In spyred The alternative EAO voice Volume 5, Issue 1 / Summer 2017 Immediate implant placement: Against all rules EAO Education Programme: Inspyred talks to the current participants Are you ready for Madrid 2017? Handling perforations of the sinus membrane Myths surrounding fixed and removable prostheses

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

InspyredThe alternative EAO voice
Volume 5, Issue 1 / Summer 2017
Immediateimplant placement:Against all rules
EAO Education Programme:
Inspyred talks to the current participants
Are you ready for Madrid 2017?
Handling perforations of the sinus membrane
Myths surrounding fi xed and removable
prostheses

Enrol for the EAO Education ProgrammeJoin this prestigious hands-on programme and obtain the EAO's Postgraduate Diploma in Implant Dentistry
� 6 modules over 3 years in 6 prestigious universities
� 3 day on-site training for each module
� expert advice from your mentors
� unique online learning platform
Covers surgery, prosthodontics, periodontics, treatment planning and maintenance in every module. Visit www.eao.org for more information or email [email protected] to register your interest.
Places are limited. Register today.
GR
ON
ING
EN
MALMÖ
DÜSSELDO
RF
LISB
ON
MADRID
ZU
RIC
H
Learn from the leading experts in implant dentistry at Europe's most prestigious universities

03 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
W elcome to the summer 2017 edition of Inspyred! This has been an exciting issue for us to put together, and we are thrilled to launch the
fifth volume of Inspyred with some new regular and one-time contributors alongside our usual features. As ever, you’ll find the full versions of each article along with the complete sets of figures and references online.
For this issue, we reached out to a number of active EAO members, such as participants of the recent Master Clinician Course in Geneva and recipients of the EAO’s Certificate in Implant-based Therapy. We received a record number of submissions, and as a result we have been able to add an extra four pages to the magazine.
We are delighted to include contributions from Edith Groenendijk, José Pinheiro Torres and Sawako Yokoyama, all of whom received certification from the EAO in 2016. Edith has written a case report which involves the immediate replacement of four maxillary incisors in a periodontally reduced dentition. José’s article on page 33 describes an approach using guided surgery in a demanding clinical case. Sawako’s article on page 20 looks at ‘Myths surrounding fixed and removable prostheses’ and explores the difference between a patient’s perception of Oral Health Related Quality of Life and a clinician’s.
We have also selected articles by Georgi Iliev and his colleagues, who explore the use of STL
subtraction for digital treatment planning, and Alberto Salgado and Lino Esteve, who discuss how they have handled various cases involving perforations of the sinus membrane.
On page 27 you’ll find our latest wiki-implant case, which describes a complication involving vertical bone augmentation. Our wiki-implant articles describe the cases which don’t go to plan, so you can read about complications which have been encountered in real-life situations and how they were managed.
We are also pleased to include articles which will give you the inside scoop on a number of member benefits so you can get the most out of your EAO membership. Get the low-down on the findings presented at the scientific meeting in Paris 2016 on page 26 and discover how to unlock full and unlimited access to EAO publications online on page 36.
This issue also includes an interview with the president of the EAO, Alberto Sicilia, as he talks about the 26th annual scientific meeting which will be held in Madrid in October 2017 and what to look out for at the congress!
As ever, we look forward to hearing your feedback and suggestions for this and future editions. Please do not hesitate to get in touch by emailing us at [email protected].
Isabella Rocchietta and David Nisand
Editors welcomeGet the inside scoop on summer 2017
To get the most out of Inspyred, visit our website, where you can view all articles in full, along with additional content.
www.eao.org/inspyred
Editorial Committee
David Nisand, France (Editor)Isabella Rocchietta, UK (Editor)Martin Brient, FranceStefan Fickl, GermanyJaime Jiménez Garcia, SpainAilsa Nicol, UKIrena Sailer, SwitzerlandAlberto Sicilia, SpainTommie Van de Velde, Belgium

Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 04
EAO Education Programme:Inspyred talks to two participants from the programme's 2016 intake
T he EAO’s Education Programme launched in 2016 and has been taking the dental community in Europe by storm. It is one of the most prestigious, comprehensive, and talked-about educational initiatives in recent years with modules
hosted at some of Europe’s top universities. Inspyred caught up with two of the participants from the programme’s 2016 intake to discuss their experiences on the programme so far.
Tell us a bit about yourself: where are you based?
Mads Krabbe: I’ve been practising for 14 years, and I’m currently based at two different clinics in Copenhagen. There are five dentists at the two clinics, and at both I’m the one who is mostly responsible for surgery. I’m a general dentist but the focus in my daily practice is on dental alveolar surgery.
Karleif Taksdal: I’m based in the south west of Norway, in a town south of Stavanger. I have a clinic there with five dentists, a hygienist, and seven nurses/assistants. I’m also a general practitioner, and I like to be involved in the full range of dental treatments. I don’t want to focus on one area, so only part of my work involves implants.
In Norway, we have a programme where patients can receive government reimbursement for some implant treatments. This means that you need to be a specialised implant dentist to do most treatments involving implants, so – as a general practitioner – I don’t get the opportunity to place as many implants. When I do, it’s usually treatments in the aesthetic zone where there has been trauma or resorption.
How did you first hear about the Education Programme (EP), and
what attracted you to it?
MK: Through social media – I saw the advert first on Facebook then on the EAO’s website. I had completed a formal course with the Danish Dental Organisation a few years ago, but wanted to educate myself further and was looking for a more structured course – the EP was offering that. The programme also appealed to me because many well-known universities were hosting the Live Learning Events. I was impressed by how prestigious the course leaders and institutions who were involved in the programme were; that was definitely one of the biggest things that attracted me.
KT: On the EAO’s homepage. When I saw that the EP would help lead to the Certificate in Implant-Based Therapy I was even more interested. Once I’ve completed this course I plan to go for EAO Certification.
I’ve already been on a few of the EAO’s educational courses in the past. I attended two of the Master Clinician Courses – one in Switzerland in December 2015 and one in Paris in March 2016. The course in Switzerland focused on implants in the aesthetic zone, and in Paris the topic was sinus lifts and bone grafting with cadaver dissection. So I’d already been to quite a few EAO courses, and knew the EP would be just as valuable an experience.
What set the EAO’s programme apart from other postgraduate/
further education courses that are available?
MK: The fact that it covers so much. The EP has a very broad and comprehensive curriculum and it features a lot of disciplines within implant dentistry. This is exactly what I was looking for in an educational course. It’s also hugely important to me that the course has the EAO’s backing. The EAO stands behind the Education Programme and organises each event, so I know the EP has the EAO stamp of approval and that the modules and course materials will be of the highest quality.
KT: For me, it was mostly the scope of the topics covered in the programme. I wanted to immerse myself in implant dentistry, so it was the obvious choice. It suits me and the way I like to work: I like to be able to perform a full range of treatments, from prosthodontics to endodontics, and not have to refer my patients elsewhere. It’s my belief that it’s better for the patient to have one dentist, not a whole array of different people. I think this kind of consistency makes it easier to follow up with patients and spot and address any issues.
The six modules are split into Straightforward (S), Advanced (A),
and Complex (C). So far, you have attended two modules ranked
Straightforward. Have you found the ‘back to basics’ approach useful?
MK: Yes, definitely – you can’t start a race from the middle, you have to start from the beginning and work from there. It’s the same with education. You have to have a solid foundation of knowledge, especially if you want to cover a lot of ground. It made sense for us to start from the beginning as we have. I think it’s always helpful for us as clinicians to get back to the basics. With implants everything is connected, so it’s even more important to have a firm grip on the fundamentals.
KT: Absolutely. I think it’s always useful to take a few steps back and look at your treatment protocols, and I mean really evaluate how you treat your patients and how you can improve. And I’ve found that my treatment protocols are okay – they are aligning with the treatment plans we’ve discussed at Malmö and at Groningen – so this gives me more confidence in my treatments, which itself is hugely valuable.

05 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
You have just started the third module, which is ranked Advanced.
Has the level of difficulty increased?
MK: Yes – the difficulty has definitely increased. We’ve just started the module but already you can tell that it’s more difficult. We’re dealing with topics like insufficient bone volume and other common challenges associated with implant dentistry. Even from the preliminary material we’ve received from the Online Classroom, I can see that the content is more advanced than the previous two modules. I’m really looking forward to progressing through this module and going to Düsseldorf for the next LLE.
KT: I’m also looking forward to Düsseldorf. I haven’t noticed a huge difference just yet, but I think the step-up in difficulty will become really apparent when we go to the first Advanced LLE. I found the Straightforward modules quite straightforward, so I’m looking forward to seeing how advanced the Advanced LLEs will be.
What have you learnt from the EP that you find yourself implementing
in daily practice?
MK: The Live Learning Events have been incredibly useful. At the LLE in Groningen I got some really useful surgical tips and insights from Professor Gerry Raghoebar. He was taking some of the live surgery sessions. I’ve already incorporated all of his tips, no matter how small, into my daily practice. Everything we learn is very practical and applicable to everyday situations, so the EP has been very useful in that way.
KT: I’ve found the discussions we have with the professors and fellow students very useful. I’m also particularly enjoying the surgical aspects – the professors always have these tips and tricks on how to do things. They’re the experts, and they’ve been placing implants for 20, maybe 30 years, and they have this wealth of knowledge which they share with us which is so valuable.
Tell us about the EAO’s Online Classroom. What impact has it had on
your learning process?
MK: The Online Classroom has been a very useful learning tool. It’s an online platform where students can gather information on the upcoming teaching modules. It contains a lot of materials, like videos and papers or articles on the topics set by the mentors. It’s like having a knowledge database that you can access at any time, and it’s constantly growing as you progress through the course.
It has had a noticeable impact on my learning process. The way the course is structured, you have to prepare for each module using the Online Classroom. That way you’re well prepared for the live sessions. The Classroom makes you go a bit deeper into the theory and subject-matter, so it better prepares you for applications during live events. Because of this I’ve found myself getting much more out of each topic we’ve covered.
KT: I’ve been using the Online Classroom a lot. You can access the lectures and case presentation sections, where participants can discuss different cases and share their findings. At the heart of it there’s a collaborative element between the students. We can present our cases and see what others have done, or how they would treat a particular case. It’s very nice and really interesting to see how other students do things in other countries. It makes you see different approaches from across Europe.
In the EP you can choose what format your mentor meetings take,
whether to have group or one-to-one sessions. What format do you
have? Is this useful?
MK: So far I’ve been using the group format. I think that for me, that’s the best way. A group atmosphere allows you to discuss treatment options and present your choices to your mentor and fellow students, while letting you give input into other people’s treatment plans. Because you have more minds collaborating on the topic, the discussions are more valuable.
I’m also glad that I can have an ongoing dialogue with my mentor. My mentors have been Professor Stavropoulos and Professor Hallström, and they’ve been very helpful in this respect. I have been in contact with them both as part of a group and sometimes one-to-one. Being in contact with these expert clinicians and getting their support and feedback has been great.
KT: I opted for group meetings. But actually, at one meeting I had two teachers to myself as the others in the group couldn’t attend! So that was great, as I got to discuss all my cases in depth and really steer the discussion myself. Although a group setting can be very beneficial, sometimes the discussion can be limited and you can’t go deep enough into one topic. I found the one-to-one set-up hugely beneficial, as we were able to discuss my case presentation and feedback in great detail. My two mentors have been Andreas Stavropoulos and Hadar Hallström. They were actually both at the LLEs – they were the ones who took the surgical sessions with the groups – so it was nice to have familiar faces providing mentorship.
What has been your favourite aspect/moment of the EP so far?
MK: It’s really quite easy for me to answer that – being able to take part in the live surgery sessions. I’ve always enjoyed that aspect of my work. Now I have the opportunity to see some of the best guys in the field and watch them do surgical procedures, and I can even assist during the sessions and take part in surgery with them! At the events in Groningen and Malmö I was able to assist Professor Stavropoulos and Professor Raghoebar, which, for me, has been my favourite part.

Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 06
KT: I’ve enjoyed everything. I don’t think I can choose any one aspect specifically. But I have particularly enjoyed the hands-on elements and live surgery events where we’ve been able to assist during procedures.
In Malmö we were just observing the teachers during surgery, but in Groningen we were assisting, too. And that was great – it has been the best moment so far. When you assist it’s really quite different as you get a much closer look at the surgical field and you can get so much more from the experience. And of course during these surgical sessions you get lots of the small tips and hints which you can’t learn any way other than being there and seeing it and doing it. It’s amazing to be able to learn from these experts who have been placing implants for up to 30 years. You always learn a lot from those sessions and get to improve your own skills and expertise.
Is there anything you are particularly looking forward to on the
course’s curriculum?
MK: I’m looking forward to seeing how different universities approach everyday problems, like missing bone, which we all face in everyday practice. I’m looking forward to the Advanced modules, where things will be getting a little more difficult and technical. I’m also looking forward to seeing my fellow participants again at the next LLE. It’s a very nice group of people on the course. We’ve developed a nice little social circle and I’ve enjoyed discussing things student-to-student with them.
KT: I’m just looking forward to the whole thing! The previous LLEs have been great, and I’m eager to learn more. I’m also looking forward to the LLE in Zurich which will be lead by Professor Christoph Hämmerle and Ronald Jung.
The Live Learning Events are just that: they’re learning events, and the whole environment is perfect for it. The EAO has set everything up to be as informative and engaging as possible for you while you’re there. And then once the event is over, you go back to your office and you have all these new ideas and new things that you have learnt and taken away from it.
Is there anything you would like to add, or general comments you
would like to make about the course?
MK: Being in the first intake, we were the guinea pigs if you like. But it has never once felt that way – it has run so smoothly, and it’s been very successful. I think the programme itself is very good and has been structured well for dentists like me who are general practitioners. The modules that we cover are all very interesting and they offer so many good opportunities to learn. I would definitely recommend the course – it has been a truly great experience!
KT: I’ve been very satisfied with the course – it has met my expectations and so much more. I would recommend it to anyone wanting to expand their knowledge in the field of implant dentistry.
What I have also found incredibly interesting has been discussing treatments with practitioners from other countries. At the Groningen LLE I saw that in the Netherlands teeth are generally extracted earlier, so there’s more bone for placing implants. That was a new experience for me and my English colleagues on the course. Seeing different treatment approaches has had a profound impact on the way I think about implant dentistry and how I treat my patients. It has been great working with people from across Europe in this way. But, I’m the only Norwegian guy on the course, so I hope other Norwegians will take part in the EP in the future, too!
07 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
Against all rules – a case reportImmediate replacement of four maxillary incisors in a periodontally reduced dentition
Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 07
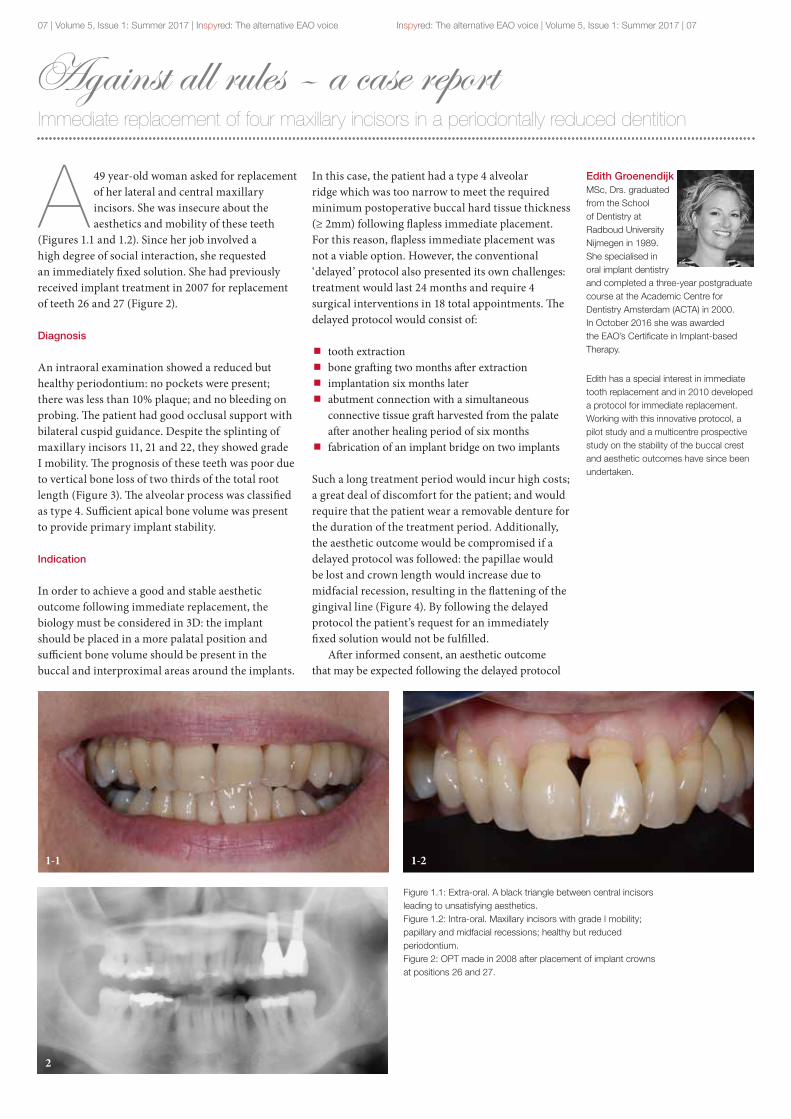
A 49 year-old woman asked for replacement of her lateral and central maxillary incisors. She was insecure about the aesthetics and mobility of these teeth
(Figures 1.1 and 1.2). Since her job involved a high degree of social interaction, she requested an immediately fixed solution. She had previously received implant treatment in 2007 for replacement of teeth 26 and 27 (Figure 2).
Diagnosis
An intraoral examination showed a reduced but healthy periodontium: no pockets were present; there was less than 10% plaque; and no bleeding on probing. The patient had good occlusal support with bilateral cuspid guidance. Despite the splinting of maxillary incisors 11, 21 and 22, they showed grade I mobility. The prognosis of these teeth was poor due to vertical bone loss of two thirds of the total root length (Figure 3). The alveolar process was classified as type 4. Sufficient apical bone volume was present to provide primary implant stability.
Indication
In order to achieve a good and stable aesthetic outcome following immediate replacement, the biology must be considered in 3D: the implant should be placed in a more palatal position and sufficient bone volume should be present in the buccal and interproximal areas around the implants.
In this case, the patient had a type 4 alveolar ridge which was too narrow to meet the required minimum postoperative buccal hard tissue thickness (≥ 2mm) following flapless immediate placement. For this reason, flapless immediate placement was not a viable option. However, the conventional ‘delayed’ protocol also presented its own challenges: treatment would last 24 months and require 4 surgical interventions in 18 total appointments. The delayed protocol would consist of:
tooth extraction bone grafting two months after extraction implantation six months later abutment connection with a simultaneous connective tissue graft harvested from the palate after another healing period of six months
fabrication of an implant bridge on two implants
Such a long treatment period would incur high costs; a great deal of discomfort for the patient; and would require that the patient wear a removable denture for the duration of the treatment period. Additionally, the aesthetic outcome would be compromised if a delayed protocol was followed: the papillae would be lost and crown length would increase due to midfacial recession, resulting in the flattening of the gingival line (Figure 4). By following the delayed protocol the patient’s request for an immediately fixed solution would not be fulfilled.
After informed consent, an aesthetic outcome that may be expected following the delayed protocol
Edith Groenendijk MSc, Drs. graduated from the School of Dentistry at Radboud University Nijmegen in 1989. She specialised in oral implant dentistry and completed a three-year postgraduate course at the Academic Centre for Dentistry Amsterdam (ACTA) in 2000. In October 2016 she was awarded the EAO’s Certificate in Implant-based Therapy.
Edith has a special interest in immediate tooth replacement and in 2010 developed a protocol for immediate replacement. Working with this innovative protocol, a pilot study and a multicentre prospective study on the stability of the buccal crest and aesthetic outcomes have since been undertaken.
Figure 1.1: Extra-oral. A black triangle between central incisors leading to unsatisfying aesthetics.Figure 1.2: Intra-oral. Maxillary incisors with grade I mobility; papillary and midfacial recessions; healthy but reduced periodontium.Figure 2: OPT made in 2008 after placement of implant crowns at positions 26 and 27.
1-1 1-2
2

Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 08
was accepted by the patient. It was decided that an approach combining immediate replacement with an additional bone graft would meet the patient’s request for an immediately fixed solution. Additionally, for aesthetic reasons, replacement of tooth 12 was recommended. For biomechanical reasons, immediate replacement using four implants instead of two was advised.
Planning
To determine whether immediate implant placement would be feasible, a digital 3D planning was made using a small field-of-view (6x6cm) low resolution CBCT scan (Scanora®, Soredex). To achieve an optimal aesthetic outcome, soft tissue stability may be created by hard tissue support. A minimal inter-implant distance and buccal hard tissue thickness of 3mm was therefore defined to create long-term hard tissue stability.
In adjacent implants, the expected papilla height is 2mm lower than in natural dentition. To create as much dimension as possible for the surrounding hard and soft tissues, small diameter implants were planned; the lateral and central incisors would be replaced by 3.0mm and 3.5mm diameter implants respectively (Figure 5). An additional buccal bone graft was indicated to achieve a postoperative hard tissue thickness of 3mm (Figure 6).
Procedure
incisors 12, 11, 21 and 22 were extracted under local anaesthesia a flap was raised from the distal of tooth 13 to the distal of tooth 23 implant positioning was performed according to the treatment plan following decorticalisation of the residual alveolar ridge, an additional bone graft was performed using a bone substitute (Bio-Oss®, Geistlich) and two resorbable membranes (CreOss®, Nobel Biocare)
four customised titanium abutments (Procera®, Nobel Biocare) were connected
the flap was closed with resorbable sutures (Vicryl Rapide® 4x0, Ethicon) (Figure 7.1)
under rubber dam, temporary crowns were fabricated using a thermoform mould and composite (Protemp®, 3M Espe) (Figure 7.2)
at a two-week follow-up, wound healing was evaluated (Figure 8) and additional oral hygiene instructions were given
three months later, the screw-retained temporary crowns were removed in order to make an impression of the implants using Impregum® (3M Espe) (Figures 9.1 and 9.2)
two weeks later, permanent abutments and crowns were placed (Figures 10 and 11)
Result
The aesthetic outcome after immediate implant placement was good. The gingiva line flattened slightly (as expected), although the peri-implant soft tissue remained clearly scalloped (Figure 11). The implant at tooth 12 was placed slightly buccally, which caused minor midfacial recession.
In the space of four months and in total four appointments, with only one surgical intervention, a direct fixed construction was made. An optimal aesthetic result was achieved. The patient was satisfied with the treatment and experienced little to no discomfort (Figure 12).
Conclusion
Although the aesthetic outcome following this procedure is promising, this may not be considered a standard procedure. Further long-term prospective research is necessary to determine the long-term aesthetic and functional outcomes.
Figure 3: Sagittal cross-sections of teeth 12, 11, 21 and 22.Figure 4: Intra-oral images of another case treated from 2005–2007 involving a delayed protocol: before (left) and after (right).Figure 5: Occlusal image of the digital 3D planning. Implant positions in red; numbers (mm) indicate bone dimensions.
3-23-1
4-1
5
4-2
3-3 3-4

