MODERATOR – Prof. DR. - ANIL MODERATOR – Prof. DR. - ANIL KAPOOR KAPOOR

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

MODERATOR – Prof. DR. - ANIL KAPOORMODERATOR – Prof. DR. - ANIL KAPOOR
What Is Myelodysplastic Syndrome?The myelodysplastic syndromes are a group of
disorders characterized by one or more peripheral blood cytopenias secondary to bone marrow dysfunction.
In MDS the bone marrow cannot produce blood cells effectively, and many of the blood cells formed are defective.
These abnormal blood cells are usually destroyed before they leave the bone marrow or shortly after entering the bloodstream.
As a result, patients have shortages of blood cells, which are reflected in their low blood
CharacteristicsVarying degree of tri-lineage cytopenia ( red
blood cells, white blood cells and platelets).Dysplasia Normocellular or hypercellular B.M.May progress to acute leukaemia

Incidence1- Disease of elderly. 2- Median age is 65 years.3- <10% are younger than 50 years.4- Incidence rates 1/100,000 pop./ years.5- Incidence rise to 1/1000 / years in > 60 years
old. 6- Male slightly higher than female

MDS EtiologyTwo etiologic categories of MDS: 1.) De Novo:
Associated with: -benzene exposure (gasoline) -cigarette smoking -viruses -Fanconi’s anemia 2.) Therapy related:
Associated with: -alkylating agent chemotherapy
-radiation

Aetiological Agents Tobacco smoke. Ionizing radiation. Organic chemicals (such as benzene, toluene, xylene,
and chloramphenicol). Heavy metals. Herbicides. Pesticides. Fertilizers. Stone and cereal dusts. Exhaust gases. Nitro-organic explosives. Petroleum and diesel derivatives. Alkylating agents. Marrow-damaging agents used in cancer
chemotherapy.
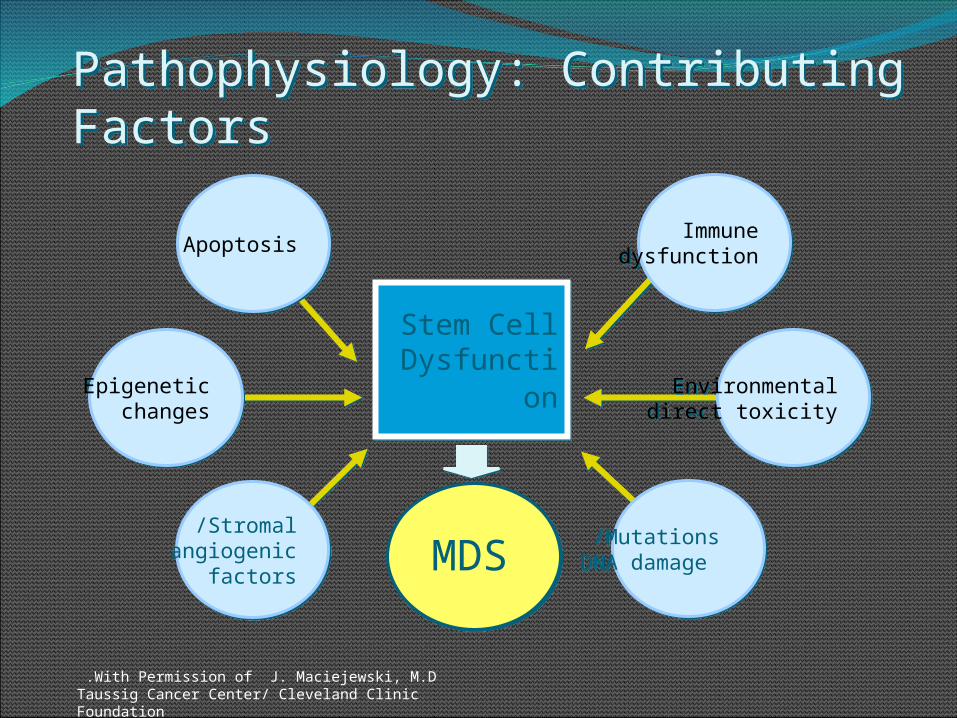
Pathophysiology: Contributing Factors
MDS
Stem cell dysfunction Stem Cell
Dysfunction
Apoptosis
Stromal/angiogenic
factors
Epigenetic changes
Immunedysfunction
Environmentaldirect toxicity
Mutations/ DNA damage
With Permission of J. Maciejewski, M.D .Taussig Cancer Center/ Cleveland Clinic Foundation
Myelodysplastic SyndromeDyserythropoiesisDysmyelopoiesisDysmegakaryopoies
isRing SideroblastType I and II blasts

