Multistakeholder Consultation on Programming to Promote Adolescent Well-Being in the WHO South-East Asia Region 27-28 July 2021 (Virtual) Meeting Report

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Multistakeholder Consultation on Programming to Promote Adolescent Well-Being in the
WHO South-East Asia Region
27-28 July 2021 (Virtual)
Meeting Report
Report of the Multistakeholder Consultation on Programming to Promote Adolescent Well-Being in the WHO South-East Asia Region SEA-CAH-42
© World Health Organization 2021
Some rights reserved. This work is available under the Creative Commons Attribution-Non Commercial-Share Alike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization (http://www.wipo.int/amc/en/mediation/rules/).
Suggested citation Report of Multistakeholder Consultation on Programming to Promote Adolescent Well-Being in the
WHO South-East Asia Region Development. Licence: CC BY-NC-SA 3.0 IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.
SEA-CAH-42
Multistakeholder Consultation on Programming to Promote Adolescent Well-Being in the
WHO South-East Asia Region
27-28 July 2021 (Virtual)
Meeting Report
Contents
Introduction ....................................................................................................................................... 1
Overview ..................................................................................................................................................................................... 1
Context ....................................................................................................................................................................................... 1
Definition of adolescent well-being ............................................................................................................................................ 1
Objectives of the consultation .................................................................................................................................................... 2
Scope and format ....................................................................................................................................................................... 2
Adolescent participation............................................................................................................................................................. 3
Findings from the consultation ........................................................................................................... 3
Reaching consensus on programmatic interventions: priorities across the multiple domains of adolescent well-being ......... 3
Avoiding a siloed approach when designing, implementing, and monitoring adolescent well-being programmes .................. 4
Considerations for monitoring progress towards adolescent well-being................................................................................... 4
How to build the case for investment in adolescent well-being ................................................................................................ 4
How digital technologies could be harnessed to promote adolescent well-being ..................................................................... 5
Capacity building is needed across sectors (health, administration, governance) to improve policies and programmes for adolescent well-being ................................................................................................................................................................. 5
Ensuring inclusivity in the approach to adolescent programming and policy making ............................................................... 5
Gaps in knowledge and challenges in current practices ............................................................................................................. 6
What evidence-based policies and programmes are needed for adolescent well-being? ......................................................... 7
Suggestions and recommendations..................................................................................................... 7
Conclusions .................................................................................................................................. Error! Bookmark not defined.
1 | P a g e
Introduction
Overview
Adolescent well-being is central to the achievement of Sustainable Development Goal (SDG) 3, which aims to “ensure healthy lives and promote well-being for all at all ages”. The United Nations Secretary-General’s Global Strategy for Women’s, Children’s, and Adolescents’ Health (2016–2030), which aims to “ensure health and well-being for every woman, child and adolescent” within the context of the SDGs, recognizes that young people are central to the overall success of the Strategy. Adolescence is a critical period of the life course when many of the factors that contribute to lifelong well-being can learned and adopted for life-long wellbeing.
Until recently, young people’s needs were often overlooked because they fell outside of policies and programmes designed for children or adults, which ignored the specific needs of adolescents in their transition to adulthood. The direct and indirect effects on adolescent well-being of the COVID-19 pandemic and the responses to it have reinforced the importance of systems to support the well-being of adolescents.
Context
The World Health Organization (WHO) Regional Office for South-East Asia has supported the development and implementation of national adolescent health programmes. A regional network of youth groups has been established to build capacity for meaningful adolescent and youth engagement in national adolescent health programmes. Stakeholders in countries in the WHO South-East Asia Region have sufficient experience in adolescent health programming to contribute meaningfully to the regional consultation on global adolescent well-being initiative. Consultations have been planned as part of the Adolescent Well-Being Initiative, led by the UN H6+ Technical Working Group on Adolescent Health and Well-Being.
It is envisaged that the regional consultations will help identify gaps in knowledge and inform the development of the next version of the “Global Accelerated Action for the Health of Adolescents (AA-HA!): Guidance to Support Country Implementation” and a collection of articles to be published in The BMJ on programming to promote adolescent well-being. These activities will form part of the build-up to a Global Summit on Adolescent Well-Being, planned for autumn 2023. They will also become a comprehensive resource informing the design of a multisectoral response to promote adolescent well-being.
Definition of adolescent well-being
Adolescent well-being is defined1 as a situation in which “adolescents thrive and are able to achieve their full potential”. The expanded definition is a situation in which they “have the support, confidence and resources to thrive in contexts of secure and healthy relationships, realizing their full potential and rights”.
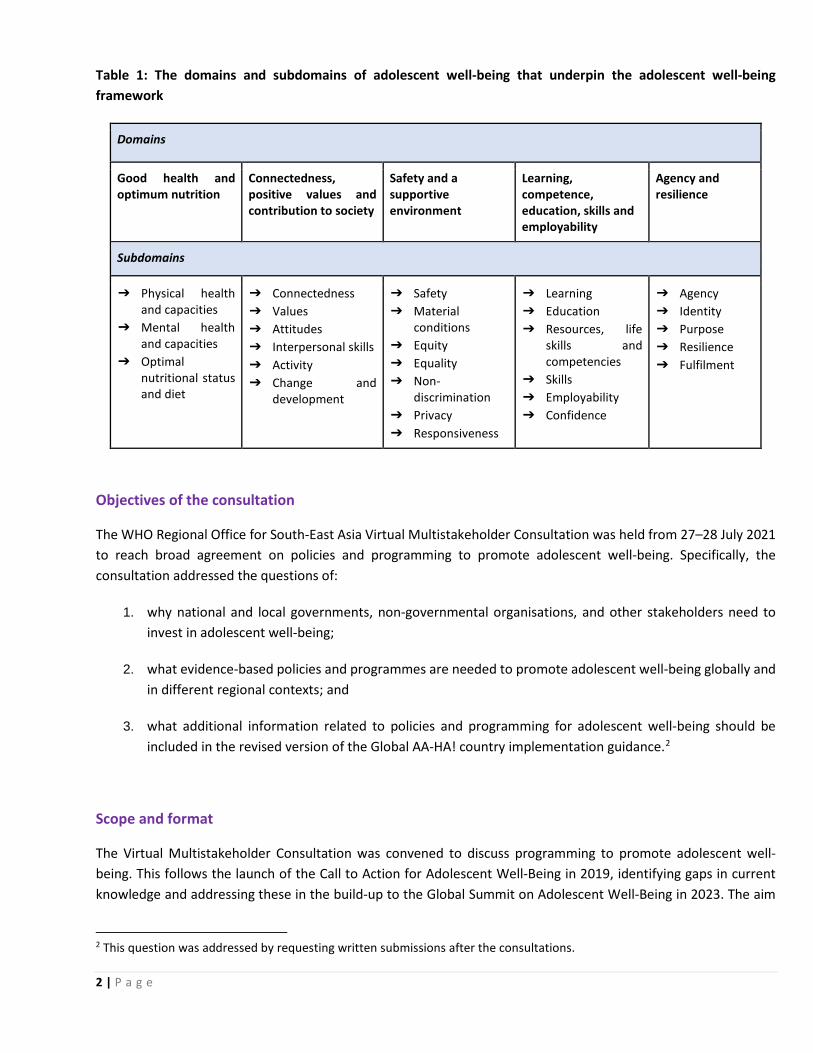
This definition has been further expanded according to a conceptual framework which includes five interconnected domains of adolescent well-being, and which sets out the requirements for supporting adolescents to achieve well-being within each domain (see Table 1).