09 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
Figure 6: Sagittal image showing planned implant positions.Figure 7.1: Occlusal image following implant placement; abutment connection; bone grafting; and flap closure.Figure 7.2: Direct postoperative fabrication of four temporary splinted crowns using thermofold mould and composite.Figure 8: Wound healing and temporary crowns at two-week follow-up.
Figure 9.1: Removal of screw-retained temporary crowns after three months.Figure 9.2: Impression copings in situ.Figure 10: Occlusal aspect of permanent abutments and buccal volume of peri-implant soft tissue.Figure 11: Implant crowns after placement.Figure 12: Intra-oral image before (left) and after (right) treatment.
6-26-1
7-1
8
7-2
9-1
10
12
9-2
11
6-3 6-4

CONTACT USPhone: +33 (0)1 42 36 62 20Email: [email protected]: www.eao.org
Early bird rates are available until 30 June.
EAO members: 990 EURNon members: 1,290 EUR
Places are limited: book now!
Master Clinician CourseMilan, Italy1–2 December 2017
The formulation of a treatment plan: Planned roadmap or extemporaneous improvisation?
Dr Stefano Gracis and Dr Antonello Appiani
� create an optimal treatment plan � balance predicted treatment outcomes
with patient-specific factors � learn when to use
articulators and try-ins � formulate a treatment plan combining
optimal aesthetics and function

11 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
Handling perforations of the sinus membraneA new approach using advanced platelet-rich fi brin (A-PRF)
O ne in four sinus lift procedures can be expected to result in perforations of the Schneiderian membrane. Although the clinical signifi cance of this complication
remains controversial, a careful assessment of the risk factors can help us prevent perforations, along with the use of prudent surgical techniques.
Several techniques for repairing the sinus membrane have been proposed which vary depending on the location and size of the perforation. Th is article will present three case reports involving sinus membrane perforations which were treated using advanced platelet-rich fi brin (A-PRF).
Incidence
Resorbed alveolar ridges can frequently be found in the posterior maxilla. In these cases, augmentation procedures in the maxillary sinus are oft en required before implants can be placed. Sinus augmentation is one of the best documented procedures in the literature with predictable long-term success rates regularly exceeding 90%1–5.
Th is is a technique-sensitive procedure, however, and it is not without complications. Perforations of the sinus membrane are the most common complications reported, with a mean incidence rate of 25–30%6. In a recent meta-analysis of 1,652 sinus lift procedures reported across 12 studies, the weighted incidence rate of perforation was 23.5% (95% CI), ranging from 3.6% to 41.8%7. Th is disparity may be due to several contributing factors, or even to perforations remaining undetected. As a practical conclusion, we can therefore expect to encounter one membrane perforation in every four sinus lift procedures.
Risk factors
Perforations can occur as a result of human error at a variety of stages, including when the bone is drilled; the Schneiderian membrane detached; or the
graft fi lled. In addition, perforations are frequently encountered in cases involving anatomic variations such as thinner or thicker membranes; the presence of septae; and sinus pathology8, 13, 14. Decreased incidence was recorded in several studies where piezoelectric instrumentation was used7.
Clinical consequences
Th e clinical consequences of sinus membrane perforations have not yet been clearly established. It is well known that implants perforating the sinus fl oor and protruding up to 3mm into the sinus cavity do not show lower success rates15. When the Schneiderian membrane is perforated, however, the graft material is not confi ned and could be dislodged and neo-vascularisation disturbed, thus hindering bone regeneration. Moreover, it has been shown that the sinus membrane possesses osteogenic capabilities; contains stem cells; and participates in bone formation aft er the sinus fl oor has been lift ed16, 17.
Membrane perforations have been linked to higher postoperative complications; impaired graft healing; and implant failure1, 6, 9, 12. Other studies, however, have found no correlation between them7, 8, 11. A proper diagnosis and careful surgical management of the membrane seem to be the best methods for handling perforations.
Classifi cation and handling
Membrane perforations have been classifi ed into fi ve categories, depending on their location and how diffi cult they are to repair18. Th is classifi cation was retroactively simplifi ed by the same authors19. Based on the size of the perforations, Hernández-Alfaro and colleagues defi ned three types:
less than 5mm between 5mm and 10mm more than 10mm6
Figure 1.1.1 Figure 1.1.2
Alberto Salgado
Velázquez received the Best Academic Award from the University Complutense Madrid in 2001. There, he also qualifi ed as a Master of Oral Surgery and Master of Implants. He is currently a professor of the Master of Implants course at the Universidad Miguel Hernández de Elche. Dr Salgado is also a member of the Aula Dental Avanzada group.
Lino Esteve
Colomina received his DMD from University Complutense Madrid in 1980 and has been working in the fi eld of implant dentistry since 1988. He is a past president of the College of Dentists and the Group of Dental Studies in Alicante, and a board member of the Sociedad Española de Implantes (SEI). He was the chairman of the SEI’s 20th international congress. Since 2012, Dr Esteve has been the director of the postgraduate programme in oral implantology at the Universidad Miguel Hernández.

Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 12
Figure 1.2.1
Figure 1.3.1
Figure 1.4.2
Figure 1.4.1
Figure 1.5.2
Figure 1.3.2
Figure 1.5.1
Figure 1.2.2
As a general rule, the bigger the perforation, the more diffi cult it is to manage. Various methods for repairing perforations have been proposed6, 9, 20–23.
Small (<5mm) perforations can oft en self-resolve because of folding that occurs when the Schneiderian membrane is refl ected.
Medium (5–10mm) perforations must be occluded with the use of collagen tape or a collagen membrane. Some authors have also recommended suturing the perforation, although this approach is diffi cult to perform. Sometimes, by extending the osteotomy, the Schneiderian membrane can be refl ected beyond the margins ofthe perforation.
A resorbable membrane can be inserted into the sinus cavity with its ends extruding from the window to be secured to the bony borders with fi xation tacks. Th us a containing pouch for the graft material is created.
Large (>10mm) perforations must be covered by means of a lamellar bone sheet or a bone block. A pedicled buccal fat pad fl ap has also been suggested.
Our technique
We strongly recommend the use of advanced platelet-rich fi brin (A-PRF) to repair any type of sinus membrane perforation. Th is paper will present three cases involving diff erent perforations, all of which were treated using A-PRF.
A-PRF is a clot obtained by simple centrifugation of venous blood without adding anticoagulants, according to a previously described protocol24. Although there is increasing evidence of its role in facilitating wound healing, we use it because of its adhesiveness and resistance, which makes it very suitable for repairing the tissue barrier. In addition to its physical properties, the three-dimensional fi brin network also off ers the greatest possibilities for the cells to attach to it.
Case 1: small perforation
During the elevation of the sinus membrane, a small class I perforation occurred in the superior medial corner of the window (Figure 1.1). We were able to proceed with the elevation without enlarging the hole and lift ed the bony wall into the sinus cavity like a trap door (Figure 1.2).
Because the perforation was small, no collagen membrane was needed. An A-PRF membrane was suffi cient to protect the upper space and repair the barrier (Figure 1.3). Next, the space under the repaired membrane was fi lled with biomaterial; another A-PRF membrane and a collagen membrane were placed to protect the graft laterally(Figures 1.4–1.5).
Case 2: multiple perforations
Th e patient presented with a distobuccal root of tooth 26 on the distal aspect of the lateral bony wall of the sinus and was completely asymptomatic. Direct extraction could not be performed in case the membrane was torn. We therefore performed an osteotomy

13 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
Figure 2.2.1
Figure 2.3.2
Figure 2.5.1
Figure 2.3.1
Figure 2.4.2
Figure 2.6.1
Figure 2.6.2
Figure 2.2.2
Figure 2.4.1
Figure 2.5.2
Figure 2.1.1 Figure 2.1.2
around the root using piezosurgery to create the bony window (Figure 2.1). Th e Schneiderian membrane was then detached and two small perforations occurred; one was class I, the other class II (Figure 2.2).
We were then able to isolate and remove the root without further damage to the membrane. Th e bony wall was refl ected and the membrane was folded to provide a suitable roof for the augmented subantral space (Figure 2.3). An A-PRF membrane was applied and moulded towards the new roof to thicken it. Th is was easily achieved due to the adherent characteristics of this membrane (Figure 2.4).
Because there were two diff erent perforations, the roof needed to be strengthened further. To do so, we placed a resorbable collagen membrane to create a self-containing space and fi lled it with bovine bone granules (Figure 2.5).
To cover the lateral window, we placed another A-PRF membrane and a collagen membrane; repositioned the fl ap; and closed the wound with interrupted sutures (Figure 2.6).

Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 14
Figure 3.1.1
Figure 3.2.1
Figure 3.3.2
Figure 3.2.2
Figure 3.4.1 Figure 3.4.2
Figure 3.3.1
Figure 3.1.2
Case 3: large perforation
In the third case, the Schneiderian membrane began to tear in the inferior border forming a class III perforation, and then a new large perforation measuring nearly 20mm occurred in the superior border (Figure 3.1).
To manage this case we found the following approach very benefi cial:
keep the excised bony wall and try to use it in the new barrier which will be created (Figure 3.2)
place up to six A-PRF membranes which will adhere to bone perform the Valsalva manoeuvre. A positive result indicates that a new barrier was successfully created (Figure 3.3)
to strengthen the barrier, add a resorbable collagen membrane (Figure 3.4). Our rationale for this is that an A-PRF membrane can be expected to last up to 4 weeks – half the time the Schneiderian membrane takes to regenerate (about 8 weeks)
insert another collagen membrane with its borders extruding from the bony window
ensure the creation of a self-containing space which is ready to receive the graft , as described by Fugazzotto & Vlassis18, 19 (Figure 3.5)
fi nally, cover the graft laterally with an A-PRF membrane and another collagen membrane above it and suture the wound (Figure 3.6)
References
1. Jensen OT et al (1998) Report of the sinus consensus conference of 1996. IJOMI, 13(suppl.): 11–45.
2. Wallace SS & Froum SJ (2003) Eff ect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann Periodontol, 8: 328–43.
3. Del Fabbro M et al (2004) Systematic review of survival rates for implants placed in the graft ed maxillary sinus. Int J Periodontics Restorative Dent, 24: 565–77.
4. Pjetursson BE et al (2008) A systematic review of the success of sinus fl oor elevation and survival of implants inserted in combination with sinus fl oor elevation. J Clin Periodontol, 35(suppl.): 216–40.
5. Nkenke E & Stelzle F (2009) Clinical outcomes of sinus fl oor augmentation for implant placement using autogenous bone or bone substitutes: a systematic review. COIR 20(suppl. 4): 124–33.
6. Hernández-Alfaro F et al(2008) Prevalence and management of Schneiderian membrane perforations during sinus-lift procedures. COIR, 2008, 19: 91–8.
7. Al-Dajani M (2016) Incidence, Risk Factors, and Complications of Schneiderian Membrane Perforation in Sinus Lift Surgery: A Meta-Analysis. Implant Dent, 25(3): 409–15.
8. Schwartz-Arad D et al (2004) Th e prevalence of surgical complications of the sinus graft procedure and their impact on implant survival. J Periodontol, 2004; 75: 511–6.

