Multidisciplinary lifestyle intervention in the obese: Its impact on patients’ perception of the disease, food and physical exercise N. Piana, D. Battistini, L. Urbani, G. Romani, C. Fatone, C. Pazzagli, L. Laghezza, C. Mazzeschi, P. De Feo* Healthy Lifestyle Institute, (C.U.R.I.A.MO.: Centro Universitario di Ricerca Interdipartimentale Attivita`Motoria), University of Perugia, CURIAMO, Via G. Bambagioni 19, 06126 Perugia, Italy Received 7 June 2011; received in revised form 8 December 2011; accepted 12 December 2011 Available online 11 April 2012 KEYWORDS Exercise; Nutrition; Education; Motivation; Obesity Abstract Background and aims: To be successful, lifestyle intervention in obesity must take into account patients’ views. The aim of the present study, conducted using a narrative- autobiographical approach, was to report on the perception of disease, food and physical exer- cise in a group of 80 obese patients during a structured multidisciplinary lifestyle intervention. Methods and Results: Patients underwent lifestyle intervention, of three months’ duration, structured in the following steps: 1) an initial medical examination; 2) an interview by a psychologist; 3) an assessment by a dietician, 4) a physical examination by a specialist in sports medicine; 5) an individualized program consisting of 24 sessions (two per week) of struc- tured indoor exercise 6) eight sessions of group therapeutic education; 7) Nordic walking activity combined with walking excursions during weekends. All the narrative autobiographic texts obtained during the lifestyle intervention were submitted for content analysis; data were analysed according to the ‘‘grounded theory’’ method. According to patients’ descriptions at the end of the intervention, lifestyle intervention re- sulted in enhanced self-efficacy and a reduction in their dependency on food and people; their fear of change was also diminished because, by undergoing intervention, they had experienced change. Conclusion: The findings made in the present qualitative analysis suggest that whenever multi- disciplinary lifestyle intervention is planned for patients with obesity, it is of the utmost impor- tance to tailor the approach while taking the following key aspects into account: motivation, barriers and/or facilitators in lifestyle change, patients’ perceptions of obesity and relation- ship with food, diet and exercise. ª 2011 Elsevier B.V. All rights reserved. * Corresponding author. Tel.: þ39 07533320; fax: þ39 0755837307. E-mail address: [email protected] (P. De Feo). URL: http://www.unipg.it/curiamo. 0939-4753/$ - see front matter ª 2011 Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.numecd.2011.12.008 Available online at www.sciencedirect.com journal homepage: www.elsevier.com/locate/nmcd Nutrition, Metabolism & Cardiovascular Diseases (2013) 23, 337e343

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Nutrition, Metabolism & Cardiovascular Diseases (2013) 23, 337e343
Available online at www.sciencedirect.com
journal homepage: www.elsevier .com/locate /nmcd
Multidisciplinary lifestyle intervention in the obese:Its impact on patients’ perception of the disease,food and physical exercise
N. Piana, D. Battistini, L. Urbani, G. Romani, C. Fatone, C. Pazzagli,L. Laghezza, C. Mazzeschi, P. De Feo*
Healthy Lifestyle Institute, (C.U.R.I.A.MO.: Centro Universitario di Ricerca Interdipartimentale Attivita Motoria),University of Perugia, CURIAMO, Via G. Bambagioni 19, 06126 Perugia, Italy
Received 7 June 2011; received in revised form 8 December 2011; accepted 12 December 2011Available online 11 April 2012
KEYWORDSExercise;Nutrition;Education;Motivation;Obesity
* Corresponding author. Tel.: þ39 07E-mail address: pierpaolodefeo@gURL: http://www.unipg.it/curiamo
0939-4753/$ - see front matter ª 201http://dx.doi.org/10.1016/j.numecd.
Abstract Background and aims: To be successful, lifestyle intervention in obesity must takeinto account patients’ views. The aim of the present study, conducted using a narrative-autobiographical approach, was to report on the perception of disease, food and physical exer-cise in a group of 80 obese patients during a structured multidisciplinary lifestyle intervention.Methods and Results: Patients underwent lifestyle intervention, of three months’ duration,structured in the following steps: 1) an initial medical examination; 2) an interview bya psychologist; 3) an assessment by a dietician, 4) a physical examination by a specialist insports medicine; 5) an individualized program consisting of 24 sessions (two per week) of struc-tured indoor exercise 6) eight sessions of group therapeutic education; 7) Nordic walkingactivity combined with walking excursions during weekends. All the narrative autobiographictexts obtained during the lifestyle intervention were submitted for content analysis; data wereanalysed according to the ‘‘grounded theory’’ method.
