Be a Surgical “Multiplier” in MIGS Inspire Brilliance Through Teamwork Scientific Program Chair Jubilee Brown, MD Honorary Chair Barbara S. Levy, MD President Marie Fidela R. Paraiso, MD SYLLABUS MYO-613 : Multiple Modalities of Myomectomy

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Be a Surgical “Multiplier” in MIGS Inspire Brilliance Through Teamwork
�
��
�
Scientific Program ChairJubilee Brown, MD
Honorary ChairBarbara S. Levy, MD
PresidentMarie Fidela R. Paraiso, MD
SYLLABUSMYO-613:
Multiple Modalities of Myomectomy

Professional Education Information
Target Audience This educational activity is developed to meet the needs of surgical gynecologists in practice and in training, as well as other healthcare professionals in the field of gynecology. Accreditation AAGL is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. The AAGL designates this live activity for a maximum of 3.75 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. Disclosure of Relevant Financial Relationships As a provider accredited by the Accreditation Council for Continuing Medical Education, AAGL must ensure balance, independence, and objectivity in all CME activities to promote improvements in health care and not proprietary interests of a commercial interest. The provider controls all decisions related to identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the activity. Course chairs, planning committee members, presenters, authors, moderators, panel members, and others in a position to control the content of this activity are required to disclose relevant financial relationships with commercial interests related to the subject matter of this educational activity. Learners are able to assess the potential for commercial bias in information when complete disclosure, resolution of conflicts of interest, and acknowledgment of commercial support are provided prior to the activity. Informed learners are the final safeguards in assuring that a CME activity is independent from commercial support. We believe this mechanism contributes to the transparency and accountability of CME. Anti-Harassment Statement AAGL encourages its members to interact with each other for the purposes of professional development and scholarly interchange so that all members may learn, network, and enjoy the company of colleagues in a professional atmosphere. Consequently, it is the policy of the AAGL to provide an environment free from all forms of discrimination, harassment, and retaliation to its members and guests at all regional educational meetings or courses, the annual global congress (i.e. annual meeting), and AAGL-hosted social events (AAGL sponsored activities). Every individual associated with the AAGL has a duty to maintain this environment free of harassment and intimidation. AAGL encourages reporting all perceived incidents of harassment, discrimination, or retaliation. Any individual covered by this policy who believes that he or she has been subjected to such an inappropriate incident has two (2) options for reporting:
1. By toll free phone to AAGL’s confidential 3rd party hotline: (833) 995-AAGL (2245) during the AAGL Annual or Regional Meetings.
2. By email or phone to: The Executive Director, Linda Michels, at [email protected] or (714) 503-6200.
All persons who witness potential harassment, discrimination, or other harmful behavior during AAGL sponsored activities may report the incident and be proactive in helping to mitigate or avoid that harm and to alert appropriate authorities if someone is in imminent physical danger. For more information or to view the policy please go to: https://www.aagl.org/wp-content/uploads/2018/02/AAGL-Anti-Harassment-Policy.pdf

Table of Contents Course Description ........................................................................................................................................ 1 Disclosure ...................................................................................................................................................... 3
Myomectomy vs. Hysterectomy: Rationale, Safety, and Outcome Data W.H. Parker ................................................................................................................................................... 4
Preoperative Evaluation and Optimization for Myomectomy M.T. Siedhoff ............................................................................................................................................... 13
Hysteroscopic Myomectomy K.N. Wright .................................................................................................................................................. 24
Laparoscopic Myomectomy: Instruments and Techniques M.T. Siedhoff ............................................................................................................................................... 28
Robotic-Assisted Myomectomy: Instruments and Techniques M.D. Truong ............................................................................................................................................... 34
Tissue Extraction M.D. Truong ............................................................................................................................................... 39
Abdominal Myomectomy: A Minimally-Invasive Alternative to Laparoscopic Hysterectomy, Instruments and Techniques W.H. Parker ................................................................................................................................................ 46
Postop Management K.N. Wright ................................................................................................................................................. 53
Cultural and Linguistics Competency ......................................................................................................... 58

MYO-613: Didactic: Multiple Modalities of Myomectomy
Co-Chair: William H. Parker, Matthew T. Siedhoff Faculty: Mireille D. Truong, Kelly N. Wright
Course Description This course provides a comprehensive review of the principles and techniques of various modalities of uterine-preserving myomectomy for fibroids. Video will be used extensively to illustrate techniques that allow successful outcomes. For centuries, the “preferred” surgery for women with these benign growths has been removal of the entire organ (i.e., hysterectomy), but the reasons for that preference—that hysterectomy is safer, and a better operation—will be questioned by review of the medical literature. The course will demonstrate, with high-quality evidence and video presentation, all of the modalities of minimally-invasive myomectomy, including hysteroscopy, laparoscopy, robotic-assisted, and laparotomy. We will also demonstrate appropriate workup to optimize patients for the OR and discuss how to counsel and manage these women postoperatively.
Course Objectives At the conclusion of this activity, the participant will be able to: 1) Complete an appropriate workup for patients undergoing myomectomy; 2) choose the appropriate route of surgery for the individual fibroid pathology; 3) describe instruments and surgical techniques for different approaches to myomectomy; and 4) counsel patients on the risk of leiomyosarcoma.
Course Outline 12:30 Welcome, Introductions, and Course Overview W.H. Parker,
M.T. Siedhoff12:35 Myomectomy vs. Hysterectomy: Rationale, Safety, and Outcome Data
• Debunking myths of myomectomy• LMS risk• Myoma “recurrence”
W.H. Parker
1:00 Preoperative Evaluation and Optimization for Myomectomy • Exam, US, SIS, MRI, LDH, EMB• Choosing the appropriate route of surgery, fertility issues• Correction of anemia, Iron infusions, GnRH, Ulipristal• Pre-op meds—tranexamic
acid/misoprostol/vasopressin/tourniquets
M.T. Siedhoff
1:25 Hysteroscopic Myomectomy: • Instruments and Techniques for resection, morcellation, cold
loop
K.N. Wright
1:50 Laparoscopic Myomectomy: Instruments and Techniques M.T. Siedhoff
2:15 Questions & Answers All Faculty
2:25 Break
2:40 Robotic-Assisted Myomectomy: Instruments and Techniques M.D. Truong
3:05 Tissue Extraction: • Uncontained extraction• Contained extraction
W.H. Parker,M.D. Truong
3:30 Abdominal Myomectomy: A Minimally-Invasive Alternative to Laparoscopic Hysterectomy, Instruments and Techniques
W.H. Parker
Page 1

3:55 Postop Management: • ERAS for open and MIS cases• Mode of future obstetric delivery, risk of uterine rupture
K.N. Wright
4:20 Questions & Answers All Faculty
4:30 Adjourn
Page 2

PLANNER DISCLOSURE The following members of AAGL have been involved in the educational planning of this workshop (listed in alphabetical order by last name). Art Arellano, Professional Education Director, AAGL* Linda D. Bradley, Medical Director, AAGL* Erin T. Carey Consultant: MedIQ Mark W. Dassel Contracted Research: Myovant Sciences Erica Dun* Adi Katz* Linda Michels, Executive Director, AAGL* Erinn M. Myers Speakers Bureau: Laborie Medical Technologies, Teleflex Medical Other: Unrestricted educational grant to support NC FPMRS Fellow Cadaver Lab: Boston Scientific Corp. Inc. Amy Park* William H. Parker Consultant: Abbvie Grace Phan, Professional Education Specialist, AAGL* Matthew T. Siedhoff Consultant: Applied Medical, Caldera Medical, CooperSurgical, Olympus Harold Y. Wu* Linda C. Yang Other: Ownership Interest: KLAAS LLC SCIENTIFIC PROGRAM COMMITTEE Linda D. Bradley, Medical Director, AAGL* Jubilee Brown* Nichole Mahnert* Shanti Indira Mohling* Fariba Mohtashami Consultant: Hologic Marie Fidela R. Paraiso* Shailesh P. Puntambekar* Matthew T. Siedhoff Consultant: Applied Medical, Caldera Medical, CooperSurgical, Olympus Amanda C. Yunker Consultant: Olympus Linda Michels, Executive Director, AAGL*
FACULTY DISCLOSURE The following have agreed to provide verbal disclosure of their relationships prior to their presentations. They have also agreed to support their presentations and clinical recommendations with the “best available evidence” from medical literature (in alphabetical order by last name). William H. Parker Consultant: Abbvie Matthew T. Siedhoff Consultant: Applied Medical, Caldera Medical, CooperSurgical, Olympus Mireille D. Truong* Kelly N. Wright Consultant: Acessa, Applied Medical, Boston Scientific Corp. Inc., Hologic, Karl Storz Content Reviewer has nothing to disclose. Asterisk (*) denotes no financial relationships to disclose.
Page 3

William H. Parker, MD
Clinical Professor
UC San Diego School of Medicine
Disclosures
�Consultant: Abbvie
Objectives
Following this talk, attendees will be able to:
� Estimate the Risk of subsequent fibroid treatment following myomectomy
� Summarize the benefits to quality‐of‐life for women having a myomectomy
� Discuss the intra‐operative risks of hysterectomy and myomectomy
� Approximate the risk of leiomyosarcoma among women having surgery for presumed fibroids
Question ?
~ 200,000 hysterectomies a year for fibroids
What surgical specialties routinelyremove entire organs for
benign tumors?
Breast Cancer Surgery Radical Mastectomy
Modified radical
SimpleLumpectomy & Lymphadenectomy
Lumpectomy, Sentinel node Paradigm Shift
MISOrgan Conservation
Fibroids : Quality‐of‐Life
�Women having hysterectomies because of
fibroid‐related symptoms
�Significantly worse SF‐36 quality‐of‐life scores than women with:
‐ Heart disease
‐ Chronic lung disease
‐ Arthritis
Rowe MK. Obstet Gynecol 1999;93:915-21.
Page 4

“The restoration and maintenance of physiologic function is, or should be, the ultimate goal of surgical treatment”
Victor Bonney
early advocate of myomectomy, 1931
Myomectomy
30,000 Myomectomies per year
Why Don’t Gynecologists Perform More Myomectomies ?
Questions ?
How Many Hysterectomies (TAH + VH + TLH) Does the RRC Require for Residency Completion ?
85
How Many Myomectomies (Open + Lap) Does the RRC Require for Residency Completion ?
0
Myomectomy Myths
� Hysterectomy is Safer than Myomectomy
�Myomectomy Has More Blood Loss than Hysterectomy
� Uterus Will Look Like Swiss Cheese After Myomectomy
� Fibroids Will Grow Back After Myomectomy
� Hysterectomy (with Ovarian Conservation) Will Not Change Your Hormones
� Fibroid Growth (pre‐menopause) Indicates Sarcoma
�Myomectomy Will Not Improve Symptoms
� Your Fibroids Will Continue to Grow and Get Too Large to Remove
Hysterectomy is Safer than Myomectomy
MYTH
HysterectomySurgical Considerations
Ureter ?
Bowel ?
PelvicSidewall ?
Uterine Vessels ?
Page 5