DyserythropoiesisAnemiaNormocytic or macro-ovalocytesLow retic countNRBCMegaloblastic changesRinged sideroblastPappenheimer bodiesBasophilic stippling




Dyserythropoiesis
Ringed sideroblast

DysmyelopoiesisNeutropeniaMonocytosisPseudo Pelger-HuetHypogranular PMN<20% blasts in BMType I and type II blasts



Blasts in MDSType I blasts
No granulesProminent
nucleoliCentral nucleus
Type II and III blastsFew 1o granulesProminent
nucleoliCentral nucleusAuer rods
PromyelocyteMany 1o
granulesLess prominent
nucleoliEccentric
nucleus
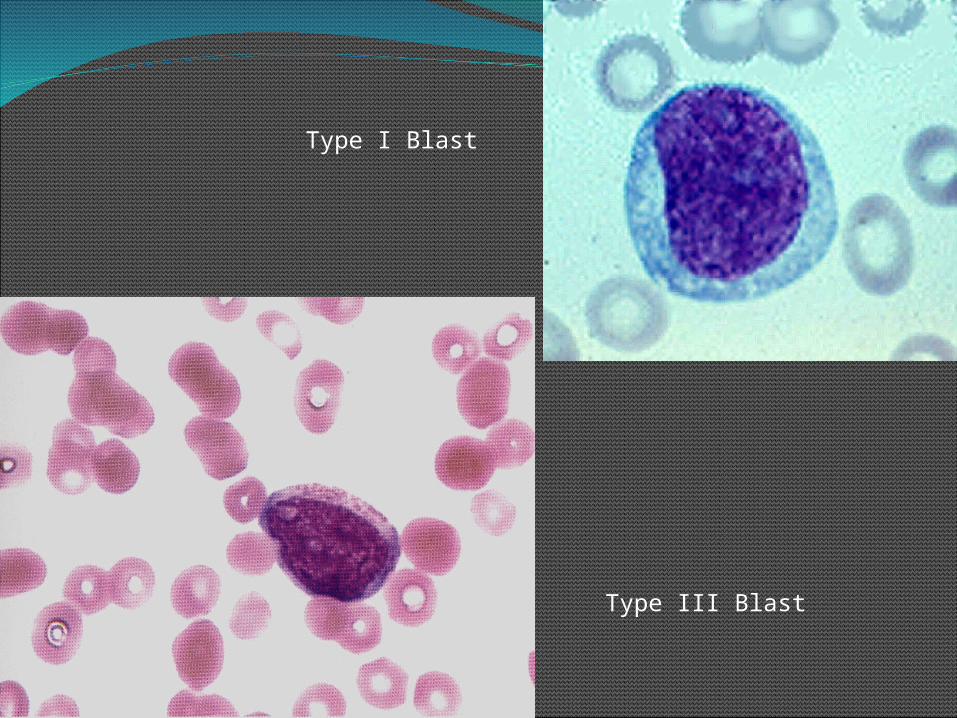
Type I Blast
Type III Blast
DysmegakaryopoiesisLow platelet countGiant PlateletDwarf (micro) megakaryocyte

