Nursing Care of Clients With Musculoskeletal Disorders Lecturer: Isaac Amankwaa

Muskuoloskeletal System CS
Dec 10, 2015
lecture notes
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Nursing Care of Clients With Musculoskeletal
Disorders
Lecturer: Isaac Amankwaa

Outline Fractures: Types Management & complications Traction (Skin and Skeletal) Casts (Compartment Syndrome,
Infection, Cast Syndrome)
Isaac Amankwaa

Class Objectives: Describe the anatomy and physiology of the
musculoskeletal system including the significance of health history.
Discuss the significance of assessment and diagnosis of musculoskeletal problems including diagnostic tests.
Explain the pathophysiology, manifestations, complications & collaborative care of clients with fractures.
Describe the preventative health teaching needs of the client with a cast.
Describe the various types of traction and appropriate nursing care.
Isaac Amankwaa

Fracture Definition
A Fracture is a break in the continuity of a bone, separating it into two or more parts that may be accompanied by injury of surrounding soft tissue producing swelling and discoloration.
Isaac Amankwaa

Fracture ctd When # occurs, muscles are also
disrupted & pull fracture fragments out of position.
Adjacent structures are affected – soft tissue edema, hemorrhage, joint dislocations, ruptured tendons, severed nerves, damaged blood vessels
Isaac Amankwaa

Causes of fracture
Direct blow Crushing force Sudden twisting motion Extreme muscle contraction
Isaac Amankwaa

Types of Fracture Open: (compound or complex) break in
tissue over site of the bone injury
Complete: break across entire cross-section of bone & often displaced
Incomplete: (greenstick) through only part of the cross-section
Closed: (simple) intact skin over site of injury
Comminuted: produces several bone fragment
Isaac Amankwaa

COMMON TYPES OF FRACTURES
Table 6.1
Isaac A
mankw
aa

COMMON TYPES OF FRACTURES
Table 6.1
Isaac A
mankw
aa

COMMON TYPES OF FRACTURES
Table 6.1
Isaac A
mankw
aa

COMMON TYPES OF FRACTURES
Table 6.1
Isaac A
mankw
aa

Isaac Amankwaa

PHYSIOLOGICAL RESPONSES
Local Response Blood vessels within the bone, the
periosteum and surrounding tissues are torn, resulting in haemorrhage and the formation of a haematoma.
The periosteum at the site may be stripped away from the underlying bone tissue, interrupting the blood supply into the area and thus contributing to the death of bone cells.
Isaac Amankwaa

PHYSIOLOGICAL RESPONSES Systemic Response
The client suffers some degree of shock which is influenced by the severity of the injury, the amount of soft tissue damage, associated disorders or multiple injuries and the patient’s age and general condition at the time of injury.
In addition there is also the psychological dimension to consider as different people respond to different ways to same injury.
Isaac Amankwaa

Clinical Manifestations Deformity (hemorrhage or spasm) Shortening Swelling Muscle spasm Pain, tenderness Loss of function, altered mobility &
crepitus Neurovascular changes shock
Isaac Amankwaa

Signs and SymptomsSigns and Symptoms
Isaac Amankwaa

Diagnostic Investigations X-ray examination to confirm location
and direction of fracture line. Signs and symptoms Magnetic resonance imaging (MRI) Angiography with blood vessel injury Differential diagnostic studies with
pathological fracture Nerve conduction and
electromyogram studies with nerve injury
Blood studies e.g. Complete blood count
Isaac Amankwaa

HEALING OF FRACTUREBone is different from many of the
specialized tissues because of its ability to
regenerate and hence restore the continuity Haematoma formation Granulation tissue formation Callous formation Ossification Remodeling and Consolidation
Isaac Amankwaa

Stages of Healing a Fracture
Figure 6.14Isaac Amankwaa

FACTORS ENHANCING FRACTURE HEALING
1. Immobilization of the fracture fragments
2. Maximum bone fragment contact3. Sufficient blood supply 4. Proper nutrition5. Exercise-Weight-bearing for long
bones6. Hormones-growth hormone, thyroid,
calcitonin, insulin, vitamins A and D, anabolic steroids.
Isaac Amankwaa

Factors Inhibiting Fracture Healing
Extensive local trauma Bone loss Inadequate immobilization Space/tissue between bone
fragments Infection Local malignancy Metabolic bone diseases (e.g.
Paget’s disease)Isaac Amankwaa

Factors Inhibiting Fracture Healing
Irradiated bone (radiation necrosis) Avascular necrosis Age (elderly persons heal more slowly) Corticosteroids (inhibit the repair rate) Denervation
Isaac Amankwaa

Complications of fracture Early complications include:
Shock Nerve damage, arterial damage Infection Cast syndrome Compartmental Syndrome Fat Embolism Syndrome Deep Vein thrombosis & Pulmonary
Embolism
Isaac Amankwaa