Fibroids = Onions
�Push away myometrium
�Pseudocapsule
�Do not invade
�ureters, bladder, bowel
Myomectomy vs. Hysterectomy
�Surgical Complications
�Hysterectomy
� 2 – ureteral injuries
� 1 – bladder injury
� 1 – bowel injury
� 1 – femoral nerve injury
�Myomectomy
� No injuries
Iverson, Obstet Gyn 1996;88:415
Myomectomy v. HysterectomySystematic Review
� 6 studies, 1520 women, up to 18 weeks uterine size
Pundir J. J Obstet Gynecol 2013;33:655‐62
Myomectomy Hysterectomy
Visceral Injury 1.3% 2.0%
Life threatening 0.4% 0.4%
Return to OR 0.7% 0.9%
Readmission 1.1% 0.5%
EBL 582 ml 869 ml (p<0.00001)
Transfusion 19% 22% NS
NS
NS
NS
NS
Your uterus will look like
Swiss cheese after a myomectomy
MYTH
Swiss Cheese Theory
� Abdominal Myomectomy (n=14)
� 65‐380 gms of fibroids removed
�MRI at 12 months
�Uterine volume = 65 ml (+/‐ 20 ml)
� Normal = 57 ml (+/‐ 18 ml)
Tsuji S, Gynecol Obstet Invest, 2006
Page 6

6 Months Post-op
Fibroids will just grow back
after myomectomy
New Appearance
MYTH
New Appearance ‐ US
�67 women
�9 year follow‐up
�Sonographic evaluation
� 34 = 50%
(Prevalence at age 50 = 77%)
Sudik. Eur J Obstet Gyn Reprod Biol 1996;65:209
> 1 cm
Require Further Treatment
�Re‐operation�7 studies, 10 – 25 year follow‐up
�872 women
� 95 (10.9%) ‐ reoperation
�89% did not require surgery
Fauconnier. Hum Reprod Update 2000;6:595
Myomectomy Will Not Improve Symptoms
MYTH
Myomectomy and Quality‐of‐Life
Before treatment 1 Year after
Symptom Severity 55.9 18.3
HRQL 46.4 86.3
Activities 49 88
Mood 47.2 84
Control (health, life, future)
46.8 87.9
Sex function 46.6 88.8
Concern 44.2 86.2
Monyonda I. Cardiovasc Intervent Radiol 2012;35:530–536
Page 7

Myomectomy and Quality‐of‐Life
Thank you, Mariana Alpern
Hysterectomy (with Ovarian Conservation)
Will Not Change Your Hormones
MYTH
Hysterectomy and Menopause
�Hysterectomy = 257 / No Hysterectomy = 259
�Matched – age, FSH, BMI, smoking, parity
� Followed for 5 years, annual FSH
�Menopause
�21% hysterectomy / 7 % no hysterectomy� Average of 3 years early
Farquhar C, Int J Obstet Gynecol 2005;112:956‐2.
� Baseline AMH Similar
� 148 hysterectomy/ovarian retention (1.1, 0.4‐2.2)
� 172 referent (1.0, 0.5‐2.8)
� AMH ‐ 1 year post hysterectomy
� 21% referent
� 41% hysterectomy, ovarian retention (p< 0.001)� More pronounced in black women than white women
Hysterectomy and Menopause
Trabuco E. Obstet Gynecol 2016;127:819‐27
Myomectomy Has More Blood Loss than Hysterectomy
MYTH
Myomectomy, n = 103
Hysterectomy, n = 89
Myomectomy vs. Hysterectomy
No difference in blood loss when corrected for uterine size
Iverson, Obstet Gyn 1996;88:415
No difference in blood transfusions
Page 8

Reducing Intraoperative Blood Loss�Misoprostol (cytotec)
� 400 mcg vaginally 30 min before surgery
� ‐ 149 ml
� Vasopressin (20U / 100 ml NS)
� ‐ 299 ml
� Tranexamic Acid (1 gm IVPB in OR)
� ‐ 150 ml
�Tourniquet Uterine Vessels
� ‐ 1,870 ml
Cochrane Reviews: 2007
Your Fibroids Will Grow and Be
Too Big to Remove
MYTH
Fibroid Growth
Interactions Among:�Genetics
� mutations – t(12;14), del(7q), trisomy 12
�Hormones
�Estrogen (a, b), Progesterone (A, B)
�Growth factors
�TGF‐b, bFGF, EGF, PDGF, IGF, VEGF, PRL
Flake G. Environ Health Perspect 2003;111:1037‐1054
Fibroid Growth 262 fibroids in 72 women (38 black, 34 white)
Serial MRI q 6 months
Median growth rate
9% per year
range: ‐89% to +138%
7% regressed (>20% shrinkage)
Peddada S. Proc Natl Acad Sci U S A. 2008;105:19887‐92.
One Woman, Three Fibroids
Fibroid Growth (pre‐menopause) Indicates Sarcoma
MYTH
Page 9

Prevalence of LMS among women operated upon for presumed
uterine fibroids�1332 women
� myomectomy or hysterectomy
1 LMS = 0.07%
2014 re‐analysis = 0 “atypical”
Parker, Obstet Gynecol 1994;83:414‐18
Rapid Growth of FibroidsIncrease in uterine size
6 weeks in 1 year (Buttram)
�371 surgery for rapid growth
1 sarcoma = 0.27%
2014 re‐analysis = 0
Parker, Obstet Gynecol 1994;83:414‐18
“Everyone is entitled to their own opinion,
but not to their own facts.”
― Daniel Patrick MoynihanSenator, New York
Studies Analyzed by FDA
10 / 13,699 = 0.07% = 1/1,428
Non‐peer reviewed abstract, unpublished
57, bleeding, pelvic mass
1
2
3
4
5
6
7
8
9
4
0
Meta‐analysis: Pathology Reported in Detail
�Prospective: 64 studies5,223 women, 3 LMS
1 in 1,741
Pritts E et al. Gynecol Surg. 2015;12:165‐177.
Agency for Health Research and Quality (AHRQ)
�156,726 women in 160 studies
�LMS = 1/3,000
https://www.effectivehealthcare.ahrq.gov/topics/uterine‐fibroids/research‐2017
Page 10

Myomectomy Post‐FDA Communication
�1823 women before� 659 women after
64% in myomectomies (P < .001)
� Laparoscopic procedures 71%
�Abdominal myomectomy 56%
Stentz, 2016 ASRM, University of Pennsylvania
Hysterectomy, Fibroids
Pre‐FDA Post‐FDA p
Laparotomy 37% 43%
TLH, LSH 56% 50%
Minor Complications 2.7% 3.3% (1,534) .01
Major Complications 1.9% 2.4% (1,278) .02
Multinu F. JAMA Surg 2018; 153(6):e180141
ACSNSQIP, n = 25,571
ConclusionsMyomectomy is Safer than Hysterectomy
Uterus Does Not Look Like Swiss Cheese After Myomectomy
Fibroids Will Not Grow Back After Myomectomy
Hysterectomy (Ovarian Conservation) Changes Your Hormones
Myomectomy Improves Symptoms and Quality of Life
Myomectomy Has Similar Blood Loss as Hysterectomy
Fibroid Growth (pre‐menopause) Does Not Indicate Sarcoma
ConclusionsMyomectomy has many advantages over hysterectomy
Many women want organ conservation
Ob/Gyns are women’s health advocates
0 myomectomies is not acceptable training
Disservice to our Patients
RRC needs to Mandate Performance of Myomectomy (10)
or it will not happen
THANK YOU
Questions / Comments ?
References
� Rowe MK. Obstet Gynecol 1999;93:915‐21.
� Borah BJ, Am J Obstet Gynecol 2013;209:319.e1‐20.
� Groff J. J Women’s Health & Gender Based Medicine 2000
� Iverson, Obstet Gyn 1996;88:415
� Pundir J. J Obstet Gynecol 2013;33:655‐62
�West S, Parker W. Fert Stert 2006;85:36‐9
� Tsuji S, Gynecol Obstet Invest, 2006
� Sudik. Eur J Obstet Gyn Reprod Biol 1996;65:209
� Fauconnier. Hum Reprod Update 2000;6:595
�Monyonda I. Cardiovasc Intervent Radiol 2012;35:530–536
� Rodriguez V (in press)
Page 11

References
� Farquhar C, Int J Obstet Gynecol 2005;112:956‐2.
�Wang H. Eur J Obstet Gynecol Reprod Biol. 2013;171:368-71� Trabuco E. Obstet Gynecol 2016;127:819‐27
� Hillis, Obstet Gynecol 1996;87:539
� Cochrane Reviews: 2007
� Flake G. Environ Health Perspect 2003;111:1037‐1054
� Peddada S. Proc Natl Acad Sci U S A. 2008;105:19887‐92.
Page 12

Preoperative Evaluation and Optimization for MyomectomyMatthew Siedhoff, MD MSCRVice Chair for GynecologyAssociate ProfessorMinimally Invasive Gynecologic SurgeryCedars-Sinai ®UCLA David Geffen School of Medicine
2
Disclosures
Consultant: Applied Medical, Caldera Medical, CooperSurgical, Olympus
3
Objectives
• Perform proper workup for patients undergoing myomectomy
• Choose appropriate route of surgery (laparoscopy vs. laparotomy vs. hysteroscopy)
• Optimize patients in terms of hemoglobin, fibroid size
• Counsel patients on the intersection between fibroids and fertility
4
Case
• 27 yo g0 acutely worsening bulk symptoms 5 months prior to presentation
Pressure, urinary frequency, cyclic back pain, constipation
• Exam: 20 weeks size uterus filling the culdesac
• Ultrasound demonstrates large fibroid
• Heavy bleeding and dysmenorrhea controlled with COCs
h/h = 14.4 / 43.6 g/dL
• Would like to become pregnant in the next 2-3yrs
• Desires surgical management with myomectomy
5
Preop considerations
• Imaging
• Laparoscopy vs. laparotomy vs. hysteroscopy
• Optimize hemoglobin
• Decrease myoma size
• Timing
Pregnancy
Risk of expectant management
6
Preop considerations
• Imaging
Dueholm 2002, Levens 2009 , Spielmann 2006, Goto 2002, Sato 2014
Page 13