1 Ross DA, Hinton R, Melles-Brewer M, Engel D, Zeck W, Fagan L et al. Commentary: Adolescent well-being: A definition and conceptual framework. J Adolescent Health 2020;67:472–476.
2 | P a g e
Table 1: The domains and subdomains of adolescent well-being that underpin the adolescent well-being framework
Domains
Good health and optimum nutrition
Connectedness, positive values and contribution to society
Safety and a supportive environment
Learning, competence, education, skills and employability
Agency and resilience
Subdomains
➔ Physical health and capacities
➔ Mental health and capacities
➔ Optimal nutritional status and diet
➔ Connectedness ➔ Values ➔ Attitudes ➔ Interpersonal skills ➔ Activity ➔ Change and
development
➔ Safety ➔ Material
conditions ➔ Equity ➔ Equality ➔ Non-
discrimination ➔ Privacy ➔ Responsiveness
➔ Learning ➔ Education ➔ Resources, life
skills and competencies
➔ Skills ➔ Employability ➔ Confidence
➔ Agency ➔ Identity ➔ Purpose ➔ Resilience ➔ Fulfilment
Objectives of the consultation
The WHO Regional Office for South-East Asia Virtual Multistakeholder Consultation was held from 27–28 July 2021 to reach broad agreement on policies and programming to promote adolescent well-being. Specifically, the consultation addressed the questions of:
1. why national and local governments, non-governmental organisations, and other stakeholders need to invest in adolescent well-being;
2. what evidence-based policies and programmes are needed to promote adolescent well-being globally and in different regional contexts; and
3. what additional information related to policies and programming for adolescent well-being should be included in the revised version of the Global AA-HA! country implementation guidance.2
Scope and format
The Virtual Multistakeholder Consultation was convened to discuss programming to promote adolescent well-being. This follows the launch of the Call to Action for Adolescent Well-Being in 2019, identifying gaps in current knowledge and addressing these in the build-up to the Global Summit on Adolescent Well-Being in 2023. The aim
2 This question was addressed by requesting written submissions after the consultations.
3 | P a g e
of the consultation is to make a strong case to countries and partners for enhanced and continued investment in adolescent well-being. The two-day consultation included discussions and recommendations on various aspects of adolescent well-being, as well as the nature of interventions and programming that need to be adopted or developed in the South-East Asia Region.
The consultation was attended by over 150 stakeholders, including adolescents, young people and representatives of national and local governments, UN agencies, NGOs (including youth-led and youth-serving organizations), academics, funders, and professional associations. There was diverse representation across genders, age groups and fields of expertise across all five domains of adolescent well-being (see Table 1).
Adolescent participation
The consultation included significant participation by adolescents in line with the current thinking of the importance of including adolescents more centrally to achieve universal health coverage as highlighted in the 2019 publication “Adolescent Health: The Missing Population in Universal Health Coverage”. The principles of meaningful adolescent and youth engagement were adopted as an inclusive, intentional, mutually respectful partnership between adolescents, youths, and adults to ensure that their contributions are valued, and their ideas, perspectives are integrated into the consultation.
Findings from the consultation
The Global AA-HA! country implementation guidance emphasizes that investment in adolescent health yields a triple dividend of benefits: improving health and well-being now, enhancing it throughout the life course, and contributing to the health and well-being of future generations. This consultation helped identify gaps in current knowledge and will inform the development of the next version of the AA-HA! guidance, as well the Adolescent Well-Being Framework. The consultation highlighted that prioritizing adolescent well-being needs to be adopted through a top-down approach: reflected in the policy and programming of governmental institutions and using a multisectoral approach.
Reaching consensus on programmatic interventions: priorities across the multiple domains of adolescent well-being
Stakeholders across sectors need to reach consensus among the multiple domains of adolescent well-being through the setting of priorities. Priorities can be identified from local evidence, such as needs assessments, landscape analyses, national surveys, situational analyses and baseline and end line surveys. The process of prioritization should begin by considering existing plans and strategies and discussing them at the national level to reach agreement on the indicators of adolescent well-being across the five domains. Reaching consensus through multisectoral engagement with key stakeholders is essential while developing policies and programmes.
Priority areas revealed during the consultation include comprehensive sexuality education, life skills education and adolescent-friendly health services. Crucial actors who need to be brought to the table are ministries of finance and planning, local civil society organizations, youth representatives and government bureaus of statistics, planning, health, and education. It is essential that inclusion and diversity form the foundation of these processes, which highlights the need to include out-of-school and unmarried adolescents, women, children, and young people from marginalized communities.
4 | P a g e
Avoiding a siloed approach when designing, implementing, and monitoring adolescent well-being programmes
To avoid a siloed approach, we need to consider which mechanisms will ensure coordination and coherence across sectors. Engagement at national and subnational levels is required by, for example, by strengthening existing committees at district and subdistrict levels and using existing platforms and networks for appropriate coordination.