Long-term Complications Joint stiffness or post-traumatic
arthritis Avascular necrosis Nonfunctional union after a
fracture Complex regional pain syndrome Reaction to internal fixation
device Isaac Amankwaa

Avascular NecrosisAvascular Necrosis
Isaac Amankwaa

Emergency mgt of fractures Immediately immobilize affected limb. Unless there is bleeding apply splints
and padding (above and below fracture site) directly over the clothing.
If bleeding is present visualization may be necessary before pressure can be applied where bleeding is originating.
Keep patient covered to preserve body heat
Isaac Amankwaa

Emergency mgt of fractures If the fractured extremity is a leg
bone, the unaffected extremity can be used as a splint by bandaging both legs together.
An arm can be bandaged to the chest or put into a sling to minimize further tissue damage
Assess color, warmth, circulation, and movement (CWCM) of the limb distal to the fracture.
Isaac Amankwaa

Emergency mgt of fractures Open fractures require the
protruding bone be covered with a clean (sterile preferred) dressing.
Do not attempt to “straighten” or realign the fractured extremity. Move the affected limb as little as necessary.
Transport to an emergency department as soon as possible
Isaac Amankwaa

Principles for fracture management The management process is a
three-step process: Reduction—setting the bone; refers
to restoration of the fracture fragments into anatomic position and alignment.
Immobilization—maintains reduction until bone healing occurs
Rehabilitation—regaining normal function of the affected part.
Isaac Amankwaa

Fracture fragments brought into their pre-injury position.
It consists of pulling the broken bone ends to correct alignment and regain continuity.(Bone setting)
Fracture Reduction
Isaac Amankwaa

Reduction is necessary only if there
is some displacement of the
fragment.
It is carried out as soon as possible
to achieve satisfactory alignment
FRACTURE REDUCTION
Isaac Amankwaa

Methods of fracture reduction
Isaac Amankwaa
Includes;1. Closed manipulative
reduction2. Open (Internal )reduction3. Traction

Methods of fracture Reduction
Closed Reduction Minimal manipulation carried out to
bring bone fragments into contact. Afterwards a cast, bandage or splint is
applied to immobilize, support and protect the part.
The procedure may require administration of anesthesia/analgesia
X-rays are taken before and after the procedure to ensure correct alignment
Isaac Amankwaa

Methods of reduction Open reduction
Bone fragments are directly visualized. Internal fixation devices are used to hold
bone fragments in position until solid bone healing occurs
Examples of internal fixation devices include metal pins, wires, screws, plates, nails and rods.
The devices may be removed when bone is healed.
After closure of the wound, splints or casts may be used for additional stabilization and support.
Isaac Amankwaa

Open Reduction
Closed vs. Open ReductionClosed vs. Open Reduction
Isaac Amankwaa

Traction Pulling force applied to accomplish
and maintain reduction and alignment Used for fractures of long bones. Techniques
Skin traction—force applied to the skin using foam rubber, tape.
Skeletal traction-force applied to the bony skeleton directly, using wires, pins, or tongs placed into or through the bone.
Isaac Amankwaa

Immobilization or fixation This follows reduction It involves holding the bone fragments in
correct position and alignment until union has had time to take place.
Immobilization may be accomplished externally with external fixation devices
(e.g. cast, splint, brace), traction, or external fixators; or
internally with metal plates, pins, screws and nails, alone or in combination with bone grafts or prosthetic implants
Isaac Amankwaa

Immobilization or fixation External Fixation
External fixation is a technique of fracture immobilization in which a series of transfixing pins is inserted through bone and attached to a rigid external metal frame.
Isaac Amankwaa

Immobilization or fixation External fixation devices
include: Splint Brace Cast External Fixator Traction Bandage
Isaac Amankwaa

FRACTURES - METHODS FOR MAINTAINING IMMOBILIZATION
Internal devices Nail Plates Screws Wires Rods Metal implants used
for internal fixation serve as internal splints to immobilize the fracture.
Isaac A
mankw
aa

Alignment & Immobilization
External Fixation (advantages)1. Permits rigid support of severely
comminuted open fractures, infected non-unions, and infected unstable joints.
2. Facilitates wound care3. Allows early function of muscles and
joints.4. Allows early patient comfort
Isaac Amankwaa

External fixation The method is
used mainly in the management of open fractures with severe soft-tissue damage.
Common sites include face & jaw, pelvis, fingers.
Isaac Amankwaa

Open Reduction &Internal fixation
The bone ends are realigned (reduced) by direct visualization through a surgical incision (open reduction [OR]).
The bone ends are held in place by internal fixation (IF) devices
Internal fixation devices include metal pins, wires, screws, plates, nails, rods
After closure of the wound, splints or casts may be used for additional stabilization and support.
Isaac Amankwaa

