Myopathy working group: Myopathy SSc database Lori Chung, Oliver Distler, Vivien Hsu, Veronika Jäger, Britta Maurer, Lesley Saketkoo, Uli Walker, and all SCTC and EUSTAR members

Myopathy working group: Myopathy SSc database Lori Chung, Oliver Distler, Vivien Hsu, Veronika Jäger, Britta Maurer, Lesley Saketkoo, Uli Walker, and all.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Myopathy working group:Myopathy SSc database
Lori Chung, Oliver Distler, Vivien Hsu, Veronika Jäger, Britta Maurer, Lesley Saketkoo, Uli Walker, and all SCTC and EUSTAR members
Objective
To establish a prospective observational cohort for SSc patients with
suspected muscle involvement.
Inclusion criteria are (any one is sufficient for inclusion):• Elevated levels CK or aldolase without obvious explanation
(e.g. extensive exercise, intramuscular injections, muscle injury)
• Proximal muscle weakness on physical examination not explainable by other causes (e.g. neuropathogenic, genetic, metabolic, endocrinologic, infectious disorders, drug-induced, cachexia)
• Muscle atrophy on physical examination not explainable by other causes (e.g. neuropathy, genetic disorders, cachexia)
• Positive myositis-associated autoantibodies (Jo-1, PM-Scl, U1-RNP, Ku, Mi-2, SRP, PL-7, PL-12, OJ, EJ, p155/140, MDA5, NXP2)
Data obtained - Domains
All EUSTAR SSc data, Myopathy Domains: History, Lab Markers, Physician
Outcome Assessment (Muscle Strength etc.), Patient Reported Outcomes,
Muscle Biopsy, EMG, Imaging (MRI)
Start: May 2014
November 2014: 72 patients enrolled from 15 centers
Basel, Zurich, Paris Cochin Hospital, Verona, Niska Banja (Serbia), Roma La
Sapienza, Bucharest Cantacuzino Hospital, Istanbul, Marseille, Madrid, New
Orleans, New Brunswick/New Jersey, Strasbourg, Stanford
Please join!
Ethic approval observational study, EUSTAR membership, annual follow
recommended

Calcinosis Working Group
• Multidisciplinary effort:– Members from US, Europe, Canada,
Australia, Mexico– Rheumatology, Radiology, Dermatology
• How to get involved:– Please contact Dr. Lorinda Chung (
[email protected]) or Antonia Valenzuela ([email protected])

Calcinosis Working Group
• Current projects and status– Validated radiographic scoring system1 – Multicenter retrospective study of 5280 patients
• Prevalence of calcinosis 24%• Strong association of calcinosis with digital ulcers (OR=3.9)
and osteoporosis (OR=4.7)– Next steps:
• Prospective database study - SCTC grant submission • Collection of preliminary data on PAH-specific medications
for treatment of calcinosis to support design of prospective clinical trial
1Chung L, Valenzuela A, Fiorentino D, Stevens K, Li S, Harris J, Hutchinson C, Assassi S, Beretta L, Lakshminarayanan S, Rodriguez-Reyna TS, Denton CP, Taillefer RG, Herrick AL, Baron M; on behalf of the Scleroderma Clinical Trials Consortium Calcinosis Working Group. Validation of a Novel Radiographic Scoring System for Calcinosis Affecting the Hands of Patients with Systemic clerosis.Arthritis Care Res. 2014 Aug 22.

SCTC GI Working Group Update
Zsuzsanna McMahan, MD, MHSDinesh Khanna, MBBS, MSc; Tracy Frech, MD, MS
ACR 2014, Boston
Overview
• Brief background• Purpose and goals• Status update• Come and join us!
Review of Previous SCTC Meetings and Outcomes
2012 consensus: Investigational modalities are available, but validating outcomes are needed for SSc patients with symptomatic:
• Reflux• Gastroparesis• SIBO• Constipation• Fecal incontinence
Recommendations summarized in article: Khanna D, Nagaraja V, Gladue H, et al. Measuring response in the gastrointestinal tract in systemic sclerosis. Curr Opin Rheumatol 2013;25:700 6.‐