According to patients’ descriptions at the end of the intervention, lifestyle intervention re-sulted in enhanced self-efficacy and a reduction in their dependency on food and people; theirfear of change was also diminished because, by undergoing intervention, they had experiencedchange.Conclusion: The findings made in the present qualitative analysis suggest that whenever multi-disciplinary lifestyle intervention is planned for patients with obesity, it is of the utmost impor-tance to tailor the approach while taking the following key aspects into account: motivation,barriers and/or facilitators in lifestyle change, patients’ perceptions of obesity and relation-ship with food, diet and exercise.ª 2011 Elsevier B.V. All rights reserved.
533320; fax: þ39 0755837307.mail.com (P. De Feo)..
1 Elsevier B.V. All rights reserved.2011.12.008
338 N. Piana et al.
Introduction
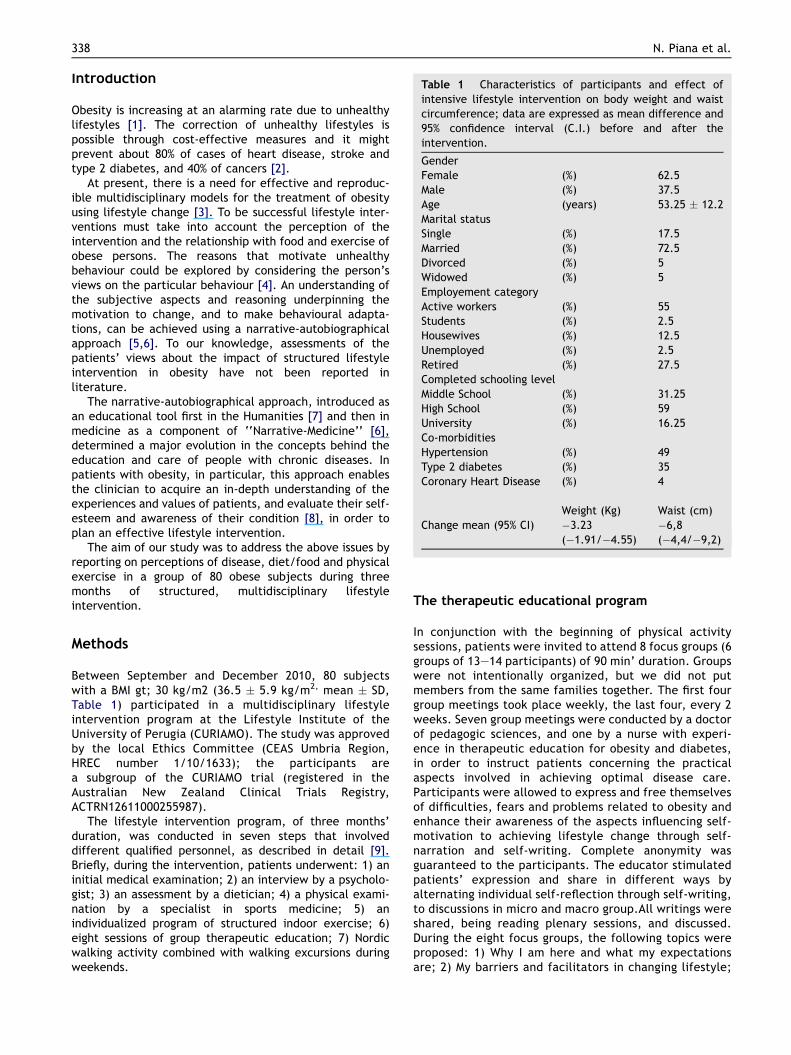
Table 1 Characteristics of participants and effect ofintensive lifestyle intervention on body weight and waist circumference; data are expressed as mean difference and95% confidence interval (C.I.) before and after theintervention.GenderFemale (%) 62.5Male (%) 37.5Age (years) 53.25 � 12.2Marital statusSingle (%) 17.5Married (%) 72.5Divorced (%) 5Widowed (%) 5Employement categoryActive workers (%) 55Students (%) 2.5Housewives (%) 12.5Unemployed (%) 2.5Retired (%) 27.5Completed schooling levelMiddle School (%) 31.25High School (%) 59University (%) 16.25Co-morbiditiesHypertension (%) 49Type 2 diabetes (%) 35Coronary Heart Disease (%) 4
Weight (Kg) Waist (cm)Change mean (95% CI) �3.23
(�1.91/�4.55)�6,8(�4,4/�9,2)
Obesity is increasing at an alarming rate due to unhealthylifestyles [1]. The correction of unhealthy lifestyles ispossible through cost-effective measures and it mightprevent about 80% of cases of heart disease, stroke andtype 2 diabetes, and 40% of cancers [2].
