical di erence was observed between the two groups. The quality of evi-dence was high and the risk of publication bias was low. Patient Satisfaction . Only one study 71 reported satisfaction with pain relief. Qualitatively, patients receiving liposomal bupivacaine were more satis ed than those receiving and nonliposomal bupivacaine.
Fig. 3. Graphical representation of the area under the curve of the pooled weighted mean pain scores at rest as measured by the visual analog scale (0 to 10 cm) over time for liposomal bupivacaine versus nonliposomal bupivacaine.
ALNV134N2_Text.indb 155ALNV134N2_Text.indb 155 29-Dec-20 19:43:0729-Dec-20 19:43:07
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
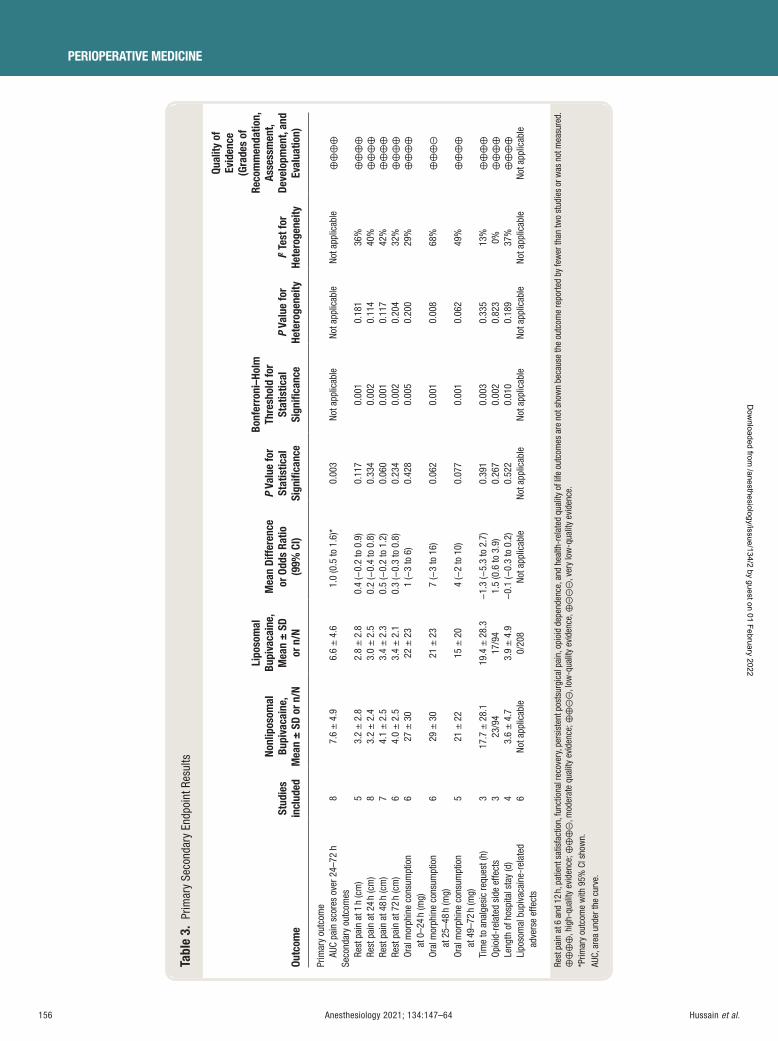
156 Anesthesiology 2021; 134:147–64
PERIOPERATIVE MEDICINE
Hussain et al .
Tabl
e 3.
Prim
ary
Seco
ndar
y En
dpoi
nt R
esul
ts
Outc
ome
Stud
ies
incl
uded
Nonl
ipos
omal
Bu
piva
cain
e,
Mea
n ±
SD
or n
/N
Lipo
som
al
Bupi
vaca
ine,
M
ean
± S
D or
n/N
Mea
n Di
ffere
nce
or O
dds
Ratio
(9
9% C
I)
P Va
lue
for
Stat
istic
al
Sign
ifi ca
nce
Bonf
erro
ni – H
olm
Th
resh
old
for
Stat
istic
al
Sign
ifi ca
nce
P Va
lue
for
Hete
roge
neity
I 2 T
est f
or
Hete
roge
neity
Qual
ity o
f Ev
iden
ce
(Gra
des
of
Reco
mm
enda
tion,
As
sess
men
t, De
velo
pmen
t, an
d Ev
alua
tion)
Prim
ary
outc
ome
AUC
pain
sco
res
over
24 –
72 h
8
7.6
± 4
.9
6.6
± 4
.6
1.0
(0.5
to 1
.6) *
0.
003
Not a
pplic
able
No
t app
licab
le
Not a
pplic
able
⊕
⊕ ⊕
⊕
Seco
ndar
y ou
tcom
es
Rest
pai
n at
1 h
(cm
) 5
3.2
± 2
.8
2.8
± 2
.8
0.4
( − 0.
2 to
0.9
) 0.
117
0.00
1 0.
181
36%
⊕
⊕ ⊕
⊕
Re
st p
ain
at 2
4 h
(cm
) 8
3.2
± 2
.4
3.0
± 2
.5
0.2
( − 0.
4 to
0.8
) 0.
334
0.00
2 0.
114
40%
⊕
⊕ ⊕
⊕
Re
st p
ain
at 4
8 h
(cm
) 7
4.1
± 2
.5
3.4
± 2
.3
0.5
( − 0.
2 to
1.2
) 0.
060
0.00
1 0.
117
42%
⊕
⊕ ⊕
⊕
Re
st p
ain
at 7
2 h
(cm
) 6
4.0
± 2
.5
3.4
± 2
.1
0.3
( − 0.
3 to
0.8
) 0.
234
0.00
2 0.
204
32%
⊕
⊕ ⊕
⊕
Or
al m
orph
ine
cons
umpt
ion
at 0
– 24
h (m
g)
6 27
± 3
0 22
± 2
3 1
( − 3
to 6
) 0.
428
0.00
5 0.
200
29%
⊕
⊕ ⊕
⊕
Or
al m
orph
ine
cons
umpt
ion
at 2
5 – 48
h (m
g)
6 29
± 3
0 21
± 2
3 7
( − 3
to 1
6)
0.06
2 0.
001
0.00
8 68
%
⊕ ⊕
⊕ ⊝
Or
al m
orph
ine
cons
umpt
ion
at 4
9 – 72
h (m
g)
5 21
± 2
2 15
± 2
0 4
( − 2
to 1
0)
0.07
7 0.
001
0.06
2 49
%
⊕ ⊕
⊕ ⊕
Ti
me
to a
nalg
esic
requ
est (
h)
3 17
.7 ±
28.
1 19
.4 ±
28.
3 −
1.3
( − 5.
3 to
2.7
) 0.
391
0.00
3 0.
335
13%
⊕
⊕ ⊕
⊕
Op
ioid
-rel
ated
sid
e ef
fect
s 3
23/9
4 17
/94
1.5
(0.6
to 3
.9)
0.26
7 0.
002
0.82
3 0%
⊕
⊕ ⊕
⊕
Le
ngth
of h
ospi
tal s
tay
(d)
4 3.
6 ±
4.7
3.
9 ±
4.9
−
0.1
( − 0.
3 to
0.2
) 0.
522
0.01
0 0.
189
37%
⊕
⊕ ⊕
⊕
Li
poso
mal
bup
ivac
aine
-rel
ated
ad
vers
e ef
fect
s 6
Not a
pplic
able
0/
208
Not a
pplic
able
No
t app
licab
le
Not a
pplic
able
No
t app
licab
le
Not a
pplic
able
No
t app
licab
le
Rest
pai
n at
6 a
nd 1
2 h,
pat
ient
sat
isfa
ctio
n, fu
nctio
nal r
ecov
ery,
pers
iste
nt p
osts
urgi
cal p
ain,
opi
oid
depe
nden
ce, a
nd h
ealth
-rel
ated
qua
lity
of li
fe o
utco
mes
are
not
sho
wn
beca
use
the
outc
ome
repo
rted
by fe
wer
than
two
stud
ies
or w
as n
ot m
easu
red.
⊕
⊕ ⊕
⊕ , h
igh-
qual
ity e
vide
nce;
⊕ ⊕
⊕ ⊝
, mod
erat
e qu
ality
evi
denc
e; ⊕
⊕ ⊝
⊝ , lo
w-q
ualit
y ev
iden
ce, ⊕
⊝ ⊝
⊝ , v
ery
low
-qua
lity
evid
ence
. * P
rimar
y ou
tcom
e w
ith 9
5% C
I sho
wn.
AU
C, a
rea
unde
r the
cur
ve.
ALNV134N2_Text.indb 156ALNV134N2_Text.indb 156 29-Dec-20 19:43:0729-Dec-20 19:43:07
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
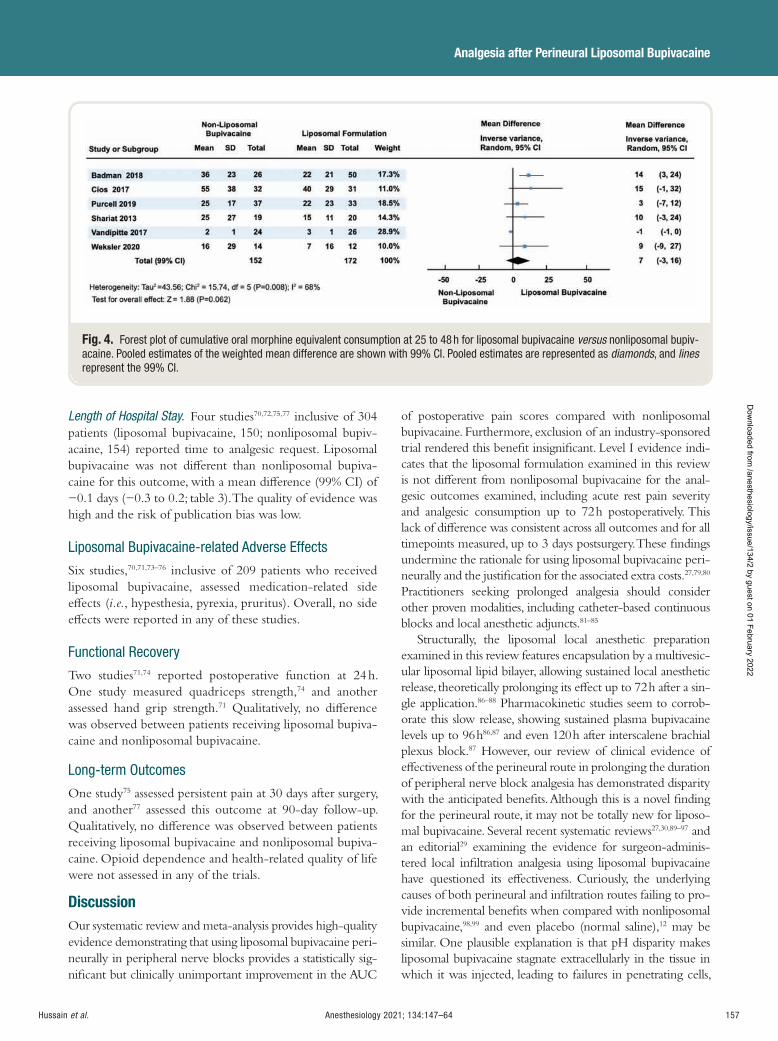
Anesthesiology 2021; 134:147–64 157
Analgesia after Perineural Liposomal Bupivacaine
Hussain et al .
Length of Hospital Stay . Four studies 70 , 72 , 75 , 77 inclusive of 304 patients (liposomal bupivacaine, 150; nonliposomal bupiv-acaine, 154) reported time to analgesic request. Liposomal bupivacaine was not di erent than nonliposomal bupiva-caine for this outcome, with a mean di erence (99% CI) of − 0.1 days ( − 0.3 to 0.2; table 3 ). The quality of evidence was high and the risk of publication bias was low.
Liposomal Bupivacaine-related Adverse Effects
Six studies, 70 , 71 , 73 – 76 inclusive of 209 patients who received liposomal bupivacaine, assessed medication-related side e ects ( i.e. , hypesthesia, pyrexia, pruritus). Overall, no side e ects were reported in any of these studies.
Functional Recovery
Two studies 71 , 74 reported postoperative function at 24 h. One study measured quadriceps strength, 74 and another assessed hand grip strength. 71 Qualitatively, no di erence was observed between patients receiving liposomal bupiva-caine and nonliposomal bupivacaine.
Long-term Outcomes
One study 75 assessed persistent pain at 30 days after surgery, and another 77 assessed this outcome at 90-day follow-up. Qualitatively, no di erence was observed between patients receiving liposomal bupivacaine and nonliposomal bupiva-caine. Opioid dependence and health-related quality of life were not assessed in any of the trials.
Discussion Our systematic review and meta-analysis provides high-quality evidence demonstrating that using liposomal bupivacaine peri-neurally in peripheral nerve blocks provides a statistically sig-ni cant but clinically unimportant improvement in the AUC
of postoperative pain scores compared with nonliposomal bupivacaine. Furthermore, exclusion of an industry-sponsored trial rendered this bene t insigni cant. Level I evidence indi-cates that the liposomal formulation examined in this review is not di erent from nonliposomal bupivacaine for the anal-gesic outcomes examined, including acute rest pain severity and analgesic consumption up to 72 h postoperatively. This lack of di erence was consistent across all outcomes and for all timepoints measured, up to 3 days postsurgery. These ndings undermine the rationale for using liposomal bupivacaine peri-neurally and the justi cation for the associated extra costs. 27 , 79 , 80
Practitioners seeking prolonged analgesia should consider other proven modalities, including catheter-based continuous blocks and local anesthetic adjuncts. 81 – 85
Structurally, the liposomal local anesthetic preparation examined in this review features encapsulation by a multivesic-ular liposomal lipid bilayer, allowing sustained local anesthetic release, theoretically prolonging its e ect up to 72 h after a sin-gle application. 86 – 88 Pharmacokinetic studies seem to corrob-orate this slow release, showing sustained plasma bupivacaine levels up to 96 h 86 , 87 and even 120 h after interscalene brachial plexus block. 87 However, our review of clinical evidence of e ectiveness of the perineural route in prolonging the duration of peripheral nerve block analgesia has demonstrated disparity with the anticipated bene ts. Although this is a novel nding for the perineural route, it may not be totally new for liposo-mal bupivacaine. Several recent systematic reviews 27 , 30 , 89 – 97 and an editorial 29 examining the evidence for surgeon-adminis-tered local in ltration analgesia using liposomal bupivacaine have questioned its e ectiveness. Curiously, the underlying causes of both perineural and in ltration routes failing to pro-vide incremental bene ts when compared with nonliposomal bupivacaine, 98 , 99 and even placebo (normal saline), 12 may be similar. One plausible explanation is that pH disparity makes liposomal bupivacaine stagnate extracellularly in the tissue in which it was injected, leading to failures in penetrating cells,
Fig. 4. Forest plot of cumulative oral morphine equivalent consumption at 25 to 48 h for liposomal bupivacaine versus nonliposomal bupiv-acaine. Pooled estimates of the weighted mean difference are shown with 99% CI. Pooled estimates are represented as diamonds , and lines represent the 99% CI.
ALNV134N2_Text.indb 157ALNV134N2_Text.indb 157 29-Dec-20 19:43:0729-Dec-20 19:43:07
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

158 Anesthesiology 2021; 134:147–64
PERIOPERATIVE MEDICINE
Hussain et al .
interrupting signal transmission, and providing analgesia. As bupivacaine makes its initial contact with the tissue in which it is injected, it triggers a localized in ammatory response 100
that renders the medium acidotic, 101 impeding further tissue penetration by the subsequent bupivacaine molecules that are slowly released from the lipid-based depots (DepoFoam; Pacira Pharmaceuticals, USA). 102 Thus, local anesthetic-induced in ammatory changes may be the main reason that liposomal bupivacaine was unable to surpass the clinical e ectiveness of nonliposomal bupivacaine.
Our review comes with several strengths. First, our sys-temic search strategy was exhaustive and captured both published and ongoing studies from the U.S. Clinical Trials Registry. Second, all estimates of e ect were of high quality and characterized by low levels of heterogeneity, strength-ening the internal validity of this review. Third, although a Cochrane review has addressed this topic in 2017, 30 we were able to provide readers with additional results for out-comes that have not been previously investigated because of a lack of data, such as AUC of pain analysis and analge-sic consumption at 48 and 72 h postoperatively. Fourth, we presented 99% CI for all secondary outcomes to reduce the risk of type I error and multiple testing bias. Finally, the sen-sitivity analysis, by excluding the industry-sponsored trial, seems to have successfully eliminated bias, as the excluded data in uenced the initial analysis toward a robust bene t favoring perineural liposomal bupivacaine.
Our review also comes with notable limitations. First, we investigated perineural liposomal bupivacaine across a variety of surgical procedures and block techniques. This could potentially limit the external validity of our results and limit their broad applicability; nonetheless, the low level of statistical heterogeneity disputes this possibility. Second, the choice of AUC for pain severity scores as a primary outcome limited our ability to perform additional ancillary analyses, such as meta-regression, to investigate the impact of potentially relevant covariates on the estimate of e ect. In addition, AUC analysis may be more prone to bias given that a signi cant di erence is more likely to be detected than in individual timepoint analysis. Nonetheless, analysis of individual timepoints was con rmatory of the ndings. Third, variabilities in the analgesic regimens used in the included studies may have played a confounding e ect. Fourth, we cannot exclude the possibility of publication bias, because we did not include unpublished negative trials or missing studies. Finally, owing to scarcity of data, we were unable to statistically evaluate clinically important long-term outcomes such as pain-related disability, persistent pain, opioid-dependence, and health-related quality of life.
Conclusions
Used perineurally in peripheral nerve blocks, liposomal bupivacaine provides a clinically unimportant improve-ment in the AUC of postoperative pain scores compared with nonliposomal bupivacaine. Furthermore, excluding an
industry-sponsored trial rendered this bene t insigni cant. We also found liposomal bupivacaine to be not di erent from nonliposomal bupivacaine for all other analgesic and func-tional outcomes. High-quality evidence does not support the use of perineural liposomal bupivacaine over nonliposomal bupivacaine for peripheral nerve blocks.
Acknowledgments
The authors thank Laura Ban eld, M.L.S., Ph.D. (Health Sciences Library, McMaster University, Hamilton, Ontario, Canada), for creating the search strategy for this meta-analysis.
Research Support
Support for this study was provided solely from institutional and/or departmental sources.
Competing Interests
Dr. Essandoh is a consultant for Boston Scienti c (Marlborough, Massachusetts) and S4 Medical (Cleveland, Ohio). Dr. Weaver is a consultant for Medtronic (Dublin, Ireland). The remaining authors declare no competing interests.
Correspondence
Address correspondence to Dr. Abdallah: Department of Anesthesiology and Pain Medicine, University of Toronto, North York General Hospital, 4001 Leslie St., Toronto, ON M2K 1E1, Canada. [email protected] . This article may be accessed for personal use at no charge through the Journal Web site, www.anesthesiology.org.
References
1. Knudson RA , Dunlavy PW , Franko J , Raman SR , Kraemer SR : E ectiveness of liposomal bupivacaine in colorectal surgery: A pragmatic nonsponsored prospec-tive randomized double blinded trial in a community hospital. Dis Colon Rectum 2016 ; 59 : 862 – 9
2. Ma P , Lloyd A , McGrath M , Shuchleib Cung A , Akusoba I , Jackson A , Swartz D , Boone K , Higa K : E cacy of liposomal bupivacaine versus bupivacaine in port site injections on postoperative pain within enhanced recov-ery after bariatric surgery program: A randomized clini-cal trial. Surg Obes Relat Dis 2019 ; 15 : 1554 – 62
3. Motakef S , Wong WW , Ingargiola MJ , Nguyen D , Galdyn IA , Kim HY , Gupta SC : Liposomal bupivacaine in implant-based breast reconstruction. Plast Reconstr Surg Glob Open 2017 ; 5 : e1559
4. Nadeau MH , Saraswat A , Vasko A , Elliott JO , Vasko SD : Bupivacaine versus liposomal bupivacaine for postop-erative pain control after augmentation mammaplasty: A prospective, randomized, double-blind trial. Aesthet Surg J 2016 ; 36 : NP47 – 52
ALNV134N2_Text.indb 158ALNV134N2_Text.indb 158 29-Dec-20 19:43:0729-Dec-20 19:43:07
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:147–64 159
Analgesia after Perineural Liposomal Bupivacaine
Hussain et al .
5. Evans SKL , Abimbola O , Myers EM , Tarr ME : A novel injection technique for extended-release local anes-thetic after posterior colporrhaphy and perineorrha-phy : A randomized controlled study. Female Pelvic Med Reconstr Surg 2020 [Epub ahead of print]
6. Propst K , O ’ Sullivan DM , Steinberg AC : Randomized double-blind trial of short- versus long-acting analgesia at the sacrospinous ligament. Int Urogynecol J 2019 ; 30 : 123 – 30
7. Barron KI , Lamvu GM , Schmidt RC , Fisk M , Blanton E , Patanwala I : Wound in ltration with extended-re-lease versus short-acting bupivacaine before laparo-scopic hysterectomy: A randomized controlled trial. J Minim Invasive Gynecol 2017 ; 24 : 286 – 92
8. Iwano C , Salamon C : Liposomal bupivacaine ver-sus bupivacaine hydrochloride with lidocaine during midurethral sling placement: A randomized controlled trial. J Minim Invasive Gynecol 2019 ; 26 : 1133 – 8
9. Iero PT , Mulherin DR , Jensen O , Berry T , Danesi H , Razook SJ : A prospective, randomized, open-label study comparing an opioid-sparing postsurgical pain management protocol with and without liposomal bupivacaine for full-arch implant surgery. Int J Oral Maxillofac Implants 2018 ; 33 : 1155 – 64
10. Glenn B , Drum M , Reader A , Fowler S , Nusstein J , Beck M : Does liposomal bupivacaine (Exparel) sig-ni cantly reduce postoperative pain/numbness in symptomatic teeth with a diagnosis of necrosis? A pro-spective, randomized, double-blind trial. J Endod 2016 ; 42 : 1301 – 6
11. Bultema K , Fowler S , Drum M , Reader A , Nusstein J , Beck M : Pain reduction in untreated symptomatic irre-versible pulpitis using liposomal bupivacaine (Exparel): A prospective, randomized, double-blind trial. J Endod 2016 ; 42 : 1707 – 12
12. Prabhu M , Clapp MA , McQuaid-Hanson E , Ona S , O ’ Donnell T , James K , Bateman BT , Wylie BJ , Barth WH Jr : Liposomal bupivacaine block at the time of cesarean delivery to decrease postoperative pain: A randomized controlled trial. Obstet Gynecol 2018 ; 132 : 70 – 8
13. Gor ne SR , Onel E , Patou G , Krivokapic ZV : Bupivacaine extended-release liposome injection for prolonged postsurgical analgesia in patients undergo-ing hemorrhoidectomy: A multicenter, randomized, double-blind, placebo-controlled trial. Dis Colon Rectum 2011 ; 54 : 1552 – 9
14. Haas E , Onel E , Miller H , Ragupathi M , White PF : A double-blind, randomized, active-controlled study for post-hemorrhoidectomy pain management with lipo-some bupivacaine, a novel local analgesic formulation. Am Surg 2012 ; 78 : 574 – 81
15. Johnson RL , Amundson AW , Abdel MP , Sviggum HP , Mabry TM , Mantilla CB , Schroeder DR , Pagnano MW , Kopp SL : Continuous posterior lumbar plexus
nerve block versus periarticular injection with ropiv-acaine or liposomal bupivacaine for total hip arthro-plasty: A three-arm randomized clinical trial. J Bone Joint Surg Am 2017 ; 99 : 1836 – 45
16. Perets I , Walsh JP , Mu BH , Yuen LC , Ashberg L , Battaglia MR , Domb BG : Intraoperative in ltration of liposomal bupivacaine vs bupivacaine hydrochloride for pain management in primary total hip arthroplasty: A prospective randomized trial. J Arthroplasty 2018 ; 33 : 441 – 6
17. Alter TH , Liss FE , Ilyas AM : A prospective random-ized study comparing bupivacaine hydrochloride versus bupivacaine liposome for pain management after distal radius fracture repair surgery. J Hand Surg Am 2017 ; 42 : 1003 – 8
18. Dale EL , Kluemper CT , Cowart SJ , Jemison M , Kennedy JW , Gao L , Brzezienski MA , Rehm J : Bupivacaine extended-release liposomal injection versus bupiva-caine HCl for early postoperative pain control follow-ing wrist operations: A prospective, randomized control trial. J Hand Surg Am 2020 ; 45 : 550.e1 – 8
19. Gatherwright J , Knackstedt RW , Ghaznavi AM , Bernard S , Schwarz G , Moreira A , Gurunluoglu R , Djohan R : Prospective, randomized, controlled com-parison of bupivacaine versus liposomal bupivacaine for pain management after unilateral delayed deep infe-rior epigastric perforator free ap reconstruction. Plast Reconstr Surg 2018 ; 141 : 1327 – 30
20. Hutchins JL , Kesha R , Blanco F , Dunn T , Hochhalter R : Ultrasound-guided subcostal transversus abdominis plane blocks with liposomal bupivacaine vs . non-li-posomal bupivacaine for postoperative pain control after laparoscopic hand-assisted donor nephrectomy: A prospective randomised observer-blinded study. Anaesthesia 2016 ; 71 : 930 – 7
21. Wong KA , Cabrera AG , Argiro AL , Pechman DM , Parides MK , Vazzana JT , Moran-Atkin EM , Choi JJ , Camacho DR : Transversus abdominis plane block with liposomal bupivacaine and its e ect on opiate use after weight loss surgery: A randomized controlled trial. Surg Obes Relat Dis 2020 ; 16 : 886 – 93
22. Ha AY , Keane G , Parikh R , Odom E , Tao Y , Zhang L , Myckatyn TM , Gu ey R : The analgesic e ects of liposomal bupivacaine versus bupivacaine hydrochlo-ride administered as a transversus abdominis plane block after abdominally based autologous microvas-cular breast reconstruction: A prospective, single-blind, randomized, controlled trial. Plast Reconstr Surg 2019 ; 144 : 35 – 44
23. Hutchins J , Delaney D , Vogel RI , Ghebre RG , Downs LS Jr , Carson L , Mullany S , Teoh D , Geller MA : Ultrasound guided subcostal transversus abdominis plane (TAP) in ltration with liposomal bupivacaine for patients undergoing robotic assisted hysterectomy:
ALNV134N2_Text.indb 159ALNV134N2_Text.indb 159 29-Dec-20 19:43:0729-Dec-20 19:43:07
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
160 Anesthesiology 2021; 134:147–64
PERIOPERATIVE MEDICINE
Hussain et al .
A prospective randomized controlled study. Gynecol Oncol 2015 ; 138 : 609 – 13
24. Gasanova I , Alexander J , Ogunnaike B , Hamid C , Rogers D , Minhajuddin A , Joshi GP : Transversus abdominis plane block versus surgical site in ltration for pain management after open total abdominal hys-terectomy. Anesth Analg 2015 ; 121 : 1383 – 8
25. Hutchins J , Argenta P , Berg A , Habeck J , Kaizer A , Geller MA : Ultrasound-guided subcostal transversus abdominis plane block with liposomal bupivacaine compared to bupivacaine in ltration for patients undergoing robot-ic-assisted and laparoscopic hysterectomy: A prospective randomized study. J Pain Res 2019 ; 12 : 2087 – 94
26. Bramlett K , Onel E , Viscusi ER , Jones K : A randomized, double-blind, dose-ranging study comparing wound in ltration of DepoFoam bupivacaine, an extended-re-lease liposomal bupivacaine, to bupivacaine HCl for postsurgical analgesia in total knee arthroplasty. Knee 2012 ; 19 : 530 – 6
27. Abildgaard JT , Chung AS , Tokish JM , Hattrup SJ : Clinical e cacy of liposomal bupivacaine: A systematic review of prospective, randomized controlled trials in orthopaedic surgery. JBJS Rev 2019 ; 7 : e8
28. US Food and Drug Administration, Center for Drug Evaluation and Research: EXPAREL NDA 022496 Approval letter. 2013. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2011/022496Orig1s000Approv.pdf . Accessed May 2, 2020.
29. Ilfeld BM , Gabriel RA , Eisenach JC : Liposomal bupiva-caine in ltration for knee arthroplasty: Signi cant anal-gesic bene ts or just a bunch of fat? A nesthesiology 2018 ; 129 : 623 – 6
30. Hamilton TW , Athanassoglou V , Mellon S , Strickland LH , Trivella M , Murray D , Pandit HG : Liposomal bupi-vacaine in ltration at the surgical site for the manage-ment of postoperative pain. Cochrane Database Syst Rev 2017 ; 2 : CD011419
31. Moher D , Liberati A , Tetzla J , Altman DG ; PRISMA Group : Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J Clin Epidemiol 2009 ; 62 : 1006 – 12
32. Higgins JP , Altman DG , G ø tzsche PC , J ü ni P , Moher D , Oxman AD , Savovic J , Schulz KF , Weeks L , Sterne JA ; Cochrane Bias Methods Group; Cochrane Statistical Methods Group : The Cochrane Collaboration ’ s tool for assessing risk of bias in randomised trials. BMJ 2011 ; 343 : d5928
33. Guyatt GH , Oxman AD , Kunz R , Falck-Ytter Y , Vist GE , Liberati A , Sch ü nemann HJ ; GRADE Working Group : Going from evidence to recommendations. BMJ 2008 ; 336 : 1049 – 51
34. Guyatt G , Oxman AD , Akl EA , Kunz R , Vist G , Brozek J , Norris S , Falck-Ytter Y , Glasziou P , DeBeer H , Jaeschke R , Rind D , Meerpohl J , Dahm P , Sch ü nemann HJ : GRADE guidelines: 1. Introduction-GRADE
evidence pro les and summary of ndings tables. J Clin Epidemiol 2011 ; 64 : 383 – 94
35. Mont MA , Beaver WB , Dysart SH , Barrington JW , Del Gaizo DJ : Local in ltration analgesia with liposomal bupivacaine improves pain scores and reduces opioid use after total knee arthroplasty: Results of a random-ized controlled trial. J Arthroplasty 2018 ; 33 : 90 – 6
36. Ilfeld BM , Viscusi ER , Hadzic A , Minkowitz HS , Morren MD , Lookabaugh J , Joshi GP : Safety and side e ect pro le of liposome bupivacaine (Exparel) in peripheral nerve blocks. Reg Anesth Pain Med 2015 ; 40 : 572 – 82
37. Breivik EK , Bj ö rnsson GA , Skovlund E : A comparison of pain rating scales by sampling from clinical trial data. Clin J Pain 2000 ; 16 : 22 – 8
38. Thorlund K , Walter SD , Johnston BC , Furukawa TA , Guyatt GH : Pooling health-related quality of life out-comes in meta-analysis-a tutorial and review of meth-ods for enhancing interpretability. Res Synth Methods 2011 ; 2 : 188 – 203
39. Canadian Pharmacists Association: Compendium of Pharmaceuticals and Specialties: The Canadian Drug Reference for Health Professionals , 45th edition . Ottawa, Canada , Canadian Pharmacists Assoc . , 2010
40. Wan X , Wang W , Liu J , Tong T : Estimating the sam-ple mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 2014 ; 14 : 135
41. Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0. Hoboken, New Jersey, The Cochrane Collaboration, 2011.
42. Furukawa TA , Barbui C , Cipriani A , Brambilla P , Watanabe N : Imputing missing standard deviations in meta-analyses can provide accurate results. J Clin Epidemiol 2006 ; 59 : 7 – 10
43. Moore A , McQuay H , Gavaghan D : Deriving dichot-omous outcome measures from continuous data in randomised controlled trials of analgesics. Pain 1996 ; 66 : 229 – 37
44. S á nchez-Meca J , Mar í n-Mart í nez F , Chac ó n-Moscoso S : E ect-size indices for dichotomized outcomes in meta-analysis. Psychol Methods 2003 ; 8 : 448 – 67
45. Murad MH , Wang Z , Chu H , Lin L : When contin-uous outcomes are measured using di erent scales: Guide for meta-analysis and interpretation. BMJ 2019 ; 364 : k4817
46. DerSimonian R , Laird N : Meta-analysis in clinical tri-als. Control Clin Trials 1986 ; 7 : 177 – 88
47. Holm S : A simple sequentially rejective multiple test procedure. Scand J Stat 1979 ; 6 : 65 – 70
48. Myles PS , Myles DB , Galagher W , Boyd D , Chew C , MacDonald N , Dennis A : Measuring acute postoper-ative pain using the visual analog scale: the minimal clinically important di erence and patient acceptable symptom state. Br J Anaesth 2017 ; 118 : 424 – 9
ALNV134N2_Text.indb 160ALNV134N2_Text.indb 160 29-Dec-20 19:43:0729-Dec-20 19:43:07
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:147–64 161
Analgesia after Perineural Liposomal Bupivacaine
Hussain et al .
49. Cheung BW , Cartier LL , Russlie HQ , Sawchuk RJ : The application of sample pooling methods for determining AUC, AUMC and mean residence times in pharmacoki-netic studies. Fundam Clin Pharmacol 2005 ; 19 : 347 – 54
50. Abdallah FW , MacLean D , Madjdpour C , Cil T , Bhatia A , Brull R : Pectoralis and serratus fascial plane blocks each provide early analgesic bene ts following ambulatory breast cancer surgery: A retrospective propensity-matched cohort study. Anesth Analg 2017 ; 125 : 294 – 302
51. Egger M , Davey Smith G , Schneider M , Minder C : Bias in meta-analysis detected by a simple, graphical test. BMJ 1997 ; 315 : 629 – 34
52. Nair S : 0.25% Bupivacaine versus a mixture of 0.25% bupivacaine and 1.3% liposomal bupivacaine in patients undergoing Tka , 2017 . Available at: https://clinicaltrials.gov/ct2/show/NCT03303794 . Accessed May 2, 2020.
53. Premkumar A , Samady H , Slone H , Hash R , Karas S , Xerogeanes J : Liposomal bupivacaine for pain control after anterior cruciate ligament reconstruction: A pro-spective, double-blinded, randomized, positive-con-trolled trial. Am J Sports Med 2016 ; 44 : 1680 – 6
54. Marino J , Scuderi G , Dowling O , Farquhar R , Freycinet B , Overdyk F : Periarticular knee injection with liposomal bupivacaine and continuous femoral nerve block for postoperative pain management after total knee arthroplasty: A randomized controlled trial. J Arthroplasty 2019 ; 34 : 495 – 500
55. Okoroha KR , Lynch JR , Keller RA , Korona J , Amato C , Rill B , Kolowich PA , Muh SJ : Liposomal bupiva-caine versus interscalene nerve block for pain control after shoulder arthroplasty: A prospective randomized trial. J Shoulder Elbow Surg 2016 ; 25 : 1742 – 8
56. Sober ó n JR Jr , Ericson-Neilsen W , Sisco-Wise LE , Gasta ñ aduy M , Beck DE : Perineural liposomal bupi-vacaine for postoperative pain control in patients undergoing upper extremity orthopedic surgery: A prospective and randomized pilot study. Ochsner J 2016 ; 16 : 436 – 42
57. Sabesan VJ , Shahriar R , Petersen-Fitts GR , Whaley JD , Bou-Akl T , Sweet M , Milia M : A prospective ran-domized controlled trial to identify the optimal post-operative pain management in shoulder arthroplasty: Liposomal bupivacaine versus continuous interscalene catheter. J Shoulder Elbow Surg 2017 ; 26 : 1810 – 7
58. Namdari S , Nicholson T , Abboud J , Lazarus M , Steinberg D , Williams G : Interscalene block with and without intraoperative local in ltration with lipo-somal bupivacaine in shoulder arthroplasty: A ran-domized controlled trial. J Bone Joint Surg Am 2018 ; 100 : 1373 – 8
59. Namdari S , Nicholson T , Abboud J , Lazarus M , Steinberg D , Williams G : Randomized controlled trial of interscalene block compared with injectable liposo-mal bupivacaine in shoulder arthroplasty. J Bone Joint Surg Am 2017 ; 99 : 550 – 6
60. Abildgaard JT , Lonergan KT , Tolan SJ , Kissenberth MJ , Hawkins RJ , Washburn R 3 rd , Adams KJ , Long CD , Shealy EC , Motley JR , Tokish JM : Liposomal bupiv-acaine versus indwelling interscalene nerve block for postoperative pain control in shoulder arthroplasty: A prospective randomized controlled trial. J Shoulder Elbow Surg 2017 ; 26 : 1175 – 81
61. Sethi PM , Brameier DT , Mandava NK , Miller SR : Liposomal bupivacaine reduces opiate consumption after rotator cu repair in a randomized controlled trial. J Shoulder Elbow Surg 2019 ; 28 : 819 – 27
62. McGraw-Tatum MA , Groover MT , George NE , Urse JS , Heh V : A prospective, randomized trial comparing liposomal bupivacaine vs fascia iliaca compartment block for postoperative pain control in total hip arthro-plasty. J Arthroplasty 2017 ; 32 : 2181 – 5
63. Okoroha KR , Keller RA , Marshall NE , Jung EK , Mehran N , Owashi E , Moutzouros V : Liposomal bupi-vacaine versus femoral nerve block for pain control after anterior cruciate ligament reconstruction: A prospec-tive randomized trial. Arthroscopy 2016 ; 32 : 1838 – 45
64. Surdam JW , Licini DJ , Baynes NT , Arce BR : The use of Exparel (liposomal bupivacaine) to manage postopera-tive pain in unilateral total knee arthroplasty patients. J Arthroplasty 2015 ; 30 : 325 – 9
65. Talmo CT , Kent SE , Fredette AN , Anderson MC , Hassan MK , Mattingly DA : Prospective randomized trial com-paring femoral nerve block with intraoperative local anesthetic injection of liposomal bupivacaine in total knee arthroplasty. J Arthroplasty 2018 ; 33 : 3474 – 8
66. Felling DR , Jackson MW , Ferraro J , Battaglia MA , Albright JJ , Wu J , Genord CK , Brockhaus KK , Bhave RA , McClure AM , Shanker BA , Cleary RK : Liposomal bupivacaine transversus abdominis plane block ver-sus epidural analgesia in a colon and rectal surgery enhanced recovery pathway: A randomized clinical trial. Dis Colon Rectum 2018 ; 61 : 1196 – 204
67. Torgeson M , Kileny J , Pfeifer C , Narkiewicz L , Obi S : Conventional epidural vs transversus abdominis plane block with liposomal bupivacaine: A randomized trial in colorectal surgery. J Am Coll Surg 2018 ; 227 : 78 – 83
68. Colibaseanu DT , Osagiede O , Merchea A , Ball CT , Bojaxhi E , Panchamia JK , Jacob AK , Kelley SR , Naessens JM , Larson DW : Randomized clinical trial of liposomal bupivacaine transverse abdominis plane block versus intrathecal analgesia in colorectal surgery. Br J Surg 2019 ; 106 : 692 – 9
69. Sethi P : Interscalene block with and without liposo-mal bupivacaine in shoulder surgery, 2018. Available at: https://clinicaltrials.gov/ct2/show/NCT03728946 . Accessed May 2, 2020.
70. Purcell RL , Brooks DI , Steelman TJ , Christensen DL , Dickens JF , Kent ML , McCabe MP , Anderson TD : Fascia iliaca blockade with the addition of liposomal bupiv-acaine versus plain bupivacaine for perioperative pain
ALNV134N2_Text.indb 161ALNV134N2_Text.indb 161 29-Dec-20 19:43:0729-Dec-20 19:43:07
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
162 Anesthesiology 2021; 134:147–64
PERIOPERATIVE MEDICINE
Hussain et al .
management during hip arthroscopy: A double-blinded prospective randomized control trial. Arthroscopy 2019 ; 35 : 2608 – 16
71. Vandepitte C , Kuroda M , Witvrouw R , Anne L , Bellemans J , Corten K , Vanelderen P , Mesotten D , Leunen I , Heylen M , Van Boxstael S , Golebiewski M , Van de Velde M , Knezevic NN , Hadzic A : Addition of liposome bupivacaine to bupivacaine HCl versus bupiv-acaine HCl alone for interscalene brachial plexus block in patients having major shoulder surgery. Reg Anesth Pain Med 2017 ; 42 : 334 – 41
72. Zhang L , Jiyong L , Chen Z : The postoperative analge-sia e ect of liposome bupivacaine ultrasound-guided PECS blockade after total mammectomy. J Pract Med 2019 ; 35 : 3214 – 3217
73. Badman B : Single shot liposomal bupivacaine in rotator cu surgery, 2018. Available at: https://clinicaltrials.gov/ct2/show/NCT03822182 . Accessed May 2, 2020.
74. Cios H : Liposomal bupivacaine versus standard bupiv-acaine in the adductor canal for total knee arthroplasty, 2017. Available at: https://clinicaltrials.gov/ct2/show/NCT03182933 . Accessed May 2, 2020.
75. Khandhar S : Pain management in response to Exparel vs . standard bupivacaine (VATS Exparel), 2015. Available at: https://clinicaltrials.gov/ct2/show/NCT02499159 . Accessed May 2, 2020.
76. Shariat A : E cacy of interscalene brachial plexus block with liposomal bupivacaine for arthroscopic shoulder surgery, 2013. Available at: https://clinicaltrials.gov/ct2/show/NCT01977352 . Accessed May 2, 2020.
77. Weksler B , Sullivan JL , Schumacher LY : Randomized trial of bupivacaine with epinephrine versus bupivacaine liposome suspension in patients undergoing minimally invasive lung resection . J Thorac Cardiovasc Surg 2020 [Epub ahead of print]
78. Xie D , Nicholson M , Azaiza M , Gheiler V , Lopez I , Nehrenz GM , Klopukh B , Bianco FJ , Perito P , Gheiler E : E ect of operative local anesthesia on postoperative pain outcomes of in atable penile prosthesis: Prospective comparison of two medications. Int J Impot Res 2018 ; 30 : 93 – 6
79. Alijanipour P , Tan TL , Matthews CN , Viola JR , Purtill JJ , Rothman RH , Parvizi J , Austin MS : Periarticular injection of liposomal bupivacaine o ers no bene t over standard bupivacaine in total knee arthroplasty: A prospective, ran-domized, controlled trial. J Arthroplasty 2017 ; 32 : 628 – 34
80. Amundson AW , Johnson RL , Abdel MP , Mantilla CB , Panchamia JK , Taunton MJ , Kralovec ME , Hebl JR , Schroeder DR , Pagnano MW , Kopp SL : A three-arm randomized clinical trial comparing continuous femo-ral plus single-injection sciatic peripheral nerve blocks versus periarticular injection with ropivacaine or lipo-somal bupivacaine for patients undergoing total knee arthroplasty. A nesthesiology 2017 ; 126 : 1139 – 50
81. Hussain N , Grzywacz VP , Ferreri CA , Atrey A , Ban eld L , Shaparin N , Vydyanathan A : Investigating the
e cacy of dexmedetomidine as an adjuvant to local anesthesia in brachial plexus block: A systematic review and meta-analysis of 18 randomized controlled trials. Reg Anesth Pain Med 2017 ; 42 : 184 – 96
82. Abdallah FW , Brull R : Facilitatory e ects of perineural dexmedetomidine on neuraxial and peripheral nerve block: A systematic review and meta-analysis. Br J Anaesth 2013 ; 110 : 915 – 25
83. Albrecht E , Vorobeichik L , Jacot-Guillarmod A , Fournier N , Abdallah FW : Dexamethasone is superior to dexmedetomidine as a perineural adjunct for supra-clavicular brachial plexus block: Systematic review and indirect meta-analysis. Anesth Analg 2019 ; 128 : 543 – 54
84. Hussain N , Van den Langenbergh T , Sermer C , Fontes ML , Atrey A , Shaparin N , Sawyer TR , Vydyanathan A : Equivalent analgesic e ectiveness between perineu-ral and intravenous dexamethasone as adjuvants for peripheral nerve blockade: A systematic review and meta-analysis. Can J Anaesth 2018 ; 65 : 194 – 206
85. Sun C , Zhang X , Song F , Zhao Z , Du R , Wu S , Ma Q , Cai X : Is continuous catheter adductor canal block better than single-shot canal adductor canal block in primary total knee arthroplasty?: A GRADE analy-sis of the evidence through a systematic review and meta-analysis. Medicine (Baltimore) 2020 ; 99 : e20320
86. Prabhakar A , Ward CT , Watson M , Sanford J , Fiza B , Moll V , Kaye RJ , Morgan Hall O , Cornett EM , Urman RD , Kaye AD : Liposomal bupivacaine and novel local anesthetic formulations. Best Pract Res Clin Anaesthesiol 2019 ; 33 : 425 – 32
87. Pharmaceuticals P : EXPAREL (bupivacaine lipo-some injectable suspension) [Highlights of Prescribing information] . San Diego, California, 2018. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/022496s9lbl.pdf . Accessed May 7, 2020.
88. Ilfeld BM : Liposome bupivacaine in peripheral nerve blocks and epidural injections to manage postoperative pain. Expert Opin Pharmacother 2013 ; 14 : 2421 – 31
89. Cao X , Pan F : Comparison of liposomal bupiva-caine in ltration versus interscalene nerve block for pain control in total shoulder arthroplasty: A meta-analysis of randomized control trails. Medicine (Baltimore) 2017 ; 96 : e8079
90. Kolade O , Patel K , Ihejirika R , Press D , Friedlander S , Roberts T , Rokito AS , Virk MS : E cacy of lipo-somal bupivacaine in shoulder surgery: A systematic review and meta-analysis. J Shoulder Elbow Surg 2019 ; 28 : 1824 – 34
91. Ma TT , Wang YH , Jiang YF , Peng CB , Yan C , Liu ZG , Xu WX : Liposomal bupivacaine versus tradi-tional bupivacaine for pain control after total hip arthroplasty: A meta-analysis. Medicine (Baltimore) 2017 ; 96 : e7190
92. Ma J , Zhang W , Yao S : Liposomal bupivacaine in l-tration versus femoral nerve block for pain control
ALNV134N2_Text.indb 162ALNV134N2_Text.indb 162 29-Dec-20 19:43:0729-Dec-20 19:43:07
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
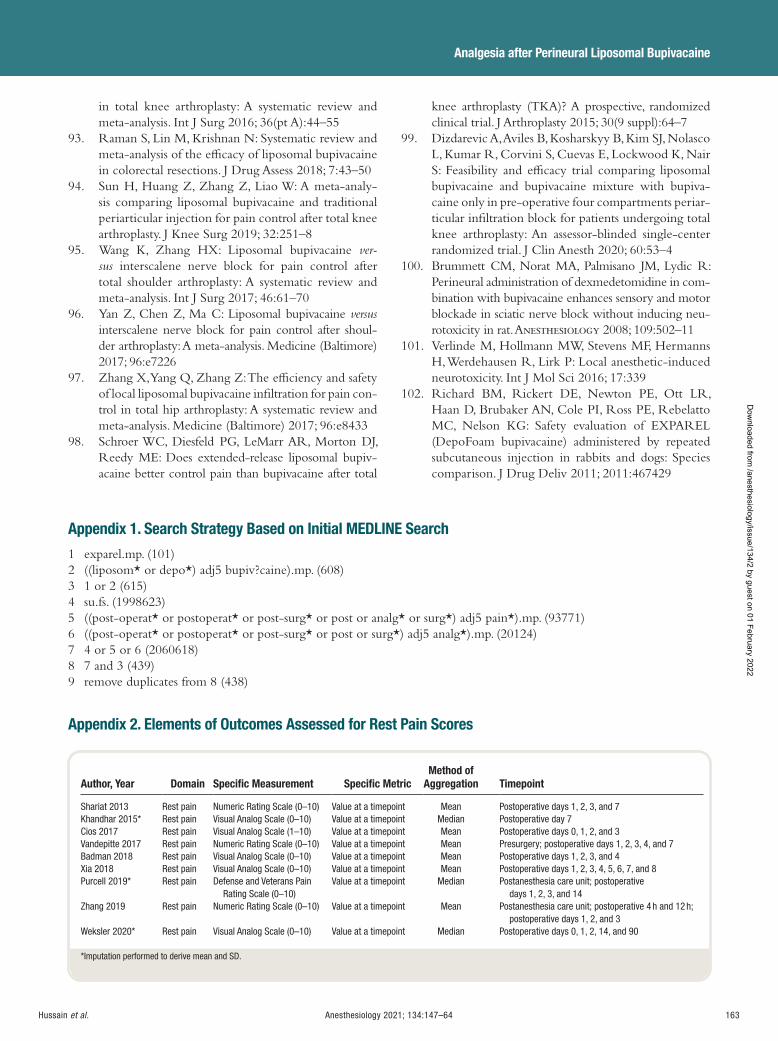
Anesthesiology 2021; 134:147–64 163
Analgesia after Perineural Liposomal Bupivacaine
Hussain et al .
in total knee arthroplasty: A systematic review and meta-analysis. Int J Surg 2016 ; 36 ( pt A ): 44 – 55
93. Raman S , Lin M , Krishnan N : Systematic review and meta-analysis of the e cacy of liposomal bupivacaine in colorectal resections. J Drug Assess 2018 ; 7 : 43 – 50
94. Sun H , Huang Z , Zhang Z , Liao W : A meta-analy-sis comparing liposomal bupivacaine and traditional periarticular injection for pain control after total knee arthroplasty. J Knee Surg 2019 ; 32 : 251 – 8
95. Wang K , Zhang HX : Liposomal bupivacaine ver-sus interscalene nerve block for pain control after total shoulder arthroplasty: A systematic review and meta-analysis. Int J Surg 2017 ; 46 : 61 – 70
96. Yan Z , Chen Z , Ma C : Liposomal bupivacaine versus interscalene nerve block for pain control after shoul-der arthroplasty: A meta-analysis. Medicine (Baltimore) 2017 ; 96 : e7226
97. Zhang X , Yang Q , Zhang Z : The e ciency and safety of local liposomal bupivacaine in ltration for pain con-trol in total hip arthroplasty: A systematic review and meta-analysis. Medicine (Baltimore) 2017 ; 96 : e8433
98. Schroer WC , Diesfeld PG , LeMarr AR , Morton DJ , Reedy ME : Does extended-release liposomal bupiv-acaine better control pain than bupivacaine after total
knee arthroplasty (TKA)? A prospective, randomized clinical trial. J Arthroplasty 2015 ; 30 ( 9 suppl ): 64 – 7
99. Dizdarevic A , Aviles B , Kosharskyy B , Kim SJ , Nolasco L , Kumar R , Corvini S , Cuevas E , Lockwood K , Nair S : Feasibility and e cacy trial comparing liposomal bupivacaine and bupivacaine mixture with bupiva-caine only in pre-operative four compartments periar-ticular in ltration block for patients undergoing total knee arthroplasty: An assessor-blinded single-center randomized trial. J Clin Anesth 2020 ; 60 : 53 – 4
100. Brummett CM , Norat MA , Palmisano JM , Lydic R : Perineural administration of dexmedetomidine in com-bination with bupivacaine enhances sensory and motor blockade in sciatic nerve block without inducing neu-rotoxicity in rat. A nesthesiology 2008 ; 109 : 502 – 11
101. Verlinde M , Hollmann MW , Stevens MF , Hermanns H , Werdehausen R , Lirk P : Local anesthetic-induced neurotoxicity. Int J Mol Sci 2016 ; 17 : 339
102. Richard BM , Rickert DE , Newton PE , Ott LR , Haan D , Brubaker AN , Cole PI , Ross PE , Rebelatto MC , Nelson KG : Safety evaluation of EXPAREL (DepoFoam bupivacaine) administered by repeated subcutaneous injection in rabbits and dogs: Species comparison. J Drug Deliv 2011 ; 2011 : 467429
Appendix 1. Search Strategy Based on Initial MEDLINE Search
1 exparel.mp. (101) 2 ((liposom * or depo * ) adj5 bupiv?caine).mp. (608) 3 1 or 2 (615) 4 su.fs. (1998623) 5 ((post-operat * or postoperat * or post-surg * or post or analg * or surg * ) adj5 pain * ).mp. (93771) 6 ((post-operat * or postoperat * or post-surg * or post or surg * ) adj5 analg * ).mp. (20124) 7 4 or 5 or 6 (2060618) 8 7 and 3 (439) 9 remove duplicates from 8 (438)
Appendix 2. Elements of Outcomes Assessed for Rest Pain Scores
Author, Year Domain Specifi c Measurement Specifi c Metric Method of
Aggregation Timepoint
Shariat 2013 Rest pain Numeric Rating Scale (0 – 10) Value at a timepoint Mean Postoperative days 1, 2, 3, and 7 Khandhar 2015 * Rest pain Visual Analog Scale (0 – 10) Value at a timepoint Median Postoperative day 7 Cios 2017 Rest pain Visual Analog Scale (1 – 10) Value at a timepoint Mean Postoperative days 0, 1, 2, and 3 Vandepitte 2017 Rest pain Numeric Rating Scale (0 – 10) Value at a timepoint Mean Presurgery; postoperative days 1, 2, 3, 4, and 7 Badman 2018 Rest pain Visual Analog Scale (0 – 10) Value at a timepoint Mean Postoperative days 1, 2, 3, and 4 Xia 2018 Rest pain Visual Analog Scale (0 – 10) Value at a timepoint Mean Postoperative days 1, 2, 3, 4, 5, 6, 7, and 8 Purcell 2019 * Rest pain Defense and Veterans Pain
Rating Scale (0 – 10) Value at a timepoint Median Postanesthesia care unit; postoperative
days 1, 2, 3, and 14 Zhang 2019 Rest pain Numeric Rating Scale (0 – 10) Value at a timepoint Mean Postanesthesia care unit; postoperative 4 h and 12 h;
postoperative days 1, 2, and 3 Weksler 2020 * Rest pain Visual Analog Scale (0 – 10) Value at a timepoint Median Postoperative days 0, 1, 2, 14, and 90
* Imputation performed to derive mean and SD.
ALNV134N2_Text.indb 163ALNV134N2_Text.indb 163 29-Dec-20 19:43:0829-Dec-20 19:43:08
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
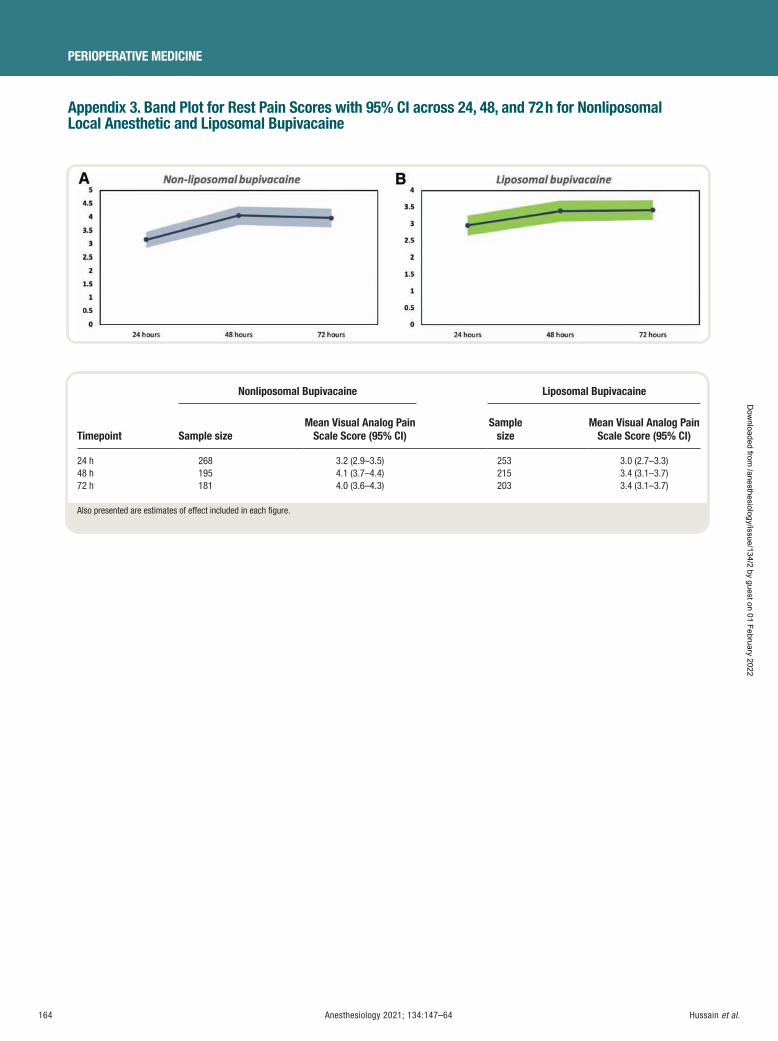
164 Anesthesiology 2021; 134:147–64
PERIOPERATIVE MEDICINE
Hussain et al .
Appendix 3. Band Plot for Rest Pain Scores with 95% CI across 24, 48, and 72 h for Nonliposomal Local Anesthetic and Liposomal Bupivacaine
Timepoint
Nonliposomal Bupivacaine Liposomal Bupivacaine
Sample size Mean Visual Analog Pain
Scale Score (95% CI) Sample
size Mean Visual Analog Pain
Scale Score (95% CI)
24 h 268 3.2 (2.9 – 3.5) 253 3.0 (2.7 – 3.3) 48 h 195 4.1 (3.7 – 4.4) 215 3.4 (3.1 – 3.7) 72 h 181 4.0 (3.6 – 4.3) 203 3.4 (3.1 – 3.7)
Also presented are estimates of effect included in each fi gure.
ALNV134N2_Text.indb 164ALNV134N2_Text.indb 164 29-Dec-20 19:43:0829-Dec-20 19:43:08
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
PERIOPERATIVE MEDICINE
ANESTHESIOLOGY, V 134 • NO 2 FEBRUARY 2021 165
EDITOR ’ S PERSPECTIVE
What We Already Know about This Topic
• Tranexamic acid is an antifibrinolytic agent that reduces postopera-tive blood loss and rates of erythrocyte transfusion and rethoracot-omy in cardiopulmonary bypass surgery
• There appears to be a dose – response relationship between tranexamic acid and the risk of postoperative seizure
• Model-based meta-analysis is an extension of traditional meta-anal-ysis that includes parametric models to describe the effect of dose
What This Article Tells Us That Is New
• This model-based meta-analysis found that low-dose tranexamic acid (total dose, approximately 20 mg/kg) was sufficient to reduce postoperative blood loss and erythrocyte transfusion in cardiopul-monary bypass surgery
• Although higher tranexamic acid doses were found to achieve a marginal gain in effectiveness, they increased the risk of postop-erative seizure, particularly in procedures involving a high risk of bleeding
Tranexamic acid is an anti brinolytic agent that reduces postoperative blood loss and rates of erythrocyte trans-
fusion and rethoracotomy in cardiopulmonary bypass sur-gery. 1 Guidelines on patient blood management recommend the routine use of tranexamic acid for adult cardiac surgery. 2
However, there is no consensus on the dosing regimen of tranexamic acid to be administered. One dose – response
study reported that low-dose tranexamic acid (10 mg/kg followed by 1 mg · kg –1 · h –1 over 12 h) was su cient to reduce blood loss and that there was no evidence to support the use of higher doses. 3
Yet on the basis of pharmacokinetic models, 4 , 5 some authors have proposed regimens targeting tranexamic acid plasma levels that were shown to fully inhibit brinolysis in in vitro studies. 6 These regimens involve the administration of high doses of tranexamic acid ( e.g. , 30 mg/kg followed by 16 mg · kg –1 · h –1 during surgery with 2 mg/kg added to the pump prime, or a preoperative bolus of 100 mg/
ABSTRACT Background: It is unclear whether high-dose regimens of tranexamic acid in cardiac surgery (total dose, 80 to 100 mg/kg) confer a clinical advantage over low-dose regimens (total dose, approximately 20 mg/kg), particularly as tranexamic acid – associated seizure may be dose-related. The authors’ aim was to characterize the exposure – response relationship of this drug.
Methods: Databases were searched for randomized controlled trials of intravenous tranexamic acid in adult patients undergoing cardiopulmonary bypass surgery. Observational studies were added for seizure assessment. Tranexamic acid concentrations were predicted in each arm of each study using a population pharmacokinetic model. The exposure – response relation-ship was evaluated by performing a model-based meta-analysis using nonlin-ear mixed-effect models.
Results: Sixty-four randomized controlled trials and 18 observational stud-ies (49,817 patients) were included. Seventy-three different regimens of tranexamic acid were identifi ed, with the total dose administered ranging from 5.5 mg/kg to 20 g. The maximum effect of tranexamic acid for post-operative blood loss reduction was 40% (95% credible interval, 34 to 47%), and the EC
50 was 5.6 mg/l (95% credible interval, 0.7 to 11 mg/l). Exposure
values with low-dose regimens approached the 80% effective concentration, whereas with high-dose regimens, they exceeded the 90% effective concen-tration. The predicted cumulative blood loss up to 48 h postsurgery differed by 58 ml between the two regimens, and the absolute difference in erythro-cyte transfusion rate was 2%. Compared to no tranexamic acid, low-dose and high-dose regimens increased the risk of seizure by 1.2-fold and 2-fold, respectively. However, the absolute risk increase was only clinically meaning-ful in the context of prolonged open-chamber surgery.
Conclusions: In cardiopulmonary bypass surgery, low-dose tranexamic acid seems to be an appropriate regimen for reducing bleeding outcomes. This meta-analysis has to be interpreted with caution because the results are observational and dependent on the lack of bias of the predicted tranexamic acid exposures and the quality of the included studies.
(ANESTHESIOLOGY 2021 ; 134 : 165 – 78 )
Exposure – Response Relationship of Tranexamic Acid in Cardiac Surgery A Model-based Meta-analysis Paul Jacques Zufferey , M.D., Ph.D. , Julien Lanoisel é e , M.D. , Billal Graouch , M.B.S.S. , Baptiste Vieille , M.B.S.S. , Xavier Delavenne , Pharm.D., Ph.D. , Edouard Ollier , M.D., Ph.D.
ANESTHESIOLOGY 2021 ; 134 : 165 – 78
This article is featured in “This Month in Anesthesiology,” page 1A. This article is accompanied by an editorial on p. 143. Supplemental Digital Content is available for this article. Direct URL citations appear in the printed text and are available in both the HTML and PDF versions of this article. Links to the digital fi les are provided in the HTML text of this article on the Journal’s Web site (www.anesthesiology.org). This article has a visual abstract available in the online version.
Submitted for publication June 6, 2020. Accepted for publication November 2, 2020. Published online fi rst on December 14, 2020. From Institut National de la Santé et de la Recherche Médicale (INSERM), U1059, Vascular Dysfunction and Hemostasis, Saint-Etienne, France (P.J.Z., J.L., X.D., E.O.); Department of Anesthesia and Intensive Care (P.J.Z., J.L., B.G., B.V.), Clinical Pharmacology Department (P.J.Z., X.D., E.O.), University Hospital of Saint-Etienne, Saint-Etienne, France; and University of Lyon, Saint-Etienne, France (X.D., E.O.).
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved. Anesthesiology 2021 ; 134 : 165 – 78 . DOI: 10.1097/ALN.0000000000003633
ALNV134N2_Text.indb 165ALNV134N2_Text.indb 165 29-Dec-20 19:43:0829-Dec-20 19:43:08
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
166 Anesthesiology 2021; 134:165–78
PERIOPERATIVE MEDICINE
Zufferey et al .
kg). Although the relationship between in vivo blood con-centrations of tranexamic acid, brinolytic inhibition, and blood loss reduction has never been validated, several trials have shown a greater reduction in blood loss with these high doses compared to lower doses. 1 , 7 , 8 Unfortunately, tranexamic acid administration increases the risk of post-operative seizure, 1 a risk that appears to be dose-related. 9
The optimal tranexamic acid regimen for cardiopulmonary bypass surgery, in terms of both e ectiveness and safety, therefore remains uncertain.
Model-based meta-analysis is an extension of traditional meta-analysis including parametric models to describe the e ect of dose. 10 , 11 It also allows the impact of covariates such as surgical or demographic characteristics on the dose – response relationship to be taken into account. Using this meta-analytic technique, we aimed to quantify the e ect of tranexamic acid exposure on postoperative bleeding events and seizure with the ultimate objective of clarifying the optimal dosing regi-men of this agent in cardiopulmonary bypass surgery.
Materials and Methods This systematic review and meta-analysis is reported in accordance with the 2009 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 12 The protocol was submitted to International Prospective Register of Systematic Reviews (PROSPERO) for registration in March 2019 and was registered in April 2020 (registration No. CRD42020132076).
Eligibility Criteria
We searched for trials that included adult patients (aged 18 yr or older) undergoing cardiopulmonary bypass (CPB) for cardiac or thoracic aortic surgery. To assess the exposure – re-sponse relationship of tranexamic acid with regard to e ec-tiveness, we restricted our search to randomized controlled trials that compared an intravenous dose of tranexamic acid to another intravenous tranexamic acid dose or to no treatment (including placebo). Trial arms that administered topical tranexamic acid, oral tranexamic acid, or another anti- brinolytic were excluded. The e cacy outcomes selected were postoperative blood loss, allogeneic erythrocyte transfu-sion, and rethoracotomy for any reason. Postoperative blood loss, the primary outcome, was recorded as the volume of chest tube drainage. All measurements up to drain removal were collected. For the other e cacy outcomes, there was no restriction on the timing of measurements of the events concerned. To assess the exposure – response relationship with respect to safety, the endpoint of interest was postoperative seizure. As this event is rare and its occurrence in relation to the use of tranexamic acid has been reported only since 2008 in cardiac surgery, 13 we extended our search to observational studies and also included arms of randomized controlled tri-als of intravenous tranexamic acid that had an ineligible com-parator for the e ectiveness analysis. These latter trial arms were considered as observational studies in this review. There
was no restriction as to the type or cause of seizure. Seizures occurring after intensive care ( i.e. , 24 to 48 h after the end of surgery) were not taken into consideration.
Search Strategy and Study Selection
Relevant trials were identi ed by a computerized search in Medical Literature Analysis and Retrieval System Online (MEDLINE, PubMed) and the Cochrane Central Registry of Controlled Trials (Central) from the inception of these databases up to June 2019. The systematic search strategy used for both databases is shown in the Supplemental Digital Content 1 (http://links.lww.com/ALN/C513). In addition, we checked the reference lists of the trials selected and those of relevant systematic reviews. To identify eligible trials in progress or unpublished, we searched the International Clinical Trials Registry Platform and ClinicalTrials.gov. No language, publication date, or publication status restrictions were imposed. Foreign papers were translated. Three of the authors (B.G., B.V., and P.J.Z.) developed and independently conducted the search. Studies were rst screened on the basis of title and/or abstract. The full texts of potentially eli-gible trials were then retrieved and evaluated for inclusion. Any disagreements were resolved by consensus.
Data Collection and Risk of Bias Assessment
Data were extracted using a data extraction sheet speci cally designed for this review in Excel (Microsoft, USA). One of the authors conducting the literature search (P.J.Z.) extracted the data from the studies selected. The two others (B.G. and B.V.) checked the extracted data. In the event of disagreement with regard to data extraction, the decision of a fourth author (E.O.) was nal. The authors of the selected trials were contacted to supply any missing information or clari cations required in June 2019. A reminder was sent in July 2019 if necessary. Data were extracted from each trial included with respect to (1) the characteristics of the trial participants (including age, weight, and type and duration of surgery); (2) the tranexamic acid regimen used; (3) risk factors for postoperative bleed-ing, 14 erythrocyte transfusion, 15 and seizure; 9 , 16 (4) outcome data; and (5) the number of patients randomized and the number of patients available for the analyses. A full description of the extracted data is provided in the Supplemental Digital Content 1 (http://links.lww.com/ALN/C513). The risk of bias for each randomized control trial was assessed (by P.J.Z.) using the Cochrane risk of bias tool. Trials were considered to be at low summary risk of bias if allocation concealment, blinding of participants, and study personnel, and blinding of outcome assessment were all judged to be adequate. The risk of bias for each observational study was assessed (by B.V.) using the Newcastle – Ottawa quality scale. 17
Data Synthesis and Analysis
Summary Measure s . For each postoperative blood loss observation, the timing of the measurement relative to the
ALNV134N2_Text.indb 166ALNV134N2_Text.indb 166 29-Dec-20 19:43:0829-Dec-20 19:43:08
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:165–78 167
Exposure – Response Relationship of Tranexamic Acid
Zufferey et al .
end of surgery and the mean and corresponding SD were collected. When the median and range (or minimum – max-imum range) were reported rather than the mean and SD, approximation methods were used to estimate these latter values. 18 Normally distributed postoperative blood loss val-ues were then converted to the logarithmic scale. 19
The proportions of patients requiring erythrocyte trans-fusion and rethoracotomy, respectively, and the proportion experiencing seizure were calculated. In the case of zero events, a continuity correction of 0.5 was applied.
Tranexamic acid exposure in each treatment arm was evaluated by simulation. The mean tranexamic acid kinetic was simulated on the basis of the characteristics of each arm (dosing regimen, mean patient body weight) and the phar-macokinetic model developed by Grassin-Delyle et al. 5 In the event of missing information on mean body weight, CPB duration, or surgery duration, a multivariate imputa-tion was performed using the multivariate imputation by chained equations, mice package in R software (R core team, Austria). 20 The mean tranexamic acid concentration from the start of surgery up to 12 h ( TXA
h[ ] −0 12 ) was calcu-
lated for each arm of each study. Synthesis of Result s . The relationship between tranexamic acid exposure and outcome data was evaluated by perform-ing a model-based meta-analysis using nonlinear mixed-ef-fect models. 10 For each outcome, the analysis provided an estimation of maximum-e ect and EC
50 parameters corre-
sponding respectively to the maximum e ect of tranexamic acid and the value of TXA
h[ ] −0 12 required to achieve 50%
of this maximum e ect. For postoperative blood loss, we also modeled tranexamic acid exposure as a time-varying covariate to identify the period when tranexamic acid exposure contributed the most to blood loss reduction.
We rst performed a longitudinal model-based meta-analysis to describe the time course of blood loss and the relationship between TXA
h[ ] −0 12 and postoperative
blood loss. 11 The following model was used:
LBLBL E TXA
EC TXAijk
MAXi ijk
ijk
MAXi ij
h
=×
+× −
× [ ]+
−
logτ
τ τ50
0 12
50
1[[ ]
+ ×−ij
h ijk ijk0 12 σ ε
where LBLijk and τ ijk correspond to the observed postop-erative blood loss (on a logarithmic scale) and to the sam-pling time in the j th arm of the i th study at the k th sampling point, respectively. The parameters τ50 and EC50 corre-spond, respectively, to the time to attainment of 50% of the maximum blood loss and to the mean tranexamic acid concentration achieving 50% of the maximum e ect. The parameters BLMAX i and EMAX i correspond, respectively, to the study-speci c maximum blood loss and to the maxi-mum e ect. These parameters were assumed to conform to a log-normal and a logit-normal distribution, respectively:
log ( ) ~ ,BL u with u NMAX i BL i i BLMAX MAX= + ( )µ σ0 2
logit ( ) ~ ,E v with v NMAX i E i i EMAX MAX= + ( )µ σ0 2
where u i and v
i are the random e ects representing inter-
study variability. Unexplained intrastudy variability was accounted for using a residual error term that was assumed to be normally distributed ( ε σijk eN~ ( , )0 2 ) and scaled according to the standard error of each observation ( σ ijk )
To explore tranexamic acid as a time-varying covariate during the rst 48 h after the start of the surgery, the data were tted to a second model:
LBL
BL
tE C t
EC
ijk
MAXi ijk
ijk
MAXi ij
=
×+
×
− ×× ( )+
log
( , , )
ττ τ
π δ γ
50
50
1CC t
dtij
ijk ijk
( )
+ ×
∫0
48σ ε
where C tij ( ) is the simulated mean tranexamic acid concen-tration in the j th arm of the i th study. The function π ( , , )δ γ tis a weighting function. The periods associated with high values of π δ γ( , , )t correspond to those contributing the most to the overall e ect of tranexamic acid. The weighting function is based on a reparametrized gamma distribution:
π δ γ α βα δ β
βδ δ γ
γ
, , ( ; , )t G t( ) == + ×
=+ + ×
×
1
4
2
2 2
2
with G t( ; , )α β representing the density of a gamma distri-bution with a shape parameter α and a rate parameter β . The parameter δ corresponds to the mode of the distribu-tion ( i.e. , to the time at which the weighting is maximal and consequently to the time at which tranexamic acid expo-sure contributes the most to the overall e ect of the drug) and γ to the SD of the distribution.
The relationship between TXAh[ ] −0 12 and erythrocyte
transfusion to compensate for blood loss was assessed using the following model:
logit logit 1Trans TransE TXA
EC TXAij 0i
MAXi ij
0 12h
50
( ) =[ ][ ]
× −×
+
−
iij
0 12h−
+ ×σ ij ijε
where Transij corresponds to the proportion of patients who received erythrocyte transfusion to compensate for blood loss in the j th arm of the i th study. The parame-ter Trans i0 corresponds to the study-speci c transfusion rate in the absence of tranexamic acid exposure. It is assumed to follow a logit-normal distribution:
logit ( ) ~ ,Trans02
0 00i Trans i i Transw withw N= + ( )µ σ
The relationship between TXAh[ ] −0 12 and seizure was
assessed using the following logit-linear model:
ALNV134N2_Text.indb 167ALNV134N2_Text.indb 167 29-Dec-20 19:43:2229-Dec-20 19:43:22
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

168 Anesthesiology 2021; 134:165–78
PERIOPERATIVE MEDICINE
Zufferey et al .
logit Conv TXAij ij
0 12h( ) = + × [ ] + + ×β β ω σ ε0 TXA i ij ij−
where Convij corresponds to the proportion of patients
experiencing seizure in the j th arm of the i th study. Parameter ωi corresponds to the random intercept and is assumed to be normally distributed ( ω σ ωi N~ ,0 2( ) ).
To explore the heterogeneity between studies, we eval-uated the impact of covariates on the exposure – response relationships. We evaluated risk factors for postoperative bleeding, erythrocyte transfusion, and seizure (described in Supplemental Digital Content 1, http://links.lww.com/ALN/C513) and also the risk of bias within studies. Each of these covariates were included in the previous models to assess their impact on BLMAX i , EMAX i , Trans i0 , and Convij .
For example, the e ect of the mean patient body weight (BW
i ) within each study on the study-speci c transfusion
rate was implemented as follows:
logit( ) ( ) ~ ,Trans BW w with w Ni Trans BW i i i Trans02
0 076 0= + × − + ( )µ θ σ
where θBW corresponds to the e ect of mean patient body weight on the study-speci c transfusion rate.
For seizure, the e ect of the proportion of patients under-going open-chamber surgery within each study (OC
i ) on
the study-speci c probability of seizure was implemented as follows:
logit Conv TXA OCij ij
0 12hOC i i ij ij( ) = + × [ ]TXAβ β σ ε0
− θ ω+ × + + ×
where θOC corresponds to the e ect of the percentage of open chamber surgery on the study-speci c seizure probability. Parameter Estimation . Data analysis was performed using R software. 21 The meta-analysis model was estimated by a Bayesian approach using the rstan package in R. As no previ-ous information on exposure response parameters was avail-able, noninformative previous distributions were assumed for all the parameters ( U −∞ +∞( ); for mean parameters and U 0;+∞( ) for SD)) except EC
50 , for which a weakly
informative uniform previously was assumed ( U 0 100;( ) ). During the modeling process, the robustness of the results to the choice of previous distribution was explored. The models for covariate selection were compared by leave-one-out cross-validation using the loo package in R. 22 The nal model was assessed in terms of basic goodness-of- t plots using a visual predictive check. All graphics were gen-erated using the ggplot2 package in R. 23
Sensitivity Analyses . Two sensitivity analyses were performed to assess the impact of the uncertainty of the pharmaco-kinetic predictions on the exposure – response relation-ships. We rst limited our analysis to studies for which no imputation had been used for estimating tranexamic acid exposure. The second analysis considered uncertainty in the predictions of tranexamic acid exposure. We generated 500 data sets. In each data set, tranexamic acid exposures
( TXAh[ ] −0 12 ) were simulated using the standard errors of
the tranexamic acid pharmacokinetic parameters reported by Grassin-Delyle et al. 5 Posterior mean of the parameters of the model-based meta-analyses were calculated for each data set. The distributions of the obtained values were pre-sented as histograms. Simulations of the Effect of Differe nt Dosing Regimens . We simulated the outcomes in two hypothetical trials to exam-ine the e ect of di erent tranexamic acid dosing regimens on postoperative bleeding events and seizure. The rst trial included patients undergoing coronary artery bypass graft (CABG) surgery (closed-chamber procedure) with a mean duration of surgery and CPB of 3 h and 1.5 h, respectively. The second trial included patients undergoing complex open-chamber surgery with a mean duration of surgery and CPB of 4 h and 2.5 h, respectively. In both cases, the body weight value used for simulation was the mean weight observed in the meta-analysis. The dosing regimens were chosen on the basis of the total dose administered (high- vs.low-dose) and the duration of tranexamic acid adminis-tration (single bolus vs. bolus plus infusion). For high-dose tranexamic acid, we chose administration of a single preop-erative bolus as proposed by Karski et al. (100 mg/kg) 7 and a second regimen corresponding to that used in the Blood Conservation Using Anti brinolytics in a Randomized Trial (BART) study (30 mg/kg followed by 16 mg · kg –1 · h –1
during surgery, with a further 2 mg/kg being added to the pump prime). 24 For low-dose tranexamic acid, we chose a single preoperative bolus of 20 mg/kg as proposed by Lambert et al. , 25 and nally the regimen proposed by Horrow et al. (10 mg/kg followed by 1 mg · kg –1 · h –1 for 12 h). 3
Results
Study Selection
A total of 82 clinical trials (49,817 patients) were selected, comprising 64 randomized controlled studies (12,378 patients) for the e ectiveness analysis and 18 additional observational studies (37,439 patients) for the analysis of seizure. The ow chart of the study selection process is pre-sented in gure 1 . Altogether, 61 authors reporting 73 trials were contacted, of whom 34 replied, with 19 providing sup-plementary information for 20 trials (see Acknowledgments).
Study Characteristics
In total, 36 (44%) studies included CABG surgery, and 55 (66%) studies included open-chamber surgery. The mean duration of CPB was 1 h 48 min (range, 1 h 2 min to 5 h 28 min), and the mean duration of surgery was 4 h 7 min (range, 2 h 19 min to 7 h 45 min). Women comprised 31% of the patients. The mean age was 62 yr (range, 36 to 77 yr), and the mean weight was 74 kg (range, 49 to 89 kg). Altogether, 73 di erent intravenous tranexamic acid reg-imens were identi ed, with the total dose of tranexamic
ALNV134N2_Text.indb 168ALNV134N2_Text.indb 168 29-Dec-20 19:43:2929-Dec-20 19:43:29
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
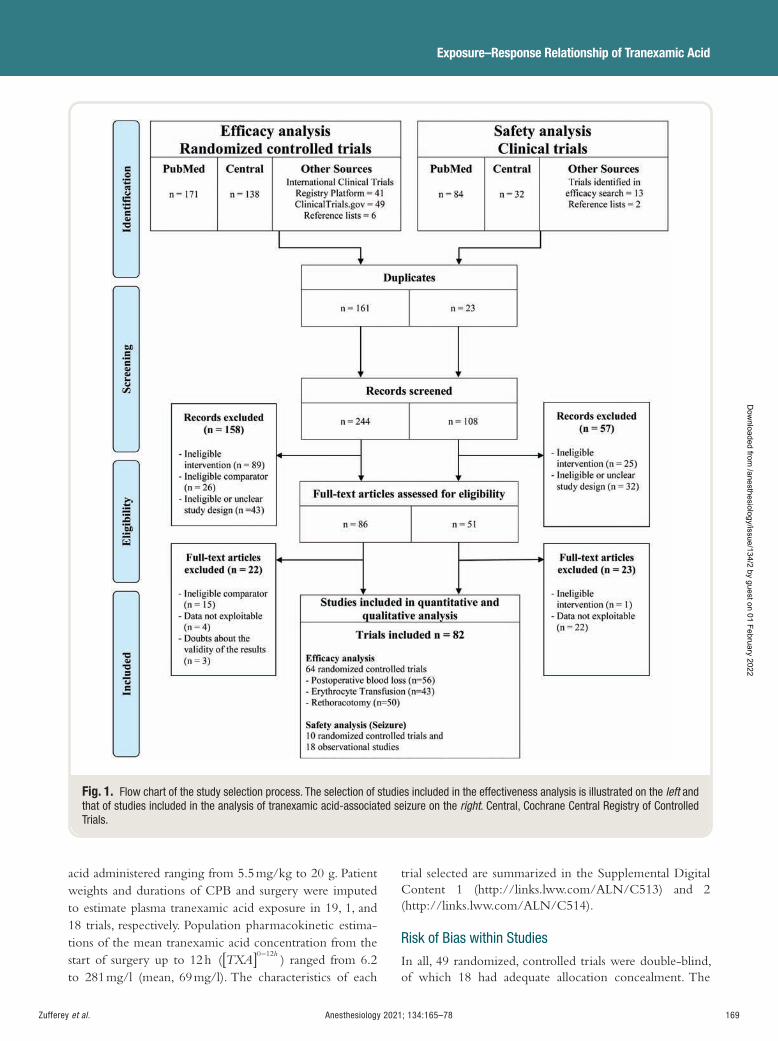
Anesthesiology 2021; 134:165–78 169
Exposure – Response Relationship of Tranexamic Acid
Zufferey et al .
acid administered ranging from 5.5 mg/kg to 20 g. Patient weights and durations of CPB and surgery were imputed to estimate plasma tranexamic acid exposure in 19, 1, and 18 trials, respectively. Population pharmacokinetic estima-tions of the mean tranexamic acid concentration from the start of surgery up to 12 h ( TXA
h[ ] −0 12 ) ranged from 6.2
to 281 mg/l (mean, 69 mg/l). The characteristics of each
trial selected are summarized in the Supplemental Digital Content 1 (http://links.lww.com/ALN/C513) and 2 (http://links.lww.com/ALN/C514).
Risk of Bias within Studies
In all, 49 randomized, controlled trials were double-blind, of which 18 had adequate allocation concealment. The
Fig. 1. Flow chart of the study selection process. The selection of studies included in the effectiveness analysis is illustrated on the left and that of studies included in the analysis of tranexamic acid-associated seizure on the right . Central, Cochrane Central Registry of Controlled Trials.
ALNV134N2_Text.indb 169ALNV134N2_Text.indb 169 29-Dec-20 19:43:3029-Dec-20 19:43:30
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
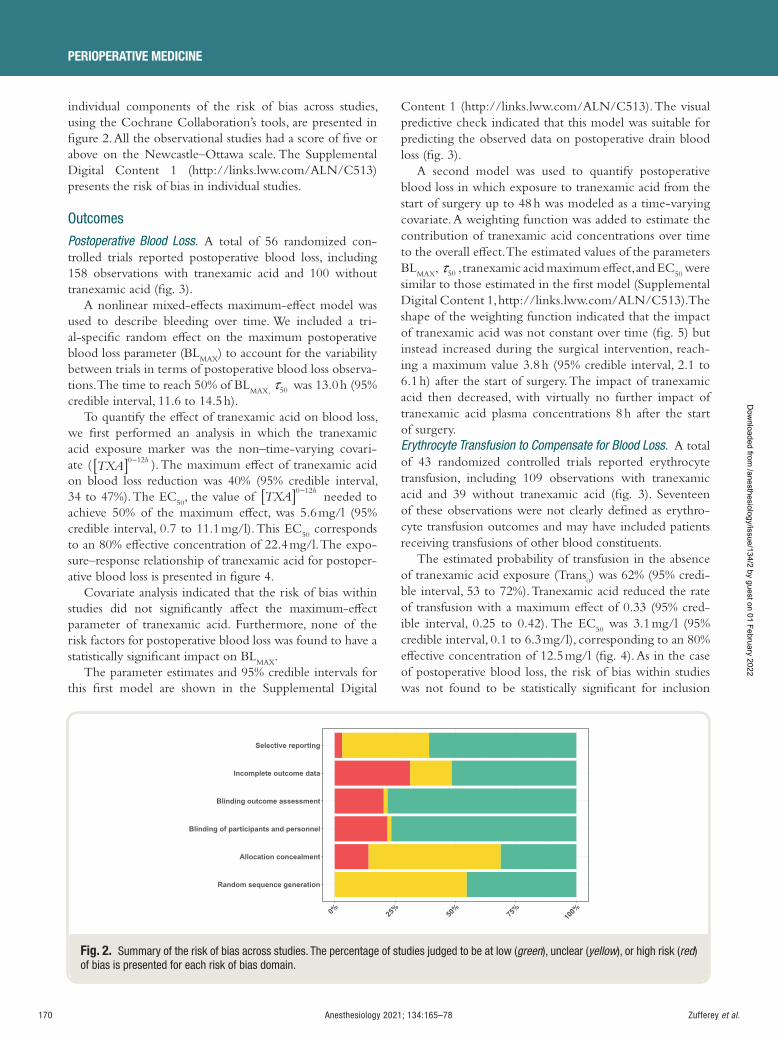
170 Anesthesiology 2021; 134:165–78
PERIOPERATIVE MEDICINE
Zufferey et al .
individual components of the risk of bias across studies, using the Cochrane Collaboration ’ s tools, are presented in gure 2 . All the observational studies had a score of ve or above on the Newcastle – Ottawa scale. The Supplemental Digital Content 1 (http://links.lww.com/ALN/C513) presents the risk of bias in individual studies.
Outcomes
Postoperative Blood Los s . A total of 56 randomized con-trolled trials reported postoperative blood loss, including 158 observations with tranexamic acid and 100 without tranexamic acid ( g. 3 ).
A nonlinear mixed-e ects maximum-e ect model was used to describe bleeding over time. We included a tri-al-speci c random e ect on the maximum postoperative blood loss parameter (BL
MAX ) to account for the variability
between trials in terms of postoperative blood loss observa-tions. The time to reach 50% of BL
MAX, τ50 was 13.0 h (95% credible interval, 11.6 to 14.5 h).
To quantify the e ect of tranexamic acid on blood loss, we rst performed an analysis in which the tranexamic acid exposure marker was the non – time-varying covari-ate ( TXA
h[ ] −0 12 ). The maximum e ect of tranexamic acid on blood loss reduction was 40% (95% credible interval, 34 to 47%). The EC
50 , the value of TXA
h[ ] −0 12 needed to
achieve 50% of the maximum e ect, was 5.6 mg/l (95% credible interval, 0.7 to 11.1 mg/l). This EC
50 corresponds
to an 80% e ective concentration of 22.4 mg/l. The expo-sure – response relationship of tranexamic acid for postoper-ative blood loss is presented in gure 4 .
Covariate analysis indicated that the risk of bias within studies did not signi cantly a ect the maximum-e ect parameter of tranexamic acid. Furthermore, none of the risk factors for postoperative blood loss was found to have a statistically signi cant impact on BL
MAX .
The parameter estimates and 95% credible intervals for this rst model are shown in the Supplemental Digital
Content 1 (http://links.lww.com/ALN/C513). The visual predictive check indicated that this model was suitable for predicting the observed data on postoperative drain blood loss ( g. 3 ).
A second model was used to quantify postoperative blood loss in which exposure to tranexamic acid from the start of surgery up to 48 h was modeled as a time-varying covariate. A weighting function was added to estimate the contribution of tranexamic acid concentrations over time to the overall e ect. The estimated values of the parameters BL
MAX , τ50 , tranexamic acid maximum e ect, and EC
50 were
similar to those estimated in the rst model (Supplemental Digital Content 1, http://links.lww.com/ALN/C513). The shape of the weighting function indicated that the impact of tranexamic acid was not constant over time ( g. 5 ) but instead increased during the surgical intervention, reach-ing a maximum value 3.8 h (95% credible interval, 2.1 to 6.1 h) after the start of surgery. The impact of tranexamic acid then decreased, with virtually no further impact of tranexamic acid plasma concentrations 8 h after the start of surgery. Erythrocyte Transfusion to Compensate for Blood Loss . A total of 43 randomized controlled trials reported erythrocyte transfusion, including 109 observations with tranexamic acid and 39 without tranexamic acid ( g. 3 ). Seventeen of these observations were not clearly de ned as erythro-cyte transfusion outcomes and may have included patients receiving transfusions of other blood constituents.
The estimated probability of transfusion in the absence of tranexamic acid exposure (Trans
0 ) was 62% (95% credi-
ble interval, 53 to 72%). Tranexamic acid reduced the rate of transfusion with a maximum e ect of 0.33 (95% cred-ible interval, 0.25 to 0.42). The EC
50 was 3.1 mg/l (95%
credible interval, 0.1 to 6.3 mg/l), corresponding to an 80% e ective concentration of 12.5 mg/l ( g. 4 ). As in the case of postoperative blood loss, the risk of bias within studies was not found to be statistically signi cant for inclusion
Fig. 2. Summary of the risk of bias across studies. The percentage of studies judged to be at low ( green ), unclear ( yellow ), or high risk ( red ) of bias is presented for each risk of bias domain.
ALNV134N2_Text.indb 170ALNV134N2_Text.indb 170 29-Dec-20 19:43:3329-Dec-20 19:43:33
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
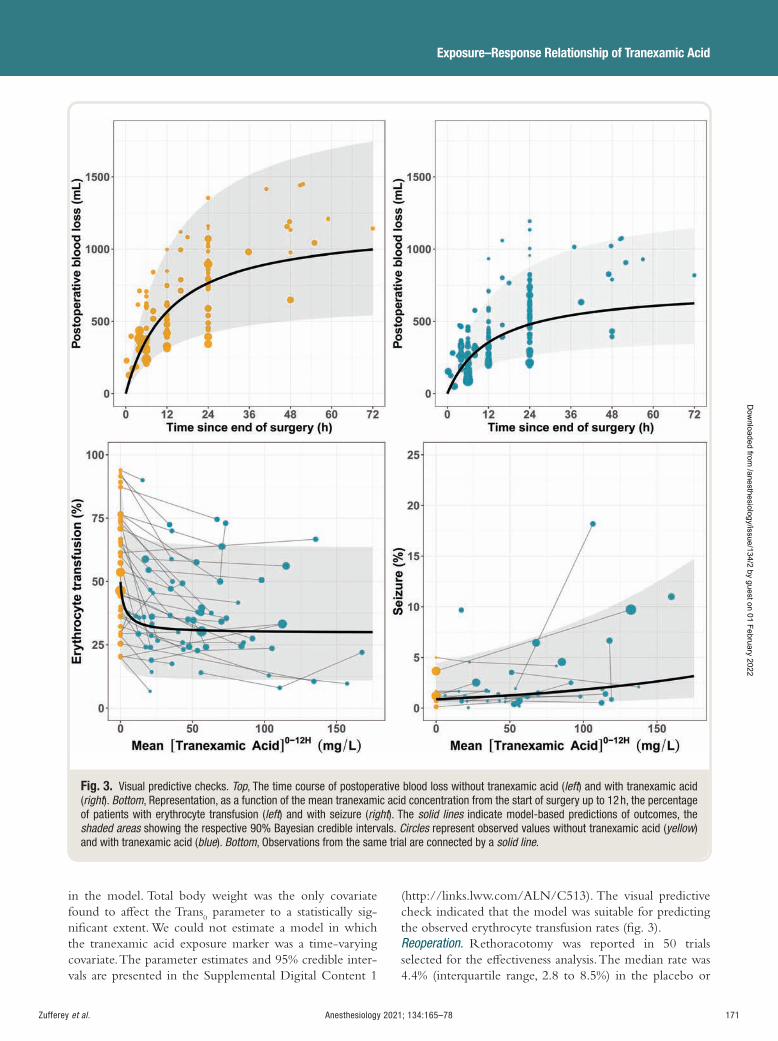
Anesthesiology 2021; 134:165–78 171
Exposure – Response Relationship of Tranexamic Acid
Zufferey et al .
in the model. Total body weight was the only covariate found to a ect the Trans
0 parameter to a statistically sig-
ni cant extent. We could not estimate a model in which the tranexamic acid exposure marker was a time-varying covariate. The parameter estimates and 95% credible inter-vals are presented in the Supplemental Digital Content 1
(http://links.lww.com/ALN/C513). The visual predictive check indicated that the model was suitable for predicting the observed erythrocyte transfusion rates ( g. 3 ). Reoperation . Rethoracotomy was reported in 50 trials selected for the e ectiveness analysis. The median rate was 4.4% (interquartile range, 2.8 to 8.5%) in the placebo or
Fig. 3. Visual predictive checks. Top , The time course of postoperative blood loss without tranexamic acid ( left ) and with tranexamic acid ( right ). Bottom , Representation, as a function of the mean tranexamic acid concentration from the start of surgery up to 12 h, the percentage of patients with erythrocyte transfusion ( left ) and with seizure ( right ). The solid lines indicate model-based predictions of outcomes, the shaded areas showing the respective 90% Bayesian credible intervals. Circles represent observed values without tranexamic acid ( yellow ) and with tranexamic acid ( blue ). Bottom , Observations from the same trial are connected by a solid line .
ALNV134N2_Text.indb 171ALNV134N2_Text.indb 171 29-Dec-20 19:43:3429-Dec-20 19:43:34
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
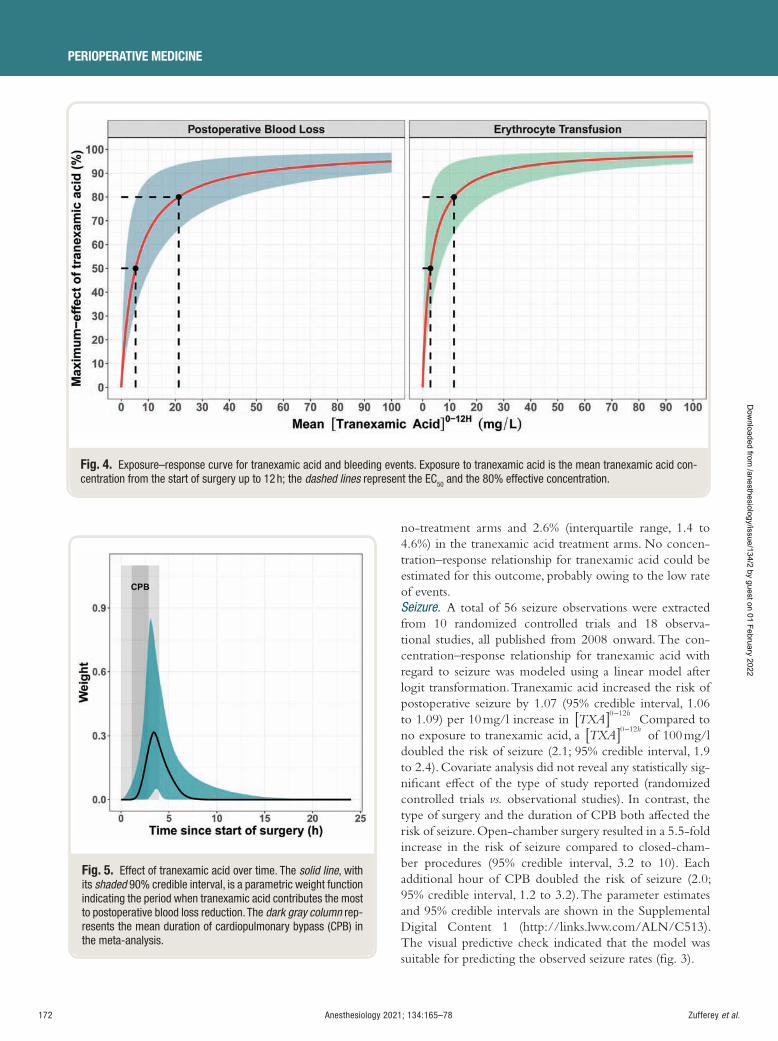
172 Anesthesiology 2021; 134:165–78
PERIOPERATIVE MEDICINE
Zufferey et al .
no-treatment arms and 2.6% (interquartile range, 1.4 to 4.6%) in the tranexamic acid treatment arms. No concen-tration – response relationship for tranexamic acid could be estimated for this outcome, probably owing to the low rate of events. Seizure . A total of 56 seizure observations were extracted from 10 randomized controlled trials and 18 observa-tional studies, all published from 2008 onward. The con-centration – response relationship for tranexamic acid with regard to seizure was modeled using a linear model after logit transformation. Tranexamic acid increased the risk of postoperative seizure by 1.07 (95% credible interval, 1.06 to 1.09) per 10 mg/l increase in TXA
h[ ] −0 12
. Compared to
no exposure to tranexamic acid, a TXAh[ ] −0 12 of 100 mg/l
doubled the risk of seizure (2.1; 95% credible interval, 1.9 to 2.4). Covariate analysis did not reveal any statistically sig-ni cant e ect of the type of study reported (randomized controlled trials vs. observational studies). In contrast, the type of surgery and the duration of CPB both a ected the risk of seizure. Open-chamber surgery resulted in a 5.5-fold increase in the risk of seizure compared to closed-cham-ber procedures (95% credible interval, 3.2 to 10). Each additional hour of CPB doubled the risk of seizure (2.0; 95% credible interval, 1.2 to 3.2). The parameter estimates and 95% credible intervals are shown in the Supplemental Digital Content 1 (http://links.lww.com/ALN/C513). The visual predictive check indicated that the model was suitable for predicting the observed seizure rates ( g. 3 ).
Fig. 4. Exposure – response curve for tranexamic acid and bleeding events. Exposure to tranexamic acid is the mean tranexamic acid con-centration from the start of surgery up to 12 h; the dashed lines represent the EC 50 and the 80% effective concentration.
Fig. 5. Effect of tranexamic acid over time. The solid line , with its shaded 90% credible interval, is a parametric weight function indicating the period when tranexamic acid contributes the most to postoperative blood loss reduction. The dark gray column rep-resents the mean duration of cardiopulmonary bypass (CPB) in the meta-analysis.
ALNV134N2_Text.indb 172ALNV134N2_Text.indb 172 29-Dec-20 19:43:3729-Dec-20 19:43:37
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:165–78 173
Exposure – Response Relationship of Tranexamic Acid
Zufferey et al .
Sensitivity Analyses
Two sensitivity analyses were performed to assess the impact of imputing data for pharmacokinetic predictions and the uncertainty in the parameter estimates of the pharmaco-kinetic model used for predictions. Both analyses showed results similar to the primary analysis. Exclusion of studies in which imputation was performed increased the credi-ble interval of the EC
50 parameters. The results are shown
in the Supplemental Digital Content 1 (http://links.lww.com/ALN/C513).
Simulations
We simulated the outcomes in two hypothetical trials to examine the e ect of di erent tranexamic acid dosing regi-mens on postoperative bleeding events and seizure.
The rst trial included patients undergoing CABG sur-gery (closed-chamber procedure) with a mean duration of surgery and CPB of 3 h and 1.5 h, respectively. The con-centration-time courses of tranexamic acid for the di erent dosing regimens are presented in gure 6 . With low-dose tranexamic acid, the mean exposure values were 21 mg/l, close to the 80% e ective concentration for postoperative blood loss. With high-dose tranexamic acid, the mean expo-sure values were above the 90% e ective concentration. The estimated cumulative blood loss up to 48 h after the end of surgery without tranexamic acid was 909 ml (95% credi-ble interval, 815 to 1,016 ml). Low-dose tranexamic acid, given either as a single preoperative bolus or as a preoper-ative bolus followed by an intraoperative infusion, reduced postoperative blood loss by 32% (95% credible interval, 27 to 37%; g. 6 and Supplemental Digital Content 1, http://links.lww.com/ALN/C513). Compared to low-dose tranexamic acid, high-dose tranexamic acid reduced cumulative postoperative blood loss up to 48 h postsurgery by a further 58 ml (95% credible interval, 54 to 65 ml). The probability of erythrocyte transfusion as a function of tranexamic acid exposure ( TXA
h[ ] −0 12 ) is illustrated in
gure 6 . Exposure values for all tranexamic acid regimens were above the 80% e ective concentration for erythro-cyte transfusion. Without tranexamic acid, the probability of transfusion was 66% (95% credible interval, 57 to 74%), with low-dose tranexamic acid it was 46% (95% credible interval, 38 to 54%), and with high-dose tranexamic acid it was 44% (95% credible interval, 36 to 52%; g. 6 ). The absolute rate di erence in erythrocyte transfusion between low- and high-dose tranexamic acid was 2% (95% credible interval, 0.4 to 4.3%). In this rst case scenario, the prob-ability of postoperative seizure remained low, less than 1%, regardless of the tranexamic acid regimen ( g. 6 ).
The second trial included patients undergoing open-chamber surgery with a mean duration of surgery and CPB of 4 h and 2.5 h, respectively. Simulated bleed-ing events were similar to those in the rst scenario, as our models for bleeding events did not include surgical
covariates. However, the risk of seizure was increased in this second scenario as both open-chamber surgery and CPB duration were associated with a higher risk of this event. Without administration of tranexamic acid, the probabil-ity of seizure was 2.85% (95% credible interval, 1.82 to 4.63%). The probability was increased 1.2-fold with low-dose tranexamic acid and was doubled with high-dose tranexamic acid ( g. 6 ).
Discussion With regard to e ectiveness, our results indicated a reduc-tion in postoperative blood loss and erythrocyte transfu-sion as exposure to tranexamic acid increased. We chose the commonly used maximum-e ect model to describe the e ect of tranexamic acid exposure. With this model, the increase in e ectiveness progressively declined with increasing exposure. Once the concentration exceeds the 80% e ective concentration, further changes in drug con-centration appear to have little impact on drug e ect. 26 The exposure value with the low-dose tranexamic acid regi-men proposed by Horrow et al. 3 (10 mg/kg followed by 1 mg · kg –1 · h –1 over 12 h) was close to the 80% e ective concentration for postoperative blood loss and above the 80% e ective concentration for erythrocyte transfusion. Compared to this regimen, a vefold increase in total dose (100 mg/kg) achieved only a 58 ml (95% credible interval, 54 to 65 ml) increment in the reduction of postoperative blood loss, up to 48 h postsurgery, with a decrease in eryth-rocyte transfusion rate from 46% to 44%. Our exposure – re-sponse relationship for erythrocyte transfusion corroborates the results of a previous meta-analysis in cardiac surgery showing in a subgroup analysis that tranexamic acid at doses less than 2 g and at doses of 2 to 10 g achieved similar reduc-tions in erythrocyte transfusion rate. 27
To examine when tranexamic acid should be initiated and for how long, we modeled tranexamic acid exposure as a time-varying covariate. The result ( g. 5 ) suggests that tranexamic acid administration should be initiated before CPB, as proposed by Brown et al. , 28 and should be designed to achieve e ective concentrations approximately 4 h after the start of surgery ( i.e. , toward the end of surgery) when tranexamic acid contributes the most to blood loss reduc-tion. Concentrations close to 80% e ective concentration can be achieved at the end of surgery with a low-dose reg-imen administered either as a preoperative bolus plus infu-sion (10 mg/kg followed by 1 mg · kg –1 · h –1 ) 5 , 29 or as a single preoperative loading dose of 20 mg/kg ( g. 6 ). Postoperative administration of tranexamic acid appears unnecessary because tranexamic acid concentrations will decrease but nevertheless remain su cient (greater than or equal to EC
50 ) up to the end of the drug ’ s contribution to blood
loss reduction (8 h after the start of surgery). This supports the ndings of Casati et al . showing that tranexamic acid administration after cardiac surgery was not advantageous. 30
ALNV134N2_Text.indb 173ALNV134N2_Text.indb 173 29-Dec-20 19:43:3829-Dec-20 19:43:38
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
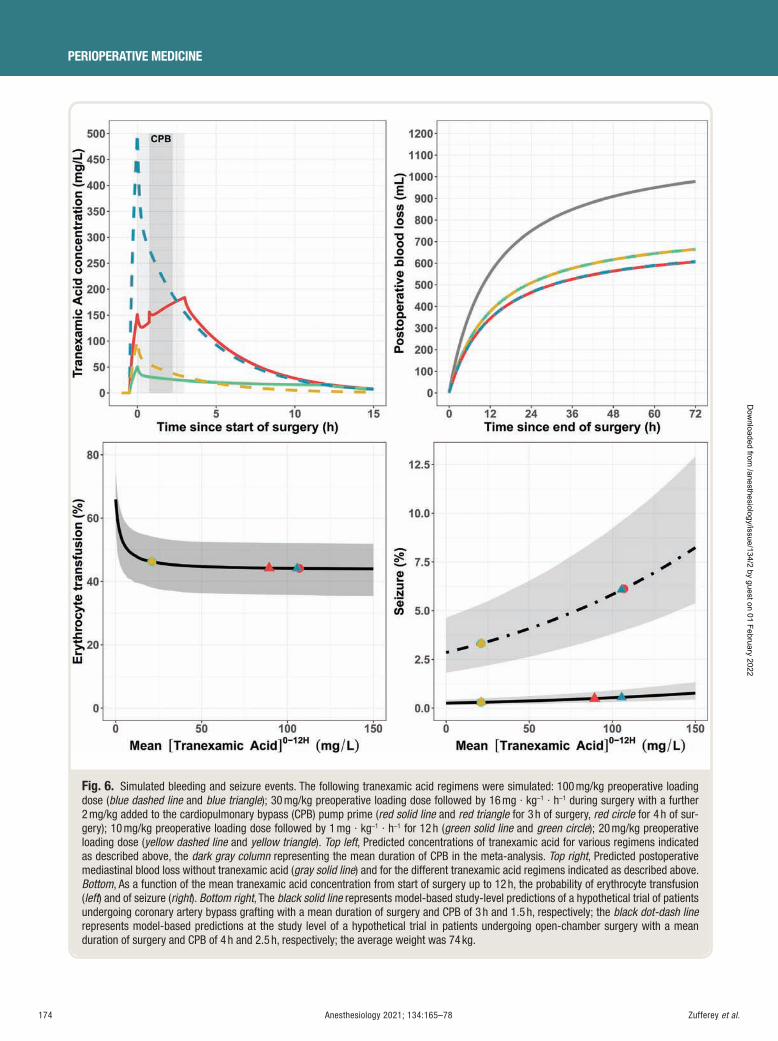
174 Anesthesiology 2021; 134:165–78
PERIOPERATIVE MEDICINE
Zufferey et al .
Fig. 6. Simulated bleeding and seizure events. The following tranexamic acid regimens were simulated: 100 mg/kg preoperative loading dose ( blue dashed line and blue triangle ); 30 mg/kg preoperative loading dose followed by 16 mg · kg –1 · h –1 during surgery with a further 2 mg/kg added to the cardiopulmonary bypass (CPB) pump prime ( red solid line and red triangle for 3 h of surgery, red circle for 4 h of sur-gery); 10 mg/kg preoperative loading dose followed by 1 mg · kg –1 · h –1 for 12 h ( green solid line and green circle ); 20 mg/kg preoperative loading dose ( yellow dashed line and yellow triangle ). Top left , Predicted concentrations of tranexamic acid for various regimens indicated as described above, the dark gray column representing the mean duration of CPB in the meta-analysis. Top right , Predicted postoperative mediastinal blood loss without tranexamic acid ( gray solid line ) and for the different tranexamic acid regimens indicated as described above. Bottom , As a function of the mean tranexamic acid concentration from start of surgery up to 12 h, the probability of erythrocyte transfusion ( left ) and of seizure ( right ). Bottom right , The black solid line represents model-based study-level predictions of a hypothetical trial of patients undergoing coronary artery bypass grafting with a mean duration of surgery and CPB of 3 h and 1.5 h, respectively; the black dot-dash linerepresents model-based predictions at the study level of a hypothetical trial in patients undergoing open-chamber surgery with a mean duration of surgery and CPB of 4 h and 2.5 h, respectively; the average weight was 74 kg.
ALNV134N2_Text.indb 174ALNV134N2_Text.indb 174 29-Dec-20 19:43:3929-Dec-20 19:43:39
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:165–78 175
Exposure – Response Relationship of Tranexamic Acid
Zufferey et al .
Tranexamic acid administration increases the risk of postoperative seizure, 1 a risk that appears to be dose-re-lated. 9 Our meta-analysis indicated that intraoperative administration of high-dose tranexamic acid (total dose, 80 to 100 mg/kg) resulted in a twofold increase in post-operative seizures, whereas low-dose tranexamic acid (total dose, approximately 20 mg/kg) was associated with a less than 1.2-fold increase in seizure rate. However, the abso-lute increase in the incidence of postoperative seizures with tranexamic acid also depends on the coexistence of other risk factors for such seizures, such as the duration of CPB, open-heart procedures, older age, renal failure, or redux sur-gery. 9 , 16 Our covariate analysis suggested that open-cham-ber surgery and duration of CPB were associated with a higher rate of seizure independently of tranexamic acid exposure. The simulation suggested that during isolated CABG surgery, tranexamic acid had virtually no e ect on postoperative seizure rate, but this was not true for complex open-heart procedures ( g. 6 ). Unfortunately, most of the risk factors for postoperative bleeding adverse events 14 , 15 are also risk factors for postoperative seizure in the context of cardiac surgery. The administration of high-dose tranexamic acid to patients at high risk of bleeding may expose patients to an increased risk of seizure for a minimal reduction in bleeding events. Based on a bene t – risk analysis, the use of high-dose tranexamic acid is questionable.
Our study has several limitations that need to be addressed. First, the exposure – response relationships are strongly dependent on the lack of bias of the predicted tranexamic acid exposures. Blood concentrations of tranexamic acid were simulated because real concentrations were not avail-able. We chose the pharmacokinetic model developed by Grassin-Delyle et al. 5 over other models 4 , 31 – 33 as it included the largest number of patients, it covered a wide range of patients ’ characteristics, and it requires only one covariate, body weight, for pharmacokinetic simulation. The presence of variability and uncertainty in the parameter estimates of this pharmacokinetic model, the model extrapolations, and the imputation of body weight and surgical duration in some studies all contributed to a degree of uncertainty in the pharmacokinetic predictions. To account for this uncer-tainty, we performed sensitivity analyses that showed results similar to those obtained with the primary analysis.
Second, the exposure – response relationships are also dependent on the unbiased assessment of outcomes. For e cacy outcomes, our assessment of the risk of bias within studies was not found to be statistically signi cant for inclu-sion in the models. Yet for seizure, the risk of information bias was noticeable and probably resulted in an underes-timation of the true incidence of events. None of the included studies was designed to assess this safety outcome. The detection or con rmation of seizure with an objec-tive test (electroencephalogram or computed tomography scans) was not mandatory. Also, patients may have been deeply sedated when seizures would be expected. As in a
previously reported meta-analysis, 34 we combined data from randomized and observational studies for the assessment of tranexamic acid – associated seizure to increase the power of the analysis and help o set the limitations of analyzing this rare outcome. Yet the risk of selection and confounding bias is nonnegligible in observational studies. 35 Because of this, great care should be taken when interpreting our covariate analysis for seizure that did not reveal any statistically sig-ni cant e ect of the type of study reported (randomized controlled trials vs. observational studies).
Finally, the exposure – response relationships are also dependent on the data analysis. Our analyses were limited by statistical power as model-based meta-analysis requires the estimation of multiple parameters compared to con-ventional meta-analyses. We could not estimate a dose – ef-fect relationship for rethoracotomy, probably owing to the low rate of events. It is therefore not possible to conclude for this outcome an advantage of a dosage regimen over another. We could not estimate the time course of the e ect of tranexamic acid on either erythrocyte transfusion or sei-zure. The dosing regimen proposals relative to the timing of surgery for postoperative blood loss reduction cannot be applied to erythrocyte transfusion and seizure. For these two outcomes, exposure to tranexamic acid was calculated as the mean tranexamic acid concentration from the start of surgery up to 12 h ( TXA
h[ ] −0 12 ). A 12-h range was cho-sen to account for postoperative exposure. Yet this exposure marker smooths out peak and trough e ects (a 20 mg/kg bolus and a 10 mg/kg bolus plus 1 mg/kg for 12 h have sim-ilar TXA
h[ ] −0 12 ; g. 6 ). This is an important issue for the
evaluation of seizure as the toxicity of tranexamic acid in the cortex and spinal cord is concentration-dependent. 36
Thus, as proposed by a reviewer, we also tested tranexamic acid blood peak concentrations. Both tranexamic acid blood peak concentrations and TXA
h[ ] −0 12 showed a relationship
with seizure. Unfortunately, these exposure markers are correlated with each other, and it is unknown how these markers re ect the concentration of tranexamic acid at the e ect site, the cerebrospinal uid.
Studies included in a meta-analysis vary in their study characteristics. We performed covariate analyses with the aim to explain part of the interstudy heterogeneity. These analyses used summary-level data ( e.g. , average patient weight in a study) and have several pitfalls. 37 The relation-ships we described are observational associations across tri-als. There is risk of a false-positive conclusion as we tested multiple covariates (although they were prespeci ed) and because bias by confounding cannot be ruled out. An exam-ple of bias is the ecological fallacy when results based on summary-level data are extrapolated to individual patients. Our covariate analysis for seizure should be interpreted as follows: studies with the highest proportion of patients undergoing open-chamber surgery showed a greater risk of seizure, rather than patients undergoing open-chamber surgery necessarily being the actual patients who are more
ALNV134N2_Text.indb 175ALNV134N2_Text.indb 175 29-Dec-20 19:43:4129-Dec-20 19:43:41
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

176 Anesthesiology 2021; 134:165–78
PERIOPERATIVE MEDICINE
Zufferey et al .
likely to convulse. Thus, our models cannot be used for pre-dictions in individuals. The use of mean values for contin-uous variables may also have limited our covariate analyses due to the limited di erence in means between studies. In addition, the scope of covariate analyses was limited by the fact that certain variables were not reported in all the studies included. For example, we could not assess the e ect of renal dysfunction, which increases exposure to tranexamic acid and is a risk factor for tranexamic acid – associated seizure. 9
Tranexamic acid doses should be lowered in patients with chronic renal dysfunction presenting for cardiac surgery. 33
In conclusion, this model-based meta-analysis suggested that low-dose tranexamic acid (total dose, approximately 20 mg/kg) was su cient for reducing postoperative blood loss and erythrocyte transfusion in CPB surgery. Higher doses achieved a marginal gain in e ectiveness but increased the risk of postoperative seizure, particularly in procedures involving a high risk of bleeding. These results have to be interpreted with caution because they are observational. They are wholly dependent on the lack of bias of the pre-dicted tranexamic acid exposures and of the quality of the included studies.
Acknowledgments
The authors are grateful to the following investigators who provided supplementary information for the meta-analy-sis: J. J. Corbeau, M.D., Department of Anesthesia and Intensive Care, University Hospital of Angers, Angers, France; P. Diprose, M.D., Anesthetic Department, University Hospital Southampton, Southampton, United Kingdom; Y. Du, M.D., Department of Anesthesia, Shengjing Hospital of China Medical University, Shenyang, China; D. Faraoni, M.D., Division of Cardiac Anesthesia, Department of Anesthesiology and Pain Medicine, The Hospital for Sick Children, University of Toronto, Toronto, Canada; G. Grei , M.D., Department of Cardiothoracic Anesthesia and Intensive Care, St. Olav University Hospital, Trondheim, Norway; J. J. Jimenez, Critical Care Department, University Hospital of the Canary Islands, La Cuesta, La Laguna, Spain; C. Keyl, M.D., Department of Anesthesiology, University Heart Center Freiburg, Bad Krozingen, Germany; T. Maeda, M.D., Department of Anesthesiology and Division of Transfusion Medicine, National Cerebral and Cardiovascular Center, Fujishirodai Suita City, Osaka, Japan; N. Makhija, M.D., Department of Cardiac Anesthesia, Cardiothoracic Center, New Delhi, India; K. Martin, M.D., Institute of Anesthesiology, German Heart Center Munich, Clinic at the Technical University Munich, Munich, Germany; M. Misfeld, M.D., University Department for Cardiac Surgery, Leipzig Heart Center, Leipzig, Germany; E. Moret, M.D., Department of Anesthesiology, Surgical Intensive Care Unit and Pain Treatment Department, Germans Trias i Pujol University Hospital, Barcelona, Spain; P. S. Myles, M.D., Department of Anesthesiology and Perioperative Medicine, Alfred
Hospital and Monash University, Melbourne, Australia; H. Pleym, M.D., Department of Cardiothoracic Anesthesia and Intensive Care, St. Olav University Hospital, Trondheim, Norway; L. Shore-Lesserson, M.D., Department of Anesthesiology, Zucker School of Medicine at Hofstra/Northwell, Manhasset, New York, New York; S. Sigaut, M.D., Department of Anesthesia and Intensive Care, Beaujon Hospital, Clichy, France; R. G. H. Speekenbrink, M.D., Department of Cardiothoracic Surgery, Medisch Spectrum Twente, Enschede, The Netherlands; M. Yan, M.D., and Z. Zhou, M.D., Department of Anesthesiology, The Second A liated Hospital, School of Medicine, Zhejiang University, Hangzhou, China; and C. Van Aelbrouck, M.D., Department of Anesthesiology, Erasme University Hospital, the Free University of Brussels, Brussels, Belgium. The authors also thank Paula Harry, Ph.D., freelance medical writer and translator, 11 ave-nue Guy de Coubertin, 78470 Saint Rémy lès Chevreuse, France, for revision of the English text.
Research Support
Support was provided solely from institutional and/or departmental sources.
Competing Interests
The authors declare no competing interests.
Correspondence
Address correspondence to Dr. Zu erey: Department of Anesthesiology and Intensive Care, University Hospital of Saint-Etienne, 42055 Saint-Etienne cedex 02, France. paul.zu [email protected] . This article may be accessed for personal use at no charge through the Journal Web site, www.anesthesiology.org.
References
1. Myles PS , Smith JA , Forbes A , Silbert B , Jayarajah M , Painter T , Cooper DJ , Marasco S , McNeil J , Bussi è res JS , McGuinness S , Byrne K , Chan MT , Landoni G , Wallace S ; ATACAS Investigators of the ANZCA Clinical Trials Network : Tranexamic acid in patients undergoing cor-onary-artery surgery. N Engl J Med 2017 ; 376 : 136 – 48
2. Task Force on Patient Blood Management for Adult Cardiac Surgery of the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Cardiothoracic Anaesthesiology (EACTA) , Boer C , Meesters MI , Milojevic M , Benedetto U , Bolliger D , Heymann C von , Jeppsson A , Koster A , Osnabrugge RL , Ranucci M , Ravn HB , Vonk ABA , Wahba A , Pagano D : 2017 EACTS/EACTA Guidelines on patient blood management for adult cardiac surgery. J Cardiothorac Vasc Anesth 2018 ; 32 : 88 – 120
ALNV134N2_Text.indb 176ALNV134N2_Text.indb 176 29-Dec-20 19:43:4129-Dec-20 19:43:41
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:165–78 177
Exposure – Response Relationship of Tranexamic Acid
Zufferey et al .
3. Horrow JC , Van Riper DF , Strong MD , Grunewald KE , Parmet JL : The dose-response relationship of tranexamic acid. A nesthesiology 1995 ; 82 : 383 – 92
4. Dowd NP , Karski JM , Cheng DC , Carroll JA , Lin Y , James RL , Butterworth J : Pharmacokinetics of tranexamic acid during cardiopulmonary bypass. A nesthesiology 2002 ; 97 : 390 – 9
5. Grassin-Delyle S , Tremey B , Abe E , Fischler M , Alvarez JC , Devillier P , Urien S : Population pharmacokinetics of tranexamic acid in adults undergoing cardiac sur-gery with cardiopulmonary bypass. Br J Anaesth 2013 ; 111 : 916 – 24
6. Andersson L , Nilsoon IM , Colleen S , Granstrand B , Melander B : Role of urokinase and tissue activator in sustaining bleeding and the management thereof with EACA and AMCA. Ann N Y Acad Sci 1968 ; 146 : 642 – 58
7. Karski JM , Dowd NP , Joiner R , Carroll J , Peniston C , Bailey K , Glynn MF , Teasdale SJ , Cheng DC : The e ect of three di erent doses of tranexamic acid on blood loss after cardiac surgery with mild systemic hypother-mia (32 degrees C). J Cardiothorac Vasc Anesth 1998 ; 12 : 642 – 6
8. Sigaut S , Tremey B , Ouattara A , Couturier R , Taberlet C , Grassin-Delyle S , Dreyfus JF , Schlumberger S , Fischler M : Comparison of two doses of tranexamic acid in adults undergoing cardiac surgery with cardiopulmo-nary bypass. A nesthesiology 2014 ; 120 : 590 – 600
9. Kalavrouziotis D , Voisine P , Mohammadi S , Dionne S , Dagenais F : High-dose tranexamic acid is an indepen-dent predictor of early seizure after cardiopulmonary bypass. Ann Thorac Surg 2012 ; 93 : 148 – 54
10. Mandema JW , Gibbs M , Boyd RA , Wada DR , P ster M : Model-based meta-analysis for comparative e -cacy and safety: Application in drug development and beyond. Clin Pharmacol Ther 2011 ; 90 : 766 – 9
11. Demin I , Hamr é n B , Luttringer O , Pillai G , Jung T : Longitudinal model-based meta-analysis in rheuma-toid arthritis: An application toward model-based drug development. Clin Pharmacol Ther 2012 ; 92 : 352 – 9
12. Liberati A , Altman DG , Tetzla J , Mulrow C , G ø tzsche PC , Ioannidis JP , Clarke M , Devereaux PJ , Kleijnen J , Moher D : The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009 ; 339 : b2700
13. Martin K , Wiesner G , Breuer T , Lange R , Tassani P : The risks of aprotinin and tranexamic acid in cardiac surgery: A one-year follow-up of 1188 consecutive patients. Anesth Analg 2008 ; 107 : 1783 – 90
14. Vuylsteke A , Pagel C , Gerrard C , Reddy B , Nashef S , Aldam P , Utley M : The Papworth Bleeding Risk Score: A strati cation scheme for identifying cardiac surgery patients at risk of excessive early postoperative bleed-ing. Eur J Cardiothorac Surg 2011 ; 39 : 924 – 30
15. Klein AA , Collier T , Yeates J , Miles LF , Fletcher SN , Evans C , Richards T ; Contributors : The ACTA PORT-score for predicting perioperative risk of blood trans-fusion for adult cardiac surgery. Br J Anaesth 2017 ; 119 : 394 – 401
16. Sharma V , Katznelson R , Jerath A , Garrido-Olivares L , Carroll J , Rao V , Wasowicz M , Djaiani G : The associa-tion between tranexamic acid and convulsive seizures after cardiac surgery: A multivariate analysis in 11 529 patients. Anaesthesia 2014 ; 69 : 124 – 30
17. Wells G , Shea B , O ’ Connell D , Peterson J , Welch V , Losos M , Tugwell P: The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp . Accessed September 17, 2020.
18. Wan X , Wang W , Liu J , Tong T : Estimating the sam-ple mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 2014 ; 14 : 135
19. Higgins JP , White IR , Anzures-Cabrera J : Meta-analysis of skewed data: Combining results reported on log-transformed or raw scales. Stat Med 2008 ; 27 : 6072 – 92
20. Buuren S van , Groothuis-Oudshoorn K : mice: Multivariate Imputation by Chained Equations in R. J Stat Softw 2011 ; 45 : 1 – 67
21. R: The R Project for Statistical Computing. Available at: https://www.r-project.org/ . Accessed September 17, 2020.
22. Vehtari A , Gelman A , Gabry J : Practical Bayesian model evaluation using leave-one-out cross-validation and WAIC. Stat Comput 2017 ; 27 : 1413 – 32
23. Wickham H : ggplot2. WIREs Comput Stat 2011 ; 3 : 180 – 5
24. Fergusson DA , H é bert PC , Mazer CD , Fremes S , MacAdams C , Murkin JM , Teoh K , Duke PC , Arellano R , Blajchman MA , Bussi è res JS , C ô t é D , Karski J , Martineau R , Robblee JA , Rodger M , Wells G , Clinch J , Pretorius R ; BART Investigators : A comparison of aprotinin and lysine analogues in high-risk cardiac sur-gery. N Engl J Med 2008 ; 358 : 2319 – 31
25. Lambert W , Brisebois FJ , Wharton TJ , Carrier RC , Boyle D , Rowe BH : The e ectiveness of low dose tranexamic acid in primary cardiac surgery. Can J Anaesth 1998 ; 45 : 571 – 4
26. Holford NH , Sheiner LB : Understanding the dose-ef-fect relationship: Clinical application of pharmacoki-netic-pharmacodynamic models. Clin Pharmacokinet 1981 ; 6 : 429 – 53
27. Henry DA , Carless PA , Moxey AJ , O ’ Connell D , Stokes BJ , Fergusson DA , Ker K : Anti- brinolytic use for minimising perioperative allogeneic blood transfu-sion. Cochrane Database Syst Rev 2011 : CD001886 doi: 10.1002/14651858.CD001886.pub4
ALNV134N2_Text.indb 177ALNV134N2_Text.indb 177 29-Dec-20 19:43:4129-Dec-20 19:43:41
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
178 Anesthesiology 2021; 134:165–78
PERIOPERATIVE MEDICINE
Zufferey et al .
28. Brown RS , Thwaites BK , Mongan PD : Tranexamic acid is e ective in decreasing postoperative bleeding and transfusions in primary coronary artery bypass operations: A double-blind, randomized, placebo-con-trolled trial. Anesth Analg 1997 ; 85 : 963 – 70
29. Fiechtner BK , Nuttall GA , Johnson ME , Dong Y , Sujirattanawimol N , Oliver WC Jr , Sarpal RS , Oyen LJ , Ereth MH : Plasma tranexamic acid concentrations during cardiopulmonary bypass. Anesth Analg 2001 ; 92 : 1131 – 6
30. Casati V , Bellotti F , Gerli C , Franco A , Oppizzi M , Cossolini M , Calori G , Benussi S , Al eri O , Torri G : Tranexamic acid administration after cardiac surgery: A prospective, randomized, double-blind, placebo-con-trolled study. A nesthesiology 2001 ; 94 : 8 – 14
31. Sharma V , Fan J , Jerath A , Pang KS , Bojko B , Pawliszyn J , Karski JM , Yau T , McCluskey S , W ą sowicz M : Pharmacokinetics of tranexamic acid in patients undergoing cardiac surgery with use of cardiopulmo-nary bypass. Anaesthesia 2012 ; 67 : 1242 – 50
32. Yang QJ , Jerath A , Bies RR , W ą sowicz M , Pang KS : Pharmacokinetic modeling of tranexamic acid for
patients undergoing cardiac surgery with normal renal function and model simulations for patients with renal impairment. Biopharm Drug Dispos 2015 ; 36 : 294 – 307
33. Jerath A , Yang QJ , Pang KS , Looby N , Reyes-Garces N , Vasiljevic T , Bojko B , Pawliszyn J , Wijeysundera D , Beattie WS , Yau TM , W ą sowicz M : Tranexamic acid dosing for cardiac surgical patients with chronic renal dysfunction: A new dosing regimen. Anesth Analg 2018 ; 127 : 1323 – 32
34. Hutton B , Joseph L , Fergusson D , Mazer CD , Shapiro S , Tinmouth A : Risks of harms using anti brinolyt-ics in cardiac surgery: Systematic review and network meta-analysis of randomised and observational studies. BMJ 2012 ; 345 : e5798
35. Grimes DA , Schulz KF : Bias and causal associations in observational research. Lancet 2002 ; 359 : 248 – 52
36. Lecker I , Wang DS , Whissell PD , Avramescu S , Mazer CD , Orser BA : Tranexamic acid-associated seizures: Causes and treatment. Ann Neurol 2016 ; 79 : 18 – 26
37. Thompson SG , Higgins JP : How should meta-regres-sion analyses be undertaken and interpreted? Stat Med 2002 ; 21 : 1559 – 73
ALNV134N2_Text.indb 178ALNV134N2_Text.indb 178 29-Dec-20 19:43:4129-Dec-20 19:43:41
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
PERIOPERATIVE MEDICINE
ANESTHESIOLOGY, V 134 • NO 2 FEBRUARY 2021 179
ABSTRACT Background: The optimal method for blood pressure monitoring in obese surgical patients remains unknown. Arterial catheters can cause potential complications, and noninvasive oscillometry provides only intermittent values. Finger cuff methods allow continuous noninvasive monitoring. The authors tested the hypothesis that the agreement between fi nger cuff and intraarte-rial measurements is better than the agreement between oscillometric and intraarterial measurements.
Methods: This prospective study compared intraarterial (reference method), fi nger cuff, and oscillometric (upper arm, forearm, and lower leg) blood pres-sure measurements in 90 obese patients having bariatric surgery using Bland – Altman analysis, four-quadrant plot and concordance analysis (to assess the ability of monitoring methods to follow blood pressure changes), and error grid analysis (to describe the clinical relevance of measurement differences).
Results: The difference (mean ± SD) between fi nger cuff and intraarterial measurements was − 1 mmHg ( ± 11 mmHg) for mean arterial pressure, − 7 mmHg ( ± 14 mmHg) for systolic blood pressure, and 0 mmHg ( ± 11 mmHg) for diastolic blood pressure. Concordance between changes in fi nger cuff and intraarterial measurements was 88% (mean arterial pressure), 85% (systolic blood pressure), and 81% (diastolic blood pressure). In error grid analysis comparing fi nger cuff and intraarterial measurements, the proportions of measurements in risk zones A to E were 77.1%, 21.6%, 0.9%, 0.4%, and 0.0% for mean arterial pressure, respectively, and 89.5%, 9.8%, 0.2%, 0.4%, and 0.2%, respectively, for systolic blood pressure. For mean arterial pres-sure and diastolic blood pressure, absolute agreement and trending agree-ment between fi nger cuff and intraarterial measurements were better than between oscillometric (at each of the three measurement sites) and intraarte-rial measurements. Forearm performed better than upper arm and lower leg monitoring with regard to absolute agreement and trending agreement with intraarterial monitoring.
Conclusions: The agreement between fi nger cuff and intraarterial mea-surements was better than the agreement between oscillometric and intraar-terial measurements for mean arterial pressure and diastolic blood pressure in obese patients during surgery. Forearm oscillometry exhibits better measure-ment performance than upper arm or lower leg oscillometry.
(ANESTHESIOLOGY 2021 ; 134 : 179 – 88 )
Intraoperative Blood Pressure Monitoring in Obese Patients Arterial Catheter, Finger Cuff, and Oscillometry Roman Schumann , M.D. , Agnes S. Meidert , M.D. , Iwona Bonney , Ph.D. , Christos Koutentis , M.B., Ch.B., M.S. , Wilbert Wesselink , Ph.D. , Karim Kouz , M.D. , Bernd Saugel , M.D.
ANESTHESIOLOGY 2021 ; 134 : 179 – 88
This article is featured in “This Month in Anesthesiology,” page 1A. Supplemental Digital Content is available for this article. Direct URL citations appear in the printed text and are available in both the HTML and PDF versions of this article. Links to the digital fi les are provided in the HTML text of this article on the Journal ’ s Web site (www.anesthesiology.org). This article has a video abstract. This article has a visual abstract available in the online version. Part of the work presented in this article has been presented at the American Society of Anesthesiologists annual meeting in Chicago, Illinois, October 22 to 26, 2016. R.S. and A.S.M. contributed equally to this article.
Submitted for publication April 8, 2020. Accepted for publication November 3, 2020. Published online fi rst on December 15, 2020. From the Department of Anesthesiology and Perioperative Medicine, Tufts University School of Medicine, Boston, Massachusetts (R.S., I.B.); Department of Anaesthesiology, University Hospital Ludwig Maximilian University of Munich, Munich, Germany (A.S.M.); Department of Anesthesiology, State University of New York Downstate Health Sciences University, New York, New York (C.K.); Edwards Lifesciences, Irvine, California (W.W.); Department of Anesthesiology, Center of Anesthesiology and Intensive Care Medicine, University Medical Center Hamburg-Eppendorf, Hamburg, Germany (K.K., B.S.); and Outcomes Research Consortium, Cleveland, Ohio (B.S.).
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved. Anesthesiology 2021 ; 134 : 179 – 88 . DOI: 10.1097/ALN.0000000000003636
EDITOR ’ S PERSPECTIVE
What We Already Know about This Topic
• Optimal blood pressure monitoring in obese surgical patients remains unknown because multiple invasive and noninvasive moni-toring methods are available with little understanding of agreement between different methods.
What This Article Tells Us That Is New
• In a study of 90 obese patients having bariatric surgery, the agree-ment between finger cuff and intraarterial measurements was better than the agreement between oscillometric and intraarterial measurements for mean arterial and diastolic blood pressure, but not systolic blood pressure. Forearm oscillometry demonstrated better measurement performance than upper arm or lower leg oscillometry.
Close blood pressure monitoring is important in obese patients having surgery because those patients are at
high risk of cardiac complications. 1 , 2 However, in clinical practice, choosing the optimal method for perioperative blood pressure monitoring in obese patients is a challenge.
Invasive continuous blood pressure monitoring using an arterial catheter ( i.e. , intraarterial blood pressure monitoring)
is the clinical reference method, but is associated with potential complications such as permanent ischemic damage (mean incidence, 0.1%), bleeding (mean incidence, 0.5%), or local infection (mean incidence, 0.7%). 3 , 4 Additionally, arterial catheter placement can be technically challenging
ALNV134N2_Text.indb 179ALNV134N2_Text.indb 179 29-Dec-20 19:43:4229-Dec-20 19:43:42
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

180 Anesthesiology 2021; 134:179–88
PERIOPERATIVE MEDICINE
Schumann et al.
in morbidly obese patients. Oscillometry using an in at-able cu enables noninvasive blood pressure monitoring, but provides blood pressure values only intermittently, and the measurement performance depends on the selection of the appropriate cu size and cu positioning. 5 , 6 Ideally, the cu size needs to be matched to the circumference of the extremity used for oscillometry — usually the upper arm — to obtain reliable measurements. Obesity is frequently asso-ciated with an increased circumference and a conical rather than cylindrical shape of the upper arm. These changes can make correct cu placement di cult. Therefore, it has been proposed to use the forearm instead of the upper arm for oscillometry in obese patients. 7
Considering the limitations of both continuous intraar-terial and intermittent noninvasive oscillometric blood pressure monitoring, innovative technologies allowing for continuous noninvasive blood pressure monitoring may be a promising option in obese patients during surgery. One of those continuous noninvasive blood pressure monitor-ing technologies is the nger cu – based vascular unload-ing technology that is also referred to as the volume clamp method. 8
For the nger cu technology to be considered for routine blood pressure monitoring, its measurement per-formance needs to be investigated in comparison to the established reference methods: continuous intraarterial blood pressure monitoring using an arterial catheter and intermittent noninvasive blood pressure monitoring using oscillometry.
We therefore compared continuous noninvasive nger cu with continuous intraarterial blood pressure measure-ments using a radial artery catheter in a prospective method comparison study in obese patients having bariatric surgery. We also compared intermittent noninvasive oscillometric blood pressure measurements at the upper arm, forearm, and lower leg with intraarterial blood pressure measurements.
Materials and Methods
Study Design and Patients
This prospective method comparison study was reviewed and approved by the Tufts Health Sciences Institutional Review Board (Boston, Massachusetts; No. 9743). We obtained written informed consent from all patients. Adult patients with a body mass index greater than or equal to 40 kg/m 2 scheduled for elective laparoscopic bariatric sur-gery (gastric bypass, sleeve gastrectomy, and gastric banding) and an American Society of Anesthesiologists Physical Status classi cation of less than IV were eligible for study inclusion. Exclusion criteria were the presence of peripheral upper or lower extremity edema, vascular or anatomical abnormal-ities, history of ipsilateral axillary or inguinal lymph node dissection, carpal tunnel syndrome, negative modi ed Allen test and absence of a palpable ipsilateral ulnar pulse, and atrial
brillation. Data were collected between September 2011 and February 2013.
Anesthesia Management
All patients received a similar general anesthetic regimen at the discretion of the anesthesia team. A representative com-bination of medications to facilitate induction of general anesthesia and endotracheal intubation consisted of intra-venous propofol (1 to 2 mg/kg adjusted body weight), fen-tanyl (1 µ g/kg adjusted body weight), lidocaine 100 mg, and rocuronium bromide (0.8 mg/kg adjusted body weight), or succinylcholine (1.5 mg/kg adjusted body weight). Either sevo urane or des urane in combination with fentanyl and hydromorphone was administered for maintenance of gen-eral anesthesia. During surgical preparation of the abdomen and at skin closure, the patients were positioned horizon-tally, and during surgery, a reverse Trendelenburg position was maintained. Both arms were extended and secured on padded arm boards.
Blood Pressure Measurements
We recorded continuous intraarterial blood pressure using a radial artery catheter (reference method), as well as con-tinuous noninvasive nger cu blood pressure and inter-mittent noninvasive oscillometric upper arm, forearm, and lower leg blood pressure (test methods).
To measure continuous intraarterial blood pressure, we inserted a 20-gauge arterial catheter in the radial artery after induction of general anesthesia and connected it to a disposable pressure transducer. The pressure transducer was leveled to the level of the right atrium throughout the study. The transducer system was examined for its damping prop-erties with a fast ush test, and, if necessary, actions were taken to correct abnormal damping.
To record continuous noninvasive nger cu blood pres-sure, we used the nger cu system ccNex n (BMEYE B.V., The Netherlands) — now ClearSight (Edwards Lifesciences, USA). The ccNex n/ClearSight system uses an in atable nger cu with an infrared plethysmograph to measure the blood volume in the nger arteries, keep the blood volume constant throughout the cardiac cycle based on an auto-mated feedback system that in ates and de ates the nger cu , and indirectly reconstruct the blood pressure wave-form based on the required cu pressure. The nger cu was tted and placed on the middle phalanx of the third or fourth nger according to the manufacturer ’ s speci cation for proper t. The heart reference system that compensates for hydrostatic pressure di erences between the level of the heart and the nger cu was positioned at the level of the right atrium during the entire study period.
Intermittent noninvasive oscillometric blood pressure was measured using a standard large cu at the upper arm, a stan-dard adult cu at the forearm, and a standard large cu at the lower leg (all cu s Criticon; GE Healthcare, USA). To re ect
ALNV134N2_Text.indb 180ALNV134N2_Text.indb 180 29-Dec-20 19:43:4229-Dec-20 19:43:42
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:179–88 181
Blood Pressure Monitoring in Obese Patients
Schumann et al.
daily clinical practice, cu t was accepted when blood pressure measurements could be obtained. A cu that would not allow for circumferential closure or that would spontaneously come undone during an in ation cycle despite the most feasible limb alignment was considered a cu failure for that limb site, and no aids such as tape were used to rescue potential measure-ments. Oscillometric lower leg blood pressure measurements obtained during steep reverse Trendelenburg positioning were not included in the analysis because hydrostatic pressure di er-ences would have in uenced the di erence between lower leg and intraarterial blood pressure measurements.
Intraarterial, nger cu , upper arm, and forearm blood pressure measurements were taken at the ipsilateral arm of the patient so as to avoid any e ect of blood pressure di erences between both upper extremities on study mea-surements. For lower leg blood pressure measurements, the cu was applied to the right leg. Intraarterial and oscillo-metric blood pressure measurements were displayed on the patient monitor (Philips Intellivue MP 90 anesthesia mon-itor; Philips Healthcare, USA). Finger cu blood pressure measurements were displayed on and extracted from the proprietary monitor of the ccNex n system.
We recorded mean arterial pressure, systolic blood pres-sure, and diastolic blood pressure at six di erent time points during the study period. Each measurement cycle com-menced with the simultaneous recording of intraarterial and nger cu blood pressure measurements followed by forearm, upper arm, and nally, lower leg blood pressure measurements. The six time points were chosen as follows: within 15 min before abdominal insu ation in the hori-zontal position; 3, 15, 30, and 45 min after the beginning of insu ation in the 30 ° reverse Trendelenburg position; and 3 min after desu ation in the horizontal position. Visual inspection of the intraarterial blood pressure waveform just before each point of observation allowed for correction of any observed obvious blood pressure waveform artifacts or abnormalities.
Statistical Analysis
Patient characteristics are described as mean ± SD or abso-lute numbers with percentages, blood pressure values as mean ± SD and range. To illustrate the distribution of nger cu , upper arm, forearm, and lower leg blood pressure measure-ments and their relation to intraarterial blood pressure mea-surements, we calculated the Pearson correlation coe cient.
To assess the agreement between nger cu and intraar-terial blood pressure measurements, as well as between upper arm, forearm, and lower leg blood pressure measure-ments and intraarterial blood pressure measurements, we performed Bland – Altman analysis accounting for repeated measurements, 9 , 10 and calculated the mean of the di er-ences (bias), SD, and 95% limits of agreement (mean of the di erences ± 1.96 × SD). The relationships between means and di erences are shown in the Bland – Altman plots and were examined by linear regression analyses.
We computed four-quadrant plots with an exclusion zone of 5 mmHg and calculated the concordance rate to describe the trending ability of nger cu , upper arm, fore-arm, and lower leg blood pressure measurements in com-parison with intraarterial blood pressure measurements. 11
We performed continuous error grid analysis to classify measurement di erences between blood pressure monitor-ing methods according to their clinical importance. 12 , 13 An error grid is a scatter plot with reference blood pressure mea-surements on the x-axis and corresponding blood pressure measurements from the investigated method on the y-axis, and it contains ve risk zones. 12 , 13 Each blood pressure mea-surement pair is classi ed into one of ve di erent risk zones. Those risk zones describe the risk for patients resulting from therapeutic interventions that may be triggered by measure-ment di erences between the investigated method and the reference method and are classi ed as follows: risk zone A: no risk; risk zone B: low risk; risk zone C: moderate risk; risk zone D: signi cant risk; and risk zone E: dangerous risk. 12 , 13
The risk zone boundaries in the error grid result from a survey among 25 experts who were rst asked to de ne ve blood pressure ranges that would, according to the experts ’ experience and judgment, need to result in the following therapeutic reactions: emergency treatment for low blood pressure necessary; treatment of low blood pressure appro-priate; no intervention needed; treatment of high blood pressure appropriate; and emergency treatment for high blood pressure necessary. 12 , 13 The experts then attributed risk levels to combinations of “ blood pressure measurement with investigated method is in range i” and “ reference blood pressure measurement is in range j, ” considering patient risk that would result from measurement di erences. 12 , 13 The experts ’ aggregated and weighted answers regarding the ve risk levels resulted in the error grid risk zones. 12 , 13 Details on how smoothing polygons were tted to the boundar-ies between the zones including coordinates of the result-ing polygons and the aggregated risk scores are provided in our original paper. 12 , 13 To better illustrate the di erent risk zones in the error grid, colors are used ranging from green (no risk) to red (dangerous risk). 12 , 13 Patient risk resulting from measurement di erences can thus be visually assessed from the color-coded continuous error grid and quantita-tively analyzed by calculating absolute and relative numbers of measurement pairs within the risk zones. 12 , 13
For statistical analysis, we used Excel (Version 1912; Microsoft, USA), R (Version 3.6.2.; The R Foundation for Statistical Computing, Vienna, Austria), and, for error grid analysis, MATLAB (The MathWorks Inc., USA).
No statistical power calculation was conducted before the study. The sample size was based on our previous expe-rience with method comparison studies.
Results We enrolled 108 patients in this study. Eighteen patients dropped out for the following reasons: technical di culties
ALNV134N2_Text.indb 181ALNV134N2_Text.indb 181 29-Dec-20 19:43:4229-Dec-20 19:43:42
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