7
Preop considerations
• Imaging
MRI
Especially helpful for fibroids over 4cm
Greater inter-observer reliability than TVS, SIS, HSG, hysteroscopy
Out-performs ultrasound for number and size of fibroids
Better able to determine relationship to endometrial cavity, pedunculated, etc.
View uterus in multiple planes
Also reliably evaluates the adnexae (sometimes difficult w u/s and lg fibroids)
No good test for evaluating sarcoma, but best available
More expensive
Dueholm 2002, Levens 2009 , Spielmann 2006, Goto 2002, Sato 2014
8
Preop considerations
• Imaging
Benign leiomyoma vs leiomyosarcoma
Goto 2002, Di Cell0 2019, Sato 2014, Hinchcliff 2016
9
Preop considerations
• Imaging
Benign leiomyoma vs leiomyosarcoma
Dynamic MRI + LDH + LDH isoenzyme-3 (degenerating myomas vs. LMS)
Diffusion-weighted-imaging (DWI), apparent diffusion coefficient (ADC)
o High risk and low risk categories
LDH “risk index”
o LDH3 +24/LDH1 < 29 = benign
• 9 false positives in 2k benign fibroid surgeries; no false negatives in 43 LMS
Uterine biopsy – may miss disease or seed cells
Endometrial biopsy
o 50% sensitivity (abnl pathology), 35% (LMS specifically)
Goto 2002, Di Cell0 2019, Sato 2014, Hinchcliff 2016
Case
10
MRI: large intrauterine mass 12x12x14 arising ant myometrium, displacing endometrium anteriorly into the right, likely fibroid. Ovaries nl.
Case
11
Case
12
Page 14

13
Preop considerations
• Laparoscopy vs. laparotomy
Chittawar 2014
14
Preop considerations
• Laparoscopy vs. laparotomy
Decreased pain*
Decreased fever*
No increased risk in recurrence*
Decreased EBL
Shorter hospital stay
Lower risk VTE
Shorter convalescence
Lower risk adhesions
Similar fertility outcomes
Better cosmesis
Chittawar 2014
15
Preop considerations
• Laparoscopy vs. laparotomy
No increased risk in recurrence*
Chittawar 2014, Jin 2009, Buckley 2015, Yoo 2007, Hanafi 2005, Radosa 2014, Nezhat 1998
16
Preop considerations
• Laparoscopy vs. laparotomy
No increased risk in recurrence*
Chittawar 2014, Jin 2009, Buckley 2015, Yoo 2007, Hanafi 2005, Radosa 2014, Nezhat 1998
17
Preop considerations
• Laparoscopy vs. laparotomy
No increased risk in recurrence*
When recurrence defined by u/s: 12% (1yr), 36% (3yrs), 53% (5yrs), 84% (8yrs)
Single (11%) vs multiple (74%)
Younger age increases risk of recurrence
Not all recurrences need intervention
1/3 of those at 3yrs required re-intervention of symptoms
Chittawar 2014, Jin 2009, Buckley 2015, Yoo 2007, Hanafi 2005, Radosa 2014, Nezhat 1998
18
Preop considerations
• Pre-op considerations
Laparoscopy vs. laparotomy
Page 15

19
Preop considerations
• Pre-op considerations
Laparoscopy vs. laparotomy
20
Preop considerations
• Pre-op considerations
Laparoscopy vs. laparotomy
21
Preop considerations
• Pre-op considerations
Laparoscopy vs. laparotomy
22
Preop considerations
• Pre-op considerations
Laparoscopy vs. laparotomy
23
Preop considerations
• Pre-op considerations
Laparoscopy vs. laparotomy
24
Preop considerations
• Pre-op considerations
Laparoscopy vs. laparotomy
Page 16

25
Preop considerations
• Pre-op considerations
Laparoscopy vs. laparotomy
26
Preop considerations
• Pre-op considerations
Laparoscopy vs. laparotomy
27
Preop considerations
• Pre-op considerations
Laparoscopy vs. laparotomy
28
Preop considerations
• Pre-op considerations
Laparoscopy vs. hysteroscopy
29
Preop considerations
• Pre-op considerations
Laparoscopy vs. hysteroscopy
Munro 2011
30
Preop considerations
• Pre-op considerations
Laparoscopy vs. hysteroscopy
Page 17
31
Preop considerations
• Pre-op considerations
Laparoscopy vs. hysteroscopy
32
Preop considerations
• Pre-op considerations
Laparoscopy vs. hysteroscopy
33
Preop considerations
• Pre-op considerations
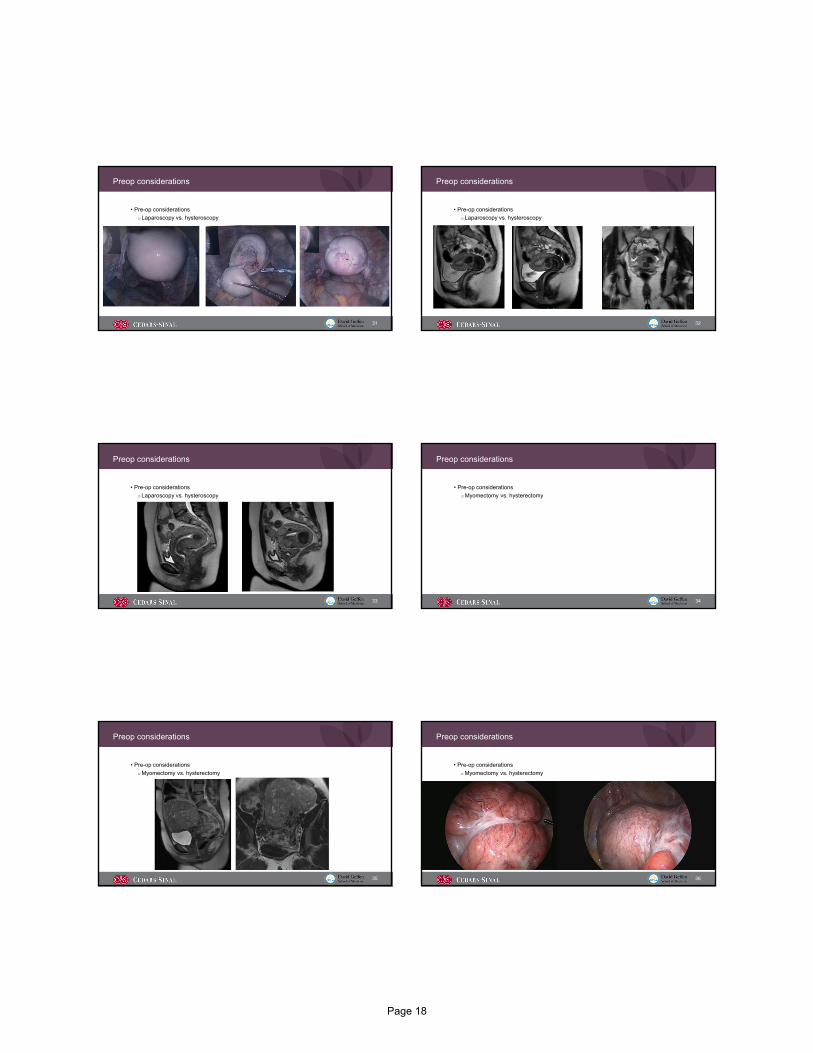
Laparoscopy vs. hysteroscopy
34
Preop considerations
• Pre-op considerations
Myomectomy vs. hysterectomy
35
Preop considerations
• Pre-op considerations
Myomectomy vs. hysterectomy
36
Preop considerations
• Pre-op considerations
Myomectomy vs. hysterectomy
Page 18

37
Preop considerations
• Optimize hemoglobin
Lethaby 2017, Peyrin‐Biroulet 2015, Stoffel 2017, Auerbach 2017
38
Preop considerations
• Optimize hemoglobin
Hormonal suppression
GnRHa, progestins, COCs, UPA
Tranexamic acid
Mean decrease EBL 200-250mL
Iron supplementation
Ferrous fumarate = ferrous gluconate = ferrous sulfate
QOD dosing, vitamin C on empty stomach
IV: non-adherent, cannot tolerate oral iron, or who have malabsorption (gastric bypass, chronic kidney disease, or IBD)
Lethaby 2017, Peyrin‐Biroulet 2015, Stoffel 2017, Auerbach 2017, Topsoee 2017, Fusca 2019
39
Preop considerations
• Decrease myoma size
Lethaby 2017, Ghiaroni 2013
40
Preop considerations
• Decrease myoma size
GnRHa vs. UPA
Greater reduction in size with GnRHa
No difference in pre-op bleeding or Hgb levels
Vasomotor symptoms, worse with GnRHa
? Oral GnRH antagonists (elagolix)
Uterine artery embolization
Clinical series but no good comparative data
Lethaby 2017, Ghiaroni 2013
41
Preop considerations
• Timing
Pregnancy
42
Preop considerations
• Timing
Pregnancy Mechanisms of pathogenesis
o Abnormal vascularizationo Abnormal endometrial developmento Chronic intracavitary inflammationo Abnormal endocrine milieuo Dysfunctional uterine contractility
Pritts 2001, Fortin 2018
Page 19

43
Preop considerations
• Timing
Pregnancy
Contribution of fibroids to infertility difficult to completely assess
o Fibroids are highly prevalent (70% of white women, over 80% black women by age 50)
o Fibroids more common w increasing age, also true of infertility
o Fibroids present in about 5-10% of women with infertility
o Fibroids sole abnormality in approximately 1-2% of infertile women
Cook 2010, Donnez 2002
44
Preop considerations
• Timing
Pregnancy
Submucosal fibroids
o Compared w infertile women w/o fibroids, those w SM fibroids have lower clinical pregnancy rates, lower implantation rates, lower continuing pregnancy/live birth rate
o Compared with placebo or no intervention, hysteroscopic myomectomy of submucosal fibroids results in improved pregnancy rates
Intramural fibroids
o Varying quality of studies regarding IM fibroids, but probable difference in clinical pregnancy, implantation, ongoing pregnancy rates
Subserosal fibroids no significant effect on any fertility outcomes
Pritts 2009
45
Preop considerations
• Timing
Pregnancy
Pritts 2009
46
Preop considerations
• Timing Pregnancy Effect of myomectomy Data are sparse Two types of controls:
o Women s/p myomectomy vs women w fibroids in situ• SM: Women s/p myomectomy have higher clinical pregnancy rates, but not
necessarily higher live birth rates• IM: no difference
o Infertile women s/p myomectomy vs infertile women without fibroids• SM: Women s/p myomectomy have similar fertility outcomes to infertile
women without fibroids• IM: no data
Pritts 2009
47
Preop considerations
• Timing
Pregnancy
Risk of recurrence and need for additional surgery
Uterine healing and risk of uterine rupture
o 3-6 months
o 6 wks: Volume, length, and myometrium stabilized
o 12 wks: EM stabilized, 86% normal healing at enucleation site
Age and ovarian reserve
Tsuji 2006, Koo 2015
48
Preop considerations
• Timing
Risk of expectant management
ASRM 2017, Benson 2001, Strobelt 1994, Klatsky 2008, Moulder 2016
Page 20