15 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
Figure 3.5.1
Figure 3.6.1
Figure 3.5.2
Figure 3.6.2
9. Proussaefs P, Lozada J, Kim J, et al (2004) Repair of the perforated sinus membrane with a resorbable collagen membrane: A human study. IJOMI, 19(3): 413–20.
10. Timmenga NM, Raghoebar GM, Boering G, et al (1997) Maxillary sinus function aft er sinus lift s for the insertion of dental implants. J Oral Maxillofac Surg, 55: 936–9.
11. Ardekian L et al (2006) Th e clinical signifi cance of sinus membrane perforation during augmentation of the maxillary sinus. J Oral Maxillofac Surg, 64: 277–82.
12. Nolan PJ, Freeman K, Kraut RA (2014) Correlation between Schneiderian membrane perforation and sinus lift graft outcome: A retrospective evaluation of 359 augmented sinus. J Oral Maxillofac Surg, 72: 47–52.
13. Wallace SS, Mazor Z, Froum SJ, et al (2007) Schneiderian membrane perforation rate during sinus elevation using piezosurgery: Clinical results of 100 consecutive cases. Int J Periodontics Restorative Dent, 27: 413–419.
14. Lum AG, et al (2017) Th e Association Between Sinus Membrane Th ickness and Membrane Perforation in Lateral Window Sinus Augmentation: A Retrospective Study. J Periodontol, (0): 1–11.
15. Brånemark P-I, Adell R, Albrektsson T, Lekholm U, Lindstrom J, Rockler B (1984) An Experimental and Clinical Study of Osseointegrated Implants Penetrating the Nasal Cavity and Maxillary Sinus. J Oral Maxillofac Surg, 42: 497–505.
16. Srouji S, et al (2013) Evaluation of the osteoconductive potential of bone substitutes embedded with Schneiderian membrane‐or maxillary bone marrow‐derived osteoprogenitor cells. COIR, 24(12): 1288–94.
17. Derjac‐Aramă AI et al (2015) Regenerative Potential of Human Schneiderian Membrane: Progenitor Cells and Epithelial‐Mesenchymal Transition. Anat Rec, 298(12): 2132–40.
18. Vlassis JM & Fugazzotto PA (1999) A classifi cation system for sinus membrane perforations during augmentation procedures with options for repair. J Periodontol, 70(6): 692–9.
19. Fugazzotto PA & Vlassis J (2003) A Simplifi ed Classifi cation and Repair System for Sinus Membrane Perforations. J Periodontol, 74: 1534–41.
20. Pikos MA (1999) Maxillary sinus membrane repair. Report of a technique for large perforations. Implant Dent, 8: 36–46.
21. Choi BH et al (2006) Cyanoacrylate adhesive for closing sinus membrane perforations during sinus lift s. J Craniomaxillofac Surg, 34: 505–9.
22. Shlomi B et al (2004) Th e eff ect of sinus membrane perforation and repair with Lambone on the outcome of maxillary sinus augmentation: A radiographic assessment. IJOMI, 19: 559–62.
23. Massei G et al (2015) An Innovative Technique to Manage Sinus Membrane Perforations: Report of Two Cases. Int J Periodontics Restorative Dent, 35: 373–9.
24. Dohan DM, Choukroun J, Diss A et al (2006) Platelet-rich fi brin (PRF): a second-generation platelet concentrate. Part I: technological concepts and evolution. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 101(3): e37–44.

C. Coachman M. Fradeani A. Happe F. Hernandez-Alfaro M. Quirynen I. Urban G. Urde W. Att E. Berroeta G. Calesini
J. Casas V. Clavijo L. De Stavola S. Gracis M. Hürzeler J. Kan P.F. Mesquita R. Mitrani A. Ortiz J. Caramês
M. Rosa I. Sanz Martín I. Sanz Sanchez F. Schwartz C. Suarez T. van de Velde
X. Vela S. Wolfart O. Zuhr K.L. Ackermann J. Blanco A. Bruguera
R. Burkhardt P. Cortellini V. Fehmer G. Gallucci C. Hämmerle L. Heitz-Mayfield P. Johansson R. Kohal C. Larsson O. Llena Blasco
I. Zabalegui D. Wismeijer D. Thoma M. Simion M. Roccuzzo G. Pradies N. Pietrobon J. Pi Urgell J. Perez M. Merli
MORE THAN 80 SPEAKERS WILL BE TAKING PART OF MORE THAN 30 SESSIONS INCLUDING
THE ONE BELOW
More info on:www.eao-sepes2017.comwww.eao.org www.sepes.org www.sepa.es
Thursday October 5th
From standard to advanced protocols of implant placement
Debate: When should we follow each approach?
The Brånemark legacy, the conservative approachMarc Quirynen (Belgium)
Evolution of surgical protocols in implant dentistryGöran Urde (Sweden)
Flapless, immediate implant placement and immediate restorationArndt Happe (Germany)
MADRID - october 5th–7th, 2017

17 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
Behind the scenes at Madrid 2017Interview with Alberto Sicilia, chair of the joint meeting in Madrid
I nspyred recently caught up with Alberto Sicilia, president of the EAO and chair of the forthcoming annual scientifi c meeting in Madrid in October. We asked him about how the meeting is being
organised and what he’s most looking forward to about the joint meeting.
How will this year’s annual meeting differ from
previous years?
Th is is a very exciting year. Madrid 2017 will be the EAO’s 26th annual scientifi c meeting, which is quite a milestone in itself, and we’re celebrating 25 years of EAO congresses. It will also be a joint meeting between the EAO and la Sociedad Española de Prótesis Estomatológica y Estética (SEPES). We have combined our annual scientifi c meeting with SEPES’ annual congress to create one joint conference. It will be a truly unique event.
Th is is something we’ve never done before – joining forces with one of the biggest national prosthodontics and aesthetics associations in Europe. It’s going to be one of the world’s biggest events in the calendar for implant dentistry. What’s more, we are also working with the Spanish Society of Periodontology (SEPA) to organise the EAO-SEPA European Symposium.
We’re expecting record numbers of delegates to turn out for the event. Th e meeting will be held in the IFEMA convention centre. It’s one of the biggest centres of its kind in Spain and Europe, so it will be perfectly equipped to host the international audience we are anticipating.
Th is collaboration has also allowed us to introduce a number of new features to our scientifi c
programme. We have been able to include additional session formats, like interactive surgical video sessions and diagnosis sessions. Th ese will provide a variety of diff erent presentation styles and cater to a broad and diverse range of topics within the fi eld.
EAO, SEPES and SEPA – that’s a lot of organisations
to be collaborating with. Has it been diffi cult working
with so many different committees?
When you organise an event on this scale it’s never easy – there are so many factors to consider and logistics to work out. But there has been this fantastic camaraderie and support which has been present throughout the whole process and which has made it a hugely enjoyable experience.
I couldn’t have done it without my fellow EAO co-chairs, Jaime A. Gil and Mariano Sanz, as well as our counterparts, Nacho Rodriguez and Jaume Llena on the SEPES scientifi c committee and Adrián Guerrero who is chair of the EAO-SEPA symposium. And of course, there have been countless others doing really admirable work behind the scenes and they have made it all possible. Th is has very much been the product of true collaboration, and it has been an absolute joy to work with everybody involved.
The theme of the 2017 congress is ‘Twenty-fi ve
years of Implant Dentistry. What have we learned?’
Do you have any personal opinions about this?
Th ere’s no question of how far we have come over the past 25 years. One thing that has struck me is how much the scientifi c programmes have changed. If you look at the programmes from early years, you can tell that osseointegration was a relatively new concept. People were still fi guring out how to place implants and learning about the diff erent areas and applications within the fi eld. But now, you look at the programme for Madrid, and there are so many more sessions which focus on developing technologies and techniques. It’s clear that as a whole we have a much greater understanding of implant dentistry, and we’re refi ning our techniques. We’re not discovering it for the fi rst time, but honing our skills. Now we’re able to delve deeper into the science behind everything than ever before.
Of course there are still discoveries being made; there is always research being done and studies being conducted – you can never stop learning. But the EAO is constantly evolving with the research and re-adapting to meet current requirements. Th at’s something you can also see in the scientifi c programmes year-to-year. What I’m really excited about is seeing how the programme will have changed in the next 25 years!
www.eao-sepes2017.com
Twenty-five yearsof Implant Dentistry.What have we learned?
MADRIDFrom October 5th
To October 7th, 2017Invited region:latin America
26th
annualscientificmeetingof theeuropeanassociationfor osseointegration
47Congreso
Anualde la
SociedadEspañola de Prótesis
Estomatológicay Estética
WITH A JOINT SYMPOSIUM
programmE overview

Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 18
Which five topics do you think participants will enjoy the most?
1. Main session 1: From standard to advanced protocols of implant
placement. This session represents the heart and soul of the scientific programme for Madrid 2017, I think, so it’s only fitting that it will kick off the whole conference. It tackles the congress theme straight away, and explores what we have learned about implant dentistry. The speakers will consider the different treatment protocols that are available now, and explore the evolution of each approach. It will be a very interesting session, and will end with a debate about when we should follow each approach. I can think of no better way to open the scientific programme.
2. Battle of concepts session: The restorative treatment of the partially
edentulous periodontitis patient. This session will be set up as a debate between the speakers. It will be extremely thought-provoking, and each speaker will present and defend their case. I’m also looking forward to it because my speciality is in periodontology, so I will personally find this session very interesting.
3. 3D interactive surgical video session 3: The biological and clinical
keys for periodontal, bone and peri-implant regeneration. I think delegates will really enjoy this new format: speakers will screen videos of surgical cases and comment on them in real-time. It will be a really excellent way to present findings, and will throw into relief how far we have come in terms of surgical techniques and technologies used in implant dentistry.
4. Main session 3: Diagnosis and treatment planning in implant
dentistry in light of the prevalence of peri-implant diseases. This is one of the dedicated EAO-SEPA symposium sessions, and delegates who are interested in implant dentistry and periodontology will find it especially interesting. The prevalence of peri-implant disease is a growing concern in the field, so speakers will cover how to detect the disease at its early stages and how to control the infection. This will be a very topical session, and will be extremely relevant for a lot of delegates.
5. Master Clinician session: Get a taste of the future EAO Master
Clinician Course topics. This session will also be very enjoyable. Speakers from upcoming Master Clinician Courses will give attendees a taster session from their forthcoming courses. The EAO specifically introduced the MCCs as an opportunity for experts who had presented at the annual conference to give participants hands-on tuition in a variety of topics. Since they were established, the MCCs have really taken off in terms of popularity. The future course topics which will be covered in this session are fascinating: formulating treatment plans and ridge augmentation. Delegates will enjoy this session as it will open their eyes to the other events that the EAO runs throughout the year, besides the annual scientific meeting.
What are you most excited about?
I am hugely excited for the whole thing to get started. The scientific committee has put together a really interesting and diverse programme, and we have an excellent faculty of invited speakers from the EAO, SEPES and SEPA lined up.
1 KM
ME
TR
O L
INE
10
METRO LINE 8
CITY OF MADRIDCITY CENTRE
METRO LINE 1
IFEMAEAO-SEPESCONGRESS
ATOCHA
BARAJASAIRPORT
SANTIAGOBERNABEU
PUERTADE TOLEDO
MUSEODEL PRADO
CIBELES
PUERTADEL SOL
PLAZAMAYOR
PALACIOREAL
CATEDRAL DELA ALMUDENA
PUERTADE EUROPA
1
2
5
6
7
4
3
8
NuevosMinisterios
Campode las Naciones
CASINODE MADRID