182 Anesthesiology 2021; 134:179–88
PERIOPERATIVE MEDICINE
Schumann et al.
with the insertion of the arterial catheter (n = 11); technical failures with blood pressure monitoring equipment during the procedure (n = 3); change of the surgical procedure (n = 1); patient ’ s withdrawal from participation (n = 1); discovery of missed exclusion criterion (n = 1); and case canceled (n = 1). Hence, we included 90 patients in the nal analysis with a mean ± SD body mass index of 48 ± 7 kg/m 2 . Patient characteristics are summarized in table 1 . Of paired blood pressure measurements available for anal-ysis, 538 were nger cu , 443 were upper arm, 535 were forearm, and 111 were lower leg (Supplemental Digital Content 1, http://links.lww.com/ALN/C516). Cu fail-ure occurred in 8 upper arm, 1 forearm, and 11 lower leg blood pressure measurements. In some cases, there was no cu large enough to t the upper arm (6 patients) or the lower leg (24 patients), whereas this problem did not occur on the forearm. Details on missing values are provided in Supplemental Digital Content 2 (http://links.lww.com/ALN/C517).
The distribution of nger cu , upper arm, forearm, and lower leg blood pressure measurements and their relation to intraarterial blood pressure measurements are shown in Supplemental Digital Content 3 (http://links.lww.com/ALN/C518).
Bland – Altman analysis revealed a mean of the di er-ences ( ± SD, 95% limits of agreement) between nger cu and intraarterial blood pressure measurements of − 1 mmHg ( ± 11 mmHg, − 23 to 21 mmHg) for mean arterial pressure, of − 7 mmHg ( ± 14 mmHg, − 35 to 20 mmHg) for systolic blood pressure, and of 0 mmHg ( ± 11 mmHg, − 22 to 22 mmHg) for diastolic blood pressure ( g. 1A ; table 2 ). Bland – Altman analyses for the comparison of upper arm, forearm, and lower leg blood pressure measurements with intraarterial blood pressure measurements are shown in g-ure 1 , B through D, and table 2 . For mean arterial pressure
and diastolic blood pressure, the mean of the di erences and SD between oscillometric (at each of the three measure-ment sites) and intraarterial blood pressure measurements was higher than between nger cu and intraarterial blood pressure measurements.
Four-quadrant plot analysis revealed a concordance rate between changes in nger cu and in intraarterial blood pressure measurements of 88% for mean arterial pres-sure, 85% for systolic blood pressure, and 81% for diastolic blood pressure ( g. 2 ; table 2 ). Four-quadrant plot analyses for upper arm and forearm blood pressure measurements in comparison with intraarterial blood pressure measure-ments are shown in table 2 and Supplemental Digital Content 4 (http://links.lww.com/ALN/C519). For mean arterial pressure, the concordance rate between changes in oscillometric (at each of the three measurement sites) and intraarterial blood pressure measurements was lower than between changes in nger cu and intraarterial blood pres-sure measurements.
Error grid analysis for the comparison between nger cu and intraarterial blood pressure measurements revealed that the proportions of measurement pairs in risk zones A to E were 77.1%, 21.6%, 0.9%, 0.4%, and 0.0%, respectively, for mean arterial pressure and 89.5%, 9.8%, 0.2%, 0.4%, and 0.2%, respectively, for systolic blood pressure ( g. 3 , A and B; table 3 ). Error grids analyses for upper arm, forearm, and lower leg blood pressure measurements in comparison with intraarterial blood pressure measurements are provided in table 3 and Supplemental Digital Content 5 (http://links.lww.com/ALN/C520).
Discussion In this method comparison study, we compared intraarte-rial with nger cu blood pressure measurements and with upper arm, forearm, and lower leg blood pressure measure-ments in obese patients during bariatric surgery across a wide range of blood pressure values. The absolute agree-ment and the trending agreement of nger cu blood pres-sure measurements compared to intraarterial blood pressure measurements were only moderate. However, error grid analysis showed that about 99% of nger cu blood pres-sure measurements lay in risk zones A ( “ no risk ” ) and B ( “ low risk ” ). For mean arterial pressure and diastolic blood pressure, the absolute agreement and the trending agree-ment between nger cu and intraarterial blood pressure measurements were better than between oscillometric (at each of the three measurement sites) and intraarterial blood pressure measurements. Forearm blood pressure monitor-ing performed better than upper arm and lower leg blood pressure monitoring with regard to absolute and trending agreement with intraarterial blood pressure monitoring.
Several previous studies compared ccNex n/ClearSight blood pressure measurements with intraarterial reference blood pressure measurements using an arterial catheter in mixed patient populations not explicitly focusing on obese
Table 1. Patient Characteristics
Demographic and biometric data (n = 90 patients)
Age, yr 47 ± 13 Male, n (%) 26 (29) Weight, kg 136 ± 27 Height, cm 167 ± 10 Body mass index, kg/m 2 48 ± 7 American Society of Anesthesiologists Physical Status class II, n (%) 16 (18) III, n (%) 74 (82) Extremity circumference Upper arm, cm 43 ± 5 Forearm, cm 31 ± 3 Lower leg, cm 49 ± 6 Type of bariatric surgery Gastric bypass, n (%) 51 (57) Sleeve gastrectomy, n (%) 38 (42) Gastric banding, n (%) 1 (1)
Categorial variables are presented as absolute frequencies and percentages, con-tinuous variables as mean ± SD.
ALNV134N2_Text.indb 182ALNV134N2_Text.indb 182 29-Dec-20 19:43:4229-Dec-20 19:43:42
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
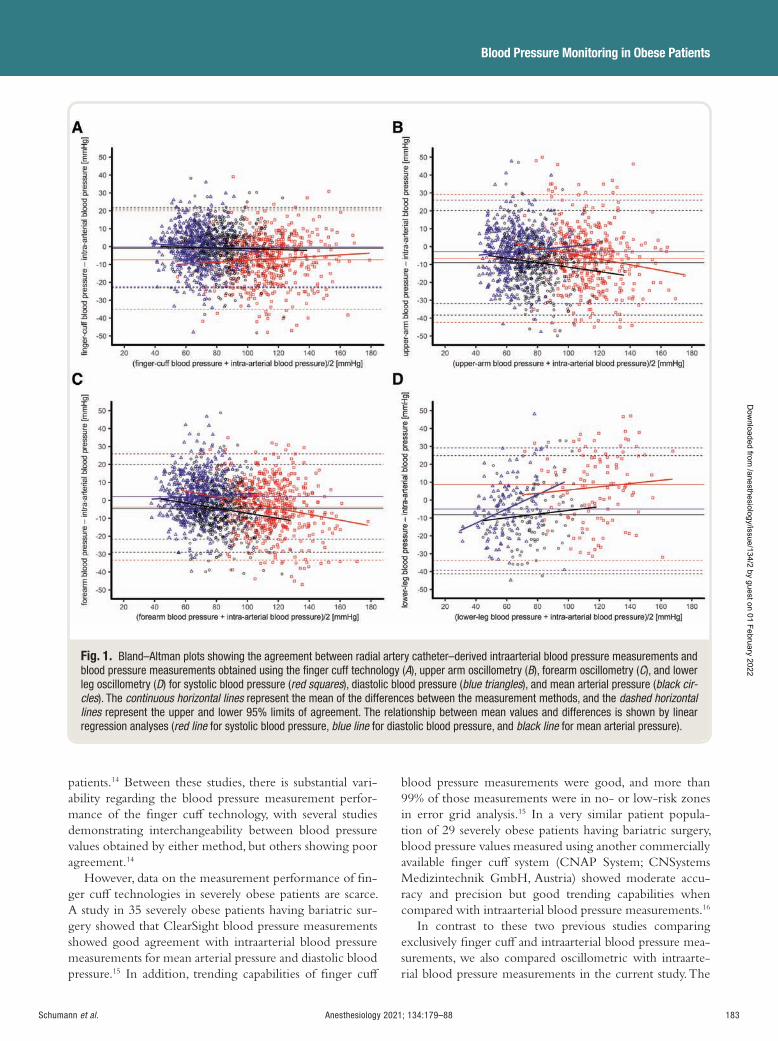
Anesthesiology 2021; 134:179–88 183
Blood Pressure Monitoring in Obese Patients
Schumann et al.
patients. 14 Between these studies, there is substantial vari-ability regarding the blood pressure measurement perfor-mance of the nger cu technology, with several studies demonstrating interchangeability between blood pressure values obtained by either method, but others showing poor agreement. 14
However, data on the measurement performance of n-ger cu technologies in severely obese patients are scarce. A study in 35 severely obese patients having bariatric sur-gery showed that ClearSight blood pressure measurements showed good agreement with intraarterial blood pressure measurements for mean arterial pressure and diastolic blood pressure. 15 In addition, trending capabilities of nger cu
blood pressure measurements were good, and more than 99% of those measurements were in no- or low-risk zones in error grid analysis. 15 In a very similar patient popula-tion of 29 severely obese patients having bariatric surgery, blood pressure values measured using another commercially available nger cu system (CNAP System; CNSystems Medizintechnik GmbH, Austria) showed moderate accu-racy and precision but good trending capabilities when compared with intraarterial blood pressure measurements. 16
In contrast to these two previous studies comparing exclusively nger cu and intraarterial blood pressure mea-surements, we also compared oscillometric with intraarte-rial blood pressure measurements in the current study. The
Fig. 1. Bland – Altman plots showing the agreement between radial artery catheter – derived intraarterial blood pressure measurements and blood pressure measurements obtained using the fi nger cuff technology ( A ), upper arm oscillometry ( B ), forearm oscillometry ( C ), and lower leg oscillometry ( D ) for systolic blood pressure ( red squares ), diastolic blood pressure ( blue triangles ), and mean arterial pressure ( black cir-cles ). The continuous horizontal lines represent the mean of the differences between the measurement methods, and the dashed horizontal lines represent the upper and lower 95% limits of agreement. The relationship between mean values and differences is shown by linear regression analyses ( red line for systolic blood pressure, blue line for diastolic blood pressure, and black line for mean arterial pressure).
ALNV134N2_Text.indb 183ALNV134N2_Text.indb 183 29-Dec-20 19:43:4329-Dec-20 19:43:43
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
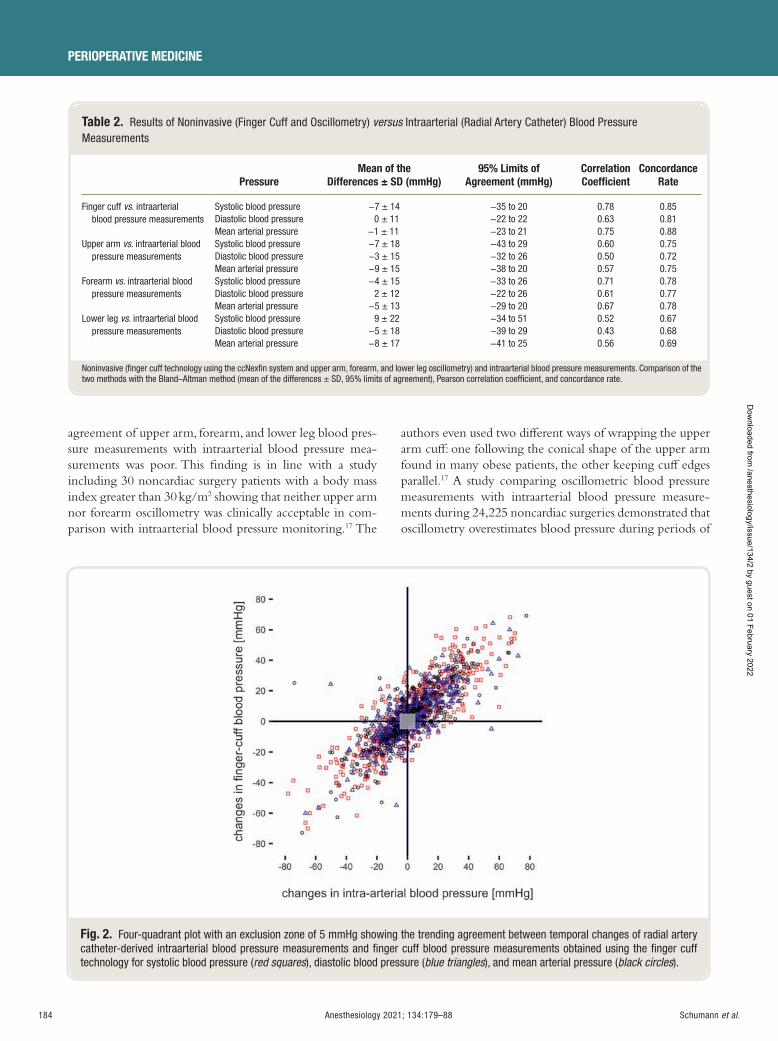
184 Anesthesiology 2021; 134:179–88
PERIOPERATIVE MEDICINE
Schumann et al.
agreement of upper arm, forearm, and lower leg blood pres-sure measurements with intraarterial blood pressure mea-surements was poor. This nding is in line with a study including 30 noncardiac surgery patients with a body mass index greater than 30 kg/m 2 showing that neither upper arm nor forearm oscillometry was clinically acceptable in com-parison with intraarterial blood pressure monitoring. 17 The
authors even used two di erent ways of wrapping the upper arm cu : one following the conical shape of the upper arm found in many obese patients, the other keeping cu edges parallel. 17 A study comparing oscillometric blood pressure measurements with intraarterial blood pressure measure-ments during 24,225 noncardiac surgeries demonstrated that oscillometry overestimates blood pressure during periods of
Table 2. Results of Noninvasive (Finger Cuff and Oscillometry) versus Intraarterial (Radial Artery Catheter) Blood Pressure Measurements
Pressure Mean of the
Differences ± SD (mmHg) 95% Limits of
Agreement (mmHg) Correlation Coeffi cient
Concordance Rate
Finger cuff vs . intraarterial blood pressure measurements
Systolic blood pressure − 7 ± 14 − 35 to 20 0.78 0.85 Diastolic blood pressure 0 ± 11 − 22 to 22 0.63 0.81 Mean arterial pressure − 1 ± 11 − 23 to 21 0.75 0.88
Upper arm vs . intraarterial blood pressure measurements
Systolic blood pressure − 7 ± 18 − 43 to 29 0.60 0.75 Diastolic blood pressure − 3 ± 15 − 32 to 26 0.50 0.72 Mean arterial pressure − 9 ± 15 − 38 to 20 0.57 0.75
Forearm vs . intraarterial blood pressure measurements
Systolic blood pressure − 4 ± 15 − 33 to 26 0.71 0.78 Diastolic blood pressure 2 ± 12 − 22 to 26 0.61 0.77 Mean arterial pressure − 5 ± 13 − 29 to 20 0.67 0.78
Lower leg vs . intraarterial blood pressure measurements
Systolic blood pressure 9 ± 22 − 34 to 51 0.52 0.67 Diastolic blood pressure − 5 ± 18 − 39 to 29 0.43 0.68 Mean arterial pressure − 8 ± 17 − 41 to 25 0.56 0.69
Noninvasive (fi nger cuff technology using the ccNexfi n system and upper arm, forearm, and lower leg oscillometry) and intraarterial blood pressure measurements. Comparison of the two methods with the Bland – Altman method (mean of the differences ± SD, 95% limits of agreement), Pearson correlation coeffi cient, and concordance rate.
Fig. 2. Four-quadrant plot with an exclusion zone of 5 mmHg showing the trending agreement between temporal changes of radial artery catheter-derived intraarterial blood pressure measurements and fi nger cuff blood pressure measurements obtained using the fi nger cuff technology for systolic blood pressure ( red squares ), diastolic blood pressure ( blue triangles ), and mean arterial pressure ( black circles ).
ALNV134N2_Text.indb 184ALNV134N2_Text.indb 184 29-Dec-20 19:43:4329-Dec-20 19:43:43
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
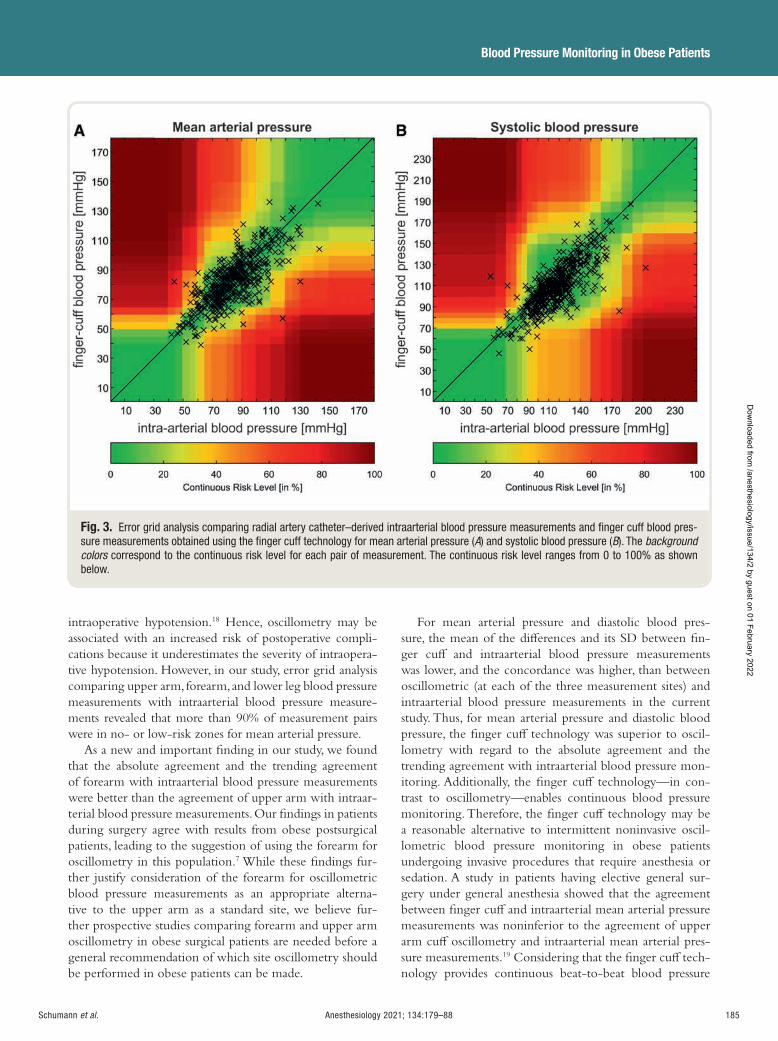
Anesthesiology 2021; 134:179–88 185
Blood Pressure Monitoring in Obese Patients
Schumann et al.
intraoperative hypotension. 18 Hence, oscillometry may be associated with an increased risk of postoperative compli-cations because it underestimates the severity of intraopera-tive hypotension. However, in our study, error grid analysis comparing upper arm, forearm, and lower leg blood pressure measurements with intraarterial blood pressure measure-ments revealed that more than 90% of measurement pairs were in no- or low-risk zones for mean arterial pressure.
As a new and important nding in our study, we found that the absolute agreement and the trending agreement of forearm with intraarterial blood pressure measurements were better than the agreement of upper arm with intraar-terial blood pressure measurements. Our ndings in patients during surgery agree with results from obese postsurgical patients, leading to the suggestion of using the forearm for oscillometry in this population. 7 While these ndings fur-ther justify consideration of the forearm for oscillometric blood pressure measurements as an appropriate alterna-tive to the upper arm as a standard site, we believe fur-ther prospective studies comparing forearm and upper arm oscillometry in obese surgical patients are needed before a general recommendation of which site oscillometry should be performed in obese patients can be made.
For mean arterial pressure and diastolic blood pres-sure, the mean of the di erences and its SD between n-ger cu and intraarterial blood pressure measurements was lower, and the concordance was higher, than between oscillometric (at each of the three measurement sites) and intraarterial blood pressure measurements in the current study. Thus, for mean arterial pressure and diastolic blood pressure, the nger cu technology was superior to oscil-lometry with regard to the absolute agreement and the trending agreement with intraarterial blood pressure mon-itoring. Additionally, the nger cu technology — in con-trast to oscillometry — enables continuous blood pressure monitoring. Therefore, the nger cu technology may be a reasonable alternative to intermittent noninvasive oscil-lometric blood pressure monitoring in obese patients undergoing invasive procedures that require anesthesia or sedation. A study in patients having elective general sur-gery under general anesthesia showed that the agreement between nger cu and intraarterial mean arterial pressure measurements was noninferior to the agreement of upper arm cu oscillometry and intraarterial mean arterial pres-sure measurements. 19 Considering that the nger cu tech-nology provides continuous beat-to-beat blood pressure
Fig. 3. Error grid analysis comparing radial artery catheter – derived intraarterial blood pressure measurements and fi nger cuff blood pres-sure measurements obtained using the fi nger cuff technology for mean arterial pressure ( A ) and systolic blood pressure ( B ). The background colors correspond to the continuous risk level for each pair of measurement. The continuous risk level ranges from 0 to 100% as shown below.
ALNV134N2_Text.indb 185ALNV134N2_Text.indb 185 29-Dec-20 19:43:4429-Dec-20 19:43:44
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
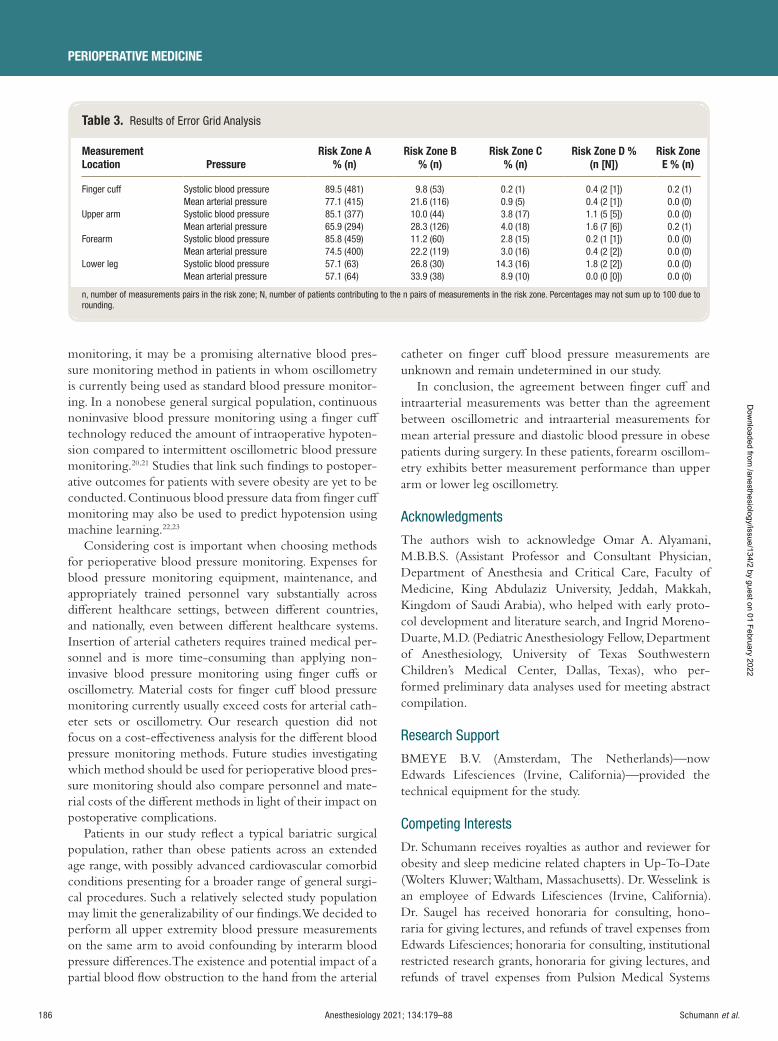
186 Anesthesiology 2021; 134:179–88
PERIOPERATIVE MEDICINE
Schumann et al.
monitoring, it may be a promising alternative blood pres-sure monitoring method in patients in whom oscillometry is currently being used as standard blood pressure monitor-ing. In a nonobese general surgical population, continuous noninvasive blood pressure monitoring using a nger cu technology reduced the amount of intraoperative hypoten-sion compared to intermittent oscillometric blood pressure monitoring. 20 , 21 Studies that link such ndings to postoper-ative outcomes for patients with severe obesity are yet to be conducted. Continuous blood pressure data from nger cu monitoring may also be used to predict hypotension using machine learning. 22 , 23
Considering cost is important when choosing methods for perioperative blood pressure monitoring. Expenses for blood pressure monitoring equipment, maintenance, and appropriately trained personnel vary substantially across di erent healthcare settings, between di erent countries, and nationally, even between di erent healthcare systems. Insertion of arterial catheters requires trained medical per-sonnel and is more time-consuming than applying non-invasive blood pressure monitoring using nger cu s or oscillometry. Material costs for nger cu blood pressure monitoring currently usually exceed costs for arterial cath-eter sets or oscillometry. Our research question did not focus on a cost-e ectiveness analysis for the di erent blood pressure monitoring methods. Future studies investigating which method should be used for perioperative blood pres-sure monitoring should also compare personnel and mate-rial costs of the di erent methods in light of their impact on postoperative complications.
Patients in our study re ect a typical bariatric surgical population, rather than obese patients across an extended age range, with possibly advanced cardiovascular comorbid conditions presenting for a broader range of general surgi-cal procedures. Such a relatively selected study population may limit the generalizability of our ndings. We decided to perform all upper extremity blood pressure measurements on the same arm to avoid confounding by interarm blood pressure di erences. The existence and potential impact of a partial blood ow obstruction to the hand from the arterial
catheter on nger cu blood pressure measurements are unknown and remain undetermined in our study.
In conclusion, the agreement between nger cu and intraarterial measurements was better than the agreement between oscillometric and intraarterial measurements for mean arterial pressure and diastolic blood pressure in obese patients during surgery. In these patients, forearm oscillom-etry exhibits better measurement performance than upper arm or lower leg oscillometry.
Acknowledgments
The authors wish to acknowledge Omar A. Alyamani, M.B.B.S. (Assistant Professor and Consultant Physician, Department of Anesthesia and Critical Care, Faculty of Medicine, King Abdulaziz University, Jeddah, Makkah, Kingdom of Saudi Arabia), who helped with early proto-col development and literature search, and Ingrid Moreno-Duarte, M.D. (Pediatric Anesthesiology Fellow, Department of Anesthesiology, University of Texas Southwestern Children ’ s Medical Center, Dallas, Texas), who per-formed preliminary data analyses used for meeting abstract compilation.
Research Support
BMEYE B.V. (Amsterdam, The Netherlands) — now Edwards Lifesciences (Irvine, California) — provided the technical equipment for the study.
Competing Interests
Dr. Schumann receives royalties as author and reviewer for obesity and sleep medicine related chapters in Up-To-Date (Wolters Kluwer; Waltham, Massachusetts). Dr. Wesselink is an employee of Edwards Lifesciences (Irvine, California). Dr. Saugel has received honoraria for consulting, hono-raria for giving lectures, and refunds of travel expenses from Edwards Lifesciences; honoraria for consulting, institutional restricted research grants, honoraria for giving lectures, and refunds of travel expenses from Pulsion Medical Systems
Table 3. Results of Error Grid Analysis
Measurement Location Pressure
Risk Zone A % (n)
Risk Zone B % (n)
Risk Zone C % (n)
Risk Zone D % (n [N])
Risk Zone E % (n)
Finger cuff Systolic blood pressure 89.5 (481) 9.8 (53) 0.2 (1) 0.4 (2 [1]) 0.2 (1) Mean arterial pressure 77.1 (415) 21.6 (116) 0.9 (5) 0.4 (2 [1]) 0.0 (0)
Upper arm Systolic blood pressure 85.1 (377) 10.0 (44) 3.8 (17) 1.1 (5 [5]) 0.0 (0) Mean arterial pressure 65.9 (294) 28.3 (126) 4.0 (18) 1.6 (7 [6]) 0.2 (1)
Forearm Systolic blood pressure 85.8 (459) 11.2 (60) 2.8 (15) 0.2 (1 [1]) 0.0 (0) Mean arterial pressure 74.5 (400) 22.2 (119) 3.0 (16) 0.4 (2 [2]) 0.0 (0)
Lower leg Systolic blood pressure 57.1 (63) 26.8 (30) 14.3 (16) 1.8 (2 [2]) 0.0 (0) Mean arterial pressure 57.1 (64) 33.9 (38) 8.9 (10) 0.0 (0 [0]) 0.0 (0)
n, number of measurements pairs in the risk zone; N, number of patients contributing to the n pairs of measurements in the risk zone. Percentages may not sum up to 100 due to rounding.
ALNV134N2_Text.indb 186ALNV134N2_Text.indb 186 29-Dec-20 19:43:4429-Dec-20 19:43:44
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:179–88 187
Blood Pressure Monitoring in Obese Patients
Schumann et al.
SE (Feldkirchen, Germany); institutional restricted research grants, honoraria for giving lectures, and refunds of travel expenses from CNSystems Medizintechnik GmbH (Graz, Austria); institutional restricted research grants from Retia Medical LLC (Valhalla, New York); honoraria for giving lectures from Philips Medizin Systeme B ö blingen GmbH (B ö blingen, Germany); and honoraria for consulting, insti-tutional restricted research grants, and refunds of travel expenses from Tensys Medical Inc. (San Diego, California). The other authors declare no competing interesta.
Correspondence
Address correspondence to Dr. Saugel: Department of Anesthesiology, Center of Anesthesiology and Intensive Care Medicine, University Medical Center Hamburg-Eppendorf, Martinistrasse 52, 20246 Hamburg, Germany. [email protected] ; [email protected] . This article may be accessed for personal use at no charge through the Journal Web site, www.anesthesiology.org.
References
1. Cullen A , Ferguson A : Perioperative management of the severely obese patient: A selective pathophysiologi-cal review. Can J Anaesth 2012 ; 59 : 974 – 96
2. Adams JP , Murphy PG : Obesity in anaesthesia and intensive care. Br J Anaesth 2000 ; 85 : 91 – 108
3. Scheer B , Perel A , Pfei er UJ : Clinical review: Complications and risk factors of peripheral arte-rial catheters used for haemodynamic monitoring in anaesthesia and intensive care medicine. Crit Care 2002 ; 6 : 199 – 204
4. Nuttall G , Burckhardt J , Hadley A , Kane S , Kor D , Marienau MS , Schroeder DR , Handlogten K , Wilson G , Oliver WC : Surgical and patient risk factors for severe arterial line complications in adults. A nesthesiology 2016 ; 124 : 590 – 7
5. Bur A , Hirschl MM , Herkner H , Oschatz E , Ko er J , Woisetschl ä ger C , Laggner AN : Accuracy of oscillome-tric blood pressure measurement according to the rela-tion between cu size and upper-arm circumference in critically ill patients. Crit Care Med 2000 ; 28 : 371 – 6
6. Loenneke JP , Loprinzi PD , Abe T , Thiebaud RS , Allen KM , Grant Mouser J , Bemben MG : Arm circumfer-ence in uences blood pressure even when applying the correct cu size: Is a further correction needed? Int J Cardiol 2016 ; 202 : 743 – 4
7. Leblanc M È , Auclair A , Leclerc J , Bussi è res J , Agharazii M , Hould FS , Marceau S , Brassard P , Godbout C , Grenier A , Cloutier L , Poirier P : Blood pressure mea-surement in severely obese patients: Validation of the forearm approach in di erent arm positions. Am J Hypertens 2019 ; 32 : 175 – 85
8. Saugel B , Dueck R , Wagner JY : Measurement of blood pressure. Best Pract Res Clin Anaesthesiol 2014 ; 28 : 309 – 22
9. Bland JM , Altman DG : Measuring agreement in method comparison studies. Stat Methods Med Res 1999 ; 8 : 135 – 60
10. Bland JM , Altman DG : Agreement between methods of measurement with multiple observations per indi-vidual. J Biopharm Stat 2007 ; 17 : 571 – 82
11. Saugel B , Grothe O , Wagner JY : Tracking changes in cardiac output: Statistical considerations on the 4-quad-rant plot and the polar plot methodology. Anesth Analg 2015 ; 121 : 514 – 24
12. Saugel B , Grothe O , Nicklas JY : Error grid analysis for arterial pressure method comparison studies. Anesth Analg 2018 ; 126 : 1177 – 85
13. Grothe O , Kaplan A , Kouz K , Saugel B : Computer program for error grid analysis in arterial blood pres-sure method comparison studies . Anesth Analg 2020 ; 130 : e71 – e74
14. Saugel B , Hoppe P , Nicklas JY , Kouz K , K ö rner A , Hempel JC , Vos JJ , Sch ö n G , Scheeren TWL : Continuous noninvasive pulse wave analysis using n-ger cu technologies for arterial blood pressure and cardiac output monitoring in perioperative and inten-sive care medicine: A systematic review and meta-anal-ysis. Br J Anaesth 2020 ; 125 : 25 – 37
15. Rogge DE , Nicklas JY , Sch ö n G , Grothe O , Haas SA , Reuter DA , Saugel B : Continuous noninvasive arterial pressure monitoring in obese patients during bariat-ric surgery: An evaluation of the vascular unloading technique (ClearSight system). Anesth Analg 2019 ; 128 : 477 – 83
16. Rogge DE , Nicklas JY , Haas SA , Reuter DA , Saugel B : Continuous noninvasive arterial pressure mon-itoring using the vascular unloading technique (CNAP System) in obese patients during laparo-scopic bariatric operations. Anesth Analg 2018 ; 126 : 454 – 63
17. Anast N , Olejniczak M , Ingrande J , Brock-Utne J : The impact of blood pressure cu location on the accuracy of noninvasive blood pressure measurements in obese patients: An observational study. Can J Anaesth 2016 ; 63 : 298 – 306
18. Wax DB , Lin HM , Leibowitz AB : Invasive and con-comitant noninvasive intraoperative blood pressure monitoring: Observed di erences in measurements and associated therapeutic interventions. A nesthesiology 2011 ; 115 : 973 – 8
19. Vos JJ , Poterman M , Mooyaart EA , Weening M , Struys MM , Scheeren TW , Kalmar AF : Comparison of con-tinuous non-invasive nger arterial pressure monitor-ing with conventional intermittent automated arm arterial pressure measurement in patients under general anaesthesia. Br J Anaesth 2014 ; 113 : 67 – 74
ALNV134N2_Text.indb 187ALNV134N2_Text.indb 187 29-Dec-20 19:43:4429-Dec-20 19:43:44
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

188 Anesthesiology 2021; 134:179–88
PERIOPERATIVE MEDICINE
Schumann et al.
20. Maheshwari K , Khanna S , Bajracharya GR , Makarova N , Riter Q , Raza S , Cywinski JB , Argalious M , Kurz A , Sessler DI : A randomized trial of continuous non-invasive blood pressure monitoring during noncardiac surgery. Anesth Analg 2018 ; 127 : 424 – 31
21. Meidert AS , Nold JS , Hornung R , Paulus AC , Zwi ß ler B , Czerner S : The impact of continuous non-invasive arte-rial blood pressure monitoring on blood pressure stabil-ity during general anaesthesia in orthopaedic patients: A randomised trial. Eur J Anaesthesiol 2017 ; 34 : 716 – 22
22. Hatib F , Jian Z , Buddi S , Lee C , Settels J , Sibert K , Rinehart J , Cannesson M : Machine-learning algorithm to pre-dict hypotension based on high- delity arterial pressure waveform analysis. A nesthesiology 2018 ; 129 : 663 – 74
23. Maheshwari K , Buddi S , Jian Z , Settels J , Shimada T , Cohen B , Sessler DI , Hatib F : Performance of the Hypotension Prediction Index with non-in-vasive arterial pressure waveforms in non-cardiac surgical patients . J Clin Monit Comput 2020 ; doi: 10.1007/s10877-020-00463-5 [Epub ahead of print]
ALNV134N2_Text.indb 188ALNV134N2_Text.indb 188 29-Dec-20 19:43:4429-Dec-20 19:43:44
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
PERIOPERATIVE MEDICINE
ANESTHESIOLOGY, V 134 • NO 2 FEBRUARY 2021 189
ABSTRACT Background: Despite evidence suggesting detrimental effects of perioper-ative hyperoxia, hyperoxygenation remains commonplace in cardiac surgery. Hyperoxygenation may increase oxidative damage and neuronal injury leading to potential differences in postoperative neurocognition. Therefore, this study tested the primary hypothesis that intraoperative normoxia, as compared to hyperoxia, reduces postoperative cognitive dysfunction in older patients hav-ing cardiac surgery.
Methods: A randomized double-blind trial was conducted in patients aged 65 yr or older having coronary artery bypass graft surgery with cardiopulmo-nary bypass. A total of 100 patients were randomized to one of two intra-operative oxygen delivery strategies. Normoxic patients (n = 50) received a minimum fraction of inspired oxygen of 0.35 to maintain a Pa o
2 above 70
mmHg before and after cardiopulmonary bypass and between 100 and 150 mmHg during cardiopulmonary bypass. Hyperoxic patients (n = 50) received a fraction of inspired oxygen of 1.0 throughout surgery, irrespective of Pa o
2 lev-
els. The primary outcome was neurocognitive function measured on postop-erative day 2 using the Telephonic Montreal Cognitive Assessment. Secondary outcomes included neurocognitive function at 1, 3, and 6 months, as well as postoperative delirium, mortality, and durations of mechanical ventilation, intensive care unit stay, and hospital stay.
Results: The median age was 71 yr (interquartile range, 68 to 75), and the median baseline neurocognitive score was 17 (16 to 19). The median intraoperative Pa o
2 was 309 (285 to 352) mmHg in the hyperoxia group and
153 (133 to 168) mmHg in the normoxia group ( P < 0.001). The median Telephonic Montreal Cognitive Assessment score on postoperative day 2 was 18 (16 to 20) in the hyperoxia group and 18 (14 to 20) in the normoxia group ( P = 0.42). Neurocognitive function at 1, 3, and 6 months, as well as second-ary outcomes, were not statistically different between groups.
Conclusions: In this randomized controlled trial, intraoperative normoxia did not reduce postoperative cognitive dysfunction when compared to intraop-erative hyperoxia in older patients having cardiac surgery. Although the opti-mal intraoperative oxygenation strategy remains uncertain, the results indicate that intraoperative hyperoxia does not worsen postoperative cognition after cardiac surgery.
(ANESTHESIOLOGY 2021 ; 134 : 189 – 201 )
Intraoperative Oxygen Concentration and Neurocognition after Cardiac Surgery A Randomized Clinical Trial Shahzad Shaefi , M.D. , Puja Shankar , M.D. , Ariel L. Mueller , M.A. , Brian P. O ’ Gara , M.D. , Kyle Spear , C.C.P. , Kamal R. Khabbaz , M.D. , Aranya Bagchi , M.B.B.S. , Louis M. Chu , M.D. , Valerie Banner-Goodspeed , M.P.H. , David E. Leaf , M.D. , Daniel S. Talmor , M.D. , Edward R. Marcantonio , M.D. , Balachundhar Subramaniam , M.D.
ANESTHESIOLOGY 2021 ; 134 : 189 – 201
This article is featured in “This Month in Anesthesiology,” page 1A. Supplemental Digital Content is available for this article. Direct URL citations appear in the printed text and are available in both the HTML and PDF versions of this article. Links to the digital fi les are provided in the HTML text of this article on the Journal ’ s Web site (www.anesthesiology.org). This article has an audio podcast. This article has a visual abstract available in the online version. Part of the work presented in this article has been presented as a poster and oral presentation at the Anesthesiology Annual Meeting in Orlando, Florida, October 20, 2019.
Submitted for publication June 25, 2020. Accepted for publication November 16, 2020. Published online fi rst on December 16, 2020. From the Department of Anesthesia, Critical Care and Pain Medicine (S.S., P.S., A.L.M., B.P.O., V.B.-G., D.S.T., B.S.), the Division of Cardiac Surgery, Department of Surgery (K.S., K.R.K., L.M.C.), and the Division of General Medicine, Department of Medicine (E.R.M.), Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Massachusetts; the Department of Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts (A.L.M., A.B.); and the Division of Renal Medicine, Brigham and Women ’ s Hospital, Harvard Medical School, Boston, Massachusetts (D.E.L.).
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved. Anesthesiology 2021 ; 134 : 189 – 201 . DOI: 10.1097/ALN.0000000000003650
EDITOR ’ S PERSPECTIVE
What We Already Know about This Topic
• High intraoperative inspired oxygen concentration may promote inflammation and consequent neurocognitive injury.
What This Article Tells Us That Is New
• A total of 100 cardiac surgical patients were randomly assigned to 35 or 100% inspired oxygen before and after cardiopulmonary bypass.
• Neurocognitive function 2 days, 1 month, 3 months, and 6 months after surgery was similar in each group.
• Supplemental intraoperative oxygen does not worsen postoperative neurocognitive function. Inspired oxygen fraction should be chosen on the basis of other considerations.
Each year, over one million patients undergo cardiac sur-gery utilizing cardiopulmonary bypass (CPB) 1 globally,
with approximately 300,000 of those operations performed in the United States. 2 Morbid neurologic sequelae of
cardiac surgery, including delayed neurocognitive recovery and postoperative neurocognitive disorder, 3 are common, with reported incidences of up to 80% at hospital discharge and 20 to 40% after 6 months. 4 The more vulnerable older surgical patient increasingly comprises a larger subset of the
ALNV134N2_Text.indb 189ALNV134N2_Text.indb 189 29-Dec-20 19:43:4429-Dec-20 19:43:44
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

190 Anesthesiology 2021; 134:189–201
PERIOPERATIVE MEDICINE
Shaefi et al.
cardiac surgical population and is at a substantially higher risk for developing long-term cognitive decline, reduced level of overall cognitive function, lower quality of life, and increased mortality. 4 – 9
Oxygen, the most widely administered therapy in modern hospitals, has classically been administered lib-erally to avoid hypoxemia and maintain tissue oxygen-ation. 10 However, the excessive use of oxygen leading to hyperoxia has recently been shown to be potentially injurious, especially in the context of ischemia – reperfu-sion injury. 11 – 15 Cardiac surgery with CPB is associated with a profound exposure to ischemia – reperfusion, and patients in this high-risk setting are frequently treated with higher concentrations of oxygen to guard against myocardial and cerebral hypoxia. 16 , 17 Given the burden of disease from postoperative neurocognitive disorders and the possible link between hyperoxia and poorer outcomes in cardiac surgery, a prospective investigation of regulated intraoperative normoxia to ameliorate postoperative neu-rocognitive disorders after cardiac surgery is warranted. 18
Investigation into such a potentially simple cost-e ective intervention could impact hundreds of thousands of car-diac surgery patients a year.
Therefore, we conducted a clinical trial with the objec-tive of determining the e ect of intraoperative normoxia versus hyperoxia on postoperative neurocognition. Our hypothesis was that titration of intraoperative oxygenation to achieve normoxia, as compared to standard practice hyperoxia, reduces postoperative cognitive dysfunction on postoperative day 2 in older patients having cardiac sur-gery. Second, we tested the hypotheses that intraoperative normoxia reduces the incidence, severity, and duration of delirium; the length of stay and time to extubation; and neurocognitive function at longitudinal follow-up after 6 months when compared to intraoperative hyperoxia.
Materials and Methods
Study Design
This parallel-group randomized controlled trial enrolled patients at Beth Israel Deaconess Medical Center in Boston, Massachusetts, between July 2015 and July 2017. Institutional Review Board approval was obtained on February 2, 2015, from the Committee on Clinical Investigations, and all patients provided written informed consent. Full details of the study protocol have been previously published. 19 The trial was registered with ClinicalTrials.gov (NCT02591589, https://clinicaltrials.gov/ct2/show/NCT02591589 , principal investigator: Shahzad Shae , registration date: October 29, 2015). The study protocol is available at ClinicalTrials.gov. The trial was designed to assess the e ect of two intraoperative oxy-gen titration strategies, namely hyperoxia and normoxia, with postoperative neurocognitive function among older patients having cardiac surgery.
Study Participants
Patients 65 yr or older having elective or urgent coronary artery bypass graft (CABG) surgery requiring CPB were eligible for trial inclusion. Patients who were undergoing emergent CABG, procedures requiring single lung ventila-tion, or o -pump CABG, or patients with signs of cardio-genic shock, as dictated by preoperative inotropic, intraaortic balloon counterpulsation, or mechanical circulatory sup-port, were excluded. Non – English-speaking patients were excluded because the neurocognitive assessments could not be administered in languages other than English.
Randomization and Masking
The patients were randomized using a permuted block randomization schedule with block sizes of four, in which patients were randomly assigned in a 1:1 allocation to the normoxia or hyperoxia arm. Randomization assignments were allocated using sealed, sequentially numbered opaque envelopes. The randomization schema was generated by a unblinded statistician and concealed from study investi-gators. At the time of randomization, the anesthesiologist would open the next sequentially numbered envelope to obtain the randomization assignment. Study team members assessing neurocognitive function and postoperative clini-cal outcomes were blinded to patient arm, as were patients. Surgeons, anesthesiologists, and perfusionists involved in providing clinical care intraoperatively were not blinded due to the need for protocol adherence.
Study Procedures
Study ventilator settings were applied after induction of general anesthesia and successful endotracheal intubation and continued throughout surgery. In the normoxia group, the fraction of inspired oxygen (F io
2 ) was set at a minimum
of 0.35 to maintain an arterial partial pressure of oxygen above 70 mmHg, or oxygen saturations measured by pulse oximetry greater than or equal to 92%. If required, the F io
2
was titrated up to prevent hypoxemia (oxygen saturations less than 92%) during the pre- and postbypass periods. During CPB, a blended air/oxygen mixture was titrated to arterial blood gas analysis to maintain the Pa o
2 between
100 and 150 mmHg. In the hyperoxic arm, the F io2 was
set at 1.0 throughout the intraoperative period including CPB. Both groups received an anesthetic regimen at the discretion of the treating provider. Mechanical ventilation was based on the institutional standard of care, with a tidal volume of 6 to 8 ml/kg (employing ideal body weight) and positive end-expiratory pressure of 5 cmH
2 O.
Outcomes
The primary outcome was postoperative cognition, as assessed by the Telephonic Montreal Cognitive Assessment score on postoperative day 2. Cognitive function was measured
ALNV134N2_Text.indb 190ALNV134N2_Text.indb 190 29-Dec-20 19:43:4429-Dec-20 19:43:44
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:189–201 191
Intraoperative Oxygen and Cognition after Surgery
Shaefi et al.
preoperatively as baseline and subsequently postoperatively daily until discharge, unless the participant was in the intensive care unit (ICU) and nonverbal. The telephonic assessment is an adaptation of the Montreal Cognitive Assessment, a validated screening instrument that is highly sensitive for detecting mild cognitive impairment. 20 – 23 The Telephonic Montreal Cognitive Assessment is evaluated on a 22-point scale, with lower scores indicating worse cognitive status. The assessment comprises an aggregate score of individual assessments of attention and con-centration, executive functions, memory, language, concep-tual thinking, calculations, and orientation. The items do not require writing or visual cues to complete and therefore can be easily adapted to either in-person or telephone administration. In addition to the primary outcome, neurocognitive scores at 1, 3, and 6 months were evaluated via telephone interviews as secondary outcomes. Patients were contacted by telephone for 1-, 3-, and 6-month assessments. Research sta attempted to reach patients until their call window expired (before or after 7 days for the 1-month follow-up call and before or after 14 days for the 3- and 6-month follow-up call) or for up to 10 attempts. The rationale for using the abbreviated Telephonic Montreal Cognitive Assessment was to facilitate the use of a consistent scale continuously throughout the study from the inpatient, in-person assessments to over-the-phone assessments at 1, 3, and 6 months.
Additional secondary outcomes included the incidence and severity of postoperative delirium, time to extubation, days of mechanical ventilation, length of ICU and hospital stay, and mortality at 30 days and 6 months. Postoperative delirium was assessed each postoperative day until discharge with the Confusion Assessment Method or Confusion Assessment Method – ICU for nonverbal (intubated) patients. As with the Telephonic Montreal Cognitive Assessment, delirium assessments were administered by study sta mem-bers who were blinded to group assignment. Delirium severity was scored using the long Confusion Assessment Method Severity score, which assigns points from 0 to 19, with worsening delirium characterized by higher scores. 24
The worst Confusion Assessment Method Severity score for their hospital stay was analyzed. Time to extubation was reported as the number of hours from when patients were initially intubated for surgery to when they were last extu-bated. Hospital length of stay was de ned as the number of days spent in the hospital after surgery, and ICU length of stay was de ned as the number of days spent in the ICU before transfer to the general inpatient cardiac surgery ward.
Adverse Events
Because the patient population under study is by de ni-tion critically ill, we collected data on serious adverse events and unexpected nonserious adverse events that were pos-sibly related to the study. Patients were assessed daily while in the hospital for a maximum of 3 days postoperatively. Additional adverse outcome data were collected from the Society of Thoracic Surgeons (Chicago, Illinois) database,
including sternal wound infection, renal failure, myocardial infarction, reoperation, and stroke. This trial did not include any interim analyses to stop for safety, e cacy, or futility; thus, the trial was not stopped early, nor was there a ded-icated data safety monitoring board. Adverse event moni-toring was performed by members of the study team and reviewed by the principal investigator at regular intervals.
Sample Size Calculation
The minimal clinically important di erence on the Mini-Mental State Examination in postoperative change after cardiac surgery has been shown to be 2 points, with postop-erative day 2 reported as the in-hospital postoperative nadir time point. 25 Because there is no reported minimal clinically important di erence for the Telephonic Montreal Cognitive Assessment, we utilized 2 points as our minimal clinically important di erence based on previous validated crosswalk methods. 26 , 27 Using a two-sided alpha of 0.05 and 80% power, we determined that a sample size of 74 patients was needed to detect a mean di erence in Telephonic Montreal Cognitive Assessment scores of two points (SD of 3) between the hyper-oxia and normoxia groups. To allow for potential longer-term attrition from loss to follow-up or withdrawal, a total of 100 participants were enrolled and underwent surgery.
Statistical Analysis
Descriptive statistics of the data are presented as means ± SD, medians (interquartile range), or counts and proportions, depending on variable type and distribution. Normality of continuous data was assessed with the Shapiro – Wilk test. Di erences in continuous variables were assessed using independent sample t tests or Wilcoxon rank-sum tests as appropriate. Di erences in categorical data were assessed with a chi-square or Fisher ’ s exact test. Our primary out-come, the Telephonic Montreal Cognitive Assessment score on postoperative day 2, was assessed with a nonparametric Wilcoxon rank-sum test. The Hodges – Lehmann estimation of shift is reported as the location shift and associated 95% CI. Di erences in neurocognition at the follow-up time periods was also assessed between groups with the use of a Wilcoxon rank-sum test. In a post hoc analysis, the inci-dence of delirium was assessed among all participants, and the time to delirium and delirium severity was reported among only those who developed delirium. Full details of the statistical analysis plan were previously published in the protocol paper. 19 SAS 9.4 (SAS Institute Inc., USA) was uti-lized for analysis. For all analyses, two-sided P values of less than 0.05 were considered statistically signi cant.
Results
Study Population
A total of 492 patients were screened, of whom 343 met eligibility criteria. A total of 100 patients were randomized,
ALNV134N2_Text.indb 191ALNV134N2_Text.indb 191 29-Dec-20 19:43:4429-Dec-20 19:43:44
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
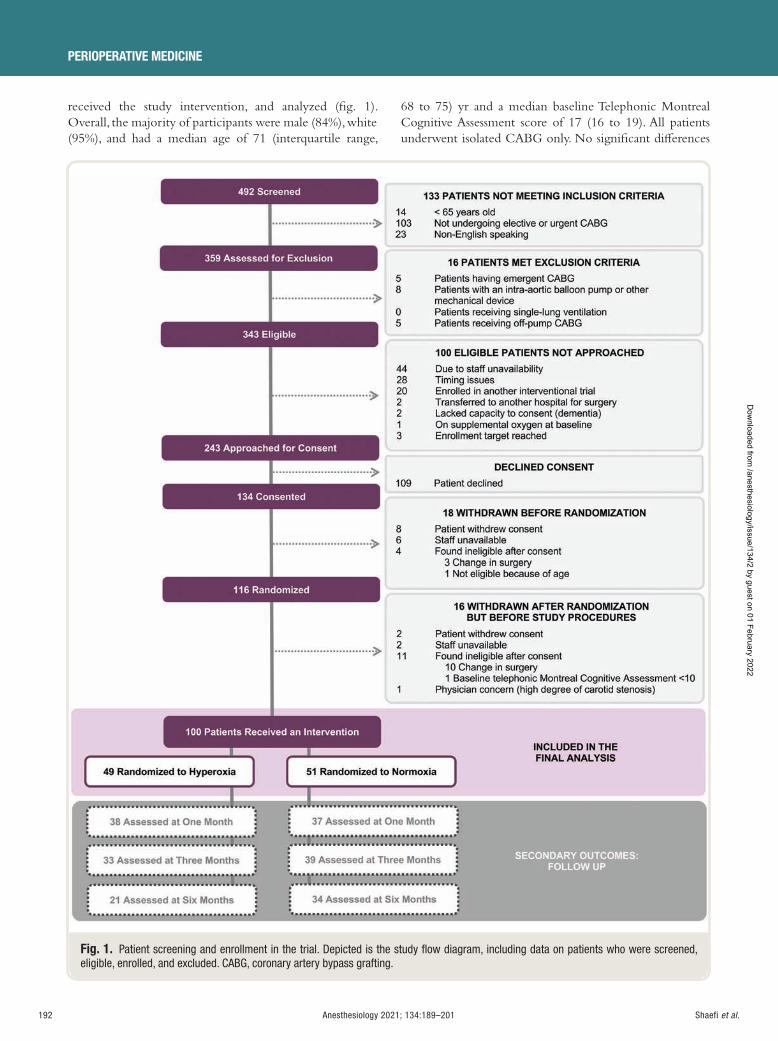
192 Anesthesiology 2021; 134:189–201
PERIOPERATIVE MEDICINE
Shaefi et al.
received the study intervention, and analyzed ( g. 1 ). Overall, the majority of participants were male (84%), white (95%), and had a median age of 71 (interquartile range,
68 to 75) yr and a median baseline Telephonic Montreal Cognitive Assessment score of 17 (16 to 19). All patients underwent isolated CABG only. No signi cant di erences
Fig. 1. Patient screening and enrollment in the trial. Depicted is the study fl ow diagram, including data on patients who were screened, eligible, enrolled, and excluded. CABG, coronary artery bypass grafting.
ALNV134N2_Text.indb 192ALNV134N2_Text.indb 192 29-Dec-20 19:43:4629-Dec-20 19:43:46
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
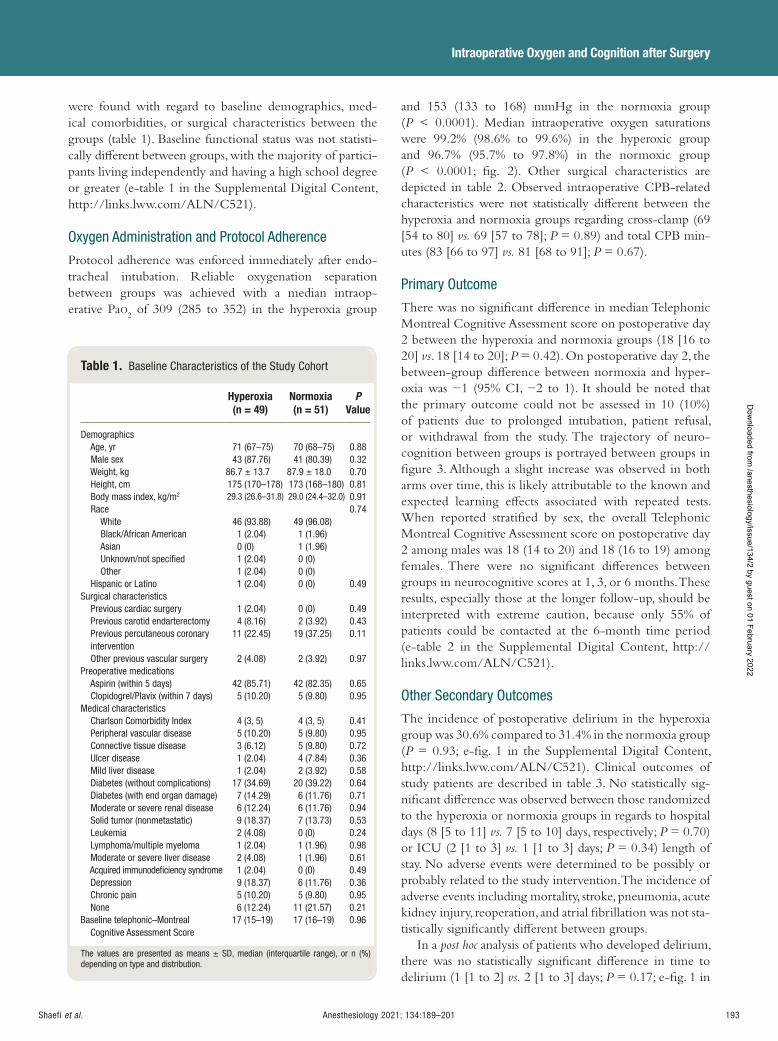
Anesthesiology 2021; 134:189–201 193
Intraoperative Oxygen and Cognition after Surgery
Shaefi et al.
were found with regard to baseline demographics, med-ical comorbidities, or surgical characteristics between the groups ( table 1 ). Baseline functional status was not statisti-cally di erent between groups, with the majority of partici-pants living independently and having a high school degree or greater (e-table 1 in the Supplemental Digital Content, http://links.lww.com/ALN/C521).
Oxygen Administration and Protocol Adherence
Protocol adherence was enforced immediately after endo-tracheal intubation. Reliable oxygenation separation between groups was achieved with a median intraop-erative Pa o
2 of 309 (285 to 352) in the hyperoxia group
and 153 (133 to 168) mmHg in the normoxia group ( P < 0.0001). Median intraoperative oxygen saturations were 99.2% (98.6% to 99.6%) in the hyperoxic group and 96.7% (95.7% to 97.8%) in the normoxic group ( P < 0.0001; g. 2 ). Other surgical characteristics are depicted in table 2 . Observed intraoperative CPB-related characteristics were not statistically di erent between the hyperoxia and normoxia groups regarding cross-clamp (69 [54 to 80] vs. 69 [57 to 78]; P = 0.89) and total CPB min-utes (83 [66 to 97] vs. 81 [68 to 91]; P = 0.67).
Primary Outcome
There was no signi cant di erence in median Telephonic Montreal Cognitive Assessment score on postoperative day 2 between the hyperoxia and normoxia groups (18 [16 to 20] vs . 18 [14 to 20]; P = 0.42). On postoperative day 2, the between-group di erence between normoxia and hyper-oxia was − 1 (95% CI, − 2 to 1). It should be noted that the primary outcome could not be assessed in 10 (10%) of patients due to prolonged intubation, patient refusal, or withdrawal from the study. The trajectory of neuro-cognition between groups is portrayed between groups in gure 3 . Although a slight increase was observed in both arms over time, this is likely attributable to the known and expected learning e ects associated with repeated tests. When reported strati ed by sex, the overall Telephonic Montreal Cognitive Assessment score on postoperative day 2 among males was 18 (14 to 20) and 18 (16 to 19) among females. There were no signi cant di erences between groups in neurocognitive scores at 1, 3, or 6 months. These results, especially those at the longer follow-up, should be interpreted with extreme caution, because only 55% of patients could be contacted at the 6-month time period (e-table 2 in the Supplemental Digital Content, http://links.lww.com/ALN/C521).
Other Secondary Outcomes
The incidence of postoperative delirium in the hyperoxia group was 30.6% compared to 31.4% in the normoxia group ( P = 0.93; e- g. 1 in the Supplemental Digital Content, http://links.lww.com/ALN/C521). Clinical outcomes of study patients are described in table 3 . No statistically sig-ni cant di erence was observed between those randomized to the hyperoxia or normoxia groups in regards to hospital days (8 [5 to 11] vs. 7 [5 to 10] days, respectively; P = 0.70) or ICU (2 [1 to 3] vs. 1 [1 to 3] days; P = 0.34) length of stay. No adverse events were determined to be possibly or probably related to the study intervention. The incidence of adverse events including mortality, stroke, pneumonia, acute kidney injury, reoperation, and atrial brillation was not sta-tistically signi cantly di erent between groups.
In a post hoc analysis of patients who developed delirium, there was no statistically signi cant di erence in time to delirium (1 [1 to 2] vs. 2 [1 to 3] days; P = 0.17; e- g. 1 in
Table 1. Baseline Characteristics of the Study Cohort
Hyperoxia (n = 49)
Normoxia (n = 51)
PValue
Demographics Age, yr 71 (67 – 75) 70 (68 – 75) 0.88 Male sex 43 (87.76) 41 (80.39) 0.32 Weight, kg 86.7 ± 13.7 87.9 ± 18.0 0.70 Height, cm 175 (170 – 178) 173 (168 – 180) 0.81 Body mass index, kg/m 2 29.3 (26.6 – 31.8) 29.0 (24.4 – 32.0) 0.91 Race 0.74 White 46 (93.88) 49 (96.08) Black/African American 1 (2.04) 1 (1.96) Asian 0 (0) 1 (1.96) Unknown/not specifi ed 1 (2.04) 0 (0) Other 1 (2.04) 0 (0) Hispanic or Latino 1 (2.04) 0 (0) 0.49 Surgical characteristics Previous cardiac surgery 1 (2.04) 0 (0) 0.49 Previous carotid endarterectomy 4 (8.16) 2 (3.92) 0.43 Previous percutaneous coronary
intervention 11 (22.45) 19 (37.25) 0.11
Other previous vascular surgery 2 (4.08) 2 (3.92) 0.97 Preoperative medications Aspirin (within 5 days) 42 (85.71) 42 (82.35) 0.65 Clopidogrel/Plavix (within 7 days) 5 (10.20) 5 (9.80) 0.95 Medical characteristics Charlson Comorbidity Index 4 (3, 5) 4 (3, 5) 0.41 Peripheral vascular disease 5 (10.20) 5 (9.80) 0.95 Connective tissue disease 3 (6.12) 5 (9.80) 0.72 Ulcer disease 1 (2.04) 4 (7.84) 0.36 Mild liver disease 1 (2.04) 2 (3.92) 0.58 Diabetes (without complications) 17 (34.69) 20 (39.22) 0.64 Diabetes (with end organ damage) 7 (14.29) 6 (11.76) 0.71 Moderate or severe renal disease 6 (12.24) 6 (11.76) 0.94 Solid tumor (nonmetastatic) 9 (18.37) 7 (13.73) 0.53 Leukemia 2 (4.08) 0 (0) 0.24 Lymphoma/multiple myeloma 1 (2.04) 1 (1.96) 0.98 Moderate or severe liver disease 2 (4.08) 1 (1.96) 0.61 Acquired immunodefi ciency syndrome 1 (2.04) 0 (0) 0.49 Depression 9 (18.37) 6 (11.76) 0.36 Chronic pain 5 (10.20) 5 (9.80) 0.95 None 6 (12.24) 11 (21.57) 0.21 Baseline telephonic – Montreal
Cognitive Assessment Score 17 (15–19) 17 (16–19) 0.96
The values are presented as means ± SD, median (interquartile range), or n (%) depending on type and distribution.
ALNV134N2_Text.indb 193ALNV134N2_Text.indb 193 29-Dec-20 19:43:4629-Dec-20 19:43:46
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
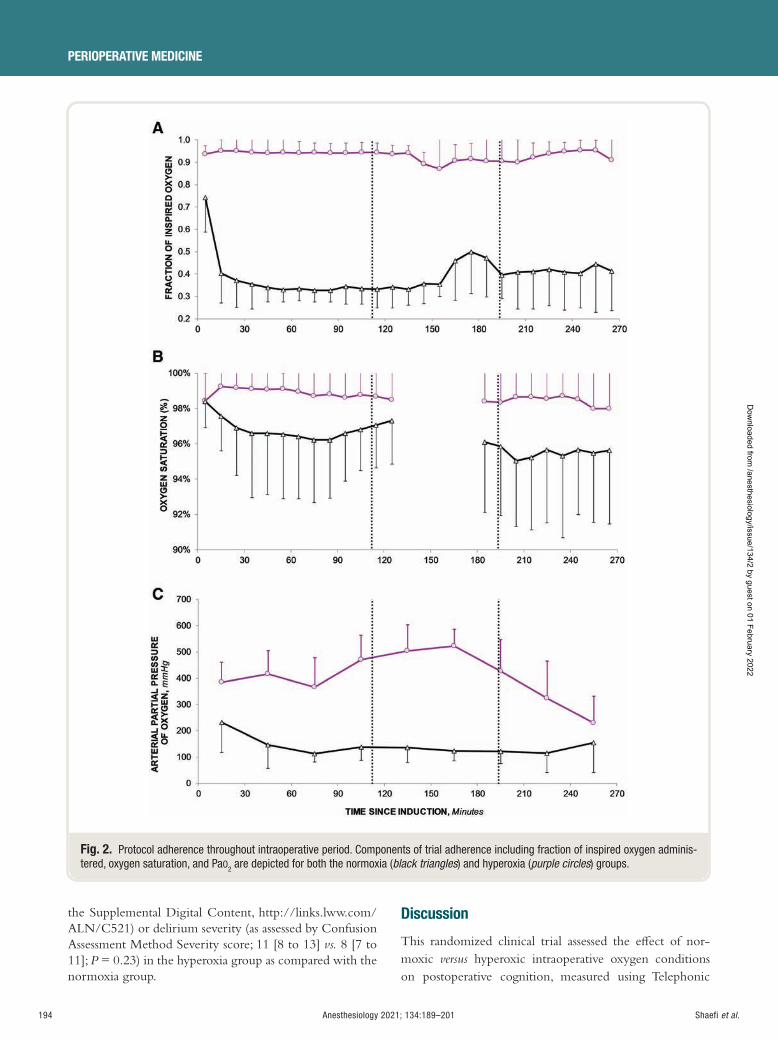
194 Anesthesiology 2021; 134:189–201
PERIOPERATIVE MEDICINE
Shaefi et al.
the Supplemental Digital Content, http://links.lww.com/ALN/C521) or delirium severity (as assessed by Confusion Assessment Method Severity score; 11 [8 to 13] vs. 8 [7 to 11]; P = 0.23) in the hyperoxia group as compared with the normoxia group.
Discussion
This randomized clinical trial assessed the e ect of nor-moxic versus hyperoxic intraoperative oxygen conditions on postoperative cognition, measured using Telephonic
Fig. 2. Protocol adherence throughout intraoperative period. Components of trial adherence including fraction of inspired oxygen adminis-tered, oxygen saturation, and Pa O2 are depicted for both the normoxia ( black triangles ) and hyperoxia ( purple circles ) groups.
ALNV134N2_Text.indb 194ALNV134N2_Text.indb 194 29-Dec-20 19:43:4729-Dec-20 19:43:47
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
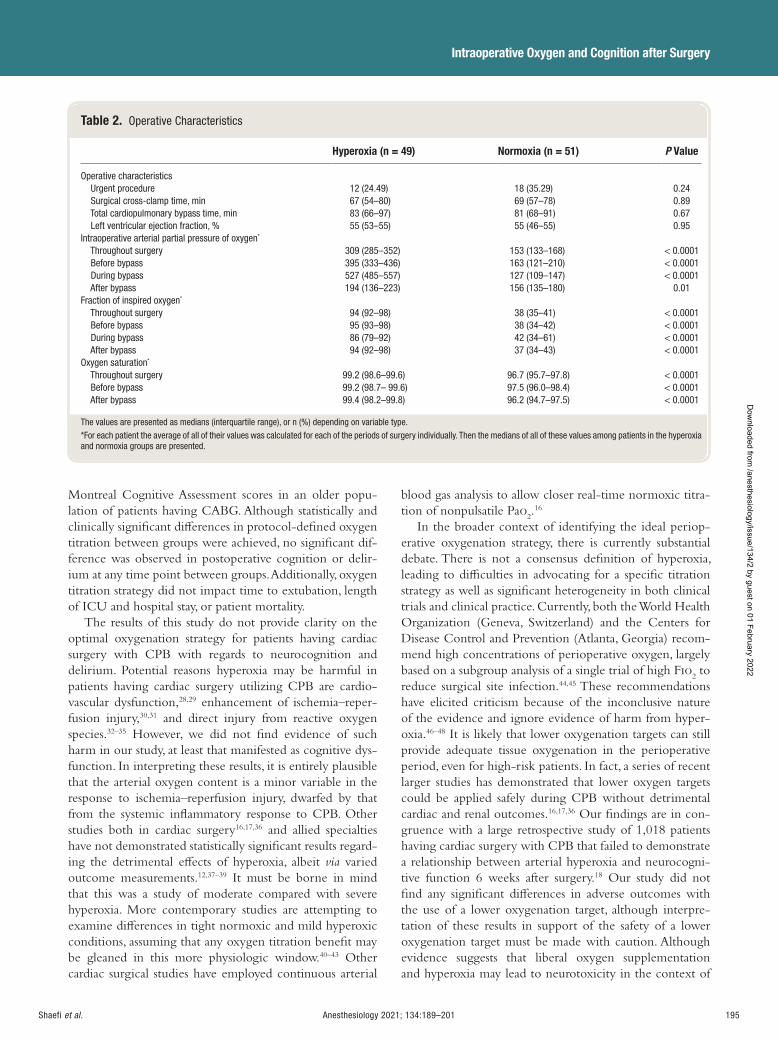
Anesthesiology 2021; 134:189–201 195
Intraoperative Oxygen and Cognition after Surgery
Shaefi et al.
Montreal Cognitive Assessment scores in an older popu-lation of patients having CABG. Although statistically and clinically signi cant di erences in protocol-de ned oxygen titration between groups were achieved, no signi cant dif-ference was observed in postoperative cognition or delir-ium at any time point between groups. Additionally, oxygen titration strategy did not impact time to extubation, length of ICU and hospital stay, or patient mortality.
The results of this study do not provide clarity on the optimal oxygenation strategy for patients having cardiac surgery with CPB with regards to neurocognition and delirium. Potential reasons hyperoxia may be harmful in patients having cardiac surgery utilizing CPB are cardio-vascular dysfunction, 28 , 29 enhancement of ischemia – reper-fusion injury, 30 , 31 and direct injury from reactive oxygen species. 32 – 35 However, we did not nd evidence of such harm in our study, at least that manifested as cognitive dys-function. In interpreting these results, it is entirely plausible that the arterial oxygen content is a minor variable in the response to ischemia – reperfusion injury, dwarfed by that from the systemic in ammatory response to CPB. Other studies both in cardiac surgery 16 , 17 , 36 and allied specialties have not demonstrated statistically signi cant results regard-ing the detrimental e ects of hyperoxia, albeit via varied outcome measurements. 12 , 37 – 39 It must be borne in mind that this was a study of moderate compared with severe hyperoxia. More contemporary studies are attempting to examine di erences in tight normoxic and mild hyperoxic conditions, assuming that any oxygen titration bene t may be gleaned in this more physiologic window. 40 – 43 Other cardiac surgical studies have employed continuous arterial
blood gas analysis to allow closer real-time normoxic titra-tion of nonpulsatile Pa o
2 . 16
In the broader context of identifying the ideal periop-erative oxygenation strategy, there is currently substantial debate. There is not a consensus de nition of hyperoxia, leading to di culties in advocating for a speci c titration strategy as well as signi cant heterogeneity in both clinical trials and clinical practice. Currently, both the World Health Organization (Geneva, Switzerland) and the Centers for Disease Control and Prevention (Atlanta, Georgia) recom-mend high concentrations of perioperative oxygen, largely based on a subgroup analysis of a single trial of high F io
2 to
reduce surgical site infection. 44 , 45 These recommendations have elicited criticism because of the inconclusive nature of the evidence and ignore evidence of harm from hyper-oxia. 46 – 48 It is likely that lower oxygenation targets can still provide adequate tissue oxygenation in the perioperative period, even for high-risk patients. In fact, a series of recent larger studies has demonstrated that lower oxygen targets could be applied safely during CPB without detrimental cardiac and renal outcomes. 16 , 17 , 36 Our ndings are in con-gruence with a large retrospective study of 1,018 patients having cardiac surgery with CPB that failed to demonstrate a relationship between arterial hyperoxia and neurocogni-tive function 6 weeks after surgery. 18 Our study did not nd any signi cant di erences in adverse outcomes with the use of a lower oxygenation target, although interpre-tation of these results in support of the safety of a lower oxygenation target must be made with caution. Although evidence suggests that liberal oxygen supplementation and hyperoxia may lead to neurotoxicity in the context of
Table 2. Operative Characteristics
Hyperoxia (n = 49) Normoxia (n = 51) P Value
Operative characteristics Urgent procedure 12 (24.49) 18 (35.29) 0.24 Surgical cross-clamp time, min 67 (54 – 80) 69 (57 – 78) 0.89 Total cardiopulmonary bypass time, min 83 (66 – 97) 81 (68 – 91) 0.67 Left ventricular ejection fraction, % 55 (53 – 55) 55 (46 – 55) 0.95 Intraoperative arterial partial pressure of oxygen *
Throughout surgery 309 (285–352) 153 (133–168) < 0.0001 Before bypass 395 (333–436) 163 (121–210) < 0.0001 During bypass 527 (485–557) 127 (109–147) < 0.0001 After bypass 194 (136–223) 156 (135–180) 0.01 Fraction of inspired oxygen *
Throughout surgery 94 (92–98) 38 (35–41) < 0.0001 Before bypass 95 (93–98) 38 (34–42) < 0.0001 During bypass 86 (79–92) 42 (34–61) < 0.0001 After bypass 94 (92–98) 37 (34–43) < 0.0001 Oxygen saturation * Throughout surgery 99.2 (98.6–99.6) 96.7 (95.7–97.8) < 0.0001 Before bypass 99.2 (98.7– 99.6) 97.5 (96.0–98.4) < 0.0001 After bypass 99.4 (98.2 – 99.8) 96.2 (94.7 – 97.5) < 0.0001
The values are presented as medians (interquartile range), or n (%) depending on variable type. * For each patient the average of all of their values was calculated for each of the periods of surgery individually. Then the medians of all of these values among patients in the hyperoxia and normoxia groups are presented.
ALNV134N2_Text.indb 195ALNV134N2_Text.indb 195 29-Dec-20 19:43:4829-Dec-20 19:43:48
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
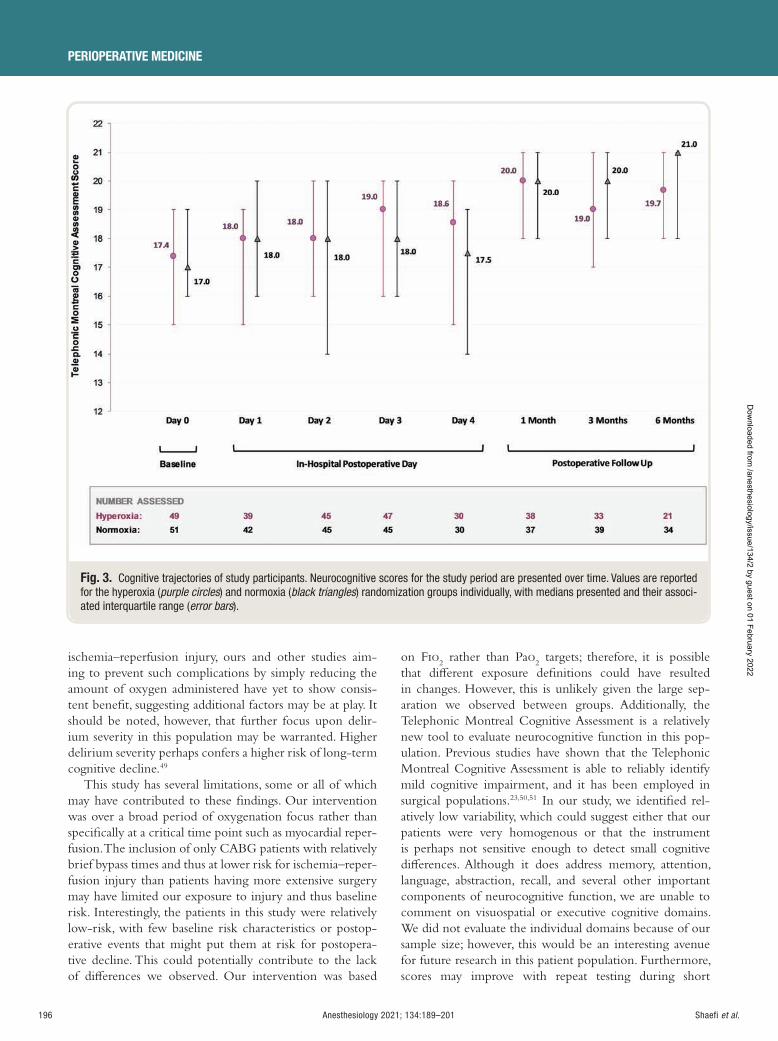
196 Anesthesiology 2021; 134:189–201
PERIOPERATIVE MEDICINE
Shaefi et al.
ischemia – reperfusion injury, ours and other studies aim-ing to prevent such complications by simply reducing the amount of oxygen administered have yet to show consis-tent bene t, suggesting additional factors may be at play. It should be noted, however, that further focus upon delir-ium severity in this population may be warranted. Higher delirium severity perhaps confers a higher risk of long-term cognitive decline. 49
This study has several limitations, some or all of which may have contributed to these ndings. Our intervention was over a broad period of oxygenation focus rather than speci cally at a critical time point such as myocardial reper-fusion. The inclusion of only CABG patients with relatively brief bypass times and thus at lower risk for ischemia – reper-fusion injury than patients having more extensive surgery may have limited our exposure to injury and thus baseline risk. Interestingly, the patients in this study were relatively low-risk, with few baseline risk characteristics or postop-erative events that might put them at risk for postopera-tive decline. This could potentially contribute to the lack of di erences we observed. Our intervention was based
on F io2 rather than Pa o
2 targets; therefore, it is possible
that di erent exposure de nitions could have resulted in changes. However, this is unlikely given the large sep-aration we observed between groups. Additionally, the Telephonic Montreal Cognitive Assessment is a relatively new tool to evaluate neurocognitive function in this pop-ulation. Previous studies have shown that the Telephonic Montreal Cognitive Assessment is able to reliably identify mild cognitive impairment, and it has been employed in surgical populations. 23 , 50 , 51 In our study, we identi ed rel-atively low variability, which could suggest either that our patients were very homogenous or that the instrument is perhaps not sensitive enough to detect small cognitive di erences. Although it does address memory, attention, language, abstraction, recall, and several other important components of neurocognitive function, we are unable to comment on visuospatial or executive cognitive domains. We did not evaluate the individual domains because of our sample size; however, this would be an interesting avenue for future research in this patient population. Furthermore, scores may improve with repeat testing during short
Fig. 3. Cognitive trajectories of study participants. Neurocognitive scores for the study period are presented over time. Values are reported for the hyperoxia ( purple circles ) and normoxia ( black triangles ) randomization groups individually, with medians presented and their associ-ated interquartile range ( error bars ).
ALNV134N2_Text.indb 196ALNV134N2_Text.indb 196 29-Dec-20 19:43:4929-Dec-20 19:43:49
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
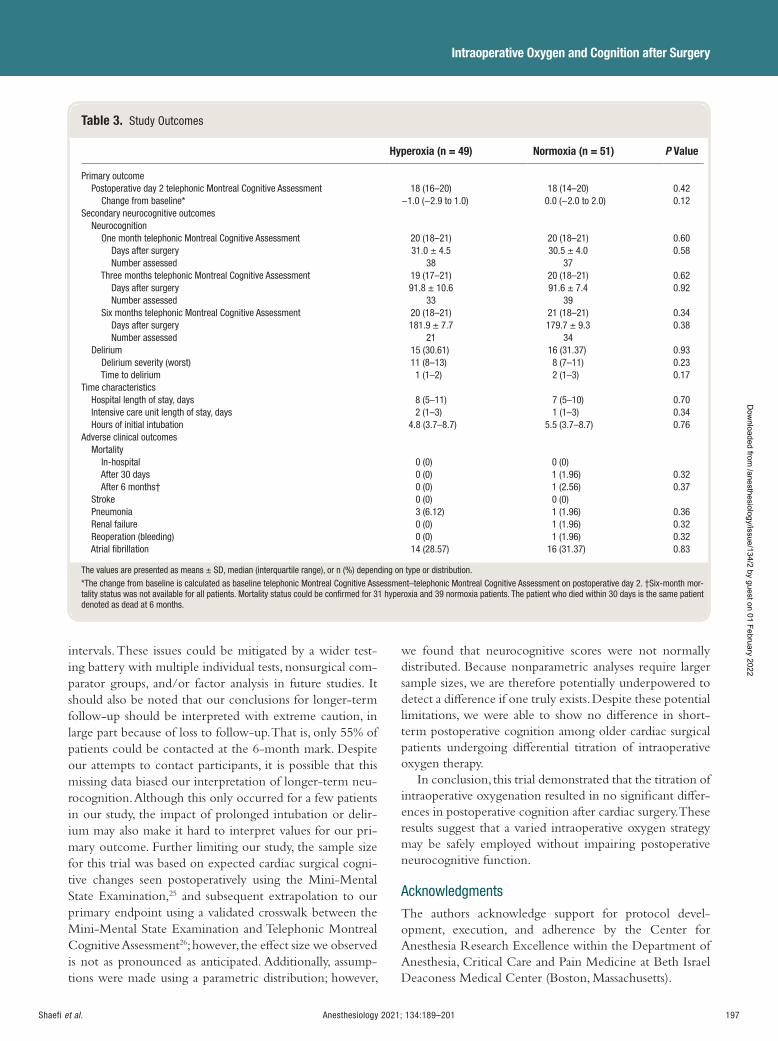
Anesthesiology 2021; 134:189–201 197
Intraoperative Oxygen and Cognition after Surgery
Shaefi et al.
intervals. These issues could be mitigated by a wider test-ing battery with multiple individual tests, nonsurgical com-parator groups, and/or factor analysis in future studies. It should also be noted that our conclusions for longer-term follow-up should be interpreted with extreme caution, in large part because of loss to follow-up. That is, only 55% of patients could be contacted at the 6-month mark. Despite our attempts to contact participants, it is possible that this missing data biased our interpretation of longer-term neu-rocognition. Although this only occurred for a few patients in our study, the impact of prolonged intubation or delir-ium may also make it hard to interpret values for our pri-mary outcome. Further limiting our study, the sample size for this trial was based on expected cardiac surgical cogni-tive changes seen postoperatively using the Mini-Mental State Examination, 25 and subsequent extrapolation to our primary endpoint using a validated crosswalk between the Mini-Mental State Examination and Telephonic Montreal Cognitive Assessment 26 ; however, the e ect size we observed is not as pronounced as anticipated. Additionally, assump-tions were made using a parametric distribution; however,
we found that neurocognitive scores were not normally distributed. Because nonparametric analyses require larger sample sizes, we are therefore potentially underpowered to detect a di erence if one truly exists. Despite these potential limitations, we were able to show no di erence in short-term postoperative cognition among older cardiac surgical patients undergoing di erential titration of intraoperative oxygen therapy.
In conclusion, this trial demonstrated that the titration of intraoperative oxygenation resulted in no signi cant di er-ences in postoperative cognition after cardiac surgery. These results suggest that a varied intraoperative oxygen strategy may be safely employed without impairing postoperative neurocognitive function.
Acknowledgments
The authors acknowledge support for protocol devel-opment, execution, and adherence by the Center for Anesthesia Research Excellence within the Department of Anesthesia, Critical Care and Pain Medicine at Beth Israel Deaconess Medical Center (Boston, Massachusetts).
Table 3. Study Outcomes
Hyperoxia (n = 49) Normoxia (n = 51) P Value
Primary outcome Postoperative day 2 telephonic Montreal Cognitive Assessment 18 (16 – 20) 18 (14 – 20) 0.42 Change from baseline * − 1.0 ( − 2.9 to 1.0) 0.0 ( − 2.0 to 2.0) 0.12 Secondary neurocognitive outcomes Neurocognition One month telephonic Montreal Cognitive Assessment 20 (18 – 21) 20 (18 – 21) 0.60 Days after surgery 31.0 ± 4.5 30.5 ± 4.0 0.58 Number assessed 38 37 Three months telephonic Montreal Cognitive Assessment 19 (17 – 21) 20 (18 – 21) 0.62 Days after surgery 91.8 ± 10.6 91.6 ± 7.4 0.92 Number assessed 33 39 Six months telephonic Montreal Cognitive Assessment 20 (18 – 21) 21 (18 – 21) 0.34 Days after surgery 181.9 ± 7.7 179.7 ± 9.3 0.38 Number assessed 21 34 Delirium 15 (30.61) 16 (31.37) 0.93 Delirium severity (worst) 11 (8 – 13) 8 (7 – 11) 0.23 Time to delirium 1 (1 – 2) 2 (1 – 3) 0.17 Time characteristics Hospital length of stay, days 8 (5 – 11) 7 (5 – 10) 0.70 Intensive care unit length of stay, days 2 (1 – 3) 1 (1 – 3) 0.34 Hours of initial intubation 4.8 (3.7 – 8.7) 5.5 (3.7 – 8.7) 0.76 Adverse clinical outcomes Mortality In-hospital 0 (0) 0 (0) After 30 days 0 (0) 1 (1.96) 0.32 After 6 months † 0 (0) 1 (2.56) 0.37 Stroke 0 (0) 0 (0) Pneumonia 3 (6.12) 1 (1.96) 0.36 Renal failure 0 (0) 1 (1.96) 0.32 Reoperation (bleeding) 0 (0) 1 (1.96) 0.32 Atrial fi brillation 14 (28.57) 16 (31.37) 0.83
The values are presented as means ± SD, median (interquartile range), or n (%) depending on type or distribution. * The change from baseline is calculated as baseline telephonic Montreal Cognitive Assessment – telephonic Montreal Cognitive Assessment on postoperative day 2. † Six-month mor-tality status was not available for all patients. Mortality status could be confi rmed for 31 hyperoxia and 39 normoxia patients. The patient who died within 30 days is the same patient denoted as dead at 6 months.
ALNV134N2_Text.indb 197ALNV134N2_Text.indb 197 29-Dec-20 19:43:4929-Dec-20 19:43:49
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

198 Anesthesiology 2021; 134:189–201
PERIOPERATIVE MEDICINE
Shaefi et al.
Research Support
Supported by the Foundation for Anesthesia Education and Research (American Society of Anesthesiologists, Schaumburg, Illinois) in the form of a Mentored Training Research Grant to support principal investigator time and e ort and by additional funds through the Beth Israel Deaconess Medical Center (Boston, Massachusetts) Chief Academic O cer Pilot Award for supporting study sta sal-ary, statistical support, and regulatory compliance consulting.
Competing Interests
Dr. Shae received a speaking honorarium for a University of North Carolina (Chapel Hill, North Carolina) Visiting Professorship lecture. Ms. Mueller receives statistical con-sulting fees from the University of Chicago (Chicago, Illinois). Dr. O ’ Gara receives consulting fees from Sedana Medical (Sweden). Dr. Bagchi receives consulting fees from Lungpacer Medical Inc. (Canada). Ms. Banner-Goodspeed received salary support from several National Institutes of Health (Bethesda, Maryland) and Department of Defense (Arlington, Virginia) grants, unrelated to this project. Dr. Subramaniam receives grant support from Mallinckrodt Pharmaceuticals (United Kingdom) and Edward Lifesciences (Irvine, California). The remaining authors declare no competing interests.
Reproducible Science
Full protocol available at: sshae @bidmc.harvard.edu . Raw data available at: sshae @bidmc.harvard.edu .
Correspondence
Address correspondence to Dr. Shae : Beth Israel Deaconess Medical Center, 330 Brookline Avenue, W/RB-4, Boston, Massachusetts 02215. sshae @bidmc.harvard.edu . This arti-cle may be accessed for personal use at no charge through the Journal Web site, www.anesthesiology.org.
References
1. Punjabi PP , Taylor KM : The science and practice of cardiopulmonary bypass: From cross circulation to ECMO and SIRS. Glob Cardiol Sci Pract 2013 ; 2013 : 249 – 60
2. Bowdish ME , D’Agostino RS , Thourani VH , Desai N , Shahian DM , Fernandez FG , Badhwar V : The Society of Thoracic Surgeons Adult Cardiac Surgery Database : 2020 update on outcomes and research. Ann Thorac Surg 2020 ; 109 : 1646 – 55
3. Evered L , Silbert B , Knopman DS , Scott DA , DeKosky ST , Rasmussen LS , Oh ES , Crosby G , Berger M , Eckenho RG ; Nomenclature Consensus Working Group : Recommendations for the nomenclature of
cognitive change associated with anaesthesia and sur-gery — 2018. Anesthesiology 2018 ; 129 : 872 – 9
4. Newman MF , Kirchner JL , Phillips-Bute B , Gaver V , Grocott H , Jones RH , Mark DB , Reves JG , Blumenthal JA ; Neurological Outcome Research Group and the Cardiothoracic Anesthesiology Research Endeavors Investigators : Longitudinal assessment of neurocogni-tive function after coronary-artery bypass surgery. N Engl J Med 2001 ; 344 : 395 – 402
5. Phillips-Bute B , Mathew JP , Blumenthal JA , Grocott HP , Laskowitz DT , Jones RH , Mark DB , Newman MF : Association of neurocognitive function and quality of life 1 year after coronary artery bypass graft (CABG) surgery. Psychosom Med 2006 ; 68 : 369 – 75
6. Newman MF , Grocott HP , Mathew JP , White WD , Landolfo K , Reves JG , Laskowitz DT , Mark DB , Blumenthal JA ; Neurologic Outcome Research Group and the Cardiothoracic Anesthesia Research Endeavors (CARE) Investigators of the Duke Heart Center : Report of the substudy assessing the impact of neurocognitive function on quality of life 5 years after cardiac surgery. Stroke 2001 ; 32 : 2874 – 81
7. Berger M , Terrando N , Smith SK , Browndyke JN , Newman MF , Mathew JP : Neurocognitive function after cardiac surgery: From phenotypes to mechanisms. A nesthesiology 2018 ; 129 : 829 – 51
8. Tully PJ , Baune BT , Baker RA : Cognitive impairment before and six months after cardiac surgery increase mortality risk at median 11 year follow-up: A cohort study. Int J Cardiol 2013 ; 168 : 2796 – 802
9. Fontes MT , Swift RC , Phillips-Bute B , Podgoreanu MV , Sta ord-Smith M , Newman MF , Mathew JP ; Neurologic Outcome Research Group of the Duke Heart Center : Predictors of cognitive recovery after cardiac surgery. Anesth Analg 2013 ; 116 : 435 – 42
10. O ’ Driscoll BR , Howard LS , Bucknall C , Welham SA , Davison AG ; British Thoracic Society : British Thoracic Society emergency oxygen audits. Thorax 2011 ; 66 : 734 – 5
11. Baigrie RJ , Lamont PM , Kwiatkowski D , Dallman MJ , Morris PJ : Systemic cytokine response after major sur-gery. Br J Surg 1992 ; 79 : 757 – 60
12. Girardis M , Busani S , Damiani E , Donati A , Rinaldi L , Marudi A , Morelli A , Antonelli M , Singer M : E ect of conservative vs. conventional oxygen therapy on mortality among patients in an intensive care unit: The oxygen – ICU randomized clinical trial. JAMA 2016 ; 316 : 1583 – 9
13. Stub D , Smith K , Bernard S , Nehme Z , Stephenson M , Bray JE , Cameron P , Barger B , Ellims AH , Taylor AJ , Meredith IT , Kaye DM ; AVOID Investigators : Air ver-sus oxygen in ST-segment-elevation myocardial infarc-tion. Circulation 2015 ; 131 : 2143 – 50
14. Kilgannon JH , Jones AE , Shapiro NI , Angelos MG , Milcarek B , Hunter K , Parrillo JE , Trzeciak S ; Emergency
ALNV134N2_Text.indb 198ALNV134N2_Text.indb 198 29-Dec-20 19:43:4929-Dec-20 19:43:49
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:189–201 199
Intraoperative Oxygen and Cognition after Surgery
Shaefi et al.
Medicine Shock Research Network (EMShockNet) Investigators : Association between arterial hyperoxia following resuscitation from cardiac arrest and in-hos-pital mortality. JAMA 2010 ; 303 : 2165 – 71
15. Rincon F , Kang J , Maltenfort M , Vibbert M , Urtecho J , Athar MK , Jallo J , Pineda CC , Tzeng D , McBride W , Bell R : Association between hyperoxia and mortality after stroke: A multicenter cohort study. Crit Care Med 2014 ; 42 : 387 – 96
16. McGuinness SP , Parke RL , Drummond K , Willcox T , Bailey M , Kruger C , Baker M , Cowdrey KA , Gilder E , McCarthy L , Painter T ; SO-COOL investigators : A multicenter, randomized, controlled phase IIb trial of avoidance of hyperoxemia during cardiopulmonary bypass. A nesthesiology 2016 ; 125 : 465 – 73
17. Smit B , Smulders YM , de Waard MC , Boer C , Vonk AB , Veerhoek D , Kamminga S , de Grooth HJ , Garc í a-Vallejo JJ , Musters RJ , Girbes AR , Oudemans-van Straaten HM , Spoelstra-de Man AM : Moderate hyper-oxic versus near-physiological oxygen targets during and after coronary artery bypass surgery: A randomised controlled trial. Crit Care 2016 ; 20 : 55
18. Fontes MT , McDonagh DL , Phillips-Bute B , Welsby IJ , Podgoreanu MV , Fontes ML , Sta ord-Smith M , Newman MF , Mathew JP ; Neurologic Outcome Research Group (NORG) of the Duke Heart Center : Arterial hyperoxia during cardiopulmonary bypass and postoperative cognitive dysfunction. J Cardiothorac Vasc Anesth 2014 ; 28 : 462 – 6
19. Shae S , Marcantonio ER , Mueller A , Banner-Goodspeed V , Robson SC , Spear K , Otterbein LE , O ’ Gara BP , Talmor DS , Subramaniam B : Intraoperative oxygen concentration and neurocognition after cardiac surgery: Study protocol for a randomized controlled trial. Trials 2017 ; 18 : 600
20. Horton DK , Hynan LS , Lacritz LH , Rossetti HC , Weiner MF , Cullum CM : An abbreviated Montreal Cognitive Assessment (MoCA) for dementia screening. Clin Neuropsychol 2015 ; 29 : 413 – 25
21. Wong A , Nyenhuis D , Black SE , Law LS , Lo ES , Kwan PW , Au L , Chan AY , Wong LK , Nasreddine Z , Mok V : Montreal Cognitive Assessment 5-minute protocol is a brief, valid, reliable, and feasible cog-nitive screen for telephone administration. Stroke 2015 ; 46 : 1059 – 64
22. Nasreddine ZS , Phillips NA , Bedirian V , Charbonneau S , Whitehead V , Collin I , Cummings JL , Chertkow H , Zietemann V , Kopczak A , Muller C , Wollenweber FA , Dichgans M : The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment: Validation of the Telephone Interview of Cognitive Status and Telephone Montreal Cognitive Assessment against detailed cognitive testing and clini-cal diagnosis of mild cognitive impairment after stroke. J Am Geriatr Soc 2005 ; 53 : 695 – 9
23. Austin CA , O ’ Gorman T , Stern E , Emmett D , St ü rmer T , Carson S , Busby-Whitehead J : Association between postoperative delirium and long-term cognitive func-tion after major nonemergent surgery. JAMA Surg 2019 ; 154 : 328 – 34
24. Inouye SK , Kosar CM , Tommet D , Schmitt EM , Puelle MR , Saczynski JS , Marcantonio ER , Jones RN : The CAM-S: Development and validation of a new scoring system for delirium severity in 2 cohorts. Ann Intern Med 2014 ; 160 : 526 – 33
25. Saczynski JS , Marcantonio ER , Quach L , Fong TG , Gross A , Inouye SK , Jones RN : Cognitive trajecto-ries after postoperative delirium. N Engl J Med 2012 ; 367 : 30 – 9
26. Saczynski JS , Inouye SK , Guess J , Jones RN , Fong TG , Nemeth E , Hodara A , Ngo L , Marcantonio ER : The Montreal Cognitive Assessment: Creating a crosswalk with the Mini-Mental State Examination. J Am Geriatr Soc 2015 ; 63 : 2370 – 4
27. Roalf DR , Moore TM , Mechanic-Hamilton D , Wolk DA , Arnold SE , Weintraub DA , Moberg PJ : Bridging cognitive screening tests in neurologic disorders: A crosswalk between the short Montreal Cognitive Assessment and Mini-Mental State Examination. Alzheimers Dement 2017 ; 13 : 947 – 52
28. Spoelstra-de Man AM , Smit B , Oudemans-van Straaten HM , Smulders YM : Cardiovascular e ects of hyperoxia during and after cardiac surgery . Anaesthesia 2015 ; 70 : 1307 – 19
29. Farquhar H , Weatherall M , Wijesinghe M , Perrin K , Ranchord A , Simmonds M , Beasley R : Systematic review of studies of the e ect of hyperoxia on coronary blood ow. Am Heart J 2009 ; 158 : 371 – 7
30. Peng YW , Mohammed A , Deatrick KB , Major T , Cheng D , Charpie I , Charpie JR : Di erential e ects of nor-moxic and hyperoxic reperfusion on global myocardial ischemia – reperfusion injury. Semin Thorac Cardiovasc Surg 2019 ; 31 : 188 – 98
31. Brueckl C , Kaestle S , Kerem A , Habazettl H , Krombach F , Kuppe H , Kuebler WM : Hyperoxia-induced reac-tive oxygen species formation in pulmonary capillary endothelial cells in situ . Am J Respir Cell Mol Biol 2006 ; 34 : 453 – 63
32. Topcu AC , Bolukcu A , Ozeren K , Kavasoglu T , Kayacioglu I : Normoxic management of cardiopul-monary bypass reduces myocardial oxidative stress in adult patients undergoing coronary artery bypass graft surgery . Perfusion 2020 : 267659120946733
33. Peng YW , Major T , Mohammed A , Deatrick KB , Charpie JR : Normoxic re-oxygenation ameliorates end-organ injury after cardiopulmonary bypass. J Cardiothorac Surg 2020 ; 15 : 134
34. Lopez MG , Hughes CG , DeMatteo A , O ’ Neal JB , McNeil JB , Shotwell MS , Morse J , Petracek MR , Shah AS , Brown NJ , Billings FT 4th : Intraoperative
ALNV134N2_Text.indb 199ALNV134N2_Text.indb 199 29-Dec-20 19:43:4929-Dec-20 19:43:49
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
200 Anesthesiology 2021; 134:189–201
PERIOPERATIVE MEDICINE
Shaefi et al.
oxidative damage and delirium after cardiac surgery. A nesthesiology 2020 ; 132 : 551 – 61
35. Lopez MG , Pandharipande P , Morse J , Shotwell MS , Milne GL , Pretorius M , Shaw AD , Roberts LJ 2nd , Billings FT 4th : Intraoperative cerebral oxygenation, oxidative injury, and delirium following cardiac sur-gery. Free Radic Biol Med 2017 ; 103 : 192 – 8
36. Abou-Arab O , Huette P , Martineau L , Beauvalot C , Beyls C , Josse E , Touati G , Bouchot O , Bouhemad B , Diouf M , Lorne E , Guinot PG : Hyperoxia during cardiopulmonary bypass does not decrease cardiovas-cular complications following cardiac surgery: The CARDIOX randomized clinical trial. Intensive Care Med 2019 ; 45 : 1413 – 21
37. Hofmann R , James SK , Jernberg T , Lindahl B , Erlinge D , Witt N , Arefalk G , Frick M , Alfredsson J , Nilsson L , Ravn-Fischer A , Omerovic E , Kellerth T , Sparv D , Ekelund U , Linder R , Ekstr ö m M , Lauermann J , Haaga U , Pernow J , Ö stlund O , Herlitz J , Svensson L ; DETO2X – SWEDEHEART Investigators : Oxygen therapy in suspected acute myocardial infarction. N Engl J Med 2017 ; 377 : 1240 – 9
38. Mackle D , Bellomo R , Bailey M , Beasley R , Deane A , Eastwood G , Finfer S , Freebairn R , King V , Linke N , Litton E , McArthur C , McGuinness S , Panwar R , Young P ; ICU-ROX Investigators and the Australian and New Zealand Intensive Care Society Clinical Trials Group: Conservative oxygen therapy during mechanical ventilation in the ICU. N Engl J Med 2020 ; 382 : 989 – 98
39. Ro e C , Nevatte T , Sim J , Bishop J , Ives N , Ferdinand P , Gray R ; Stroke Oxygen Study Investigators and the Stroke OxygenStudy Collaborative Group : E ect of routine low-dose oxygen supplementation on death and disability in adults with acute stroke: The stroke oxygen study randomized clinical trial. JAMA 2017 ; 318 : 1125 – 35
40. Young P , Mackle D , Bellomo R , Bailey M , Beasley R , Deane A , Eastwood G , Finfer S , Freebairn R , King V , Linke N , Litton E , McArthur C , McGuinness S , Panwar R ; ICU-ROX Investigators the Australian New Zealand Intensive Care Society Clinical Trials Group : Conservative oxygen therapy for mechanically ventilated adults with sepsis: A post hoc analysis of data from the intensive care unit randomized trial compar-ing two approaches to oxygen therapy (ICU-ROX). Intensive Care Med 2020 ; 46 : 17 – 26
41. Schj ø rring OL , Perner A , Wetterslev J , Lange T , Keus F , Laake JH , Okkonen M , Siegemund M , Morgan M , Thormar KM , Rasmussen BS ; HOT-ICU Investigators : Handling oxygenation targets in the intensive care unit (HOT-ICU): Protocol for a ran-domised clinical trial comparing a lower vs. a higher oxygenation target in adults with acute hypoxaemic
respiratory failure. Acta Anaesthesiol Scand 2019 ; 63 : 956 – 65
42. Barrot L , Asfar P , Mauny F , Winiszewski H , Montini F , Badie J , Quenot JP , Pili-Floury S , Bouhemad B , Louis G , Souweine B , Collange O , Pottecher J , Levy B , Puyraveau M , Vettoretti L , Constantin JM , Capellier G ; LOCO2 Investigators and REVA Research Network : Liberal or conservative oxygen therapy for acute respiratory dis-tress syndrome. N Engl J Med 2020 ; 382 : 999 – 1008
43. Lopez MG , Pretorius M , Shotwell MS , Deegan R , Eagle SS , Bennett JM , Sileshi B , Liang Y , Gelfand BJ , Kingeter AJ , Siegrist KK , Lombard FW , Richburg TM , Fornero DA , Shaw AD , Hernandez A , Billings FT 4th : The Risk of Oxygen during Cardiac Surgery (ROCS) trial: Study protocol for a randomized clinical trial. Trials 2017 ; 18 : 295
44. Berr í os-Torres SI , Umscheid CA , Bratzler DW , Leas B , Stone EC , Kelz RR , Reinke CE , Morgan S , Solomkin JS , Mazuski JE , Dellinger EP , Itani KMF , Berbari EF , Segreti J , Parvizi J , Blanchard J , Allen G , Kluytmans JAJW , Donlan R , Schecter WP ; Healthcare Infection Control Practices Advisory Committee : Centers for Disease Control and Prevention guideline for the pre-vention of surgical site infection, 2017. JAMA Surg 2017 ; 152 : 784 – 91
45. Allegranzi B , Zayed B , Bischo P , Kubilay NZ , de Jonge S , de Vries F , Gomes SM , Gans S , Wallert ED , Wu X , Abbas M , Boermeester MA , Dellinger EP , Egger M , Gastmeier P , Guirao X , Ren J , Pittet D , Solomkin JS ; WHO Guidelines Development Group : New WHO recommendations on intraoperative and postoperative measures for surgical site infection prevention: An evidence-based global perspec-tive. Lancet Infect Dis 2016 ; 16 : e288 – 303
46. Meyho CS : Perioperative hyperoxia: Why guidelines, research and clinical practice collide. Br J Anaesth 2019 ; 122 : 289 – 91
47. Mattishent K , Thavarajah M , Sinha A , Peel A , Egger M , Solomkin J , de Jonge S , Latif A , Berenholtz S , Allegranzi B , Loke YK : Safety of 80% vs. 30 – 35% frac-tion of inspired oxygen in patients undergoing surgery: A systematic review and meta-analysis. Br J Anaesth 2019 ; 122 : 311 – 24
48. de Jonge S , Egger M , Latif A , Loke YK , Berenholtz S , Boermeester M , Allegranzi B , Solomkin J : E ectiveness of 80% vs. 30 – 35% fraction of inspired oxygen in patients undergoing surgery: An updated systematic review and meta-analysis. Br J Anaesth 2019 ; 122 : 325 – 34
49. Vasunilashorn SM , Fong TG , Albuquerque A , Marcantonio ER , Schmitt EM , Tommet D , Gou Y , Travison TG , Jones RN , Inouye SK : Delirium severity post-surgery and its relationship with long-term cog-nitive decline in a cohort of patients without dementia. J Alzheimers Dis 2018 ; 61 : 347 – 58
50. Shelton KT , Qu J , Bilotta F , Brown EN , Cudemus G , D ’ Alessandro DA , Deng H , DiBiasio A , Gitlin JA ,
ALNV134N2_Text.indb 200ALNV134N2_Text.indb 200 29-Dec-20 19:43:4929-Dec-20 19:43:49
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:189–201 201
Intraoperative Oxygen and Cognition after Surgery
Shaefi et al.
Hahm EY , Hobbs LE , Houle TT , Ibala R , Loggia ML , Pavone KJ , Shae S , Tolis G , Westover MB , Akeju O : Minimizing ICU Neurological Dysfunction with Dexmedetomidine-induced Sleep (MINDDS): Protocol for a randomised, double-blind, parallel-arm, placebo-controlled trial. BMJ Open 2018 ; 8 : e020316
51. Zietemann V , Kopczak A , M ü ller C , Wollenweber FA , Dichgans M : Validation of the Telephone Interview of Cognitive Status and Telephone Montreal Cognitive Assessment against detailed cognitive testing and clini-cal diagnosis of mild cognitive impairment after stroke. Stroke 2017 ; 48 : 2952 – 7
ALNV134N2_Text.indb 201ALNV134N2_Text.indb 201 29-Dec-20 19:43:4929-Dec-20 19:43:49
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
PERIOPERATIVE MEDICINE
202 FEBRUARY 2021 ANESTHESIOLOGY, V 134 • NO 2
ABSTRACT Background: Nitrous oxide produces non – γ -aminobutyric acid seda-tion and psychometric impairment and can be used as scientifi c model for understanding mechanisms of progressive cognitive disturbances. Temporal complexity of the electroencephalogram may be a sensitive indicator of these effects. This study measured psychometric performance and the temporal complexity of the electroencephalogram in participants breathing low-dose nitrous oxide.
Methods: In random order, 20, 30, and 40% end-tidal nitrous oxide was administered to 12 participants while recording 32-channel electroenceph-alogram and psychometric function. A novel metric quantifying the spatial distribution of temporal electroencephalogram complexity, comprised of (1) absolute cross-correlation calculated between consecutive 0.25-s time sam-ples; 2) binarizing these cross-correlation matrices using the median of all channels as threshold; (3) using quantitative recurrence analysis, the com-plexity in temporal changes calculated by the Shannon entropy of the proba-bility distribution of the diagonal line lengths; and (4) overall spatial extent and intensity of brain complexity, was quantifi ed by calculating median temporal complexity of channels whose complexities were above 1 at baseline. This region approximately overlay the brain ’ s default mode network, so this sum-mary statistic was termed “ default-mode-network complexity. ”
Results: Nitrous oxide concentration correlated with psychometric impair-ment ( r = 0.50, P < 0.001). Baseline regional electroencephalogram com-plexity at midline was greater than in lateral temporal channels (1.33 ± 0.14 bits vs . 0.81 ± 0.12 bits, P < 0.001). A dose of 40% N
2 O decreased midline
(mean difference [95% CI], 0.20 bits [0.09 to 0.31], P = 0.002) and prefrontal electroencephalogram complexity (mean difference [95% CI], 0.17 bits [0.08 to 0.27], P = 0.002). The lateral temporal region did not change signifi cantly (mean difference [95% CI], 0.14 bits [ − 0.03 to 0.30], P = 0.100). Default-mode-network complexity correlated with N
2 O concentration ( r = − 0.55,
P < 0.001). A default-mode-network complexity mixed-effects model cor-related with psychometric impairment ( r2 = 0.67; receiver operating charac-teristic area [95% CI], 0.72 [0.59 to 0.85], P < 0.001).
Conclusions: Temporal complexity decreased most markedly in medial cortical regions during low-dose nitrous oxide exposures, and this change tracked psychometric impairment.
(ANESTHESIOLOGY 2021 ; 134 : 202 – 18 )
An Electroencephalogram Metric of Temporal Complexity Tracks Psychometric Impairment Caused by Low-dose Nitrous Oxide Xavier C. E. Vrijdag , M.Sc. , Hanna van Waart , Ph.D. , Simon J. Mitchell , Ph.D., F.A.N.Z.C.A. , Jamie W. Sleigh , M.D., F.A.N.Z.C.A.
ANESTHESIOLOGY 2021 ; 134 : 202 – 18
This article is featured in “This Month in Anesthesiology,” page 1A. Supplemental Digital Content is available for this article. Direct URL citations appear in the printed text and are available in both the HTML and PDF versions of this article. Links to the digital fi les are provided in the HTML text of this article on the Journal ’ s Web site (www.anesthesiology.org). This article has a visual abstract available in the online version.
Submitted for publication June 24, 2020. Accepted for publication October 23, 2020. Published online fi rst on December 2, 2020. From the Department of Anaesthesiology, University of Auckland, Auckland, New Zealand (X.C.E.V., H.v.W., S.J.M., J.W.S.); the Department of Anaesthesia, Auckland City Hospital, Auckland, New Zealand (S.J.M.); and the Department of Anaesthesia, Waikato Hospital, Hamilton, New Zealand (J.W.S.).
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved. Anesthesiology 2021 ; 134 : 202 – 18 . DOI: 10.1097/ALN.0000000000003628
EDITOR ’ S PERSPECTIVE
What We Already Know about This Topic
• Low-dose nitrous oxide is known to increase reaction time and error rate in psychometric tests, but no electrophysiologic measurement has been capable of measuring this effect
What This Article Tells Us That Is New
• A quantitative electroencephalogram analysis can identify associ-ations between treatment with low-dose nitrous oxide and perfor-mance on psychometric tests
• Temporal complexity decreases in the medial cortical regions during nitrous oxide administration and is correlated with psycho-metric performance
Nitrous oxide is a weak anesthetic gas mostly used in dentistry, obstetrics, and acute trauma. 1 It has anal-
gesic and hypnotic properties, as well as strong dissociative e ects. 2 In the operating theater, it is used to supple-ment more potent anesthetic vapors in achieving general anesthesia. 3
The electroencephalogram (EEG) and derivative anes-thetic monitors have been used intensively to under-stand the neurologic e ects of various anesthetic agents and consciousness. 4 , 5 Most of the research has focused on
γ -aminobutyric acid – mediated (GABAergic) drugs and the transition into unconsciousness. Limited research e ort has gone into understanding the narcotic e ects of N -methyl-d -aspartate antagonists like nitrous oxide and ketamine. Various articles have shown that anesthetic depth monitors that are calibrated for GABAergic-induced unconscious-ness are insensitive to nitrous oxide 6 – 9 due to its di erent
ALNV134N2_Text.indb 202ALNV134N2_Text.indb 202 29-Dec-20 19:43:4929-Dec-20 19:43:49
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:202–18 203
Low-dose Nitrous Oxide Electroencephalogram Metric
Vrijdag et al.
mechanism of action. The EEG e ects of subanesthetic concentrations of nitrous oxide have been even less well studied. Although the excellent clinical safety record of this gas precludes any necessity to develop an EEG index of its e ects, nitrous oxide can be used as a scienti c model to understand mechanisms of how cognition is progres-sively impaired by non-GABAergic sedation. Accordingly, these experiments were performed to establish methodol-ogies — in a normobaric environment — that could later be applied to studies of hyperbaric nitrogen narcosis or other scenarios involving non-GABAergic sedation.
Nitrous oxide has been reported to cause inconsistent changes in the EEG power spectrum, but often there is an increase in power (amplitude) in high-frequency bands ( > 14 Hz, beta and gamma), with a relative decrease in power in the alpha and delta frequency bands (7 to 14 and 1 to 4 Hz). 10 The power reduction in alpha and delta bands 11
is localized in the frontal region 12 , 13 and most pronounced at higher inspired concentrations (40 to 60%). 12 , 14 , 15 Nitrous oxide also reduces spatial connectivity in parietal (at 60% N
2 O) and frontal (16 to 30% N
2 O) regions. 13 , 16 Changes in
spatial connectivity are often accompanied by changes in complexity in the time domain.
Complexity is a nonspeci c term used broadly to des-ignate the use of various algorithms including Lempel – Ziv, Kolmogorov – Chaitin, a variety of di erent entropies, and recurrence analysis. 17 In this study, we were interested in the evolution in time of EEG motifs, because these indi-cate the dynamics of cortical transitions between metastable states. This “ temporal complexity ” has been shown to cor-relate with cognitive task performance, 18 and we hypothe-sized that nitrous oxide would reduce this. The “ temporal complexity ” can be measured with the diagonal line lengths calculated from recurrence plots. 19 , 20 These line lengths indicate the evolution of brain states over time, by their correlation between successive time samples. 18
Therefore, in this exploratory study, we used low-dose nitrous oxide as a perturbation of cognition. Nitrous oxide is known to increase reaction time and error rate in psy-chometric tests. 21 – 24 We present a novel quantitative EEG analysis method that is sensitive to low-dose nitrous oxide exposures and correlates with the levels of psychometric impairment. The proposed analysis method quanti es the spatial distribution of the temporal complexity of the EEG signal.
Materials and Methods
Trial Design and Participants
This multidose (in randomized order), single-blind, cross-over trial took place at the laboratory at Waikato Clinical School, University of Auckland, in July and August 2018. The study protocol was approved by the Health and Disability Ethics Committee, Auckland, New Zealand (ref-erence 16/NTA/93), and was registered with the Australian
New Zealand Clinical Trial Registry (registry No. U1111-1181-9722) on December 3, 2018, by S.J.M. The sample size was based on similar studies previously published. 16 , 22 – 24
This study was a prelude to further work investigating EEG e ects of gas narcosis in divers, so participants were recruited from that community. Eligible subjects were cer-ti ed, healthy divers (checked with the Recreational Scuba Training Council [Jacksonville, Florida] screening question-naire for tness), aged between 18 and 60 yr, with normal visual acuity, either corrected or uncorrected. Exclusion criteria were the use of recreational drugs, tobacco, psycho-active medication, excessive alcohol (more than 21 standard drinks per week), or over ve ca eine-containing beverages a day. All participants provided written informed consent.
Participants abstained from any ca einated drink on the measurement day and from alcohol at least 24 h before. Participants had at least 6 h of sleep and fasted for 4 h before the measurement.
Experimental Procedures
Breathing Circuit and Monitoring . Participants were seated and breathed from a closed-circuit anesthesia loop (Vital Signs, Mexico) attached to an anesthesia machine (S/5 Aespire, Datex-Ohmeda, USA). A mouthpiece and dispos-able anesthetic antibacterial lter (Ultipor 25, Pall, USA) were replaced for each participant. The nose was occluded with a nose clip. The inspired fraction of oxygen, end-tidal pressure of carbon dioxide (P etco
2 ), and end-tidal percent-
age of nitrous oxide were continuously sampled from the mouthpiece lter and were recorded every minute. Oxygen saturation and breathing frequency were monitored for par-ticipant safety. Measurement Protoco l . Every participant started with a baseline measurement while breathing 50% oxygen (bal-ance nitrogen) on the circuit. The subjects then breathed a titrated nitrous oxide mixture (balance oxygen) to achieve an end-tidal level of 20%, 30%, or 40% N
2 O, followed by
20 min of breathing air between each nitrous oxide expo-sure. Participants were blinded to the dose of nitrous oxide, which was administered in random order of doses dictated by a ticket drawn by the researcher when the participant arrived (order: 20-30-40%; 20-40-30%; 30-20-40%; 30-40-20%; 40-20-30%; or 40-30-20%).
Every exposure started with a 3- to 5-min wash-in period, during which the inspired fraction of nitrous oxide was manually adjusted to establish and maintain the desired end-tidal level. Then a set of measurements was undertaken consisting of EEG recording over 1 min with eyes open and 1 min with eyes closed, completion of psychometric tests, and a pupillometry measurement (pupillometry results were published elsewhere 25 ). Finally, the 1-min eyes-open and -closed EEG recordings were repeated. At the end of each exposure, nitrous oxide was washed out using oxygen with a ow of 6 l · min − 1 and was followed by a 20-min air breathing rest period. A nal measurement set during 50%
ALNV134N2_Text.indb 203ALNV134N2_Text.indb 203 29-Dec-20 19:43:4929-Dec-20 19:43:49
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
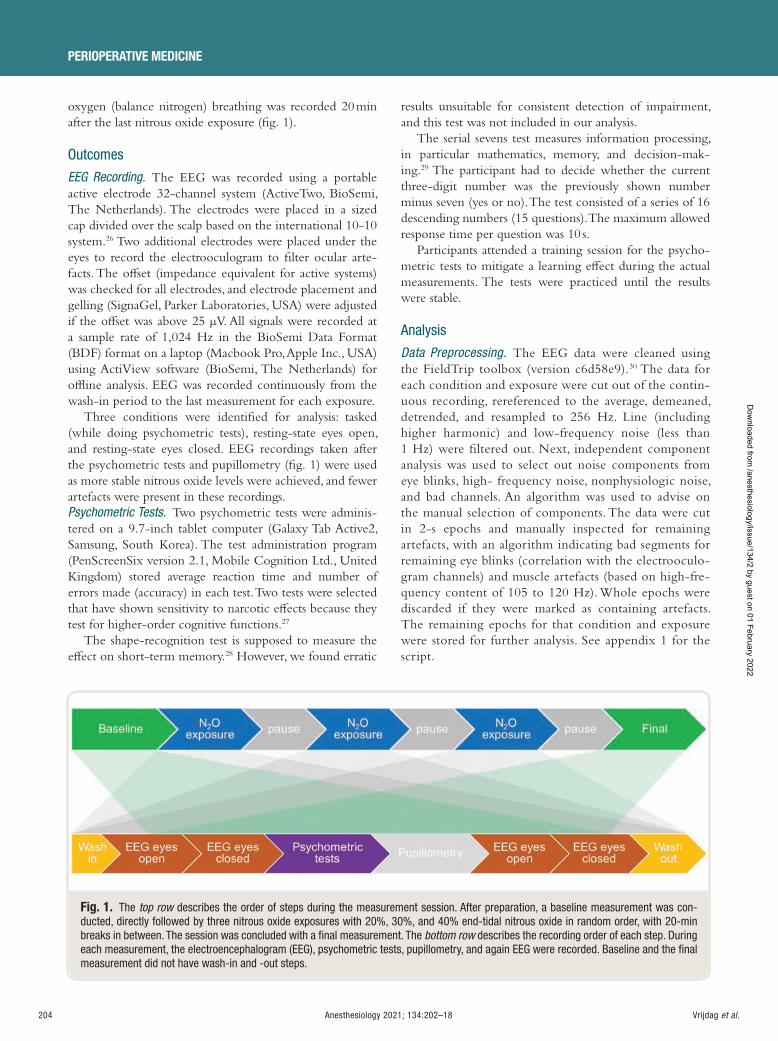
204 Anesthesiology 2021; 134:202–18
PERIOPERATIVE MEDICINE
Vrijdag et al.
oxygen (balance nitrogen) breathing was recorded 20 min after the last nitrous oxide exposure ( g. 1 ).
Outcomes
EEG Recording . The EEG was recorded using a portable active electrode 32-channel system (ActiveTwo, BioSemi, The Netherlands). The electrodes were placed in a sized cap divided over the scalp based on the international 10-10 system. 26 Two additional electrodes were placed under the eyes to record the electrooculogram to lter ocular arte-facts. The o set (impedance equivalent for active systems) was checked for all electrodes, and electrode placement and gelling (SignaGel, Parker Laboratories, USA) were adjusted if the o set was above 25 µ V. All signals were recorded at a sample rate of 1,024 Hz in the BioSemi Data Format (BDF) format on a laptop (Macbook Pro, Apple Inc., USA) using ActiView software (BioSemi, The Netherlands) for o ine analysis. EEG was recorded continuously from the wash-in period to the last measurement for each exposure.
Three conditions were identi ed for analysis: tasked (while doing psychometric tests), resting-state eyes open, and resting-state eyes closed. EEG recordings taken after the psychometric tests and pupillometry ( g. 1 ) were used as more stable nitrous oxide levels were achieved, and fewer artefacts were present in these recordings. Psychometric Tests . Two psychometric tests were adminis-tered on a 9.7-inch tablet computer (Galaxy Tab Active2, Samsung, South Korea). The test administration program (PenScreenSix version 2.1, Mobile Cognition Ltd., United Kingdom) stored average reaction time and number of errors made (accuracy) in each test. Two tests were selected that have shown sensitivity to narcotic e ects because they test for higher-order cognitive functions. 27
The shape-recognition test is supposed to measure the e ect on short-term memory. 28 However, we found erratic
results unsuitable for consistent detection of impairment, and this test was not included in our analysis.
The serial sevens test measures information processing, in particular mathematics, memory, and decision-mak-ing. 29 The participant had to decide whether the current three-digit number was the previously shown number minus seven (yes or no). The test consisted of a series of 16 descending numbers (15 questions). The maximum allowed response time per question was 10 s.
Participants attended a training session for the psycho-metric tests to mitigate a learning e ect during the actual measurements. The tests were practiced until the results were stable.
Analysis
Data Preprocessing . The EEG data were cleaned using the FieldTrip toolbox (version c6d58e9). 30 The data for each condition and exposure were cut out of the contin-uous recording, rereferenced to the average, demeaned, detrended, and resampled to 256 Hz. Line (including higher harmonic) and low-frequency noise (less than 1 Hz) were ltered out. Next, independent component analysis was used to select out noise components from eye blinks, high- frequency noise, nonphysiologic noise, and bad channels. An algorithm was used to advise on the manual selection of components. The data were cut in 2-s epochs and manually inspected for remaining artefacts, with an algorithm indicating bad segments for remaining eye blinks (correlation with the electrooculo-gram channels) and muscle artefacts (based on high-fre-quency content of 105 to 120 Hz). Whole epochs were discarded if they were marked as containing artefacts. The remaining epochs for that condition and exposure were stored for further analysis. See appendix 1 for the script.
Fig. 1. The top row describes the order of steps during the measurement session. After preparation, a baseline measurement was con-ducted, directly followed by three nitrous oxide exposures with 20%, 30%, and 40% end-tidal nitrous oxide in random order, with 20-min breaks in between. The session was concluded with a fi nal measurement. The bottom row describes the recording order of each step. During each measurement, the electroencephalogram (EEG), psychometric tests, pupillometry, and again EEG were recorded. Baseline and the fi nal measurement did not have wash-in and -out steps.
ALNV134N2_Text.indb 204ALNV134N2_Text.indb 204 29-Dec-20 19:43:5029-Dec-20 19:43:50
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
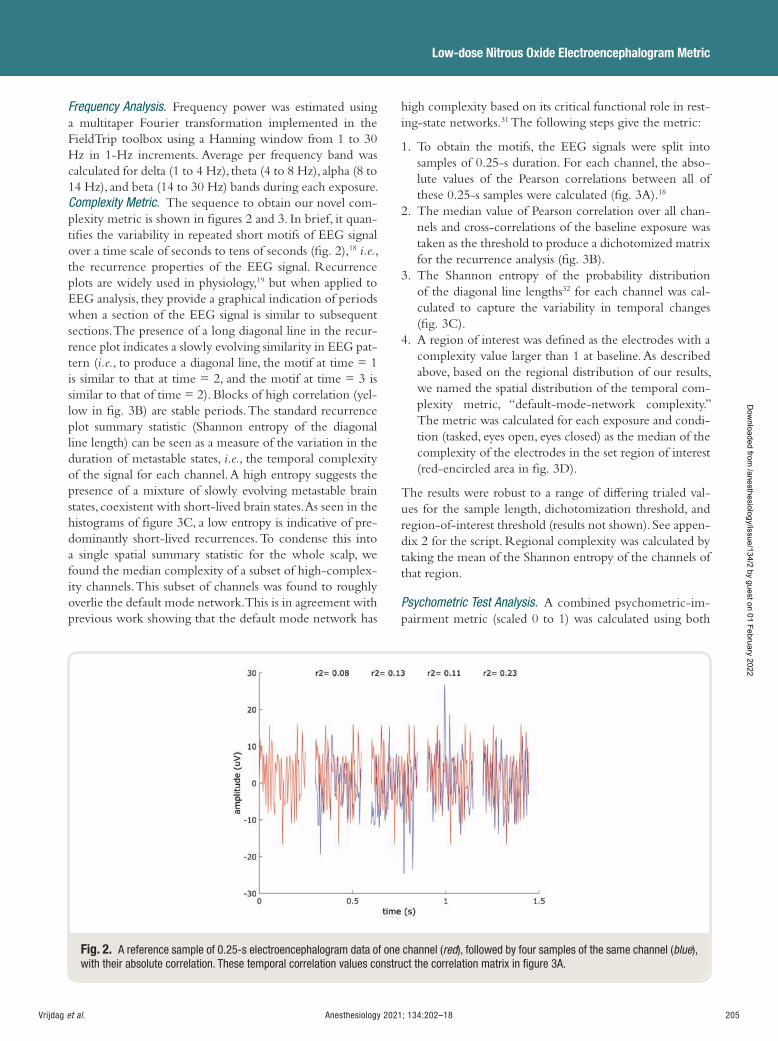
Anesthesiology 2021; 134:202–18 205
Low-dose Nitrous Oxide Electroencephalogram Metric
Vrijdag et al.
Frequency Analysis . Frequency power was estimated using a multitaper Fourier transformation implemented in the FieldTrip toolbox using a Hanning window from 1 to 30 Hz in 1-Hz increments. Average per frequency band was calculated for delta (1 to 4 Hz), theta (4 to 8 Hz), alpha (8 to 14 Hz), and beta (14 to 30 Hz) bands during each exposure. Complexity Metric . The sequence to obtain our novel com-plexity metric is shown in gures 2 and 3. In brief, it quan-ti es the variability in repeated short motifs of EEG signal over a time scale of seconds to tens of seconds ( g. 2 ), 18 i.e. , the recurrence properties of the EEG signal. Recurrence plots are widely used in physiology, 19 but when applied to EEG analysis, they provide a graphical indication of periods when a section of the EEG signal is similar to subsequent sections. The presence of a long diagonal line in the recur-rence plot indicates a slowly evolving similarity in EEG pat-tern ( i.e. , to produce a diagonal line, the motif at time = 1 is similar to that at time = 2, and the motif at time = 3 is similar to that of time = 2). Blocks of high correlation (yel-low in g. 3B ) are stable periods. The standard recurrence plot summary statistic (Shannon entropy of the diagonal line length) can be seen as a measure of the variation in the duration of metastable states, i.e. , the temporal complexity of the signal for each channel. A high entropy suggests the presence of a mixture of slowly evolving metastable brain states, coexistent with short-lived brain states. As seen in the histograms of gure 3C , a low entropy is indicative of pre-dominantly short-lived recurrences. To condense this into a single spatial summary statistic for the whole scalp, we found the median complexity of a subset of high-complex-ity channels. This subset of channels was found to roughly overlie the default mode network. This is in agreement with previous work showing that the default mode network has
high complexity based on its critical functional role in rest-ing-state networks. 31 The following steps give the metric:
1. To obtain the motifs, the EEG signals were split into samples of 0.25-s duration. For each channel, the abso-lute values of the Pearson correlations between all of these 0.25-s samples were calculated ( g. 3A ). 18
2. The median value of Pearson correlation over all chan-nels and cross-correlations of the baseline exposure was taken as the threshold to produce a dichotomized matrix for the recurrence analysis ( g. 3B ).
3. The Shannon entropy of the probability distribution of the diagonal line lengths 32 for each channel was cal-culated to capture the variability in temporal changes ( g. 3C ).
4. A region of interest was de ned as the electrodes with a complexity value larger than 1 at baseline. As described above, based on the regional distribution of our results, we named the spatial distribution of the temporal com-plexity metric, “ default-mode-network complexity. ” The metric was calculated for each exposure and condi-tion (tasked, eyes open, eyes closed) as the median of the complexity of the electrodes in the set region of interest (red-encircled area in g. 3D ).
The results were robust to a range of di ering trialed val-ues for the sample length, dichotomization threshold, and region-of-interest threshold (results not shown). See appen-dix 2 for the script. Regional complexity was calculated by taking the mean of the Shannon entropy of the channels of that region.
Psychometric Test Analysis . A combined psychometric-im-pairment metric (scaled 0 to 1) was calculated using both
Fig. 2. A reference sample of 0.25-s electroencephalogram data of one channel ( red ), followed by four samples of the same channel ( blue ), with their absolute correlation. These temporal correlation values construct the correlation matrix in fi gure 3A .
ALNV134N2_Text.indb 205ALNV134N2_Text.indb 205 29-Dec-20 19:43:5029-Dec-20 19:43:50
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
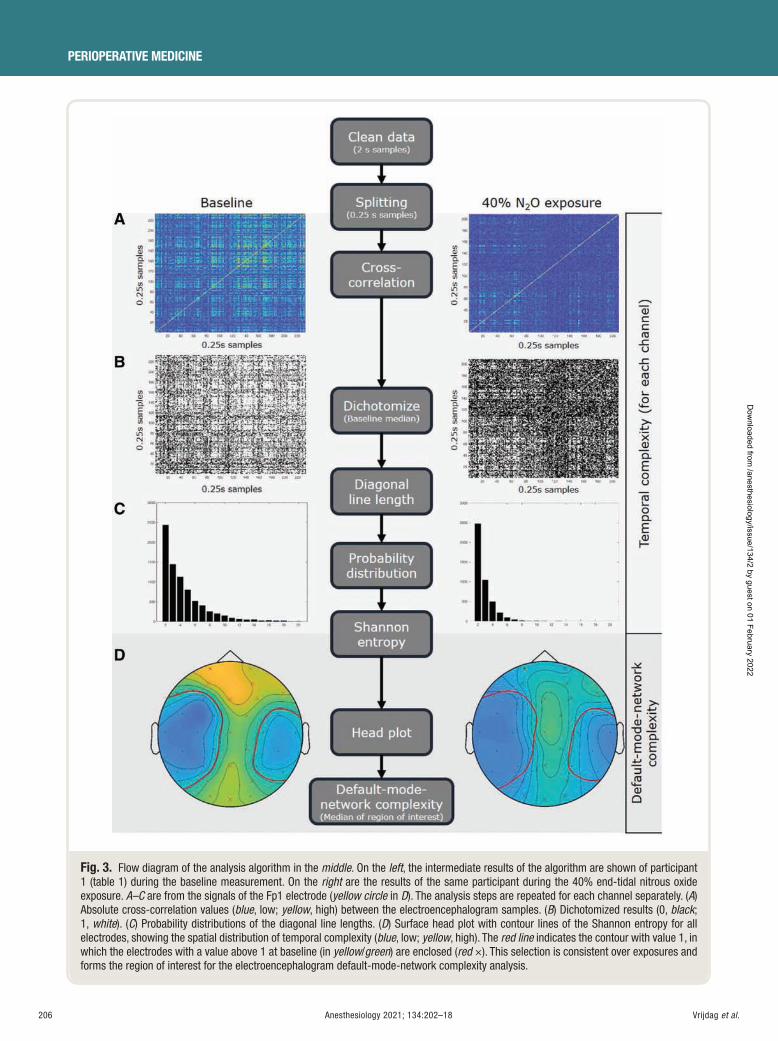
206 Anesthesiology 2021; 134:202–18
PERIOPERATIVE MEDICINE
Vrijdag et al.
Fig. 3. Flow diagram of the analysis algorithm in the middle . On the left , the intermediate results of the algorithm are shown of participant 1 ( table 1 ) during the baseline measurement. On the right are the results of the same participant during the 40% end-tidal nitrous oxide exposure. A – C are from the signals of the Fp1 electrode ( yellow circle in D ). The analysis steps are repeated for each channel separately. ( A ) Absolute cross-correlation values ( blue , low; yellow , high) between the electroencephalogram samples. ( B ) Dichotomized results (0, black ; 1, white ). ( C ) Probability distributions of the diagonal line lengths. ( D ) Surface head plot with contour lines of the Shannon entropy for all electrodes, showing the spatial distribution of temporal complexity ( blue , low; yellow , high). The red line indicates the contour with value 1, in which the electrodes with a value above 1 at baseline (in yellow / green ) are enclosed ( red × ). This selection is consistent over exposures and forms the region of interest for the electroencephalogram default-mode-network complexity analysis.
ALNV134N2_Text.indb 206ALNV134N2_Text.indb 206 29-Dec-20 19:43:5129-Dec-20 19:43:51
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:202–18 207
Low-dose Nitrous Oxide Electroencephalogram Metric
Vrijdag et al.
the mean reaction time and error rate to counteract the speed-accuracy trade-o (equation 1). 33
mean reaction timerespons time
number of errorsnumber of questmax
+iions
2
(1)
Statistical Analysis
All data were analyzed with Matlab version 2018a (Mathworks, USA) except the carbon dioxide data, which were analyzed with SPSS version 25 (IBM, USA). The idea of EEG data analysis using temporal complexity was pre-planned, based on previous published work. 20 , 34 , 35 However, the speci c values of various parameters in the algorithm and the default mode network region of interest were data-driven, as part of the exploratory study. The comparison between the EEG metric and psychometric test score was prede ned. All outcome measures were tested for normal-ity and subsequently characterized by their mean and SD. Comparisons of regional complexity were done using a two-tailed paired t test and reported as mean di erence and 95% CI. P values were regarded as signi cant at P < 0.05, with Bonferroni correction for multiple comparisons.
For all exposures and individuals, a linear mixed-ef-fects model was used to calculate the relationship between the EEG default-mode-network complexity metric ( DMNcomplexity ) and the psychometric test metric ( S77 ) using equation 2.
S DMNcomplexity DMNcomplexity participant77 1 1~ ( | )+ + + (2)
The between-participant variation was included as a ran-dom e ect, with a random intercept and slope. This design can capture variation in baseline complexity and dose response for each subject. The models for the three con-ditions were compared using a likelihood ratio test with 1,000 simulations.
To research the possible in uence of hypercapnia, car-bon dioxide levels were analyzed. The P etco
2 value at the
start of the psychometric test was added as a xed-e ect parameter to the mixed-e ects model for the tasked con-dition (EEG recording during the psychometric test). This model was compared to the model without carbon dioxide level (same method as above).
The in uence of the power in each frequency band (delta [1 to 4 Hz], theta [4 to 8 Hz], alpha [8 to 14 Hz], beta [14 to 30 Hz], and gamma [30 to 45 Hz]) on the nal model was also investigated. For this subanalysis, the EEG data of the eyes-open condition were bandpass- ltered with a Butterworth lter (order 4) in both directions using a Hamming window for each frequency band.
A receiver operating characteristic analysis was used to compare the default-mode-network complexity metric against the serial sevens test results. The serial sevens data were dichotomized to “ impaired ” (greater than 0.16) and
“ not impaired ” (less than or equal to 0.16), based on the upper value of the interquartile range ( g. 4 ) of the baseline exposure.
Results The 12 participants (8 male), aged between 23 and 55 yr (mean. 36 yr), had an average body mass index of 26.3 kg/m 2 (22.7 to 31.3). On average, 1.7 of 30, 1.3 of 30, and 19.5 of 108 (eyes open, eyes closed, and tasked, respectively) of the 2-s EEG samples were removed due to artefacts. The latter were mostly muscle artefacts. EEG frequency anal-ysis shows an increase in power in the beta band, with a relative decrease in the delta band, most prominent in the frontal region and most visible in the 20% and 40% expo-sures (Supplemental Digital Content 1, http://links.lww.com/ALN/C512, shows the frequency band analysis). This is similar to previous studies. 10 – 14 In general, the serial sevens test results worsened ( g. 4A ) and the complexity metric decreased ( g. 4B ) at increased end-tidal concentrations of nitrous oxide, particularly once the 40% concentration was reached. End-tidal nitrous oxide concentrations exhibited a moderate correlation with both the serial sevens scores and the EEG default-mode-network complexity ( r = 0.50, P < 0.001 and r = − 0.55, P < 0.001, respectively).
Regional Differences
At baseline ( g. 5 ), regional temporal complexity was greater in the midline (1.33 ± 0.14 bits), which approxi-mately overlies the default mode network, than in channels overlying lateral temporal brain regions (0.81 ± 0.12 bits; mean di erence, 0.52 [0.39 to 0.65], P < 0.001). Increasing nitrous oxide exposure caused a decrease in brain complex-ity predominantly in the midline (baseline vs . 40% N
2 O:
mean di erence, 0.20 bits [0.09 to 0.31], P = 0.002) and prefrontal (baseline vs . 40% N
2 O: mean di erence, 0.17
bits [0.08 to 0.27], P = 0.002) regions, whereas complexity in the lateral temporal region did not change signi cantly (baseline vs . 40% N
2 O: mean di erence, 0.14 bits [ − 0.03 to
0.30], P = 0.100). These changes were reversed after cessa-tion of nitrous oxide.
Mixed-effects Modeling
At baseline, the EEG default-mode-network complexity metric ranged from 1.13 to 1.38 bits between subjects. The e ects of the di erent doses of nitrous oxide were variable between subjects. For some participants, the ranking order of the nitrous oxide concentrations did not correlate with the ranking order of both the psychometric tests (y axis) and EEG default-mode-network complexity (x axis; g. 6 ). There was a signi cant di erence between the models for only the eyes-closed versus tasked conditions ( P = 0.003), but the log likelihoods of the models for the three conditions were very similar (52.3, 47.4, and 42.7). Therefore, gure 7shows the results of the model based on the eyes-open data.
ALNV134N2_Text.indb 207ALNV134N2_Text.indb 207 29-Dec-20 19:43:5129-Dec-20 19:43:51
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
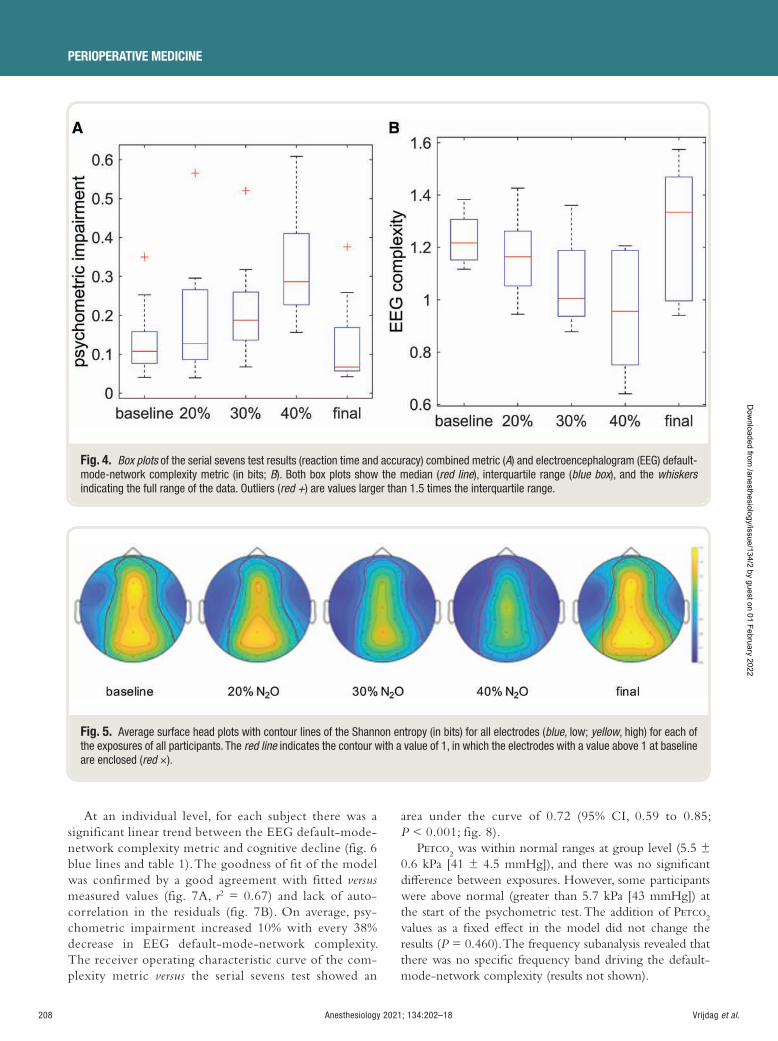
208 Anesthesiology 2021; 134:202–18
PERIOPERATIVE MEDICINE
Vrijdag et al.
At an individual level, for each subject there was a significant linear trend between the EEG default-mode-network complexity metric and cognitive decline ( fig. 6 blue lines and table 1 ). The goodness of fit of the model was confirmed by a good agreement with fitted versusmeasured values ( fig. 7A , r2 = 0.67) and lack of auto-correlation in the residuals ( fig. 7B ). On average, psy-chometric impairment increased 10% with every 38% decrease in EEG default-mode-network complexity. The receiver operating characteristic curve of the com-plexity metric versus the serial sevens test showed an
area under the curve of 0.72 (95% CI, 0.59 to 0.85; P < 0.001; fig. 8 ).
P etco2 was within normal ranges at group level (5.5 ±
0.6 kPa [41 ± 4.5 mmHg]), and there was no signi cant di erence between exposures. However, some participants were above normal (greater than 5.7 kPa [43 mmHg]) at the start of the psychometric test. The addition of P etco
2
values as a xed e ect in the model did not change the results ( P = 0.460). The frequency subanalysis revealed that there was no speci c frequency band driving the default-mode-network complexity (results not shown).
Fig. 4. Box plots of the serial sevens test results (reaction time and accuracy) combined metric ( A ) and electroencephalogram (EEG) default-mode-network complexity metric (in bits; B ). Both box plots show the median ( red line ), interquartile range ( blue box ), and the whiskersindicating the full range of the data. Outliers ( red + ) are values larger than 1.5 times the interquartile range.
Fig. 5. Average surface head plots with contour lines of the Shannon entropy (in bits) for all electrodes ( blue , low; yellow , high) for each of the exposures of all participants. The red line indicates the contour with a value of 1, in which the electrodes with a value above 1 at baseline are enclosed ( red × ).
ALNV134N2_Text.indb 208ALNV134N2_Text.indb 208 29-Dec-20 19:43:5329-Dec-20 19:43:53
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
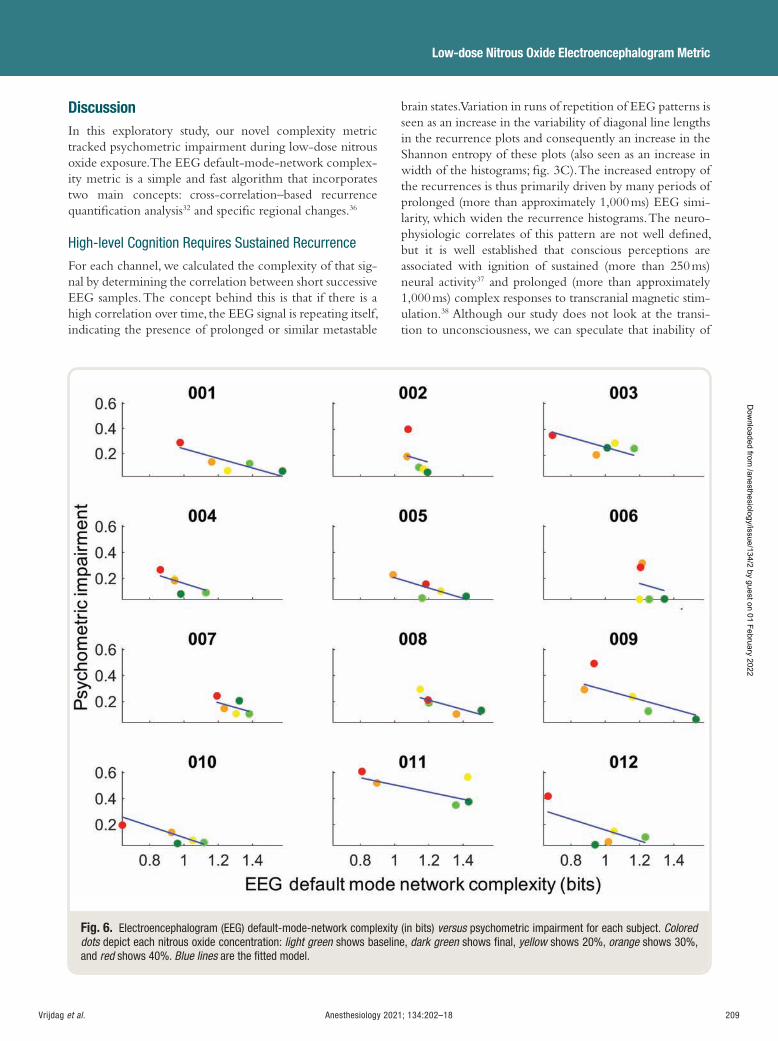
Anesthesiology 2021; 134:202–18 209
Low-dose Nitrous Oxide Electroencephalogram Metric
Vrijdag et al.
Discussion In this exploratory study, our novel complexity metric tracked psychometric impairment during low-dose nitrous oxide exposure. The EEG default-mode-network complex-ity metric is a simple and fast algorithm that incorporates two main concepts: cross-correlation – based recurrence quanti cation analysis 32 and speci c regional changes. 36
High-level Cognition Requires Sustained Recurrence
For each channel, we calculated the complexity of that sig-nal by determining the correlation between short successive EEG samples. The concept behind this is that if there is a high correlation over time, the EEG signal is repeating itself, indicating the presence of prolonged or similar metastable
brain states. Variation in runs of repetition of EEG patterns is seen as an increase in the variability of diagonal line lengths in the recurrence plots and consequently an increase in the Shannon entropy of these plots (also seen as an increase in width of the histograms; g. 3C ). The increased entropy of the recurrences is thus primarily driven by many periods of prolonged (more than approximately 1,000 ms) EEG simi-larity, which widen the recurrence histograms. The neuro-physiologic correlates of this pattern are not well de ned, but it is well established that conscious perceptions are associated with ignition of sustained (more than 250 ms) neural activity 37 and prolonged (more than approximately 1,000 ms) complex responses to transcranial magnetic stim-ulation. 38 Although our study does not look at the transi-tion to unconsciousness, we can speculate that inability of
Fig. 6. Electroencephalogram (EEG) default-mode-network complexity (in bits) versus psychometric impairment for each subject. Colored dots depict each nitrous oxide concentration: light green shows baseline, dark green shows fi nal, yellow shows 20%, orange shows 30%, and red shows 40%. Blue lines are the fi tted model.
ALNV134N2_Text.indb 209ALNV134N2_Text.indb 209 29-Dec-20 19:43:5329-Dec-20 19:43:53
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
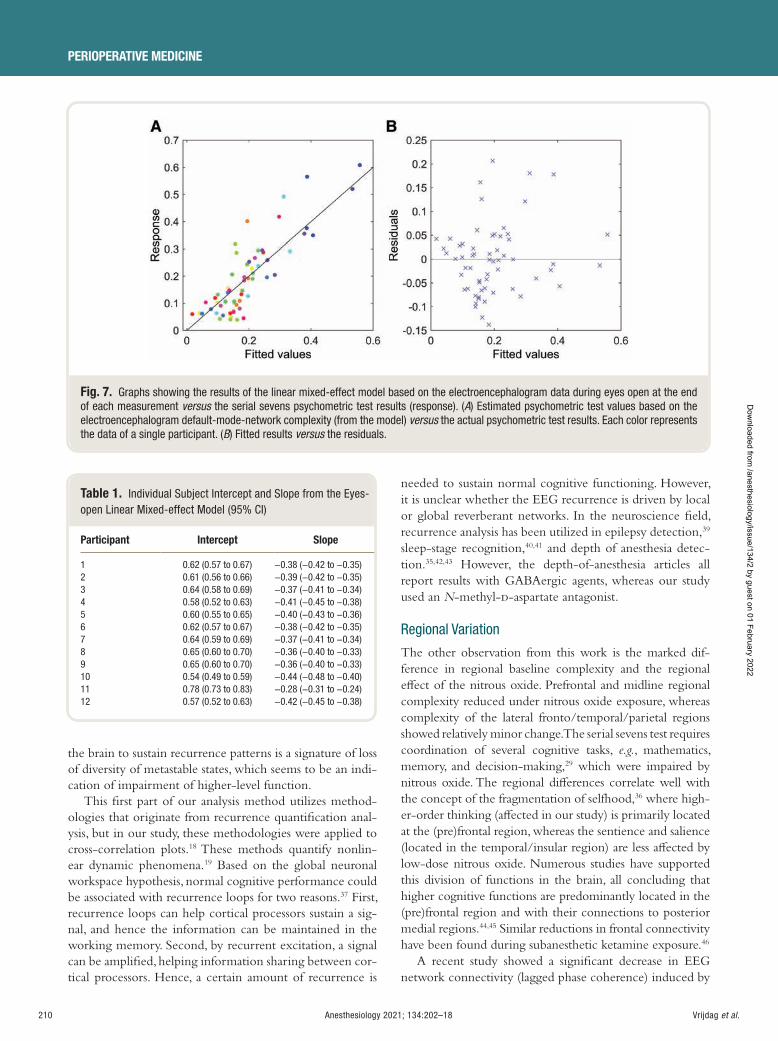
210 Anesthesiology 2021; 134:202–18
PERIOPERATIVE MEDICINE
Vrijdag et al.
the brain to sustain recurrence patterns is a signature of loss of diversity of metastable states, which seems to be an indi-cation of impairment of higher-level function.
This rst part of our analysis method utilizes method-ologies that originate from recurrence quanti cation anal-ysis, but in our study, these methodologies were applied to cross-correlation plots. 18 These methods quantify nonlin-ear dynamic phenomena. 19 Based on the global neuronal workspace hypothesis, normal cognitive performance could be associated with recurrence loops for two reasons. 37 First, recurrence loops can help cortical processors sustain a sig-nal, and hence the information can be maintained in the working memory. Second, by recurrent excitation, a signal can be ampli ed, helping information sharing between cor-tical processors. Hence, a certain amount of recurrence is
needed to sustain normal cognitive functioning. However, it is unclear whether the EEG recurrence is driven by local or global reverberant networks. In the neuroscience eld, recurrence analysis has been utilized in epilepsy detection, 39
sleep-stage recognition, 40 , 41 and depth of anesthesia detec-tion. 35 , 42 , 43 However, the depth-of-anesthesia articles all report results with GABAergic agents, whereas our study used an N -methyl- d -aspartate antagonist.
Regional Variation
The other observation from this work is the marked dif-ference in regional baseline complexity and the regional e ect of the nitrous oxide. Prefrontal and midline regional complexity reduced under nitrous oxide exposure, whereas complexity of the lateral fronto/temporal/parietal regions showed relatively minor change. The serial sevens test requires coordination of several cognitive tasks, e.g. , mathematics, memory, and decision-making, 29 which were impaired by nitrous oxide. The regional di erences correlate well with the concept of the fragmentation of selfhood, 36 where high-er-order thinking (a ected in our study) is primarily located at the (pre)frontal region, whereas the sentience and salience (located in the temporal/insular region) are less a ected by low-dose nitrous oxide. Numerous studies have supported this division of functions in the brain, all concluding that higher cognitive functions are predominantly located in the (pre)frontal region and with their connections to posterior medial regions. 44 , 45 Similar reductions in frontal connectivity have been found during subanesthetic ketamine exposure. 46
A recent study showed a signi cant decrease in EEG network connectivity ( lagged phase coherence) induced by
Fig. 7. Graphs showing the results of the linear mixed-effect model based on the electroencephalogram data during eyes open at the end of each measurement versus the serial sevens psychometric test results (response). ( A ) Estimated psychometric test values based on the electroencephalogram default-mode-network complexity (from the model) versus the actual psychometric test results. Each color represents the data of a single participant. ( B ) Fitted results versus the residuals.
Table 1. Individual Subject Intercept and Slope from the Eyes-open Linear Mixed-effect Model (95% CI)
Participant Intercept Slope
1 0.62 (0.57 to 0.67) − 0.38 ( − 0.42 to − 0.35) 2 0.61 (0.56 to 0.66) − 0.39 ( − 0.42 to − 0.35) 3 0.64 (0.58 to 0.69) − 0.37 ( − 0.41 to − 0.34) 4 0.58 (0.52 to 0.63) − 0.41 ( − 0.45 to − 0.38) 5 0.60 (0.55 to 0.65) − 0.40 ( − 0.43 to − 0.36) 6 0.62 (0.57 to 0.67) − 0.38 ( − 0.42 to − 0.35) 7 0.64 (0.59 to 0.69) − 0.37 ( − 0.41 to − 0.34) 8 0.65 (0.60 to 0.70) − 0.36 ( − 0.40 to − 0.33) 9 0.65 (0.60 to 0.70) − 0.36 ( − 0.40 to − 0.33) 10 0.54 (0.49 to 0.59) − 0.44 ( − 0.48 to − 0.40) 11 0.78 (0.73 to 0.83) − 0.28 ( − 0.31 to − 0.24) 12 0.57 (0.52 to 0.63) − 0.42 ( − 0.45 to − 0.38)
ALNV134N2_Text.indb 210ALNV134N2_Text.indb 210 29-Dec-20 19:43:5429-Dec-20 19:43:54
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:202–18 211
Low-dose Nitrous Oxide Electroencephalogram Metric
Vrijdag et al.
50% inhaled nitrous oxide. 47 This disruptive e ect of rela-tively high-dose nitrous oxide on the ow of information between brain regions is consistent with the default mode network regional decrease in complexity found in our study. The nitrous oxide – impaired cognitive performance was strongly associated with loss of complexity in the medial default mode network regions (the so-called “ hot zone ” ). 38 The exact role of these brain regions (precuneus, posterior, and anterior cingulate cortices) is still intensely debated, 48 but seems to be more closely aligned with over-all higher-order brain integration and coordination 49 rather than speci c tasks. In particular, activity is associated with semantic processing and memory retrieval, which are nec-essary for the serial sevens test. 50
Limitations
Our study had some strengths. It was performed in a lab-oratory where the environment was well controlled to
optimize the EEG recording, with full-scalp 32 channels. By controlling the end-tidal concentrations of nitrous oxide, we were able to control the exposure to a narcotic agent precisely at three distinct levels, without the interference of other drugs. However, the psychometric tests showed a high level of personal variability in participants ’ responses to nitrous oxide. The variability could be explained by a car-ryover or learning e ect between the exposures, although we did incorporate a 20-min pause between exposures and randomized the order of exposures to minimize this e ect. We measured end-tidal carbon dioxide and found that an increased P etco2
above a normal value of 5.7 kPa (43 mmHg), which was found in some participants/exposures, did not contribute to the narcotic e ects found, similar to the results of Foster and Liley. 11
Our study also had some weaknesses. First, the partici-pant group was relatively small. In mitigation, it was reas-suring that the EEG default-mode-network complexity
Fig. 8. Receiver operating characteristic graph comparing the sensitivity and specifi city of the electroencephalogram default-mode-network complexity calculated with the eyes open at the end of the measurement versus the results of the serial sevens psychometric test.
ALNV134N2_Text.indb 211ALNV134N2_Text.indb 211 29-Dec-20 19:43:5429-Dec-20 19:43:54
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