49
Preop considerations
• Timing
Risk of expectant management
Fibroids during pregnancy
o Miscarriage
o Fibroid growth
o Pain
o Degeneration
o Torsion
o PTL/PTB
o Antepartum bleeding/abruption
o Dysfunctional labor
o Malpresentation
o Cesarean delivery
o Postpartum hemorrhage
o Peripartum hysterectomy
Visceral obstruction
o Urinary retention
o Hydroureter
o GI function
VTE
ASRM 2017, Benson 2001, Strobelt 1994, Klatsky 2008, Moulder 2016
50
Preop considerations
• Timing
Risk of expectant management
Fibroids during pregnancy
o Miscarriage
o Fibroid growth
o Pain
o Degeneration
o Torsion
o PTL/PTB
o Antepartum bleeding/abruption
o Dysfunctional labor
o Malpresentation
o Cesarean delivery
o Postpartum hemorrhage
o Peripartum hysterectomy
Visceral obstruction
o Urinary retention
o Hydroureter
o GI function
VTE
ASRM 2017, Benson 2001, Strobelt 1994, Klatsky 2008, Moulder 2016
51
Preop considerations
• Asymptomatic (or tolerable) fibroids
ACOG:
“As with any woman with asymptomatic leiomyomas, those who desire future fertility should be managed expectantly because they have no indication for surgery. ”
What about fibroid noted incidentally and during surveillance noted to be growing?
ACOG 2008, reaffirmed 2016
52
Preop considerations
• Asymptomatic (or tolerable) fibroids
What about fibroid noted incidentally and during surveillance noted to be growing?
Reasonable to intervene at a time when surgery less complex?
o Growth pattern is highly variable
• Median = ~10%
• Some actually shrink in size
• 1/3 experience a “growth spurt” (>30% in 3 mos)
o Increased ability to use MIS
o Shorter duration of surgery
o Decreased blood loss/transfusion
o Especially for single myoma when recurrence risk is low
Peddada 2008, Baird 2011
53
Preop considerations
• Asymptomatic (or tolerable) fibroids
Peri-menopausal women
Large fibroids may still cause bulk symptoms
Fibroids near the endometrial cavity may cause post-menopausal bleeding
Hormone replacement replacement
o Most won’t grow, but they won’t shrink
o Progestin likely responsible for growth
Obesity may preserve fibroid size in menopause
Palomba 2001, Sommer 2015
54
Preop considerations
• Asymptomatic (or tolerable) fibroids
Peri-menopausal women
Large fibroids may still cause bulk symptoms
Fibroids near the endometrial cavity may cause post-menopausal bleeding
Hormone replacement replacement
o Most won’t grow, but they won’t shrink
o Progestin likely responsible for growth
Obesity may preserve fibroid size in menopause
Palomba 2001, Sommer 2015
Page 21

55
References
• Dueholm M, Lundorf E, Sørensen JS, Ledertoug S, Olesen F, Laursen H. Reproducibility of evaluation of the uterus by transvaginal sonography, hysterosonographic examination, hysteroscopy and magnetic resonance imaging. Hum Reprod. 2002 Jan;17(1):195-200.
• Levens ED, Wesley R, Premkumar A, Blocker W, Nieman LK. Magnetic resonance imaging and transvaginal ultrasound for determining fibroid burden: implications for research and clinical care. Am J Obstet Gynecol. 2009 May;200(5):537.e1-7.
• Spielmann AL, Keogh C, Forster BB, Martin ML, Machan LS. Comparison of MRI and sonography in the preliminary evaluation for fibroid embolization. AJR Am J Roentgenol. 2006 Dec;187(6):1499-504.
• Goto A, Takeuchi S, Sugimura K, Maruo T. Usefulness of Gd-DTPA contrast-enhanced dynamic MRI and serum determination of LDH and its isozymes in the differential diagnosis of leiomyosarcoma from degenerated leiomyoma of the uterus. Int J Gynecol Cancer. 2002 Jul-Aug;12(4):354-61.
56
References
• Di Cello A, Borelli M, Marra ML, Franzon M, D'Alessandro P, Di Carlo C, Venturella R, Zullo F. A more accurate method to interpret lactate dehydrogenase (LDH) isoenzymes' results in patients with uterine masses. Eur J Obstet Gynecol Reprod Biol. 2019 May;236:143-147.
• Sato K, Yuasa N, Fujita M, Fukushima Y. Clinical application of diffusion-weighted imaging for preoperative differentiation between uterine leiomyoma and leiomyosarcoma. Am J ObstetGynecol. 2014 Apr;210(4):368.e1-368.e8.
• Hinchcliff EM, Esselen KM, Watkins JC, Oduyebo T, Rauh-Hain JA, Del Carmen MG, Quade BJ, Muto MG. The Role of Endometrial Biopsy in the Preoperative Detection of Uterine Leiomyosarcoma. J Minim Invasive Gynecol. 2016 May-Jun;23(4):567-72.
• Bhave Chittawar P, Franik S, Pouwer AW, Farquhar C. Minimally invasive surgical techniques versus open myomectomy for uterine fibroids. Cochrane Database Syst Rev. 2014 Oct 21;(10):CD004638.
57
References
• Jin C, Hu Y, Chen XC, Zheng FY, Lin F, Zhou K, Chen FD, Gu HZ. Laparoscopic versus open myomectomy--a meta-analysis of randomized controlled trials. Eur JObstet Gynecol ReprodBiol. 2009 Jul;145(1):14-21.
• Buckley VA, Nesbitt-Hawes EM, Atkinson P, Won HR, Deans R, Burton A, Lyons SD, Abbott JA. Laparoscopic myomectomy: clinical outcomes and comparative evidence. J Minim Invasive Gynecol. 2015 Jan;22(1):11-25.
• Yoo EH, Lee PI, Huh CY, Kim DH, Lee BS, Lee JK, Kim D. Predictors of leiomyoma recurrence after laparoscopic myomectomy. J Minim Invasive Gynecol. 2007 Nov-Dec;14(6):690-7.
• Hanafi M. Predictors of leiomyoma recurrence after myomectomy. Obstet Gynecol. 2005 Apr;105(4):877-81.
58
References
• Radosa MP, Owsianowski Z, Mothes A, Weisheit A, Vorwergk J, Asskaryar FA, Camara O, Bernardi TS, Runnebaum IB. Long-term risk of fibroid recurrence after laparoscopic myomectomy. Eur J Obstet Gynecol Reprod Biol. 2014 Sep;180:35-9.
• Nezhat FR, Roemisch M, Nezhat CH, Seidman DS, Nezhat CR. Recurrence rate after laparoscopic myomectomy. J Am Assoc Gynecol Laparosc. 1998 Aug;5(3):237-40.
• Munro MG, Critchley HO, Fraser IS; FIGO Menstrual Disorders Working Group. The FIGO classification of causes of abnormal uterine bleeding in the reproductive years. FertilSteril. 2011 Jun;95(7):2204-8, 2208.e1-3.
• Lethaby A, Puscasiu L, Vollenhoven B. Preoperative medical therapy before surgery for uterine fibroids. Cochrane Database Syst Rev. 2017 Nov 15;11:CD000547.
• Peyrin-Biroulet L, Williet N, Cacoub P. Guidelines on the diagnosis and treatment of iron deficiency across indications: a systematic review. Am J Clin Nutr. 2015 Dec;102(6):1585-94.
59
References
• Stoffel NU, Cercamondi CI, Brittenham G, Zeder C, Geurts-Moespot AJ, Swinkels DW, Moretti D, Zimmermann MB. Iron absorption from oral iron supplements given on consecutive versus alternate days and as single morning doses versus twice-daily split dosing in iron-depleted women: two open-label, randomised controlled trials. Lancet Haematol. 2017 Nov;4(11):e524-e533.
• Auerbach M, Schrier S. Treatment of iron deficiency is getting trendy. Lancet Haematol. 2017 Nov;4(11):e500-e501.
• Topsoee MF, Settnes A, Ottesen B, Bergholt T. A systematic review and meta-analysis of the effect of prophylactic tranexamic acid treatment in major benign uterine surgery. Int J GynaecolObstet. 2017 Feb;136(2):120-127.
• Fusca L, Perelman I, Fergusson D, Boutet M, Chen I. The Effectiveness of Tranexamic Acid at Reducing Blood Loss and Transfusion Requirement for Women Undergoing Myomectomy: A Systematic Review and Meta-analysis. J Obstet Gynaecol Can. 2019 Aug;41(8):1185-1192.e1.
60
References
• Pritts EA. Fibroids and infertility: a systematic review of the evidence. Obstet Gynecol Surv. 2001 Aug;56(8):483-91.
• Fortin C, Flyckt R, Falcone T. Alternatives to hysterectomy: The burden of fibroids and the quality of life. Best Pract Res Clin Obstet Gynaecol. 2018 Jan;46:31-42.
• Cook H, Ezzati M, Segars JH, McCarthy K. The impact of uterine leiomyomas on reproductive outcomes. Minerva Ginecol. 2010 Jun; 62(3):225-36.
• Donnez J, Jadoul P. What are the implications of myomas on fertility? A need for a debate? Hum Reprod. 2002 Jun; 17(6):1424-30.
• Pritts EA, Parker WH, Olive DL. Fibroids and infertility: an updated systematic review of the evidence. Fertil Steril. 2009 Apr;91(4):1215-23.
Page 22

