SELF ASSESSMENT QUESTIONS A case of migratory lymphadenopathy and cutaneous anergy in an Asian woman Haider M Al Attia, Yasser H Al Ahmed, Afaf El Hag, Rima N El Abassi A 40 year old Pakistani woman presented with one month history of fever, night sweats, and progressive and painful swelling in the right side of the neck. She was febrile (temperature 38–40ºC). Right deep cervical, occipital, and jugulodiagastric lymph nodes were palpable, firm, and tender. Save for a moderately severe asymmetrical arthralgia of right wrist, shoulder and proximal interphalangeal joints, the rest of her physical examination was unremarkable. Laboratory data showed, mild leucopenia of 3.6 × 10 9 /l with 64% neutrophils, 26% lym- phocytes (no atypical form), and 10% mono- cytes, erythrocyte sedimentation rate (ESR) 64 mm/hour, and C reactive protein of 105 mg/l (normal <10 mg/l). A skin test for tuberculin reactivity was negative. Results of chest radio- graphy, blood chemistry, urine and stool analy- sis, throat swab, blood cultures, Venereal Disease Research Laboratory test, test for HIV, heterophil antibodies, and serological studies for salmonella serotypes, brucellosis, toxo- plasmosis, Lyme disease, Epstein-Barr virus, cytomegalovirus, human T cell leukaemia virus-1, herpes simplex and hepatitis B and C, as well as serum immunoglobulins were normal or negative. Assays for antinuclear fac- tors, anti-dsDNA, neutrophil cytoplasmic anti- bodies, and rheumatoid factor were also nega- tive. Computed tomography of the chest and abdomen showed normal findings. Cervical lymph node biopsy showed an intact architec- ture and a reactive proliferation of histiocytes, transformed lymphocytes of CD8 phenotype and plasma cells, surrounding areas of karyor- rhectic necrosis without neutrophils. There were no demonstrable organisms on special stains. A periadenitis was present together with a vasculities with no fibrinoid necrosis present (fig 1). A diagnosis was made and she was treated accordingly. There was rapid resolution of fever and arthralgia within 24 hours, and the lymphadenopathy in two weeks. Follow up at three months was uneventful. After being well for two years, she presented again in June 1998 with a one month history of the same symptoms, but this time there was a non-tender, left supraclaviular, posterior trian- gle, and jugulodigastric lymphadenopathy. Leucopenia of 3.1 × 10 9 /l with 7% monocytes and ESR of 36 mm/hour were documented. All the tests that had been carried out during her previous admission were repeated. The results showed no abnormal findings. The tuberculin test was again negative. Biopsy of a left deep cervical node showed identical changes to those of the previous biopsy. She was conserva- tively managed with bed rest and administra- tion of paracetamol. The fever subsided completely after 10 days and lymphadenopathy resolved in two weeks. The patient remains well to date. During the follow up, the tuberculin test was repeatedly found to be positive. Questions (1) What was the overall diagnosis? (2) What two unusual features are described in this case? Figure 1 Area of karyorrhectic necrosis (arrow) surrounded by histiocytes (pale zone), lymphoctyes, and plasma cells (dark zone). Answers on p 663. Postgrad Med J 2000;76:660–662 660 Department of Internal Medicine and Histopathology, Mafraq Hospital, Abu Dhabi, United Arab Emirates H M Al Attia Y H Al Ahmed A El Hag R N El Abassi Correspondence to: Dr Haider M Al Attia, Mafraq Hospital, PO Box 2951, Abu Dhabi, UAE Submitted 9 March 1999 Accepted 14 October 1999 www.postgradmedj.com group.bmj.com on April 18, 2012 - Published by pmj.bmj.com Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
SELF ASSESSMENT QUESTIONS
A case of migratory lymphadenopathy andcutaneous anergy in an Asian woman
Haider M Al Attia, Yasser H Al Ahmed, Afaf El Hag, Rima N El Abassi
A 40 year old Pakistani woman presented withone month history of fever, night sweats, andprogressive and painful swelling in the rightside of the neck. She was febrile (temperature38–40ºC). Right deep cervical, occipital, andjugulodiagastric lymph nodes were palpable,firm, and tender. Save for a moderately severeasymmetrical arthralgia of right wrist, shoulderand proximal interphalangeal joints, the rest ofher physical examination was unremarkable.Laboratory data showed, mild leucopenia of3.6 × 109/l with 64% neutrophils, 26% lym-phocytes (no atypical form), and 10% mono-cytes, erythrocyte sedimentation rate (ESR) 64mm/hour, and C reactive protein of 105 mg/l(normal <10 mg/l). A skin test for tuberculinreactivity was negative. Results of chest radio-graphy, blood chemistry, urine and stool analy-sis, throat swab, blood cultures, VenerealDisease Research Laboratory test, test for HIV,heterophil antibodies, and serological studiesfor salmonella serotypes, brucellosis, toxo-plasmosis, Lyme disease, Epstein-Barr virus,cytomegalovirus, human T cell leukaemia