212 Anesthesiology 2021; 134:202–18
PERIOPERATIVE MEDICINE
Vrijdag et al.
metric consistently decreased in every subject as psycho-metric impairment increased. Second, our exploratory analysis was directed toward a time-domain analysis. We did not use source localization to re ne the locations of tem-poral complexity further; hence, we chose to use general descriptors of locations. This increased the speed of analysis, kept the analysis method simple, and avoided the assump-tions underlying all source localization methods. We also acknowledge that our limited spatial resolution means that we have used the term “ default-mode-network complex-ity ” as a descriptive shorthand rather than being able to establish its full anatomical detail.
In conclusion, our novel quantitative EEG default-mode-network complexity metric based on tempo-ral complexity is sensitive to psychometric impairment caused by low-dose nitrous oxide. However, further research is needed to evaluate its functionality, because this was an exploratory study. If robust, this algorithm may be useful in quantifying and studying mild narcosis in situa-tions where patients are less self-aware due to the disso-ciative e ects of nitrous oxide or other non-GABAergic sedatives.
Acknowledgments
The authors are grateful to all participants in this study. Furthermore, the authors acknowledge Jonathan Termaat, Dip.R.N., Gay Mans, N.Z.R.G.O.N., Amy Gaskell, M.B.Ch.B., F.A.N.Z.C.A. (all Department of Anaesthesia, Waikato Hospital, Hamilton, New Zealand), Rebecca Pullon, Ph.D., and Marta Seretny, M.D., M.P.H., Ph.D., F.R.C.A. (both Department of Anaesthesiology, University of Auckland, Auckland, New Zealand), for their support during the data collection.
Research Support
This study was supported by funding from the O ce for Naval Research Global (Tokyo, Japan), U.S. Navy grant No. N62909-18-1-2007.
Competing Interests
The authors declare no competing interests.
Reproducible Science
Full protocol available at: [email protected] . Raw data available at: [email protected] .
Correspondence
Address correspondence to Mr. Vrijdag: School of Medicine, University of Auckland, Private Bag 92019, Auckland 1142, New Zealand. [email protected] . This article may be accessed for personal use at no charge through the Journal Web site, www.anesthesiology.org.
References
1. O ’ Sullivan I , Benger J : Nitrous oxide in emergency medicine. Emerg Med J 2003 ; 20 : 214 – 7
2. Brown EN , Purdon PL , Van Dort CJ : General anesthe-sia and altered states of arousal: A systems neuroscience analysis. Annu Rev Neurosci 2011 ; 34 : 601 – 28
3. Myles PS , Leslie K , Silbert B , Paech MJ , Peyton P : A review of the risks and bene ts of nitrous oxide in cur-rent anaesthetic practice. Anaesth Intensive Care 2004 ; 32 : 165 – 72
4. Marchant N , Sanders R , Sleigh J , Vanhaudenhuyse A , Bruno MA , Brichant JF , Laureys S , Bonhomme V : How electroencephalography serves the anesthesiologist. Clin EEG Neurosci 2014 ; 45 : 22 – 32
5. Kaiser HA , Hight D , Avidan MS : A narrative review of electroencephalogram-based monitoring during cardiovascular surgery. Curr Opin Anaesthesiol 2020 ; 33 : 92 – 100
6. Rampil IJ , Kim JS , Lenhardt R , Negishi C , Sessler DI : Bispectral EEG index during nitrous oxide administra-tion. A nesthesiology 1998 ; 89 : 671 – 7
7. Barr G , Jakobsson JG , Owall A , Anderson RE : Nitrous oxide does not alter bispectral index: Study with nitrous oxide as sole agent and as an adjunct to i.v. anaesthesia. Br J Anaesth 1999 ; 82 : 827 – 30
8. Anderson RE , Jakobsson JG : Entropy of EEG during anaesthetic induction: A comparative study with propofol or nitrous oxide as sole agent. Br J Anaesth 2004 ; 92 : 167 – 70
9. Voss L , Sleigh J : Monitoring consciousness: The cur-rent status of EEG-based depth of anaesthesia moni-tors. Best Pract Res Clin Anaesthesiol 2007 ; 21 : 313 – 25
10. Purdon PL , Sampson A , Pavone KJ , Brown EN : Clinical electroencephalography for anesthesiologists: Part I: Background and basic signatures. A nesthesiology 2015 ; 123 : 937 – 60
11. Foster BL , Liley DT : Nitrous oxide paradoxically modu-lates slow electroencephalogram oscillations: Implications for anesthesia monitoring. Anesth Analg 2011 ; 113 : 758 – 65
12. Foster BL , Liley DT : E ects of nitrous oxide sedation on resting electroencephalogram topography. Clin Neurophysiol 2013 ; 124 : 417 – 23
13. Pelentritou A , Kuhlmann L , Cormack J , Mcguigan S , Woods W , Muthukumaraswamy S , Liley D : Source-level cortical power changes for xenon and nitrous oxide – induced reductions in consciousness in healthy male volunteers. A nesthesiology 2020 ; 132 : 1017 – 33
14. Pelentritou A , Kuhlmann L , Cormack J , Woods W , Sleigh J , Liley D : Recording brain electromagnetic activity during the administration of the gaseous anes-thetic agents xenon and nitrous oxide in healthy vol-unteers. J Vis Exp 2018 ; 131 : 56881
15. Kuhlmann L , Liley DTJ : Assessing nitrous oxide e ect using electroencephalographically-based depth of
ALNV134N2_Text.indb 212ALNV134N2_Text.indb 212 29-Dec-20 19:43:5429-Dec-20 19:43:54
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:202–18 213
Low-dose Nitrous Oxide Electroencephalogram Metric
Vrijdag et al.
anesthesia measures cortical state and cortical input. J Clin Monit Comput 2018 ; 32 : 173 – 88
16. Kuhlmann L , Foster BL , Liley DT : Modulation of functional EEG networks by the NMDA antagonist nitrous oxide. PLoS One 2013 ; 8 : e56434
17. Bai Y , Xia X , Li X : A review of resting-state electro-encephalography analysis in disorders of consciousness. Front Neurol 2017 ; 8 : 471
18. Parameshwaran D , Subramaniyam NP , Thiagarajan TC : Waveform complexity: A new metric for EEG analysis. J Neurosci Methods 2019 ; 325 : 108313
19. Marwan N , Romano MC , Thiel M , Kurths J : Recurrence plots for the analysis of complex systems. Phys Rep 2007 ; 438 : 237 – 329
20. Shalbaf R , Behnam H , Sleigh JW , Steyn-Ross DA , Steyn-Ross ML : Frontal-temporal synchronization of EEG signals quanti ed by order patterns cross recur-rence analysis during propofol anesthesia. IEEE Trans Neural Syst Rehabil Eng 2015 ; 23 : 468 – 74
21. Biersner RJ : Selective performance e ects of nitrous oxide. Hum Factors 1972 ; 14 : 187 – 94
22. Biersner RJ , Hall DA , Neuman TS , Linaweaver PG : Learning rate equivalency of two narcotic gases. J Appl Psychol 1977 ; 62 : 747 – 50
23. Hamilton K , Lalibert é MF , Heslegrave R : Subjective and behavioral e ects associated with repeated expo-sure to narcosis. Aviat Space Environ Med 1992 ; 63 : 865 – 9
24. Fowler B , Granger S , Ackles KN , Holness DE , Wright GR : The e ects of inert gas narcosis on certain aspects of serial response time. Ergonomics 1983 ; 26 : 1125 – 38
25. Vrijdag XC , van Waart H , Sleigh JW , Mitchell SJ : Pupillometry is not sensitive to gas narcosis in divers breathing hyperbaric air or normobaric nitrous oxide. Diving Hyperb Med 2020 ; 50 : 115 – 20
26. Klem GH , L ü ders HO , Jasper HH , Elger C : The ten-twenty electrode system of the International Federation. Electroencephalogr Clin Neurophysiol 1999 ; 52 : 3 – 6
27. Zacny JP , Sparacino G , Ho mann P , Martin R , Lichtor JL : The subjective, behavioral and cognitive e ects of subanesthetic concentrations of iso urane and nitrous oxide in healthy volunteers. Psychopharmacology (Berl) 1994 ; 114 : 409 – 16
28. Tiplady B , Degia A , Dixon P : Assessment of driver impairment: Evaluation of a two-choice tester using ethanol. Transp Res Part F Tra c Psychol Behav 2005 ; 8 : 299 – 310
29. Hayman MAX : Two minute clinical test for measure-ment of intellectual impairment in psychiatric disor-ders. Arch Neurol Psychiatry 1942 ; 47 : 454 – 64
30. Oostenveld R , Fries P , Maris E , Scho elen JM : FieldTrip: Open source software for advanced analysis of MEG, EEG, and invasive electrophysiological data. Comput Intell Neurosci 2011 ; 2011 : 156869
31. Beim Graben P , Jimenez-Marin A , Diez I , Cortes JM , Desroches M , Rodrigues S : Metastable resting state brain dynamics. Front Comput Neurosci 2019 ; 13 : 62
32. Marwan N , Kurths J : Nonlinear analysis of bivariate data with cross recurrence plots. Phys Lett A 2002 ; 302 : 299 – 307
33. Dennis I , Evans JSBT : The speed – error trade-o problem in psychometric testing. Br J Psychol 1996 ; 87 : 105 – 29
34. Darracq M , Sleigh J , Banks MI , Sanders RD : Characterising the e ect of propofol on complexity and stability in the EEG power spectrum. Br J Anaesth 2018 ; 121 : 1368 – 9
35. Shalbaf R , Behnam H , Sleigh J : Order patterns recur-rence analysis of electroencephalogram during sevo- urane anesthesia. Biomed Eng Appl Basis Commun 2015 ; 27 : 1550049
36. Sleigh J , Warnaby C , Tracey I : General anaesthesia as fragmentation of selfhood: Insights from electroen-cephalography and neuroimaging. Br J Anaesth 2018 ; 121 : 233 – 40
37. Mashour GA , Roelfsema P , Changeux JP , Dehaene S : Conscious processing and the global neuronal work-space hypothesis. Neuron 2020 ; 105 : 776 – 98
38. Koch C , Massimini M , Boly M , Tononi G : Neural cor-relates of consciousness: Progress and problems. Nat Rev Neurosci 2016 ; 17 : 307 – 21
39. Acharya UR , Hagiwara Y , Deshpande SN , Suren S , Koh JEW , Oh SL , Arunkumar N , Ciaccio EJ , Lim CM : Characterization of focal EEG signals: A review. Futur Gener Comput Syst 2019 ; 91 : 290 – 9
40. Tripathy RK , Rajendra Acharya U : Use of features from RR-time series and EEG signals for automated classi cation of sleep stages in deep neural network framework. Biocybern Biomed Eng 2018 ; 38 : 890 – 902
41. Ma Y , Shi W , Peng CK , Yang AC : Nonlinear dynam-ical analysis of sleep electroencephalography using fractal and entropy approaches. Sleep Med Rev 2018 ; 37 : 85 – 93
42. Liu Q , Ma L , Fan SZ , Abbod MF , Shieh JS : Sample entropy analysis for the estimating depth of anaesthe-sia through human EEG signal at di erent levels of unconsciousness during surgeries. PeerJ 2018 ; 6 : e4817
43. Nicolaou N , Georgiou J : The study of EEG dynamics during anesthesia with cross-recurrence rate. Cureus 2014 ; 6 : e195
44. Le ó n-Dom í nguez U , Le ó n-Carri ó n J : Prefrontal neu-ral dynamics in consciousness. Neuropsychologia 2019 ; 131 : 25 – 41
45. Lee U , Mashour GA : Role of network science in the study of anesthetic state transitions. A nesthesiology 2018 ; 129 : 1029 – 44
46. Zacharias N , Musso F , M ü ller F , Lammers F , Saleh A , London M , de Boer P , Winterer G : Ketamine e ects on default mode network activity and vigilance: A
ALNV134N2_Text.indb 213ALNV134N2_Text.indb 213 29-Dec-20 19:43:5529-Dec-20 19:43:55
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
214 Anesthesiology 2021; 134:202–18
PERIOPERATIVE MEDICINE
Vrijdag et al.
randomized, placebo-controlled crossover simulta-neous fMRI/EEG study. Hum Brain Mapp 2020 ; 41 : 107 – 19
47. Lee JM , Kim PJ , Kim HG , Hyun HK , Kim YJ , Kim JW , Shin TJ : Analysis of brain connectivity during nitrous oxide sedation using graph theory. Sci Rep 2020 ; 10 : 1 – 11
48. Raichle ME : The brain ’ s default mode network. Annu Rev Neurosci 2015 ; 38 : 433 – 47
49. Smith V , Mitchell DJ , Duncan J : Role of the default mode network in cognitive transitions. Cereb Cortex 2018 ; 28 : 3685 – 96
50. Murphy C , Je eries E , Rueschemeyer SA , Sormaz M , Wang HT , Margulies DS , Smallwood J : Distant from input: Evidence of regions within the default mode network supporting perceptually-decoupled and conceptually-guided cognition. Neuroimage 2018 ; 171 : 393 – 401
Appendix 1. EEG Data Cleaning Script Based on FieldTrip Toolbox close all clear clc
epochtype= ‘ closed end ’ ;% ’ math ’ ;% ‘ open end ’ ;
[datasetselection,datapath] = data_selector;
for i=1:length(datasetselection) %all selected data folders lepath=[datapath datasetselectioni lesep]; lelist=dir([ lepath ‘ * .bdf ’ ]);% nd all.bdf les
%creating folder for cleaned les to be stored new lepath=[ lepath lesep ‘ cleaned ’ lesep]; mkdir(new lepath);
for j=2:length( lelist.name) % all BDF les in the folder
%de ne epoch trial data cfg = [ ]; cfg.dataset = [ lepath lelist(j).name]; cfg.trialfun = ‘ EEG_trialfunc_narcosis ’ ; % my function
to read epochtimes from excel le cfg.trialdef.epochtype = epochtype; cfg.trialdef.pretrial = 1; % add sec of data before trial cfg.trialdef.posttrial = 1; % add sec of data after trial cfg = ft_de netrial(cfg);
%read dataset based on trial de nition cfg.channel = 1:34; cfg.reref = ‘ yes ’ ; cfg.refchannel = ‘ EEG ’ ; % average of all EEG channels cfg.demean = ‘ yes ’ ; cfg.detrend = ‘ yes ’ ; data = ft_preprocessing(cfg);
% downsample data cfg = [ ]; cfg.resamplefs = 256; %Hz data = ft_resampledata(cfg, data);
% removing line and low freq noise cfg = [ ]; cfg.channel = ‘ all ’ ; cfg.bs lter = ‘ yes ’ ; % band-stop method cfg.bsfreq = [49 51];
cfg.hp lter = ‘ yes ’ ; cfg.hpfreq = 1; % removing all activity below 1 Hz data = ft_preprocessing(cfg,data);
% clean high harmonic of line noise cfg=[ ]; cfg.channel = channels; cfg.bs lter = ‘ yes ’ ; % band-stop method cfg.bsfreq = [99 101]; cfg.demean = ‘ yes ’ ; cfg.detrend = ‘ yes ’ ; data = ft_preprocessing(cfg,cleandata);
% calculate ICA components to project out eye and cardiac artefacts
cfg = [ ]; cfg.method = ‘ runica ’ ; comp = ft_componentanalysis(cfg, data);
cfg = [ ]; cfg.layout = ‘ biosemi32.lay ’ ; cfg.viewmode = ‘ component ’ ; cfg.ylim = [-0.0002 0.0002]; cfg.zlim = ‘ maxmin ’ ; cfg.compscale = ‘ local ’ ; % scale each component
separately cfg.blocksize = 62; cfg.artifactalpha = 0.8; cfg.position = [0 0 3000 2000]; ft_databrowser(cfg, comp);
% calculating properties to suggest, select and reject bad components
EOG_chans = [33 34]; [bad_comps,reasons] = ICAbadICdetection(data,comp,
EOG_chans); for k=1:length(bad_comps) ft_info( ‘ Suggested bad component: %d because of
%s ’ ,bad_comps(k),reasonsk) end ic.artifact = input( ‘ ICs to reject (i.e. [8] or 0 for all
suggested bad components): ‘ );
if ic.artifact==0 ic.artifact=bad_comps; end
ALNV134N2_Text.indb 214ALNV134N2_Text.indb 214 29-Dec-20 19:43:5529-Dec-20 19:43:55
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:202–18 215
Low-dose Nitrous Oxide Electroencephalogram Metric
Vrijdag et al.
cfg = [ ]; cfg.component = ic.artifact; data = ft_rejectcomponent(cfg, comp, data);
% remove padding of 1 sec before and after and correct time axes
cfg = [ ]; cfg.toilim = [1 data.time1,1(end)-1]; data = ft_rede netrial(cfg, data); cfg = [ ]; cfg.o set = -data.fsample; data = ft_rede netrial(cfg, data);
%cut in 2 second “ trials ” cfg = [ ]; cfg.length = 2; cfg.overlap = 0; data_segmented = ft_rede netrial(cfg, data);
% detect artefacts cfg=[ ]; cfg.artfctdef.eog.channel = ‘ EXG1 ’ , ‘ EXG2 ’ ; cfg.artfctdef.eog.cuto = 7; cfg.artfctdef.muscle.channel = ‘ EEG ’ ; cfg.artfctdef.muscle.bpfreq = [105 120]; cfg.artfctdef.muscle.cuto = 10; [cfg, ~] = ft_artifact_eog(cfg, data_segmented); [cfg, ~] = ft_artifact_muscle(cfg, data_segmented);
%visually inspect data and de ned artefacts cfg.channel = ‘ all ’ ; cfg.viewmode = ‘ vertical ’ ; cfg.ylim = [-40 40]; cfg.position = [0 0 3000 2000]; cfg.blocksize = 10; % time window to browse cfg.artifactalpha = 0.8; % this make the colors less
transparent and thus more vibrant cfg = ft_databrowser(cfg, data);
%rejecting trials with artefacts cfg.artftdef.reject = ‘ complete ’ ; cleandata=ft_rejectartifact(cfg,data_segmented);
%store cleaned data [~,new lename,~]= leparts( lelist(j).name); new lename=[ ‘ CLEAN ’ new lename ‘ ‘ epochtype
‘ .mat ’ ]; save(strcat(newfilepath,newfilename), ’ cleanda-
ta ’ , ’ -v7.3 ’ ) end
end
Supporting Functions
function [bad_comps,reasons] = ICAbadICdetection(data,comp, EOG_chans) % ICA bad components detection function % detection scripts are from the FASTER toolbox % utilising functions from the EEGlab toolbox
list_properties = component_properties(data,comp,EOG_chans); rejection_options.measure=ones(1,size(list_properties,2)); %use all properties rejection_options.z=3 * ones(1,size(list_properties,2));% z-value of 3 for each property
[lengths,all_l] = min_z(list_properties,rejection_options); bad_comps= nd(lengths); properties= ‘ High freq noise ’ ‘ Kurtosis ’ ‘ Hurst ’ ‘ Eyeblink ’ ; for i=1:length(bad_comps) reasonsi=cell2str(properties(all_l(bad_comps(i),:))); end end
function string1 = cell2str(cellarray) string1=[ ]; for i=1:length(cellarray)
string1=[string1 cellarrayi]; if length(cellarray) > i
string1=[string1 ‘ & ‘ ]; end
end end function list_properties = component_properties (data,comp, blink_chans) list_properties = zeros(size(comp.trial,1),4); %This 4 corre-sponds to number of properties.
for u=1:size(comp.trial1,1) measure = 1; % TEMPORAL PROPERTIES
% Median gradient value, for high frequency artefacts list_properties(u,measure) = median(di (comp.trial1(u,:))); measure = measure + 1;
% SPATIAL PROPERTIES
% Kurtosis of spatial map (if v peaky, i.e. one or two points high
% and everywhere else low, then it ’ s probably noise on a single
% channel) list_properties(u,measure) = kurt(comp.topo(:,u)); measure = measure + 1;
% OTHER PROPERTIES
% Hurst exponent - detects nonphysiological signals list_properties(u,measure) = hurst_exponent(comp.trial1
(u,:)); measure = measure + 1;
% Eyeblink correlations if (exist( ‘ blink_chans ’ , ’ var ’ ) & & ~isempty(blink_chans))
for v = 1:length(blink_chans) if ~(max(data.trial1(blink_chans(v),:))==0 & &
min(data.trial1(blink_chans(v),:))==0)
ALNV134N2_Text.indb 215ALNV134N2_Text.indb 215 29-Dec-20 19:43:5529-Dec-20 19:43:55
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
216 Anesthesiology 2021; 134:202–18
PERIOPERATIVE MEDICINE
Vrijdag et al.
f = corrcoef(comp.trial1(u,:),data.trial1(blink_chans(v),:));
x(v) = abs(f(1,2)); else
x(v) = v; end
end list_properties(u,measure) = max(x); measure = measure + 1; end
end
for u = 1:size(list_properties,2) list_properties(isnan(list_properties(:,u)),u)=nan-
mean(list_properties(:,u)); list_properties(:,u) = list_properties(:,u)
- median(list_properties(:,u)); end end
function [lengths,all_l] = min_z(list_properties,rejection_options) rejection_options.measure=logical(rejection_options.measure); zs=list_properties-repmat(mean(list_properties,1),size(list_properties,1),1); zs=zs./repmat(std(zs,[],1),size(list_properties,1),1); zs(isnan(zs))=0; all_l = abs(zs) > repmat(rejection_options.z,size(list_prop-erties,1),1); lengths = any(all_l(:,rejection_options.measure),2); end
Appendix 2. Complexity Script close all; clear; clc
%settings Ts=0.25; %duration of sample in sec RQAselect=3; % entropy Rnpercentile=50; % percentile for threshold channels= 1:32;
%select dataset %for model gure select participant 1 [datasetselection,datapath] = data_selector; epochtype= ‘ open end ’ ; % ‘ closed end ’ ;% ‘ math ’ ; % ‘ open end ’ ; % exposures= ‘ baseline ’ ‘ 20% ’ ‘ 30% ’ ‘ 40% ’ ‘ nal ’ ;
for k=1:length(datasetselection) %all selected data folders lepath=[datapath datasetselectionk lesep ‘ cleaned ’
lesep];
RnThreshold=[ ]; for l=1:length(exposures) % loop over all exposures
% load data le
lename=[ ‘ CLEAN ’ datasetselectionk ‘ ‘ expo-suresl ‘ ‘ epochtype ‘ .mat ’ ];
load([ lepath lename])
% split previously de ned trials (2 second) into smaller samples
a=1; samples=[ ]; N=Ts * data.fsample; for i=1:length(data.trial)
for j=1:( oor(length(data.trial1)/N)) samples(a,:,:)=data.triali(:,1 + (j-1) * N:N * j); a=a + 1;
end end
%DIMORD samples = samples * channels * time
% calculate the Pierson correlation between the sam-ples for all channels
Rn=[ ]; for i=1:size(samples,2)
Rn(i,:,:)=corr(squeeze(samples(:,i,:)) ’ ); end
% convert the correlation values Rn=abs(Rn);
% set threshold at baseline exposure for all exposures for each de ned percentile
if l==1 RnT=Rn; RnT(RnT==0)=NaN; RnThreshold=prctile(reshape(RnT,1,[ ]),Rnperc
entile); end
% Convert to logical values based on threshold RnLogic = (Rn > RnThreshold); %calculate the de ned RQA metrics for each
channel for i=1:size(RnLogic,1)
RQresults(k,l,i) = Recu_RQA(squeeze(RnLogic (i,:,:)),1,RQAselect);
end
% DIMORD RQresults participants, exposures, channels
% calculate DMN complexity: median of the region of % interest which are the electrodes that have entropy
> 1 at baseline if l==1
DMN= nd(RQresults(k,l,:) > 1); end DMNcomplexity(k,l)=median(RQresults(k,l,DMN)); % DIMORD participants, exposures
end end
Supporting Functions function [RQA] = Recu_RQA(RP,I,metrics)
% Recurrence quanti cation analysis of recurrence plots
ALNV134N2_Text.indb 216ALNV134N2_Text.indb 216 29-Dec-20 19:43:5529-Dec-20 19:43:55
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:202–18 217
Low-dose Nitrous Oxide Electroencephalogram Metric
Vrijdag et al.
% RP: the Recurrence Plot % I: the indication marks (I=0 RP is the symmetry matrix % I=1 RP is the asymmetry matrix) %outputs in RQA % 1 RR: Recurrence rate RR, The percentage of recur-rence points in an RP % Corresponds to the correlation sum; % 2 DET: Determinism DET, The percentage of recurrence points which form % diagonal lines % 3 ENTR: Entropy ENTR, The Shannon entropy of the probability distribution of the diagonal % line lengths p(l) % 4 L: Averaged diagonal line length L, The average length of the diagonal lines % 5 LAM: Laminnarity, The percentage of recurrence points which form vertical lines % 6 TT: Trapping time, The average length of the vertical lines % 7 Clust:global clustering coe cient, Network analysis % 8 Trans:Transitivity, Network analysis
% If you need these codes that implement critical functions with (fast) C code, please visit my website: % http://www.escience.cn/people/gxouyang/Tools.html
% revise time: May 5 2014, Ouyang,Gaoxiang % Email: [email protected]
%% minimal length of diagonal and vertical line structures Lmin=2; %diagonal Vmin=2; %vertical if nargin < 2
I=0; end
%% calculate diagonals N1=size(RP,1);
Yout=zeros(1,N1);
for k=2:N1 On=1; while On < =N1 + 1-k
if RP(On,k + On-1)==1 A=1;o =0; while o ==0 & On~=N1 + 1-k
if RP(On + 1,k + On)==1 A=A + 1;On=On + 1;
else o =1;
end end Yout(A)=Yout(A) + 1;
end On=On + 1;
end end
if I==0 S=2 * Yout;
end if I==1
RP=RP ’ ; for k=2:N1
On=1; while On < =N1 + 1-k
if RP(On,k + On-1)==1 A=1;o =0; while o ==0 & On~=N1 + 1-k
if RP(On + 1,k + On)==1 A=A + 1;On=On + 1;
else o =1;
end end Yout(A)=Yout(A) + 1;
end On=On + 1;
end end S=Yout;
end
%% calculate the recurrence rate (RR) SR=0; for i=1:N1
SR=SR + i * S(i); end RR=SR/(N1 * (N1-1));
%% calculate the determinism (%DET) if SR==0
DET=0; else
DET=(SR-sum(S(1:Lmin-1)))/SR; end
%% calculate the ENTR = entropy (ENTR) pp=S/sum(S); entropy=0; F= nd(S(Lmin:end)); l=length(F); if l==0
ENTR=0; else
F=F + Lmin-1; ENTR=-sum(pp(F). * log(pp(F)));
end
%% calculate Averaged diagonal line length (L) L = ( S R - s u m ( [ 1 : L m i n - 1 ] . * S ( 1 : L m i n - 1 ) ) ) /sum(S(Lmin:end));
%% calculate Laminarity (LAM) and Trapping time (TT) (Marwan et al. 2002) [~, d, ~]=tt(RP);
ALNV134N2_Text.indb 217ALNV134N2_Text.indb 217 29-Dec-20 19:43:5529-Dec-20 19:43:55
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

218 Anesthesiology 2021; 134:202–18
PERIOPERATIVE MEDICINE
Vrijdag et al.
d(d < Vmin)=[]; if sum(RP(:)) > 0
LAM=sum(d)/sum(sum(RP)); else
LAM=NaN; end TT=mean(d);
%% network measures % global clustering coe cient (Marwan et al., 2009) kv = sum(RP,1); % degree of nodes Clust = nanmean(diag(double(RP) * double(RP) * dou-ble(RP)) ’ ./ (kv. * (kv-1))); % transitivity
denom = sum(sum(double(RP) * double(RP))); Trans = trace(double(RP) * double(RP) * double(RP))/denom;
aa=1; if ismember(1,metrics);RQA(aa)=RR;aa=aa + 1;end if ismember(2,metrics);RQA(aa)=DET;aa=aa + 1;end if ismember(3,metrics);RQA(aa)=ENTR;aa=aa + 1;end if ismember(4,metrics);RQA(aa)=L;aa=aa + 1;end if ismember(5,metrics);RQA(aa)=LAM;aa=aa + 1;end if ismember(6,metrics);RQA(aa)=TT;aa=aa + 1;end if ismember(7,metrics);RQA(aa)=Clust;aa=aa + 1;end if ismember(8,metrics);RQA(aa)=Trans;end
ANESTHESIOLOGY REFLECTIONS FROM THE WOOD LIBRARY-MUSEUM
Life from Death: The Tragedy and Heroism of Dr. Paluel J. Flagg
As a young physician in New York City, Paluel J. Flagg, M.D. (1886 to 1970, right ), lost his daughter to neo-natal asphyxia in 1912. His wife also died that year. Grief-stricken, Dr. Flagg found solace in easing human su ering, and began treating leprosy patients in Haiti. In 1912, he also committed his life to the prevention and treatment of asphyxia. What better profession to accomplish this than anesthesiology? In his landmark text-book The Art of Anesthesia (1916), Flagg presaged the modern intensive care unit by calling anesthesiologists pneumatologists — respiratory experts who should extend their practice beyond the operating room. Naturally, Flagg took to re ning devices for airway management. He introduced his two-piece metal endotracheal tube ( left ) in 1928. Spiral wires made the outer catheter exible, and a rigid inner stylet prevented kinking during insertion. Later, Flagg would develop the rst laryngoscope with batteries in the handle. As founder of the National Resuscitation Society and the Society for the Prevention of Asphyxial Death, the heroic physi-cian taught resuscitation maneuvers to countless doctors and paramedics. A good friend of aviator Charles Lindbergh, Flagg, when his soul ew to the heavens, left behind a legacy of patient safety and abundant liv-ing progeny — 8 sons, 4 daughters, 56 grandchildren, and 3 great-grandchildren. (Copyright © the American Society of Anesthesiologists ’ Wood Library-Museum of Anesthesiology, Schaumburg, Illinois.)
Jane S. Moon, M.D., University of California, Los Angeles, and Melissa L. Coleman, M.D., Penn State College of Medicine, Hershey, Pennsylvania .
RE-FLEC-TION
ALNV134N2_Text.indb 218ALNV134N2_Text.indb 218 29-Dec-20 19:43:5529-Dec-20 19:43:55
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
PERIOPERATIVE MEDICINE
ANESTHESIOLOGY, V 134 • NO 2 FEBRUARY 2021 219
ABSTRACT Background: The general anesthetic propofol induces frontal alpha rhythm in the cerebral cortex at a dose suffi cient to induce loss of consciousness. The authors hypothesized that propofol-induced facilitation of unitary inhibitory postsynaptic currents would result in fi ring synchrony among postsynaptic pyramidal neurons that receive inhibition from the same presynaptic inhibitory fast-spiking neurons.
Methods: Multiple whole cell patch clamp recordings were performed from one fast-spiking neuron and two or three pyramidal neurons with at least two inhibitory connections in rat insular cortical slices. The authors examined how inhibitory inputs from a presynaptic fast-spiking neuron modulate the timing of spontaneous repetitive spike fi ring among pyramidal neurons before and during 10 μ M propofol application.
Results: Responding to activation of a fast-spiking neuron with 150-ms intervals, pyramidal cell pairs that received common inhibitory inputs from the presynaptic fast-spiking neuron showed propofol-dependent decreases in average distance from the line of identity, which evaluates the coeffi cient of variation in spike timing among pyramidal neurons: average distance from the line of identity just after the fi rst activation of fast-spiking neuron was 29.2 ± 24.1 (mean ± SD, absolute value) in control and 19.7 ± 19.2 during propofol application ( P < 0.001). Propofol did not change average distance from the line of identity without activating fast-spiking neurons and in pyramidal neuron pairs without common inhibitory inputs from presynaptic fast-spiking neurons. The synchronization index, which refl ects the degree of spike synchronization among pyramidal neurons, was increased by propofol from 1.4 ± 0.5 to 2.3 ± 1.5 (absolute value, P = 0.004) and from 1.5 ± 0.5 to 2.2 ± 1.0 ( P = 0.030) when a presynaptic fast-spiking neuron was activated at 6.7 and 10 Hz, respec-tively, but not at 1, 4, and 13.3 Hz.
Conclusions: These results suggest that propofol facilitates pyramidal neu-ron fi ring synchrony by enhancing inhibitory inputs from fast-spiking neurons. This synchrony of pyramidal neurons may contribute to the alpha rhythm associated with propofol-induced loss of consciousness.
(ANESTHESIOLOGY 2021 ; 134 : 219 – 33 )
Fast-spiking Interneurons Contribute to Propofol-induced Facilitation of Firing Synchrony in Pyramidal Neurons of the Rat Insular Cortex Yuko Koyanagi , D.D.S., Ph.D., Yoshiyuki Oi , M.D., Ph.D. , Masayuki Kobayashi , D.D.S., Ph.D.
ANESTHESIOLOGY 2021 ; 134 : 219 – 33
This article is featured in “This Month in Anesthesiology,” page 1A. This work was presented at the 9th International Symposium on Memory and Awareness in Anesthesia in Tokyo, Japan, July 20 to 23, 2014, and Neuroscience 2015 in Chicago, Illinois, October 17 to 21, 2015. This article has a visual abstract available in the online version.
Submitted for publication May 11, 2020. Accepted for publication November 16, 2020. Published online fi rst on December 17, 2020. From the Departments of Anesthesiology (Y.K., Y.O.) and Pharmacology (M.K.), Nihon University School of Dentistry, Tokyo, Japan; the Divisions of Immunology and Pathobiology (Y.K., Y.O.) and Oral and Craniomaxillofacial Research (M.K.), Dental Research Center, Nihon University School of Dentistry, Tokyo, Japan; and the Molecular Dynamics Imaging Unit, RIKEN Center for Life Science Technologies, Kobe, Japan (M.K.).
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved. Anesthesiology 2021 ; 134 : 219 – 33 . DOI: 10.1097/ALN.0000000000003653
EDITOR ’ S PERSPECTIVE
What We Already Know about This Topic
• Propofol-induced loss of consciousness correlates with the appearance of a synchronized alpha rhythm on the frontal cortical electroencephalogram
• Well-coordinated thalamocortical alpha oscillation induced by propofol exposure is the prevailing mechanistic view to explain this phenomenon
• The role of local cortical circuits in propofol-induced synchronized neuronal activity is incompletely understood
What This Article Tells Us That Is New
• Multiple whole cell patch clamp recordings in rat cortical slices reveal that propofol facilitates firing synchrony among pyramidal neurons
• Propofol-induced activation of presynaptic fast-spiking interneu-rons was necessary to achieve firing synchrony of postsynaptic pyramidal neurons
• These observations suggest that propofol facilitates pyramidal neu-ron firing synchrony in the cerebral cortex by enhancing inhibitory inputs from fast-spiking interneurons
The anesthetic agent propofol elicits frontal alpha rhythm in an electroencephalogram (EEG). 1 – 3 The
propofol-induced alpha rhythm is spatially distinct from the
classic occipital alpha rhythm that appears when subjects have their eyes closed and is well-correlated with propo-fol-induced loss of consciousness. 1 , 4 Several studies based on EEGs have demonstrated that both the cortex and the thalamus play a critical role in the propofol-induced alpha rhythm. 5 , 6 Ching et al. 1 developed a computational thalam-ocortical model that demonstrates propofol-induced intra-cortical alpha synchrony. Cortical alpha activity recruits the thalamus into the same alpha frequency, which enhances cortical alpha oscillation through the thalamocortical loop. However, it is controversial whether the cortical local
ALNV134N2_Text.indb 219ALNV134N2_Text.indb 219 29-Dec-20 19:43:5629-Dec-20 19:43:56
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

220 Anesthesiology 2021; 134:219–33
PERIOPERATIVE MEDICINE
Koyanagi et al.
circuits themselves have an intrinsic mechanism that leads to propofol-induced synchronized activity.
Propofol modulates various ionic channels, including γ -aminobutyric acid (GABA) type A (GABA
A ) receptors,
voltage-gated Na + channels, 7 , 8 and hyperpolarization-acti-vated cyclic nucleotide-gated cation channels. 9 , 10 Among these channels, propofol primarily potentiates GABA-mediated (GABAergic) inhibitory synaptic transmission in the cerebral cortex. 11 , 12 GABAergic neurons in the cortical local circuits are classi ed into several subtypes according to their electrophysiologic, morphological, and immunohisto-chemical features. 13 Fast-spiking GABAergic neurons, most of which are parvalbumin-immunopositive, are a major cortical GABAergic neuron subtype. 14 Fast-spiking neu-rons preferentially target somata, proximal dendrites, and initial segments of pyramidal neurons and induce a large amplitude of inhibitory postsynaptic currents to postsyn-aptic neurons. 15 Therefore, fast-spiking neurons are consid-ered the principal inhibitory neurons in the cerebral cortex. Our previous study demonstrated that propofol enhances unitary inhibitory postsynaptic currents, most preferentially in fast-spiking neuron – to – pyramidal neuron connections. 16
In this study, we propose a hypothesis that propo-fol-induced facilitation of unitary inhibitory postsynaptic currents results in ring synchrony among postsynaptic pyramidal neurons that receive inhibitory input from the same presynaptic fast-spiking neuron. To test this hypothe-sis, we obtained whole cell patch clamp recordings simul-taneously from one fast-spiking neuron and two or three pyramidal neurons in rat insular cortical slice preparations and examined the e ects of presynaptic fast-spiking neuron action currents on the modulation of spike timing in post-synaptic pyramidal neurons.
Materials and Methods All experiments were performed in accordance with the National Institutes of Health (Bethesda, Maryland) Guide for the Care and Use of Laboratory Animals and were approved by the Institutional Animal Care and Use Committee at Nihon University (Tokyo, Japan). All e orts were made to minimize the number of animals used and the su ering of these animals in experiments.
Slice Preparations
The techniques for preparing and maintaining rat cor-tical slices in vitro were similar to those described previ-ously. 12 , 16 , 17 Brie y, vesicular GABA transporter – Venus line A transgenic rats 18 of either sex, ranging in age from 3 to 4 weeks, were deeply anesthetized with sodium pentobar-bital (100 mg/kg, intraperitoneal) and decapitated. Tissue blocks including the insular cortex were rapidly removed and stored for 3 min in ice-cold modi ed arti cial cerebro-spinal uid (230 mM sucrose, 2.5 mM KCl, 10 mM MgSO
4 ,
1.25 mM NaH 2 PO
4 , 26 mM NaHCO
3 , 0.5 mM CaCl
2 , and
10 mM D-glucose). Coronal slices were cut with a thickness of 350 μ m using a microslicer (Linearslicer Pro 7, Dosaka EM, Japan). Slices were incubated at 32 ° C for 40 min in a submersion-type holding chamber that contained 50% modi ed arti cial cerebrospinal uid and 50% normal arti- cial cerebrospinal uid (pH 7.35 to 7.40). Normal arti- cial cerebrospinal uid contained 126 mM NaCl, 3 mM KCl, 2 mM MgSO
4 , 1.25 mM NaH
2 PO
4 , 26 mM NaHCO
3 ,
2 mM CaCl 2 , and 10 mM D-glucose. Modi ed and normal
arti cial cerebrospinal uid were continuously aerated with a mixture of 95% O
2 /5% CO
2 . The slices were then placed
in normal arti cial cerebrospinal uid at 32 ° C for 1 h and thereafter maintained at room temperature until they were used for recording.
Cell Identifi cation and Paired Whole Cell Patch Clamp Recording
The slices were transferred to a recording chamber that was perfused continuously with normal arti cial cerebrospi-nal uid at a rate of 2.0 ml/min. Multiple whole cell patch clamp recordings were obtained from a Venus-positive uo-rescent interneuron and Venus-negative pyramidal neurons identi ed in layer V by a uorescence microscope equipped with Nomarski optics ( × 40, Olympus BX51W1, Japan) and an infrared-sensitive video camera (C3077-78, Hamamatsu Photonics, Japan). The distance between recorded neurons was less than 200 μ m. Electrical signals were recorded by ampli ers (Multiclamp 700B, Molecular Devices, USA), digitized (Digidata 1440A, Molecular Devices), observed online, and stored on a computer hard disk using Clampex (pClamp 10, Molecular Devices).
The composition of the pipette solution for recordings was 135 mM potassium gluconate, 5 mM KCl, 20 mM bio-cytin, 0.5 mM CaCl
2 , 2 mM MgCl
2 , 5 mM EGTA, 5 mM
HEPES, and 5 mM magnesium adenosine triphosphate. The pipette solution had a pH of 7.3 and an osmolarity of 300 mOsm. The liquid junction potentials for current clamp and voltage clamp recordings were − 9 mV. In the current study, the voltage was not corrected. Thin-wall borosilicate patch electrodes (2 to 5 M Ω ) were pulled on a Flaming – Brown micropipette puller (P-97, Sutter Instruments, USA).
Recordings were obtained at 30 to 31 ° C to avoid the rundown of GABAergic inhibitory postsynaptic currents. The seal resistance was more than 10 G Ω , and only data obtained from electrodes with access resistance of 6 to 20 M Ω and less than 20% change during recordings were included in this study. Before the unitary inhibitory post-synaptic current recordings, the voltage responses of presyn-aptic and postsynaptic neurons were recorded by injecting long hyperpolarizing and depolarizing current pulses (300 to 1,000 ms) to examine basic electrophysiologic proper-ties, including the input resistance, single-spike kinetics, voltage – current relationship, and repetitive ring patterns. Among Venus-positive uorescent interneurons, fast-spik-ing neurons were identi ed by the following characteristics:
ALNV134N2_Text.indb 220ALNV134N2_Text.indb 220 29-Dec-20 19:43:5629-Dec-20 19:43:56
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:219–33 221
Propofol Facilitates Spike Synchrony
Koyanagi et al.
a large afterhyperpolarization amplitude with very rapid repolarization, a short spike duration, and repetitive ring at an extremely high frequency (over 100 Hz) without adap-tation ( g. 1 ). 19 All neurons were recorded under the volt-age clamp condition (holding potential = − 45 mV) during unitary inhibitory postsynaptic current recording. Short depolarizing voltage step pulses (1 ms, 80 mV) were applied to the presynaptic fast-spiking neurons to induce action currents ( g. 2 ). Postsynaptic pyramidal neurons were depolarized by direct current injection. Then 2,6-diisopro-pylphenol (propofol; Sigma-Aldrich, USA) was dissolved in dimethyl sulfoxide at a concentration of 10 mM and diluted to 10 μ M in the perfusate. In a part of the experiment, the e ect of propofol was tested at 1 μ M. The membrane cur-rents and potentials were low pass – ltered at 5 to 10 kHz and digitized at 20 kHz.
Clamp t (pClamp 10, Molecular Devices) was used for analyses of electrophysiologic data. We de ned the period between 150 ms before the rst presynaptic action current up to the rst presynaptic action current (0 ms) as epoch 0 ( g. 3 ). Similarly, the subsequent periods (150 ms each) were de ned as epochs 1 to 7. To quantify the synchrony between two postsynaptic pyramidal neurons, the delay from the onset of the rst action current in presynaptic fast-spiking neuron to the action potentials in postsynap-tic pyramidal neurons was measured in each epoch in each trace ( g. 3C ). The delay obtained from one of the postsyn-aptic pyramidal neurons was plotted against that of another postsynaptic pyramidal neuron ( g. 3D ), and the distance from the line of identity was measured ( g. 3F ). In each neuron, 10 traces were used for the measurement of line of identity, and each line of identity was obtained from each trace.
Synchronization Index
The synchronization index was calculated from the cross-correlogram obtained from 10 subsequent trials. The period for the analysis was set 50 ms before and after the rst fast-spiking neuron spike. The synchronization index was obtained by dividing the number of spikes that occurred within the period of − 25 to 25 ms by those within the peri-ods of − 50 ms to − 25 ms and 25 to 50 ms. The synchroni-zation index data in epochs 0, 5, 6, and 7 and in epochs 1 to 4 were summed as synchronization index in the period without and with presynaptic fast-spiking neuron stim-uli, respectively. Pairs of pyramidal neurons were catego-rized into two classes: (1) connected pyramidal neurons, which received common inhibitory inputs from presynap-tic fast-spiking neuron ( e.g. , g. 3A ); and (2) unconnected pyramidal neurons, which did not receive common pre-synaptic fast-spiking neuron inputs ( e.g. , g. 4A ). Therefore, the synchronization index was obtained from four cate-gories: (1) connected pyramidal neurons without presyn-aptic fast-spiking neuron stimuli, (2) connected pyramidal neurons with presynaptic fast-spiking neuron stimuli, (3)
unconnected pyramidal neurons without presynaptic fast-spiking neuron stimuli, and (4) unconnected pyramidal neurons with presynaptic fast-spiking neuron stimuli.
Statistical Analysis
The data are mean ± SD. The sample size was based on the available data. Comparisons of the average distance from the line of identity between the control and propofol applica-tion conditions were conducted using a two-tailed unpaired t test. The synchronization index between the control and propofol application conditions was compared using a two-tailed paired t test. The normality of the data was tested by the Shapiro – Wilk test. No multiple comparisons were per-formed in this study. No outliers were excluded from anal-yses. Blinding was not used in this study. Statistical analyses were performed using SPSS (version 12.0, IBM, USA) and Prism (version 8.3.0, GraphPad Software, USA), and values of P < 0.05 were de ned as statistically signi cant. No sta-tistical power calculation was conducted before the study.
Results Among several subtypes of GABAergic interneurons, fast-spiking neurons send the most potent inhibitory inputs to pyramidal neurons, 20 and our previous study demon-strated that fast-spiking neuron – to – pyramidal neuron connections are the most sensitive to propofol-induced facilitation of unitary inhibitory postsynaptic currents. 16
Therefore, in this study, triple or quadruple whole cell patch clamp recordings were performed from a fast-spiking neuron, which was Venus-positive and showed a short spike duration with a large afterhyperpolarization and a high frequency of repetitive spike ring without spike adapta-tion, and pyramidal neurons, which were Venus-negative and showed spike adaptation during repetitive spike ring ( g. 1 ). We focused on the e ects of propofol-induced facil-itation of GABAergic synaptic transmission, particularly mediated by fast-spiking neurons, on spike synchronization between pyramidal neurons. The connection rate between a fast-spiking neuron and a pyramidal neuron was approxi-mately 50%, which was almost comparable to what we pre-viously reported. 16 Therefore, in the case of triple whole cell patch clamp recording from a fast-spiking neuron and two pyramidal neurons, the rate at which both pyramidal neu-rons received fast-spiking neuron inputs was approximately one quarter. In contrast, few pyramidal neuron – pyramidal neuron connections were observed in the current study.
Propofol Facilitates Spike Synchronization of Pyramidal Neurons
Figure 2 shows a typical example of propofol-induced spike synchrony of pyramidal neurons. Triple whole cell patch clamp recordings were performed from one Venus-positive fast-spiking neuron and two Venus-negative pyramidal neu-rons (pyramidal neuron 1 and pyramidal neuron 2; g. 2A ).
ALNV134N2_Text.indb 221ALNV134N2_Text.indb 221 29-Dec-20 19:43:5629-Dec-20 19:43:56
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
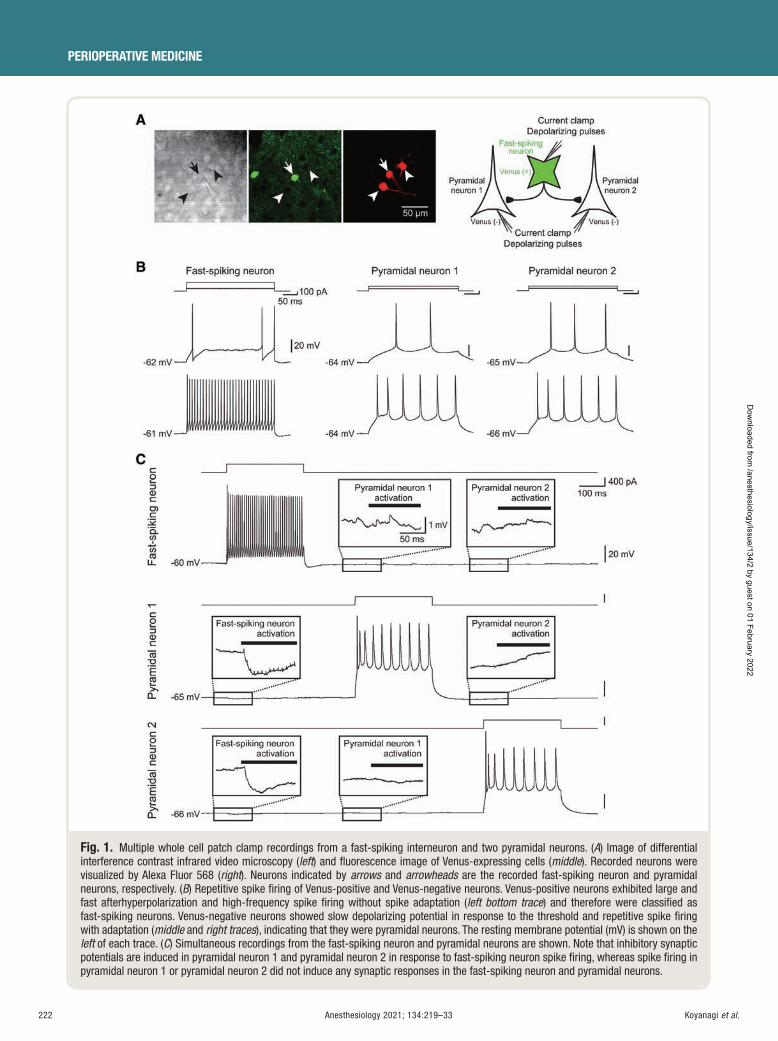
222 Anesthesiology 2021; 134:219–33
PERIOPERATIVE MEDICINE
Koyanagi et al.
Fig. 1. Multiple whole cell patch clamp recordings from a fast-spiking interneuron and two pyramidal neurons. ( A ) Image of differential interference contrast infrared video microscopy ( left ) and fl uorescence image of Venus-expressing cells ( middle ). Recorded neurons were visualized by Alexa Fluor 568 ( right ). Neurons indicated by arrows and arrowheads are the recorded fast-spiking neuron and pyramidal neurons, respectively. ( B ) Repetitive spike fi ring of Venus-positive and Venus-negative neurons. Venus-positive neurons exhibited large and fast afterhyperpolarization and high-frequency spike fi ring without spike adaptation ( left bottom trace ) and therefore were classifi ed as fast-spiking neurons. Venus-negative neurons showed slow depolarizing potential in response to the threshold and repetitive spike fi ring with adaptation ( middle and right traces ), indicating that they were pyramidal neurons. The resting membrane potential (mV) is shown on the left of each trace. ( C ) Simultaneous recordings from the fast-spiking neuron and pyramidal neurons are shown. Note that inhibitory synaptic potentials are induced in pyramidal neuron 1 and pyramidal neuron 2 in response to fast-spiking neuron spike fi ring, whereas spike fi ring in pyramidal neuron 1 or pyramidal neuron 2 did not induce any synaptic responses in the fast-spiking neuron and pyramidal neurons.
ALNV134N2_Text.indb 222ALNV134N2_Text.indb 222 29-Dec-20 19:43:5729-Dec-20 19:43:57
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
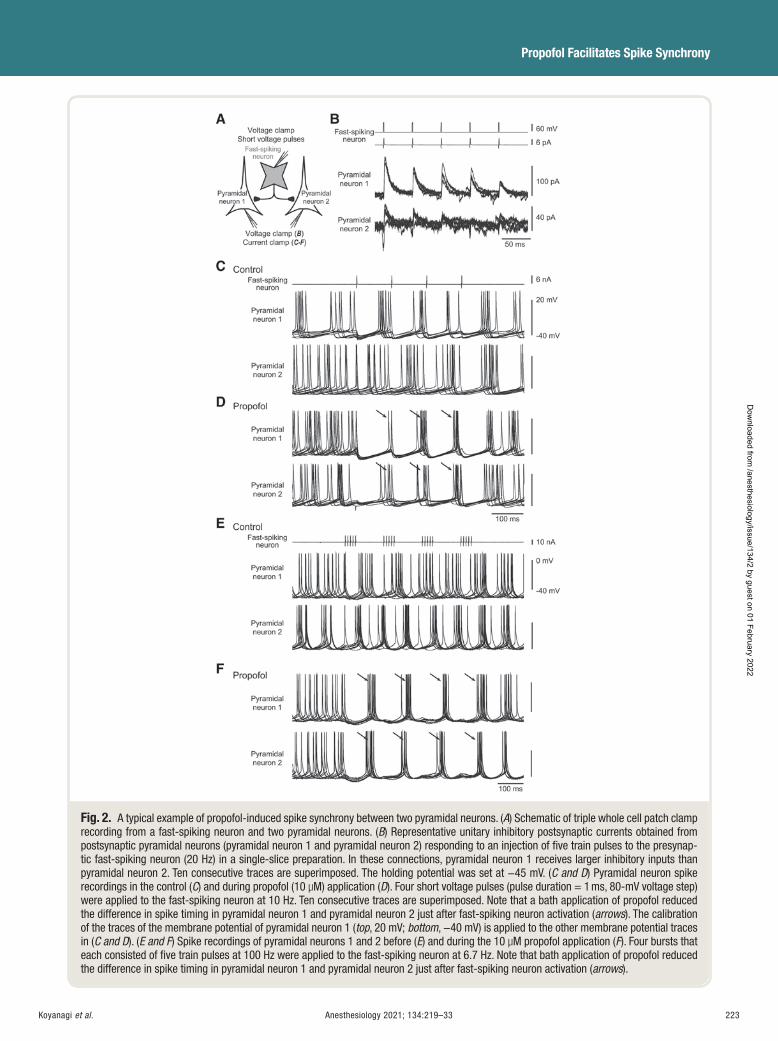
Anesthesiology 2021; 134:219–33 223
Propofol Facilitates Spike Synchrony
Koyanagi et al.
Fig. 2. A typical example of propofol-induced spike synchrony between two pyramidal neurons. ( A ) Schematic of triple whole cell patch clamp recording from a fast-spiking neuron and two pyramidal neurons. ( B ) Representative unitary inhibitory postsynaptic currents obtained from postsynaptic pyramidal neurons (pyramidal neuron 1 and pyramidal neuron 2) responding to an injection of fi ve train pulses to the presynap-tic fast-spiking neuron (20 Hz) in a single-slice preparation. In these connections, pyramidal neuron 1 receives larger inhibitory inputs than pyramidal neuron 2. Ten consecutive traces are superimposed. The holding potential was set at − 45 mV. ( C and D ) Pyramidal neuron spike recordings in the control ( C ) and during propofol (10 μ M) application ( D ). Four short voltage pulses (pulse duration = 1 ms, 80-mV voltage step) were applied to the fast-spiking neuron at 10 Hz. Ten consecutive traces are superimposed. Note that a bath application of propofol reduced the difference in spike timing in pyramidal neuron 1 and pyramidal neuron 2 just after fast-spiking neuron activation ( arrows ). The calibration of the traces of the membrane potential of pyramidal neuron 1 ( top , 20 mV; bottom , − 40 mV) is applied to the other membrane potential traces in ( C and D ). ( E and F ) Spike recordings of pyramidal neurons 1 and 2 before ( E ) and during the 10 μ M propofol application ( F ). Four bursts that each consisted of fi ve train pulses at 100 Hz were applied to the fast-spiking neuron at 6.7 Hz. Note that bath application of propofol reduced the difference in spike timing in pyramidal neuron 1 and pyramidal neuron 2 just after fast-spiking neuron activation ( arrows ).
ALNV134N2_Text.indb 223ALNV134N2_Text.indb 223 29-Dec-20 19:43:5729-Dec-20 19:43:57
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
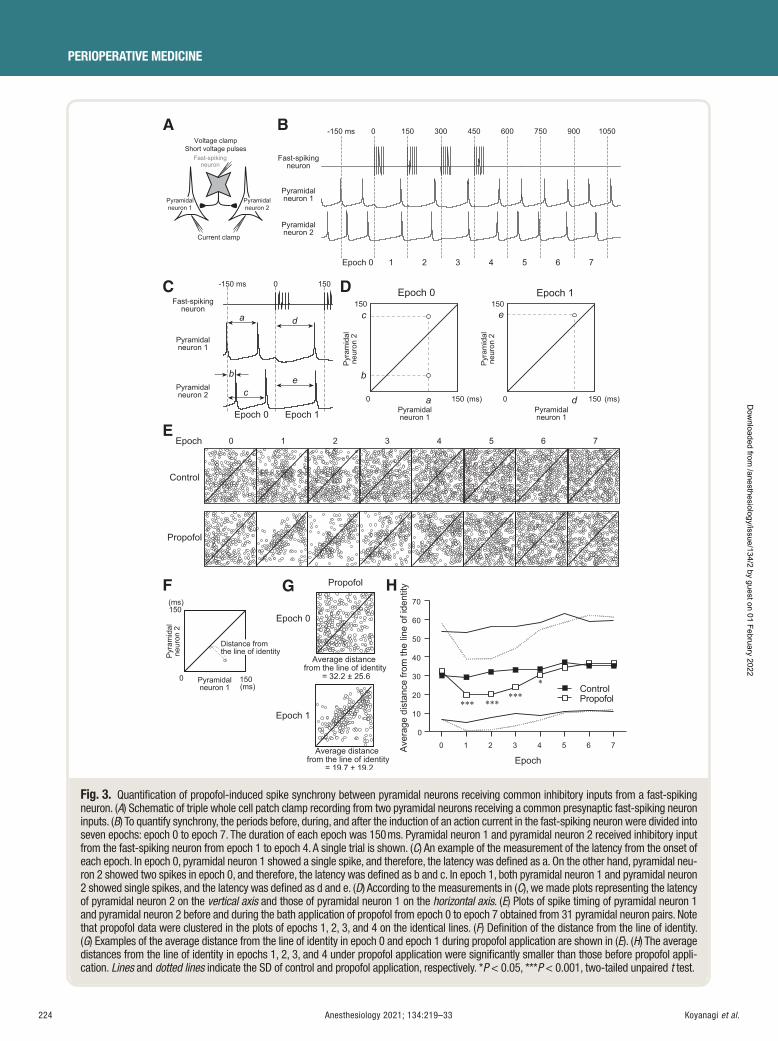
224 Anesthesiology 2021; 134:219–33
PERIOPERATIVE MEDICINE
Koyanagi et al.
A
E
F
C D
HG
B
Fig. 3. Quantifi cation of propofol-induced spike synchrony between pyramidal neurons receiving common inhibitory inputs from a fast-spiking neuron. ( A ) Schematic of triple whole cell patch clamp recording from two pyramidal neurons receiving a common presynaptic fast-spiking neuron inputs. ( B ) To quantify synchrony, the periods before, during, and after the induction of an action current in the fast-spiking neuron were divided into seven epochs: epoch 0 to epoch 7. The duration of each epoch was 150 ms. Pyramidal neuron 1 and pyramidal neuron 2 received inhibitory input from the fast-spiking neuron from epoch 1 to epoch 4. A single trial is shown. ( C ) An example of the measurement of the latency from the onset of each epoch. In epoch 0, pyramidal neuron 1 showed a single spike, and therefore, the latency was defi ned as a. On the other hand, pyramidal neu-ron 2 showed two spikes in epoch 0, and therefore, the latency was defi ned as b and c. In epoch 1, both pyramidal neuron 1 and pyramidal neuron 2 showed single spikes, and the latency was defi ned as d and e. ( D ) According to the measurements in ( C ), we made plots representing the latency of pyramidal neuron 2 on the vertical axis and those of pyramidal neuron 1 on the horizontal axis . ( E ) Plots of spike timing of pyramidal neuron 1 and pyramidal neuron 2 before and during the bath application of propofol from epoch 0 to epoch 7 obtained from 31 pyramidal neuron pairs. Note that propofol data were clustered in the plots of epochs 1, 2, 3, and 4 on the identical lines. ( F ) Defi nition of the distance from the line of identity. ( G ) Examples of the average distance from the line of identity in epoch 0 and epoch 1 during propofol application are shown in ( E ). ( H ) The average distances from the line of identity in epochs 1, 2, 3, and 4 under propofol application were signifi cantly smaller than those before propofol appli-cation. Lines and dotted lines indicate the SD of control and propofol application, respectively. * P < 0.05, * * * P < 0.001, two-tailed unpaired t test.
ALNV134N2_Text.indb 224ALNV134N2_Text.indb 224 29-Dec-20 19:43:5929-Dec-20 19:43:59
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
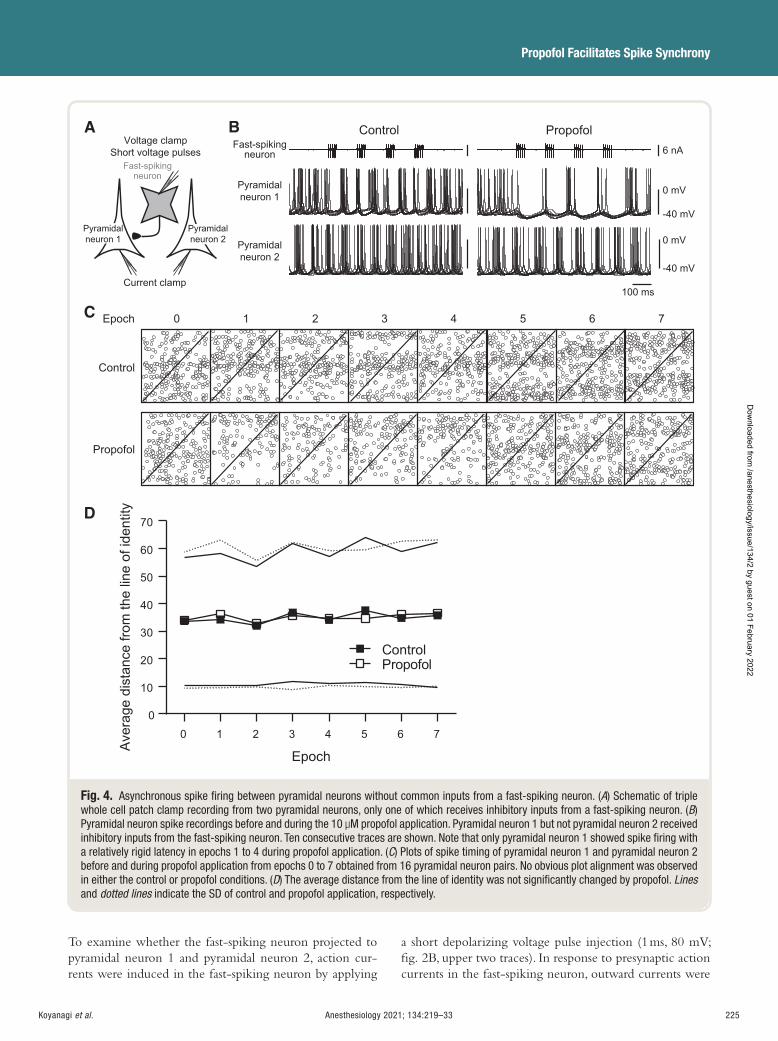
Anesthesiology 2021; 134:219–33 225
Propofol Facilitates Spike Synchrony
Koyanagi et al.
To examine whether the fast-spiking neuron projected to pyramidal neuron 1 and pyramidal neuron 2, action cur-rents were induced in the fast-spiking neuron by applying
a short depolarizing voltage pulse injection (1 ms, 80 mV; g. 2B , upper two traces). In response to presynaptic action currents in the fast-spiking neuron, outward currents were
A B
C
D
Fig. 4. Asynchronous spike fi ring between pyramidal neurons without common inputs from a fast-spiking neuron. ( A ) Schematic of triple whole cell patch clamp recording from two pyramidal neurons, only one of which receives inhibitory inputs from a fast-spiking neuron. ( B ) Pyramidal neuron spike recordings before and during the 10 μ M propofol application. Pyramidal neuron 1 but not pyramidal neuron 2 received inhibitory inputs from the fast-spiking neuron. Ten consecutive traces are shown. Note that only pyramidal neuron 1 showed spike fi ring with a relatively rigid latency in epochs 1 to 4 during propofol application. ( C ) Plots of spike timing of pyramidal neuron 1 and pyramidal neuron 2 before and during propofol application from epochs 0 to 7 obtained from 16 pyramidal neuron pairs. No obvious plot alignment was observed in either the control or propofol conditions. ( D ) The average distance from the line of identity was not signifi cantly changed by propofol. Linesand dotted lines indicate the SD of control and propofol application, respectively.
ALNV134N2_Text.indb 225ALNV134N2_Text.indb 225 29-Dec-20 19:44:0129-Dec-20 19:44:01
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

226 Anesthesiology 2021; 134:219–33
PERIOPERATIVE MEDICINE
Koyanagi et al.
observed in both pyramidal neuron 1 and pyramidal neuron 2, which were voltage clamped at − 45 mV ( g. 2B , lower traces), indicating that both pyramidal neurons received inhibitory inputs from the fast-spiking neuron.
After con rming synaptic connections from the fast-spiking neuron to pyramidal neurons, postsynaptic pyramidal neuron 1 and pyramidal neuron 2 were recorded under a current clamp condition. To examine the e ect of presynaptic inhibitory inputs from the fast-spiking neu-ron on spike synchrony between pyramidal neuron 1 and pyramidal neuron 2, repetitive spike ring was induced by depolarized direct currents to both pyramidal neurons. The depolarizing currents were set at the intensity (approxi-mately 200 pA) that induced repetitive spike ring at 5 to 15 Hz.
In the rst series of the experiment, four action currents were applied at the alpha range (100-ms interspike intervals, 10 Hz). Although the fast-spiking neuron sent inhibitory inputs to pyramidal neuron 1 and pyramidal neuron 2, pre-synaptic fast-spiking neuron activation had little e ect on postsynaptic pyramidal neuron synchrony between pyrami-dal neuron 1 and pyramidal neuron 2 under the control conditions ( g. 2C ). On the other hand, a bath applica-tion of 10 μ M propofol facilitated spike synchrony between pyramidal neuron 1 and pyramidal neuron 2 just after the action current was induced in the fast-spiking neuron ( g. 2D , arrows).
In in vivo preparations, fast-spiking neurons often show burst ring in which several spikes are elicited at a high frequency, such as more than 20 Hz, 21 , 22 and thus, it is rea-sonable to estimate postsynaptic spike synchronization by applying presynaptic train pulses. Therefore, we applied four sequential voltage pulses ( ve train pulses at 100 Hz) with interburst intervals of 150 ms to the fast-spiking neu-ron ( g. 2E ) during repetitive spike ring of pyramidal neuron 1 and pyramidal neuron 2. Even though the train pulses to the fast-spiking neuron induced a larger impact on postsynaptic pyramidal neurons, most pyramidal neuron pairs showed asynchronous spike ring under the control conditions. However, well-synchronized ring patterns were observed when propofol was administered ( g. 2F ). Therefore, in the following experiment, we used this train pulse protocol to estimate the e ect of the fast-spiking neu-ron → pyramidal neuron connection on synchronous spike ring among pyramidal neurons.
Quantifi cation of Spike Synchrony in Pyramidal Neurons
Figure 3 , A to D, shows another example obtained from one presynaptic fast-spiking neuron and two postsynaptic pyramidal neuron connections. The spike latencies from the onset of each epoch (vertical dotted lines in g. 3B ) were measured in pyramidal neuron 1 and pyramidal neuron 2 ( g. 3C ), and the latency of pyramidal neuron 2 was plotted against that of pyramidal neuron 1 ( g. 3D ). The horizontal
and vertical axes show the spike latency of pyramidal neu-ron 1 and pyramidal neuron 2, respectively. Figure 3E shows the plots of spike timing of pyramidal neuron 1 and pyra-midal neuron 2 obtained from 31 pyramidal neuron pairs. In epoch 0 in the control, the plots were widely distributed. Some plots showed a cluster around the identical lines in epochs 1 and 2 in the control; however, epochs 3 to 7 again showed randomly distributed plots in the control ( g. 3E ).
Similar to the results obtained for the controls, epoch 0 during the bath application of propofol showed a random distribution of plots. In contrast, the propofol group showed a cluster in the spike timing plots on the line of identity in epoch 1, suggesting spike synchronization between pyra-midal neuron 1 and pyramidal neuron 2. This propofol-in-duced e ect was also observed in epochs 2 and 3 and was weakly observed in epoch 4 ( g. 3E ). However, epochs 5 to 7 did not show such de ection of plots. This result indicates that propofol facilitates the spike synchrony between pyra-midal neuron 1 and pyramidal neuron 2.
For a quantitative analysis of the synchronized spike ring in pyramidal neuron 1 and pyramidal neuron 2, an absolute value, l, was measured and averaged ( g. 3 , F and G). In the case in which spikes in pyramidal neuron 1 were completely synchronized to those in pyramidal neuron 2, the plots were aligned on the identical line, and average dis-tance from the line of identity was 0. Figure 3G shows typ-ical asynchronized and synchronized examples, as shown in gure 3E (epochs 0 and 1 during propofol application). The index, average distance from the line of identity, in epoch 1, in which the presynaptic fast-spiking neuron was activated, was smaller (average distance from the line of identity = 19.7 ± 19.2) than that in epoch 0 (average distance from the line of identity = 32.2 ± 25.6), supporting that aver-age distance from the line of identity re ects the degree of synchronization.
Figure 3H shows the summary of average distance from the line of identity obtained from 31 pyramidal neuron pairs in the control and under the 10 μ M propofol appli-cation. In comparison to the control, average distance from the line of identity in the propofol application was signi -cantly smaller in epoch 1 (29.2 ± 24.1 [number of spikes: n = 510] to 19.7 ± 19.2 [n = 242], P < 0.001, di er-ence in means = − 9.4, 95% CI = − 12.6 to − 6.2), epoch 2 (32.0 ± 24.3 [n = 518] to 20.0 ± 19.0 [n = 255], P < 0.001, di erence in means = − 11.9, 95% CI = − 15.1 to − 8.8), epoch 3 (33.0 ± 23.5 [n = 535] to 23.9 ± 20.7 [n = 316], P < 0.001, di erence in means = − 9.2, 95% CI = − 12.2 to − 6.1), and epoch 4 (33.4 ± 24.8 [n = 613] to 30.4 ± 24.2 [n = 446], P = 0.048, di erence in means = − 3.0, 95% CI = − 6.0 to − 0.0). In contrast, propofol had little e ect on the distances from the line of identity in epoch 0 (30.1 ± 23.4 [n = 430] to 32.2 ± 25.6 [n = 348], P = 0.225), epoch 5 (37.2 ± 26.3 [n = 692] to 34.3 ± 24.2 [n = 505], P = 0.056), epoch 6 (35.3 ± 23.9 [n = 609] to 36.6 ± 25.8 [n = 500], P = 0.371),
ALNV134N2_Text.indb 226ALNV134N2_Text.indb 226 29-Dec-20 19:44:0129-Dec-20 19:44:01
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:219–33 227
Propofol Facilitates Spike Synchrony
Koyanagi et al.
and epoch 7 (35.2 ± 24.4 [n = 634] to 36.6 ± 24.8 [n = 465], P = 0.367). These results suggest that propofol facilitates spike synchronization just after GABAergic inputs are received from fast-spiking neurons but has little e ect on the synchrony of spontaneous spike ring patterns.
Uncommon Inputs from Fast-spiking Neurons Do Not Induce Synchronization of Pyramidal Neuron Spike Firing
If inhibitory inputs from fast-spiking neurons regulate the synchronization of pyramidal neuron spike ring, it is likely that uncommon inhibitory inputs do not induce syn-chronization in pyramidal neurons. To test this possibility, we next examined the e ects of propofol on spike syn-chrony between two pyramidal neurons, only one of which received inhibitory input from the presynaptic fast-spiking neuron ( g. 4A ).
In epochs 1 to 4, in which pyramidal neuron 1 received inhibitory inputs from the fast-spiking neuron, propofol synchronized the spikes in pyramidal neuron 1 ( g. 4B ). In contrast, propofol had little e ect on spike timing in pyra-midal neuron 2 that did not receive inhibitory inputs from the fast-spiking neuron ( g. 4B ). Consequently, propofol failed to facilitate spike synchrony between pyramidal neu-ron 1 and pyramidal neuron 2 even immediately after the action current was induced in the fast-spiking neuron; spike timing plots were almost randomly distributed in the con-trol and during propofol application ( g. 4C ).
In fact, average distance from the line of identity values obtained from 16 pyramidal neuron pairs was not signi -cantly changed by propofol in each epoch: 33.7 ± 23.2 (n = 284) to 34.0 ± 24.7 (n = 229, P = 0.870) in epoch 0; 34.3 ± 23.8 (n = 271) to 36.3 ± 26.8 (n = 140, P = 0.447) in epoch 1; 32.0 ± 21.7 (n = 250) to 32.7 ± 22.9 (n = 139, P = 0.751) in epoch 2; 36.7 ± 25.0 (n = 259) to 35.5 ± 26.7 (n = 175, P = 0.644) in epoch 3; 34.1 ± 23.1 (n = 256) to 34.8 ± 24.5 (n = 166, P = 0.765) in epoch 4; 37.6 ± 26.3 (n = 346) to 34.7 ± 24.8 (n = 246, P = 0.180) in epoch 5; 34.8 ± 24.2 (n = 323) to 36.1 ± 26.6 (n = 263, P = 0.531) in epoch 6; and 35.8 ± 26.4 (n = 352) to 36.6 ± 26.6 (n = 263, P = 0.716) in epoch 7 ( g. 4 , C and D). These results sup-port the aforementioned idea that propofol-induced spike synchrony between pyramidal neurons is mediated by com-mon inhibitory inputs from fast-spiking neurons.
Frequency Specifi city of Propofol-induced Pyramidal Neuron Spike Synchrony
The current experiment revealed that fast-spiking neu-ron → pyramidal neuron inhibitory inputs synchronized postsynaptic pyramidal neuron spikes during the bath application of propofol. Although thalamocortical projec-tions play a critical role in propofol-induced alpha rhythm generation in the cerebral cortex, 5 , 6 cortical local circuits should have the capacity to maintain alpha oscillation.
However, it remains unknown whether the propofol-in-duced synchronization of postsynaptic spike ring in pyra-midal neurons occurs even when presynaptic fast-spiking neurons are activated at a di erent frequency range. To answer this question, the presynaptic fast-spiking neuron was activated with interburst intervals of 1,050 ms (1 Hz), 250 ms (4 Hz), 150 ms (6.7 Hz), 100 ms (10 Hz), and 75 ms (13.3 Hz).
Figure 5 shows a typical example of postsynaptic pyra-midal neuron ring responding to the presynaptic fast-spik-ing neuron action potentials induced at the frequencies described above. At all frequencies, the rst burst of the fast-spiking neuron action currents in epoch 1 induced a period without spikes for 50 to 150 ms (arrowheads; blank period), in which GABA A receptor – mediated inhibitory postsynaptic potentials occurred ( g. 1C ), in each pyrami-dal neuron. However, the subsequent epochs (epochs 2 to 4) exhibited a less obvious blank period in the controls.
The blank period was more prominent, had a longer duration, and had a larger hyperpolarization during propo-fol application than in the controls. This blank period was induced with similar timing, and therefore, the subsequent spikes were aligned among pyramidal neurons. However, the subsequent bursts (second, third, and fourth spike trains in the fast-spiking neuron) at 1, 4, and 13.3 Hz showed less synchronized spike ring among pyramidal neurons during propofol application. In contrast, remarkable propo-fol-induced spike synchrony among pyramidal neurons was observed in the period when the presynaptic fast-spiking neuron was activated at 6.7 and 10 Hz.
To quantify the relationship between the synchrony of pyramidal neuron spike ring and the frequency of pre-synaptic fast-spiking neuron burst spike ring, we made a cross-correlogram, and the synchronization index was calculated (see Materials and Methods). Figure 6 , A and B, shows examples of the cross-correlograms obtained from the results shown in gure 5 . The synchronization index was compared between the control and propofol applica-tion ( g. 6C ). In the cases of 1-, 4-, and 13.3-Hz stim-ulation, the synchronization index obtained from each category showed no statistically signi cant change in the propofol application (connected pyramidal neurons with-out presynaptic stimuli: for 1 Hz stimulation [1.2 ± 0.6 to 1.2 ± 0.5, n = 26 pyramidal neuron pairs, P = 0.869], for 4 Hz stimulation [1.2 ± 0.3 to 1.1 ± 0.3, n = 28 pyramidal neuron pairs, P = 0.328], and for 13.3 Hz stimulation [1.6 ± 0.7 to 2.1 ± 1.0, n = 18 pyramidal neuron pairs, P = 0.074]; connected pyramidal neurons with presynaptic stimuli: for 1 Hz stimulation [1.0 ± 0.2 to 1.0 ± 0.2, n = 28 pyramidal neuron pairs, P = 0.950], for 4 Hz stimulation [1.3 ± 0.5 to 1.6 ± 1.0, n = 28 pyramidal neuron pairs, P = 0.135], and for 13.3 Hz stimulation [1.2 ± 0.7 to 1.5 ± 0.7, n = 8 pyramidal neuron pairs, P = 0.532]; unconnected pyramidal neurons without presynaptic stimuli: for 1 Hz stimulation [1.2 ± 0.5 to 1.2 ± 0.5, n = 22 pyramidal neuron pairs,
ALNV134N2_Text.indb 227ALNV134N2_Text.indb 227 29-Dec-20 19:44:0129-Dec-20 19:44:01
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
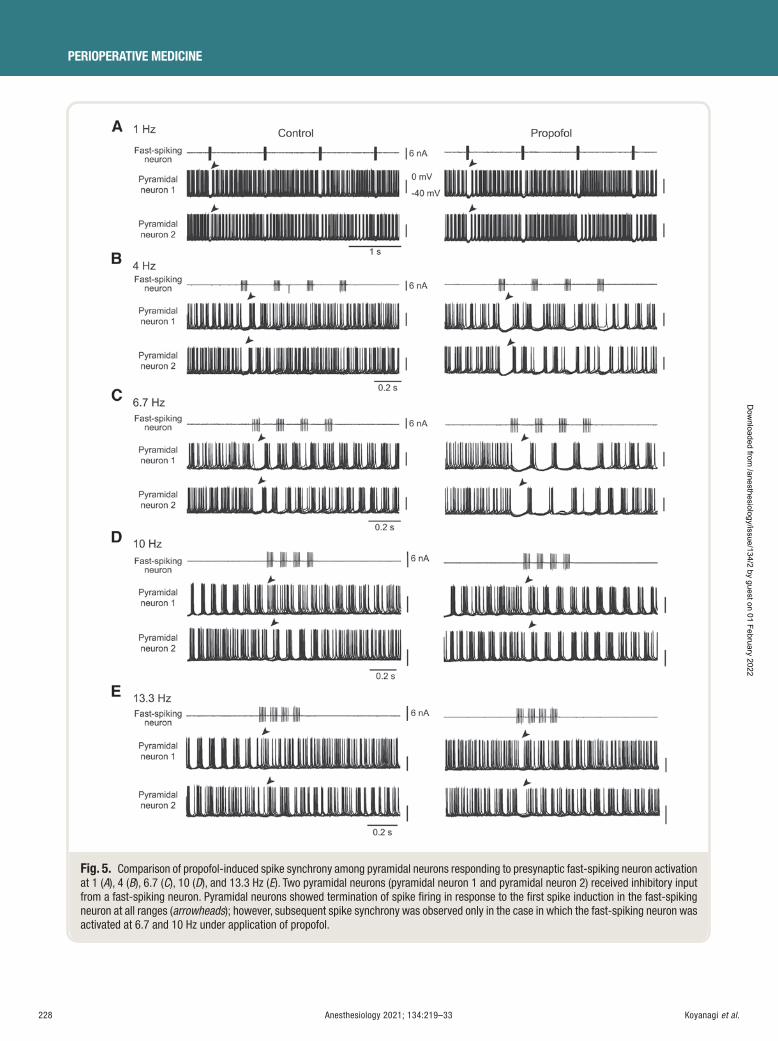
228 Anesthesiology 2021; 134:219–33
PERIOPERATIVE MEDICINE
Koyanagi et al.
Fig. 5. Comparison of propofol-induced spike synchrony among pyramidal neurons responding to presynaptic fast-spiking neuron activation at 1 ( A ), 4 ( B ), 6.7 ( C ), 10 ( D ), and 13.3 Hz ( E ). Two pyramidal neurons (pyramidal neuron 1 and pyramidal neuron 2) received inhibitory input from a fast-spiking neuron. Pyramidal neurons showed termination of spike fi ring in response to the fi rst spike induction in the fast-spiking neuron at all ranges ( arrowheads ); however, subsequent spike synchrony was observed only in the case in which the fast-spiking neuron was activated at 6.7 and 10 Hz under application of propofol.
ALNV134N2_Text.indb 228ALNV134N2_Text.indb 228 29-Dec-20 19:44:0229-Dec-20 19:44:02
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
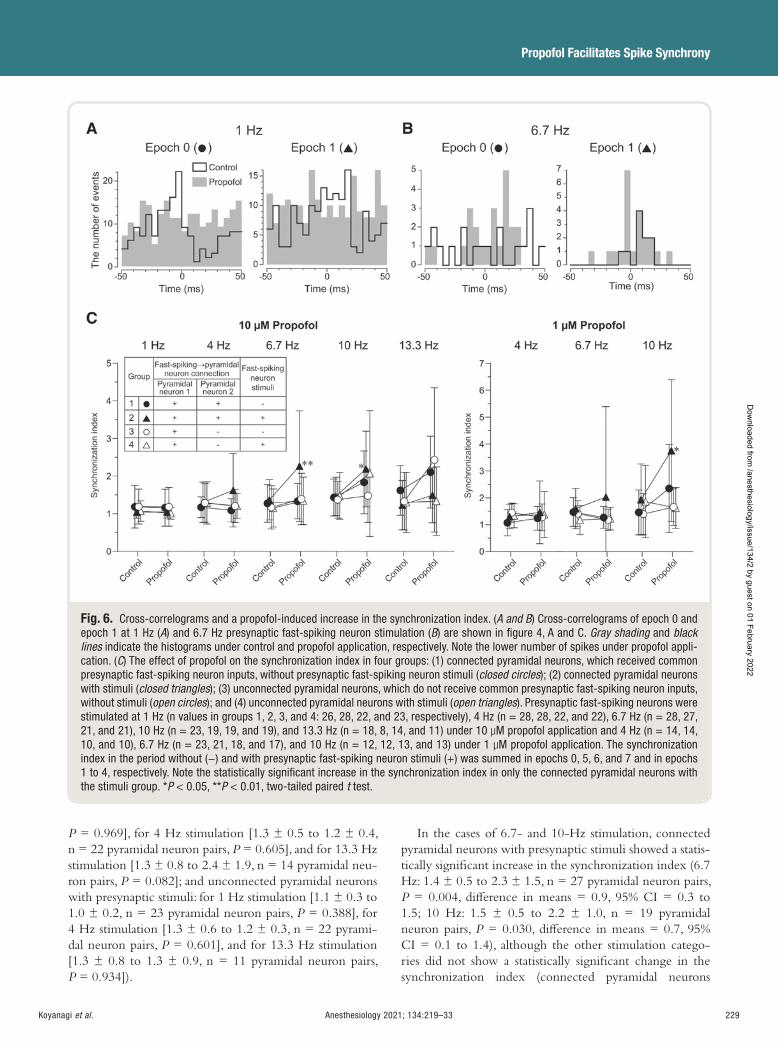
Anesthesiology 2021; 134:219–33 229
Propofol Facilitates Spike Synchrony
Koyanagi et al.
P = 0.969], for 4 Hz stimulation [1.3 ± 0.5 to 1.2 ± 0.4, n = 22 pyramidal neuron pairs, P = 0.605], and for 13.3 Hz stimulation [1.3 ± 0.8 to 2.4 ± 1.9, n = 14 pyramidal neu-ron pairs, P = 0.082]; and unconnected pyramidal neurons with presynaptic stimuli: for 1 Hz stimulation [1.1 ± 0.3 to 1.0 ± 0.2, n = 23 pyramidal neuron pairs, P = 0.388], for 4 Hz stimulation [1.3 ± 0.6 to 1.2 ± 0.3, n = 22 pyrami-dal neuron pairs, P = 0.601], and for 13.3 Hz stimulation [1.3 ± 0.8 to 1.3 ± 0.9, n = 11 pyramidal neuron pairs, P = 0.934]).
In the cases of 6.7- and 10-Hz stimulation, connected pyramidal neurons with presynaptic stimuli showed a statis-tically signi cant increase in the synchronization index (6.7 Hz: 1.4 ± 0.5 to 2.3 ± 1.5, n = 27 pyramidal neuron pairs, P = 0.004, di erence in means = 0.9, 95% CI = 0.3 to 1.5; 10 Hz: 1.5 ± 0.5 to 2.2 ± 1.0, n = 19 pyramidal neuron pairs, P = 0.030, di erence in means = 0.7, 95% CI = 0.1 to 1.4), although the other stimulation catego-ries did not show a statistically signi cant change in the synchronization index (connected pyramidal neurons
Fig. 6. Cross-correlograms and a propofol-induced increase in the synchronization index. ( A and B ) Cross-correlograms of epoch 0 and epoch 1 at 1 Hz ( A ) and 6.7 Hz presynaptic fast-spiking neuron stimulation ( B ) are shown in fi gure 4 , A and C. Gray shading and black lines indicate the histograms under control and propofol application, respectively. Note the lower number of spikes under propofol appli-cation. ( C ) The effect of propofol on the synchronization index in four groups: (1) connected pyramidal neurons, which received common presynaptic fast-spiking neuron inputs, without presynaptic fast-spiking neuron stimuli ( closed circles ); (2) connected pyramidal neurons with stimuli ( closed triangles ); (3) unconnected pyramidal neurons, which do not receive common presynaptic fast-spiking neuron inputs, without stimuli ( open circles ); and (4) unconnected pyramidal neurons with stimuli ( open triangles ). Presynaptic fast-spiking neurons were stimulated at 1 Hz (n values in groups 1, 2, 3, and 4: 26, 28, 22, and 23, respectively), 4 Hz (n = 28, 28, 22, and 22), 6.7 Hz (n = 28, 27, 21, and 21), 10 Hz (n = 23, 19, 19, and 19), and 13.3 Hz (n = 18, 8, 14, and 11) under 10 μ M propofol application and 4 Hz (n = 14, 14, 10, and 10), 6.7 Hz (n = 23, 21, 18, and 17), and 10 Hz (n = 12, 12, 13, and 13) under 1 μ M propofol application. The synchronization index in the period without ( − ) and with presynaptic fast-spiking neuron stimuli ( + ) was summed in epochs 0, 5, 6, and 7 and in epochs 1 to 4, respectively. Note the statistically signifi cant increase in the synchronization index in only the connected pyramidal neurons with the stimuli group. * P < 0.05, * * P < 0.01, two-tailed paired t test.
ALNV134N2_Text.indb 229ALNV134N2_Text.indb 229 29-Dec-20 19:44:0229-Dec-20 19:44:02
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

230 Anesthesiology 2021; 134:219–33
PERIOPERATIVE MEDICINE
Koyanagi et al.
without presynaptic stimuli: for 6.7 Hz stimulation [1.3 ± 0.5 to 1.3 ± 0.5, n = 28 pyramidal neuron pairs, P = 0.591] and for 10 Hz stimulation [1.4 ± 0.5 to 1.8 ± 0.8, n = 23 pyramidal neuron pairs, P = 0.056]; uncon-nected pyramidal neurons without presynaptic stimuli: for 6.7 Hz stimulation [1.2 ± 0.6 to 1.4 ± 0.7, n = 21 pyra-midal neuron pairs, P = 0.267] and for 10 Hz stimulation [1.4 ± 0.5 to 1.5 ± 0.7, n = 19 pyramidal neuron pairs, P = 0.576]; unconnected pyramidal neurons with presynaptic stimuli: for 6.7 Hz stimulation [1.2 ± 0.5 to 1.3 ± 0.6, n = 21 pyramidal neuron pairs, P = 0.358] and for 10 Hz stim-ulation [1.5 ± 0.6 to 2.1 ± 1.7, n = 19 pyramidal neuron pairs, P = 0.141]).
In agreement with the result of the synchronization index increase by 10 μ M propofol in the category of connected pyramidal neurons with presynaptic stimuli, 1 μ M propo-fol signi cantly increased the synchronization index at 10 Hz (1.9 ± 1.3 to 3.7 ± 2.6, n = 12 pyramidal neuron pairs, P = 0.042, di erence in means = 1.8, 95% CI = 0.1 to 3.5) without changing the synchronization index at 4 Hz (1.3 ± 0.5 to 1.5 ± 1.2, n = 14 pyramidal neuron pairs, P = 0.577). On the other hand, 1 μ M propofol induced a slight but insigni cant increase in the synchronization index at 6.7 Hz (1.6 ± 0.7 to 2.0 ± 3.4, n = 21 pyramidal neuron pairs, P = 0.587), which contradicts the result obtained for 10 μ M propofol. These results indicate that pyramidal neurons show synchronous ring in response to fast-spiking neuron activation with an interburst interval of 100 to 150 ms.
Discussion Using a triple or quadruple whole cell patch clamp tech-nique, we found that the intravenous anesthetic propofol facilitates spike synchrony among pyramidal neurons by enhancing inhibitory input from fast-spiking neurons in rat cortical slices. The bath application of 1 and 10 μ M propofol promoted postsynaptic pyramidal neuron ring synchrony when a presynaptic fast-spiking neuron was activated with 100- and 100/150-ms interburst intervals, respectively. On the other hand, propofol failed to synchronize pyramidal neuron ring when the presynaptic fast-spiking neuron was activated with 1,050-, 250-, or 75-ms interburst intervals. These ndings suggest that fast-spiking neurons play a crit-ical role in inducing the synchronization of pyramidal neu-ron ring during propofol application.
Propofol Induces Spike Synchrony via Fast-spiking Neuron Activation
Propofol prolongs the decay time of GABA A recep-
tor – mediated inhibitory currents, and among the connec-tions from various interneurons to pyramidal neurons, the fast-spiking neuron → pyramidal neuron connection is the most sensitive to propofol. 16 Propofol-induced increases in GABA
A receptor – mediated Cl − conductance reduce the
spike ring frequency. 12 Several studies have demonstrated
that the enhancement of inhibitory input results in facil-itating neural synchronization. For example, spike-timing precision and neuronal synchrony are enhanced by synaptic inhibition in the amygdala. 23 In the somatosensory cortex, synchrony of spike ring between interneurons correlates with inhibitory synaptic transmission. 24 Therefore, the propofol-induced enhancement of inhibitory input from fast-spiking neurons is likely to increase spike synchrony in the insular cortex, part of which may be mediated by a propofol-induced reduction of asynchronous spike ring.
To test this hypothesis, the e ects of propofol on pyra-midal neuron synchrony were examined in minimum neuronal circuits consisting of two or three postsynaptic pyramidal neurons and one presynaptic fast-spiking neuron using multiple whole cell recordings. We found that propo-fol e ectively synchronized spike ring among the pyrami-dal neurons. It is worth noting that fast-spiking neurons are electrically coupled via gap junctions because these electrical synapses contribute to the synchronization of spike ring among fast-spiking neurons. 25 , 26 Therefore, the synchro-nized activity in the minimum circuits may propagate to the adjacent local circuits, resulting in spike ring synchrony of pyramidal neurons distributed in a large cortical area. The weaker synchronization in epoch 4 compared with that in epochs 1 to 3 may be due to the subsequent depression of inhibitory postsynaptic currents in fast-spiking neuron → pyramidal neuron connections, as we previously reported. 16
We chose ve train bursts to activate fast-spiking neu-rons because of the lower number of the inhibitory inputs from fast-spiking neuron to pyramidal neurons in the slice preparation compared with those in in vivo preparations; this lower number of inputs in the slice preparation means that some chemical and electrical connections are lost. In the minimum local circuit, 1 and 10 μ M propofol consistently promoted fast-spiking neuron-activated synchronization when the fast-spiking neuron was activated with 100 ms of the interburst interval. However, there was a partial discrep-ancy in propofol-induced fast-spiking neuron-activated synchronization between 10 and 1 μ M propofol: synchroni-zation induced by fast-spiking neuron activation at 150 ms of the interburst interval was potentiated by 10 μ M but not 1 μ M propofol. The larger e ect on GABAergic currents induced by 10 μ M propofol may expand the e ective range of synchronization compared with that induced by 1 μ M propofol. We consider that propofol-induced alpha oscilla-tion is not always induced in the cortical circuit. As previ-ously reported, thalamocortical and corticothalamic circuits play an essential role in the induction of alpha oscillations (8 to 13 Hz) in the cerebral cortex, and alpha oscillations cannot be induced without thalamic inputs. 5 , 6 In sensory cortices such as the visual and barrel cortices, layer IV neu-rons are the principal target of thalamocortical inputs and project to layers II/III. Layer II/III glutamatergic neurons then project to layer V/VI neurons, some of which project their axons to the thalamus. 27 These glutamatergic circuits
ALNV134N2_Text.indb 230ALNV134N2_Text.indb 230 29-Dec-20 19:44:0229-Dec-20 19:44:02
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:219–33 231
Propofol Facilitates Spike Synchrony
Koyanagi et al.
also receive GABAergic inputs. Therefore, in addition to the thalamocortical and corticothalamic circuits, the corti-cal local circuits between them possibly contribute to alpha oscillations by mediating alpha oscillation activity from thalamocortical inputs to corticothalamic outputs. Our nding of propofol-induced synchrony close to the alpha range in the minimum cortical circuits shows the capacity of the cortical circuit for maintaining alpha synchrony, at least when cortical fast-spiking neurons are activated.
Other Mechanisms for Propofol-induced Spike Synchrony
The current study demonstrated that 10 μ M propofol increased synchronized activity among pyramidal neurons by fast-spiking neuron activation not only at 10 Hz (alpha rhythm) but also at 6.7 Hz, which is slightly lower than the frequency of the alpha rhythm. This nding suggests that other mechanisms, such as non – fast-spiking neuron → pyramidal neuron connections and inhibitory connec-tions among fast-spiking neurons and non – fast-spiking neurons, are involved in alpha rhythm generation in addi-tion to fast-spiking neuron → pyramidal neuron connec-tions. In the insular cortex, there are several other types of GABAergic interneurons: late-spiking, regular-spiking, and low-threshold spike neurons. 19 Several studies have demonstrated the critical role of non – fast-spiking neurons in propofol-induced alpha rhythms. For example, compu-tational models showed that low-threshold spike neurons, a subtype of non – fast-spiking neurons, are crucial for propo-fol-induced alpha rhythms, 1 , 28 although low-threshold spike neurons can be replaced with fast-spiking neurons. 1
On the other hand, somatostatin-expressing non – fast-spiking neurons show preferential inhibition of other interneurons, including fast-spiking neurons, rather than pyramidal neurons. 20 In addition, somatostatin-expressing non – fast-spiking neurons are principal targets of vasoac-tive intestinal peptide – expressing non – fast-spiking neurons, whereas parvalbumin-expressing fast-spiking neurons pref-erentially inhibit other fast-spiking neurons and pyramidal neurons. 20 With this information, along with our previous study demonstrating the preferential facilitation of inhib-itory input in fast-spiking neuron → pyramidal neuron rather than non – fast-spiking neuron → pyramidal neuron/interneurons and fast-spiking neuron → interneurons by propofol, 16 it is reasonable to postulate that non – fast-spik-ing neurons play a minor role in the spike synchrony of pyramidal neurons. Further studies are required to identify the modulatory e ect of a non – fast-spiking neuron net-work on fast-spiking neuron ring during anesthesia.
Mechanisms of the Preference of Alpha Rhythm Induction by Propofol
GABA release from fast-spiking neurons to pyramidal neurons induces inhibitory postsynaptic currents that are
principally mediated by GABA A receptors. 19 Our previous
study demonstrated that the 80% to 20% decay time of uni-tary inhibitory postsynaptic currents in fast-spiking neuron → pyramidal neuron connections in the insular cortex was 12 ms, 16 and as shown in gure 1B , the duration of inhib-itory postsynaptic currents at baseline was approximately 50 ms. The time course of inhibitory postsynaptic currents often overlies the afterhyperpolarization evoked by an action potential. Therefore, the summative e ect of inhib-itory postsynaptic potentials and afterhyperpolarization may be potentiated by propofol (10 μ M), which prolongs the decay kinetics approximately twofold (approximately 25 ms) with a slight increase in the peak amplitude. 16 This propofol-induced modulation of the temporal kinetics of inhibitory postsynaptic currents may play a critical role in regulating the spike timing of postsynaptic pyramidal neurons. Under current clamp mode, repetitive spike r-ing is reset by unitary inhibitory postsynaptic potentials. This role of GABA
A receptors was potentiated by propofol,
and therefore, spikes rarely occurred during this inhibitory postsynaptic potential period ( g. 2D ). As a result, the next spike was temporally aligned among pyramidal neurons that received inhibitory postsynaptic potentials from a common fast-spiking neuron.
Fast-spiking neuron spike ring at the alpha range is necessary for pyramidal neuron spike ring around the alpha range because fast-spiking neuron spike ring at other bands does not induce synchronized activities in pyramidal neurons. Autapses are a crucial factor in reg-ulating fast-spiking neuron ring. Autaptic transmission mediated by GABA
A receptors is frequently observed
in cortical fast-spiking neurons and improves the pre-cision of spike timing rigidity. 29 , 30 Propofol is likely to prolong decay times of autaptic inhibitory postsynaptic current, which may result in slowing fast-spiking neuron ring so that it is within the alpha range. In fact, when single action currents were generated in the presynap-tic fast-spiking neuron at the alpha range, postsynaptic pyramidal neurons tended to show synchronous ring ( g. 2D ), although the modulatory e ect of the fast-spik-ing neuron on pyramidal neuron ring was lower for ve train pulses.
Functional Implication of the Alpha-range Preference of Synchrony Induced by Propofol
The current study demonstrated that cortical pyramidal neurons tend to be synchronized at a certain frequency that includes the alpha range by the bath application of propofol using slice preparations. Such synchronization preferences among pyramidal neurons may be dependent on the mod-ulation of the excitatory and inhibitory balance of inputs to pyramidal neurons, and the other anesthetics may estab-lish synchronous ring at di erent ranges. This modulation might be a mechanism for various states of consciousness, e.g. , hypersynchrony during seizure and alpha coma. 31 Our
ALNV134N2_Text.indb 231ALNV134N2_Text.indb 231 29-Dec-20 19:44:0329-Dec-20 19:44:03
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

232 Anesthesiology 2021; 134:219–33
PERIOPERATIVE MEDICINE
Koyanagi et al.
ndings may elucidate some of the mechanisms at the cel-lular level for how anesthetics and pathophysiological status cause a certain EEG pattern in humans.
Acknowledgments
The authors thank Drs. Keisuke Kaneko, D.D.S., Ph.D., and Kiyofumi Yamamoto, Ph.D., Department of Pharmacology, Nihon University School of Dentistry, Tokyo, Japan, for their excellent technical support with the experiments. Vesicular GABA transporter – Venus transgenic rats were generated by Yuchio Yanagawa, M.D., Ph.D., Department of Genetic and Behavioral Neuroscience, Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan; Masumi Hirabayashi, Ph.D., Section of Mammalian Transgenesis, Center for Genetic Analysis of Behavior, National Institute for Physiological Sciences, Okazaki, Japan; and Yasuo Kawaguchi, M.D., Ph.D., Division of Cerebral Circuitry, National Institute for Physiological Sciences, Okazaki, Japan, using pCS2-Venus provided by Atsushi Miyawaki, M.D., Ph.D., Laboratory for Cell Function and Dynamics, Brain Science Institute, RIKEN, Wako, Japan.
Research Support
This work was supported by Grant-in-Aid for Scienti c Research Nos. 15K20561 and 18K09731 (to Dr. Koyanagi), 16K11765 and 19K10345 (to Dr. Oi), and 16H05507 and 19H03821 (to Dr. Kobayashi) from the Japan Society for the Promotion of Science, Tokyo, Japan, and by the Sato Fund and research grants from the Dental Research Center, Nihon University School of Dentistry, Tokyo, Japan.
Competing Interests
The authors declare no competing interests.
Correspondence
Address correspondence to Dr. Kobayashi: Nihon University School of Dentistry, 1-8-13 Kanda-Surugadai, Chiyoda-ku, Tokyo 101-8310, Japan. [email protected] . A nesthesiology ’ s articles are made freely accessible to all readers on www.anesthesiology.org, for personal use only, 6 months from the cover date of the issue.
References
1. Ching S , Cimenser A , Purdon PL , Brown EN , Kopell NJ : Thalamocortical model for a propofol-induced alpha-rhythm associated with loss of consciousness. Proc Natl Acad Sci USA 2010 ; 107 : 22665 – 70
2. Purdon PL , Pierce ET , Mukamel EA , Prerau MJ , Walsh JL , Wong KF , Salazar-Gomez AF , Harrell PG , Sampson AL , Cimenser A , Ching S , Kopell NJ , Tavares-Stoeckel C , Habeeb K , Merhar R , Brown EN : Electroencephalogram signatures of loss and recovery
of consciousness from propofol. Proc Natl Acad Sci USA 2013 ; 110 : E1142 – 51
3. Feshchenko VA , Veselis RA , Reinsel RA : Propofol-induced alpha rhythm. Neuropsychobiology 2004 ; 50 : 257 – 66
4. Cimenser A , Purdon PL , Pierce ET , Walsh JL , Salazar-Gomez AF , Harrell PG , Tavares-Stoeckel C , Habeeb K , Brown EN : Tracking brain states under general anes-thesia by using global coherence analysis. Proc Natl Acad Sci USA 2011 ; 108 : 8832 – 7
5. Vijayan S , Kopell NJ : Thalamic model of awake alpha oscillations and implications for stimulus processing. Proc Natl Acad Sci USA 2012 ; 109 : 18553 – 8
6. Vijayan S , Ching S , Purdon PL , Brown EN , Kopell NJ : Thalamocortical mechanisms for the anteriorization of α rhythms during propofol-induced unconsciousness. J Neurosci 2013 ; 33 : 11070 – 5
7. Martella G , De Persis C , Bonsi P , Natoli S , Cuomo D , Bernardi G , Calabresi P , Pisani A : Inhibition of per-sistent sodium current fraction and voltage-gated L-type calcium current by propofol in cortical neu-rons: Implications for its antiepileptic activity. Epilepsia 2005 ; 46 : 624 – 35
8. Ratnakumari L , Hemmings HC Jr : E ects of propo-fol on sodium channel – dependent sodium in ux and glutamate release in rat cerebrocortical synaptosomes. A nesthesiology 1997 ; 86 : 428 – 39
9. Cacheaux LP , Topf N , Tibbs GR , Schaefer UR , Levi R , Harrison NL , Abbott GW , Goldstein PA : Impairment of hyperpolarization-activated, cyclic nucleotide-gated channel function by the intravenous general anesthetic propofol. J Pharmacol Exp Ther 2005 ; 315 : 517 – 25
10. Chen X , Shu S , Bayliss DA : Suppression of I h contrib-utes to propofol-induced inhibition of mouse cortical pyramidal neurons. J Neurophysiol 2005 ; 94 : 3872 – 83
11. Kitamura A , Marszalec W , Yeh JZ , Narahashi T : E ects of halothane and propofol on excitatory and inhibi-tory synaptic transmission in rat cortical neurons. J Pharmacol Exp Ther 2003 ; 304 : 162 – 71
12. Kaneko K , Koyanagi Y , Oi Y , Kobayashi M : Propofol-induced spike ring suppression is more pronounced in pyramidal neurons than in fast-spiking neurons in the rat insular cortex. Neuroscience 2016 ; 339 : 548 – 60
13. Kawaguchi Y , Kondo S : Parvalbumin, somatostatin and cholecystokinin as chemical markers for speci c GABAergic interneuron types in the rat frontal cortex. J Neurocytol 2002 ; 31 : 277 – 87
14. Kubota Y , Hattori R , Yui Y : Three distinct subpopula-tions of GABAergic neurons in rat frontal agranular cortex. Brain Res 1994 ; 649 : 159 – 73
15. Kawaguchi Y , Kubota Y : GABAergic cell subtypes and their synaptic connections in rat frontal cortex. Cereb Cortex 1997 ; 7 : 476 – 86
16. Koyanagi Y , Oi Y , Yamamoto K , Koshikawa N , Kobayashi M : Fast-spiking cell to pyramidal cell
ALNV134N2_Text.indb 232ALNV134N2_Text.indb 232 29-Dec-20 19:44:0329-Dec-20 19:44:03
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:219–33 233
Propofol Facilitates Spike Synchrony
Koyanagi et al.
connections are the most sensitive to propofol-induced facilitation of GABAergic currents in rat insular cortex. A nesthesiology 2014 ; 121 : 68 – 78
17. Yamamoto K , Takei H , Koyanagi Y , Koshikawa N , Kobayashi M : Presynaptic cell type-dependent regu-lation of GABAergic synaptic transmission by nitric oxide in rat insular cortex. Neuroscience 2015 ; 284 : 65 – 77
18. Uematsu M , Hirai Y , Karube F , Ebihara S , Kato M , Abe K , Obata K , Yoshida S , Hirabayashi M , Yanagawa Y , Kawaguchi Y : Quantitative chemical composition of cortical GABAergic neurons revealed in transgenic Venus-expressing rats. Cereb Cortex 2008 ; 18 : 315 – 30
19. Koyanagi Y , Yamamoto K , Oi Y , Koshikawa N , Kobayashi M : Presynaptic interneuron subtype- and age-dependent modulation of GABAergic synaptic transmission by β -adrenoceptors in rat insular cortex. J Neurophysiol 2010 ; 103 : 2876 – 88
20. Pfe er CK , Xue M , He M , Huang ZJ , Scanziani M : Inhibition of inhibition in visual cortex: The logic of connections between molecularly distinct interneu-rons. Nat Neurosci 2013 ; 16 : 1068 – 76
21. Kato R , Yamanaka M , Yokota E , Koshikawa N , Kobayashi M : Spike timing rigidity is maintained in bursting neurons under pentobarbital-induced anesthetic conditions. Front Neural Circuits 2016 ; 10 : 86
22. Cardin JA , Carl é n M , Meletis K , Knoblich U , Zhang F , Deisseroth K , Tsai LH , Moore CI : Driving fast-spik-ing cells induces gamma rhythm and controls sensory responses. Nature 2009 ; 459 : 663 – 7
23. Ryan SJ , Ehrlich DE , Jasnow AM , Daftary S , Madsen TE , Rainnie DG : Spike-timing precision and neuro-nal synchrony are enhanced by an interaction between synaptic inhibition and membrane oscillations in the amygdala. PLoS One 2012 ; 7 : e35320
24. Hu H , Ma Y , Agmon A : Submillisecond ring syn-chrony between di erent subtypes of cortical inter-neurons connected chemically but not electrically. J Neurosci 2011 ; 31 : 3351 – 61
25. Gibson JR , Beierlein M , Connors BW : Two networks of electrically coupled inhibitory neurons in neocor-tex. Nature 1999 ; 402 : 75 – 9
26. Galarreta M , Hestrin S : A network of fast-spiking cells in the neocortex connected by electrical synapses. Nature 1999 ; 402 : 72 – 5
27. Petersen CC , Crochet S : Synaptic computation and sensory processing in neocortical layer 2/3. Neuron 2013 ; 78 : 28 – 48
28. Ching S , Brown EN : Modeling the dynamical e ects of anesthesia on brain circuits. Curr Opin Neurobiol 2014 ; 25 : 116 – 22
29. Bacci A , Huguenard JR : Enhancement of spike-timing precision by autaptic transmission in neocortical inhib-itory interneurons. Neuron 2006 ; 49 : 119 – 30
30. Bacci A , Huguenard JR , Prince DA : Functional autap-tic neurotransmission in fast-spiking interneurons: A novel form of feedback inhibition in the neocortex. J Neurosci 2003 ; 23 : 859 – 66
31. Kaplan PW , Genoud D , Ho TW , Jallon P : Etiology, neu-rologic correlations, and prognosis in alpha coma. Clin Neurophysiol 1999 ; 110 : 205 – 13
ALNV134N2_Text.indb 233ALNV134N2_Text.indb 233 29-Dec-20 19:44:0329-Dec-20 19:44:03
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
PERIOPERATIVE MEDICINE
234 FEBRUARY 2021 ANESTHESIOLOGY, V 134 • NO 2
ABSTRACT Background: Pharmacologic modulation has previously shown that tran-sient receptor potential canonical (TRPC) channels play an important role in the pathogenesis of malignant hyperthermia. This study tested the hypothesis that genetically suppressing the function of TRPC6 can partially ameliorate muscle cation dyshomeostasis and the response to halothane in a mouse model relevant to malignant hyperthermia.
Methods: This study examined the effect of overexpressing a muscle-spe-cifi c nonconducting dominant-negative TRPC6 channel in 20 RYR1 -p.R163C and 20 wild-type mice and an equal number of nonexpressing controls, using calcium- and sodium-selective microelectrodes and Western blots.
Results: RYR1- p.R163C mouse muscles have chronically elevated intracel-lular calcium and sodium levels compared to wild-type muscles. Transgenic expression of the nonconducting TRPC6 channel reduced intracellular cal-cium from 331 ± 34 nM (mean ± SD) to 190 ± 27 nM ( P < 0.0001) and sodium from 15 ± 1 mM to 11 ± 1 mM ( P < 0.0001). Its expression lowered the increase in intracellular Ca 2 + of the TRPC6-specifi c activator hyperforin in RYR1- p.R163C muscle fi bers from 52% (348 ± 37 nM to 537 ± 70 nM) to 14% (185 ± 11 nM to 210 ± 44 nM). Western blot analysis of TRPC3 and TRPC6 expression showed the expected increase in TRPC6 caused by over-expression of its dominant-negative transgene and a compensatory increase in expression of TRPC3. Although expression of the muscle-specifi c domi-nant-negative TRPC6 was able to modulate the increase in intracellular cal-cium during halothane exposure and prolonged life (35 ± 5 min vs. 15 ± 3 min; P < 0.0001), a slow, steady increase in calcium began after 20 min of halothane exposure, which eventually led to death.
Conclusions: These data support previous fi ndings that TRPC channels play an important role in causing the intracellular calcium and sodium dysho-meostasis associated with RYR1 variants that are pathogenic for malignant hyperthermia. However, they also show that modulating TRPC channels alone is not suffi cient to prevent the lethal effect of exposure to volatile anesthetic malignant hyperthermia – triggering agents.
(ANESTHESIOLOGY 2021 ; 134 : 234 – 47 )
Molecular Modifi cation of Transient Receptor Potential Canonical 6 Channels Modulates Calcium Dyshomeostasis in a Mouse Model Relevant to Malignant Hyperthermia Jose Rafael Lopez , M.D., Ph.D. , Arkady Uryash , M.D., Ph.D. , Jose Adams , M.D. , Philip M. Hopkins , M.D., F.R.C.A. , Paul D. Allen , M.D., Ph.D.
ANESTHESIOLOGY 2021 ; 134 : 234 – 47
Supplemental Digital Content is available for this article. Direct URL citations appear in the printed text and are available in both the HTML and PDF versions of this article. Links to the digital fi les are provided in the HTML text of this article on the Journal ’ s Web site (www.anesthesiology.org).
Submitted for publication July 21, 2020. Accepted for publication October 29, 2020. Published online fi rst on December 10, 2020. From the Department of Molecular Biosciences, University of California at Davis, Davis, California (J.R.L., P.D.A.); the Departments of Research (J.R.L.) and Neonatology (A.U., J.A.), Mount Sinai Medical Center, Miami Beach, Florida; and the Institute of Medical Research at St. James ’ s University Hospital, University of Leeds, Leeds, United Kingdom (P.M.H., P.D.A.).
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved. Anesthesiology 2021 ; 134 : 234 – 47 . DOI: 10.1097/ALN.0000000000003635
EDITOR ’ S PERSPECTIVE
What We Already Know about This Topic
• The type 1 ryanodine receptor ( RYR1 ) gene encoding the skeletal muscle sarcoplasmic reticulum Ca 2 + release channel is the primary locus for malignant hyperthermia susceptibility
• Secondary loci have been identified in other proteins involved with RyR1 in excitation – contraction coupling that are thought to sensi-tize the RyR1 channel
• Transient receptor potential canonical channels constitute a large and functionally versatile superfamily of cation channel proteins expressed in many cell types that control influxes of Ca 2 + and other cations to regulate diverse cellular processes
What This Article Tells Us That Is New
• Muscle-specific overexpression of the nonconducting transient receptor potential canonical 6 channel both reduced intracellular Ca 2 + concentration in RYR1-p.R163C mice at rest and reduced the absolute maximum levels of intracellular Ca 2 + concentration reached during exposure to halothane
• Despite this, its overexpression did not restore intracellular Ca 2 +
concentration to wild-type levels, and although its overexpression increased the length of survival after halothane exposure, it was unable to rescue the lethal phenotype
Malignant hyperthermia (MH) is an autosomal dom-inant hypermetabolic condition triggered by vol-
atile anesthetics, such as iso urane and succinylcholine. 1 – 4
Molecular genetic studies have established the type 1 ryan-odine receptor gene ( RYR1 ) encoding the skeletal muscle sarcoplasmic reticulum Ca 2 + release channel as the primary locus for both MH susceptibility and central core disease. 2 – 6
A common characteristic of muscle expressing MH- RYR1 variants, both in patients 7 and in experimental models, 8 – 12 is an increased intracellular Ca 2 + concentration compared to muscle from nonsusceptible subjects. In three experimental
ALNV134N2_Text.indb 234ALNV134N2_Text.indb 234 29-Dec-20 19:44:0329-Dec-20 19:44:03
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:234–47 235
TRPC6 Modulation in Malignant Hyperthermia
Lopez et al.
murine models of MH with variants in RYR1 that are known to be pathogenic in humans, we have shown that exposure to halothane or iso urane at clinically relevant concentrations causes intracellular Ca 2 + concentration to rise several-fold in their muscles, whereas exposure to the same concentrations of halothane or iso urane has no e ect in muscles from mice without RYR1 variants. 10 – 12 Previously, we introduced a new paradigm that implicates nonspeci c sarcolemmal cation entry via transient receptor potential canonical (TRPC) channels both as the predominant source of acutely elevated intracellular Ca 2 + and sodium concentra-tion during fulminant MH and as important contributors to chronically elevated intracellular Ca 2 + and sodium concen-trations in quiescent MH-susceptible muscles. 13 , 14
Our aim in this study was to use molecular methods in combination with pharmacologic agents to further test the primary hypothesis that TRPC3 and TRPC6 channels are directly responsible for the high intracellular Ca 2 + concentra-tion seen in resting MH-susceptible muscles, with a secondary hypothesis that blocking TRPC6 could prevent the massively elevated intracellular Ca 2 + concentration observed during the MH crisis after exposure to triggering agents and sub-sequent death. We have done this using our RYR1 -p.R163C knock-in murine model of MH 10 crossed with a transgenic animal overexpressing a dominant-negative nonconducting TRPC6 channel in their skeletal muscles. 15 , 16 This transgene exerts its e ect by blocking the activity of TRPC6 and per-haps also by modulating TRPC3 because these two closely related TRPC channel isoforms are known to form hetero-tetramers at the plasma membrane. 17 In a previous study in two murine models of muscular dystrophy, expressing this nonconducting channel relieved their muscle pathology and restored muscle function to near normal levels. 15
Materials and Methods
Animals
The animals used in this study were (1) wild-type C57BL/6J mice, (2) C57BL/6J knock-in mice heterozygous for the RYR1 variant resulting in the amino acid change p.R163C in the RyR1 protein (R163C), (3) transgenic mice with skeletal muscle – speci c overexpression of a nonconducting TRPC6 channel, 15 and (4) mice heterozygous for RYR1 -p.R163C with skeletal muscle – speci c expression of a non-conducting TRPC6 channel (the result of crossing RYR1 -p.R163C with mice with skeletal muscle – speci c expression of a nonconducting TRPC6 channel). The mice were used as close as possible to the time they achieved 3 months of age. In all, 91 mice (39 females and 52 males) were used as experimental animals. The animals for any phase of the study were chosen by their date of birth (oldest rst) and their availability in the animal colony. All experimental procedures on animals were in accordance with the Care and Use Handbook of Laboratory Animals published by the U.S. National Institutes of Health (Bethesda, Maryland;
publication No. 85-23, revised 1996) and approved by the Institutional Animal Care and Use Committees at the University of California at Davis, Davis, California; the Mount Sinai Hospital, Miami Beach, Florida, and the Home O ce in the United Kingdom (London).
Experimental Preparations
The experiments were conducted (1) in vitro using single muscle bers obtained by enzymatic digestion of exor digitorum brevis muscles dissected from 3- to 5-month-old anesthetized mice killed by cervical dislocation; 18 with exor digitorum brevis bers used for measurements of intracellular ion concentrations 4 to 6 h after isolation; or (2) in vivo by measurement of intracellular ion concentra-tions in surgically exposed vastus lateralis bers of mice anesthetized using a mixture of intraperitoneal ketamine (100 mg/kg) and xylazine (5 mg/kg). 13
Ca 2 + - and Sodium-selective Microelectrodes
Double-barreled Ca 2 + - and sodium -selective microelec-trodes were prepared and individually calibrated before and after the determination of intracellular calcium concen-tration or intracellular sodium concentration as described previously. 13 , 19 Only those Ca 2 + selective microelectrodes with a linear relationship between one micromolar and one hundred nanomolar (Nernstian response, 30.5 milivolts per negative logarithm of the calcium concentration unit) or those sodium microelectrodes with Nernstian responses between 100 and 10 mM and a sub-Nernstian response (40 to 45 millivolts) between 1 and 10 mM were used experi-mentally. The sensitivity of the Ca 2 + - and sodium -selective microelectrodes were not a ected by any of the drugs used in the current study. After making measurements of rest-ing intracellular free calcium concentration for [Ca 2+ ]
r and
resting intracellular sodium concentration for [Na + ] r , all
microelectrodes were recalibrated, and if the two calibra-tion curves did not agree within 5 millivolts, data from that microelectrode were discarded. This resulted in the removal of the data of 11 animals from the nal analysis.
Recording of Intracellular Ca 2 + and Sodium in Muscle Fibers In Vitro and In Vivo Intracellular Ca 2 + and sodium determinations were per-formed in vitro on single exor digitorum brevis muscle bers as described previously 18 and in vivo on vastus later-alis bers in anesthetized wild-type and RYR1 -p.R163C mice. 10 The muscle bers were impaled with double-bar-reled Ca 2 + -selective or sodium-selective microelectrodes, and their potentials were recorded via a high-impedance ampli er (WPI Duo 773 electrometer; WPI, USA). 10 The data were not collected in any muscle cell whose mem-brane potential was less negative than minus 80 millivolts, and if that occurred at any time during the experiment, the data for that cell were not used for analysis.
ALNV134N2_Text.indb 235ALNV134N2_Text.indb 235 29-Dec-20 19:44:0329-Dec-20 19:44:03
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

