Mulyanto Basuki

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Mulyanto Basuki

1818
Partnering to protect
Precious Life

1818
Partnering to protect
Precious Life
“Good Partner is Essential”

1818• A history
• Ortho Clinical Diagnostics
• Immunohematology
• Technique and Technology
• Transfusion Medicine
• Screening Antibody
• DAT/DCT
• Identification
• Product
The Agenda
19th Century Blood Banking
1818 James Blundell, Obstetrician
First successful human to human
transfusion…
Only 10 documented
transfusions, 5 were
successful, the others…not so
sucessful…

20th Century Blood Banking
1901 AB Group discovered
1907Importance of crossmatching
blood between donor & recipient
1914Sodium Citrate proposed as
anticoagulant
1936First Blood Bank:
Barcelona, Spanish Civil War
1940 Levine, Rh blood Group System

Ortho Clinical Diagnostics

Ortho Clinical Diagnostics
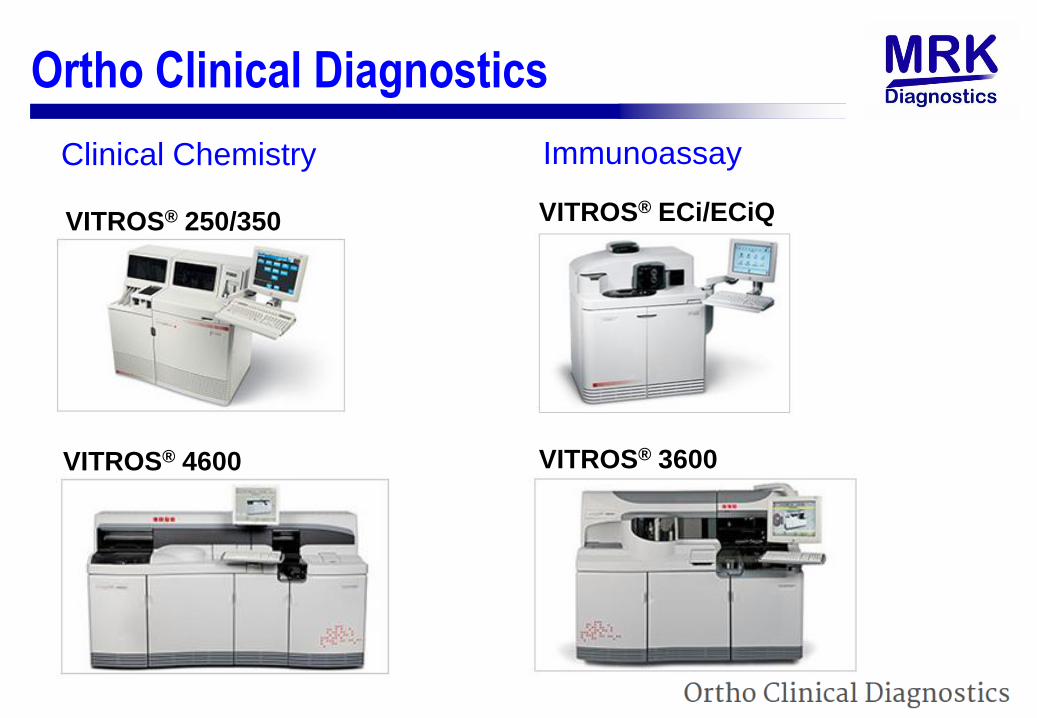
Ortho Clinical Diagnostics
Clinical Chemistry
VITROS® 250/350
VITROS® 4600
Immunoassay
VITROS® ECi/ECiQ
VITROS® 3600

Ortho Clinical Diagnostics
Integrated System
VITROS® 5600
Laboratory Automation SystemenGen®

Ortho Clinical Diagnostics
Immunohematology / Blood Bank
ORTHOTM Workstation ORTHO AutoVue ® Innova

Ortho Clinical Diagnostics
Immunohematology / Blood Bank
ORTHOTM Workstation ORTHO VisionTM

Ortho Clinical Diagnostics
Immunohematology / Blood Bank
ORTHOTM Workstation ORTHO VisionTM MAX

Immunohematology

● Part of hematology
● Antigen – Antibody
● Antigen : Carbohydrate on the surface of Red Blood Cells
● Antibodi : Complex protein moleculs produced in response to antigen.
Natural : Anti-A Antibody, Anti-B antibody.
Unexpected : anti-D
Causes of transfusion reactions
Immunohematology