At present, there is a need for effective and reproduc-ible multidisciplinary models for the treatment of obesityusing lifestyle change [3]. To be successful lifestyle inter-ventions must take into account the perception of theintervention and the relationship with food and exercise ofobese persons. The reasons that motivate unhealthybehaviour could be explored by considering the person’sviews on the particular behaviour [4]. An understanding ofthe subjective aspects and reasoning underpinning themotivation to change, and to make behavioural adapta-tions, can be achieved using a narrative-autobiographicalapproach [5,6]. To our knowledge, assessments of thepatients’ views about the impact of structured lifestyleintervention in obesity have not been reported inliterature.
The narrative-autobiographical approach, introduced asan educational tool first in the Humanities [7] and then inmedicine as a component of ‘‘Narrative-Medicine’’ [6],determined a major evolution in the concepts behind theeducation and care of people with chronic diseases. Inpatients with obesity, in particular, this approach enablesthe clinician to acquire an in-depth understanding of theexperiences and values of patients, and evaluate their self-esteem and awareness of their condition [8], in order toplan an effective lifestyle intervention.
The aim of our study was to address the above issues byreporting on perceptions of disease, diet/food and physicalexercise in a group of 80 obese subjects during threemonths of structured, multidisciplinary lifestyleintervention.
Methods
Between September and December 2010, 80 subjectswith a BMI gt; 30 kg/m2 (36.5 � 5.9 kg/m2, mean � SD,Table 1) participated in a multidisciplinary lifestyleintervention program at the Lifestyle Institute of theUniversity of Perugia (CURIAMO). The study was approvedby the local Ethics Committee (CEAS Umbria Region,HREC number 1/10/1633); the participants area subgroup of the CURIAMO trial (registered in theAustralian New Zealand Clinical Trials Registry,ACTRN12611000255987).
The lifestyle intervention program, of three months’duration, was conducted in seven steps that involveddifferent qualified personnel, as described in detail [9].Briefly, during the intervention, patients underwent: 1) aninitial medical examination; 2) an interview by a psycholo-gist; 3) an assessment by a dietician; 4) a physical exami-nation by a specialist in sports medicine; 5) anindividualized program of structured indoor exercise; 6)eight sessions of group therapeutic education; 7) Nordicwalking activity combined with walking excursions duringweekends.
The therapeutic educational program
In conjunction with the beginning of physical activitysessions, patients were invited to attend 8 focus groups (6groups of 13e14 participants) of 90 min’ duration. Groupswere not intentionally organized, but we did not putmembers from the same families together. The first fourgroup meetings took place weekly, the last four, every 2weeks. Seven group meetings were conducted by a doctorof pedagogic sciences, and one by a nurse with experi-ence in therapeutic education for obesity and diabetes,in order to instruct patients concerning the practicalaspects involved in achieving optimal disease care.Participants were allowed to express and free themselvesof difficulties, fears and problems related to obesity andenhance their awareness of the aspects influencing self-motivation to achieving lifestyle change through self-narration and self-writing. Complete anonymity wasguaranteed to the participants. The educator stimulatedpatients’ expression and share in different ways byalternating individual self-reflection through self-writing,to discussions in micro and macro group.All writings wereshared, being reading plenary sessions, and discussed.During the eight focus groups, the following topics wereproposed: 1) Why I am here and what my expectationsare; 2) My barriers and facilitators in changing lifestyle;

Lifestyle intervention in obesity 339
3) My relationship with physical activity; a positive anda negative memory about physical activity; my relation-ship with my body; 4) An image for obesity; 5) Words todescribe obesity: difficulty, nuisance, fear, renounce-ment, my relationship with others and my limits; 6) Myobesity and how it affects my relationship with food; 7)The biomedical aspects of my disease, and the utility ofhelp from a nurse with experience in therapeuticeducation; 8) What my experience at CURIAMO hasmeant?