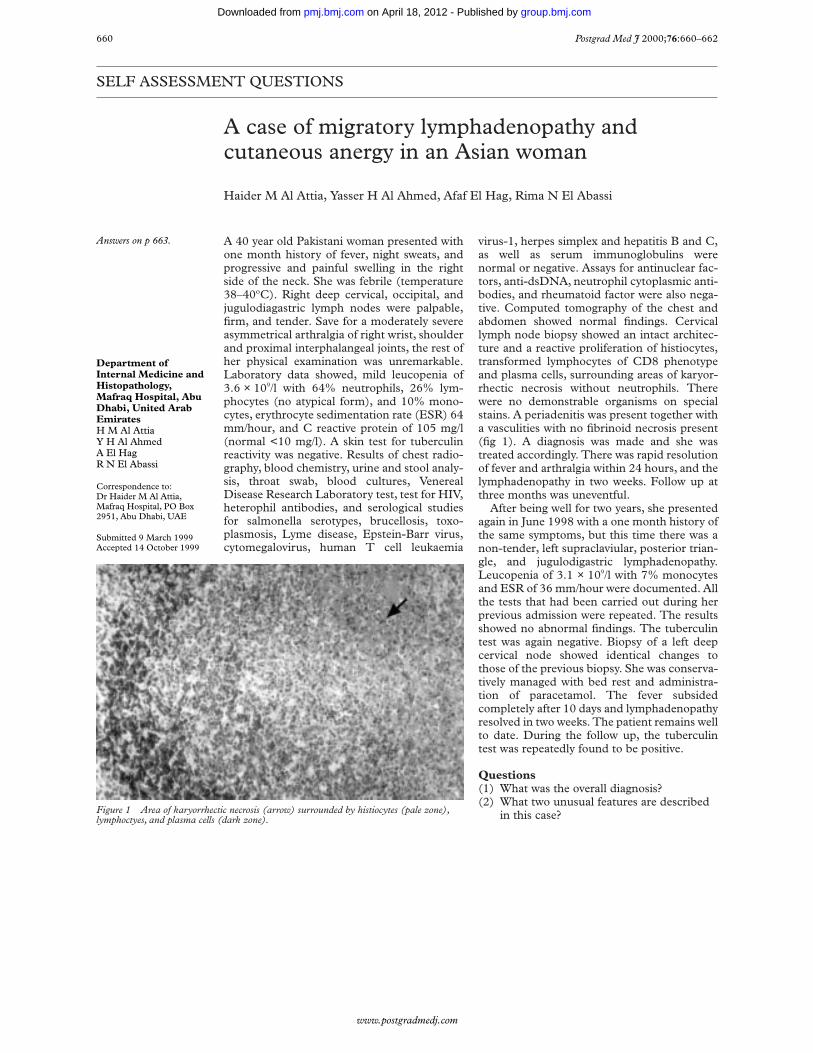
virus-1, herpes simplex and hepatitis B and C,as well as serum immunoglobulins werenormal or negative. Assays for antinuclear fac-tors, anti-dsDNA, neutrophil cytoplasmic anti-bodies, and rheumatoid factor were also nega-tive. Computed tomography of the chest andabdomen showed normal findings. Cervicallymph node biopsy showed an intact architec-ture and a reactive proliferation of histiocytes,transformed lymphocytes of CD8 phenotypeand plasma cells, surrounding areas of karyor-rhectic necrosis without neutrophils. Therewere no demonstrable organisms on specialstains. A periadenitis was present together witha vasculities with no fibrinoid necrosis present(fig 1). A diagnosis was made and she wastreated accordingly. There was rapid resolutionof fever and arthralgia within 24 hours, and thelymphadenopathy in two weeks. Follow up atthree months was uneventful.
After being well for two years, she presentedagain in June 1998 with a one month history ofthe same symptoms, but this time there was anon-tender, left supraclaviular, posterior trian-gle, and jugulodigastric lymphadenopathy.Leucopenia of 3.1 × 109/l with 7% monocytesand ESR of 36 mm/hour were documented. Allthe tests that had been carried out during herprevious admission were repeated. The resultsshowed no abnormal findings. The tuberculintest was again negative. Biopsy of a left deepcervical node showed identical changes tothose of the previous biopsy. She was conserva-tively managed with bed rest and administra-tion of paracetamol. The fever subsidedcompletely after 10 days and lymphadenopathyresolved in two weeks. The patient remains wellto date. During the follow up, the tuberculintest was repeatedly found to be positive.
Questions(1) What was the overall diagnosis?(2) What two unusual features are described
in this case?Figure 1 Area of karyorrhectic necrosis (arrow) surrounded by histiocytes (pale zone),lymphoctyes, and plasma cells (dark zone).
Answers on p 663.
Postgrad Med J 2000;76:660–662660
Department ofInternal Medicine andHistopathology,Mafraq Hospital, AbuDhabi, United ArabEmiratesH M Al AttiaY H Al AhmedA El HagR N El Abassi
Correspondence to:Dr Haider M Al Attia,Mafraq Hospital, PO Box2951, Abu Dhabi, UAE
Submitted 9 March 1999Accepted 14 October 1999
www.postgradmedj.com
group.bmj.com on April 18, 2012 - Published by pmj.bmj.comDownloaded from

Multiple focal lesions in liver and spleen in acuteleukaemia
Sangeet Ghai, Sanjay Thulkar, Prakash Neduvelil Purushothaman, Sanjay Sharma
An 18 year old girl presented with a twomonth history of fever and bleeding tendency.On examination, she had multiple petechialhaemorrhages all over her body. There
was no organomegaly or peripheral lympha-denopathy. Systemic examination wasunremarkable. Total leucocyte count was117 × 109/l and platelet count 45 × 109/l.Peripheral smear showed presence of blastcells. Bone marrow biopsy revealed 60%–70%myeloblasts. The patient was diagnosed ashaving myeloid leukaemia. After two cycles ofchemotherapy, the patient went into remis-sion.
After three weeks, she became febrile againand developed diVuse upper abdominal ten-derness and jaundice. Abdominal sonography(fig 1) and computed tomography (figs 2 and3) were performed. Total leucocyte count atthis time was 9.5 × 109/l.
Questions(1) What are the findings on ultrasound and
computed tomography?(2) What is the radiological diagnosis?(3) How can the diagnosis be confirmed?
Answers on p 664.
Figure 1 Sonogram of the spleen shows multiple, roundedhypoechoic lesions, some with typical bull’s eye appearance.
Figure 2 Computed tomogram of the upper abdomenshowing multiple small low attenuation lesions in the liverand spleen. Incidentally old calcified granulomas are alsoseen in liver and spleen.
Figure 3 Computed tomogram shows multiple, lowattenuation, rounded lesions in the spleen. One of the lesions(arrow) also shows a central nidus of high attenuation.
Self assessment questions 661
Institute RotaryCancer Hospital, AllIndia Institute ofMedical Sciences, NewDelhi 110 029, India:Department ofRadio-diagnosisS GhaiS ThulkarS Sharma
Department ofMedical OncologyP N Purushothaman
Correspondence and reprintrequests to: Dr SanjaySharma, A-86, Inderpuri,New Delhi 110012, India(email:[email protected])
Submitted 1 June 1999Accepted 8 October 1999
www.postgradmedj.com
group.bmj.com on April 18, 2012 - Published by pmj.bmj.comDownloaded from

A pregnant patient with bilateral ischaemic limbs
N B Teo, N Mamode, D P Leiberman
A 29 year old pregnant woman, at 35 weeks’gestation, was admitted with a three day historyof a painful left thigh and calf which was exac-erbated by walking. She also complained ofparaesthesiae, muscle weakness, and coldnessof the left foot which at times becamecyanosed. These symptoms were associatedwith dyspnoea on exertion.