19 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
I should also say that I’m really looking forward to the Members’ Dinner. It will be held at the Casino de Madrid, which is a beautiful historic building in the heart of Madrid. It houses an exquisite collection of artworks, and the building itself is absolutely breath-taking. Every year, the Members’ Dinner is an excuse to meet up with old friends and enjoy a terrific evening of fine dining in a beautiful location – this year will be no exception, and I can’t wait to be showing off Madrid to the rest of the EAO.
Where is your favourite place to visit in Madrid?
Madrid is really worth a visit. It’s a fantastic city where the possibilities are endless for history, art, gastronomy, shopping and entertainment and can cover any interests. If you have time, I would recommend that you visit the Museo del Prado or the Museo Thyssen-Bornemisza – both are located on the Paseo del Prado so you can hop between them. It would also be a great idea to spend some time visiting the classic Barrio de Salamanca to do some shopping.
If you would like to sample the local cuisine then you should visit Calle Cava Baja – it’s a street lined with tapas bars and lovely places to eat and relax, and it’s filled with the history and kind of ambience which embodies the city. Viejo Madrid is one of my favourite restaurants on that street – you really must pay them a visit there.
One of the great advantages of partnering with a local association like SEPES is that they are real connoisseurs of the city. Their staff at the SEPES booth will be more than happy to give delegates advice on where to go in town, so be sure to ask them for their recommendations too!
Madrid city gemsOur pick of stylish destinations for visitors to Madrid this October
Prado Museum
Houses an extensive and extraordinary collection of fine Spanish art. Admission is free after 6pm.
Royal Palace of Madrid
The magnificent Palacio is the largest royal
palace in Europe by floor area and has a
beautiful art collection.
Retiro Park
Be sure to visit the idyllic Buen Retiro Park, where you'll find sculptures, water features and – if you're lucky – peacocks!
Temple of Debod
An ancient Egyptian temple located in the
heart of the city. A truly unique landmark.

Myths surrounding fixed and removable prosthesesIs there a discrepancy between a clinician’s perception and the patient’s?
Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 20
P atients can suffer from differing degrees of edentulism depending on the number of teeth they have lost1. Generally, the more teeth lost, the more they suffer.
An epidemiological study conducted in Japan found that 70% of people aged 65–70 have bilateral occlusion, and over 60% aged 80–90 have no posterior occlusal support (Figure 1). Especially among older populations, missing teeth can critically damage people’s Oral Health Related Quality of Life (OHRQoL) and their general health.
Worldwide, implant therapy is an established method for treating edentulism and implant survival rates are high2. Implant-supported prostheses are reliable solutions for cases involving multiple missing teeth, such as those presented in this paper. In cases 1 and 2, neither patient was satisfied with their original removable dentures because of poor functionality and/or aesthetic problems.
Case 1
The patient was a 64 year-old female who worked in an office (Figure 2). Her chief complaint was that she did not want to wear removable dentures any more.
Several treatment options were considered:1. Implant-supported full-arch bridge from tooth 16
to tooth 26; immediate placement and loading
2. Implant-supported full-arch bridge from tooth 16 to tooth 26; delayed placement following extraction of teeth 22–24; and immediate or delayed loading
3. Implant-supported bridges on teeth 16–21 and teeth 25–26; natural tooth-supported prostheses on teeth 22–24
After discussing the patient’s preferences, it was determined that she wanted to complete treatment as soon as possible as she was moving abroad. The patient selected option 1. There were several advantages associated with this treatment course:
it matched the patient’s preferences the prosthesis would be relatively easy to maintain while the patient lived in another country
it meant that there would be no further concerns about her remaining natural teeth (22–24)
Treatment
The patient’s occlusal condition was good; a radiographic guide (fitted with an assembly type for immediate placement) was made following her first visit; CT images were taken; and the treatment plan was consulted (Figure 3). Guided surgery with immediate placement and function was then performed (Figure 4).
Sawako
Yokoyama, DDS, PhD, graduated from Tokyo Medical and Dental University in 2001. In 2005 she received her PhD from the same university in the field of implant biomechanics. From 2007–2011 she worked in the implant industry and for a pharmaceutical company. In 2014, she opened a private practice in Tokyo and has since lectured and conducted research at Showa University. Her areas of special interest and research are implantology and prosthodontics. She has received certification from the Japanese Society of Oral Implantology and the EAO.
0 20 40 60 80 100
UnknownNo posterior occlusal support
Occlusion on one side
Occlusion on both sides
85+80–8475–7970–7465–6960–6455–5950–5445–4940–4435–3930–3425–2920–2415–19
Figure 1: Table showing the results of national dental epidemiology research conducted in Japan, 2011.Figure 2: Case 1, 64y female. Intraoral photos and panoramic X-ray at first visit.
2-1
1
2-2 2-3

21 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
Figure 2 (continued): Case 1, 64y female. Intraoral photos and panoramic X-ray at first visit.Figure 3: Radiographic guide and 3D planning.Figure 4: First surgery, immediate placement and function with four anterior implants.
Two months after surgery, periapical intraoral x-rays were carried out using the bisecting angle technique to confirm there were no complications.
Four months after surgery, an impression was made for the second provisional restoration. At that time, while retightening the abutment screw to the manufacturer’s recommended torque, the implant at 24 began to move and the patient felt pain (Figure 5). After a few weeks of observation, the situation remained unchanged and a plan was finalised for another operation. The implant at 24 was removed and a new tilted implant was simultaneously placed; a second provisional was delivered (Figure 6).
After four months, the final prosthesis was delivered (Figure 7).
2-6
3-3
2-4
4-1
4-4
2-5
4-2
4-5
3-1
3-4
3-2
2-6
4-3
4-6

Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 22
5-1 6-1
5-25-3 6-2
6-5
7-2
6-4
7-1
6-3
6-6
7-47-3
Figure 5: Four months after first operation. Disintegrated implant is indicated by red circle.Figure 6: Re-operation, removing implant number 24 and immediately replacing with a new tilted implant.Figure 7: Eight months after treatment.

23 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
Case 2
The patient was a 79 year-old female who was a housewife (Figure 8). Her chief concerns were that she wanted to have a stable complete mandibular denture and increased functionality while chewing food.
Medical history
The patient suffered from Hashimoto’s disease (Hashimoto’s thyroiditis); osteoporosis; and lumbar spinal stenosis. The patient’s medical history also revealed that she had been prescribed: Thyradin; Pravastatin; Alendronate sodium hydrate; Methylcobalamin; and Limaprost alfadex.
Treatment options
1. Complete denture with implants (overdenture)2. All-on-4 fixed implant-supported full-arch bridge
The patient had expressed a desire for minimally invasive treatment options and could not afford to cover the full cost of a fixed prosthesis herself. Because of this and her pre-existing medical conditions, option 1 was selected: implant overdenture with immediate function.
Treatment
A temporary denture (to be used as a radiographic guide too) was made during a preoperative drug interruption period for Alendronate sodium hydrate (Figure 9). CT images were obtained using the double scan technique; the treatment plan was finalised (Figure 10).
During the first implant surgery an approach using guided surgery with a mini-flap was selected in order to preserve non-mobile mucosa. A magnetic abutment-retained denture with immediate function was placed (Figure 11). After making a Conus crowned telescopic denture of the maxilla, a flame-treated zirconia denture (Figure 12) was finalised in the mandible.
During the one-year maintenance visit the patient reported that she had removed a small, hard substance from the left side of peri-implant area. Initially, she had thought it was a fish-bone. She reported no pain and no other symptoms. Ultimately, it was deemed to be a sharp piece of bone which had not been recontoured during implant placement. Slight bone resorption in the area was observed on an x-ray. No further complications have been reported up to three years after prosthesis insertion. In retrospect, it would have been prudent to trim away the sharp bone edge at the time of implant placement to avoid concentration of stress and fracture.
8-4
8-1 8-2
8-5
9-1
9-4
8-6
9-2
9-5
8-3
8-7
9-3
Figure 8: Case 2, 79y female. Intraoral photos and panoramic X-ray at first visit.Figure 9: Preparation for radiographic guide/immediate denture.

Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 24
Discussion
Removable options can often be more technically challenging than fixed alternatives. The differential degree of support which is provided by implants, natural teeth and soft tissue must be harmonised and reconciled by the removable prosthesis itself. It is strongly recommended that a careful examination, including 3D CBCT scanning and digital treatment planning, is conducted.
Both patients in cases 1 and 2 were satisfied with their functional and aesthetic results. Their Japanese Oral Health Impact Profile (OHIP-J) summary scores before treatment were 121 in Case 1 and 58 in Case 2; after treatment they were 32 and 4 respectively.
Various criteria for measuring the success of clinical treatment have been defined3–5; however these generally represent outcomes which are valued by the clinician. It is necessary for us to keep our focus on patient-based outcomes and the aspects of treatment which most affect the patient (for example how surgically invasive a procedure is; how long treatment lasts; and how high the economic burden may be6). To do so, an assessment oriented towards the patient’s subjective evaluation of treatment outcomes must be carried out.
OHRQoL is an important patient-reported outcome which captures the impact of oral diseases and dental treatments. Oral Health Impact Profile (OHIP) is the most widely used and reliable tool for measuring OHRQoL. OHIP consists of a multi-dimensional questionnaire, and lower OHIP summary scores indicate a better OHRQoL. A previous study reported OHIP summary scores in the general population group at 19.7 ± 24.37. The OHIP summary scores of the patients described in this study were significantly lower after treatment; both had improved quality of life, regardless of that fact that different therapies had been provided.
Recently, severe cases involving multiple missing teeth – such as those with an Eichner index of B3, B4, C1, C2 or C3 – have been researched at Showa University Dental Hospital. Initial results have suggested that, where appropriate case selection and thoughtful analysis of how best to meet patient expectations and preferences have been applied, there may be little or no significant improvement of OHIP summary scores where
fixed implant-supported bridges were used instead of removable implant-supported dentures (Figure 13). In this study a total of 30 patients participated; 12 received fixed implant bridges and 18 received removable implant overdentures (IOD) or implant-assisted removable partial dentures (IARPD). Patients each completed an OHIP questionnaire before receiving treatment – to provide baseline results – and after. The number of subjects participating is currently limited, and we will continue with patient recruitment and enrolment to increase sample size.
In general, clinicians (using their perception of objective criteria) view fixed prostheses as being superior to removable prostheses, both functionally and aesthetically. However, treatment outcomes are multidimensional and should be evaluated while incorporating the patient’s subjective assessment. Ideally, a treatment plan should be created using patient information (like age; economic status; and general health) gathered at the time of pre-treatment examination and counselling.
Patients’ needs are multifaceted, and often present a constellation of individual desires. Clinicians are obligated to seek treatments which best fit each patient. To borrow a phrase from our medical colleagues, we are seeking to practise ‘individualised dentistry’ which should be grounded in patient-based outcomes, not clinician-based outcomes.
The treatments described in cases 1 and 2 had similar treatment periods (both involved immediate function) and both improved the patient’s OHRQoL, but the economic burden of case 1 was almost four times higher than that of case 2. Implant overdentures and implant-assisted RPDs can therefore be considered as promising and effective solutions, especially in an aging society.
References
1. Gerritsen AE, Allen PF, Witter DJ, Bronkhorst EM, Creugers NH. Tooth loss and oral health-related quality of life: a systematic review and meta-analysis. Health Qual Life Outcomes, 2010, 5;8: 126.
2. Pjetursson BE, Thoma D, Jung R, Zwahlen M, Zembic A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin Oral Implants Res, 2012; 23: 22–32.
3. Zarb GA, Schmitt A. The longitudinal clinical effectiveness of osseointegrated dental implants: the Toronto study. Part I: Surgical results. J Prosthet Dent, 1990; 63: 451–7.
4. Zarb GA, Schmitt A. The longitudinal clinical effectiveness of osseointegrated dental implants: the Toronto Study. Part II: The prosthetic results. J Prosthet Dent, 1990; 64: 53–61.
5. Zarb GA, Schmitt A. The longitudinal clinical effectiveness of osseointegrated dental implants: the Toronto study. Part III: Problems and complications encountered. J Prosthet Dent, 1990; 64: 185–94.
6. Kim Y, Park JY, Park SY, Oh SH, Jung Y, Kim JM, Yoo SY, Kim SK. Economic evaluation of single-tooth replacement: dental implant versus fixed partial denture. Int J Oral Maxillofac Implants, 2014; 29: 600–7.
7. Reissmann DR, John MT, Schierz O, Kriston L, Hinz A. Association between perceived oral and general health. J Dent, 2013; 41: 581–9.
9-6 9-89-7
10-1 10-2
10-410-3 Figure 9 (continued): Preparation for radiographic guide/immediate denture.Figure 10: Radiographic guide and 3D planning.