Data analysis
All the narrative autobiographic texts were submitted forcontent analysis; data analysis carried out using the‘‘grounded theory’’ method [10e12]. The aim of thisanalytical approach is to construct a theory well-groundedin empirical data. Semantic units, extracted from thewritings by means of the so-called ‘‘conceptual labelling’’process, are grouped into micro- and macro-categoriesthrough a process of understanding and interpretation[13]. Following the categorization and grouping, accom-plished by a member of our team (NP), the analysis wassystematically repeated by an independent educator (GR).Whenever a difference in labelling or categorization arose,opinions were compared until the two experts involvedreached an agreement. Saturation was considered achievedwith, at least, ten narratives reporting the same content.The writings were collected after each of the eight groupsessions; the analysis of all the texts was performed at theend of the intervention. An example of the conceptuallabelling and of micro- and macro-categorization of texts isgiven in Table 2.
Results
Based on the significance found through analysis, and thenumbers of concepts, seven key aspects were identified: 1)motivation for lifestyle change; 2) barriers to lifestylechange; 3) facilitators in lifestyle change; 4) perceptions ofobesity; 5) relationship with food; 6) relationship withexercise; 7) perceptions and impact of lifestyle change atthe end of the intervention period.
Motivation for lifestyle change (Table S1)
The data obtained revealed that one of the internal drivesinducing obese subjects to change their lifestyle is theirawareness of the health risks associated with being over-weight; this leads to a wish to lose weight mainly byadopting healthy pursuits and the desire to take control ofone’s own body and disease.
The findings showed that the majority of patients feela pressing need to re-acquire time and to give themselvespriority.
Changing lifestyle and losing weight lead to enhancedphysical and psychological well-being, and greaterconfidence, both in oneself and in one’s future. Many ofthe patients referred for treatment suffered frompsychological conditions, such as distress, depression,anxiety or stress, and reported experiences of grief,
trauma and/or separation. Their motivation for lifestylechange originated in a desire for help, and their awarenessthat they could not cope with their condition single-handed.
Another factor found to play a decisive role in thepatients’ motivation, was the desire to share their experi-ence of obesity, and its treatment, with others like them-selves; the group served both as a resource and a stimulus,as well as a means of escaping from loneliness andsocializing.
Barriers to lifestyle change (Table S1)
One of the most common barriers to lifestyle change isorganization of daily life, a balance being required betweenwork, family and other duties, finding the time to devote tooneself and to physical activity. A further barrier to changehas been found to be lack of determination in pursuing setgoals; subjects being inconstant and lazy, but also fearingfailure.
Achieving change calls for a process of introspection,and brings one’s own world into question, and people arenot always ready to do this. Often one creates an excuse toavoid facing a problem. In some cases, individuals prefer to“let themselves go”, thus surrendering to their difficultywithout reacting. Resistance to change is motivated by thefear of losing the consolidated security of habitualbehaviour.
One of the most critical barriers for most patients istheir difficulty to manage negative moods, which finds animmediate alternative solution in food. Anxiety, stress,loneliness, boredom, a sense of dissatisfaction with one’slife, disappointments and conflicts in relationships withothers are emotional criticalities that find an immediatecomfort in food.
Factors facilitating change in lifestyle (Table S1)
All patients are aware of the importance of motivation asa discriminating factor in achieving the treatment goal.Motivation is, in turn, influenced by several factors. Tosucceed, an important resource is positive thinking,believing in the project with determination, being confi-dent about one’s abilities, and accepting the challenge inorder to prove to oneself, and to others, that success canbe achieved. The key is found in one’s relationship with his/herself. One needs time and space for oneself, one needs tolove oneself and believe in one’s own resources to be ableto make the change.