61
References
• Ghiaroni J, Lopez GE, Coutinho Junior AC, Schanaider A. Uterine artery embolization with spherical PVA-PVAc particles as preparation for surgical resection of myomas. Rev Col Bras Cir. 2013 Sep-Oct;40(5):386-91.
• Tsuji S, Takahashi K, Imaoka I, Sugimura K, Miyazaki K, Noda Y. MRI evaluation of the uterine structure after myomectomy. Gynecol Obstet Invest. 2006;61(2):106-10.
• Koo YJ, Lee JK, Lee YK, Kwak DW, Lee IH, Lim KT, Lee KH, Kim TJ. Pregnancy Outcomes and Risk Factors for Uterine Rupture After Laparoscopic Myomectomy: A Single-Center Experience and Literature Review. J Minim Invasive Gynecol. 2015 Sep-Oct;22(6):1022-8.
• Practice Committee of the American Society for Reproductive Medicine. Removal of myomas in asymptomatic patients to improve fertility and/or reduce miscarriage rate: a guideline. FertilSteril. 2017 Sep;108(3):416-425.
62
References
• Benson CB, Chow JS, Chang-Lee W, Hill JA 3rd, Doubilet PM. Outcome of pregnancies in women with uterine leiomyomas identified by sonography in the first trimester. J Clin Ultrasound. 2001 Jun;29(5):261-4.
• Strobelt N, Ghidini A, Cavallone M, Pensabene I, Ceruti P, Vergani P. Natural history of uterine leiomyomas in pregnancy. J Ultrasound Med. 1994 May;13(5):399-401.
• Klatsky PC, Tran ND, Caughey AB, Fujimoto VY. Fibroids and reproductive outcomes: a systematic literature review from conception to delivery. Am J Obstet Gynecol. 2008 Apr;198(4):357-66.
• Moulder JK, Siedhoff MT, Till SR, Moll S. Management considerations for patients with uterine fibroids and concurrent venous thromboembolism. Curr Opin Obstet Gynecol. 2016 Aug;28(4):329-35.
63
References
• ACOG practice bulletin. Alternatives to hysterectomy in the management of leiomyomas. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2008 Aug;112(2 Pt 1):387-400.
• Peddada SD, Laughlin SK, Miner K, Guyon JP, Haneke K, Vahdat HL, Semelka RC, Kowalik A, ArmaoD, Davis B, Baird DD. Growth of uterine leiomyomata among premenopausal black and white women. Proc Natl Acad Sci U S A. 2008 Dec 16;105(50):19887-92.
• Baird DD, Garrett TA, Laughlin SK, Davis B, Semelka RC, Peddada SD. Short-term change in growth of uterine leiomyoma: tumor growth spurts. Fertil Steril. 2011 Jan;95(1):242-6.
• Palomba S, Sena T, Noia R, Di Carlo C, Zullo F, Mastrantonio P. Transdermal hormone replacement therapy in postmenopausal women with uterine leiomyomas. Obstet Gynecol. 2001 Dec;98(6):1053-8.
• Sommer EM, Balkwill A, Reeves G, Green J, Beral DV, Coffey K; Million Women Study Collaborators. Effects of obesity and hormone therapy on surgically-confirmed fibroids in postmenopausal women. Eur J Epidemiol. 2015 Jun;30(6):493-9.
Page 23

Hysteroscopic myomectomyKelly Wright, MDProgram Director, Center for Minimally Invasive Gynecologic SurgeryAssistant ProfessorCedars-Sinai Medical CenterUCLA David Geffen School of Medicine
2
Disclosures
• Consultant: Acessa, Applied Medical, Boston Scientific Corp. Inc., Hologic, Karl Storz
3
Objectives
• Discuss the difficulties inherent in hysteroscopic myomectomy
• Choose appropriate tool for surgery (resectoscope vs. morcellator)
• Optimize surgical technique for completion
The problem with fibroids
Classification of fibroids The problem with fibroids
Page 24

The problem with fibroids The problem with fibroids
Hysteroscopic resection – monopolar vs. bipolar Hysteroscopic resection – monopolar vs. bipolar
Hysteroscopic resection – monopolar vs. bipolar Hysteroscopic resection – monopolar vs. bipolar
Page 25

Morcellation• Removes tissue pieces
• Shorter procedures
• Easy to use
• No coagulation
• Incomplete removal
• 0 degree lens
• High volume fluid usage
Resection• Coagulation
• Remove deep tissue fragments
• More versatile
• Pieces get in the way
• Need energy source
• Longer procedures
• Decreasing surgeon skill
Morcellation vs Resection
14
Morcellation vs Resection
Shazly SA, et al. J Minim Invasive Gynecol. 2016 Sep‐Oct;23(6)867‐77.
15
Preop preparation
16
Preop preparation
• Injection of vasopressin
RCT showed intracervical injection of dilute vasopressin had:
Lower EBL
Lower fluid deficit
Shorter operative time
RCT showed injection of vasopressin directly into fibroid:
Lower EBL
Lower fluid deficit
Improved visibility
20U vasopressin mixed in 100mL normal saline
Inject 40mL intracervically
Inject 10mL intrauterine (fundal/fibroid)
Phillips DR, et al. Obstet Gynecol. 1996;88(5):761‐6Wong AS, et al. Obstet Gynecol. 2014;124(5):897‐903
17
Preop preparation
• Have all equipment available
• Typically for type 0 or large intracavitary type 1, I will start with hysteroscopic morcellator
• Typically for deep type 1 or 2, I will start with bipolar resectoscope
• For a large fibroid (greater than 2-3cm), have both available in the largest sizes Resectoscopes often come in 22-26Fr Hysteroscopic morcellators often come in 18-24Fr
• For a failed prior myomectomy, I will use bipolar resectoscope, but have both available
18
Special considerations
• Lower uterine segment and cervical fibroids
• Calcified fibroids
Page 26

19
Video techniques
Type 2 posterior fibroid: Difficult to see upon entry with high pressure, easier to see when pressure lowered
20
Video techniques
Type 2 anterior fibroid: Tip of the iceberg – appears small at first, but when you “unroof” endometrium, it extends all the way into the lateral wall
Overlying myometrium
Fibroid
21
Video techniques
Using the resectoscope: Place into the plane between fibroid and myometrium and pull forward (toward you) prior to activating(loop will move and lift the fibroid tissue away from underlying myometrium)
22
Video techniques
Using the morcellator: Place into the plane between fibroid and myometrium and typically use lateral force to push into the fibroid
Overlying myometrium
Fibroid
Thank you!
23
Page 27
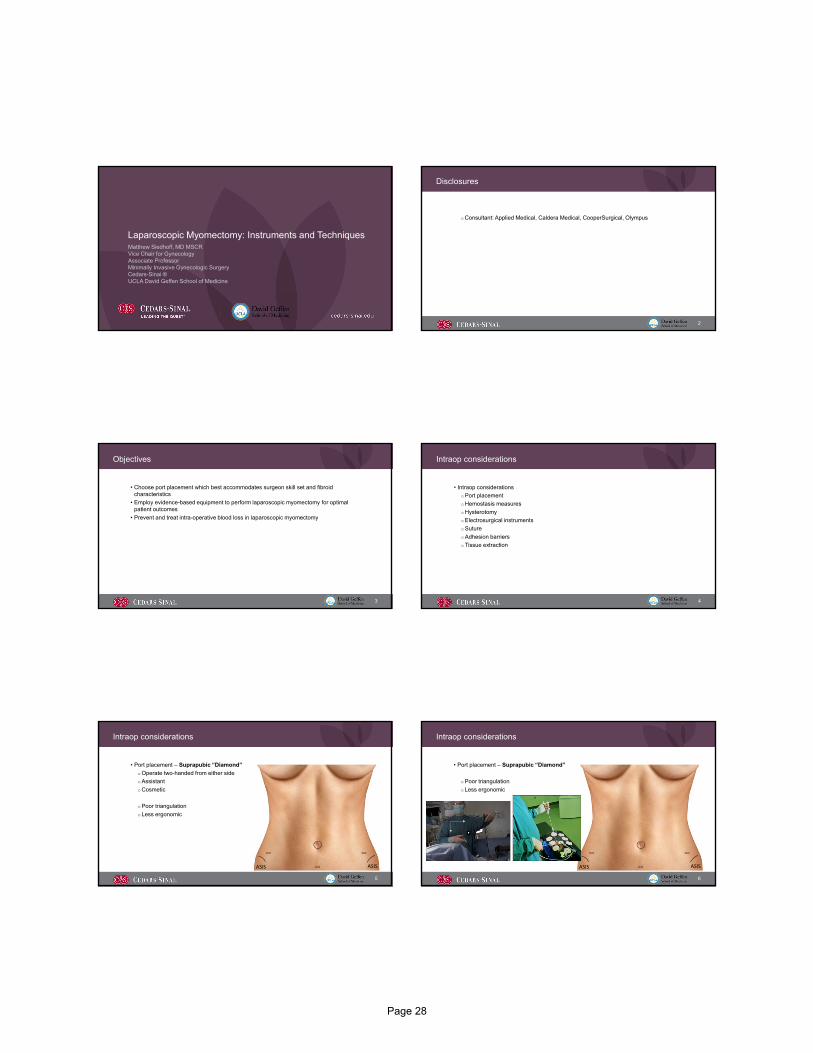
Laparoscopic Myomectomy: Instruments and TechniquesMatthew Siedhoff, MD MSCRVice Chair for GynecologyAssociate ProfessorMinimally Invasive Gynecologic SurgeryCedars-Sinai ®UCLA David Geffen School of Medicine
2
Disclosures
Consultant: Applied Medical, Caldera Medical, CooperSurgical, Olympus
3
Objectives
• Choose port placement which best accommodates surgeon skill set and fibroid characteristics
• Employ evidence-based equipment to perform laparoscopic myomectomy for optimal patient outcomes
• Prevent and treat intra-operative blood loss in laparoscopic myomectomy
4
Intraop considerations
• Intraop considerations
Port placement
Hemostasis measures
Hysterotomy
Electrosurgical instruments
Suture
Adhesion barriers
Tissue extraction
Intraop considerations
• Port placement – Suprapubic “Diamond”
Operate two-handed from either side
Assistant
Cosmetic
Poor triangulation
Less ergonomic
ASIS ASIS
5
Intraop considerations
• Port placement – Suprapubic “Diamond”
Poor triangulation
Less ergonomic
ASIS ASIS
6
Page 28

7
Intraop considerations
• Port placement – Ipsilateral
Improved triangulation
Better ergnomics
Less cosmetic
ASIS ASIS
8
Intraop considerations
• Port placement – Ipsilateral
Improved triangulation
Better ergnomics
Less cosmetic
ASIS ASIS
9
Intraop considerations
• Port placement – Ipsilateral
Improved triangulation
Better ergnomics
Less cosmetic
ASIS ASIS
10
Intraop considerations
• Port placement – Ipsilateral
Improved triangulation
Better ergnomics
Less cosmetic
ASIS ASIS
11
Intraop considerations
• Port placement – Ipsilateral
Improved triangulation
Better ergnomics
Less cosmetic
ASIS ASIS
12
Intraop considerations
• Port placement – Ipsilateral
Improved triangulation
Better ergnomics
Less cosmetic
ASIS ASIS
Page 29

13
Intraop considerations
• Port placement – Ipsilateral
Improved triangulation
Better ergnomics
Less cosmetic
14
Intraop considerations
• Port placement – Ipsilateral
Improved triangulation
Better ergnomics
Less cosmetic
ASIS ASIS
15
Intraop considerations
• Port placement –Supraumbilical
ASIS ASIS
16
Intraop considerations
• Methods to decrease blood loss
Medical interventions
Surgical intervention
Hickman 2016
17
Intraop considerations
Hickman 2016, Topsoee 2017, Fusca 2019
18
Intraop considerations
Hickman 2016
Page 30