Another aspect requiring consideration is the allocation of budgets across sectors. There is already strong evidence for investing in adolescent health, and the case for improved financial (re)allocations can be encouraged through strong partnerships with governmental institutions (planning offices, ministries of finance, prime minister’s office etc.) The cost-effectiveness of any proposed intervention can be reviewed using data and evidence from local and regional contexts. While adopting a multisectoral approach, there should be one coordinating authority that builds the capacities of other sectors, takes on or delegates crucial roles and volume of work, and ensures accountability.
There are many ways to encourage multisectoral engagement of relevant stakeholders. While advocating for investment in adolescent health and well-being, one approach is to highlight the benefits that investing in adolescent health brings to stakeholders’ own work. By taking a non-siloed approach, the availability of and access to resources can be maximized, demonstrating the far-reaching benefits of investing in adolescent health and wellbeing. It is also recommended that multisectoral engagement should involve a bottoms-up approach focusing on the experiences and involvement of adolescents and young people as they are the primary stakeholders. By involving adolescents their felt needs and preferences can also be accurately mapped.
Considerations for monitoring progress towards adolescent well-being
Domain-specific indicators are necessary, with a data entry system at subnational or subdistrict level and an information management system. This can be used by various levels of government. Critical indicators for all five domains need to be validated and used at district level. The capacity of national information systems in different sectors would vary from country to country and could be used by national or international organizations.
Involving adolescents in monitoring and evaluation involves asking them about their own perception of well-being. The engagement of an adolescent resource group at the national level is recommended. There is an urgent need to establish an Adolescent Secretariat, or resource group, with focal points in various sectors, to monitor data.
How to build the case for investment in adolescent well-being
A thriving adolescent population fuels economic growth, helping to increase productivity, decrease health expenditure and reduce inequities across generations. Physical and mental health, learning, sexual maturation and the connectedness, safety, and supportiveness of the community context in which the adolescent matures are all interlinked. Some of these aspects of health and growth during adolescence affect maternal health during pregnancy, which is essential for providing a healthy start to life. These linkages, both within and across generations, are of vital importance. Given this complex mosaic of influences and interactions, the approach to adolescent health and well-being must be both holistic and multidimensional.
Currently, in the WHO South-East Asia Region, all countries (except DPR Korea) have adolescent health policies, strategies and programmes. School health programmes, adolescent-friendly health services and adolescent nutrition programmes are good examples of government initiatives.
5 | P a g e
Constituencies for adolescent well-being need to be built, including community partnerships, civil society organizations and youth voices that engage with national and subnational governments. Current investments and budget allocations at national and subnational levels of adolescent programming need to be reviewed. Specific measures are required for comprehensive, multisectoral investments. Existing laws that are inconsistent with current policies and act as roadblocks to adolescent well-being (E.g. sexual and reproductive health and rights) also need to be changed. Countries need to develop legislative and regulatory strategies to support a protective environment for adolescent health and wellbeing and to counter the negative commercial determinants like promotion of tobacco and alcohol use, unhealthy food, unethical beauty and social media influences.
How digital technologies could be harnessed to promote adolescent well-being
In the context of the COVID-19 pandemic and associated mobility restrictions, young people are relying more than ever on digital platforms to interact with each other, accessing information on health and peer-to-peer interventions. Owing to the digital divide, COVID-19 has exacerbated inequalities because many services and learning interventions are being provided only through digital channels.
For addressing the digital inequity during and beyond the pandemic enhanced connectivity is required for improving adolescents’ access to digital technologies. Public funding needs to be increased and directed to improving and increasing overall connectivity infrastructure. Greater and more equitable access to devices for adolescents and young people must also be prioritized, together with digital literacy education policies for adolescents and parents/guardians. Digital platforms that provide high-quality content and reliable information need to be developed while keeping in mind the diversity of language. Age-appropriate and youth-friendly content is also needed. When designing and/or developing digital platform content, neuroplasticity and adolescent cognitive development, and its association with risk taking and impulsivity, must be kept in mind. Depending on the context and the internet and technology penetration rate, it has been recommended that blended learning approaches (online and offline) are adopted in education systems, rather than a complete switch to digital technologies.
Capacity building is needed across sectors (health, administration, governance) to improve policies and programmes for adolescent well-being
The consultation highlighted the need to promote capacity building for effective policy making and programming. It also revealed a need for sustained advocacy at all levels for sustaining the initiatives and augmenting further expansion. Increasing awareness and skill building among adolescents and young people about the common adolescent health issues, are also required.
Professionals in the relevant sectors need to be trained on the how’s and why’s of working with young people. The areas that require special attention include vulnerable populations, reduction of stigma and discrimination, treatment of young people as young adults with agency, dealing appropriately with social norms, barriers, myths, and misconceptions. It is important to empower adolescents to talk and to question existing practices. Parent/guardian partnerships need to be brought into the fold as well, where they can be sensitized to the situations and aspirations of young people.
Ensuring inclusivity in the approach to adolescent programming and policy making
It is imperative to engage and serve subpopulations previously left out of account. Usage of services by marginalized and vulnerable sections tends to be low due to gaps in availability and accessibility. These services should cater to
6 | P a g e
all youth populations while also prioritizing customizability and accessibility based on contextual needs. Adolescents need to be made aware of available services, and a rights-based approach must be adopted when working with adolescents to ensure wider coverage and utilization. Creating more awareness of and understanding about available services can enhance access to them.
Services must continue to be redesigned according to the needs and perspectives of adolescents. Requirements include friendly infrastructure, convenient timing, engaging demand generators from young people, ensuring privacy, approachable service providers, easy access, and trained human resources. Systemic change is also required to make clear that adolescent health services not only treat illness and malnutrition, but can also provide information on sexual and reproductive health, mental health, emotional support etc. For example, access to sexual and reproductive health information and services is a right for all adolescents and vulnerable populations, especially the LGBTQIA+ community and people with disability.
Gaps in knowledge and challenges in current practices
The consultation revealed some key gaps in knowledge and some persistent challenges affecting programme and policy implementation in the WHO South-East Asia Region.
Stronger coordination between stakeholders is required as there are competing priorities on which consensus has not been reached. This is exacerbated by insufficient prioritization of adolescent health programming and inadequate allocation of financial and other resources for policy, strategy, and programme implementation. The health sector needs structural improvements to enable the promotion of adolescent health and well-being, being understaffed and with existing resources being stretched thin. For example, studies and research are not up-to-date or comprehensive enough to address contemporary challenges.