Purpose and Plans
• 2014 SCTC seed grant funding – PI: Dinesh Khanna (University of Michigan)
– Develop and maintain an electronic database that can facilitate collaboration among scleroderma experts internationally for patients with symptomatic GI involvement.
– Inclusion/exclusion criteria, assessment and outcome measures have been discussed among the GI working group via conference call and with GI experts at several institutions, including Michigan and Hopkins
Recruitment
• Who do we want to recruit?– Patients with scleroderma who have active GI
symptoms for which there is a plan to make a change in management
• Inclusion and exclusion criteria– Vary depending on the GI complication– Discussed in more detail in the GI working group
meeting
Data Collection• Baseline Visit
– Consent– MD CRF– Inclusion criteria for each condition– Symptom specific questionnaires– UCLA SCTC GIT 2.0– NIH PROMIS
• Follow up– MD Anchor – Symptom specific questionnaires– UCLA SCTC GIT 2.0– NIH PROMIS
• REDCap (Research Electronic Data Capture)
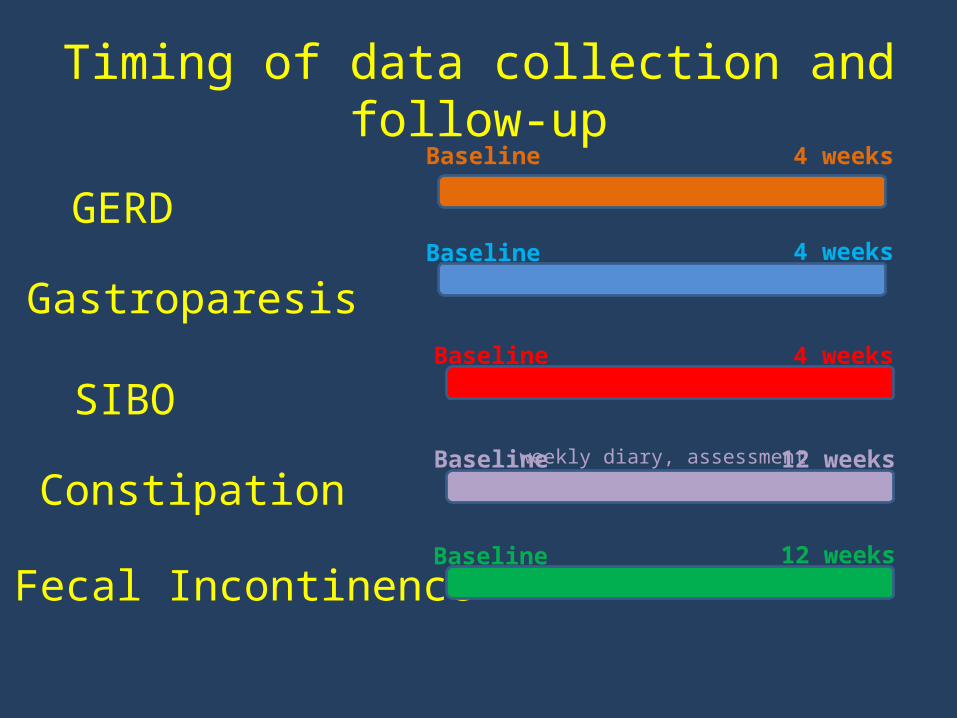
Timing of data collection and follow-up
GERD
Gastroparesis
SIBO
Constipation
Fecal Incontinence
Baseline 4 weeks
Baseline 4 weeks
Baseline 4 weeks
Baseline 12 weeksweekly diary, assessment
Baseline 12 weeks
Symptom specific questionnaires• Reflux
– Reflux Disease Questionnaire, GERD-Q, Quality of Life in Reflux and Dyspepsia (QOLRAD)
• Gastroparesis – Gastroparesis Cardinal Symptom Index
• SIBO – Likert scale
• Constipation – Constipation weekly assessment– Includes the Bristol stool chart
• Fecal incontinence – Quality of life scale for fecal incontinence
Status update
• Currently the protocol is IRB approved at 3 centers
• Recruitment began in August 2014 at the University of Michigan
• Thus far, 7 patients enrolled as of November 3,2014
• Our goal for recruitment is 500 patients
Ultimate Goals
• Validate outcome measures for clinical trials in scleroderma gastrointestinal disease
• Improve strategies to treat GI dysmotility in our patients
Come and join us!