Abnormal platelets
Micromegakaryocyte
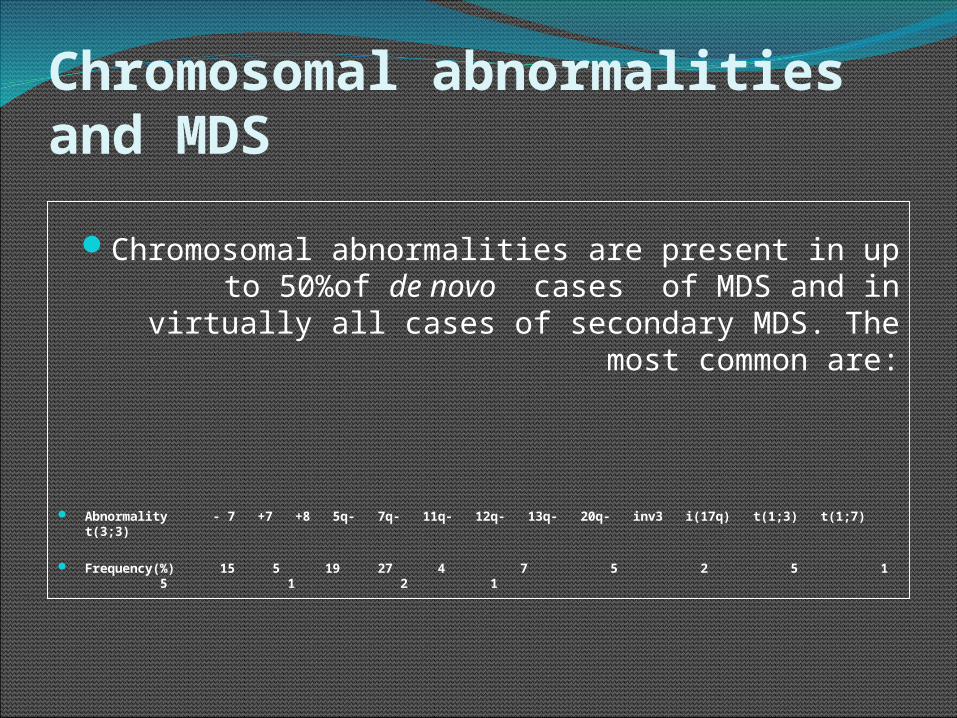
Chromosomal abnormalities and MDS
Chromosomal abnormalities are present in up to 50%of de novo cases of MDS and in virtually all cases of secondary MDS. The most common are:
Abnormality - 7 +7 +8 5q- 7q- 11q- 12q- 13q- 20q- inv3 i(17q) t(1;3) t(1;7) t(3;3) Frequency(%) 15 5 19 27 4 7 5 2 5 1 5 1 2 1
Deletion of the long arm of chromosome 5 (5q- syndrome )
Strongly associated with RA.
5q- accounts for up to 70% of cytogenetic abnormalities in this subtype.
The q arm of chromosome 5 is particularly rich in genes, which encoded haemopoietic growth factors and their receptors. For example , IL-3 , IL-4 , IL-5 , GM-CSF and the M-CSF receptor are located in this region.
The potential for the loss of any or all of these genes contribute to the disruption of ordered haemopoiesis.

Monosmy 7 and 7q-Most strongly associated with secondary
MDS. Associated with the loss of a major surface
glycoprotein (gp 130) in neutrophile and susceptibility to bacterial infection secondary to impaired granulocyte monocyte chemotatic activity.

Deletion of the q arm of chromosome 11 (11q-)
Account for 20% of the chromosomal abnormalities in RAS.
This abnormality is associated with raised
iron stores and high ring sidroblast counts.
The presence of the gene , which encoded the H-subunit of ferritin at chromosome 11 , may explain this
Abnormalities of chromosome 17 (i17q)It involves the loss or disruption of the Р53
tumor suppressor gene are seen in CML in association with transformation to the blastic phase and in up to 5% of cases of primary MDS.
This predisposes to certain dysplastic features and neutrophil vaculation.