Types of Internal Fixation Devices
Isaac Amankwaa

Open reduction and internal fixation of Comminuted mandibular fracture
Isaac Amankwaa

Differences between Internal fixation and external fixation
Isaac Amankwaa

Immobilization or fixation
Casts Cast is a substance made into a rigid
material to immobilize support and protect a broken bone or correct deformities.
Purpose of cast Immobilization prevention or correction of deformity to realign bone promotion of healing
Isaac Amankwaa

CASTING MATERIALS Non-plaster
Referred to as fiberglass casts, are lighter in weight, stronger, water resistant, and durable.
are porous and therefore diminish skin problems.
Plaster (P.O.P) The traditional cast Rolls of plaster bandage are wet in cool water
and applied smoothly to the body. A crystallizing reaction occurs, and heat is
given off polyester-cotton
Isaac Amankwaa

Types of cast Short arm cast
Extends from below the elbow to the palmar crease
Isaac Amankwaa

Types of cast Long arm cast
Extends from the upper level of the axillary fold to the proximal palmar crease
Isaac Amankwaa

Types of cast Short leg cast
Extends from below the knee to the base of the toes. The foot is flexed at a right angle in a neutral position.
Isaac Amankwaa

Types of cast Long leg cast
Extends from the junction of the upper and middle third of the thigh to the base of the toes. The knee may be slightly flexed
Isaac Amankwaa

SHORT & LONG CASTS
Isaac Amankwaa

BODY / SPICA CASTS
Isaac Amankwaa

POLYESTER/FIBERGLASS

Nursing care of pt in cast
Isaac Amankwaa
The nurse: Keep the cast and extremity elevated Allows a wet cast 24 to 48 hours to dry
(synthetic casts dry in 20 minutes) Handle a wet cast with the palms of the
hand until dry Turn the extremity unless
contraindicated, so that all sides of the wet cast will dry
Heat can be used to dry the cast. The cast will change from a dull to a shiny substance when dry

Nursing care of pt in cast The nurse:
Examine the skin and cast for pressure areas Monitor the extremity for circulatory impairment
such as pain, swelling, discoloration, tingling, numbness, coolness, or diminished pulse
Notify the physician immediately if circulatory compromise occurs
Prepare for bivalving or cutting the cast if circulatory impairment occurs
Petal the cast; maintain smooth edges around the cast to prevent crumbling of the cast material
Monitor the client’s temperature
Isaac Amankwaa

Nursing care of pt in cast The nurse:
Monitor for the presence of a foul odor, which may indicate infection
Monitor drainage and circle the area of drainage on the cast
Monitor for warmth on the cast. Monitor for wet spots, which may indicate a need for drying, or the presence of drainage under the cast
Isaac Amankwaa

Nursing care of pt in cast The Nurse
If an open draining area exists on the affected extremity, a cut-out portion of the cast or a window will be made by the physician
Instruct the client not to stick objects inside the cast
Teach the client to keep the cast clean and dry
Instruct the client on isometric exercises to prevent muscle atrophy
Isaac Amankwaa

Windows maybe cut in dried casts: relieve pressure from abd. distension (body
cast) To prevent “Cast Syndrome” To assess radial pulse (check circulation in a
casted arm) To inspect areas of discomfort or areas of
suspected tissue damage To remove drains or care for wounds
Windowing and Bivalving of cast
Isaac Amankwaa

Bivalving a cast
Isaac Amankwaa

Bivalving a Cast Window Cast
Isaac Amankwaa

Potential complications of cast Hidden bleeding Neurovascular compromise Hidden infection from wound Skin breakdown
Isaac Amankwaa

Other complications of cast
Fat emboli Infection DVT Cast syndrome
Isaac Amankwaa

Traction Traction is the mechanism by
which a steady pull is placed on a part or parts of the body.
Isaac Amankwaa

Purposes of traction
It aligns the ends of a fracture by pulling the limb into a straight position.
It ends muscle spasm. It relieves pain. It takes the pressure off the bone
ends by relaxing the muscle.
Isaac Amankwaa

Terminologies Counter traction. pulling force equal and
opposite the traction weights Traction: is the application of a pulling
force Trapeze: an overhead patient helping
device to promote mobility in bed.
Isaac Amankwaa

Principles of effective traction
Traction must be continuous to be effective
Skeletal traction is never interrupted. Weights are not removed unless
intermittent traction is prescribed. The patient must be in good body
alignment Ropes must be unobstructed Weights must hang free and not rest on
the bed or floorIsaac Amankwaa

Indications for traction
Isaac Amankwaa
To reduce fractures Immobilization of an area
before surgery Control and relieve of painful
muscle spasm stretching adhesions correct deformities

Contraindications Patients with structural diseases
secondary to tumor or infection, Acute strains, sprains and
inflammation conditions Malignancy Aneurysm
Isaac Amankwaa