SCTC Cardiac Sub-Committee
Updates
ALESSANDRA VACCA
S.C. e Cattedra di Reumatologia
A.O.U. di CAGLIARI
Present progress
Future Research Project
• Examination of Mortality and the Need for Electrical Device Implantation in Systemic Sclerosis Patients with Cardiac Conduction and Rhythm Abnormalities.
Objective
•1) to retrospectively collect, among EUSTAR centers, SSc patients:
A. who required pace-maker or implantable cardioverter devices
B.who died because of arrhythmia or conduction abnormalities
•2) to investigate possible correlations with disease phenotype in these subgroups
•3) To identify markers predictive of severe arrhythmias and conduction abnormalities in SSc

Patients and Methods• Patients will be selected from EUSTAR database
• EUSTAR centers will be invited to fill out a standardized form for patients meeting inclusion criteria, with the additional variables.
• A control group of SSc patients with no symptoms and normal ECG, matched for age, sex and disease duration for comparison will be selected.
• We will consider correlations with demographic data, disease duration, disease phenotype looking in particular at organ involvement, auto-antibodies, specific therapies.
• All EUSTAR participating centers would be co-author(s) in this work.
Expected Results
• 40-50 patients to be included in this study.
• High prevalence of rhythm and conduction defects, but few and out-dated studies which lacked focus on severe rhythm and conduction defects requiring electrical devices.
• Eustar cohort is a unique opportunity to better define the prevalence, the specificities, risk factors and management of this subgroup of patients.
• This may help to differentiate between mild abnormalities and those leading to a fatal outcome with the potential of providing data for the development of appropriate treatment guidelines to improve the overall prognosis of SSc patients.
Agenda
• A preliminary description of the project will be soon available on SCTC web-site
• End of November: submission for approval to EUSTAR board
• February 2015: submission to SCTC and EUSTAR centers.
For suggestions/comments:
Systemic Sclerosis Damage Index Working Group Update
Co-chairs: Mandy Nikpour (Melbourne) and Murray Baron (Montreal)SCTC Annual Business Meeting, Saturday November 15th 2014
Develop a disease damage index to systematically quantify organ damage in SSc.
Potential applications:◦End-point in observational and interventional studies◦Quantifying disease burden in epidemiologic studies◦Describing differences between cohorts◦Enriching studies
Goal

• 25 international members• Steering committee comprised of 7 of these
members– Mandy Nikpour, Murray Baron– Marie Hudson, Susanna Proudman, Wendy Stevens – Research Fellows: Tien Tay and Nava Ferdowsi
(Melbourne)• Expert panel of non-rheumatologist advisors with a special interest
in SSc • Methodologists/biostatisticians
SSc-DI Working Group

• 3 patient partners representing USA, UK and Australia– Conceptual definition of damage– Items included in the SSc-DI survey– Reduced/final list of items
Patient partners
• First Working Group meeting at ACR ASM 2013• Two-round survey to obtain consensus regarding
the conceptual definition of damage in SSc• Systematic review of existing measures of disease
status in SSc• Item generation• Online survey hosted on REDCap currently open
Progress over 12 months
• Permanent and irreversible loss of anatomical structure and physiologic function
• Directly caused by SSc or its treatment and not due to comorbidities
• Differentiated from disease activity (potentially reversible) and severity (no distinction between damage and activity)
• PRO not included
• Predictive of morbidity and/or mortality
• Duration that an item must be present before being called damage depends on the item
Conceptual definition of damage in SSc

Systematic review of measures of disease status in SSc – Poster 721 (Sunday 9-11 am)

Based on systematic review Input from expert advisors Input from Working Group members
◦ Total of 83 items in 7 domains 1. Musculoskeletal and skin (19 items)
2. Vascular system (8 items)
3. Cardiac system (20 items)
4. Respiratory system (6 items)
5. Gastrointestinal system (17 items)
6. Renal system (4 items)
7. Damage from treatment (9 items)
Item generation
• Each item rated according to its appropriateness (importance and feasibility) for inclusion in the damage index.
• Duration that an item must be present before constituting damage also addressed
• One round only
Online REDCap Survey
69 complete responses to date Further 12 as yet incomplete responses
100-140 respondents required to power the planned statistical analyses to reduce the items.
All respondents acknowledged in publications.
Survey
Asia n=1Australia = 15Europe = 34North America = 16South America = 3
Profile of respondents to date
• Rasch modeling to reduce the items• Structural equation modeling (SEM) to weight
the items against mortality using Australian (and Canadian) cohort data
Planned analyses (next 6 months)
L201 – 2nd floor School of Medicine (L-Building) at 72E◦ Further discussion of points arising from
preliminary analysis of survey data
◦ Please address enquiries to
Mandy Nikpour
Murray Baron
Working Group Meeting 8:30-9:30 pm
Please respond to the survey if you have not done so already.
The success of this project depends on your response.
Related Documents