25 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
Baseline Follow-up ΔT
Average (SD) Average (SD) Average (SD)
Fixed (n=12) 74.5 (31.6) 28.3 (22.7) 46.3 (31.7)
Removable (n=18) 72.3 (41.0) 39.7 (24.6) 32.6 (38.5)
P 0.6 0.1 0.2
11-4
12-4
12-8
11-1
12-1
12-7
11-2
12-2
11-5
12-5
13
11-6
12-6
11-3
12-3
Figure 11: First Surgery, guided surgery and immediate loading.Figure 12: Final prosthesis two years after treatment.Figure 13: OHIP summary score at baseline and follow-up, and volume of improvement (ΔT).Fixed: Female 42%, ave. age 57.0±8.4y, missing teeth #16.4±5.1, implant #7.9±2.3. Removable: Female 89%, ave. age 72.9±7.2y, missing teeth #22.3±5.0, implant #3.3±2.0. P-values obtained from paired t-test *P<0.05. ΔT: Follow-up scores – Baseline scores.

2016 Congress Scientific Report:Your guide to the EAO’s 25th annual scientific meeting
Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 26
T he hotly anticipated 2016 edition of the Congress Scientific Report is now available. This essential guide provides a write-up of 16 principal sessions which took place during
the EAO’s landmark 25th annual congress.The report is the second of its kind to be published
by the EAO. In 2015 the first issue was published exclusively for EAO members, summarising the proceedings of the 24th scientific meeting in Stockholm. Following its success, the second edition of the CSR is now available and it contains an unprecedented number of sessions. Selections of many of the speakers’ slides are also included alongside the majority of session summaries.
16 sessions and a total of 48 individual presentations are included in this edition. The topics featured are as varied and cutting-edge as the meeting’s scientific programme was, ranging from bone biology to the digital revolution; and from tissue management to complication prevention. Whether
you couldn’t attend all the sessions in Paris – or couldn’t attend the meeting itself – this year’s report will serve as a helpful reminder or an informative summary of each session.
Find out who won the quick-fire, out-of-the-box presentation which was chaired by the Junior committee – ‘7 minutes to convince’ – or read about the spirited debate between EAO past presidents Massimo Simion and Daniel Buser on ‘Machined vs rough implants’. Discover tips and tricks for managing
your daily practice and optimising long-term results, or hear experts’ opinions on treatment planning.
The report was written by a team of dentist delegates, to whom the EAO would like to extend its warmest thanks. Their methodology for writing the report was as follows:
the team attended all the sessions covered in the report during the meeting in Paris
they provided a draft summary of each presentation to the EAO, which arranged for a copywriting team to edit it
the editors returned the summaries to the delegates for review
these were then forwarded to each of the speakers from the meeting in Paris for their feedback, along with a request for a selection of their slides
each speaker was contacted up to three times; the majority gave feedback on the text and supplied their slides
The report is a useful and informative summary of the EAO’s unforgettable 25th annual scientific meeting. It was published online as an open-access document and is available for downloading at www.eao.org/congress-scientific-reports. A special printed edition of the report was circulated exclusively among EAO members in early March.
Acknowledgements
The EAO would like to gratefully acknowledge the substantial work carried out by Lino Esteve and Alberto Salgado in writing the report. They were supported by David Esteve, Guillem Esteve, Javier Amigo, Juan Navarro, Sandra Ferri, Tatiana Fernández, Alfonso Díaz, Vicente Belvis and Andrés Valdés.
This essential guide provides a write-up of 16 principal sessions which took place during the EAO’s 25th annual congress.
Co
ng
ress S
cien
tific Re
po
rt – E
AO
25th A
nn
ual S
cien
tific Me
etin
g, P
aris, 29 S
ep
tem
be
r – 1 O
ctob
er 20
16
Congress Scientific ReportEAO 25th Annual Scientific MeetingParis, 29 September – 1 October 2016
Issue 2, February 2017
Congress Scientifi c Report, Issue 2, February 201726
Treatment planning session: a clinical case with a ‘complex’ problem or involving extensive rehabilitationTwo teams of three clinicians – each specialising in a different area of implant dentistry – discussed a complex case presented by the moderator. Details of the case, which had been selected because of its complexity and scope for a multidisciplinary approach, were circulated to the participants before the session.
After an initial presentation of the patient data, both teams proposed their treatment plan and described their decision-making process to support it. This gave the audience an insight into how comprehensive and interdisciplinary treatment plans can be developed. A team from North America and a team from Europe each discussed the approach they would take.
Case presentationSession coordinator: Stefano GracisSession moderator: Michael CohenCase presenter: Andrea Ricci
The patient is a 54-year-old male with severe chronic periodontitis. He is partially edentulous; has diffi culty chewing; complains of mobility of his frontal teeth; and wants to improve his smile. Radiographs taken during his fi rst consultation
show generalised bone loss which is mostly horizontal (Figures 6.1.1–6.1.3). He has a history of periodontitis, and had three implants placed three years ago (Figure 6.1.4). The patient’s periodontal charts can be seen in Figures 6.1.5–6.1.6.
Figure 6.1.1 Figure 6.1.2
Figure 6.1.4Figure 6.1.3
Figure 6.1.6Figure 6.1.5
Front cover and sample page from the 2016 Congress Scientific Report

Wiki-implants case:Complication involving vertical bone augmentation
27 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
V ertical bone augmentation can be challenging. When using non-resorbable membranes in particular, complications such as wound dehiscence and
infection have been widely reported.In the following case, vertical bone augmentation was performed using
a titanium-reinforced d-PTFE membrane and a xenogenous bone substitute simultaneous with implant placement (Figures 1–4). Six months after implant placement and bone augmentation, the clinical situation presented intact (Figure 5); the peri-apical radiograph, however, revealed a failed augmentation with additional bone loss around the implant fixture (Figure 6). After flap reflection, major bone loss was revealed in the area around the implant fixture (Figures 7–8).
After membrane removal and thorough decontamination of the implant fixture using air abrasion and hydrogen peroxide gel (Figure 9), bone augmentation was performed with a resorbable collagen membrane and a xenogenous bone substitute (Figure 10). Six months after secondary bone augmentation, a provisional was placed. The peri-apical radiograph suggests bone regeneration to a certain extent; however, the prognosis of the implant remains critical (Figure 11).
Removing the implant and re-grafting the clinical situation could also be a suitable approach to this complication. The surgeon believed that it was a ‘sterile’ infection, and therefore chose to preserve the implant and use a long-term provisional to monitor the situation. In the surgeon’s opinion, the reason for this complication was that the cover screw attaching the membrane in the coronal position had become loose, and had disturbed hard tissue healing.
Submitted by: Stefan Fickl, DMD, PhD
Figure 1 Figure 2
Figure 4 Figure 6
Figure 3
Figure 8
Figure 9
Figure 10
Figure 5
Figure 7

STL subtraction:A new method for digital treatment planning
Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 28
W hen combined with traditional treatment planning methods, digital tools can offer a more conservative approach and more predictable
final results3, 6. The merging of 2D designs and 3D digital models allows prosthetic constructions to be completed digitally1, and scanned models can now be transferred to the final design of the restoration17. Detailed functional analysis of dentition using provisionals to change or adapt the smile design is also needed4, 16. The success of an aesthetic treatment relies on good planning and screening of patients; this is the case whether it is a crown-lengthening procedure or implant treatment. Optimal aesthetic results require a suitable smile design which fulfils the patient’s expectations10, 11.
When planning a crown-lengthening procedure, the volume of soft and hard tissues which needs to be removed should be carefully calculated. 3D surgical guides can assist with this, allowing us to visualise and measure the alveolar bone; plan the positions of prosthetic designs; and produce wax-ups and mock-ups inside the patient’s mouth.
Initially, implant therapy was surgically-led and implants were placed according to the amount of available bone which was detected using traditional radiography. This approach often led to incorrect positioning of prostheses because implants were placed in the wrong 3D position. The consensus today is that the starting point for treatment planning should be the final design of the prosthesis, and the use of digitally planned surgical guides is common.
This paper describes a fully digital protocol which allows clinicians to plan, visualise, and functionally test designs, enabling the design of digital surgical
guides and provisional constructions for complex aesthetic cases before irreversible dental procedures are carried out.
Material and methods
For this prospective study, patients requiring complex aesthetic therapy (including crown-lengthening and/or implant treatment) were recruited. Our procedure involved surgical guides using digital subtraction. Patients were selected at random, although the following groups were excluded: those with medical conditions which could compromise treatment results; pregnant women; anyone with a drug addiction or strong smoking habit; anyone suffering from a mental disorder; or anyone currently undergoing chemotherapy. All patients signed a declaration of informed consent. The treatment planning protocol consisted of two stages: 2D digital planning and 3D digital planning.
2D digital planning
We used VisagiSMile software to create 2D digital designs of restorations which reflected patients’ requests and expectations3, 6, 15. The 2D design was used as a guideline for creating a diagnostic mock-up of the patient’s mouth. This was done with the edges of the central incisors aligned.
Two photographs are required to create designs with VisagiSMile: one of the patient’s full face with a forced smile showing their dentition, and another of the upper jaw with lips retracted against a contrasting black background. These were captured, and patients
Figure 1: Full-face picture showing (from left to right) central occlusion; rest position; and full smile with visible dentition.Figure 2: Position of the incisal edge superimposed with 2D VisagiSMile design – initial situation.Figure 3: Position of the incisal edge superimposed with 2D VisagiSMile design – mock-up.
Figure 2 Figure 3
Figure 1
Georgi Iliev DMD, PhD, is an assistant professor in the department of Prosthetic Dental Medicine in the Faculty of Dental Medicine at Medical University of Sofia, Bulgaria.
Rosen Borisov DMD, PhD, is an assistant professor in the department of Imaging and Oral Diagnostics at Medical University of Sofia.
Dimitar Filtchev DMD, PhD, is also an associate professor in the Prosthetic Dental Medicine department at MU-Sofia.
Elitsa Ruseva DMD, is a privately practising periodontist in Sofia, Bulgaria.