Challenges in pushing programming forward are increased by lack of support from stakeholders with their own priorities and mandates and amplified by a fragmented and sector-specific approach. Some countries’ legal frameworks and policies are mutually contradictory, with different sectors having incompatible requirements, such as compulsory school education policies that conflict with labour laws. Privatization without multisectoral support risks increasing inequalities across health and education. In addition, political instability further undermines policy and programmatic progress.
There is also a lack of adolescent-friendly health services across the various adolescent health domains. The importance of certain adolescent health issues over others are country or context specific. However, certain adolescent health priorities have received inadequate attention across countries of the Region. For example, sexual and reproductive health is insufficiently prioritized and there are too few trained counsellors and health workers to meet current needs. Another example is prevention and treatment of noncommunicable diseases among adolescents: these are often addressed too late, with interventions typically starting only at 30 years, rather than at a younger age.
COVID-19 has changed the way in which adolescents access health services and information: digital technologies have assumed greater importance as a delivery channel. However, limited, or weak infrastructure and low internet penetration rates have hindered access in many places. Due to the digital divide, digital platforms are leaving the least connected adolescents behind, especially the marginalized and vulnerable young people whose need of these services is higher. Even for those who are connected, lack of linguistic diversity and the limited number of reliable digital platforms reduce learning opportunities and access to appropriate services.
7 | P a g e
While efforts have been made to include adolescents and young people, lack of meaningful youth engagement has been a recurring theme in planning processes. Adolescents are often poorly represented in political decision-making processes. Furthermore, adolescents are often targeted as consumers by alcohol and tobacco companies. Finally, there is insufficient investment in building adolescents’ capacity to become civically engaged.
It is necessary to encourage the development of monitoring frameworks, data-driven decision-making, collaboration, and accountability. Lack of comprehensive monitoring and evaluation frameworks also make it difficult to measure the impact of policy investment and hold governmental stakeholders accountable. There is also a lack of systemic mechanisms from governments to monitor programmes for adolescents, such as adolescent-friendly health services. Critical indicators of real-time progress, success and impact are also often unavailable.
What evidence-based policies and programmes are needed for adolescent well-being?
Effective advocacy for adolescent and youth well-being requires, not only evidence-based policy and programming, but also specific types of evidence backing contextual requirements. The consultation revealed a significant need for advocacy tools and policy briefs tailored to local contexts, especially briefs that link adolescent well-being to a post-COVID reprioritization. Policy analysis is needed at the national and subnational levels, to be made available and accessible to stakeholders, from regional to grass-roots players. Providing strong local evidence on potential governmental interventions suggests the need for academic collaboration, with academics playing an important role in research and converting recommendations into actionable plans. Evidence-based research is needed on successes and failures of interventions for adolescent well-being at subnational and local levels.
Stakeholders need to assess their thematic/sector/field specific value addition while integrating adolescent and their experiences into their advocacy plans. Ministries must have strategies for cross-sectoral interventions and plans for how multiple sectors can come together, for example by intersectoral collaboration between education, youth, and sports ministries. Furthermore, dialogue with ministries of finance and parliamentary health committees (for example) should highlight the dividends from investing in adolescent well-being, which points to a need for cost–benefit analyses, include return on investment.
Policymakers must be oriented towards and made aware of the importance of well-being, such as pre-sensitization regarding adolescent health, prior to key events. Informed by global guidance on convergent action, there is a requirement for implementation plans and specific goals for adolescent well-being, such as targets for adolescent health like those in the SDG targets for maternal health, child health and family planning.
Suggestions and recommendations The foremost priority is to enhance the meaningful engagement of adolescents and young people in national programmes. Environments must be created which are conducive to high-quality engagement, for example by developing platforms for young people to voice their opinions and encouraging participation. Adolescents also need to be provided with appropriate and consistent support and resources. This can be achieved by funding youth programmes and interventions, providing direction and organizational support to youth-led organizations, and building their capacities to assume leadership roles. Structural barriers and sociocultural and environmental determinants of health affecting vulnerable adolescent groups need to be further investigated through suitable research. Overall, more investment is needed in young people and youth-led initiatives, especially those working at the grass-roots level in low-priority areas.

8 | P a g e
The pandemic has also revealed the importance of digital technologies for emergency preparedness and response. It is essential to address inequities (e.g. socioeconomic, gender and digital divides) and to increase public funding to improve connectivity infrastructures. In the policy environment, strengthening policies for online safety and digital literacy education will achieve long-lasting positive impacts, and involving adolescents and young people in the design, implementation and monitoring of digital platforms will improve functionality and access.
Another recurring theme of the consultation was improving training and awareness within the adolescent health sector. Health workers need better information about and capacity-building for working with adolescents, especially the vulnerable. Properly funded and comprehensive training programmes need to be created for implementers, focusing on a practical approach. Advocacy skills among both programme planners and adolescents also need to be strengthened. Addressing stigma and discrimination in different settings, including health care, is an essential requirement and should form the foundation of every programme.
Data mapping and resource mapping are needed to identify resources and strengths in communities to enable better service delivery. Stronger evidence and data disaggregated for different cultures/regions/groups allows for focused advocacy and successful implementation. One suggestion is to compile a list of core indicators that measure adolescent well-being, including both objective and subjective indicators, and to operationalize and validate those indicators in specific country contexts. Different countries make different ministries responsible for young people, and it is important that the presidential or prime ministerial office supports these efforts. Gathering relevant information will remain challenging until standard list of indicators is shared with stakeholders in ministries and agencies other than health. In order to enhance work already being done by different ministries, collaboration, harmonization, and strong leadership are required.
Structural barriers and the sociocultural and environmental determinants of health of vulnerable adolescent groups need to be further investigated through detailed research. This requires an inclusive policy, which goes beyond just adding different vulnerable groups. Policies need to be revisited to ensure that implementation strategies in each country are appropriate and that existing policies are inclusive. Policies need to be designed with indicators and targets to ensure that programmes are delivered to the intended beneficiaries while also ensuring meaningful engagement by vulnerable adolescents. Education curricula need to be reviewed to ensure that they all include adolescent health and gender sensitization. The H6+, PMNCH and partners should work with representatives of diverse youth populations – from rural and urban areas, married and unmarried, in- and out-of-school young people – and give them greater visibility.