Types of traction Straight or running traction
applies the pulling force in a straight line with the body part resting on the bed.
E.g. Bucks extension traction
Isaac Amankwaa

Types of traction Balanced suspension traction
supports the affected extremity off the bed and allows for some patient movement without disruption of the line of pull
Isaac Amankwaa

Methods of applying traction Traction may be applied to
the skin (skin traction) or directly to the bony skeleton
(skeletal traction).
Isaac Amankwaa

Skin Traction Application of a pulling force
directly to the skin through the use of strips, boots or foam splints.
Apply traction to underlying bones and other structures (muscles).
It is used temporally due to skin breakdown
Isaac Amankwaa

Forms of skin traction
1. Buck’s traction (buck’s extension)
2. Russel’s traction (balanced traction)
3. Bryant’s traction
Isaac Amankwaa

Buck’s SKIN TRACTION
The traction is exerted by a straight pull on one or both legs.
Can be used to immobilize a limb for a short time (# hip prior to surgery) or reduce muscle spasm
Isaac Amankwaa

Russel’s traction (balanced traction)
Has an additional overhead pulley system with the leg supported by a sling.
The pull is up & toward the foot of the bed.
Isaac Amankwaa

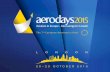
Bryant's Traction
It is used to immobilize a fracture of the femur in children who weigh less than 18.2 kg.
Isaac Amankwaa

Skeletal Traction: Is accomplished by surgically
inserting metal wires or pins thru distal bones to the # site or by anchoring metal tongs in the skull.
A traction bow is attached to wire or pin and traction force is applied .
Used to reduce unstable fractures of long bones
Isaac Amankwaa

• Skeletal traction is performed when • more pulling force is needed, or • when the part of the body needing traction is
positioned so that skin traction is impossible. • It requires the placement of tongs, pins, or screws
into the bone so that the weight is applied directly to the bone.
• This is an invasive procedure that is done in an operating room under general, regional, or local anesthesia
Skeletal traction
Isaac Amankwaa

Comparison of skin and skeletal traction
Skin tractionAdvantage:•Relative ease of use and ability to maintain comfortDisadvantage:•Wt required to maintain Normal body alignment or fracture alignment can not exceed 6 lbs per extremity.
Skeletal tractionAdvantage:–Increases mobility without threatening joint continuity. Easier to change linen, backcare
Disadvantage:
Need to use multiple wts makes client slide in bed more.
Isaac Amankwaa

Bucks
Isaac Amankwaa

Risk associated with skin traction Bone inflammation. Infection can occur at the pin sites. Both types of traction have complications
associated with long periods of immobility: bed sores reduced respiratory function urinary & and circulatory problems occasionally, fractures fail to heal emotional toll of prolonged bedrest Kidney/gallstones
Isaac Amankwaa

Check the four P’s of traction maintenance
Pounds: Inspect traction setup. Is the correct weight in place?
Pull: Is the direction of pull aligned with the long axis of affected bone?
Pulleys: Is the rope gliding smoothly over pulley?
Pressure: Are clamps and connections tight?
Isaac Amankwaa

USUAL PIN SITE CARE With gloves remove gauze dressings from
around pins Inspect sites for drainage or inflammation. Prepare supplies and apply new gloves. Clean each pin site with NaCl by placing sterile
applicator close to the pin and cleaning away from the insertion site. Dispose of applicator.
Continue process for each pin site. Using a sterile applicator, apply a small
amount of topical antibiotic ointment as ordered
Provide pin site care according to hospital policy/ Dr. orders.
Cover with a sterile 2 X 2 split gauze dressing or leave site open to air (OTA) as prescribed
Isaac Amankwaa

More care for traction client Assess level of discomfort and provide
nonpharmacological and pharmacological relief as indicated.
Encourage active and passive exercises and use of unaffected extremities for ADLs.
Encourage use of trapeze bar for repositioning in bed.
Provide a fracture pan for elimination prn
Evaluate effectiveness of care & need for intervention
Isaac Amankwaa

Care of the Client in Traction• When caring for a client in continuous,
balanced, skeletal traction with a Thomas Splint what should the nurse know? Wow, what a question!
• Consider skin, infection, personal care, ROM/exercises
• Care of ropes, pulleys• What to do when transporting
client/bed elsewhere
Isaac Amankwaa

Relieving Pain Initiate activities to prevent or modify pain.
Assist patient with pain-reduction technique, e.g. guided imagery
Immobilize injured part. Position patient in correct alignment. Reposition patient with slow and steady
motion; use additional personnel as needed. Elevate painful extremity to diminish venous
congestion. Apply heat or cold modalities as prescribed.
Heat versus cold is controversial. Modify environment to facilitate rest and
relaxation.Isaac Amankwaa
Related Documents