236 Anesthesiology 2021; 134:234–47
PERIOPERATIVE MEDICINE
Lopez et al.
The resting membrane potential from the 3 M KCl microelectrode was subtracted electronically from either the potential of the Ca 2 + microelectrode or the sodium micro-electrode to produce a di erential Ca 2 + -speci c potential or sodium-speci c potential that represents the intracellu-lar Ca 2 + or intracellular sodium concentrations, respectively. All voltage signals were stored in a computer for further analysis. Solutions . Normal Ringer solution contained 135 mM NaCl, 5 mM KCl, 1.8 mM CaCl
2 , 1 mM MgCl
2 , 18 mM
NaHCO 3 , 1.5 mM NaH
2 PO, and 5 mM glucose, pH 7.2 to
7.3. 1-Oleoyl-2-acetyl- sn -glycerol, ethyl-1-(4-(2,3,3-tri-chloroacrylamide)phenyl)-5-(tri uoromethyl)-1H-pyra-zole-4-carboxylate, and hyperforin solutions were made by adding the desired concentration of the reagent to normal Ringer solution. All in vitro experiments were performed at 37 ° C. Halothane Survival Curve . To investigate the e ects of over-expressing a dominant-negative nonconducting TRPC6 in RYR1 -p.R163C mice on the response to exposure to 2% halothane, we conducted a survival study on cohorts (7 mice per group) of 8- to 12-week-old wild-type, wild-type/dominant-negative TRPC6, RYR1 -p.R163C, and RYR1 -p.R163C/dominant-negative TRPC6 mice. Survival time was measured during an up to 60-min expo-sure to 2% halothane. Western Blot Analysis of Protein Expression . Gastrocnemius muscles from all genotypes were dissected, minced, and homogenized in modi ed radioimmunoassay precipita-tion assay bu er as described before. 20 Total protein con-centration was determined using the Pierce BCA protein assay kit (Thermo-Fisher Scienti c, USA). Proteins were separated on sodiumdodecylsulfate gel and transferred to nitrocellulose membrane. To avoid having errors added by attempting to measure all of the proteins on a single gel, by stripping the antibodies after making the rst measure-ment, we performed the analysis by rst slicing each mem-brane horizontally according to the molecular weight of proteins of interest. Each individual membrane strip was incubated with the primary anti-TRPC3, -TRPC6, and – glyceraldehyde-3-phosphate dehydrogenase antibodies based on the known protein size and protein standard markers. The levels of TRPC proteins were normalized to loading control using the housekeeping protein glyceralde-hyde-3-phosphate dehydrogenase. Each strip from a single gel is shown as the example. Gels for each sample were run in triplicate and incubated with primary TRPC3, TRPC6, or glyceraldehyde-3-phosphate dehydrogenase followed by secondary uorescent antibodies (Abcam, USA). All antibody dilutions and signals were validated previously in our laboratory and by others. 14 , 21 Signals of the protein of interest were detected with Storm 860 uorescent imag-ing system (GE Bio-Sciences, USA). Protein signals were quanti ed using MyImageAnalysis software (Thermo-Fisher Scienti c), and the density of the TRPC proteins
was normalized to the density of glyceraldehyde-3-phos-phate dehydrogenase expression, which is thought not to be di erentially expressed in these models.
Statistics
No speci c power calculation was conducted before experimentation. The sample sizes used were based on our previous studies using other MH and non-MH animal models. Randomization methods were not used to assign the animals to be studied, and blinding of the investiga-tors was not used. All values are expressed as means ± SD . Statistical analysis used two-tailed hypothesis testing. For studies done on muscle bers both in vitro and in vivo , a one-way between-subjects ANOVA was performed with Tukey ’ s posttest for multiple measurements to determine signi cance ( P < 0.05). We used histograms (most com-monly used graph to show frequency distributions) and the D ’ Agostino and Pearson test to assess the distribution of the data. Statistical analyses of Western blots were carried out using an unpaired Student ’ s independent t test. To do this, we used an independent samples t test; namely, we com-pared two sample means from di erent populations regard-ing the same variable. The Mantel – Cox test was used to test for di erences in survival between groups. All data col-lected were analyzed, and no outliers were removed from our analyses. Statistical analysis was done using GraphPad Prism 7.03 (GraphPad Software, Inc., USA). Data from 11 mice were discarded because of (1) the loss of microelec-trode sensitivity to calcium detected by a drift of more than 5 millivolts between the rst and the second microelectrode calibration curves in the range between pCa 6 and pCa 7; (2) broken microelectrode tips that did not allow us to carry out the postmeasurement calibration curves; and (3) the unexpected occurrence of electronic noise during the ion measurements that compromised the accuracy of the ion-speci c voltage recorded.
Results
Intracellular Ca 2 + and Sodium Concentrations in Muscle Fibers Expressing a Dominant-negative TRPC6 Channel
In vivo intracellular Ca 2 + concentrations were 175% higher and intracellular sodium concentrations were 88% higher in RYR1 -p.R163C vastus lateralis muscle bers than those observed in wild-type muscle bers ( P < 0.0001; g. 1 ). Expression of the dominant-negative TRPC6 reduced skeletal muscle intracellular Ca 2 + and sodium concentra-tions in both wild-type and RYR1- p.R163C mice; how-ever, the decreases caused by its expression were greater in RYR1- p.R163C/dominant-negative TRPC6 than in wild-type/dominant-negative TRPC6 mice (43% [ P < 0.0001] vs. 21% [ P < 0.0001] and 27% [ P < 0.001] vs. 11% [ P = 0.002] for intracellular Ca 2 + and sodium con-centrations, respectively; g. 1 ). There were no di erences
ALNV134N2_Text.indb 236ALNV134N2_Text.indb 236 29-Dec-20 19:44:0329-Dec-20 19:44:03
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
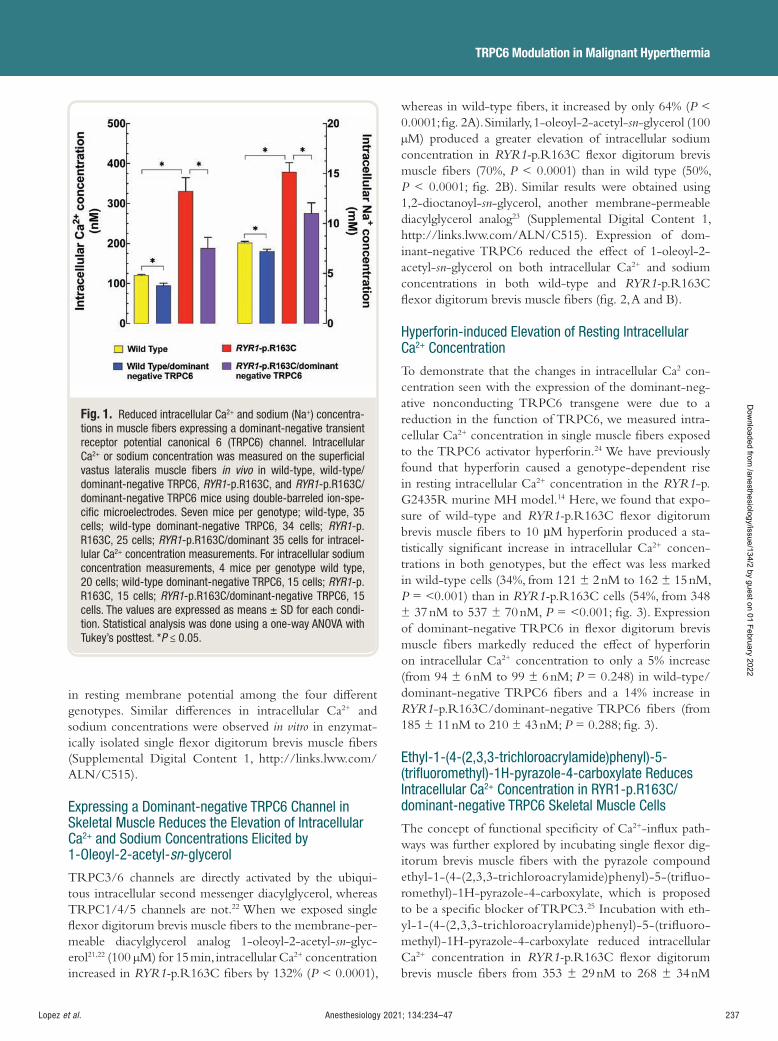
Anesthesiology 2021; 134:234–47 237
TRPC6 Modulation in Malignant Hyperthermia
Lopez et al.
in resting membrane potential among the four di erent genotypes. Similar di erences in intracellular Ca 2 + and sodium concentrations were observed in vitro in enzymat-ically isolated single exor digitorum brevis muscle bers (Supplemental Digital Content 1, http://links.lww.com/ALN/C515).
Expressing a Dominant-negative TRPC6 Channel in Skeletal Muscle Reduces the Elevation of Intracellular Ca 2 + and Sodium Concentrations Elicited by 1-Oleoyl-2-acetyl- sn -glycerol
TRPC3/6 channels are directly activated by the ubiqui-tous intracellular second messenger diacylglycerol, whereas TRPC1/4/5 channels are not. 22 When we exposed single exor digitorum brevis muscle bers to the membrane-per-meable diacylglycerol analog 1-oleoyl-2-acetyl- sn -glyc-erol 21 , 22 (100 μ M) for 15 min, intracellular Ca 2 + concentration increased in RYR1- p.R163C bers by 132% ( P < 0.0001),
whereas in wild-type bers, it increased by only 64% ( P < 0.0001; g. 2A ). Similarly, 1-oleoyl-2-acetyl- sn -glycerol (100 μ M) produced a greater elevation of intracellular sodium concentration in RYR1- p.R163C exor digitorum brevis muscle bers (70%, P < 0.0001) than in wild type (50%, P < 0.0001; g. 2B ). Similar results were obtained using 1,2-dioctanoyl- sn -glycerol, another membrane-permeable diacylglycerol analog 23 (Supplemental Digital Content 1, http://links.lww.com/ALN/C515). Expression of dom-inant-negative TRPC6 reduced the e ect of 1-oleoyl-2-acetyl- sn -glycerol on both intracellular Ca 2 + and sodium concentrations in both wild-type and RYR1- p.R163C exor digitorum brevis muscle bers ( g. 2 , A and B).
Hyperforin-induced Elevation of Resting Intracellular Ca 2 + Concentration
To demonstrate that the changes in intracellular Ca 2 con-centration seen with the expression of the dominant-neg-ative nonconducting TRPC6 transgene were due to a reduction in the function of TRPC6, we measured intra-cellular Ca 2 + concentration in single muscle bers exposed to the TRPC6 activator hyperforin. 24 We have previously found that hyperforin caused a genotype-dependent rise in resting intracellular Ca 2 + concentration in the RYR1 -p.G2435R murine MH model. 14 Here, we found that expo-sure of wild-type and RYR1- p.R163C exor digitorum brevis muscle bers to 10 µ M hyperforin produced a sta-tistically signi cant increase in intracellular Ca 2 + concen-trations in both genotypes, but the e ect was less marked in wild-type cells (34%, from 121 ± 2 nM to 162 ± 15 nM, P = < 0.001) than in RYR1- p.R163C cells (54%, from 348 ± 37 nM to 537 ± 70 nM, P = < 0.001; g. 3 ). Expression of dominant-negative TRPC6 in exor digitorum brevis muscle bers markedly reduced the e ect of hyperforin on intracellular Ca 2 + concentration to only a 5% increase (from 94 ± 6 nM to 99 ± 6 nM; P = 0.248) in wild-type/dominant-negative TRPC6 bers and a 14% increase in RYR1 -p.R163C/dominant-negative TRPC6 bers (from 185 ± 11 nM to 210 ± 43 nM; P = 0.288; g. 3 ).
Ethyl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(trifl uoromethyl)-1H-pyrazole-4-carboxylate Reduces Intracellular Ca 2 + Concentration in RYR1-p.R163C/dominant-negative TRPC6 Skeletal Muscle Cells
The concept of functional speci city of Ca 2 + -in ux path-ways was further explored by incubating single exor dig-itorum brevis muscle bers with the pyrazole compound ethyl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(tri uo-romethyl)-1H-pyrazole-4-carboxylate, which is proposed to be a speci c blocker of TRPC3. 25 Incubation with eth-yl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(tri uoro-methyl)-1H-pyrazole-4-carboxylate reduced intracellular Ca 2 + concentration in RYR1- p.R163C exor digitorum brevis muscle bers from 353 ± 29 nM to 268 ± 34 nM
Fig. 1. Reduced intracellular Ca 2 + and sodium (Na + ) concentra-tions in muscle fi bers expressing a dominant-negative transient receptor potential canonical 6 (TRPC6) channel. Intracellular Ca 2 + or sodium concentration was measured on the superfi cial vastus lateralis muscle fi bers in vivo in wild-type, wild-type/dominant-negative TRPC6, RYR1 -p.R163C, and RYR1 -p.R163C/dominant-negative TRPC6 mice using double-barreled ion-spe-cifi c microelectrodes. Seven mice per genotype; wild-type, 35 cells; wild-type dominant-negative TRPC6, 34 cells; RYR1 -p.R163C, 25 cells; RYR1 -p.R163C/dominant 35 cells for intracel-lular Ca 2 + concentration measurements. For intracellular sodium concentration measurements, 4 mice per genotype wild type, 20 cells; wild-type dominant-negative TRPC6, 15 cells; RYR1 -p.R163C, 15 cells; RYR1 -p.R163C/dominant-negative TRPC6, 15 cells. The values are expressed as means ± SD for each condi-tion. Statistical analysis was done using a one-way ANOVA with Tukey ’ s posttest. * P ≤ 0.05.
ALNV134N2_Text.indb 237ALNV134N2_Text.indb 237 29-Dec-20 19:44:0429-Dec-20 19:44:04
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
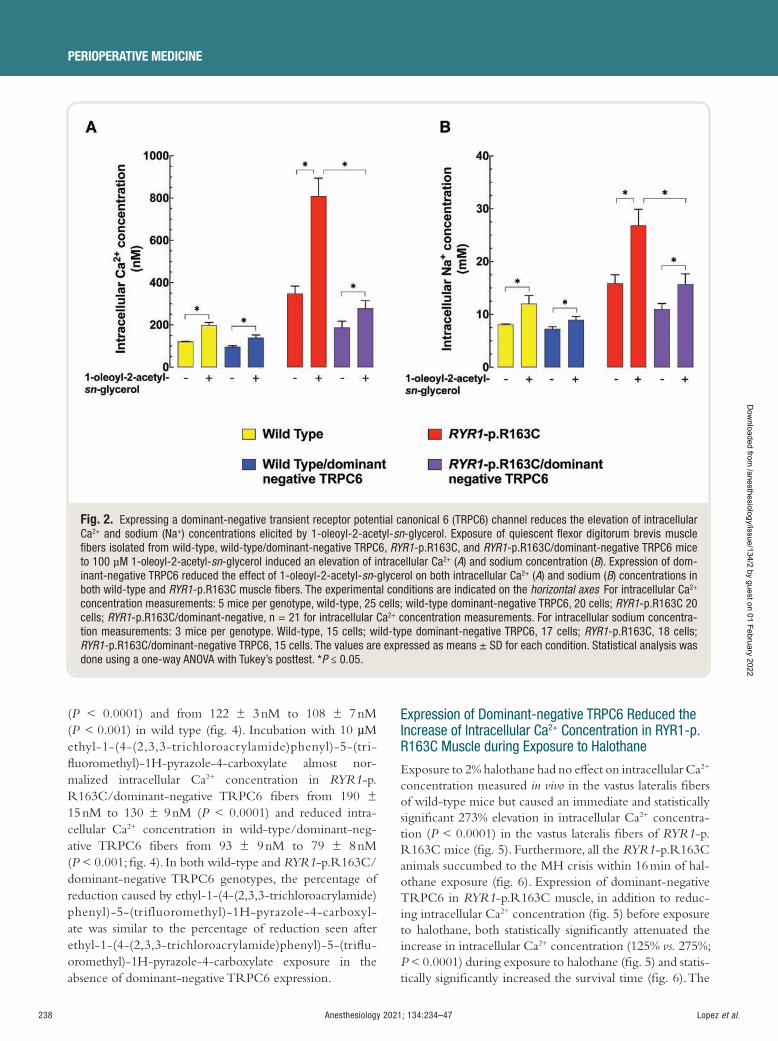
238 Anesthesiology 2021; 134:234–47
PERIOPERATIVE MEDICINE
Lopez et al.
( P < 0.0001) and from 122 ± 3 nM to 108 ± 7 nM ( P < 0.001) in wild type ( g. 4 ). Incubation with 10 µ M ethyl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(tri- uoromethyl)-1H-pyrazole-4-carboxylate almost nor-malized intracellular Ca 2 + concentration in RYR1 -p.R163C/dominant-negative TRPC6 bers from 190 ± 15 nM to 130 ± 9 nM ( P < 0.0001) and reduced intra-cellular Ca 2 + concentration in wild-type/dominant-neg-ative TRPC6 bers from 93 ± 9 nM to 79 ± 8 nM ( P < 0.001; g. 4 ). In both wild-type and RYR1 -p.R163C/dominant-negative TRPC6 genotypes, the percentage of reduction caused by ethyl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(trifluoromethyl)-1H-pyrazole-4-carboxyl-ate was similar to the percentage of reduction seen after ethyl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(tri u-oromethyl)-1H-pyrazole-4-carboxylate exposure in the absence of dominant-negative TRPC6 expression.
Expression of Dominant-negative TRPC6 Reduced the Increase of Intracellular Ca 2 + Concentration in RYR1-p.R163C Muscle during Exposure to Halothane
Exposure to 2% halothane had no e ect on intracellular Ca 2 +
concentration measured in vivo in the vastus lateralis bers of wild-type mice but caused an immediate and statistically signi cant 273% elevation in intracellular Ca 2 + concentra-tion ( P < 0.0001) in the vastus lateralis bers of RYR1 -p.R163C mice ( g. 5 ). Furthermore, all the RYR1 -p.R163C animals succumbed to the MH crisis within 16 min of hal-othane exposure ( g. 6 ). Expression of dominant-negative TRPC6 in RYR1 -p.R163C muscle, in addition to reduc-ing intracellular Ca 2 + concentration ( g. 5 ) before exposure to halothane, both statistically signi cantly attenuated the increase in intracellular Ca 2 + concentration (125% vs. 275%; P < 0.0001) during exposure to halothane ( g. 5 ) and statis-tically signi cantly increased the survival time ( g. 6 ). The
Fig. 2. Expressing a dominant-negative transient receptor potential canonical 6 (TRPC6) channel reduces the elevation of intracellular Ca 2 + and sodium (Na + ) concentrations elicited by 1-oleoyl-2-acetyl- sn -glycerol. Exposure of quiescent fl exor digitorum brevis muscle fi bers isolated from wild-type, wild-type/dominant-negative TRPC6, RYR1 -p.R163C, and RYR1 -p.R163C/dominant-negative TRPC6 mice to 100 µ M 1-oleoyl-2-acetyl- sn -glycerol induced an elevation of intracellular Ca 2 + ( A ) and sodium concentration ( B ). Expression of dom-inant-negative TRPC6 reduced the effect of 1-oleoyl-2-acetyl- sn -glycerol on both intracellular Ca 2 + ( A ) and sodium ( B ) concentrations in both wild-type and RYR1 -p.R163C muscle fi bers. The experimental conditions are indicated on the horizontal axes . For intracellular Ca 2 +
concentration measurements: 5 mice per genotype, wild-type, 25 cells; wild-type dominant-negative TRPC6, 20 cells; RYR1 -p.R163C 20 cells; RYR1 -p.R163C/dominant-negative, n = 21 for intracellular Ca 2 + concentration measurements. For intracellular sodium concentra-tion measurements: 3 mice per genotype. Wild-type, 15 cells; wild-type dominant-negative TRPC6, 17 cells; RYR1 -p.R163C, 18 cells; RYR1 -p.R163C/dominant-negative TRPC6, 15 cells. The values are expressed as means ± SD for each condition. Statistical analysis was done using a one-way ANOVA with Tukey ’ s posttest. * P ≤ 0.05.
ALNV134N2_Text.indb 238ALNV134N2_Text.indb 238 29-Dec-20 19:44:0429-Dec-20 19:44:04
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
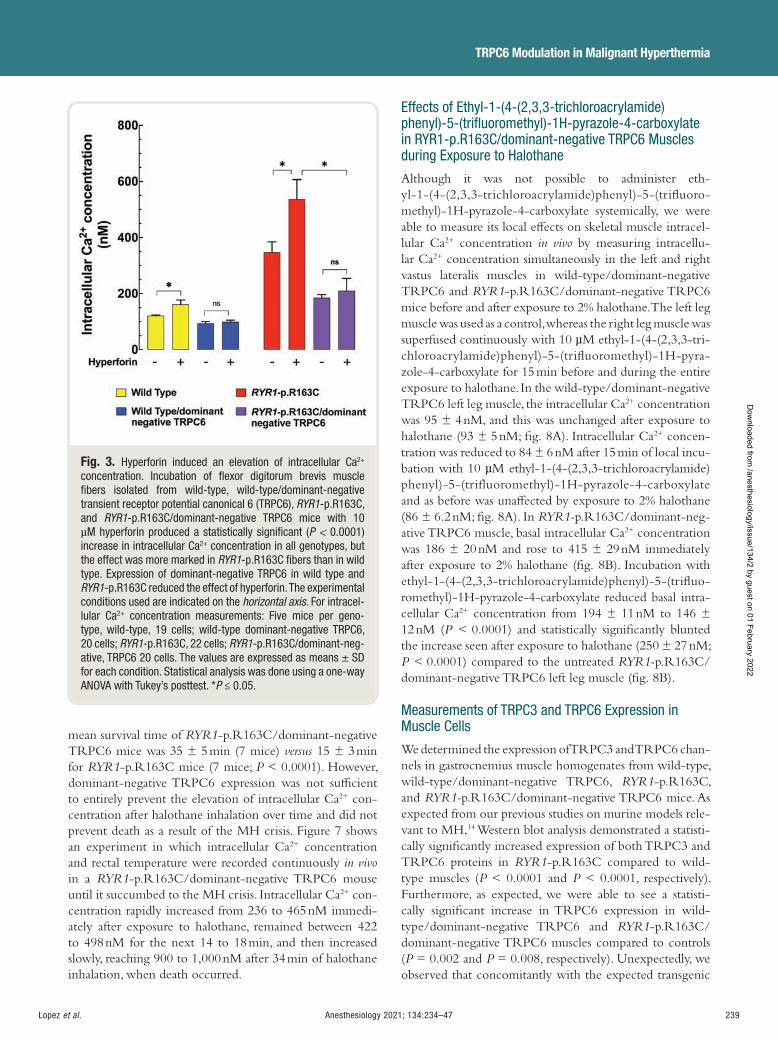
Anesthesiology 2021; 134:234–47 239
TRPC6 Modulation in Malignant Hyperthermia
Lopez et al.
mean survival time of RYR1 -p.R163C/dominant-negative TRPC6 mice was 35 ± 5 min ( 7 mice) versus 15 ± 3 min for RYR1 -p.R163C mice ( 7 mice; P < 0.0001). However, dominant-negative TRPC6 expression was not su cient to entirely prevent the elevation of intracellular Ca 2 + con-centration after halothane inhalation over time and did not prevent death as a result of the MH crisis. Figure 7 shows an experiment in which intracellular Ca 2 + concentration and rectal temperature were recorded continuously in vivo in a RYR1 -p.R163C/dominant-negative TRPC6 mouse until it succumbed to the MH crisis. Intracellular Ca 2 + con-centration rapidly increased from 236 to 465 nM immedi-ately after exposure to halothane, remained between 422 to 498 nM for the next 14 to 18 min, and then increased slowly, reaching 900 to 1,000 nM after 34 min of halothane inhalation, when death occurred.
Effects of Ethyl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(trifl uoromethyl)-1H-pyrazole-4-carboxylate in RYR1-p.R163C/dominant-negative TRPC6 Muscles during Exposure to Halothane
Although it was not possible to administer eth-yl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(tri uoro-methyl)-1H-pyrazole-4-carboxylate systemically, we were able to measure its local e ects on skeletal muscle intracel-lular Ca 2 + concentration in vivo by measuring intracellu-lar Ca 2 + concentration simultaneously in the left and right vastus lateralis muscles in wild-type/dominant-negative TRPC6 and RYR1 -p.R163C/dominant-negative TRPC6 mice before and after exposure to 2% halothane. The left leg muscle was used as a control, whereas the right leg muscle was superfused continuously with 10 µ M ethyl-1-(4-(2,3,3-tri-chloroacrylamide)phenyl)-5-(tri uoromethyl)-1H-pyra-zole-4-carboxylate for 15 min before and during the entire exposure to halothane. In the wild-type/dominant-negative TRPC6 left leg muscle, the intracellular Ca 2 + concentration was 95 ± 4 nM, and this was unchanged after exposure to halothane (93 ± 5 nM; g. 8A ). Intracellular Ca 2 + concen-tration was reduced to 84 ± 6 nM after 15 min of local incu-bation with 10 µ M ethyl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(trifluoromethyl)-1H-pyrazole-4-carboxylate and as before was una ected by exposure to 2% halothane (86 ± 6.2 nM; g. 8A ). In RYR1- p.R163C/dominant-neg-ative TRPC6 muscle, basal intracellular Ca 2 + concentration was 186 ± 20 nM and rose to 415 ± 29 nM immediately after exposure to 2% halothane ( g. 8B ). Incubation with ethyl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(tri uo-romethyl)-1H-pyrazole-4-carboxylate reduced basal intra-cellular Ca 2 + concentration from 194 ± 11 nM to 146 ± 12 nM ( P < 0.0001) and statistically signi cantly blunted the increase seen after exposure to halothane (250 ± 27 nM; P < 0.0001) compared to the untreated RYR1- p.R163C/dominant-negative TRPC6 left leg muscle ( g. 8B ).
Measurements of TRPC3 and TRPC6 Expression in Muscle Cells
We determined the expression of TRPC3 and TRPC6 chan-nels in gastrocnemius muscle homogenates from wild-type, wild-type/dominant-negative TRPC6, RYR1 -p.R163C, and RYR1- p.R163C/dominant-negative TRPC6 mice. As expected from our previous studies on murine models rele-vant to MH, 14 Western blot analysis demonstrated a statisti-cally signi cantly increased expression of both TRPC3 and TRPC6 proteins in RYR1 -p.R163C compared to wild-type muscles ( P < 0.0001 and P < 0.0001, respectively). Furthermore, as expected, we were able to see a statisti-cally signi cant increase in TRPC6 expression in wild-type/dominant-negative TRPC6 and RYR1 -p.R163C/dominant-negative TRPC6 muscles compared to controls ( P = 0.002 and P = 0.008, respectively). Unexpectedly, we observed that concomitantly with the expected transgenic
Fig. 3. Hyperforin induced an elevation of intracellular Ca 2 +
concentration. Incubation of fl exor digitorum brevis muscle fi bers isolated from wild-type, wild-type/dominant-negative transient receptor potential canonical 6 (TRPC6), RYR1 -p.R163C, and RYR1 -p.R163C/dominant-negative TRPC6 mice with 10 µ M hyperforin produced a statistically signifi cant ( P < 0.0001) increase in intracellular Ca 2 + concentration in all genotypes, but the effect was more marked in RYR1 -p.R163C fi bers than in wild type. Expression of dominant-negative TRPC6 in wild type and RYR1 -p.R163C reduced the effect of hyperforin. The experimental conditions used are indicated on the horizontal axis . For intracel-lular Ca 2 + concentration measurements: Five mice per geno-type, wild-type, 19 cells; wild-type dominant-negative TRPC6, 20 cells; RYR1 -p.R163C, 22 cells; RYR1 -p.R163C/dominant-neg-ative, TRPC6 20 cells. The values are expressed as means ± SD for each condition. Statistical analysis was done using a one-way ANOVA with Tukey ’ s posttest. * P ≤ 0.05.
ALNV134N2_Text.indb 239ALNV134N2_Text.indb 239 29-Dec-20 19:44:0529-Dec-20 19:44:05
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
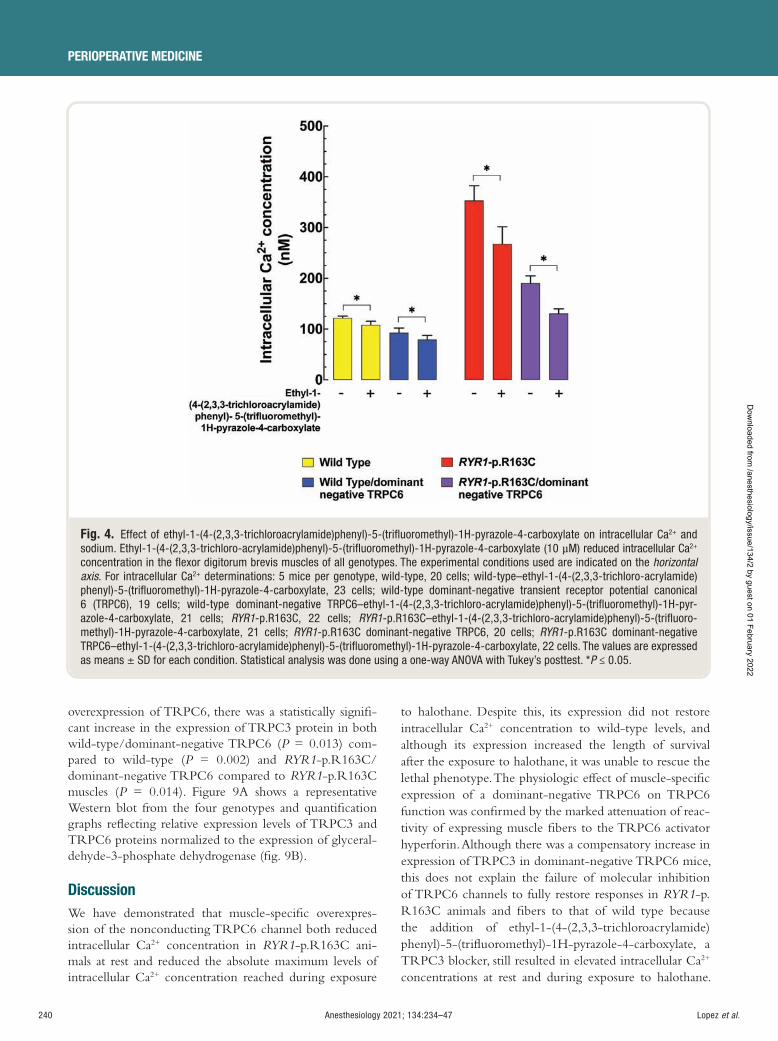
240 Anesthesiology 2021; 134:234–47
PERIOPERATIVE MEDICINE
Lopez et al.
overexpression of TRPC6, there was a statistically signi -cant increase in the expression of TRPC3 protein in both wild-type/dominant-negative TRPC6 ( P = 0.013) com-pared to wild-type ( P = 0.002) and RYR1 -p.R163C/dominant-negative TRPC6 compared to RYR1 -p.R163C muscles ( P = 0.014). Figure 9A shows a representative Western blot from the four genotypes and quanti cation graphs re ecting relative expression levels of TRPC3 and TRPC6 proteins normalized to the expression of glyceral-dehyde-3-phosphate dehydrogenase ( g. 9B ).
Discussion We have demonstrated that muscle-speci c overexpres-sion of the nonconducting TRPC6 channel both reduced intracellular Ca 2 + concentration in RYR1 -p.R163C ani-mals at rest and reduced the absolute maximum levels of intracellular Ca 2 + concentration reached during exposure
to halothane. Despite this, its expression did not restore intracellular Ca 2 + concentration to wild-type levels, and although its expression increased the length of survival after the exposure to halothane, it was unable to rescue the lethal phenotype. The physiologic e ect of muscle-speci c expression of a dominant-negative TRPC6 on TRPC6 function was con rmed by the marked attenuation of reac-tivity of expressing muscle bers to the TRPC6 activator hyperforin. Although there was a compensatory increase in expression of TRPC3 in dominant-negative TRPC6 mice, this does not explain the failure of molecular inhibition of TRPC6 channels to fully restore responses in RYR1 -p.R163C animals and bers to that of wild type because the addition of ethyl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(tri uoromethyl)-1H-pyrazole-4-carboxylate, a TRPC3 blocker, still resulted in elevated intracellular Ca 2 +
concentrations at rest and during exposure to halothane.
Fig. 4. Effect of ethyl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(trifl uoromethyl)-1H-pyrazole-4-carboxylate on intracellular Ca 2 + and sodium. Ethyl-1-(4-(2,3,3-trichloro-acrylamide)phenyl)-5-(trifl uoromethyl)-1H-pyrazole-4-carboxylate (10 µ M) reduced intracellular Ca 2 +
concentration in the fl exor digitorum brevis muscles of all genotypes. The experimental conditions used are indicated on the horizontal axis . For intracellular Ca 2 + determinations: 5 mice per genotype, wild-type, 20 cells; wild-type – ethyl-1-(4-(2,3,3-trichloro-acrylamide)phenyl)-5-(trifl uoromethyl)-1H-pyrazole-4-carboxylate, 23 cells; wild-type dominant-negative transient receptor potential canonical 6 (TRPC6), 19 cells; wild-type dominant-negative TRPC6 – ethyl-1-(4-(2,3,3-trichloro-acrylamide)phenyl)-5-(trifl uoromethyl)-1H-pyr-azole-4-carboxylate, 21 cells; RYR1 -p.R163C, 22 cells; RYR1 -p.R163C – ethyl-1-(4-(2,3,3-trichloro-acrylamide)phenyl)-5-(trifl uoro-methyl)-1H-pyrazole-4-carboxylate, 21 cells; RYR1 -p.R163C dominant-negative TRPC6, 20 cells; RYR1 -p.R163C dominant-negative TRPC6 – ethyl-1-(4-(2,3,3-trichloro-acrylamide)phenyl)-5-(trifl uoromethyl)-1H-pyrazole-4-carboxylate, 22 cells. The values are expressed as means ± SD for each condition. Statistical analysis was done using a one-way ANOVA with Tukey ’ s posttest. * P ≤ 0.05.
ALNV134N2_Text.indb 240ALNV134N2_Text.indb 240 29-Dec-20 19:44:0529-Dec-20 19:44:05
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
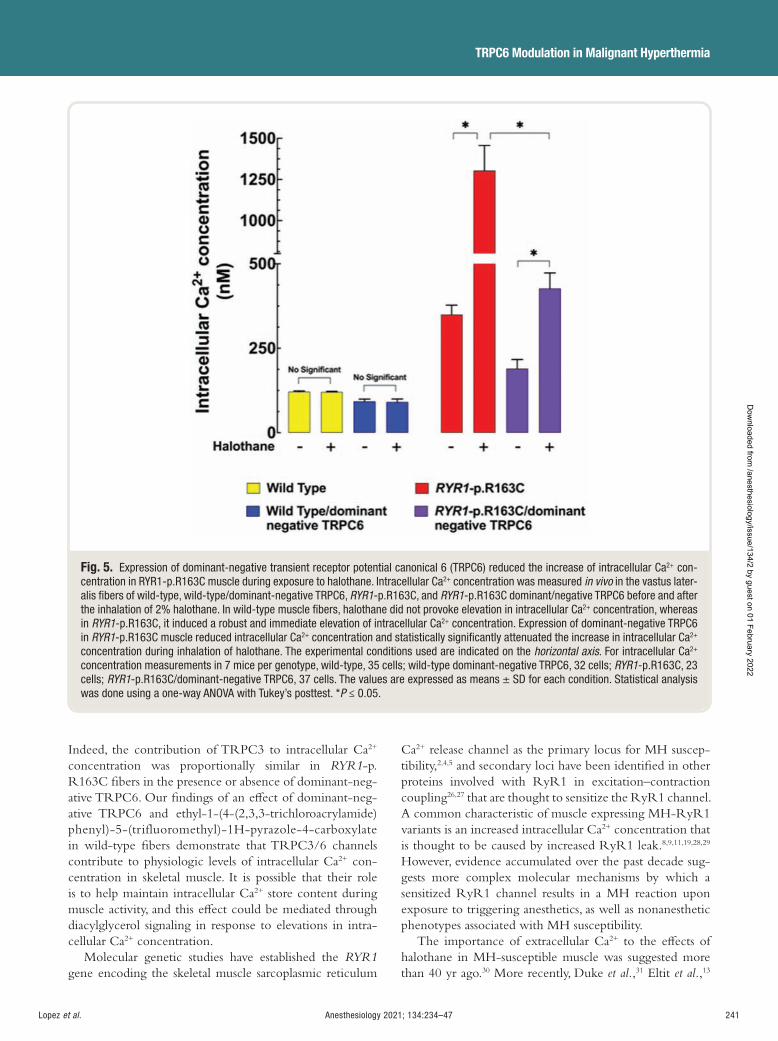
Anesthesiology 2021; 134:234–47 241
TRPC6 Modulation in Malignant Hyperthermia
Lopez et al.
Indeed, the contribution of TRPC3 to intracellular Ca 2 +
concentration was proportionally similar in RYR1 -p.R163C bers in the presence or absence of dominant-neg-ative TRPC6. Our ndings of an e ect of dominant-neg-ative TRPC6 and ethyl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(trifluoromethyl)-1H-pyrazole-4-carboxylate in wild-type bers demonstrate that TRPC3/6 channels contribute to physiologic levels of intracellular Ca 2 + con-centration in skeletal muscle. It is possible that their role is to help maintain intracellular Ca 2 + store content during muscle activity, and this e ect could be mediated through diacylglycerol signaling in response to elevations in intra-cellular Ca 2 + concentration.
Molecular genetic studies have established the RYR1 gene encoding the skeletal muscle sarcoplasmic reticulum
Ca 2 + release channel as the primary locus for MH suscep-tibility, 2 , 4 , 5 and secondary loci have been identi ed in other proteins involved with RyR1 in excitation – contraction coupling 26 , 27 that are thought to sensitize the RyR1 channel. A common characteristic of muscle expressing MH-RyR1 variants is an increased intracellular Ca 2 + concentration that is thought to be caused by increased RyR1 leak. 8 , 9 , 11 , 19 , 28 , 29
However, evidence accumulated over the past decade sug-gests more complex molecular mechanisms by which a sensitized RyR1 channel results in a MH reaction upon exposure to triggering anesthetics, as well as nonanesthetic phenotypes associated with MH susceptibility.
The importance of extracellular Ca 2 + to the e ects of halothane in MH-susceptible muscle was suggested more than 40 yr ago. 30 More recently, Duke et al. , 31 Eltit et al. , 13
Fig. 5. Expression of dominant-negative transient receptor potential canonical 6 (TRPC6) reduced the increase of intracellular Ca 2 + con-centration in RYR1-p.R163C muscle during exposure to halothane. Intracellular Ca 2 + concentration was measured in vivo in the vastus later-alis fi bers of wild-type, wild-type/dominant-negative TRPC6, RYR1 -p.R163C, and RYR1 -p.R163C dominant/negative TRPC6 before and after the inhalation of 2% halothane. In wild-type muscle fi bers, halothane did not provoke elevation in intracellular Ca 2 + concentration, whereas in RYR1 -p.R163C, it induced a robust and immediate elevation of intracellular Ca 2 + concentration. Expression of dominant-negative TRPC6 in RYR1 -p.R163C muscle reduced intracellular Ca 2 + concentration and statistically signifi cantly attenuated the increase in intracellular Ca 2 +
concentration during inhalation of halothane. The experimental conditions used are indicated on the horizontal axis . For intracellular Ca 2 +
concentration measurements in 7 mice per genotype, wild-type, 35 cells; wild-type dominant-negative TRPC6, 32 cells; RYR1 -p.R163C, 23 cells; RYR1 -p.R163C/dominant-negative TRPC6, 37 cells. The values are expressed as means ± SD for each condition. Statistical analysis was done using a one-way ANOVA with Tukey ’ s posttest. * P ≤ 0.05.
ALNV134N2_Text.indb 241ALNV134N2_Text.indb 241 29-Dec-20 19:44:0629-Dec-20 19:44:06
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
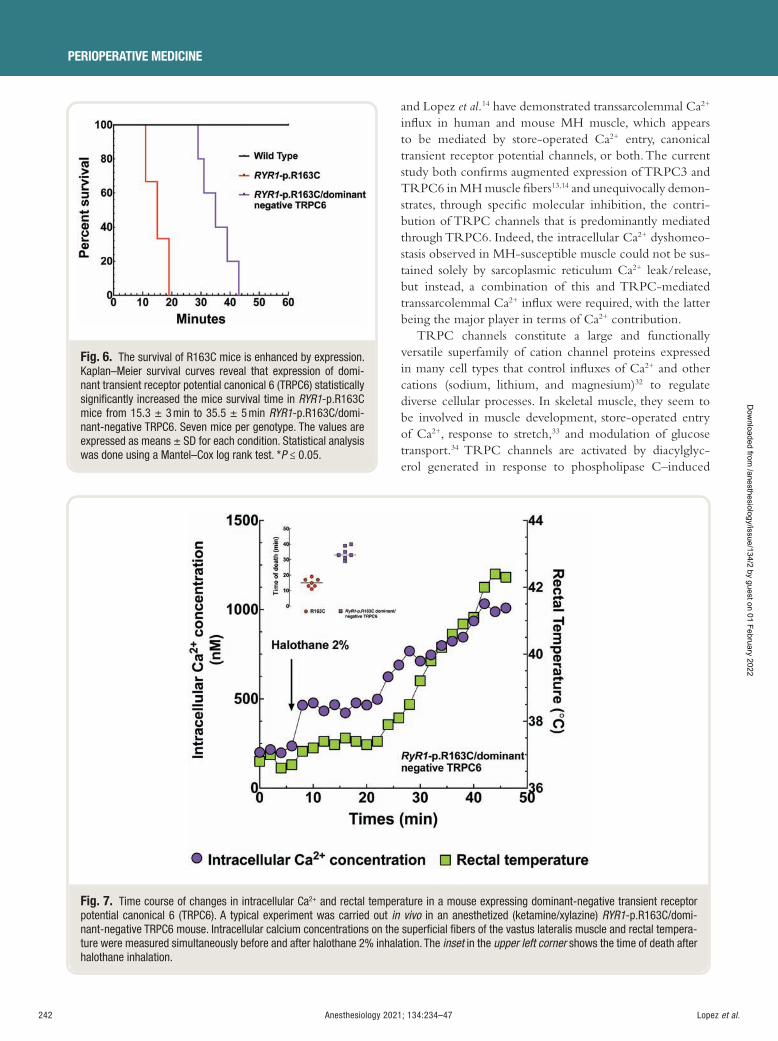
242 Anesthesiology 2021; 134:234–47
PERIOPERATIVE MEDICINE
Lopez et al.
and Lopez et al. 14 have demonstrated transsarcolemmal Ca 2 +
in ux in human and mouse MH muscle, which appears to be mediated by store-operated Ca 2 + entry, canonical transient receptor potential channels, or both. The current study both con rms augmented expression of TRPC3 and TRPC6 in MH muscle bers 13 , 14 and unequivocally demon-strates, through speci c molecular inhibition, the contri-bution of TRPC channels that is predominantly mediated through TRPC6. Indeed, the intracellular Ca 2 + dyshomeo-stasis observed in MH-susceptible muscle could not be sus-tained solely by sarcoplasmic reticulum Ca 2 + leak/release, but instead, a combination of this and TRPC-mediated transsarcolemmal Ca 2 + in ux were required, with the latter being the major player in terms of Ca 2 + contribution.
TRPC channels constitute a large and functionally versatile superfamily of cation channel proteins expressed in many cell types that control in uxes of Ca 2 + and other cations (sodium, lithium, and magnesium) 32 to regulate diverse cellular processes. In skeletal muscle, they seem to be involved in muscle development, store-operated entry of Ca 2 + , response to stretch, 33 and modulation of glucose transport. 34 TRPC channels are activated by diacylglyc-erol generated in response to phospholipase C – induced
Fig. 6. The survival of R163C mice is enhanced by expression. Kaplan – Meier survival curves reveal that expression of domi-nant transient receptor potential canonical 6 (TRPC6) statistically signifi cantly increased the mice survival time in RYR1 -p.R163C mice from 15.3 ± 3 min to 35.5 ± 5 min RYR1 -p.R163C/domi-nant-negative TRPC6. Seven mice per genotype. The values are expressed as means ± SD for each condition. Statistical analysis was done using a Mantel – Cox log rank test. * P ≤ 0.05.
Fig. 7. Time course of changes in intracellular Ca 2 + and rectal temperature in a mouse expressing dominant-negative transient receptor potential canonical 6 (TRPC6). A typical experiment was carried out in vivo in an anesthetized (ketamine/xylazine) RYR1 -p.R163C/domi-nant-negative TRPC6 mouse. Intracellular calcium concentrations on the superfi cial fi bers of the vastus lateralis muscle and rectal tempera-ture were measured simultaneously before and after halothane 2% inhalation. The inset in the upper left corner shows the time of death after halothane inhalation.
ALNV134N2_Text.indb 242ALNV134N2_Text.indb 242 29-Dec-20 19:44:0729-Dec-20 19:44:07
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
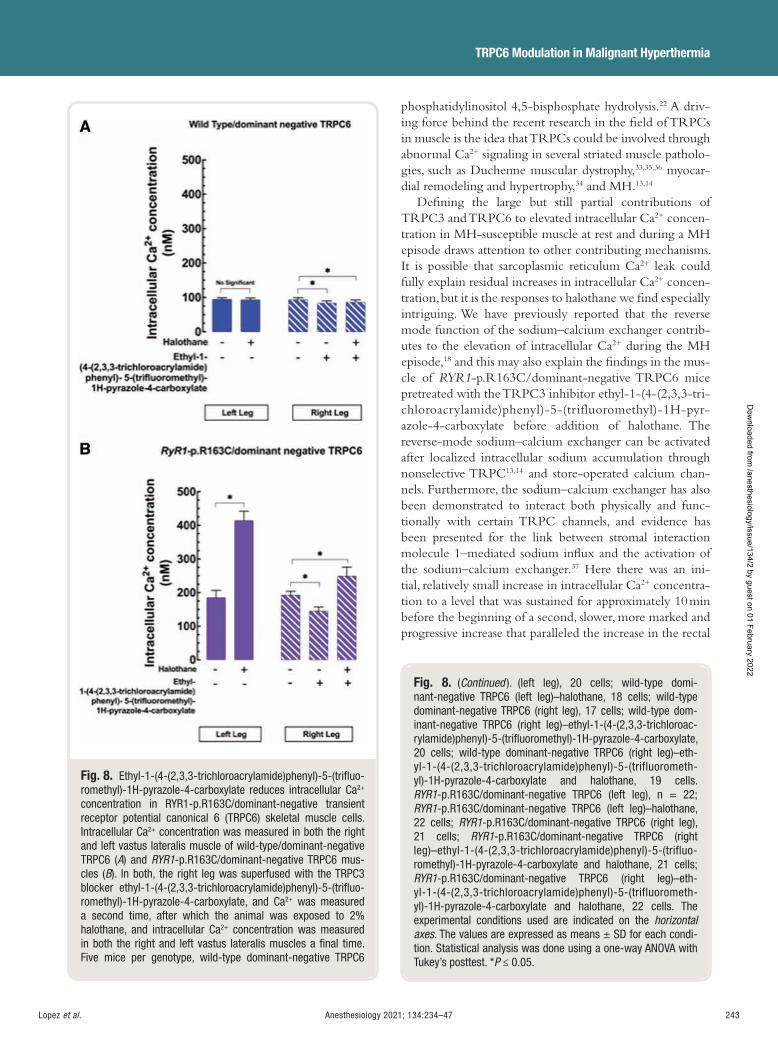
Anesthesiology 2021; 134:234–47 243
TRPC6 Modulation in Malignant Hyperthermia
Lopez et al.
phosphatidylinositol 4,5-bisphosphate hydrolysis. 22 A driv-ing force behind the recent research in the eld of TRPCs in muscle is the idea that TRPCs could be involved through abnormal Ca 2 + signaling in several striated muscle patholo-gies, such as Duchenne muscular dystrophy, 33 , 35 , 36 myocar-dial remodeling and hypertrophy, 34 and MH. 13 , 14
De ning the large but still partial contributions of TRPC3 and TRPC6 to elevated intracellular Ca 2 + concen-tration in MH-susceptible muscle at rest and during a MH episode draws attention to other contributing mechanisms. It is possible that sarcoplasmic reticulum Ca 2 + leak could fully explain residual increases in intracellular Ca 2 + concen-tration, but it is the responses to halothane we nd especially intriguing. We have previously reported that the reverse mode function of the sodium – calcium exchanger contrib-utes to the elevation of intracellular Ca 2 + during the MH episode, 18 and this may also explain the ndings in the mus-cle of RYR1 -p.R163C/dominant-negative TRPC6 mice pretreated with the TRPC3 inhibitor ethyl-1-(4-(2,3,3-tri-chloroacrylamide)phenyl)-5-(trifluoromethyl)-1H-pyr-azole-4-carboxylate before addition of halothane. The reverse-mode sodium – calcium exchanger can be activated after localized intracellular sodium accumulation through nonselective TRPC 13 , 14 and store-operated calcium chan-nels. Furthermore, the sodium – calcium exchanger has also been demonstrated to interact both physically and func-tionally with certain TRPC channels, and evidence has been presented for the link between stromal interaction molecule 1 – mediated sodium in ux and the activation of the sodium – calcium exchanger. 37 Here there was an ini-tial, relatively small increase in intracellular Ca 2 + concentra-tion to a level that was sustained for approximately 10 min before the beginning of a second, slower, more marked and progressive increase that paralleled the increase in the rectal
Fig. 8. Ethyl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(trifl uo-romethyl)-1H-pyrazole-4-carboxylate reduces intracellular Ca 2 +
concentration in RYR1-p.R163C/dominant-negative transient receptor potential canonical 6 (TRPC6) skeletal muscle cells. Intracellular Ca 2 + concentration was measured in both the right and left vastus lateralis muscle of wild-type/dominant-negative TRPC6 ( A ) and RYR1 -p.R163C/dominant-negative TRPC6 mus-cles ( B ). In both, the right leg was superfused with the TRPC3 blocker ethyl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(trifl uo-romethyl)-1H-pyrazole-4-carboxylate, and Ca 2 + was measured a second time, after which the animal was exposed to 2% halothane, and intracellular Ca 2 + concentration was measured in both the right and left vastus lateralis muscles a fi nal time. Five mice per genotype, wild-type dominant-negative TRPC6
Fig. 8. ( Continued ). (left leg), 20 cells; wild-type domi-nant-negative TRPC6 (left leg) – halothane, 18 cells; wild-type dominant-negative TRPC6 (right leg), 17 cells; wild-type dom-inant-negative TRPC6 (right leg) – ethyl-1-(4-(2,3,3-trichloroac-rylamide)phenyl)-5-(trifl uoromethyl)-1H-pyrazole-4-carboxylate, 20 cells; wild-type dominant-negative TRPC6 (right leg) – eth-yl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(trifluorometh-yl)-1H-pyrazole-4-carboxylate and halothane, 19 cells. RYR1 -p.R163C/dominant-negative TRPC6 (left leg), n = 22; RYR1 -p.R163C/dominant-negative TRPC6 (left leg) – halothane, 22 cells; RYR1 -p.R163C/dominant-negative TRPC6 (right leg), 21 cells; RYR1 -p.R163C/dominant-negative TRPC6 (right leg) – ethyl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(trifluo-romethyl)-1H-pyrazole-4-carboxylate and halothane, 21 cells; RYR1 -p.R163C/dominant-negative TRPC6 (right leg) – eth-yl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(trifluorometh-yl)-1H-pyrazole-4-carboxylate and halothane, 22 cells. The experimental conditions used are indicated on the horizontal axes . The values are expressed as means ± SD for each condi-tion. Statistical analysis was done using a one-way ANOVA with Tukey ’ s posttest. * P ≤ 0.05.
ALNV134N2_Text.indb 243ALNV134N2_Text.indb 243 29-Dec-20 19:44:0729-Dec-20 19:44:07
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
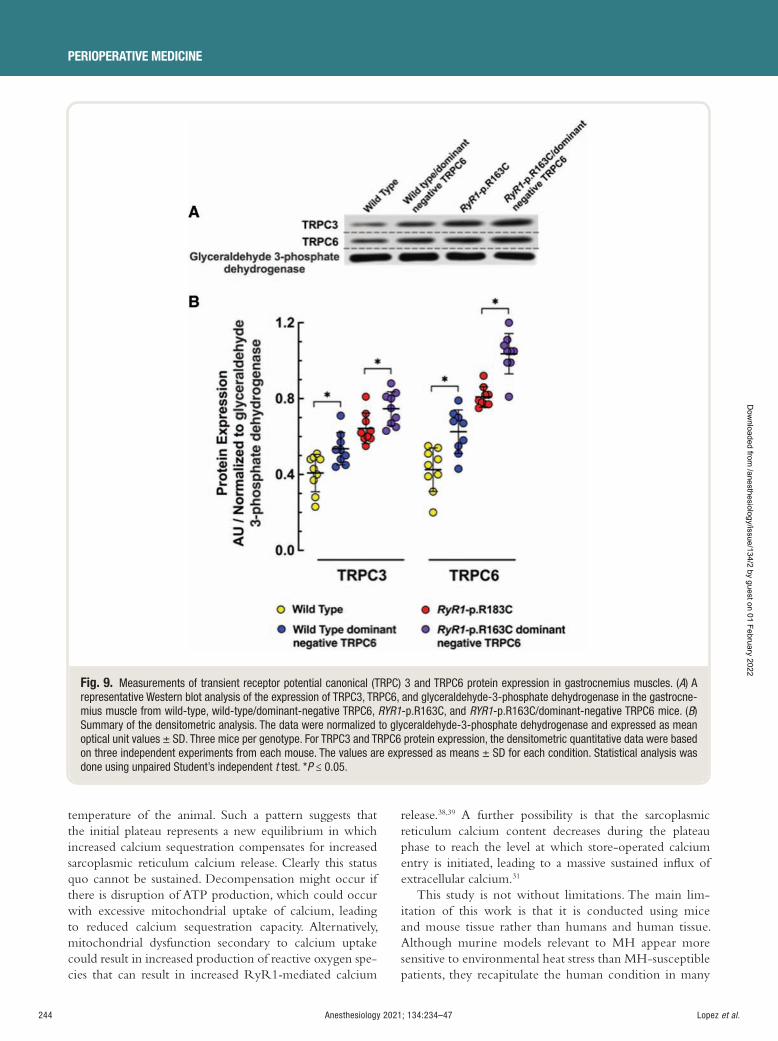
244 Anesthesiology 2021; 134:234–47
PERIOPERATIVE MEDICINE
Lopez et al.
temperature of the animal. Such a pattern suggests that the initial plateau represents a new equilibrium in which increased calcium sequestration compensates for increased sarcoplasmic reticulum calcium release. Clearly this status quo cannot be sustained. Decompensation might occur if there is disruption of ATP production, which could occur with excessive mitochondrial uptake of calcium, leading to reduced calcium sequestration capacity. Alternatively, mitochondrial dysfunction secondary to calcium uptake could result in increased production of reactive oxygen spe-cies that can result in increased RyR1 - mediated calcium
release. 38 , 39 A further possibility is that the sarcoplasmic reticulum calcium content decreases during the plateau phase to reach the level at which store-operated calcium entry is initiated, leading to a massive sustained in ux of extracellular calcium. 31
This study is not without limitations. The main lim-itation of this work is that it is conducted using mice and mouse tissue rather than humans and human tissue. Although murine models relevant to MH appear more sensitive to environmental heat stress than MH-susceptible patients, they recapitulate the human condition in many
Fig. 9. Measurements of transient receptor potential canonical (TRPC) 3 and TRPC6 protein expression in gastrocnemius muscles. ( A ) A representative Western blot analysis of the expression of TRPC3, TRPC6, and glyceraldehyde-3-phosphate dehydrogenase in the gastrocne-mius muscle from wild-type, wild-type/dominant-negative TRPC6, RYR1 -p.R163C, and RYR1 -p.R163C/dominant-negative TRPC6 mice. ( B ) Summary of the densitometric analysis. The data were normalized to glyceraldehyde-3-phosphate dehydrogenase and expressed as mean optical unit values ± SD. Three mice per genotype. For TRPC3 and TRPC6 protein expression, the densitometric quantitative data were based on three independent experiments from each mouse. The values are expressed as means ± SD for each condition. Statistical analysis was done using unpaired Student ’ s independent t test. * P ≤ 0.05.
ALNV134N2_Text.indb 244ALNV134N2_Text.indb 244 29-Dec-20 19:44:0829-Dec-20 19:44:08
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:234–47 245
TRPC6 Modulation in Malignant Hyperthermia
Lopez et al.
other respects, including increased intracellular Ca 2 +
concentration, 9 , 28 , 40 dependence on extracellular cal-cium, 31 and mitochondrial dysfunction. 41 We have also not demonstrated that skeletal muscle – speci c expression of a nonconducting dominant-negative TRPC6 com-pletely abolishes TRPC6 conductance, although pre-vious work with this construct suggests this is likely. 15
Finally, although we have used molecular inhibition of TRPC6, our conclusions concerning the e ect of eth-yl-1-(4-(2,3,3-trichloroacrylamide)phenyl)-5-(trifluo-romethyl)-1H-pyrazole-4-carboxylate on TRPC3 must be more guarded because selectivity of pharmacologic reagents can never be guaranteed.
In summary, these results demonstrate that nonselective sarcolemmal cation permeability mediated by TRPC6 and TRPC3 plays a critical role in causing cytosolic Ca 2 + over-load both at rest and during a MH crisis. This improved understanding of the underlying mechanisms of MH may assist in the design of new therapies and the identi cation of more selective pharmacologic agents other than our cur-rent accepted standard, dantrolene, to prevent or reverse the MH episodes.
Acknowledgments
The authors are grateful to Je ery D. Molkentin, Ph.D., Howard Hughes Medical Institute, Molecular Cardiovascular Biology, Cincinnati Children ’ s Hospital Medical Center, Cincinnati, Ohio, for generously providing us with the transgenic mice with skeletal muscle – speci c overexpression of a nonconducting TRPC6 channel; and Shane Antrobus, B.S., Department of Molecular Biosciences, School of Veterinary Medicine, University of California at Davis, Davis, California, for his valuable technical assistance.
Research Support
Supported by grant Nos. 1R01AR068897 and P01AR-05235 from the National Institute of Arthritis, Musculoskeletal and Skin Diseases, National Institutes of Health (Bethesda, Maryland; to Drs. Allen, Hopkins, and Lopez), grant No. 21543 from the French Muscular Dystrophy Association (AFM; Evry, France; to Dr. Lopez), and funds from the Florida Heart Foundation (Miami, Florida; to Drs. Lopez, Uryash, and Adams).
Competing Interests
The authors declare no competing interests.
Correspondence
Address correspondence to Dr. Allen: St. James ’ s University Hospital, Leeds, LS9 7TF United Kingdom. [email protected] . A nesthesiology ’ s articles are made freely acces-sible to all readers on www.anesthesiology.org, for personal use only, 6 months from the cover date of the issue.
References
1. Rosenberg H , Pollock N , Schiemann A , Bulger T , Stowell K : Malignant hyperthermia: A review. Orphanet J Rare Dis 2015 ; 10 : 93
2. MacLennan DH , Du C , Zorzato F , Fujii J , Phillips M , Korneluk RG , Frodis W , Britt BA , Worton RG : Ryanodine receptor gene is a candidate for predis-position to malignant hyperthermia. Nature 1990 ; 343 : 559 – 61
3. Kausch K , Lehmann-Horn F , Janka M , Wieringa B , Grimm T , M ü ller CR : Evidence for linkage of the central core disease locus to the proximal long arm of human chromosome 19. Genomics 1991 ; 10 : 765 – 9
4. Robinson R , Carpenter D , Shaw MA , Halsall J , Hopkins P : Mutations in RYR1 in malignant hyperthermia and central core disease. Hum Mutat 2006 ; 27 : 977 – 89
5. Jurkat-Rott K , McCarthy T , Lehmann-Horn F : Genetics and pathogenesis of malignant hyperthermia. Muscle Nerve 2000 ; 23 : 4 – 17
6. Miller DM , Daly C , Aboelsaod EM , Gardner L , Hobson SJ , Riasat K , Shepherd S , Robinson RL , Bilmen JG , Gupta PK , Shaw MA , Hopkins PM : Genetic epide-miology of malignant hyperthermia in the UK. Br J Anaesth 2018 ; 121 : 944 – 52
7. L ó pez JR , Alamo L , Caputo C , Wikinski J , Ledezma D : Intracellular ionized calcium concentration in muscles from humans with malignant hyperthermia. Muscle Nerve 1985 ; 8 : 355 – 8
8. Lopez JR , Alamo LA , Jones DE , Papp L , Allen PD , Gergely J , Sr é ter FA : [Ca 2 + ]
i in muscles of malignant
hyperthermia susceptible pigs determined in vivo with Ca 2 + selective microelectrodes. Muscle Nerve 1986 ; 9 : 85 – 6
9. Yang T , Esteve E , Pessah IN , Molinski TF , Allen PD , L ó pez JR : Elevated resting [Ca 2 + ]
i in myotubes
expressing malignant hyperthermia RyR1 cDNAs is partially restored by modulation of passive calcium leak from the SR. Am J Physiol Cell Physiol 2007 ; 292 : C1591 – 8
10. Eltit JM , Bannister RA , Moua O , Altamirano F , Hopkins PM , Pessah IN , Molinski TF , L ó pez JR , Beam KG , Allen PD : Malignant hyperthermia susceptibility aris-ing from altered resting coupling between the skeletal muscle L-type Ca 2 + channel and the type 1 ryanodine receptor. Proc Natl Acad Sci USA 2012 ; 109 : 7923 – 8
11. L ó pez JR , Allen PD , Alamo L , Jones D , Sreter FA : Myoplasmic free [Ca 2 + ] during a malignant hyperther-mia episode in swine. Muscle Nerve 1988 ; 11 : 82 – 8
12. Yuen B , Boncompagni S , Feng W , Yang T , Lopez JR , Matthaei KI , Goth SR , Protasi F , Franzini-Armstrong C , Allen PD , Pessah IN : Mice expressing T4826I-RYR1 are viable but exhibit sex- and genotype-de-pendent susceptibility to malignant hyperthermia and muscle damage. FASEB J 2012 ; 26 : 1311 – 22
ALNV134N2_Text.indb 245ALNV134N2_Text.indb 245 29-Dec-20 19:44:0829-Dec-20 19:44:08
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
246 Anesthesiology 2021; 134:234–47
PERIOPERATIVE MEDICINE
Lopez et al.
13. Eltit JM , Ding X , Pessah IN , Allen PD , Lopez JR : Nonspeci c sarcolemmal cation channels are crit-ical for the pathogenesis of malignant hyperthermia. FASEB J 2013 ; 27 : 991 – 1000
14. Lopez JR , Kaura V , Hopkins P , Liu X , Uryach A , Adams J , Allen PD : Transient receptor potential cation chan-nels and calcium dyshomeostasis in a mouse model relevant to malignant hyperthermia. A nesthesiology 2020 ; 133 : 364 – 7 6
15. Millay DP , Goonasekera SA , Sargent MA , Maillet M , Aronow BJ , Molkentin JD : Calcium in ux is su -cient to induce muscular dystrophy through a TRPC-dependent mechanism. Proc Natl Acad Sci USA 2009 ; 106 : 19023 – 8
16. Hofmann T , Schaefer M , Schultz G , Gudermann T : Subunit composition of mammalian transient receptor potential channels in living cells. Proc Natl Acad Sci USA 2002 ; 99 : 7461 – 6
17. Tang Q , Guo W , Zheng L , Wu JX , Liu M , Zhou X , Zhang X , Chen L : Structure of the receptor-activated human TRPC6 and TRPC3 ion channels. Cell Res 2018 ; 28 : 746 – 55
18. Altamirano F , Eltit JM , Robin G , Linares N , Ding X , Pessah IN , Allen PD , L ó pez JR : Ca 2 + in ux via the Na + /Ca 2 + exchanger is enhanced in malignant hyperthermia skeletal muscle. J Biol Chem 2014 ; 289 : 19180 – 90
19. L ó pez JR , Alamo L , Caputo C , DiPolo R , Vergara S : Determination of ionic calcium in frog skeletal muscle bers. Biophys J 1983 ; 43 : 1 – 4
20. Altamirano F , Perez CF , Liu M , Widrick J , Barton ER , Allen PD , Adams JA , Lopez JR : Whole body peri-odic acceleration is an e ective therapy to ameliorate muscular dystrophy in mdx mice. PLoS One 2014 ; 9 : e106590
21. Laemmli UK : Cleavage of structural proteins during the assembly of the head of bacteriophage T4. Nature 1970 ; 227 : 680 – 5
22. Hofmann T , Obukhov AG , Schaefer M , Harteneck C , Gudermann T , Schultz G : Direct activation of human TRPC6 and TRPC3 channels by diacylglycerol. Nature 1999 ; 397 : 259 – 63
23. Aires V , Hichami A , Boulay G , Khan NA : Activation of TRPC6 calcium channels by diacylglycerol (DAG) – containing arachidonic acid: A comparative study with DAG-containing docosahexaenoic acid. Biochimie 2007 ; 89 : 926 – 37
24. Leuner K , Kazanski V , M ü ller M , Essin K , Henke B , Gollasch M , Harteneck C , M ü ller WE : Hyperforin: A key constituent of St. John ’ s wort speci cally activates TRPC6 channels. FASEB J 2007 ; 21 : 4101 – 11
25. Kiyonaka S , Kato K , Nishida M , Mio K , Numaga T , Sawaguchi Y , Yoshida T , Wakamori M , Mori E , Numata T , Ishii M , Takemoto H , Ojida A , Watanabe K , Uemura A , Kurose H , Morii T , Kobayashi T , Sato Y , Sato C ,
Hamachi I , Mori Y : Selective and direct inhibition of TRPC3 channels underlies biological activities of a pyrazole compound. Proc Natl Acad Sci USA 2009 ; 106 : 5400 – 5
26. Robinson RL , Monnier N , Wolz W , Jung M , Reis A , Nuernberg G , Curran JL , Monsieurs K , Stieglitz P , Heytens L , Fricker R , van Broeckhoven C , Deufel T , Hopkins PM , Lunardi J , Mueller CR : A genome wide search for susceptibility loci in three European malig-nant hyperthermia pedigrees. Hum Mol Genet 1997 ; 6 : 953 – 61
27. Stamm DS , Powell CM , Stajich JM , Zismann VL , Stephan DA , Chesnut B , Aylsworth AS , Kahler SG , Deak KL , Gilbert JR , Speer MC : Novel congenital myopathy locus identi ed in Native American Indians at 12q13.13 – 14.1. Neurology 2008 ; 71 : 1764 – 9
28. Yang T , Riehl J , Esteve E , Matthaei KI , Goth S , Allen PD , Pessah IN , Lopez JR : Pharmacologic and func-tional characterization of malignant hyperthermia in the R163C RyR1 knock-in mouse. A nesthesiology 2006 ; 105 : 1164 – 75
29. Lopez JR , Kaura V , Diggle CP , Hopkins PM , Allen PD : Malignant hyperthermia, environmental heat stress, and intracellular calcium dysregulation in a mouse model expressing the p.G2435R variant of RYR1. Br J Anaesth 2018 ; 121 : 953 – 61
30. Nelson TE , Bedell DM , Jones EW : Porcine malignant hyperthermia: E ects of temperature and extracellular calcium concentration on halothane-induced contrac-ture of susceptible skeletal muscle. A nesthesiology 1975 ; 42 : 301 – 6
31. Duke AM , Hopkins PM , Calaghan SC , Halsall JP , Steele DS : Store-operated Ca 2 + entry in malignant hyperthermia-susceptible human skeletal muscle. J Biol Chem 2010 ; 285 : 25645 – 53
32. Owsianik G , Talavera K , Voets T , Nilius B : Permeation and selectivity of TRP channels. Annu Rev Physiol 2006 ; 68 : 685 – 717
33. Lopez JR , Uryash A , Faury G , Est è ve E , Adams JA : Contribution of TRPC channels to intracellular Ca 2 +
dyshomeostasis in smooth muscle from mdx mice. Front Physiol 2020 ; 11 : 126
34. Eder P : Cardiac remodeling and disease: SOCE and TRPC signaling in cardiac pathology. Adv Exp Med Biol 2017 ; 993 : 505 – 21
35. Mijares A , Altamirano F , Kolster J , Adams JA , L ó pez JR : Age-dependent changes in diastolic Ca 2 + and Na +
concentrations in dystrophic cardiomyopathy: Role of Ca 2 + entry and IP3. Biochem Biophys Res Commun 2014 ; 452 : 1054 – 9
36. Matsumura CY , Taniguti AP , Pertille A , Santo Neto H , Marques MJ : Stretch-activated calcium channel pro-tein TRPC1 is correlated with the di erent degrees of the dystrophic phenotype in mdx mice. Am J Physiol Cell Physiol 2011 ; 301 : C1344 – 50
ALNV134N2_Text.indb 246ALNV134N2_Text.indb 246 29-Dec-20 19:44:0829-Dec-20 19:44:08
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:234–47 247
TRPC6 Modulation in Malignant Hyperthermia
Lopez et al.
37. Liu B , Peel SE , Fox J , Hall IP : Reverse mode Na + /Ca 2 + exchange mediated by STIM1 contributes to Ca 2 + in ux in airway smooth muscle following agonist stimulation. Respir Res 2010 ; 11 : 168
38. Dridi H , Yehya M , Barsotti R , Reiken S , Angebault C , Jung B , Jaber S , Marks AR , Lacampagne A , Matecki S : Mitochondrial oxidative stress induces leaky ryanodine receptor during mechanical ventilation. Free Radic Biol Med 2020 ; 146 : 383 – 91
39. Lotteau S , Ivarsson N , Yang Z , Restagno D , Colyer J , Hopkins P , Weightman A , Himori K , Yamada T , Bruton
J , Steele D , Westerblad H , Calaghan S : A mechanism for statin-induced susceptibility to myopathy. JACC Basic Transl Sci 2019 ; 4 : 509 – 23
40. Yang T , Allen PD , Pessah IN , Lopez JR : Enhanced exci-tation-coupled calcium entry in myotubes is associated with expression of RyR1 malignant hyperthermia mutations. J Biol Chem 2007 ; 282 : 37471 – 8
41. Chang L , Daly C , Miller DM , Allen PD , Boyle JP , Hopkins PM , Shaw MA : Permeabilised skeletal muscle reveals mitochondrial de ciency in malignant hyperthermia-sus-ceptible individuals. Br J Anaesth 2019 ; 122 : 613 – 21
ALNV134N2_Text.indb 247ALNV134N2_Text.indb 247 29-Dec-20 19:44:0829-Dec-20 19:44:08
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
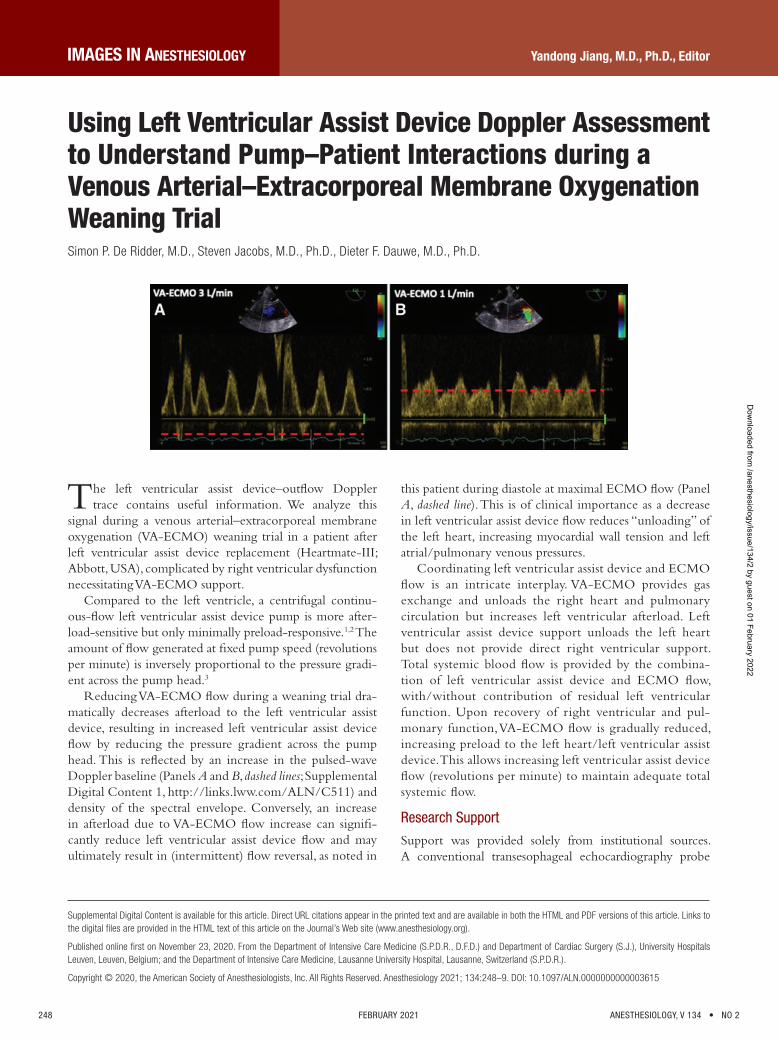
248 FEBRUARY 2021 ANESTHESIOLOGY, V 134 • NO 2
Yandong Jiang, M.D., Ph.D., Editor
Supplemental Digital Content is available for this article. Direct URL citations appear in the printed text and are available in both the HTML and PDF versions of this article. Links to the digital fi les are provided in the HTML text of this article on the Journal ’ s Web site ( www.anesthesiology.org ).
Published online fi rst on November 23, 2020. From the Department of Intensive Care Medicine (S.P.D.R., D.F.D.) and Department of Cardiac Surgery (S.J.), University Hospitals Leuven, Leuven, Belgium; and the Department of Intensive Care Medicine, Lausanne University Hospital, Lausanne, Switzerland (S.P.D.R.).
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved. Anesthesiology 2021 ; 134 : 248 – 9 . DOI: 10.1097/ALN.0000000000003615
Using Left Ventricular Assist Device Doppler Assessment to Understand Pump – Patient Interactions during a Venous Arterial – Extracorporeal Membrane Oxygenation Weaning Trial Simon P. De Ridder , M.D. , Steven Jacobs , M.D., Ph.D. , Dieter F. Dauwe , M.D., Ph.D.
The left ventricular assist device – out ow Doppler trace contains useful information. We analyze this
signal during a venous arterial – extracorporeal membrane oxygenation (VA-ECMO) weaning trial in a patient after left ventricular assist device replacement (Heartmate-III; Abbott, USA), complicated by right ventricular dysfunction necessitating VA-ECMO support.
Compared to the left ventricle, a centrifugal continu-ous- ow left ventricular assist device pump is more after-load-sensitive but only minimally preload-responsive. 1 , 2 The amount of ow generated at xed pump speed (revolutions per minute) is inversely proportional to the pressure gradi-ent across the pump head. 3
Reducing VA-ECMO ow during a weaning trial dra-matically decreases afterload to the left ventricular assist device, resulting in increased left ventricular assist device ow by reducing the pressure gradient across the pump head. This is re ected by an increase in the pulsed-wave Doppler baseline (Panels A and B, dashed lines ; Supplemental Digital Content 1, http://links.lww.com/ALN/C511 ) and density of the spectral envelope. Conversely, an increase in afterload due to VA-ECMO ow increase can signi -cantly reduce left ventricular assist device ow and may ultimately result in (intermittent) ow reversal, as noted in
this patient during diastole at maximal ECMO ow (Panel A, dashed line ). This is of clinical importance as a decrease in left ventricular assist device ow reduces “ unloading ” of the left heart, increasing myocardial wall tension and left atrial/pulmonary venous pressures.
Coordinating left ventricular assist device and ECMO ow is an intricate interplay. VA-ECMO provides gas exchange and unloads the right heart and pulmonary circulation but increases left ventricular afterload. Left ventricular assist device support unloads the left heart but does not provide direct right ventricular support. Total systemic blood ow is provided by the combina-tion of left ventricular assist device and ECMO ow, with/without contribution of residual left ventricular function. Upon recovery of right ventricular and pul-monary function, VA-ECMO ow is gradually reduced, increasing preload to the left heart/left ventricular assist device. This allows increasing left ventricular assist device ow (revolutions per minute) to maintain adequate total systemic ow.
Research Support
Support was provided solely from institutional sources. A conventional transesophageal echocardiography probe
IMAGES IN ANESTHESIOLOGY
ALNV134N2_Text.indb 248ALNV134N2_Text.indb 248 29-Dec-20 19:44:0829-Dec-20 19:44:08
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

IMAGES IN ANESTHESIOLOGY
Anesthesiology 2021; 134:248–9 249Images in Anesthesiology
(Philips Healthcare, The Netherlands) was used for obtain-ing the transesophageal echocardiography images. No addi-tional funding was required.
Competing Interests
The authors declare no competing interests.
Correspondence
Address correspondence to Dr. Dauwe: [email protected]
References
1. Rich JD , Burkho D : HVAD ow waveform mor-phologies: Theoretical foundation and implications for clinical practice. ASAIO J 2017 ; 63 : 526 – 35
2. Chatterjee A , Feldmann C , Hanke JS , Ricklefs M , Shrestha M , Dogan G , Haverich A , Schmitto JD : The momentum of HeartMate 3: a novel active magneti-cally levitated centrifugal left ventricular assist device (LVAD). J Thorac Dis 2018 ; 10 ( suppl 15 ): 1790 – 3
3. Pratt AK , Shah NS , Boyce SW : Left ventricular assist device management in the ICU. Crit Care Med 2014 ; 42 : 158 – 68
ALNV134N2_Text.indb 249ALNV134N2_Text.indb 249 29-Dec-20 19:44:0829-Dec-20 19:44:08
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

CLINICAL FOCUS REVIEW
250 FEBRUARY 2021 ANESTHESIOLOGY, V 134 • NO 2
Jerrold H. Levy, M.D., F.A.H.A., F.C.C.M., Editor
Submitted for publication June 12, 2020. Accepted for publication October 5, 2020. Published online fi rst on November 18, 2020. From the Department of Anesthesiology, Center of Anesthesiology and Intensive Care Medicine, University Medical Center Hamburg-Eppendorf, Hamburg, Germany (B.S.); Outcomes Research Consortium, Cleveland, Ohio (B.S.); and Department of Outcomes Research, Anesthesiology Institute, Cleveland Clinic, Cleveland, Ohio (D.I.S.).
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved. Anesthesiology 2021 ; 134 : 250 – 61 . DOI: 10.1097/ALN.0000000000003610
Perioperative Blood Pressure Management Bernd Saugel , M.D. , Daniel I. Sessler , M.D.
Intraoperative mortality has decreased by a factor of a 100 during the last century, and deaths during surgery are
now rare. 1 In contrast, mortality within the rst postoper-ative month remains common, with about 2% of patients having inpatient noncardiac surgery dying within 30 days after surgery 2 — corresponding to more than 4 million deaths per year worldwide. 3 Postoperative deaths are most strongly associated with complications, including myocar-dial and acute kidney injury. 2 The risk for postoperative myocardial and acute kidney injury is largely determined by baseline factors. 4 , 5 But intraoperative and postoperative hypotension are also associated with myocardial and acute kidney injury, and mortality 6 – 12 — and di er from other risk factors in being potentially modi able.
Hypotension during and after noncardiac surgery is multifactorial in origin, involving combinations of patient, pharmacologic, and procedural factors. 13 , 14 Intraoperative hypotension occurs despite frequent or even continuous intraoperative hemodynamic monitoring. Postoperative hypotension is common, profound, and prolonged — and largely missed with conventional intermittent vital sign monitoring. 15
Avoiding perioperative hypotension is a physiologic complex challenge for anesthesiologists. 16 In this Clinical Focus Review, we summarize and discuss current evidence and open research questions regarding intraoperative and postoperative blood pressure management in patients hav-ing noncardiac surgery.
Physiology of Blood Pressure Arterial blood pressure is the product of cardiac output and systemic vascular resistance. Blood pressure is a complex physiologic variable described clinically by systolic blood pressure, mean arterial pressure, and diastolic blood pres-sure. These blood pressure components result from di er-ent periods of the cardiac cycle with ventricular relaxation during diastole and contraction during systole and re ect various physiologic functions ( g. 1 ).
Blood pressure is regulated by multiple interrelated sys-tems for short-term and long-term blood pressure con-trol. The sympathetic nervous system facilitates short-term blood pressure control by local and systemic release of vaso-constrictors. In response to blood pressure changes, carotid
and aortic baroreceptors transmit impulses to the auto-nomic nervous system to maintain normal blood pressure. Long-term blood pressure control is promoted by renal humoral control systems regulating blood volume, includ-ing the renin-angiotensin-aldosterone system. Endogenous vasopressin released from the pituitary gland increases water reabsorption from the renal tubules.
Autoregulatory mechanisms promote near-constant blood ow across various organ systems within certain blood pressure limits. 16 , 17 The brain and kidneys are espe-cially protected by robust autoregulation. 17 Various factors directly or indirectly in uence autoregulatory thresh-olds, 16 , 17 and the impact of vasoactive and anesthetic drugs on blood ow regulation is complex. 16
Normal ambulatory blood pressure varies considerably among individuals, 18 and the incidence of chronic arterial hypertension increases with age. 19 Within individuals, cir-cadian rhythms, as well as neural and hormonal changes, induce short-term uctuations in blood pressure. 16 , 20 Single blood pressure measurements may therefore poorly re ect patients ’ blood pressure pro les.
Defi nitions of Perioperative Hypotension There are no clear or widely accepted de nitions of intraop-erative or postoperative hypotension. Hypotension is gener-ally de ned using absolute or relative thresholds for various blood pressure components, and may specify a duration of exposure. In a systematic review, Bijker et al. 21 identi ed 140 de nitions for intraoperative hypotension in 130 articles. De nitions were based on either systolic blood pressure or mean arterial pressure or a combination of both, considering either absolute thresholds or thresholds relative to a base-line. 21 The most common de nition was a 20% reduction in systolic blood pressure from baseline. 21 Applying these de nitions to a retrospective cohort of more than 15,000 adults who had noncardiac surgery showed that the inci-dence of intraoperative hypotension varies substantially depending on the selected de nition. 21 For example, con-sidering a 20% reduction in systolic blood pressure resulted in an incidence of intraoperative hypotension of 93% for a greater than or equal to 1-min exposure, 88% for a greater than or equal to 5-min exposure, and 78% for a greater than or equal to 10-min exposure. 21 Applying an absolute mean
ALNV134N2_Text.indb 250ALNV134N2_Text.indb 250 29-Dec-20 19:44:0829-Dec-20 19:44:08
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
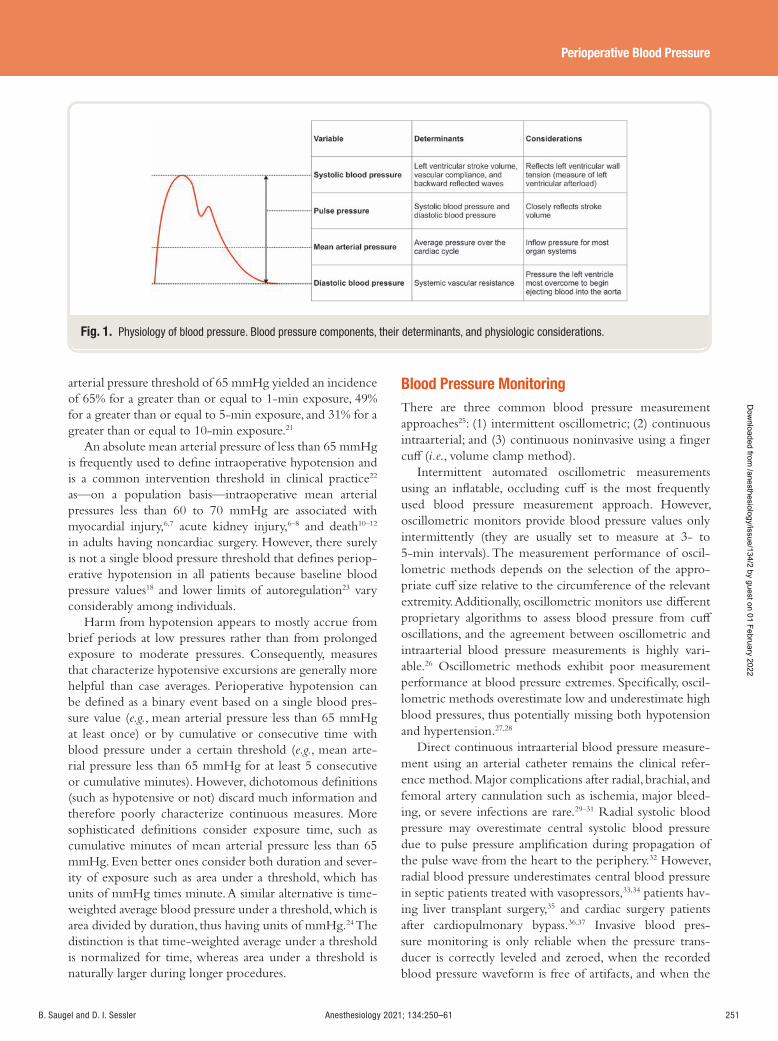
Anesthesiology 2021; 134:250–61 251
Perioperative Blood Pressure
B. Saugel and D. I. Sessler
arterial pressure threshold of 65 mmHg yielded an incidence of 65% for a greater than or equal to 1-min exposure, 49% for a greater than or equal to 5-min exposure, and 31% for a greater than or equal to 10-min exposure. 21
An absolute mean arterial pressure of less than 65 mmHg is frequently used to de ne intraoperative hypotension and is a common intervention threshold in clinical practice 22
as — on a population basis — intraoperative mean arterial pressures less than 60 to 70 mmHg are associated with myocardial injury, 6 , 7 acute kidney injury, 6 – 8 and death 10 – 12
in adults having noncardiac surgery. However, there surely is not a single blood pressure threshold that de nes periop-erative hypotension in all patients because baseline blood pressure values 18 and lower limits of autoregulation 23 vary considerably among individuals.
Harm from hypotension appears to mostly accrue from brief periods at low pressures rather than from prolonged exposure to moderate pressures. Consequently, measures that characterize hypotensive excursions are generally more helpful than case averages. Perioperative hypotension can be de ned as a binary event based on a single blood pres-sure value ( e.g. , mean arterial pressure less than 65 mmHg at least once) or by cumulative or consecutive time with blood pressure under a certain threshold ( e.g. , mean arte-rial pressure less than 65 mmHg for at least 5 consecutive or cumulative minutes). However, dichotomous de nitions (such as hypotensive or not) discard much information and therefore poorly characterize continuous measures. More sophisticated de nitions consider exposure time, such as cumulative minutes of mean arterial pressure less than 65 mmHg. Even better ones consider both duration and sever-ity of exposure such as area under a threshold, which has units of mmHg times minute. A similar alternative is time-weighted average blood pressure under a threshold, which is area divided by duration, thus having units of mmHg. 24 The distinction is that time-weighted average under a threshold is normalized for time, whereas area under a threshold is naturally larger during longer procedures.
Blood Pressure Monitoring There are three common blood pressure measurement approaches 25 : (1) intermittent oscillometric; (2) continuous intraarterial; and (3) continuous noninvasive using a nger cu ( i.e. , volume clamp method).
Intermittent automated oscillometric measurements using an in atable, occluding cu is the most frequently used blood pressure measurement approach. However, oscillometric monitors provide blood pressure values only intermittently (they are usually set to measure at 3- to 5-min intervals). The measurement performance of oscil-lometric methods depends on the selection of the appro-priate cu size relative to the circumference of the relevant extremity. Additionally, oscillometric monitors use di erent proprietary algorithms to assess blood pressure from cu oscillations, and the agreement between oscillometric and intraarterial blood pressure measurements is highly vari-able. 26 Oscillometric methods exhibit poor measurement performance at blood pressure extremes. Speci cally, oscil-lometric methods overestimate low and underestimate high blood pressures, thus potentially missing both hypotension and hypertension. 27 , 28
Direct continuous intraarterial blood pressure measure-ment using an arterial catheter remains the clinical refer-ence method. Major complications after radial, brachial, and femoral artery cannulation such as ischemia, major bleed-ing, or severe infections are rare. 29 – 31 Radial systolic blood pressure may overestimate central systolic blood pressure due to pulse pressure ampli cation during propagation of the pulse wave from the heart to the periphery. 32 However, radial blood pressure underestimates central blood pressure in septic patients treated with vasopressors, 33 , 34 patients hav-ing liver transplant surgery, 35 and cardiac surgery patients after cardiopulmonary bypass. 36 , 37 Invasive blood pres-sure monitoring is only reliable when the pressure trans-ducer is correctly leveled and zeroed, when the recorded blood pressure waveform is free of artifacts, and when the
Fig. 1. Physiology of blood pressure. Blood pressure components, their determinants, and physiologic considerations.
ALNV134N2_Text.indb 251ALNV134N2_Text.indb 251 29-Dec-20 19:44:0929-Dec-20 19:44:09
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

252 Anesthesiology 2021; 134:250–61 B. Saugel and D. I. Sessler
CLINICAL FOCUS REVIEW
dynamic response of the catheter/tubing/transducer system ( i.e. , “ damping ” ) is adequate. 38 Continuous invasive blood pressure monitoring detects twice as many hypotensive minutes, and triggers a third more vasopressor boluses than intermittent oscillometric blood pressure measurements in patients having major noncardiac surgery. 39
Noninvasive nger cu methods using the volume clamp method (also called vascular unloading technology) allow continuous blood pressure monitoring without arte-rial cannulation. 25 These systems use nger cu s housing an infrared photodiode and light detector to plethysmograph-ically estimate the blood volume in the nger arteries as it changes during the cardiac cycle. The system controls n-ger cu pressure to keep blood volume in the nger arter-ies constant. The arterial blood pressure waveform is then reconstructed from the cu pressure needed to keep blood volume in the nger arteries constant. 25 Because pulsatile blood ow in the nger is a prerequisite for nger cu pres-sure assessment, the method is unreliable during circulatory shock or high-dose vasopressor therapy.
Finger cu devices from various manufacturers use dif-ferent methods to account for changes in vascular tone, to obtain the nger blood pressure signal, and to esti-mate brachial blood pressure from nger blood pressure (either by using proprietary scaling algorithms or by cal-ibrating nger blood pressure to oscillometric upper-arm cu blood pressure measurements). 25 , 40 Thus each device needs to be validated separately against reference methods. Validation studies comparing continuous nger cu blood pressure measurements to arterial catheter – derived mea-surements show heterogeneous results, but several studies demonstrated interchangeability between blood pressure measurements obtained by either method. 41 In pilot ran-domized trials, continuous noninvasive nger cu blood pressure monitoring reduced intraoperative hypotension compared to intermittent oscillometric blood pressure monitoring. 24 , 42
Other blood pressure monitoring methods — such as the hydraulic coupling method, 43 applanation tonometry, 44 the pulse wave transit time method, 45 or the pulse decompo-sition method 46 — may prove to be important alternatives to conventional perioperative blood pressure monitoring methods, but all have inherent technical limitations and need meticulous validation before being broadly adopted in routine care. 47 , 48
Anesthesia professionals routinely evaluate blood pressure changes and try to predict when patients will become hypo-tensive. A recent advance is using machine learning, which is a subset of arti cial intelligence, to analyze features of the blood pressure waveform to predict hypotension. Hatib et al. 49 proposed a machine learning algorithm that predicts hypotension, de ned as mean arterial pressure less than 65 mmHg for at least 1 min, 5 or more min in advance — thus giving clinicians an opportunity to intervene and perhaps prevent hypotension. 49 , 50 This “ hypotension prediction
index ” indicates the probability of impending hypotension as a unitless number ranging from 0 to 100. The nal pre-diction model is based on 51 features of the arterial blood pressure waveform that were selected from more than 3,000 individual and more than 2.6 million combinatorial wave-form features. 49 The algorithm was trained on blood pres-sure waveforms of 1,334 surgical or critically ill patients and externally validated in 204 patients having surgery, showing a sensitivity of 88% and a speci city of 87% to predict hypo-tension 15 min before the event. 49 In another validation study in 255 patients having major surgery, the hypotension prediction index predicted intraoperative hypotension up to 15 min before the event with a sensitivity and speci city of 81% each. 51 Naturally, the hypotension prediction index algorithm cannot predict hypotension consequent to clini-cal interventions, including hypotension caused by pressure on major vessels by surgeons or changes in patient position such as reverse Trendelenburg position. In a single-cen-ter trial in patients having hip arthroplasty, intraoperative hypotension occurred less frequently and for shorter dura-tions in 25 patients randomized to hypotension prediction index – guided blood pressure management compared to 24 patients with routine blood pressure management and 50 patients from a historic control group. 52 In another small preliminary single-center trial in 68 noncardiac surgery patients, hypotension prediction index – guided blood pres-sure management markedly reduced the time-weighted average of a mean arterial pressure less than 65 mmHg, as well as the incidence and absolute and relative duration of hypotension compared with routine care. 53 However, in another trial of 214 patients having moderate- to high-risk inpatient noncardiac surgery, no reduction in the amount of hypotension was observed in patients randomized to man-agement with hypotension prediction index-guided hemo-dynamic and uid management. 54
Perioperative Blood Pressure and Postoperative Outcomes Acute kidney injury and myocardial injury are major post-operative outcomes associated with hypotension in adults having noncardiac surgery. Many studies de ne postop-erative acute kidney injury based on the Kidney Disease: Improving Global Outcomes (KDIGO) de nition that de nes acute kidney injury as any of the following criteria: increase in serum creatinine by greater than or equal to 0.3 mg/dl within 48 h, increase in serum creatinine greater than or equal to 1.5 times the baseline value (which is known or presumed to have occurred within the previous 7 days), or urine volume less than 0.5 ml · kg -1 · h -1 for 6 h. 55 Many studies on postoperative acute kidney injury exclude the oliguria criteria of the KDIGO de nition. Additionally, many studies only consider the rst 48 h after surgery when using the greater than or equal to 0.3 mg/dl serum creatinine increase criterion, although the KDIGO de nition refers to a greater than or equal to 0.3 mg/dl
ALNV134N2_Text.indb 252ALNV134N2_Text.indb 252 29-Dec-20 19:44:0929-Dec-20 19:44:09
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:250–61 253
Perioperative Blood Pressure
B. Saugel and D. I. Sessler
serum creatinine increase within any 48-h window within the observation period. 56
Myocardial infarction is de ned by fourth Universal De nition of Myocardial Infarction. 57 However, it is now known that more than 90% of postoperative myocar-dial injury is asymptomatic, and that most injury is not accompanied by clinical signs such as electrocardiogram changes that are required for diagnosis of myocardial infarc-tion. 58 – 60 Troponin elevation of apparently ischemic origin, with or without symptoms and signs, is therefore termed “ myocardial injury after noncardiac surgery. ” 61 Although most myocardial injury patients have underlying coronary artery disease, the etiology of myocardial injury after non-cardiac surgery seems to predominantly result from oxy-gen supply – demand mismatch rather than thrombosis. 61 , 62
Myocardial injury after noncardiac surgery is common, with a reported incidence ranging from 8 to 18% in surgical inpatients depending on baseline and operative risk, 2 , 58 – 60
and is associated with postoperative nonfatal cardiac arrest, congestive heart failure, stroke, and 30-day mortality. 2 , 58 – 60
Mortality in patients with myocardial injury after noncar-diac surgery is 4 to 10%. 56 – 58 Mortality after myocardial injury not ful lling the additional criteria required for a diagnosis of myocardial infarction is nearly as high as after myocardial infarction. 59 , 60
Baseline patient risk factors such as age and cardiovas-cular history are far more strongly associated with postop-erative acute kidney injury 4 , 5 and myocardial injury 5 than intraoperative hypotension. But hypotension, in contrast to most baseline risk factors, is potentially modi able — and therefore of special interest.
Intraoperative Blood Pressure
Various registry analyses have identi ed population harm thresholds for intraoperative hypotension by exploring associations between blood pressure and postoperative out-comes in patients who had noncardiac surgery with general anesthesia. 22 , 63
Cumulative evidence suggests that on a population basis, intraoperative mean arterial pressures less than 60 to 70 mmHg are associated with myocardial injury, 6 , 7 acute kidney injury, 6 – 8 and death 10 – 12 in adults having noncardiac surgery. The association between organ injury and hypotension is a function of both severity and duration, with lower pressures requiring shorter exposures. 6 , 7 , 63 A systematic review of 42 studies summarized reported risks of myocardial injury, acute kidney injury, and death depending on the severity and duration of intraoperative hypotension. 63 The risk of any end-organ injury was slightly increased when mean arterial pressures were sustained at less than 70 mmHg for just 10 min. 63 The risk was moderately increased with expo-sures to mean arterial pressures less than 65 to 60 mmHg for at least 5 min, or any exposure to mean arterial pressures less than 55 to 50 mmHg. 63 High risk of any end-organ injury was reported for exposures to mean arterial pressures less
than 65 mmHg for at least 20 min, mean arterial pressures less than 50 mmHg for at least 5 min, or any exposure to mean arterial pressures less than 40 mmHg. 63
Over a wide range of preoperative baseline blood pres-sures, the association between intraoperative hypotension and postoperative myocardial injury is comparably strong when intraoperative hypotension is de ned by absolute or relative mean arterial pressure thresholds. 7 For example, an absolute mean arterial pressure threshold of 65 mmHg and a relative reduction from clinic baseline pressure of 30% are comparably predictive for myocardial injury ( g. 2 ). 7
However, absolute thresholds are easier to use than relative thresholds. Immediate preinduction blood pressures poorly re ect ambulatory blood pressures, 18 which are considered the best characterization of baseline blood pressure. 16 , 64
Systolic blood pressure and mean arterial pressure are roughly comparably associated with postoperative acute kidney and myocardial injury, but of course at di erent harm thresholds. For systolic blood pressure, harm begins to accrue below about 90 mmHg, whereas the threshold is about 65 mmHg for mean arterial pressure. 5 Blood pressure variability is only marginally associated with postoperative mortality. 10
Clinically important hypotension occurs not only during surgery but also between anesthetic induction and incision. 65 Although the preincision period is short com-pared to the entire intraoperative duration, in one study it accounted for a third of all hypotension observed through-out the entire anesthetic and was independently associated with major complications. 66 Hypotension occurring before surgical incision is presumably largely determined by base-line patient risk factors and anesthetic management. A cor-ollary is that blood pressure during anesthesia induction is at least mostly under control of anesthesiologists.
Postoperative Blood Pressure
Postoperative hypotension during the initial days after sur-gery is common 9 and is independently associated with post-operative myocardial injury 67 and a composite of myocardial infarction and death, 9 even after adjusting for intraoperative hypotension. Interestingly, in one cohort of patients having intermediate- to high-risk noncardiac surgery, only post-operative hypotension — and not intraoperative hypoten-sion — was associated with myocardial injury. 67 In patients admitted to the intensive care unit after noncardiac surgery, postoperative hypotension is associated with acute kidney injury and a composite of myocardial injury and death. 68
Postoperative hypotension may thus be a poten-tially modi able risk factor for organ injury. The relation between intraoperative and postoperative blood pressures requires further investigation as the incidence and severity of intraoperative hypotension may help identify patients at risk for postoperative hypotension.
While frequent blood pressure assessment is routine in operating rooms and intensive care units, postoperative
ALNV134N2_Text.indb 253ALNV134N2_Text.indb 253 29-Dec-20 19:44:0929-Dec-20 19:44:09
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
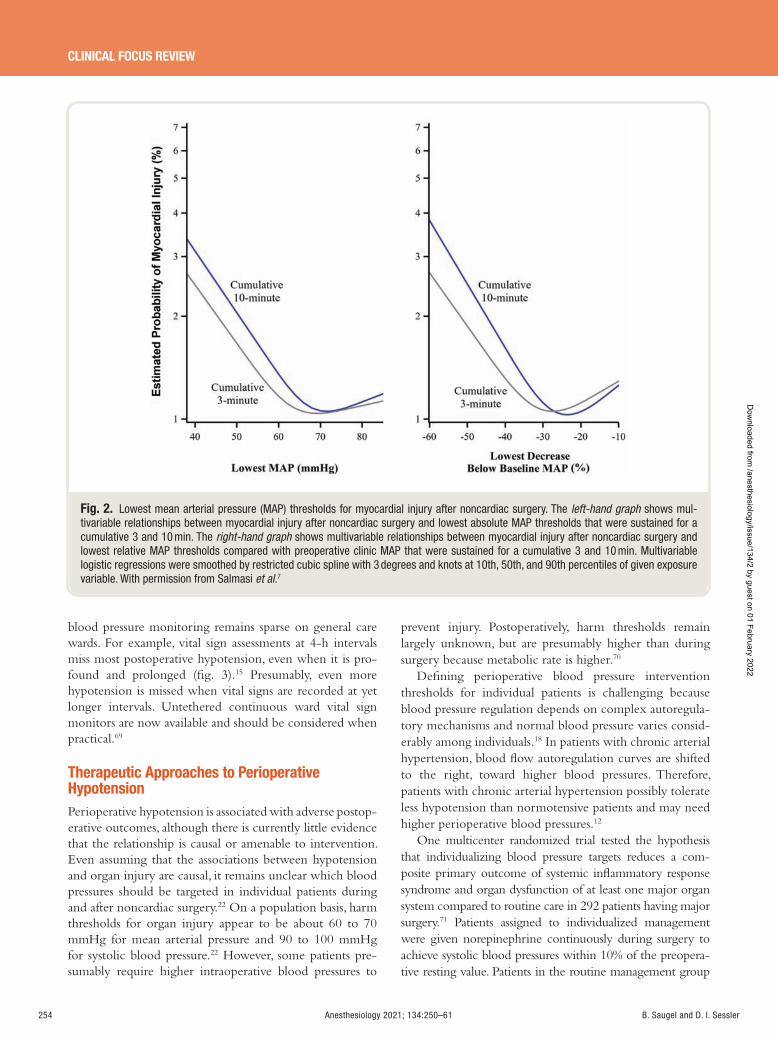
254 Anesthesiology 2021; 134:250–61 B. Saugel and D. I. Sessler
CLINICAL FOCUS REVIEW
blood pressure monitoring remains sparse on general care wards. For example, vital sign assessments at 4-h intervals miss most postoperative hypotension, even when it is pro-found and prolonged ( g. 3 ). 15 Presumably, even more hypotension is missed when vital signs are recorded at yet longer intervals. Untethered continuous ward vital sign monitors are now available and should be considered when practical. 69
Therapeutic Approaches to Perioperative Hypotension Perioperative hypotension is associated with adverse postop-erative outcomes, although there is currently little evidence that the relationship is causal or amenable to intervention. Even assuming that the associations between hypotension and organ injury are causal, it remains unclear which blood pressures should be targeted in individual patients during and after noncardiac surgery. 22 On a population basis, harm thresholds for organ injury appear to be about 60 to 70 mmHg for mean arterial pressure and 90 to 100 mmHg for systolic blood pressure. 22 However, some patients pre-sumably require higher intraoperative blood pressures to
prevent injury. Postoperatively, harm thresholds remain largely unknown, but are presumably higher than during surgery because metabolic rate is higher. 70
De ning perioperative blood pressure intervention thresholds for individual patients is challenging because blood pressure regulation depends on complex autoregula-tory mechanisms and normal blood pressure varies consid-erably among individuals. 18 In patients with chronic arterial hypertension, blood ow autoregulation curves are shifted to the right, toward higher blood pressures. Therefore, patients with chronic arterial hypertension possibly tolerate less hypotension than normotensive patients and may need higher perioperative blood pressures. 12
One multicenter randomized trial tested the hypothesis that individualizing blood pressure targets reduces a com-posite primary outcome of systemic in ammatory response syndrome and organ dysfunction of at least one major organ system compared to routine care in 292 patients having major surgery. 71 Patients assigned to individualized management were given norepinephrine continuously during surgery to achieve systolic blood pressures within 10% of the preopera-tive resting value. Patients in the routine management group
Fig. 2. Lowest mean arterial pressure (MAP) thresholds for myocardial injury after noncardiac surgery. The left-hand graph shows mul-tivariable relationships between myocardial injury after noncardiac surgery and lowest absolute MAP thresholds that were sustained for a cumulative 3 and 10 min. The right-hand graph shows multivariable relationships between myocardial injury after noncardiac surgery and lowest relative MAP thresholds compared with preoperative clinic MAP that were sustained for a cumulative 3 and 10 min. Multivariable logistic regressions were smoothed by restricted cubic spline with 3 degrees and knots at 10th, 50th, and 90th percentiles of given exposure variable. With permission from Salmasi et al. 7
ALNV134N2_Text.indb 254ALNV134N2_Text.indb 254 29-Dec-20 19:44:0929-Dec-20 19:44:09
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
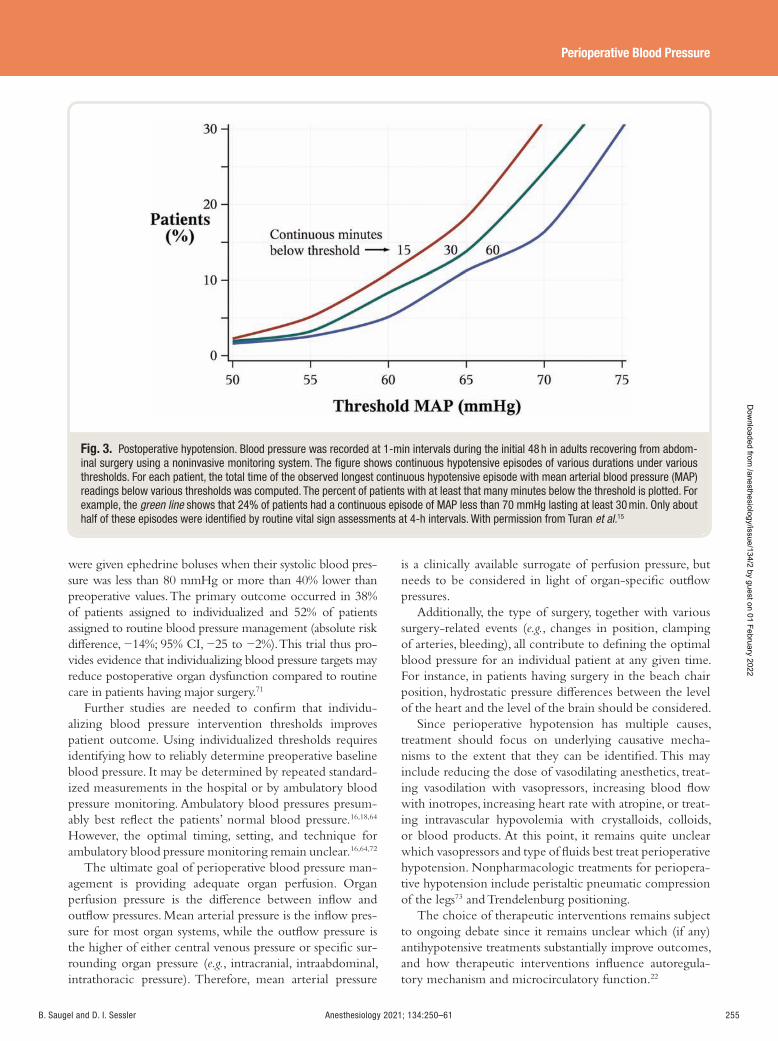
Anesthesiology 2021; 134:250–61 255
Perioperative Blood Pressure
B. Saugel and D. I. Sessler
were given ephedrine boluses when their systolic blood pres-sure was less than 80 mmHg or more than 40% lower than preoperative values. The primary outcome occurred in 38% of patients assigned to individualized and 52% of patients assigned to routine blood pressure management (absolute risk di erence, − 14%; 95% CI, − 25 to − 2%). This trial thus pro-vides evidence that individualizing blood pressure targets may reduce postoperative organ dysfunction compared to routine care in patients having major surgery. 71
Further studies are needed to con rm that individu-alizing blood pressure intervention thresholds improves patient outcome. Using individualized thresholds requires identifying how to reliably determine preoperative baseline blood pressure. It may be determined by repeated standard-ized measurements in the hospital or by ambulatory blood pressure monitoring. Ambulatory blood pressures presum-ably best re ect the patients ’ normal blood pressure. 16 , 18 , 64
However, the optimal timing, setting, and technique for ambulatory blood pressure monitoring remain unclear. 16 , 64 , 72
The ultimate goal of perioperative blood pressure man-agement is providing adequate organ perfusion. Organ perfusion pressure is the di erence between in ow and out ow pressures. Mean arterial pressure is the in ow pres-sure for most organ systems, while the out ow pressure is the higher of either central venous pressure or speci c sur-rounding organ pressure ( e.g. , intracranial, intraabdominal, intrathoracic pressure). Therefore, mean arterial pressure
is a clinically available surrogate of perfusion pressure, but needs to be considered in light of organ-speci c out ow pressures.
Additionally, the type of surgery, together with various surgery-related events ( e.g. , changes in position, clamping of arteries, bleeding), all contribute to de ning the optimal blood pressure for an individual patient at any given time. For instance, in patients having surgery in the beach chair position, hydrostatic pressure di erences between the level of the heart and the level of the brain should be considered.
Since perioperative hypotension has multiple causes, treatment should focus on underlying causative mecha-nisms to the extent that they can be identi ed. This may include reducing the dose of vasodilating anesthetics, treat-ing vasodilation with vasopressors, increasing blood ow with inotropes, increasing heart rate with atropine, or treat-ing intravascular hypovolemia with crystalloids, colloids, or blood products. At this point, it remains quite unclear which vasopressors and type of uids best treat perioperative hypotension. Nonpharmacologic treatments for periopera-tive hypotension include peristaltic pneumatic compression of the legs 73 and Trendelenburg positioning.
The choice of therapeutic interventions remains subject to ongoing debate since it remains unclear which (if any) antihypotensive treatments substantially improve outcomes, and how therapeutic interventions in uence autoregula-tory mechanism and microcirculatory function. 22
Fig. 3. Postoperative hypotension. Blood pressure was recorded at 1-min intervals during the initial 48 h in adults recovering from abdom-inal surgery using a noninvasive monitoring system. The fi gure shows continuous hypotensive episodes of various durations under various thresholds. For each patient, the total time of the observed longest continuous hypotensive episode with mean arterial blood pressure (MAP) readings below various thresholds was computed. The percent of patients with at least that many minutes below the threshold is plotted. For example, the green line shows that 24% of patients had a continuous episode of MAP less than 70 mmHg lasting at least 30 min. Only about half of these episodes were identifi ed by routine vital sign assessments at 4-h intervals. With permission from Turan et al. 15
ALNV134N2_Text.indb 255ALNV134N2_Text.indb 255 29-Dec-20 19:44:0929-Dec-20 19:44:09
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

256 Anesthesiology 2021; 134:250–61 B. Saugel and D. I. Sessler
CLINICAL FOCUS REVIEW
Future Research Perhaps the most important remaining research question is whether there is a causal relationship between intraoperative and/or postoperative blood pressures and organ injury. The relationship between hypotension and serious complications is currently supported by many observational analyses, but only by sparse randomized data. 71 Thus, robust randomized trials testing the hypothesis that avoiding intraoperative and post-operative hypotension improves postoperative outcomes are needed. Similarly, which blood pressure intervention thresholds should be used intraoperatively and postoperatively remains to be determined, as well as whether they should be de ned by absolute thresholds or relative blood pressure changes.
Trials are needed to determine the best treatment strategy for intraoperative and postoperative hypotension. Presumably, interventions targeting various causes of intra-operative and postoperative hypotension are preferable to pragmatic approaches such as simply giving vasopressors. And nally, trials are needed to evaluate potential bene ts from current and future monitoring technologies, as well as treatment recommendations based on machine learning and arti cial intelligence.
Conclusions
Hypotension is common during noncardiac surgery, and is associated with myocardial injury, 6 , 7 acute kidney injury, 6 – 8
and death. 10 – 12 Postoperative hypotension is common, often prolonged, and associated with myocardial injury and death. 9 , 67 Postoperative hypotension on general care wards is largely missed by conventional intermittent blood pres-sure monitoring. 15
Evidence from registry analyses suggests that the intra-operative population harm thresholds for organ injury are 60 to 70 mmHg for mean arterial pressure and 90 to 100 mmHg for systolic blood pressure. 22 Postoperative harm thresholds remain unclear, but are probably slightly higher.
Serious cardiovascular 5 and renal complications 4 , 5 are more strongly associated with baseline risk than hypo-tension, but hypotension di ers from other risk factors in being potentially modi able. The question, then, is whether observed associations between hypotension and complica-tions are causal, and thus amenable to intervention. There is currently only sparse evidence from trials to establish a causal connection and identify treatment e ects. For that matter, when and how best to intervene also remains unknown.
Pressing research needs include determining whether preventing and treating hypotension reduces complications, and to what extent. If the relationship is indeed causal, the next steps will be to determine when intervention is help-ful, and which interventions are safe and e ective.
In the meantime, clinicians should consider hypotension to be a modi able risk factor that is associated with renal and myocardial injury, as well as death. Pending results from robust
clinical trials, avoiding hypotension seems prudent. Based on current evidence and pathophysiologic rationale, we suggest that mean arterial pressure should be kept above 65 mmHg during surgery and somewhat higher postoperatively.
Research Support
Support was provided solely from institutional and/or departmental sources.
Competing Interests
Dr. Saugel received honoraria for consulting and giv-ing lectures, and refunds of travel expenses from Edwards Lifesciences Inc. (Irvine, California); honoraria for con-sulting and giving lectures, institutional restricted research grants, and refunds of travel expenses from Pulsion Medical Systems SE (Feldkirchen, Germany); institutional restricted research grants, honoraria for giving lectures, and refunds of travel expenses from CNSystems Medizintechnik GmbH (Graz, Austria); institutional restricted research grants from Retia Medical LLC (Valhalla, New York); honoraria for giving lectures from Philips Medizin Systeme Böblingen GmbH (Böblingen, Germany); and honoraria for consulting, institutional restricted research grants, and refunds of travel expenses from Tensys Medical Inc. (San Diego, California). Dr. Sessler is a consultant for Edwards Lifesciences (Irvine, California), Pacira Biosciences (Parsippany, New Jersey), and Sensifree (Cupertino, California).
Correspondence
Address correspondence to Dr. Saugel: Department of Anesthesiology, Center of Anesthesiology and Intensive Care Medicine, University Medical Center Hamburg-Eppendorf, Martinistrasse 52, 20246 Hamburg, Germany. [email protected] . Anesthesiology’s articles are made freely accessible to all readers on www.anesthesiology.org, for personal use only, 6 months from the cover date of the issue.
References
1. Li G , Warner M , Lang BH , Huang L , Sun LS : Epidemiology of anesthesia-related mortality in the United States, 1999-2005. A nesthesiology 2009 ; 110 : 759 – 65
2. Investigators VEiNSPCEVS : Association between complications and death within 30 days after noncar-diac surgery . CMAJ 2019 ; 191 : E830 – 7
3. Nepogodiev D , Martin J , Biccard B , Makupe A , Bhangu A ; National Institute for Health Research Global Health Research Unit on Global Surgery : Global bur-den of postoperative death. Lancet 2019 ; 393 : 401
4. Mathis MR , Naik BI , Freundlich RE , Shanks AM , Heung M , Kim M , Burns ML , Colquhoun DA , Rangrass G , Janda A , Engoren MC , Saager L , Tremper
ALNV134N2_Text.indb 256ALNV134N2_Text.indb 256 29-Dec-20 19:44:1029-Dec-20 19:44:10
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:250–61 257
Perioperative Blood Pressure
B. Saugel and D. I. Sessler
KK , Kheterpal S , Aziz MF , Co man T , Durieux ME , Levy WJ , Schonberger RB , Soto R , Wilczak J , Berman MF , Berris J , Biggs DA , Coles P , Craft RM , Cummings KC , Ellis TA 2nd , Fleishut PM , Helsten DL , Jameson LC , van Klei WA , Kooij F , LaGorio J , Lins S , Miller SA , Molina S , Nair B , Paganelli WC , Peterson W , Tom S , Wanderer JP , Wedeven C ; Multicenter Perioperative Outcomes Group Investigators : Preoperative risk and the association between hypotension and postop-erative acute kidney injury. A nesthesiology 2020 ; 132 : 461 – 75
5. Ahuja S , Mascha EJ , Yang D , Maheshwari K , Cohen B , Khanna AK , Ruetzler K , Turan A , Sessler DI : Associations of intraoperative radial arterial systolic, diastolic, mean, and pulse pressures with myocardial and acute kidney injury after noncardiac surgery: A retrospective cohort analysis. A nesthesiology 2020 ; 132 : 291 – 306
6. Walsh M , Devereaux PJ , Garg AX , Kurz A , Turan A , Rodseth RN , Cywinski J , Thabane L , Sessler DI : Relationship between intraoperative mean arterial pressure and clinical outcomes after noncardiac sur-gery: Toward an empirical de nition of hypotension. A nesthesiology 2013 ; 119 : 507 – 15
7. Salmasi V , Maheshwari K , Yang D , Mascha EJ , Singh A , Sessler DI , Kurz A : Relationship between intraoperative hypotension, de ned by either reduction from baseline or absolute thresholds, and acute kidney and myocar-dial injury after noncardiac surgery: A retrospective cohort analysis. A nesthesiology 2017 ; 126 : 47 – 65
8. Sun LY , Wijeysundera DN , Tait GA , Beattie WS : Association of intraoperative hypotension with acute kidney injury after elective noncardiac surgery. A nesthesiology 2015 ; 123 : 515 – 23
9. Sessler DI , Meyho CS , Zimmerman NM , Mao G , Leslie K , V á squez SM , Balaji P , Alvarez-Garcia J , Cavalcanti AB , Parlow JL , Rahate PV , Seeberger MD , Gossetti B , Walker SA , Premchand RK , Dahl RM , Duceppe E , Rodseth R , Botto F , Devereaux PJ : Period-dependent associations between hypotension during and for four days after noncardiac surgery and a com-posite of myocardial infarction and death: A substudy of the POISE-2 Trial. A nesthesiology 2018 ; 128 : 317 – 27
10. Mascha EJ , Yang D , Weiss S , Sessler DI : Intraoperative mean arterial pressure variability and 30-day mortality in patients having noncardiac surgery. A nesthesiology 2015 ; 123 : 79 – 91
11. Monk TG , Bronsert MR , Henderson WG , Mangione MP , Sum-Ping ST , Bentt DR , Nguyen JD , Richman JS , Meguid RA , Hammermeister KE : Association between intraoperative hypotension and hypertension and 30-day postoperative mortality in noncardiac sur-gery. A nesthesiology 2015 ; 123 : 307 – 19
12. Stapelfeldt WH , Yuan H , Dryden JK , Strehl KE , Cywinski JB , Ehrenfeld JM , Bromley P : The SLUScore: A novel method for detecting hazardous hypotension in adult patients undergoing noncardiac surgical pro-cedures. Anesth Analg 2017 ; 124 : 1135 – 52
13. Reich DL , Hossain S , Krol M , Baez B , Patel P , Bernstein A , Bodian CA : Predictors of hypotension after induc-tion of general anesthesia. Anesth Analg 2005 ; 101 : 622 – 8, table of contents
14. Cheung CC , Martyn A , Campbell N , Frost S , Gilbert K , Michota F , Seal D , Ghali W , Khan NA : Predictors of intraoperative hypotension and bradycardia. Am J Med 2015 ; 128 : 532 – 8
15. Turan A , Chang C , Cohen B , Saasouh W , Essber H , Yang D , Ma C , Hovsepyan K , Khanna AK , Vitale J , Shah A , Ruetzler K , Maheshwari K , Sessler DI : Incidence, severity, and detection of blood pressure perturbations after abdominal surgery: A prospective blinded obser-vational study. A nesthesiology 2019 ; 130 : 550 – 9
16. Ackland GL , Brudney CS , Cecconi M , Ince C , Irwin MG , Lacey J , Pinsky MR , Grocott MP , Mythen MG , Edwards MR , Miller TE ; Perioperative Quality Initiative-3 Workgroup; POQI Chairs; Physiology Group; Preoperative Blood Pressure Group; Intraoperative Blood Pressure Group; Postoperative Blood Pressure Group : Perioperative Quality Initiative consensus statement on the physiology of arterial blood pressure control in perioperative medicine. Br J Anaesth 2019 ; 122 : 542 – 51
17. Meng L , Wang Y , Zhang L , McDonagh DL : Heterogeneity and variability in pressure autoregula-tion of organ blood ow: Lessons learned over 100 + years. Crit Care Med 2019 ; 47 : 436 – 48
18. Saugel B , Reese PC , Sessler DI , Burfeindt C , Nicklas JY , Pinnschmidt HO , Reuter DA , S ü dfeld S : Automated ambulatory blood pressure measurements and intra-operative hypotension in patients having noncardiac surgery with general anesthesia: A prospective observa-tional study. A nesthesiology 2019 ; 131 : 74 – 83
19. Whelton PK , Carey RM , Aronow WS , Casey DE Jr , Collins KJ , Dennison Himmelfarb C , DePalma SM , Gidding S , Jamerson KA , Jones DW , MacLaughlin EJ , Muntner P , Ovbiagele B , Smith SC Jr , Spencer CC , Sta ord RS , Taler SJ , Thomas RJ , Williams KA Sr , Williamson JD , Wright JT Jr : 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018 ; 71 : 1269 – 324
20. Millar-Craig MW , Bishop CN , Raftery EB : Circadian variation of blood-pressure. Lancet 1978 ; 1 : 795 – 7
ALNV134N2_Text.indb 257ALNV134N2_Text.indb 257 29-Dec-20 19:44:1029-Dec-20 19:44:10
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
258 Anesthesiology 2021; 134:250–61 B. Saugel and D. I. Sessler
CLINICAL FOCUS REVIEW
21. Bijker JB , van Klei WA , Kappen TH , van Wolfswinkel L , Moons KG , Kalkman CJ : Incidence of intraopera-tive hypotension as a function of the chosen de nition: Literature de nitions applied to a retrospective cohort using automated data collection. A nesthesiology 2007 ; 107 : 213 – 20
22. Sessler DI , Bloomstone JA , Aronson S , Berry C , Gan TJ , Kellum JA , Plumb J , Mythen MG , Grocott MPW , Edwards MR , Miller TE , Miller TE , Mythen MG , Grocott MP , Edwards MR ; Perioperative Quality Initiative-3 Workgroup; POQI Chairs; Physiology Group; Preoperative Blood Pressure Group; Intra-operative Blood Pressure Group; Postoperative Blood Pressure Group : Perioperative Quality Initiative consensus statement on intraoperative blood pressure, risk and out-comes for elective surgery. Br J Anaesth 2019 ; 122 : 563 – 74
23. Brady KM , Hudson A , Hood R , DeCaria B , Lewis C , Hogue CW : Personalizing the de nition of hypo-tension to protect the brain. A nesthesiology 2020 ; 132 : 170 – 9
24. Maheshwari K , Khanna S , Bajracharya GR , Makarova N , Riter Q , Raza S , Cywinski JB , Argalious M , Kurz A , Sessler DI : A randomized trial of continuous non-invasive blood pressure monitoring during noncardiac surgery. Anesth Analg 2018 ; 127 : 424 – 31
25. Saugel B , Dueck R , Wagner JY : Measurement of blood pressure. Best Pract Res Clin Anaesthesiol 2014 ; 28 : 309 – 22
26. Picone DS , Schultz MG , Otahal P , Aakhus S , Al-Jumaily AM , Black JA , Bos WJ , Chambers JB , Chen CH , Cheng HM , Cremer A , Davies JE , Dwyer N , Gould BA , Hughes AD , Lacy PS , Laugesen E , Liang F , Melamed R , Muecke S , Ohte N , Okada S , Omboni S , Ott C , Peng X , Pereira T , Pucci G , Rajani R , Roberts-Thomson P , Rossen NB , Sueta D , Sinha MD , Schmieder RE , Smulyan H , Srikanth VK , Stewart R , Stou er GA , Takazawa K , Wang J , Westerhof BE , Weber F , Weber T , Williams B , Yamada H , Yamamoto E , Sharman JE : Accuracy of cu -measured blood pressure: Systematic reviews and meta-analyses. J Am Coll Cardiol 2017 ; 70 : 572 – 86
27. Wax DB , Lin HM , Leibowitz AB : Invasive and con-comitant noninvasive intraoperative blood pressure monitoring: observed di erences in measurements and associated therapeutic interventions. A nesthesiology 2011 ; 115 : 973 – 8
28. Lehman LW , Saeed M , Talmor D , Mark R , Malhotra A : Methods of blood pressure measurement in the ICU. Crit Care Med 2013 ; 41 : 34 – 40
29. Scheer B , Perel A , Pfei er UJ : Clinical review: Complications and risk factors of peripheral arte-rial catheters used for haemodynamic monitoring in anaesthesia and intensive care medicine. Crit Care 2002 ; 6 : 199 – 204
30. Nuttall G , Burckhardt J , Hadley A , Kane S , Kor D , Marienau MS , Schroeder DR , Handlogten K , Wilson G ,
Oliver WC : Surgical and patient risk factors for severe arterial line complications in adults. A nesthesiology 2016 ; 124 : 590 – 7
31. Singh A , Bahadorani B , Wake eld BJ , Makarova N , Kumar PA , Tong MZ , Sessler DI , Duncan AE : Brachial arterial pressure monitoring during cardiac surgery rarely causes complications. A nesthesiology 2017 ; 126 : 1065 – 76
32. Pauca AL , Wallenhaupt SL , Kon ND , Tucker WY : Does radial artery pressure accurately re ect aortic pressure? Chest 1992 ; 102 : 1193 – 8
33. Dorman T , Breslow MJ , Lipsett PA , Rosenberg JM , Balser JR , Almog Y , Rosenfeld BA : Radial artery pres-sure monitoring underestimates central arterial pres-sure during vasopressor therapy in critically ill surgical patients. Crit Care Med 1998 ; 26 : 1646 – 9
34. Kim WY , Jun JH , Huh JW , Hong SB , Lim CM , Koh Y : Radial to femoral arterial blood pressure di erences in septic shock patients receiving high-dose norepineph-rine therapy. Shock 2013 ; 40 : 527 – 31
35. Lee M , Weinberg L , Pearce B , Scurrah N , Story DA , Pillai P , McCall PR , McNicol LP , Peyton PJ : Agreement between radial and femoral arterial blood pressure measurements during orthotopic liver transplantation. Crit Care Resusc 2015 ; 17 : 101 – 7
36. Gravlee GP , Wong AB , Adkins TG , Case LD , Pauca AL : A comparison of radial, brachial, and aortic pressures after cardiopulmonary bypass. J Cardiothorac Anesth 1989 ; 3 : 20 – 6
37. Fuda G , Denault A , Deschamps A , Bouchard D , Fortier A , Lambert J , Couture P : Risk factors involved in cen-tral-to-radial arterial pressure gradient during cardiac surgery. Anesth Analg 2016 ; 122 : 624 – 32
38. Saugel B , Kouz K , Meidert AS , Schulte-Uentrop L , Romagnoli S : How to measure blood pressure using an arterial catheter: A systematic 5-step approach. Crit Care 2020 ; 24 : 172
39. Naylor AJ , Sessler DI , Maheshwari K , Khanna AK , Yang D , Mascha EJ , Suleiman I , Reville EM , Cote D , Hutcherson MT , Nguyen BM , Elsharkawy H , Kurz A : Arterial catheters for early detection and treat-ment of hypotension during major noncardiac sur-gery: A randomized trial . Anesth Analg 2019 ; doi: 10.1213/ANE.000000000000437
40. Saugel B , Cecconi M , Hajjar LA : Noninvasive cardiac output monitoring in cardiothoracic surgery patients: Available methods and future directions. J Cardiothorac Vasc Anesth 2019 ; 33 : 1742 – 52
41. Saugel B , Hoppe P , Nicklas JY , Kouz K , K ö rner A , Hempel JC , Vos JJ , Sch ö n G , Scheeren TWL : Continuous noninvasive pulse wave analysis using n-ger cu technologies for arterial blood pressure and cardiac output monitoring in perioperative and inten-sive care medicine: A systematic review and meta-anal-ysis. Br J Anaesth 2020 ; 125 : 25 – 37
ALNV134N2_Text.indb 258ALNV134N2_Text.indb 258 29-Dec-20 19:44:1029-Dec-20 19:44:10
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:250–61 259
Perioperative Blood Pressure
B. Saugel and D. I. Sessler
42. Meidert AS , Nold JS , Hornung R , Paulus AC , Zwi ß ler B , Czerner S : The impact of continuous non-invasive arterial blood pressure monitoring on blood pressure stability during general anaesthesia in orthopaedic patients: A randomised trial. Eur J Anaesthesiol 2017 ; 34 : 716 – 22
43. Briegel J , B ä hner T , Kreitmeier A , Conter P , Fraccaroli L , Meidert AS , Tholl M , Papadakis G , Deunert A , Bauer A , Hoeft A , Pfei er UJ : Clinical evaluation of a high- -delity upper arm cu to measure arterial blood pres-sure during noncardiac surgery. A nesthesiology 2020 ; 133 : 997 – 1006
44. Dueck R , Goedje O , Clopton P : Noninvasive con-tinuous beat-to-beat radial artery pressure via TL-200 applanation tonometry. J Clin Monit Comput 2012 ; 26 : 75 – 83
45. Kim SH , Song JG , Park JH , Kim JW , Park YS , Hwang GS : Beat-to-beat tracking of systolic blood pressure using noninvasive pulse transit time during anesthesia induction in hypertensive patients. Anesth Analg 2013 ; 116 : 94 – 100
46. Gratz I , Deal E , Spitz F , Baruch M , Allen IE , Seaman JE , Pukenas E , Jean S : Continuous non-invasive nger cu CareTaker ® comparable to invasive intra-arterial pressure in patients undergoing major intra-abdominal surgery. BMC Anesthesiol 2017 ; 17 : 48
47. Michard F , Sessler DI , Saugel B : Non-invasive arte-rial pressure monitoring revisited. Intensive Care Med 2018 ; 44 : 2213 – 5
48. Michard F , Scheeren TWL , Saugel B : A glimpse into the future of postoperative arterial blood pressure monitoring. Br J Anaesth 2020 ; 125 : 113 – 5
49. Hatib F , Jian Z , Buddi S , Lee C , Settels J , Sibert K , Rinehart J , Cannesson M : Machine-learning algorithm to predict hypotension based on high- delity arterial pressure waveform analysis. A nesthesiology 2018 ; 129 : 663 – 74
50. Saugel B , Kouz K , Hoppe P , Maheshwari K , Scheeren TWL : Predicting hypotension in perioperative and intensive care medicine. Best Pract Res Clin Anaesthesiol 2019 ; 33 : 189 – 97
51. Davies SJ , Vistisen ST , Jian Z , Hatib F , Scheeren TWL : Ability of an arterial waveform analysis-derived hypo-tension prediction index to predict future hypoten-sive events in surgical patients. Anesth Analg 2020 ; 130 : 352 – 9
52. Schneck E , Schulte D , Habig L , Ruhrmann S , Edinger F , Markmann M , Habicher M , Rickert M , Koch C , Sander M : Hypotension prediction index based pro-tocolized haemodynamic management reduces the incidence and duration of intraoperative hypotension in primary total hip arthroplasty: A single centre fea-sibility randomised blinded prospective interventional trial. J Clin Monit Comput 2020 ; 34 : 1149 – 58
53. Wijnberge M , Geerts BF , Hol L , Lemmers N , Mulder MP , Berge P , Schenk J , Terwindt LE , Hollmann MW , Vlaar AP , Veelo DP : E ect of a machine learning-de-rived early warning system for intraoperative hypo-tension vs standard care on depth and duration of intraoperative hypotension during elective noncardiac surgery: The HYPE randomized clinical trial. JAMA 2020 ; 323 : 1052 – 60
54. Maheshwari K , Shimada T , Yang D , Khanna S , Cywinski JB , Ire n SA , Ayad S , Turan A , Ruetzler K , Qiu Y , Saha P , Mascha EJ , Sessler DI : Hypotension prediction index for prevention of hypotension during moderate- to high-risk noncardiac surgery . A nesthesiology 2020 ; 133 : 1214 – 22
55. Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group : KDIGO Clinical Practice Guideline for acute kidney injury . Kidney Inter Suppl 2012; 2:1–138
56. McIlroy DR , Bellomo R , Billings FT 4th , Karkouti K , Prowle JR , Shaw AD , Myles PS : Systematic review and consensus de nitions for the Standardised Endpoints in Perioperative Medicine (StEP) initiative: Renal end-points. Br J Anaesth 2018 ; 121 : 1013 – 24
57. Thygesen K , Alpert JS , Ja e AS , Chaitman BR , Bax JJ , Morrow DA , White HD , Group ESD : Fourth universal de nition of myocardial infarction (2018) . Eur Heart J 2018 ; 40 : 237 – 269
58. Botto F , Alonso-Coello P , Chan MT , Villar JC , Xavier D , Srinathan S , Guyatt G , Cruz P , Graham M , Wang CY , Berwanger O , Pearse RM , Biccard BM , Abraham V , Malaga G , Hillis GS , Rodseth RN , Cook D , Polanczyk CA , Szczeklik W , Sessler DI , Sheth T , Ackland GL , Leuwer M , Garg AX , Lemanach Y , Pettit S , Heels-Ansdell D , Luratibuse G , Walsh M , Sapsford R , Sch ü nemann HJ , Kurz A , Thomas S , Mrkobrada M , Thabane L , Gerstein H , Paniagua P , Nagele P , Raina P , Yusuf S , Devereaux PJ , Devereaux PJ , Sessler DI , Walsh M , Guyatt G , McQueen MJ , Bhandari M , Cook D , Bosch J , Buckley N , Yusuf S , Chow CK , Hillis GS , Halliwell R , Li S , Lee VW , Mooney J , Polanczyk CA , Furtado MV , Berwanger O , Suzumura E , Santucci E , Leite K , Santo JA , Jardim CA , Cavalcanti AB , Guimaraes HP , Jacka MJ , Graham M , McAlister F , McMurtry S , Townsend D , Pannu N , Bagshaw S , Bessissow A , Bhandari M , Duceppe E , Eikelboom J , Ganame J , Hankinson J , Hill S , Jolly S , Lamy A , Ling E , Magloire P , Pare G , Reddy D , Szalay D , Tittley J , Weitz J , Whitlock R , Darvish-Kazim S , Debeer J , Kavsak P , Kearon C , Mizera R , O ’ Donnell M , McQueen M , Pinthus J , Ribas S , Simunovic M , Tandon V , Vanhelder T , Winemaker M , Gerstein H , McDonald S , O ’ Bryne P , Patel A , Paul J , Punthakee Z , Raymer K , Salehian O , Spencer F , Walter S , Worster A , Adili A , Clase C , Cook D , Crowther M , Douketis J , Gangji A , Jackson P , Lim W , Lovrics P , Mazzadi S , Orovan W , Rudkowski J , Soth M , Tiboni M , Acedillo R , Garg A , Hildebrand
ALNV134N2_Text.indb 259ALNV134N2_Text.indb 259 29-Dec-20 19:44:1029-Dec-20 19:44:10
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
260 Anesthesiology 2021; 134:250–61 B. Saugel and D. I. Sessler
CLINICAL FOCUS REVIEW
A , Lam N , Macneil D , Mrkobrada M , Roshanov PS , Srinathan SK , Ramsey C , John PS , Thorlacius L , Siddiqui FS , Grocott HP , McKay A , Lee TW , Amadeo R , Funk D , McDonald H , Zacharias J , Villar JC , Cort é s OL , Chaparro MS , V á squez S , Casta ñ eda A , Ferreira S , Coriat P , Monneret D , Goarin JP , Esteve CI , Royer C , Daas G , Chan MT , Choi GY , Gin T , Lit LC , Xavier D , Sigamani A , Faruqui A , Dhanpal R , Almeida S , Cherian J , Furruqh S , Abraham V , Afzal L , George P , Mala S , Sch ü nemann H , Muti P , Vizza E , Wang CY , Ong GS , Mansor M , Tan AS , Shari uddin II , Vasanthan V , Hashim NH , Undok AW , Ki U , Lai HY , Ahmad WA , Razack AH , Malaga G , Valderrama-Victoria V , Loza-Herrera JD , De Los Angeles Lazo M , Rotta-Rotta A , Szczeklik W , Sokolowska B , Musial J , Gorka J , Iwaszczuk P , Kozka M , Chwala M , Raczek M , Mrowiecki T , Kaczmarek B , Biccard B , Cassimjee H , Gopalan D , Kisten T , Mugabi A , Naidoo P , Naidoo R , Rodseth R , Skinner D , Torborg A , Paniagua P , Urrutia G , Maestre ML , Santal ó M , Gonzalez R , Font A , Mart í nez C , Pelaez X , De Antonio M , Villamor JM , Garc í a JA , Ferr é MJ , Popova E , Alonso-Coello P , Garutti I , Cruz P , Fern á ndez C , Palencia M , D í az S , Del Castillo T , Varela A , de Miguel A , Mu ñ oz M , Pi ñ eiro P , Cusati G , Del Barrio M , Membrillo MJ , Orozco D , Reyes F , Sapsford RJ , Barth J , Scott J , Hall A , Howell S , Lobley M , Woods J , Howard S , Fletcher J , Dewhirst N , Williams C , Rushton A , Welters I , Leuwer M , Pearse R , Ackland G , Khan A , Niebrzegowska E , Benton S , Wragg A , Archbold A , Smith A , McAlees E , Ramballi C , Macdonald N , Januszewska M , Stephens R , Reyes A , Paredes LG , Sultan P , Cain D , Whittle J , Del Arroyo AG , Sessler DI , Kurz A , Sun Z , Finnegan PS , Egan C , Honar H , Shahinyan A , Panjasawatwong K , Fu AY , Wang S , Reineks E , Nagele P , Blood J , Kalin M , Gibson D , Wildes T ; Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Writing Group, on behalf of The Vascular events In noncar-diac Surgery patIents cOhort evaluatioN (VISION) Investigators; Appendix 1. The Vascular events In non-cardiac Surgery patIents cOhort evaluatioN (VISION) Study Investigators Writing Group; Appendix 2. The Vascular events In noncardiac Surgery patIents cOhort evaluatioN Operations Committee; Vascular events In noncardiac Surgery patIents cOhort evaluatioN VISION Study Investigators : Myocardial injury after noncardiac surgery: A large, international, prospective cohort study establishing diagnostic criteria, character-istics, predictors, and 30-day outcomes. A nesthesiology 2014 ; 120 : 564 – 78
59. Devereaux PJ , Biccard BM , Sigamani A , Xavier D , Chan MTV , Srinathan SK , Walsh M , Abraham V , Pearse R , Wang CY , Sessler DI , Kurz A , Szczeklik W , Berwanger O , Villar JC , Malaga G , Garg AX , Chow CK , Ackland G , Patel A , Borges FK , Belley-Cote EP , Duceppe E , Spence J , Tandon V , Williams C , Sapsford
RJ , Polanczyk CA , Tiboni M , Alonso-Coello P , Faruqui A , Heels-Ansdell D , Lamy A , Whitlock R , LeManach Y , Roshanov PS , McGillion M , Kavsak P , McQueen MJ , Thabane L , Rodseth RN , Buse GAL , Bhandari M , Garutti I , Jacka MJ , Schunemann HJ , Cortes OL , Coriat P , Dvirnik N , Botto F , Pettit S , Ja e AS , Guyatt GH : Association of postoperative high-sensitivity tro-ponin levels with myocardial injury and 30-day mor-tality among patients undergoing noncardiac surgery . JAMA 2017 ; 317 : 1642 – 1651
60. Puelacher C , Lurati Buse G , Seeberger D , Sazgary L , Marbot S , Lampart A , Espinola J , Kindler C , Hammerer A , Seeberger E , Strebel I , Wildi K , Twerenbold R , du Fay de Lavallaz J , Steiner L , Gurke L , Breidthardt T , Rentsch K , Buser A , Gualandro DM , Osswald S , Mueller C ; BASEL-PMI Investigators : Perioperative myocardial injury after noncardiac surgery: Incidence, mortality, and characterization. Circulation 2018 ; 137 : 1221 – 32
61. Devereaux PJ , Szczeklik W : Myocardial injury after non-cardiac surgery: Diagnosis and management. Eur Heart J 2020 ; 41 : 3083 – 91
62. Ruetzler K , Khanna AK , Sessler DI : Myocardial injury after noncardiac surgery: Preoperative, intraoperative, and postoperative aspects, implications, and directions. Anesth Analg 2020 ; 131 : 173 – 86
63. Wesselink EM , Kappen TH , Torn HM , Slooter AJC , van Klei WA : Intraoperative hypotension and the risk of postoperative adverse outcomes: A systematic review. Br J Anaesth 2018 ; 121 : 706 – 21
64. McEvoy MD , Gupta R , Koepke EJ , Feldheiser A , Michard F , Levett D , Thacker JKM , Hamilton M , Grocott MPW , Mythen MG , Miller TE , Edwards MR , Miller TE , Mythen MG , Grocott MP , Edwards MR ; POQI-3 Workgroup; POQI Chairs; Physiology Group; Preoperative Blood Pressure Group; Intraoperative Blood Pressure Group; Postoperative Blood Pressure Group : Perioperative Quality Initiative consensus statement on postoperative blood pressure, risk and outcomes for elective surgery. Br J Anaesth 2019 ; 122 : 575 – 86
65. S ü dfeld S , Brechnitz S , Wagner JY , Reese PC , Pinnschmidt HO , Reuter DA , Saugel B : Post-induction hypotension and early intraoperative hypotension asso-ciated with general anaesthesia. Br J Anaesth 2017 ; 119 : 57 – 64
66. Maheshwari K , Turan A , Mao G , Yang D , Niazi AK , Agarwal D , Sessler DI , Kurz A : The association of hypotension during non-cardiac surgery, before and after skin incision, with postoperative acute kidney injury: A retrospective cohort analysis. Anaesthesia 2018 ; 73 : 1223 – 8
67. Liem VGB , Hoeks SE , Mol KHJM , Potters JW , Gr ü ne F , Stolker RJ , van Lier F : Postoperative hypotension
ALNV134N2_Text.indb 260ALNV134N2_Text.indb 260 29-Dec-20 19:44:1029-Dec-20 19:44:10
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:250–61 261
Perioperative Blood Pressure
B. Saugel and D. I. Sessler
after noncardiac surgery and the association with myo-cardial injury. A nesthesiology 2020 ; 133 : 510 – 22
68. Khanna AK , Maheshwari K , Mao G , Liu L , Perez-Protto SE , Chodavarapu P , Schacham YN , Sessler DI : Association between mean arterial pressure and acute kidney injury and a composite of myocardial injury and mortality in postoperative critically ill patients: A retro-spective cohort analysis. Crit Care Med 2019 ; 47 : 910 – 7
69. Sessler DI , Saugel B : Beyond ‘ failure to rescue ’ : The time has come for continuous ward monitoring. Br J Anaesth 2019 ; 122 : 304 – 6
70. Matsukawa T , Sessler DI , Sessler AM , Schroeder M , Ozaki M , Kurz A , Cheng C : Heat ow and dis-tribution during induction of general anesthesia. A nesthesiology 1995 ; 82 : 662 – 73
71. Futier E , Lefrant JY , Guinot PG , Godet T , Lorne E , Cuvillon P , Bertran S , Leone M , Pastene B , Piriou V , Molliex S , Albanese J , Julia JM , Tavernier B , Imho E , Bazin JE , Constantin JM , Pereira B , Jaber S ; INPRESS Study Group : E ect of individualized vs standard
blood pressure management strategies on postoperative organ dysfunction among high-risk patients undergo-ing major surgery: A randomized clinical Trial. JAMA 2017 ; 318 : 1346 – 57
72. Sanders RD , Hughes F , Shaw A , Thompson A , Bader A , Hoeft A , Williams DA , Grocott MPW , Mythen MG , Miller TE , Edwards MR ; Perioperative Quality Initiative-3 Workgroup; POQI Chairs; Physiology Group; Preoperative Blood Pressure Group; Intraoperative Blood Pressure Group; Postoperative Blood Pressure Group : Perioperative Quality Initiative consensus statement on preoperative blood pressure, risk and outcomes for elective surgery. Br J Anaesth 2019 ; 122 : 552 – 62
73. Kiefer N , Theis J , Putensen-Himmer G , Hoeft A , Zenker S : Peristaltic pneumatic compression of the legs reduces uid demand and improves hemodynamic sta-bility during surgery: A randomized, prospective study. A nesthesiology 2011 ; 114 : 536 – 44
RE-FLEC-TION
A “ Soothing ” Syrup? How “ Father ” Wiley Saved Infants from “ Mother ” Winslow ’ s Morphine Elixir
From the early nineteenth to the early twentieth century, Mrs. Winslow ’ s Soothing Syrup ( top ) was marketed in the United States as a panacea for ailments that plagued infants: teething, diarrhea, colic, etc. To ensure happy or sleeping children like those depicted above ( lower left ), Charlotte “ Mother ” Winslow and her legacy rms spiked her Soothing Syrup with morphine and alcohol. Over the course of a century, sales of millions of bottles world-wide caused thousands of infant deaths. Fortunately, Dr. Harvey Washington Wiley ( lower right ), Chief Chemist at the U.S. Department of Agriculture and future “ Father of the Food and Drug Administration, ” intervened by facilitating passage of the Pure Food and Drug Act (1906). Several amendments further limited the sale of opioids, leading to the removal of morphine from a syrup that was more sinister than soothing. (Copyright © the American Society of Anesthesiologists ’ Wood Library-Museum of Anesthesiology, Schaumburg, Illinois.)
Melissa L. Coleman, M.D., Penn State College of Medicine, Hershey, Pennsylvania, and Jane S. Moon, M.D., University of California, Los Angeles.
ANESTHESIOLOGY REFLECTIONS FROM THE WOOD LIBRARY-MUSEUM
ALNV134N2_Text.indb 261ALNV134N2_Text.indb 261 29-Dec-20 19:44:1029-Dec-20 19:44:10
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
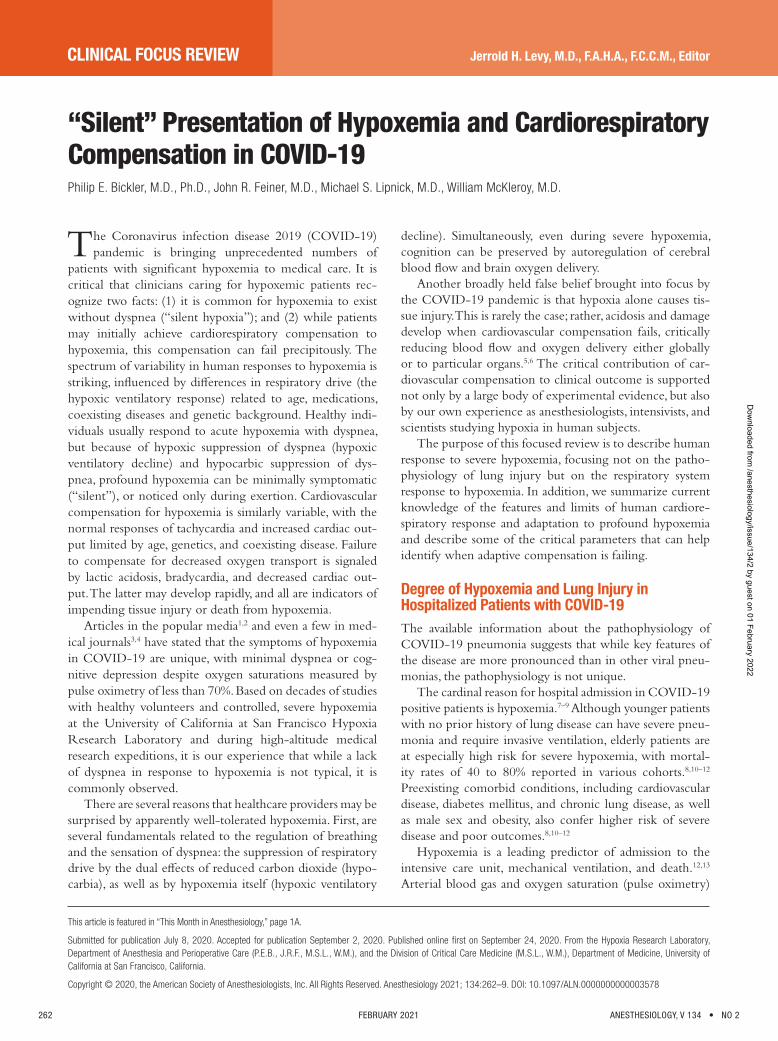
CLINICAL FOCUS REVIEW
262 FEBRUARY 2021 ANESTHESIOLOGY, V 134 • NO 2
Jerrold H. Levy, M.D., F.A.H.A., F.C.C.M., Editor
This article is featured in “This Month in Anesthesiology,” page 1A.
Submitted for publication July 8, 2020. Accepted for publication September 2, 2020. Published online fi rst on September 24, 2020. From the Hypoxia Research Laboratory, Department of Anesthesia and Perioperative Care (P.E.B., J.R.F., M.S.L., W.M.), and the Division of Critical Care Medicine (M.S.L., W.M.), Department of Medicine, University of California at San Francisco, California.
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved. Anesthesiology 2021 ; 134 : 262 – 9 . DOI: 10.1097/ALN.0000000000003578
“ Silent ” Presentation of Hypoxemia and Cardiorespiratory Compensation in COVID-19 Philip E. Bickler , M.D., Ph.D. , John R. Feiner , M.D. , Michael S. Lipnick , M.D. , William McKleroy , M.D.
The Coronavirus infection disease 2019 (COVID-19) pandemic is bringing unprecedented numbers of
patients with signi cant hypoxemia to medical care. It is critical that clinicians caring for hypoxemic patients rec-ognize two facts: (1) it is common for hypoxemia to exist without dyspnea ( “ silent hypoxia ” ); and (2) while patients may initially achieve cardiorespiratory compensation to hypoxemia, this compensation can fail precipitously. The spectrum of variability in human responses to hypoxemia is striking, in uenced by di erences in respiratory drive (the hypoxic ventilatory response ) related to age, medications, coexisting diseases and genetic background. Healthy indi-viduals usually respond to acute hypoxemia with dyspnea, but because of hypoxic suppression of dyspnea (hypoxic ventilatory decline) and hypocarbic suppression of dys-pnea, profound hypoxemia can be minimally symptomatic ( “ silent ” ), or noticed only during exertion. Cardiovascular compensation for hypoxemia is similarly variable, with the normal responses of tachycardia and increased cardiac out-put limited by age, genetics, and coexisting disease. Failure to compensate for decreased oxygen transport is signaled by lactic acidosis, bradycardia, and decreased cardiac out-put. The latter may develop rapidly, and all are indicators of impending tissue injury or death from hypoxemia.
Articles in the popular media 1 , 2 and even a few in med-ical journals 3 , 4 have stated that the symptoms of hypoxemia in COVID-19 are unique, with minimal dyspnea or cog-nitive depression despite oxygen saturations measured by pulse oximetry of less than 70%. Based on decades of studies with healthy volunteers and controlled, severe hypoxemia at the University of California at San Francisco Hypoxia Research Laboratory and during high-altitude medical research expeditions, it is our experience that while a lack of dyspnea in response to hypoxemia is not typical, it is commonly observed.
There are several reasons that healthcare providers may be surprised by apparently well-tolerated hypoxemia. First, are several fundamentals related to the regulation of breathing and the sensation of dyspnea: the suppression of respiratory drive by the dual e ects of reduced carbon dioxide (hypo-carbia), as well as by hypoxemia itself (hypoxic ventilatory
decline). Simultaneously, even during severe hypoxemia, cognition can be preserved by autoregulation of cerebral blood ow and brain oxygen delivery.
Another broadly held false belief brought into focus by the COVID-19 pandemic is that hypoxia alone causes tis-sue injury. This is rarely the case; rather, acidosis and damage develop when cardiovascular compensation fails, critically reducing blood ow and oxygen delivery either globally or to particular organs. 5 , 6 The critical contribution of car-diovascular compensation to clinical outcome is supported not only by a large body of experimental evidence, but also by our own experience as anesthesiologists, intensivists, and scientists studying hypoxia in human subjects.
The purpose of this focused review is to describe human response to severe hypoxemia, focusing not on the patho-physiology of lung injury but on the respiratory system response to hypoxemia. In addition, we summarize current knowledge of the features and limits of human cardiore-spiratory response and adaptation to profound hypoxemia and describe some of the critical parameters that can help identify when adaptive compensation is failing.
Degree of Hypoxemia and Lung Injury in Hospitalized Patients with COVID-19 The available information about the pathophysiology of COVID-19 pneumonia suggests that while key features of the disease are more pronounced than in other viral pneu-monias, the pathophysiology is not unique.
The cardinal reason for hospital admission in COVID-19 positive patients is hypoxemia. 7 – 9 Although younger patients with no prior history of lung disease can have severe pneu-monia and require invasive ventilation, elderly patients are at especially high risk for severe hypoxemia, with mortal-ity rates of 40 to 80% reported in various cohorts. 8 , 10 – 12
Preexisting comorbid conditions, including cardiovascular disease, diabetes mellitus, and chronic lung disease, as well as male sex and obesity, also confer higher risk of severe disease and poor outcomes. 8 , 10 – 12
Hypoxemia is a leading predictor of admission to the intensive care unit, mechanical ventilation, and death. 12 , 13
Arterial blood gas and oxygen saturation (pulse oximetry)
ALNV134N2_Text.indb 262ALNV134N2_Text.indb 262 29-Dec-20 19:44:1129-Dec-20 19:44:11
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:262–9 263
Hypoxemia and COVID-19
Bickler et al.
data often show severe hypoxemia at time of presentation, with wide alveolar-arterial P o
2 gradients and low P ao
2 /F io
2
ratios. Increased oxygen requirements have been addressed with increased use of noninvasive oxygen therapy (including high ow nasal oxygen), prone positioning, invasive ventila-tion, and in some cases, extracorporeal membrane oxygen. Hypercarbic respiratory failure has not been a prominent presenting feature in existing reports or in our experience at University of California at San Francisco.
Intrapulmonary shunt and ventilation/perfusion mis-match are the chief gas exchange abnormalities causing hypoxemia in COVID-19, as they are in other viral pneu-monias, bacterial pneumonias, 14 and acute respiratory distress syndrome. 15 However, some features of COVID-19 may be more pronounced than in other viral pneumonias, including substantial endothelial damage and micro-/macro-emboli formation. 16 Limitation of di usion across the alveolar mem-brane can cause hypoxemia, but while this is seen in humans at high altitude due to low inspired and alveolar P o
2 , 17 in
patients with loss of functional lung units (such as in inter-stitial lung disease or emphysema), and in some elite athletes at extremely high levels of cardiac output 18 it does not sig-ni cantly contribute to hypoxemia in ARDS. 15 Unique to shunt physiology is that increased ventilation decreases car-bon dioxide more than it increases oxygenation. The reduced carbon dioxide limits respiratory drive and dyspnea ( g. 1 ).
Although intrapulmonary shunt is the dominant present-ing gas exchange abnormality in COVID-19, dead space may signi cantly worsen with progression of ARDS. Hypoxemia that does not resolve with supplemental oxygen clearly indi-cates that gas exchange impairment has progressed beyond ventilation/perfusion ration (V·/Q· ) mismatch and includes substantial intrapulmonary shunt. Alveolar lling, a cardi-nal feature of ARDS, correlates with lung radiographs and impaired gas exchange. Of note, the pathophysiology of ARDS is di erent from that of high-altitude pulmonary edema , in that COVID-19 involves an in ammation medi-ated alveolar uid leak and that of high-altitude pulmonary edema is related to elevated transcapillary pressure. 19
The mechanisms by which COVID-19 produces ARDS that a ects large proportions of lung parenchyma may involve both a reduced innate immune response and an exaggerated in ammatory cytokine response ( “ cytokine storm ” ). 20 While the novelty of this pattern of immuno-logic disturbance is debated, 21 the impacts on pulmonary gas exchange do not appear to be unique. The known physiology of viral pneumonia and ARDS involves well characterized disturbances that produce intrapulmonary shunt, ventilation-perfusion mismatch, 22 increased dead space ventilation, and decreased compliance. 23 Profound gas exchange abnormalities persist after initiation of high- ow nasal oxygen or invasive ventilation despite lung protective ventilator protocols, prone positioning, and maximal F io
2 . 8 , 24 , 25 As with other pneumonias, some
patients maintain near normal lung compliance, and others
su er decreased compliance as disease progresses, 26 rep-resenting a diversity of pathology. 27 Appropriate manage-ment of invasive ventilation in ARDS has been recently reviewed and no strong data exist to support modi -cation of existing ARDS protocols for COVID-19. 28 , 29
Readers are referred to the frequently updated consensus statements concerning treatment of COVID-19 by the World Health Organization: ( https://www.who.int/publi-cations/i/item/clinical-management-of-covid-19 ; accessed September 24, 2020).
Hypoxemia and Breathlessness: Variability in Humans Hypoxemia can present in a highly variable manner, with some patients dyspneic with labored breathing and pan-icked, and others calm, despite oxygen saturations in the 70% range or below. The processes that produce intrapul-monary shunt do not necessarily decrease lung compliance or produce dyspnea. For many hypoxemic patients, oxygen saturations less than 70% can be tolerated for some time with only moderate and transient alterations in mentation or other signs and symptoms. 30 Dyspnea may only occur with exertion, although decreased exercise tolerance is a nonspeci c symptom in acute illness. Decreased lung com-pliance contributes to dyspnea, but as previously discussed, early COVID-19 pneumonia may present with shunt and normal lung compliance. 26 In our experience with pro-found experimental hypoxemia to oxygen saturations as low as 50% in healthy humans, subjective symptoms of hypoxia may go unnoticed in some individuals, with no appearance of discomfort and minimal hyperpnea. 30 Given this variability in individual responses to hypoxemia, it is not surprising that some COVID-19 patients have been described as asymptomatic “ silent ” or “ happy hypoxia. ” 3
Tobin et al. recently reviewed some of the factors account-ing for reduced dyspnea in COVID-19 patients. 4
One of the key reasons that COVID-19 patients may not present with marked dyspnea is that the main gas exchange abnormality involves shunt. Intrapulmonary shunt and V /Q mismatch has minimal e ects on carbon dioxide excretion compared to oxygen uptake. 31 Thus, even mild hyperven-tilation is capable of signi cantly reducing arterial carbon dioxide and decreasing respiratory drive mediated by both the carotid and central chemoreceptors 32 ( g. 1 ). Carbon dioxide retention is more strongly correlated with breath-lessness in lung disease than is hypoxemia. 33 In patients who can increase breathing and lower arterial partial pressure of carbon dioxide , breathlessness will be limited. 34 This is simi-lar to what is experienced by most people on ascent to high altitude: arterial hypoxemia is present but subjective breath-lessness is limited by subtle, often unnoticed increases in the respiratory rate that helps the lungs “ blow o ” enough arte-rial carbon dioxide to mitigate the sensation of dyspnea. 35
Breathing responses to hypoxia are experimentally quanti ed by the hypoxic ventilatory response, 36 a response
ALNV134N2_Text.indb 263ALNV134N2_Text.indb 263 29-Dec-20 19:44:1129-Dec-20 19:44:11
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
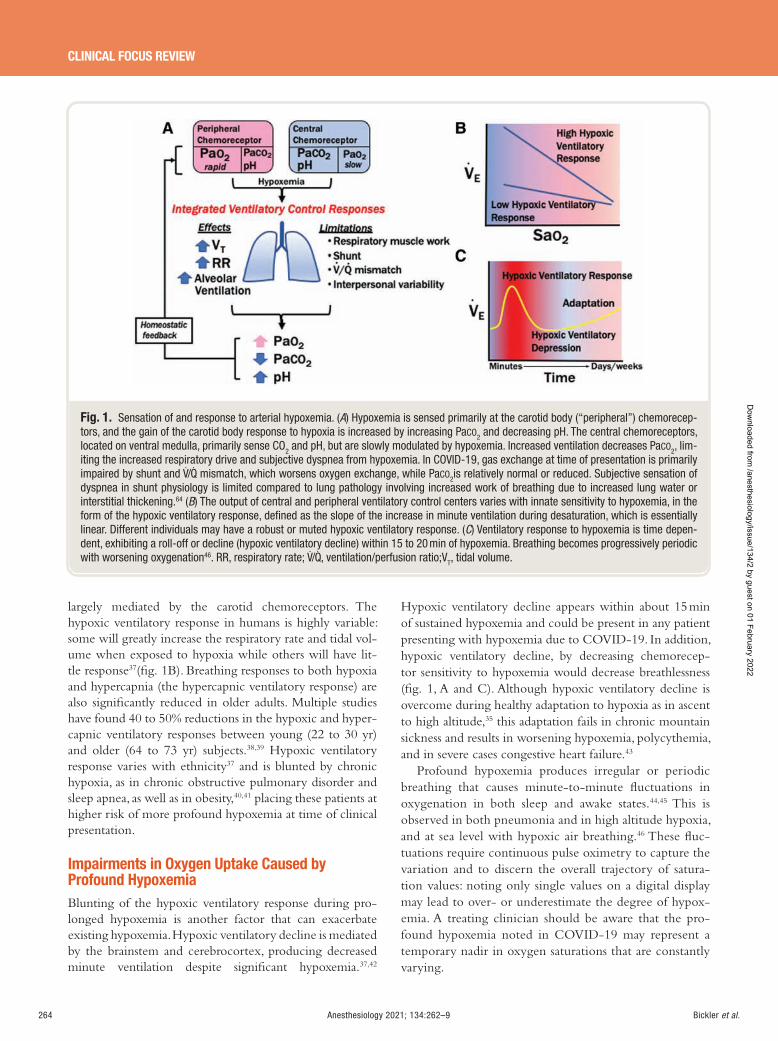
264 Anesthesiology 2021; 134:262–9 Bickler et al.
CLINICAL FOCUS REVIEW
largely mediated by the carotid chemoreceptors. The hypoxic ventilatory response in humans is highly variable: some will greatly increase the respiratory rate and tidal vol-ume when exposed to hypoxia while others will have lit-tle response 37 ( g. 1B ). Breathing responses to both hypoxia and hypercapnia (the hypercapnic ventilatory response) are also signi cantly reduced in older adults. Multiple studies have found 40 to 50% reductions in the hypoxic and hyper-capnic ventilatory responses between young (22 to 30 yr) and older (64 to 73 yr) subjects. 38 , 39 Hypoxic ventilatory response varies with ethnicity 37 and is blunted by chronic hypoxia, as in chronic obstructive pulmonary disorder and sleep apnea, as well as in obesity, 40 , 41 placing these patients at higher risk of more profound hypoxemia at time of clinical presentation.
Impairments in Oxygen Uptake Caused by Profound Hypoxemia Blunting of the hypoxic ventilatory response during pro-longed hypoxemia is another factor that can exacerbate existing hypoxemia. Hypoxic ventilatory decline is mediated by the brainstem and cerebrocortex, producing decreased minute ventilation despite signi cant hypoxemia. 37 , 42
Hypoxic ventilatory decline appears within about 15 min of sustained hypoxemia and could be present in any patient presenting with hypoxemia due to COVID-19. In addition, hypoxic ventilatory decline, by decreasing chemorecep-tor sensitivity to hypoxemia would decrease breathlessness ( g. 1 , A and C). Although hypoxic ventilatory decline is overcome during healthy adaptation to hypoxia as in ascent to high altitude, 35 this adaptation fails in chronic mountain sickness and results in worsening hypoxemia, polycythemia, and in severe cases congestive heart failure. 43
Profound hypoxemia produces irregular or periodic breathing that causes minute-to-minute uctuations in oxygenation in both sleep and awake states. 44 , 45 This is observed in both pneumonia and in high altitude hypoxia, and at sea level with hypoxic air breathing. 46 These uc-tuations require continuous pulse oximetry to capture the variation and to discern the overall trajectory of satura-tion values: noting only single values on a digital display may lead to over- or underestimate the degree of hypox-emia. A treating clinician should be aware that the pro-found hypoxemia noted in COVID-19 may represent a temporary nadir in oxygen saturations that are constantly varying.
Fig. 1. Sensation of and response to arterial hypoxemia. ( A ) Hypoxemia is sensed primarily at the carotid body ( “ peripheral ” ) chemorecep-tors, and the gain of the carotid body response to hypoxia is increased by increasing Pa CO2 and decreasing pH. The central chemoreceptors, located on ventral medulla, primarily sense CO 2 and pH, but are slowly modulated by hypoxemia. Increased ventilation decreases Pa CO2 , lim-iting the increased respiratory drive and subjective dyspnea from hypoxemia. In COVID-19, gas exchange at time of presentation is primarily impaired by shunt and V·/ ·Q mismatch, which worsens oxygen exchange, while Pa CO2 is relatively normal or reduced. Subjective sensation of dyspnea in shunt physiology is limited compared to lung pathology involving increased work of breathing due to increased lung water or interstitial thickening. 64 ( B ) The output of central and peripheral ventilatory control centers varies with innate sensitivity to hypoxemia, in the form of the hypoxic ventilatory response, defi ned as the slope of the increase in minute ventilation during desaturation, which is essentially linear. Different individuals may have a robust or muted hypoxic ventilatory response. ( C ) Ventilatory response to hypoxemia is time depen-dent, exhibiting a roll-off or decline (hypoxic ventilatory decline) within 15 to 20 min of hypoxemia. Breathing becomes progressively periodic with worsening oxygenation 46 . RR , respiratory rate; V·/ ·Q, ventilation/perfusion ratio;V T , tidal volume.
ALNV134N2_Text.indb 264ALNV134N2_Text.indb 264 29-Dec-20 19:44:1129-Dec-20 19:44:11
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:262–9 265
Hypoxemia and COVID-19
Bickler et al.
Hypoxemia can increase the severity right-to-left shunt by elevating pulmonary artery pressures, increasing blood ow through a patent foramen ovale or other venous chan-nels. Shunting through a patent foramen ovale is observed in about 15% of normal subjects during acute hypoxemia during breathing hypoxic air mixtures to saturations of 70 to 80%. It is also seen during exercise at high altitude. This added intracardiac shunt may worsen hypoxemia out of proportion to the apparent lung injury. Furthermore, because shunt and decreased mixed venous P o
2 shift gas
exchange to the steep portion of the oxyhemoglobin disso-ciation curve, small changes in ventilation, inspired oxygen, and shunt fraction produce large changes in arterial oxygen saturation.
Cardiovascular Response and Limitations during Profound Hypoxemia Hypoxemia is well tolerated when compensated by cardio-vascular responses ( g. 2 ). Cardiovascular adaptation is the key component of a suite of responses enabling humans to adapt to high altitude hypoxia, endure prolonged breath-hold dives, survive profound acute anemia (hemoglobin less than 5 g/100 ml 47 ) and endure other physiologic stressors. 30
While biochemical adaptation to hypoxia is also import-ant especially for long term adaptation, 48 , 49 cardiovascular adaptation is both the component most strongly coupled
to immediate clinical outcomes and the one most easily assessed by clinicians.
The proximal cause of tissue injury in profound hypox-emia is failure of cardiovascular compensation, not hypoxia per se . A study in cats 5 illustrates the critical importance of the circulation in predicting tissue injury during severe hypoxemia: when animals were experimentally exposed to 25 min of severe hypoxia (F io
2 = 3.4%; P ao
2 = 17 mmHg)
with adequate blood pressure (mean arterial blood pressure greater than 65 mmHg) not one animal su ered any end-or-gan injury. In contrast, 12 of 13 cats exposed to the same degree of hypoxemia but with reductions in mean arterial pressure to less than 45 mmHg for only 4 min developed a pattern of brain injury closely resembling that of humans surviving in a persistent vegetative state after cardiorespi-ratory arrest. Similarly, brain injury in hypoxemic primates only occurs when hypoxia causes low cardiac output. 6
Cardiovascular compensation underlies the preserva-tion of cognitive function in well compensated profound hypoxemia. Cerebral blood ow increases during hypoxia, preserving cerebral oxygenation out of proportion to sys-temic hypoxemia 50 and leaving most cognitive domains little e ected by hypoxia. 51 Other studies 52 have reported intact executive and motor function and mild de cits in memory.
It is of critical importance for clinicians caring for COVID-19 patients to understand that, just as for respiratory system adaptation, cardiovascular compensatory responses
Fig. 2. Cardiovascular compensation for mild (85 to 90% Sa O2 ), moderate (75 to 85% Sa O2 ), severe (50 to 75% Sa O2 ), and profound ( < 50% Sa O2 ) hypoxemia. Increased cardiac output, mainly mediated by increased heart rate, is the main cardiovascular response to hypoxemia, but is limited by age and cardiovascular disease. Mild to moderate hypoxemia causes increased cellular glycolysis, which generates 2,3 diphos-phoglycerate and increases the P 50 of hemoglobin. Decreased tolerance of physical exertion or even normal activity is a sensitive indicator of the adequacy of early cardiovascular response to hypoxemia. Loss of consciousness becomes likely at saturations less than 50%. Failure of cardiovascular adaptation ultimately involves bradycardia, asystole, or pulseless electrical activity, with rapidly ensuing tissue injury and death. CO , cardiac output; HR, heart rate; PVR, pulmonary vascular resistance; SVR, systemic vascular resistance.
ALNV134N2_Text.indb 265ALNV134N2_Text.indb 265 29-Dec-20 19:44:1129-Dec-20 19:44:11
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