When admitted to the obstetric ward, the leftlower limb pulses were impalpable. The leftlower leg was mottled and cold but was viable.
The electrocardiogram showed ST changesin the septal leads with R waves in V1 sugges-tive of right ventricular hypertrophy as well asT wave inversion in the anterolateral leadsthought by the cardiologist to be suggestive ofpulmonary thromboembolism. Chest radio-graphy showed cardiomegaly. Full bloodcount, concentrations of urea and electrolytes,and thrombophilia screen were normal.
On review by the vascular team, it was notedthat apart from a very weak right femoral pulse,there was absence of pulses in both lowerlimbs, which were significantly ischaemic.
After cardiological review, a transthoracicechocardiogram showed a large right ventriclewith a dilated pulmonary artery. No atrial sep-tal defect was seen and there was no evidenceof thrombus.
Doppler ultrasound showed a 10 cm leftpopliteal venous thrombus as well as occlusionof bilateral common femoral and superficialarteries. This was followed by a transradialarteriogram that showed the thrombus causinga left common iliac occlusion and a right com-mon femoral arterial occlusion (fig 1).
Questions(1) What is the diagnosis?(2) Describe the pathogenesis of this clinical
condition?(3) How should the diagnosis be made?(4) Describe the most recent development in
the diagnosis of this condition?(5) What is the treatment?
Severe symptomatic hypercalcaemia
José María Calvo-Romero, María del Carmen Bonilla-Gracia
A 49 year old man had a six week history ofdepression, constipation, proximal muscleweakness, anorexia, and weight loss of about 20kg. The patient was not taking any medicationand there was no history of nephrolithiasis,peptic ulcer, headache, or visual defects. Physi-cal examination showed light proximal muscleweakness without atrophy, dehydration, and noother remarkable findings. The blood pressurewas 140/85 mm Hg. The patient’s bloodchemical values were: glucose 5.2 mmol/l, ureanitrogen 13.2 mmol/l, creatinine 141 µmol/l,sodium 136 mmol/l, potassium 4.1 mmol/l,chloride 101 mmol/l, phosphorus 1.3 mmol/l,magnesium 0.98 mmol/l, alkaline phosphatase115 U/l, creatine kinase 82 U/l, protein 76 g/l,
and albumin 43 g/l. The blood calcium was 4.8mmol/l, confirmed by repeated determinations.The 24 hour urinary calcium excretion was 12.3mmol. An electrocardiogram revealed sinusrhythm and shortened QT interval. Free thyrox-ine and thyrotrophin serum concentrations werenormal. Serum intact parathyroid hormone was488 µg/l (normal values 10–65 µg/l).
Questions(1) What is your diVerential diagnosis for this
case?(2) What further investigations would you
perform?(3) What is the therapy for the severe hyper-
calcaemia in this case?
Internal MedicineService, InfantaCristina UniversityHospital, Badajoz,SpainJ M Calvo-RomeroM C Bonilla-Gracia
Correspondence to:José María Calvo-Romero,Héroes de Cascorro 9, 31A,06004 Badajoz, Spain
Submitted 7 July 1999Accepted 8 October 1999
Answers on p 666.
Figure 1 Transradial arteriogram: left common iliac andright common femoral arterial occlusions.
Answers on p 668.
662 Self assessment questions
Peripheral VascularUnit, Royal InfirmaryGlasgow, Glasgow, UKN B TeoN MamodeD P Leiberman
Correspondence to:Mr N B Teo, PathologyDepartment, University ofLiverpool, Duncan Building,Daulby Street, LiverpoolL69 3GA, UK(email:[email protected])
Submitted 27 August 1999Accepted 8 October 1999
www.postgradmedj.com
group.bmj.com on April 18, 2012 - Published by pmj.bmj.comDownloaded from

SELF ASSESSMENT ANSWERS
A case of migratory lymphadenopathyand cutaneous anergy in an Asian woman
Q1: What was the overall diagnosis?Histiocytic necrotising lymphadenitis (KikuchiFujimoto disease)
Q2: What two unusual features aredescribed in this case?(1) The transient cutaneous anergy during theacute phase of the illness and (2) the migratorypattern of lymphadenopathy after a prolongedremission.
DiscussionHistiocytic necrotising lymphadenitis orKikuchi Fujimoto disease (KFD) is an uncom-mon, self limiting disease that primarily aVectsthe cervical lymph nodes in young adults,mainly females. The aetiology seems unknownbut an infective origin seems likely. Though thecondition commonly aVects patients of Asiandescent, it has been more and more seen inother populations.1 2
KFD is a peculiar condition with broadmorphological spectrum that can readily bemistaken for malignant lymphoma or lupus,3
thus an accurate distinction is crucial. Patientsusually develop painless, often unilateral cervi-cal lymphadenopathy in the context of fever,night sweats, arthralgia, rash, and asthenia.4
Painful lymphadenopathy may also develop.3
Generalised lymphadenopathy occursinfrequently3 and has recently been associatedwith human T cell leukaemia virus-1infection.5 The true nature of the lesionbecomes evident on a lymph node biopsyrather than fine needle aspiration samples.6
Other infectious agents of possible relevance topathogenesis include herpes virus 6, Epstein-Barr virus, cytomegalovirus, parvovirus B-19,Yersinia enterocolitica, and brucella species.7–12
KFD has been repeatedly linked with systemiclupus erythematosus3–13 and described in as-sociation with Hashimoto’s thyroiditis,13
Sweet’s syndrome,14 and Still’s disease.15 Thecondition has a low recurrence rate of 3%–4%and rarely recurs after a prolonged remission.The acute phase of illness usually responds tobed rest and symptomatic treatment. Thesymptoms resolve within 1–4 months; howeverthere have been cases that recurred3 orpersisted as long as a year.4
In this case the migratory pattern of cervicallymphadenopathy, which was painful andtender at first presentation and painless onrelapse, has led to a clinical diagnostic
dilemma; a situation that would have not beensettled without a second lymph node biopsy.Such a migratory characteristic, however, hasnot been specifically referred to in the previousliterature. KFD should be considered in thediVerential diagnosis of any clinical setting withmigratory lymphadenopathy. The repeatedlynegative tuberculin test during acute illnesswas another issue of interest. Unless the cellu-lar mediated immune reaction is stunted, thetuberculin test is expected to be positive in anAsian adult, even in the absence of activetuberculous disease. Thus, the negative reac-tion in our patient was likely to be a sign oftransient cutaneous anergy possibly induced bythe disease activity and recovered duringremission. To the best of our knowledge thisphenomenon was also not reported before, andis worthy of further study in future cases.