√ Slide
√ Tabung
√ CAT ( Gel Tes ???? )
Technique and Technology

√ Slide
√ Tabung
√ CAT ( Gel Tes ???? )
Technique and Technology

• Slide & Tiles
√ T
Technique and Technology

• Tube
CAT (
Technique and Technology

• Tube
Technique and Technology

• Microplate
CAT ( Gel Tes ???? )
Technique and Technology

• Microplate
Technique and Technology

• CAT ( Gel Tes ? )
Technique and Technology

• CAT ( Gel Tes ? )
Glass beads dan gel act a sieve
Technique and Technology

So, What does our past tell us ?
• What we are detecting hasn‟t changed…
• As our knowledge increase, and the technology
improves, our testing becomes better. We have
various methods available to us…but there is a
need to standardise our testing method…
• To improve patient safety and the service provided
by laboratories, we need to be up to date with our
skills and testing procedures…errors need to be
reduced…

Transfusion Medicine
Global Trends Continuing need for safe and effective blood supply:
Demand for safe and effective blood supply
Increasing aging population
Growing requirement for operational effectiveness:
Work loads increasing
Economic pressures
Challenges1. Increased demand for better laboratory services
• Workload (multi-tasking), Staffing
2. Increased focus on medical errors and frequency of “near misses”
3. Errors due to result transcription
• Manually record results on file cards, Manually enter into LIS
4. Increased regulatory pressures

UK‟s haemovigilance program (SHOT- Serious Hazards Of
Transfusion) has been monitoring errors related to
transfusion medicine since 1996. In 2011, 98.4% of all NHS
hospitals participated in the program.
“Human error remains the most common cause of Serious Adverse Events. Transfusion teams should be encouraged to consider strategies to minimise the effects of human error by focusing on root causes such as distraction, tiredness and over-familiarity with repetitive tasks.” 2011 SHoT report
Error in the Laboratory
Transfusion Medicine

Benefite using latest technology
Patients :
Safer blood- errors reduced when testing for compatible units.
Laboratory :
Increased safety
Increased capacity- able to do more with less resources.
Improvements in the quality of results
Compliance to best practices
Hospital / Institution :
Enhances the service levels and the reputation of the hospital
as a modern facility, with the latest technology for testing.
Transfusion Medicine
• Reagent red cells used to detect presence/absence ofunexpected antibody in serum/plasma
• Unexpected antibodies• Red blood cell antibodies other than „expected‟ Anti A or Anti B.
• These antibodies are not naturally occurring and are called irregular
antibodies.
• They occur due to immunization either by
- Transfusion / Pregnancy / Transplantation
• Clinically significant antibodies against Rh and other minorblood group system antigens.• Prevent transfusion reaction (acute or delayed)
• Effective transfusion (RBC survival)
• A Key Process in pre-transfusion compatibility testing in bothdonors and recipients
Screening Antibody
Transfusion Medicine

Screening Antibody
• As per literature, the clinical significant unexpected antibodies
can be classified into 3 groups based on their clinical
significance.
• Group 1 : Most clinically significant antibodies : D, C, c, E, e, K, k.
• Group 2 : Fya, Fyb, Jka, Jkb, S, s, Cw, M
• Group 3 : P1, N, Lea, Leb, Lua, Lub, Kpa, Kpb, Jsa, Jsb, Coa, Cob, Dia
• Detection and monitoring of pregnant patiens at risk ofdelivering infants with HDN
• Investigation of potential hemolytic transfusion reactions andimmune hemolytic anemia
• Important for future treatment to know the antibody specificityor specificities
Transfusion Medicine

• Once immunized, more chance to develop more antibodies
• Antibody Screen used to detect antibodies • 2-3 cells are typical
• Additional cells cells may be used for specific antigens (Mia, Dia )
Screening Antibody
Transfusion Medicine

Transfusion – Development of Antibody, Primary response
IgM antibody
Transfusion Medicine

Transfusion – Development of Antibody, Secondary response
IgG antibody
Transfusion Medicine

Pregnancy – Primary Immune Response
Slow response. Predominantly IgM, large in size, cannot cross
placenta. Normally 1st Baby is safe
FMH during pregnancy
Or delivery
Fetal RBC Leak
Transfusion Medicine

Pregnancy – Primary Immune Response
IgM
( First exposure of Rh –ve
women to Rh +ve RBCs )
• Slow ( several weeks )
• Weak
• Predominantly IgM antibodies which do not cross the
placenta
Transfusion Medicine