Conclusion This virtual consultation yielded valuable insights and feedback from a diverse set of players in adolescent health, especially youth representatives who actively engaged to promote inclusivity and holistic interventions. These insights will represent regional contributions to the global process in preparation for the 2023 Global Summit. Participants of this consultation especially the government delegates and youth networks were urged to join the Call To Action for Adolescent Well-being. The delegates were requested to participate in the e-survey to provide feedback for the next iteration of the Global AA-HA! guidance.
Overall, the consultation bolstered efforts to promote and advance adolescent health and well-being in the region and gave stakeholders the opportunity to initiate or continue collaborative efforts to strengthen the national programme in their respective countries.
9 | P a g e
ANNEXES
10 | P a g e
Annex-1: Tentative Programme
Day 1: 27 July 2021
• Welcome remarks and Objectives • Perspectives of young people • Regional overview of AH and methodology of the consultation
Session 1
• Introduction to the Global Call to Action and adolescent wellbeing initiatives • Meaningful Adolescent and Youth Engagement
Session 2: Groupwork
• Introduction to the groupwork • Groupwork: 7 Groups in Breakout Rooms
1. Multisectoral approach to design, implement & monitor adolescent well-being 2. Investment case for promotion of adolescent well-being: 3. Digital technologies to promote adolescent well-being: 4. Monitoring progress towards adolescent well-being: 5. Capacity building needed to improve polices & programmes for AWB: 6. Ensuring inclusive approach – bringing in the left out 7. Implication for AWB during the pandemic and emergencies:
DAY 2: 28 July 2021
Session 3 • Presentations on the outcomes of the working groups
Session 4
• Service delivery channels for adolescent wellbeing interventions
Session 5
• Way forward • Guiding Questions for discussion: 60 Min
1- What are the most important barriers to operationalization of the adolescent well-being definition and conceptual framework within the SE Asia Region? • What can be done to overcome these barriers?
2- What are the most important gaps in what countries in the SE Asia Region and other stakeholders will want to know to make commitments to increase their investment in adolescent well-being at the Global Summit in 2023?
Session 6: Closing
11 | P a g e
Annex-2: List of Participants Government delegates
Bangladesh
1. Dr. Md. Sabizur Rahman Program Manager, Adolescent and School Health program, MNC&AH Directorate General of Health Services Email: [email protected]
2. Dr. Manjur Hossain Deputy Program Manager of Adolescent Health, MCH Service Unit Directorate General of Family Planning Email: [email protected]
3. Dr. Md. Jaynal Haque Program Manager-Adolescent and Reproductive Health MCH Services Unit Directorate General of Family Planning Email: [email protected]
4. Mr. Khadiza Begum Additional Secretary (Admin & Film) Ministry of Information and Broadcasting Dhaka, Bangladesh Email: [email protected]
5. Dr Hasan Shahriar Kabir Director (Chittagong Division) The Directorate General of Health Services Dhaka, Bangladesh Email: [email protected]
6. Mr. Md. Sadekul Islam Deputy Secretary (WH-l) Health System Department (HSD) Ministry of Health and Family Welfare (MoHFW) Dhaka, Bangladesh Email: [email protected]
7. Mr. Nazma Begum Deputy Secretary Ministry of Youth & Sports, Dhaka, Bangladesh Email: [email protected]
Bhutan
8. Dr. Sonam Wangchuk Deputy Chief Program Officer High Priority Districts (HPD)
Department of Public Health (DoPH) Ministry of Health Email: [email protected]
9. Dr. Chimmi Dem
Senior Program Officer Non-Communicable Diseases Division (NCDD) Department of Public Health (DoPH) Ministry of Health Email: [email protected]
10. Dr Hari Prasad Pokhrel Senior Program Officer Non-Communicable Diseases Division (NCDD) Department of Public Health (DoPH) Ministry of Health Email: [email protected]
11. Dr Dil Kumar Subba Program Officer Non-Communicable Diseases Division (NCDD) Department of Public Health (DoPH) Ministry of Health Email: [email protected]
12. Dr Yeshey Pelden Assistant Program Officer High Priority Districts (HPD) Department of Public Health (DoPH) Ministry of Health Email: [email protected]
13. Mr Karma Wangchuk Chief Program Officer School Health and Nutrition Division (SHND) Department of School Education (DSE) Ministry of Education Email: [email protected]
14. Mr Choening Sherab Deputy Chief Program Officer School Health and Nutrition Division (SHND) Department of School Education (DSE) Ministry of Education Email: [email protected]
15. Mrs Reena Thapa Chief Counsellor Career Education & Counselling Division (CECD) Department of Youth and Sports (DYS)
12 | P a g e
Ministry of Education [email protected]
India
16. Dr Zoya Ali Rizvi Deputy Commissioner (AH) Ministry of Health and Family Welfare Nirman Bhawan New Delhi Email: [email protected]
17. Mr Sujeet Nath Charan Section Officer (International Health), Ministry of Health and Family Welfare, Government of India, R.No. 648, A-Wing, Nirman Bhavan, Maulana Azad Road, New Delhi, India - 110 011
Indonesia 18. Dr Dessy Rosmelita
Secretary General Indonesia anti-doping agency Ministry of Youth and Sports Email: [email protected]
19. drg Wara Pertiwi Osing, MA Deputy Director for School-Age and Adolescent Health Ministry of Health Republic of Indonesia Jakarta, Indonesia Email: [email protected]
20. Dr Utary Rezki Sakinah, SKM Title: Staff for Deputi of Health Quality Improvement and Population Development Coordinating Ministry for Human Development and Cultural Affairs Email: [email protected]