A further important factor in re-acquiring a healthylifestyle is having correct information on the benefits ofhealthy eating and physical activity. Tangible healthbenefits are important motivators to changing lifestyle.Although patients express an awareness of the importanceof others in their life, they are somewhat ambivalentregarding this issue: “others” can be a barrier if they area source of conflict, but, on the other hand they areconsidered a resource if they provide support. It is impor-tant for patients to realize that they need others in order toeffect change, since asking for help is the first step towardsa cure.

Table 2 An example of the content analysis of text related to physical activity elicited. Only a few examples of conceptuallabels are shown, plus all the categories that contribute to one macro-category.
Conceptual labels Micro-category Macro-category
“Muscle pain” Injuries Before starting the path, negative aspects ofphysical activity prevailed linked to injuries,fatigue, fear of not succeeding and resistance tocertain activities that are not practiced withpleasure and where laziness and low motivationprevail. The bad memories related to physicalactivity strongly influence the current relationshipwith movement
“Injuries, accidents”“Difficulty of movement causedby obesity”
Difficulty of movement
“ Difficulty in tying my shoe-lacesand/or standing up”
“Fatigue, loneliness”“Laziness” Laziness“Little motivation”“Fear of failing” Fear of failure, little
tenacity“Not achieving the target”“Why am I trying?”“I hate running, and doing physicalactivity is unpleasant”
Lack of pleasure
"At school they called me "fatty" andlet me off the activity. I feltexcluded, discriminated against”
Previous negativeexperiences related tophysical activity
"During the secondary school I neverdid sports because I was ashamedof my body, and I was stuck in a rut"
“It frees me from stress and helps meto breathe”
Pleasure, amusement,wellbeing, freedom
Once started with physical activity, one candiscover all the benefits and one changes fromrefusal to awakening. Physical activity helps bothbody and mind, improves personality, helps tofeel alive, free from tensions.It helps one recover self-confidence, improvingthe relationship with the body and leads to amore active life.It enhances health status and brings physicalbenefits.It’s a pleasure, relationship with nature, freedomand it allows one to interact with others
“It gives me a feeling of well-being”“It’s a great pleasure, also for my mind”“It relaxes me above all when done inthe open air”
“A reward after an effort” Satisfaction“When in trouble, say “I did it!”“A new perception of my body” A different relationship
with the body“It helps to find a new and moreconcrete relationship with my body”
“I can have a new, better bodyshape”
“The group” Socialization“Socialization”“The group makes me feel better”“It’s important for my health” Health benefits“It’s a natural way to feel better”“One can see the benefits”“Enjoy the beauty of surrounding nature” Relationship with nature“Relationship with nature”
340 N. Piana et al.
Perceptions of obesity (Table S2)
The writings on disease-related subjective experiences tellof a profound existential unease linked to the condition ofbeing obese. A fat body creates unease, not only in itscarrier, but also in others: the sufferer, considering itcumbersome and unsightly, feels it is better hidden or atleast “disguised”, although, the very fat providesa “protective coat”, thus assuring the obese subject phys-ical and psychological distance from the others.
All the above-described difficulties make obesitya condition incurring social consequences: it is not easy forthe obese to tell others about their problems and feelings,or to share their relationship with food with the non-obese.
Nor is it easy to feel accepted and loved because “theothers” are considered bad, judgmental, and discrimina-tory: the obese are considered inferior and others expressonly a feeling of pain and compassion towards them.Therefore, in order to avoid suffering because of this atti-tude of “others”, obese patients are forced into choosingloneliness and isolation. Frequently family members fail tounderstand an obese family member and behave like all theothers, stressing his or her need to eat less and lose weight.
Relationship with food (Table S2)
Food is a critical factor for obese people because of itsconnotations, and the feelings it can trigger. Often,

Lifestyle intervention in obesity 341
negative feelings find an easy and immediate comfort infood, which becomes a refuge and assures containment ofanxiety.
The family that controls and criticizes generates conflictand triggers negative reactions. Food thus becomes aninstrument in a power struggle, used to protest, expressand demand autonomy.
Change calls for a reorganization of eating behaviour,it becomes necessary to correct inappropriate habitslinked to: greed, disorder, hurried eating, and night-timehunger fits.
Obese patients state that they eat poorly and use verystrong sauces; they can neither satisfy their taste for food,resist the temptation to eat, even though they are aware ofthe damage they are causing themselves.
