Ryotaro Nakamura, MD Associated Professor Hematology and Hematopoietic Cell Transplantation Myelodysplastic Syndrome

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Ryotaro Nakamura, MD
Associated Professor
Hematology and Hematopoietic Cell Transplantation
Myelodysplastic
Syndrome

CONFLICTS OF INTEREST
Advisory Board meeting: Seattle Genetics Inc.

Translation for lay people
• Myelo (=bone marrow)
• dysplastic (=looks funny)
• Syndrome (=we don’t really know what
it is, but just pretending to know it)

Patients: limited understanding, lack of insight
An Internet-based survey of 348 MDS patients
80% reported that their MDS was first described as a
“bone marrow disorder,”
6% to 7% indicated their MDS was first described as
either “cancer” or “leukemia.”
42% did not know their blast percentage.
A separate Internet-based survey of 349 MDS patients
33% did not know their MDS subtype.
Oncologist 2011;16(6):904-911
Leuk Res 2008;32(5):691-698
Ineffective hematopoiesis with cytopenia
Clonal disease of hematopoietic stem cell
Dysplastic morphology
Tendency to evolve to acute leukemia
Characteristics of this “syndrome”

WHO 2008

WHO 2008 - MDS/MPD

Blood, Vol 89, No 6 (March 15), 1997: pp 2079-2088
IPSS
Prognosis - IPSS

IPSS-R

Nature Reviews Cancer 12, 849-859
Cytogenetic Abnormalities

Somatic Mutations
Bejar and Steensma, Blood. 2014;124(18):2793

Landscape of genetic lesions
Leukemia (2014) 28, 241–247
N=944

N Engl J Med 2011;364:2496-506.
- Genomic approaches: next-generation sequencing
and mass spectrometry–based genotyping,
- Bone marrow aspirate from 439 patients wit MDS.
- Association with clinical variables

Mutations of genes involved in tyrosinesignaling pathways (JAK2, CBL, and NRAS–
KRAS– BRAF) were largely mutually exclusive (Fig. 1). TET2 mutations, in contrast,
overlapped with lesions in nearly every other mutated gene, suggesting that TET2
mutations have a pathogenic role that is at least partially independent of other
abnormalities. N Engl J Med 2011;364:2496-506.

N Engl J Med 2011;364:2496-506.

N Engl J Med 2011;364:2496-506.


Diagnostic Challenges
Overlap “bone marrow failure” syndrome
Aplastic anemia
“Hypoplastic MDS”
Large granular lymphocyte disease (CD3/CD8/CD57,
TCR gene rearrangement)
PNH clone
Idiopathic cytopenias of undetermined significance (ICUS)
Clonal hematopoiesis of indeterminate potential (CHIP).
Metabolic (B12, copper deficiency, liver disease)
“Idiopathic” thrombocytopenic purpura

45yo female with hypocellular BM, 45,X in 15/20 metaphases
-> slowly responded to ATG/CSA (turned to be mosaic Turner)
62yo male with common variable immune deficiency, later dx’d with
thymoma, then severe anemia with dysplastic BM
-> likely immune mediated. TCR gene rearrangement negative,
but responded to CSA
50yo female, thrombicytopenia, trisomy 8, morphologic dysplasia in BM,
Plt-assoc Ab positive
-> responded to prednisone/eltrombopag
Diagnostic Challenges - Examples

Diagnostic Challenges - Examples
51yo male: thrombocytopenia (~50k/ul), mild anemia, no PNH, hypocellular
marrow, no clear dysplasia
Cytogenetics: Clone 1: 46,XY,+1,der(1;7)(q10;p10)[4]
Clone 2: 46,XY,+1,der(1;12)(q10;q10)[5]

Diagnostic Challenges - Examples
50 yo female presented with pancytopenia
WBC 2,300/uL, Hb 7g/dL, plts 15,000/uL.
Bone Marrow: variable cellularity, mild dysplasia
No clonal T or B cell population
Sucrose test negative (in 1996)
Cytogenetics: trisomy 8 in 2~5/20 metaphases
Treated with ATG and CSA, achieved transfusion
independence, but remains dependent on GCSF and
Epo for anemia. Later evolved into hemolytic PNH,
currently on eculizumab (age 69)

Somatic Mutations and Clonal Hematopoiesis
in Aplastic Anemia
N Engl J Med 2015;373:35-47.