Nepal
21. Dr Tara Nath Pokharel Director Family Welfare Division Department of Health Services Ministry of Health and Population Email: [email protected]
22. Mr Dipendra Paudel Under Secretary, Policy, Planning, Monitoring & Evaluation Division Ministry of Labour, Employment and Social Security Email: [email protected]
23. Mr Rajesh Gautam Section Officer Ministry of Youth and Sports Email: [email protected]
Sri Lanka
24. Ms Jalinie Suriyaarachchi Assistant Director Ministry of Youth & Sports Email: [email protected]
25. Ms. Nadeeka Dharmadasa Deputy Director (Services) Department of Social Services, State Ministry of Primary Health Care, Epidemics and COVID Disease Control Email: [email protected]
26. Dr Deepa Saranajeewa Director Youth elderly & disabled Ministry of Health Email: [email protected] [email protected]
27. Ms Kamani Gunarathna Director of Education School Health & Nutrition Branch Ministry of Education Colombo Sri Lanka Email: [email protected]; [email protected]
28. Dr Ayesha Lokubalasooruya CCP/School Health FHB Sri Lanka Email: [email protected]
29. Mrs Jalani Sooriyaarachchi Assistant Director Ministry of Youth & Sports Sri Lanka Email: [email protected]
30. Dr Anoma Basnayake Consultant Community Physician (CCP) Nutrition Division Ministry of Health Sri Lanka Email: anomamb@ gmail.com
Adolescents and Youth representatives
31. Ms Ayeshwini Lama Core Member Y-PEER AP Center Email: [email protected]
13 | P a g e
32. Ms Pelden Lhamo Member YPEER Bhutan Email: [email protected]
33. Mr Tshewang dorji Member YPEER Bhutan (Sherubtshe Y-PEER Unit) Bhutan Email: [email protected]
34. Mr Shikhar Gupta Youth Health Ambassador HRIDAY India Email: [email protected]
35. Ms Naayaa Mehta Deputy Social Initiatives & Projects, TSRS Moulsari, Gurugram India Email: [email protected]
36. Ms Arunida Khumukcham Member Ya_All, Youth LEAD India Email: [email protected]
37. Ms. Diksha Verma Campaign Volunteer Me for Myself Campaign on Mental Health (M4M) India Email: [email protected]
38. Ms Ikka Noviyanti Advocacy Officer Youth LEAD Indonesia Email: [email protected]
39. Ms Simrin Kafle Program Coordinator Nepal Development Society Nepal Email: [email protected]
40. Ms Pooja Kunwar Board Member of YL Youth LEAD Nepal Email: [email protected]
41. Ms Situ Shrestha Core Member Me for Myself Campaign on Mental
Health (M4M) Nepal Email: [email protected]
42. Ms. Prapti Dhodari Volunteer Y-PEER Nepal Nepal Email: [email protected]
43. Ms Sasanka Sandamali Project Head Youth Action Network Sri Lanka Sri Lanka Email: [email protected]
44. Mr Kaushal Ranasinghe Director Youth for Tomorrow Sri Lanka Email: [email protected]
45. Ms Mahiska Dias Core Volunteer Me for Myself Campaign on Mental Health (M4M) Sri Lanka Email: [email protected]
46. Ms Sangeet Kayastha Coordinator Y-PEER APC Thailand/Nepal Email: [email protected]
47. Mr Abhinav Pandey Stepping Towards Policy Enhancement (STEP) India Email: [email protected]
48. Ms Ragini Bordoloi Policy advocacy Stepping Towards Policy Enhancement Sexual & Reproductive Health and Rights Assam, India Email: [email protected]
49. Mr Suhail Mohd Stepping Towards Policy Enhancement Karnataka, India Email: [email protected]
50. Ms Amita Singh Stepping Towards Policy Enhancement Odisha, India Email: [email protected]
14 | P a g e
51. Ms Zuhra Program and organizational management Aliansi Remaja Independen (ARI) Indonesia Email: [email protected]
52. Ms Phyu Nwe Win Colourful Girls Myanmar Email: [email protected]
53. Ms Shilpa Lamichane Visible Impact Nepal Email: [email protected]
54. Ms Shelani Palihawadana YAN-SL Sri Lanka Email: [email protected]
55. Mr Jose de Jesus MAHON Timor-Leste Email: [email protected]
56. Mr Mohammed Shahriar Habib Campaign Volunteer Me for Myself Campaign on Mental Health (M4M) Bangladesh Email: [email protected]
Experts
57. Dr. Fariha Haseen, Associate Professor Department of Public Health and Informatics Bangabandhu Sheikh Mujib Medical University Dhaka, Bangladesh Email: [email protected]
58. Dr Shamima Chowdhury Free LancerConsultant Dhaka, Bangladesh Email: [email protected]
59. Dr Swati Bhave Adolescent Pediatrics Consultant Head of Adolescent Clinic Jahangir Hospital Pune, India Email: [email protected]
60. Prof. Monika Arora Director of Health Promotion Division Public Health Foundation of India (PHFI) India Email: [email protected]
61. Dr Om Sai Child Psychiatrist LHMC New Delhi, India Email: [email protected]
62. Dr Swati Ghate Pediatrician and member of IAP Adolescent Health Academy India Email: [email protected]
63. Dr Tanu Anand Public Health Specialist Indian Council of Medical Research (ICMR) New Delhi, India Email: [email protected] ‘
64. Ms Vijay Luxmi Bose Senior Health Communication Specialist New Delhi, India Email: [email protected]
65. Anastasia Satriyo Child and adolescent Psychologist, Jakarta Development Centre Email: [email protected]
66. Dr Nendra Primonik Rengganis Chief Executive Officer (CEO) Konten Baik Indonesia Email: [email protected]
UNICEF 67. Michelle Dynes
Health Section UNICEF East Asia and Pacific Regional Office Email: [email protected]
68. Ms Paba Dharshini Seneviratne Regional Adviser for Adolescent Development and Participation (ADAP) UNICEF Regional Office for South Asia Email: [email protected]
69. Ms Maha Elaine Muna Regional Advisor for Gender UNICEF Regional Office for South Asia Email: [email protected]
15 | P a g e
70. Ms Afrika Mukaneto Consultant U Report South Asia, Adolescent Development and Participation (ADAP) section, UNICEF-ROSA Email: [email protected]
71. Dr Adriana Rietsema Manager, Health UNICEF Regional Office for South Asia Email: [email protected]