Final diagnosisHistiocytic necrotising lymphadenitis (KikuchiFujimoto disease).
1 Simonsen K, StormT L. Histiocytic necrotizing lymphad-enitis (Kikuchi’s disease). Ugeskr Laeger 1991;153:2836–7.
2 Depree C, Pelte MF, Delacretaz F, et al. Histiocyticnecrotizing lymphadenitis or Kikuchi’s disease. Anatomo-clinical study of 4 cases. Nouv Rev Fr Hematol 1990;32:241–7.
3 Kuo TT. Kikuchi’s disease (histiocytic necrotizing lymphad-enitis). A clinicopathologic study of 79 cases with an analy-sis of histologic subtypes, immunohistology, and DNAploidy. Am J Surg Pathol 1995;19:798–809.
4 Dylewski J, Berry G, Pham-Dang H. An unusual cause ofcervical lymphadenitis: Kikuchi-Fujimoto disease. Rev InfDis 1991;13:823–5.
5 Bataille V, Harland CC, Behrens J, et al. Kikuchi disease(histiocytic necrotizing lymphadenitis) in association withHTLV 1. Br J Dermatol 1997;136:610–12.
6 Kung IT, Ng WF, Yuen RW, et al. Kikuchi’s histiocytic lym-phadenitis. Diagnosis by fine needle aspiration. ActaCytolocica 1990;34:323–6.
7 HoVman A, Kirn E, Kuerten A, et al. Active humanherpesvirus-6 (HHV-6) infection associated with Kikuchi-Fujimoto disease and systemic lupus erythematosus. In vivo1991;5:265–9.
8 Yen A, Fearneyhough P, Raimer SS, et al. EBV- associatedKikuchi’s histiocytic lymphadenitis with cutaneous manifes-tations. J Am Acad Dermatol 1997;36:342–6.
9 Biasi D, Caramaschi P, Carletto A, et al. Three clinicalreports of Kikuchi’s lymphadenitis combined with systemiclupus erythematosus. Clin Rheumatol 1996;15:81–3.
10 Yufu Y, Matsumoto M, Miyamura T, et al. PavovirusB19-associated haemophagocytic syndrome with lymphad-enopathy resembling histiocytic necrotizing lymphadenitis(Kikuchi’s disease). Br J Haematol 1997;96:868–71.
11 Heikens J, Tel W, van de Stadt J, et al. Kikuchi’slymphadenitis: report of a Yersinia enterocolitica-associatedcase and an overview of aetiology and clinical outcome. NethJ Med 1992;41:222–8.
12 Rodr’iguez Martorell J, Mart’in MV, B’aez JM, et al.Kikuchi-Fujimoto necrotizing lynphadenitis associated withbrucellosis. Sangre 1992;37:201–4.
13 Bousquet E, Tubery M, Brousset P, et al. Kikuchi syndrome,Hashimoto thyroiditis and lupus serology. A propos of acase. Rev Med Interne 1996;17:836–8.
14 Itoh H, Shimasaki S, Nakashima A, et al. Sweet’s syndromeassociated with subacute necrotizing lymphadenitis. InternMed 1992;31:686–9.
15 Ohta A, Matsumoto Y, Ohta T, et al. Still’s diseaseassociated with necrotizing lymphadenitis (Kikuchi’sdisease): report of 3 cases. J Rheumatol 1988;15:981–3.
Postgrad Med J 2000;76:663–669 663
www.postgradmedj.com
group.bmj.com on April 18, 2012 - Published by pmj.bmj.comDownloaded from

Multiple focal lesions in liver and spleenin acute leukaemia
Q1: What are the findings on ultrasoundand computed tomography?Abdominal ultrasound shows multiple hypo-echoic focal lesions in the spleen, some of themhaving central echogenic foci producing bull’seye or target configuration. Contrast enhancedcomputed tomography shows multiple, non-enhancing, hypodense focal areas in liver inaddition to the spleen. Few of the spleniclesions demonstrate central hyperdense foci.Incidentally, a few old healed calcified foci arealso seen in the liver and spleen.
Q2: What is the radiological diagnosis?The image morphology of liver and spleniclesions in this immunocompromised patient isstrongly suggestive of fungal infection.
Q3: How can the diagnosis be confirmed?Image guided fine needle aspiration andmicroscopic examination of the aspirate can bedone to confirm the diagnosis. An aspiratefrom the centre of the focal lesion is most likelyto yield a positive result as the fungal elementsare most abundant in these central necroticareas. Blood and tissue cultures may be falselynegative, particularly with candidal infections.In our patient, ultrasound guided fine needleaspiration was performed. The aspirate dem-onstrated mycelia and budding yeast cells con-firming the diagnosis of hepatosplenic candi-diasis.
DiscussionFungal infections of the liver and spleen occuralmost exclusively in individuals with underly-ing defects of host immune defence mech-anism. The most commonly implicated organ-ism is Candida albicans, but infections withother fungi such as aspergillus and cryptococ-cus may also occur.1 The presenting symptomsare generally non-specific, consisting of fever,pain referable to the area of involvement,tenderness on direct palpation, enlargement ofliver and/or spleen, and rarely, jaundice.Usually both liver and spleen are involved,though either organ may be aVected inisolation.2
Initially hepatomegaly and/or splenomegalyare present. Subsequently focal lesions developthat later spread throughout the parenchyma.They may be single or multiple. Whenmultiple, they tend to be located adjacent toone another or may become partiallyconfluent.3 Their size varies from 0.3 cm to 4.0cm and they have relatively well definedborders. Five sonographic patterns of hepato-splenic candidiasis have been described.3 Pat-tern 1 represents an early active phase of thedisease in which ultrasound demonstrateseither a “wheel within wheel” (type a) or“wagon wheel” (type b) appearance. In theformer appearance, the outer hypoechoic rim isformed by fibrosis while the inner hyperechoicrim is composed of the inflammatory process.In the centre of the inner hyperechoic zone,there is an area of necrosis identified as the
hypoechoic nidus. In the wagon wheel appear-ance, echogenic radial strands are seen whichimitate the spokes of a wheel. These “spokes”represent the inflammatory process, whereashypoechoic regions between the spokes is thefibrous component. The axis of the wheel isformed by hypoechoic, necrotic nidus.