Somatic Mutations and Clonal Hematopoiesis
in Aplastic Anemia
N Engl J Med 2015;373:35-47.
- “unfavorable” mutations: DNMT3A, ASXL1, TP53,
RUNX1, JAK2, JAK3, or CSMD1
- “favorable” mutations: PIGA or BCOR and BCORL1

Young NS. Ann Int Med 2002
Possible relationship among bone
marrow failure syndromes

Management Approaches
Supportive care
- Transfusions
- Growth factors (EPO if EPO level <500mu/ml, G/E for
RARS)
- IV access, iron chelation
MDS-directed therapy
- 5-azacitidine, decitabine, revlimid
- Immunosuppressive therapy (selected cases)
Potentially curative therapy
- Allogeneic HCT
Conventional chemotherapy
- 7+3, FLAG, MEC, cloforabine, low-dose cytarabine,etc.

Goals of Therapy
Cure
Improve the natural history
- prolong life
- delay transformation
Symptomatic support
Weigh against side effects/risks
Can’t get wrong by referring to clinical trials.

RBC transfusions, EPO
- RBC transfusion parameter: to be individualized (7-
9g/dl)
- Lower parameters might not always reduce
transfusions…
- EPO: if <500iu/l
- EPO plus GCSF: to be considered for RARS

- Survival benefit? Benefit in hematopoiesis by reducing free
radicals? in retrospective studies (no prospective randomized
trial data)
- Currently approved agents are inconvenient (deferroxamine) or
costly and not well-tolerated by many patients (deferasirox).
- TELESTO trial: multicenter, randomized, double-blind,
placebo-controlled trial of deferasirox on low-risk MDS patients
with iron overload (NCT00940602)
- New formulation of deferasirox: Jadenu
Iron Chelation
NCCN guideline: IPSS low, int-1, Target ferritin: 1000 ng/ml
- >20 transfusions, or
- Anticipated ongoing RBC transfusions, or
- Serum ferritin >2500 ng/ml