Abnormalities of chromosome 3
Dysmegakaryopiesis and thombocytosis appear to be associated with Abnormalities of chromosome 3

The importance of indication of chromosomal abnormalities
To confirm diagnoses . To know the stage of disease.To know the direction of progression of
disease.Multiple genetic abnormalities indicate late
events in MDS.

Abnormal localization of immature precursors
Presence of 3 or more small clusters of myeloblasts and promyelocytes (5 – 8 cells) in marrow trephine biopsy in the central portion of the marrow away from the vascular structure and the endosteal surface of the bone trabeculae
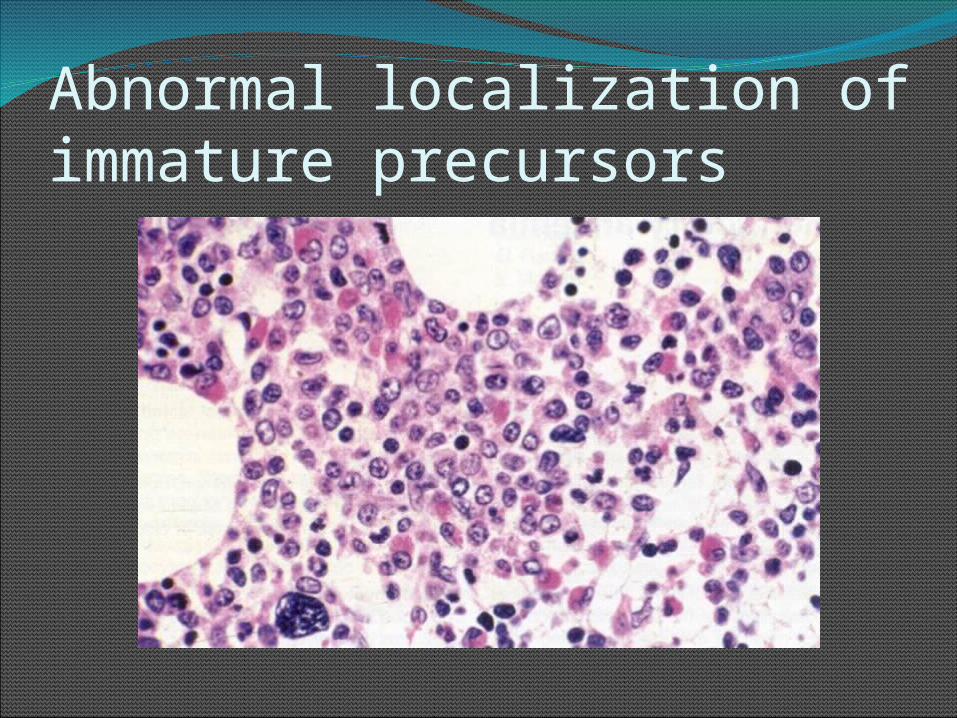
Abnormal localization of immature precursors
Signs and Symptoms Excessive tiredness, shortness of breath, and pale
skin can be caused by anemia (shortage of red blood cells).
Serious infections with high fevers can be caused by
leukopenia (not having enough normal white blood cells) and, in particular, by having neutropenia or granulocytopenia (too few mature granulocytes).
Excessive bruising and bleeding, for example, frequent or severe nosebleeds and/or bleeding from the gums, can be due to thrombocytopenia (not having enough of the blood platelets needed for plugging holes in damaged blood vessels).
Physical Exam
Hepatomegaly, splenomegaly, LAD: uncommonExcept CMML
Cutaneous manifestations: uncommonSweet’s syndrome( neutrophilic
dermatosis): transformation to acute leukemia ( IL-6)
Granulocytic sarcoma (chloroma): herald disease transformation into acute leukemia
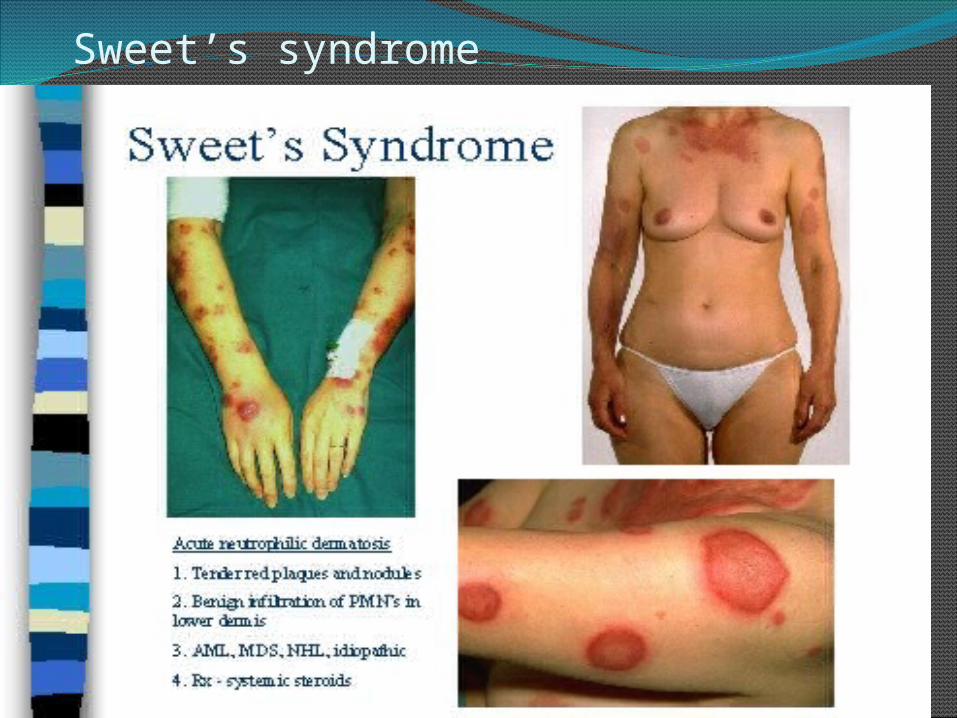
Sweet’s syndrome