Fraction of FMH
during
pregnancy
Instant response. Predominantly IgG, small in size, may cross placenta. Cause HDN
Pregnancy – Secondary Immune Response
Transfusion Medicine

Pregnancy – Secondary Immune Response
• Rapid ( 1 day )
• Strong
• Predom. IgG antibodies which cross the placenta
IgG
( Second exposure of Rh –
ve women to fraction of ml
of Rh +ve RBCs)
Transfusion Medicine

Blood Group Antibodies :
• IgM - A, B, H
I
M, N
Lea, Leb
P1
• IgG - Rh
Kell IgG can cross placenta
Duffy Identified in AHG phase
Kidd Reacts at 37◦C
Ss
IgM - Immediate spin phase
Reacts at Room temperature
cannot cross placenta
Transfusion Medicine

Antibody Screening – Recommendations :
Ref : Guidelines for pre-transfusion testing, 4th Edition, 2002
Transfusion Medicine

Antibody Screening – Local Regulation :
Transfusion Medicine
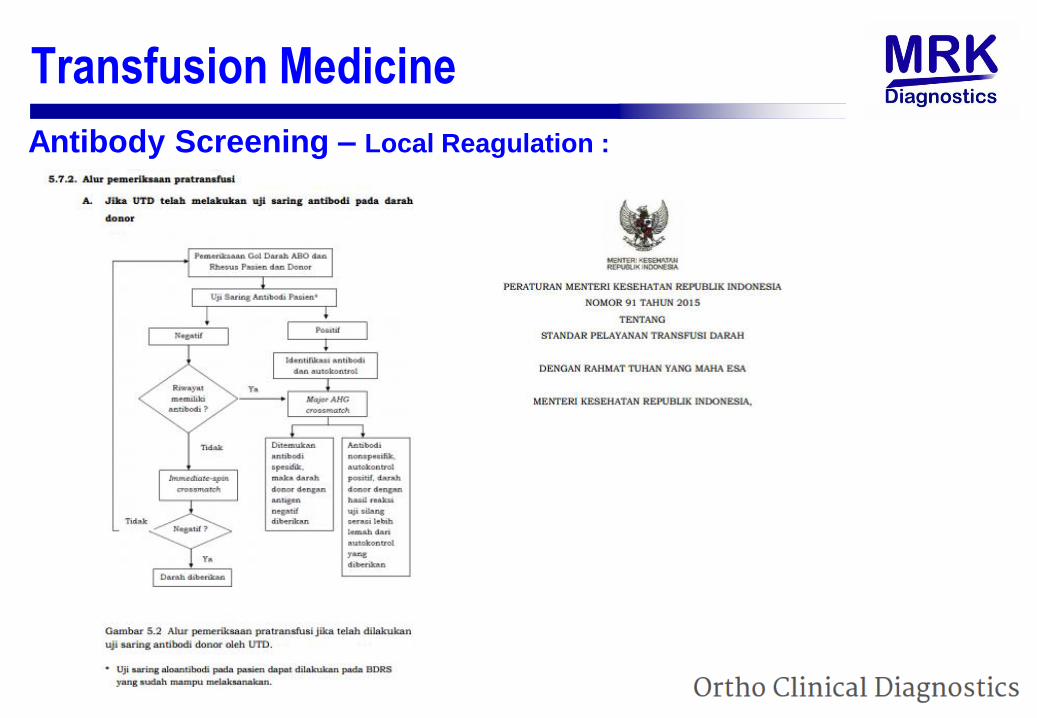
Antibody Screening – Local Reagulation :
Transfusion Medicine
Have you seen this ??
• A patient‟s serum sample was cross matched with three donorcells matching for the ABORh group
• All were compatible
• Yet the patient showed mild transfusion reaction after transfusion
• Cause ??
• The XM units probably did not have the homozygous
expression of antigen against the unexpected Ab in the
patient !
Transfusion Medicine

Transfusion Medicine
DAT* / DCT :
• Direct Antiglobulin test/ Direct Coombs Test.
• Detects antibody bound to the patients red cells
• Aid in detection/diagnosis• AIHA (Autoimmune haemolytic anemia)• HDN (Haemolytic Disease of the Newborn)• Transfusion Reactions
• Detect in vivo RBC sensitization • Immunoglobulins: IgG, IgA, IgM• Complement: C3d
* Previously called Direct Coombs Test

Transfusion Medicine
• Although not always performed in routine pretransfusion testing, a positiveDAT can offer valuable information
• If the patient has been transfused, the patient may have an alloantibody coating the transfused cells
• If the patient has NOT been transfused, the patient may have an autoantibody coating their own cells
DAT* / DCT : What can the DAT / DCT tell us ?