A controlled diet, considered deprivation, often leadsto transgression with a consequent sense of guilt. Food be-comes an obsession, signifying identity, social recognition,tradition, memory, culture and values; giving it up meanssacrificing something even greater than the food itself.
Relationship with exercise (Table 2)
The negative attitude towards physical activity that pre-vailed in our subjects prior to therapy were linked to a fearof injury, fatigue, failure, and a reluctance to partake inactivities that are not associated with immediate gratifi-cation, laziness and low motivation being prevalent;moreover unpleasant memories related to physical activityhad a markedly negative influence on the patients’ attitudetowards it.
During therapy, the participants started to acknowledgethe positive aspects of physical activity, describing it as anexperience of pleasure, fun and well-being, especiallywhen exercising was undertaken outdoors and in thecompany of others. Movement has positive psychologicaleffects, it makes an individual feel free and combats stress,reinforces self-confidence and enhances harmony betweenbody and mind in general.
Perceptions and impact of lifestyle change at theend of the intervention
According to the patients, the multidisciplinary inter-vention was effective because it integrated expertisewith a genuine desire to help, and technique with affec-tion, thus promoting a feeling of self- confidence andsecurity. The group-members were allowed to expressthemselves freely without incurring judgment; for themajority this provided an outlet, from loneliness inparticular. The patients stated that they experienceda strong emotional involvement, and considered one ofmost beneficial aspects of the group the chance to gothrough again their pain and suffering, and overcomethem. The group generated well-being, serenity and joy;many reported that it had given them, for the first time,the feeling of being really understood, acknowledged andaccepted.
Importantly, the patients’ accounts indicated that theend result of the experience was a change in:
1. self-perception (Table S3);2. relationship with food and physical activity (Table S3);3. health status.
Discussion
Our qualitative analysis suggests tailored lifestyle inter-vention for treatment of obesity, with key requirementsbeing taken into account; some have already been reportedin qualitative studies on obesity [14e18], whereas others,related to the process of lifestyle change, like motivation,facilitators, and barriers, have been identified in thepresent study.
Increased motivation: the factors favouring the decisionto adopt [19,20] a healthy lifestyle are fear of obesity co-morbidities, poor quality of life and a desire to givethemselves priority. Obesity incurs a heaviness of thoughtand movement, limiting small daily acts; obese patients livein fear of not being accepted, and this leads to a wish fora more welcoming world. Consequent to the fear of beingunable to lose weight is the fear of related diseases, whichcan lead to life-long disability.
Change facilitators: (a) a pleasant setting with quali-fied empathetic and enthusiastic operators, (b) the exer-cise program must take into account the poor self-efficacy[19] of patients, who should be followed step by step[19,21]; (c) group activities must also be implemented forexercise training, along with educational sessions dealingwith nutrition and disease and specifically designed tosustain motivation [22e25]. The group meetings triggeredgreater motivation and socialization, allowing participantsto share problems and to find the strength to overcomethem [26].
Addressing barriers to change: barriers to changeinclude lack of self-esteem, loneliness, depression andanxiety, emotional eating [27,28], as well as being ashamedof one’s body [29], laziness, inconstancy, and a reluctanceto acknowledge that obesity is a disease [17,30]. Patients’misgivings should be addressed by the provision of qualifiedsupport, which enhances motivation and ensures constantencouragement. The integrated care model proposed byCURIAMO is thus seen by many as key to success inaddressing obesity.
Knowledge of disease: patients should be made aware ofthe biomedical aspects of obesity and its related compli-cations, an issue that they frequently underestimate. Infact, self-awareness is crucial to the decisional balance tochange [19]. In our experience, the contribution of theeducator nurse was extremely useful.
Exercise program: this, tailored on the basis of indi-vidual abilities, is designed to improve patients’ self-efficacy by means of progressive increments of workloads.Patients appreciated the opportunity given them to shareexercise sessions with others. The small group enhancedthe perception of exercise as a positive experience, it wasno longer considered a sacrifice. According to patients’view, it is important to preserve the change followingcompletion of the intensive training program.
Nutritional Intervention: following the assessment ofthe nutritional behaviour of patients, counselling shouldbe provided to them to optimize their nutrient intake;

342 N. Piana et al.
nutrition educational groups conducted by dieticians havebeen found effective in achieving this end. Many patientsare discouraged by previous unhelpful attempts and dislikeleaflets with diets that involve weighing the food theyintend to eat.