FAB classification scheme in 1985 for MDS
Refractory AnemiaRA Definition:Dyplasia of the erythroid series only.Clinically, anemia is refractory to hematinic
therapyMyeloblasts < 1% blood and < 5% marrow<15% ringed sideroblasts in marrowNo Auer rodsOther etiologies of erythroid abnormalities
must be excluded. These include:drug/toxin exposure -vitamin deficiencyviral infection -congenital disease

Refractory AnemiaEpidemiology:5-10% of MDS cases. Older patientsMorphology:Anisopoikilocytosis on peripheral smearsDyserythropoiesis with nuclear abnormalities
(megaloblastoid change)< 15% ringed sideroblasts

Refractory AnemiaGenetics:25% may have genetic abnormalities
Prognosis:Median survival is 66 months6% rate of progression to acute leukemia

Peripheral Smear - Anisopoikilocytosis

Megaloblastoid Change on Bone Marrow Aspirate

Refractory Anemia with Ringed Sideroblasts RARS definition:Dyplasia of the erythroid series only.Clinically, anemia is refractory to
hematinic therapyMyeloblasts < 5% in marrow, absent in
blood>15% ringed sideroblasts in marrowNo Auer rodsOther etiologies of ringed sideroblasts
must be excluded. These include:Anti- tuberculosis drugsAlcoholism

Refractory Anemia with Ringed SideroblastsEpidemiology:10-12% of MDS cases. Older patientsMales > femalesMorphology:Dimorphic pattern on peripheral smears
Majority RBC’s normochromic, 2nd population hypochromic
Dyserythropoiesis with nuclear abnormalities (megaloblastoid change)

Refractory Anemia with Ringed SideroblastsGenetics:Clonal chromosomal abnormalities in <10%; in fact, development of such an
abnormality should prompt reassessment of diagnosis.
Prognosis: Median survival 6 years (72 months)1-2% rate of progression to acute leukemia