19
Intraop considerations
• Methods to decrease blood loss Uterotonics Misoprostol Oxytocin
Chemical hemostasis (preoperative treatment) GnRH agonists Ulipristal
Chemical hemostasis (intraoperative) Bupivacaine / epinephrine Vasopressin Tranexamic acid Mesna
Tourniquet, temporary vascular clamps Uterine artery emoblization / LSC ligation
Kongnyuy 2014
20
Intraop considerations
• Methods to decrease blood loss Uterotonics Misoprostol Oxytocin
Chemical hemostasis (preoperative treatment) GnRH agonists Ulipristal
Chemical hemostasis (intraoperative) Bupivacaine / epinephrine Vasopressin Tranexamic acid Mesna
Tourniquet, temporary vascular clamps Uterine artery emoblization / LSC ligation
Kongnyuy 2014
21
Intraop considerations
• Uterine incision/hysterotomy
22
Intraop considerations
• Uterine incision/hysterotomy
Arguments made for better hemostasis w/ vertical, transverse incisions
Transverse generally easier to close
Use pre-op imaging to help guide decision
23
• Electrosurgical instruments
Intraop considerations
24
• Electrosurgical instruments
• Monopolar
Inexpensive
Intraop considerations
• Ultrasonic
Less plume
Less tissue damage to myometrium
Greater hemostasis
Page 31

25
Intraop considerations
• Hysterotomy closure
Giampaolino 2015, Tinelli 2016, Alessandri 2010
26
Intraop considerations
• Hysterotomy closure
Conventional suturing
Intracorporeal knots
Extracorporeal knots
Absorbable suture clips
Barbed suture
Giampaolino 2015, Tinelli 2016, Alessandri 2010
27
Intraop considerations
• Hysterotomy closure
Conventional suturing
Intracorporeal knots
Extracorporeal knots
Absorbable suture clips
Barbed suture
Decreased OR time
Decreased EBL
Giampaolino 2015, Tinelli 2016, Alessandri 2010
28
Intraop considersations
• Adhesion barriers
Tulandi 2016
29
Intraop considersations
• Adhesion barriers
Tulandi 2016
30
Intraop considersations
• Adhesion barriers
No proven clinical benefit in laparoscopic myomectomy• Complications during subsequent surgery• Fertility outcomes• Bowel obstruction
Fever and ileusTulandi 2016
Page 32

31
Preop & Intraop considerations
• Preop considerations
Keep in mind data and recommendations based on RCTs
Not everyone candidate for LM vs. AM
Findings for interventions may not apply to the unusual cases
o Individualize care
o Patient goals
o “Art” of medicine / surgery
Case
32
33
References
• Hickman LC, Kotlyar A, Shue S, Falcone T. Hemostatic Techniques for Myomectomy: An Evidence-Based Approach. J Minim Invasive Gynecol. 2016 May-Jun;23(4):497-504.
• Topsoee MF, Settnes A, Ottesen B, Bergholt T. A systematic review and meta-analysis of the effect of prophylactic tranexamic acid treatment in major benign uterine surgery. Int J Gynaecol Obstet. 2017 Feb;136(2):120-127.
• Fusca L, Perelman I, Fergusson D, Boutet M, Chen I. The Effectiveness of Tranexamic Acid at Reducing Blood Loss and Transfusion Requirement for Women Undergoing Myomectomy: A Systematic Review and Meta-analysis. J Obstet Gynaecol Can. 2019 Aug;41(8):1185-1192.e1.
• Kongnyuy EJ, Wiysonge CS. Interventions to reduce haemorrhage during myomectomy for fibroids. Cochrane Database Syst Rev. 2014 Aug 15;(8):CD005355.
34
References
• Giampaolino P, De Rosa N, Tommaselli GA, Santangelo F, Nappi C, Sansone A, Bifulco G. Comparison of bidirectional barbed suture Stratafix and conventional suture with intracorporeal knots in laparoscopic myomectomy by office transvaginal hydrolaparoscopic follow-up: a preliminary report. Eur J Obstet GynecolReprod Biol. 2015
• Tinelli R, Litta P, Angioni S, Bettocchi S, Fusco A, Leo L, Landi S, Cicinelli E. A multicenter study comparing surgical outcomes and ultrasonographic evaluation of scarring after laparoscopic myomectomy with conventional versus barbed sutures. Int J Gynaecol Obstet. 2016 Jul;134(1):18-21.
• Alessandri F, Remorgida V, Venturini PL, Ferrero S. Unidirectional barbed suture versus continuous suture with intracorporeal knots in laparoscopic myomectomy: a randomized study. J Minim Invasive Gynecol. 2010 Nov-Dec;17(6):725-9.
• Tulandi T, Closon F, Czuzoj-Shulman N, Abenhaim H. Adhesion Barrier Use After Myomectomy and Hysterectomy: Rates and Immediate Postoperative Complications. Obstet Gynecol. 2016 Jan;127(1):23-8.
Page 33

Robotic-Assisted Myomectomy: Instruments and TechniquesMireille Truong, MDCo-director, Women’s Guild Simulation Center for Advanced Clinical SkillsAssistant ProfessorMinimally Invasive Gynecologic SurgeryCedars-Sinai Medical Center
2
Disclosures
I have no financial relationships to disclose
JMIG Editorial Board‐ Social Media Editor
3
Objectives
By the end of this presentation, participants will be able to:
•Deconstruct robotic myomectomy into systematic steps
•Apply evidence-based practices to optimize robotic myomectomy
4
Deconstructing robotic myomectomy
•Procedure preparation & set-up
Patient positioning
Intra-abdominal entry & Trocar Placement
Intra-operative setup
•Procedural steps
Hemostasis strategy
Hysterotomy
Dissection & Enucleation
Hysterotomy Closure
Tissue extraction
5
Setup: Patient Positioning
Hip abduction<900
Jackson, T. et al. 20146
Setup: Patient Positioning
Knee Flexion 90‐1200
Hip flexion90‐1200
Hip abduction<900
Align knee tocontralateral shoulder
Arms tuckedw/ elbow, wrists, hand protected
Jackson, T. et al. 2014
Page 34

7
Setup: Uterine manipulation & positioning system
8
Setup: Port placement
Assistant port
Robotic ports Camera
9
Setup: Port placement
10
Setup: Port placement
11
Setup: Port placement
12
Setup: Insufflation
Madueke‐ Laveaux et al. 2019
Better visualization with valveless insufflation (vs standard)
Page 35

13
Setup: Instrumentation
•Vasopressin (20units in 50-200cc saline)
•Spinal need 22 gauge, 7 inch •AirSeal insufflation system•Xi: Arm 1 (L or R)- TenaculumArm 2 (L)- Maryland/Fenestrated bipolar Arm 3- Camera (300 vs 00)Arm 4 (R) – Monopolar Scissors
Monopolarscissors
Tenaculum
Bipolar
INSTRUMENTATION
14
Trendelenberg
No need for steep trendelenberg
Mean T‐berg degree: 16o
15
Keys steps
1. Hemostasis strategy
2. Hysterotomy
3. Dissection and Enucleation
4. Hysterotomy closure
5. Tissue extraction
16
Step 1: Injection of vasopressin
17
Step 2: Hysterotomy
Key points:• Tranverse if possible
(vs vertical)• Identify& Avoid cornua• Move quickly down to
level of pseudocapsuleplane
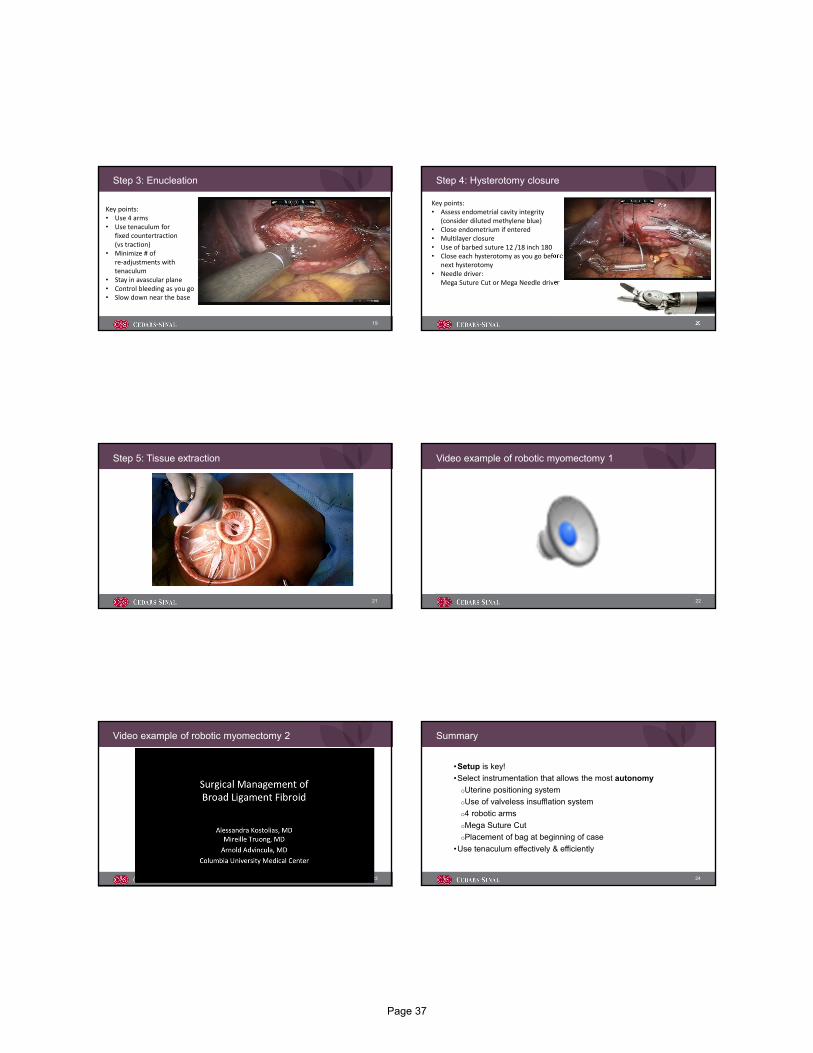
18
Step 3: Enucleation
Key points:• Use 4 arms• Use tenaculum for
fixed countertraction(vs traction)
• Minimize # of re‐adjustments with tenaculum
• Stay in avascular plane• Control bleeding as you go• Slow down near the base
Page 36
19
Step 3: Enucleation
Key points:• Use 4 arms• Use tenaculum for
fixed countertraction(vs traction)
• Minimize # of re‐adjustments with tenaculum
• Stay in avascular plane• Control bleeding as you go• Slow down near the base
20
Step 4: Hysterotomy closure
Key points:• Assess endometrial cavity integrity
(consider diluted methylene blue)• Close endometrium if entered• Multilayer closure • Use of barbed suture 12 /18 inch 180• Close each hysterotomy as you go before starting
next hysterotomy• Needle driver:
Mega Suture Cut or Mega Needle driver
21
Step 5: Tissue extraction Video example of robotic myomectomy 1
22
23
Video example of robotic myomectomy 2
24
Summary
•Setup is key!
•Select instrumentation that allows the most autonomy
Uterine positioning system
Use of valveless insufflation system
4 robotic arms
Mega Suture Cut
Placement of bag at beginning of case
•Use tenaculum effectively & efficiently
Page 37