72. Dr Syed Hubbe Ali Health Specialist United Nations Children’s Fund (UNICEF) New Delhi India Email: [email protected]
73. Dr Praina Koul National Adolescent Consultant United Nations Children’s Fund (UNICEF) New Delhi – 110 003 Email: [email protected]
74. Dr Ticiana Garcia-Tapia Youth & Adolescent Develop. Specialist United Nations Children’s Fund (UNICEF) Indonesia Email: [email protected]
75. Dr Artha Camellia Health Specialist United Nations Children’s Fund (UNICEF) Indonesia Email: [email protected]
76. Dr Martha Gercelina Silaen Health Officer United Nations Children’s Fund (UNICEF) Indonesia Email: [email protected]
77. Mr. Ghanshyam Kandel UNICEF- NEPAL Email: [email protected]
78. Ms Pragya Shah Karki Child Protection UNICEF-NEPAL Email: [email protected]
79. Mr. Naveen Poudyal Nutrition
UNICEF-NEPAL Email: [email protected]>
80. Ms. Purnima Gurung Education UNICEF-NEPAL Email: [email protected]
UNFPA
81. Dr Jo Sauvarin, Adviser on Adolescents and Youth, UNFPA APRO Email: [email protected]
82. Ms Maki Akiyama UNFPA APRO Email: [email protected]
83. Dr. Muhammad Munir Hussain, Programme analyst A&Y, UNFPA Bangladesh Email: [email protected]
84. Ms Iliza Azyei, Programme specialist A&Y, UNFPA Bangladesh Email: [email protected]
85. Dr Jigme Choden, Consultant, Youth, and Gender UNFPA Bhutan Email: [email protected]
86. Dr Ugyen Thinley, Program and Admin Associate UNFPA Bhutan Email: [email protected]
87. Ms Ankita Singh Programme analyst Adolescent and Youth, UNFPA India Email: [email protected]
88. Dr Margaretha Sitanggang Programme Analyst for Youth and ASRH UNFPA Indonesia Email: [email protected]
89. Dr. Tiara Marthias Consultant UNFPA Indonesia Email: [email protected]
16 | P a g e
90. Ms. Citra Kusuma
Consultant UNFPA Indonesia Email: [email protected]
91. Mr Abhiram Roy Comprehensive Sexuality Education (CSE) Project Coordinator UNFPA Nepal Email: [email protected]
92. Dr Neeta Shrestha RH Specialist UNFPA- NEPAL Email: [email protected]
93. Ms Sarah Soysa National Programme Analyst - SRHR UNFPA Sri Lanka Email: [email protected]
UNESCO
94. Ms Jenelle Babb Email: [email protected]
95. Ms Sarita Jadav National Programme Officer The United Nations Educational, Scientific and Cultural Organization (UNESCO) Email: [email protected]
96. Ms Nandini Chatterjee UNESCO Mahatma Gandhi Institute of Education for Peace and Sustainable Development (MGIEP) New Delhi India Email: [email protected]
97. Mr Prashant Yadav Consultant The United Nations Educational, Scientific and Cultural Organization (UNESCO) Email: [email protected]
UNWOMEN
98. Dr Rajnish Prasad Programme Specialist (Gender Equality & HIV/AIDS) UN Women
Bangkok, Thailand Email: [email protected]
99. Dr Fanny Arendt Civil Society Coordination Women’s Access to Justice UN Women Uppsala, Sweden Email: [email protected]
100. Ms. Prerna Kumar Senior Technical Specialist International Center for Research on Women (ICRW) Mumbai, Maharashtra India Email: [email protected]
101. Mr. Rabin Rai Youth Monitoring and Evaluation Officer UN WOMEN – Nepal Email: [email protected]
102. Ms Dia Yonzon Youth Programme Support Officer UN WOMEN- NEPAL Email: [email protected]
UNAIDS
103. Dr Salil Panakadan Senior Adviser Evaluation United Nations Joint Programme on HIV/AIDS (UNAIDS) Geneva Email: [email protected]
104. Dr Michela Polesana Advocacy Advisor The Joint United Nations Programme on HIV and AIDS (UNAIDS) Bangkok, Thailand Email: [email protected]
105. Dr Edward John Rudram The Joint United Nations Programme on HIV and AIDS (UNAIDS) Bangkok, Thailand Email: [email protected]
WHO Collaborating Centre
106. Dr Susan Sawyer President of IAAH
17 | P a g e
Director, Centre for Adolescent Health Royal Children’s Hospital Melbourne, Australia Email: [email protected]
107. Dr Quamrun Nahar Head of Research Maternal and Child Health Division International Centre for Diarrohoeal Diseases Research, Bangladesh (icddr,b) Dhaka, Bangladesh
108. Dr B.S Garg Director Professor and Secretary Kasturba Health Society (KHS) Mahatma Gandhi Institute of Medical Sciences (MGIMS) Sewagram – 442 102, District of Wardha Maharashtra, India Email: [email protected]
109. Dr Subodh S Gupta Professor (Social Pediatrics) Dr Sushila Nayar School of Public Health Mahatma Gandhi Institute of Medical Sciences (MGIMS) Sewagram – 442 102, District of Wardha Maharashtra, India Email: [email protected]
110. Dr Chetna Maliye Professor Director Professor and Secretary Kasturba Health Society (KHS) Mahatma Gandhi Institute of Medical Sciences (MGIMS) Sewagram – 442 102, District of Wardha Maharashtra, India Email: [email protected]
111. Dr Harish K Pemde Director Professor of Pediatrics In-Charge, Center for Adolescent Health Head, WHO Collaborating Center for Training and Research in Adolescent Health Kalawati Saran Children's Hospital Email: [email protected]
112. Dr Sanjay L Chauhan
Scientist- G Indian Council of Medical Research (ICMR) National Institute for Research in reproductive Health (NIRRH)
Maharashtra, India Email: [email protected]
113. Dr. Beena Joshi Scientist-F Department of Operational Research (DOR) National Institute for Research in Reproductive Health (NIRRH) Email: [email protected] ;[email protected]
114. Dr. Ragini Kulkarni Scientist-E Department of Operational Research (DOR) National Institute for Research in Reproductive Health (NIRRH) Email: [email protected]
Professional Associations
115. Prof Manzoor Hussain President Bangladesh Pediatrics Association (BPA) Dhaka, Bangladesh
116. Prof. Dr Ferdousi Begum Obstetrical and Gynaecological Society of Bangladesh Bangladesh Email: [email protected]
117. Prof Gulshan Ara Secretary General Obstetrical and Gynaecological Society of Bangladesh