Changes after the intervention: the impact of thelifestyle intervention on patients’ previous perception ofdisease, food and physical exercise was positive becausethey had experienced change. In particular, they re-ported that they had regained confidence in their owncapacity to cope with obesity; they eat better and witha greater awareness; they are no longer scared aboutexercise, but, on the contrary, it is becoming a pleasantexperience to be included in their everyday life. Thewritings related to what the intervention had meant forthem, were useful to understand that both the group andthe different experts helped the individuals to improvetheir lifestyle.
Any conclusions based on our patients’ perceptionsand views should be interpreted in view of the limitationsof the present study. The views of our patients, ratherthan reflecting those of the obese population at large,pertain to obese individuals desirous of treatment fortheir condition. Most of our patients considered obesitya problem and this contradicts the observation made inliterature on the obese, according to which often peopledo not seek a cure [17,30]. A further limitation is themethodology used by us for the qualitative analysis ofpatients’ perceptions that typically remains “open”. Notheoretical construct can ever be considered finallyshaped, and the process of generating theories can neverbe considered conclusive [13]. In performing a contentanalysis of the participants writings, we fragmentedthem into semantic micro-units, thus sacrificing theoverview of each individual’s entirety and favouringa theoretical choral reconstruction of the group. This isan unavoidable limitation of a method aiming to identifycommon themes through a multiple-eye, cross-sectionalreading of texts.
The present paper, firstly exploring patients’ narrativesduring lifestyle intervention for obesity, indicates thata significant improvement in lifestyle change is possible andthat facilitators to change are the group, a multidisci-plinary approach and the empathetic support of differentoperators, whereas the most significant barriers are lack ofmotivation, low self-esteem, and fear of change. Otherauthors [15] exploring physical activity facilitators andbarriers during and following a supervised exercise programin type 2 diabetes, reached similar conclusions that shouldbe taken into deep consideration in planning lifestyleintervention in obesity.
Acknowledgements
The CURIAMO project is supported by a grant from theDepartment of Health of the Umbria Region (Italy). TheUniversity of Oxford kindly granted us a free licence for theuse of the UKPS outcomes model. Dr. Cristina Fatone isa recipient of a post-doctoral fellowship, supported byNovo Nordisk, Italy. Lifescan Italy kindly donated the soft-ware Eurotouch for clinical data storage.
Appendix A. Supplementary data
Tables S1, S2 and S3 can be found as supplementary dataassociated with this article online at http://dx.doi.org/10.1016/j.numecd.2011.12.008.
References
[1] Finucane MM, Stevens GA, Cowan MJ, Danaei G, Lin JK,Paciorek CJ, et al. National, regional, and global trends inbody-mass index since 1980: systematic analysis of healthexamination surveys and epidemiological studies with 960country-years and 9.1 million participants. Lancet 2011;vol.377:557e67.
[2] Preventing Non-communicable diseases in the workplacethrough diet and physical activity. WH /World Economic forumreport of a joint event. Available from: http://www.weforum.org/pdf/Wellness/WHO-WEF-NCDprevention.pdf. accessed23.05.2011.
[3] Puterbaugh JS. The emperor’s tailors: the failure of themedical weight loss paradigm and its causal role in the obesityof America. Diabetes Obes Metab 2009;11:557e70.
[4] Lidelof A, Nielsen CV, Pedersen BD. Obesity treatment e morethan food and exercise: a qualitative study exploring obeseadolescents’ and their parents’ views on the former’s obesity.International Journal Qualitative Study Health Well-being2010;vol. 5:50e73.
[5] Charon R. Narrative medicine: a model for empathy, reflec-tion, profession, and trust. JAMA 2001;286:1897e990.
[6] Greenhalgh T, Hurwitz B. Narrative based medicine: why studynarrative? BMJ 1999;318:48e50.
[7] Lejeune P. Le pacte autobiographique. Paris: Seuil; 1975.[8] Maldonato A, Piana N, Bloise D, Baldelli A. Optimizing patient
education for people with obesity: possible use of the auto-biographical approach. Patient Education and Counseling2010;79:287e90.