Tissue ExtractionMireille Truong, MDCo-director, Women’s Guild Simulation Center for Advanced Clinical SkillsAssistant ProfessorMinimally Invasive Gynecologic SurgeryCedars-Sinai Medical Center
2
Disclosures
I have no financial relationships to disclose
JMIG Editorial Board‐ Social Media Editor
3
Objectives
By the end of this presentation, participants will be able to:
•Discuss current recommendations for tissue extraction
•Describe techniques for tissue extraction
•Develop strategies for safe and efficient tissue extraction
6
3 Steps for tissue extraction
1. Retrieval
a. Abdominal vs vaginal
b. Contained vs non-contained
2. Exposure
3. Extraction
a. Power morcellation
b. Manual morcellation
(i.e. ExCITE)
RETRIEVAL EXPOSURE
EXTRACTION
Page 39

STEP 1: SPECIMEN RETRIEVAL
FDA approved tissue extraction system
Salvay 2015
tenaculum
camera
Abdominal Specimen retrieval (Endocatch)
Bag
Vaginal Specimen retrieval (Endocatch)
Kliethermes 2016
Page 40

Specimen retrieval with ACES bag (part 1)
Truong 2018 Anterior and posterior edges of
bag pinched together with “suture loop”
Abdominal wall opening
Prep bag for insertion
Vaginal Specimen retrieval (ACES)
STEP 2: EXPOSURE
Abdominal
Abdominal Vaginal
Page 41

TOWEL CLAMPS LAHEY TENACULUM SCHROEDER
STEP 3: EXTRACTION
Power vs Manual Morcellation
22
Cholkeri‐Singh et al., 2015
Schibley, 2014
Manual Extraction- ExCITE techniqueExCITE technique
Simulation model with Tips & tricks
Truong M, Advincula A. ExCITE: Minimally invasive tissue extraction made simple with simulation. OBG Manag. 2015;27(11)40‐45.
Page 42

Simulation model
Beef tongueSilicone ringsPantyhosePlastic bagScalpelTissue grasperBox (cardboard or plastic)
< $10/use
ExCITE techniqueExtracorporeal C-Incision Tissue Extraction
INTRAOP SIM MODEL
Contained vaginal morcellation
Favero et al., 2012 Courtesy of M. TruongKho 2015
Start with cervix at opening
Non-contained vaginal morcellation
Maintain orientation with cervical clamps bilaterally
Stay within the serosa
Contained power morcellation
Page 43

32
3 Steps for tissue extraction
1. Retrieval
a. Abdominal vs vaginal
b. Contained vs non-contained
2. Exposure
3. Extraction
a. Power morcellation
b. Manual morcellation
(i.e. ExCITE)
RETRIEVAL EXPOSURE
EXTRACTION
Questions? Comments?
@MIS_MDT
@drMtruong
Thank you!
35
Video references
Page 44

References• AAGL Advancing Minimally Invasive Gynecology Worldwide. AAGL practice report: Morcellation during uterine tissue
extraction. J Minim Invasive Gynecol. 2014 Jul‐Aug;21(4):517‐30. • Barron KI, Richard T, Robinson PS, Lamvu G. Association of the U.S. Food and Drug Administration Morcellation Warning With Rates of
Minimally Invasive Hysterectomy and Myomectomy. Obstet Gynecol. 2015 Dec;126(6):1174‐80. • Cholkeri‐Singh A, Miller CE. Power morcellation in a specimen bag. J Minim Invasive Gynecol. 2015 Feb;22(2):160. • Cohen SL, Einarsson JI, Wang KC, Brown D, Boruta D, Scheib SA, Fader AN, Shibley T. Contained power morcellation within an insufflated
isolation bag. Obstet Gynecol. 2014 Sep;124(3):491‐7.• Favero G, Anton C, Silva e Silva A, et al. Vaginal morcellation: A new strategy for large gynecological malignant tumor extraction: a pilot
study. Gynecol Oncol. 2012;126(3):443–447.• Ikhena DE, Paintal A, Milad MP. Feasibility of Washings at The Time of Laparoscopic Power Morcellation: A Pilot Study. J Minim Invasive
Gynecol. 2016 Apr 8. • McKenna JB, Kanade T, Choi S, Tsai BP, Rosen DM, Cario GM, Chou D. The Sydney Contained In Bag Morcellation technique. J Minim
Invasive Gynecol. 2014 Nov‐Dec;21(6):984‐5. doi: 10.1016/j.jmig.2014.07.007. Epub 2014 Jul 15
• Milad MP, Milad EA. Laparoscopic morcellator‐related complications. J Minim Invasive Gynecol. 2014 May‐Jun;21(3):486‐91. doi: 10.1016/j.jmig.2013.12.003. Epub 2013 Dec 10. Review.
• Serur E, Lakhi N. Laparoscopic hysterectomy with manual morcellation of the uterus: An original technique that permits the safe and quick removal of a large uterus. Am J Obstet Gynecol. 2011;204(6):556.e1–e2.
• Shibley KA, Enclosed morcellation using a large bowel isolation bag. OBG Manag. 2014 Nov.• Truong MD, Advincula AP. The Extracorporeal C‐Incision Tissue Extraction (ExCITE) technique. OBG Manag. 2014;26(11):56.• Vargas MV, Cohen SL, Fuchs‐Weizman N, Wang KC, Manoucheri E, Vitonis AF, Einarsson JI. Open power morcellation versus contained
power morcellation within an insufflated isolation bag: comparison of perioperative outcomes. J Minim Invasive Gynecol. 2015 Mar‐
Apr;22(3):433‐8.
Morcellation statements (references)
• SGO: https://www.sgo.org/newsroom/position-statements-2/morcellation/
• ACOG: https://www.acog.org/Clinical-Guidance-and-Publications/Task-Force-and-Work-Group-Reports/Power-Morcellation-and-Occult-Malignancy-in-Gynecologic-Surgery
• AAGL: https://www.aagl.org/wp-content/uploads/2014/05/Tissue_Extraction_TFR.pdf
• AUGS: https://www.augs.org/assets/1/6/AUGS_position_statement_morcellation_FINAL-1.pdf
Page 45

William H. Parker, MD
Clinical Professor
UC San Diego School of Medicine
Disclosures
�Consultant: Abbvie
Objectives
� Discuss the minimally‐invasive alternative to laparoscopic hysterectomy, instruments and techniques for the abdominal myomectomy
Pre‐op MRI
Page 46

Start skin incision higher – 3‐4 cm above symphysis (wider area)
Curve FASCIAL incision up at lateral borders
Incise linea alba up to umbilicus
Free rectus lateral attachments to fascia to gain mobility – more room
If needed, cut fascia vertically underneath umbilicus to allow it to separate
Towel clips to elevate leading fibroid
Place tourniquet first, if possible, to decrease bleeding from towel clips
Extending the Pfannensteil Incision
Start incision higher – 3‐4 cm above symphysis (wider area)
Extending the Pfannensteil Incision Extending the Pfannensteil Incision
Cut Fascia Up, Not Out, At Lateral Borders Detach Linea Alba Up To Umbilicus
Page 47

Notes
�Explore abdomen for adhesions due to fibroid degeneration
�Try to deliver most cephalad fibroid first, grasp with towel clip if needed
� If lower uterine segment is narrow, place tourniquet with uterus in‐situ
�Or, deliver uterus and then place tourniquet under ovaries and tubes
Deliver Fibroid Uterus
Apply Tourniquet Under Ovaries and Tubes Inject Vasopressin (20 U/100 ml) Under Pseudo‐capsule
Reducing Blood Loss
�? Vertical v Horizontal incisions
�Stay inside pseudo‐capsule
�Avoid tunneling uterine incisions
�Tight closure of uterine incisions and dead space for hemostasis
Stanley West, MD, New York Discepola F, Obstet Gynecol 2007;110:1301.
Reducing Blood LossVertical v Horizontal Incisions
Page 48

Avoid Tunneling IncisionsClose dead spaceHemostasis – best adhesion prevention
Video – Fibroid Removal
� Incise myometrium deep into fibroid
�Below pseudo‐capsule
�Wiping technique
�Dry lap pad
�Stay below vascular layer
�Cut thick adherent bands with Bovie
Stanley West, MD, New York
PseudocapsuleIncise and Wipe Under Pseudo‐capsule
Running Suture, Baseball Suture Suture, Seprafilm
�Myometrium
� Close dead space to prevent hematomas
� Tight running 0‐vicryl
� Cinch down
� Serosa
�O‐Monocryl baseball
� Bipolar oozing areas
� Apply Seprafilm
� Bend back paper and stick Seprafilm to suture line
� Pull away paper and use Asepto with saline to apply Seprafilm (doesn’t stick)
Page 49

Seprafilm Application
Pain Management
ON‐Q PUMP
ON‐Q Pain Pump
�Close peritoneum to prevent Bupivicaine tracking into peritoneal cavity
�Close 1/3 of fascia
�Elevate fascia on opposite side
�Place introducer needle through skin and fascia
�Remove needle and slide catheter in to thickest dark line
�Steri‐strip catheter to skin to stabilize catheter
�Close fascia and avoid suturing catheter in !!
�Place 2nd catheter through skin into sub‐q and close sub‐q
�Close skin – 2‐0 nylon and remove in 5‐7 days
Insert ON‐Q Catheters
34 y/o G 0 woman
5 gyns ‐hysterectomy only
option
Stopped seeing gynecologists
Minimally Invasive
Page 50