Pattern 2, manifested by the “bull’s eye” ortarget configuration, lacks the central necrotichypoechoic nidus. The lesion consists of theinflammatory process forming the echogeniccentre, which is surrounded by fibrosis seen asthe hypoechoic rim.3 Pattern 3 is characterisedby a purely hypoechoic lesion. It is seen whenthe inflammatory process is being replaced byfibrosis.3 Later this hypoehoic lesion is trans-formed into a completely echogenic lesion(pattern 4) with a varying degree of posterioracoustic shadow. This sonographic appearanceis produced by scar tissue with or without cal-cification. This echogenic lesion is usuallysmaller than pattern 2 or 3 lesions and mayeven disappear completely in the course of thehealing process.3
In acute phase of the disease, lesions of pat-terns 1 and 2 prevail. As disease progresses,pattern 3 lesions are identified, however,pattern 1 and 2 lesions may still be present.When pattern 4 lesions appear, pattern 1 is nolonger seen and the lesions of other patternsregress in size. This is recognised late in thecourse of the disease.3
Fungal abscesses in liver and spleen of neu-tropenic patients are not always detectable onsonography, even in the presence of dissemi-nated infection. The lesions become apparentwhen the neutrophil count returns to normal.4
It is important to identify pattern 1 or 2 in atleast one lesion, as these appear only when the
Box 1: Various patterns of candidalinfection of liver and spleen onultrasoundx Pattern 1a: wheel within wheel
appearance
x Pattern 1b: wagon wheel appearance
x Pattern 2: bull’s eye appearance/targetconfiguration
x Pattern 3: pure hypoechoic defect
x Pattern 4: echogenic lesion with avarying intensity of posterior acousticshadow
Box 2: DiVerential diagnosis ofmultiple hypodense/hypoechoic splenicand liver lesionsx Lymphoma
x Leukaemia
x Metastatic disease
x Bacterial infection
x Fungal infection
x Parasitic infection
x Sarcoid
664 Self assessment answers
www.postgradmedj.com
group.bmj.com on April 18, 2012 - Published by pmj.bmj.comDownloaded from

neutrophil count in a previously neutropenicpatient is returning to normal and infection isactive.5 This fact suggests that the inflamma-tory response of the host plays a part in defin-ing the characteristic appearance.6 Pattern 3and 4 lesions occur later in course of thedisease and suggest that the infection issubsiding.5
Computed tomography may demonstratesimilar appearances. Pastakia et al reported thatpattern 1 lesions were not seen on computedtomograms and pattern 2 lesions were demon-strated only occasionally.5 Pattern 3 lesions(multiple rounded areas of decreased attenua-tion scattered throughout the liver and spleen)were most common. Pattern 4 lesions, repre-senting areas of calcification, were seen late incourse of the disease. In our patient, no focalhepatic lesion could be detected on ultrasound,while computed tomography showed multiplepattern 3 and one pattern 2 lesion in the liverand multiple pattern 2 and 3 lesions in thespleen. Similar observation was also made byPastakia et al. A computed tomogram is moresensitive in detecting the focal lesions; however,it is less specific as the characteristic pattern 1and 2 lesions are demonstrated only occasion-ally. Periportal areas of increased attenuationseen on computed tomography are also re-ported which correlate pathologically withfocal linear fibrosis in these immunocompro-mised patients.5
The usual diVerential diagnosis of multiple,focal lesions in liver and spleen includelymphoma, leukaemia deposits, metastasis,
bacterial and fungal infection, and sarcoid.Most of these diseases give rise to non-specificfocal hypoechoic lesions on sonography. Targetlesions may however be seen in metastatic dis-ease, although metastatic disease is unusual inthe spleen. Deposits of lymphoma and leukae-mia show rapid regression after cytostatictreatment, a fact which may help to diVerenti-ate them from the lesions of other aetiologies.6
To summarise, the detection of focal hepaticand splenic lesions with characteristic imagemorphology should suggest a possible underly-ing fungal disease in a febrile leukaemicpatient. Apart from the aetiological diagnosisof fungal infection, the imaging features alsoprovide understanding of their evolution overtime.
Final diagnosisMultiple candidal abscesses in liver and spleenin acute myeloid leukaemia.
1 Berlow ME, Spirit BA, Weil L. CT follow-up of hepatic andsplenic fungal micro-abcesses. J Comput Assist Tomogr1984;8:42–5.
2 Maxwell AJ, Mamtora H. Fungal liver abcesses in acuteleukemia—a report of two cases. Clin Radiol 1988;39:197–201.
3 Grunebaum M, Ziv N, Kaplinsky C, et al. Livercandidiasis—the various sonographic patterns in the immu-nocompromised child. Pediatr Radiol 1991;21:497–500.
4 Chew FS, Smith PL, Barboriak D. Candidal splenicabcesses. AJR Am J Roentgenology 1991;156:474.
5 Pastakia B, Shawker TH, Thaler M, et al. Hepatospleniccandidiasis: wheels within wheels. Radiology 1988;166:417–21.
6 Gorg C, Wiede R, Schwerk WB, et al. Ultrasound evaluationof hepatic and splenic microabscesses in the immunocom-promised patient: sonographic patterns, diVerential diagno-sis and follow-up. J Clin Ultrasound 1994;22:525–9.
Self assessment answers 665
www.postgradmedj.com
group.bmj.com on April 18, 2012 - Published by pmj.bmj.comDownloaded from

A pregnant patient with bilateralischaemic limbs
Q1: What is the diagnosis?The patient has paradoxical embolism andpatent foramen ovale.