266 Anesthesiology 2021; 134:262–9 Bickler et al.
CLINICAL FOCUS REVIEW
are both variable 53 and limited. The limits of cardiovascular compensation de ne increasing acidosis and impending car-diovascular collapse and death, as shown in gure 2 .
Normal compensated cardiovascular adaptation to acute hypoxemia involves increased cardiac output, mediated pre-dominately by tachycardia, with only moderate augmenta-tion of blood pressure. As with the breathing response to hypoxemia, this heart rate and blood pressure response to hypoxia vary enormously in healthy individuals. 53 The heart rate response to hypoxemia parallels the ventilatory response, so that individuals who do not present with shortness of breath, may also present without signi cant tachycardia. 54
Cardiovascular compensation to hypoxemia also var-ies with age and coexisting disease. We expect that most younger patients with profound hypoxemia have nor-mal or elevated cardiac output, which is one of the most important factors for tolerating hypoxemia. Aging is known to decrease sympathetic nervous system/cardiovascular responses to hypoxic stress, and thereby contribute to a decreased tolerance of hypoxia in older individuals. 38 , 39 , 55
The highest mortality rate in COVID-19 has been reported among older patients 12 who may be less capable of adequate cardiovascular compensation. Individuals with coexisting cardiovascular or pulmonary disease may be limited in the scope or tolerance of sympathetic nervous system activation by systemic hypoxia, 56 resulting in elevated heart rate, and increases in pulmonary and systemic vascular resistance.
Deterioration in oxygen saturation and cardiovascular compensation can occur rapidly in hypoxemic patients, particularly in patients with profound shunt physiology. It is important to realize that deterioration in oxygenation most often is caused by a combination of factors. These factors include increasing shunt, reduced cardiac output, decreased ventilation, and gas exchange on the steep por-tion of the oxyhemoglobin dissociation curve. Low cardiac output also worsens pulmonary gas exchange because of decreased mixed venous P o2
, 57 right shift of the oxyhemo-globin dissociation curve caused by acidosis, and decreased e ectiveness of hypoxic/hypercapnic pulmonary vasocon-striction. In the presence of a xed intrapulmonary shunt, a lower mixed-venous P o
2 will have a large e ect on arte-
rial saturation because of the shape of the oxyhemoglobin dissociation curve 58 ( g. 1 ). Because alveolar gas exchange is on the steep portion of the oxyhemoglobin dissociation curve, small changes in cardiac output or alveolar P o
2 result
in large changes in oxygen saturation via this decrease in mixed venous P o
2 . Taken together, these e ects explain the
seemingly unpredictable precipitous changes in oxygen-ation that can occur in all severe pneumonias.
Predicting the Limits of Cardiovascular Compensation in Profound Hypoxemia The precise limits of tolerance of reduced oxygen delivery are di cult to predict in an individual patient, but a critical threshold is when oxygen delivery is reduced to less than 25%
of normal. 59 The clinical assessment of the transition from compensated to poorly compensated cardiovascular adapta-tion to hypoxemia includes the following: (1) worsened aci-demia or plasma lactate 60 , 61 ; (2) decreased mixed venous P o
2
or decreased tissue oximetry (near infrared spectroscopy); (3) increased requirements for vasoactive medications to support blood pressure despite adequate uid resuscitation; (4) increase in blood pressure reactivity to changes in body position, e.g., not tolerating prone or head-up positions; (5) bradycardia, arrhythmias, electrocardiogram changes con-cerning for ischemia, and increased in heart rate variability; and (6) increased troponin levels or ultrasound evidence of decreased myocardial contractility. These assessments re ect a focus on the cardiovascular compensation/tissue oxygen delivery for hypoxemia rather than on the degree of hypox-emia or hypercarbia per se . Bradycardia and decreased cardiac output/myocardial function are described in severe cases of hypoxemic respiratory failure, including COVID-19 disease, and often represent premorbid events. 62 Given reports of acute cardiomyopathy among patients with COVID-19, 62 , 63
clinicians must be keenly aware that the changes listed above may also re ect development or progression of myocardial injury; similarly, patients with low ejection fraction may have signi cantly less ability to augment cardiac output to com-pensate for any degree of hypoxemia.
Conclusions COVID-19 is bringing large numbers of severely hypox-emic patients to medical care and highlighting a known phenomenon of ” silent hypoxia. ” The variability in human breathing response to hypoxemia, as well as the preponder-ance of shunt physiology early in the course of COVID pneumonia , likely explains lack of dyspnea in some hypox-emic COVID-19 patients. Cardiovascular compensation to hypoxemia is critical for preservation of tissue oxygen delivery. The limits of cardiovascular compensation to hypoxemia are more likely to de ne clinical outcomes in COVID-19 than is the degree of hypoxemia per se .
Acknowledgments
The authors thank John W. Severinghaus, M.D., University of California at San Francisco, for decades of discussions on the topics presented in this paper.
Research Support
Support was provided solely from departmental sources.
Competing Interests
The authors declare no competing interests.
Correspondence
Address correspondence to Dr. Bickler: University of California at San Francisco, 513 Parnassus Ave, Medical
ALNV134N2_Text.indb 266ALNV134N2_Text.indb 266 29-Dec-20 19:44:1129-Dec-20 19:44:11
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:262–9 267
Hypoxemia and COVID-19
Bickler et al.
Sciences 256, San Francisco, California 94143-0543. [email protected] . A nesthesiology ’ s articles are made freely accessible to all readers, for personal use only, 6 months from the cover date of the issue.
References
1. Hohman M : What is ‘ silent hypoxia ’ ? Experts weigh in on COVID-19 symptom. USA Today, May 8, 2020 2020 . Available at: https://www.today.com/health/happy-hypoxia-meaning-experts-discuss-coronavi-rus-symptom-signs-t181080 . Accessed September 24, 2020.
2. Levitan R : The infection that ’ s silently kill-ing Coronavirus patients. The New York Times, April 20, 2020 . Available at: https://www.nytimes.com/2020/04/20/opinion/sunday/coronavirus-test-ing-pneumonia.html . Accessed September 24, 2020.
3. Ottestad W , Seim M , Maehlen JO : COVID-19 with silent hypoxemia. Tidsskr Nor Laegeforen 2020 ; 140
4. Tobin MJ , Laghi F , Jubran A : Why COVID-19 silent hypoxemia is ba ing to physicians. Am J Respir Crit Care Med 2020 ; 202 : 356 – 60
5. de Courten-Myers GM , Yamaguchi S , Wagner KR , Ting P , Myers RE : Brain injury from marked hypoxia in cats: Role of hypotension and hyperglycemia. Stroke 1985 ; 16 : 1016 – 21
6. Selkoe DJ , Myers RE : Neurologic and cardiovascular e ects of hypotension in the monkey. Stroke 1979 ; 10 : 147 – 57
7. Bhatraju PK , Ghassemieh BJ , Nichols M , Kim R , Jerome KR , Nalla AK , Greninger AL , Pipavath S , Wurfel MM , Evans L , Kritek PA , West TE , Luks A , Gerbino A , Dale CR , Goldman JD , O ’ Mahony S , Mikacenic C : Covid-19 in critically ill patients in the Seattle region - case series. N Engl J Med 2020 ; 382 : 2012 – 22
8. Grasselli G , Zangrillo A , Zanella A , Antonelli M , Cabrini L , Castelli A , Cereda D , Coluccello A , Foti G , Fumagalli R , Iotti G , Latronico N , Lorini L , Merler S , Natalini G , Piatti A , Ranieri MV , Scandroglio AM , Storti E , Cecconi M , Pesenti A ; COVID-19 Lombardy ICU Network : Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy. JAMA 2020 ; 323 : 1574 – 81
9. Yang X , Yu Y , Xu J , Shu H , Xia J , Liu H , Wu Y , Zhang L , Yu Z , Fang M , Yu T , Wang Y , Pan S , Zou X , Yuan S , Shang Y : Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir Med 2020 ; 8 : 475 – 81
10. Gold JAW , Wong KK , Szablewski CM , Patel PR , Rossow J , da Silva J , Natarajan P , Morris SB , Fanfair RN , Rogers-Brown J , Bruce BB , Browning SD , Hernandez-Romieu AC , Furukawa NW , Kang M ,
Evans ME , Oosmanally N , Tobin-D ’ Angelo M , Drenzek C , Murphy DJ , Hollberg J , Blum JM , Jansen R , Wright DW , Sewell WM 3 rd , Owens JD , Lefkove B , Brown FW , Burton DC , Uyeki TM , Bialek SR , Jackson BR : Characteristics and clinical outcomes of adult patients hospitalized with COVID-19 - Georgia, March 2020. MMWR Morb Mortal Wkly Rep 2020 ; 69 : 545 – 50
11. Richardson S , Hirsch JS , Narasimhan M , Crawford JM , McGinn T , Davidson KW , Barnaby DP , Becker LB , Chelico JD , Cohen SL , Cookingham J , Coppa K , Diefenbach MA , Dominello AJ , Duer-Hefele J , Falzon L , Gitlin J , Hajizadeh N , Harvin TG , Hirschwerk DA , Kim EJ , Kozel ZM , Marrast LM , Mogavero JN , Osorio GA , Qiu M , Zanos TP ; and the Northwell COVID-19 Research Consortium : Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA 2020 ; 323 : 2052 – 9
12. Wu C , Chen X , Cai Y , Xia J , Zhou X , Xu S , Huang H , Zhang L , Zhou X , Du C , Zhang Y , Song J , Wang S , Chao Y , Yang Z , Xu J , Zhou X , Chen D , Xiong W , Xu L , Zhou F , Jiang J , Bai C , Zheng J , Song Y : Risk factors associated with acute respiratory distress syndrome and death in patients with Coronavirus disease 2019 pneu-monia in Wuhan, China. JAMA Intern Med 2020 ; 180 : 1 – 11
13. Petrilli CM , Jones SA , Yang J , Rajagopalan H , O ’ Donnell L , Chernyak Y , Tobin KA , Cerfolio RJ , Francois F , Horwitz LI : Factors associated with hos-pital admission and critical illness among 5279 peo-ple with coronavirus disease 2019 in New York City: Prospective cohort study. BMJ 2020 ; 369 : m1966
14. Light RB : Pulmonary pathophysiology of pneumococ-cal pneumonia. Semin Respir Infect 1999 ; 14 : 218 – 26
15. Radermacher P , Maggiore SM , Mercat A : Fifty years of research in ARDS. Gas exchange in acute respiratory distress syndrome. Am J Respir Crit Care Med 2017 ; 196 : 964 – 84
16. Ackermann M , Verleden SE , Kuehnel M , Haverich A , Welte T , Laenger F , Vanstapel A , Werlein C , Stark H , Tzankov A , Li WW , Li VW , Mentzer SJ , Jonigk D : Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in Covid-19. N Engl J Med 2020 ; 383 : 120 – 8
17. Schoene RB : Limits of human lung function at high altitude. J Exp Biol 2001 ; 204 ( Pt 18 ): 3121 – 7
18. Dempsey JA , Wagner PD : Exercise-induced arterial hypoxemia. J Appl Physiol (1985) 1999 ; 87 : 1997 – 2006
19. Luks AM , Freer L , Grissom CK , McIntosh SE , Schoene RB , Swenson ER , Hackett PH : COVID-19 lung injury is not high altitude pulmonary edema. High Alt Med Biol 2020 ; 21 : 192 – 3
20. Giamarellos-Bourboulis EJ , Netea MG , Rovina N , Akinosoglou K , Antoniadou A , Antonakos N ,
ALNV134N2_Text.indb 267ALNV134N2_Text.indb 267 29-Dec-20 19:44:1129-Dec-20 19:44:11
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
268 Anesthesiology 2021; 134:262–9 Bickler et al.
CLINICAL FOCUS REVIEW
Damoraki G , Gkavogianni T , Adami M-E , Katsaounou P , Ntaganou M , Kyriakopoulou M , Dimopoulos G , Koutsodimitropoulos I , Velissaris D , Koufargyris P , Karageorgos A , Katrini K , Lekakis V , Lupse M , Kotsaki A , Renieris G , Theodoulou D , Panou V , Koukaki E, Koulouris N , Gogos C , Koutsoukou A : Complex immune dysregulation in COVID-19 patients with severe respiratory failure. Cell 2020 ; doi: 10.1016/j.chom.2020.04.009
21. Sinha P , Matthay MA , Calfee CS : Is a “ cytokine storm ” relevant to COVID-19? JAMA Intern Med 2020 June 30 [Epub ahead of print]
22. Dantzker DR , Brook CJ , Dehart P , Lynch JP , Weg JG : Ventilation-perfusion distributions in the adult respi-ratory distress syndrome. Am Rev Respir Dis 1979 ; 120 : 1039 – 52
23. Kallet RH , Ho K , Lipnick MS , Matthay MA : Pulmonary mechanics and gas exchange characteristics in uncommon etiologies of acute respiratory distress syndrome. J Thorac Dis 2018 ; 10 : 5030 – 8
24. Arentz M , Yim E , Kla L , Lokhandwala S , Riedo FX , Chong M , Lee M : Characteristics and outcomes of 21 critically ill patients with COVID-19 in Washington state. JAMA 2020 ; 323 : 1612 – 4
25. Guan WJ , Ni ZY , Hu Y , Liang WH , Ou CQ , He JX , Liu L , Shan H , Lei CL , Hui DSC , Du B , Li LJ , Zeng G , Yuen KY , Chen RC , Tang CL , Wang T , Chen PY , Xiang J , Li SY , Wang JL , Liang ZJ , Peng YX , Wei L , Liu Y , Hu YH , Peng P , Wang JM , Liu JY , Chen Z , Li G , Zheng ZJ , Qiu SQ , Luo J , Ye CJ , Zhu SY , Zhong NS ; China Medical Treatment Expert Group for Covid-19 : Clinical characteristics of Coronavirus disease 2019 in China. N Engl J Med 2020 ; 382 : 1708 – 20
26. Marini JJ , Gattinoni L : Management of COVID-19 respiratory distress. JAMA 2020 ; 323 : 2329 – 30
27. Haudebourg AF , Perier F , Tu et S , de Prost N , Razazi K , Mekontso Dessap A , Carteaux G : Respiratory mechan-ics of COVID-19- versus non-COVID-19-associated acute respiratory distress syndrome. Am J Respir Crit Care Med 2020 ; 202 : 287 – 90
28. Matthay MA , Aldrich JM , Gotts JE : Treatment for severe acute respiratory distress syndrome from COVID-19. Lancet Respir Med 2020 ; 8 : 433 – 4
29. Fan E , Beitler JR , Brochard L , Calfee CS , Ferguson ND , Slutsky AS , Brodie D : COVID-19-associated acute respi-ratory distress syndrome: Is a di erent approach to man-agement warranted? Lancet Respir Med 2020 ; 8 : 816 – 21
30. Bickler PE , Feiner JR , Lipnick MS , Batchelder P , MacLeod DB , Severinghaus JW : E ects of acute, pro-found hypoxia on healthy humans: Implications for safety of tests evaluating pulse oximetry or tissue oxim-etry performance. Anesth Analg 2017 ; 124 : 146 – 53
31. Petersson J , Glenny RW : Gas exchange and ventila-tion-perfusion relationships in the lung. Eur Respir J 2014 ; 44 : 1023 – 41
32. Forster HV , Smith CA : Contributions of central and peripheral chemoreceptors to the ventilatory response to CO2/H + . J Appl Physiol (1985) 2010 ; 108 : 989 – 94
33. Kobayashi S , Nishimura M , Yamomoto M , Akiyama Y , Miyamoto K , Kawamaki Y : Relationship between breathlessness and hypoxic and hypercapnic ventilatory response in patients with COPD. Eur Respir J 1996 ; 9 : 2340 – 5
34. Prabhakar N : O 2 and CO
2 detection by the carotid
and aortic bodies , Chemosensory Transduction . Edited by Zufall F , Munger S . Philadelphia, Elsevier , 2016 , pp 321 – 38
35. Sato M , Severinghaus JW , Bickler P : Time course of augmentation and depression of hypoxic ventila-tory responses at altitude. J Appl Physiol (1985) 1994 ; 77 : 313 – 6
36. Bisgard GE , Neubauer JA : Peripheral and central e ects of hypoxia , Regulation of Breathing . Edited by Dempsey J , Pack A . New York , Marcel Dekker , 1995 , pp 617 – 68
37. Powell FL , Milsom WK , Mitchell GS : Time domains of the hypoxic ventilatory response. Respir Physiol 1998 ; 112 : 123 – 34
38. Kronenberg RS , Drage CW : Attenuation of the venti-latory and heart rate responses to hypoxia and hyper-capnia with aging in normal men. J Clin Invest 1973 ; 52 : 1812 – 9
39. Peterson DD , Pack AI , Silage DA , Fishman AP : E ects of aging on ventilatory and occlusion pressure responses to hypoxia and hypercapnia. Am Rev Respir Dis 1981 ; 124 : 387 – 91
40. Zwillich CW , Sutton FD , Pierson DJ , Greagh EM , Weil JV : Decreased hypoxic ventilatory drive in the obesity-hypoventilation syndrome. Am J Med 1975 ; 59 : 343 – 8
41. Garay SM , Rapoport D , Sorkin B , Epstein H , Feinberg I , Goldring RM : Regulation of ventilation in the obstructive sleep apnea syndrome. Am Rev Respir Dis 1981 ; 124 : 451 – 7
42. Robbins PA : Hypoxic ventilatory decline: Site of action. J Appl Physiol (1985) 1995 ; 79 : 373 – 4
43. Wilkins MR , Ghofrani HA , Weissmann N , Aldashev A , Zhao L : Pathophysiology and treatment of high-al-titude pulmonary vascular disease. Circulation 2015 ; 131 : 582 – 90
44. Berssenbrugge A , Dempsey J , Iber C , Skatrud J , Wilson P : Mechanisms of hypoxia-induced periodic breathing during sleep in humans. J Physiol 1983 ; 343 : 507 – 24
45. Pramsohler S , Schilz R , Patzak A , Rausch L , Netzer NC : Periodic breathing in healthy young adults in nor-mobaric hypoxia equivalent to 3500 m, 4500 m, and 5500 m altitude. Sleep Breath 2019 ; 23 : 703 – 9
46. Chadha TS , Birch S , Sackner MA : Periodic breath-ing triggered by hypoxia in normal awake adults. Modi cation by naloxone. Chest 1985 ; 88 : 16 – 23
ALNV134N2_Text.indb 268ALNV134N2_Text.indb 268 29-Dec-20 19:44:1129-Dec-20 19:44:11
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:262–9 269
Hypoxemia and COVID-19
Bickler et al.
47. Weiskopf RB , Viele MK , Feiner J , Kelley S , Lieberman J , Noorani M , Leung JM , Fisher DM , Murray WR , Toy P , Moore MA : Human cardiovascular and metabolic response to acute, severe isovolemic anemia. JAMA 1998 ; 279 : 217 – 21
48. Semenza GL : Regulation of mammalian O2 homeo-stasis by hypoxia-inducible factor 1. Annu Rev Cell Dev Biol 1999 ; 15 : 551 – 78
49. West JB : Physiological e ects of chronic hypoxia. N Engl J Med 2017 ; 376 : 1965 – 71
50. Schober A , Feiner JR , Bickler PE , Rollins MD : E ects of Changes in Arterial Carbon Dioxide and Oxygen Partial Pressures on Cerebral Oximeter Performance. A nesthesiology 2018 ; 128 : 97 – 108
51. Lei OK , Kong Z , Loprinzi PD , Shi Q , Sun S , Zou L , Hu Y , Nie J : Severe hypoxia does not o set the bene ts of exercise on cognitive function in seden-tary young women. Int J Environ Res Public Health 2019 ; 16
52. Le erts WK , Hughes WE , White CN , Brutsaert TD , He ernan KS : E ect of acute nitrate supplementa-tion on neurovascular coupling and cognitive perfor-mance in hypoxia. Appl Physiol Nutr Metab 2016 ; 41 : 133 – 41
53. Botek M , Krej č í J , De Smet S , G á ba A , McKune AJ : Heart rate variability and arterial oxygen saturation response during extreme normobaric hypoxia. Auton Neurosci 2015 ; 190 : 40 – 5
54. Dripps RD , Comroe JH Jr : The e ect of the inhalation of high and low oxygen concentrations on respiration, pulse rate, ballistocardiogram and arterial oxygen satu-ration (oximeter) of normal individuals. Am J Physiol 1947 ; 149 : 277 – 91
55. Lhuissier FJ , Canou ï -Poitrine F , Richalet JP : Ageing and cardiorespiratory response to hypoxia. J Physiol 2012 ; 590 : 5461 – 74
56. Jouett NP , Watenpaugh DE , Dunlap ME , Smith ML : Interactive e ects of hypoxia, hypercapnia and lung volume on sympathetic nerve activity in humans. Exp Physiol 2015 ; 100 : 1018 – 29
57. Kelman GR , Nunn JF , Prys-Roberts C , Greenbaum R : The in uence of cardiac output on arterial oxygen-ation: A theoretical study. Br J Anaesth 1967 ; 39 : 450 – 8
58. Cheney FW , Colley PS : The e ect of cardiac output on arterial blood oxygenation. A nesthesiology 1980 ; 52 : 496 – 503
59. Ronco JJ , Fenwick JC , Tweeddale MG , Wiggs BR , Phang PT , Cooper DJ , Cunningham KF , Russell JA , Walley KR : Identi cation of the critical oxygen deliv-ery for anaerobic metabolism in critically ill septic and nonseptic humans. JAMA 1993 ; 270 : 1724 – 30
60. Okorie ON , Dellinger P : Lactate: Biomarker and potential therapeutic target. Crit Care Clin 2011 ; 27 : 299 – 326
61. Liu W , Peng L , Hua S : Clinical signi cance of dynamic monitoring of blood lactic acid, oxygenation index and C-reactive protein levels in patients with severe pneu-monia. Exp Ther Med 2015 ; 10 : 1824 – 8
62. Akhmerov A , Marb á n E : COVID-19 and the Heart. Circ Res 2020 ; 126 : 1443 – 55
63. Guo T , Fan Y , Chen M , Wu X , Zhang L , He T , Wang H , Wan J , Wang X , Lu Z : Cardiovascular implications of fatal outcomes of patients with Coronavirus disease 2019 (COVID-19). JAMA Cardiol 2020 ; 5 : 1 – 8
64. Burki NK , Lee LY : Mechanisms of dyspnea. Chest 2010 ; 138 : 1196 – 201
ALNV134N2_Text.indb 269ALNV134N2_Text.indb 269 29-Dec-20 19:44:1129-Dec-20 19:44:11
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
CLINICAL FOCUS REVIEW
270 FEBRUARY 2021 ANESTHESIOLOGY, V 134 • NO 2
Jerrold H. Levy, M.D., F.A.H.A., F.C.C.M., Editor
G.W.W. and N.K.B. contributed equally to this article.
Acute Respiratory Distress Syndrome Contemporary Management and Novel Approaches during COVID -19 George W. Williams , M.D. , Nathaniel K. Berg , B.S. , Alexander Reskallah , M.D. , Xiaoyi Yuan , Ph.D. , Holger K. Eltzschig , M.D., Ph.D.
Acute respiratory distress syndrome (ARDS) is de ned as hypoxemia secondary to a rapid onset of noncardio-
genic pulmonary edema. 1 Etiologic risk factors for ARDS encompass both direct and indirect lung injuries including but not limited to pneumonia, sepsis, noncardiogenic shock, aspiration, trauma, contusion, transfusion, and inhalation injuries. Although clinical recognition and management of ARDS have improved signi cantly over the past 25 yr, it is still a leading cause of death in critically ill patients, with mortality rates consistently reported around 30 to 40%. 2
An important factor in the high mortality rate in ARDS is that treatment is mainly focused on clinical management and no targeted therapies currently exist. Furthermore, ARDS management is often challenging as it commonly occurs in a clinical setting of multiple organ failure and can also lead to the development of nonpulmonary organ injury, such as acute kidney injury. 3 Recently, the pandemic caused by coronavirus disease 2019 (COVID-19), which results from infection by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), has led to a dramatic inci-dence in COVID-19 – related ARDS. Thirty to forty per-cent of COVID-19 hospitalized patients develop ARDS, and it is associated with 70% of fatal cases. 4 , 5 At the time of this writing (July 31, 2020), there are more than 4.5 million COVID-19 cases and 152,000 related deaths in the United States. 6 Here, we describe select management strategies that have become foundations of ARDS clinical management and provide an update of emerging approaches for the treatment of ARDS related to COVID-19.
Clinical Treatment Concepts
Nationally Organized Research Consortia to Study ARDS
To improve outcomes and develop treatment protocols for ARDS, the National Heart, Lung, and Blood Institute of the National Institutes of Health (Bethesda, Maryland) funded a series of multicenter clinical trials, which formed a research collaboration called the ARDS Network ( http://ardsnet.org , accessed July 22, 2020). 7 Beginning in 1994, the network studies enrolled more than 5,500 patients, included 10 clinical trials and one observational study, led
to the development of new clinical parameters such as ventilator-free days, 8 and resulted in seminal advances that have helped to shape current ARDS management. National Heart, Lung, and Blood Institute – funded clinical trials con-tinue currently under the Prevention and Early Treatment of Acute Lung Injury (PETAL) Network ( http://petalnet.org , accessed July 22, 2020). Figure 1 and table 1 brie y summarize the results and implications of the results for ARDS and PETAL Network trials, along with other important trials performed internationally.
Small Tidal Volumes
Among the best-established guidelines in managing ARDS patients is the use of small tidal volumes during mechanical ventilation ( g. 1 ). In 2000, investigators from the ARDSNet Lower Tidal Volume (ARMA) trial reported signi cantly decreased rates of mortality (31.0% vs . 39.8%) in ARDS patients ventilated with 6 ml/kg of predicted body weight tidal volumes versus those with 12 ml/kg of predicted body weight. 9 While small tidal volume ventilation remains a tenet of lung-protective ventilation during ARDS, recent e orts have sought to determine whether small tidal volumes play a lung-pro-tective role more broadly in all critically ill ventilated patients. In 2018, the Protective Ventilation in Patients Without ARDS (PReVENT) trial indicated that venti-lation with low tidal volumes may not be more e ective than intermediate volumes in non-ARDS intensive care unit patients. 10
Positive End-expiratory Pressure
In their seminal 1967 report of ARDS cases, Ashbaugh et al . reported that improvement of hypoxemia and atelectasis was achieved by the implementation of positive end-ex-piratory pressure (PEEP). 11 Since then, PEEP continues to be employed in ARDS management and remains the focus of many clinical research e orts. Conceptually, PEEP is administered in order to reduce atelectrauma (repetitive opening and closing of alveoli) by recruiting collapsed alveoli. 12 Much attention has been directed at
Submitted for publication June 10, 2020. Accepted for publication August 31, 2020. Published online fi rst on October 5, 2020. From the Department of Anesthesiology, University of Texas Health Science Center at Houston, McGovern Medical School, Houston, Texas.
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved. Anesthesiology 2021 ; 134 : 270 – 82 . DOI: 10.1097/ALN.0000000000003571
ALNV134N2_Text.indb 270ALNV134N2_Text.indb 270 29-Dec-20 19:44:1229-Dec-20 19:44:12
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
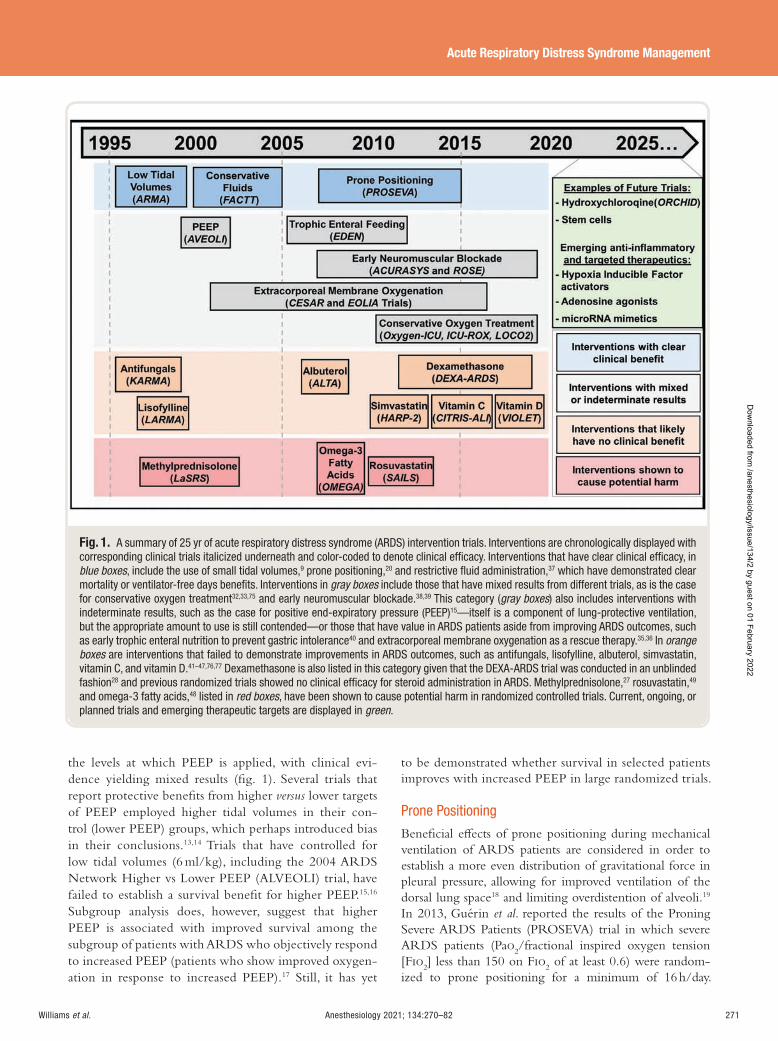
Anesthesiology 2021; 134:270–82 271
Acute Respiratory Distress Syndrome Management
Williams et al .
the levels at which PEEP is applied, with clinical evi-dence yielding mixed results ( g. 1 ). Several trials that report protective bene ts from higher versus lower targets of PEEP employed higher tidal volumes in their con-trol (lower PEEP) groups, which perhaps introduced bias in their conclusions. 13 , 14 Trials that have controlled for low tidal volumes (6 ml/kg), including the 2004 ARDS Network Higher vs Lower PEEP (ALVEOLI) trial, have failed to establish a survival bene t for higher PEEP. 15 , 16
Subgroup analysis does, however, suggest that higher PEEP is associated with improved survival among the subgroup of patients with ARDS who objectively respond to increased PEEP (patients who show improved oxygen-ation in response to increased PEEP). 17 Still, it has yet
to be demonstrated whether survival in selected patients improves with increased PEEP in large randomized trials.
Prone Positioning
Bene cial e ects of prone positioning during mechanical ventilation of ARDS patients are considered in order to establish a more even distribution of gravitational force in pleural pressure, allowing for improved ventilation of the dorsal lung space 18 and limiting overdistention of alveoli. 19
In 2013, Gu é rin et al . reported the results of the Proning Severe ARDS Patients (PROSEVA) trial in which severe ARDS patients (Pa o
2 /fractional inspired oxygen tension
[F io 2 ] less than 150 on F io
2 of at least 0.6) were random-
ized to prone positioning for a minimum of 16 h/day.
Fig. 1. A summary of 25 yr of acute respiratory distress syndrome (ARDS) intervention trials. Interventions are chronologically displayed with corresponding clinical trials italicized underneath and color-coded to denote clinical effi cacy. Interventions that have clear clinical effi cacy, in blue boxes , include the use of small tidal volumes, 9 prone positioning, 20 and restrictive fl uid administration, 37 which have demonstrated clear mortality or ventilator-free days benefi ts. Interventions in gray boxes include those that have mixed results from different trials, as is the case for conservative oxygen treatment 32 , 33 , 75 and early neuromuscular blockade. 38 , 39 This category ( gray boxes ) also includes interventions with indeterminate results, such as the case for positive end-expiratory pressure (PEEP) 15 — itself is a component of lung-protective ventilation, but the appropriate amount to use is still contended — or those that have value in ARDS patients aside from improving ARDS outcomes, such as early trophic enteral nutrition to prevent gastric intolerance 40 and extracorporeal membrane oxygenation as a rescue therapy. 35 , 36 In orange boxes are interventions that failed to demonstrate improvements in ARDS outcomes, such as antifungals, lisofylline, albuterol, simvastatin, vitamin C, and vitamin D. 41 – 47,76,77 Dexamethasone is also listed in this category given that the DEXA-ARDS trial was conducted in an unblinded fashion 28 and previous randomized trials showed no clinical effi cacy for steroid administration in ARDS. Methylprednisolone, 27 rosuvastatin, 49
and omega-3 fatty acids, 48 listed in red boxes , have been shown to cause potential harm in randomized controlled trials. Current, ongoing, or planned trials and emerging therapeutic targets are displayed in green .
ALNV134N2_Text.indb 271ALNV134N2_Text.indb 271 29-Dec-20 19:44:1329-Dec-20 19:44:13
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
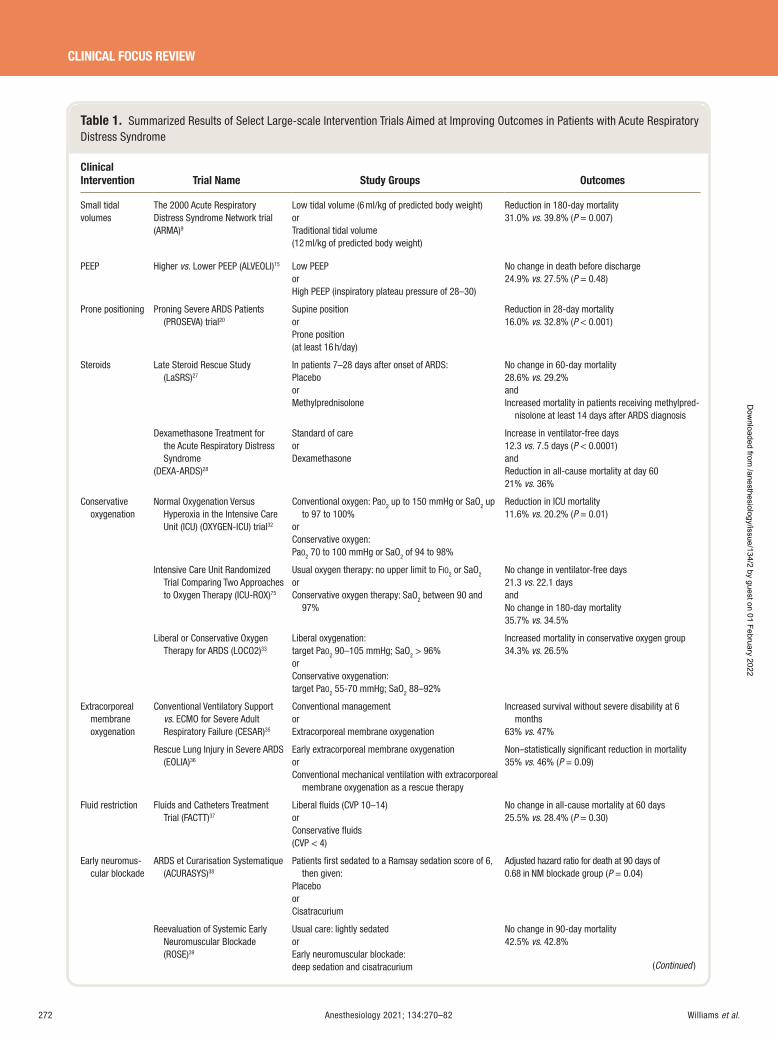
272 Anesthesiology 2021; 134:270–82 Williams et al .
CLINICAL FOCUS REVIEW
Table 1. Summarized Results of Select Large-scale Intervention Trials Aimed at Improving Outcomes in Patients with Acute Respiratory Distress Syndrome
Clinical Intervention Trial Name Study Groups Outcomes
Small tidal volumes
The 2000 Acute Respiratory Distress Syndrome Network trial (ARMA) 9
Low tidal volume (6 ml/kg of predicted body weight) or Traditional tidal volume (12 ml/kg of predicted body weight)
Reduction in 180-day mortality 31.0% vs . 39.8% ( P = 0.007)
PEEP Higher vs. Lower PEEP (ALVEOLI) 15 Low PEEP or High PEEP (inspiratory plateau pressure of 28 – 30)
No change in death before discharge24.9% vs . 27.5% ( P = 0.48)
Prone positioning Proning Severe ARDS Patients (PROSEVA) trial 20
Supine position or Prone position (at least 16 h/day)
Reduction in 28-day mortality 16.0% vs . 32.8% ( P < 0.001)
Steroids Late Steroid Rescue Study (LaSRS) 27
In patients 7 – 28 days after onset of ARDS: Placebo or Methylprednisolone
No change in 60-day mortality 28.6% vs . 29.2% and Increased mortality in patients receiving methylpred-
nisolone at least 14 days after ARDS diagnosis
Dexamethasone Treatment for the Acute Respiratory Distress Syndrome
(DEXA-ARDS) 28
Standard of care or Dexamethasone
Increase in ventilator-free days 12.3 vs. 7.5 days ( P < 0.0001) and Reduction in all-cause mortality at day 60 21% vs . 36%
Conservative oxygenation
Normal Oxygenation Versus Hyperoxia in the Intensive Care Unit (ICU) (OXYGEN-ICU) trial 32
Conventional oxygen: Pa O 2 up to 150 mmHg or SaO 2 up to 97 to 100%
or Conservative oxygen: Pa O 2 70 to 100 mmHg or SaO 2 of 94 to 98%
Reduction in ICU mortality 11.6% vs . 20.2% ( P = 0.01)
Intensive Care Unit Randomized Trial Comparing Two Approaches to Oxygen Therapy (ICU-ROX) 75
Usual oxygen therapy: no upper limit to F IO 2 or SaO 2
or Conservative oxygen therapy: SaO 2 between 90 and
97%
No change in ventilator-free days 21.3 vs . 22.1 days and No change in 180-day mortality 35.7% vs . 34.5%
Liberal or Conservative Oxygen Therapy for ARDS (LOCO2) 33
Liberal oxygenation: target Pa O 2 90 – 105 mmHg; SaO 2 > 96% or Conservative oxygenation: target Pa O 2 55-70 mmHg; SaO 2 88 – 92%
Increased mortality in conservative oxygen group 34.3% vs . 26.5%
Extracorporeal membrane oxygenation
Conventional Ventilatory Support vs . ECMO for Severe Adult Respiratory Failure (CESAR) 35
Conventional management or Extracorporeal membrane oxygenation
Increased survival without severe disability at 6 months
63% vs . 47%
Rescue Lung Injury in Severe ARDS (EOLIA) 36
Early extracorporeal membrane oxygenation or Conventional mechanical ventilation with extracorporeal
membrane oxygenation as a rescue therapy
Non – statistically signifi cant reduction in mortality 35% vs . 46% ( P = 0.09)
Fluid restriction Fluids and Catheters Treatment Trial (FACTT) 37
Liberal fl uids (CVP 10 – 14) or Conservative fl uids (CVP < 4)
No change in all-cause mortality at 60 days 25.5% vs . 28.4% ( P = 0.30)
Early neuromus-cular blockade
ARDS et Curarisation Systematique (ACURASYS) 38
Patients fi rst sedated to a Ramsay sedation score of 6, then given:
Placebo or Cisatracurium
Adjusted hazard ratio for death at 90 days of 0.68 in NM blockade group ( P = 0.04)
Reevaluation of Systemic Early Neuromuscular Blockade (ROSE) 39
Usual care: lightly sedated or Early neuromuscular blockade: deep sedation and cisatracurium
No change in 90-day mortality 42.5% vs . 42.8%
(Continued )
ALNV134N2_Text.indb 272ALNV134N2_Text.indb 272 29-Dec-20 19:44:1329-Dec-20 19:44:13
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:270–82 273
Acute Respiratory Distress Syndrome Management
Williams et al .
Patients randomized to prone positioning had a 50% reduc-tion in mortality (16% vs. 32.8%) at 28 days ( g. 1 ). 20 A recent meta-analysis corroborates these results and sup-ports the survival bene ts of prolonged prone positioning (greater than 12 h) in patients with severe ARDS. 21 Despite these encouraging results in reducing mortality with the use of prone positioning, data from a large, multinational pro-spective observational study indicate that the maneuver was employed in only 16.3% of severe ARDS patients. 2 Possible reasons for this low implementation could be attributed to the relative complexity and logistic considerations of prone positioning ( e.g. , multiple persons required for the maneuver, increased workloads, management of secretions, and nutri-tion) or to the inherent risks of the procedure such as endo-tracheal tube and vascular line displacement. Nonetheless,
the use of prone positioning for more than 12 h/day remains a strong recommendation for patients with severe ARDS. 22
Although the e cacy of prone positioning is almost exclusively suggested in patients with Pa o
2 /F io
2 ratios of
150 or less, trials that failed to show e cacy in mild and moderate ARDS are largely underpowered and failed to administer prone positioning for recommended lengths of time. 23 As such, randomized trials implementing early prone positioning in mild to moderate cases of ARDS are neces-sary to determine any survival bene ts and to make recom-mendations for clinical implementation.
Steroids in Non – COVID-19 ARDS
In the report of ARDS patients by Ashbaugh et al. in 1967, it was suggested that corticosteroids appeared to have
Table 1. (Continued)
Clinical Intervention Trial Name Study Groups Outcomes
Statin treatment Simvastatin in the Acute Respiratory Distress Syndrome (HARP-2) 47
Placebo or Simvastatin for maximum 28 days
No signifi cant change in ventilator-free days 12.6 vs . 11.5 days or 28-day mortality 22% vs . 26.8%
Statins for Acutely Injured Lungs from Sepsis (SAILS) 49
Placebo or Rosuvastatin for maximum 28 days
No change in 60-day mortality 28.5% vs . 24.9% and Fewer days free of renal or hepatic failure
Vitamins, nutrition, and supplements
Early vs . Delayed Enteral Nutrition (EDEN) 40
Trophic enteral feeding: 10 – 20 kcal/h or Full enteral feeding: 25 – 30 kcal/kg per day of nonpro-
tein calories and 1.2 to 1.6 g/kg per day of protein
No change in ventilator-free days 14.9 vs . 15 days and No change in 60-day mortality 23.2% vs . 22.2%
Omega Nutrition Supplement Trial (Omega) 48
Enteral supplementation of omega -3 fatty acids, γ -lino-lenic acid, and antioxidants
or An isocaloric control
Reduction in ventilator-free days 14.0 vs . 17.2 days and Non-statistically signifi cant increase in mortality
26.6% vs . 16.3% ( P = 0.054) Vitamin C Infusion for Treatment
in Sepsis Induced Acute Lung Injury
(CITRIS-ALI) 76
Matched placebo (5% dextrose in water) or Vitamin C 50 mg/kg total body weight every 6 h for 96 h
No change in Sequential Organ Failure Assessment (SOFA) score
3 vs . 3.5
Vitamin D to Improve Outcomes by Leveraging Early Treatment (VIOLET) 77
Placebo or Vitamin D3
No difference in 90-day mortality 23.5% vs . 20.6% ( P = 0.26)
β 2 -Agonist Albuterol for the Treatment of ALI (ALTA) 41
Aerosolized albuterol (5 mg) or Placebo (aerosolized saline)
No difference in ventilator-free days 14 .4 vs . 16.6 and No difference in mortality before hospital discharge 23% vs . 17.7%
Antifungals Ketoconazole for ALI/ARDS (KARMA) 46
Ketoconazole, 400 mg/day or Placebo
No difference in in-hospital mortality 34.1% vs . 35.2%
Lisofylline Lisofylline for ALI/ARDS (LARMA) 45 Lisofylline (3 mg/kg with a maximum dose of 300 mg) or Placebo
No difference in mortality 31.9% vs . 24.7% ( P = 0.215)
ARDS, acute respiratory distress syndrome; CVP, central venous pressure; F IO 2 , fractional inspired oxygen tension; ICU, intensive care unit; PEEP, positive end-expiratory pressure; Sa O 2 , arterial oxygen saturation.
ALNV134N2_Text.indb 273ALNV134N2_Text.indb 273 29-Dec-20 19:44:1329-Dec-20 19:44:13
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

274 Anesthesiology 2021; 134:270–82 Williams et al .
CLINICAL FOCUS REVIEW
clinical value in cases associated with fat emboli and viral pneumonia. 11 Randomized control trials conducted in the 1980s have since demonstrated that early administration of methylprednisolone did not result in improved ARDS sur-vival. 24 , 25 However, in 1998 a prospective trial by Meduri et al . showed an improved outcome in ARDS patients treated with prolonged methylprednisolone. 26 The results of the study were subject to scrutiny due to the small sample size (n = 8) of the control group, signi cant crossover into the methylprednisolone group (all of whom died), and a rel-atively large mortality rate of 60%. Subsequently, in 2006 the ARDS Network addressed the role of corticosteroid administration late in ARDS with the Late Steroid Rescue Study (LaSRS) in which 180 patients were randomized to methylprednisolone administration 7 to 28 days after diag-nosis of ARDS. Administration of methylprednisolone was not linked with signi cant reduction in mortality ( g. 1 ). 27
Furthermore, patients who started steroid treatment after 14 days of diagnosis experienced increased mortality.
Based on the postulate that, compared to other cor-ticosteroids, dexamethasone has an improved potency, lengthened duration of action, and weak mineralocorticoid e ect, Villar et al . performed a prospective trial random-izing ARDS patients to receive either dexamethasone or placebo. 28 Compared to patients in the control group, the dexamethasone treatment group showed a reduced time on mechanical ventilation and 60-day mortality; however, drug allocation and data analysis were performed in an unblinded fashion, potentially leading to bias. Furthermore, 250 patients were excluded for already receiving steroids before randomization, indicating that participating phy-sicians already favored the use of corticosteroids, which might have in uenced clinical decisions to modify mechan-ical ventilation duration. In summary, guidelines support-ing routine glucocorticoid administration in ARDS based on rigorously performed randomized controlled trials are currently not supporting their use. However, as discussed later in this review in the section of “Steroids in COVID-19 ARDS”, dexamethasone treatment has been the rst ther-apy to show mortality improvement in mechanically venti-lated COVID-19 patients. 29
Conservative Oxygenation
Among the most common therapies implemented in criti-cally ill patients and nearly all ARDS patients is the supple-mental provision of oxygen. Oxygen is frequently delivered generously in order to increase Pa o
2 , and oftentimes patients
become hyperoxic while attempting to reverse tissue hypoxia. However, evidence indicates that liberal oxygen use is associated with vasoconstriction, decreased cardiac output, absorption atelectasis, increased proin ammatory responses, and increased mortality. 30 , 31 As such, establish-ing a protocol of oxygen treatment that balances essen-tial delivery to organs while preventing excessive harmful e ects of hyperoxia has been an important subject of recent
investigations ( g. 1 ). In a single-center randomized trial published in 2016, critically ill intensive care unit patients with a length of stay of 3 days or longer who were assigned to receive conservative oxygen therapy (Pa o
2 between
70 and 100 mmHg) had lower mortality than those who received more conventional care (Pa o
2 up to 150 mmHg). 32
A more recent study, the 2020 Liberal Oxygenation versus Conservative Oxygenation in Acute Respiratory Distress Syndrome (LOCO
2 ) trial, Barrot et al. recruited ARDS
patients to conservative (oxygen saturation measured by pulse oximetry [Sp o
2 ] between 88 and 92%) or liberal (Sp o
2
greater than 96%) oxygen treatment arms. The trial was terminated early due to an associated increase in mortality at 28 days and ve episodes of mesenteric ischemia in the conservative oxygen treatment group. 33 Worse outcomes in conservative oxygenation may be attributed to the deteri-orated gas exchange in ARDS patients, making them more prone to hypoxemia in the conservative oxygen treatment arm. Going forward, trials will need to carefully assess how to determine target oxygenation levels ( e.g. , Sp o
2 and Pa o
2
targets, measurements from mixed venous blood, di erent targets for di erent organ injuries) to better answer how oxygen concentrations are selected.
Extracorporeal Membrane Oxygenation
Extracorporeal membrane oxygenation is a rescue ther-apy that has been employed in ARDS patients who fail to improve on mechanical ventilation management and as a means to avoid potential injurious aspects of venti-lator-associated lung injury. Advances in extracorporeal membrane oxygenation delivery have been associated with an increase in the number of centers and cases using it, particularly since the 2009 in uenza A virus subtype (H1N1) in uenza pandemic. 34 Investigators from the 2009 Conventional Ventilatory Support versus Extracorporeal Membrane Oxygenation for Severe Adult Respiratory Failure (CESAR) trial group sought to answer whether the use of extracorporeal membrane oxygenation during severe ARDS would provide a survival bene t when com-pared to conventional support by mechanical ventilation ( g. 1 ). 35 The results of the trial indicated that there was a survival bene t in favor of patients being randomized to extracorporeal membrane oxygenation treatment, but this di erence was not statistically signi cant. Furthermore, the study was impaired by the use of heterogeneous mechanical ventilation strategies in the control group (including the use of large tidal volumes). Additionally, a large percentage of patients in the extracorporeal membrane oxygenation group who were transferred to extracorporeal membrane oxygenation – capable hospitals never received extracor-poreal membrane oxygenation, allowing for the potential confounding e ects attributed to the fact that extracorpo-real membrane oxygenation – capable hospitals may attain enhanced ARDS survival regardless of whether patients actually received extracorporeal membrane oxygenation. A
ALNV134N2_Text.indb 274ALNV134N2_Text.indb 274 29-Dec-20 19:44:1329-Dec-20 19:44:13
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:270–82 275
Acute Respiratory Distress Syndrome Management
Williams et al .
subsequent international multicenter study was conducted to speci cally address weaknesses of previous trials imple-menting extracorporeal membrane oxygenation in early severe ARDS, the 2018 ECMO to Rescue Lung Injury in Severe ARDS (EOLIA) trial. 36 Despite achieving a high quality of control for ventilation strategies in both groups and nearly universal implementation of extracorporeal membrane oxygenation in patients randomized to receive it, the results demonstrated that there was no signi cant di erence in mortality between the extracorporeal mem-brane oxygenation group and the control group. Given the lack of strong evidence supporting the use of extracorpo-real membrane oxygenation as a routine early treatment for ARDS, it is recommended that extracorporeal membrane oxygenation is reserved as rescue therapy in patients who remain hypoxemic despite conventional evidence-based approaches.
Other Investigated Therapeutic Approaches
A large number of pharmacologic approaches have been tested in large, randomized controlled trials in order to improve clinical outcomes in patients with ARDS. These trials have included approaches such as the use of β
2 -adren-
ergics, ketoconazole, lisofylline, vitamin C and D, omega fatty acids, restrictive uid administration, and statins ( g. 1 and table 1 ). 37 – 49 Although none of these trials have demon-strated a mortality bene t in ARDS patients, it should be highlighted that recent advancements in our understand-ing of ARDS pathophysiology indicate that there are likely important subtypes of injury that predict bene cial response to particular therapies. 50 Appropriate identi ca-tion and selection of patients with speci c subphenotypes of ARDS may allow for a targeted approach to e ective treatments and more e cient clinical trials.
ARDS in COVID-19 ARDS in COVID-19 patients ( g. 2 ) presents with sev-eral unique characteristics that are not regularly described in non – COVID-19 – associated ARDS. Among these char-acteristics is the signi cant development of microvascu-lar thrombosis within the lung vasculature that contributes to ventilation-perfusion mismatch and right ventricular stress. 5 , 51 , 52 Although the cause for widespread activation of the coagulation cascade is not yet fully understood, dysreg-ulated in ammation and direct injury to endothelial cells by SARS-CoV-2 contribute to the development of micro-thrombotic immunopathology. 51 – 53 Additionally, endothelial cell damage in SARS-CoV-2 infection impairs pulmonary vasoconstriction that normally occurs in response to hypoxia to restrict blood ow to poorly ventilated areas of the lung. Disruption in this physiologic adaptation in COVID-19 patients results in shunting of blood. To this end, treatment for COVID-19 – related ARDS has been focused on mitigation of these drivers of disease pathophysiology through the use of antivirals, steroids, anticoagulants, and prone positioning.
Antiviral Therapy
The use of antiviral therapeutics in COVID-19 – related ARDS is an approach that has gained tremendous e ort and attention. Their mechanisms of action are directed at speci c viral components that are necessary for SARS-CoV-2 replication and pathogenicity. In this way, antivi-rals are unique in that they target the inciting virus instead of host-related factors, such as tissue in ammation and immune cell functions, to prevent lung injury and subse-quent excessive in ammation. Remdesivir, an inhibitor of viral RNA-dependent RNA polymerase, is perhaps the most noted antiviral currently under investigation. 54 In mere months after the emergence of SARS-CoV-2, Beigel et al. published the preliminary results of the Adaptive COVID-19 Treatment Trial (ACTT-1), a large randomized, placebo-controlled trial for the antiviral drug remdesivir. 55
The results demonstrate a statistically signi cant reduction in time to recovery in severe COVID-19 patients who received remdesivir. The shortened time to recovery e ect was strongest in the early severe disease group (patients requiring oxygen, but not yet intubated), which likely indi-cates that the timing of administration will be critical for future use. Unfortunately, the trial did not demonstrate e cacy for remdesivir in patients who began treatment after already requiring mechanical ventilation. Indeed, the follow-up time may have been too short to evaluate these patients, and the results for the complete cohort are still pending.
Additional antiviral treatments that have been proposed for the treatment of hospitalized COVID-19 patients include hydroxychloroquine, an antimalarial drug, and lopinavir-ritonavir, a protease inhibitor cocktail used for treating human immunode ciency virus. Indeed, both drugs have demonstratable e cacy in reducing SARS-CoV-2 infection in vitro , but both have failed to translate into therapeutic results in COVID-19 patients. 56 – 58 On June 29, 2020, the Randomized Evaluation of COVID-19 Therapy (RECOVERY) trial terminated its lopinavir-ri-tonavir arm due to lack of clinical bene t ( http://www.recoverytrial.net/results/lopinavar-results , accessed July 5, 2020). Similarly, on June 20, 2020, the National Institutes of Health PETAL Network halted its trial investigating hydroxychloroquine use ( http://www.nih.gov/news-events/news-releases/nih-halts-clinical-trial-hydroxychlo-roquine , accessed July 5, 2020).
Anticoagulation and Thrombolytics
Given that a key pathologic nding in COVID-19 is the prevalence of thrombotic coagulopathy within lung vas-culature, a great deal of attention has been directed at whether anticoagulation or thrombolytic therapy may pro-vide therapeutic e cacy in COVID-19 ARDS. Indeed, a French multicenter prospective study identi ed a statis-tically signi cant increase in thromboses in COVID-19 – related ARDS when compared with a historic cohort in
ALNV134N2_Text.indb 275ALNV134N2_Text.indb 275 29-Dec-20 19:44:1329-Dec-20 19:44:13
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
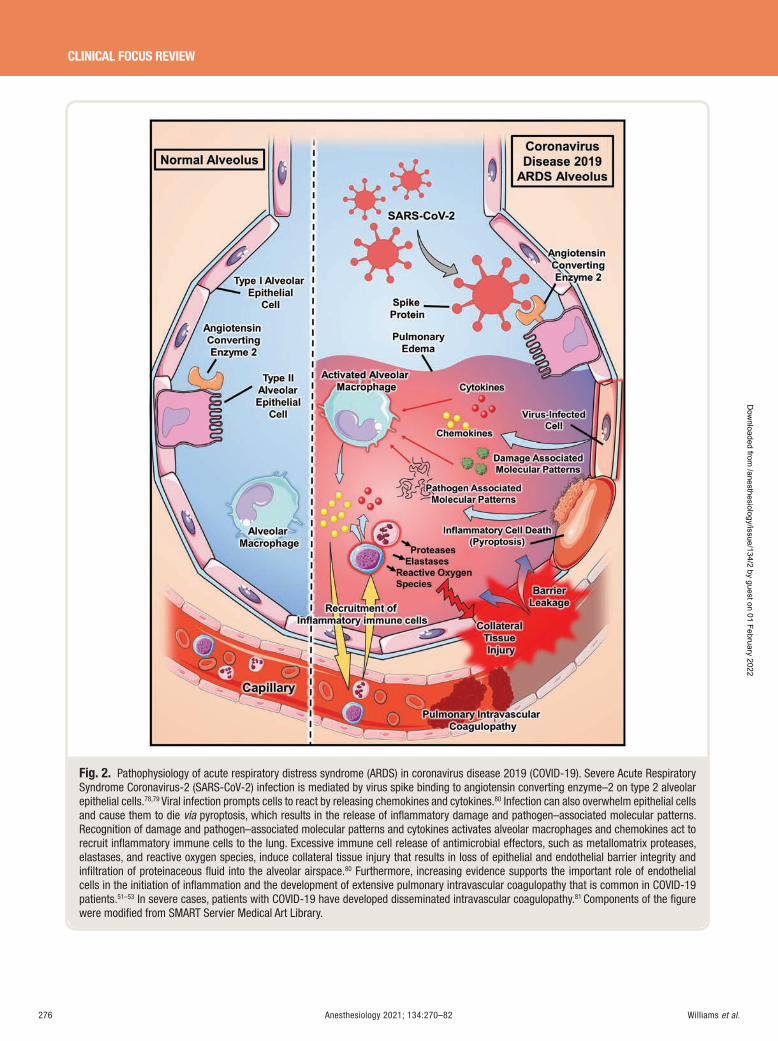
276 Anesthesiology 2021; 134:270–82 Williams et al .
CLINICAL FOCUS REVIEW
Fig. 2. Pathophysiology of acute respiratory distress syndrome (ARDS) in coronavirus disease 2019 (COVID-19). Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) infection is mediated by virus spike binding to angiotensin converting enzyme – 2 on type 2 alveolar epithelial cells. 78 , 79 Viral infection prompts cells to react by releasing chemokines and cytokines. 80 Infection can also overwhelm epithelial cells and cause them to die via pyroptosis, which results in the release of infl ammatory damage and pathogen – associated molecular patterns. Recognition of damage and pathogen – associated molecular patterns and cytokines activates alveolar macrophages and chemokines act to recruit infl ammatory immune cells to the lung. Excessive immune cell release of antimicrobial effectors, such as metallomatrix proteases, elastases, and reactive oxygen species, induce collateral tissue injury that results in loss of epithelial and endothelial barrier integrity and infi ltration of proteinaceous fl uid into the alveolar airspace. 80 Furthermore, increasing evidence supports the important role of endothelial cells in the initiation of infl ammation and the development of extensive pulmonary intravascular coagulopathy that is common in COVID-19 patients. 51 – 53 In severe cases, patients with COVID-19 have developed disseminated intravascular coagulopathy. 81 Components of the fi gure were modifi ed from SMART Servier Medical Art Library.
ALNV134N2_Text.indb 276ALNV134N2_Text.indb 276 29-Dec-20 19:44:1529-Dec-20 19:44:15
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology 2021; 134:270–82 277
Acute Respiratory Distress Syndrome Management
Williams et al .
non – COVID-19 ARDS. 59 Although there is currently a lack of evidence from randomized control trials that support the use of intermediate or treatment-level doses of prophy-lactic anticoagulation, some centers have adopted the use of such strategies. In an early Chinese retrospective analysis of severe COVID-19, anticoagulation therapy was associated with reduced 28-day mortality. 60 Furthermore, in another retrospective observational study of 2,773 patients hospital-ized for COVID-19 in New York City, patients receiving mechanical ventilation (n = 395) had signi cantly reduced in-hospital mortality when treated with treatment-dose lev-els of anticoagulation (29.1% vs . 62.7%). 61 In light of these observations and the current recognition for the pathophysi-ologic role for coagulopathy in SARS-CoV-2 infection, sev-eral clinical trials aimed at ascertaining the role of empiric therapeutic dosing with anticoagulation in COVID-19 ARDS have been initiated.
In addition to anticoagulation, thrombolytic treatment in COVID-19 ARDS patients has been proposed as a salvage therapy. Current evidence for the use of thrombolytic treat-ment in ARDS is limited to a 2001 phase I trial in which 20 patients with severe ARDS were treated with urokinase, which demonstrated improved oxygenation and no risk of bleeding. 62 Indeed, some groups have published case series for patients with COVID-19 ARDS who were treated with salvage antithrombolytic agents. 63 – 65 All patients had some level of improvement in oxygenation and/or hemodynam-ics after the administration of tissue plasminogen activator, but in most cases, patients ultimately died. Nonetheless, the scienti c rationale for using brinolytic therapy in COVID-19 ARDS — namely, the consistent ndings of pulmonary microvascular thrombosis — has resulted in the initiation of urgently needed clinical trials studying the role of antithrombotic agents in COVID-19 ARDS. 66
Prone Positioning in COVID-19 ARDS
Based on the signi cant prevalence for ventilation-perfu-sion mismatch as a result of microvascular thromboses in COVID-19 patients, prone positioning in mechanically ventilated patients is recommended in order to improve lung recruitability and oxygenation. 67 – 70 In a detailed char-acterization of mechanically ventilated COVID-19 patients in two hospitals in Boston, Massachusetts, patients who underwent prone positioning had increased median Pa o
2 /
F io 2 ratios from 150 to 232, an improvement that persisted
72 h later when Pa o 2 /F io
2 ratios of 233 were measured
while patients were supine. 71 Although there are cur-rently not enough data to conclude that prone positioning improves long-term outcomes and mortality in mechani-cally ventilated patients, the National Institutes of Health COVID-19 treatment guidelines currently suggest its use. 72
Steroids in COVID-19 ARDS
Recent data from the United Kingdom Randomised Evaluation of COVid-19 thERapY (RECOVERY) trial
investigating the use of dexamethasone in hospitalized COVID-19 patients have demonstrated that dexamethasone is the rst drug to improve mortality. 29 Mechanically venti-lated patients who were randomized to receive 6 mg once per day for 10 days were found to have a reduction of mor-tality by one third when compared to patients who under-went usual care. Interestingly, this mortality bene t was not observed in patients who did not require respiratory support. In response to these ndings, current COVID-19 treatment guidelines from the National Institutes of Health recommend its use in patients who are mechanically ventilated or require oxygen supplementation. 72 Moreover, similar to ARDS and PETAL Network studies, the RECOVERY trial provides an example of the power of organized multicenter investi-gations for new treatment approaches in critically ill patients, especially those with ARDS. Moving forward, data from the dexamethasone arm are likely to reinvigorate studies for its use in non – COVID-19 ARDS patients that may support the open-label dexamethasone studies previously mentioned. 28
Conclusions
The past 25 yr of large, randomized clinical trial e orts have contributed a tremendous amount of insight that has advanced the clinical practice of lung-protective mechani-cal ventilation. Indeed, implementation of clinically proven management interventions, such as the use of low tidal vol-umes and prone positioning, has dramatically improved the outcomes for ARDS. However, mortality remains high, and there is a lack of targeted treatment options. Nonetheless, emerging basic science research has resulted in novel ther-apeutic targets, such as hypoxia, adenosine, and microRNA signaling, that might pave the way for new pharmacologic ARDS treatments. Advancements in our appreciation for pathologic and clinical subtypes of ARDS will likely also play a critical role in designing clinical trials to identify e -cacy for treatments in speci c cohorts of ARDS patients. 50
Furthermore, the recent COVID-19 pandemic has stimu-lated the rapid initiation of clinical trials aimed at target-ing ARDS. At the time of this writing, there are over 100 registered controlled trials for COVID-19 ARDS listed on ClinicalTrials.gov. Potential interventions that demon-strate clinical e cacy in COVID-19 ARDS could also pro-vide usefulness in treating ARDS patients independent of SARS-CoV-2 infection. It is important to note, however, that insights gained from proven therapies for COVID-19 ARDS could translate to non – COVID-19 ARDS subtypes that share pathophysiologic components with COVID-19 cases. For example, the e cacy reported with dexametha-sone could indicate speci c use for patients with viral-as-sociated ARDS who are characterized by immune pro les similar to what is seen in COVID-19 and not for patients with other etiologic types of ARDS. Additional clinical studies will be required to carefully address such hypothe-ses. Last, to establish e cacy for novel ARDS interventions, collaborative e orts, such as the multicenter trials ongoing
ALNV134N2_Text.indb 277ALNV134N2_Text.indb 277 29-Dec-20 19:44:1529-Dec-20 19:44:15
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

278 Anesthesiology 2021; 134:270–82 Williams et al .
CLINICAL FOCUS REVIEW
in the PETAL Network, will continue to be vital for the successful improvement of ARDS outcomes. In addition to these large-scale studies, a network of smaller clinical trials investigating the e cacy of novel treatment concepts 73 , 74
may be required to identify new approaches for ARDS therapy. Channeling enthusiasm for new trials targeting COVID-19 ARDS may provide a catalyst and framework for these important collaborations going forward.
Research Support
Supported by grant No. T32GM120011 from the National Institutes of Health (Bethesda, Maryland; to Mr. Berg); unrestricted grant from the American Thoracic Society (New York, New York); grant No. 19CDA34660279, an American Heart Association (Dallas, Texas) Career Development Award; grant No. CA-622265, an American Lung Association (Chicago, Illinois) Catalyst Award; grant No. 1UL1TR003167 – 01, a Center for Clinical and Translational Sciences, McGovern Medical School (Houston, Texas) Pilot Award; a Parker B. Francis Fellowship (Kansas City, Missouri; to Dr. Yuan); and National Institutes of Health (Bethesda, Maryland) grant Nos. R01-DK097075, R01-HL098294, POI-HL114457, R01-DK082509, R01-HL109233, R01-DK109574, R01-HL119837, and R01-HL133900 (to Dr. Eltzshig).
Competing Interests
Dr. Williams is a scienti c speaker about sugammadex for Merck Pharmaceuticals (Kenilworth, New Jersey). The other authors declare no competing interests.
Correspondence
Address correspondence to Dr. Yuan: Department of Anesthesiology, University of Texas Health Science Center at Houston, McGovern Medical School, 6431 Fannin Street, Houston, Texas 77030. [email protected] . A nesthesiology ’ s articles are made freely accessible to all readers on www.anesthesiology.org, for personal use only, 6 months from the cover date of the issue.
References
1. Ranieri VM , Rubenfeld GD , Thompson BT , Ferguson ND , Caldwell E , Fan E , Camporota L , Slutsky AS , Force ADT : Acute respiratory distress syndrome: The Berlin de nition. JAMA 2012 ; 307 : 2526 – 33
2. Bellani G , La ey JG , Pham T , Fan E , Brochard L , Esteban A , Gattinoni L , van Haren F , Larsson A , McAuley DF , Ranieri M , Rubenfeld G , Thompson BT , Wrigge H , Slutsky AS , Pesenti A ; LUNG SAFE Investigators; ESICM Trials Group : Epidemiology, patterns of care, and mortality for patients with acute respiratory dis-tress syndrome in intensive care units in 50 countries. JAMA 2016 ; 315 : 788 – 800
3. Gumbert SD , Kork F , Jackson ML , Vanga N , Ghebremichael SJ , Wang CY , Eltzschig HK : Perioperative acute kidney injury. A nesthesiology 2020 ; 132 : 180 – 204
4. Wu C , Chen X , Cai Y , Xia Ja , Zhou X , Xu S , Huang H , Zhang L , Zhou X , Du C , Zhang Y , Song J , Wang S , Chao Y , Yang Z , Xu J , Zhou X , Chen D , Xiong W , Xu L , Zhou F , Jiang J , Bai C , Zheng J , Song Y : Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneu-monia in Wuhan, China. JAMA Internal Medicine 2020 ; 180 : 934 – 943
5. Zhou F , Yu T , Du R , Fan G , Liu Y , Liu Z , Xiang J , Wang Y , Song B , Gu X , Guan L , Wei Y , Li H , Wu X , Xu J , Tu S , Zhang Y , Chen H , Cao B : Clinical course and risk fac-tors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020 ; 395 : 1054 – 62
6. Dong E , Du H , Gardner L : An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect Dis 2020 ; 20 : 533 – 4
7. Thompson BT , Bernard GR : ARDS Network (NHLBI) studies: Successes and challenges in ARDS clinical research. Crit Care Clin 2011 ; 27 : 459 – 68
8. Schoenfeld DA , Bernard GR ; ARDS Network : Statistical evaluation of ventilator-free days as an e -cacy measure in clinical trials of treatments for acute respiratory distress syndrome. Crit Care Med 2002 ; 30 : 1772 – 7
9. Brower RG , Matthay MA , Morris A , Schoenfeld D , Thompson BT , Wheeler A , Network ARDS : Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000 ; 342 : 1301 – 8
10. Writing Group for the PReVENT Investigators : E ect of a low vs intermediate tidal volume strategy on ven-tilator-free days in intensive care unit patients with-out ARDS: A randomized clinical trial. JAMA 2018 ; 320 : 1872 – 80
11. Ashbaugh D , Boyd Bigelow D , Petty T , Levine B : Acute respiratory distress in adults. Lancet 1967 ; 290 : 319 – 23
12. Tremblay LN , Slutsky AS : Ventilator-induced lung injury: From the bench to the bedside. Intensive Care Med 2006 ; 32 : 24 – 33
13. Amato MB , Barbas CS , Medeiros DM , Magaldi RB , Schettino GP , Lorenzi-Filho G , Kairalla RA , Deheinzelin D , Munoz C , Oliveira R , Takagaki TY , Carvalho CR : E ect of a protective-ventilation strat-egy on mortality in the acute respiratory distress syn-drome. N Engl J Med 1998 ; 338 : 347 – 54
14. Villar J , Kacmarek RM , P é rez-M é ndez L , Aguirre-Jaime A : A high positive end-expiratory pressure, low tidal volume ventilatory strategy improves outcome in persistent acute respiratory distress syndrome: A
ALNV134N2_Text.indb 278ALNV134N2_Text.indb 278 29-Dec-20 19:44:1529-Dec-20 19:44:15
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:270–82 279
Acute Respiratory Distress Syndrome Management
Williams et al .
randomized, controlled trial. Crit Care Med 2006 ; 34 : 1311 – 8
15. Brower RG , Lanken PN , MacIntyre N , Matthay MA , Morris A , Ancukiewicz M , Schoenfeld D , Taylor Thompson B ; National Heart, Lung, and Blood Institute ARDS Clinical Trials Network : Higher ver-sus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N Engl J Med 2004 ; 351 : 327 – 36
16. Meade MO , Cook DJ , Guyatt GH , Slutsky AS , Arabi YM , Cooper DJ , Davies AR , Hand LE , Zhou Q , Thabane L , Austin P , Lapinsky S , Baxter A , Russell J , Skrobik Y , Ronco JJ , Stewart TE ; Lung Open Ventilation Study Investigators : Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: A randomized controlled trial. JAMA 2008 ; 299 : 637 – 45
17. Guo L , Xie J , Huang Y , Pan C , Yang Y , Qiu H , Liu L : Higher PEEP improves outcomes in ARDS patients with clinically objective positive oxygenation response to PEEP: A systematic review and meta-analysis. BMC Anesthesiol 2018 ; 18 : 172
18. Lamm WJ , Graham MM , Albert RK : Mechanism by which the prone position improves oxygenation in acute lung injury. Am J Respir Crit Care Med 1994 ; 150 : 184 – 93
19. Broccard A , Shapiro RS , Schmitz LL , Adams AB , Nahum A , Marini JJ : Prone positioning attenuates and redistributes ventilator-induced lung injury in dogs. Crit Care Med 2000 ; 28 : 295 – 303
20. Gu é rin C , Reignier J , Richard JC , Beuret P , Gacouin A , Boulain T , Mercier E , Badet M , Mercat A , Baudin O , Clavel M , Chatellier D , Jaber S , Rosselli S , Mancebo J , Sirodot M , Hilbert G , Bengler C , Richecoeur J , Gainnier M , Bayle F , Bourdin G , Leray V , Girard R , Baboi L , Ayzac L ; PROSEVA Study Group : Prone positioning in severe acute respiratory distress syn-drome. N Engl J Med 2013 ; 368 : 2159 – 68
21. Munshi L , Del Sorbo L , Adhikari NKJ , Hodgson CL , Wunsch H , Meade MO , Uleryk E , Mancebo J , Pesenti A , Ranieri VM , Fan E : Prone position for acute respi-ratory distress syndrome. A systematic review and meta-analysis. Ann Am Thorac Soc 2017 ; 14 ( suppl 4 ): S280 – 8
22. Fan E , Del Sorbo L , Goligher EC , Hodgson CL , Munshi L , Walkey AJ , Adhikari NKJ , Amato MBP , Branson R , Brower RG , Ferguson ND , Gajic O , Gattinoni L , Hess D , Mancebo J , Meade MO , McAuley DF , Pesenti A , Ranieri VM , Rubenfeld GD , Rubin E , Seckel M , Slutsky AS , Talmor D , Thompson BT , Wunsch H , Uleryk E , Brozek J , Brochard LJ ; American Thoracic Society, European Society of Intensive Care Medicine, and Society of Critical Care Medicine : An o cial American Thoracic Society/European Society
of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: Mechanical ven-tilation in adult patients with acute respiratory dis-tress syndrome. Am J Respir Crit Care Med 2017 ; 195 : 1253 – 63
23. Albert RK : Prone ventilation for patients with mild or moderate acute respiratory distress syndrome. Ann Am Thorac Soc 2020 ; 17 : 24 – 9
24. Weigelt JA , Norcross JF , Borman KR , Snyder WH 3rd : Early steroid therapy for respiratory failure. Arch Surg 1985 ; 120 : 536 – 40
25. Bernard GR , Luce JM , Sprung CL , Rinaldo JE , Tate RM , Sibbald WJ , Kariman K , Higgins S , Bradley R , Metz CA : High-dose corticosteroids in patients with the adult respiratory distress syndrome. N Engl J Med 1987 ; 317 : 1565 – 70
26. Meduri GU , Headley AS , Golden E , Carson SJ , Umberger RA , Kelso T , Tolley EA : E ect of prolonged methylprednisolone therapy in unresolving acute respiratory distress syndrome: A randomized controlled trial. JAMA 1998 ; 280 : 159 – 65
27. Steinberg KP , Hudson LD , Goodman RB , Hough CL , Lanken PN , Hyzy R , Thompson BT , Ancukiewicz M ; National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network : E cacy and safety of corticosteroids for per-sistent acute respiratory distress syndrome. N Engl J Med 2006 ; 354 : 1671 – 84
28. Villar J , Ferrando C , Mart í nez D , Ambr ó s A , Mu ñ oz T , Soler JA , Aguilar G , Alba F , Gonz á lez-Higueras E , Conesa LA , Mart í n-Rodr í guez C , D í az-Dom í nguez FJ , Serna-Grande P , Rivas R , Ferreres J , Belda J , Capilla L , Tallet A , A ñ ó n JM , Fern á ndez RL , Gonz á lez-Mart í n JM ; Dexamethasone in ARDS Network : Dexamethasone treatment for the acute respiratory distress syndrome: A multicentre, randomised con-trolled trial. Lancet Respir Med 2020 ; 8 : 267 – 76
29. RECOVERY Collaborative Group , Horby P , Lim WS , Emberson JR , Mafham M , Bell JL , Linsell L , Staplin N , Brightling C , Ustianowski A , Elmahi E , Prudon B , Green C , Felton T , Chadwick D , Rege K , Fegan C , Chappell LC , Faust SN , Jaki T , Je ery K , Montgomery A , Rowan K , Juszczak E , Baillie JK , Haynes R , Landray MJ : Dexamethasone in hospitalized patients with Covid-19 - preliminary report. N Engl J Med 2020
30. Helmerhorst HJ , Roos-Blom MJ , van Westerloo DJ , de Jonge E : Association between arterial hyperoxia and outcome in subsets of critical illness: A systematic review, meta-analysis, and meta-regression of cohort studies. Crit Care Med 2015 ; 43 : 1508 – 19
31. Asfar P , Schortgen F , Boisram é -Helms J , Charpentier J , Gu é rot E , Megarbane B , Grimaldi D , Grelon F , Anguel N , Lasocki S , Henry-Lagarrigue M , Gonzalez F , Legay F , Guitton C , Schenck M , Doise JM , Devaquet J , Van Der Linden T , Chatellier D , Rigaud JP , Dellamonica
ALNV134N2_Text.indb 279ALNV134N2_Text.indb 279 29-Dec-20 19:44:1529-Dec-20 19:44:15
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
280 Anesthesiology 2021; 134:270–82 Williams et al .
CLINICAL FOCUS REVIEW
J , Tamion F , Meziani F , Mercat A , Dreyfuss D , Seegers V , Radermacher P ; HYPER2S Investigators; REVA Research Network : Hyperoxia and hypertonic saline in patients with septic shock (HYPERS2S): A two-by-two factorial, multicentre, randomised, clinical trial. Lancet Respir Med 2017 ; 5 : 180 – 90
32. Girardis M , Busani S , Damiani E , Donati A , Rinaldi L , Marudi A , Morelli A , Antonelli M , Singer M : E ect of conservative vs conventional oxygen therapy on mortality among patients in an intensive care unit: The Oxygen-ICU Randomized Clinical Trial. JAMA 2016 ; 316 : 1583 – 9
33. Barrot L , Asfar P , Mauny F , Winiszewski H , Montini F , Badie J , Quenot JP , Pili-Floury S , Bouhemad B , Louis G , Souweine B , Collange O , Pottecher J , Levy B , Puyraveau M , Vettoretti L , Constantin JM , Capellier G ; LOCO2 Investigators and REVA Research Network : Liberal or conservative oxygen therapy for acute respiratory dis-tress syndrome. N Engl J Med 2020 ; 382 : 999 – 1008
34. April I : Extracorporeal membrane oxygenation for 2009 in uenza A (H1N1) acute respiratory distress syndrome. JAMA 2009 ; 302 : 1888 – 95
35. Peek GJ , Mugford M , Tiruvoipati R , Wilson A , Allen E , Thalanany MM , Hibbert CL , Truesdale A , Clemens F , Cooper N , Firmin RK , Elbourne D ; CESAR Trial Collaboration : E cacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009 ; 374 : 1351 – 63
36. Combes A , Hajage D , Capellier G , Demoule A , Lavou é S , Guervilly C , Da Silva D , Zafrani L , Tirot P , Veber B , Maury E , Levy B , Cohen Y , Richard C , Kalfon P , Bouadma L , Mehdaoui H , Beduneau G , Lebreton G , Brochard L , Ferguson ND , Fan E , Slutsky AS , Brodie D , Mercat A ; EOLIA Trial Group, REVA, and ECMONet : Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N Engl J Med 2018 ; 378 : 1965 – 75
37. National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network , Wiedemann HP , Wheeler AP , Bernard GR , Thompson BT , Hayden D , deBoisblanc B , Connors AF Jr , Hite RD , Harabin AL : Comparison of two u-id-management strategies in acute lung injury. N Engl J Med 2006 ; 354 : 2564 – 75
38. Papazian L , Forel JM , Gacouin A , Penot-Ragon C , Perrin G , Loundou A , Jaber S , Arnal JM , Perez D , Seghboyan JM , Constantin JM , Courant P , Lefrant JY , Gu é rin C , Prat G , Morange S , Roch A ; ACURASYS Study Investigators : Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med 2010 ; 363 : 1107 – 16
39. Moss M , Huang DT , Brower RG , Ferguson ND , Ginde AA , Gong MN , Grissom CK , Gundel S , Hayden D ,
Hite RD , Hou PC , Hough CL , Iwashyna TJ , Khan A , Liu KD , Talmor D , Thompson BT , Ulysse CA , Yealy DM , Angus DC , National Heart, Lung, and Blood Institute PETAL Clinical Trials Network : Early neu-romuscular blockade in the acute respiratory distress syndrome. N Engl J Med 2019 ; 380 : 1997 – 2008
40. Rice TW , Wheeler AP , Thompson BT , Steingrub J , Hite RD , Moss M , Morris A , Dong N , Rock P : Initial trophic vs full enteral feeding in patients with acute lung injury: The EDEN randomized trial. JAMA 2012 ; 307 : 795 – 803
41. Matthay MA , Brower RG , Carson S , Douglas IS , Eisner M , Hite D , Holets S , Kallet RH , Liu KD , MacIntyre N , Moss M , Schoenfeld D , Steingrub J , Thompson BT : Randomized, placebo-controlled clinical trial of an aerosolized beta(2)-agonist for treatment of acute lung injury. Am J Respir Crit Care Med 2011 ; 184 : 561 – 8
42. Ranieri VM , Pettila V , Karvonen MK , Jalkanen J , Nightingale P , Brealey D , Mancebo J , Ferrer R , Mercat A , Patroniti N , Quintel M , Vincent JL , Okkonen M , Meziani F , Bellani G , MacCallum N , Creteur J , Kluge S , Artigas-Raventos A , Maksimow M , Piippo I , Elima K , Jalkanen S , Jalkanen M , Bellingan G , INTEREST Study Group : E ect of intravenous interferon beta-1a on death and days free from mechanical ventilation among patients with moderate to severe acute respi-ratory distress syndrome: A randomized clinical trial . JAMA 2020 ; 323 : 725 – 733
43. Miller AC , Elamin EM , Su redini AF : Inhaled antico-agulation regimens for the treatment of smoke inhala-tion-associated acute lung injury: A systematic review. Crit Care Med 2014 ; 42 : 413 – 9
44. Mahmoodpoor A , Hamishehkar H , Shadvar K , Ostadi Z , Sanaie S , Saghaleini SH , Nader ND : The e ect of intravenous selenium on oxidative stress in critically ill patients with acute respiratory distress syndrome. Immunol Invest 2019 ; 48 : 147 – 59
45. Randomized, placebo-controlled trial of lisofylline for early treatment of acute lung injury and acute respira-tory distress syndrome. Crit Care Med 2002 ; 30 : 1 – 6
46. Ketoconazole for early treatment of acute lung injury and acute respiratory distress syndrome: A randomized controlled trial. The ARDS Network. JAMA 2000 ; 283 : 1995 – 2002
47. McAuley DF , La ey JG , O ’ Kane CM , Perkins GD , Mullan B , Trinder TJ , Johnston P , Hopkins PA , Johnston AJ , McDowell C , McNally C ; HARP-2 Investigators; Irish Critical Care Trials Group : Simvastatin in the acute respiratory distress syndrome. N Engl J Med 2014 ; 371 : 1695 – 703
48. Rice TW , Wheeler AP , Thompson BT , deBoisblanc BP , Steingrub J , Rock P ; NIH NHLBI Acute Respiratory Distress Syndrome Network of Investigators; NHLBI ARDS Clinical Trials Network : Enteral omega-3 fatty acid, gamma-linolenic acid, and antioxidant
ALNV134N2_Text.indb 280ALNV134N2_Text.indb 280 29-Dec-20 19:44:1529-Dec-20 19:44:15
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology 2021; 134:270–82 281
Acute Respiratory Distress Syndrome Management
Williams et al .
supplementation in acute lung injury. JAMA 2011 ; 306 : 1574 – 81
49. National Heart, Lung, and Blood Institute ARDS Clinical Trials Network , Truwit JD , Bernard GR , Steingrub J , Matthay MA , Liu KD , Albertson TE , Brower RG , Shanholtz C , Rock P , Douglas IS , deBoisblanc BP , Hough CL , Hite RD , Thompson BT. Rosuvastatin for sepsis-associated acute respiratory distress syndrome. N Engl J Med 2014 ; 370 : 2191 – 200
50. Wilson JG , Calfee CS : ARDS subphenotypes: Understanding a heterogeneous syndrome. Crit Care 2020 ; 24 : 102
51. McGonagle D , O ’ Donnell JS , Sharif K , Emery P , Bridgewood C : Immune mechanisms of pulmonary intravascular coagulopathy in COVID-19 pneumonia. Lancet Rheumatol 2020 ; 2 : e437 – 45
52. Teuwen LA , Geldhof V , Pasut A , Carmeliet P : COVID-19: The vasculature unleashed. Nat Rev Immunol 2020 ; 20 : 389 – 91
53. Cao W , Li T : COVID-19: Towards understanding of pathogenesis. Cell Res 2020 ; 30 : 367 – 9
54. Pruijssers AJ , George AS , Sch ä fer A , Leist SR , Gralinksi LE , Dinnon KH 3rd , Yount BL , Agostini ML , Stevens LJ , Chappell JD , Lu X , Hughes TM , Gully K , Martinez DR , Brown AJ , Graham RL , Perry JK , Du Pont V , Pitts J , Ma B , Babusis D , Murakami E , Feng JY , Bilello JP , Porter DP , Cihlar T , Baric RS , Denison MR , Sheahan TP : Remdesivir inhibits SARS-CoV-2 in human lung cells and chimeric SARS-CoV expressing the SARS-CoV-2 RNA polymerase in mice. Cell Rep 2020 ; 32 : 107940
55. Beigel JH , Tomashek KM , Dodd LE , Mehta AK , Zingman BS , Kalil AC , Hohmann E , Chu HY , Luetkemeyer A , Kline S , Lopez de Castilla D , Finberg RW , Dierberg K , Tapson V , Hsieh L , Patterson TF , Paredes R , Sweeney DA , Short WR , Touloumi G , Lye DC , Ohmagari N , Oh M-d , Ruiz-Palacios GM , Ben eld T , F ä tkenheuer G , Kortepeter MG , Atmar RL , Creech CB , Lundgren J , Babiker AG , Pett S , Neaton JD , Burgess TH , Bonnett T , Green M , Makowski M , Osinusi A , Nayak S , Lane HC : Remdesivir for the treatment of Covid-19 — preliminary report. N Engl J Med 2020; doi:10.1056/NEJMoa2007764
56. Liu J , Cao R , Xu M , Wang X , Zhang H , Hu H , Li Y , Hu Z , Zhong W , Wang M : Hydroxychloroquine, a less toxic derivative of chloroquine, is e ective in inhibiting SARS-CoV-2 infection in vitro . Cell Discov 2020 ; 6 : 16
57. Ford N , Vitoria M , Rangaraj A , Norris SL , Calmy A , Doherty M : Systematic review of the e cacy and safety of antiretroviral drugs against SARS, MERS or COVID-19: Initial assessment. J Int AIDS Soc 2020 ; 23 : e25489
58. Cao B , Wang Y , Wen D , Liu W , Wang J , Fan G , Ruan L , Song B , Cai Y , Wei M , Li X , Xia J , Chen N , Xiang J , Yu T , Bai T , Xie X , Zhang L , Li C , Yuan Y , Chen H , Li H ,
Huang H , Tu S , Gong F , Liu Y , Wei Y , Dong C , Zhou F , Gu X , Xu J , Liu Z , Zhang Y , Li H , Shang L , Wang K , Li K , Zhou X , Dong X , Qu Z , Lu S , Hu X , Ruan S , Luo S , Wu J , Peng L , Cheng F , Pan L , Zou J , Jia C , Wang J , Liu X , Wang S , Wu X , Ge Q , He J , Zhan H , Qiu F , Guo L , Huang C , Jaki T , Hayden FG , Horby PW , Zhang D , Wang C : A trial of lopinavir – ritonavir in adults hos-pitalized with severe Covid-19. N Engl J Med 2020 ; 382 : 1787 – 99
59. Helms J , Tacquard C , Severac F , Leonard-Lorant I , Ohana M , Delabranche X , Merdji H , Clere-Jehl R , Schenck M , Fagot Gandet F , Fa -Kremer S , Castelain V , Schneider F , Grunebaum L , Angl é s-Cano E , Sattler L , Mertes PM , Meziani F ; CRICS TRIGGERSEP Group (Clinical Research in Intensive Care and Sepsis Trial Group for Global Evaluation and Research in Sepsis) : High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter pro-spective cohort study. Intensive Care Med 2020 ; 46 : 1089 – 98
60. Tang N , Bai H , Chen X , Gong J , Li D , Sun Z : Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thromb Haemost 2020 ; 18 : 1094 – 9
61. Paranjpe I , Fuster V , Lala A , Russak AJ , Glicksberg BS , Levin MA , Charney AW , Narula J , Fayad ZA , Bagiella E , Zhao S , Nadkarni GN : Association of treatment dose anticoagulation with in-hospital survival among hospi-talized patients with COVID-19. J Am Coll Cardiol 2020 ; 76 : 122 – 4
62. Hardaway RM , Harke H , Tyroch AH , Williams CH , Vazquez Y , Krause GF : Treatment of severe acute respi-ratory distress syndrome: A nal report on a phase I study. Am Surg 2001 ; 67 : 377 – 82
63. Poor HD , Ventetuolo CE , Tolbert T , Chun G , Serrao G , Zeidman A , Dangayach NS , Olin J , Kohli-Seth R , Powell CA : COVID-19 critical illness pathophysiology driven by di use pulmonary thrombi and pulmonary endothelial dysfunction responsive to thrombolysis. Clin Transl Med 2020 ; 202010 : e44
64. Wang J , Hajizadeh N , Moore EE , McIntyre RC , Moore PK , Veress LA , Ya e MB , Moore HB , Barrett CD : Tissue plasminogen activator (tPA) treatment for COVID-19 associated acute respiratory distress syndrome (ARDS): A case series. J Thromb Haemost 2020 ; 18 : 1752 – 5
65. Barrett CD , Oren-Grinberg A , Chao E , Moraco AH , Martin MJ , Reddy SH , Ilg AM , Jhunjhunwala R , Uribe M , Moore HB , Moore EE , Baedorf-Kassis EN , Krajewski ML , Talmor DS , Shae S , Ya e MB : Rescue therapy for severe COVID-19-associated acute respi-ratory distress syndrome with tissue plasminogen acti-vator: A case series. J Trauma Acute Care Surg 2020 ; 89 : 453 – 7
66. Barrett CD , Moore HB , Moore EE , McIntyre RC , Moore PK , Burke J , Hua F , Apgar J , Talmor DS , Sauaia
ALNV134N2_Text.indb 281ALNV134N2_Text.indb 281 29-Dec-20 19:44:1529-Dec-20 19:44:15
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