29 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
Figure 9: STL file repositioned over CBCT model along tooth outlines.
Figure 4: Full-face picture of the initial situation; digital design; and diagnostic mock-up in patient’s mouth.Figure 5: CBCT of the patient in front view and sagittal view before treatment.Figure 6: TRIOS 3Shape scans of the initial situation before treatment, occlusal view and front view.Figure 7: TRIOS 3Shape scan of composite mask according to new prosthetic design, front view.Figure 8: TRIOS 3Shape images (with and without crowns) processed and converted into STL files.
were filmed while going from resting to smiling. Patients were also asked to discuss their expectations and concerns about the aesthetic outcome.
VisagiSMile employs facial analysis and a short interview to gauge the patient’s personality type and calculate the main parameters of an individual’s smile frame. Various features are measured, including: the incisal projection; tooth inclination; dominance; and shape8, 9. Patients’ preferences regarding the design are taken into consideration.
Once the position of the incisal edge of the central incisors was defined, we used the 2D design to create new tooth proportions, extending the length of the tooth in coronary or apical directions with periodontal surgery. By analysing the position of the incisal edge of the central incisors in the patient’s picture we could define the new position (Figure 1).
The proportions provided by the software are highly personalised and optimised for each case. Final designs can be exported as PDF, PNG or STL files containing detailed information of size, correlation, inclination and shapes of teeth, as well as the whole composition. A diagnostic wax-up was created based on the treatment plan provided by the software’s digital proposal. Based on this, the first additive composite mock-up was made. Prototypes were made on wax models using silicone keys with high durability. Bis-acryl self-cured composite was applied to the silicone keys and the design was recreated in the mouth using a composite mask over the patient’s natural, non-prepped teeth (Figures 2 and 3).
New full-face and intraoral pictures were taken; any changes were discussed with the patient by comparing the relevant before and after mock-up pictures7 (Figure 4). Once the patient had given consent, the treatment plan was finalised7.
Conventional crown-lengthening approaches include manufacturing the surgical guide from thermal vacuum adapted film or silicon. The level of the alveolar bone is measured by sounding and mapping2, 13. However, these methods generally lack geometrical accuracy and 3D buccolingual data. Therefore, innovative 3D studies are necessary to allow visualisation and measurement of the alveolar bone and position-planning for future prosthetics. The use of conventional impression and model materials is considered one of the main reasons for differences between planned and achieved positions of implants and surgical guides2.
Surgical guides can be made with CAD/CAM technology by using 3D images from CBCT scans and 3D printing. Treatment planning with surgical guides allows prosthetic construction or repair to be carried out in the patient’s mouth immediately after surgery.
3D digital planning
We performed CBCT (ProMax® 3D Mid, Planmeca) with contrast and resolution of 200 microns along with 3D intraoral scanning of the initial situation. Using data from these scans we created a design in the patient’s mouth. Studies on the use of intraoral scanners in the production of surgical guides are limited and so it is our hope that this research will contribute to a greater understanding of their use/advantages5 (Figures 5–7).
3Shape scans (with and without crowns) were processed and converted into STL files by Ortho Analyzer software and imported using SimPlant® Pro (Materialise NV) (Figure 8). The intraoral images were superimposed in all three planes along the contours of the CBCT model.
All models were imported into CAD 3-matic® (Materialise NV) software. The highly detailed intraoral images allowed exact repositioning on the CBCT model. Repositioning was done along the contours of the STL files over the direct outlines of the same structures (Figure 9).
Two types of digital subtraction were performed: first, a 3D intraoral model was subtracted from the 3D model without crowns. This created a ‘shell’ STL model of the crowns (Figure 10). The STL model of the CBCT
Figure 4
Figure 5
Figure 7
Figure 6
Figure 8
Figure 9

Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 30
scan was then united with the scanned 3D model without crowns (Figure 11). Second, the shell model was subtracted from the united model.
The results are either positive or negative. When the residual amount of subtraction is from intraoral scanner values, the results are negative; in cases where the volume of the residual subtraction is part of the CBCT it is a positive value (Figure 12).
Comparing the results of the subtraction allows us to estimate the difference between the root surfaces and crowns. The visual definition of the residual volume of the subtraction allows the identification of the measured areas.
Figure 13 shows the visualisation of the ideal preparation of the teeth so that the veneers can lie flat on the root surface.
Digital planning allows us to create stereolithographic (SLA) printer guides to perform the gingivectomy; osteotomy; selective tooth preparation; and the printing and fixing of the temporary veneers in one clinical procedure.
We converted the file into an STL open format. The final prosthetic was milled using CAD/CAM technology with biocompatible acrylic material and completed by manually adding details and effects (Figures 14–16).
Detailed functional analyses of the dentition were made with diagnostic provisional constructions. Occlusal relationships between both jaws were verified and occlusal contacts were adjusted where necessary (Figure 17).
Surgical protocol
The crown-lengthening procedure was carried out using a conventional technique: a flap was elevated; recontouring was done using a diamond bur. Once the provisional was placed, the new position of the soft tissue was measured. More than 2mm of keratinised gingiva was removed; the bone was reshaped around the new level, which should be 3mm apical from the planned gingival margin. In this case only bone reshaping was required, because the teeth had periodontal resorption and the vertical level of the bone meant that they were already sufficient for the desired gingival level. A gingivectomy was carried out on the incisors, canines and premolars on both sides. O-shaped sutures (Propylene 7-0) were used to close the flap.
The final fit was impressive. It did not require any significant relining or adjusting in the marginal area. Constructions were fixed
Figure 12
Figure 11Figure 10
Figure 16
Figure 14
Figure 15
Figure 13
Figure 10: ‘Shell’ STL model of the crowns.Figure 11: STL model united with scanned 3D model without crowns.Figure 12: United model combined with shell STL model.Figure 13: Visualisation of the ideal design for veneers to lie flat on the root surface.Figure 14: SLA printed model from the CBCT.Figure 15: CAD/CAM milled acrylic prosthetic positioned on model.Figure 16: Provisional construction created used the shell STL model.

31 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
with composite to allow for better marginal adaptation and to prevent microleakage. The patient was advised to treat the tissues with chlorhexidine gel every day for one week; following that, to brush their teeth with a soft brush and rinse their mouth with chlorhexidine 2% mouthwash. Sutures were removed after 7–10 days. Final maturation of the tissues occurred after one month. Because of the patient’s existing periodontal problems, at the end of the healing period the shape of their papillae was not optimal.
Discussion
The digital protocol described above was initially developed for implant treatment planning. The starting point for treatment planning should be the final design of the definitive prosthetic construction. It is also important that the implant position be correctly identified before any irreversible dental procedures are carried out.
The use of surgical guides, based on the future prosthetic design and the available bone, is becoming increasingly common. Surgical guides can be created with double scans. A scanned diagnostic mock-up in the patient’s mouth is repositioned on the tomographic image, and in groups of two scans the model depicts the mucosal side of the treatment area. Adjustable software images can be positioned on identical points on both models12. This allows us to achieve the desired implant position, ensuring the predictability and long-term prognosis of treatment13.
The use of intraoral scanners in the production of surgical guides in implant dentistry is a new concept; the workflow outlined in this paper details our experience with the technology. Detailed explanations of our research will be the topic of future articles.
The intraoral scans were superimposed in all three planes along the contours of the CBCT model. Finally, both models were imported using CAD 3-matic software (Materialise MV). The highly detailed intraoral images allow precise repositioning on the CBCT model. This was done using direct outlines and structures in cases with no artefacts, and indirect outlines with existing ones (Figure 19).
The patients were called for follow-ups 3, 10 and 15 days after the surgery. Sutures were removed at the ten-day follow-up. Vertical levels corresponded to desired aesthetic outcomes and harmonised with provisional constructions at the gingival level of the adjacent teeth. The stability of the implant was calculated using ultrasound with ISQ units (Osstell Mentor, Integration Diagnostics) during surgery and checked again during the replacement of the abutment.
Conclusion
The proposed methodology improves diagnosis, digital planning and the visualisation of created designs. It also provides completely digital surgical guides and provisional constructions for complex aesthetic cases in one clinical step.
Figure 17: Functionally adjusted provisional three days after surgery.Figure 18: TRIOS 3Shape scan of initial situation before treatment – occlusal view and STL.Figure 19: STL model of CBCT united with 3D scanned model; planned implant position on CBCT – frontal.Figure 20: Digital model representing the correct implant position; STL file of final surgical guide.Figure 21: Printed surgical guide and positioning of Trabecular Metal implants (Zimmer).Figure 22: Mattress stitches with 6/0 monofilament PTFE sutures (Omnia).
Figure 17
Figure 18-1
Figure 19-1
Figure 22-1
Figure 20-2
Figure 20-1
Figure 21-2
Figure 18-2
Figure 19-2
Figure 22-2
Figure 21-1

Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 32
References
1. Clup, L., E. McLaren, L. Swann. Smile analysis Converting digital design to the Final smile: Part II. Journal of Cosmetic Dentistry, Summer 2013, 29(2): 98–108.
2. Farley, N.E. et al. Split-mouth comparison of accuracy of computer generated and conventional surgical guides. The International journal of oral and maxillofacial implants, 2011, 28(2): 563–72.
3. Feraru M, Bichacho N, Muzella V. Individualizing a smile makeover. Current strategies for predictable results. J Cosmet Dent, 2016, 32: 109–119.
4. Gürel, G., N. Bichacho. Permanent diagnostic provisional restorations for predictable results when redesigning smiles. Pract Proced Aesthet Dent, 2006,18: 281–286.
5. Goracci C. et al. Accuracy, reliability and efficiency of intraoral scanners for full-arch impressions: a systematic review of clinical evidence. European journal of orthodontics, 2016, 38(4):422–8.
6. Iliev, G. Personalized Digital Smile Design for Predictable Aesthetic Results. Balkan Journal of Dental Medicine, 2016, 20: 172–177.
7. Imburgia, M., Ch. Coachman. Using digital devices to improve communications between clinicians and patients during implant-prosthetic treatment A clinical study. Presented at the 23rd Annual Scientific Meeting of the European Association for Osseointegration, Rome, Italy, 25–27 September 2014.
8. Morley, J., J. Eubank. Macroesthetic elements of smile design. JADA, 2001, 132: 39–45.
9. Nold, S., S. Horvath, S. Stampf, M. Blatz. Analysis of Select Facial and Dental Esthetic Parameters. The International Journal of Periodontics & Restorative Dentistry, 2014, 34(5): 623–629.
10. Paolucci B, Calamita M, Coachman Ch, Gurel G, Shaider A, Hallawell Ph. Visagism: The art of dental composition. Quintess Dent Technol, 2012; 35: 187–201.
11. Pauwels R et al. CBCT-based bone quality assessment are: Hounsfield units applicable. Dent Maxillofac radiology. 2015, 44(1): 238 223.
12. Tardeu P.B, Vrielinck L, Escolano E. Computer-assisted implant placement. A case report: treatment of mandible. The International journal of oral and maxillofacial implants, 2003,18(4): 599–604
13. Turbush S.K., Turkyilmaz I., Accuracy of three different types stereolithographic surgical guides in implant placement: an in vitro study. The journal of prosthetic dentistry, 2012, 180(3): 181–8.
14. Walter C et al. Three-dimensional imaging as preoperative tool in decision making for furcation surgery. Journal of clinical periodontology, 2009, 36(3): 250–7.
15. Yankov, B., G, Iliev., D, Filtchev., G, Gurel., B, Paolucci., A, Schayder., I, Misheva. Software Application for Smile Design Automation Using the Visagism Theory. Proceedings of the 17th International Conference on Computer Systems and Technologies, CompSysTech’16, June 23–24, Palermo, Italy, ACM International Conference Proceeding Series, Vol. 1164, ACM Inc., N.Y. USA, pp. 237–244, doi>10.1145/2983468.2983521.
16. Zaccaria, M., N. Squadrito. Photographic-assisted prosthetic design technique for the anterior teeth. The International Journal of Esthetic Dentistry, Spring 2015, 10(1): 49–67.
17. Zimmermann, M., A. Mehl. Virtual smile design systems: a current review. International Journal of Computerized Dentistry, 2015, 18(4): 303–317.