Q2: Describe the pathogenesis of thisclinical condition?A favourable right to left pressure gradient,secondary to raised right atrial pressure (RAP),must exist to promote shunting of venousthrombi through the intracardiac defect. Pul-monary thromboembolism is the most com-mon cause of acute elevation of RAP. Occlu-sion of left pulmonary artery causes a rise inmean pulmonary arterial pressures with asimultaneous fall in systemic arterial pressure.Favourable pressure gradient only exists whenat least one third of the pulmonary arterial treeis occluded or when the mean pulmonary arte-rial for right to left shunting at least 30 mmHg.1
Q3: How should the diagnosis be made?Four criteria have to be met for diagnosis: (1)deep vein thrombosis and/or pulmonarythromboembolism, (2) an abnormal communi-cation between the venous systemic circula-tion, (3) clinical, angiographic, and pathologi-cal evidence for systemic embolism, and (4)pressure gradient allowing right to left shuntingat some point in the cardiac cycle.1 Clinically,the diagnosis of paradoxical embolism ispresumptive, relying on circumstantial evi-dence as well as a high index of suspicion. Pre-morbid diagnosis of patent foramen ovale isusually made by transthoracic or transoesopha-geal colour Doppler echocardiography (TTEor TOE). Studies as well as our case confirmthe superiority of TOE over TTE in detectingpatent foramen ovale.1 2 For the diagnosis,Chen et al reported that TOE had a sensitivityof 100% and a specificity of 97%, while theywere 63% and 78% respectively for TTE.2
In this case, postoperative TOE revealed alarge atrial septal defect with a free left to rightflow and thrombus in the right middle pulmo-nary artery.
Q4: Describe the most recentdevelopment in the diagnosis of thiscondition?It was suggested that contrast echocardio-graphy is a useful and probably more eVectivemanoeuvre to exclude patent foramen ovale.1 Itinvolves high pressure injection into the venouscirculation of a saline solution containingmicrobubbles in suspension. A valsalva ma-noeuvre can increase the sensitivity of the con-trast study. However, it was also reported thatthe cough test is superior to the valsalvamanoeuvre in the contrast study.
Recently, contrast transcranial Doppler(TCD) was shown to have a sensitivity andspecificity of 100% in comparison with con-trast TOE.1 Therefore, contrast TCD can bean alternative method for detection of right toleft shunting.
Q5: What is the treatment?Our patient was started on intravenous heparininfusion. She was taken to theatre for an emer-gency caesarean section and bilateral femoralembolectomies. The baby was delivered un-eventfully. Anticoagulation was continuedpostoperatively and the mother made anuncomplicated recovery. It is planned to closethe atrial septal defect in the near future.
As part of acute management,3 most authorsagree that immediate anticoagulation shouldbe started in the absence of any contradiction.Thrombolysis or embolectomy is indicated totreat peripheral embolism which threatens limbviability. In suspected cases of paradoxicalembolism, thrombolysis is indicated in thepresence of both pulmonary thromboembo-lism and acute cor pulmonale.
Thrombolysis can reduce RAP and minimiserecurrence of paradoxical embolism.1 As forthe patient who is haemodynamically compro-mised, pulmonary embolectomy should beperformed if indicated and feasible. Rarely,impending paradoxical embolism is best man-aged with intracardiac embolectomy and clo-sure of patent foramen ovale.1
Current long term therapeutic options are:(1) long term anticoagulation therapy, (2) longterm antithrombotic therapy, (3) surgicalclosure of patent foramen ovale either openheart surgery or transcatheter placement of thedouble umbrella device, or (4) inferior venacava (Greenfield) filter. Until now, there hasbeen little information regarding the long termoutcome of any particular treatment modality.1
DiscussionFor venous thromboses to travel into thesystemic circulation the clot has to bypass thepulmonary bed by passage through an abnor-mal communication. This may be a fixed atrialseptal defect or a patent foramen ovale whichallows right to left shunting when the rightatrial pressure RAP is raised by a pulmonarythromboembolism.1 It was first diagnosed in1877 by Cohnheim,4 and although cases arenot infrequently reported, it was rarely de-scribed in pregnancy.5
Aburahma reported that 56% of cases ofemboli had probable or possible paradoxicalembolism,3 while Caplan et al reported that36% of embolic strokes had an unidentifiablecardiac source.6 Importantly, Lechat et alshowed that patent foramen ovale was found in40% of patients with unexplained embolicstroke compared with 10% in a control group.7
Patent foramen ovale occurs in 11% to 35% ofthe normal population and grows larger withage.8
In our case, the clinical features werestrongly suggestive of a large pulmonarythromboembolism in association with acuteperipheral arterial ischaemia, giving a strongsuspicion of the diagnosis of paradoxicalembolism. It is interesting that the TTE didnot suggest paradoxical embolism but thepostoperative TOE did show the atrial septaldefect and clot in the pulmonary artery. This isin keeping with studies which have shown the
666 Self assessment answers
www.postgradmedj.com
group.bmj.com on April 18, 2012 - Published by pmj.bmj.comDownloaded from

superiority of TOE against TTE in detectingpatent foramen ovale.2
The contrast echocardiogram, especiallywith the valsalva manoeuvre and cough test, isuseful for excluding patent foramen ovale.1
Contrast transcranial Doppler can be an alter-native method for detection of right to leftshunting. We showed the extent of the periph-eral clot in our patient by angiography, which issafe for the fetus in the third trimester, but wehad considered magnetic resonance angio-graphy, which is less invasive and also safe inpregnancy.9
Normally, management of patients withparadoxical embolism would be determined bythe need to re-establish peripheral flow, if pos-sible; to prevent further arterial embolisation;and to reduce the haemodynamic threat fromthe pulmonary embolus. This may require that,in addition to immediate anticoagulation, bothvenous and peripheral thrombolysis should beconsidered. We felt that thrombolysis, whichhas been advocated to reduce RAP andminimise recurrence of paradoxical embolism,would threaten the pregnancy,10 and that surgi-cal embolectomy and caesarean delivery wouldoVer the safest solution. Placement of an infe-rior vena cava filter before section to preventfurther pulmonary emboli was considered but
as the pelvic veins were patent on ultrasound, itwas considered unnecessary. After successfuldelivery, the TOE confirmed atrial septaldefect and the patient is awaiting surgicalclosure at present. The complexity of thiscase—which requires specialist obstetric, imag-ing, surgical, intensive care, and anaestheticexpertise—could be used as an argument forlocating obstetric units within general hospitalcentres.