282 Anesthesiology 2021; 134:270–82 Williams et al .
CLINICAL FOCUS REVIEW
A , Liptzin DR , Veress LA , Ya e MB : Fibrinolytic ther-apy for refractory COVID-19 acute respiratory distress syndrome: Scienti c rationale and review. Res Pract Thromb Haemost 2020 ; 4 : 524 – 31
67. Tobin MJ : Basing respiratory management of COVID-19 on physiological principles. Am J Respir Crit Care Med 2020 ; 201 : 1319 – 20
68. Lang M , Som A , Mendoza DP , Flores EJ , Reid N , Carey D , Li MD , Witkin A , Rodriguez-Lopez JM , Shepard JO , Little BP : Hypoxaemia related to COVID-19: Vascular and perfusion abnormalities on dual-energy CT. Lancet Infect Dis 2020 : 10.1016/S1473-3099(20)30367-4
69. Mauri T , Spinelli E , Scotti E , Colussi G , Basile MC , Crotti S , Tubiolo D , Tagliabue P , Zanella A , Grasselli G , Pesenti A : Potential for lung recruitment and venti-lation-perfusion mismatch in patients with the acute respiratory distress syndrome from coronavirus disease 2019. Crit Care Med 2020 ; 48 : 1129 – 1134
70. Pan C , Chen L , Lu C , Zhang W , Xia JA , Sklar MC , Du B , Brochard L , Qiu H : Lung recruitability in COVID-19-associated acute respiratory distress syndrome: A single-center observational study. Am J Respir Crit Care Med 2020 ; 201 : 1294 – 7
71. Ziehr DR , Alladina J , Petri CR , Maley JH , Moskowitz A , Medo BD , Hibbert KA , Thompson BT , Hardin CC : Respiratory pathophysiology of mechanically ventilated patients with COVID-19: A cohort study. Am J Respir Crit Care Med 2020 ; 201 : 1560 – 4
72. COVID-19 Treatment Guidelines Panel : Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available at: https://www.covid19treatmentguidelines.nih.gov/ . Accessed July 12, 2020.
73. Lee TJ , Yuan X , Kerr K , Yoo JY , Kim DH , Kaur B , Eltzschig HK : Strategies to modulate microRNA functions for the treatment of cancer or organ injury. Pharmacol Rev 2020 ; 72 : 639 – 67
74. Neudecker V , Haneklaus M , Jensen O , Khailova L , Masterson JC , Tye H , Biette K , Jedlicka P , Brodsky KS , Gerich ME , Mack M , Robertson AAB , Cooper MA , Furuta GT , Dinarello CA , O ’ Neill LA , Eltzschig HK , Masters SL , McNamee EN : Myeloid-derived miR-223 regulates intestinal in ammation via repression of the NLRP3 in ammasome. J Exp Med 2017 ; 214 : 1737 – 52
75. Mackle D , Bellomo R , Bailey M , Beasley R , Deane A , Eastwood G , Finfer S , Freebairn R , King V , Linke N : Conservative oxygen therapy during mechanical ven-tilation in the ICU. N Engl J Med 2019 ; 382 : 989 – 998
76. Fowler AA III , Truwit JD , Hite RD , Morris PE , DeWilde C , Priday A , Fisher B , Thacker LR II , Natarajan R , Brophy DF , Sculthorpe R , Nanchal R , Syed A , Sturgill J , Martin GS , Sevransky J , Kashiouris M , Hamman S , Egan KF , Hastings A , Spencer W , Tench S , Mehkri O , Bindas J , Duggal A , Graf J , Zellner S , Yanny L , McPolin C , Hollrith T , Kramer D , Ojielo C , Damm T , Cassity E , Wieliczko A , Halquist M : E ect of vitamin C infusion on organ failure and biomarkers of in ammation and vascular injury in patients with sepsis and severe acute respiratory failure: The CITRIS-ALI Randomized Clinical Trial. JAMA 2019 ; 322 : 1261 – 70
77. National Heart, Lung, and Blood Institute PETAL Clinical Trials Network , Ginde AA , Brower RG , Caterino JM , Finck L , Banner-Goodspeed VM , Grissom CK , Hayden D , Hough CL , Hyzy RC , Khan A , Levitt JE , Park PK , Ringwood N , Rivers EP , Self WH , Shapiro NI , Thompson BT , Yealy DM , Talmor D : Early high-dose vitamin D3 for critically ill, vitamin D-de cient patients. N Engl J Med 2019 ; 381 : 2529 – 40
78. Ho mann M , Kleine-Weber H , Schroeder S , Kr ü ger N , Herrler T , Erichsen S , Schiergens TS , Herrler G , Wu NH , Nitsche A , M ü ller MA , Drosten C , P ö hlmann S : SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven prote-ase inhibitor. Cell 2020 ; 181 : 271 – 280.e8
79. Zhou P , Yang XL , Wang XG , Hu B , Zhang L , Zhang W , Si HR , Zhu Y , Li B , Huang CL , Chen HD , Chen J , Luo Y , Guo H , Jiang RD , Liu MQ , Chen Y , Shen XR , Wang X , Zheng XS , Zhao K , Chen QJ , Deng F , Liu LL , Yan B , Zhan FX , Wang YY , Xiao GF , Shi ZL : A pneumonia outbreak associated with a new coronavirus of proba-ble bat origin. Nature 2020 ; 579 : 270 – 3
80. Tay MZ , Poh CM , R é nia L , MacAry PA , Ng LFP : The trinity of COVID-19: Immunity, in ammation and intervention. Nat Rev Immunol 2020 ; 20 : 363 – 74
81. Tang N , Li D , Wang X , Sun Z : Abnormal coagula-tion parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost 2020 ; 18 : 844 – 7
ALNV134N2_Text.indb 282ALNV134N2_Text.indb 282 29-Dec-20 19:44:1529-Dec-20 19:44:15
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
REVIEW ARTICLE
ANESTHESIOLOGY, V 134 • NO 2 FEBRUARY 2021 283
ABSTRACT The authors provide a comprehensive summary of all randomized, controlled trials (n = 76) involving the clinical administration of liposomal bupivacaine (Exparel; Pacira Pharmaceuticals, USA) to control postoperative pain that are currently published. When infi ltrated surgically and compared with unencap-sulated bupivacaine or ropivacaine, only 11% of trials (4 of 36) reported a clinically relevant and statistically signifi cant improvement in the primary out-come favoring liposomal bupivacaine. Ninety-two percent of trials (11 of 12) suggested a peripheral nerve block with unencapsulated bupivacaine provides superior analgesia to infi ltrated liposomal bupivacaine. Results were mixed for the 16 trials comparing liposomal and unencapsulated bupivacaine, both within peripheral nerve blocks. Overall, of the trials deemed at high risk for bias, 84% (16 of 19) reported statistically signifi cant differences for their pri-mary outcome measure(s) compared with only 14% (4 of 28) of those with a low risk of bias. The preponderance of evidence fails to support the routine use of liposomal bupivacaine over standard local anesthetics.
(ANESTHESIOLOGY 2021 ; 134 : 283 – 344 )
Deborah J. Culley, M.D., Editor
Clinical Effectiveness of Liposomal Bupivacaine Administered by Infi ltration or Peripheral Nerve Block to Treat Postoperative Pain A Narrative Review Brian M. Ilfeld , M.D., M.S. , James C. Eisenach , M.D., Rodney A. Gabriel , M.D., M.S.
Anesthesiology 2021 ; 134 : 283 – 344
This article has been selected for the Anesthesiology CME Program. Learning objectives and disclosure and ordering information can be found in the CME section at the front of this issue. This article is featured in “This Month in Anesthesiology,” page 1A. This article is accompanied by an editorial on p. 139 and an article on p. 147. This article has a related Infographic on p. 17A.
Submitted for publication August 7, 2020. Accepted for publication October 30, 2020. From the Department of Anesthesiology, University of California, San Diego, San Diego, California (B.M.I., R.A.G.); Outcomes Research Consortium, Cleveland, Ohio (B.M.I., R.A.G.); and Wake Forest School of Medicine, Winston-Salem, North Carolina (J.C.E.).
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved. Anesthesiology 2021 ; 134 : 283 – 344 . DOI: 10.1097/ALN.0000000000003630
The pain of many surgical procedures extends beyond the duration of analgesia provided with a single admin-
istration of standard local anesthetic. Bupivacaine hydro-chloride is currently the longest-acting local anesthetic approved by the U.S. Food and Drug Administration (Silver Spring, Maryland), with a duration of up to 18 h when administered in some peripheral nerve blocks. While multi-ple adjuvants such as dexamethasone and dexmedetomidine have been proposed, there is currently no Food and Drug Administration – approved medication that reliably extends the duration of action of local anesthetic beyond 24 h. 1
However, by encasing standard local anesthetic within vari-ous carriers, a sustained release may be achieved that extends the analgesic duration, perhaps to multiple days. Many such formulations have been described, 2 but only a single sus-tained released local anesthetic is currently approved for clinical use by the Food and Drug Administration: liposo-mal bupivacaine. Currently, a number of publications are available that review the use of liposomal bupivacaine, but all involve a speci c topic area ( e.g. , shoulder surgery), and therefore include only a small subset (n = 7 to 27 studies) of available randomized, controlled trials. 3 – 7 The current arti-cle aims to provide a comprehensive summary of all the published randomized, controlled trials (n = 76) involving the clinical use of liposomal bupivacaine when adminis-tered to control acute postsurgical pain.
Liposomal Local Anesthetic Liposomes consist of a hydrophilic head and two hydropho-bic tails and come in multiple permutations. Unilamellar vesicles are created with a single outer bilayer — e ectively a hollow sphere — that may hold medication within its cav-ity. 8 Far larger multilamellar liposomes are basically a sphere containing additional nested concentric spheres, much like a Russian matryoshka or babushka doll. 9 In contrast, noncon-centric multivesicular liposomes are essentially an uncoor-dinated mass creating a myriad of cavities that may be lled with medication. 10 Their large size creates a “ medication depot, ” which gradually discharges the contents with natu-ral liposome membrane breakdown. This creates a sustained release, which enables prolonged pharmacologic e ects. First proposed as a medication carrier in 1965, multivesicular liposomes have been used to encapsulate pharmaceuticals as diverse as ibuprofen, neostigmine, chemotherapeutics, and opioids. 11 In 2004, liposome morphine (DepoDur; Pacira Pharmaceuticals, USA) became the rst liposome-encased medication to be approved for postoperative analgesia by the U.S. Food and Drug Administration. 12 – 14
Extending the duration of local anesthetic (lidocaine) using liposomes was rst proposed in 1979, 15 followed a year later by the rst in vivo use in guinea pigs (dibucaine), 16
and the rst use in humans in 1988 (topical tetracaine). 17
The rst report of treating postoperative pain with lipo-somal local anesthetic occurred in 1994: subjects under-going major abdominal, thoracic, or orthopedic surgery were given a single epidural injection of either liposomal bupivacaine 0.5% or “ standard ” bupivacaine hydrochloride
REVIEW ARTICLE
Ilfeld et al.Liposomal Bupivacaine to Treat Postoperative Pain
Ilfeld et al. Liposomal Bupivacaine to Treat Postoperative Pain
2020
ALNV134N2_Text.indb 283ALNV134N2_Text.indb 283 29-Dec-20 19:44:1529-Dec-20 19:44:15
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Ilfeld et al.284 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
0.5% (subject- and observer-masked, although not ran-domized). 18 Subjects receiving unencapsulated bupivacaine experienced a mean ± SD duration of analgesia of 3.2 ± 0.4 h versus 6.3 ± 1.1 h for those receiving liposomal bupi-vacaine ( P < 0.05). Such encouraging results helped propel future preclinical and human subject research. 19
Clinical Availability
In 2011 the U.S. Food and Drug Administration approved a liposome encapsulated bupivacaine (Exparel; Pacira Pharmaceuticals) with an explicit indication: single-dose in ltration into the surgical site to produce postsurgical analgesia in adults. 20 The label was subsequently expanded to explicitly approve use in transversus abdominis plane blocks, as well as interscalene blocks speci cally for shoulder surgery. 21 The medication is provided in 20-ml ampules that contain the maximum-approved dose: 266 mg (13.3 mg/ml or 1.33%). 22 Of note, the milligram dose is expressed as the free base, so 266 mg of liposomal bupivacaine is roughly equivalent to 300 mg of unencapsulated bupivacaine hydro-chloride. 23 Each ampule should be administered within 4 h of opening, diluted with normal saline or lactated Ringer ’ s solution (up to 1:14), and administered with a 25-gauge or larger bore needle. 24 Local anesthetics other than bupi-vacaine hydrochloride may result in a premature release of bupivacaine from the liposome vesicles if administered together locally. 24 Therefore, liposomal bupivacaine should be administered after a minimum delay of 20 min after injec-tion of a di erent local anesthetic. 25 In contrast, bupivacaine hydrochloride may be administered simultaneously — even admixed within the same syringe — up to a maximum dose of 50% of the liposomal bupivacaine. 26
Liposomal bupivacaine exhibits a biphasic plasma peak when in ltrated directly into tissues. 27 The initial peak occurring within 1 to 2 h is due to the extra-liposomal bupivacaine hydrochloride included in every ampule (less than 3% of all bupivacaine in vial), which also provides an onset similar to unencapsulated bupivacaine. 28 This is fol-lowed by a second peak due to the slow release of bupi-vacaine hydrochloride from the liposomes at nearly twice the plasma concentration 24 to 48 h after administration compared to unencapsulated bupivacaine (even longer with a mixture of encapsulated and unencapsulated bupi-vacaine). 26 , 27 Bupivacaine can still be detected within the plasma 3 to 14 days after administration, depending on the route, dose, and additional factors. 27 , 29 , 30 However, local pharmacologic e ect does not necessarily mirror plasma concentration, and analgesic duration cannot be inferred from the time of bupivacaine detectability within the blood. For example, tissue in ltration with 150 mg of bupivacaine hydrochloride results in detectable plasma concentrations for over 72 h, 31 yet no clinical trial has demonstrated an analgesic e ect of even 24 h duration: blood concentration is correlated with systemic toxicity, not local e ect. 24 After liposome release, the bupivacaine absorption, distribution,
metabolism, and excretion are similar to the bupivacaine hydrochloride formulation. 24
Safety Profi le
Due to the gradual — versus immediate — release of bupi-vacaine, determining the safety pro le of liposomal bupi-vacaine requires medication-speci c investigations. 32
Preclinical studies demonstrate a similar or larger margin of safety with liposomal bupivacaine than unencapsulated bupivacaine. 32 – 39 For example, in rabbits, roughly twice as much liposomal bupivacaine must be intravenously infused to induce seizures, ventricular tachycardia, and asystole compared with bupivacaine hydrochloride. 40 In humans, 823 subjects exposed to liposomal bupivacaine within 10 randomized, controlled trials involving surgical site in l-tration experienced no more adverse events than subjects receiving bupivacaine hydrochloride, 41 a nding repro-duced when liposomal bupivacaine was administered as part of a peripheral nerve block in 335 patients among six studies. 42 Liposomal bupivacaine appears to have no nega-tive in uence on wound healing when in ltrated into the surgical site, 43 and it is compatible with common implanted materials such as titanium, silicone, and polypropylene. 44 , 45
While local anesthetic systemic toxicity can occur with liposomal bupivacaine, 46 it appears to have a favor-able cardiac safety pro le compared to bupivacaine hydro-chloride. 47 – 51 In humans, there have been three suspected intravenous injections of liposomal bupivacaine, involving 150 to 450 mg of injectate intended for surgical site tissue in ltration after knee arthroplasty. 47 Other subjects within this study had mean bupivacaine plasma concentrations of 255 ng/ml (for 150 mg group) and 520 ng/ml (450 mg group). In contrast, the three subjects with suspected intra-vascular injections had concentrations of approximately 8,000 to 34,000 ng/ml. Yet none had symptoms or signs of local anesthetic toxicity, including no electrocardio-gram/QTcF changes from baseline. 47 Toxicity has resulted from far lower doses of unencapsulated long-acting local anesthetics. 52 – 54
Clinical Effectiveness
Early in the development of new medications and devices, case reports and retrospective studies are of great service to generate hypotheses that may then be tested with ran-domized, controlled trials. This was the case for liposomal bupivacaine during much of the last decade, with 28 of 30 (93%) of reviewed retrospective studies reporting positive ndings. 55 – 84 However, in the last few years, there has been a substantial increase in the number of randomized, con-trolled trials, with 76 published at the time of this writing ( tables 1 – 10 ). Given the new plethora of data from inves-tigations with a design considered the accepted standard when evaluating medical interventions, this review will focus on published randomized, controlled trials.
ALNV134N2_Text.indb 284ALNV134N2_Text.indb 284 29-Dec-20 19:44:1529-Dec-20 19:44:15
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Ilfeld et al. Anesthesiology 2021; 134:283–344 285
Liposomal Bupivacaine to Treat Postoperative Pain
Unfortunately, 30 (40%) of these trials were either unregistered or registered after enrollment, and 26 (35%) failed to de ne a primary outcome measure or had a signif-icant problem with the de nition ( e.g. , discrepancy between registry and published article). Interpretation of results can be problematic for investigations lacking prospective regis-tration and/or a predetermined primary outcome measure. The latter is critical in evaluating randomized, controlled trials with multiple endpoints (outcomes) since the risk of erroneously nding a di erence when none truly exists (type I error) is greatly multiplied with each comparison without statistical control ( e.g. , a Bonferroni correction). 85
To illustrate, one trial designated three daily variables during a 7 to 14 day period as coprimary outcomes without a sta-tistical plan managing multiple endpoints, and reported P values greater than 0.05 for all but a single comparison (pain on postoperative day 2). 86 With 35 comparisons, the risk of erroneously nding at least one positive outcome is 83%; yet, within the abstract the single statistically signi -cant nding was emphasized, greatly skewing interpretation of the results. Designating a priori and subsequently focusing on a single comparison — the primary outcome — reduces the risk of a type I error to (typically) 5% (minimizing the type II risk as well).
Infi ltration with Liposomal Bupivacaine versus Placebo There are 12 placebo-controlled randomized trials investi-gating the use of liposomal bupivacaine in ltrated into the surgical site to control postoperative pain after procedures of the trunk, extremities, and dentition ( tables 1 and 2 ). 86 – 97
Seven of the 12 (58%) failed to nd a statistically signi -cant di erence for the primary outcome measure between active and placebo treatments, 86 – 92 and all but one had an overall low risk of bias based on the Cochrane risk-of-bias tool for randomized trials. 98 , 99 In contrast, 5 of the 12 (42%) reported a statistically signi cant di erence between active and placebo treatments for either the primary outcome measure or most of the outcomes (for studies which did not prede ne a speci c primary outcome); and, all ve of these randomized, controlled trials had a high risk of bias based on the Cochrane tool. 93 – 97 We will discuss the study meth-odology and interpretation of results for key investigations and then draw conclusions regarding clinical e ectiveness.
The Food and Drug Administration used data from three pivotal phase III studies to evaluate — and ultimately approve — the use of liposomal bupivacaine for surgical site in ltration. 94 , 95 Two of these randomized, controlled trials were published in the peer-reviewed literature and reported that liposomal bupivacaine in ltration compared with pla-cebo resulted in reduced pain scores for up to 36 and 72 h after bunion removal and hemorrhoidectomy, respectively ( table 1 ). 94 , 95 Total opioid use, time until rst opioid use, and patient satisfaction were all improved with liposomal
bupivacaine. However, two notable factors greatly in u-ence interpretation of these results. The rst is that the pain and opioid consumption outcomes were calculated using the area under the receiver operating characteristics curve (AUC), which essentially compares the integral of all val-ues over a period of time between the two treatments. If di erences are large for a short period of time but non-existent subsequently, the AUC can still be statistically sig-ni cant over the total study period, giving the impression of extended duration when none exists. Indeed, the Food and Drug Administration clinical review stated that for the hemorrhoidectomy study, “ although the primary endpoint was the AUC for pain intensity during the rst 72 h post-operatively, the two treatments (bupivacaine liposomal and placebo) di ered signi cantly and clinically only during the rst 24 h ” ( g. 1A ). 100 Similarly, for this same study, cumu-lative opioid use was reported as lower at 0 to 72 h, yet there is only an improvement within the rst 12 postoperative hours, and there are virtually no di erences between the groups over the subsequent 60 h (group di erences of 0.2 to 1.2 mg during each 12-h period, with the treatment group requiring more opioid in three of the ve 12-h periods). 95
The same issue may be found with the pivotal bunion removal randomized, controlled trial, with no di erences in e ect on pain measures after 24 h ( g. 1B ). 94 , 100 So, while it is reassuring that liposomal bupivacaine was an improve-ment over placebo for up to 24 h, it is not compelling evi-dence for clinical use.
A second important and frequently overlooked factor when interpreting the results of these two placebo-con-trolled trials is that pain score AUCs were not deter-mined exclusively using actual pain scores, but rather with the “ windowed worst-observation-carried-forward + last-observation-carried-forward ( “ wWOCF + LOCF ” ) imputation method ” in which “ NRS [Numeric Rating Scale] scores were recorded within a time window for patients who took postsurgical rescue pain medication (6 h, based on the half-life of rescue medication … ) and replaced by the ‘ worst ’ observation ( i.e. , the highest pain score before taking their rst rescue medication). ” Furthermore, miss-ing scores were replaced by one of three methods includ-ing last-observation-carried-forward. While imputation techniques such as last-observation-carried-forward were accepted by the Food and Drug Administration at the time of the original liposomal bupivacaine submission, it subse-quently determined that “ single imputation methods like last observation carried forward … should not be used as the primary approach to the treatment of missing data ” because it can result in an “ exaggerated positive e ect, biased in favor of treatment. ” 101
Moreover, the windowed worst-observation-car-ried-forward imputation — while unquestionably a valid statistical technique — remains an arti cial construct of the randomized, controlled trial and decreases generalizability of the results to patients outside of the investigation. For
ALNV134N2_Text.indb 285ALNV134N2_Text.indb 285 29-Dec-20 19:44:1629-Dec-20 19:44:16
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
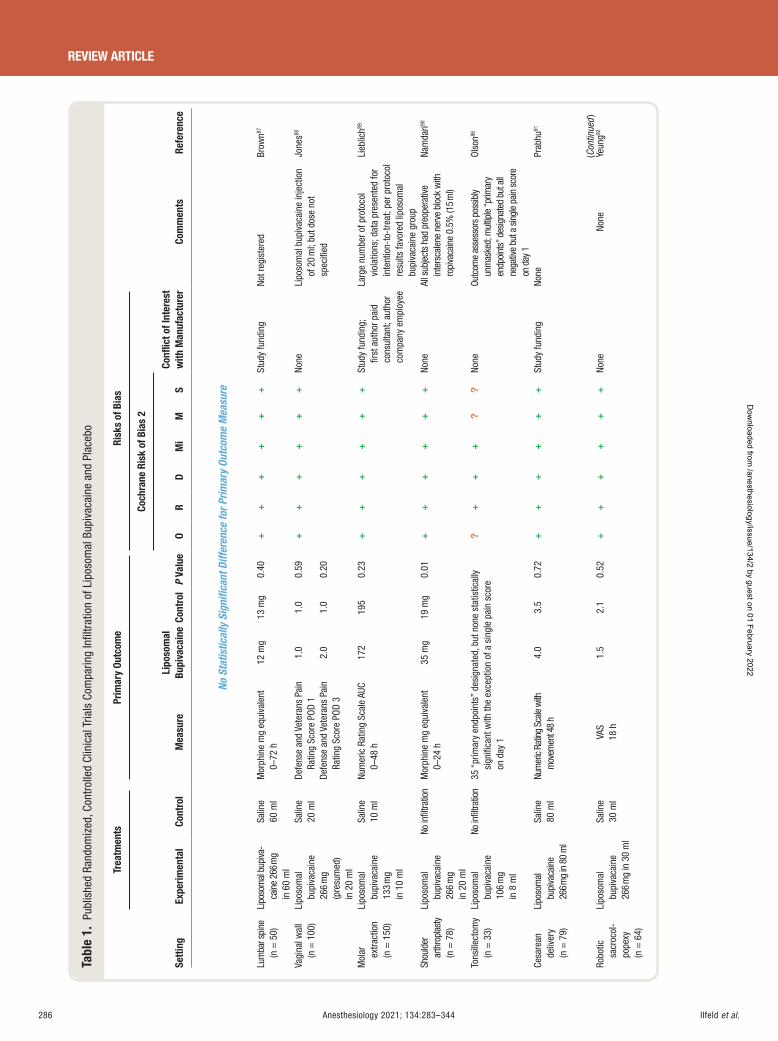
Ilfeld et al.286 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 1.
Pub
lishe
d Ra
ndom
ized
, Con
trol
led
Clin
ical
Tria
ls C
ompa
ring
Infi l
trat
ion
of L
ipos
omal
Bup
ivac
aine
and
Pla
cebo
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f Int
eres
t w
ith M
anuf
actu
rer
O R
D M
i M
S
No S
tatis
tical
ly S
igni
fi can
t Diff
eren
ce fo
r Prim
ary
Outc
ome
Mea
sure
Lum
bar s
pine
(n
= 5
0)
Lipo
som
al b
upiva
-ca
ine
266 m
g in
60
ml
Salin
e 60
ml
Mor
phin
e m
g eq
uiva
lent
0 –
72 h
12
mg
13 m
g 0.
40
++
++
++
Stud
y fu
ndin
g No
t reg
iste
red
Brow
n 87
Vagi
nal w
all
(n =
100
) Li
poso
mal
bu
piva
cain
e 26
6 m
g
(pre
sum
ed)
in 2
0 m
l
Salin
e
20 m
l De
fens
e an
d Ve
tera
ns P
ain
Ratin
g Sc
ore
POD
1 1.
0 1.
0 0.
59+
++
++
+ No
ne
Lipo
som
al b
upiv
acai
ne in
ject
ion
of 2
0 m
l; bu
t dos
e no
t sp
ecifi
ed
Jone
s 88
Defe
nse
and
Vete
rans
Pai
n Ra
ting
Scor
e PO
D 3
2.0
1.0
0.20
Mol
ar
extra
ctio
n (n
= 1
50)
Lipo
som
al
bupi
vaca
ine
133
mg
in 1
0 m
l
Salin
e
10 m
l Nu
mer
ic R
atin
g Sc
ale
AUC
0 – 48
h
172
195
0.23
+
++
++
+ St
udy
fund
ing;
fi r
st a
utho
r pai
d co
nsul
tant
; aut
hor
com
pany
em
ploy
ee La
rge
num
ber o
f pro
toco
l vi
olat
ions
; dat
a pr
esen
ted
for
inte
ntio
n-to
-tre
at; p
er p
roto
col
resu
lts fa
vore
d lip
osom
al
bupi
vaca
ine
grou
p
Lieb
lich 89
Shou
lder
ar
thro
plas
ty
(n =
78)
Lipo
som
al
bupi
vaca
ine
266
mg
in 2
0 m
l
No in
fi ltra
tion
Mor
phin
e m
g eq
uiva
lent
0 –
24 h
35
mg
19 m
g 0.
01
++
++
+ +
No
ne
All s
ubje
cts
had
preo
pera
tive
inte
rsca
lene
ner
ve b
lock
with
ro
piva
cain
e 0.
5% (1
5 ml)
Nam
dari 90
Tons
illec
tom
y (n
= 3
3)
Lipo
som
al
bupi
vaca
ine
106
mg
in 8
ml
No in
fi ltra
tion
35 “
prim
ary
endp
oint
s ” d
esig
nate
d, b
ut n
one
stat
istic
ally
si
gnifi
cant
with
the
exce
ptio
n of
a s
ingl
e pa
in s
core
on
day
1
?+
++
??
None
Ou
tcom
e as
sess
ors
poss
ibly
un
mas
ked;
mul
tiple
“ prim
ary
endp
oint
s ” d
esig
nate
d bu
t all
nega
tive
but a
sin
gle
pain
sco
re
on d
ay 1
Olso
n 86
Cesa
rean
de
liver
y (n
= 7
9)
Lipo
som
al
bupi
vaca
ine
266 m
g in
80
ml
Salin
e 80
ml
Num
eric
Ratin
g Sc
ale w
ith
mov
emen
t 48
h 4.
0 3.
5 0.
72
++
++
++
Stud
y fu
ndin
g No
ne
Prab
hu 91
Robo
tic
sacr
ocol
-po
pexy
(n
= 6
4)
Lipo
som
al
bupi
vaca
ine
266
mg
in 3
0 m
l
Salin
e
30 m
l VA
S 18
h
1.5
2.1
0.52
+
++
++
+ No
ne
None
Ye
ung 92
(C
ontin
ued )
ALNV134N2_Text.indb 286ALNV134N2_Text.indb 286 29-Dec-20 19:44:1629-Dec-20 19:44:16
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
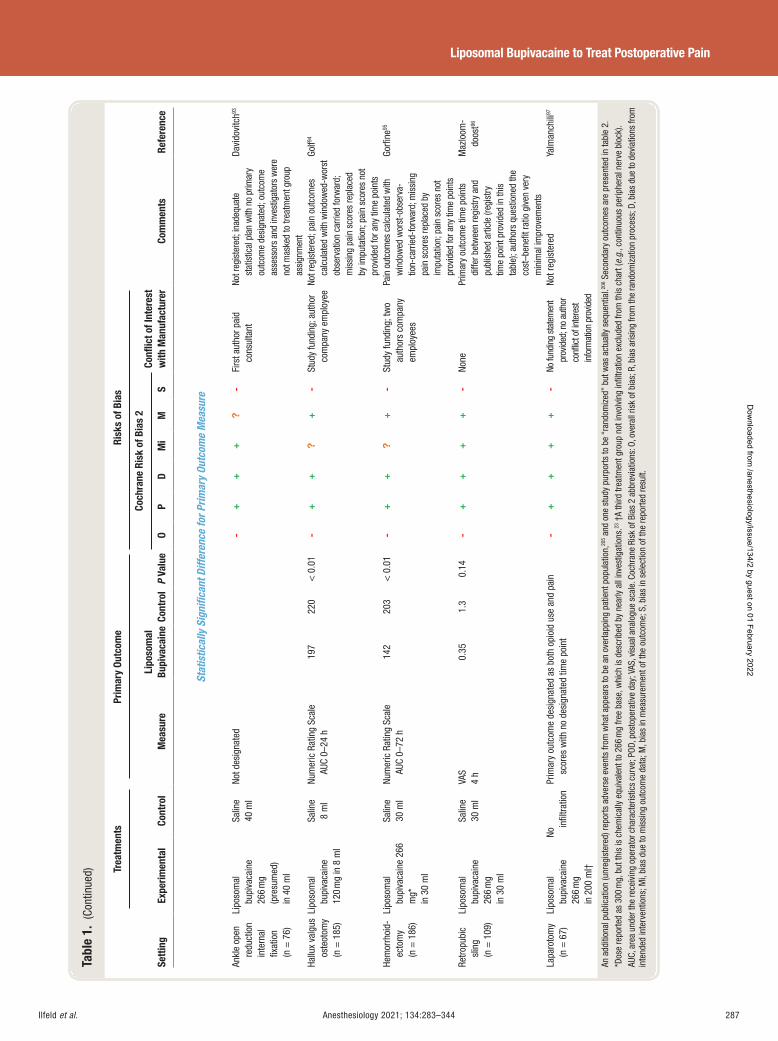
Ilfeld et al. Anesthesiology 2021; 134:283–344 287
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 1.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f Int
eres
t w
ith M
anuf
actu
rer
O P
DM
iM
S
Stat
istic
ally
Sig
nifi c
ant D
iffer
ence
for P
rimar
y Ou
tcom
e M
easu
re
Ankl
e op
en
redu
ctio
n in
tern
al
fi xat
ion
(n =
76)
Lipo
som
al
bupi
vaca
ine
266
mg
(pre
sum
ed)
in 4
0 m
l
Salin
e
40 m
l No
t des
igna
ted
-+
++
?-
Firs
t aut
hor p
aid
cons
ulta
nt
Not r
egis
tere
d; in
adeq
uate
st
atis
tical
pla
n w
ith n
o pr
imar
y ou
tcom
e de
sign
ated
; out
com
e as
sess
ors
and
inve
stig
ator
s w
ere
not m
aske
d to
trea
tmen
t gro
up
assi
gnm
ent
Davi
dovi
tch 93
Hallu
x va
lgus
os
teot
omy
(n =
185
)
Lipo
som
al
bupi
vaca
ine
120
mg
in 8
ml
Salin
e
8 m
l Nu
mer
ic R
atin
g Sc
ale
AU
C 0 –
24 h
19
7 22
0 <
0.0
1 -
++
?+
- St
udy
fund
ing;
aut
hor
com
pany
em
ploy
ee No
t reg
iste
red;
pai
n ou
tcom
es
calc
ulat
ed w
ith w
indo
wed
-wor
st
obse
rvat
ion
carr
ied
forw
ard;
m
issi
ng p
ain
scor
es re
plac
ed
by im
puta
tion;
pai
n sc
ores
not
pr
ovid
ed fo
r any
tim
e po
ints
Golf 94
Hem
orrh
oid-
ecto
my
(n =
186
)
Lipo
som
al
bupi
vaca
ine
266
mg *
in
30
ml
Salin
e
30 m
l Nu
mer
ic R
atin
g Sc
ale
AUC
0 – 72
h
142
203
< 0
.01
-+
+?
+-
Stud
y fu
ndin
g; tw
o au
thor
s co
mpa
ny
empl
oyee
s
Pain
out
com
es c
alcu
late
d w
ith
win
dow
ed w
orst
-obs
erva
-tio
n-ca
rrie
d-fo
rwar
d; m
issi
ng
pain
sco
res
repl
aced
by
impu
tatio
n; p
ain
scor
es n
ot
prov
ided
for a
ny ti
me
poin
ts
Gorfi
ne 95
Retro
pubi
c sl
ing
(n =
109
)
Lipo
som
al
bupi
vaca
ine
266
mg
in 3
0 m
l
Salin
e 30
ml
VAS
4 h
0.35
1.
3 0.
14
-+
++
+-
None
Pr
imar
y ou
tcom
e tim
e po
ints
di
ffer b
etw
een
regi
stry
and
pu
blis
hed
artic
le (r
egis
try
time
poin
t pro
vide
d in
this
ta
ble)
; aut
hors
que
stio
ned
the
cost
– ben
efi t
ratio
giv
en v
ery
min
imal
impr
ovem
ents
Maz
loom
-do
ost 96
Lapa
roto
my
(n =
67)
Li
poso
mal
bu
piva
cain
e 26
6 m
g in
200
ml †
No in
fi ltra
tion
Prim
ary
outc
ome
desi
gnat
ed a
s bo
th o
pioi
d us
e an
d pa
in
scor
es w
ith n
o de
sign
ated
tim
e po
int
-+
++
+-
No fu
ndin
g st
atem
ent
prov
ided
; no
auth
or
confl
ict o
f int
eres
t in
form
atio
n pr
ovid
ed
Not r
egis
tere
d Ya
lman
chili
97
An a
dditi
onal
pub
licat
ion
(unr
egis
tere
d) re
ports
adv
erse
eve
nts
from
wha
t app
ears
to b
e an
ove
rlapp
ing
patie
nt p
opul
atio
n, 20
5 and
one
stu
dy p
urpo
rts to
be
“ ran
dom
ized
” bu
t was
act
ually
seq
uent
ial. 20
6 Sec
onda
ry o
utco
mes
are
pre
sent
ed in
tabl
e 2 .
* D
ose
repo
rted
as 3
00 m
g, b
ut th
is is
che
mic
ally
equ
ival
ent t
o 26
6 m
g fre
e ba
se, w
hich
is d
escr
ibed
by
near
ly a
ll in
vest
igat
ions
. 23 †
A th
ird tr
eatm
ent g
roup
not
invo
lvin
g in
fi ltra
tion
excl
uded
from
this
cha
rt ( e
.g. ,
cont
inuo
us p
erip
hera
l ner
ve b
lock
). AU
C, a
rea
unde
r the
rece
ivin
g op
erat
or c
hara
cter
istic
s cu
rve;
POD
, pos
tope
rativ
e da
y; V
AS, v
isua
l ana
logu
e sc
ale.
Coc
hran
e Ri
sk o
f Bia
s 2
abbr
evia
tions
: O, o
vera
ll ris
k of
bia
s; R
, bia
s ar
isin
g fro
m th
e ra
ndom
izat
ion
proc
ess;
D, b
ias
due
to d
evia
tions
from
in
tend
ed in
terv
entio
ns; M
i, bi
as d
ue to
mis
sing
out
com
e da
ta; M
, bia
s in
mea
sure
men
t of t
he o
utco
me;
S, b
ias
in s
elec
tion
of th
e re
porte
d re
sult.
ALNV134N2_Text.indb 287ALNV134N2_Text.indb 287 29-Dec-20 19:44:1629-Dec-20 19:44:16
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
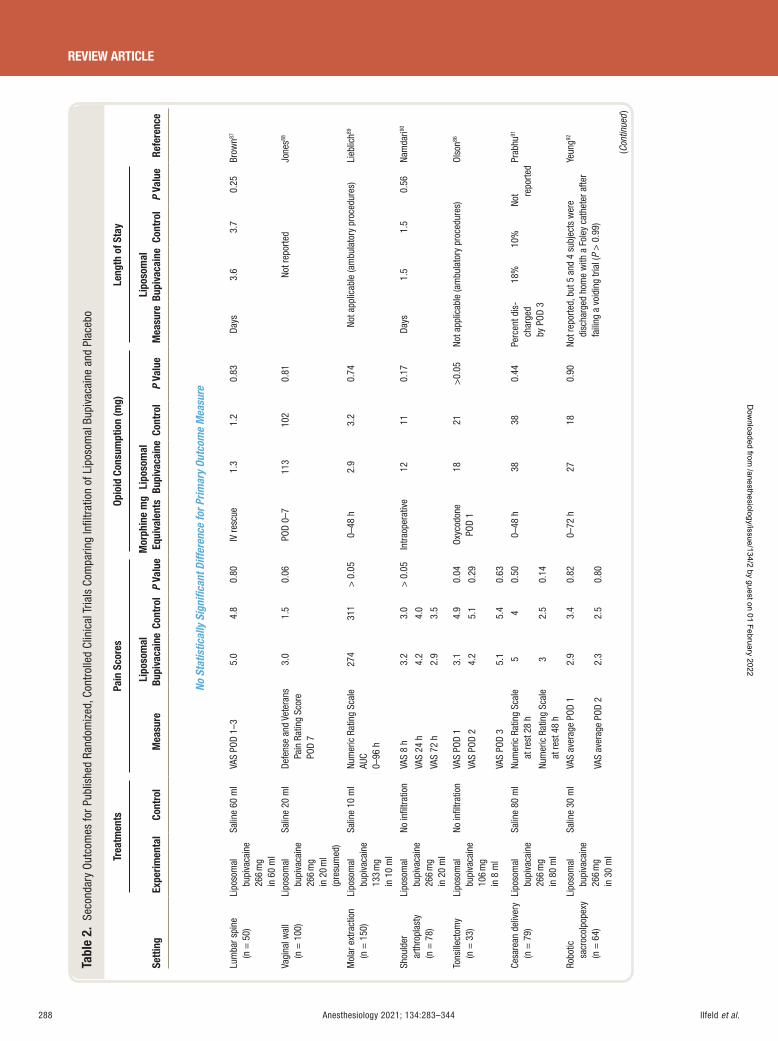
Ilfeld et al.288 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 2.
Sec
onda
ry O
utco
mes
for P
ublis
hed
Rand
omiz
ed, C
ontr
olle
d Cl
inic
al T
rials
Com
parin
g In
fi ltr
atio
n of
Lip
osom
al B
upiv
acai
ne a
nd P
lace
bo
Setti
ng
Trea
tmen
ts
Pain
Sco
res
Opio
id C
onsu
mpt
ion
(mg)
Le
ngth
of S
tay
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mor
phin
e m
g Eq
uiva
lent
s Li
poso
mal
Bu
piva
cain
e Co
ntro
l P
Valu
e M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
No S
tatis
tical
ly S
igni
fi can
t Diff
eren
ce fo
r Prim
ary
Outc
ome
Mea
sure
Lum
bar s
pine
(n
= 5
0)
Lipo
som
al
bupi
vaca
ine
266
mg
in 6
0 m
l
Salin
e 60
ml
VAS
POD
1 – 3
5.0
4.8
0.80
IV
resc
ue
1.3
1.2
0.83
Da
ys
3.6
3.7
0.25
Br
own 87
Vagi
nal w
all
(n =
100
) Li
poso
mal
bu
piva
cain
e 26
6 m
g in
20
ml
(pre
sum
ed)
Salin
e 20
ml
Defe
nse
and
Vete
rans
Pa
in R
atin
g Sc
ore
POD
7
3.0
1.5
0.06
PO
D 0 –
7 11
3 10
2 0.
81
Not r
epor
ted
Jone
s 88
Mol
ar e
xtra
ctio
n (n
= 1
50)
Lipo
som
al
bupi
vaca
ine
133
mg
in 1
0 m
l
Salin
e 10
ml
Num
eric
Rat
ing
Scal
e AU
C 0 –
96 h
274
311
> 0
.05
0 – 48
h
2.9
3.2
0.74
No
t app
licab
le (a
mbu
lato
ry p
roce
dure
s)
Lieb
lich 89
Shou
lder
ar
thro
plas
ty (n
= 7
8)
Lipo
som
al
bupi
vaca
ine
266
mg
in 2
0 m
l
No in
fi ltra
tion
VAS
8 h
3.2
3.0
> 0
.05
Intra
oper
ativ
e 12
11
0.
17
Days
1.
5 1.
5 0.
56
Nam
dari 90
VAS
24 h
4.
2 4.
0
VAS
72 h
2.
9 3.
5
Tons
illec
tom
y (n
= 3
3)
Lipo
som
al
bupi
vaca
ine
106
mg
in 8
ml
No in
fi ltra
tion
VAS
POD
1 3.
1 4.
9 0.
04
Oxyc
odon
e PO
D 1
18
21
> 0.
05
Not a
pplic
able
(am
bula
tory
pro
cedu
res)
Ol
son 86
VAS
POD
2 4.
2 5.
1 0.
29
VAS
POD
3 5.
1 5.
4 0.
63
Cesa
rean
del
iver
y (n
= 7
9)
Lipo
som
al
bupi
vaca
ine
266
mg
in 8
0 m
l
Salin
e 80
ml
Num
eric
Rat
ing
Scal
e at
rest
28
h 5
4 0.
50 0 –
48 h
38
38
0.
44
Perc
ent d
is-
char
ged
by P
OD 3
18%
10
%
Not re
porte
d Pr
abhu
91
Num
eric
Rat
ing
Scal
e at
rest
48
h 3
2.5
0.14
Robo
tic
sacr
ocol
pope
xy (n
= 6
4)
Lipo
som
al
bupi
vaca
ine
266
mg
in 3
0 m
l
Salin
e 30
ml
VAS
aver
age
POD
1 2.
9 3.
4 0.
82 0 –
72 h
27
18
0.
90
Not r
epor
ted,
but
5 a
nd 4
sub
ject
s w
ere
disc
harg
ed h
ome
with
a F
oley
cat
hete
r afte
r fa
iling
a v
oidi
ng tr
ial (
P >
0.9
9)
Yeun
g 92
VAS
aver
age
POD
2 2.
3 2.
5 0.
80
(Con
tinue
d )
ALNV134N2_Text.indb 288ALNV134N2_Text.indb 288 29-Dec-20 19:44:1629-Dec-20 19:44:16
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
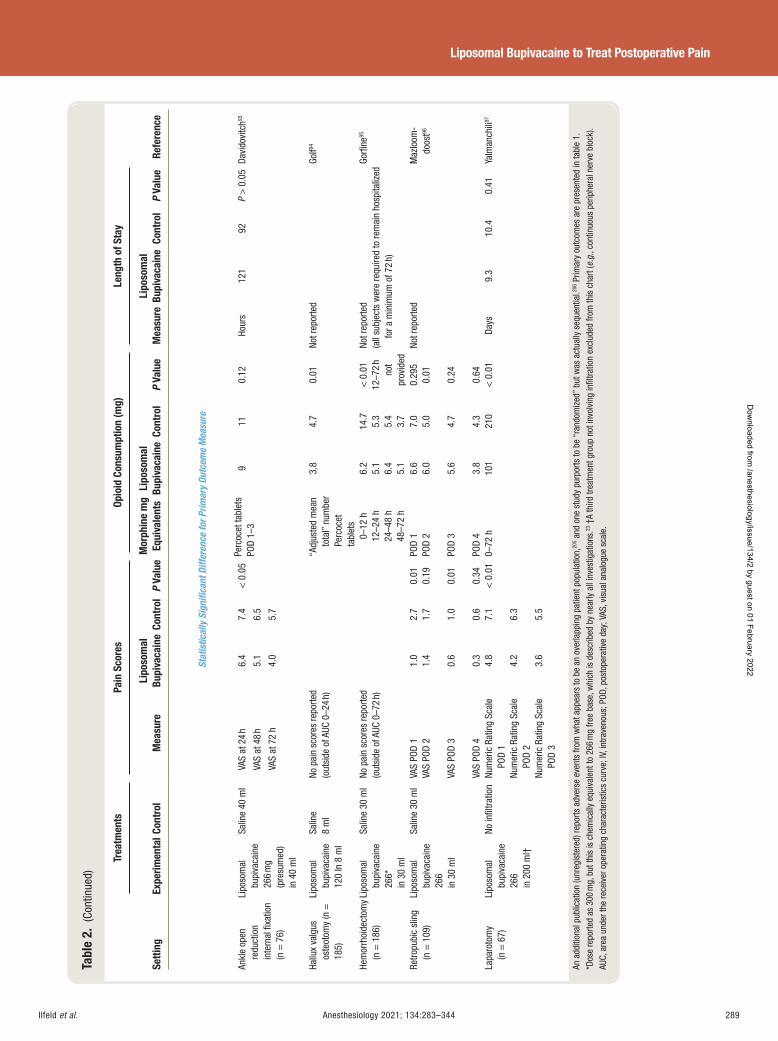
Ilfeld et al. Anesthesiology 2021; 134:283–344 289
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 2.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Pain
Sco
res
Opio
id C
onsu
mpt
ion
(mg)
Le
ngth
of S
tay
Refe
renc
e Ex
perim
enta
l Con
trol
M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mor
phin
e m
g Eq
uiva
lent
s Li
poso
mal
Bu
piva
cain
e Co
ntro
l P
Valu
e M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Stat
istic
ally
Sig
nifi c
ant D
iffer
ence
for P
rimar
y Ou
tcom
e M
easu
re
Ankl
e op
en
redu
ctio
n in
tern
al fi
xatio
n (n
= 7
6)
Lipo
som
al
bupi
vaca
ine
266
mg
(pre
sum
ed)
in 4
0 m
l
Salin
e 40
ml
VAS
at 2
4 h
6.4
7.4
< 0
.05
Perc
ocet
tabl
ets
POD
1 – 3
9 11
0.
12
Hour
s 12
1 92
P
> 0
.05
Davi
dovi
tch 93
VAS
at 4
8 h
5.1
6.5
VAS
at 7
2 h
4.0
5.7
Hallu
x va
lgus
os
teot
omy
(n =
18
5)
Lipo
som
al
bupi
vaca
ine
120
In 8
ml
Salin
e 8
ml
No p
ain
scor
es re
porte
d (o
utsi
de o
f AUC
0 – 2
4 h)
“ A
djus
ted
mea
n to
tal ”
num
ber
Perc
ocet
ta
blet
s
3.8
4.7
0.01
No
t rep
orte
d Go
lf 94
Hem
orrh
oide
ctom
y (n
= 1
86)
Lipo
som
al
bupi
vaca
ine
266 *
in
30
ml
Salin
e 30
ml
No p
ain
scor
es re
porte
d (o
utsi
de o
f AUC
0 – 7
2 h)
0 –
12 h
6.
2 14
.7
< 0
.01
Not r
epor
ted
(all
subj
ects
wer
e re
quire
d to
rem
ain
hosp
italiz
ed
for a
min
imum
of 7
2 h)
Gorfi
ne 95
12 – 2
4 h
5.1
5.3
12 – 7
2 h
not
prov
ided
24
– 48
h 6.
4 5.
4 48
– 72
h 5.
1 3.
7 Re
tropu
bic
slin
g (n
= 1
09)
Lipo
som
al
bupi
vaca
ine
266
in 3
0 m
l
Salin
e 30
ml
VAS
POD
1 1.
0 2.
7 0.
01
POD
1 6.
6 7.
0 0.
295
Not r
epor
ted
Maz
loom
-do
ost 96
VA
S PO
D 2
1.4
1.7
0.19
POD
2 6.
0 5.
0 0.
01
VAS
POD
3 0.
6 1.
0 0.
01 PO
D 3
5.6
4.7
0.24
VAS
POD
4 0.
3 0.
6 0.
34
POD
4 3.
8 4.
3 0.
64
Lapa
roto
my
(n =
67)
Li
poso
mal
bu
piva
cain
e 26
6 in
200
ml †
No in
fi ltra
tion
Num
eric
Rat
ing
Scal
e PO
D 1
4.8
7.1
< 0
.01
0 – 72
h
101
210
< 0
.01
Days
9.
3 10
.4
0.41
Ya
lman
chili
97
Num
eric
Rat
ing
Scal
e PO
D 2
4.2
6.3
Num
eric
Rat
ing
Scal
e PO
D 3
3.6
5.5
An a
dditi
onal
pub
licat
ion
(unr
egis
tere
d) re
ports
adv
erse
eve
nts
from
wha
t app
ears
to b
e an
ove
rlapp
ing
patie
nt p
opul
atio
n, 20
5 and
one
stu
dy p
urpo
rts to
be
“ ran
dom
ized
” bu
t was
act
ually
seq
uent
ial. 20
6 Prim
ary
outc
omes
are
pre
sent
ed in
tabl
e 1 .
* D
ose
repo
rted
as 3
00 m
g, b
ut th
is is
che
mic
ally
equ
ival
ent t
o 26
6 m
g fre
e ba
se, w
hich
is d
escr
ibed
by
near
ly a
ll in
vest
igat
ions
. 23 †
A th
ird tr
eatm
ent g
roup
not
invo
lvin
g in
fi ltra
tion
excl
uded
from
this
cha
rt ( e
.g. ,
cont
inuo
us p
erip
hera
l ner
ve b
lock
). AU
C, a
rea
unde
r the
rece
iver
ope
ratin
g ch
arac
teris
tics
curv
e; IV
, int
rave
nous
; POD
, pos
tope
rativ
e da
y; V
AS, v
isua
l ana
logu
e sc
ale.
ALNV134N2_Text.indb 289ALNV134N2_Text.indb 289 29-Dec-20 19:44:1629-Dec-20 19:44:16
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
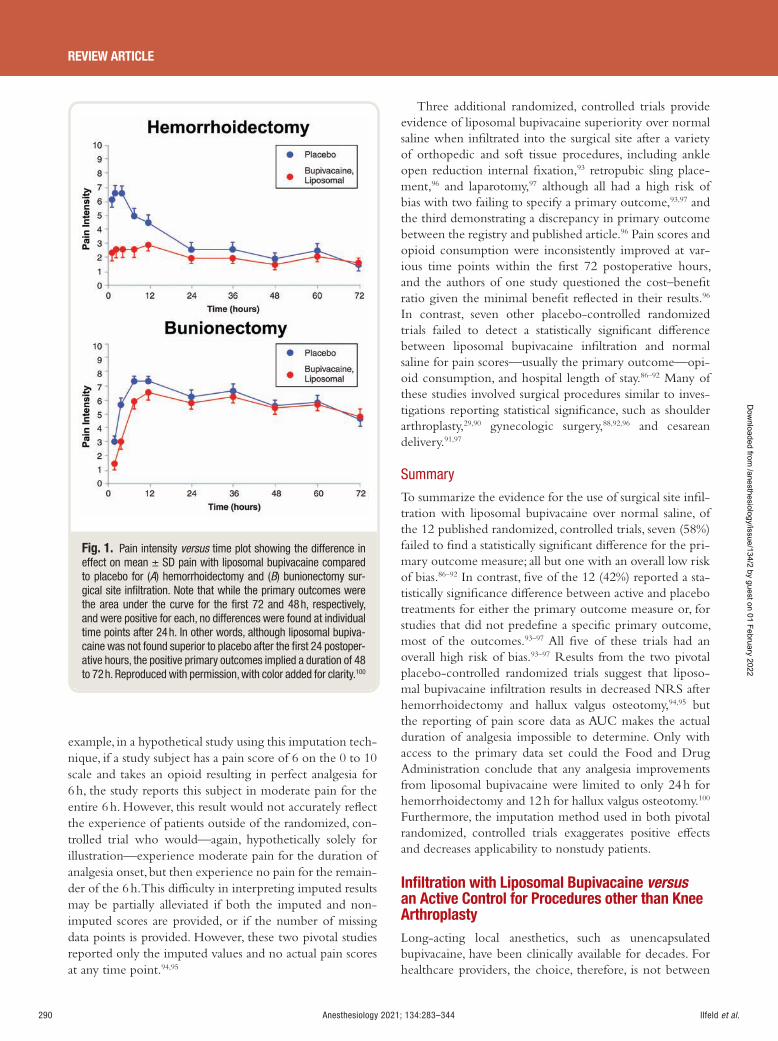
Ilfeld et al.290 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
example, in a hypothetical study using this imputation tech-nique, if a study subject has a pain score of 6 on the 0 to 10 scale and takes an opioid resulting in perfect analgesia for 6 h, the study reports this subject in moderate pain for the entire 6 h. However, this result would not accurately re ect the experience of patients outside of the randomized, con-trolled trial who would — again, hypothetically solely for illustration — experience moderate pain for the duration of analgesia onset, but then experience no pain for the remain-der of the 6 h. This di culty in interpreting imputed results may be partially alleviated if both the imputed and non-imputed scores are provided, or if the number of missing data points is provided. However, these two pivotal studies reported only the imputed values and no actual pain scores at any time point. 94 , 95
Three additional randomized, controlled trials provide evidence of liposomal bupivacaine superiority over normal saline when in ltrated into the surgical site after a variety of orthopedic and soft tissue procedures, including ankle open reduction internal xation, 93 retropubic sling place-ment, 96 and laparotomy, 97 although all had a high risk of bias with two failing to specify a primary outcome, 93 , 97 and the third demonstrating a discrepancy in primary outcome between the registry and published article. 96 Pain scores and opioid consumption were inconsistently improved at var-ious time points within the rst 72 postoperative hours, and the authors of one study questioned the cost – bene t ratio given the minimal bene t re ected in their results. 96
In contrast, seven other placebo-controlled randomized trials failed to detect a statistically signi cant di erence between liposomal bupivacaine in ltration and normal saline for pain scores — usually the primary outcome — opi-oid consumption, and hospital length of stay. 86 – 92 Many of these studies involved surgical procedures similar to inves-tigations reporting statistical signi cance, such as shoulder arthroplasty, 29 , 90 gynecologic surgery, 88 , 92 , 96 and cesarean delivery. 91 , 97
Summary
To summarize the evidence for the use of surgical site in l-tration with liposomal bupivacaine over normal saline, of the 12 published randomized, controlled trials, seven (58%) failed to nd a statistically signi cant di erence for the pri-mary outcome measure; all but one with an overall low risk of bias. 86 – 92 In contrast, ve of the 12 (42%) reported a sta-tistically signi cance di erence between active and placebo treatments for either the primary outcome measure or, for studies that did not prede ne a speci c primary outcome, most of the outcomes. 93 – 97 All ve of these trials had an overall high risk of bias. 93 – 97 Results from the two pivotal placebo-controlled randomized trials suggest that liposo-mal bupivacaine in ltration results in decreased NRS after hemorrhoidectomy and hallux valgus osteotomy, 94 , 95 but the reporting of pain score data as AUC makes the actual duration of analgesia impossible to determine. Only with access to the primary data set could the Food and Drug Administration conclude that any analgesia improvements from liposomal bupivacaine were limited to only 24 h for hemorrhoidectomy and 12 h for hallux valgus osteotomy. 100
Furthermore, the imputation method used in both pivotal randomized, controlled trials exaggerates positive e ects and decreases applicability to nonstudy patients.
Infi ltration with Liposomal Bupivacaine versus an Active Control for Procedures other than Knee Arthroplasty Long-acting local anesthetics, such as unencapsulated bupivacaine, have been clinically available for decades. For healthcare providers, the choice, therefore, is not between
Fig. 1. Pain intensity versus time plot showing the difference in effect on mean ± SD pain with liposomal bupivacaine compared to placebo for ( A ) hemorrhoidectomy and ( B ) bunionectomy sur-gical site infi ltration. Note that while the primary outcomes were the area under the curve for the fi rst 72 and 48 h, respectively, and were positive for each, no differences were found at individual time points after 24 h. In other words, although liposomal bupiva-caine was not found superior to placebo after the fi rst 24 postoper-ative hours, the positive primary outcomes implied a duration of 48 to 72 h. Reproduced with permission, with color added for clarity. 100
ALNV134N2_Text.indb 290ALNV134N2_Text.indb 290 29-Dec-20 19:44:1729-Dec-20 19:44:17
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Ilfeld et al. Anesthesiology 2021; 134:283–344 291
Liposomal Bupivacaine to Treat Postoperative Pain
liposomal bupivacaine and a placebo, but rather replacing an older medication with the new. Only studies includ-ing an active control can provide data on which to base a decision. Fortunately, at the time of this writing, there are 36 randomized, controlled trials involving surgical site in ltration comparing liposomal bupivacaine and unen-capsulated bupivacaine or ropivacaine ( tables 3-6 ). 23 , 31 , 102 – 131
Since nearly half of these include a single surgical proce-dure — knee arthroplasty — we will present these studies separately ( tables 5 and 6 ). 23 , 31 , 117 – 131
Of the 19 randomized, active-controlled trials involving surgical procedures other than knee arthroplasty, 15 (79%) failed to nd a statistically signi cant di erence for their primary outcome measure ( tables 3 and 4 ). 23 , 102 – 112 These included both open and laparoscopic orthopedic and soft tissue procedures of the trunk, extremities, and dentition. While a few detected improvements favoring liposo-mal bupivacaine in some secondary endpoints, 102 , 103 , 105 , 109
the majority failed to detect statistically signi cant dif-ferences between treatments for all variables at all time points. 23 , 104 , 106 – 108 , 110 – 112 Overall risk of bias was deemed low in eight, 23 , 105 – 108 , 110 some concerns in three, 104 , 111 , 112 and high in three studies. 102 , 103 , 109 Multiple investigations were unregistered and/or did not specify a primary outcome measure time point, although the impact of these de cien-cies appears minimal with the near total lack of statistical signi cance between treatments. Furthermore, some of the negative studies were phase II and III dose – response tri-als that were not speci cally designed to investigate clinical e ectiveness. 23 However, they were included in a manu-facturer-supported review article that highlighted positive ndings in various secondary and tertiary endpoints 23 ; thus, it appears reasonable to include the negative ndings here as well.
In contrast, 4 of the 19 randomized, controlled trials (21%) reported a statistically signi cant di erence for their primary outcome measure(s) between liposomal bupiva-caine and unencapsulated local anesthetic. 113 – 116 Three of these were rated as having a high risk of bias, 113 , 114 , 116 while one was rated as “ some concerns. ” 115 The investigation with the strongest ndings involved oral/dental implant surgery, with liposomal bupivacaine resulting in lower cumulative pain scores at all time points during the rst postoperative week. 114 Satisfaction with analgesia was higher within the rst 24 h after surgery, although there were no di erences in opioid consumption. 114 Unfortunately, only 12.5 ml (63 mg) of bupivacaine hydrochloride was utilized for the comparison/control group — less than half of the 30 ml fre-quently used for simple molar extraction — while the maxi-mum approved liposomal bupivacaine dose was utilized for the experimental group. 132 The registry provided no details as to how the primary outcome measure would be ana-lyzed ( “ postsurgical pain severity [time frame: 7 days] ” ), and the published article did not mention a primary outcome measure (but stated that “ no sample size calculation was
performed ” ). Therefore, this trial was deemed to be at high risk of bias. 98 , 99
Another randomized, controlled trial reporting a statisti-cally signi cant di erence for its primary outcome measure involved hemorrhoidectomy, which demonstrated liposo-mal bupivacaine bene ts in pain scores, opioid consump-tion, and opioid-related side e ects. 113 Pain scores were provided only in the cumulative 0 to 72 h AUC format, without daily totals, precluding assessment of the time win-dow of true di erence. 113 It is also noteworthy that compar-ing the maximum approved dose of liposomal bupivacaine (266 mg) to 75 mg of bupivacaine hydrochloride in this study resulted in a statistically signi cant di erence; how-ever, a very similar randomized, controlled trial that used a 100 mg bupivacaine hydrochloride dose did not detect a statistically signi cant di erence between treatments. 23
Importantly, 100 mg still remains far below the maximum Food and Drug Administration – approved dose of bupiv-acaine hydrochloride — 2.5 mg/kg up to 175 mg (3 mg/kg up to 225 mg with the addition of epinephrine) — while the maximum approved liposomal bupivacaine dose of 266 mg was utilized. 100 Due to a discrepancy between the regis-try description of the primary outcome measure and the published manuscript, this study was rated at high risk of bias. 98 , 99
The remaining two investigations with statistically sig-ni cant di erences for their primary endpoints involved soft tissue surgical procedures. 115 , 116 The rst examined in ltrating liposomal bupivacaine after midurethral sling placement and identi ed lower pain scores exclusively on the rst postoperative day of seven. 115 The investigators concluded that liposomal bupivacaine “ did not result in a clinically signi cant [emphasis added] di erence in POD [postoperative day] 1 pain scores, ” and given the lack of analgesic improvement and opioid at other time points, “ the cost of this anesthetic … may not justify its use … ” 115
Similarly, while the authors of the second article found a statistically signi cant reduction in pain scores within the 72 h after mammoplasty, these improvements were less than 1.0 point on the 0 to 10 Numeric Rating Scale, leading the authors to conclude “ that the additional cost of liposomal bupivacaine is unjusti ed for this particular use. ” 116
Both of the two positive trials used a dose of bupivacaine hydrochloride for the control arm at less than half of the Food and Drug Administration – approved and frequently used maximum for these surgical procedures. 23 , 113 , 114 , 132
Both liposomal and unencapsulated bupivacaine have a dose – response relationship with increasing doses resulting in increased e ects/duration and, conversely, decreasing dose resulting in decreased e ects/duration. 23 Therefore, when evaluating active-controlled trials, lower dosing of the comparator local anesthetic reduces con dence in the clinical applicability of the results.
ALNV134N2_Text.indb 291ALNV134N2_Text.indb 291 29-Dec-20 19:44:1729-Dec-20 19:44:17
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
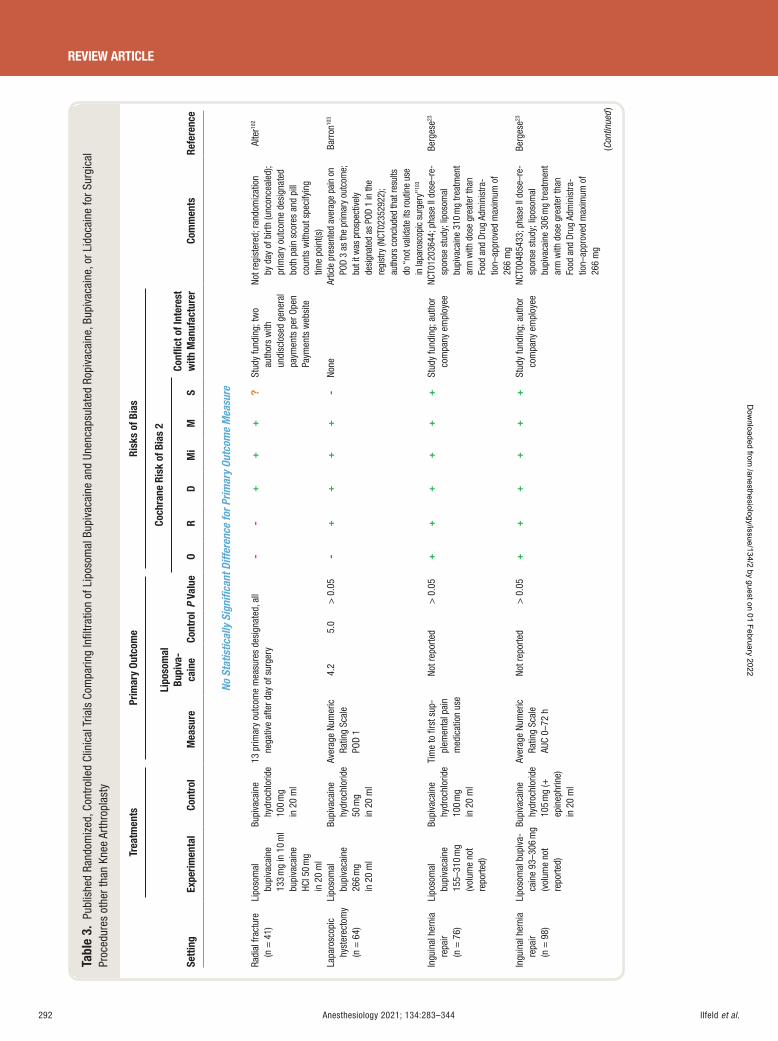
Ilfeld et al.292 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 3.
Pub
lishe
d Ra
ndom
ized
, Con
trol
led
Clin
ical
Tria
ls C
ompa
ring
Infi l
trat
ion
of L
ipos
omal
Bup
ivac
aine
and
Une
ncap
sula
ted
Ropi
vaca
ine,
Bup
ivac
aine
, or L
idoc
aine
for S
urgi
cal
Proc
edur
es o
ther
than
Kne
e Ar
thro
plas
ty
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
va-
cain
e Co
ntro
l P
Valu
e
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f Int
eres
t w
ith M
anuf
actu
rer
O R
D M
i M
S
No S
tatis
tical
ly S
igni
fi can
t Diff
eren
ce fo
r Prim
ary
Outc
ome
Mea
sure
Radi
al fr
actu
re
(n =
41)
Li
poso
mal
bu
piva
cain
e 13
3 m
g in
10
ml
bupi
vaca
ine
HCl 5
0 m
g in
20
ml
Bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g in
20
ml
13 p
rimar
y ou
tcom
e m
easu
res
desi
gnat
ed, a
ll ne
gativ
e af
ter d
ay o
f sur
gery
-
-+
+
+?
Stud
y fu
ndin
g; tw
o au
thor
s w
ith
undi
sclo
sed
gene
ral
paym
ents
per
Ope
n Pa
ymen
ts w
ebsi
te
Not r
egis
tere
d; ra
ndom
izat
ion
by d
ay o
f birt
h (u
ncon
ceal
ed);
prim
ary
outc
ome
desi
gnat
ed
both
pai
n sc
ores
and
pill
co
unts
with
out s
peci
fyin
g tim
e po
int(s
)
Alte
r 102
Lapa
rosc
opic
hy
ster
ecto
my
(n =
64)
Lipo
som
al
bupi
vaca
ine
266
mg
in 2
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 50
mg
in 2
0 m
l
Aver
age
Num
eric
Ra
ting
Scal
ePO
D 1
4.2
5.0
> 0
.05
-+
++
+-
None
Ar
ticle
pre
sent
ed a
vera
ge p
ain
on
POD
3 as
the
prim
ary
outc
ome;
bu
t it w
as p
rosp
ectiv
ely
desi
gnat
ed a
s PO
D 1
in th
e re
gist
ry (N
CT02
3529
22);
auth
ors
conc
lude
d th
at re
sults
do
“ no
t val
idat
e its
rout
ine
use
in la
paro
scop
ic s
urge
ry ” 10
3
Barr
on 10
3
Ingu
inal
her
nia
repa
ir (n
= 7
6)
Lipo
som
al
bupi
vaca
ine
155 –
310
mg
(vol
ume
not
repo
rted)
Bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g in
20
ml
Tim
e to
fi rs
t sup
-pl
emen
tal p
ain
med
icat
ion
use
Not r
epor
ted
> 0
.05
++
++
++
Stud
y fu
ndin
g; a
utho
r co
mpa
ny e
mpl
oyee
NC
T012
0364
4; p
hase
II d
ose –
re-
spon
se s
tudy
; lip
osom
al
bupi
vaca
ine
310
mg
treat
men
t ar
m w
ith d
ose
grea
ter t
han
Food
and
Dru
g Ad
min
istra
-tio
n – ap
prov
ed m
axim
um o
f 26
6 m
g
Berg
ese 23
Ingu
inal
her
nia
repa
ir (n
= 9
8)
Lipo
som
al b
upiv
a-ca
ine
93 – 3
06 m
g (v
olum
e no
t re
porte
d)
Bupi
vaca
ine
hydr
ochl
orid
e 10
5 m
g ( +
ep
inep
hrin
e)
in 2
0 m
l
Aver
age
Num
eric
Ra
ting
Scal
e AU
C 0 –
72 h
Not r
epor
ted
> 0
.05
++
++
++
Stud
y fu
ndin
g; a
utho
r co
mpa
ny e
mpl
oyee
NC
T004
8543
3; p
hase
II d
ose –
re-
spon
se s
tudy
; lip
osom
al
bupi
vaca
ine
306
mg
treat
men
t ar
m w
ith d
ose
grea
ter t
han
Food
and
Dru
g Ad
min
istra
-tio
n – ap
prov
ed m
axim
um o
f 26
6 m
g
Berg
ese 23
(Con
tinue
d )
ALNV134N2_Text.indb 292ALNV134N2_Text.indb 292 29-Dec-20 19:44:1729-Dec-20 19:44:17
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
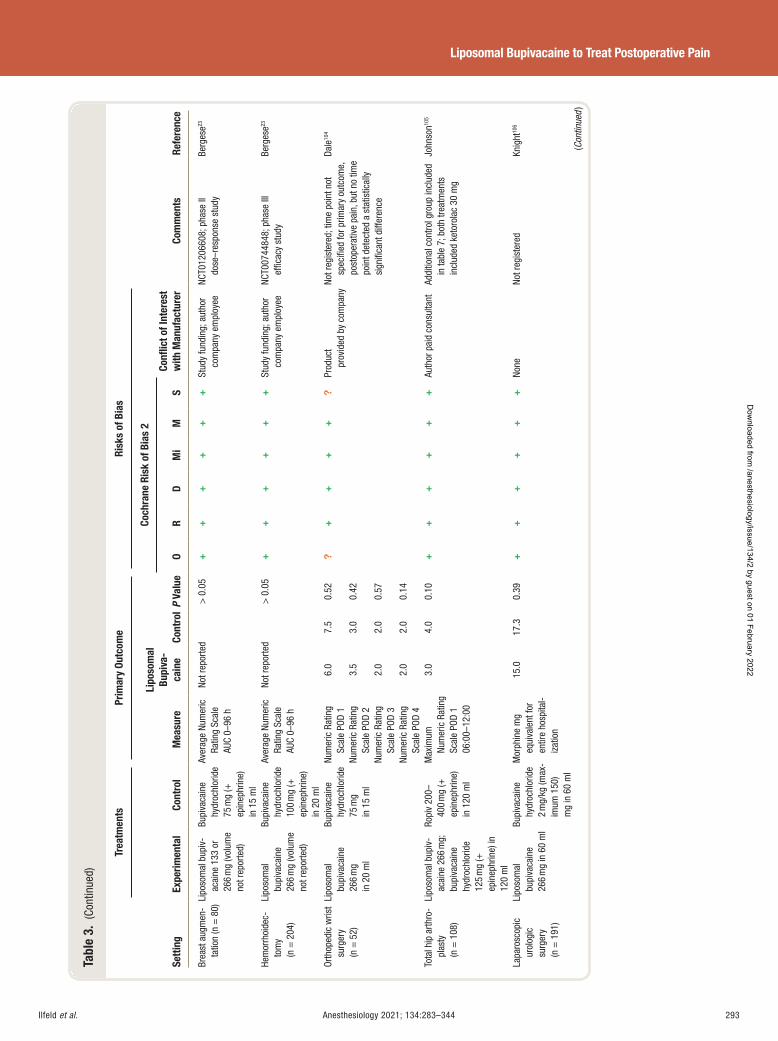
Ilfeld et al. Anesthesiology 2021; 134:283–344 293
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 3.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
va-
cain
e Co
ntro
l P
Valu
e
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f Int
eres
t w
ith M
anuf
actu
rer
O R
D M
i M
S
Brea
st a
ugm
en-
tatio
n (n
= 8
0) Li
poso
mal
bup
iv-
acai
ne 1
33 o
r 26
6 m
g (v
olum
e no
t rep
orte
d)
Bupi
vaca
ine
hydr
ochl
orid
e 75
mg
( +
epin
ephr
ine)
in
15
ml
Aver
age
Num
eric
Ra
ting
Scal
e AU
C 0 –
96 h
Not r
epor
ted
> 0
.05
++
++
++
Stud
y fu
ndin
g; a
utho
r co
mpa
ny e
mpl
oyee
NC
T012
0660
8; p
hase
II
dose
– res
pons
e st
udy
Berg
ese 23
Hem
orrh
oide
c-to
my
(n =
204
)
Lipo
som
al
bupi
vaca
ine
266
mg
(vol
ume
not r
epor
ted)
Bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g ( +
ep
inep
hrin
e)
in 2
0 m
l
Aver
age
Num
eric
Ra
ting
Scal
e AU
C 0 –
96 h
Not r
epor
ted
> 0
.05
++
++
++
Stud
y fu
ndin
g; a
utho
r co
mpa
ny e
mpl
oyee
NC
T007
4484
8; p
hase
III
effi c
acy
stud
y Be
rges
e 23
Orth
oped
ic w
rist
surg
ery
(n =
52)
Lipo
som
al
bupi
vaca
ine
266
mg
in 2
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 75
mg
in 1
5 m
l
Num
eric
Rat
ing
Scal
e PO
D 1
6.0
7.5
0.52
?+
++
+?
Prod
uct
prov
ided
by
com
pany
Not r
egis
tere
d; ti
me
poin
t not
sp
ecifi
ed fo
r prim
ary
outc
ome,
po
stop
erat
ive
pain
, but
no
time
poin
t det
ecte
d a
stat
istic
ally
si
gnifi
cant
diff
eren
ce
Dale
104
Num
eric
Rat
ing
Scal
e PO
D 2
3.5
3.0
0.42
Num
eric
Rat
ing
Scal
e PO
D 3
2.0
2.0
0.57
Num
eric
Rat
ing
Scal
e PO
D 4
2.0
2.0
0.14
Tota
l hip
arth
ro-
plas
ty
(n =
108
)
Lipo
som
al b
upiv
-ac
aine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide
125
mg
( +
epin
ephr
ine)
in
120
ml
Ropi
v 20
0 – 40
0 m
g ( +
ep
inep
hrin
e)
in 1
20 m
l
Max
imum
Nu
mer
ic R
atin
g Sc
ale
POD
1 06
:00 –
12:0
0
3.0
4.0
0.10
+
++
++
+ Au
thor
pai
d co
nsul
tant
Ad
ditio
nal c
ontro
l gro
up in
clud
ed
in ta
ble
7 ; b
oth
treat
men
ts
incl
uded
ket
orol
ac 3
0 m
g
John
son 10
5
Lapa
rosc
opic
ur
olog
ic
surg
ery
(n =
191
)
Lipo
som
al
bupi
vaca
ine
266
mg
in 6
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 2
mg/
kg (m
ax-
imum
150
) m
g in
60
ml
Mor
phin
e m
g eq
uiva
lent
for
entir
e ho
spita
l-iz
atio
n
15.0
17
.3
0.39
+
++
++
+ No
ne
Not r
egis
tere
d Kn
ight
106
(Con
tinue
d )
ALNV134N2_Text.indb 293ALNV134N2_Text.indb 293 29-Dec-20 19:44:1729-Dec-20 19:44:17
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
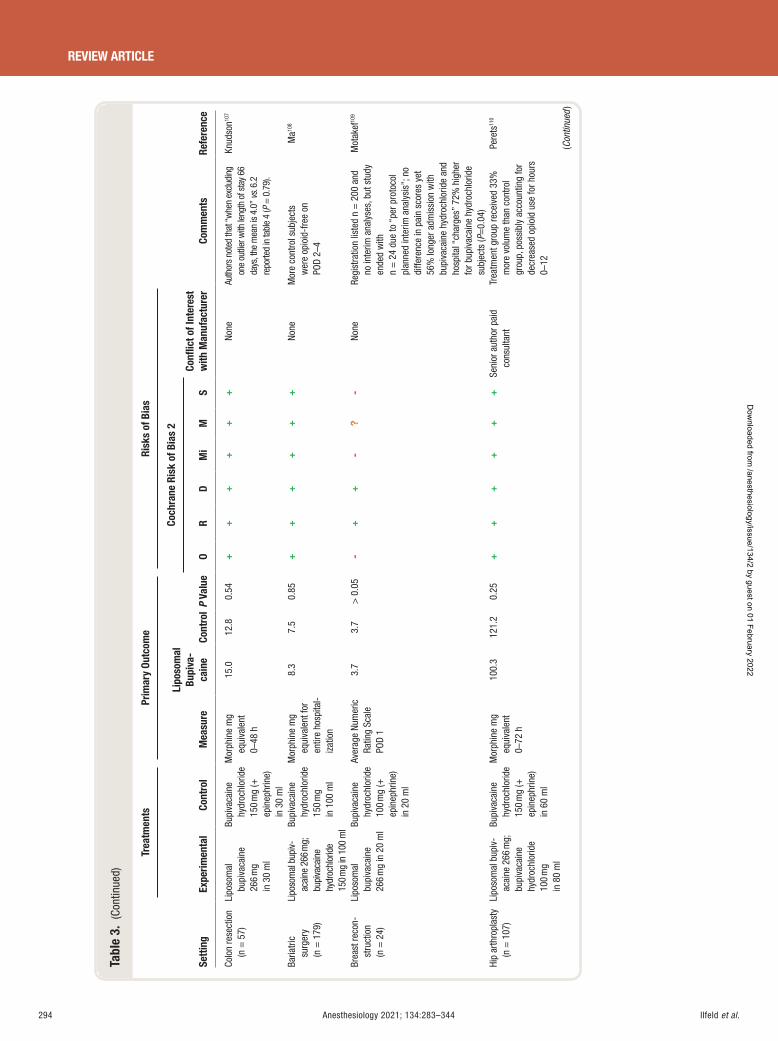
Ilfeld et al.294 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 3.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
va-
cain
e Co
ntro
l P
Valu
e
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f Int
eres
t w
ith M
anuf
actu
rer
O R
D M
i M
S
Colo
n re
sect
ion
(n =
57)
Li
poso
mal
bu
piva
cain
e 26
6 m
g in
30
ml
Bupi
vaca
ine
hydr
ochl
orid
e 15
0 m
g ( +
ep
inep
hrin
e)
in 3
0 m
l
Mor
phin
e m
g eq
uiva
lent
0 –
48 h
15.0
12
.8
0.54
+
++
++
+ No
ne
Auth
ors
note
d th
at “ w
hen
exclu
ding
on
e ou
tlier
with
leng
th o
f sta
y 66
da
ys, t
he m
ean
is 4.
0 ” vs
. 6.2
re
porte
d in
tabl
e 4
( P =
0.7
9).
Knud
son 10
7
Baria
tric
surg
ery
(n =
179
)
Lipo
som
al b
upiv-
acai
ne 2
66 m
g;
bupi
vaca
ine
hydr
ochl
orid
e 15
0 mg
in 1
00 m
l Bupi
vaca
ine
hydr
ochl
orid
e 15
0 m
g in
100
ml
Mor
phin
e m
g eq
uiva
lent
for
entir
e ho
spita
l-iz
atio
n
8.3
7.5
0.85
+
++
++
+ No
ne
Mor
e co
ntro
l sub
ject
s w
ere
opio
id-f
ree
on
POD
2 – 4
Ma 10
8
Brea
st re
con-
stru
ctio
n (n
= 2
4)
Lipo
som
al
bupi
vaca
ine
266
mg
in 2
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g ( +
ep
inep
hrin
e)
in 2
0 m
l
Aver
age
Num
eric
Ra
ting
Scal
e PO
D 1
3.7
3.7
> 0
.05
-+
+-
?-
None
Re
gist
ratio
n lis
ted
n =
200
and
no
inte
rim a
naly
ses,
but
stu
dy
ende
d w
ith
n =
24
due
to “
per p
roto
col
plan
ned
inte
rim a
naly
sis ”
; no
diffe
renc
e in
pai
n sc
ores
yet
56
% lo
nger
adm
issi
on w
ith
bupi
vaca
ine
hydr
ochl
orid
e an
d ho
spita
l “ ch
arge
s ” 7
2% h
ighe
r fo
r bup
ivac
aine
hyd
roch
lorid
e su
bjec
ts ( P
=0.0
4)
Mot
akef
109
Hip
arth
ropl
asty
(n
= 1
07)
Lipo
som
al b
upiv
-ac
aine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide
100
mg
in 8
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 15
0 m
g ( +
ep
inep
hrin
e)
in 6
0 m
l
Mor
phin
e m
g eq
uiva
lent
0 –
72 h
100.
3 12
1.2
0.25
+
++
++
+ Se
nior
aut
hor p
aid
cons
ulta
nt
Trea
tmen
t gro
up re
ceiv
ed 3
3%
mor
e vo
lum
e th
an c
ontro
l gr
oup,
pos
sibl
y ac
coun
ting
for
decr
ease
d op
ioid
use
for h
ours
0 –
12
Pere
ts 11
0
(Con
tinue
d )
ALNV134N2_Text.indb 294ALNV134N2_Text.indb 294 29-Dec-20 19:44:1829-Dec-20 19:44:18
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
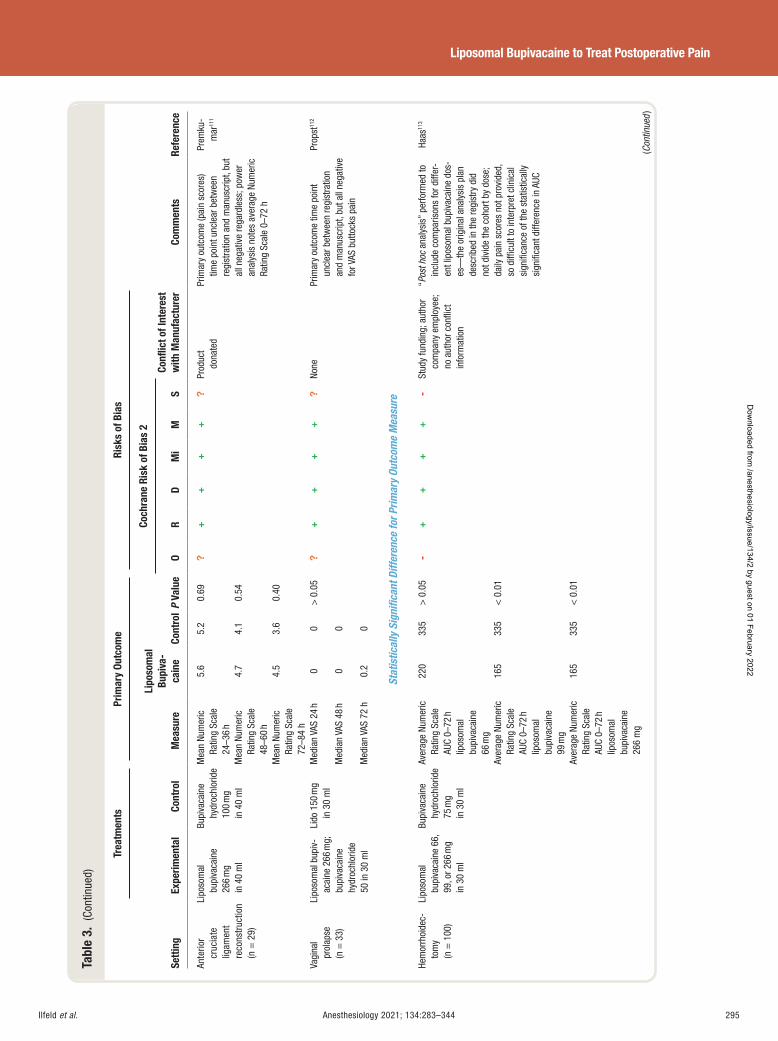
Ilfeld et al. Anesthesiology 2021; 134:283–344 295
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 3.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
va-
cain
e Co
ntro
l P
Valu
e
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f Int
eres
t w
ith M
anuf
actu
rer
O R
D M
i M
S
Ante
rior
cruc
iate
lig
amen
t re
cons
truc
tion
(n =
29)
Lipo
som
al
bupi
vaca
ine
266
mg
in 4
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g in
40
ml
Mea
n Nu
mer
ic
Ratin
g Sc
ale
24 – 3
6 h
5.6
5.2
0.69
?+
++
+?
Prod
uct
dona
ted
Prim
ary
outc
ome
(pai
n sc
ores
) tim
e po
int u
ncle
ar b
etw
een
regi
stra
tion
and
man
uscr
ipt,
but
all n
egat
ive
rega
rdle
ss; p
ower
an
alys
is n
otes
ave
rage
Num
eric
Ra
ting
Scal
e 0 –
72 h
Prem
ku-
mar
111
Mea
n Nu
mer
ic
Ratin
g Sc
ale
48 – 6
0 h
4.7
4.1
0.54
Mea
n Nu
mer
ic
Ratin
g Sc
ale
72 – 8
4 h
4.5
3.6
0.40
Vagi
nal
prol
apse
(n
= 3
3)
Lipo
som
al b
upiv
-ac
aine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide
50 in
30
ml
Lido
150
mg
in 3
0 m
l M
edia
n VA
S 24
h
0 0
> 0
.05
? +
++
+?
None
Pr
imar
y ou
tcom
e tim
e po
int
uncl
ear b
etw
een
regi
stra
tion
and
man
uscr
ipt,
but a
ll ne
gativ
e fo
r VAS
but
tock
s pa
in
Prop
st 11
2
Med
ian
VAS
48 h
0
0
Med
ian
VAS
72 h
0.
2 0
Stat
istic
ally
Sig
nifi c
ant D
iffer
ence
for P
rimar
y Ou
tcom
e M
easu
re
Hem
orrh
oide
c-to
my
(n =
100
)
Lipo
som
al
bupi
vaca
ine
66,
99, o
r 266
mg
in 3
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 75
mg
in 3
0 m
l
Aver
age
Num
eric
Ra
ting
Scal
e AU
C 0 –
72 h
lip
osom
al
bupi
vaca
ine
66 m
g
220
335
> 0
.05
-+
++
+-
Stud
y fu
ndin
g; a
utho
r co
mpa
ny e
mpl
oyee
; no
aut
hor c
onfl i
ct
info
rmat
ion
“ Pos
t hoc
ana
lysi
s ” p
erfo
rmed
to
incl
ude
com
paris
ons
for d
iffer
-en
t lip
osom
al b
upiv
acai
ne d
os-
es —
the
orig
inal
ana
lysi
s pl
an
desc
ribed
in th
e re
gist
ry d
id
not d
ivid
e th
e co
hort
by d
ose;
da
ily p
ain
scor
es n
ot p
rovi
ded,
so
diffi
cul
t to
inte
rpre
t clin
ical
si
gnifi
canc
e of
the
stat
istic
ally
si
gnifi
cant
diff
eren
ce in
AUC
Haas
113
Aver
age
Num
eric
Ra
ting
Scal
e AU
C 0 –
72 h
lip
osom
al
bupi
vaca
ine
99 m
g
165
335
< 0
.01
Aver
age
Num
eric
Ra
ting
Scal
e AU
C 0 –
72 h
lip
osom
al
bupi
vaca
ine
266
mg
165
335
< 0
.01
(Con
tinue
d )
ALNV134N2_Text.indb 295ALNV134N2_Text.indb 295 29-Dec-20 19:44:1829-Dec-20 19:44:18
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
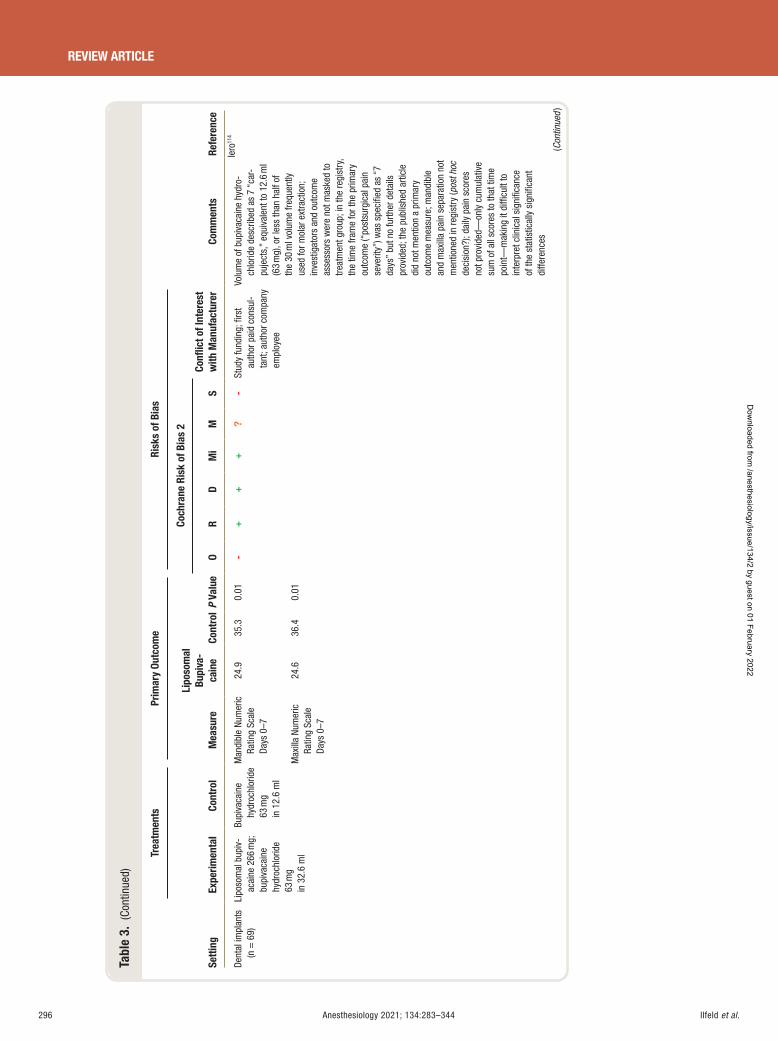
Ilfeld et al.296 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 3.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
va-
cain
e Co
ntro
l P
Valu
e
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f Int
eres
t w
ith M
anuf
actu
rer
O R
D M
i M
S
Dent
al im
plan
ts
(n =
69)
Li
poso
mal
bup
iv-
acai
ne 2
66 m
g;
bupi
vaca
ine
hydr
ochl
orid
e 63
mg
in 3
2.6
ml
Bupi
vaca
ine
hydr
ochl
orid
e 63
mg
in 1
2.6
ml
Man
dibl
e Nu
mer
ic
Ratin
g Sc
ale
Days
0 – 7
24.9
35.3
0.01
-+
++
?-
Stud
y fu
ndin
g; fi
rst
auth
or p
aid
cons
ul-
tant
; aut
hor c
ompa
ny
empl
oyee
Volu
me
of b
upiv
acai
ne h
ydro
-ch
lorid
e de
scrib
ed a
s 7
“ car
-pu
ject
s, ”
equi
vale
nt to
12.
6 m
l (6
3 m
g), o
r les
s th
an h
alf o
f th
e 30
ml v
olum
e fre
quen
tly
used
for m
olar
ext
ract
ion;
in
vest
igat
ors
and
outc
ome
asse
ssor
s w
ere
not m
aske
d to
tre
atm
ent g
roup
; in
the
regi
stry
, th
e tim
e fra
me
for t
he p
rimar
y ou
tcom
e ( “
post
surg
ical
pai
n se
verit
y ” ) w
as s
peci
fi ed
as “
7 da
ys ”
but n
o fu
rther
det
ails
pr
ovid
ed; t
he p
ublis
hed
artic
le
did
not m
entio
n a
prim
ary
outc
ome
mea
sure
; man
dibl
e an
d m
axill
a pa
in s
epar
atio
n no
t m
entio
ned
in re
gist
ry ( p
ost h
oc
deci
sion
?); d
aily
pai
n sc
ores
no
t pro
vide
d — on
ly c
umul
ativ
e su
m o
f all
scor
es to
that
tim
e po
int —
mak
ing
it di
ffi cu
lt to
in
terp
ret c
linic
al s
igni
fi can
ce
of th
e st
atis
tical
ly s
igni
fi can
t di
ffere
nces
Iero
114
Max
illa
Num
eric
Ra
ting
Scal
e Da
ys 0
– 7
24.6
36
.4
0.01
(Con
tinue
d )
ALNV134N2_Text.indb 296ALNV134N2_Text.indb 296 29-Dec-20 19:44:1829-Dec-20 19:44:18
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
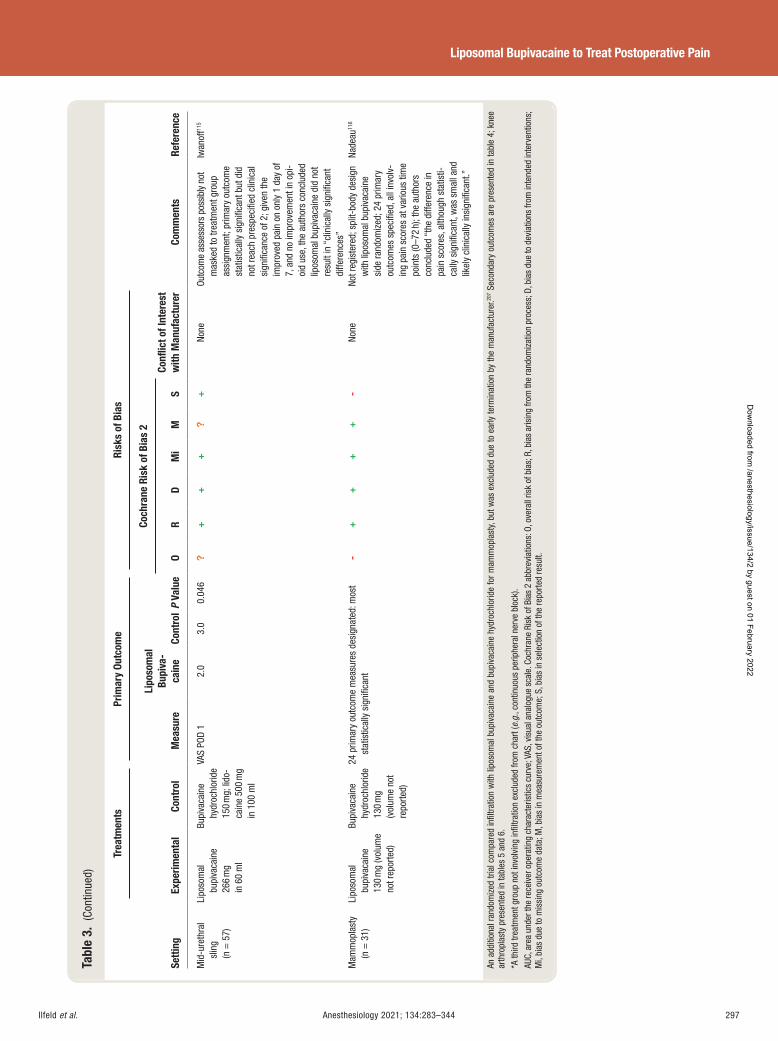
Ilfeld et al. Anesthesiology 2021; 134:283–344 297
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 3.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
va-
cain
e Co
ntro
l P
Valu
e
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f Int
eres
t w
ith M
anuf
actu
rer
O R
D M
i M
S
Mid
-ure
thra
l sl
ing
(n =
57)
Lipo
som
al
bupi
vaca
ine
266
mg
in 6
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 15
0 m
g; li
do-
cain
e 50
0 m
g in
100
ml
VAS
POD
1 2.
0 3.
0 0.
046
?+
++
?+
None
Ou
tcom
e as
sess
ors
poss
ibly
not
m
aske
d to
trea
tmen
t gro
up
assi
gnm
ent;
prim
ary
outc
ome
stat
istic
ally
sig
nifi c
ant b
ut d
id
not r
each
pre
spec
ifi ed
clin
ical
si
gnifi
canc
e of
2; g
iven
the
impr
oved
pai
n on
onl
y 1
day
of
7, a
nd n
o im
prov
emen
t in
opi-
oid
use,
the
auth
ors
conc
lude
d lip
osom
al b
upiv
acai
ne d
id n
ot
resu
lt in
“ cl
inic
ally
sig
nifi c
ant
diffe
renc
es ”
Iwan
off 11
5
Mam
mop
last
y
(n =
31)
Li
poso
mal
bu
piva
cain
e 13
0 m
g (v
olum
e no
t rep
orte
d)
Bupi
vaca
ine
hydr
ochl
orid
e 13
0 m
g (v
olum
e no
t re
porte
d)
24 p
rimar
y ou
tcom
e m
easu
res
desi
gnat
ed: m
ost
stat
istic
ally
sig
nifi c
ant
-+
++
+-
None
No
t reg
iste
red;
spl
it-bo
dy d
esig
n w
ith li
poso
mal
bup
ivac
aine
si
de ra
ndom
ized
; 24
prim
ary
outc
omes
spe
cifi e
d, a
ll in
volv
-in
g pa
in s
core
s at
var
ious
tim
e po
ints
(0 – 7
2 h)
; the
aut
hors
co
nclu
ded
“ the
diff
eren
ce in
pa
in s
core
s, a
lthou
gh s
tatis
ti-ca
lly s
igni
fi can
t, w
as s
mal
l and
lik
ely
clin
ical
ly in
sign
ifi ca
nt. ”
Nade
au 11
6
An a
dditi
onal
rand
omiz
ed tr
ial c
ompa
red
infi l
tratio
n w
ith li
poso
mal
bup
ivac
aine
and
bup
ivac
aine
hyd
roch
lorid
e fo
r mam
mop
last
y, bu
t was
exc
lude
d du
e to
ear
ly te
rmin
atio
n by
the
man
ufac
ture
r. 207 S
econ
dary
out
com
es a
re p
rese
nted
in ta
ble
4 ; k
nee
arth
ropl
asty
pre
sent
ed in
tabl
es 5
and
6 .
* A th
ird tr
eatm
ent g
roup
not
invo
lvin
g in
fi ltra
tion
excl
uded
from
cha
rt ( e
.g. ,
cont
inuo
us p
erip
hera
l ner
ve b
lock
). AU
C, a
rea
unde
r the
rece
iver
ope
ratin
g ch
arac
teris
tics
curv
e; V
AS, v
isua
l ana
logu
e sc
ale.
Coc
hran
e Ri
sk o
f Bia
s 2
abbr
evia
tions
: O, o
vera
ll ris
k of
bia
s; R
, bia
s ar
isin
g fro
m th
e ra
ndom
izat
ion
proc
ess;
D, b
ias
due
to d
evia
tions
from
inte
nded
inte
rven
tions
; M
i, bi
as d
ue to
mis
sing
out
com
e da
ta; M
, bia
s in
mea
sure
men
t of t
he o
utco
me;
S, b
ias
in s
elec
tion
of th
e re
porte
d re
sult.
ALNV134N2_Text.indb 297ALNV134N2_Text.indb 297 29-Dec-20 19:44:1829-Dec-20 19:44:18
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
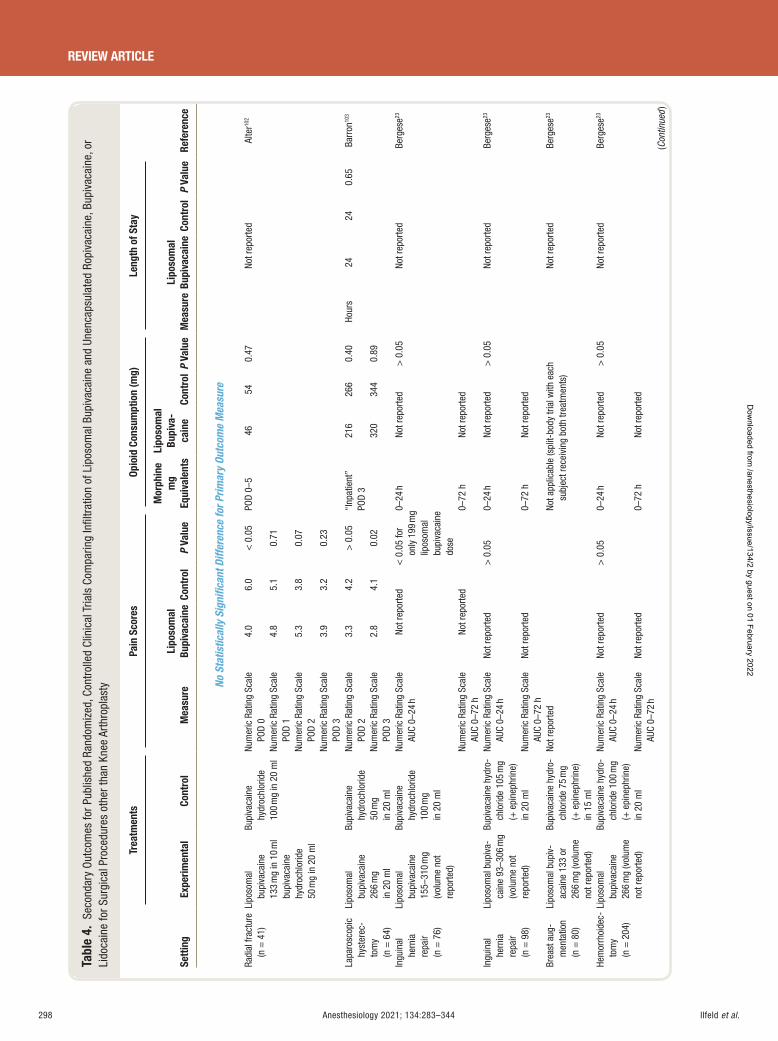
Ilfeld et al.298 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 4.
Sec
onda
ry O
utco
mes
for P
ublis
hed
Rand
omiz
ed, C
ontr
olle
d Cl
inic
al T
rials
Com
parin
g In
fi ltr
atio
n of
Lip
osom
al B
upiv
acai
ne a
nd U
nenc
apsu
late
d Ro
piva
cain
e, B
upiv
acai
ne, o
r Li
doca
ine
for S
urgi
cal P
roce
dure
s ot
her t
han
Knee
Art
hrop
last
y
Setti
ng
Trea
tmen
ts
Pain
Sco
res
Opio
id C
onsu
mpt
ion
(mg)
Le
ngth
of S
tay
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mor
phin
e m
g Eq
uiva
lent
s
Lipo
som
al
Bupi
va-
cain
e Co
ntro
l P
Valu
e M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
No S
tatis
tical
ly S
igni
fi can
t Diff
eren
ce fo
r Prim
ary
Outc
ome
Mea
sure
Radi
al fr
actu
re
(n =
41)
Li
poso
mal
bu
piva
cain
e 13
3 m
g in
10
ml
bupi
vaca
ine
hydr
ochl
orid
e 50
mg
in 2
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g in
20
ml
Num
eric
Rat
ing
Scal
e PO
D 0
4.0
6.0
< 0
.05
POD
0 – 5
46
54
0.47
No
t rep
orte
d Al
ter 10
2
Num
eric
Rat
ing
Scal
e PO
D 1
4.8
5.1
0.71
Num
eric
Rat
ing
Scal
e PO
D 2
5.3
3.8
0.07
Num
eric
Rat
ing
Scal
e PO
D 3
3.9
3.2
0.23
Lapa
rosc
opic
hy
ster
ec-
tom
y (n
= 6
4)
Lipo
som
al
bupi
vaca
ine
266
mg
in 2
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 50
mg
in 2
0 m
l
Num
eric
Rat
ing
Scal
e PO
D 2
3.3
4.2
> 0
.05
“ Inp
atie
nt ”
POD
3 21
6 26
6 0.
40 Ho
urs
24
24
0.65
Ba
rron
103
Num
eric
Rat
ing
Scal
e PO
D 3
2.8
4.1
0.02
32
0 34
4 0.
89
Ingu
inal
he
rnia
re
pair
(n =
76)
Lipo
som
al
bupi
vaca
ine
155 –
310
mg
(vol
ume
not
repo
rted)
Bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g
in 2
0 m
l
Num
eric
Rat
ing
Scal
e AU
C 0 –
24 h
No
t rep
orte
d <
0.0
5 fo
r on
ly 1
99 m
g lip
osom
al
bupi
vaca
ine
dose
0 – 24
h No
t rep
orte
d >
0.0
5 No
t rep
orte
d Be
rges
e 23
Num
eric
Rat
ing
Scal
e AU
C 0 –
72 h
No
t rep
orte
d 0 –
72 h
No
t rep
orte
d
Ingu
inal
he
rnia
re
pair
(n =
98)
Lipo
som
al b
upiv
a-ca
ine
93 – 3
06 m
g (v
olum
e no
t re
porte
d)
Bupi
vaca
ine
hydr
o-ch
lorid
e 10
5 m
g ( +
epi
neph
rine)
in
20
ml
Num
eric
Rat
ing
Scal
e AU
C 0 –
24 h
Not r
epor
ted
> 0
.05
0 – 24
h No
t rep
orte
d >
0.0
5 No
t rep
orte
d Be
rges
e 23
Num
eric
Rat
ing
Scal
e AU
C 0 –
72 h
No
t rep
orte
d 0 –
72 h
No
t rep
orte
d
Brea
st a
ug-
men
tatio
n (n
= 8
0)
Lipo
som
al b
upiv
-ac
aine
133
or
266
mg
(vol
ume
not r
epor
ted)
Bupi
vaca
ine
hydr
o-ch
lorid
e 75
mg
( + e
pine
phrin
e)
in 1
5 m
l
Not r
epor
ted
Not a
pplic
able
(spl
it-bo
dy tr
ial w
ith e
ach
subj
ect r
ecei
ving
bot
h tre
atm
ents
) No
t rep
orte
d Be
rges
e 23
Hem
orrh
oide
c-to
my
(n =
204
)
Lipo
som
al
bupi
vaca
ine
266
mg
(vol
ume
not r
epor
ted)
Bupi
vaca
ine
hydr
o-ch
lorid
e 10
0 m
g ( +
epi
neph
rine)
in
20
ml
Num
eric
Rat
ing
Scal
e AU
C 0 –
24 h
Not r
epor
ted
> 0
.05
0 – 24
h No
t rep
orte
d >
0.0
5 No
t rep
orte
d Be
rges
e 23
Num
eric
Rat
ing
Scal
e AU
C 0 –
72 h
No
t rep
orte
d 0 –
72 h
No
t rep
orte
d
(Con
tinue
d )
ALNV134N2_Text.indb 298ALNV134N2_Text.indb 298 29-Dec-20 19:44:1829-Dec-20 19:44:18
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
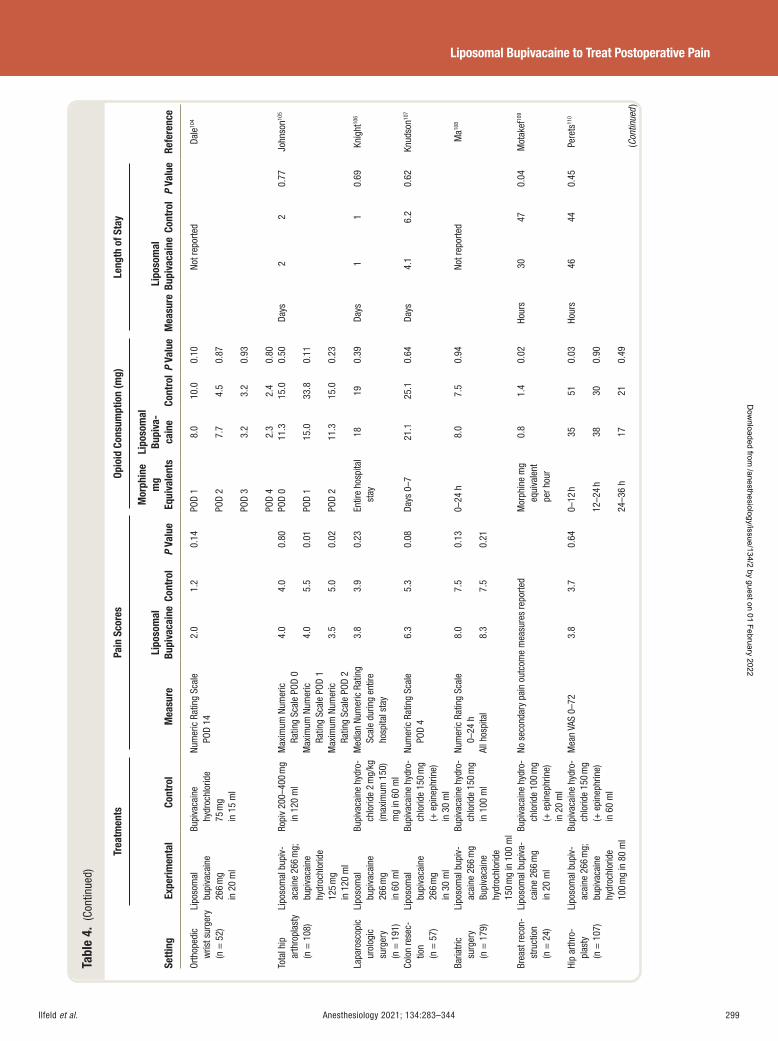
Ilfeld et al. Anesthesiology 2021; 134:283–344 299
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 4.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Pain
Sco
res
Opio
id C
onsu
mpt
ion
(mg)
Le
ngth
of S
tay
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mor
phin
e m
g Eq
uiva
lent
s
Lipo
som
al
Bupi
va-
cain
e Co
ntro
l P
Valu
e M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Orth
oped
ic
wris
t sur
gery
(n
= 5
2)
Lipo
som
al
bupi
vaca
ine
266
mg
in 2
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 75
mg
in 1
5 m
l
Num
eric
Rat
ing
Scal
e PO
D 14
2.
0 1.
2 0.
14
POD
1 8.
0 10
.0 0.
10 No
t rep
orte
d Da
le 10
4
POD
2 7.
7 4.
5 0.
87
POD
3 3.
2 3.
2 0.
93
POD
4 2.
3 2.
4 0.
80
Tota
l hip
ar
thro
plas
ty
(n =
108
)
Lipo
som
al b
upiv
-ac
aine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide
125
mg
in 1
20 m
l
Ropi
v 20
0 – 40
0 m
g in
120
ml
Max
imum
Num
eric
Ra
ting
Scal
e PO
D 0
4.0
4.0
0.80
POD
0 11
.3 15
.0 0.
50 Da
ys
2 2
0.77
Jo
hnso
n 105
Max
imum
Num
eric
Ra
ting
Scal
e PO
D 1
4.0
5.5
0.01
POD
1 15
.0 33
.8 0.
11
Max
imum
Num
eric
Ra
ting
Scal
e PO
D 2
3.5
5.0
0.02
PO
D 2
11.3
15
.0
0.23
Lapa
rosc
opic
ur
olog
ic
surg
ery
(n =
191
)
Lipo
som
al
bupi
vaca
ine
266
mg
in 6
0 m
l
Bupi
vaca
ine
hydr
o-ch
lorid
e 2
mg/
kg
(max
imum
150
) m
g in
60
ml
Med
ian
Num
eric
Rat
ing
Scal
e du
ring
entir
e ho
spita
l sta
y
3.8
3.9
0.23
En
tire
hosp
ital
stay
18
19
0.
39
Days
1
1 0.
69
Knig
ht 10
6
Colo
n re
sec-
tion
(n =
57)
Lipo
som
al
bupi
vaca
ine
266
mg
in 3
0 m
l
Bupi
vaca
ine
hydr
o-ch
lorid
e 15
0 m
g ( +
epi
neph
rine)
in
30
ml
Num
eric
Rat
ing
Scal
e PO
D 4
6.3
5.3
0.08
Da
ys 0
– 7
21.1
25
.1
0.64
Da
ys
4.1
6.2
0.62
Kn
udso
n 107
Baria
tric
surg
ery
(n =
179
)
Lipo
som
al b
upiv
-ac
aine
266
mg
Bupi
vaca
ine
hydr
ochl
orid
e 15
0 m
g in
100
ml Bu
piva
cain
e hy
dro-
chlo
ride
150
mg
in 1
00 m
l
Num
eric
Rat
ing
Scal
e 0 –
24 h
8.
0 7.
5 0.
13
0 – 24
h
8.0
7.5
0.94
No
t rep
orte
d M
a 108
All h
ospi
tal
8.3
7.5
0.21
Brea
st re
con-
stru
ctio
n (n
= 2
4)
Lipo
som
al b
upiv
a-ca
ine
266
mg
in 2
0 m
l
Bupi
vaca
ine
hydr
o-ch
lorid
e 10
0 m
g ( +
epi
neph
rine)
in
20
ml
No s
econ
dary
pai
n ou
tcom
e m
easu
res
repo
rted
Mor
phin
e m
g eq
uiva
lent
pe
r hou
r
0.8
1.4
0.02
Ho
urs
30
47
0.04
M
otak
ef 10
9
Hip
arth
ro-
plas
ty
(n =
107
)
Lipo
som
al b
upiv
-ac
aine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide
100
mg
in 8
0 m
l
Bupi
vaca
ine
hydr
o-ch
lorid
e 15
0 m
g ( +
epi
neph
rine)
in
60
ml
Mea
n VA
S 0 –
72
3.8
3.7
0.64
0 –
12 h
35 51
0.03
Hour
s 46
44
0.
45
Pere
ts 11
0
12 – 2
4 h
38 30
0.90
24 – 3
6 h
17
21
0.49
(C
ontin
ued )
ALNV134N2_Text.indb 299ALNV134N2_Text.indb 299 29-Dec-20 19:44:1829-Dec-20 19:44:18
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
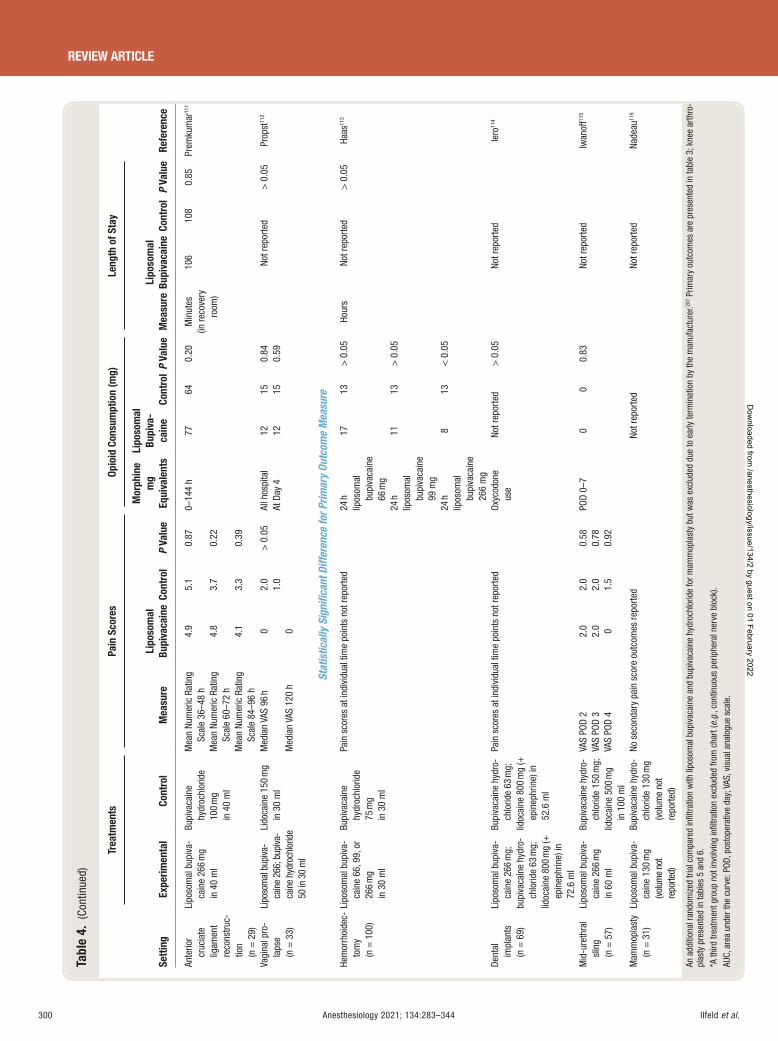
Ilfeld et al.300 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 4.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Pain
Sco
res
Opio
id C
onsu
mpt
ion
(mg)
Le
ngth
of S
tay
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mor
phin
e m
g Eq
uiva
lent
s
Lipo
som
al
Bupi
va-
cain
e Co
ntro
l P
Valu
e M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Ante
rior
cruc
iate
lig
amen
t re
cons
truc-
tion
(n =
29)
Lipo
som
al b
upiv
a-ca
ine
266
mg
in 4
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g in
40
ml
Mea
n Nu
mer
ic R
atin
g Sc
ale
36 – 4
8 h
4.9
5.1
0.87
0 – 14
4 h
77
64
0.20
M
inut
es (in
reco
very
ro
om)
106
108
0.85
Pr
emku
mar
111
Mea
n Nu
mer
ic R
atin
g Sc
ale
60 – 7
2 h
4.8
3.7
0.22
Mea
n Nu
mer
ic R
atin
g Sc
ale
84 – 9
6 h
4.1
3.3
0.39
Vagi
nal p
ro-
laps
e (n
= 3
3)
Lipo
som
al b
upiva
-ca
ine
266;
bup
iva-
cain
e hy
droc
hlor
ide
50 in
30
ml
Lido
cain
e 15
0 m
g in
30
ml
Med
ian
VAS
96 h
0
2.0
1.0
> 0
.05
All h
ospi
tal
At D
ay 4
12 12
15 15
0.
84 0.
59
Not r
epor
ted
> 0
.05
Prop
st 11
2
Med
ian
VAS
120
h 0
Stat
istic
ally
Sig
nifi c
ant D
iffer
ence
for P
rimar
y Ou
tcom
e M
easu
re
Hem
orrh
oide
c-to
my
(n =
100
)
Lipo
som
al b
upiv
a-ca
ine
66, 9
9, o
r 26
6 m
g in
30
ml
Bupi
vaca
ine
hydr
ochl
orid
e 75
mg
in 3
0 m
l
Pain
sco
res
at in
divi
dual
tim
e po
ints
not
repo
rted
24 h
lipos
omal
bu
piva
cain
e 66
mg
17 13
> 0
.05
Hour
s No
t rep
orte
d >
0.0
5 Ha
as 11
3
24 h
lipos
omal
bu
piva
cain
e 99
mg
11 13
> 0
.05
24 h
lipos
omal
bu
piva
cain
e 26
6 m
g
8 13
<
0.0
5
Dent
al
impl
ants
(n
= 6
9)
Lipo
som
al b
upiv
a-ca
ine
266
mg;
bu
piva
cain
e hy
dro-
chlo
ride
63 m
g;
lidoc
aine
800
mg
( +
epin
ephr
ine)
in
72.6
ml
Bupi
vaca
ine
hydr
o-ch
lorid
e 63
mg;
lidoc
aine
800
mg
( +
epin
ephr
ine)
in
52.6
ml
Pain
sco
res
at in
divi
dual
tim
e po
ints
not
repo
rted
Oxyc
odon
e us
e No
t rep
orte
d >
0.0
5 No
t rep
orte
d Ie
ro 11
4
Mid
-ure
thra
l sl
ing
(n =
57)
Lipo
som
al b
upiv
a-ca
ine
266
mg
in 6
0 m
l
Bupi
vaca
ine
hydr
o-ch
lorid
e 15
0 m
g;
lidoc
aine
500
mg
in 1
00 m
l
VAS
POD
2 2.
0 2.
0 0.
58
POD
0 – 7
0 0
0.83
No
t rep
orte
d Iw
anof
f 115
VAS
POD
3 2.
0 2.
0 0.
78
VAS
POD
4 0
1.5
0.92
Mam
mop
last
y (n
= 3
1)
Lipo
som
al b
upiv
a-ca
ine
130
mg
(vol
ume
not
repo
rted)
Bupi
vaca
ine
hydr
o-ch
lorid
e 13
0 m
g (v
olum
e no
t re
porte
d)
No s
econ
dary
pai
n sc
ore
outc
omes
repo
rted
Not r
epor
ted
Not r
epor
ted
Nade
au 11
6
An a
dditi
onal
rand
omiz
ed tr
ial c
ompa
red
infi l
tratio
n w
ith li
poso
mal
bup
ivac
aine
and
bup
ivac
aine
hyd
roch
lorid
e fo
r mam
mop
last
y bu
t was
exc
lude
d du
e to
ear
ly te
rmin
atio
n by
the
man
ufac
ture
r. 207 P
rimar
y ou
tcom
es a
re p
rese
nted
in ta
ble
3 ; k
nee
arth
ro-
plas
ty p
rese
nted
in ta
bles
5 a
nd 6
. * A
third
trea
tmen
t gro
up n
ot in
volv
ing
infi l
tratio
n ex
clud
ed fr
om c
hart
( e.g
. , co
ntin
uous
per
iphe
ral n
erve
blo
ck).
AUC,
are
a un
der t
he c
urve
; POD
, pos
tope
rativ
e da
y; V
AS, v
isua
l ana
logu
e sc
ale.
ALNV134N2_Text.indb 300ALNV134N2_Text.indb 300 29-Dec-20 19:44:1829-Dec-20 19:44:18
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Ilfeld et al. Anesthesiology 2021; 134:283–344 301
Liposomal Bupivacaine to Treat Postoperative Pain
Summary
To summarize the evidence for the use of in ltration with liposomal bupivacaine over unencapsulated bupivacaine, of the 19 randomized, active-controlled trials (excluding knee arthroplasty), only two (11%) reported both a statistically and clinically signi cant di erence for their primary out-come measure. 113 , 114 Both of these trials compared the max-imum approved dose of liposomal bupivacaine (266 mg) to submaximal doses of the unencapsulated bupivacaine com-parator. 113 , 114 This discrepancy greatly decreases con dence that the di erence would remain had a maximum dose of both treatments been compared. 113 Furthermore, both trials were rated at high risk of bias for multiple reasons, the most critical being discrepancies between the registry entries and published articles involving the primary outcome measures. Therefore, there is currently no published evidence with a low risk of bias for surgical procedures other than knee arthroplasty demonstrating that in ltration with the max-imum approved liposomal bupivacaine dose is superior to unencapsulated bupivacaine to a statistically and clinically signi cant degree.
Infi ltration with Liposomal Bupivacaine versus an Active Control for Knee Arthroplasty Knee arthroplasty is among the most common and pain-ful surgical procedures, with more than 700,000 performed annually within the United States alone. In ltrating the sur-gical site with local anesthetic is frequently performed by surgeons to provide postoperative analgesia, although the duration of e ect is far less than the duration of surgically related pain.
Of the 17 randomized, active-controlled trials involving knee arthroplasty, 15 (88%) failed to nd a statistically signif-icant di erence for their primary outcome measure ( tables 5 and 6 ). 23 , 31 , 117 – 129 Risk of bias for these 15 trials was deemed low in eight studies 23 , 31 , 119 , 122 – 124 , 126 , 127 and “ some concerns ” in seven trials. 117 , 118 , 120 , 121 , 125 , 128 , 129 Within these studies, di erences between treatments for nearly every secondary endpoint involving pain level, opioid use, physical therapy, or discharge day also failed to reach statistical signi cance. Nearly no statistically signi cant di erences between in ltration with liposomal bupivacaine and unencapsulated bupivacaine after total knee arthroplasty were identi ed. Of the few excep-tions, the unencapsulated local anesthetic control was found superior to liposomal bupivacaine 118 , 126 – 128 more times than vice versa . 119 Multiple investigations were unregistered and/or did not specify a primary outcome measure time point, although the impact of these de ciencies appears minimal with the near-total lack of statistical signi cance between treatments. A unique and illuminating investigation random-ized each side of subjects having bilateral knee arthroplasty (n = 29) to either a combination of liposomal bupivacaine (266 mg) and bupivacaine hydrochloride (75 mg) or ropiv-acaine hydrochloride (250 mg) plus epinephrine, ketorolac,
and clonidine. 121 This split-body study design is especially powerful since it inherently controls for intersubject di er-ences in pain evaluation and supplemental opioid consump-tion between treatment groups (each subject receives both treatments, and therefore each treatment is associated with identical opioid doses). No statistically signi cant or clini-cally relevant (de ned by the authors as greater than 18 mm on the 0 to 100 mm visual analogue scale [VAS]) di erences between treatments were detected, mirroring the vast major-ity of published trials ( tables 5 and 6 ).
In contrast, two of the 17 randomized, controlled tri-als (12%) reported a statistically signi cant di erence for their primary outcome measure(s) between liposomal bupivacaine and unencapsulated local anesthetic. 130 , 131 The rst randomized subjects (n = 70) to either a maximum dose of liposomal bupivacaine (266 mg) or a multicom-ponent injection of ropivacaine (400 mg), ketorolac, mor-phine, and epinephrine. 131 Considering the Food and Drug Administration – recommended maximum dose of ropiva-caine (with epinephrine) is 4 mg/kg up to 225 mg, an opti-mized control group was certainly provided with 400 mg used in this study. Statistically signi cant di erences were identi ed not only for the primary outcome of pain level on postoperative day 1 but also in pain scores within the recovery room and postoperative day 2. Di erences were also detected in opioid consumption in the recovery room and postoperative days 1 and 2, and the risk of bias was evaluated as low using the Cochrane risk-of-bias tool. 98 , 99
The second randomized, controlled trial, the PILLAR trial, randomized subjects (n = 140) to in ltration with either a combination of liposomal (266 mg) and unencapsulated (100 mg) bupivacaine, or solely bupivacaine hydrochloride (100 mg). 130 The results of this investigation were overwhelmingly positive not only for the two coprimary outcomes of pain scores (AUC, 12 to 48 h) and opioid consumption (cumulative, 0 to 48 h), 133
but also for secondary and tertiary endpoints at 24, 48, and 72 h. 130 , 133 , 134 For example, mean total opioid con-sumption in the rst 48 h postsurgery was 16 versus 80 mg for the experimental versus control groups, respectively ( P = 0.0029). 133 More subjects receiving liposomal bupiva-caine remained opioid-free, exhibited a greater amount of time until request for rst opioid rescue, were more satis ed with postoperative analgesia, and met discharge criteria ear-lier than in the control group. 130 , 133 , 134
The authors attribute their dramatically di erent results compared to most other randomized, active-controlled tri-als to their use of a large volume of injectate (120 ml); 135 the “ use of a small-bore (22-gauge), 1.5-inch needle to reduce the leakage of anesthetic solution from the injection site and for achievement of maximal tissue exposure ” 135 – 137 ; and their “ use of a meticulous and standardized in ltra-tion protocol. ” 130 , 138 This protocol entailed the use of six 20-ml syringes of study uid with 94 to 103 separate needle passes/injections. 130 , 135 However, six of the trials that did not
ALNV134N2_Text.indb 301ALNV134N2_Text.indb 301 29-Dec-20 19:44:1929-Dec-20 19:44:19
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
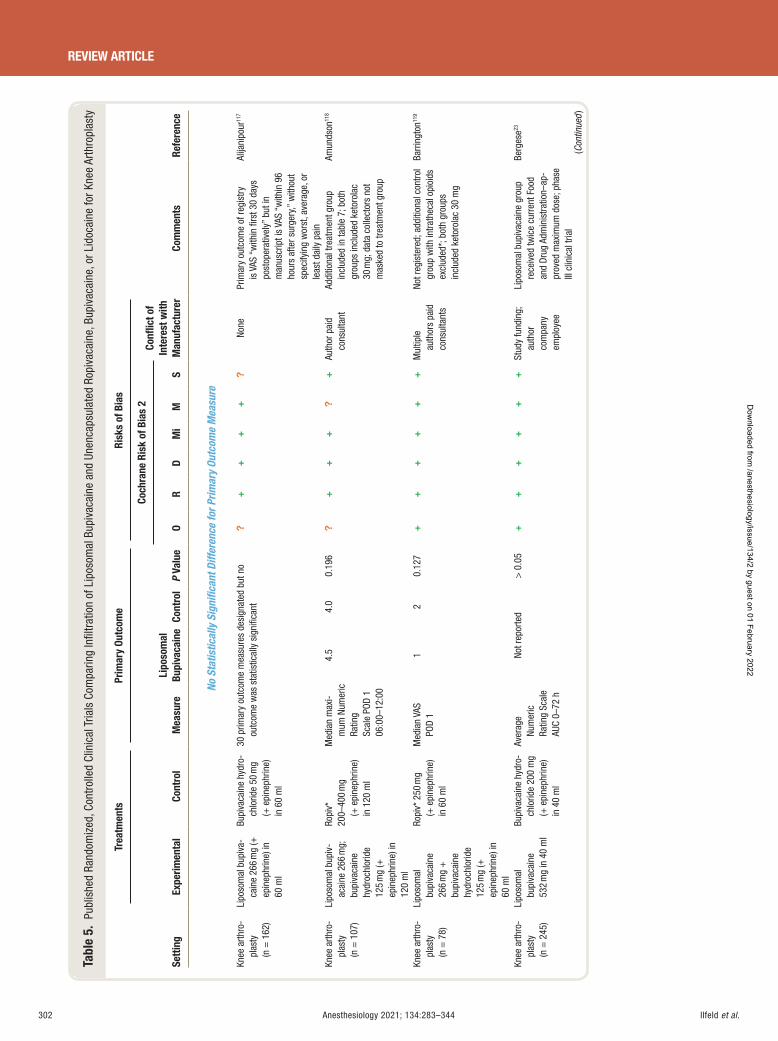
Ilfeld et al.302 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 5.
Pub
lishe
d Ra
ndom
ized
, Con
trol
led
Clin
ical
Tria
ls C
ompa
ring
Infi l
trat
ion
of L
ipos
omal
Bup
ivac
aine
and
Une
ncap
sula
ted
Ropi
vaca
ine,
Bup
ivac
aine
, or L
idoc
aine
for K
nee
Arth
ropl
asty
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f In
tere
st w
ith
Man
ufac
ture
r O
R D
Mi
M
S
No S
tatis
tical
ly S
igni
fi can
t Diff
eren
ce fo
r Prim
ary
Outc
ome
Mea
sure
Knee
arth
ro-
plas
ty
(n =
162
)
Lipo
som
al b
upiv
a-ca
ine
266
mg
( +
epin
ephr
ine)
in
60 m
l
Bupi
vaca
ine
hydr
o-ch
lorid
e 50
mg
( + e
pine
phrin
e)
in 6
0 m
l
30 p
rimar
y ou
tcom
e m
easu
res
desi
gnat
ed b
ut n
o ou
tcom
e w
as s
tatis
tical
ly s
igni
fi can
t ?
++
++
? No
ne
Prim
ary
outc
ome
of re
gist
ry
is V
AS “
with
in fi
rst 3
0 da
ys
post
oper
ativ
ely ”
but
in
man
uscr
ipt i
s VA
S “ w
ithin
96
hour
s af
ter s
urge
ry, ”
with
out
spec
ifyin
g w
orst
, ave
rage
, or
leas
t dai
ly p
ain
Alija
nipo
ur 11
7
Knee
arth
ro-
plas
ty
(n =
107
)
Lipo
som
al b
upiv
-ac
aine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide
125
mg
( +
epin
ephr
ine)
in
120
ml
Ropi
v *
200 –
400
mg
( + e
pine
phrin
e)
in 1
20 m
l
Med
ian
max
i-m
um N
umer
ic
Ratin
g Sc
ale
POD
1 06
:00 –
12:0
0
4.5
4.0
0.19
6 ?
++
+?
+ Au
thor
pai
d co
nsul
tant
Ad
ditio
nal t
reat
men
t gro
up
incl
uded
in ta
ble
7 ; b
oth
grou
ps in
clud
ed k
etor
olac
30
mg;
dat
a co
llect
ors
not
mas
ked
to tr
eatm
ent g
roup
Amun
dson
118
Knee
arth
ro-
plas
ty
(n =
78)
Lipo
som
al
bupi
vaca
ine
266
mg
+
bupi
vaca
ine
hydr
ochl
orid
e 12
5 m
g ( +
ep
inep
hrin
e) in
60
ml
Ropi
v * 2
50 m
g ( +
epi
neph
rine)
in
60
ml
Med
ian
VAS
POD
1 1
2 0.
127
++
++
++
Mul
tiple
au
thor
s pa
id
cons
ulta
nts
Not r
egis
tere
d; a
dditi
onal
con
trol
grou
p w
ith in
trath
ecal
opi
oids
ex
clud
ed * ;
bot
h gr
oups
in
clud
ed k
etor
olac
30
mg
Barr
ingt
on 11
9
Knee
arth
ro-
plas
ty
(n =
245
)
Lipo
som
al
bupi
vaca
ine
532
mg
in 4
0 m
l
Bupi
vaca
ine
hydr
o-ch
lorid
e 20
0 m
g ( +
epi
neph
rine)
in
40
ml
Aver
age
Num
eric
Ra
ting
Scal
e AU
C 0 –
72 h
Not r
epor
ted
> 0
.05
++
++
++
Stud
y fu
ndin
g;
auth
or
com
pany
em
ploy
ee
Lipo
som
al b
upiv
acai
ne g
roup
re
ceiv
ed tw
ice
curr
ent F
ood
and
Drug
Adm
inis
tratio
n – ap
-pr
oved
max
imum
dos
e; p
hase
III
clin
ical
tria
l
Berg
ese 23
(Con
tinue
d )
ALNV134N2_Text.indb 302ALNV134N2_Text.indb 302 29-Dec-20 19:44:1929-Dec-20 19:44:19
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
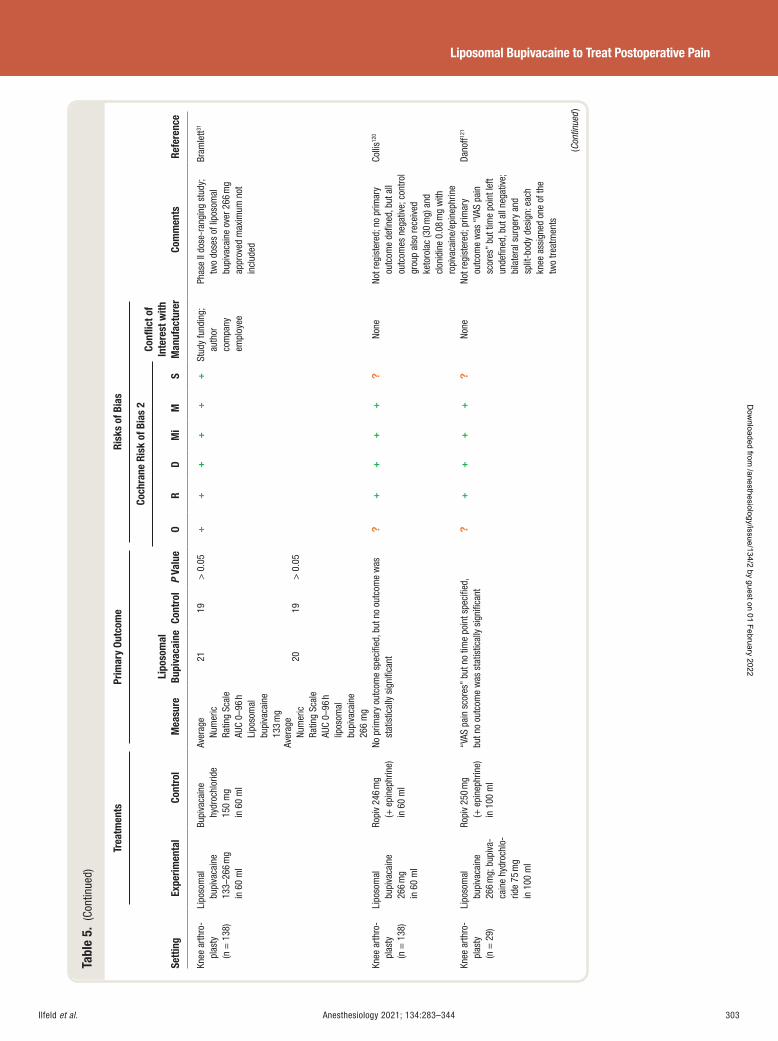
Ilfeld et al. Anesthesiology 2021; 134:283–344 303
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 5.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f In
tere
st w
ith
Man
ufac
ture
r O
R D
Mi
M
S
Knee
arth
ro-
plas
ty
(n =
138
)
Lipo
som
al
bupi
vaca
ine
133 –
266
mg
in 6
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 15
0 m
g in
60
ml
Aver
age
Num
eric
Ra
ting
Scal
e AU
C 0 –
96 h
Li
poso
mal
bu
piva
cain
e 13
3 m
g
21 19
> 0
.05
++
++
++
Stud
y fu
ndin
g;
auth
or
com
pany
em
ploy
ee
Phas
e II
dose
-ran
ging
stu
dy;
two
dose
s of
lipo
som
al
bupi
vaca
ine
over
266
mg
appr
oved
max
imum
not
in
clud
ed
Bram
lett 31
Aver
age
Num
eric
Ra
ting
Scal
e AU
C 0 –
96 h
lip
osom
al
bupi
vaca
ine
266
mg
20
19
> 0
.05
Knee
arth
ro-
plas
ty
(n =
138
)
Lipo
som
al
bupi
vaca
ine
266
mg
in 6
0 m
l
Ropi
v 24
6 m
g ( +
epi
neph
rine)
in
60
ml
No p
rimar
y ou
tcom
e sp
ecifi
ed, b
ut n
o ou
tcom
e w
as
stat
istic
ally
sig
nifi c
ant
?+
++
+?
None
No
t reg
iste
red;
no
prim
ary
outc
ome
defi n
ed, b
ut a
ll ou
tcom
es n
egat
ive;
con
trol
grou
p al
so re
ceiv
ed
keto
rola
c (3
0 m
g) a
nd
clon
idin
e 0.
08 m
g w
ith
ropi
vaca
ine/
epin
ephr
ine
Colli
s 120
Knee
arth
ro-
plas
ty
(n =
29)
Lipo
som
al
bupi
vaca
ine
266
mg;
bup
iva-
cain
e hy
droc
hlo-
ride
75 m
g in
100
ml
Ropi
v 25
0 m
g ( +
epi
neph
rine)
in
100
ml
“ VAS
pai
n sc
ores
” bu
t no
time
poin
t spe
cifi e
d, bu
t no
outc
ome
was
sta
tistic
ally
sig
nifi c
ant
?+
++
+?
None
No
t reg
iste
red;
prim
ary
outc
ome
was
“ VA
S pa
in
scor
es ”
but t
ime
poin
t lef
t un
defi n
ed, b
ut a
ll ne
gativ
e;
bila
tera
l sur
gery
and
sp
lit-b
ody
desi
gn: e
ach
knee
ass
igne
d on
e of
the
two
treat
men
ts
Dano
ff 121
(Con
tinue
d )
ALNV134N2_Text.indb 303ALNV134N2_Text.indb 303 29-Dec-20 19:44:1929-Dec-20 19:44:19
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
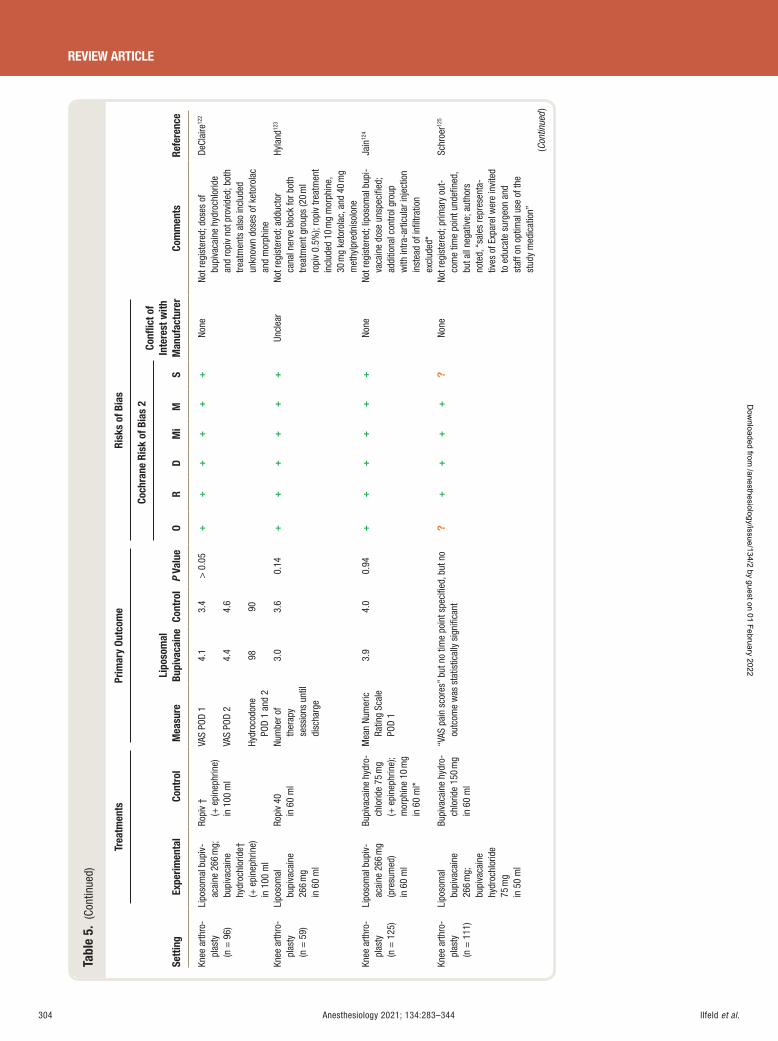
Ilfeld et al.304 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 5.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f In
tere
st w
ith
Man
ufac
ture
r O
R D
Mi
M
S
Knee
arth
ro-
plas
ty
(n =
96)
Lipo
som
al b
upiv
-ac
aine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide †
( +
epi
neph
rine)
in
100
ml
Ropi
v †
( + e
pine
phrin
e)
in 1
00 m
l
VAS
POD
1 4.
1 3.
4 >
0.0
5 +
++
++
+ No
ne
Not r
egis
tere
d; d
oses
of
bupi
vaca
ine
hydr
ochl
orid
e an
d ro
piv
not p
rovi
ded;
bot
h tre
atm
ents
als
o in
clud
ed
unkn
own
dose
s of
ket
orol
ac
and
mor
phin
e
DeCl
aire
122
VAS
POD
2 4.
4 4.
6
Hydr
ocod
one
POD
1 an
d 2
98
90
Knee
arth
ro-
plas
ty
(n =
59)
Lipo
som
al
bupi
vaca
ine
266
mg
in 6
0 m
l
Ropi
v 40
in
60
ml
Num
ber o
f th
erap
y se
ssio
ns u
ntil
disc
harg
e
3.0
3.6
0.14
+
++
++
+ Un
clea
r No
t reg
iste
red;
add
ucto
r ca
nal n
erve
blo
ck fo
r bot
h tre
atm
ent g
roup
s (2
0 m
l ro
piv
0.5%
); ro
piv
treat
men
t in
clud
ed 1
0 m
g m
orph
ine,
30
mg
keto
rola
c, a
nd 4
0 m
g m
ethy
lpre
dnis
olon
e
Hyla
nd 12
3
Knee
arth
ro-
plas
ty
(n =
125
)
Lipo
som
al b
upiv
-ac
aine
266
mg
(pre
sum
ed)
in 6
0 m
l
Bupi
vaca
ine
hydr
o-ch
lorid
e 75
mg
( + e
pine
phrin
e);
mor
phin
e 10
mg
in 6
0 m
l *
Mea
n Nu
mer
ic
Ratin
g Sc
ale
POD
1
3.9
4.0
0.94
+
++
++
+ No
ne
Not r
egis
tere
d; li
poso
mal
bup
i-va
cain
e do
se u
nspe
cifi e
d;
addi
tiona
l con
trol g
roup
w
ith in
tra-a
rticu
lar i
njec
tion
inst
ead
of in
fi ltra
tion
excl
uded
*
Jain
124
Knee
arth
ro-
plas
ty
(n =
111
)
Lipo
som
al
bupi
vaca
ine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide
75 m
g in
50
ml
Bupi
vaca
ine
hydr
o-ch
lorid
e 15
0 m
g in
60
ml
“ VAS
pai
n sc
ores
” bu
t no
time
poin
t spe
cifi e
d, b
ut n
o ou
tcom
e w
as s
tatis
tical
ly s
igni
fi can
t ?
++
++
? No
ne
Not r
egis
tere
d; p
rimar
y ou
t-co
me
time
poin
t und
efi n
ed,
but a
ll ne
gativ
e; a
utho
rs
note
d, “
sale
s re
pres
enta
-tiv
es o
f Exp
arel
wer
e in
vite
d to
edu
cate
sur
geon
and
st
aff o
n op
timal
use
of t
he
stud
y m
edic
atio
n ”
Schr
oer 12
5
(Con
tinue
d )
ALNV134N2_Text.indb 304ALNV134N2_Text.indb 304 29-Dec-20 19:44:1929-Dec-20 19:44:19
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
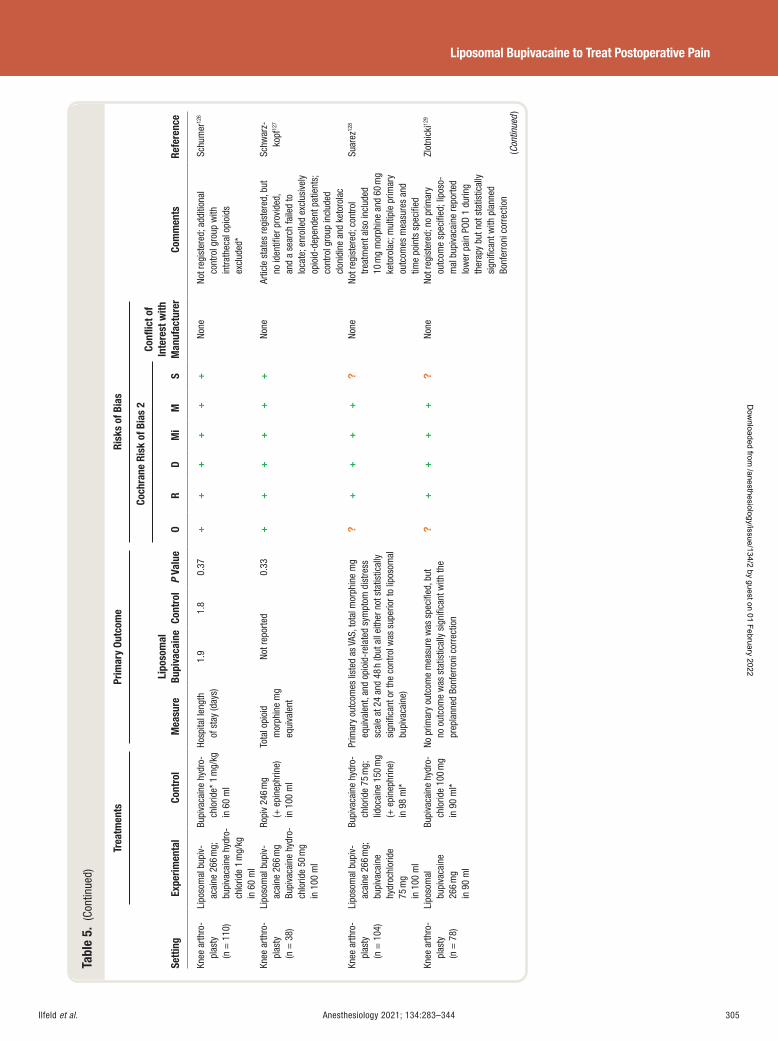
Ilfeld et al. Anesthesiology 2021; 134:283–344 305
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 5.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f In
tere
st w
ith
Man
ufac
ture
r O
R D
Mi
M
S
Knee
arth
ro-
plas
ty
(n =
110
)
Lipo
som
al b
upiv
-ac
aine
266
mg;
bu
piva
cain
e hy
dro-
chlo
ride
1 m
g/kg
in
60
ml
Bupi
vaca
ine
hydr
o-ch
lorid
e * 1
mg/
kg
in 6
0 m
l
Hosp
ital l
engt
h of
sta
y (d
ays)
1.
9 1.
8 0.
37
++
++
++
None
No
t reg
iste
red;
add
ition
al
cont
rol g
roup
with
in
trath
ecal
opi
oids
ex
clud
ed *
Schu
mer
126
Knee
arth
ro-
plas
ty
(n =
38)
Lipo
som
al b
upiv
-ac
aine
266
mg
Bupi
vaca
ine
hydr
o-ch
lorid
e 50
mg
in 1
00 m
l
Ropi
v 24
6 m
g ( +
epi
neph
rine)
in
100
ml
Tota
l opi
oid
mor
phin
e m
g eq
uiva
lent
Not r
epor
ted
0.33
+
++
++
+ No
ne
Artic
le s
tate
s re
gist
ered
, but
no
iden
tifi e
r pro
vide
d,
and
a se
arch
faile
d to
lo
cate
; enr
olle
d ex
clus
ivel
y op
ioid
-dep
ende
nt p
atie
nts;
co
ntro
l gro
up in
clud
ed
clon
idin
e an
d ke
toro
lac
Schw
arz-
kopf
127
Knee
arth
ro-
plas
ty
(n =
104
)
Lipo
som
al b
upiv
-ac
aine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide
75 m
g in
100
ml
Bupi
vaca
ine
hydr
o-ch
lorid
e 75
mg;
lid
ocai
ne 1
50 m
g ( +
epi
neph
rine)
in
98
ml *
Prim
ary
outc
omes
list
ed a
s VA
S, to
tal m
orph
ine
mg
equi
vale
nt, a
nd o
pioi
d-re
late
d sy
mpt
om d
istre
ss
scal
e at
24
and
48 h
(but
all
eith
er n
ot s
tatis
tical
ly
sign
ifi ca
nt o
r the
con
trol w
as s
uper
ior t
o lip
osom
al
bupi
vaca
ine)
?+
++
+?
None
No
t reg
iste
red;
con
trol
treat
men
t als
o in
clud
ed
10 m
g m
orph
ine
and
60 m
g ke
toro
lac;
mul
tiple
prim
ary
outc
omes
mea
sure
s an
d tim
e po
ints
spe
cifi e
d
Suar
ez 12
8
Knee
arth
ro-
plas
ty
(n =
78)
Lipo
som
al
bupi
vaca
ine
266
mg
in 9
0 m
l
Bupi
vaca
ine
hydr
o-ch
lorid
e 10
0 m
g in
90
ml *
No p
rimar
y ou
tcom
e m
easu
re w
as s
peci
fi ed,
but
no
out
com
e w
as s
tatis
tical
ly s
igni
fi can
t with
the
prep
lann
ed B
onfe
rron
i cor
rect
ion
?+
++
+?
None
No
t reg
iste
red;
no
prim
ary
outc
ome
spec
ifi ed
; lip
oso-
mal
bup
ivac
aine
repo
rted
low
er p
ain
POD
1 du
ring
ther
apy
but n
ot s
tatis
tical
ly
sign
ifi ca
nt w
ith p
lann
ed
Bonf
erro
ni c
orre
ctio
n
Zlot
nick
i 129
(Con
tinue
d )
ALNV134N2_Text.indb 305ALNV134N2_Text.indb 305 29-Dec-20 19:44:1929-Dec-20 19:44:19
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
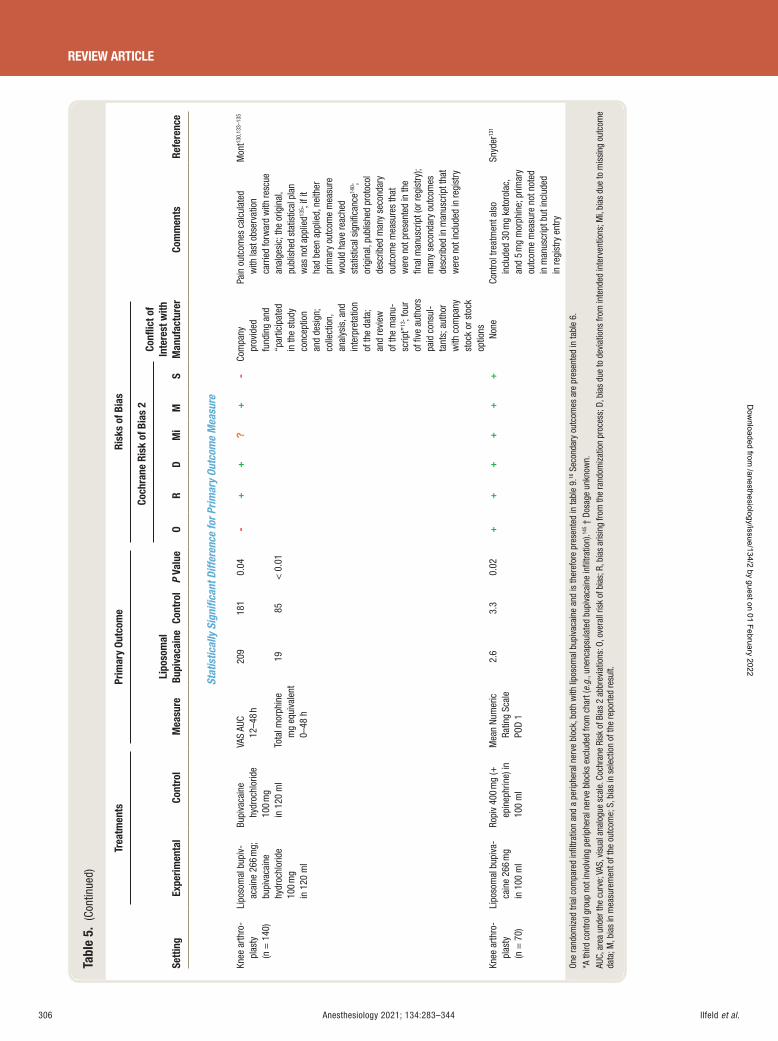
Ilfeld et al.306 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 5.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f In
tere
st w
ith
Man
ufac
ture
r O
R D
Mi
M
S
Stat
istic
ally
Sig
nifi c
ant D
iffer
ence
for P
rimar
y Ou
tcom
e M
easu
re
Knee
arth
ro-
plas
ty
(n =
140
)
Lipo
som
al b
upiv
-ac
aine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide
100
mg
in 1
20 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g in
120
ml
VAS
AUC
12 – 4
8 h
209
181
0.04
-+
+?
+-
Com
pany
pr
ovid
ed
fund
ing
and
“ par
ticip
ated
in
the
stud
y co
ncep
tion
and
desi
gn;
colle
ctio
n,
anal
ysis
, and
in
terp
reta
tion
of th
e da
ta;
and
revi
ew
of th
e m
anu-
scrip
t ” 13
; fou
r of
fi ve
aut
hors
pa
id c
onsu
l-ta
nts;
aut
hor
with
com
pany
st
ock
or s
tock
op
tions
Pain
out
com
es c
alcu
late
d w
ith la
st o
bser
vatio
n ca
rrie
d fo
rwar
d w
ith re
scue
an
alge
sic;
the
orig
inal
, pu
blis
hed
stat
istic
al p
lan
was
not
app
lied 13
5 ; if
it ha
d be
en a
pplie
d, n
eith
er
prim
ary
outc
ome
mea
sure
w
ould
hav
e re
ache
d st
atis
tical
sig
nifi c
ance
140 ;
orig
inal
, pub
lishe
d pr
otoc
ol
desc
ribed
man
y se
cond
ary
outc
ome
mea
sure
s th
at
wer
e no
t pre
sent
ed in
the
fi nal
man
uscr
ipt (
or re
gist
ry);
man
y se
cond
ary
outc
omes
de
scrib
ed in
man
uscr
ipt t
hat
wer
e no
t inc
lude
d in
regi
stry
Mon
t 130 ,
133 –
135
Tota
l mor
phin
e m
g eq
uiva
lent
0 –
48 h
19
85
< 0
.01
Knee
arth
ro-
plas
ty
(n =
70)
Lipo
som
al b
upiv
a-ca
ine
266
mg
in 1
00 m
l
Ropi
v 40
0 m
g ( +
ep
inep
hrin
e) in
10
0 m
l
Mea
n Nu
mer
ic
Ratin
g Sc
ale
POD
1
2.6
3.3
0.02
+
++
++
+ No
ne
Cont
rol t
reat
men
t als
o in
clud
ed 3
0 m
g ke
toro
lac,
an
d 5
mg
mor
phin
e; p
rimar
y ou
tcom
e m
easu
re n
ot n
oted
in
man
uscr
ipt b
ut in
clud
ed
in re
gist
ry e
ntry
Snyd
er 13
1
One
rand
omiz
ed tr
ial c
ompa
red
infi l
tratio
n an
d a
perip
hera
l ner
ve b
lock
, bot
h w
ith li
poso
mal
bup
ivac
aine
and
is th
eref
ore
pres
ente
d in
tabl
e 9 .
16 S
econ
dary
out
com
es a
re p
rese
nted
in ta
ble
6 .
* A th
ird c
ontro
l gro
up n
ot in
volv
ing
perip
hera
l ner
ve b
lock
s ex
clud
ed fr
om c
hart
( e.g
. , un
enca
psul
ated
bup
ivac
aine
infi l
tratio
n). 14
5 † D
osag
e un
know
n.
AUC,
are
a un
der t
he c
urve
; VAS
, vis
ual a
nalo
gue
scal
e. C
ochr
ane
Risk
of B
ias
2 ab
brev
iatio
ns: O
, ove
rall
risk
of b
ias;
R, b
ias
aris
ing
from
the
rand
omiz
atio
n pr
oces
s; D
, bia
s du
e to
dev
iatio
ns fr
om in
tend
ed in
terv
entio
ns; M
i, bi
as d
ue to
mis
sing
out
com
e da
ta; M
, bia
s in
mea
sure
men
t of t
he o
utco
me;
S, b
ias
in s
elec
tion
of th
e re
porte
d re
sult.
ALNV134N2_Text.indb 306ALNV134N2_Text.indb 306 29-Dec-20 19:44:1929-Dec-20 19:44:19
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
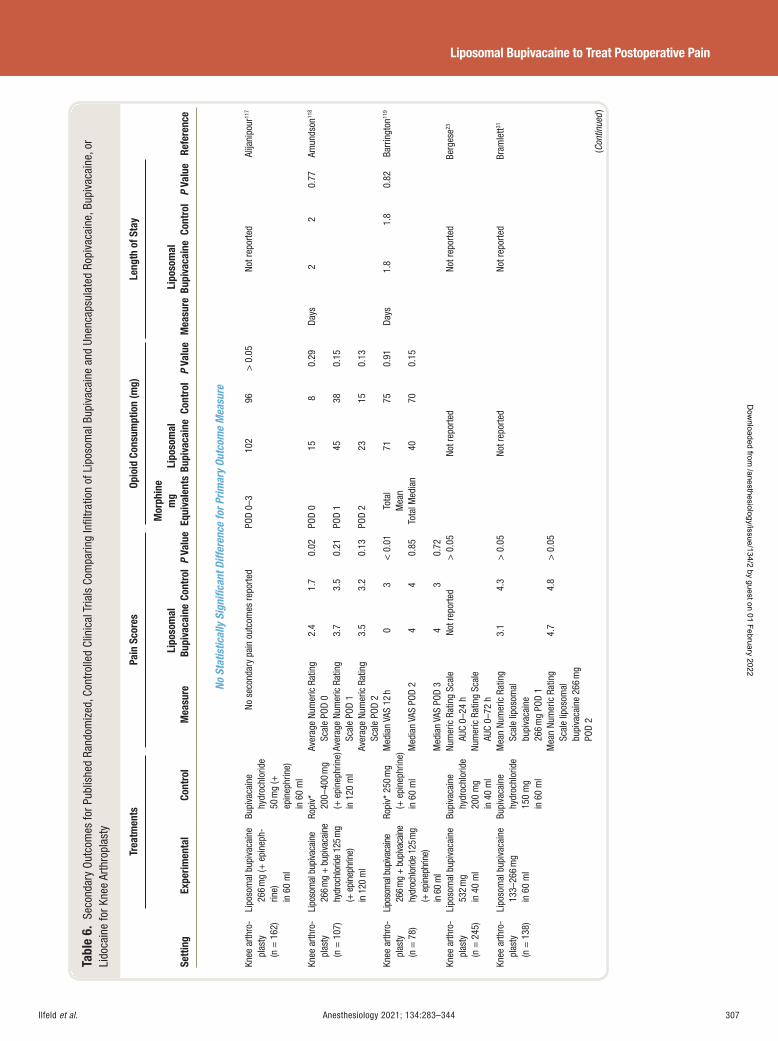
Ilfeld et al. Anesthesiology 2021; 134:283–344 307
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 6.
Sec
onda
ry O
utco
mes
for P
ublis
hed
Rand
omiz
ed, C
ontr
olle
d Cl
inic
al T
rials
Com
parin
g In
fi ltr
atio
n of
Lip
osom
al B
upiv
acai
ne a
nd U
nenc
apsu
late
d Ro
piva
cain
e, B
upiv
acai
ne, o
r Li
doca
ine
for K
nee
Arth
ropl
asty
Setti
ng
Trea
tmen
ts
Pain
Sco
res
Opio
id C
onsu
mpt
ion
(mg)
Le
ngth
of S
tay
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mor
phin
e m
g Eq
uiva
lent
s Li
poso
mal
Bu
piva
cain
e Co
ntro
l P
Valu
e M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
No S
tatis
tical
ly S
igni
fi can
t Diff
eren
ce fo
r Prim
ary
Outc
ome
Mea
sure
Knee
arth
ro-
plas
ty
(n =
162
)
Lipo
som
al b
upiv
acai
ne
266
mg
( + e
pine
ph-
rine)
in
60
ml
Bupi
vaca
ine
hydr
ochl
orid
e 50
mg
( +
epin
ephr
ine)
in
60
ml
No s
econ
dary
pai
n ou
tcom
es re
porte
d PO
D 0 –
3 10
2 96
>
0.0
5 No
t rep
orte
d Al
ijani
pour
117
Knee
arth
ro-
plas
ty
(n =
107
)
Lipo
som
al b
upiva
cain
e 26
6 mg
+ b
upiva
cain
e hy
droc
hlor
ide
125 m
g ( +
epi
neph
rine)
in
120
ml
Ropi
v *
200 –
400
mg
( + e
pine
phrin
e)
in 1
20 m
l
Aver
age
Num
eric
Rat
ing
Scal
e PO
D 0
2.4
1.7
0.02
POD
0 15
8 0.
29 Da
ys
2 2
0.77
Am
unds
on 11
8
Aver
age
Num
eric
Rat
ing
Scal
e PO
D 1
3.7
3.5
0.21
POD
1 45
38 0.
15
Aver
age
Num
eric
Rat
ing
Scal
e PO
D 2
3.5
3.2
0.13
PO
D 2
23
15
0.13
Knee
arth
ro-
plas
ty
(n =
78)
Lipo
som
al b
upiva
cain
e 26
6 mg
+ bu
piva
cain
e hy
droc
hlor
ide
125 m
g ( +
epi
neph
rine)
in
60
ml
Ropi
v * 2
50 m
g
( + e
pine
phrin
e)
in 6
0 m
l
Med
ian
VAS
12 h
0 3
< 0
.01
Tota
l M
ean
71 75
0.91
Days
1.
8 1.
8 0.
82
Barr
ingt
on 11
9
Med
ian
VAS
POD
2 4
4 0.
85To
tal M
edia
n 40
70
0.
15
Med
ian
VAS
POD
3 4
3 0.
72
Knee
arth
ro-
plas
ty
(n =
245
)
Lipo
som
al b
upiv
acai
ne
532
mg
in 4
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 20
0 m
g in
40
ml
Num
eric
Rat
ing
Scal
e AU
C 0 –
24 h
No
t rep
orte
d >
0.0
5 No
t rep
orte
d No
t rep
orte
d Be
rges
e 23
Num
eric
Rat
ing
Scal
e AU
C 0 –
72 h
Kn
ee a
rthro
-pl
asty
(n
= 1
38)
Lipo
som
al b
upiv
acai
ne
133 –
266
mg
in 6
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 15
0 m
g in
60
ml
Mea
n Nu
mer
ic R
atin
g Sc
ale
lipos
omal
bu
piva
cain
e 26
6 m
g PO
D 1
3.1
4.3
> 0
.05
Not r
epor
ted
Not r
epor
ted
Bram
lett 31
Mea
n Nu
mer
ic R
atin
g Sc
ale
lipos
omal
bu
piva
cain
e 26
6 m
g PO
D 2
4.7
4.8
> 0
.05
(Con
tinue
d )
ALNV134N2_Text.indb 307ALNV134N2_Text.indb 307 29-Dec-20 19:44:2029-Dec-20 19:44:20
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
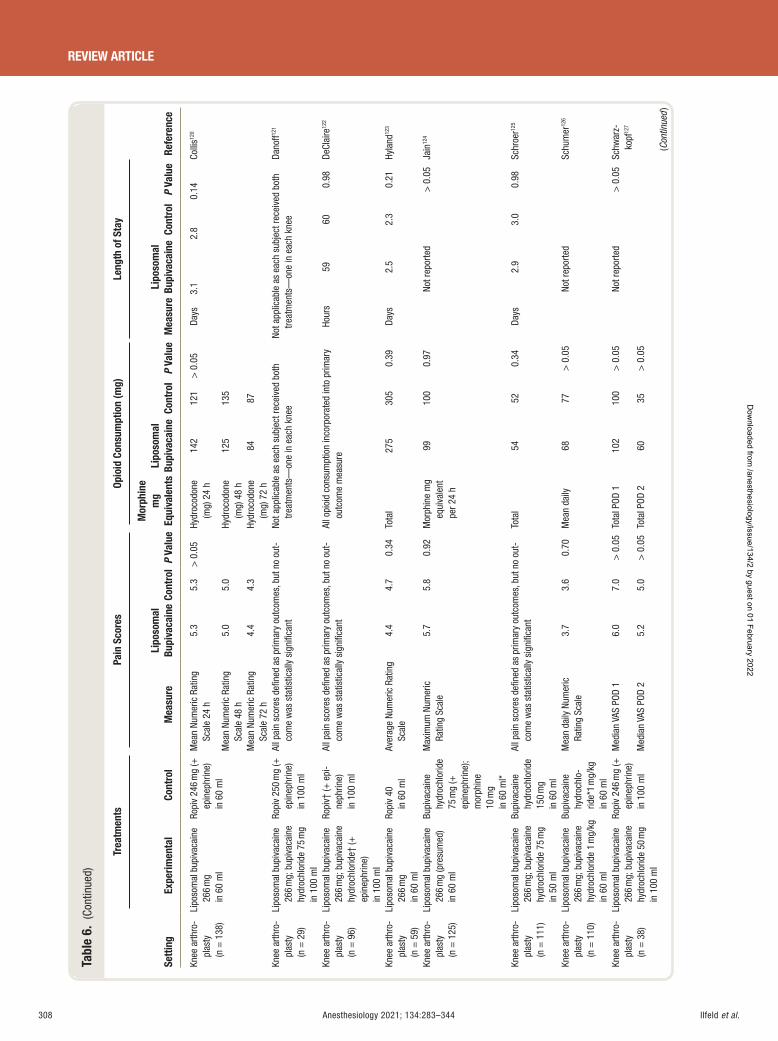
Ilfeld et al.308 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 6.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Pain
Sco
res
Opio
id C
onsu
mpt
ion
(mg)
Le
ngth
of S
tay
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mor
phin
e m
g Eq
uiva
lent
s Li
poso
mal
Bu
piva
cain
e Co
ntro
l P
Valu
e M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Knee
arth
ro-
plas
ty
(n =
138
)
Lipo
som
al b
upiv
acai
ne
266
mg
in 6
0 m
l
Ropi
v 24
6 m
g ( +
ep
inep
hrin
e)
in 6
0 m
l
Mea
n Nu
mer
ic R
atin
g Sc
ale
24 h
5.
3 5.
3 >
0.0
5 Hy
droc
odon
e (m
g) 2
4 h
142
121
> 0
.05
Days
3.
1 2.
8 0.
14
Colli
s 120
Mea
n Nu
mer
ic R
atin
g Sc
ale
48 h
5.
0 5.
0 Hy
droc
odon
e (m
g) 4
8 h
125
135
Mea
n Nu
mer
ic R
atin
g Sc
ale
72 h
4.
4 4.
3 Hy
droc
odon
e (m
g) 7
2 h
84
87
Knee
arth
ro-
plas
ty
(n =
29)
Lipo
som
al b
upiv
acai
ne
266
mg;
bup
ivac
aine
hy
droc
hlor
ide
75 m
g in
100
ml
Ropi
v 25
0 m
g ( +
ep
inep
hrin
e)
in 1
00 m
l
All p
ain
scor
es d
efi n
ed a
s pr
imar
y ou
tcom
es, b
ut n
o ou
t-co
me
was
sta
tistic
ally
sig
nifi c
ant
Not a
pplic
able
as
each
sub
ject
rece
ived
bot
h tre
atm
ents
— on
e in
eac
h kn
ee
Not a
pplic
able
as
each
sub
ject
rece
ived
bot
h tre
atm
ents
— on
e in
eac
h kn
ee
Dano
ff 121
Knee
arth
ro-
plas
ty
(n =
96)
Lipo
som
al b
upiv
acai
ne
266
mg;
bup
ivac
aine
hy
droc
hlor
ide †
( +
epin
ephr
ine)
in
100
ml
Ropi
v † ( +
epi
-ne
phrin
e)
in 1
00 m
l
All p
ain
scor
es d
efi n
ed a
s pr
imar
y ou
tcom
es, b
ut n
o ou
t-co
me
was
sta
tistic
ally
sig
nifi c
ant
All o
pioi
d co
nsum
ptio
n in
corp
orat
ed in
to p
rimar
y ou
tcom
e m
easu
re
Hour
s 59
60
0.
98
DeCl
aire
122
Knee
arth
ro-
plas
ty
(n =
59)
Lipo
som
al b
upiv
acai
ne
266
mg
in 6
0 m
l
Ropi
v 40
in
60
ml
Aver
age
Num
eric
Rat
ing
Scal
e 4.
4 4.
7 0.
34
Tota
l 27
5 30
5 0.
39
Days
2.
5 2.
3 0.
21
Hyla
nd 12
3
Knee
arth
ro-
plas
ty
(n =
125
)
Lipo
som
al b
upiv
acai
ne
266
mg
(pre
sum
ed)
in 6
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 75
mg
( +
epin
ephr
ine)
; m
orph
ine
10 m
g in
60
ml *
Max
imum
Num
eric
Ra
ting
Scal
e 5.
7 5.
8 0.
92
Mor
phin
e m
g eq
uiva
lent
pe
r 24
h
99
100
0.97
No
t rep
orte
d >
0.0
5 Ja
in 12
4
Knee
arth
ro-
plas
ty
(n =
111
)
Lipo
som
al b
upiv
acai
ne
266
mg;
bup
ivac
aine
hy
droc
hlor
ide
75 m
g in
50
ml
Bupi
vaca
ine
hydr
ochl
orid
e 15
0 m
g in
60
ml
All p
ain
scor
es d
efi n
ed a
s pr
imar
y ou
tcom
es, b
ut n
o ou
t-co
me
was
sta
tistic
ally
sig
nifi c
ant
Tota
l 54
52
0.
34
Days
2.
9 3.
0 0.
98
Schr
oer 12
5
Knee
arth
ro-
plas
ty
(n =
110
)
Lipo
som
al b
upiv
acai
ne
266
mg;
bup
ivac
aine
hy
droc
hlor
ide
1 m
g/kg
in
60
ml
Bupi
vaca
ine
hydr
ochl
o-rid
e * 1
mg/
kg
in 6
0 m
l
Mea
n da
ily N
umer
ic
Ratin
g Sc
ale
3.7
3.6
0.70
M
ean
daily
68
77
>
0.0
5 No
t rep
orte
d Sc
hum
er 12
6
Knee
arth
ro-
plas
ty
(n =
38)
Lipo
som
al b
upiv
acai
ne
266
mg;
bup
ivac
aine
hy
droc
hlor
ide
50 m
g in
100
ml
Ropi
v 24
6 m
g ( +
ep
inep
hrin
e)
in 1
00 m
l
Med
ian
VAS
POD
1 6.
0 7.
0 >
0.0
5 To
tal P
OD 1
10
2 10
0 >
0.0
5 No
t rep
orte
d >
0.0
5 Sc
hwar
z-ko
pf 12
7
Med
ian
VAS
POD
2 5.
2 5.
0 >
0.0
5 To
tal P
OD 2
60
35
>
0.0
5
(Con
tinue
d )
ALNV134N2_Text.indb 308ALNV134N2_Text.indb 308 29-Dec-20 19:44:2029-Dec-20 19:44:20
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
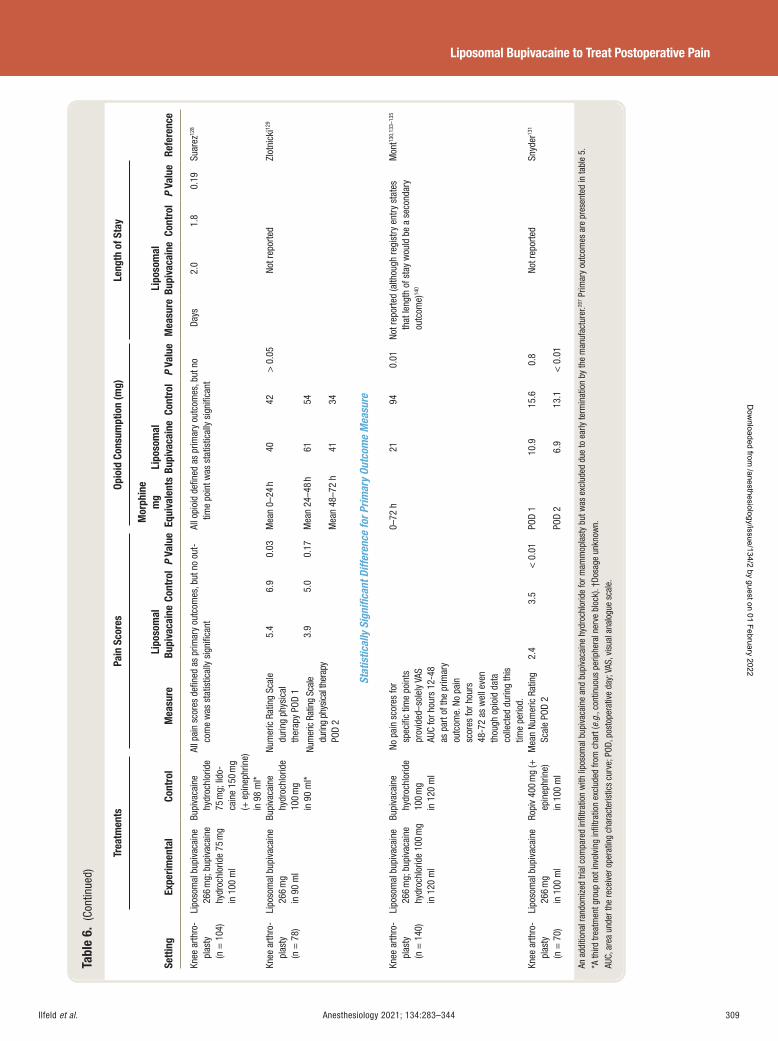
Ilfeld et al. Anesthesiology 2021; 134:283–344 309
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 6.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Pain
Sco
res
Opio
id C
onsu
mpt
ion
(mg)
Le
ngth
of S
tay
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mor
phin
e m
g Eq
uiva
lent
s Li
poso
mal
Bu
piva
cain
e Co
ntro
l P
Valu
e M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Knee
arth
ro-
plas
ty
(n =
104
)
Lipo
som
al b
upiv
acai
ne
266
mg;
bup
ivac
aine
hy
droc
hlor
ide
75 m
g in
100
ml
Bupi
vaca
ine
hydr
ochl
orid
e 75
mg;
lido
-ca
ine
150
mg
( + e
pine
phrin
e)
in 9
8 m
l *
All p
ain
scor
es d
efi n
ed a
s pr
imar
y ou
tcom
es, b
ut n
o ou
t-co
me
was
sta
tistic
ally
sig
nifi c
ant
All o
pioi
d de
fi ned
as
prim
ary
outc
omes
, but
no
time
poin
t was
sta
tistic
ally
sig
nifi c
ant
Days
2.
0 1.
8 0.
19
Suar
ez 12
8
Knee
arth
ro-
plas
ty
(n =
78)
Lipo
som
al b
upiv
acai
ne
266
mg
in 9
0 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g in
90
ml *
Num
eric
Rat
ing
Scal
e du
ring
phys
ical
th
erap
y PO
D 1
5.4
6.9
0.03
Mea
n 0 –
24 h
40 42
> 0
.05
Not r
epor
ted
Zlot
nick
i 129
Num
eric
Rat
ing
Scal
e du
ring
phys
ical
ther
apy
POD
2
3.9
5.0
0.17
M
ean
24 – 4
8 h
61 54
Mea
n 48
– 72
h 41
34
Stat
istic
ally
Sig
nifi c
ant D
iffer
ence
for P
rimar
y Ou
tcom
e M
easu
re
Knee
arth
ro-
plas
ty
(n =
140
)
Lipo
som
al b
upiv
acai
ne
266
mg;
bup
ivac
aine
hy
droc
hlor
ide
100
mg
in 1
20 m
l
Bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g in
120
ml
No
pain
sco
res
for
spec
ifi c
time
poin
ts
prov
ided
–sol
ely
VAS
AUC
for h
ours
12-
48
as p
art o
f the
prim
ary
outc
ome.
No
pain
sc
ores
for h
ours
48
-72
as w
ell e
ven
thou
gh o
pioi
d da
ta
colle
cted
dur
ing
this
tim
e pe
riod.
0 –
72 h
21
94
0.
01
Not r
epor
ted
(alth
ough
regi
stry
ent
ry s
tate
s th
at le
ngth
of s
tay
wou
ld b
e a
seco
ndar
y ou
tcom
e) 14
0
Mon
t 130 ,
133 –
135
Knee
arth
ro-
plas
ty
(n =
70)
Lipo
som
al b
upiv
acai
ne
266
mg
in 1
00 m
l
Ropi
v 40
0 m
g ( +
ep
inep
hrin
e)
in 1
00 m
l
Mea
n Nu
mer
ic R
atin
g Sc
ale
POD
2 2.
4 3.
5 <
0.0
1 PO
D 1
10.9
15.6
0.8
Not r
epor
ted
Snyd
er 13
1
POD
2 6.
9 13
.1
< 0
.01
An a
dditi
onal
rand
omiz
ed tr
ial c
ompa
red
infi l
tratio
n w
ith li
poso
mal
bup
ivac
aine
and
bup
ivac
aine
hyd
roch
lorid
e fo
r mam
mop
last
y bu
t was
exc
lude
d du
e to
ear
ly te
rmin
atio
n by
the
man
ufac
ture
r. 207 P
rimar
y ou
tcom
es a
re p
rese
nted
in ta
ble
5 .
* A th
ird tr
eatm
ent g
roup
not
invo
lvin
g in
fi ltra
tion
excl
uded
from
cha
rt ( e
.g. ,
cont
inuo
us p
erip
hera
l ner
ve b
lock
). † D
osag
e un
know
n.
AUC,
are
a un
der t
he re
ceiv
er o
pera
ting
char
acte
ristic
s cu
rve;
POD
, pos
tope
rativ
e da
y; V
AS, v
isua
l ana
logu
e sc
ale.
ALNV134N2_Text.indb 309ALNV134N2_Text.indb 309 29-Dec-20 19:44:2029-Dec-20 19:44:20
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Ilfeld et al.310 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
detect statistically signi cant di erences in their primary outcome measure(s) employed similarly high injection vol-umes of 90 to 120 ml, 118 , 121 , 122 , 127 – 129 and a seventh described administering “ approximately 50 injections, ” although the total volume was not speci ed. 119 In addition, authors of many of the trials without statistically signi cant ndings describe an involved in ltration protocol very similar to the PILLAR technique, including one group of authors who pointedly noted that “ the collaborating surgeon received extensive printed and in-person education on appropri-ate installation technique as recommended by the manu-facturer before study initiation, and a drug manufacturer representative was present in the operating room to provide support on proper drug administration as needed for the rst study patients. ” 123
An additional possible di erence among studies account-ing for the vastly dissimilar analgesic ndings might be that the PILLAR trial was unique in applying the windowed worst-observation-carried-forward method, specifying that “ pain intensity scores during periods of rescue medi-cation administration were replaced by the highest observed score before rescue medication use ” [emphasis added] . 130
The results without the “ window ” adjustments were not provided — unlike other manufacturer-supported random-ized, controlled trials 29 , 139 — so it remains unknown whether the relatively small di erence in pain scores between treatments (approximately 180 vs. 207 AUC during 36 h; P = 0.038) would have remained statistically signi cant without replacing the lower with higher scores. The authors had published their protocol — including details of the sta-tistical plan — before beginning enrollment, 135 but the win-dowed technique was not mentioned in that publication or the clinicaltrials.gov registry (NCT02713490). More importantly, the ultimate statistical analysis deviated from the prespeci ed statistical plan in three critical aspects, and if the original plan had been adhered to, the primary out-come measures would not have reached statistical signi -cance, even with the “ window ” imputation. 140 These two factors resulted in a high risk of bias using the Cochrane tool. 98 , 99 Last, while for the experimental group the max-imum Food and Drug Administration – approved liposomal bupivacaine (266 mg) combined with an additional 100 mg of bupivacaine hydrochloride was employed, the control group received only 57% of the possible maximum unen-capsulated bupivacaine dose, and without epinephrine, which is commonly included to increase both the maxi-mum dose (to 225 mg) and duration of e ect.
Summary
To summarize the evidence for the use of in ltration with liposomal bupivacaine over unencapsulated bupivacaine during knee arthroplasty, of the 17 available randomized, active-controlled trials, only two (12%) reported a statis-tically signi cant di erence for their primary outcome measure(s), 130 , 131 with the remainder observing few if any
statistically signi cant di erences in secondary and ter-tiary endpoints ( tables 5 and 6 ). 23 , 31 , 117 – 129 For one of the two trials with statistically signi cant ndings, 130 deviation from the published prespeci ed statistical plan resulted in a positive outcome when adherence to the original design would have rendered neither of the two coprimary end-points statistically signi cant. 140 In addition, this study used a submaximal dose of unencapsulated bupivacaine for the comparison group, while subjects of the treatment group received the maximum approved dose of liposomal bupi-vacaine plus additional bupivacaine hydrochloride. 130 This discrepancy greatly decreases con dence that the statisti-cally signi cant di erences would remain had a maximum dose of both treatments been compared. 130 Consequently, there is currently little published evidence with a low risk of bias demonstrating that administration of the maximum approved liposomal bupivacaine dose is superior to unen-capsulated bupivacaine hydrochloride when surgically in l-trated for knee arthroplasty.
Infi ltration with Liposomal Bupivacaine versus a Peripheral Nerve Block with Unencapsulated Long-acting Local Anesthetic
Single-injection Peripheral Nerve Block
A single-injection peripheral nerve block using the lon-gest acting local anesthetic approved in the United States, bupivacaine hydrochloride, provides a sensory and motor block with a typical duration of 8 to 12 h, although a lon-ger period may occur depending on the anatomic location, inclusion of additives, and other factors. Regardless, nearly all bupivacaine hydrochloride – based regional anesthet-ics resolve in less than 24 h. Since peripheral nerve blocks require additional equipment ( e.g. , ultrasound), expertise, and time to administer, surgical in ltration of a sustained released local anesthetic may be a useful alternative if found to deliver at least equivalent analgesia.
Eleven randomized, controlled trials compare a sin-gle-injection peripheral nerve block of unencapsulated long-acting local anesthetic with surgical in ltration of liposomal bupivacaine ( tables 7 and 8 ). 90 , 105 , 118 , 141 – 148 Of the eight that involve shoulder and knee procedures, 90 , 118 , 141 – 146
all were deemed to have some concerns regarding bias due mainly to a lack of treatment group masking. All either had an inadequately de ned primary outcome measure or used a primary outcome that included a longer duration than anticipated for the unencapsulated local anesthetic periph-eral nerve block (greater than 12 h). 90 , 118 , 141 – 146 However, the secondary outcomes allow a comparison of liposomal bupivacaine in ltration and peripheral nerve blocks. All eight reported statistically signi cant and clinically rele-vant improvements in pain scores in favor of the peripheral nerve block during the anticipated duration of the block (8 to 12 h). Of these, half also found that the peripheral nerve
ALNV134N2_Text.indb 310ALNV134N2_Text.indb 310 29-Dec-20 19:44:2029-Dec-20 19:44:20
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
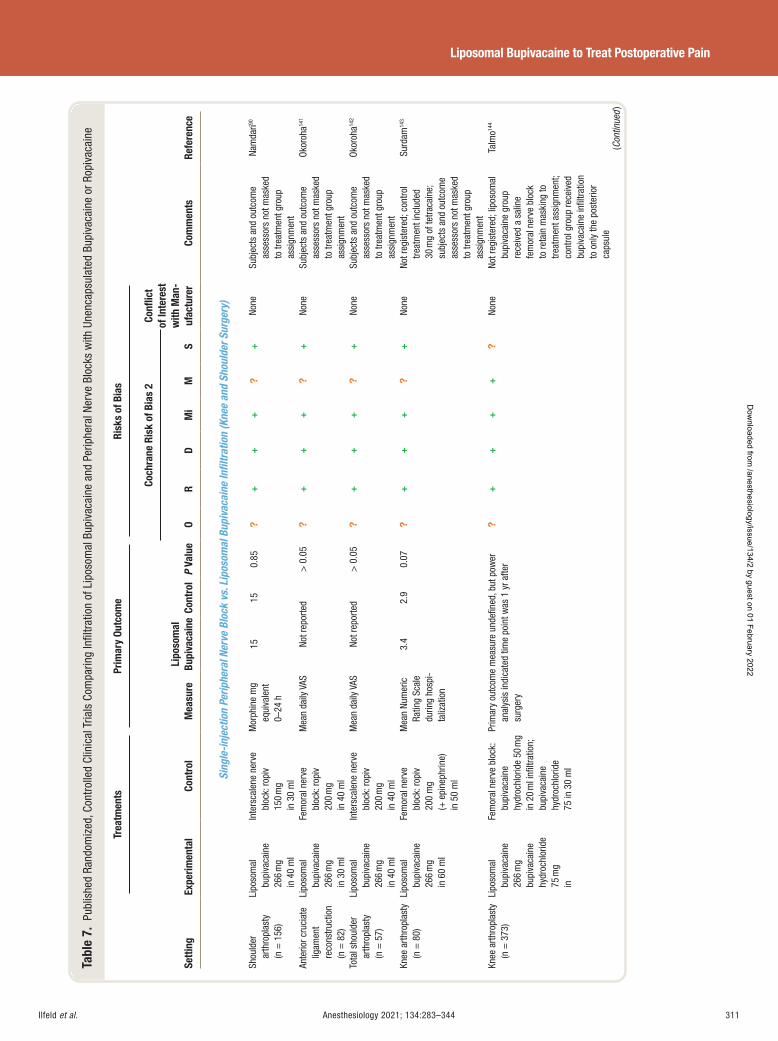
Ilfeld et al. Anesthesiology 2021; 134:283–344 311
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 7.
Pub
lishe
d Ra
ndom
ized
, Con
trol
led
Clin
ical
Tria
ls C
ompa
ring
Infi l
trat
ion
of L
ipos
omal
Bup
ivac
aine
and
Per
iphe
ral N
erve
Blo
cks
with
Une
ncap
sula
ted
Bupi
vaca
ine
or R
opiv
acai
ne
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict
of In
tere
st
with
Man
-uf
actu
rer
O R
D M
i M
S
Sing
le-in
ject
ion
Perip
hera
l Ner
ve B
lock
vs.
Lip
osom
al B
upiv
acai
ne In
fi ltr
atio
n (K
nee
and
Shou
lder
Sur
gery
)
Shou
lder
ar
thro
plas
ty
(n =
156
)
Lipo
som
al
bupi
vaca
ine
266
mg
in 4
0 m
l
Inte
rsca
lene
ner
ve
bloc
k: ro
piv
150
mg
in 3
0 m
l
Mor
phin
e m
g eq
uiva
lent
0 –
24 h
15
15
0.85
?
++
+?
+ No
ne
Subj
ects
and
out
com
e as
sess
ors
not m
aske
d to
trea
tmen
t gro
up
assi
gnm
ent
Nam
dari 90
Ante
rior c
ruci
ate
ligam
ent
reco
nstru
ctio
n (n
= 8
2)
Lipo
som
al
bupi
vaca
ine
266
mg
in 3
0 m
l
Fem
oral
ner
ve
bloc
k: ro
piv
200
mg
in 4
0 m
l
Mea
n da
ily V
AS
Not r
epor
ted
> 0
.05
?+
++
?+
None
Su
bjec
ts a
nd o
utco
me
asse
ssor
s no
t mas
ked
to tr
eatm
ent g
roup
as
sign
men
t
Okor
oha 14
1
Tota
l sho
ulde
r ar
thro
plas
ty
(n =
57)
Lipo
som
al
bupi
vaca
ine
266
mg
in 4
0 m
l
Inte
rsca
lene
ner
ve
bloc
k: ro
piv
200
mg
in 4
0 m
l
Mea
n da
ily V
AS
Not r
epor
ted
> 0
.05
?+
++
?+
None
Su
bjec
ts a
nd o
utco
me
asse
ssor
s no
t mas
ked
to tr
eatm
ent g
roup
as
sign
men
t
Okor
oha 14
2
Knee
arth
ropl
asty
(n
= 8
0)
Lipo
som
al
bupi
vaca
ine
266
mg
in 6
0 m
l
Fem
oral
ner
ve
bloc
k: ro
piv
200
mg
( + e
pine
phrin
e)
in 5
0 m
l
Mea
n Nu
mer
ic
Ratin
g Sc
ale
durin
g ho
spi-
taliz
atio
n
3.4
2.9
0.07
?
++
+?
+ No
ne
Not r
egis
tere
d; c
ontro
l tre
atm
ent i
nclu
ded
30 m
g of
tetra
cain
e;
subj
ects
and
out
com
e as
sess
ors
not m
aske
d to
trea
tmen
t gro
up
assi
gnm
ent
Surd
am 14
3
Knee
arth
ropl
asty
(n
= 3
73)
Lipo
som
al
bupi
vaca
ine
266
mg
bu
piva
cain
e hy
droc
hlor
ide
75 m
g in
Fem
oral
ner
ve b
lock
: bu
piva
cain
e hy
droc
hlor
ide
50 m
g in
20
ml i
nfi lt
ratio
n;
bupi
vaca
ine
hydr
ochl
orid
e 75
in 3
0 m
l
Prim
ary
outc
ome
mea
sure
und
efi n
ed, b
ut p
ower
an
alys
is in
dica
ted
time
poin
t was
1 y
r afte
r su
rger
y
?+
++
+?
None
No
t reg
iste
red;
lipo
som
al
bupi
vaca
ine
grou
p re
ceiv
ed a
sal
ine
fem
oral
ner
ve b
lock
to
reta
in m
aski
ng to
tre
atm
ent a
ssig
nmen
t; co
ntro
l gro
up re
ceiv
ed
bupi
vaca
ine
infi l
tratio
n to
onl
y th
e po
ster
ior
caps
ule
Talm
o 144
(Con
tinue
d )
ALNV134N2_Text.indb 311ALNV134N2_Text.indb 311 29-Dec-20 19:44:2029-Dec-20 19:44:20
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
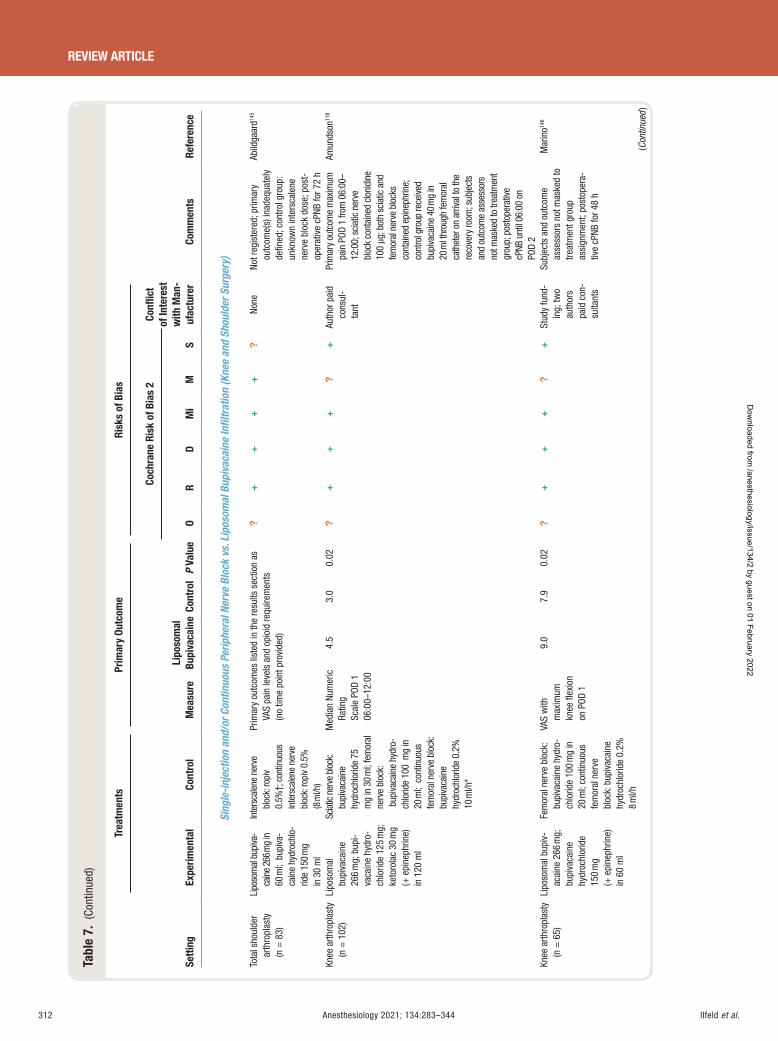
Ilfeld et al.312 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 7.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict
of In
tere
st
with
Man
-uf
actu
rer
O R
D M
i M
S
Sing
le-in
ject
ion
and/
or C
ontin
uous
Per
iphe
ral N
erve
Blo
ck v
s. L
ipos
omal
Bup
ivac
aine
Infi l
trat
ion
(Kne
e an
d Sh
ould
er S
urge
ry)
Tota
l sho
ulde
r ar
thro
plas
ty
(n =
83)
Lipo
som
al b
upiva
-ca
ine
266 m
g in
60
ml;
bup
iva-
cain
e hy
droc
hlo-
ride
150
mg
in 3
0 m
l
Inte
rsca
lene
ner
ve
bloc
k: ro
piv
0.5%
† ; c
ontin
uous
in
ters
cale
ne n
erve
bl
ock:
ropi
v 0.
5%
(8 m
l/h)
Prim
ary
outc
omes
list
ed in
the
resu
lts s
ectio
n as
VA
S pa
in le
vels
and
opi
oid
requ
irem
ents
(n
o tim
e po
int p
rovi
ded)
?+
++
+?
None
No
t reg
iste
red;
prim
ary
outc
ome(
s) in
adeq
uate
ly
defi n
ed; c
ontro
l gro
up:
unkn
own
inte
rsca
lene
ne
rve
bloc
k do
se; p
ost-
oper
ativ
e cP
NB fo
r 72
h
Abild
gaar
d 145
Knee
arth
ropl
asty
(n
= 1
02)
Lipo
som
al
bupi
vaca
ine
266
mg;
bup
i-va
cain
e hy
dro-
chlo
ride
125
mg;
ke
toro
lac
30 m
g ( +
epi
neph
rine)
in
120
ml
Scia
tic n
erve
bloc
k:
bupi
vaca
ine
hydr
ochl
orid
e 75
m
g in
30
ml;
fem
oral
ne
rve
bloc
k: b
upiv
acai
ne h
ydro
-ch
lorid
e 10
0 m
g in
20
ml;
con
tinuo
us
fem
oral
ner
ve b
lock
: bu
piva
cain
e hy
droc
hlor
ide
0.2%
10
ml/h
*
Med
ian
Num
eric
Ra
ting
Scal
e PO
D 1
06:0
0 – 12
:00
4.5
3.0
0.02
?
++
+?
+ Au
thor
pai
d co
nsul
-ta
nt
Prim
ary
outc
ome
max
imum
pa
in P
OD 1
from
06:
00 –
12:0
0; s
ciat
ic n
erve
bl
ock
cont
aine
d clo
nidi
ne
100
µ g; b
oth
scia
tic a
nd
fem
oral
ner
ve b
lock
s co
ntai
ned
epin
ephr
ine;
co
ntro
l gro
up re
ceive
d bu
piva
cain
e 40
mg
in
20 m
l thr
ough
fem
oral
ca
thet
er o
n ar
rival
to th
e re
cove
ry ro
om; s
ubje
cts
and
outc
ome
asse
ssor
s no
t mas
ked
to tr
eatm
ent
grou
p; p
osto
pera
tive
cPNB
unt
il 06
:00
on
POD
2
Amun
dson
118
Knee
arth
ropl
asty
(n
= 6
5)
Lipo
som
al b
upiv
-ac
aine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide
150
mg
( + e
pine
phrin
e)
in 6
0 m
l
Fem
oral
ner
ve b
lock
: bu
piva
cain
e hy
dro-
chlo
ride
100
mg
in
20 m
l; co
ntin
uous
fe
mor
al n
erve
bl
ock:
bup
ivac
aine
hy
droc
hlor
ide
0.2%
8
ml/h
VAS
with
m
axim
um
knee
fl ex
ion
on P
OD 1
9.0
7.9
0.02
?
++
+?
+ St
udy
fund
-in
g; tw
o au
thor
s pa
id c
on-
sulta
nts
Subj
ects
and
out
com
e as
sess
ors
not m
aske
d to
tre
atm
ent g
roup
as
sign
men
t; po
stop
era-
tive
cPNB
for 4
8 h
Mar
ino 14
6
(Con
tinue
d )
ALNV134N2_Text.indb 312ALNV134N2_Text.indb 312 29-Dec-20 19:44:2029-Dec-20 19:44:20
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
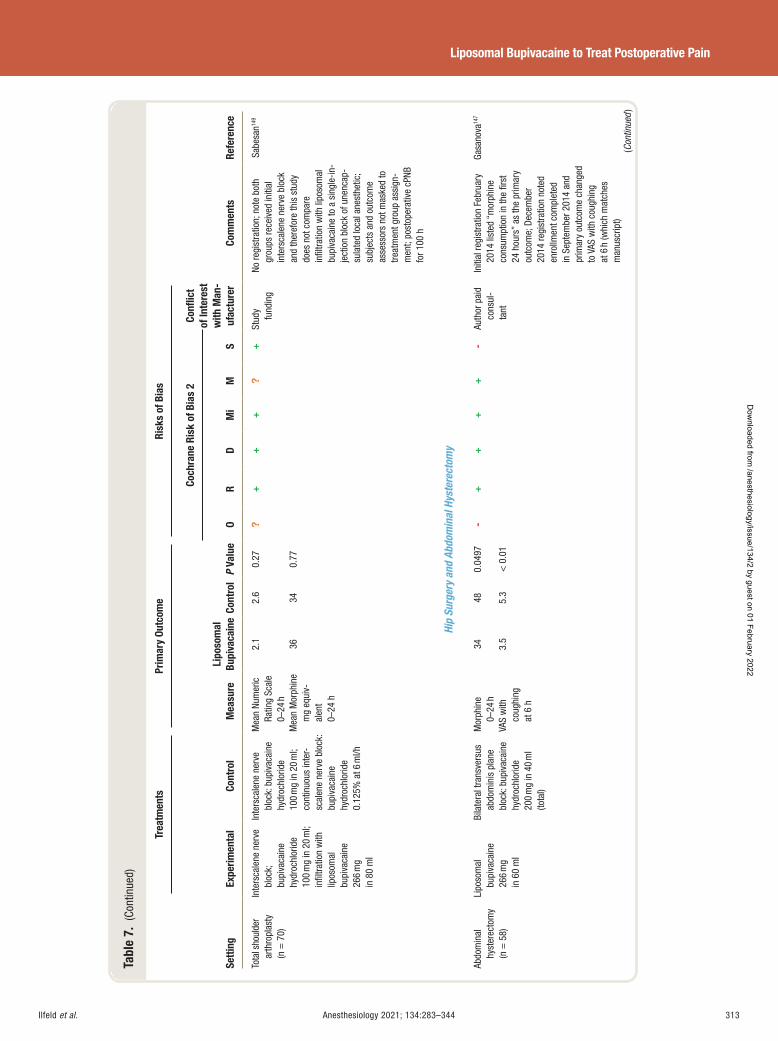
Ilfeld et al. Anesthesiology 2021; 134:283–344 313
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 7.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict
of In
tere
st
with
Man
-uf
actu
rer
O R
D M
i M
S
Tota
l sho
ulde
r ar
thro
plas
ty
(n =
70)
Inte
rsca
lene
ner
ve
bloc
k;
bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g in
20
ml;
infi l
tratio
n w
ith
lipos
omal
bu
piva
cain
e 26
6 m
g in
80
ml
Inte
rsca
lene
ner
ve
bloc
k: b
upiv
acai
ne
hydr
ochl
orid
e 10
0 m
g in
20
ml;
cont
inuo
us in
ter-
scal
ene
nerv
e bl
ock:
bu
piva
cain
e hy
droc
hlor
ide
0.12
5% a
t 6 m
l/h
Mea
n Nu
mer
ic
Ratin
g Sc
ale
0 – 24
h
2.1
2.6
0.27
?+
++
?+
Stud
y fu
ndin
g No
regi
stra
tion;
not
e bo
th
grou
ps re
ceiv
ed in
itial
in
ters
cale
ne n
erve
blo
ck
and
ther
efor
e th
is s
tudy
do
es n
ot c
ompa
re
infi l
tratio
n w
ith li
poso
mal
bu
piva
cain
e to
a s
ingl
e-in
-je
ctio
n bl
ock
of u
nenc
ap-
sula
ted
loca
l ane
sthe
tic;
subj
ects
and
out
com
e as
sess
ors
not m
aske
d to
tre
atm
ent g
roup
ass
ign-
men
t; po
stop
erat
ive
cPNB
fo
r 100
h
Sabe
san 14
9
Mea
n M
orph
ine
mg
equi
v-al
ent
0 – 24
h
36
34
0.77
Hip
Surg
ery
and
Abdo
min
al H
yste
rect
omy
Abdo
min
al
hyst
erec
tom
y (n
= 5
8)
Lipo
som
al
bupi
vaca
ine
266
mg
in 6
0 m
l
Bila
tera
l tra
nsve
rsus
ab
dom
inis
pla
ne
bloc
k: b
upiv
acai
ne
hydr
ochl
orid
e 20
0 m
g in
40
ml
(tota
l)
Mor
phin
e 0 –
24 h
34
48 0.
0497
-+
++
+-
Auth
or p
aid
cons
ul-
tant
Initi
al re
gist
ratio
n Fe
brua
ry
2014
list
ed “
mor
phin
e co
nsum
ptio
n in
the
fi rst
24
hou
rs ”
as th
e pr
imar
y ou
tcom
e; D
ecem
ber
2014
regi
stra
tion
note
d en
rollm
ent c
ompl
eted
in
Sep
tem
ber 2
014
and
prim
ary
outc
ome
chan
ged
to V
AS w
ith c
ough
ing
at 6
h (w
hich
mat
ches
m
anus
crip
t)
Gasa
nova
147
VAS
with
co
ughi
ng
at 6
h
3.5
5.3
< 0
.01
(Con
tinue
d )
ALNV134N2_Text.indb 313ALNV134N2_Text.indb 313 29-Dec-20 19:44:2029-Dec-20 19:44:20
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
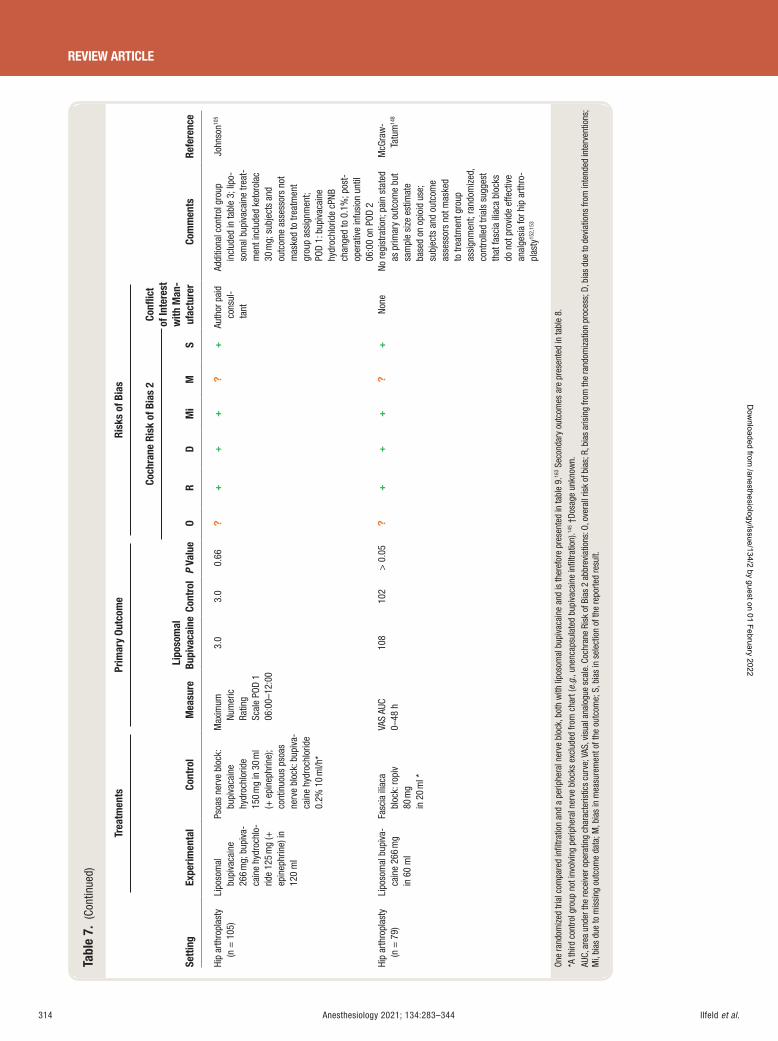
Ilfeld et al.314 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 7.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict
of In
tere
st
with
Man
-uf
actu
rer
O R
D M
i M
S
Hip
arth
ropl
asty
(n
= 1
05)
Lipo
som
al
bupi
vaca
ine
266
mg;
bup
iva-
cain
e hy
droc
hlo-
ride
125
mg
( +
epin
ephr
ine)
in
120
ml
Psoa
s ne
rve
bloc
k:
bupi
vaca
ine
hydr
ochl
orid
e 15
0 m
g in
30
ml
( + e
pine
phrin
e);
cont
inuo
us p
soas
ne
rve
bloc
k: b
upiv
a-ca
ine
hydr
ochl
orid
e 0.
2% 1
0 m
l/h *
Max
imum
Nu
mer
ic
Ratin
g Sc
ale
POD
1 06
:00 –
12:0
0
3.0
3.0
0.66
?
++
+?
+ Au
thor
pai
d co
nsul
-ta
nt
Addi
tiona
l con
trol g
roup
in
clud
ed in
tabl
e 3 ;
lipo
-so
mal
bup
ivac
aine
trea
t-m
ent i
nclu
ded
keto
rola
c 30
mg;
sub
ject
s an
d ou
tcom
e as
sess
ors
not
mas
ked
to tr
eatm
ent
grou
p as
sign
men
t; PO
D 1:
bup
ivac
aine
hy
droc
hlor
ide
cPNB
ch
ange
d to
0.1
%; p
ost-
oper
ativ
e in
fusi
on u
ntil
06:0
0 on
POD
2
John
son 10
5
Hip
arth
ropl
asty
(n
= 7
9)
Lipo
som
al b
upiv
a-ca
ine
266
mg
in 6
0 m
l
Fasc
ia il
iaca
bl
ock:
ropi
v
80 m
g in
20
ml *
VAS
AUC
0 – 48
h
108
102
> 0
.05
?+
++
?+
None
No
regi
stra
tion;
pai
n st
ated
as
prim
ary
outc
ome
but
sam
ple
size
est
imat
e ba
sed
on o
pioi
d us
e;
subj
ects
and
out
com
e as
sess
ors
not m
aske
d to
trea
tmen
t gro
up
assi
gnm
ent;
rand
omiz
ed,
cont
rolle
d tri
als
sugg
est
that
fasc
ia il
iaca
blo
cks
do n
ot p
rovi
de e
ffect
ive
anal
gesi
a fo
r hip
arth
ro-
plas
ty 15
2 , 15
3
McG
raw
-Ta
tum
148
One
rand
omiz
ed tr
ial c
ompa
red
infi l
tratio
n an
d a
perip
hera
l ner
ve b
lock
, bot
h w
ith li
poso
mal
bup
ivac
aine
and
is th
eref
ore
pres
ente
d in
tabl
e 9 .
163 S
econ
dary
out
com
es a
re p
rese
nted
in ta
ble
8 .
* A th
ird c
ontro
l gro
up n
ot in
volv
ing
perip
hera
l ner
ve b
lock
s ex
clud
ed fr
om c
hart
( e.g
. , un
enca
psul
ated
bup
ivac
aine
infi l
tratio
n). 14
5 † Do
sage
unk
now
n.
AUC,
are
a un
der t
he re
ceiv
er o
pera
ting
char
acte
ristic
s cu
rve;
VAS
, vis
ual a
nalo
gue
scal
e. C
ochr
ane
Risk
of B
ias
2 ab
brev
iatio
ns: O
, ove
rall
risk
of b
ias;
R, b
ias
aris
ing
from
the
rand
omiz
atio
n pr
oces
s; D
, bia
s du
e to
dev
iatio
ns fr
om in
tend
ed in
terv
entio
ns;
Mi,
bias
due
to m
issi
ng o
utco
me
data
; M, b
ias
in m
easu
rem
ent o
f the
out
com
e; S
, bia
s in
sel
ectio
n of
the
repo
rted
resu
lt.
ALNV134N2_Text.indb 314ALNV134N2_Text.indb 314 29-Dec-20 19:44:2129-Dec-20 19:44:21
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
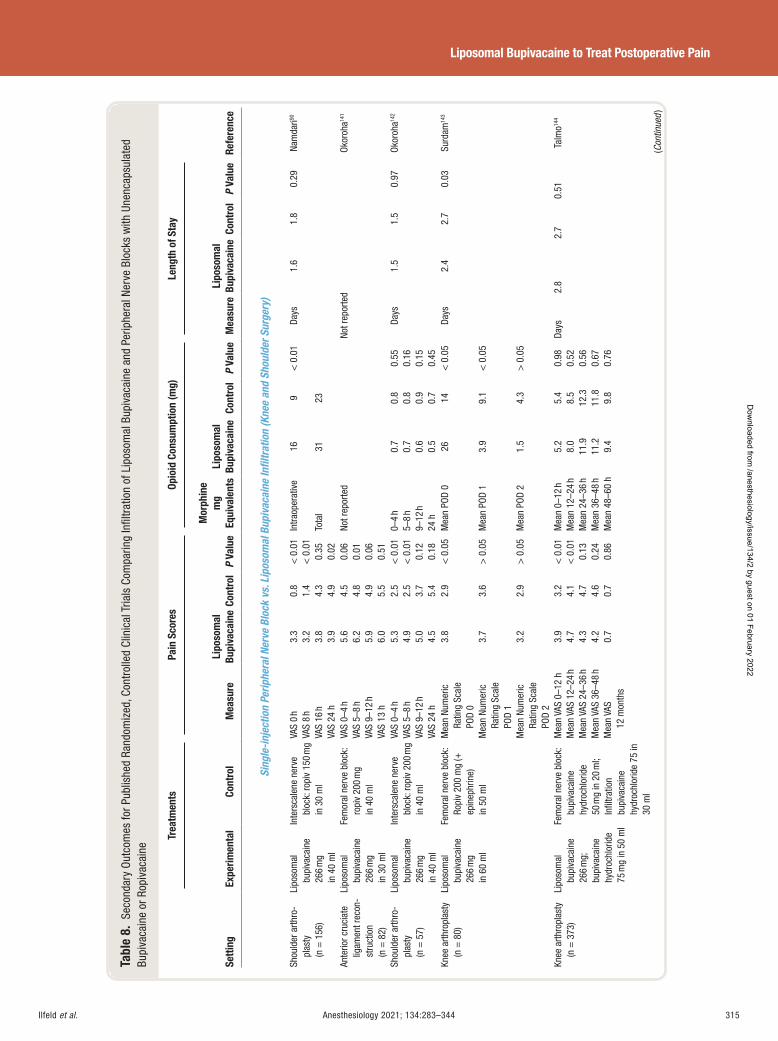
Ilfeld et al. Anesthesiology 2021; 134:283–344 315
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 8.
Sec
onda
ry O
utco
mes
for P
ublis
hed
Rand
omiz
ed, C
ontr
olle
d Cl
inic
al T
rials
Com
parin
g In
fi ltr
atio
n of
Lip
osom
al B
upiv
acai
ne a
nd P
erip
hera
l Ner
ve B
lock
s w
ith U
nenc
apsu
late
d Bu
piva
cain
e or
Rop
ivac
aine
Setti
ng
Trea
tmen
ts
Pain
Sco
res
Opio
id C
onsu
mpt
ion
(mg)
Le
ngth
of S
tay
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mor
phin
e m
g Eq
uiva
lent
s Li
poso
mal
Bu
piva
cain
e Co
ntro
l P
Valu
e M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Sing
le-in
ject
ion
Perip
hera
l Ner
ve B
lock
vs.
Lip
osom
al B
upiv
acai
ne In
fi ltr
atio
n (K
nee
and
Shou
lder
Sur
gery
)
Shou
lder
arth
ro-
plas
ty
(n =
156
)
Lipo
som
al
bupi
vaca
ine
266
mg
in 4
0 m
l
Inte
rsca
lene
ner
ve
bloc
k: ro
piv
150
mg
in 3
0 m
l
VAS
0 h
3.3
0.8
< 0
.01
Intra
oper
ativ
e 16
9 <
0.0
1 Da
ys
1.6
1.8
0.29
Na
mda
ri 90
VAS
8 h
3.2
1.4
< 0
.01
VAS
16 h
3.
8 4.
3 0.
35
Tota
l 31
23
VA
S 24
h
3.9
4.9
0.02
An
terio
r cru
ciat
e lig
amen
t rec
on-
stru
ctio
n (n
= 8
2)
Lipo
som
al
bupi
vaca
ine
266
mg
in 3
0 m
l
Fem
oral
ner
ve b
lock
: ro
piv
200
mg
in 4
0 m
l
VAS
0 – 4
h 5.
6 4.
5 0.
06
Not r
epor
ted
Not r
epor
ted
Okor
oha 14
1
VAS
5 – 8
h 6.
2 4.
8 0.
01
VAS
9 – 12
h
5.9
4.9
0.06
VA
S 13
h
6.0
5.5
0.51
Sh
ould
er a
rthro
-pl
asty
(n
= 5
7)
Lipo
som
al
bupi
vaca
ine
266
mg
in 4
0 m
l
Inte
rsca
lene
ner
ve
bloc
k: ro
piv
200
mg
in 4
0 m
l
VAS
0 – 4
h 5.
3 2.
5 <
0.0
1 0 –
4 h
0.7
0.8
0.55
Da
ys
1.5
1.5
0.97
Ok
oroh
a 142
VAS
5 – 8
h 4.
9 2.
5 <
0.0
1 5 –
8 h
0.7
0.8
0.16
VA
S 9 –
12 h
5.
0 3.
7 0.
12
9 – 12
h
0.6
0.9
0.15
VA
S 24
h
4.5
5.4
0.18
24
h
0.5
0.7
0.45
Kn
ee a
rthro
plas
ty
(n =
80)
Li
poso
mal
bu
piva
cain
e 26
6 m
g in
60
ml
Fem
oral
ner
ve b
lock
: Ro
piv
200
mg
( +
epin
ephr
ine)
in
50
ml
Mea
n Nu
mer
ic
Ratin
g Sc
ale
POD
0
3.8
2.9
< 0
.05
Mea
n PO
D 0
26 14
< 0
.05
Days
2.
4 2.
7 0.
03
Surd
am 14
3
Mea
n Nu
mer
ic
Ratin
g Sc
ale
POD
1
3.7
3.6
> 0
.05
Mea
n PO
D 1
3.9
9.1
< 0
.05
Mea
n Nu
mer
ic
Ratin
g Sc
ale
POD
2
3.2
2.9
> 0
.05
Mea
n PO
D 2
1.5
4.3
> 0
.05
Knee
arth
ropl
asty
(n
= 3
73)
Lipo
som
al
bupi
vaca
ine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide
75 m
g in
50
ml Fe
mor
al n
erve
blo
ck:
bupi
vaca
ine
hydr
ochl
orid
e 50
mg
in 2
0 m
l;
Infi l
tratio
n bu
piva
cain
e hy
droc
hlor
ide
75 in
30
ml
Mea
n VA
S 0 –
12 h
3.
9 3.
2 <
0.0
1 M
ean
0 – 12
h
5.2
5.4
0.98
Da
ys
2.8
2.7
0.51
Ta
lmo 14
4
Mea
n VA
S 12
– 24
h 4.
7 4.
1 <
0.0
1 M
ean
12 – 2
4 h
8.0
8.5
0.52
M
ean
VAS
24 – 3
6 h
4.3
4.7
0.13
M
ean
24 – 3
6 h
11.9
12
.3
0.56
M
ean
VAS
36 – 4
8 h
4.2
4.6
0.24
M
ean
36 – 4
8 h
11.2
11
.8
0.67
M
ean
VAS
12
mon
ths
0.7
0.7
0.86
M
ean
48 – 6
0 h
9.4
9.8
0.76
(Con
tinue
d )
ALNV134N2_Text.indb 315ALNV134N2_Text.indb 315 29-Dec-20 19:44:2129-Dec-20 19:44:21
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
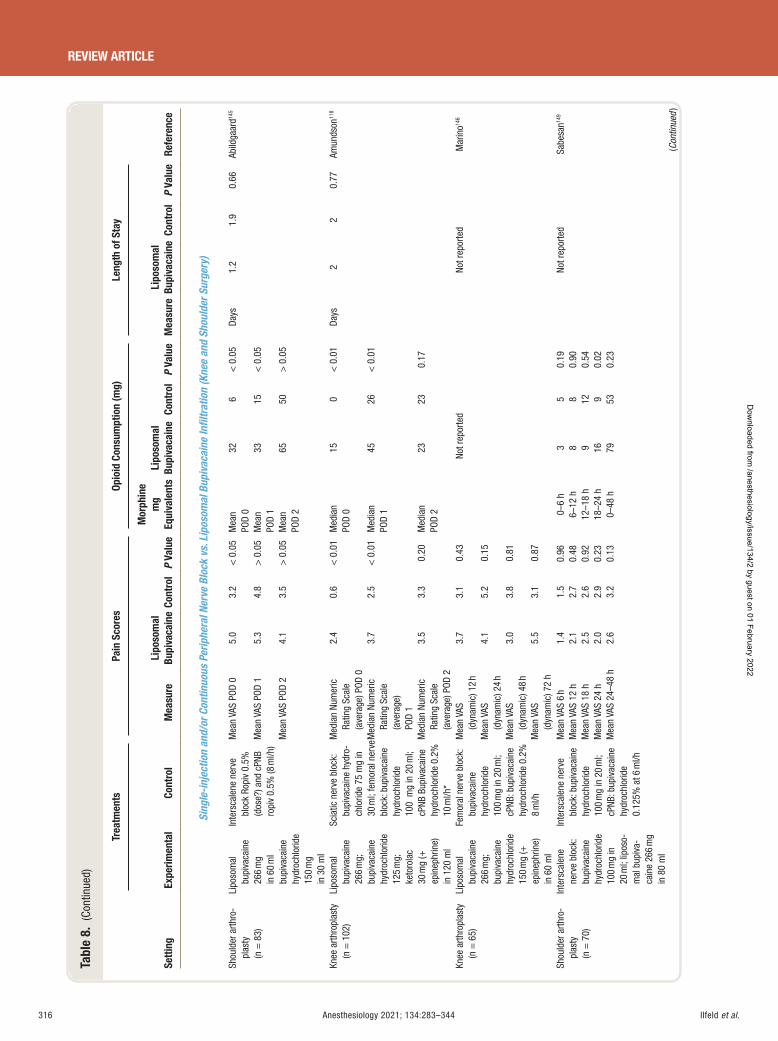
Ilfeld et al.316 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 8.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Pain
Sco
res
Opio
id C
onsu
mpt
ion
(mg)
Le
ngth
of S
tay
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mor
phin
e m
g Eq
uiva
lent
s Li
poso
mal
Bu
piva
cain
e Co
ntro
l P
Valu
e M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Sing
le-in
ject
ion
and/
or C
ontin
uous
Per
iphe
ral N
erve
Blo
ck v
s. L
ipos
omal
Bup
ivac
aine
Infi l
trat
ion
(Kne
e an
d Sh
ould
er S
urge
ry)
Shou
lder
arth
ro-
plas
ty
(n =
83)
Lipo
som
al
bupi
vaca
ine
266
mg
in 6
0 m
l bu
piva
cain
e hy
droc
hlor
ide
150
mg
in 3
0 m
l
Inte
rsca
lene
ner
ve
bloc
k Ro
piv
0.5%
(d
ose?
) and
cPN
B ro
piv
0.5%
(8 m
l/h)
Mea
n VA
S PO
D 0
5.0
3.2
< 0
.05
Mea
n PO
D 0
32
6 <
0.0
5 Da
ys
1.2
1.9
0.66
Ab
ildga
ard 14
5
Mea
n VA
S PO
D 1
5.3
4.8
> 0
.05
Mea
n PO
D 1
33
15 <
0.0
5
Mea
n VA
S PO
D 2
4.1
3.5
> 0
.05
Mea
n PO
D 2
65
50
> 0
.05
Knee
arth
ropl
asty
(n
= 1
02)
Lipo
som
al
bupi
vaca
ine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide
125
mg;
ke
toro
lac
30 m
g ( +
ep
inep
hrin
e)
in 1
20 m
l
Scia
tic n
erve
blo
ck:
bupi
vaca
ine
hydr
o-ch
lorid
e 75
mg
in
30 m
l; fe
mor
al n
erve
bl
ock:
bup
ivac
aine
hy
droc
hlor
ide
100
mg
in 2
0 m
l; cP
NB B
upiv
acai
ne
hydr
ochl
orid
e 0.
2%
10 m
l/h *
Med
ian
Num
eric
Ra
ting
Scal
e (a
vera
ge) P
OD 0
2.4
0.6
< 0
.01
Med
ian
POD
0 15
0 <
0.0
1 Da
ys
2 2
0.77
Am
unds
on 11
8
Med
ian
Num
eric
Ra
ting
Scal
e (a
vera
ge)
POD
1
3.7
2.5
< 0
.01
Med
ian
POD
1 45
26 <
0.0
1
Med
ian
Num
eric
Ra
ting
Scal
e (a
vera
ge) P
OD 2
3.5
3.3
0.20
M
edia
n PO
D 2
23
23
0.17
Knee
arth
ropl
asty
(n
= 6
5)
Lipo
som
al
bupi
vaca
ine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide
150
mg
( +
epin
ephr
ine)
in
60
ml
Fem
oral
ner
ve b
lock
: bu
piva
cain
e hy
droc
hlor
ide
100
mg
in 2
0 m
l; cP
NB: b
upiv
acai
ne
hydr
ochl
orid
e 0.
2%
8 m
l/h
Mea
n VA
S (d
ynam
ic) 1
2 h
3.7
3.1
0.43
Not r
epor
ted
Not r
epor
ted
Mar
ino 14
6
Mea
n VA
S (d
ynam
ic) 2
4 h
4.1
5.2
0.15
Mea
n VA
S (d
ynam
ic) 4
8 h
3.0
3.8
0.81
Mea
n VA
S (d
ynam
ic) 7
2 h
5.5
3.1
0.87
Shou
lder
arth
ro-
plas
ty
(n =
70)
Inte
rsca
lene
ne
rve
bloc
k:
bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g in
20
ml;
lipos
o-m
al b
upiv
a-ca
ine
266
mg
in 8
0 m
l
Inte
rsca
lene
ner
ve
bloc
k: b
upiv
acai
ne
hydr
ochl
orid
e 10
0 m
g in
20
ml;
cPNB
: bup
ivac
aine
hy
droc
hlor
ide
0.12
5% a
t 6 m
l/h
Mea
n VA
S 6
h
1.4
1.5
0.
96
0 – 6
h 3
5 0.
19
Not r
epor
ted
Sabe
san 14
9
Mea
n VA
S 12
h
2.1
2.7
0.
48
6 – 12
h
8 8
0.90
M
ean
VAS
18 h
2.
5 2.
6
0.92
12
– 18
h 9
12
0.54
M
ean
VAS
24 h
2.
0 2.
9
0.23
18
– 24
h 16
9
0.02
M
ean
VAS
24 – 4
8 h
2.6
3.2
0.
13
0 – 48
h
79
53
0.23
(Con
tinue
d )
ALNV134N2_Text.indb 316ALNV134N2_Text.indb 316 29-Dec-20 19:44:2129-Dec-20 19:44:21
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
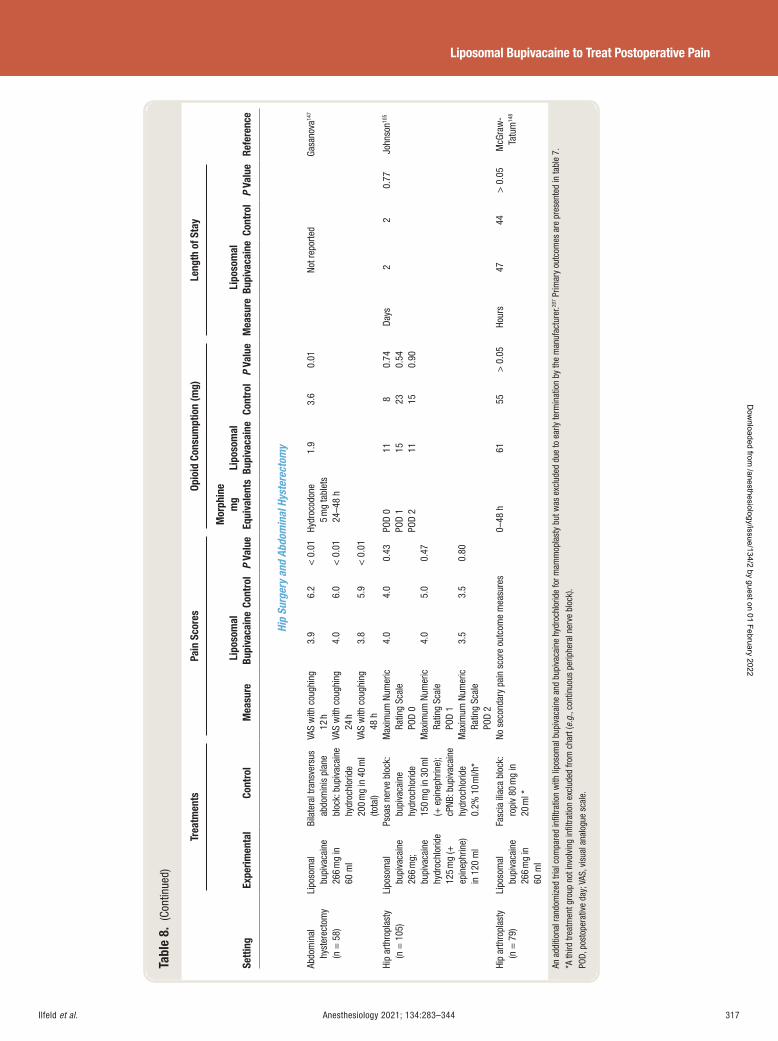
Ilfeld et al. Anesthesiology 2021; 134:283–344 317
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 8.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Pain
Sco
res
Opio
id C
onsu
mpt
ion
(mg)
Le
ngth
of S
tay
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mor
phin
e m
g Eq
uiva
lent
s Li
poso
mal
Bu
piva
cain
e Co
ntro
l P
Valu
e M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Hip
Surg
ery
and
Abdo
min
al H
yste
rect
omy
Abdo
min
al
hyst
erec
tom
y (n
= 5
8)
Lipo
som
al
bupi
vaca
ine
266
mg
in
60 m
l
Bila
tera
l tra
nsve
rsus
ab
dom
inis
pla
ne
bloc
k: b
upiv
acai
ne
hydr
ochl
orid
e 20
0 m
g in
40
ml
(tota
l)
VAS
with
cou
ghin
g 12
h
3.9
6.2
< 0
.01
Hydr
ocod
one
5 m
g ta
blet
s 24
– 48
h
1.9
3.6
0.01
No
t rep
orte
d Ga
sano
va 14
7
VAS
with
cou
ghin
g 24
h
4.0
6.0
< 0
.01
VAS
with
cou
ghin
g 48
h
3.8
5.9
< 0
.01
Hip
arth
ropl
asty
(n
= 1
05)
Lipo
som
al
bupi
vaca
ine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide
125
mg
( +
epin
ephr
ine)
in
120
ml
Psoa
s ne
rve
bloc
k:
bupi
vaca
ine
hydr
ochl
orid
e 15
0 m
g in
30
ml
( + e
pine
phrin
e);
cPNB
: bup
ivac
aine
hy
droc
hlor
ide
0.2%
10
ml/h
*
Max
imum
Num
eric
Ra
ting
Scal
e PO
D 0
4.0
4.0
0.43
PO
D 0
PO
D 1
PO
D 2
11
15
11
8 23
15
0.74
0.
54
0.90
Days
2
2 0.
77
John
son 10
5
Max
imum
Num
eric
Ra
ting
Scal
e PO
D 1
4.0
5.0
0.47
Max
imum
Num
eric
Ra
ting
Scal
e PO
D 2
3.5
3.5
0.80
Hip
arth
ropl
asty
(n
= 7
9)
Lipo
som
al
bupi
vaca
ine
266
mg
in
60 m
l
Fasc
ia il
iaca
blo
ck:
ropi
v 80
mg
in
20 m
l *
No s
econ
dary
pai
n sc
ore
outc
ome
mea
sure
s 0 –
48 h
61
55
>
0.0
5 Ho
urs
47
44
> 0
.05
McG
raw
-Ta
tum
148
An a
dditi
onal
rand
omiz
ed tr
ial c
ompa
red
infi l
tratio
n w
ith li
poso
mal
bup
ivac
aine
and
bup
ivac
aine
hyd
roch
lorid
e fo
r mam
mop
last
y bu
t was
exc
lude
d du
e to
ear
ly te
rmin
atio
n by
the
man
ufac
ture
r. 207 P
rimar
y ou
tcom
es a
re p
rese
nted
in ta
ble
7 .
* A th
ird tr
eatm
ent g
roup
not
invo
lvin
g in
fi ltra
tion
excl
uded
from
cha
rt ( e
.g. ,
cont
inuo
us p
erip
hera
l ner
ve b
lock
). PO
D, p
osto
pera
tive
day;
VAS
, vis
ual a
nalo
gue
scal
e.
ALNV134N2_Text.indb 317ALNV134N2_Text.indb 317 29-Dec-20 19:44:2129-Dec-20 19:44:21
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Ilfeld et al.318 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
block group concurrently required a lower dose of supple-mental opioids, 90 , 118 , 143 , 145 while the remainder reported little di erence during this period of time. 141 , 142 , 144 , 146 Collectively, these eight studies provide evidence that a single-injection peripheral nerve block with unencapsulated ropivacaine or bupivacaine provides superior analgesia compared with liposomal bupivacaine in ltration for the duration of the peripheral nerve block.
However, one of the proposed bene ts of using liposo-mal bupivacaine in ltration is the possibility of prolong-ing analgesia beyond the typical 8 to 12 h peripheral nerve block duration. Of the eight randomized, controlled trials just described, 90 , 118 , 141 – 146 three included an additional con-tinuous peripheral nerve block in which unencapsulated local anesthetic was infused through a percutaneous peri-neural catheter to extend analgesia beyond the duration of the initial single-injection peripheral nerve block. 118 , 145 , 146
Therefore, the remaining ve randomized, controlled trials describe a single-injection peripheral nerve block without a subsequent confounding perineural infusion: one reported that subjects receiving in ltrated liposomal bupivacaine did have less pain at 24 h (although not beyond), 90 with the remaining four trials nding no statistically signi cant dif-ferences between treatments. 141 – 144 Similarly, of these ve trials, 90 , 141 – 144 two detected lower opioid requirements for liposomal bupivacaine subjects after block resolution: one on postoperative day 1, 143 and the other during postoper-ative hours 13 through 16 (although this was reversed in favor of the peripheral nerve block group during hours 49 to 56, suggesting a high probability of type I errors for these two ndings due to multiple comparisons with a limited sample size). 142 Thus, these ve randomized, controlled tri-als failed to provide evidence that liposomal bupivacaine provided any analgesic or opioid-sparing bene ts beyond postoperative day 1.
Continuous Peripheral Nerve Block
Four randomized, controlled trials included a continu-ous peripheral nerve block for knee and shoulder surgery, allowing a comparison of liposomal bupivacaine in ltra-tion and perineural local anesthetic infusion ( tables 7 and 8 ). 118 , 145 , 146 , 149 The two involving knee arthroplasty reported lower pain scores for subjects with continuous femoral nerve blocks during the period of perineural local anes-thetic infusion based on both primary and secondary out-come measures. 118 , 146 One of these also found concurrent lower opioid use for continuous peripheral nerve block subjects, 118 while the other detected a longer time to rst use of rescue opioids for subjects who had received liposo-mal bupivacaine. 146
Two additional randomized, controlled trials involved shoulder arthroplasty; neither found di erences in pain scores after resolution of the single-injection peripheral nerve block. 145 , 149 However, both detected greater opioid sparing in favor of the continuous peripheral nerve block
during this same duration. Unfortunately, neither was reg-istered or had a well-de ned primary outcome measure. In addition, one provided no information on the perineu-ral infusion dosing in the manuscript, rendering the nd-ings for postoperative days 1 and 2 di cult to interpret. 145
Furthermore, unlike the other continuous peripheral nerve block investigations, the second trial provided a single-in-jection interscalene block to both treatment groups. 149
The reason for the nding of continuous peripheral nerve block analgesic superiority over in ltrated liposomal bupivacaine for femoral but not interscalene catheters is not readily apparent. 118 , 146 , 149 It may simply be due to the very low number of studies with underpowered sample sizes, or that in one shoulder study, both treatment groups received a single-injection peripheral nerve block. Regardless, this latter study is a good example of the potential bene t of local in ltration analgesia over continuous peripheral nerve blocks: two subjects experienced residual hand numbness that resolved with catheter removal, and ve had an inad-vertent, premature catheter dislodgement. 149 Moreover, unlike perineural infusion, tissue/joint in ltration carries little risk of inducing muscle weakness, 146 patient burden is decreased without an infusion pump and local anesthetic reservoir to carry, and provider workload is reduced with-out an infusion to manage. 1 Given these potential bene- ts of liposomal bupivacaine combined with the equivocal available comparison data, additional research is greatly needed to assist stakeholders in optimizing patients ’ periop-erative experience.
Three studies involved hip arthroplasty or abdominal hysterectomy ( tables 7 and 8 ). 105 , 148 One hip arthroplasty study compared in ltration with liposomal bupivacaine with a fascia iliaca block without a subsequent infusion, 148
while the other compared liposomal bupivacaine to sin-gle-injection and continuous psoas compartment (posterior lumbar plexus) blocks. 105 Liposomal bupivacaine in ltration was not inferior to a fascia iliaca block in the rst study, but interpretation of this result is complicated by results of multiple randomized, placebo-controlled trials demon-strating that fascia iliaca blocks provide little to no anal-gesic bene t after hip arthroplasty. 150 , 151 In contrast, psoas compartment blocks/infusions do o er pain control for hip arthroplasty, 152 , 153 and liposomal bupivacaine in ltration was not inferior to this block, which had a high incidence of motor weakness and complications, indicating bene ts from liposomal bupivacaine in this comparison. 105
Last, one randomized, controlled trial compared lipo-somal bupivacaine in ltration with a bilateral transversus abdominis block with bupivacaine hydrochloride for total abdominal hysterectomy. 147 The results were statistically sig-ni cant in favor of the liposomal bupivacaine in ltration for both the primary outcome of pain upon coughing 6 h after surgery and nearly every secondary pain (at rest and on coughing) and opioid endpoint from 2 to 48 postoperative hours. Unfortunately, a discrepancy between the primary
ALNV134N2_Text.indb 318ALNV134N2_Text.indb 318 29-Dec-20 19:44:2129-Dec-20 19:44:21
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Ilfeld et al. Anesthesiology 2021; 134:283–344 319
Liposomal Bupivacaine to Treat Postoperative Pain
outcome provided in the registry and published manuscript results in a high risk of bias for this trial.
Summary
To summarize the evidence for the use of in ltration with liposomal bupivacaine compared with a peripheral nerve block with unencapsulated local anesthetic for knee and shoulder procedures, all of eight randomized, controlled tri-als found evidence that a single-injection peripheral nerve block provides superior analgesia and concurrent opioid sparing for the duration of the block based on second-ary outcomes. 90 , 118 , 141 – 146 After block resolution, only one trial found any analgesic bene t of liposomal bupivacaine in ltration — and then only at 24 h 90 ; two detected opioid sparing on postoperative day 0 or 1. 142 , 143 Four randomized, controlled trials are available comparing liposomal bupiva-caine in ltration with a continuous peripheral nerve block, and all reported lower pain scores and/or less opioid use for subjects with continuous peripheral nerve blocks based on primary and secondary outcomes. 118 , 145 , 146 , 149 Therefore, there is evidence demonstrating the superiority of sin-gle-injection and/or continuous peripheral nerve blocks to liposomal bupivacaine in ltration for knee and shoul-der surgery. However, the improved analgesia and opioid sparing must be balanced against the time and expertise required for administration, increased patient and pro-vider burden, and other block-related limitations. Only a single randomized, controlled trial provides reliable data involving hip surgery, and while it does not demonstrate any superiority of liposomal bupivacaine over single-injec-tion and continuous peripheral nerve blocks, the lack of block-related limitations will favor the liposomal bupiva-caine in ltration method for many providers. 105 Finally, the one randomized, controlled trial investigating abdominal hysterectomy provides evidence that liposomal bupivacaine in ltration is superior to a bilateral transversus abdominis block with unencapsulated bupivacaine, 147 but this trial was deemed at high risk for bias due to a discrepancy between the primary outcome provided in the registry and pub-lished manuscript. 98 , 99
Liposomal Bupivacaine Administered as an Epidural or Peripheral Nerve Block Liposomal bupivacaine is approved by the Food and Drug Administration for use in two speci c peripheral nerve blocks: transversus abdominis plane and interscalene (exclu-sively for postoperative analgesia after shoulder surgery). However, data are available for additional anatomic locations such as the epidural space, with studies performed under investigational new drug applications. We include these published randomized, controlled trials along with those investigating currently approved applications ( tables 9 and 10 ). 29 , 139 , 154 – 167 The 16 disparate trials of this section are not easily categorized or compared due to their heterogenous
surgical procedures, experimental treatments ( e.g. , periph-eral nerve block vs. epidural), and comparison groups ( e.g. , placebo vs. liposomal bupivacaine).
Peripheral Nerve Block with Liposomal Bupivacaine versus Placebo
There are four randomized, controlled trials comparing a peripheral nerve block using liposomal bupivacaine and a placebo control. 29 , 139 , 154 , 160 The rst involved elective coro-nary artery bypass grafting through a median sternotomy and sequential intercostal nerve blocks performed through the surgical incision, as well as in ltration surrounding the mediastinal drains. 154 Although the authors designated pain scores and opioid use as primary outcomes, no time point was speci ed, warranting “ some concerns ” regarding possible bias using the Cochrane tool. At none of 10 indi-vidual time points between 0 and 72 postoperative hours was liposomal bupivacaine found to be superior to placebo. However, when overall pain scores were compared using a linear mixed-e ects model, the treatment group demon-strated lower scores ( P = 0.040). Except for the 2-h time point, the treatment group did not demonstrate a signi cant reduction in pain medication requirements either at indi-vidual time points or overall. Similarly, there were no dif-ferences in secondary outcomes such as time to extubation, hospital or intensive care unit length of stay, time to rst bowel movement, or time to return to work or daily activ-ity. Considering the comparison group was normal saline and not active unencapsulated bupivacaine, the authors concluded, “ there is currently not enough evidence to jus-tify the clinical use of this drug for this purpose. ” 154
In contrast, two other placebo-controlled trials with low risk of bias o er stronger evidence in favor of liposomal bupivacaine when administered as an ultrasound-guided femoral, or interscalene nerve block before major knee or shoulder surgery, respectively. 29 , 139 Subjects experi-enced lower pain when all scores during the rst 48 to 72 postoperative hours were evaluated together using AUC. Importantly, the windowed worst-observation-carried-for-ward technique was employed; however, the di erence between treatments remained with a post hoc analysis with-out score imputation, although the e ect size was reduced by approximately 25 to 39%. With data imputation, daily pain score AUC for the 0 to 24, 24 to 48, and 48 to 72-h periods were approximately 13 to 39% (femoral) and 26 to 51% (interscalene) lower in the treatment groups, provid-ing evidence that there is pharmacologic activity beyond 48 h. For interscalene blocks, the actual resting pain scores (not AUC) were dramatically improved for the active treat-ment — approximately 30 to 60% lower — for all three time periods, as was the opioid consumption (reduced by 66 to 86%). In contrast, bene ts for femoral blocks were far more modest, with resting pain scores and opioid consumption improved to a clinical and statistically signi cant degree only through 24 h. One important caveat is that neither
ALNV134N2_Text.indb 319ALNV134N2_Text.indb 319 29-Dec-20 19:44:2129-Dec-20 19:44:21
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
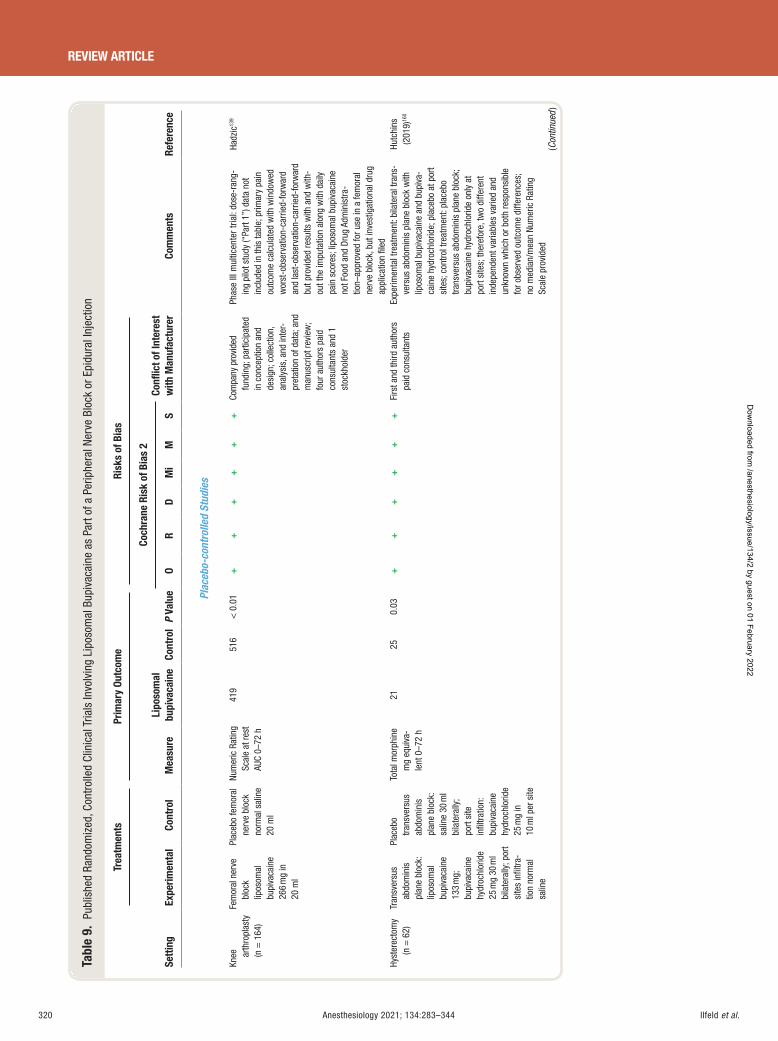
Ilfeld et al.320 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 9.
Pub
lishe
d Ra
ndom
ized
, Con
trol
led
Clin
ical
Tria
ls In
volv
ing
Lipo
som
al B
upiv
acai
ne a
s Pa
rt o
f a P
erip
hera
l Ner
ve B
lock
or E
pidu
ral I
njec
tion
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f Int
eres
t w
ith M
anuf
actu
rer
O R
D M
i M
S
Plac
ebo-
cont
rolle
d St
udie
s
Knee
ar
thro
plas
ty
(n =
164
)
Fem
oral
ner
ve
bloc
k
lipos
omal
bu
piva
cain
e 26
6 m
g in
20
ml
Plac
ebo
fem
oral
ne
rve
bloc
k no
rmal
sal
ine
20 m
l
Num
eric
Rat
ing
Scal
e at
rest
AU
C 0 –
72 h
419
516
< 0
.01
++
++
++
Com
pany
pro
vide
d fu
ndin
g; p
artic
ipat
ed
in c
once
ptio
n an
d de
sign
; col
lect
ion,
an
alys
is, a
nd in
ter-
pret
atio
n of
dat
a; a
nd
man
uscr
ipt r
evie
w;
four
aut
hors
pai
d co
nsul
tant
s an
d 1
stoc
khol
der
Phas
e III
mul
ticen
ter t
rial:
dose
-ran
g-in
g pi
lot s
tudy
( “ Pa
rt 1 ”
) dat
a no
t in
clud
ed in
this
tabl
e; p
rimar
y pa
in
outc
ome
calc
ulat
ed w
ith w
indo
wed
w
orst
-obs
erva
tion-
carr
ied-
forw
ard
and
last
-obs
erva
tion-
carr
ied-
forw
ard
but p
rovi
ded
resu
lts w
ith a
nd w
ith-
out t
he im
puta
tion
alon
g w
ith d
aily
pa
in s
core
s; li
poso
mal
bup
ivac
aine
no
t Foo
d an
d Dr
ug A
dmin
istra
-tio
n – ap
prov
ed fo
r use
in a
fem
oral
ne
rve
bloc
k, b
ut in
vest
igat
iona
l dru
g ap
plic
atio
n fi l
ed
Hadz
ic 13
9
Hyst
erec
tom
y (n
= 6
2)
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
lip
osom
al
bupi
vaca
ine
133
mg;
bu
piva
cain
e hy
droc
hlor
ide
25 m
g 30
ml
bila
tera
lly; p
ort
site
s in
fi ltra
-tio
n no
rmal
sa
line
Plac
ebo
trans
vers
us
abdo
min
is
plan
e bl
ock:
sa
line
30 m
l bi
late
rally
; po
rt si
te
infi l
tratio
n:
bupi
vaca
ine
hydr
ochl
orid
e 25
mg
in
10 m
l per
site
Tota
l mor
phin
e m
g eq
uiva
-le
nt 0
– 72
h
21
25
0.03
+
++
++
+ Fi
rst a
nd th
ird a
utho
rs
paid
con
sulta
nts
Expe
rimen
tal t
reat
men
t: bi
late
ral t
rans
-ve
rsus
abd
omin
is p
lane
blo
ck w
ith
lipos
omal
bup
ivac
aine
and
bup
iva-
cain
e hy
droc
hlor
ide;
pla
cebo
at p
ort
site
s; c
ontro
l tre
atm
ent:
plac
ebo
trans
vers
us a
bdom
inis
pla
ne b
lock
; bu
piva
cain
e hy
droc
hlor
ide
only
at
port
site
s; th
eref
ore,
two
diffe
rent
in
depe
nden
t var
iabl
es v
arie
d an
d un
know
n w
hich
or b
oth
resp
onsi
ble
for o
bser
ved
outc
ome
diffe
renc
es;
no m
edia
n/m
ean
Num
eric
Rat
ing
Scal
e pr
ovid
ed
Hutc
hins
(2
019)
160
(Con
tinue
d )
ALNV134N2_Text.indb 320ALNV134N2_Text.indb 320 29-Dec-20 19:44:2229-Dec-20 19:44:22
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
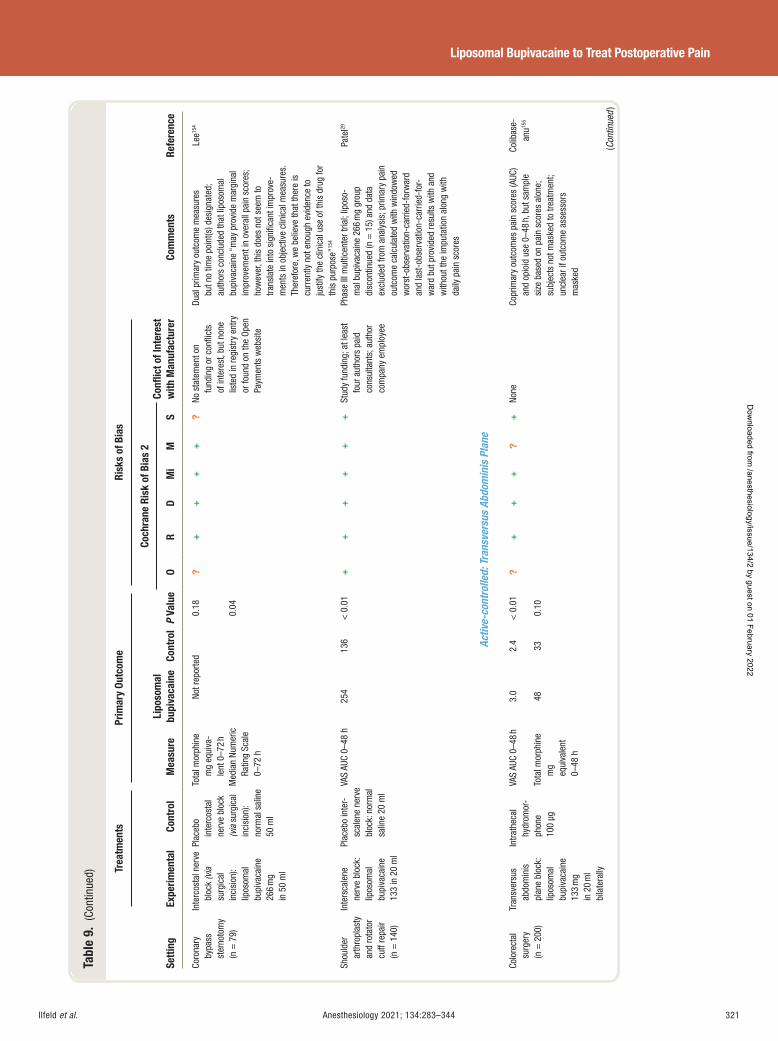
Ilfeld et al. Anesthesiology 2021; 134:283–344 321
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 9.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f Int
eres
t w
ith M
anuf
actu
rer
O R
D M
i M
S
Coro
nary
by
pass
st
erno
tom
y (n
= 7
9)
Inte
rcos
tal n
erve
bl
ock
(via
su
rgic
al
inci
sion
):
lipos
omal
bu
piva
cain
e 26
6 m
g in
50
ml
Plac
ebo
inte
rcos
tal
nerv
e bl
ock
(via
sur
gica
l in
cisi
on):
norm
al s
alin
e 50
ml
Tota
l mor
phin
e m
g eq
uiva
-le
nt 0
– 72
h
Not r
epor
ted
0.18
?
++
++
? No
sta
tem
ent o
n fu
ndin
g or
con
fl ict
s of
inte
rest
, but
non
e lis
ted
in re
gist
ry e
ntry
or
foun
d on
the
Open
Pa
ymen
ts w
ebsi
te
Dual
prim
ary
outc
ome
mea
sure
s bu
t no
time
poin
t(s) d
esig
nate
d;
auth
ors
conc
lude
d th
at li
poso
mal
bu
piva
cain
e “ m
ay p
rovi
de m
argi
nal
impr
ovem
ent i
n ov
eral
l pai
n sc
ores
; ho
wev
er, t
his
does
not
see
m to
tra
nsla
te in
to s
igni
fi can
t im
prov
e-m
ents
in o
bjec
tive
clin
ical
mea
sure
s.
Ther
efor
e, w
e be
lieve
that
ther
e is
cu
rren
tly n
ot e
noug
h ev
iden
ce to
ju
stify
the
clin
ical
use
of t
his
drug
for
this
pur
pose
” 154
Lee 15
4
Med
ian
Num
eric
Ra
ting
Scal
e 0 –
72 h
0.04
Shou
lder
ar
thro
plas
ty
and
rota
tor
cuff
repa
ir (n
= 1
40)
Inte
rsca
lene
ne
rve
bloc
k:
lipos
omal
bu
piva
cain
e 13
3 in
20
ml
Plac
ebo
inte
r-sc
alen
e ne
rve
bloc
k: n
orm
al
salin
e 20
ml
VAS
AUC
0 – 48
h
254
136
< 0
.01
++
++
++
Stud
y fu
ndin
g; a
t lea
st
four
aut
hors
pai
d co
nsul
tant
s; a
utho
r co
mpa
ny e
mpl
oyee
Phas
e III
mul
ticen
ter t
rial;
lipos
o-m
al b
upiv
acai
ne 2
66 m
g gr
oup
disc
ontin
ued
(n =
15)
and
dat
a ex
clud
ed fr
om a
naly
sis;
prim
ary
pain
ou
tcom
e ca
lcul
ated
with
win
dow
ed
wor
st-o
bser
vatio
n-ca
rrie
d-fo
rwar
d an
d la
st-o
bser
vatio
n-ca
rrie
d-fo
r-w
ard
but p
rovi
ded
resu
lts w
ith a
nd
with
out t
he im
puta
tion
alon
g w
ith
daily
pai
n sc
ores
Pate
l 29
Activ
e-co
ntro
lled:
Tra
nsve
rsus
Abd
omin
is P
lane
Colo
rect
al
surg
ery
(n =
200
)
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
lip
osom
al
bupi
vaca
ine
133
mg
in 2
0 m
l bi
late
rally
Intra
thec
al
hydr
omor
-ph
one
100
μ g
VAS
AUC
0 – 48
h
3.0
2.4
< 0
.01
?+
++
?+
None
Co
prim
ary
outc
omes
pai
n sc
ores
(AUC
) an
d op
ioid
use
0 – 4
8 h,
but
sam
ple
size
bas
ed o
n pa
in s
core
s al
one;
su
bjec
ts n
ot m
aske
d to
trea
tmen
t; un
clea
r if o
utco
me
asse
ssor
s m
aske
d
Colib
ase-
anu 15
5
Tota
l mor
phin
e m
g eq
uiva
lent
0 –
48 h
48
33
0.10
(Con
tinue
d )
ALNV134N2_Text.indb 321ALNV134N2_Text.indb 321 29-Dec-20 19:44:2229-Dec-20 19:44:22
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
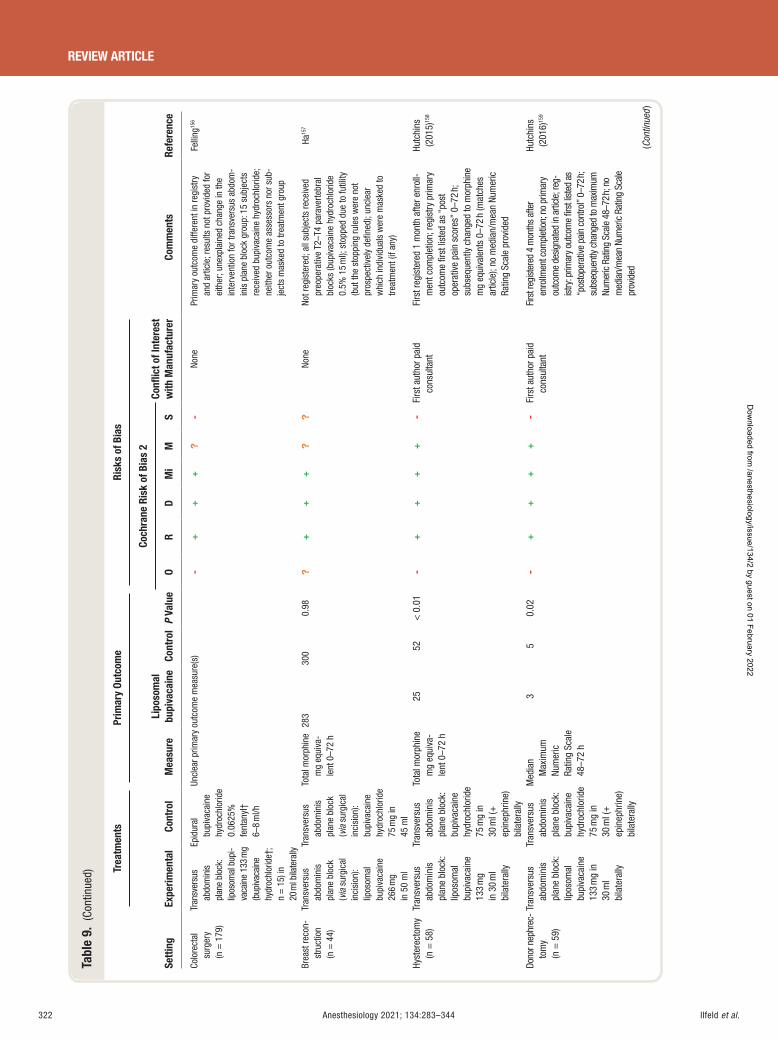
Ilfeld et al.322 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 9.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f Int
eres
t w
ith M
anuf
actu
rer
O R
D M
i M
S
Colo
rect
al
surg
ery
(n =
179
)
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
lip
osom
al b
upi-
vaca
ine
133
mg
(bup
ivac
aine
hy
droc
hlor
ide †
; n
= 1
5) in
20
ml b
ilate
rally
Epid
ural
bu
piva
cain
e hy
droc
hlor
ide
0.06
25%
fe
ntan
yl †
6 – 8
ml/h
Uncl
ear p
rimar
y ou
tcom
e m
easu
re(s
) -
++
+?
- No
ne
Prim
ary
outc
ome
diffe
rent
in re
gist
ry
and
artic
le; r
esul
ts n
ot p
rovi
ded
for
eith
er; u
nexp
lain
ed c
hang
e in
the
inte
rven
tion
for t
rans
vers
us a
bdom
-in
is p
lane
blo
ck g
roup
: 15
subj
ects
re
ceiv
ed b
upiv
acai
ne h
ydro
chlo
ride;
ne
ither
out
com
e as
sess
ors
nor s
ub-
ject
s m
aske
d to
trea
tmen
t gro
up
Felli
ng 15
6
Brea
st re
con-
stru
ctio
n (n
= 4
4)
Tran
sver
sus
abdo
min
is
plan
e bl
ock
( via
sur
gica
l in
cisi
on):
lipos
omal
bu
piva
cain
e 26
6 m
g in
50
ml
Tran
sver
sus
abdo
min
is
plan
e bl
ock
( via
sur
gica
l in
cisi
on):
bu
piva
cain
e hy
droc
hlor
ide
75 m
g in
45
ml
Tota
l mor
phin
e m
g eq
uiva
-le
nt 0
– 72
h
283
300
0.98
?
++
+?
? No
ne
Not r
egis
tere
d; a
ll su
bjec
ts re
ceiv
ed
preo
pera
tive
T2 – T
4 pa
rave
rtebr
al
bloc
ks (b
upiv
acai
ne h
ydro
chlo
ride
0.5%
15
ml);
sto
pped
due
to fu
tility
(b
ut th
e st
oppi
ng ru
les
wer
e no
t pr
ospe
ctiv
ely
defi n
ed);
uncl
ear
whi
ch in
divi
dual
s w
ere
mas
ked
to
treat
men
t (if
any)
Ha 15
7
Hyst
erec
tom
y (n
= 5
8)
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
lip
osom
al
bupi
vaca
ine
133
mg
in 3
0 m
l bi
late
rally
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
bu
piva
cain
e hy
droc
hlor
ide
75 m
g in
30
ml (
+
epin
ephr
ine)
bi
late
rally
Tota
l mor
phin
e m
g eq
uiva
-le
nt 0
– 72
h
25
52
< 0
.01
-+
++
+-
Firs
t aut
hor p
aid
cons
ulta
nt
Firs
t reg
iste
red
1 m
onth
afte
r enr
oll-
men
t com
plet
ion;
regi
stry
prim
ary
outc
ome
fi rst
list
ed a
s “ p
ost
oper
ativ
e pa
in s
core
s ” 0
– 72
h;
subs
eque
ntly
cha
nged
to m
orph
ine
mg
equi
vale
nts
0 – 72
h (m
atch
es
artic
le);
no m
edia
n/m
ean
Num
eric
Ra
ting
Scal
e pr
ovid
ed
Hutc
hins
(2
015)
158
Dono
r nep
hrec
-to
my
(n
= 5
9)
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
lip
osom
al
bupi
vaca
ine
133
mg
in
30 m
l bi
late
rally
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
bu
piva
cain
e hy
droc
hlor
ide
75 m
g in
30
ml (
+
epin
ephr
ine)
bi
late
rally
Med
ian
Max
imum
Nu
mer
ic
Ratin
g Sc
ale
48 – 7
2 h
3 5
0.02
-
++
++
- Fi
rst a
utho
r pai
d co
nsul
tant
Fi
rst r
egist
ered
4 m
onth
s af
ter
enro
llmen
t com
plet
ion;
no
prim
ary
outc
ome
desig
nate
d in
arti
cle; r
eg-
istry
: prim
ary
outc
ome
fi rst
list
ed a
s “ p
osto
pera
tive
pain
con
trol ”
0 – 72
h;
subs
eque
ntly
chan
ged
to m
axim
um
Num
eric
Rat
ing
Scal
e 48
– 72 h
; no
med
ian/
mea
n Nu
mer
ic R
atin
g Sc
ale
prov
ided
Hutc
hins
(2
016)
159
(Con
tinue
d )
ALNV134N2_Text.indb 322ALNV134N2_Text.indb 322 29-Dec-20 19:44:2229-Dec-20 19:44:22
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
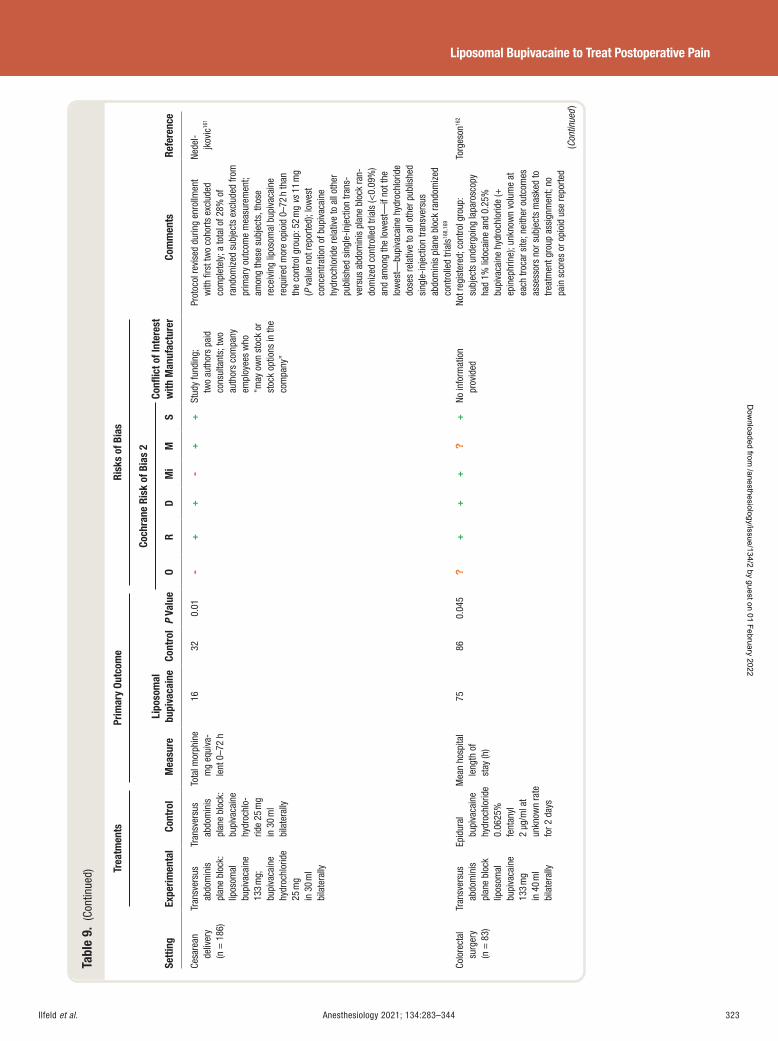
Ilfeld et al. Anesthesiology 2021; 134:283–344 323
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 9.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f Int
eres
t w
ith M
anuf
actu
rer
O R
D M
i M
S
Cesa
rean
de
liver
y (n
= 1
86)
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
lip
osom
al
bupi
vaca
ine
133
mg;
bu
piva
cain
e hy
droc
hlor
ide
25 m
g in
30
ml
bila
tera
lly
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
bu
piva
cain
e hy
droc
hlo-
ride
25 m
g in
30
ml
bila
tera
lly
Tota
l mor
phin
e m
g eq
uiva
-le
nt 0
– 72
h
16
32
0.01
-
++
-+
+ St
udy
fund
ing;
tw
o au
thor
s pa
id
cons
ulta
nts;
two
auth
ors
com
pany
em
ploy
ees
who
“ m
ay o
wn
stoc
k or
st
ock
optio
ns in
the
com
pany
”
Prot
ocol
revi
sed
durin
g en
rollm
ent
with
fi rs
t tw
o co
horts
exc
lude
d co
mpl
etel
y; a
tota
l of 2
8% o
f ra
ndom
ized
sub
ject
s ex
clud
ed fr
om
prim
ary
outc
ome
mea
sure
men
t; am
ong
thes
e su
bjec
ts, t
hose
re
ceiv
ing
lipos
omal
bup
ivac
aine
re
quire
d m
ore
opio
id 0
– 72
h th
an
the
cont
rol g
roup
: 52
mg
vs 1
1 m
g ( P
val
ue n
ot re
porte
d); l
owes
t co
ncen
tratio
n of
bup
ivac
aine
hy
droc
hlor
ide
rela
tive
to a
ll ot
her
publ
ishe
d si
ngle
-inje
ctio
n tra
ns-
vers
us a
bdom
inis
pla
ne b
lock
ran-
dom
ized
con
trolle
d tri
als
( < 0.
09%
) an
d am
ong
the
low
est —
if no
t the
lo
wes
t — bu
piva
cain
e hy
droc
hlor
ide
dose
s re
lativ
e to
all
othe
r pub
lishe
d si
ngle
-inje
ctio
n tra
nsve
rsus
ab
dom
inis
pla
ne b
lock
rand
omiz
ed
cont
rolle
d tri
als 16
8 , 16
9
Nede
l-jk
ovic
161
Colo
rect
al
surg
ery
(n =
83)
Tran
sver
sus
abdo
min
is
plan
e bl
ock
lipos
omal
bu
piva
cain
e 13
3 m
g in
40
ml
bila
tera
lly
Epid
ural
bu
piva
cain
e hy
droc
hlor
ide
0.06
25%
fe
ntan
yl
2 μ g
/ml a
t un
know
n ra
te
for 2
day
s
Mea
n ho
spita
l le
ngth
of
stay
(h)
75
86
0.04
5 ?
++
+?
+ No
info
rmat
ion
prov
ided
No
t reg
iste
red;
con
trol g
roup
: su
bjec
ts u
nder
goin
g la
paro
scop
y ha
d 1%
lido
cain
e an
d 0.
25%
bu
piva
cain
e hy
droc
hlor
ide
( +
epin
ephr
ine)
; unk
now
n vo
lum
e at
ea
ch tr
ocar
site
; nei
ther
out
com
es
asse
ssor
s no
r sub
ject
s m
aske
d to
tre
atm
ent g
roup
ass
ignm
ent;
no
pain
sco
res
or o
pioi
d us
e re
porte
d
Torg
eson
162
(Con
tinue
d )
ALNV134N2_Text.indb 323ALNV134N2_Text.indb 323 29-Dec-20 19:44:2229-Dec-20 19:44:22
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
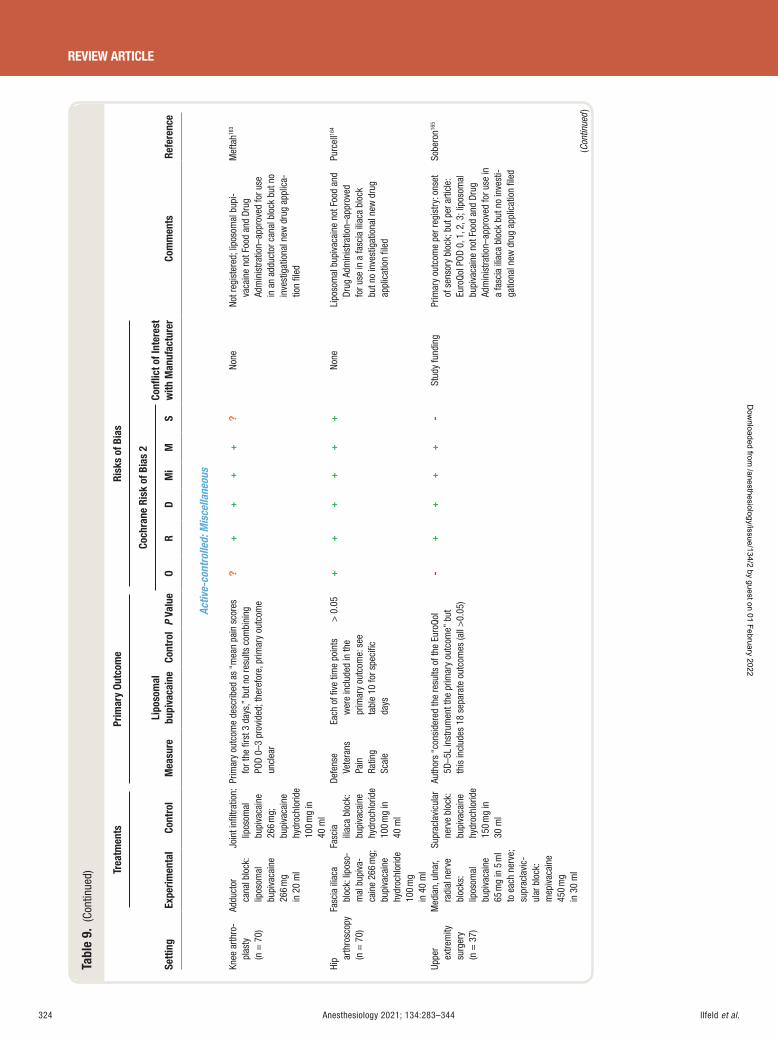
Ilfeld et al.324 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 9.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f Int
eres
t w
ith M
anuf
actu
rer
O R
D M
i M
S
Activ
e-co
ntro
lled:
Mis
cella
neou
s
Knee
arth
ro-
plas
ty
(n =
70)
Addu
ctor
ca
nal b
lock
: lip
osom
al
bupi
vaca
ine
266
mg
in 2
0 m
l
Join
t infi
ltra
tion:
lip
osom
al
bupi
vaca
ine
266
mg;
bu
piva
cain
e hy
droc
hlor
ide
100
mg
in
40 m
l
Prim
ary
outc
ome
desc
ribed
as
“ mea
n pa
in s
core
s fo
r the
fi rs
t 3 d
ays,
” bu
t no
resu
lts c
ombi
ning
PO
D 0 –
3 pr
ovid
ed; t
here
fore
, prim
ary
outc
ome
uncl
ear
?+
++
+?
None
No
t reg
iste
red;
lipo
som
al b
upi-
vaca
ine
not F
ood
and
Drug
Ad
min
istra
tion –
appr
oved
for u
se
in a
n ad
duct
or c
anal
blo
ck b
ut n
o in
vest
igat
iona
l new
dru
g ap
plic
a-tio
n fi l
ed
Mef
tah 16
3
Hip ar
thro
scop
y (n
= 7
0)
Fasc
ia il
iaca
bl
ock:
lipo
so-
mal
bup
iva-
cain
e 26
6 m
g;
bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g in
40
ml
Fasc
ia
iliac
a bl
ock:
bu
piva
cain
e hy
droc
hlor
ide
100
mg
in
40 m
l
Defe
nse
Vete
rans
Pa
in
Ratin
g Sc
ale
Each
of fi
ve
time
poin
ts
wer
e in
clud
ed in
the
prim
ary
outc
ome:
see
ta
ble
10 fo
r spe
cifi c
da
ys
> 0
.05
++
++
++
None
Li
poso
mal
bup
ivac
aine
not
Foo
d an
d Dr
ug A
dmin
istra
tion –
appr
oved
fo
r use
in a
fasc
ia il
iaca
blo
ck
but n
o in
vest
igat
iona
l new
dru
g ap
plic
atio
n fi l
ed
Purc
ell 16
4
Uppe
r ex
trem
ity
surg
ery
(n =
37)
Med
ian,
uln
ar,
radi
al n
erve
bl
ocks
: lip
osom
al
bupi
vaca
ine
65 m
g in
5 m
l to
eac
h ne
rve;
su
prac
lavi
c-ul
ar b
lock
: m
epiv
acai
ne
450
mg
in 3
0 m
l
Supr
acla
vicu
lar
nerv
e bl
ock:
bu
piva
cain
e hy
droc
hlor
ide
150
mg
in
30 m
l
Auth
ors
“ con
side
red
the
resu
lts o
f the
Eur
oQol
5D
– 5L
inst
rum
ent t
he p
rimar
y ou
tcom
e ” b
ut
this
incl
udes
18
sepa
rate
out
com
es (a
ll >
0.05
)
-+
++
+-
Stud
y fu
ndin
g Pr
imar
y ou
tcom
e pe
r reg
istr
y: o
nset
of
sen
sory
blo
ck; b
ut p
er a
rticl
e:
Euro
Qol P
OD 0
, 1, 2
, 3; l
ipos
omal
bu
piva
cain
e no
t Foo
d an
d Dr
ug
Adm
inis
tratio
n – ap
prov
ed fo
r use
in
a fa
scia
ilia
ca b
lock
but
no
inve
sti-
gatio
nal n
ew d
rug
appl
icat
ion
fi led
Sobe
ron 16
5
(Con
tinue
d )
ALNV134N2_Text.indb 324ALNV134N2_Text.indb 324 29-Dec-20 19:44:2229-Dec-20 19:44:22
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
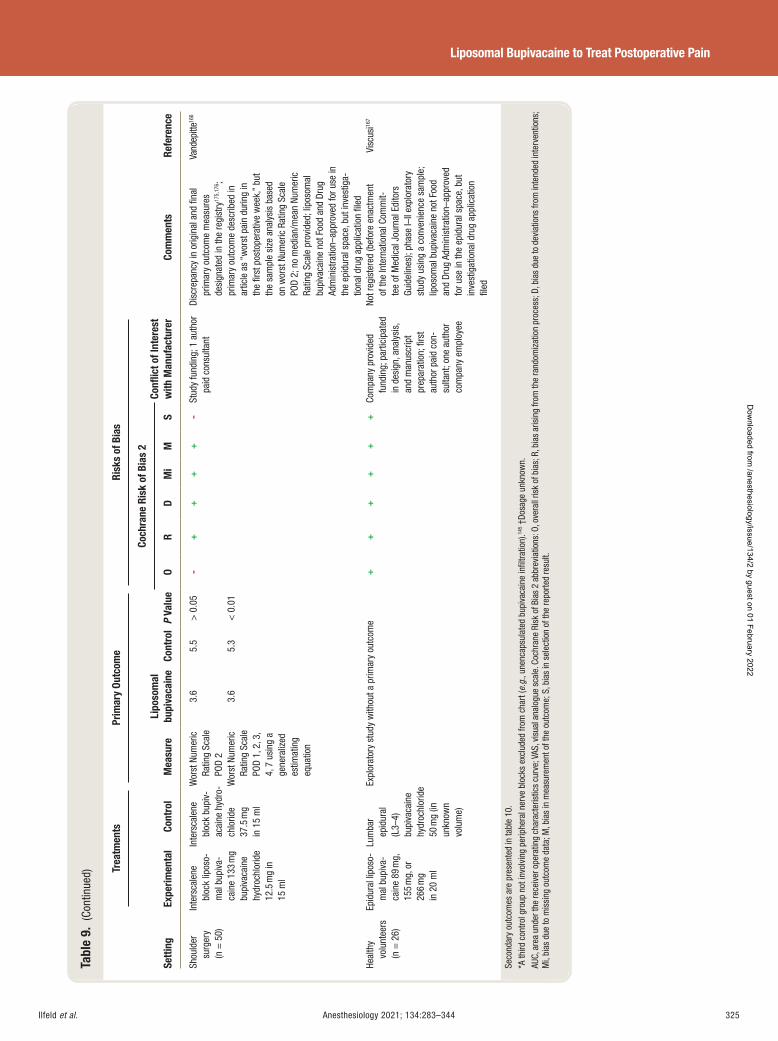
Ilfeld et al. Anesthesiology 2021; 134:283–344 325
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 9.
(Co
ntin
ued)
Setti
ng
Trea
tmen
ts
Prim
ary
Outc
ome
Risk
s of
Bia
s
Com
men
ts
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
bupi
vaca
ine
Cont
rol
P Va
lue
Coch
rane
Ris
k of
Bia
s 2
Confl
ict o
f Int
eres
t w
ith M
anuf
actu
rer
O R
D M
i M
S
Shou
lder
su
rger
y (n
= 5
0)
Inte
rsca
lene
bl
ock
lipos
o-m
al b
upiv
a-ca
ine
133
mg
bupi
vaca
ine
hydr
ochl
orid
e 12
.5 m
g in
15
ml
Inte
rsca
lene
bl
ock
bupi
v-ac
aine
hyd
ro-
chlo
ride
37.5
mg
in 1
5 m
l
Wor
st N
umer
ic
Ratin
g Sc
ale
POD
2
Wor
st N
umer
ic
Ratin
g Sc
ale
POD
1, 2
, 3,
4, 7
usi
ng a
ge
nera
lized
es
timat
ing
equa
tion
3.6
3.6
5.5
5.3
> 0
.05
< 0
.01
-+
++
+-
Stud
y fu
ndin
g; 1
aut
hor
paid
con
sulta
nt
Disc
repa
ncy
in o
rigin
al a
nd fi
nal
prim
ary
outc
ome
mea
sure
s de
sign
ated
in th
e re
gist
ry 17
5 , 17
6 ; pr
imar
y ou
tcom
e de
scrib
ed in
ar
ticle
as
“ wor
st p
ain
durin
g in
th
e fi r
st p
osto
pera
tive
wee
k, ”
but
the
sam
ple
size
ana
lysi
s ba
sed
on w
orst
Num
eric
Rat
ing
Scal
e PO
D 2;
no
med
ian/
mea
n Nu
mer
ic
Ratin
g Sc
ale
prov
ided
; lip
osom
al
bupi
vaca
ine
not F
ood
and
Drug
Ad
min
istra
tion –
appr
oved
for u
se in
th
e ep
idur
al s
pace
, but
inve
stig
a-tio
nal d
rug
appl
icat
ion
fi led
Vand
epitt
e 166
Heal
thy
volu
ntee
rs
(n =
26)
Epid
ural
lipo
so-
mal
bup
iva-
cain
e 89
mg,
15
5 m
g, o
r 26
6 m
g in
20
ml
Lum
bar
epid
ural
(L
3 – 4)
bu
piva
cain
e hy
droc
hlor
ide
50 m
g (in
un
know
n vo
lum
e)
Expl
orat
ory
stud
y w
ithou
t a p
rimar
y ou
tcom
e +
++
++
+ Co
mpa
ny p
rovi
ded
fund
ing;
par
ticip
ated
in
des
ign,
ana
lysi
s,
and
man
uscr
ipt
prep
arat
ion;
fi rs
t au
thor
pai
d co
n-su
ltant
; one
aut
hor
com
pany
em
ploy
ee
Not r
egis
tere
d (b
efor
e en
actm
ent
of th
e In
tern
atio
nal C
omm
it-te
e of
Med
ical
Jou
rnal
Edi
tors
Gu
idel
ines
); ph
ase
I – II
expl
orat
ory
stud
y us
ing
a co
nven
ienc
e sa
mpl
e;
lipos
omal
bup
ivac
aine
not
Foo
d an
d Dr
ug A
dmin
istra
tion –
appr
oved
fo
r use
in th
e ep
idur
al s
pace
, but
in
vest
igat
iona
l dru
g ap
plic
atio
n fi l
ed
Visc
usi 16
7
Seco
ndar
y ou
tcom
es a
re p
rese
nted
in ta
ble
10 .
* A th
ird c
ontro
l gro
up n
ot in
volv
ing
perip
hera
l ner
ve b
lock
s ex
clud
ed fr
om c
hart
( e.g
. , un
enca
psul
ated
bup
ivac
aine
infi l
tratio
n). 14
5 † Do
sage
unk
now
n.
AUC,
are
a un
der t
he re
ceiv
er o
pera
ting
char
acte
ristic
s cu
rve;
VAS
, vis
ual a
nalo
gue
scal
e. C
ochr
ane
Risk
of B
ias
2 ab
brev
iatio
ns: O
, ove
rall
risk
of b
ias;
R, b
ias
aris
ing
from
the
rand
omiz
atio
n pr
oces
s; D
, bia
s du
e to
dev
iatio
ns fr
om in
tend
ed in
terv
entio
ns;
Mi,
bias
due
to m
issi
ng o
utco
me
data
; M, b
ias
in m
easu
rem
ent o
f the
out
com
e; S
, bia
s in
sel
ectio
n of
the
repo
rted
resu
lt.
ALNV134N2_Text.indb 325ALNV134N2_Text.indb 325 29-Dec-20 19:44:2229-Dec-20 19:44:22
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
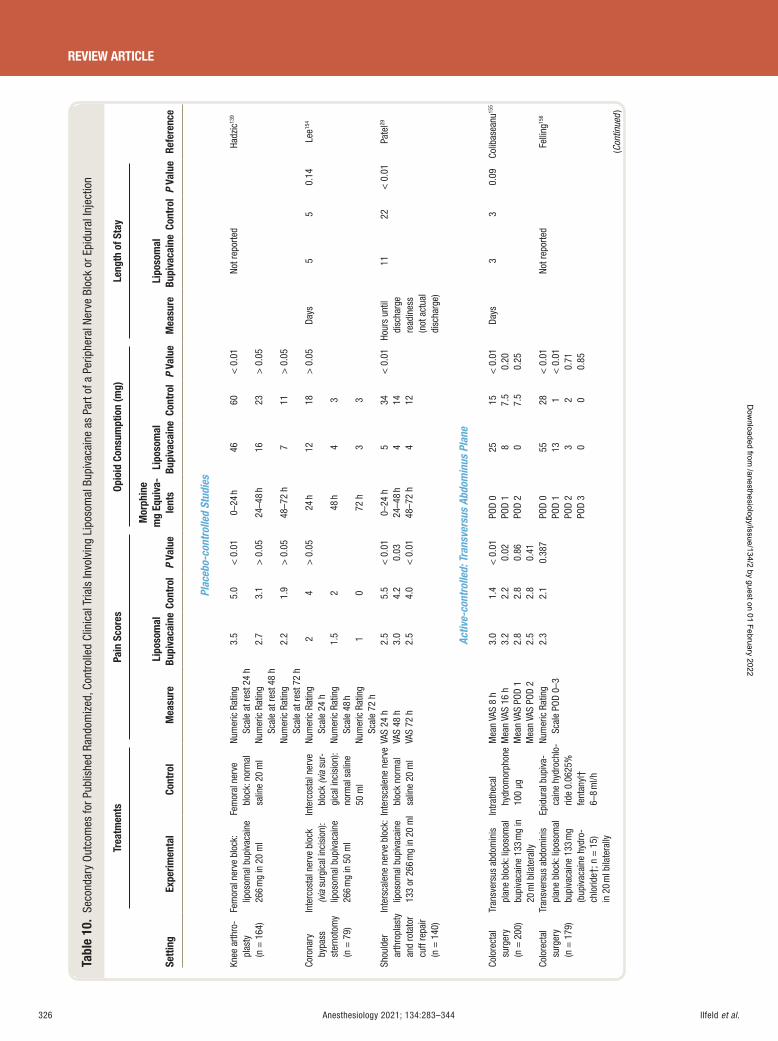
Ilfeld et al.326 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 10
. Se
cond
ary
Outc
omes
for P
ublis
hed
Rand
omiz
ed, C
ontr
olle
d Cl
inic
al T
rials
Invo
lvin
g Li
poso
mal
Bup
ivac
aine
as
Part
of a
Per
iphe
ral N
erve
Blo
ck o
r Epi
dura
l Inj
ectio
n
Setti
ng
Trea
tmen
ts
Pain
Sco
res
Opio
id C
onsu
mpt
ion
(mg)
Le
ngth
of S
tay
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mor
phin
e m
g Eq
uiva
-le
nts
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mea
sure
Li
poso
mal
Bu
piva
cain
e Co
ntro
l P
Valu
e
Plac
ebo-
cont
rolle
d St
udie
s
Knee
arth
ro-
plas
ty
(n =
164
)
Fem
oral
ner
ve b
lock
: lip
osom
al b
upiv
acai
ne
266
mg
in 2
0 m
l
Fem
oral
ner
ve
bloc
k: n
orm
al
salin
e 20
ml
Num
eric
Rat
ing
Scal
e at
rest
24
h 3.
5 5.
0 <
0.0
1 0 –
24 h
46 60
< 0
.01
Not r
epor
ted
Hadz
ic 13
9
Num
eric
Rat
ing
Scal
e at
rest
48
h 2.
7 3.
1 >
0.0
5 24
– 48
h 16
23 >
0.0
5
Num
eric
Rat
ing
Scal
e at
rest
72
h 2.
2 1.
9 >
0.0
5 48
– 72
h 7
11
> 0
.05
Coro
nary
by
pass
st
erno
tom
y (n
= 7
9)
Inte
rcos
tal n
erve
blo
ck
(via
sur
gica
l inc
isio
n):
lipos
omal
bup
ivac
aine
26
6 m
g in
50
ml
Inte
rcos
tal n
erve
bl
ock
(via
sur
-gi
cal i
ncis
ion)
: no
rmal
sal
ine
50 m
l
Num
eric
Rat
ing
Scal
e 24
h
2 4
> 0
.05
24 h
12
18
> 0
.05
Days
5
5 0.
14
Lee 15
4
Num
eric
Rat
ing
Scal
e 48
h
1.5
2 48
h 4
3
Num
eric
Rat
ing
Scal
e 72
h
1 0
72 h
3
3
Shou
lder
ar
thro
plas
ty
and
rota
tor
cuff
repa
ir (n
= 1
40)
Inte
rsca
lene
ner
ve b
lock
: lip
osom
al b
upiv
acai
ne
133
or 2
66 m
g in
20
ml In
ters
cale
ne n
erve
bl
ock
norm
al
salin
e 20
ml
VAS
24 h
2.
5 5.
5 <
0.0
1 0 –
24 h
5
34
< 0
.01
Hou
rs u
ntil
disc
harg
e re
adin
ess
(not
act
ual
disc
harg
e)
11
22
< 0
.01
Pate
l 29
VAS
48 h
3.
0 4.
2 0.
03
24 – 4
8 h
4 14
VA
S 72
h
2.5
4.0
< 0
.01
48 – 7
2 h
4 12
Activ
e-co
ntro
lled:
Tra
nsve
rsus
Abd
omin
us P
lane
Colo
rect
al
surg
ery
(n =
200
)
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
lipo
som
al
bupi
vaca
ine
133
mg
in
20 m
l bila
tera
lly
Intra
thec
al
hydr
omor
phon
e 10
0 μ g
Mea
n VA
S 8
h 3.
0 1.
4 <
0.0
1 PO
D 0
25
15
< 0
.01
Days
3
3 0.
09
Colib
asea
nu 15
5
Mea
n VA
S 16
h
3.2
2.2
0.02
PO
D 1
8 7.
5 0.
20
Mea
n VA
S PO
D 1
2.8
2.8
0.86
PO
D 2
0 7.
5 0.
25
Mea
n VA
S PO
D 2
2.5
2.8
0.41
Co
lore
ctal
su
rger
y (n
= 1
79)
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
lipo
som
al
bupi
vaca
ine
133
mg
(bup
ivac
aine
hyd
ro-
chlo
ride †
; n =
15)
in
20
ml b
ilate
rally
Epid
ural
bup
iva-
cain
e hy
droc
hlo-
ride
0.06
25%
fe
ntan
yl †
6 – 8
ml/h
Num
eric
Rat
ing
Scal
e PO
D 0 –
3 2.
3 2.
1 0.
387
POD
0 PO
D 1
POD
2 PO
D 3
55
13
3 0
28
1 2 0
< 0
.01
< 0
.01
0.71
0.
85
Not r
epor
ted
Felli
ng 15
6
(Con
tinue
d )
ALNV134N2_Text.indb 326ALNV134N2_Text.indb 326 29-Dec-20 19:44:2329-Dec-20 19:44:23
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
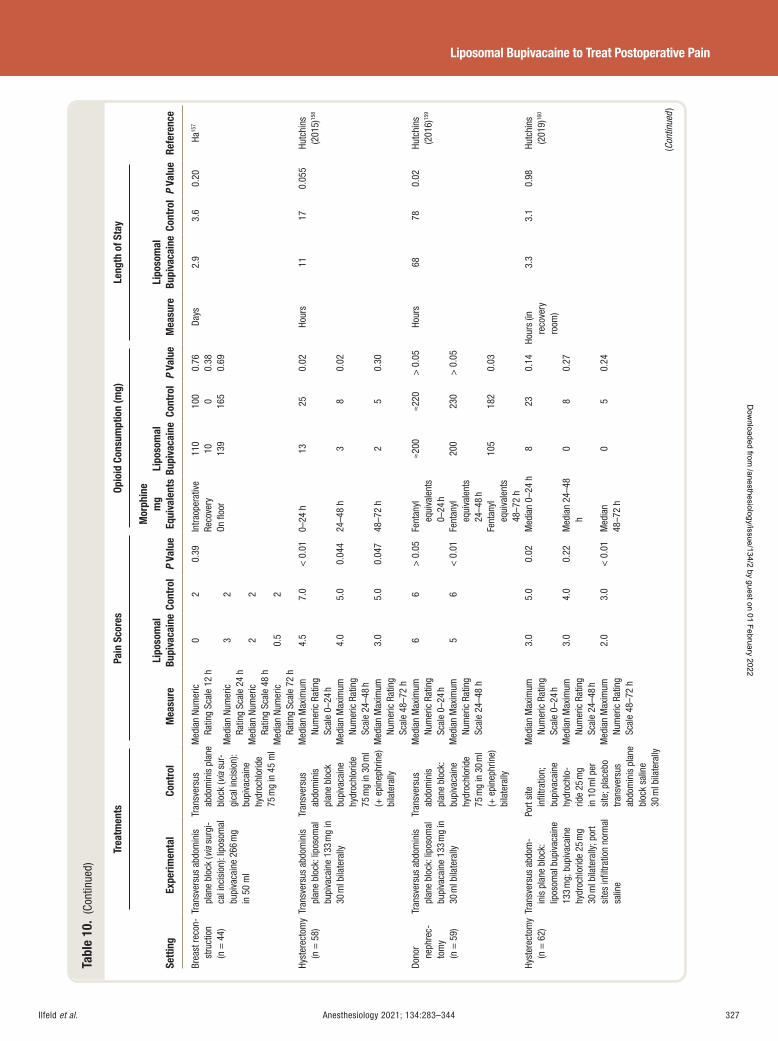
Ilfeld et al. Anesthesiology 2021; 134:283–344 327
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 10
. (C
ontin
ued)
Setti
ng
Trea
tmen
ts
Pain
Sco
res
Opio
id C
onsu
mpt
ion
(mg)
Le
ngth
of S
tay
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mor
phin
e m
g Eq
uiva
lent
s Li
poso
mal
Bu
piva
cain
e Co
ntro
l P
Valu
e M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Brea
st re
con-
stru
ctio
n (n
= 4
4)
Tran
sver
sus
abdo
min
is
plan
e bl
ock
( via
sur
gi-
cal i
ncis
ion)
: lip
osom
al
bupi
vaca
ine
266
mg
in 5
0 m
l
Tran
sver
sus
abdo
min
is p
lane
bl
ock
( via
sur
-gi
cal i
ncis
ion)
: bu
piva
cain
e hy
droc
hlor
ide
75 m
g in
45
ml
Med
ian
Num
eric
Ra
ting
Scal
e 12
h
0 2
0.39
In
traop
erat
ive
Reco
very
On
fl oo
r
110
10
139
100 0 165
0.76
0.
38
0.69
Days
2.
9 3.
6 0.
20
Ha 15
7
Med
ian
Num
eric
Ra
ting
Scal
e 24
h
3 2
Med
ian
Num
eric
Ra
ting
Scal
e 48
h
2 2
Med
ian
Num
eric
Ra
ting
Scal
e 72
h
0.5
2
Hyst
erec
tom
y (n
= 5
8)
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
lipo
som
al
bupi
vaca
ine
133
mg
in
30 m
l bila
tera
lly
Tran
sver
sus
abdo
min
is
plan
e bl
ock
bupi
vaca
ine
hydr
ochl
orid
e 75
mg
in 3
0 m
l ( +
epi
neph
rine)
bi
late
rally
Med
ian
Max
imum
Nu
mer
ic R
atin
g Sc
ale
0 – 24
h
4.5
7.0
< 0
.01
0 – 24
h
13
25
0.02
Hour
s 11
17
0.
055
Hutc
hins
(2
015)
158
Med
ian
Max
imum
Nu
mer
ic R
atin
g Sc
ale
24 – 4
8 h
4.0
5.0
0.04
4 24
– 48
h 3
8 0.
02
Med
ian
Max
imum
Nu
mer
ic R
atin
g Sc
ale
48 – 7
2 h
3.0
5.0
0.04
7 48
– 72
h 2
5 0.
30
Dono
r ne
phre
c-to
my
(n =
59)
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
lipo
som
al
bupi
vaca
ine
133
mg
in
30 m
l bila
tera
lly
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
bu
piva
cain
e hy
droc
hlor
ide
75 m
g in
30
ml
( + e
pine
phrin
e)
bila
tera
lly
Med
ian
Max
imum
Nu
mer
ic R
atin
g Sc
ale
0 – 24
h
6 6
> 0
.05
Fent
anyl
eq
uiva
lent
s 0 –
24 h
≈ 200
≈ 220
> 0
.05
Hour
s 68
78
0.
02
Hutc
hins
(2
016)
159
Med
ian
Max
imum
Nu
mer
ic R
atin
g Sc
ale
24 – 4
8 h
5 6
< 0
.01
Fent
anyl
eq
uiva
lent
s 24
– 48
h
200
230
> 0
.05
Fent
anyl
eq
uiva
lent
s 48
– 72
h
105
182
0.03
Hyst
erec
tom
y (n
= 6
2)
Tran
sver
sus
abdo
m-
inis
pla
ne b
lock
: lip
osom
al b
upiv
acai
ne
133
mg;
bup
ivac
aine
hy
droc
hlor
ide
25 m
g 30
ml b
ilate
rally
; por
t si
tes
infi l
tratio
n no
rmal
sa
line
Port
site
in
fi ltra
tion;
bu
piva
cain
e hy
droc
hlo-
ride
25 m
g in
10
ml p
er
site
; pla
cebo
tra
nsve
rsus
ab
dom
inis
pla
ne
bloc
k sa
line
30 m
l bila
tera
lly M
edia
n M
axim
um
Num
eric
Rat
ing
Scal
e 0 –
24 h
3.0
5.0
0.02
M
edia
n 0 –
24 h
8
23
0.14
Ho
urs
(in
reco
very
ro
om)
3.3
3.1
0.98
Hu
tchi
ns
(201
9) 16
0
Med
ian
Max
imum
Nu
mer
ic R
atin
g Sc
ale
24 – 4
8 h
3.0
4.0
0.22
M
edia
n 24
– 48
h 0
8 0.
27
Med
ian
Max
imum
Nu
mer
ic R
atin
g Sc
ale
48 – 7
2 h
2.0
3.0
< 0
.01
Med
ian
48 – 7
2 h
0 5
0.24
(Con
tinue
d )
ALNV134N2_Text.indb 327ALNV134N2_Text.indb 327 29-Dec-20 19:44:2329-Dec-20 19:44:23
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
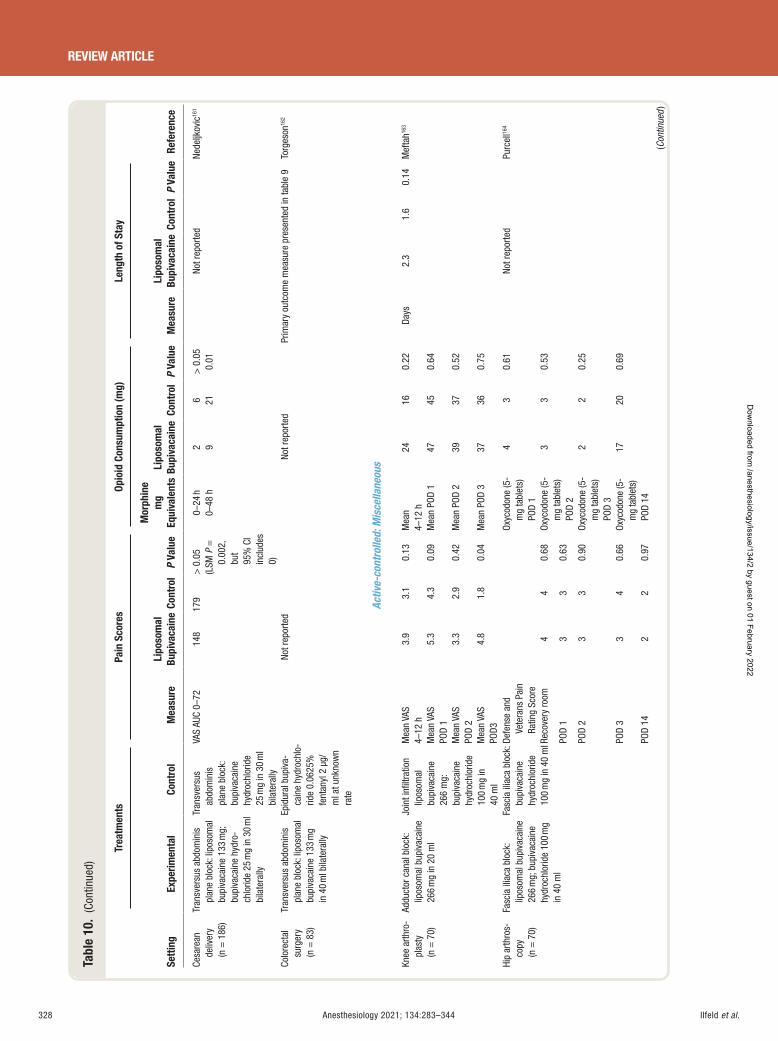
Ilfeld et al.328 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
Tabl
e 10
. (C
ontin
ued)
Setti
ng
Trea
tmen
ts
Pain
Sco
res
Opio
id C
onsu
mpt
ion
(mg)
Le
ngth
of S
tay
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mor
phin
e m
g Eq
uiva
lent
s Li
poso
mal
Bu
piva
cain
e Co
ntro
l P
Valu
e M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Cesa
rean
de
liver
y (n
= 1
86)
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
lipo
som
al
bupi
vaca
ine
133
mg;
bu
piva
cain
e hy
dro-
chlo
ride
25 m
g in
30
ml
bila
tera
lly
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
bu
piva
cain
e hy
droc
hlor
ide
25 m
g in
30
ml
bila
tera
lly
VAS
AUC
0 – 72
14
8 17
9 >
0.0
5 (L
SM P
=
0.00
2,
but
95%
CI
incl
udes
0)
0 – 24
h 0 –
48 h
2 9
6 21
> 0
.05
0.01
No
t rep
orte
d Ne
deljk
ovic
161
Colo
rect
al
surg
ery
(n =
83)
Tran
sver
sus
abdo
min
is
plan
e bl
ock:
lipo
som
al
bupi
vaca
ine
133
mg
in 4
0 m
l bila
tera
lly
Epid
ural
bup
iva-
cain
e hy
droc
hlo-
ride
0.06
25%
fe
ntan
yl 2
μ g/
ml a
t unk
now
n ra
te
Not r
epor
ted
Not r
epor
ted
Prim
ary
outc
ome
mea
sure
pre
sent
ed in
tabl
e 9
Torg
eson
162
Activ
e-co
ntro
lled:
Mis
cella
neou
s
Knee
arth
ro-
plas
ty
(n =
70)
Addu
ctor
can
al b
lock
: lip
osom
al b
upiv
acai
ne
266
mg
in 2
0 m
l
Join
t infi
ltra
tion
lipos
omal
bu
piva
cain
e 26
6 m
g:
bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g in
40
ml
Mea
n VA
S 4 –
12 h
3.
9 3.
1 0.
13 M
ean
4 – 12
h
24
16
0.22
Days
2.
3 1.
6 0.
14
Mef
tah 16
3
Mea
n VA
S PO
D 1
5.3
4.3
0.09
Mea
n PO
D 1
47
45
0.64
Mea
n VA
SPO
D 2
3.3
2.9
0.42
Mea
n PO
D 2
39
37 0.
52
Mea
n VA
S PO
D3
4.8
1.8
0.04
M
ean
POD
3 37
36
0.
75
Hip
arth
ros-
copy
(n
= 7
0)
Fasc
ia il
iaca
blo
ck:
lipos
omal
bup
ivac
aine
26
6 m
g; b
upiv
acai
ne
hydr
ochl
orid
e 10
0 m
g in
40
ml
Fasc
ia il
iaca
blo
ck:
bupi
vaca
ine
hydr
ochl
orid
e 10
0 m
g in
40
ml De
fens
e an
d Ve
tera
ns P
ain
Ratin
g Sc
ore
Oxyc
odon
e (5
-m
g ta
blet
s)
POD
1
4 3
0.61
Not r
epor
ted
Purc
ell 16
4
Reco
very
room
4
4 0.
68
Oxyc
odon
e (5
-m
g ta
blet
s)
POD
2
3 3
0.53
POD
1 3
3 0.
63
POD
2 3
3 0.
90
Oxyc
odon
e (5
-m
g ta
blet
s)
POD
3
2 2
0.25
POD
3 3
4 0.
66
Oxyc
odon
e (5
-m
g ta
blet
s)
POD
14
17
20
0.69
POD
14
2 2
0.97
(Con
tinue
d )
ALNV134N2_Text.indb 328ALNV134N2_Text.indb 328 29-Dec-20 19:44:2329-Dec-20 19:44:23
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
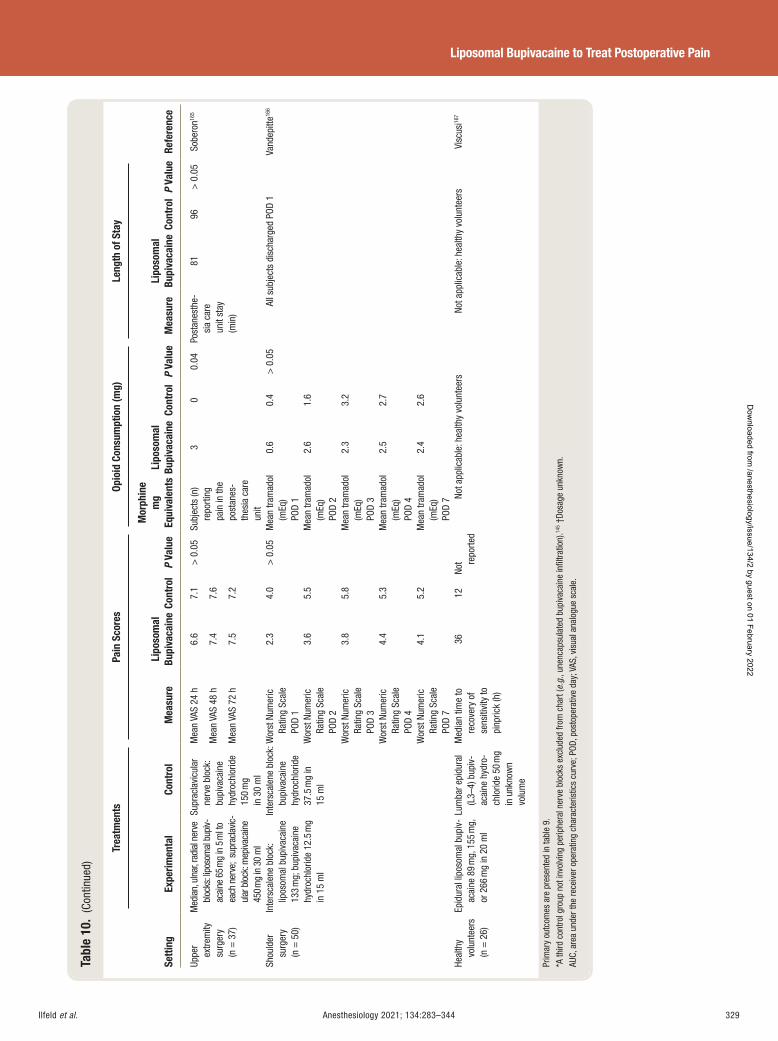
Ilfeld et al. Anesthesiology 2021; 134:283–344 329
Liposomal Bupivacaine to Treat Postoperative Pain
Tabl
e 10
. (C
ontin
ued)
Setti
ng
Trea
tmen
ts
Pain
Sco
res
Opio
id C
onsu
mpt
ion
(mg)
Le
ngth
of S
tay
Refe
renc
e Ex
perim
enta
l Co
ntro
l M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Mor
phin
e m
g Eq
uiva
lent
s Li
poso
mal
Bu
piva
cain
e Co
ntro
l P
Valu
e M
easu
re
Lipo
som
al
Bupi
vaca
ine
Cont
rol
P Va
lue
Uppe
r ex
trem
ity
surg
ery
(n
= 3
7)
Med
ian,
uln
ar, r
adia
l ner
ve
bloc
ks: li
poso
mal
bup
iv-ac
aine
65 m
g in
5 m
l to
each
ner
ve;
supr
acla
vic-
ular
blo
ck: m
epiva
cain
e 45
0 mg
in 3
0 m
l
Supr
acla
vicu
lar
nerv
e bl
ock:
bu
piva
cain
e hy
droc
hlor
ide
150
mg
in 3
0 m
l
Mea
n VA
S 24
h
6.6
7.1
> 0
.05
Subj
ects
(n)
repo
rting
pa
in in
the
post
anes
-th
esia
car
e un
it
3 0
0.04
Po
stan
esth
e-si
a ca
re
unit
stay
(m
in)
81
96
> 0
.05
Sobe
ron 16
5
Mea
n VA
S 48
h
7.4
7.6
Mea
n VA
S 72
h
7.5
7.2
Shou
lder
su
rger
y (n
= 5
0)
Inte
rsca
lene
blo
ck:
lipos
omal
bup
ivac
aine
13
3 m
g; b
upiv
acai
ne
hydr
ochl
orid
e 12
.5 m
g in
15
ml
Inte
rsca
lene
blo
ck:
bupi
vaca
ine
hydr
ochl
orid
e 37
.5 m
g in
15
ml
Wor
st N
umer
ic
Ratin
g Sc
ale
POD
1
2.3
4.0
> 0
.05
Mea
n tra
mad
ol
(mEq
) PO
D 1
0.6
0.4
> 0
.05
All s
ubje
cts
disc
harg
ed P
OD 1
Va
ndep
itte 16
6
Wor
st N
umer
ic
Ratin
g Sc
ale
POD
2
3.6
5.5
Mea
n tra
mad
ol
(mEq
) PO
D 2
2.6
1.6
Wor
st N
umer
ic
Ratin
g Sc
ale
POD
3
3.8
5.8
Mea
n tra
mad
ol
(mEq
) PO
D 3
2.3
3.2
Wor
st N
umer
ic
Ratin
g Sc
ale
POD
4
4.4
5.3
Mea
n tra
mad
ol
(mEq
) PO
D 4
2.5
2.7
Wor
st N
umer
ic
Ratin
g Sc
ale
POD
7
4.1
5.2
Mea
n tra
mad
ol
(mEq
) PO
D 7
2.4
2.6
Heal
thy
volu
ntee
rs
(n =
26)
Epid
ural
lipo
som
al b
upiv
-ac
aine
89
mg,
155
mg,
or
266
mg
in 2
0 m
l
Lum
bar e
pidu
ral
(L3 –
4) b
upiv
-ac
aine
hyd
ro-
chlo
ride
50 m
g in
unk
now
n vo
lum
e
Med
ian
time
to
reco
very
of
sens
itivi
ty to
pi
npric
k (h
)
36
12
Not re
porte
d No
t app
licab
le: h
ealth
y vo
lunt
eers
No
t app
licab
le: h
ealth
y vo
lunt
eers
Vi
scus
i 167
Prim
ary
outc
omes
are
pre
sent
ed in
tabl
e 9 .
* A
third
con
trol g
roup
not
invo
lvin
g pe
riphe
ral n
erve
blo
cks
excl
uded
from
cha
rt ( e
.g. ,
unen
caps
ulat
ed b
upiv
acai
ne in
fi ltra
tion)
. 145 †
Dosa
ge u
nkno
wn.
AU
C, a
rea
unde
r the
rece
iver
ope
ratin
g ch
arac
teris
tics
curv
e; P
OD, p
osto
pera
tive
day;
VAS
, vis
ual a
nalo
gue
scal
e.
ALNV134N2_Text.indb 329ALNV134N2_Text.indb 329 29-Dec-20 19:44:2329-Dec-20 19:44:23
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Ilfeld et al.330 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
investigation allowed unencapsulated local anesthetic in l-tration or perioperative nonsteroidal anti-in ammatory drug administration, both of which can be important com-ponents of multimodal analgesia frequently provided for major joint surgery. Regardless, these studies suggest that single-injection femoral and interscalene nerve blocks with liposomal bupivacaine have pharmacologic activity greater than 48 h when compared to placebo — far longer than would be expected for unencapsulated bupivacaine.
Somewhat less informative for liposomal bupivacaine e ectiveness is the fourth placebo-controlled study involv-ing laparoscopic hysterectomy comparing bilateral trans-versus abdominis plane with a combination of liposomal bupivacaine and bupivacaine hydrochloride to a placebo (but with port site in ltration of unencapsulated bupiv-acaine). 160 While the di erence between treatments was statistically signi cant for the primary outcome of 72-h cumulative opioid consumption, the 1.5 mg per day di er-ence suggests clinical irrelevance. However, the secondary analgesic outcomes are both statistically and clinically sig-ni cant for most of this same time period. Unfortunately, since two independent variables were varied — both the type of local anesthetic and the location of administration (trans-versus abdominis plane vs. ports) — it remains unknown if the observed outcome di erences are related to the use of liposomal bupivacaine.
Transversus Abdominis Plane Block with Liposomal Bupivacaine versus an Active Control
Of the 12 randomized, controlled trials comparing a peripheral or epidural nerve block using liposomal bupiv-acaine and an active control, seven involve the transversus abdominis plane block ( tables 9 and 10 ). 155 – 159 , 161 ,162 When the control group consisted of a transversus abdominis plane with unencapsulated bupivacaine, the results were mixed: one study involving abdominally based autologous breast reconstruction detected no statistically signi cant di erences between the two treatments, 157 while three randomized, controlled trials involving hysterectomy and donor nephrectomy reported analgesic and opioid-spar-ing bene ts of liposomal bupivacaine over unencapsulated bupivacaine. 158 , 159 , 161 Unfortunately, these last three trials were at high risk of bias: two due to registration occur-ring after enrollment completion and a change in primary outcome after the initial registration, 158 , 159 and the third resulting from protocol revisions during the enrollment period with 28% of randomized subjects excluded from the primary analysis. 161 Notably, of the 50 excluded sub-jects, total opioid consumption through 72 h was ve times higher with liposomal bupivacaine added to unencapsulated bupivacaine (52.1 mg) than with bupivacaine hydrochlo-ride alone (10.5 mg). This third study also used the low-est concentration of bupivacaine hydrochloride (less than 0.09%) and among the lowest — if not the lowest — bupiva-caine hydrochloride dose for the control group relative to
all other published single-injection transversus abdominis plane randomized, controlled trials. 168 , 169
Two of the remaining three trials involving a liposomal bupivacaine transversus abdominis plane block included an epidural infusion as the control group. 156 , 162 The rst trial involving colorectal surgery, listed di erent primary out-come measures in the registry and manuscript, lacked a power analysis for sample size, and provided a statistical plan lacking detail. 156 These factors render interpreting the study results problematic. Pain scores were collected at 11 time points during 4 days, and the registry lists three primary outcome measures as these scores on each of the rst 3 postoperative days; however, only a single unde ned pain score comparison is reported for the published article with the di erence between treatments failing to reach statistical signi cance. The investigators concluded that the two treat-ments provide “ equal ” analgesia even though superiority and not equivalence statistical tests were applied ( “ absence of proof is not proof of absence ” ). 170 In contrast, supple-mental opioid requirements for the liposomal bupivacaine transversus abdominis plane group were twice that of the epidural subjects on postoperative days 0, 1, and 0 through 3 ( P < 0.001), suggesting improved analgesia with the neuraxial technique.
The second randomized, controlled trial, also involving colorectal surgery, found that subjects with a liposomal bupi-vacaine transversus abdominis plane had a shorter hospital stay of 0.5 days (primary outcome) compared with those who received the epidural infusion for colorectal proce-dures. 162 However, interpretation is di cult as the only three secondary outcomes presented — time to atus, nausea, and urinary retention — were all negative, and no pain scores or opioid consumption were recorded. Therefore, the reason for the shorter hospitalization remains unclear. These two trials fail to bring much clarity to the issue. An unpublished, multicenter (n = 493), prospectively registered randomized, controlled trial (NCT02996227) found that after abdominal surgery, subjects with a liposomal bupivacaine transversus abdominis plane experienced noninferior analgesia com-pared with the epidural group, but required more opioids to achieve this level of pain control (principal investigator, Alparslan Turan, M.D.; presentation, American Society of Anesthesiologists 2019 by Barak Cohen, M.D.). Full publi-cation of these results will add meaningfully to this literature.
The nal randomized, controlled trial comparing lipo-somal bupivacaine transversus abdominis plane to intrathe-cal hydromorphone for colorectal procedures demonstrated lower pain scores and opioid requirements for control subjects with intrathecal hydromorphone during the rst 48 postoperative hours. 155 However, when discrete time periods were compared, di erences were detected solely during the anticipated duration of the intrathecal opioid of approximately 12 to 16 h. 171 Secondary outcomes such as the duration of hospital stay and postoperative ileus were negative with the exception of cost, which was consistently
ALNV134N2_Text.indb 330ALNV134N2_Text.indb 330 29-Dec-20 19:44:2329-Dec-20 19:44:23
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Ilfeld et al. Anesthesiology 2021; 134:283–344 331
Liposomal Bupivacaine to Treat Postoperative Pain
higher in the liposomal bupivacaine transversus abdominis plane group.
Non – Transversus Abdominis Plane Peripheral Nerve Blocks with Liposomal Bupivacaine versus an Active Control
Five remaining randomized, controlled trials involve di er-ent surgical procedures, interventions, control groups, and primary outcomes ( tables 9 and 10 ). 163 – 167 Three of these do not provide actionable information regarding liposo-mal bupivacaine when used in a peripheral nerve block, all for di erent reasons. 163 – 165 The rst compared liposomal bupivacaine as part of an adductor canal nerve block and liposomal bupivacaine in ltrated directly into the joint for knee arthroplasty, revealing essentially no di erences in analgesia or opioid consumption. 163 Since both treatment groups included liposomal bupivacaine, the results do not provide information on liposomal bupivacaine versus unen-capsulated local anesthetic. A second trial found no anal-gesic or opioid requirement di erences between liposomal bupivacaine and unencapsulated bupivacaine when used in a fascia iliaca block for hip arthroplasty. 164 Unfortunately, as noted previously, placebo-controlled clinical trials demon-strate that this peripheral nerve block provides poor, if any, analgesia for hip arthroplasty, 150 , 151 and consequently, the results of this study are not particularly enlightening . 172
A third investigation randomized subjects having upper extremity orthopedic surgery to either three forearm nerve blocks (median, ulnar, radial) followed by a supraclavicular block with mepivacaine, or a single supraclavicular block with unencapsulated bupivacaine. 165 Interpreting the results is di cult since the investigators varied two independent variables (block location and local anesthetic type), so it remains unknown to what to attribute the few di erences detected between treatments.
A fourth investigation involved subjects having major shoulder surgery who all received an interscalene block with bupivacaine hydrochloride and were then randomly administered either liposomal bupivacaine or additional bupivacaine hydrochloride. 166 Interpreting the results is dif- cult due to an unclear primary outcome measure. Within the text of the published article, the primary outcome is speci ed as the worst pain queried on postoperative day 2 (for the previous 24 h) with a matching sample size esti-mate — and the di erence between treatments was not sta-tistically signi cant for this endpoint. In contrast, the article abstract states the primary outcome as the worst pain during the entire rst postoperative week. 173 , 174 Unfortunately, the prospective registration does not help resolve this issue due to a registry – publication discrepancy. 175 , 176 Average/median pain scores and opioid consumption were not presented, and the two groups did not di er to a statistically signi cant degree in daily worst pain scores, overall bene t of anal-gesic scores, and cumulative supplemental analgesic con-sumption. However, chi-square tests of worst pain scores
and overall bene t of analgesic scores across all time points (postoperative days 1 to 7) based on generalized estimating equations were statistically signi cant. Unfortunately, no hierarchical or alpha-spending testing strategy was prespec-i ed to control type I error across outcomes, time points, and the generalized estimating equations chi-square tests. A Bonferroni correction was used to adjust P values for the ve time points within an outcome, but the chi-square test was not corrected. The P values for generalized esti-mating equations t tests applied at each time point were not reported. Combined, all of these issues decrease con -dence in the conclusion that adding liposomal bupivacaine to unencapsulated bupivacaine single-injection interscalene nerve blocks resulted in clinical bene ts. Of additional con-cern, a retrospective study of 352 patients who received liposomal bupivacaine as part of an interscalene nerve block for ambulatory shoulder surgery found that 12% returned to the emergency department due to dyspnea. 177
Epidural Administration
In preclinical studies, liposomal bupivacaine exhibited no toxicity when administered in the epidural space of both rats and dogs. 178 The only published clinical trial involved 26 volunteers given a single 20-ml injection into the lum-bar epidural space consisting of liposomal bupivacaine (89, 155, or 266 mg) or bupivacaine hydrochloride (50 mg). 167
Due to the relatively small number of subjects in each treat-ment group of this phase I study, no statistics were applied to the collected data. Nevertheless, the results of this pilot study strongly suggest a dramatic increase in analgesia dura-tion: median time until recovery of pinprick sensation was 11 h for unencapsulated bupivacaine, compared with 35 h for liposomal bupivacaine (all doses combined). In contrast, 100% of those receiving bupivacaine hydrochloride had some degree of motor block compared with only 57% for the liposomal bupivacaine group. This left 67% of those in the unencapsulated bupivacaine group unable to ambulate after 4 h versus only 39% for those who had received lipo-somal bupivacaine. There were no serious adverse events. It is emphasized that Exparel is not currently approved for use in the epidural space, and although promising, must be considered experimental at this time.
Summary
A succinct summary of the evidence for the use of liposomal bupivacaine within an epidural or peripheral nerve block is challenging due to the heterogeneity of the 16 published randomized, controlled trials ( tables 9 and 10 ). 29 , 139 , 154 – 167
The four placebo-controlled trials provide evidence of pharmacologic e ects for more than 48 h, although clinical bene t was often limited to 24 h. 139 , 154 Based on seven ran-domized, controlled trials — four with a high risk of bias and the remaining three with “ some concerns ” regarding bias — the evidence is mixed regarding the bene ts of liposomal
ALNV134N2_Text.indb 331ALNV134N2_Text.indb 331 29-Dec-20 19:44:2329-Dec-20 19:44:23
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Ilfeld et al.332 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
bupivacaine over unencapsulated bupivacaine in transver-sus abdominis plane blocks, possibly due to various surgical applications or administration protocols. 155 – 159 , 161 ,162 While the limited data suggest that epidural and intrathecal opi-oids provide superior analgesia and/or are opioid-sparing compared with liposomal bupivacaine transversus abdom-inis planes, they may also prolong hospitalization, induce hypotension, and increase overall costs. 155 , 156 , 162 Although four randomized, active-controlled trials involve using lipo-somal bupivacaine as part of a peripheral nerve other than a transversus abdominis plane block, three provide minimal useful data for various reasons, 163 – 165 and interpreting the fourth is problematic. 166 Thus, there are currently insu -cient data to conclusively support or refute the use of lipo-somal bupivacaine administered as a peripheral nerve block. Last, a single injection of liposomal bupivacaine into the epidural space more than tripled the duration of sensory e ects to skin testing while greatly decreasing any motor block in a small cohort of healthy volunteers. 167
Randomized versus Retrospective Data Discrepancies Sustained released local anesthetic o ers the possibility of prolonging postoperative analgesia beyond the normal duration of unencapsulated bupivacaine. Since liposomal bupivacaine may be detected within the serum more than twice as long as bupivacaine hydrochloride, 31 the ndings suggesting liposomal bupivacaine bene ts reported in early cohort and case-control studies appeared reasonable — even obvious. 55 – 78 However, the strength of evidence for clini-cal e ectiveness provided by randomized, controlled trials far surpasses that of nonexperimental study designs, and there are now more than 76 published experimental inves-tigations. As detailed in this review, the preponderance of high-quality evidence fails to support the retrospective data: when liposomal bupivacaine and unencapsulated local anesthetic were in ltrated directly into a surgical site, only four of 36 randomized, controlled trials (11%) were positive for their primary outcome to a clinically relevant degree. Indeed, recent meta-analyses that included exclu-sively randomized studies universally concur 3 – 7 — in contrast to meta-analyses that included retrospective investigations and universally reported liposomal bupivacaine superior-ity. 179 – 185 The overwhelming majority of randomized, con-trolled trials failed to demonstrate liposomal bupivacaine superiority even though the dose of liposomal bupivacaine was almost always maximized, while that of the comparator was rarely optimized. Even when compared to a placebo, in ltration with liposomal bupivacaine improved e ects in only a minority of randomized, controlled trials (42%).
We can only speculate on possible reasons for these unexpected ndings where most randomized, controlled trials did not support the positive e ects of liposomal bupi-vacaine suggested in retrospective studies. It may be that while bupivacaine hydrochloride is slowly released from
the liposomes and detectable in serum over a prolonged duration, the concentration of local anesthetic at the tar-get nerves is often subtherapeutic. Evidence for this may be found in the lower potency of liposomal bupivacaine: unlike bupivacaine hydrochloride, encapsulated bupiva-caine will not provide a surgical block, 186 and for this rea-son, the manufacturer recommends “ the ability to admix long-acting liposomal bupivacaine with immediate-release bupivacaine [which] can help ensure rapid onset of pain relief that spans both the acute and later postsurgical peri-ods. ” 135 Just as clinical e ects are limited to less than 18 h after administration of unencapsulated bupivacaine — even though this medication may be detected in the serum for two to three times this duration — so too might the clinical e ects of liposomal bupivacaine be limited to far less time than serum concentration might suggest. 139
Risk of Bias Of the 76 clinical trials included in this review, the Cochrane risk-of-bias tool identi ed 19 (25%) with a high overall risk of bias. 98 , 99 It is notable that of the 19 deemed at high risk for bias, 84% (16) reported statistically signi cant di er-ences for their primary outcome measure(s) compared with only 14% (4) of the 28 trials with a low risk of bias ( g. 2 ). Multiple factors accounted for trials with a high risk of bias. The most common was a lack of a prospectively designated or inadequately de ned primary outcome measure, which increases the risk of selective reporting. This was one of the primary reasons for requiring prospective registration, 187
which 29 (38%) lacked within this review. Few of the 76 randomized, controlled trials had a prospectively deter-mined plan for statistical analysis, which can greatly increase the risk of bias due to so-called “ data torturing. ” 188 Even with a prospective analytic plan, deviations can dramatically a ect the results, as evidenced by one trial involving in ltra-tion for knee arthroplasty reporting superiority of liposo-mal bupivacaine, when no statistically signi cant di erence would exist had the original published statistical plan been followed. 130 , 140 Similarly, selectively removing randomized subjects can alter study results, avoidance of which is the purpose of intention-to-treat analysis ( “ once randomized, always randomized ” ). For example, one randomized, con-trolled trial reported superiority of liposomal bupivacaine added to unencapsulated bupivacaine over bupivacaine hydrochloride alone within postcesarean delivery transver-sus abdominis plane blocks. 161 However, the protocol had multiple revisions during enrollment and excluded 28% of randomized subjects from the nal analysis. 161 Of the 50 excluded participants, total opioid consumption through 72 h was ve times higher with liposomal bupivacaine added to unencapsulated bupivacaine (52.1 mg) than with bupiva-caine hydrochloride alone (10.5 mg). 161
Explicitly excluded from the Cochrane bias tool is industry funding. It has been demonstrated that “ drug and device studies sponsored by manufacturing companies have
ALNV134N2_Text.indb 332ALNV134N2_Text.indb 332 29-Dec-20 19:44:2429-Dec-20 19:44:24
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
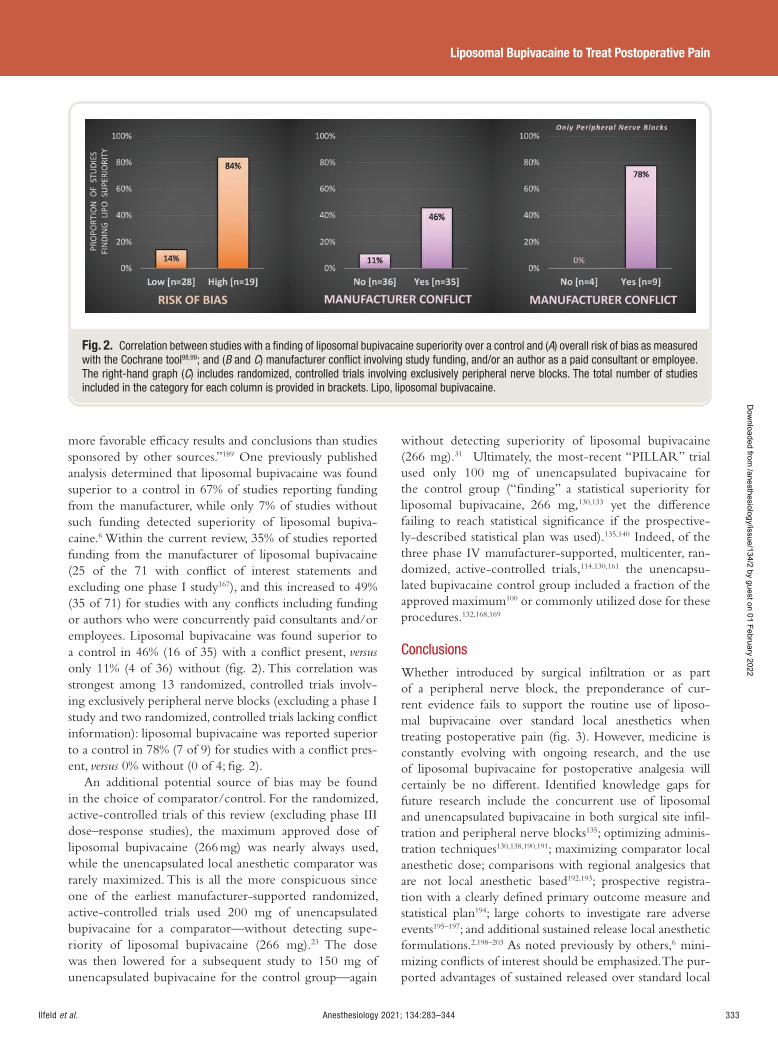
Ilfeld et al. Anesthesiology 2021; 134:283–344 333
Liposomal Bupivacaine to Treat Postoperative Pain
more favorable e cacy results and conclusions than studies sponsored by other sources. ” 189 One previously published analysis determined that liposomal bupivacaine was found superior to a control in 67% of studies reporting funding from the manufacturer, while only 7% of studies without such funding detected superiority of liposomal bupiva-caine. 6 Within the current review, 35% of studies reported funding from the manufacturer of liposomal bupivacaine (25 of the 71 with con ict of interest statements and excluding one phase I study 167 ), and this increased to 49% (35 of 71) for studies with any con icts including funding or authors who were concurrently paid consultants and/or employees. Liposomal bupivacaine was found superior to a control in 46% (16 of 35) with a con ict present, versus only 11% (4 of 36) without ( g. 2 ). This correlation was strongest among 13 randomized, controlled trials involv-ing exclusively peripheral nerve blocks (excluding a phase I study and two randomized, controlled trials lacking con ict information): liposomal bupivacaine was reported superior to a control in 78% (7 of 9) for studies with a con ict pres-ent, versus 0% without (0 of 4; g. 2 ).
An additional potential source of bias may be found in the choice of comparator/control. For the randomized, active-controlled trials of this review (excluding phase III dose – response studies), the maximum approved dose of liposomal bupivacaine (266 mg) was nearly always used, while the unencapsulated local anesthetic comparator was rarely maximized. This is all the more conspicuous since one of the earliest manufacturer-supported randomized, active-controlled trials used 200 mg of unencapsulated bupivacaine for a comparator—without detecting supe-riority of liposomal bupivacaine (266 mg). 23 The dose was then lowered for a subsequent study to 150 mg of unencapsulated bupivacaine for the control group—again
without detecting superiority of liposomal bupivacaine (266 mg). 31 Ultimately, the most-recent “PILLAR” trial used only 100 mg of unencapsulated bupivacaine for the control group (“ nding” a statistical superiority for liposomal bupivacaine, 266 mg, 130,133 yet the di erence failing to reach statistical signi cance if the prospective-ly-described statistical plan was used). 135,140 Indeed, of the three phase IV manufacturer-supported, multicenter, ran-domized, active-controlled trials, 114 , 130 , 161 the unencapsu-lated bupivacaine control group included a fraction of the approved maximum 100 or commonly utilized dose for these procedures. 132 , 168 , 169
Conclusions
Whether introduced by surgical in ltration or as part of a peripheral nerve block, the preponderance of cur-rent evidence fails to support the routine use of liposo-mal bupivacaine over standard local anesthetics when treating postoperative pain ( g. 3 ). However, medicine is constantly evolving with ongoing research, and the use of liposomal bupivacaine for postoperative analgesia will certainly be no di erent. Identi ed knowledge gaps for future research include the concurrent use of liposomal and unencapsulated bupivacaine in both surgical site in l-tration and peripheral nerve blocks 135 ; optimizing adminis-tration techniques 130 , 138 , 190 , 191 ; maximizing comparator local anesthetic dose; comparisons with regional analgesics that are not local anesthetic based 192 , 193 ; prospective registra-tion with a clearly de ned primary outcome measure and statistical plan 194 ; large cohorts to investigate rare adverse events 195 – 197 ; and additional sustained release local anesthetic formulations. 2 , 198 – 203 As noted previously by others, 6 mini-mizing con icts of interest should be emphasized. The pur-ported advantages of sustained released over standard local
Fig. 2. Correlation between studies with a fi nding of liposomal bupivacaine superiority over a control and ( A ) overall risk of bias as measured with the Cochrane tool 98 , 99 ; and ( B and C ) manufacturer confl ict involving study funding, and/or an author as a paid consultant or employee. The right-hand graph ( C ) includes randomized, controlled trials involving exclusively peripheral nerve blocks. The total number of studies included in the category for each column is provided in brackets. Lipo, liposomal bupivacaine.
ALNV134N2_Text.indb 333ALNV134N2_Text.indb 333 29-Dec-20 19:44:2429-Dec-20 19:44:24
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
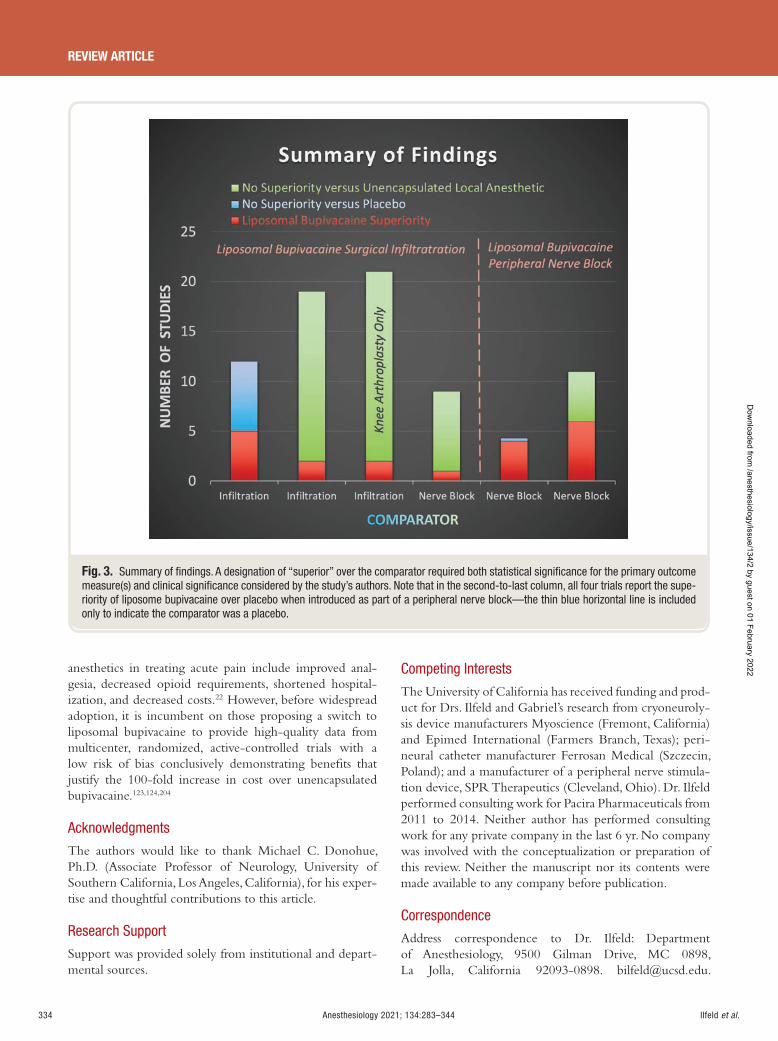
Ilfeld et al.334 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
anesthetics in treating acute pain include improved anal-gesia, decreased opioid requirements, shortened hospital-ization, and decreased costs. 22 However, before widespread adoption, it is incumbent on those proposing a switch to liposomal bupivacaine to provide high-quality data from multicenter, randomized, active-controlled trials with a low risk of bias conclusively demonstrating bene ts that justify the 100-fold increase in cost over unencapsulated bupivacaine. 123 , 124 , 204
Acknowledgments
The authors would like to thank Michael C. Donohue, Ph.D. (Associate Professor of Neurology, University of Southern California, Los Angeles, California), for his exper-tise and thoughtful contributions to this article.
Research Support
Support was provided solely from institutional and depart-mental sources.
Competing Interests
The University of California has received funding and prod-uct for Drs. Ilfeld and Gabriel ’ s research from cryoneuroly-sis device manufacturers Myoscience (Fremont, California) and Epimed International (Farmers Branch, Texas); peri-neural catheter manufacturer Ferrosan Medical (Szczecin, Poland); and a manufacturer of a peripheral nerve stimula-tion device, SPR Therapeutics (Cleveland, Ohio). Dr. Ilfeld performed consulting work for Pacira Pharmaceuticals from 2011 to 2014. Neither author has performed consulting work for any private company in the last 6 yr. No company was involved with the conceptualization or preparation of this review. Neither the manuscript nor its contents were made available to any company before publication.
Correspondence
Address correspondence to Dr. Ilfeld: Department of Anesthesiology, 9500 Gilman Drive, MC 0898, La Jolla, California 92093-0898. [email protected] .
Fig. 3. Summary of fi ndings. A designation of “ superior ” over the comparator required both statistical signifi cance for the primary outcome measure(s) and clinical signifi cance considered by the study ’ s authors. Note that in the second-to-last column, all four trials report the supe-riority of liposome bupivacaine over placebo when introduced as part of a peripheral nerve block — the thin blue horizontal line is included only to indicate the comparator was a placebo.
ALNV134N2_Text.indb 334ALNV134N2_Text.indb 334 29-Dec-20 19:44:2529-Dec-20 19:44:25
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Ilfeld et al. Anesthesiology 2021; 134:283–344 335
Liposomal Bupivacaine to Treat Postoperative Pain
Anesthesiology’s articles are made freely accessible to all readers on www.anesthesiology.org, for personal use only, 6 months from the cover date of the issue.
References
1. Ilfeld BM : Continuous peripheral nerve blocks: An update of the published evidence and comparison with novel, alternative analgesic modalities. Anesth Analg 2017 ; 124 : 308 – 35
2. Viscusi E , Gimbel JS , Pollack RA , Hu J , Lee GC : HTX-011 reduced pain intensity and opioid consumption versus bupivacaine HCl in bunionectomy: Phase III results from the randomized EPOCH 1 study. Reg Anesth Pain Med 2019
3. Hamilton TW , Athanassoglou V , Trivella M , Strickland LH , Mellon S , Murray D , Pandit HG : Liposomal bupi-vacaine peripheral nerve block for the management of postoperative pain. Cochrane Database Syst Rev 2016 : CD011476
4. Hamilton TW , Athanassoglou V , Mellon S , Strickland LH , Trivella M , Murray D , Pandit HG : Liposomal bupi-vacaine in ltration at the surgical site for the manage-ment of postoperative pain. Cochrane Database Syst Rev 2017 ; 2 : CD011419
5. Kolade O , Patel K , Ihejirika R , Press D , Friedlander S , Roberts T , Rokito AS , Virk MS : E cacy of lipo-somal bupivacaine in shoulder surgery: A systematic review and meta-analysis. J Shoulder Elbow Surg 2019 ; 28 : 1824 – 34
6. Abildgaard JT , Chung AS , Tokish JM , Hattrup SJ : Clinical e cacy of liposomal bupivacaine: A systematic review of prospective, randomized controlled trials in orthopaedic surgery. JBJS Rev 2019 ; 7 : e8
7. Kendall MC , Castro Alves LJ , De Oliveira G Jr : Liposome bupivacaine compared to plain local anes-thetics to reduce postsurgical pain: An updated meta-analysis of randomized controlled trials. Pain Res Treat 2018 ; 2018 : 5710169
8. Grant GJ , Bansinath M : Liposomal delivery systems for local anesthetics. Reg Anesth Pain Med 2001 ; 26 : 61 – 3
9. Viscusi ER : Liposomal drug delivery for postopera-tive pain management. Reg Anesth Pain Med 2005 ; 30 : 491 – 6
10. Kim S , Turker MS , Chi EY , Sela S , Martin GM : Preparation of multivesicular liposomes. Biochim Biophys Acta 1983 ; 728 : 339 – 48
11. Bangham AD , Standish MM , Miller N : Cation perme-ability of phospholipid model membranes: E ect of narcotics. Nature 1965 ; 208 : 1295 – 7
12. Viscusi ER , Martin G , Hartrick CT , Singla N , Manvelian G ; EREM Study Group : Forty-eight hours of postoperative pain relief after total hip arthroplasty with a novel, extended-release epidural morphine for-mulation. A nesthesiology 2005 ; 102 : 1014 – 22
13. Gambling D , Hughes T , Martin G , Horton W , Manvelian G : A comparison of Depodur, a novel, single-dose extended-release epidural morphine, with standard epidural morphine for pain relief after lower abdominal surgery. Anesth Analg 2005 ; 100 : 1065 – 74
14. Carvalho B , Riley E , Cohen SE , Gambling D , Palmer C , Hu nagle HJ , Polley L , Muir H , Segal S , Lihou C , Manvelian G ; DepoSur Study Group : Single-dose, sus-tained-release epidural morphine in the management of postoperative pain after elective cesarean delivery: Results of a multicenter randomized controlled study. Anesth Analg 2005 ; 100 : 1150 – 8
15. Caride V , Twickler J , Zaret B : Liposomes as carriers of cardioactive drugs: Factors a ecting incorporation of lidocaine and propranolol. Circulation 1979 ; 60 : 200
16. Okano T , Haga M , Watanabe Y , Yoshimura K : [Duration of the local anesthetic action of dibucaine by liposomes and its mechanism (author ’ s transl)]. Yakugaku Zasshi 1980 ; 100 : 1097 – 103
17. Gesztes A , Mezei M : Topical anesthesia of the skin by liposome-encapsulated tetracaine. Anesth Analg 1988 ; 67 : 1079 – 81
18. Boogaerts JG , Lafont ND , Declercq AG , Luo HC , Gravet ET , Bianchi JA , Legros FJ : Epidural adminis-tration of liposome-associated bupivacaine for the management of postsurgical pain: A rst study. J Clin Anesth 1994 ; 6 : 315 – 20
19. Rose JS , Neal JM , Kopacz DJ : Extended-duration analgesia: Update on microspheres and liposomes. Reg Anesth Pain Med 2005 ; 30 : 275 – 85
20. Bupivacaine liposomal injection (Exparel) for post sur-gical pain. Med Lett Drugs Ther 2012 ; 54 : 26 – 7
21. Charous MT , Ilfeld BM : Liposome bupivacaine for postoperative analgesia: One formulation approved for clinical use within the United States. Curr Anesthesiol Rep 2015 ; 5 : 235 – 42
22. Ilfeld BM : Liposomal bupivacaine: Its role in regional anesthesia and postoperative analgesia. Advances in Anesthesia 2014 ; 32 : 133 – 47
23. Bergese SD , Ramamoorthy S , Patou G , Bramlett K , Gor ne SR , Candiotti KA : E cacy pro le of lipo-some bupivacaine, a novel formulation of bupivacaine for postsurgical analgesia. J Pain Res 2012 ; 5 : 107 – 16
24. Saraghi M , Hersh EV : Three newly approved analge-sics: An update. Anesth Prog 2013 ; 60 : 178 – 87
25. Richard BM , Rickert DE , Doolittle D , Mize A , Liu J , Lawson CF : Pharmacokinetic compatibility study of lidocaine with EXPAREL in Yucatan miniature pigs. ISRN Pharm 2011 ; 2011 : 582351
26. Buys MJ , Murphy MF , Warrick CM , Pace NL , Gililland JM , Pelt CE , Bankhead BR , Patzkowsky JL , Johnson KB : Serum bupivacaine concentration after periartic-ular injection with a mixture of liposomal bupivacaine
ALNV134N2_Text.indb 335ALNV134N2_Text.indb 335 29-Dec-20 19:44:2529-Dec-20 19:44:25
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Ilfeld et al.336 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
and bupivacaine HCl during total knee arthroplasty. Reg Anesth Pain Med 2017 ; 42 : 582 – 7
27. Hu D , Onel E , Singla N , Kramer WG , Hadzic A : Pharmacokinetic pro le of liposome bupivacaine injection following a single administration at the surgi-cal site. Clin Drug Investig 2013 ; 33 : 109 – 15
28. Apselo G , Onel E , Patou G : Time to onset of analge-sia following local in ltration of liposome bupivacaine in healthy volunteers: A randomized, single-blind, sequential cohort, crossover study. Int J Clin Pharmacol Ther 2013 ; 51 : 367 – 73
29. Patel MA , Gadsden JC , Nedeljkovic SS , Bao X , Zeballos JL , Yu V , Ayad SS , Bendtsen TF : Brachial plexus block with liposomal bupivacaine for shoulder surgery improves analgesia and reduces opioid consumption: Results from a multicenter, randomized, double-blind, controlled trial. Pain Med 2020 ; 21 : 387 – 400
30. Rice D , Heil JW , Biernat L : Pharmacokinetic pro le and tolerability of liposomal bupivacaine following a repeated dose via local subcutaneous in ltration in healthy volunteers. Clin Drug Investig 2017 ; 37 : 249 – 57
31. Bramlett K , Onel E , Viscusi ER , Jones K : A randomized, double-blind, dose-ranging study comparing wound in ltration of DepoFoam bupivacaine, an extended-re-lease liposomal bupivacaine, to bupivacaine HCl for postsurgical analgesia in total knee arthroplasty. Knee 2012 ; 19 : 530 – 6
32. Richard BM , Rickert DE , Newton PE , Ott LR , Haan D , Brubaker AN , Cole PI , Ross PE , Rebelatto MC , Nelson KG : Safety evaluation of EXPAREL (DepoFoam Bupivacaine) administered by repeated subcutaneous injection in rabbits and dogs: Species comparison. J Drug Deliv 2011 ; 2011 : 467429
33. McAlvin JB , Reznor G , Shankarappa SA , Stefanescu CF , Kohane DS : Local toxicity from local anes-thetic polymeric microparticles. Anesth Analg 2013 ; 116 : 794 – 803
34. McAlvin JB , Padera RF , Shankarappa SA , Reznor G , Kwon AH , Chiang HH , Yang J , Kohane DS : Multivesicular liposomal bupivacaine at the sciatic nerve. Biomaterials 2014 ; 35 : 4557 – 64
35. Richard BM , Newton P , Ott LR , Haan D , Brubaker AN , Cole PI , Ross PE , Rebelatto MC , Nelson KG : The safety of EXPAREL ® (bupivacaine liposome injectable suspension) administered by peripheral nerve block in rabbits and dogs. J Drug Deliv 2012 ; 2012 : 962101
36. Damjanovska M , Cvetko E , Hadzic A , Seliskar A , Plavec T , Mis K , Vuckovic Hasanbegovic I , Stopar Pintaric T : Neurotoxicity of perineural vs intraneural-extrafas-cicular injection of liposomal bupivacaine in the por-cine model of sciatic nerve block. Anaesthesia 2015 ; 70 : 1418 – 26
37. Zel J , Hadzic A , Cvetko E , Seliskar A , Damjanovska M , Kuroda MM , Sega Jazbec S , Stopar Pintaric T : Neurological and histological outcomes after
subarachnoid injection of a liposomal bupivacaine suspension in pigs: A pilot study. Br J Anaesth 2019 ; 122 : 379 – 87
38. Damjanovska M , Cvetko E , Kuroda MM , Seliskar A , Plavec T , Mis K , Podbregar M , Pintaric TS : Neurotoxicity of intraneural injection of bupivacaine liposome injectable suspension versus bupivacaine hydrochloride in a porcine model. Vet Anaesth Analg 2019 ; 46 : 236 – 45
39. Shaw KA , Johnson PC , Zumbrun S , Chuang AH , Cameron CD : Chondrotoxicity of liposomal bupiva-caine in articular chondrocytes: Preliminary ndings. Mil Med 2017 ; 182 ( S1 ): 185 – 8
40. Boogaerts J , Declercq A , Lafont N , Benameur H , Akodad EM , Dupont JC , Legros FJ : Toxicity of bupiva-caine encapsulated into liposomes and injected intrave-nously: Comparison with plain solutions. Anesth Analg 1993 ; 76 : 553 – 5
41. Viscusi ER , Sinatra R , Onel E , Ramamoorthy SL : The safety of liposome bupivacaine, a novel local analgesic formulation. Clin J Pain 2014 ; 30 : 102 – 10
42. Ilfeld BM , Viscusi ER , Hadzic A , Minkowitz HS , Morren MD , Lookabaugh J , Joshi GP : Safety and side e ect pro- le of liposome bupivacaine (Exparel) in peripheral nerve blocks. Reg Anesth Pain Med 2015 ; 40 : 572 – 82
43. Baxter R , Bramlett K , Onel E , Daniels S : Impact of local administration of liposome bupivacaine for post-surgical analgesia on wound healing: A review of data from ten prospective, controlled clinical studies. Clin Ther 2013 ; 35 : 312 – 320.e5
44. Kharitonov V : A review of the compatibility of lipo-some bupivacaine with other drug products and com-monly used implant materials. Postgrad Med 2014 ; 126 : 129 – 38
45. Minkowitz HS , Onel E , Patronella CK , Smoot JD : A two-year observational study assessing the safety of DepoFoam bupivacaine after augmentation mamma-plasty. Aesthet Surg J 2012 ; 32 : 186 – 93
46. Aggarwal N : Local anesthetics systemic toxicity asso-ciation with Exparel (bupivacaine liposome)- A phar-macovigilance evaluation. Expert Opin Drug Saf 2018 ; 17 : 581 – 7
47. Bergese SD , Onel E , Morren M , Morganroth J : Bupivacaine extended-release liposome injection exhibits a favorable cardiac safety pro le. Reg Anesth Pain Med 2012 ; 37 : 145 – 51
48. Cohen B , Glosser L , Saab R , Walters M , Salih A , Zafeer-Khan M , Rivas E , Zhang K , Schacham NY , Chodavarapu P , Essber H , Chelnick D , Raza S , Hanline C , Khoshknabi D , Yang D , Seif J , Chhabada S , Turan A : Incidence of adverse events attributable to bupivacaine liposome injectable suspension or plain bupivacaine for postoperative pain in pediatric surgical patients: A retrospective matched cohort analysis. Paediatr Anaesth 2019 ; 29 : 169 – 74
ALNV134N2_Text.indb 336ALNV134N2_Text.indb 336 29-Dec-20 19:44:2629-Dec-20 19:44:26
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Ilfeld et al. Anesthesiology 2021; 134:283–344 337
Liposomal Bupivacaine to Treat Postoperative Pain
49. Naseem A , Harada T , Wang D , Arezina R , Lorch U , Onel E , Camm AJ , Taubel J : Bupivacaine extended release liposome injection does not prolong QTc interval in a thorough QT/QTc study in healthy vol-unteers. J Clin Pharmacol 2012 ; 52 : 1441 – 7
50. Davidson EM , Barenholz Y , Cohen R , Haroutiunian S , Kagan L , Ginosar Y : High-dose bupivacaine remotely loaded into multivesicular liposomes demonstrates slow drug release without systemic toxic plasma concen-trations after subcutaneous administration in humans. Anesth Analg 2010 ; 110 : 1018 – 23
51. Portillo J , Kamar N , Melibary S , Quevedo E , Bergese S : Safety of liposome extended-release bupivacaine for postoperative pain control. Front Pharmacol 2014 ; 5 : 90
52. Weiss E , Jolly C , Dumoulin JL , Meftah RB , Blani é P , Lalo ë PA , Tabary N , Fischler M , Le Guen M : Convulsions in 2 patients after bilateral ultrasound-guided trans ver-sus abdominis plane blocks for cesarean analgesia. Reg Anesth Pain Med 2014 ; 39 : 248 – 51
53. McCutchen T , Gerancher JC : Early intralipid therapy may have prevented bupivacaine-associated cardiac arrest. Reg Anesth Pain Med 2008 ; 33 : 178 – 80
54. Rosenblatt MA , Abel M , Fischer GW , Itzkovich CJ , Eisenkraft JB : Successful use of a 20% lipid emulsion to resuscitate a patient after a presumed bupivacaine-re-lated cardiac arrest. A nesthesiology 2006 ; 105 : 217 – 8
55. Candiotti K : Liposomal bupivacaine: An innova-tive nonopioid local analgesic for the management of postsurgical pain. Pharmacotherapy 2012 ; 32 ( 9 suppl ): 19S – 26S
56. Candiotti KA , Sands LR , Lee E , Bergese SD , Harzman AE , Marcet J , Kumar AS , Haas E : Liposome bupivacaine for postsurgical analgesia in adult patients undergoing laparoscopic colectomy: Results from prospective phase IV sequential cohort studies assessing health economic outcomes. Curr Ther Res Clin Exp 2014 ; 76 : 1 – 6
57. Cien AJ , Penny PC , Horn BJ , Popovich JM , Taunt CJ : Comparison between liposomal bupivacaine and fem-oral nerve block in patients undergoing primary total knee arthroplasty. J Surg Orthop Adv 2015 ; 24 : 225 – 9
58. Cohen SM , Vogel JD , Marcet JE , Candiotti KA : Liposome bupivacaine for improvement in economic outcomes and opioid burden in GI surgery: IMPROVE Study pooled analysis. J Pain Res 2014 ; 7 : 359 – 66
59. Domb BG , Gupta A , Hammarstedt JE , Stake CE , Sharp K , Redmond JM : The e ect of liposomal bupivacaine injection during total hip arthroplasty: A controlled cohort study. BMC Musculoskelet Disord 2014 ; 15 : 310
60. King NM , Quiko AS , Slotto JG , Connolly NC , Hackworth RJ , Heil JW : Retrospective analysis of quality improvement when using liposome bupiva-caine for postoperative pain control. J Pain Res 2016 ; 9 : 233 – 40
61. Kirkness CS , Asche CV , Ren J , Kim M , Rainville EC : Cost-bene t evaluation of liposomal bupivacaine in the
management of patients undergoing total knee arthro-plasty. Am J Health Syst Pharm 2016 ; 73 : e247 – 54
62. Marcet JE , Nfonsam VN , Larach S : An extended paIn relief trial utilizing the in ltration of a long-acting Multivesicular liPosome foRmulation Of bupiVacaine, EXPAREL (IMPROVE): A phase IV health economic trial in adult patients undergoing ileostomy reversal. J Pain Res 2013 ; 6 : 549 – 55
63. Vogel JD : Liposome bupivacaine (EXPAREL ® ) for extended pain relief in patients undergoing ileostomy reversal at a single institution with a fast-track dis-charge protocol: An IMPROVE Phase IV health eco-nomics trial. J Pain Res 2013 ; 6 : 605 – 10
64. Cohen SM : Extended pain relief trial utilizing in ltra-tion of Exparel( ® ), a long-acting multivesicular lipo-some formulation of bupivacaine: A phase IV health economic trial in adult patients undergoing open col-ectomy. J Pain Res 2012 ; 5 : 567 – 72
65. Asche CV , Ren J , Kim M , Gordon K , McWhirter M , Kirkness CS , Maurer BT : Local in ltration for post-surgical analgesia following total hip arthroplasty: A comparison of liposomal bupivacaine to traditional bupivacaine. Curr Med Res Opin 2017 ; 33 : 1283 – 90
66. Barrington JW , Olugbode O , Lovald S , Ong K , Watson H , Emerson RH Jr : Liposomal bupivacaine: A compar-ative study of more than 1000 total joint arthroplasty cases. Orthop Clin North Am 2015 ; 46 : 469 – 77
67. Beachler JA , Kopolovich DM , Tubb CC , Sayeed SA : Liposomal bupivacaine in total hip arthroplasty: Do the results justify the cost? J Orthop 2017 ; 14 : 161 – 5
68. Butz DR , Shenaq DS , Rundell VL , Kepler B , Liederbach E , Thiel J , Pesce C , Murphy GS , Sisco M , Howard MA : Postoperative pain and length of stay lowered by use of Exparel in immediate, implant-based breast reconstruc-tion. Plast Reconstr Surg Glob Open 2015 ; 3 : e391
69. Hannan CV , Albrecht MJ , Petersen SA , Srikumaran U : Liposomal bupivacaine vs interscalene nerve block for pain control after shoulder arthroplasty: A retrospective cohort analysis. Am J Orthop (Belle Mead NJ) 2016 ; 45 : 424 – 30
70. Jablonka EM , Lamelas AM , Kim JN , Molina B , Molina N , Okwali M , Samson W , Sultan MR , Dayan JH , Smith ML : Trans versus abdominis plane blocks with sin-gle-dose liposomal bupivacaine in conjunction with a nonnarcotic pain regimen help reduce length of stay following abdominally based microsurgical breast reconstruction. Plast Reconstr Surg 2017 ; 140 : 240 – 51
71. Khalil KG , Boutrous ML , Irani AD , Miller CC 3 rd , Pawelek TR , Estrera AL , Sa HJ : Operative intercostal nerve blocks with long-acting bupivacaine liposome for pain control after thoracotomy. Ann Thorac Surg 2015 ; 100 : 2013 – 8
72. Cherian JJ , Barrington J , Elmallah RK , Chughtai M , Mistry JB , Mont MA : Liposomal bupivacaine suspen-sion, can reduce length of stay and improve discharge
ALNV134N2_Text.indb 337ALNV134N2_Text.indb 337 29-Dec-20 19:44:2629-Dec-20 19:44:26
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Ilfeld et al.338 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
status of patients undergoing total hip arthroplasty. Surg Technol Int 2015 ; 27 : 235 – 9
73. Chughtai M , Cherian JJ , Mistry JB , Elmallah RD , Bennett A , Mont MA : Liposomal bupivacaine suspen-sion can reduce lengths of stay and improve discharge status of patients undergoing total knee arthroplasty. J Knee Surg 2016 ; 29 : 224 – 7
74. Rice DC , Cata JP , Mena GE , Rodriguez-Restrepo A , Correa AM , Mehran RJ : Posterior intercostal nerve block with liposomal bupivacaine: An alternative to thoracic epidural analgesia. Ann Thorac Surg 2015 ; 99 : 1953 – 60
75. Robbins J , Green CL , Parekh SG : Liposomal bupi-vacaine in forefoot surgery. Foot Ankle Int 2015 ; 36 : 503 – 7
76. Schmidt WK , Patou G , Joshi GP : Evaluating thera-peutic bene t in postsurgical analgesia requires global assessment: An example from liposome bupivacaine in hemorrhoidectomy. Hosp Pract (1995) 2012 ; 40 : 160 – 5
77. Sporer SM , Rogers T : Postoperative pain management after primary total knee arthroplasty: The value of lipo-somal bupivacaine. J Arthroplasty 2016 ; 31 : 2603 – 7
78. Torres EG , Anderson AB , Broome B , Geary SP , Burnikel B : Total knee arthroplasty performed with long-acting liposomal bupivacaine versus femoral nerve catheter. Am J Orthop (Belle Mead NJ) 2017 ; 46 : E414 – 8
79. Ayad S , Babazade R , Elsharkawy H , Nadar V , Lokhande C , Makarova N , Khanna R , Sessler DI , Turan A : Comparison of transversus abdominis plane in ltration with liposomal bupivacaine versus continuous epidural analgesia versus intravenous opioid analgesia. PLoS One 2016 ; 11 : e0153675
80. Kelley TM Jr , Bailey DW , Sparks P , Rice R , Caddell E , Currier H , Gallo D : Intercostal nerve blockade with Exparel ® results in lower opioid usage during the rst 24 hours after video-assisted thorascopic surgery. Am Surg 2018 ; 84 : 1433 – 8
81. Mehran RJ , Walsh GL , Zalpour A , Cata JP , Correa AM , Antono MB , Rice DC : Intercostal nerve blocks with liposomal bupivacaine: Demonstration of safety, and potential bene ts. Semin Thorac Cardiovasc Surg 2017 ; 29 : 531 – 7
82. Yu S , Szulc A , Walton S , Bosco J , Iorio R : Pain control and functional milestones in total knee arthroplasty: Liposomal bupivacaine versus femoral nerve block. Clin Orthop Relat Res 2017 ; 475 : 110 – 7
83. Klug MJ , Rivey MP , Carter JT : Comparison of intra-operative periarticular injections versus liposomal bupivacaine as part of a multimodal approach to pain management in total knee arthroplasty. Hosp Pharm 2016 ; 51 : 305 – 11
84. Bagsby DT , Ireland PH , Meneghini RM : Liposomal bupivacaine versus traditional periarticular injection for pain control after total knee arthroplasty. J Arthroplasty 2014 ; 29 : 1687 – 90
85. Mascha EJ , Vetter TR : Signi cance, errors, power, and sample size: The blocking and tackling of statistics. Anesth Analg 2018 ; 126 : 691 – 8
86. Olson MD , Moore EJ , Price DL : A randomized sin-gle-blinded trial of posttonsillectomy liposomal bupiv-acaine among adult patients. Otolaryngol Head Neck Surg 2018 ; 159 : 835 – 42
87. Brown L , Weir T , Shasti M , Yousaf O , Yousaf I , Tannous O , Koh E , Banagan K , Gelb D , Ludwig S : The e cacy of liposomal bupivacaine in lumbar spine surgery. Int J Spine Surg 2018 ; 12 : 434 – 40
88. Jones CL , Gruber DD , Fischer JR , Leonard K , Hernandez SL : Liposomal bupivacaine e cacy for postoperative pain following posterior vaginal surgery: A randomized, double-blind, placebo-controlled trial. Am J Obstet Gynecol 2018 ; 219 : 500.e1 – 8
89. Lieblich SE , Danesi H : Liposomal bupivacaine use in third molar impaction surgery: INNOVATE Study. Anesth Prog 2017 ; 64 : 127 – 35
90. Namdari S , Nicholson T , Abboud J , Lazarus M , Steinberg D , Williams G : Interscalene block with and without intraoperative local in ltration with lipo-somal bupivacaine in shoulder arthroplasty: A ran-domized controlled trial. J Bone Joint Surg Am 2018 ; 100 : 1373 – 8
91. Prabhu M , Clapp MA , McQuaid-Hanson E , Ona S , O’Donnell T , James K , Bateman BT , Wylie BJ , Barth WH Jr : Liposomal bupivacaine block at the time of cesarean delivery to decrease postoperative pain: A randomized controlled trial. Obstet Gynecol 2018 ; 132 : 70 – 8
92. Yeung J , Crisp CC , Mazloomdoost D , Kleeman SD , Pauls RN : Liposomal bupivacaine during robotic col-popexy and posterior repair: A randomized controlled trial. Obstet Gynecol 2018 ; 131 : 39 – 46
93. Davidovitch R , Goch A , Driesman A , Konda S , Pean C , Egol K : The use of liposomal bupivacaine administered with standard bupivacaine in ankle fractures requir-ing open reduction internal xation: A single-blinded randomized controlled trial. J Orthop Trauma 2017 ; 31 : 434 – 9
94. Golf M , Daniels SE , Onel E : A phase 3, randomized, placebo-controlled trial of DepoFoam ® bupivacaine (extended-release bupivacaine local analgesic) in bun-ionectomy. Adv Ther 2011 ; 28 : 776 – 88
95. Gor ne SR , Onel E , Patou G , Krivokapic ZV : Bupivacaine extended-release liposome injection for prolonged postsurgical analgesia in patients undergo-ing hemorrhoidectomy: A multicenter, randomized, double-blind, placebo-controlled trial. Dis Colon Rectum 2011 ; 54 : 1552 – 9
96. Mazloomdoost D , Pauls RN , Hennen EN , Yeung JY , Smith BC , Kleeman SD , Crisp CC : Liposomal bupiv-acaine decreases pain following retropubic sling place-ment: A randomized placebo-controlled trial. Am J Obstet Gynecol 2017 ; 217 : 598.e1 – 11
ALNV134N2_Text.indb 338ALNV134N2_Text.indb 338 29-Dec-20 19:44:2629-Dec-20 19:44:26
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Ilfeld et al. Anesthesiology 2021; 134:283–344 339
Liposomal Bupivacaine to Treat Postoperative Pain
97. Yalmanchili HM , Buchanan SN , Chambers LW , Thorns JD , McKenzie NA , Reiss AD , Page MP , Dizon VV , Brooks SE , Sha er LE , Lovald ST , Hartranft TH , Price PD : Postlaparotomy pain management: Comparison of patient-controlled analgesia pump alone, with subcutaneous bupivacaine infusion, or with injection of liposomal bupivacaine suspension. J Opioid Manag 2019 ; 15 : 169 – 75
98. Higgins JP , Altman DG , G ø tzsche PC , J ü ni P , Moher D , Oxman AD , Savovic J , Schulz KF , Weeks L , Sterne JA ; Cochrane Bias Methods Group; Cochrane Statistical Methods Group : The Cochrane Collaboration ’ s tool for assessing risk of bias in randomised trials. BMJ 2011 ; 343 : d5928
99. Sterne JAC , Savovi ć J , Page MJ , Elbers RG , Blencowe NS , Boutron I , Cates CJ , Cheng HY , Corbett MS , Eldridge SM , Emberson JR , Hern á n MA , Hopewell S , Hr ó bjartsson A , Junqueira DR , J ü ni P , Kirkham JJ , Lasserson T , Li T , McAleenan A , Reeves BC , Shepperd S , Shrier I , Stewart LA , Tilling K , White IR , Whiting PF , Higgins JPT : RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019 ; 366 : l4898
100. Noviasky J , Pierce DP , Whalen K , Guharoy R , Hildreth K : Bupivacaine liposomal versus bupivacaine: Comparative review. Hosp Pharm 2014 ; 49 : 539 – 43
101. O ’ Neill RT , Temple R : The prevention and treatment of missing data in clinical trials: An FDA perspective on the importance of dealing with it. Clin Pharmacol Ther 2012 ; 91 : 550 – 4
102. Alter TH , Liss FE , Ilyas AM : A prospective random-ized study comparing bupivacaine hydrochloride ver-sus bupivacaine liposome for pain management after distal radius fracture repair surgery. J Hand Surg Am 2017 ; 42 : 1003 – 8
103. Barron KI , Lamvu GM , Schmidt RC , Fisk M , Blanton E , Patanwala I : Wound in ltration with extended-re-lease versus short-acting bupivacaine before laparo-scopic hysterectomy: A randomized controlled trial. J Minim Invasive Gynecol 2017 ; 24 : 286 – 92
104. Dale EL , Kluemper CT , Cowart SJ , Jemison M , Kennedy JW , Gao L , Brzezienski MA , Rehm J : Bupivacaine extended-release liposomal injection versus bupivacaine HCl for early postoperative pain control following wrist operations: A prospective, randomized control trial. J Hand Surg Am 2020 ; 45 : 550.e1 – 8
105. Johnson RL , Amundson AW , Abdel MP , Sviggum HP , Mabry TM , Mantilla CB , Schroeder DR , Pagnano MW , Kopp SL : Continuous posterior lumbar plexus nerve block versus periarticular injection with ropiv-acaine or liposomal bupivacaine for total hip arthro-plasty: A three-arm randomized clinical trial. J Bone Joint Surg Am 2017 ; 99 : 1836 – 45
106. Knight RB , Walker PW , Keegan KA , Overholser SM , Baumgartner TS , Ebertowski JS 2nd , Aden JK , White MA : A randomized controlled trial for pain control
in laparoscopic urologic surgery: 0.25% bupivacaine versus long-acting liposomal bupivacaine. J Endourol 2015 ; 29 : 1019 – 24
107. Knudson RA , Dunlavy PW , Franko J , Raman SR , Kraemer SR : E ectiveness of liposomal bupivacaine in colorectal surgery: A pragmatic nonsponsored pro-spective randomized double blinded trial in a com-munity hospital. Dis Colon Rectum 2016 ; 59 : 862 – 9
108. Ma P , Lloyd A , McGrath M , Shuchleib Cung A , Akusoba I , Jackson A , Swartz D , Boone K , Higa K : E cacy of liposomal bupivacaine versus bupivacaine in port site injections on postoperative pain within enhanced recovery after bariatric surgery program: A randomized clinical trial. Surg Obes Relat Dis 2019 ; 15 : 1554 – 62
109. Motakef S , Wong WW , Ingargiola MJ , Nguyen D , Galdyn IA , Kim HY , Gupta SC : Liposomal bupiva-caine in implant-based breast reconstruction. Plast Reconstr Surg Glob Open 2017 ; 5 : e1559
110. Perets I , Walsh JP , Mu BH , Yuen LC , Ashberg L , Battaglia MR , Domb BG : Intraoperative in ltration of liposomal bupivacaine vs bupivacaine hydrochlo-ride for pain management in primary total hip arthro-plasty: A prospective randomized trial. J Arthroplasty 2018 ; 33 : 441 – 6
111. Premkumar A , Samady H , Slone H , Hash R , Karas S , Xerogeanes J : Liposomal bupivacaine for pain control after anterior cruciate ligament reconstruction: A pro-spective, double-blinded, randomized, positive-con-trolled trial. Am J Sports Med 2016 ; 44 : 1680 – 6
112. Propst K , O ’ Sullivan DM , Steinberg AC : Randomized double-blind trial of short- versus long-acting anal-gesia at the sacrospinous ligament. Int Urogynecol J 2019 ; 30 : 123 – 30
113. Haas E , Onel E , Miller H , Ragupathi M , White PF : A double-blind, randomized, active-controlled study for post-hemorrhoidectomy pain management with liposome bupivacaine, a novel local analgesic formu-lation. Am Surg 2012 ; 78 : 574 – 81
114. Iero PT , Mulherin DR , Jensen O , Berry T , Danesi H , Razook SJ : A prospective, randomized, open-label study comparing an opioid-sparing postsurgical pain management protocol with and without liposomal bupivacaine for full-arch implant surgery. Int J Oral Maxillofac Implants 2018 ; 33 : 1155 – 64
115. Iwano C , Salamon C : Liposomal bupivacaine ver-sus bupivacaine hydrochloride with lidocaine during midurethral sling placement: A randomized controlled trial. J Minim Invasive Gynecol 2019 ; 26 : 1133 – 8
116. Nadeau MH , Saraswat A , Vasko A , Elliott JO , Vasko SD : Bupivacaine versus liposomal bupivacaine for postop-erative pain control after augmentation mammaplasty: A prospective, randomized, double-blind trial. Aesthet Surg J 2016 ; 36 : NP47 – 52
117. Alijanipour P , Tan TL , Matthews CN , Viola JR , Purtill JJ , Rothman RH , Parvizi J , Austin MS : Periarticular
ALNV134N2_Text.indb 339ALNV134N2_Text.indb 339 29-Dec-20 19:44:2629-Dec-20 19:44:26
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Ilfeld et al.340 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
injection of liposomal bupivacaine o ers no ben-e t over standard bupivacaine in total knee arthro-plasty: A prospective, randomized, controlled trial. J Arthroplasty 2017 ; 32 : 628 – 34
118. Amundson AW , Johnson RL , Abdel MP , Mantilla CB , Panchamia JK , Taunton MJ , Kralovec ME , Hebl JR , Schroeder DR , Pagnano MW , Kopp SL : A three-arm randomized clinical trial comparing continu-ous femoral plus single-injection sciatic peripheral nerve blocks versus periarticular injection with rop-ivacaine or liposomal bupivacaine for patients under-going total knee srthroplasty. A nesthesiology 2017 ; 126 : 1139 – 50
119. Barrington JW , Emerson RH , Lovald ST , Lombardi AV , Berend KR : No di erence in early analgesia between liposomal bupivacaine injection and intra-thecal morphine after TKA. Clin Orthop Relat Res 2017 ; 475 : 94 – 105
120. Collis PN , Hunter AM , Vaughn MD , Carreon LY , Huang J , Malkani AL : Periarticular injection after total knee arthroplasty using liposomal bupivacaine vs a modi ed Ranawat suspension: A prospective, ran-domized study. J Arthroplasty 2016 ; 31 : 633 – 6
121. Dano JR , Goel R , Henderson RA , Fraser J , Sharkey PF : Periarticular ropivacaine cocktail is equivalent to liposomal bupivacaine cocktail in bilateral total knee arthroplasty. J Arthroplasty 2018 ; 33 : 2455 – 9
122. DeClaire JH , Aiello PM , Warritay OK , Freeman DC : E ectiveness of bupivacaine liposome injectable sus-pension for postoperative pain control in total knee arthroplasty: A prospective, randomized, double blind, controlled study. J Arthroplasty 2017 ; 32 ( 9S ): 268 – 71
123. Hyland SJ , Deliberato DG , Fada RA , Romanelli MJ , Collins CL , Wasielewski RC : Liposomal bupivacaine versus standard periarticular injection in total knee arthroplasty with regional anesthesia: A prospective randomized controlled trial. J Arthroplasty 2019 ; 34 : 488 – 94
124. Jain RK , Porat MD , Klingenstein GG , Reid JJ , Post RE , Schoifet SD : The AAHKS Clinical Research Award: Liposomal bupivacaine and periarticular injection are not superior to single-shot intra-artic-ular injection for pain control in total knee arthro-plasty. J Arthroplasty 2016 ; 31 ( 9 suppl ): 22 – 5
125. Schroer WC , Diesfeld PG , LeMarr AR , Morton DJ , Reedy ME : Does extended-release liposomal bupiv-acaine better control pain than bupivacaine after total knee arthroplasty (TKA)? A prospective, randomized clinical trial. J Arthroplasty 2015 ; 30 ( 9 suppl ): 64 – 7
126. Schumer G , Mann JW 3rd , Stover MD , Sloboda JF , Cdebaca CS , Woods GM : Liposomal bupivacaine uti-lization in total knee replacement does not decrease length of hospital stay. J Knee Surg 2019 ; 32 : 934 – 9
127. Schwarzkopf R , Drexler M , Ma MW , Schultz VM , Le KT , Rutenberg TF , Rinehart JB : Is there a bene t for
liposomal bupivacaine compared to a traditional peri-articular injection in total knee arthroplasty patients with a history of chronic opioid use? J Arthroplasty 2016 ; 31 : 1702 – 5
128. Suarez JC , Al-Mansoori AA , Kanwar S , Semien GA , Villa JM , McNamara CA , Patel PD : E ectiveness of novel adjuncts in pain management following total knee arthroplasty: A randomized clinical trial. J Arthroplasty 2018 ; 33 ( 7S ): 136 – 41
129. Zlotnicki JP , Hamlin BR , Plakseychuk AY , Levison TJ , Rothenberger SD , Urish KL : Liposomal bupivacaine vs plain bupivacaine in periarticular injection for con-trol of pain and early motion in total knee arthro-plasty: A randomized, prospective study. J Arthroplasty 2018 ; 33 : 2460 – 4
130. Mont MA , Beaver WB , Dysart SH , Barrington JW , Del Gaizo DJ : Local in ltration analgesia with liposomal bupivacaine improves pain scores and reduces opioid use after total knee arthroplasty: Results of a random-ized controlled trial. J Arthroplasty 2018 ; 33 : 90 – 6
131. Snyder MA , Scheuerman CM , Gregg JL , Ruhnke CJ , Eten K : Improving total knee arthroplasty periopera-tive pain management using a periarticular injection with bupivacaine liposomal suspension. Arthroplast Today 2016 ; 2 : 37 – 42
132. Dhanrajani P , Chung P : Comparative study of analge-sia with bupivacaine 0.25% versus 0.5% for third molar removal under general anesthesia. J Dent Anesth Pain Med 2016 ; 16 : 117 – 22
133. Mont MA , Beaver WB , Dysart SH , Barrington JW , Del Gaizo DJ : Corrigendum to “ local in ltration analge-sia with liposomal bupivacaine improves pain scores and reduces opioid use after total knee arthroplasty: Results of a randomized controlled trial ” [Journal of Arthroplasty 33 (2018) 90-96]. J Arthroplasty 2019 ; 34 : 399 – 400
134. Dysart SH , Barrington JW , Del Gaizo DJ , Sodhi N , Mont MA : Local in ltration analgesia with liposomal bupivacaine improves early outcomes after total knee arthroplasty: 24-hour data from the PILLAR Study. J Arthroplasty 2019 ; 34 : 882 – 886.e1
135. Dysart S , Snyder MA , Mont MA : A randomized, multicenter, double-blind study of local in ltration analgesia with liposomal bupivacaine for postsurgical pain following total knee arthroplasty: Rationale and design of the PILLAR trial. Surg Technol Int 2016 ; 30 : 261 – 7
136. Joshi GP , Cushner FD , Barrington JW , Lombardi AV Jr , Long WJ , Springer BD , Stulberg BN : Techniques for periarticular in ltration with liposomal bupiva-caine for the management of pain after hip and knee arthroplasty: A consensus recommendation. J Surg Orthop Adv 2015 ; 24 : 27 – 35
137. Connelly JO , Edwards PK , Mears SC , Barnes CL : Technique for periarticular local in ltrative anesthesia
ALNV134N2_Text.indb 340ALNV134N2_Text.indb 340 29-Dec-20 19:44:2629-Dec-20 19:44:26
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Ilfeld et al. Anesthesiology 2021; 134:283–344 341
Liposomal Bupivacaine to Treat Postoperative Pain
delivery using liposomal bupivacaine in total knee arthroplasty. J Surg Orthop Adv 2015 ; 24 : 263 – 6
138. Khlopas A , Elmallah RK , Chughtai M , Yakubek GA , Faour M , Klika AK , Higuera CA , Molloy RM , Mont MA : The learning curve associated with the admin-istration of intra-articular liposomal bupivacaine for total knee arthroplasty: A pilot study. Surg Technol Int 2017 ; 30 : 314 – 20
139. Hadzic A , Minkowitz HS , Melson TI , Berkowitz R , Uskova A , Ringold F , Lookabaugh J , Ilfeld BM : Liposome bupivacaine femoral nerve block for postsurgical analgesia after total knee arthroplasty. A nesthesiology 2016 ; 124 : 1372 – 83
140. Shafer SL : Letter to the editor on “ local in ltration analgesia with liposomal bupivacaine improves pain scores and reduces opioid use after total knee arthro-plasty: Results of a randomized controlled trial ” . J Arthroplasty 2018 ; 33 : 2694
141. Okoroha KR , Keller RA , Marshall NE , Jung EK , Mehran N , Owashi E , Moutzouros V : Liposomal bupivacaine versus femoral nerve block for pain con-trol after anterior cruciate ligament reconstruction: A prospective randomized trial. Arthroscopy 2016 ; 32 : 1838 – 45
142. Okoroha KR , Lynch JR , Keller RA , Korona J , Amato C , Rill B , Kolowich PA , Muh SJ : Liposomal bupiva-caine versus interscalene nerve block for pain control after shoulder arthroplasty: A prospective randomized trial. J Shoulder Elbow Surg 2016 ; 25 : 1742 – 8
143. Surdam JW , Licini DJ , Baynes NT , Arce BR : The use of Exparel (liposomal bupivacaine) to manage post-operative pain in unilateral total knee arthroplasty patients. J Arthroplasty 2015 ; 30 : 325 – 9
144. Talmo CT , Kent SE , Fredette AN , Anderson MC , Hassan MK , Mattingly DA : Prospective randomized trial comparing femoral nerve block with intraoper-ative local anesthetic injection of liposomal bupiva-caine in total knee arthroplasty. J Arthroplasty 2018 ; 33 : 3474 – 8
145. Abildgaard JT , Lonergan KT , Tolan SJ , Kissenberth MJ , Hawkins RJ , Washburn R 3rd , Adams KJ , Long CD , Shealy EC , Motley JR , Tokish JM : Liposomal bupiv-acaine versus indwelling interscalene nerve block for postoperative pain control in shoulder arthroplasty: A prospective randomized controlled trial. J Shoulder Elbow Surg 2017 ; 26 : 1175 – 81
146. Marino J , Scuderi G , Dowling O , Farquhar R , Freycinet B , Overdyk F : Periarticular knee injection with liposomal bupivacaine and continuous femoral nerve block for postoperative pain management after total knee arthroplasty: A randomized controlled trial. J Arthroplasty 2019 ; 34 : 495 – 500
147. Gasanova I , Alexander J , Ogunnaike B , Hamid C , Rogers D , Minhajuddin A , Joshi GP : Transversus abdominis plane block versus surgical site in ltration
for pain management after open total abdominal hys-terectomy. Anesth Analg 2015 ; 121 : 1383 – 8
148. McGraw-Tatum MA , Groover MT , George NE , Urse JS , Heh V : A prospective, randomized trial compar-ing liposomal bupivacaine vs fascia iliaca compart-ment block for postoperative pain control in total hip arthroplasty. J Arthroplasty 2017 ; 32 : 2181 – 5
149. Sabesan VJ , Shahriar R , Petersen-Fitts GR , Whaley JD , Bou-Akl T , Sweet M , Milia M : A prospective ran-domized controlled trial to identify the optimal post-operative pain management in shoulder arthroplasty: Liposomal bupivacaine versus continuous interscalene catheter. J Shoulder Elbow Surg 2017 ; 26 : 1810 – 7
150. Behrends M , Yap EN , Zhang AL , Kolodzie K , Kinjo S , Harbell MW , Aleshi P : Preoperative fascia iliaca block does not improve analgesia after arthroscopic hip sur-gery, but causes quadriceps muscles weakness: A ran-domized, double-blind trial. A nesthesiology 2018 ; 129 : 536 – 43
151. Bober K , Kadado A , Charters M , Ayoola A , North T : Pain control after total hip arthroplasty: A randomized controlled trial determining e cacy of fascia iliaca compartment blocks in the immediate postoperative period. J Arthroplasty 2020 ; 35 ( 6S ): 241 – 5
152. Siddiqui ZI , Cepeda MS , Denman W , Schumann R , Carr DB : Continuous lumbar plexus block provides improved analgesia with fewer side e ects compared with systemic opioids after hip arthroplasty: A randomized controlled trial. Reg Anesth Pain Med 2007 ; 32 : 393 – 8
153. T ü rker G , U ç kunkaya N , Yava ş ç ao ğ lu B , Yilmazlar A , Oz ç elik S : Comparison of the catheter-technique psoas compartment block and the epidural block for analgesia in partial hip replacement surgery. Acta Anaesthesiol Scand 2003 ; 47 : 30 – 6
154. Lee CY , Robinson DA , Johnson CA Jr , Zhang Y , Wong J , Joshi DJ , Wu TT , Knight PA : A randomized controlled trial of liposomal bupivacaine parasternal intercostal block for sternotomy. Ann Thorac Surg 2019 ; 107 : 128 – 34
155. Colibaseanu DT , Osagiede O , Merchea A , Ball CT , Bojaxhi E , Panchamia JK , Jacob AK , Kelley SR , Naessens JM , Larson DW : Randomized clinical trial of liposomal bupivacaine transverse abdominis plane block versus intrathecal analgesia in colorectal surgery. Br J Surg 2019 ; 106 : 692 – 9
156. Felling DR , Jackson MW , Ferraro J , Battaglia MA , Albright JJ , Wu J , Genord CK , Brockhaus KK , Bhave RA , McClure AM , Shanker BA , Cleary RK : Liposomal bupivacaine transversus abdominis plane block versus epidural analgesia in a colon and rectal surgery enhanced recovery pathway: A randomized clinical trial. Dis Colon Rectum 2018 ; 61 : 1196 – 204
157. Ha AY , Keane G , Parikh R , Odom E , Tao Y , Zhang L , Myckatyn TM , Gu ey R : The analgesic e ects of lipo-somal bupivacaine versus bupivacaine hydrochloride
ALNV134N2_Text.indb 341ALNV134N2_Text.indb 341 29-Dec-20 19:44:2629-Dec-20 19:44:26
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Ilfeld et al.342 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
administered as a transversus abdominis plane block after abdominally based autologous microvascular breast reconstruction: A prospective, single-blind, randomized, controlled trial. Plast Reconstr Surg 2019 ; 144 : 35 – 44
158. Hutchins J , Delaney D , Vogel RI , Ghebre RG , Downs LS Jr , Carson L , Mullany S , Teoh D , Geller MA : Ultrasound guided subcostal trans versus abdominis plane (TAP) in ltration with liposomal bupivacaine for patients undergoing robotic assisted hysterectomy: A prospective randomized controlled study. Gynecol Oncol 2015 ; 138 : 609 – 13
159. Hutchins JL , Kesha R , Blanco F , Dunn T , Hochhalter R : Ultrasound-guided subcostal trans versus abdominis plane blocks with liposomal bupivacaine vs. non-li-posomal bupivacaine for postoperative pain control after laparoscopic hand-assisted donor nephrectomy: A prospective randomised observer-blinded study. Anaesthesia 2016 ; 71 : 930 – 7
160. Hutchins J , Argenta P , Berg A , Habeck J , Kaizer A , Geller MA : Ultrasound-guided subcostal transversus abdomi-nis plane block with liposomal bupivacaine compared to bupivacaine in ltration for patients undergoing robot-ic-assisted and laparoscopic hysterectomy: A prospective randomized study. J Pain Res 2019 ; 12 : 2087 – 94
161. Nedeljkovic SS , Kett A , Vallejo MC , Horn JL , Carvalho B , Bao X , Cole NM , Renfro L , Gadsden JC , Song J , Yang J , Habib AS : Transversus abdominis plane block with liposomal bupivacaine for pain after cesarean delivery in a multicenter, randomized, double-blind, controlled trial . Anesth Analg 2020 ; 131 : 1830 – 9
162. Torgeson M , Kileny J , Pfeifer C , Narkiewicz L , Obi S : Conventional epidural vs transversus abdominis plane block with liposomal bupivacaine: A randomized trial in colorectal surgery. J Am Coll Surg 2018 ; 227 : 78 – 83
163. Meftah M , Boenerjous-Abel S , Siddappa VH , Kirschenbaum IH : E cacy of adductor canal block with liposomal bupivacaine: A randomized prospec-tive clinical trial. Orthopedics 2020 ; 43 : e47 – 53
164. Purcell RL , Brooks DI , Steelman TJ , Christensen DL , Dickens JF , Kent ML , McCabe MP , Anderson TD : Fascia iliaca blockade with the addition of liposo-mal bupivacaine versus plain bupivacaine for periop-erative pain management during hip arthroscopy: A double-blinded prospective randomized control trial. Arthroscopy 2019 ; 35 : 2608 – 16
165. Sober ó n JR Jr , Ericson-Neilsen W , Sisco-Wise LE , Gasta ñ aduy M , Beck DE : Perineural liposomal bupi-vacaine for postoperative pain control in patients undergoing upper extremity orthopedic surgery: A prospective and randomized pilot study. Ochsner J 2016 ; 16 : 436 – 42
166. Vandepitte C , Kuroda M , Witvrouw R , Anne L , Bellemans J , Corten K , Vanelderen P , Mesotten D , Leunen I , Heylen M , Van Boxstael S , Golebiewski M , Van de Velde M , Knezevic NN , Hadzic A : Addition
of liposome bupivacaine to bupivacaine HCl ver-sus bupivacaine HCl alone for interscalene brachial plexus block in patients having major shoulder sur-gery. Reg Anesth Pain Med 2017 ; 42 : 334 – 41
167. Viscusi ER , Candiotti KA , Onel E , Morren M , Ludbrook GL : The pharmacokinetics and pharmaco-dynamics of liposome bupivacaine administered via a single epidural injection to healthy volunteers. Reg Anesth Pain Med 2012 ; 37 : 616 – 22
168. Abdallah FW , Chan VW , Brull R : Transversus abdomi-nis plane block: A systematic review. Reg Anesth Pain Med 2012 ; 37 : 193 – 209
169. Tubog TD , Harenberg JL , Mason-Nguyen J , Kane TD : Opioid-sparing e ects of transversus abdominis plane block in elective hysterectomy: A systematic review and meta-analysis. AANA J 2018 ; 86 : 41 – 55
170. Mascha EJ : Equivalence and noninferiority testing in anesthesiology research. A nesthesiology 2010 ; 113 : 779 – 81
171. Lee YS , Park YC , Kim JH , Kim WY , Yoon SZ , Moon MG , Min TJ : Intrathecal hydromorphone added to hyperbaric bupivacaine for postoperative pain relief after knee arthroscopic surgery: A prospective, randomised, controlled trial. Eur J Anaesthesiol 2012 ; 29 : 17 – 21
172. Liu JN , Nho SJ , Faucett SC , Lynch TS , Amin NH : Regarding “ fascia iliaca blockade with the addition of liposomal bupivacaine versus plain bupivacaine for perioperative pain management during hip arthros-copy: A double-blinded prospective randomized con-trol trial ” . Arthroscopy 2020 ; 36 : 329 – 30
173. Onwochei DN , West S , Pawa A : If wishes were horses, beggars would ride. Reg Anesth Pain Med 2017 ; 42 : 546
174. Vandepitte C , Kuroda M , van Boxstael S , Hadzic A : “ Don ’ t throw the baby out with the bath water: ” A reply to Dr. Onwochei et al . Reg Anesth Pain Med 2017 ; 42 : 546 – 7
175. Hadzic A , Vandepitte C , Knezevic NN , Mesotten D , Kuroda MM , Van Boxstael S , Bellemans J , Van de Velde M , Fivez T , Corten K : Clinical research and trial reg-istries: The times they are a-changin. Reg Anesth Pain Med 2020 ; 45 : 844 – 6
176. Sites BD , Brummett CM , Buvanendran A , Capdevila X , Cohen SP , Guan Y , Liu S , Memtsoudis SG , Perlas A , Tran Q , Wu CL : Editors ’ commentary. Reg Anesth Pain Med 2020 ; 45 : 755 – 6
177. Malige A , Yeazell S , Ng-Pellegrino A , Carolan G : Risk factors for complications and return to the emergency department after interscalene block using liposomal bupivacaine for shoulder surgery. J Shoulder Elbow Surg 2020 ; 29 : 2332 – 8
178. Ilfeld BM : Liposome bupivacaine in peripheral nerve blocks and epidural injections to manage post-operative pain. Expert Opin Pharmacother 2013 ; 14 : 2421 – 31
ALNV134N2_Text.indb 342ALNV134N2_Text.indb 342 29-Dec-20 19:44:2629-Dec-20 19:44:26
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Ilfeld et al. Anesthesiology 2021; 134:283–344 343
Liposomal Bupivacaine to Treat Postoperative Pain
179. Zhao B , Ma X , Zhang J , Ma J , Cao Q : The e cacy of local liposomal bupivacaine in ltration on pain and recovery after total joint arthroplasty: A systematic review and meta-analysis of randomized controlled trials. Medicine (Baltimore) 2019 ; 98 : e14092
180. Ma TT , Wang YH , Jiang YF , Peng CB , Yan C , Liu ZG , Xu WX : Liposomal bupivacaine versus traditional bupivacaine for pain control after total hip arthro-plasty: A meta-analysis. Medicine (Baltimore) 2017 ; 96 : e7190
181. Zhang X , Yang Q , Zhang Z : The e ciency and safety of local liposomal bupivacaine in ltration for pain control in total hip arthroplasty: A systematic review and meta-analysis. Medicine (Baltimore) 2017 ; 96 : e8433
182. Wang X , Xiao L , Wang Z , Zhao G , Ma J : Comparison of peri-articular liposomal bupivacaine and standard bupivacaine for postsurgical analgesia in total knee arthroplasty: A systematic review and meta-analysis. Int J Surg 2017 ; 39 : 238 – 48
183. Raman S , Lin M , Krishnan N : Systematic review and meta-analysis of the e cacy of liposomal bupiva-caine in colorectal resections. J Drug Assess 2018 ; 7 : 43 – 50
184. Yan Z , Chen Z , Ma C : Liposomal bupivacaine ver-sus interscalene nerve block for pain control after shoulder arthroplasty: A meta-analysis. Medicine (Baltimore) 2017 ; 96 : e7226
185. Liu SQ , Chen X , Yu CC , Weng CW , Wu YQ , Xiong JC , Xu SH : Comparison of periarticular anesthe-sia with liposomal bupivacaine with femoral nerve block for pain control after total knee arthroplasty: A PRISMA-compliant meta-analysis. Medicine (Baltimore) 2017 ; 96 : e6462
186. Ilfeld BM , Malhotra N , Furnish TJ , Donohue MC , Madison SJ : Liposomal bupivacaine as a single-injec-tion peripheral nerve block: A dose-response study. Anesth Analg 2013 ; 117 : 1248 – 56
187. De Angelis C , Drazen JM , Frizelle FA , Haug C , Hoey J , Horton R , Kotzin S , Laine C , Marusic A , Overbeke AJ , Schroeder TV , Sox HC , Van Der Weyden MB ; International Committee of Medical Journal Editors : Clinical trial registration: A statement from the International Committee of Medical Journal Editors. N Engl J Med 2004 ; 351 : 1250 – 1
188. Mills JL : Data torturing. N Engl J Med 1993 ; 329 : 1196 – 9
189. Lundh A , Lexchin J , Mintzes B , Schroll JB , Bero L : Industry sponsorship and research outcome: Systematic review with meta-analysis. Intensive Care Med 2018 ; 44 : 1603 – 12
190. Ohri R , Wang JC , Pham L , Blaskovich PD , Costa D , Nichols G , Hildebrand W , Scarborough N , Herman C , Strichartz GR : Prolonged amelioration of exper-imental postoperative pain by bupivacaine released
from microsphere-coated hernia mesh. Reg Anesth Pain Med 2014 ; 39 : 97 – 107
191. Routman HD , Israel LR , Moor MA , Boltuch AD : Local injection of liposomal bupivacaine combined with intravenous dexamethasone reduces postopera-tive pain and hospital stay after shoulder arthroplasty. J Shoulder Elbow Surg 2017 ; 26 : 641 – 7
192. Visoiu M , Verdecchia N : Repeated intercostal nerve blocks with liposomal bupivacaine for chronic chest pain: A case report. A A Pract 2019 ; 13 : 260 – 3
193. Finneran JJ IV , Ilfeld BM : Letter regarding “ Repeated intercostal nerve blocks with liposomal bupivacaine for chronic chest pain: A case report. ” A A Pract 2020 ; 14 : 67
194. Fredrickson MJ , Ilfeld BM : Prospective trial registration for clinical research: What is it, what is it good for, and why do I care? Reg Anesth Pain Med 2011 ; 36 : 619 – 24
195. Sober ó n JR Jr , Sisco-Wise LE , Dunbar RM : Compartment syndrome in a patient treated with perineural liposomal bupivacaine (Exparel). J Clin Anesth 2016 ; 31 : 1 – 4
196. Olsen D , Amundson A , Kopp S : Inadvertent pro-longed femoral nerve palsy after eld block with liposomal bupivacaine for inguinal herniorrhaphy. A A Case Rep 2016 ; 6 : 362 – 3
197. Burbridge M , Ja e RA : Exparel ® : A new local anes-thetic with special safety concerns. Anesth Analg 2015 ; 121 : 1113 – 4
198. Ottoboni T , Quart B , Pawasauskas J , Dasta JF , Pollak RA , Viscusi ER : Mechanism of action of HTX-011: A novel, extended-release, dual-acting local anesthetic formulation for postoperative pain. Reg Anesth Pain Med 2019 Dec 16 [Epub ahead of print]
199. Viscusi E , Minkowitz H , Winkle P , Ramamoorthy S , Hu J , Singla N : Correction to: HTX-011 reduced pain intensity and opioid consumption versus bupiva-caine HCl in herniorrhaphy: Results from the phase 3 EPOCH 2 study. Hernia 2020 ; 24 : 679
200. Viscusi E , Minkowitz H , Winkle P , Ramamoorthy S , Hu J , Singla N : HTX-011 reduced pain intensity and opioid consumption versus bupivacaine HCl in herniorrhaphy: Results from the phase 3 EPOCH 2 study. Hernia 2019 ; 23 : 1071 – 80
201. Strichartz GR , Wang JC , Blaskovich P , Ohri R : Mitigation of experimental, chronic post-thoracotomy pain by pre-operative in ltration of local slow-release bupivacaine microspheres. Anesth Analg 2015 ; 120 : 1375 – 84
202. Davidson EM , Haroutounian S , Kagan L , Naveh M , Aharon A , Ginosar Y : A Novel proliposomal ropiva-caine oil: Pharmacokinetic-pharmacodynamic stud-ies after subcutaneous administration in pigs. Anesth Analg 2016 ; 122 : 1663 – 72
203. Shomorony A , Santamaria CM , Zhao C , Rwei AY , Mehta M , Zurakowski D , Kohane DS : Prolonged duration local anesthesia by combined delivery of
ALNV134N2_Text.indb 343ALNV134N2_Text.indb 343 29-Dec-20 19:44:2729-Dec-20 19:44:27
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Ilfeld et al.344 Anesthesiology 2021; 134:283–344
REVIEW ARTICLE
capsaicin- and tetrodotoxin-loaded liposomes. Anesth Analg 2019 ; 129 : 709 – 17
204. Corman S , Shah N , Dagenais S : Medication, equip-ment, and supply costs for common interventions providing extended post-surgical analgesia following total knee arthroplasty in US hospitals. J Med Econ 2018 ; 21 : 11 – 8
205. Brown L , Weir T , Koenig S , Shasti M , Yousaf I , Yousaf O , Tannous O , Koh E , Banagan K , Gelb D , Ludwig S : Can liposomal bupivacaine be safely utilized in elec-tive spine surgery? Global Spine J 2019 ; 9 : 133 – 7
206. Sethi PM , Brameier DT , Mandava NK , Miller SR : Liposomal bupivacaine reduces opiate con-sumption after rotator cu repair in a randomized controlled trial. J Shoulder Elbow Surg 2019 ; 28 : 819 – 27
207. Smoot JD , Bergese SD , Onel E , Williams HT , Hedden W : The e cacy and safety of DepoFoam bupivacaine in patients undergoing bilateral, cosmetic, submuscu-lar augmentation mammaplasty: A randomized, dou-ble-blind, active-control study. Aesthet Surg J 2012 ; 32 : 69 – 76
ALNV134N2_Text.indb 344ALNV134N2_Text.indb 344 29-Dec-20 19:44:2729-Dec-20 19:44:27
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Creative writing that explores the abstract side of our profession and our lives
ANESTHESIOLOGY, V 134 • NO 2 FEbruArY 2021 345
I
Accepted for publication July 6, 2020. Published online first on August 3, 2020. From the Department of Anesthesiology and Pain Managenent, University of Texas Southwestern School of Medicine, Dallas, Texas. [email protected].
Permission to reprint granted to the American Society of Anesthesiologists, Inc. by copyright author/owner. Anesthesiology 2021; 134:345. DOI: 10.1097/ALN.0000000000003490
Stephen T. Harvey, M.D., Editor
Dying AloneKristina L. Goff, M.D.
I sit next to your bed in the filtered light of this hospital room—the place I work transformed into something much more personal.And it is inexplicably quiet.We are perfect strangers really,But somehow I’m the only one here in this most intimate moment with you.
I stroke your age-worn fingers with mine, gloved,hoping the message is reaching you:
—you are not alone,You are much more deeply loved,And by many more people,Than this video screen can ever show you—
Your nails are ragged, rubbed uneven, maybe from years of working with your hands,And I find myself wondering about your life,Feeling inadequate for not knowing even the most basic things about you.
And so I begin to meditate on the sounds of your breathing rather than my own,It makes me feel closer to you as I wait for you to slip away.
I hope desperately it will be peaceful—please let me be able to give you at least that.
The white noise of my PAPR helmet and the soothing rhythm of your breath lull me to sleepfor a second, my eyes drift shutand then fly open in a panic to check on you.Nothing has changed:You are still there, your breath growing more and more shallow.Your daughter softly sobs from across the room, across the city.
I am so tired, and I know you are tired too.
ALNV134N2_Text.indb 345ALNV134N2_Text.indb 345 29-Dec-20 19:44:2729-Dec-20 19:44:27
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Creative writing that explores the abstract side of our profession and our lives
346 February 2021 aNeSTHeSIOLOGy, V 134 • NO 2
N
From the Department of Anesthesiology, Division of Pediatric Anesthesiology, University of Michigan Medical School, Ann Arbor, Michigan. [email protected].
Accepted for publication October 28, 2020. Published online first on November 9, 2020.
Permission to reprint granted to the American Society of Anesthesiologists, Inc. by copyright author/owner. Anesthesiology 2021; 134:346–8. DOI: 10.1097/ALN.0000000000003623
Stephen T. Harvey, M.D., Editor
Behind the Maskashlee e. Holman, M.D., Virginia T. Gauger, M.D.
N95 masks. Surgical masks. Homemade masks. Two months ago, if someone was
wearing a mask, we would wonder “why”; these days, we wonder “why” if someone is
not wearing one. In response to the coronavirus disease 2019 (COVID-19) pandemic,
the wearing of masks has become globally commonplace, from airports and grocery
stores to homes and neighborhoods. Many hospital systems have instituted mandatory
24/7 mask-wearing policies for all employees, visitors, and patients who walk through
their doors, with the goal of protecting patients and healthcare workers alike and with
the hope of decreasing the spread of a disease actively wreaking medical, financial,
and emotional havoc across the globe.1
And yes, face masks offer critical protection to providers on the frontline. Face masks
decrease the spread of COVID-19 and may be at least partially responsible for “flat-
tening the curve,” thus preventing our healthcare systems from becoming devastat-
ingly overwhelmed.2 But, for all their delivered security, face masks are taking a very
real toll on providers themselves: a physical, psychologic, and emotional price that is
difficult to describe and quantify.
Most think that, as anesthesiologists, wearing masks is a normal, standard practice,
but nothing is “normal” in a pandemic. The process of putting on a mask in the
hospital is no longer ordinary; it is no longer routine. It is an act accompanied by
undertones of anxiety, worry, and concern, and followed by a barrage of unsettling
questions: Does my mask fit appropriately? Is there a leak? Will my mask keep the
ALNV134N2_Text.indb 346ALNV134N2_Text.indb 346 29-Dec-20 19:44:2729-Dec-20 19:44:27
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Mind to Mind
anesthesiology 2021; 134:346–8 347Mind to Mind
Mind to Mind
Creative writing that explores the abstract side of our profession and our livesvirus out? Will it protect me from getting sick? Will this mask prevent me from infect-
ing my elderly parents, my spouse, and children? Questions that persist long after our
masks have been donned and doffed.
Face masks act as a physical barrier to the disease itself, but they also create an emo-
tional barrier against conveying empathy and compassion, instilling confidence in our
expertise, and cultivating trust and reassurance. Likewise, gloves remove the comfort-
ing aspect of the human touch. How do you foster and grow a personal relationship
with a nervous patient, child, parent, or family with a mask covering your mouth, a
shield covering your eyes, and gloves covering your hands?
From birth, humans are programed to observe, identify, and interpret facial cues
to learn safety and trust, develop situational awareness, and nurture attitudes and
beliefs.3 Our faces are now covered. Our facial cues have vanished. We are no longer
able to shake hands. We cannot smile as we comfort each patient, striving to commu-
nicate that we will provide the very best care for them, or reassure each parent that
we will treat her child as if he is our own. We are left with our words, stifled by our
face masks, difficult to understand, muffled and subdued. Words which feel fragile
and distanced, all the while hoping that we have adequately conveyed kindness and
compassion to our patients and their families, our most revered qualities for our most
treasured resource.
Our patients, too, must wear masks. With these physical barriers, clinical cues, once
taken for granted, are absent. We cannot examine an airway in preparation for intu-
bation without the fear of exposing ourselves to infection. We are unable to observe
the color of our patient’s face and lips to ensure oxygenation or feel his breath on our
wrists to confirm ventilation. Using a stethoscope is nearly impossible because of our
shield of personal protective equipment.4 We perform our duties alone, to minimize
unnecessary exposures. Our setup, once routine and predictable, is fraught with
uncertainty.
Behind our personal protective equipment, we are hot, sweaty, and uncomfortable
in our normally comfortable surroundings. Our faces hurt from the pressure of the
masks. Our skin is breaking down. We rebreathe exhaled carbon dioxide, increasing
our metabolic rate and the physiologic stress on our own bodies.5 God forbid if we
sneeze. Previously routine procedures are difficult—placing tenuous intravenous cath-
eters covered with multiple layers of gloves; auscultating the lungs of a patient without
ALNV134N2_Text.indb 347ALNV134N2_Text.indb 347 29-Dec-20 19:44:2729-Dec-20 19:44:27
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Mind to Mind
348 anesthesiology 2021; 134:346–8 Mind to Mind
MIND TO MIND
breaking suit; intubating a newborn with foggy goggles. We are uncomfortable in
our regular workspace, our own practice—vulnerable in situations our expertise has
previously allowed us to feel secure in.
Our clinical practice is changing, evolving to meet the demands of the COVID-19
pandemic. We are walking a fine line, teetering on wanting to do what is best for our
patients while in turn keeping ourselves healthy, burdened by guilt either way we
fall—am I not doing enough? Am I exposing myself too much? The practice of medi-
cine no longer feels like the safe haven it was before COVID-19. Hospitals are strange
and foreign environments, colored by unease, apprehension, and fear. Face masks
symbolize the novel challenges and struggles we now face on a daily basis.
But we still come. Despite our discomfort and uneasiness, anesthesiologists willingly
flood hospitals across the country. Every morning, we make the choice to leave the
safety of our homes, prepared to don our masks and equipment, ready to provide
care to those who depend on us. We have dedicated our lives to people and have no
intention of surrendering in the face of the beast. We are charged with the vital task of
holding our patients’ lives and well-being in our, now gloved, hands.
Yes, our masks are necessary. They keep us safe, keep our families safe. We wear them
for the greater good, for the good of society, to allow our civilization to continue, to
persevere. Our masks allow us to continue tending to those in need. They are our
crutch, what allows us to continue fighting in this war, but they are isolating. We are
practicing medicine surrounded by people but alone. Nevertheless, when we take our
masks off, we can breathe again. We are free to express ourselves as we did before. The
loneliness of wearing a mask disappears, and we are reminded of who we are, why we
do what we do, and what we are fighting for.
References
1. Desai AN, Aronoff DM: Masks and coronavirus disease 2019. JAMA 2020; 323:2103 2. Han G, Zhou YH: Possibly critical role of wearing masks in general population in controlling
COVID-19. J Med Virol 2020; 92:1779–81 3. Sugden NA, Marquis AR: Meta-analytic review of the development of face discrimination
in infancy: Face race, face gender, infant age, and methodology moderate face discrimination. Psychol Bull 2017; 143:1201–44
4. Croswell RJ, Dilley DC, Lucas WJ, Vann WF Jr: A comparison of conventional versus elec-tronic monitoring of sedated pediatric dental patients. Pediatr Dent 1995; 17:332–9
5. Kim JH, Benson SM, Roberge RJ: Pulmonary and heart rate responses to wearing N95 filtering facepiece respirators. Am J Infect Control 2013; 41:24–7
16_ALN-D-20-00758.indd 34816_ALN-D-20-00758.indd 348 29-Dec-20 22:23:4429-Dec-20 22:23:44
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
CORRESPONDENCE
ANESTHESIOLOGY, V 134 • NO 2 FEBRUARY 2021 349
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved. Anesthesiology 2021 ; 134 : 349 – 56
Perioperative Management of Glucose-lowering Drugs: Comment
To the Editor:
I would like to commend Preiser et al . for an excellent review of oral glucose-management drugs in the periop-
erative period. 1 I want to draw attention to a recent U.S. Food and Drug Administration safety labeling change for the management of patients taking sodium glucose cotrans-porter – 2 inhibitor medications that was released after the acceptance of this manuscript for publication. In March 2020, the Food and Drug Administration issued an advisory suggesting that canagli ozin, dapagli ozin, and empagli- ozin should all be discontinued 3 days before elective sur-gery, and ertugli ozin should be discontinued 4 days before elective surgery due to the risk of postoperative euglycemic diabetic ketoacidosis. 2 The additional recommended day for discontinuation of ertugli ozin appears to be related to its slightly longer half-life relative to canagli ozin, dapagli- ozin, and empagli ozin to ensure appropriate elimination of the medication before the day of surgery. In light of this guidance and existing literature, we believe that it may be appropriate to hold these medications for 3 to 4 days before surgery, especially in patients who may have a prolonged decrease in nutritional intake in the postoperative period.
Competing Interests
The author declares no competing interests.
Stephen Harrison Gregory , M.D. Washington University in St. Louis, St. Louis, Missouri. [email protected]
DOI: 10.1097/ALN.0000000000003625
References
1. Preiser JC , Provenzano B , Mongkolpun W , Halenarova K , Cnop M : Perioperative management of oral glu-cose-lowering drugs in the patient with type 2 diabe-tes. A nesthesiology 2020 ; 133 : 430 – 8
2. Thiruvenkatarajan V , Meyer EJ , Nanjappa N , Van Wijk RM , Jesudason D : Perioperative diabetic ketoacido-sis associated with sodium-glucose co-transporter-2
inhibitors: A systematic review. Br J Anaesth 2019 ; 123 : 27 – 36
(Accepted for publication October 29, 2020. Published online fi rst on December 2, 2020.)
Perioperative Management of Glucose-lowering Drugs: Comment
To the Editor:
We read with interest the review by Prieser et al . on the perioperative management of oral glucose-lowering
agents in patients with type 2 diabetes mellitus. 1 The authors recommend (table 1) that sodium glucose cotransporter – 2 inhibitors be ceased 24 h before elective interventions. 1
No allowance is made for the severity of the procedure (minor vs. major surgery) or type of procedure. However, the authors do acknowledge that other sources recommend a longer duration of withholding these medications before elective procedures. Ceasing them just on the day of the procedure may be suitable for minor interventions where early oral intake is possible. For procedures where return to preoperative state is expected to be delayed, some gov-erning bodies recommend withholding these agents more than 24 h. The Australian Diabetes Society (Melbourne, Australia) recommends withholding 2 days before surgery and also on the day of the procedure in such scenarios. 2 The half-lives of canagli ozin, dapagli ozin, and empagli ozin range between 12 to 13 h, and hence, withholding them for four to ve half-lives (around 50 to 65 h) is likely to ensure complete washout of the drug at the time of sur-gery. 3 As the half-life of ertugli ozin is 16 h, a more pro-longed interruption may be required. The U.S. Food and Drug Administration (Silver Spring, Maryland) has recently approved a label change to sodium glucose cotransporter – 2 inhibitors interruption before elective surgery. It recom-mends a 3-day cessation for canagli ozin, dapagli ozin, and empagli ozin, and 4 days for ertugli ozin. 4
Euglycemic ketoacidosis is a rare, but serious complica-tion associated with perioperative sodium glucose cotrans-porter – 2 inhibitors therapy. 5 Few reports have shown that
ALNV134N2_Text.indb 349ALNV134N2_Text.indb 349 29-Dec-20 19:44:2729-Dec-20 19:44:27
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
350 Anesthesiology 2021; 134:349–56 CORRESPONDENCE
CORRESPONDENCE
the pharmacologic e ects of sodium glucose cotrans-porter – 2 inhibitors are likely to last beyond ve half-lives of elimination (2 to 3 days). 6 – 8 Prolonged glycosuria and ketonemia persisting up to 9 to 10 days after discontinua-tion of sodium glucose cotransporter – 2 inhibitors therapy have been described with euglycemic ketoacidosis pre-sentations both in the surgical 6 , 7 and nonsurgical settings. 8
Persistent glycosuria with minimal elevation of blood glu-cose was a key manifestation in those cases, highlighting an ongoing e ect of these agents. Considering the half-lives of these agents, the renal e ects should not have lasted beyond 2 to 3 days. Nonetheless, glycosuria (and metabolic e ects) continued until 8 to 9 days with blood glucose values below the renal threshold of glucose. Sustained binding of these medications to renal transport proteins despite plasma elim-ination has been suggested as a possible mechanism of this prolonged e ect. 7
Competing Interests
Supported by The Hospital Research Foundation Project Grant (Adelaide, Australia; grant is yet to be operative due to COVID-19 restrictions; to Drs. Jesudason, Meyer, and Thiruvenkatarajan), a Diabetes South Australia Research Grant (Adelaide, Australia; grant is yet to be operative due to COVID-19 restrictions; to Drs. Jesudason, Meyer, and Thiruvenkatarajan), and an A. R. Clarkson Scholarship, Royal Adelaide Hospital Research Fund (Adelaide, Australia; to Dr. Meyer). The remaining authors declare no competing interests.
Venkatesan Thiruvenkatarajan , M.D., D.N.B., F.A.N.Z.C.A. , David Jesudason, F.R.A.C.P., Ph.D. , Nagesh Nanjappa,
M.D., D.N.B., F.A.N.Z.C.A. , Emily Jane Meyer, M.B.B.S., F.R.A.C.P. , Roelof M. Van Wijk, Ph.D., F.A.N.Z.C.A. The Queen
Elizabeth Hospital, Woodville, Australia (V.T.). [email protected]
DOI: 10.1097/ALN.0000000000003626
References
1. Preiser JC , Provenzano B , Mongkolpun W , Halenarova K , Cnop M : Perioperative management of oral glu-cose-lowering drugs in the patient with type 2 diabe-tes. A nesthesiology 2020 ; 133 : 430 – 8
2. Australian Diabetes Society : Periprocedural diabetic ketoacidoss (DKA) with SGLT2 inhibitor use . January 2020 . Available at: https://diabetessociety.com.au/doc-uments/ADS_DKA_SGLT2i_Alert_update_2020.pdf. Accessed June 18, 2020.
3. Chacko B , Murray K , Whitley M , Beckmann U , Rowley M : In reply. Anaesth Intensive Care 2018 ; 46 : 425
4. FDA Drug Safety Communication : FDA revises labels of SGLT2 inhibitors for diabetes to include warnings about too much acid in the blood and serious urinary tract infections. March 2020 . Available at: https://www.fda.gov/drugs/drug-safety-and-availability/fda-re-vises-labels-sglt2-inhibitors-diabetes-include-warn-ings-about-too-much-acid-blood-and-serious urinary tract infections . Accessed June 20, 2020.
5. Thiruvenkatarajan V , Meyer EJ , Nanjappa N , Van Wijk RM , Jesudason D : Perioperative diabetic ketoacido-sis associated with sodium-glucose co-transporter-2 inhibitors: A systematic review. Br J Anaesth 2019 ; 123 : 27 – 36
6. Wang KM , Isom RT : SGLT2 inhibitor-induced eugly-cemic diabetic ketoacidosis: A case report. Kidney Med 2020 ; 2 : 218 – 21
7. Kohli J , Goldfarb S : Quiz: Metabolic acidosis in a patient with type 2 diabetes. Am J Kidney Dis 2017 ; 69 : A11 – 3
8. Pujara S , Ioachimescu A : Prolonged ketosis in a patient with euglycemic diabetic ketoacidosis secondary to dapagli ozin. J Investig Med High Impact Case Rep 2017 ; 5 : 2324709617710040
(Accepted for publication October 29, 2020. Published online fi rst on December 2, 2020.)
Perioperative Management of Glucose-lowering Drugs: Reply
In Reply:
We thank Dr. Gregory and Thiruvenkatarajan et al . for their positive comments on our review 1 and
for pointing out the label change by the U.S. Food and Drug Administration (Silver Spring, Maryland), which appeared after our review was accepted for publication. We fully agree that it is appropriate and to be recommended to withhold sodium glucose cotransporter – 2 inhibitors 3 to 4 days before surgery to avoid euglycemic diabetic ketoacidosis. Ketoacidosis in people with diabetes is not proportional to the degree of hyperglycemia 2 and may be, treacherously, euglycemic in patients taking sodium glu-cose cotransporter – 2 inhibitors. Anesthesiologists should be aware of the risk of this serious complication.
ALNV134N2_Text.indb 350ALNV134N2_Text.indb 350 29-Dec-20 19:44:2729-Dec-20 19:44:27
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Correspondence
Correspondence Anesthesiology 2021; 134:349–56 351
Competing Interests
The authors declare no competing interests.
Jean-Charles Preiser , M.D., Ph.D. , Miriam Cnop , M.D., Ph.D. Erasmus Hospital, Universit é Libre de Bruxelles, Brussels, Belgium (J.-C.P.). [email protected]
DOI: 10.1097/ALN.0000000000003627
References
1. Preiser JC , Provenzano B , Mongkolpun W , Halenarova K , Cnop M : Perioperative management of oral glu-cose-lowering drugs in the patient with type 2 diabe-tes. A nesthesiology 2020 ; 133 : 430 – 8
2. Sheikh-Ali M , Karon BS , Basu A , Kudva YC , Muller LA , Xu J , Schwenk WF , Miles JM : Can serum beta-hy-droxybutyrate be used to diagnose diabetic ketoacido-sis? Diabetes Care 2008 ; 31 : 643 – 7
(Accepted for publication October 29, 2020. Published online fi rst on December 2 2020.)
Burst-suppression and Postoperative Delirium: Comment
To the Editor:
The recent report by Pedemonte et al. 1 of their substudy of the Minimizing ICU Neurologic
Dysfunction with Dexmedetomidine-induced Sleep (MINDDS) study 2 emphasized the relationship between electroencephalogram (EEG) burst-suppression during cardiopulmonary bypass and delirium in elderly patients undergoing cardiac surgery. It raises several important points regarding the potential for cerebral monitoring to identify patients who may be at risk for signi cant postoperative neurologic complications, including delir-ium and postoperative cognitive dysfunction. However, interpreting these complex relationships requires certain safeguards to minimize the risk of potential false discov-ery, and thus maximize the con dence in a study ’ s con-clusions. These safeguards include, but are not limited to, clear adherence to the prespeci ed substudy aims and a priori hypotheses, the development of a data statistical
analytic plan before accessing the data, and consider-ation to the potential moderating e ects in the substudy from the intervention of the parent trial. In this case, for example, the data from the substudy were derived from an ongoing randomized controlled trial investigating the potential e ects of dexmedetomidine on postoperative delirium. It would seem reasonable then for any analysis in the substudy to be adjusted for the use of dexmede-tomidine. Clari cation as to whether and how this was done would be useful.
Several other aspects of their study might also ben-e t from additional clarity. For example, adherence of reporting to the ordered prestated hypotheses seems to have been modi ed. For example, the primary hypothe-sis stated in their introduction was that “ preexisting cog-nitive impairment accounts for electroencephalogram burst-suppression during CPB. ” 1 It is curious, then, that the article ’ s title, and the subsequent analysis and reporting of the study, principally focuses on postoperative delir-ium as opposed to preexisting cognitive impairment. This is particularly notable because their power analysis states that the “ primary objective of the study was to detect the di erence in mean preoperative cognitive scores between the burst-suppression and no burst-suppression groups. ” 1
The current delirium analysis, as they state, was likely underpowered.
Although there is a potentially important relationship between preexisting cognitive impairment and delir-ium, and one that could be plausibly mediated via EEG burst-suppression, the primary analysis reported should have been the relationship between baseline cognition and EEG burst suppression, with the delirium-related analy-ses being secondary, and/or exploratory, and fully adjusted for multiple comparisons. Indeed, although some mention is made of adjustments to reduce false discovery, it is not clear where and how these were done. Furthermore, as the authors stated that the “ data and statistical analyses plans were de ned and written after the data were accessed, ” 1 it is not clear how much data and analyses mining might have been undertaken before these complex analyses were set-tled on and which results were chosen to be reported. The study ’ s actual primary objective found that the relationship between preexisting cognition (assessed using the abbrevi-ated Montreal cognitive assessment) and EEG burst-sup-pression was not statistically signi cant ( P = 0.965 in their table 1).
These limitations should not dissuade the reader from considering the potentially important relationships that the authors have described, because they may in fact be quite meaningful. However, without adequate adjustment for the unit of randomization, consideration for the analytical plan being developed after the data was accessed, and the subse-quent organization of the results around a hypothesis that was not the primary one, it does raise the question as to whether undue emphasis is being placed on the “ positive ”
ALNV134N2_Text.indb 351ALNV134N2_Text.indb 351 29-Dec-20 19:44:2829-Dec-20 19:44:28
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
352 Anesthesiology 2021; 134:349–56 CORRESPONDENCE
CORRESPONDENCE
results surrounding delirium, as opposed to the “ negative ” results related to baseline cognition.
Competing Interests
The author declares no competing interests.
Hilary P. Grocott , M.D., F.R.C.P.C., F.A.S.E . University of Manitoba, Winnipeg, Manitoba, Canada.
DOI: 10.1097/ALN.0000000000003631
References
1. Pedemonte JC , Plummer GS , Chamadia S , Locascio JJ , Hahm E , Ethridge B , Gitlin J , Ibala R , Mekonnen J , Colon KM , Westover MB , D ’ Alessandro DA , Tolis G , Houle T , Shelton KT , Qu J , Akeju O : Electroencephalogram burst-suppression during car-diopulmonary bypass in elderly patients mediates post-operative delirium. A nesthesiology 2020 ; 133 : 280 – 92
2. Shelton KT , Qu J , Bilotta F , Brown EN , Cudemus G , D ’ Alessandro DA , Deng H , DiBiasio A , Gitlin JA , Hahm EY , Hobbs LE , Houle TT , Ibala R , Loggia ML , Pavone KJ , Shae S , Tolis G , Westover MB , Akeju O : Minimizing ICU Neurological Dysfunction with Dexmedetomidine-induced Sleep (MINDDS): Protocol for a randomised, double-blind, parallel-arm, placebo-controlled trial. BMJ Open 2018 ; 8 : e020316
(Accepted for publication October 30, 2020. Published online fi rst on December 2, 2020.)
Burst-suppression and Postoperative Delirium: Reply
In Reply:
We thank Dr. Grocott 1 for his interest in our article. 2
We share his stated commitment to the core tenets of clear and transparent reporting that support scienti c reproducibility. In pursuit of this commitment, we prereg-istered (NCT02856594) and published the parent clinical trial protocol, including key elements of the statistical anal-ysis plan, 3 and clearly communicated the context of the analyses underlying our retrospective cohort substudy. 2
Dr. Grocott ’ s concerns primarily relate to our stated hypotheses and the accompanying inferential framework, nalizing our inferential framework after data access, and the positive results we emphasized. We contend that Dr. Grocott ’ s letter raises some of the challenges inherent to the closed peer review process and the need for continued education on the nuances innate to interpreting multivari-able regression models. At initial submission, we hypoth-esized an association between cognitive impairment and burst-suppression during cardiopulmonary bypass. For our inferential framework, we constructed a covariate-adjusted logistic regression model. During the peer review process, it was rightfully suggested that an analysis of postoperative delirium was of interest to our specialty despite the dou-ble-blinded ongoing parent trial. Therefore, in our revised submission, we stated an additional hypothesis, “ electroen-cephalogram burst-suppression during cardiopulmonary bypass mediates the e ect of cognitive impairment on delirium. ” Restating our initial hypothesis or increasing our sample size, at this stage, ran counter to our commitment to clear and transparent reporting (please see the Limitations section of our Discussion for the explicit acknowledg-ment that we powered our study to analyze the association between abbreviated Montreal Cognitive Assessment scores and burst suppression during cardiopulmonary bypass). Thus, our nal analysis method was re ned after the initial data were accessed to accommodate additional inferences on delirium. Indeed, we intended to convey this by the pro-vided statement concerning the development of the statisti-cal analyses after accessing the data. We acknowledge that it would have been even more precise to have stated that the analyses were modi ed during peer review.
It is important to note that we did not refer to any of our hypotheses as “ the ” hypothesis. This is because electro-encephalogram hypotheses emanating from the parent trial are exploratory, as stated in our trial protocol. 3 We addressed both our hypotheses using a structural equation model framework, which implied two estimation stages. Thus, we did not deviate from the inferential framework we used at initial submission. Speci cally, we estimated the association between burst-suppression during cardiopulmonary bypass and numerous variables in a multivariable model, includ-ing the abbreviated Montreal Cognitive Assessment, our cognitive variable of interest. This regression model should be interpreted as follows: adjusting for covariates of inter-est, the study authors asked whether cognitive impairment was associated with intraoperative electroencephalogram burst-suppression during cardiopulmonary bypass. The nal model result, which addressed this hypothesis, is appro-priately summarized in the causal diagram we presented in gure 3 (please see supplemental table 7 for univariate results). 2
In the second stage of estimation, we examined the association between delirium and the same variables in the rst stage with the addition of burst suppression. This
ALNV134N2_Text.indb 352ALNV134N2_Text.indb 352 29-Dec-20 19:44:2829-Dec-20 19:44:28
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Correspondence
Correspondence Anesthesiology 2021; 134:349–56 353
regression model should be interpreted as follows: adjusting for covariates of interest, the study authors asked whether burst suppression was associated with delirium. We reported point estimates and 95% CI for this association, and oth-ers, to allow readers to evaluate our e ect sizes and their plausible values. Thus, we ttingly minimized the sole use of P values for inferences as we fully understand that the use of null hypothesis testing can be challenging in anal-yses with nontrivial model uncertainties. Draper 4 provides additional background that helps with interpreting and assessing model uncertainties. Nevertheless, we reported False Discovery Rate P values to help the reader interpret hypothesis tests where appropriate ( i.e. , univariate regres-sion) throughout the article.
We acknowledge that most studies are rarely de nitive. As such, and as stated in our Discussion, 2 our study would bene t from replication studies, including those that adjust for covariates such as dexmedetomidine or multi-com-ponent delirium prevention interventions. However, we believe that the burst-suppression ndings and the poten-tially modi able physical function ndings we reported deserved due emphasis because they are biologically plausi-ble and have clinical implications.
Research Support
Supported by the National Institute on Aging, National Institutes of Health (Bethesda, Maryland; grant No. RO1AG053582; to Dr. Akeju).
Competing Interests
Dr. Akeju has received speaker ’ s honoraria from Masimo Corporation (Irvine, California) and is listed as an inventor on pending patents on electroencephalography monitor-ing and sleep that are assigned to Massachusetts General Hospital (Boston, Massachusetts). Dr. Houle reports nancial relationships with GlaxoSmithKline (Brentford, London, United Kingdom), Eli Lilly (Indianapolis, Indiana), and StatReviewer (North Andover, Massachusetts). The remaining authors declare no competing interests.
Juan C. Pedemonte , M.D. , Joseph J. Locascio , Ph.D. , Timothy Houle , Ph.D. , Oluwaseun Akeju , M.D., M.M.Sc . Massachusetts
General Hospital, Boston, Massachusetts (O.A.). [email protected]
DOI: 10.1097/ALN.0000000000003632
References
1. Grocott HP : Burst-suppression and postoperative delir-ium: Comment. A nesthesiology 2020 ; 134 : 351 – 2
2. Pedemonte JC , Plummer GS , Chamadia S , Locascio JJ , Hahm E , Ethridge B , Gitlin J , Ibala R , Mekonnen J , Colon KM , Westover MB , D ’ Alessandro DA ,
Tolis G , Houle T , Shelton KT , Qu J , Akeju O : Electroencephalogram burst-suppression during car-diopulmonary bypass in elderly patients mediates postoperative delirium. A nesthesiology 2020 ; 133 : 280 – 92
3. Shelton KT , Qu J , Bilotta F , Brown EN , Cudemus G , D ’ Alessandro DA , Deng H , DiBiasio A , Gitlin JA , Hahm EY , Hobbs LE , Houle TT , Ibala R , Loggia ML , Pavone KJ , Shae S , Tolis G , Westover MB , Akeju O : Minimizing ICU Neurological Dysfunction with Dexmedetomidine-induced Sleep (MINDDS): Protocol for a randomised, double-blind, paral-lel-arm, placebo-controlled trial. BMJ Open 2018 ; 8 : e020316
4. Draper D : Assessment and propagation of model uncertainty. J Royal Stat Soc 1995 ; 57 : 45 – 70
(Accepted for publication October 30, 2020. Published online fi rst on December 2, 2020.)
Balanced Crystalloid versus0.9% Sodium Chloride: What We Overlook in Our Research
To the Editor:
Infusions of crystalloid solutions are currently recommended for the treatment of critically ill patients with various patho-
logic conditions, including bleeding, sepsis, and trauma. 1 – 3 A large number of prospective randomized multicenter studies on the comparative analysis of 0.9% sodium chloride and balanced crystalloid have examined their e cacy and safety. However, the answer to the question of whether the crystal-loid composition a ects the treatment outcome in critically ill patients has not yet been received. 1 It should be noted that currently, when assessing the pharmacodynamic e ects of crys-talloid solutions, their actual physicochemical parameters, such as osmolality and pH, are not taken into account. Researchers prefer to use theoretically calculated parameters, and in our opinion, this reduces the accuracy of the results. The fact is that the theoretical osmolarity values of solutions can di er signi -cantly from their actual osmolality values. We suggested that the same crystalloid solutions provided by di erent manufac-turers may have di erent values of both osmolality and pH. To prove that, we studied physicochemical parameters (osmolality
ALNV134N2_Text.indb 353ALNV134N2_Text.indb 353 29-Dec-20 19:44:2829-Dec-20 19:44:28
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
354 Anesthesiology 2021; 134:349–56 CORRESPONDENCE
CORRESPONDENCE
and pH) of 0.9% sodium chloride by di erent manufacturers. We chose 0.9% sodium chloride because this crystalloid solu-tion is used as a reference in all randomized controlled studies on the pharmacodynamics of crystalloid solutions. The analy-sis of 0.9% sodium chloride osmolality was carried out with the help of vapor pressure osmometer model 5600 (Wescor Inc., USA). The actual pH of each solution was determined using the product speci cation sheet of 0.9% sodium chlo-ride of a certain series. The analysis of the studied physico-chemical parameters of certain series of 0.9% sodium chloride by eight di erent manufacturers revealed that the osmolality value range was from 278 mmol/kg (270319 series, Biosintez, Russia) to 305 mmol/kg (160115 series, Zavod Medsintez, Russia), and the pH value range was from 5.4 (14791119 series, Grotex, Russia) to 6.3 (B7571218 series, Pharmasyntez Tyumen, Russia). The results obtained indicate that 0.9% sodium chloride by di erent manufacturers has di erent phys-icochemical properties. Considering the fact that during the treatment of critically ill patients 0.9% sodium chloride can be introduced into the patient ’ s body in large volumes, the osmolality and pH of the solution may have a great impact on the pharmacodynamic e ect. Determining the actual values of the physicochemical parameters of 0.9% sodium chloride and balanced crystalloid can increase the accuracy of the results of randomized multicenter studies in the future.
Competing Interests
The authors declare no competing interests.
Anton Kasatkin , Ph.D. , Aleksandr Urakov , M.D . , Anna Nigmatullina , Mikhail Kopytov. Izhevsk State Medical
Academy, Izhevsk, Russia (A.K.). [email protected]
DOI: 10.1097/ALN.0000000000003614
References
1. Story DA : Intravenous uids: Which recipe? A nesthesiology 2020 ; 132 : 609 – 11
2. Lewis SR , Pritchard MW , Evans DJ , Butler AR , Alderson P , Smith AF , Roberts I : Colloids versus crys-talloids for uid resuscitation in critically ill people. Cochrane Database Syst Rev 2018 ; 8 : CD000567
3. Semler MW , Self WH , Wanderer JP , Ehrenfeld JM , Wang L , Byrne DW , Stollings JL , Kumar AB , Hughes CG , Hernandez A , Guillamondegui OD , May AK , Weavind L , Casey JD , Siew ED , Shaw AD , Bernard GR , Rice TW ; SMART Investigators and the Pragmatic Critical Care Research Group : Balanced crystalloids versus saline in critically ill adults. N Engl J Med 2018 ; 378 : 829 – 39
(Accepted for publication October 16, 2020. Published online fi rst on November 9, 2020.)
A Contemporary Reading List
To the Editor:
Have time to read during the pandemic? Want to explore ideas about clinical care, humanism in medi-
cal practice, and how best to promote wellness and support diversity and inclusion?
A reading list can help you gather information from multiple authors who have tackled these issues. Viewing and analyzing their perspectives, revealed in the books they have written, will expand your ability to formulate your mindset on these ponderables.
Educator Edward C. Halperin, M.D., M.A. (Chancellor/Chief Executive O cer, New York Medical College, and Provost for Biomedical A airs Touro College and University System, New York), recently developed an insightful per-spective to answer these questions. 1 Halperin was asked by a second-year medical student how to answer the rst-year medical student ’ s query about what to read before entering medical school. In crafting an answer, Halperin recognized that a meaningful recommendation comes from the uni-verse of books that a physician-in-training (I submit that the same is true for physicians and anesthesiologists and intensivists, speci cally) can read from a variety of venues: novels, books about medical heroes, specialties, race and medicine, infectious disease and diagnostics, and mortality or the nature of medical practice. 1
In a concise and poignant manner, Halperin provided the requested reading list, employing mini “ book reviews ” of di erent works from the aforementioned categories. Halperin ’ s perspective provides examples of classics in each of the six categories with comparative and contrasting observations of their educational value.
Peruse Halperin ’ s reading list and gain insight into medi-cal practice, wellness, diversity, and inclusion. Halperin aptly reminds us:
“ This con rms the wisdom of the late Edmund Pelligrino[ * ], ‘ Medicine is the most scienti c of the humanities and the most humane of sciences. It bridges the physical state of the human being with her
* “ Edmund D. Pellegrino (June 22, 1920 to June 13, 2013)...an American bioethicist and academic...Pellegrino was a distinguished professor of medicine and medical ethics and the Director of the Kennedy Institute of Ethics at Georgetown University...an expert both in clinical bioethics, and in the fi eld of medicine and the humanities, specifi cally, the teaching of humanities in medical school... ” From: Wikipedia con-tributors. Edmund Pellegrino. Wikipedia, The Free Encyclopedia. August 2, 2020 at 23:08 UTC. Available at: https://en.wikipedia.org/wiki/Edmund_Pellegrino . Accessed October 11, 2020.
ALNV134N2_Text.indb 354ALNV134N2_Text.indb 354 29-Dec-20 19:44:2829-Dec-20 19:44:28
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Correspondence
Correspondence Anesthesiology 2021; 134:349–56 355
psychological state, and I daresay with her spiritual state...That is not just a person ’ s religion, but those transcendent aspects of what she is — and values — be-yond the merely material domains of being. ’ ” 1 , 2
Competing Interests
The author declares no competing interests.
Alan Jay Schwartz , M.D., M.S.Ed. The Children ’ s Hospital of Philadelphia, and Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania. schwartza@email.
chop.edu
DOI: 10.1097/ALN.0000000000003616
References
1. Halperin EC : A summer reading list for new medical students during a pandemic. The Pharos 2020 ; 83 : 16 – 20
2. Giordano J : Foni phronimos - An interview with Edmund D. Pelligrino. Philosophy, Ethics, and the Humanities in Medicine 2010 ; 5 : 16
(Accepted for publication October 16, 2020. Published online fi rst on November 18, 2020.)
Podcasts from ANESTHESIOLOGY Promoting Medical English Learning in Non – English-speaking Countries
To the Editor:
Podcasts have become increasingly popular tools for medical education in recent years. Podcasts are readily
accessible to medical sta via computers or smartphones, which provide a convenient and useful way to engage learners in an easily consumed format and democra-tize knowledge from various resources. 1 , 2 Moreover, the information conveyed by podcasts does not need to be linked with any particular time or location. In the con-text of anesthesiology, it has been reported that half of the anesthesia residents included in a study used di erent podcasts as part of routine studying. 3 Many professional
magazines have their own podcasts; however, these pod-casts are mostly in English, and thus, they are usually dif- cult for medical sta in non – English-speaking countries to understand.
In non – English-speaking countries, medical English is an indispensable tool for medical sta to acquire new knowledge, publish articles, and participate in interna-tional exchanges. Therefore, it is necessary to learn some medical English at the residency stage, which is import-ant for the growth and career development of medical students. However, in our education system, after med-ical students leave school for clinical practice training, they seldom enroll in medical English courses, and few of them have the habit of actively learning medical English. In addition, the main form of medical English teaching in China involves reading medical English books. With these books, students can improve their medical vocab-ulary, acquire professional knowledge, and improve their reading ability. However, there are few available profes-sional English listening and speaking training courses. On the other hand, medical English books may not provide the latest research trends and knowledge updates of the specialty.
Fortunately, each issue of Anesthesiology has a pod-cast of the important articles of our specialty selected by editors. The research background, design, main purpose, results, and nal conclusions of each important clinical, laboratory research, or focus review article are intro-duced in a professional way in these podcasts. The con-tents of these podcasts are very helpful in following the latest research trends and knowledge updates in the eld of anesthesiology. Therefore, we selected these podcasts of Anesthesiology in English as our teaching materials for anesthesiology residents to help them learn medical English and pay attention to new knowledge updates and research trends in our specialty and to inspire clinical and basic research ideas.
We have already implemented this study program for more than 1 yr, and we learned the contents of the podcasts collectively. The following steps were implemented:
1. Podcasts with transcripts of each issue were downloaded from the website of Anesthesiology . We rst listened to these podcasts together, and then allowed residents repeat the contents or perform translations, followed by correction of the podcast transcript. Finally, we discussed research ideas from each study.
2. After a period of learning, the teachers conducted assess-ments, collected feedback of the learning, and made nec-essary adjustments according to the feedback.
3. Through a long-term study, the residents of our spe-cialty listen to podcasts as a regular habit to learn medical English, and the residents may generate research ideas and carry out clinical and basic research work in the future.
ALNV134N2_Text.indb 355ALNV134N2_Text.indb 355 29-Dec-20 19:44:2829-Dec-20 19:44:28
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