33 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
Guided surgery with a soft tissue graftMinimally invasive surgery in a highly demanding case
Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 33
S ince the introduction of guided surgery as a tool for implant placement, the principles have not changed significantly; the clinical results have. Initial studies
reported a considerable number of technique-related perioperative complications; reasonable mean accuracy; and relatively high maximum deviations1–8. These studies concluded that guided surgery was advisable only in favourable situations9, 10. On the other hand, the 2015 EAO Consensus Conference found that, providing certain preconditions are met, guided surgery can provide higher levels of accuracy than free-hand procedures. According to the Consensus Conference, guided surgery may be indicated for complex anatomical cases; minimally invasive surgeries; aesthetic optimisation; and immediate loading11.
This shift in our perception of guided surgery has occurred mainly because of how it is used and by whom. Guided surgery was originally introduced as a technique which could be used by any clinician, no matter what their level of expertise. In reality, however, high levels of surgical skill and experience are essential requirements for success and accuracy9, 10.
Different approaches are described in the literature for replacing buccal volume shrinkage concerning hard and soft tissues which have been lost due to bone resorption12. There are a variety of options for soft tissue augmentation, and although soft tissue matrices are available in many different materials, autogenous materials generally provide the best results19. They are more predictable; exhibit long-term stability; have a shorter healing period; and allow immediate
provisionalisation13, 14. They are probably the best option for horizontal tissue augmentation15, 16.
Initial situation
The patient was a 16 year-old girl. She was congenitally missing a right lateral incisor (agenesis) and had a small left lateral incisor (microdontia) which had been restored with resin (Figures 1–3). This gave her low self-esteem and kept her from smiling. It was a very challenging case due to the age of the patient and her expectations about aesthetic outcomes.
Treatment plan
One year of orthodontic treatment was necessary to make space for tooth 12 and to enlarge mesiodistal distance for tooth 22. A skeleton maturation analysis and symphysis enclosing is also mandatory to start implant therapy, confirmed by an x-ray of the left wrist (Figure 4).
Guided surgery using a pilot-drill surgical template (Nobel Biocare) was the technique selected for its accuracy and because it is a conservative procedure. It was decided that a tunnel technique would be performed17, 18 through the drilling access using micro-surgical techniques and a connective tissue graft would be placed to compensate for buccal volume recession.
Immediate provisionalisation would follow implant insertion, along with the connective tissue graft. The treatment plan also proposed a gingivectomy to augment the length of tooth 22. A
In 2000, José
Pinheiro Torres completed his Master in Implant Dentistry degree at the University of Gothenburg, Sweden. He was awarded the EAO’s Certificate in Implant Based Therapy in 2016. He qualified as a periodontist (OMD) in 2017, and currently lectures and administrates courses in the field of periodontology and implant dentistry.
w: clinicapinheirotorres.com
Figure 1 Figure 2
Figure 3 Figure 5
Figure 4

Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 34
ceramic/zirconia crown was selected to correct the congenital defect. An implant-supported ceramic/zirconia crown would also be used for tooth 12.
Implant therapy
Aft er orthodontic treatment, it is important to identify the challenges that must be dealt with before commencing implant therapy: in this case, the insuffi cient distal papilla at tooth 11 and the lack of buccal volume caused by the absence of tooth 12 (Figures 5 and 6).
1. Guided surgery plan
Due to space restrictions, a pilot-drill template for a 2mm diameter drill was chosen for the procedure. Only a single drill was required for the 3.5x15mm implant. Th e cast and wax-up could be digitalised to maximise accuracy and optimise placement (Figures 7 and 8).
2. Implant placement
Aft er adjusting the surgical template, the bone was drilled as planned with a 2mm diameter drill. A tissue punch guide was used to enlarge the aperture at the soft tissue level to the 3.5mm diameter required for the implant (NobelActive NP 3.5x15mm). Th is was done to provide a larger opening for the next procedure – a soft tissue graft (Figures 9–12).
3. Soft tissue graft
Ophthalmic blades can assist while performing the tunnel technique through a 3.5mm access. Th e key challenge was to pass the graft through the very small opening. In these situations, rolling the graft may help (Figures 13–16).
Outcome and conclusion
Immediately aft er surgery, increased buccal volume was observed as a result of the keratinised soft tissue graft (Figures 17 and 18). Aft er two years, acceptable and balanced buccal volume was maintained (Figure 19). Soft tissue development was positive, and the mesial papilla of tooth 12 was satisfactory. Th e soft tissue was able to provide high stability for the complex implant crown and was capable of compensating buccal depression caused by bone resorption. Th e patient’s expectations were fulfi lled; she felt happy and secure, and exhibited a very nice smile.
Concluding observations:
when executed by a clinician with the necessary experience, it is a very accurate procedure which can ensure highly precise positioning of the implant; it is also minimally invasive and allows immediate provisionalisation
a certain amount of time must be devoted to shaping papillae and soft tissue maintenance during the healing period
using a micro-surgical procedure to insert the soft tissue graft is a very delicate operation – the vascular integrity of the periosteum must be maintained to achieve good results
as a one-step surgical procedure, it is a comfortable option forthe patient
alternative augmentation procedures (such as GBR) usually impose fl ap surgery with all of its associated disadvantages (such as longer healing times; vascular disruption of the periosteum; and the aggressiveness of the technique)
it still is an experimental technique but has promising results (Figures 20–22)
Figure 9
Figure 12
Figure 10
Figure 13
Figure 11
Figure 14
Figure 7 Figure 8Figure 6

35 | Volume 5, Issue 1: Summer 2017 | Inspyred: The alternative EAO voice
Figure 16
Figure 18
Figure 22Figure 20
Figure 15 Figure 17
Figure 19
Figure 21
References
1. Schneider D et al. (2009) A systematic review on the accuracy and the clinical outcome of computer-guided template-based implant dentistry. Clinical Oral Implants Research 20 (Suppl. 4): 73–86
2. Brief J et al.(2005) Accuracy of image-guided Implantology. COIR. 16: 495–501.
3. Di Giacomo GA et al. (2005) Clinical application of stereolithographic surgical guides for implant placement: preliminary results. Journal of Periodontology 76: 503–507.
4. Fortin T et al. (2003) Reliability of preoperative planning of an image-guided system for oral implant placement based on 3-dimensional images: an in vivo study. IJOMI 18: 886–893.
5. Komiyama A et al. (2008) Treatment outcome of immediately loaded implants installed in edentulous jaws following computer-assisted virtual treatment planning and flapless surgery. COIR 19: 677–685.
6. Mischkowski RA et al. (2006) Comparison of static and dynamic computer-assisted guidance methods in implantology. International Journal of Computerized Dentistry 9: 23–35.
7. Laederach V et al. (2016) Deviations of different systems for guided implant surgery. COIR. 0: 1–5
8. Nickenig HJ et al. (2007) Reliability of implant placement after virtual planning of implant positions using cone beam CT data and surgical (guide) templates. Journal of Craniomaxillofacial Surgery 35: 207–211.
9. Hultin M et al. (2012) Clinical advantages of computer guided implant placement. COIR. 23 (Suppl. 6): 124–135.
10. Van Assche N et al. (2012) Accuracy of computer guided implant placement. Clinical Oral Implants Research 23 (Suppl. 6): 112–123.
11. Hämmerle C et al. (2015) Digital technologies to support planning, treatment, and fabrication processes and outcome assessments in implant dentistry. Summary and consensus statements. The 4th EAO Consensus Conference 2015. COIR. 26 (Suppl. 11): 97–101.
12. Tan WL et al. (2012) A systematic review of post-extraction alveolar hard and soft tissue dimensional changes in humans. Clin Oral Res 23 (Suppl 5):1–21
13. Kan JY et al. (2009) Facial gingival tissue stability after connective tissue graft with single immediate tooth replacement in the esthetic zone: consecutive case report. Journal of Oral and Maxillofacial Surgery; 67(11):40–8.
14. Kan JY et al. (2005) Bilaminar subepithelial connective tissue grafts for implant placement and provisionalization in the esthetic zone. Journal of the California Dental Association; 33:865.
15. Zucchelli G et al. (2012) A novel surgical–prosthetic approach for soft tissue dehiscence coverage around single implant. COIR. 00:1–6
16. Wiesner G (2010) Connective tissue grafts for thickening peri-implant tissues at implant placement. One-year results from an explanatory split-mouth randomised controlled clinical trial. Eur J Oral Implantol 3(1):27–35
17. Azzir R et al. (2002) Surgical Thickening of the Existing Gingiva and Reconstruction of Interdental Papillae Around Implant-Supported Restorations. International Journal of Periodontics & Restorative Dentistry 22 (1):70–77.
18. Zuhr O et al. (2007) Covering of Gingival Recessions with a Modified Microsurgical Tunnel Technique: Case Report. Int J Periodontics Restorative Dent 27(5):457–463.
19. Thoma D (2009) A systematic review assessing soft tissue augmentation techniques. COIR. 20(4):146–165

Issue No. 01 / September 2013
The alternative EAO voice
Inspyred
Clinical casesBy Irena Sailer, Stefan Fickl and Tommie Van de Velde
Who’s whoMeet the Editorial
Committee of Inspyred
Highlights of Dublin 2013Ailsa Nicol talks to David Harris
The True Voice CornerMarco Esposito on peri-implantitis
25th
annualscientificmeetingof theeuropeanassociationfor osseointegration
eao-congress.com
PARISfrom september 29th
to october 1st, 2016
Invited countryJapan
In collaboration with
FINAL Programme
Congress Scientific ReportEAO 24th Annual Scientific MeetingStockholm, 24–26 September 2015
Issue 1, April 2016
InspyredThe alternative EAO voice
Volume 4, Issue 1 / Summer 2016
Screw-retained implant crownsTechnical solutions for challenging situations
“Paris is always a good idea”
Countdown to the EAO Congress
Effective teamwork
for optimal outcomes
Evaluating the role of soft tissue substitutes
When and how to use d-PTFE
membranes
Inspyred: The alternative EAO voice | Volume 5, Issue 1: Summer 2017 | 36
Have you discovered the EAO Online Library?There's a whole library at your fingertips
The EAO is committed to promoting clinical excellence and helping its members reach
their full potential. A wealth of online content is now available to allow members to stay abreast of the latest research developments and clinical guidelines, including:
quick access to Inspyred articles, along with the complete sets of figures and references
downloadable Congress Scientific Reports webcasts, E-posters and abstracts from the annual scientific meetings
information on educational activities
Members can log in to the Online Library with their EAO credentials. Do not hesitate to contact the EAO Office for more information.
Published by:European Association for Osseointegration,38 rue Croix des Petits Champs,75001 Paris, FranceEmail: [email protected]: www.eao.org/inspyred
European Association for Osseointegration
europeanassociationforosseointegration
eao_association
The views expressed in the articles published in this magazine are those of the author(s) and do not necessarily represent EAO’s position on these issues. EAO cannot be held liable for any statements expressed therein.
Inspyred is designed and produced by www.publishingbureau.co.uk
MEMBERS
SELECTED CONTENTRESERVED FOR
EDUCATIONInfo on coursesCertification
SCIENTIFICCONTENT
WebcastsE-postersAbstracts
PUBLICATIONSArticlesReportsJournals
PREMIUM ACCESS
Related Documents