It is interesting to speculate about theoutcome if the peripheral embolus had lodgedin the right internal iliac as well as the left. Theuterine artery supplying the placenta wouldhave been occluded with a probable intrauter-ine death. Fortunately, however, this was notthe case and both the mother and baby havedone well.
The high prevalence of clinically occult deepvein thrombosis and the presence of patentforamen ovale in up to 35% of the populationhighlights the fact that paradoxical embolismmay be the cause of a peripheral or cerebralembolic event more often than is currentlysuggested.
The key points of management are the needfor high index of suspicion, early diagnosis, andtimely intervention with a multidisciplinaryapproach. The long term treatment of para-doxical embolism is less well defined. Morestudies are needed to assess the risk ofrecurrent arterial ischaemic events in the pres-ence of patent foramen ovale as well as toexamine the long term outcome of the respec-tive treatment strategies.
Final diagnosisParadoxical embolism and patent foramenovale.
1 Robert RM III, A Stacey H, Michael SB, et al. ImpendingPDE. Arch Intern Med 1998;158:438–48.
2 Chen W, Kuan P, Lien W, et al. Detection of patent foremenovale by contrast transechocardiogram. Chest 1992;101:1515–20.
3 Aburahma AF, Lucentre FC, Boland JP. Paradoxicalembolism: an under-estimated entity—a plea for compre-hensive workup. J Cardiovasc Surg (Torino) 1990;31:685–92.
4 Cohnheim J. Thrombose und Embolid. Vorlesungen UberAllgemeneine Pathogie.Vol 1. Berlin: Hirschwald, 1877: 136.
5 EVeney DJ, Krupski WC. Paradoxical embolism inpregnancy: an usual thromboembolic event. West J Med1984;140:287–8.
6 Caplan LR, Hier DB, D’Cruz I. Cerebral embolism in theMichael Reese Stroke Registry. Stroke 1983;14:530–6.
7 Lechat P, Mas JI, Lascault G, et al. Prevalence of patentforamen ovale in patients with stroke. N Engl J Med1988;318:1148–52.
8 Hagen PT, Scholz DG, Edwards WD. Incidence and size ofpatent foramen ovale during the first 10 decades of life: anautopsy study of 965 normal hearts. Mayo Clin Proc1984;59:12–20.
9 Dizon-Townson D, Magee KP, Twickler DM, et al. Coarcta-tion of the abdominal aorta in pregnancy: diagnosis by mag-netic resonance imaging. Obstet Gynecol 1995;85(5 pt2):817–19.
10 Turrentine MA, Braems G, Ramirez MM. Use of thrombo-lytics for the treatment of thromboembolic disease duringpregnancy. Obstet Gynecol Surv 1995;50:534–41.
Learning pointsx Prevalence of paradoxical embolism as
the cause of peripheral or cerebralembolic events has been under-estimated
x There is right to left shunting throughatrial septal defect or patent ductusarteriosus when right atrial pressure iselevated by pulmonarythromboembolism
x Transoesophageal echocardiogram issuperior to transthoracicechocardiogram in detecting patentforamen ovale
x Angiography is safe in the third trimesterand magnetic resonance arteriography isless invasive
x Thrombolysis reduces right atrialpressure and prevents recurrence ofpatent ductus arteriosus
x In pregnancy, surgical embolectomy is asafer option
x Acute management requires a high indexof suspicion, early diagnosis, and timelyintervention with a multidisciplinaryapproach
Self assessment answers 667
www.postgradmedj.com
group.bmj.com on April 18, 2012 - Published by pmj.bmj.comDownloaded from

Severe symptomatic hypercalcaemia
Q1: What is your diVerential diagnosis forthis case?The highly sensitive and specific immunomet-ric assays for intact parathyroid hormone(PTH) separates hyperparathyroidism from allother causes of hypercalcaemia.1 With fewexceptions, non-parathyroid causes of hyper-calcaemia are accompanied by low serum con-centrations of intact PTH. Chronic treatmentwith lithium may produce hypercalcaemia thatis associated with high serum intact PTH, aclinical picture indistinguishable from primaryhyperparathyroidism.2 Familial hypocalciurichypercalcaemia must be considered in healthypatients who have had hypercalcaemia sincethe first decade of life; they usually have hypo-calciuria and normal serum concentrations ofintact PTH.3
A solitary parathyroid adenoma is theunderlying pathology in more than 80% ofcases of primary hyperparathyroidism.4 5 Dif-fuse hyperplasia of all parathyroid glandsoccurs in about 15%–20% of patients and mayin about half of these be part of a multipleendocrine neoplasia (MEN).1 Multiple adeno-mas and parathyroid cysts are uncommon, andparathyroid carcinoma is very rare (<1%).1
Acute primary hyperparathyroidism is an unu-sual form of the disease characterised by lifethreatening hypercalcaemia.6 7
Q2: What further investigations wouldyou perform?Ultrasonography demonstrated a nodule of 3cm diameter in the left lower parathyroidgland. Abdominal radiography and ultrasonog-raphy did not reveal nephrocalcinosis or neph-rolithiasis. Bone series were normal. Plasmacalcitonin was 29 ng/l (normal <50 ng/l) andfasting plasma gastrin was 44 ng/l (normal<150 ng/l). The 24 hour urinary free catecho-lamines, dopamine, epinephrine, and nore-pinephrine were normal. In our case, therewere no family history, clinical or laboratoryfindings of MEN 1 (primary hyperparathy-roidism, tumours of the pituitary and pancreas,often associated with Zollinger-Ellison syn-drome) or MEN 2A (primary hyperparathy-roidism, pheochromocytoma, and medullarycarcinoma of the thyroid).
Q3: What is the therapy for the severehypercalcaemia in this case?The patient was treated with saline rehydra-tion, low doses of intravenous frusemide (afterrehydration), intravenous clodronate, and sub-cutaneous calcitonin. Four days after, theblood calcium was 2.2 mmol/l and thecreatinine was 61.9 µmol/l. Parathyroid surgi-cal exploration revealed an enlarged left lowerparathyroid gland. The other three glands werenormal. Removal of the left lower parathyroidgland was performed, and the histopathologi-cal examination demonstrated a 3 cm diameterparathyroid adenoma. Seven days after surgery,intact PTH was 43 µg/l and blood calciumremained normal. Six months later, the patient
remains asymptomatic and blood calcium andintact PTH are normal.