[9] De Feo P, Fatone C, Burani P, Piana N, Pazzagli C, Battistini D,Capezzali D, Pippi R, Chipi B, Mazzeschi C. An innovativemodel for changing the lifestyles of persons with obesityand/or type 2 diabetes mellitus. Journal of EndocrinologicalInvestigation 2011;34:e349e54.
[10] Anderson RM, Robins LS. How do we know? Reflections onqualitative research in diabetes. Diabetes Care 1998;21:1387e8.
[11] Dahlgren L, Emmelin M, Winkvist A. Qualitative methodologyfor international public health, vol. 2. Umea University; 2007.
[12] Strauss A, Corbin J. Basics of qualitative research: groundedtheory procedures and techniques. Newbury Park, CA: Sage;1980.
[13] Glaser B. Doing grounded theory: issues and discussions. MillValley (CA): Sociology Press; 1998.
[14] Lindvall K, Larsson C, Weinehall L, Emmelin M. Weight main-tenance as a tight rope walk - a Grounded Theory study. BMCPublic Health 2010; Feb 1;10:51.
[15] Casey D, De Civita M, Dasgupta K. Understanding physicalactivity facilitators and barriers during and following a super-vised exercise programme in Type 2 diabetes: a qualitativestudy. DiabeticMedicine 2010;27:79e84.
[16] Beresford SA, Locke E, Bishop S, West B, McGregor BA,Bruemmer B, et al. Worksite study promoting activity andchanges in eating (PACE): design and baseline results. Obesity(Silver Spring) 2007;15(Suppl. 1):4Se15S.
[17] Weaver NF, Hayes L, Unwin NC, Murtagh MJ. "Obesity" and"Clinical Obesity" Men’s understandings of obesity and itsrelation to the risk of diabetes: a qualitative study. BMC PublicHealth 2008; Sep 14;8:311.
Lifestyle intervention in obesity 343
[18] Groven KS, Engelsrud G. Dilemmas in the process of weightreduction: exploring how women experience training asa means of losing weight. International Journal of QualitativeStudies on Health and Well-being 2010;22:5.
[19] Bandura A. Social foundations of thought and action:a social cognitive theory. Englewood Cliffs, NJ: Prentice-Hall; 1986.
[20] Elfhag K, Rossner S. Who succeeds in maintaining weightloss? A conceptual review of factors associated with weight lossmaintenance and weight regain. Obesity Reviews 2008;6:67e85.
[21] Kirk A, De Feo P. Strategies to enhance compliance to physicalactivity for patients with insulin resistance. Appl Physiol NutrMetab 2007;32:549e56.
[22] Wadden T, West D, Neiberg R, Wing R, Ryan D, Johnson K,et al. One-Year weight Losses in the Look AHEAD study:factors associated with success. Obesity (Silver Spring) 2009;17(4):713e22.
[23] Tang TS, Funnell MM, Anderson RM. Group education Strate-gies for diabetes self-Management. Diabetes Spectrum 2006;19(2):99e105.
[24] Heller SR, Clarke P, Daly H, Davis I, McCulloch DK, Allison SP,et al. Group education for obese patients with type 2
diabetes: greater success at less cost. Diabetic Medicine 1988;5:552e6.
[25] Adolfsson ET, Smidec B, Gregebyd E, Fernstrome L, Wikblad K.Implementing empowerment group education in diabetes.Patient Education and Counseling 2004;53:319e24.
[26] Piana N, Maldonato A, Bloise D, Carboni L, Careddu G,Fraticelli E, et al. The narrative-autobiographical approach inthe group education of adolescents with diabetes: a qualita-tive research on its effects. Patient Education and Counseling2010;80:56e63.
[27] Byrne S, Cooper Z, Fairburn C. Weight maintenance andrelapse in obesity: a qualitative study. International Journal ofObesity 2003;27:955e62.
[28] Mobbs O, Crepin C, Thiery C, Golay A, Van der Linden M.Obesity and the four facets of impulsivity. Patient Educationand Counseling 2010;79:372e7.
[29] Carr D, Friedman M. Is obesity stigmatizing? Body weight,perceived discrimination and psychological well-being in theUnited States. Journal of Health and Social Behavior 2005;46:244e59.
[30] Monaghan LF. Body Mass Index, masculinities and moral worth:men’s critical understandings of “appropriates” weight-for-height. Social Health Illness 2007;29(4):584e609.
Related Documents