Dimorphic Red Cell Population

Ringed Sideroblasts

Ringed Sideroblasts

Megaloblastoid Change

Refractory Anemia with Excess BlastsRAEB definition:Refractory anemia with 5-19% myeloblasts in
the bone marrow.RAEB-1:
5-9% blasts in bone marrow and <5% blasts in blood.
RAEB-2: 10-19% blasts in the bone marrow Auer rods present

Refractory Anemia with Excess BlastsEpidemiology: 40% of MDS cases. Older patients (over 50 years) Morphology:Dysplasia of all three cell lines often presentNeutrophil abnormalities may include:
Hypogranulation Pseudo-Pelger-huet (hyposegmentation/barbells)
Megkaryocyte abnormalities may includeHypolobation -Micromegakaryocytes

Refractory Anemia with Excess BlastsMorphology (con’t.)Erythroid precursor abnormalities may include:
Abnormal lobulation -megaloblastoid changeMultinucleation
0-19% myeloblasts in the blood5-19% in the marrowBone marrow:
Usually hypercellular (10-15% hypocellular)Abnormal localization of immature precursors (ALIP)
may be presentImmunophenotype:
Blasts express CD 13, CD33 or CD117

Refractory Anemia with Excess BlastsGenetics:Clonal chromosomal abnormalities found in 30% -
50% of RAEB cases. The abnormalities include:+8 – -5 – del(5q)– -7 – del(7q) – Complex karyotypes
Prognosis: Median survival, RAEB-1 = 18 monthsMedian survival, RAEB-2 = 10 monthsRAEB-1 = 25% rate of progression to acute leukemiaRAEB-2 = 33% rate of progression to acute leukemia

Hypercellular Bone Marrow

Auer Rods

Refractory Anemia with Excess Blasts in Transformation (RAEB-t)
21-30 percent blasts in the marrow; more than 5 percent in the bloodstream
normal or hypercellular (filled with cells) marrow
accounts for about 25 percent of cases
Chronic Myelomonocytic Leukemia (CMML)
5-20 percent blasts in the marrow; less than 5 percent in the bloodstream
cytopenia of at least two cell lines normal or hypercellular (filled with cells)
marrow
accounts for 15 to 20 percent of cases.
CMML Splenomegaly (10%) Maculopapular skin infiltration Monocytic pleural or pericardial effusion JMML (MPD/MDS)1. Pallor, bleeding, hepatosplenomegaly, skin
involvement

WHORefractory anemiaRefractory anemia e ringed siderblastRefractory cytopenia e multilineage
dysplasiaRefractory cytopenia e multilineage
dysplasia & ringed sideroblastsRefractory anemia e excess blast-1Refractory anemia e excess blast-2Myelodysplastic syndrome unclassifiedMDS associated e isolated del (5q)