Surgery, with its risks, for all patients withprimary hyperparathyroidism now seems un-wise when many will have no features of meta-bolic bone or renal disease.8 When done by anexperienced parathyroid surgeon, parathyroid-ectomy is curative in more than 90% of cases.1
Medical treatment is intended to lower bloodcalcium to less dangerous levels. However, it isnot necessary to obtain normal levels ofcalcium, and surgery must be carried out assoon as the patients’s clinical condition andmetabolism improve suYciently.7 Emergencyneck exploration should be reserved forunusual patients in whom hypercalcaemia can-not be controlled medically and the clinicalpicture is severe.6
DiscussionHypercalcaemia in an adult who is asympto-matic is usually due to primary hyperparathy-roidism and severe hypercalcaemia suggestscancer or parathyroid carcinoma.1 The clinicalpicture of our case suggests malignancy.Muscle weakness is not common in primaryhyperparathyroidism but is common in acuteprimary hyperparathyroidism, due to the se-vere hypercalcaemia.6 7 The serum creatininewasn’t particularly raised, which is a surprise inview of the very high level of serum calcium;this suggests that our patient’s hypercalcaemiawas of short duration. The proportion ofsymptom-free patients with primary hyperpar-athyroidism has increased since the introduc-tion of the multichannel autoanalyser.4 5 Ourcase had acute primary hyperparathyroidismcaused by a parathyroid adenoma, an unusualform of the disease. Acute primary hyperpar-athyroidism, also called parathyroid intoxica-tion, parathyroid storm or parathyroid crisis, ischaracterised by symptomatic marked hyper-calcaemia with very high serum PTH levelsand with polyuria, dehydration, reduced renalfunction, and worsening hypercalcaemia.6 7
Most cases of acute primary hyperparathy-roidism are due to a parathyroid adenoma.6 7
Some authors do not exclude the parathyroidcarcinoma from the acute primaryhyperparathyroidism.7 Remarkable increases ofPTH are characterisitc of acute primary hyper-parathyroidism, up to values 30 times normallevels.6 7 It has excluded autonomous PTHsecretion as a possible cause of acute primaryhyperparathyroidism, and it has been sug-gested that a sudden increase in the set point ofthe diseased parathyroid cells in the presence ofa huge cell mass accounts in large part for boththe marked hypercalcaemia and elevated PTHlevels in these patients.9 Infections, recent sur-gery, immobilisation, dehydration, and traumaappear to play a prominent part in the acuteprimary hyperparathyroidism.6 7
Frusemide must be used for therapy of thehypercalcaemia after rehydration and withcaution as it counteracts the eVects of rehydra-tion. Saline rehydration reverses the increasedproximal tubular calcium reabsorption, andcalcitonin inhibits the distal tubular calciumreabsorption.
668 Self assessment answers
www.postgradmedj.com
group.bmj.com on April 18, 2012 - Published by pmj.bmj.comDownloaded from

Final diagnosisAcute primary hyperparathyroidism, caused bya solitary parathyroid adenoma.
1 Potts JT Jr. Diseases of the parathyroid gland and otherhyper- and hypocalcemic disorders. In: Fauci AS, Braun-wald E, eds. Harrison’s principles of internal medicine. NewYork: McGraw-Hill, 1998: 2227–47.
2 Mallete LE, Khouri K, Zengotita H, et al. Lithium treatmentincreases intact and midregion parathyroid hormone andparathyroid volume. J Clin Endocrinol Metab 1989;68:654–60.
3 Heath HI. Familial benign (hypocalciuric) hypercalcemia: atroublesome mimic of mild primary hyperparathyroidism.Endocrinol Metab Clin North Am 1989;18:723–40.
4 Heath HWI, Hodgson SF, Kennedy MA. Primaryhyperparathyroidism: incidence, morbidity and potentialeconomic impact in a community. N Engl J Med 1980;302:189–93.
5 Mollerup CL, Bollerslev J, Blichert-Toft M. Primaryhyperparathyroidism: incidence and clinical and biochemi-cal characteristics: a demographic study. Eur J Surg1994;160:485–9.
6 Fitzpatrick LA, Bilezikian JP. Acute primary hyperparathy-roidism. Am J Med 1987;82:275–82.
7 Sarfati E, Desportes L, Gossot D, et al. Acute primaryhyperparathyroidism: experience of 59 cases. Br J Surg1989;76:979–81.
8 Potts JT Jr, Fradkin JE, Aurbach GD, et al. Proceedings ofthe NIH Consensus Development Conference on Diagnosisand Management of Asymptomatic Primary Hyperparathy-roidism. J Bone Miner Res 1991;6(suppl 2):1–165.
9 Schachter PP, Christy MD, Avigad IS, et al. Non-autonomyof parathyroid hormone secretion in acute primary hyper-parathyroidism. Clin Endocrinol (Oxf) 1992;37:565–9.
Learning pointsx Hypercalcaemia with normal or high
PTH levels occurs in primaryhyperparthyroidism, familialhypocalciuric hypercalcaemia andchronic treatment with lithium
x Acute primary hyperparthyroidism is anunusual form of the diseasecharacterised by life threateninghypercalcaemia
x Severe hypercalcaemia suggests canceror parathyroid carcinoma, and acuteprimary hyperparthyroidism constitutesan exception of this assertion
Self assessment answers 669
www.postgradmedj.com
group.bmj.com on April 18, 2012 - Published by pmj.bmj.comDownloaded from
doi: 10.1136/pmj.76.900.661 2000 76: 661-662Postgrad Med J
Sangeet Ghai, Sanjay Thulkar, Prakash Neduvelil Purushothaman, et al. acute leukaemiaMultiple focal lesions in liver and spleen in
http://pmj.bmj.com/content/76/900/661.full.htmlUpdated information and services can be found at:
These include:
serviceEmail alerting
box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in the
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on April 18, 2012 - Published by pmj.bmj.comDownloaded from
Related Documents