- Potential risk to augment myeloblast proliferation
- The rate of progression to AML was not increased with
romiplostim therapy in lower-risk MDS,
- Platelet transfusion needs and clinically significant
bleeding events were reduced with active therapy.
- Decreased frequency of dose reductions or delays in
patients receiving lenalidomide therapy
TPO Receptor Agonists Romiplostim (Nplate) and Eltrombopag (Promacta)
Sekeres MA, Kantarjian H, Fenaux P, et al. Subcutaneous or intravenous administration of romiplostim in thrombocytopenic patients with lower risk myelodysplastic syndromes.
Cancer. 2011;117(5):992-1000.
Kantarjian H, Fenaux P, Sekeres MA, Becker PS, Boruchov A, Bowen D, Hellstrom-Lindberg E, Larson RA, Lyons RM, Muus P, Shammo J, Siegel R, Hu K, Franklin J, Berger DP.
Safety and efficacy of romiplostim in patients with lower-risk myelodysplastic syndrome and thrombocytopenia. J Clin Oncol. 2010 Jan 20;28(3):437-44
Kantarjian HM, Giles FJ, Greenberg PL, Paquette RL, Wang ES, Gabrilove JL, Garcia-Manero G, Hu K, Franklin JL, Berger DP. Phase 2 study of romiplostim in patients with low- or
intermediate-risk myelodysplastic syndrome receiving azacitidine therapy. Blood. 2010 Oct 28;116(17):3163-70.
Giagounidis A, Mufti GJ, Fenaux P, et al. Results of a randomized, double-blind study of romiplostim versus placebo in patients with low/intermediate-1-risk myelodysplastic syndrome
and thrombocytopenia. Cancer. 2014;120(12):1838-1846.
Wang ES1, Lyons RM, Larson RA, Gandhi S, Liu D, Matei C, Scott B, Hu K, Yang AS. A randomized, double-blind, placebo-controlled phase 2 study evaluating the efficacy and safety
of romiplostim treatment of patients with low or intermediate-1 risk myelodysplastic syndrome receiving lenalidomide. J Hematol Oncol. 2012 Nov 29;5:71.
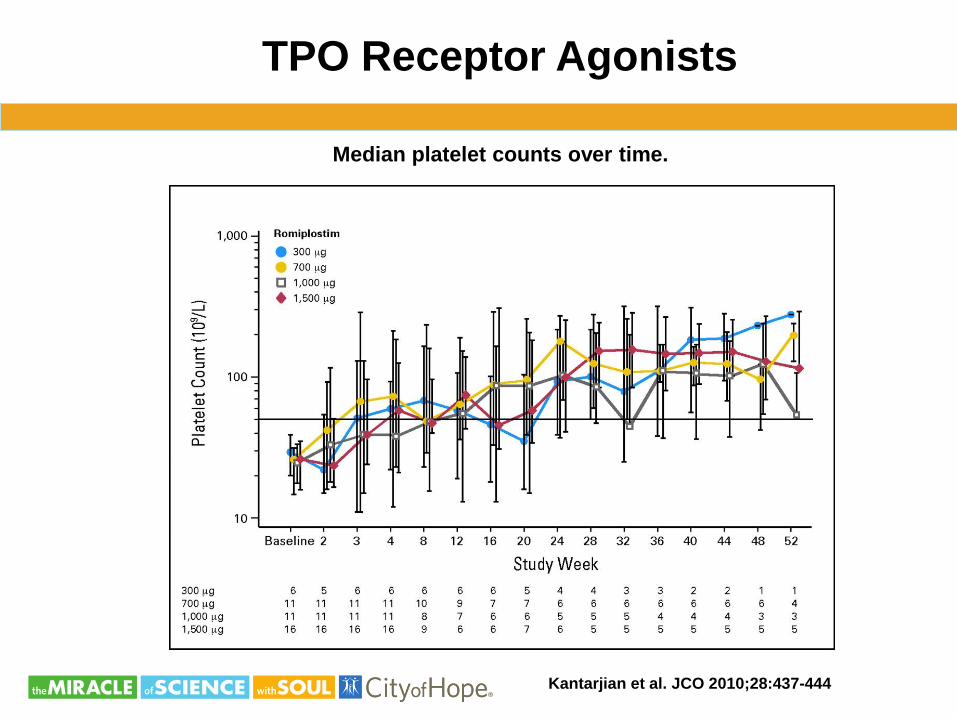
TPO Receptor Agonists
Median platelet counts over time.
Kantarjian et al. JCO 2010;28:437-444

Lenalidomide
Erythroid Response rate:
5q31.1: 83%
normal karyotype: 57%
other karyotypic abnormalities: 12%
N Engl J Med 2005;352:549-57.

Phase II, N=148, 10mg/d continuous or 21d
- 112 had a reduced (>50%) need for transfusions (76%)
- 99 patients (67%): TI regardless of the karyotype complexity.
- Median time to response, 4.6 weeks; range, 1 to 49
- Sustained response: the median duration of TI had not been
reached after a median of 104 weeks of follow-up.
- Cytogenetic response:
- 62 of 85 had cytogenetic improvement (38: complete
cytogenetic remission).
Lenalidomide in the Myelodysplastic
Syndrome with Chromosome 5q Deletion
N Engl J Med 2006;355:1456-65.