WHOSubtypeBloodBone MarrowRAAnemiaErythroid
dysplasia only
RARSAnemiaErythroid dys>15% ringed
RCMDBi- pancytopenia >10%Dysp in 2 or more cell lineage
RCMD-RSBi-pancytopenia >10%Dys 2 or more cell lineage>15% ringed
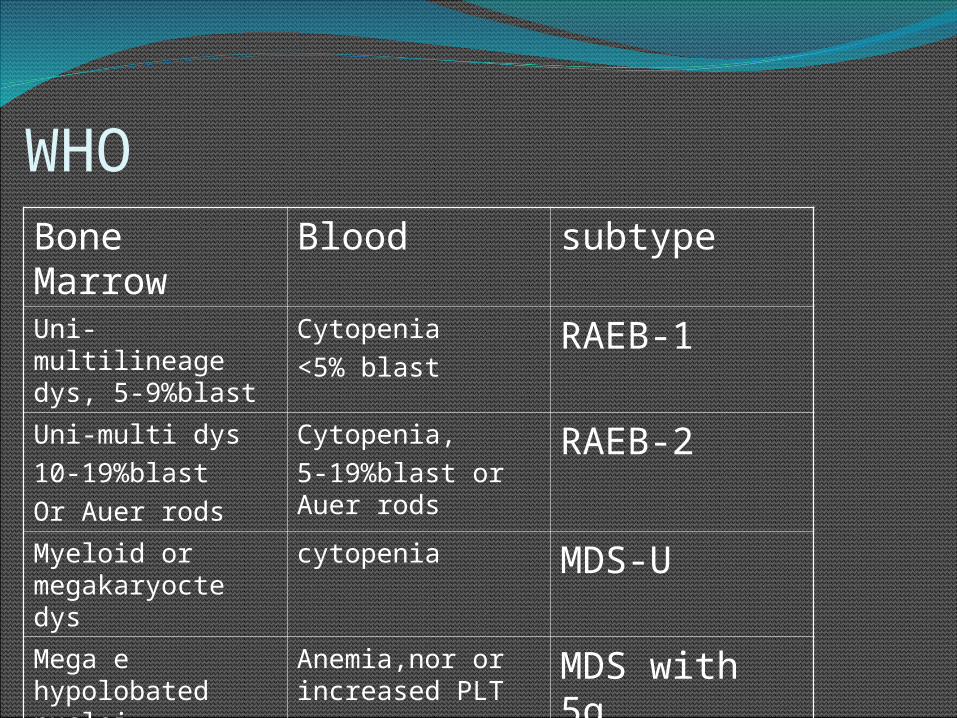
WHOsubtypeBloodBone Marrow
RAEB-1Cytopenia<5% blast
Uni-multilineage dys, 5-9%blast
RAEB-2Cytopenia,5-19%blast or Auer rods
Uni-multi dys10-19%blastOr Auer rods
MDS-UcytopeniaMyeloid or megakaryocte dys
MDS with 5qAnemia,nor or increased PLT
Mega e hypolobated nuclei, <5%blast

Prognostic GroupsTwo groups based on survival and evolution to
acute leukemia
1.) “Good” groupRefractory anemia (RA)Refractory anemia with ringed sideroblasts (RARS)5q - syndrome
2.) “Bad” groupRefractory anemia with excess blasts (RAEB)Refractory anemia with excess blasts in transformation
(RAEB-t)CMML
MDS unclassified can be either

International Prognostic Scoring System (IPSS) Factors
(1) the percentage of blasts in the bone marrow.(2)whether chromosome abnormalities are
present and, if so, which ones.(3)how low the patient's blood counts are. These
are given a score; the lowest scores have the best outlook for survival.