356 Anesthesiology 2021; 134:349–56 CORRESPONDENCE
CORRESPONDENCE
The residents of our specialty have shown great improve-ments both in terms of their medical English level and scientific research ideas (as shown by increased medi-cal English vocabulary, improved translation ability and listening level, and having some preliminary research plans), and most of them have formed the habit of lis-tening to podcasts from Anesthesiology regularly. We sincerely thank Anesthesiology for providing excel-lent podcasts for medical staff in non – English-speaking countries. Using these podcasts, our residents not only learn medical English but also pay attention to new knowledge updates and research trends in our specialty. Last, we emphasize and support spreading the pod-cast-based learning as a routine medical English teaching program for medical residents of non – English-speaking countries.
Competing Interests The authors declare no competing interests.
Chao Liang , Ph.D., Xiaoguang Zhang , Ph.D., Fang Fang , Ph.D., Jing Cang , M.D., Changhong Miao , Ph.D. Zhongshan
Hospital, Fudan University, Shanghai, China (C.M.). [email protected]
DOI: 10.1097/ALN.0000000000003621
References
1. Lomayesva NL , Martin AS , Dowley PA , Davies NW , Olyha SJ , Wijesekera TP : Five medical education pod-casts you need to know. Yale J Biol Med 2020 ; 93 : 461 – 6
2. Chin A , Helman A , Chan TM : Podcast use in under-graduate medical education. Cureus 2017 ; 9 : e1930
3. Matava CT , Rosen D , Siu E , Bould DM : eLearning among Canadian anesthesia residents: A survey of podcast use and content needs. BMC Med Educ 2013 ; 13 : 59
(Accepted for publication October 23, 2020. Published online fi rst on November 23, 2020.)
ALNV134N2_Text.indb 356ALNV134N2_Text.indb 356 29-Dec-20 19:44:2829-Dec-20 19:44:28
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