• Reagent red cells used to identify of antibody against RBC Antigen
• Used as a Follow-up test to positive screening antibody Pos
• An important component in the compability testing
• Reagent Red Blood Cells used to detect antibodies
• 10 - 11 cells are typical
Identification Antibody
Transfusion Medicine

* American society of Hematology
Transfusion Medicine

Immunohematology Products
Products
Traditional Reagents
Column
Agglutination
Technology
Automation

Traditional Reagents
Column
Agglutination
Technology
Automation
Products
Immunohematology Products
Antisera
• Anti-A, Anti-B, Anti-AB, Anti-D
• Anti-M, Anti-N, Anti-S, Anti-s, Anti-Lea, Anti Leb
RBC Reagents
• Blood Grouping ( Reverse Testing )
• Screening Antibody
• Identification Antibody
Products

● Column Agglutination Testing
● Glass Bead VS Gel ?
● Ortho Clinical Diagnostics = Glass Beads
● Inkubasi
Glass Beads : 10 menit VS Gel : 15 menit
● Centrifugasi
Glass Beads : 5 menit VS Gel : 10 menit
Products
Cassettes

● Column Agglutination Testing
● Glass Bead VS Gel ?
● Ortho Clinical Diagnostics = Glass Beads
● Inkubasi
Glass Beads : 10 menit VS Gel : 15 menit
● Centrifugasi
Glass Beads : 5 menit VS Gel : 10 menit
Products
Cassettes

● Column Agglutination Testing
● Glass Bead VS Gel ?
● Ortho Clinical Diagnostics = Glass Beads
● Incubation :
Glass Beads : 10 minutes VS Gel : 15 minutes
● Centrifugation :
Glass Beads : 5 minutes VS Gel : 10 minutes
● Blood Grouping
No Incubation required
Products
Cassettes

• 6 Columns, Glass beads
• Antisera
• Objective
• Standardize
• More saver
• Error : minimize
• Manual and Automatic
Products
Cassettes

Products
Reagent Red Blood Cells – Screening AntibodyOrtho Pooled Screening Cells ( 1 Panel )
• 0.8 % and 3 % Suspension
• Group O, HLA Negative, R1r or R2r, Homozygous for Jka, Fya
• Recommended for donor screening only
Surgiscreen ( 3 Panel )
• 0,8 % and 3 %

Products
Reagent Red Blood Cells – Screening Antibody
Selectogen ( 2 Panel )
• 0.8 % and 3 %
• Group O, HLA Negative, Only one cell Kell Posistive, Cell I : R1R1 (CDe
Phenotype ) or R1wR1, Cell II : R2R2 ( cDE Phenotype) , Homozygous for Jka,
Fya

Products
Reagent Red Blood Cells – Screening AntibodySurgiscreen ( 3 Panel )
• 0,8 % and 3 %
• Group O, HLA Negative, One Cell bu NOT ALL 3 Kell Posistive, Cell I : R1R1
(CDe Phenotype ) or R1wR1, Cell II : R2R2 ( cDE Phenotype) , Cell III : rr,
Homozygous for Jka, Jkb , Fya ,Fyb , S, M, Additional Ag ( ie. Mia )

ORTHOTM Workstation
• 2 in 1
• < 11 kG ( 10,89 )
• Integrated : Incubator dan Centrifuge
• Time :
– Cassettes Centrifugation : 5 Minutes ( 2’ : 793 RPM ; 3’ : 1508 RPM )
– Cassette Incubation : 10 MInutes
• Capacity
– Centrifuge : 10 Cassettes
– Incubator : 20 Cassettes ( @ 10 Cassettes )
• 150 VA
• T X P X L = 220 mm X 575 mm X 325 mm
Products

ORTHOTM Workstation
Products

ORTHOTM Workstation
Products

ORTHOTM Workstation
● Blood Grouping
● Crossmatch
● Screening Antibody
● Identification Antibody
● Direct comb test ( Poly and Mono )
● Rhesus phenotyping
Glass Beads :
Products
08158888940 / 085218888940
http://orthoplus.orthoclinical.com
www.transfusionnews.com
www.orthoondemand.com
Related Documents