Prognostic Scoring The International Myelodysplastic Syndrome Working
Group developed a scoring system based on 3 variables:
000.50.51.01.01.51.52.02.0% Blasts% Blasts<5<55-105-10 ----11-2011-2020-3020-30KaryotypKaryotypee
Normal, -Normal, -Y, del(5q), Y, del(5q), del(20q)del(20q)
Single Single karyotypikaryotypic c anomaly,anomaly,Double Double abnormaliabnormaliyy
≥ ≥ 3 3 abnormalitieabnormalities, chr 7 s, chr 7 abnormalitieabnormalitiessChr 3 abn.Chr 3 abn.
CytopeniCytopeniaa0-10-12-32-3
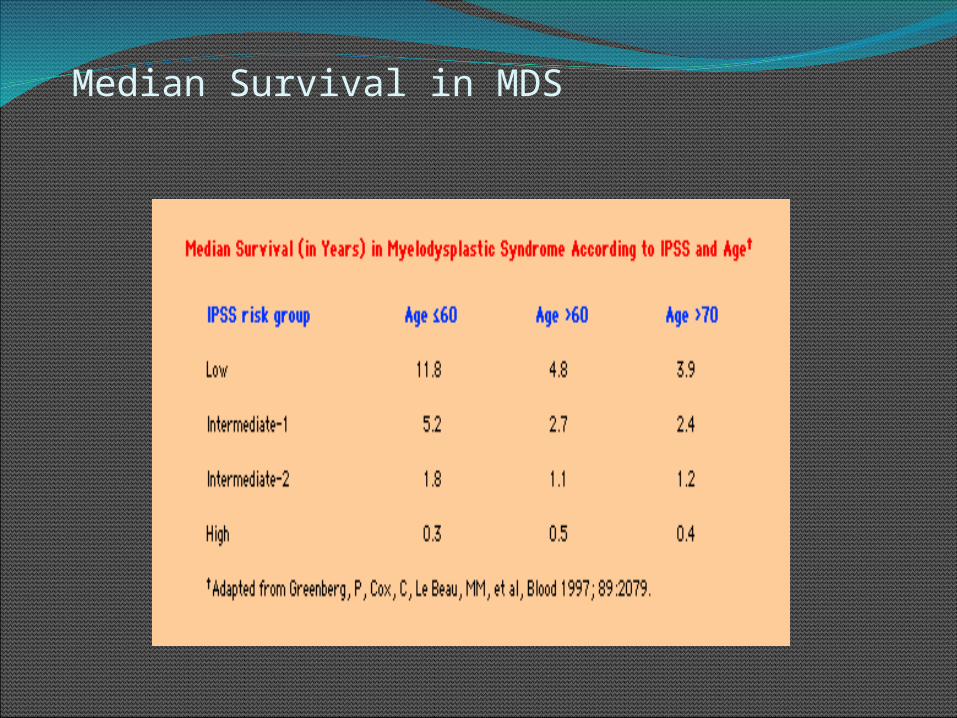
Median Survival in MDS
MDS: Differential DiagnosisB12/folate deficiencyHeavy metals (Arsenic)Congenital dyserythropoietic anemiaParvovirus B19GCSF therapy (increased blasts)

Treatmento Chemotherapy.
o Supportive therapy, such as WBCs, RBCs, Platelets transfusions.
o B.M transplantation in young patients.

THANK YOU
SPEAKER- DR. Narmada Prasad TiwariSPEAKER- DR. Narmada Prasad Tiwari
Prevention & Treatment of Infections
PreventionProphylactic antibiotics no rolePatient education know your nadirreport a feverrecognize signs of infectionavoid illness, crowdsupdate vaccinations
Treatment Febrile neutropenia guidelines
www.nccn.org/MDS v1..2008

Iron Chelation OptionsDeferoxamine (Desferal®)
Route: SQt ½: 0.5 hoursDosing: Infused over 8-12 hrs5-7 nights/week
Deferasirox (Exjade®)Route: POt ½: 12-16 hoursDosing: Dissolved in solution, taken daily
Pharmacotherapy In MDSAzacitidineDecitabineLenalidomideAnti-thymocyte Globulin (ATG)

IPSS

Median Survival in MDS

Large pronormoblast in pervovirus infection.

Differential DiagnosisNon-neoplastic simulators
Other myelodysplastic disordersNon-neoplastic disorders may simulate myelodysplasia
Vitamin/micronutrient deficienciesB12/folate
CopperRing sideroblasts present
Cytoplasmic vacuolesMay be due to
Zinc excessGastrectomy
Total parenteral nutritionInfections
HIVParvovirus
HHV-6 in childrenToxins
EthanolHeavy metals
Growth factorsGranulocyte-macrophage colony-stimulating factor (GMCSF)
ErythropoietinDrugs (numerous)
Chemotherapeutic agentse.g. megaloblastoid change with folate antagonists
Valproic acid, MMF (mycophenolate mofetil), GanciclovirPseudo-Pelger-Helger anomaly
Autoimmune/rheumatologice.g. systemic lupus erythematosus
CongenitalCongenital dyserythropoietic anemias
Inherited bone marrow failure syndromoes (Fanconi etc.)Monocytopenia immunodeficiency syndrome
Related Documents