ERRATUM
ANESTHESIOLOGY, V 134 • NO 2 FEBRUARY 2021 357
Pectoralis-II Myofascial Block and Analgesia: Comment: Erratum
In the letter beginning on page 1602 in the June 2020 issue, the author ’ s name “ Steve Melton ” is incorrect. The correct name is “ M. Stephen Melton. ”
The authors regret this error. The online version and PDF of the letter have been corrected.
DOI: 10.1097/ALN.0000000000003634
Reference
Gebhard RE , Nielsen KC , Melton S , Greengrass RA : Pectoralis-II myofascial block and analgesia: Comment. A nesthesiology 2020 ; 132 : 1602 – 4
ALNV134N2_Text.indb 357ALNV134N2_Text.indb 357 29-Dec-20 19:44:2829-Dec-20 19:44:28
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
WHERE FINDINGSBECOMEFOUNDATIONSA1 )-0 B*h18 10.80h i/ &00h6h09i0B08 h010.hg- i/ &0hi*&0h.)i90D ghi)ig.1 g.h0D ./8 &.i/ -08igi/0D B0’h0 /*) 1i-&12 &0(1i1-i// 5i/8i//1—B0’h0 &0(1i1-i// h010.hg- Bi)- i--08i.)0 i-&.g) ./8 0/80hi//5*0/8.)i*/.1 9.100:
Vi1i)
hh&&''ssllyy**AA,,--ii''uu--ii&&..ll..//yy--AAgg''uu..11ii )* 10(-i) . -./01ghi&
##44 II--&&..gg)) FF..gg))**hh 77,,;;6677——))--00 --ii//--0011)) 009900hh ii// ))--0055ii001188iiww !!"" aa ccii))..))ii**// --..11556611ii5500 **55 4444 2200..hh&&*
<;24,ce: *o89 324,#a% 671ac' Fac'2,, 324,#a% Ci'a'i2# 0e12,'* /C%a,i-a'e A#a%y'ic*, *o*o)
ALNV134N2_Text.indb 358ALNV134N2_Text.indb 358 29-Dec-20 19:44:2829-Dec-20 19:44:28
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

Anesthesiology, V. 134, No. 2, February 2021 A19Anesthesiology, V. 129, No. 4, October 2018 A31Anesthesiology, V 118, No. 5, May 2013 A23
LWW’s All Access Recruitment bundle offers advertisers access to the strongest portfolio of print jour-nals, websites and iPad® apps in medical media. Build anddeploy a powerful and targeted campaign to raise aware-ness and drive results anytime, anywhere and across allplatforms. Contact an LWW Sales Specialist to learn more.
For rates and deadlines, visit:www.lwwratecards.com
Contact:Keida SpurlockTwo Commerce Square2001 Market StreetPhiladelphia, PA [email protected]
Marketing solutions for Career, Education and Events advertisers.
Careers & Events
or
Full-time Anesthesiology Faculty Positions
Equal Opportunity Employer, M/F/D/V
The Department of Anesthesiology at the University of Mississippi Medical Center seeks applicants for full-time faculty positions who have a strong interest in clinical teaching. The ideal candidate should have a fellowship, additional background or training in OB, neuro, ICU, cardiac, liver transplant, pediatric, pediatric cardiac anesthesia. Those with TEE certification are also encouraged to apply. The applicant must be an M.D., D.O. or BC/BE. The appointment is at the tenure or non-tenure accruing level of assistant, associate, and full professor. Benefits are excellent and salary is extremely competitive (75% AAMC) and the work schedule is outstanding. The city of Jackson is a hidden treasure that is centrally located in the state and has numerous amenities. The Department of Anesthesiology, with a newly appointed, academically oriented chair, is a growing part of a large multispecialty medical center with excellent departments and hospitals.
Please send CV and letter of interest to: , c/o Department of Anesthesiology
The University of Mississippi Medical Center2500 North State Street, Jackson, MS, 39216-4505or
Delois Felder
The Department of Anesthesiology, Perioperative and Pain Medicine at Stanford University seeks a board certified or equivalent anesthesiologist to join the Department as Assistant Professor in the University Tenure Line.
™ The predominant criterion for appointment in the University Tenure Line is a major commitment to research and teaching.
The successful applicant should have developed an academic laboratory-based program in cardiovascular pharmacology relevant to the field of anesthesiology.
The successful applicant will spend a portion of time in clinical anesthesia.
We are particularly interested in candidates who have received national peer-reviewed funding at the K99 or R01 level.
Stanford University is an equal opportunity employer and is committed to increasing the diversity of its faculty. It welcomes nominations of and applications from women and members of minority groups, as well as others who would bring additional dimensions to the university’s research, teaching and clinical missions.
Department of AnesthesiologyUniversity Tenure Line
Submit CV, a brief letter, and three letters of reference to:Dr. Ronald G. Pearl, Chair, Department of Anesthesiology, Perioperative and Pain Medicine, Stanford University School of Medicine, Stanford, California 94305-5640
ALNclass118_5:May 2013 4/7/2013 10:42 AM Page 23
Excellent General/Cardiac Anesthesiology Opportunity*** Any academic rank (new grads welcome) ***
Saint Louis University, a Catholic Jesuit institution dedicated to stu-dent learning, research, health care, and service is seeking faculty with outstanding clinical abilities who share a commitment to high-quality medical care, education and professional development for an appointment at the assistant professor level in the department of Anesthesiology and Critical Care primarily at Saint Louis University Hospital.
The department is seeking candidates with interest in general OR Anesthesia with special interest and experience in cardiac anesthe-sia (fellowship in cardiac anesthesia required). Duties will include clinical service and teaching, with administrative and research op-portunities based on interest. The department serves a tertiary care hospital and a preeminent private children’s hospital with outlying ambulatory care facilities for pediatric patients. The department also encompasses an ambulatory surgery center and designated research facilities.
Candidates must be board eligible or certified in Anesthesiology and qualify for medical licensure in the State of Missouri. Interested candidates should contact us for additional information and/or send current curriculum vitae to: Wolf H. Stapelfedlt, M.D., Professor & Chairman, Department of Anesthesiology & Critical Care Medicine, St. Louis University/Cardinal Glennon Medical Center, Desloge Towers, 3rd Floor, 3635 Vista Avenue at Grand Boulevard, St. Louis, Missouri 63110; (314)268-7267; [email protected]
www.nwas.com | (800) 222-6927
Conferences to fit your busy schedule20–24 CME/CEC | Land Tours, Cruises, & Major Metropolitan Areas
Current Topics in Anesthesia Phoenix, ArizonaJanuary 8–11, 2019
Relevant Topics in AnesthesiaSan Juan, Puerto Rico
January 14–18, 2019
Topics in AnesthesiaTruckee (Lake Tahoe), California
January 28 – 2/1, 2019
EKG Interpretation SeminarLas Vegas, Nevada
February 4, 2019
Hot Topics in Anesthesia + ACLS/PALSLas Vegas, Nevada
February 5–8, 2019
Anesthesia UpdateKona, Hawaii
February 11–14, 2019
Current Topics in AnesthesiaOrlando, Florida
February 14–17, 2019
Clinical Concerns in Anesthesia10-Night Brazil Cruise
February 17–27, 2019
Clinical Concerns in AnesthesiaEcuador and The Galapagos Islands Land and Sea Tour
February 17–28, 2019
Register or discover more dates and locations on our website.
Visit Us at Anesthesiology 2018 Booth #1404
LWW’s All Access Recruitment bundle offers advertisers
access to the strongest portfolio of print journals, and
online advertising in medical media. Build and deploy a
powerful and targeted campaign to raise awareness and
drive results anytime, anywhere and across all platforms.
Contact an LWW Sales Specialist to learn more.
For rates and dealines, visit:
advertising.lww.com
Contact
Dave Wiegand
847-361-6128
Chief, Division of Pediatric Anesthesia and Medical Director of Procedural ServicesMass General Hospital for Children
Candidates should submit a letter of interest and CV to:
Zhongcong Xie, MD, PhD, Chair, Search CommitteeDepartment of Anesthesia, Critical Care and Pain Medicine
Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, [email protected], c/o Christine Kennedy, [email protected]
Massachusetts General Hospital, a major Boston teaching hospital and an affiliate of Harvard Medical School, seeks a Division Chief to lead the Pediatric Anesthesia Division of the Department of Anesthesia, Critical Care and Pain Medicine. He/she will also be appointed as the Medical Director of Procedural Services within the MGHfC. He/she will provide strategic direction and oversight for all aspects of pediatric anesthesia clinical practice, education and research. He/she will partner with leaders in pediatrics, surgery and nursing to develop appropriate plans for patient care within their clinical area of responsibility.He/she must be a role model for clinician scientists and anesthesiologists in training. The position requires a pediatric anesthesiologist who is a distinguished leader and an exemplary teacher, with a background and accomplishments in research.We are an equal opportunity employer. All qualified applicants will receive consideration for employment without regard to race, color, religion, sex, sexual orientation, gender identity, national origin, disability status, protected veteran status or any other characteristic protected by law.
JOB SUMMARY:University Anesthesiologists has an opening for a full-time, board-certified/board-eligible, fellowship-trained cardiothoracic anesthesiologist/intensivist to join our growing academic practice via a partnership tractQUALIFICATIONS:1. Current Tennessee State Medical License or in the application process2. Current D.E.A. Certificate or in the application process3. Appropriate level of specialty designations (Board Certified/Board
Eligible)4. Insurability (malpractice)5. Completion of a cardiothoracic anesthesia fellowship (required)6. Certified/Eligible in Advanced TEE (required)7. Completion of a critical care fellowship (optional)All qualified applicants will receive equal consideration for employment without regard to race, color, national origin, religion, sex, pregnancy, marital status, sexual orientation, gender identity, age, physical or mental disability, or covered veteran status.
Full-Time Cardiothoracic Anesthesiologist/Intensivist
Flexible Start Date between 9/2020 and 9/2021
TO APPLY:Please submit a cover letter that highlights how you will contribute to executing our vision and a copy of your Curriculum Vitae to Greg Broyles, at [email protected]
The Department of Anesthesiology at the University of Wisconsin School of Medicine and Public Health has openings for several anesthesiology specialties: neurosurgical, regional, and general anesthesia, at the level of Assistant Professor (CHS), Associate Professor (CHS), or Professor (CHS); or Clinical Assistant Professor, Clinical Associate Professor, or Clinical Professor. These positions will be a dual appointment with UW Madison and UW Medical Foundation.
Requirements: Wisconsin medical license or eligible for Wisconsin license. Board eligible or certified by the American Board of Anesthesiology. Subspecialty training preferred for specific subspecialty as appropriate to position.
Duties: Provision of clinical anesthetic care to patients, and specific subspecialty area (working in the OR, plus call) in an anesthesia team model or personally performed. Teaching responsibilities for residents, fellows, and medical students in the OR, and didactic sessions.
Apply at https://jobs.hr.wisc.edu/en-us/listing/.In the “Search Jobs” field, search for the type of position which you qualify by entering either “general anesthesiologist”, “neuroanesthesiologist”, or “regional anesthesiologist”.
OPPORTUNITIES FOR ANESTHESIOLOGISTS SPECIALIZING IN NEUROSURGICAL,
REGIONAL, AND GENERAL ANESTHESIA
Unless confidentiality is requested in writing, information regarding applicants and nominees must be released upon request. Finalists cannot be guaranteed
confidentiality. The UW-Madison is an EO and AAE. Wisconsin Caregiver Law applies.
ALNcar&events134_2.indd 19 21/12/20 7:26 PM
ALNV134N2_Text.indb 19ALNV134N2_Text.indb 19 29-Dec-20 19:44:2929-Dec-20 19:44:29
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
A20 Anesthesiology, V. 134, No. 2, February 2021
www.woodlibrarymuseum.org
WOOD
Keeping AnesthesiA history Alive
VISIT OUR WEBSITE
RESEARCH DONATE• •
LIBRARY-MUSEUMOF ANESTHESIOLOGY
ALNcar&events134_2.indd 20 21/12/20 7:26 PM
ALNV134N2_Text.indb 20ALNV134N2_Text.indb 20 29-Dec-20 19:44:3329-Dec-20 19:44:33
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology, V. 134, No. 2, February 2021 A21
The University of Texas Southwestern (UTSW), in cooperation with Children’s HealthSM are seeking to recruit a mid-career clinician-scientist with a dedicated clinical research or translational research focus in pediatric anesthesia/children’s health. The individual should have a solid record of publication and established record of current NIH funding and leadership within his or her research area. The successful recruit will be provided with a substantial, multi-year recruitment package and dedicated time to conduct and grow their research endeavor. They will join a rapidly growing team of NIH-funded investigators within the Department of Anesthesiology and Pain Management.
UTSW is one of the country’s leading research facilities, with approximately $489 million in total annual funding and $228 million in annual funding from the NIH in 2019. Among UTSW’s approximately 2,600 full-time and 294 part-time faculty members are six Nobel Prize winners, 22 members of the National Academy of Sciences, 17 members of the National Academy of Medicine, and 15 Howard Hughes Medical Institute investigators.
Children’s HealthSM is the eighth-largest pediatric health care provider in the nation and the leading pediatric health care system in North Texas, providing a full spectrum of health care services—from daily wellness to specialty visits and critical care. Holding eight disease-specific care certifications from The Joint Commission, Children’s Health has been consistently named one of the nation’s top pediatric providers by U.S. News & World Report. The Children’s Health system includes two full-service hospitals, Children’s Medical Center Dallas and Children’s Medical Center Plano, Our Children’s House inpatient rehabilitation hospital, multiple specialty centers and rehabilitation facilities, physician services and the Children’s Medical Center Research Institute at UT Southwestern.
Dallas is a dynamic city with a robust economy. UT Southwestern is experiencing significant growth and anticipates continued growth in the future. Ranked in the Top 10 U.S. places to live with the highest pay adjusted to cost of living, the Dallas-Fort Worth area is a culturally diverse metropolitan region with affordable housing, a thriving culinary scene, world-renowned arts districts, major professional sports teams, trendy entertainment venues, and unparalleled shopping opportunities.
Applicants must be eligible for medical licensure in the state of Texas and be Board-certified in Anesthesiology. Appointment rank and salary will be commensurate with academic accomplishments and experience.
UT Southwestern Medical Center is an Affirmative Action/Equal Opportunity Employer. Women, minorities, veterans and individuals with disabilities are encouraged to apply.
Mid-Career Clinician-Scientist
Contact Charles Whitten, Professor and Chair, Department of Anesthesiology and Pain Management at [email protected].
Chief, Division of Critical Care MedicineMass General Hospital for Children
Candidates should submit a letter of interest and CV to:
Fumito Ichinose, MD, PhD, Chair, Search CommitteeDepartment of Anesthesia, Critical Care and Pain Medicine
Massachusetts General Hospital, 55 Fruit Street Boston, MA [email protected], c/o Christine Kennedy, [email protected]
Massachusetts General Hospital, a major Boston teaching hospital and an affiliate of Harvard Medical School, seeks a Division Chief to lead the Critical Care Division of the Department of Anesthesia, Critical Care and Pain Medicine.
The Division Chief will provide strategic direction and oversight for all critical care clinical practice, education and research.
He/she will partner with leaders in surgery, medicine, neurology and nursing to develop and carry out appropriate patient care plans within their clinical area of responsibility.
The Division Chief must be a role model for clinician scientists and intensivists in training. Therefore, the position requires an outstanding intensivist who is a distinguished leader in critical care medicine and an exemplary teacher, with a background and accomplishments in research.
We are an equal opportunity employer. All qualified applicants will receive consideration for employment without regard to race, color, religion, sex, sexual orientation, gender identity, national origin, disability status, protected veteran status or any other characteristic protected by law.
ALNcar&events134_2.indd 21 21/12/20 7:26 PM
ALNV134N2_Text.indb 21ALNV134N2_Text.indb 21 29-Dec-20 19:44:3329-Dec-20 19:44:33
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022

A22 Anesthesiology, V. 134, No. 2, February 2021Anesthesiology, V. 129, No. 4, October 2018 A37
Anesthesiology, V 117, No. 5, November 2012 A25
Deliver your message in
THE SOURCE PHYSICIANS TRUST
We’ve got
your next
bright idea!
www.physiciansjobsplus.com
THE WLM FELLOWSHIPwill provide recipients with fi nancial support for one to three weeks of scholarly historical research at the Wood Library-Museum.
The Board of Trustees of the Wood Library-Museum invites applications from anesthesiologists, residents in anesthesiology, physicians in other disciplines, historians and other individuals with a developed interest in library and museum research in anesthesiology.
For further information, contact: Librarian, Wood Library-Museum of Anesthesiology at (847) 825-5586, or visit our Web site at: www.WoodLibraryMuseum.org.
Completed proposals must be received before January 31, 2013, for consideration. The Wood Library-Museum serves the membership of ASA and the anesthesiology community.
the wood library-museum
of anesthesiology
Wood Library-Museum of Anesthesiology
520 N. Northwest HighwayPark Ridge, IL 60068-2573
(847) 825-5586
www.WoodLibraryMuseum.org
ALNclass117_5:Sept 2012 10/8/2012 5:35 PM Page 25
For more information about advertising and the next avail-able issue, contact your sales managers:
Account Manager
Hilary Druker, 609-304-9187
Careers & Events Advertising Sales ManagerDave Wiegand, 847-361-6128
The University of Wisconsin School of Medicine and Public Health (SMPH) invites applications and nominations for the position of Chair of the Department of Anesthesiology.
Please send nominations to: Laurel Rice, MD and Susan Lederer, PhD, Co-Chairs of the Anesthesiology Search Committee, c/o Ms. Staci Andersen, 750 Highland Avenue, 415OQ HSLC, Madison, WI 53705-2111, [email protected]
To apply for this position, please use the University of Wisconsin applicant tracking system found at: https://jobs.wisc.edu/ and search for position #92389. Applicants will be asked to upload a current cover letter, CV, and list of three references.
To receive full consideration, applications should arrive by October 14, 2018.
17151Anesthesiology3 1/2" x 4 3/4"
CHAIR, Department of AnesthesiologyUniversity of Wisconsin
School of Medicine and Public HealthMadison, Wisconsin
The University of Wisconsin is an EEO/AA employer. Wisconsin Caregiver and Open Records laws apply. A background check will be conducted prior to employment.
School of Medicineand Public HealthUNIVERSITY OF WISCONSIN-MADISON
CHAIR, DEPARTMENT OF ANESTHESIOLOGY
THE UNIVERSITY OF TEXAS HEALTH SCIENCE
CENTER AT SAN ANTONIO JOE R. AND
TERESA LOZANO LONG SCHOOL OF MEDICINE
The Long School of Medicine at the University of Texas Health Science Center at San Antonio (dba UT Health San Antonio) seeks an individual with an outstanding record of clinical operational leadership, scientific and educational achievement, and faculty/trainee recruitment and mentoring as its Chair of the Department of Anesthesiology. Dynamic leadership, clear communication, strong interpersonal skills, and a keen strategic vision are crucial characteristics required for success. Reporting to Dean of the Long School of Medicine, the Chair will be responsible for continuing to build and maintain excellence in clinical care, robust research programs, high quality graduate medical education, and a collegial interactive culture. The UT Health San Antonio is an Equal Employment Opportunity/Affirmative Action employer and is committed to excellence through diversity among its faculty, staff and students including protected veterans and persons with disabilities.
Candidates must have an MD, board certification in Anesthesiology and academic experience consistent with eligibility for full Professor with tenure. The ideal candidate will have a widely-recognized national reputation in their field. The ability to foster a culture of collaboration, innovation, and accountability across the Health Science Center is important. This is a wonderful opportunity for a visionary leader. UT Health San Antonio is a research-intensive institution located in San Antonio and it sits in the gateway to the picturesque Texas Hill Country. San Antonio is a vibrant, multicultural city with year-round recreational activities and an attractive cost-of-living.
Interested individuals should submit a letter of interest along with a current CV electronically via the UT Health Careers portal at http://uthscsa.edu/hr/employment.asp to apply for position of Chair, Anesthesiology. Inquiries may be directed to Shelly Evans, Long School of Medicine Chief of Staff at [email protected]
A l l f a c u l t y a p p o i n t m e n t s a r e d e s i g n a t e d a s s e c u r i t y s e n s i t i v e p o s i t i o n s .
Volume 134, Number 2, February 2021
Advertiser IndexEdwards Lifesciences . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . C2
Interior Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A4
Careers & Events . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A19-A22
Masimo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . C4
The Department of Anesthesiology at the University of Kentucky seeks Board-certified or Board-eligible anesthesiologists in the areas of pediatric, cardiac, and general anesthesia. These positions are open to all ranks.UK HealthCare has undergone a sustained and remarkable growth trajectory for a decade. Clinical volumes have doubled in the past 6 years and the acuity of patient care is high. UK HealthCare’s Albert B. Chandler Hospital was named No. 1 in Kentucky in the U.S. News & World Report’s Best Hospitals rankings. The Department of Anesthesiology is a collegial group that is well-respected in the medical center. The residency program is strong and nationally recognized. The enterprise financially supports the academic and the clinical mission of the Department of Anesthesiology.
Lexington, Kentucky
Assistant, Associate, or Full Professor of Anesthesiology
Please include a CV along with application. Applications will be reviewed immediately and will continue until the position is filled.Completion of residency in AnesthesiologyFellowship training is required within subspecialty positionsCurrent license to practice medicine in the state of Kentucky, or eligibility for licensureBoard-certified or Board-eligible in AnesthesiologyEligibility for ABA subspecialty certification is required within subspecialty positions
Contact Information [email protected]://www.wildcatanesthesia.com/
The George Washington University Medical Faculty Associates’ Department of Anesthesiology and Critical Care Medicine is seeking a physician
or non-physician scientist for the position of Vice Chair of Research.
The Department’s goal is to grow its research and scholarly output while building a nationally recognized research program that combines
clinical, translational, and basic science research. The Vice Chair of Research will report directly to the Department Chair, and will provide
leadership, strategic direction, and operational oversight of the scholarly and research activities of the Department. Appointment will be made
at the Associate or Full Professor rank and salary commensurate with experience.
The Vice Chair of Research’s responsibilities will include: conduct independent research and procure extramural funding, recruit research faculty,
develop a productive research operation in the Department, oversee staff and manage the research budget, provide mentorship, establish and
support infrastructure for research training programs at GW, and collaborate within the institution.
As appropriate, the Vice Chair for Research will also be expected to demonstrate clinical and teaching excellence to supplement research
leadership.
Basic Qualifications: Applicants must have a sustained record of excellent achievement in research as demonstrated by experience, publications,
evaluations, references and regional or national recognition. Applicants must already hold a rank of Associate Professor or Professor.
Application Procedure: To be considered, please complete the online faculty application at http://www.gwu.jobs/postings/79092 and upload
a CV and personal statements of research. Only complete applications will be considered. Review of applications will begin on January 11,
2021. Employment offers are contingent on the satisfactory outcome of a standard background screening.
The George Washington University and the George Washington University Medical Faculty Associates are Equal Employment Opportunity/Affirmative Action employers that do not unlawfully discriminate in any of its programs or activities on the basis of race, color, religion, sex, national origin, age,
disability, veteran status, sexual orientation, gender identity or expression, or on any other basis prohibited by applicable law.
Vice Chair of Research - Anesthesiology & Critical Care Medicine
ALNcar&events134_2.indd 22 21/12/20 7:26 PM
ALNV134N2_Text.indb 22ALNV134N2_Text.indb 22 29-Dec-20 19:44:3429-Dec-20 19:44:34
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Over 570,000Searches
Performed Every Day
Ovid's been a vital part of
global healthcare for over
20 years!1,200+ Journals6,000+ Books
100+ DatabasesCovering
130+ Specialties
Over 850 Abstracts
Viewed Every Minute
The Leader in Evidence-Based
ResourcesOvid is cited in Methods Section
of over 6,300 medical studies!
Over 50 Million Full Text
Downloads Every Year
Over6 Million Images,
Videos, andPodcasts
Best-in-class search for usersof all experience
levels
Search simultaneously
across all of your Ovid resources using a single
query!
Thousands of Ovid Exclusive
Resources
120+ Premier
Publishing Partners
Resources for All Stages of
Learning, Research, and
Practice
Unique Mobile Access
MultimediaPoint-of-Care
Tools
100% Searchable
Full Text
Used in Over 185Countries
More than 8,500
InstitutionsWorldwide
Nearly One Million Active
Personal Accounts
Over 3 Million
Saved Searches
You
Ovid®
6-V170
Ovid®
The world’s most trusted medical research platform.
Make Ovid the source for all of yourmedical, nursing, and healthcare research needs.
VISIT YOUR LIBRARY - ASK A LIBRARIAN - EXPLORE OVID
ovid.com
6-V170-2016-Ovid-00054-Ovid Generic Filler Ad LWW Journals-7x10-FINAL.pdf 1 30/08/16 2:34 PM
ALNV134N2_Text.indb 23ALNV134N2_Text.indb 23 29-Dec-20 19:44:3429-Dec-20 19:44:34
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Getting Published is a Process.
Get started today!
authors.lww.com
9-Q098
We’re Here to Help.
9-Q098-2019-Journals-00401-EDS Editorial Services_Author Resources Filler Ads-7x10-FINAL.indd 1 07/01/19 10:41 AM
ALNV134N2_Text.indb 24ALNV134N2_Text.indb 24 29-Dec-20 19:44:3429-Dec-20 19:44:34
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Anesthesiology: Problem-OrientedPatient Management,8th EditionISBN: 978-1-4963-1170-21,248 pages
Clinical Anesthesia Fundamentals 6th EditionISBN: 978-1-4511-9437-1912 pages
Clinical AnesthesiaProcedures of theMassachusetts General Hospital9th EditionISBN: 978-1-4511-9515-6768 pages
Anesthesiologist’s Manual of SurgicalProcedures 5th EditionISBN: 978-1-4511-7660-51,720 pages
Find the answers you need to ensurethe highest standards of anesthetic practice
on today’s leading Anesthesia resources
Save 20%
Also available wherever quality medical references are sold
Visit lww.com/anesthesia and use promo code WEA103AL to save when ordering
ALNV134N2_Text.indb 25ALNV134N2_Text.indb 25 29-Dec-20 19:44:3529-Dec-20 19:44:35
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Global Research – Open for All
Wolters Kluwer’s publishing program offers peer-reviewed, open access options to meet the needs of authors and maximize article visibility.
wkopenhealth.com
9-Q095
9-Q095-2019-Journals-00399-OA Open Access_Print ads-7x10-FINAL.indd 1 02/01/19 12:51 PM
ALNV134N2_Text.indb 26ALNV134N2_Text.indb 26 29-Dec-20 19:44:3529-Dec-20 19:44:35
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
A Journal for ALL Healthcare
Providers
Journal Impact Factor: 2.028*
*2017 Journal Citation Reports (Clarivate Analytics, 2018)
www.md-journal.com9-Q100
ALNV134N2_Text.indb 27ALNV134N2_Text.indb 27 29-Dec-20 19:44:3629-Dec-20 19:44:36
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
British Journal of AnaesthesiaVolume 126 Number 1 January 2021
Visit the journal at www.bjanaesthesia.org
BJA EDITORIALS 1 Turning ‘waiting lists ’ for elective surgery into ‘preparation lists ’
N. Levy , D. A. Selwyn and D. N. Lobo 5 Bleeding, anaemia, and transfusion: an ounce of prevention is worth a pound of cure
S. M. Frank and M. M. Cushing 9 Intravenous iron administered to anaemic patients before surgery and hospital readmission in the PREVENTT study:
one answer, a potentially important health benefi t, and new questions P. Meybohm , D. M. Baron and P. Kranke
12 Tranexamic acid and trauma coagulopathy: where are we now? C. Hanley , J. Callum and A. Jerath
17 Intramuscular tranexamic acid: a real-world application of pharmacokinetics A. Cortegiani , A. R. Absalom and B. J. Hunt
20 Comparative videolaryngoscope performance in children: data from the Pediatric Diffi cult Intubation Registry A. Norris and J. Armstrong
22 Ultrasound identifi cation of the cricothyroid membrane: the new standard in preparing for front-of-neck airway access M. S. Kristensen and W. H. Teoh
27 Occam’s razor at the sharp end: simplifi ed preoperative risk assessment S. J. Davies and G. Minto
31 Resisting neural inertia: an exercise in fl occinaucinihilipilifi cation? D. J. Eleveld , P. J. Colin , A. R. Absalom and M. M. R. F. Struys
34 Anaesthetic-induced developmental neurotoxicity on (neuro)steroids A. S. Evers
37 Predictive coding as a model of sensory disconnection: relevance to anaesthetic mechanisms R. D. Sanders , C. Casey and Y. B. Saalmann
41 Argon: a noble, but not inert, treatment for brain trauma? C. J. Edge and R. Dickinson
COVID-19 AND THE ANAESTHETIST: A SPECIAL SERIES 44 The ‘third wave ’ : impending cognitive and functional decline in COVID-19 survivors
H. A. Baker , S. A. Safavynia and L. A. Evered 48 Prone positioning for patients intubated for severe acute respiratory distress syndrome (ARDS) secondary to COVID-19: a
retrospective observational cohort study T. T. Weiss , F. Cerda , J. B. Scott , R. Kaur , S. Sungurlu , S. H. Mirza , A. A. Alolaiwat , R. Kaur , A. E. Augustynovich and J. Li
CARDIOVASCULAR 56 Systematic review and consensus defi nitions for the Standardized Endpoints in Perioperative Medicine (StEP) initiative:
cardiovascular outcomes W. S. Beattie , M. Lalu , M. Bocock , S. Feng , D. N. Wijeysundera , P. Nagele , L. A. Fleisher , A. Kurz , B. Biccard , K. Leslie , S. Howell , G. Landoni , H. Grocott , A. Lamy , T. Richards , P. Myles and on behalf of the StEP COMPAC Group
67 Cardiac output estimation using pulse wave analysis — physiology, algorithms, and technologies: a narrative review B. Saugel , K. Kouz , T. W. L. Scheeren , G. Greiwe , P. Hoppe , S. Romagnoli and D. de Backer
77 A restrictive versus liberal transfusion strategy to prevent myocardial injury in patients undergoing surgery for fractured neck of femur: a feasibility randomised trial (RESULT-NOF) M. A. Gillies , S. Ghaffar , I. K. Moppett , A. B. Docherty , S. Clarke , N. Rea , J. Stephen , C. Keerie , D. C. Ray , T. O. White , A. M. J. MacLullich , N. M. Mills , M. R. Rowley , K. Murthy , R. M. Pearse , S. J. Stanworth and T. S. Walsh
87 Association between postoperative haemoglobin concentrations and composite of non-fatal myocardial infarction and all-cause mortality in noncardiac surgical patients: post hoc analysis of the POISE-2 trial A. Turan , E. Rivas , P. J. Devereaux , M. Bravo , G. Mao , B. Cohen , K. Maheshwari , X. Pu , K. Ruetzler , K. Li and D. I. Sessler
94 Association between postoperative haemoglobin and myocardial injury after noncardiac surgery: a retrospective cohort analysis A. Turan , B. Cohen , E. Rivas , L. Liu , X. Pu , K. Maheshwari , E. Farag , O. Onal , J. Wang , K. Ruetzler , P. J. Devereaux and D. I. Sessler
102 Association between self-reported functional capacity and major adverse cardiac events in patients at elevated risk undergoing noncardiac surgery: a prospective diagnostic cohort study G. A. L. Lurati Buse , C. Puelacher , D. Menosi Gualandro , A. S. Genini , R. Hidvegi , D. Bolliger , K. Arslani , L. A. Steiner , C. Kindler , C. Mueller and for the BASEL-PMI Investigators
111 New algorithm to quantify cardiopulmonary interaction in patients with atrial fi brillation: a proof-of-concept study P. A. H. Wyffels , S. De Hert and P. F. Wouters
CLINICAL PRACTICE 120 Consensus guidelines on perioperative management of malignant hyperthermia suspected or susceptible patients from the
European Malignant Hyperthermia Group H. R ü ffert , B. Bastian , D. Bendixen , T. Girard , S. Heiderich , A. Hellblom , P. M. Hopkins , S. Johannsen , M. M. Snoeck , A. Urwyler , K. P. E. Glahn and on behalf of the European Malignant Hyperthermia Group
131 Pharmacological interventions for the prevention of renal injury in surgical patients: a systematic literature review and meta-analysis S. Pathak , G. Olivieri , W. Mohamed , R. Abbasciano , M. Roman , S. Tomassini , F. Lai , M. Wozniak and G. J. Murphy
139 Patient-maintained propofol sedation for adult patients undergoing surgical or medical procedures: a scoping review of current evidence and technology D. W. Hewson , J. G. Hardman and N. M. Bedforth
149 Patient blood management interventions do not lead to important clinical benefi ts or cost-effectiveness for major surgery: a network meta-analysis M. A. Roman , R. G. Abbasciano , S. Pathak , S. Oo , S. Yusoff , M. Wozniak , S. Qureshi , F. Y. Lai , T. Kumar , T. Richards , G. Yao , L. Estcourt and G. J. Murphy
157 The PREVENNT randomised, double-blind, controlled trial of preoperative intravenous iron to treat anaemia before major abdominal surgery: an independent discussion T. E. F. Abbott and M. A. Gillies
163 Bleeding Independently associated with Mortality after noncardiac Surgery (BIMS): an international prospective cohort study establishing diagnostic criteria and prognostic importance P. S. Roshanov , J. W. Eikelboom , D. I. Sessler , C. Kearon , G. H. Guyatt , M. Crowther , V. Tandon , F. K. Borges , A. Lamy , R. Whitlock , B. M. Biccard , W. Szczeklik , M. Panju , J. Spence , A. X. Garg , M. McGillion , T. VanHelder , P. A. Kavsak , J. de Beer , M. Winemaker , Y. Le Manach , T. Sheth , J. H. Pinthus , D. Siegal , L. Thabane , M. R. I. Simunovic , R. Mizera , S. Ribas and P. J. Devereaux
172 Preoperative prediction of Bleeding Independently associated with Mortality after noncardiac Surgery (BIMS): an international prospective cohort study P. S. Roshanov , G. H. Guyatt , V. Tandon , F. K. Borges , A. Lamy , R. Whitlock , B. M. Biccard , W. Szczeklik , M. Panju , J. Spence , A. X. Garg , M. McGillion , J. W. Eikelboom , D. I. Sessler , C. Kearon , M. Crowther , T. VanHelder , P. A. Kavsak , J. de Beer , M. Winemaker , Y. Le Manach , T. Sheth , J. H. Pinthus , D. Siegal , L. Thabane , M. R. I. Simunovic , R. Mizera , S. Ribas and P. J. Devereaux
181 A simplifi ed (modifi ed) Duke Activity Status Index (M-DASI) to characterise functional capacity: a secondary analysis of the Measurement of Exercise Tolerance before Surgery (METS) study B. Riedel , M. H.-G. Li , C. H. A. Lee , H. Ismail , B. H. Cuthbertson , D. N. Wijeysundera , K. M. Ho and for the METS Study Investigators
191 Outcomes after endoscopic retrograde cholangiopancreatography with general anaesthesia versus sedation F. C. Althoff , A. Agnihotri , S. D. Grabitz , P. Santer , S. Nabel , T. Tran , T. M. Berzin , E. Sundar , X. Xu , M. S. Sawhney and M. Eikermann
CRITICAL CARE 201 Pharmacokinetics of intramuscular tranexamic acid in bleeding trauma patients: a clinical trial
S. Grassin-Delyle , H. Shakur-Still , R. Picetti , L. Frimley , H. Jarman , R. Davenport , W. McGuinness , P. Moss , J. Pott , N. Tai , E. Lamy , S. Urien , D. Prowse , A. Thayne , C. Gilliam , H. Pynn and I. Roberts
210 Automated closed-loop versus manually controlled norepinephrine infusion in patients undergoing intermediate- to high-risk abdominal surgery: a randomised controlled trial A. Joosten , D. Chirnoaga , P. Van der Linden , L. Barvais , B. Alexander , J. Duranteau , J.-L. Vincent , M. Cannesson and J. Rinehart
NEUROSCIENCE AND NEUROANAESTHESIA 219 Comparison of anaesthetic- and seizure-induced states of unconsciousness: a narrative review
B. F. Gruenbaum 230 Abnormal preoperative cognitive screening in aged surgical patients: a retrospective cohort analysis
S. H. Gregory , C. R. King , A. Ben Abdallah , A. Kronzer and T. S. Wildes
238 Effects of sevofl urane anaesthesia on radioligand binding to monoamine oxidase-B in vivo K. Varn ä s , S. J. Finnema , P. Johnstr ö m , R. Arakawa , C. Halldin , L. I. Eriksson and L. Farde
245 The T-type calcium channel isoform Ca v 3.1 is a target for the hypnotic effect of the anaesthetic neurosteroid (3 ,5 ,17 )-3-hydroxyandrostane-17-carbonitrile T. Timic Stamenic , S. Feseha , F. M. Manzella , D. Wallace , D. Wilkey , T. Corrigan , H. Fiedler , P. Doerr , K. Krishnan , Y. H. Raol , D. F. Covey , V. Jevtovic-Todorovic and S. M. Todorovic
256 Effi cacy of acute administration of inhaled argon on traumatic brain injury in mice F. Moro , F. Fossi , A. Magliocca , R. Pascente , E. Sammali , F. Baldini , D. Tolomeo , E. Micotti , G. Citerio , N. Stocchetti , F. Fumagalli , S. Magnoni , R. Latini , G. Ristagno and E. R. Zanier
265 Explaining anaesthetic hysteresis with effect-site equilibration A. Proekt and M. B. Kelz
279 Selective optogenetic activation of orexinergic terminals in the basal forebrain and locus coeruleus promotes emergence from isofl urane anaesthesia in rats D. Wang , Y. Guo , H. Li , J. Li , M. Ran , J. Guo , L. Yin , S. Zhao , Q. Yang and H. Dong
PAEDIATRIC ANAESTHESIA 293 Frontal electroencephalogram activity during emergence from general anaesthesia in children with and without emergence
delirium J. Kim , H.-C. Lee , S.-H. Byun , H. Lim , M. Lee , Y. Choung and E. Kim
PAIN 304 Perioperative Pain and Addiction Interdisciplinary Network (PAIN): consensus recommendations for perioperative
management of cannabis and cannabinoid-based medicine users by a modifi ed Delphi process K. S. Ladha , A. McLaren-Blades , A. Goel , M. J. Buys , P. Farquhar-Smith , S. Haroutounian , Y. Kotteeswaran , K. Kwofie , B. Le Foll , N. J. Lightfoot , J. Loiselle , H. Mace , J. Nicholls , A. Regev , L. A. Rosseland , H. Shanthanna , A. Sinha , A. Sutherland , R. Tanguay , S. Yafai , M. Glenny , P. Choi , S. S. J. Ladak , T. S. Leroux , I. Kawpeng , B. Samman , R. Singh and H. Clarke
RESPIRATION AND THE AIRWAY 319 Association of weaning failure from mechanical ventilation with transthoracic echocardiography parameters: a systematic
review and meta-analysis F. Sanfilippo , D. Di Falco , A. Noto , C. Santonocito , A. Morelli , E. Bignami , S. Scolletta , A. Vieillard-Baron and M. Astuto
331 A comparison of videolaryngoscopy using standard blades or non-standard blades in children in the Paediatric Diffi cult Intubation Registry J. Peyton , R. Park , S. J. Staffa , S. Sabato , T. W. Templeton , M. L. Stein , A. G. Garcia-Marcinkiewicz , E. Kiss , J. E. Fiadjoe , B. von Ungern-Sternberg , F. Chiao , P. Olomu , D. Zurakowski , P. G. Kovatsis and On behalf of the PeDI Collaborative Investigators
CORRESPONDENCE e1 Network meta-analysis of isolated patient blood management interventions leads to uncertain interpretation. Comment on
Br J Anaesth 2021; 126: 149–56 D. Faraoni , I. Gross and A. Shander
e2 Interpretation of network meta-analysis of isolated patient blood management interventions. Response to Br J Anaesth 2021; 126: e1–2 M. A. Roman , R. G. Abbasciano , F. Y. Lai and G. J. Murphy
e4 Patient blood management interventions lead to important benefi ts for major surgery. Comment on Br J Anaesth 2021; 126: 149–56 M. Javidroozi , J.-F. Hardy and S. Ozawa
e6 Is patient blood management cost-effective? Response to Br J Anaesth 2021; 126: e7–9 M. A. Roman , R. G. Abbasciano , G. Yao and G. J. Murphy
e7 Is patient blood management cost-effective? Comment on Br J Anaesth 2021; 126: 149–56 K. M. Trentino , D. R. Spahn , H. S. Mace , H. Gombotz and A. Hofmann
e9 Comparison between ultrasound-guided and digital palpation techniques for identifi cation of the cricothyroid membrane: a meta-analysis K.-C. Hung , I.-W. Chen , C.-M. Lin and C.-K. Sun
e11 Entrainment of brain network oscillations in anaesthesia. Comment on Br J Anaesth 2020; 125: 330 – 335 F. Lersch , D. Hight and F. Frohlich
e13 Brainwave entrainment to minimise sedative drug doses in paediatric surgery. Response to Br J Anaesth 2021; 126: e11–2 W. Schmid , P. Marhofer and W. Klug
e14 Counting the train-of-four twitch response: comparison of palpation with mechanomyography, acceleromyography, and electromyography. Comment on Br J Anaesth 2020; 124: 712 – 7 T. Fuchs-Buder
e15 Visualising the pressure-time burden of elevated intracranial pressure after severe traumatic brain injury: a retrospective confi rmatory study J. Donnelly , F. G ü iza , B. Depreitere , G. Meyfroidt , M. Czosnyka and P. Smielewski
e17 Overfatigue amongst Chinese anaesthesiologists from 2017 to 2019 Y.-J. Du , X.-Q. Zhang , L.-D. Liu , J.-Y. Zhang , N. Han and G.-Y. Wang
e19 State of the anaesthesia workforce in the United States: trends and geographic variation in nurse anaesthetist to physician anaesthesiologist ratios L. A. Wilson , J. Poeran , J. Liu , H. Zhong and S. G. Memtsoudis
e21 Self-citation policies in anaesthesiology journals F. Sanfilippo , S. Tigano , A. Morgana , P. Murabitol and M. Astuto
e25 Use of sphenopalatine ganglion block in patients with postdural puncture headache: a pilot meta-analysis K.-C. Hung , J.-Y. Chen , C.-N. Ho and C.-K. Sun
e27 Immunoglobulin E cross-linking or MRGPRX2 activation: clinical insights from rocuronium hypersensitivity D. G. Ebo , M.-L. Van der Poorten , J. Elst , A. L. Van Gasse , C. Mertens , C. Bridts , L. H. Garvey , T. Horiuchi and V. Sabato
e29 Factors affecting need for manipulation after total knee arthroplasty: a retrospective case – control cohort study S. B. Porter , H. Zhong , C. B. Robards , J. Liu , J. Poeran and S. Memtsoudis
e32 Normalising renal tissue oxygen tension with higher inspired oxygen concentration may be falsely reassuring. Comment on Br J Anaesth 2020;125:192 – 200 A. Ercole
COVID-19 CORRESPONDENCE e33 Potential therapeutic value of dexmedetomidine in COVID-19 patients admitted to ICU
H. Zhao , R. Davies and D. Ma e35 Dexmedetomidine: another arrow in the quiver to fi ght COVID-19 in intensive care units
A. Jain , M. Lamperti and D. J. Doyle e38 High fresh gas fl ow during non-inhalational anaesthesia during the COVID-19 pandemic. Comment on Br J Anaesth 2020;
125: 773-778 A. Hall and A. Chakladar
e39 Psychological impact of COVID-19 on staff working in paediatric and adult critical care R. ffrench-O’Carroll , T. Feeley , M. H. Tan , C. Magner , K. L’Estrange , C.-I. Efrimescu , E. O’Connor , B. Lyons , S. Crowe and Collaborators
e42 Trials in pandemics: here we go again? S. Harris , E. Palmer and K. Fong
e44 Inhaled nitric oxide minimally improves oxygenation in COVID-19 related acute respiratory distress syndrome A. Longobardo , C. Montanari , R. Shulman , S. Benhalim , M. Singer and N. Arulkumaran
e46 Response of US hospitals to elective surgical cases in the COVID-19 pandemic R. Pirracchio , O. Mavrothalassitis , M. Mathis , S. Kheterpal and M. Legrand
e48 Respiratory personal protective equipment for healthcare workers: impact of sex differences on respirator fi t test results A. Ascott , P. Crowest , E. de Sausmarez , M. Khan and A. Chakladar
e49 Infl uence of room ventilation settings on aerosol clearance and distribution N. H. Sperna Weiland , R. A. A. L. Traversari , J. S. Sinnige , F. van Someren Gr é ve , A. Timmermans , I. J. B. Spijkerman , W. Ganzevoort and M. W. Hollmann
CORRIGENDUM 340 Corrigendum to ‘Propofol-based anaesthesia versus sevofl urane-based anaesthesia for living donor kidney transplantation:
results of the VAPOR-1 randomized controlled trial ’ ( Br J Anaesth 2017; 118: 720 – 32) G. J. Nieuwenhuijs-Moeke , V. B. Nieuwenhuijs , M. A. J. Seelen , S. P. Berger , M. C. van den Heuvel , J. G. M. Burgerhof , P. J. Ottens , R. J. Ploeg , H. G. D. Leuvenink and M. M. R. F. Struys
ALNV134N2_Text.indb 28ALNV134N2_Text.indb 28 29-Dec-20 19:44:3729-Dec-20 19:44:37
Dow
nloaded from /anesthesiology/issue/134/2 by guest on 01 February 2022
Related Documents