118. Dr. Ari Kusuma Januarto– SpOG(K) President of Indonesia Obstetrician Association (POGI) Indonesia Email: [email protected]
119. Dr. Aman Bhakti Pulungan President of Indonesia Pediatric Association (IDAI) Indonesia Email: [email protected]
120. Dr. Bernie Endyarni Medise Head of Adolescent Task Force Indonesia Pediatric Association (IDAI) Indonesia Email: [email protected]
121. Dr Fransisca Handy Agung Pediatrician Adolescent health advocate Indonesia Email: [email protected]
18 | P a g e
122. Dr Ryan Fajar Febrianto Indonesia Email: [email protected]
123. Dr. Fitri Ariyanti Abidin Child and adolescent clinical psychologist Lecturer at Faculty of Psychology Padjadjaran University Indonesia Email: [email protected] [email protected]
124. Prof. Dr. Hj. Hendriati Agustiani Head of Developmental Psychology Department Faculty of Psychology Padjadjaran University Indonesia Email: [email protected]
125. Dr Ganesh Rai President Pediatric Society of Nepal Email: [email protected]
126. Dr Padam Raj Pant Vice-President, Nepal Society of Obstetrics and Gynecology Email: [email protected]
127. Dr Rajendra Bhadra National Adolescent Health Expert Email: [email protected]
128. Dr Vinya Ariyaratne Secretary Sarvodayam Movement Sri Lanka Email: [email protected]
129. Prof Muditha Vidanapathirana Chairman National Child Protection Authority Sri Lanka Email: [email protected]
130. Mr Pubudu Sumanasekara Executive DirectorI Alcohol & Drug Information Centre (ADIC) Sri Lanka Email: [email protected]
131. Dr Vinya Ariyaratne General Secretary Sarvodaya Shramadana Movement Sri Lanka Email: [email protected]
132. Ms Lyshanya Moonasinghe Creative Consultant (Freelance) Limkokwing University of Creative Technology Colombo Sri Lanka Email: [email protected]
133. Dr Chandan Kachru
Adolescent health expert and Member of The Federation of Obstetric and Gynaecological Societies of India (FOGSI) India Email:[email protected]
134. Dr Jugal Kishore Secretary Indian Association of Adolescent Health India Email: [email protected]
Partner Agencies INGOs and NGOs
USAID
135. Dr Sharmila Neogi Advisor (Adolescent Health and Gender) U.S. Agency For International Development (USAID) Health Office American Embassy, Chanakyapuri, New Delhi, 110021 Email: [email protected]
136. Dr Riad Mahmud Policy and Technical Advisor U.S. Agency for International Development (USAID) Madani Avenue
Dhaka, Bangladesh Email: [email protected]
137. Dr. Sigit Sulistyo Team Lead Maternal Child Health U.S. Agency for International Development (USAID) Indonesia Email: [email protected]
138. Mr. Netra Bhatta Senior Program Specialist-FP/RH, Health Office U.S. Agency for International Development (USAID) Nepal Email: [email protected]
19 | P a g e
SYAN
139. Ms Shannon Mathew Coordinator Policy Research and Engagement The YP Foundation (TYPF) Noida, Uttar Pradesh India Email: [email protected]
INGOs and NGOs
140. Dr Ajay Khera Country Representative EngenderHealth New Delhi, India Email: [email protected]
141. Ms Ayu Oktariani National Coordinator Indonesia Positive women network (IPPI) Indonesia Email: [email protected]
142. Ms Irene Audrey Mailoa Program Manager Intimuda Indonesia Email: [email protected]
143. Ms Yessy Deputy Coordinator East Java, Intimuda Email: [email protected]
144. Dr Rinaldi Ridwan Secretary General AKAR Indonesia Email: [email protected]
145. Dr S.M Shaikat Executive Director at SERAC Dhaka, Bangladesh Email: [email protected]
146. Mr. K P Upadhyay Senior Advisor Marie Stopes International Nepal Email: [email protected]
147. Ms Kamal Tara Bajracharya Senior Manager Program Implementation Department, PSI/NEPAL Email: [email protected]
148. Mr. Ganesh Pandey Technical Manager-Health and Nutrition, Save the Children Nepal
Email: [email protected]
149. Ms Thushara Argus Executive Director Family Planning Association Colombo Sri Lanka Email: [email protected]
150. Dr. Fatema Shabnam Adolescent and Youth Specialist Shukhi Jibon Dhaka Bangladesh Email: [email protected]
151. Dr Noor Mohammad Executive Director Population Services and Training Center (PSTC) Bangladesh Email [email protected]
152. Ms. Natassha Kaur Senior Officer Advocacy & External Relations International Planned Parenthood Federation East & South East Asia and Oceania Region (IPPF ESEAOR) Kuala Lumpur, Malaysia Email: [email protected]
153. Ms. Zara Rapoport Gender and Inclusion Lead The Asia-Pacific (APAC) Plan International New York United States Email: [email protected]
WHO Headquarters
154. Dr Valentina Baltag Scientist MCA WHO/HQ
155. Ms Narissia Mawad Adolescent Health and Well-being officer The Partnership for Maternal, Newborn and Child Health (PMNCH) World Health Organization Email: [email protected]
156. Dr David Ross Consultant The Partnership for Maternal, Newborn and
20 | P a g e
Child Health (PMNCH) World Health Organization
WHO Country offices
157. Dr Mahbuba Khan National Professional Officer WHO-Bangladesh
158. Dr Lobzang Dorji National Professional Office WHO-Bhutan
159. Dr Pooja Pradhan National Professional Officer Family Health, Gender & Life Course WHO-Nepal
Regional Office for South-East Asia
160. Dr Neena Raina Senior Adviser Reproductive, Maternal, Newborn Child & Adolescent Health and Ageing (MCA)
161. Dr Rajesh Mehta Regional Adviser Newborn, Child and Adolescent Health
162. Dr Anoma Jayathilaka MO-Maternal and Reproductive Health
163. Ms Patricia Codyre Regional Adviser, Digital Health
164. Dr Suvajee Good Regional Adviser, Health Promotion
165. Meera Upadyay Medical Officer-SRH
166. Newborn Child & Adolescent Health and Ageing (MCA-O)
167. Mr Dhiraj Kumar Executive Assistant (Data Management) Reproductive, Maternal, Newborn Child &
168. Ms Pooja Verma Executive Assistant (CAH)

2 | P a g e
3 | P a g e
Related Documents