Phase 2 study of lenalidomide in transfusion-dependent, low-
and int1–risk MDS with karyotypes other than deletion 5q
Blood. 2008;111:86-93

J Clin Oncol 20:2429-2440
Hypomethylating Agents

J Clin Oncol 20:2429-2440

J Clin Oncol 20:2429-2440

J Clin Oncol 20:2429-2440

Lancet Oncol 2009; 10: 223–32

Lancet Oncol 2009; 10: 223–32

Lancet Oncol 2009; 10: 223–32

J Clin Oncol 29:1987-1996.
• 233 patients (median age:70 years, range: 60-90)
• 53% had poor-risk cytogenetics,
• The median MDS duration at random assignment: 3 months.
• Primary end point: overall survival (OS).
• Decitabine (15 mg/m2) intravenously over 4 hours 3x/day for 3 days in
6-week cycles.
No cross over

J Clin Oncol 29:1987-1996.

Long-term outcome of higher-risk MDS patients treated with
azacitidine: an update of the GFM compassionate program cohort

Design/Therapy
Total
N Overall Survival
Cohort: Outcome after AZA-failure(1) 435 15% (2 year)
Cohort: Prognostic Factors in Compassionate
Use AZA(2) 282 ~20% (3 year by survival curve)
Cohort: Compassionate Use AZA(3) 282 17.5% (3 year)
Ph III: Low-Dose Decitabine vs. BSC(4) 233 19% (2 year)
Ph III: European AZA-001: AZA vs. BSC(5) 358 50.8% (2 year), ~30% (3 year by survival curve)
Ph III: Decitabine vs. BSC(6) 170 Not available
Ph III: CALGB AZA vs. BSC(7) 191
~45% (2 year), ~25% at (3 year by survival
curves)
Retrospective: HCT in 60-70 yo vs. No Donor +
AZA(8) 178 23% (2 year)
Decision Analysis (<60yo)(9) 184
<5% for high, ~20% for Int 2 (3 year by survival
curve)
Survival Outcomes from HMA trials

Prebet et al. J Clin Oncol 29:3322
Poor outcome after azacitidine
treatment failure

Poor outcome after azacitidine
treatment failure

Combination Therapy
A phase II trial of azacitidine (75 mg/m2/d x 5 days) in combination with
lenalidomide (10 mg/d x 21 days (28-day cycle) for higher-risk MDS.
-overall response rate of 72% (CR: 44%)
- median CR duration of 17+ months (range, 3-39+)
- median overall survival of 37+ months (range, 7-55+) for CR patients,
13.6 months for the entire cohort (range, 3-55).
Phase I study evaluated the combination of azacitidine and vorinostat
in MDS and AML patients. There were no serious non-hematologic
toxicities, and responses were seen in up to 86% of patients.

Randomized Phase II Study of Azacitidine Combined with
Lenalidomide or with Vorinostat Vs. Azacitidine Monotherapy
in Higher-Risk Myelodysplastic Syndromes (MDS) and
Chronic Myelomonocytic Leukemia (CMML): North American
Intergroup Study SWOG S1117
(Sekeres at al. ASH 2014 Late Breaking Abstract 5)
Higher-risk MDS (IPSS Int-2 or High and/or bone marrow
blasts ≥5%) and CMML patients (pts) with <20% blasts
- AZA (75 mg/m2/d on d1-7 of a 28d cycle)
- AZA + LEN (10 mg/d on d1-21), or
- AZA + VOR (300 mg BID on d3-9).
Combination Therapy


≥Grade 3 AE (AZA:AZA+LEN:AZA+VOR)
- febrile neutropenia (10:13:13)
- gastrointestinal disorders (4:11:23)
- infections (2:3:3)
- rash (2:12:1).
ORR (N=290): 33%
CR: 19%, PR: 1%, HI: 13%
RFS (median): 7 months.
ORR in study arms:
AZA: 36%
AZA+LEN: 37% (p=1.0),
AZA+VOR: 22% (p=.07)
CR/PR/HI rates:
AZA: 23%/0%/13%
AZA+LEN: 18%/1%/17% (CR p=.47)
AZA+VOR 14%/1%/7% (CR p=.18)

Allogeneic HCT
• The only potentially curative treatment
• Eliminates malignant hematopoietic clones
through conditioning chemo-radiotherapy and
graft-versus-leukemia (GVL) effects
• Restores hematopoiesis with donor-derived
progenitor cells
• Associated with significant risks of transplant-
related mortality/morbidity (GVHD, infection,
organ toxicity, graft failure)

Transplant is not a gamble….