Minimally Invasive Open Myomectomy
Enhanced Recovery After Surgery
Why Don’t Gynecologists Perform More Myomectomies
Myths and Dogma
Never Taught
1) Skin – 2‐4 cm above pubis for large uterus
2) Fascia ‐wide and up at borders
3) Linea alba – incise to umbilicus
4) Explore for adhesions – degeneration related
5) Deliver uterus – apply towel clips if needed
6) Tourniquet‐ under ovaries and tubes
7) Inject vasopressin – under pseudocapsule
8) Incision ‐ fast and deep into fibroid
9) Towel clips for traction
10) Dry lap to tease away pseudo‐capsule
11) Bipolar large vessels
12) Suture ‐ layers
13) Baseball stitch for serosa
14) Release tourniquet
15) Wait for bleeding
16) Figure of 8s, bipolar for hemostasis
17) Seprafilm application
18) Suture rectus to reduce diastasis
19) ON‐Q placement – pain pump
20) Subcuticular closure
Open Myomectomy: Procedure Steps
Page 51

THANK YOU
QUESTIONS?
Page 52

Postop ManagementKelly Wright, MDProgram Director, Center for Minimally Invasive Gynecologic SurgeryAssistant ProfessorCedars-Sinai Medical CenterUCLA David Geffen School of Medicine
2
Disclosures
• Consultant: Acessa, Applied Medical, Boston Scientific Corp. Inc., Hologic, Karl Storz
3
Objectives
• Review evidence for ERAS principles and minimization of intervention
• Discuss best practices for postop management
• Summarize postop considerations and future follow up for myomectomy patients
4
ERAS
Evidence-based approach to perioperative care shown to hasten recovery and attenuate the stress response to
surgery
5
ERAS
ERAS
Minimize and optimize interventions in outpatients
Decrease morbidity and LOS in inpatients
6
ERAS
Page 53

What’s the evidence?
- Decreased post op complications
- Superior pain control
- Shorter recovery time
Tell them they’re going home
Halaszynski TM, Juda R, Silverman DG. Optimizing postoperative outcomes with efficient preoperative assessment and management. Crit Care Med 2004; 32:S76–86. Short convalescence after inguinal herniorrhaphy with standardised recommendations: Duration and reasons for delayed return to work. Eur J Surg 1999;165:236–41.
Pre-operative counseling
Pre-operative counseling
• 13 people who were extremely allergic to poison ivy
• Each was rubbed on one arm with poison ivy and told it was harmless
• Each was rubbed on the other arm with a harmless leaf and told it was poison ivy
• All reacted to the harmless leaf
• Only 2 reacted to the real poison ivy
Clark NV, Gujral H, Wright KN. Impact of a Minimally Invasive Gynecologic Surgeon on Patient Outcomes. JSLS. 2017 Jul‐Sep;21(3).
What’s the evidence?
- Gabapentin
- PO or IV paracetamol
- Celebrex
Pre-op analgesia
Associated with decreased use of
opioids postoperatively
Ajori L, Nazari L, Mazloomfard MM, et al. Effects of gabapentin on postoperative pain, nausea and vomiting after abdominal hysterectomy: a double blind randomized clinical trial. Arch Gynecol Obstet 2012;285:677–82.
What’s the evidence?
• Female gender, gynecologic surgery, MIS
• 30-80%
• Contributes to longer LOS and decreased patient satisfaction
Apfel CC, Korttila K, Abdalla M, et al. A factorial trial of six interventions for the prevention of postoperative nausea and vomiting. N Engl J Med 2004;350: 2441–51.
Prevent post-op Nausea and Vomiting
Page 54

What’s the evidence?
• Use short-acting gas or continuous propofol
• Pre and Intraop Antiemetics
Transdermal scopolamine patch
Decadron 4mg IV
Zofran 4-8mg IV
Haldol 1-2mg IV
Apfel CC, Korttila K, Abdalla M, et al. A factorial trial of six interventions for the prevention of postoperative nausea and vomiting. N Engl J Med 2004;350: 2441–51.
What’s the evidence?
• Cochrane Review of 33 RCTs - No NGT use was associated with earlier return of bowel function (P<.001), decrease in pulmonary complications (P < .01), trend toward shorter LOS
• Data do not support the routine use of prophylactic drainage following
Avoid NGT and limit drains
What’s the evidence?
Local Anesthetic
What’s the evidence?
- Continuous wound infusion
- Open surgery only
- Avoid thoracic epidural analgesia
- No benefit in gyn surgeries
- Limited data for intraperitoneal local anesthetic
- May help in immediate post-operative period only
- TAP block
- Open surgery only
Davidson EM, Barenholz Y, Cohen R, et al. High‐dose bupivacaine remotely loaded into multivesicular liposomes demonstrates slow drug release without systemic toxic plasma concentrations after subcutaneous administration in humans. Anesth Analg 2010;110:1018–23.
What’s the evidence?
Limit the Foley
What’s the evidence?
• Urinary retention is rare
10,274 undergoing benign hysterectomy
23 urinary retention (0.2%)
Highest risk factor for ED visit was Medicaid insurance (OR 2.1)
Pain (23%), Constipation (5%)
Page 55

What’s the evidence?
• Requiring patients to void prolongs recovery
40 patients undergoing vaginal or pelvic surgery
0% retention
All had lower bladder volumes on first void
Patients undergoing active TOV had faster time to decision and higher void rate
135 min vs. 247 min
RR 1.56
Backfill TOV independent predictor for successful bladder emptying after vaginal surgery
Management of Bladder Function after Outpatient Surgery, Anesthesiology 7 1999, Vol.91, 42‐50.The infusion method trial of void vs standard catheter removal in the outpatient setting: a prospective randomized trial. BJU Int. 2011 Apr;107 Suppl 3:43‐6.A randomized, controlled trial evaluating 2 techniques of postoperative bladder testing after transvaginal surgery. Am J ObstetGynecol 2007;197:627.
What’s the evidence?
• Retrospective study of 4743 patients undergoing outpatient gynecologic surgery
• 1557 had an order to void; 3186 had no order to void
• 3 patients returned with urinary retention
All had an order to void
What’s the evidence?
• 18 junior doctors compared to ICU patients they were caring for
23% of the doctors were oliguric
More likely to be oliguric than patients (OR 1.99)
Lower mortality rate (0 vs. 18%)
Solutions
• Same day discharge
Do not require the patient to void
• Overnight admission
Remove catheter 6 hours after surgery
Remove catheter at midnight POD0
What’s the evidence?
• 27 RCTs:
Postoperative bleeding was not statistically increased
Pain control equivalent to opioids
Gobble RM, Hoang HL, Kachniarz B, et al. Ketorolac does not increase perioperative bleeding: a meta-analysis of randomized controlled trials. Plast Reconstr Surg 2014;133:741–55.
Post-operative toradol
What’s the evidence?
- Earlier return to bowel function
- Shorter length of stay
- No increase in vomiting, abdominal distention, or NGT placement
Schilder JM, Hurteau JA, Look KY, et al. A prospective controlled trial of early postoperative oral intake following major abdominal gynecologic surgery. Gynecol Oncol 1997;67:235–40.
Early Feeding
Page 56

What’s the evidence?
• Milk of mag on POD1
• Biscolic suppositories on POD2
Hansen CT, Sorensen M, Moller C, et al. Effect of laxatives on gastrointestinal functional recovery in fast-track hysterectomy: a double-blind, placebo- controlled randomized study. Am J Obstet Gynecol 2007;196:311.e1–7.
Give laxatives post opLaxatives within 6 hours after
abdominal hysterectomy resulted in earlier time to first bowel movement compared with placebo (45 hours vs 69
hours; P<.001) with no change in pain scores, PONV,
antiemetic, or opioid use.
Further considerations – mode of delivery
26
Further considerations – mode of delivery
27
Gambacorti‐PasseriniZ, et al. Acta ObstetGynecol Scand 2016; 95:724–734.
Further considerations
• When can I become pregnant? NO DATA Recommend 3-6 months
• What is the follow up? NO DATA “How do we screen for fibroids?” Annual check in Visit for change in symptoms
• How can I prevent these? Possible correlation with phthalate exposure (Zota, A, et al. Phthalates exposure and uterine
fibroid burden among women undergoing surgical treatment for fibroids: a preliminary study. FertilSteril. 2019 Jan;111(1):112-121)
28
Thank you!
29
Page 57

CULTURAL AND LINGUISTIC COMPETENCY Governor Arnold Schwarzenegger signed into law AB 1195 (eff. 7/1/06) requiring local CME providers, such as
the AAGL, to assist in enhancing the cultural and linguistic competency of California’s physicians
(researchers and doctors without patient contact are exempt). This mandate follows the federal Civil Rights Act of 1964, Executive Order 13166 (2000) and the Dymally-Alatorre Bilingual Services Act (1973), all of which
recognize, as confirmed by the US Census Bureau, that substantial numbers of patients possess limited English proficiency (LEP).
California Business & Professions Code §2190.1(c)(3) requires a review and explanation of the laws
identified above so as to fulfill AAGL’s obligations pursuant to California law. Additional guidance is provided by the Institute for Medical Quality at http://www.imq.org
Title VI of the Civil Rights Act of 1964 prohibits recipients of federal financial assistance from
discriminating against or otherwise excluding individuals on the basis of race, color, or national origin in any of their activities. In 1974, the US Supreme Court recognized LEP individuals as potential victims of national
origin discrimination. In all situations, federal agencies are required to assess the number or proportion of LEP individuals in the eligible service population, the frequency with which they come into contact with the
program, the importance of the services, and the resources available to the recipient, including the mix of oral
and written language services. Additional details may be found in the Department of Justice Policy Guidance Document: Enforcement of Title VI of the Civil Rights Act of 1964 http://www.usdoj.gov/crt/cor/pubs.htm.
Executive Order 13166,”Improving Access to Services for Persons with Limited English
Proficiency”, signed by the President on August 11, 2000 http://www.usdoj.gov/crt/cor/13166.htm was the genesis of the Guidance Document mentioned above. The Executive Order requires all federal agencies,
including those which provide federal financial assistance, to examine the services they provide, identify any
need for services to LEP individuals, and develop and implement a system to provide those services so LEP persons can have meaningful access.
Dymally-Alatorre Bilingual Services Act (California Government Code §7290 et seq.) requires every
California state agency which either provides information to, or has contact with, the public to provide bilingual
interpreters as well as translated materials explaining those services whenever the local agency serves LEP members of a group whose numbers exceed 5% of the general population.
~
If you add staff to assist with LEP patients, confirm their translation skills, not just their language skills.
A 2007 Northern California study from Sutter Health confirmed that being bilingual does not guarantee competence as a medical interpreter. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2078538.
US Population
Language Spoken at Home
English
Spanish
AsianOther
Indo-Euro
California
Language Spoken at Home
Spanish
English
OtherAsian
Indo-Euro
19.7% of the US Population speaks a language other than English at home In California, this number is 42.5%
Page 58
Related Documents