CIBMTR data

CIBMTR data

City of Hope RIC HCT experience for MDS
Initial disease control:
Focusing on patients with persistent MDS
(n=27) or persistent AML (n=7) at the time
of transplant, an early post transplant bone
marrow examination was available in
27 (MDS: 21, AML: 6). Of these, 24
patients (89%) showed no evidence of
MDS or AML around day 30.
TRM: 35%, grade II-IV GVHD: 62%
• Fludarabine (125mg/m2+Melphalan 140mg/m2)
• GVHD prophylaxis: CSA+MMF +/-miniMTX
Nakamura et al. BMT 2007
N=43

Leukemia Res 2012
City of Hope Experience with RIC-HCT
(Flu/Mel, Tacro/Siro)

• Who and when?
Age, co-morbidities?
Subtypes/IPSS risk categories?
• How?
Conditioning
Donor source (MRD, MUD, Cord, Haplo)
GVHD prophylaxis
Pre- and post-HCT therapy to reduce relapse
pre-HCT cytoreduction (HM agents, high-
intensity induction)
post-HCT HM agents/MRD monitoring
Challenges in HCT for MDS

A decision analysis of allogeneic BMT for MDS: delayed
transplantation for low-risk MDS is associated with improved outcome
Cutler et al. Blood. 2004;104:579-585
Markov decision model
BMT cohort: BM graft
ablative conditioning,
sibling donor, tacro-MTX

Coverage with Evidence Development
• CMS issued a decision memo in Aug 2010 allowing
“coverage with evidence development (CED)”
Suggests insufficient evidence
“..evidence does not demonstrate that the use of
HCT improves health outcomes in Medicare
beneficiaries with MDS.”
“paucity of evidence regarding the use of HCT in
patients with MDS who are 65 years or older”
Will cover costs of HCT if patients enrolled in a study
that will provide CMS with data (“evidence”) to
determine the value of the procedure in the
Medicare population

Biol Blood Marrow Transplant. 2014 Oct; 20(10): 1566–1572.

Role of RIC-HCT in Older Patients
With De Novo MDS: An
International Collaborative Decision Analysis
RIC, 60-70yo, MUD/MRD
Blue area: superior QALE
Koreth et al J Clin Oncol 2013; 31:2662-2670
IPSS Low/Int-1
IPSS Int-2/High

Platzbecker et al. Biol Blood Marrow Transplant 18:1415-1421, 2012
Allo-HCT in Patients Age 60-70 Years with De Novo High-Risk
MDS/2ndary AML: Comparison with Patients Lacking Donors Who
Received Azacitidine

Platzbecker et al. Biol Blood Marrow Transplant 18:1415-1421, 2012

HLA-matched allogeneic HCT improves
outcome of higher risk MDS: SFGM-TC and GFM
Robin et al. Leukemia (2015) 29, 1496–150
162 patients with MDS (50: no donor, 112: donor)
Median age: 60 years (range: 50–70).
IPSS no donor donor
Int-1 5 (10%) 8 (7%)
Int-2 28 (56%) 75 (67%)
High 12 (24%) 22 (20%)

Corey Cutler, MD MPH
Ryotaro Nakamura, MD
• 3-yr overall survival benefit (Primary Objective)
• 3-yr LFS (Secondary Objective)
• QOL benefit (Secondary Objective)
• Cost Effectiveness (Ancillary study)
Key questions
BMT CTN 1102: A Multi-Center Biologic Assignment Trial
Comparing Reduced Intensity Allogeneic Hematopoietic
Cell Transplant to Hypomethylating Therapy or Best
Supportive Care in Patients Aged 50-75 with Intermediate-2
and High Risk Myelodysplastic Syndrome

Accrual: ~50% complete (target 340-400)

Summary….
Bejar and Steensma, Blood. 2014;124(18):2793
Related Documents











