Pictorial Essay Multidetector computed tomography and 2- and 3-dimensional postprocessing in the evaluation of congenital thoracic vascular anomalies Aldo Morra, MD a *, Alberto Clemente, MD a,b , Mario Del Borrello, MD a , Salvatore Berretta, MD c , Pietro Greco, MD d a Department of Radiology, Euganea Medica Diagnostic Center, Via Colombo no. 13, 35020, Albignasego (PD), Italy; b Department of Radiology, University of Ferrara, Italy; c Department of Oncological Surgery, University of Catania, Italy; and d Department of Cardiology, Euganea Medica Diagnostic centre, Albignasego (PD), Italy OBJECTIVE: We report examples of congenital anomalies of the thoracic vessels studied with multidetector computed tomography (MDCT), with special respect to bidimensional (2D) and 3-di- mensional (3D) postprocessing. METHODS: Nonselected patients with vascular and nonvascular disorders underwent chest MDCT with the use of a 16-row scanner. Postprocessing was done to obtain 2D and 3D postprocessing images. CONCLUSION: MDCT with 2D and 3D postprocessing is helpful in evaluating complex vascular congenital anomalies of the chest. © 2008 Society of Cardiovascular Computed Tomography. All rights reserved. KEYWORDS: Congential thoracic vascular anomalies; Multidetector row CT; Postprocessing Introduction Congenital anomalies o f t h e thoracic vessels are caused by false embryogenesis and are relatively common. They may cause symptoms and be diagnosed at birth, 1 or they may be asymptomatic and discovered incidentally on imaging. Previously conventional angiography was considered the reference standard for evaluating vascular disease. How- ever, this has largely been supplanted by noninvasive im- aging methods, particularly since the introduction of sophis- ticated diagnostic tools such as magnetic resonance and multidetector computed tomography (MDCT) angiography. This latter technique is capable of studying the entire chest during a single breathhold, and it allows clinicians and radiologists to identify congenital thoracic vascular anom- alies noninvasively. 2 Methods We studied 2705 outpatients, 2103 adult subjects for a nonvascular disorder and 602 adult subjects who were suspected of having vascular or coronary artery disease; all of them were adult (mean age, 58 years), 41% were women and 59% were men. They underwent chest MDCT angiography in the period between December 2003 and December 2007. MDCT scans were performed with the use of a 16-channel MDCT scanner (LightSpeed 16; General Electric Company, Milwaukee, WI). For standard chest CT we used a craniocaudal acquisition, collimation of 3.75 mm, table increase of 27.50 mm, tube voltage of 120 kV, tube current of 250 mA; the data set was then reconstructed with a slice thickness of 1.25 mm. Conflict of interest: The authors report no conflicts of interest. * Corresponding author. E-mail address: [email protected] Submitted January 21, 2008. Accepted for publication May 21, 2008. 1934-5925/$ -see front matter © 2008 Society of Cardiovascular Computed Tomography. All rights reserved. doi:10.1016/j.jcct.2008.05.147 Journal of Cardiovascular Computed Tomography (2008) 2, 245–255

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
P
M3o
AS
a
b
a
I
bmmi
reatmTd
1d
Journal of Cardiovascular Computed Tomography (2008) 2, 245–255
ictorial Essay
ultidetector computed tomography and 2- and-dimensional postprocessing in the evaluationf congenital thoracic vascular anomalies
ldo Morra, MDa*, Alberto Clemente, MDa,b, Mario Del Borrello, MDa,alvatore Berretta, MDc, Pietro Greco, MDd
Department of Radiology, Euganea Medica Diagnostic Center, Via Colombo no. 13, 35020, Albignasego (PD), Italy;Department of Radiology, University of Ferrara, Italy; cDepartment of Oncological Surgery, University of Catania, Italy;
nd dDepartment of Cardiology, Euganea Medica Diagnostic centre, Albignasego (PD), ItalyOBJECTIVE: We report examples of congenital anomalies of the thoracic vessels studied withmultidetector computed tomography (MDCT), with special respect to bidimensional (2D) and 3-di-mensional (3D) postprocessing.
METHODS: Nonselected patients with vascular and nonvascular disorders underwent chest MDCTwith the use of a 16-row scanner. Postprocessing was done to obtain 2D and 3D postprocessing images.
CONCLUSION: MDCT with 2D and 3D postprocessing is helpful in evaluating complex vascularcongenital anomalies of the chest.© 2008 Society of Cardiovascular Computed Tomography. All rights reserved.
KEYWORDS:Congential thoracicvascular anomalies;Multidetector row CT;Postprocessing
ra
M
nsawM2w1scv
ntroduction
Congenital anomalies o f t h e thoracic vessels are causedy false embryogenesis and are relatively common. Theyay cause symptoms and be diagnosed at birth,1 or theyay be asymptomatic and discovered incidentally on
maging.Previously conventional angiography was considered the
eference standard for evaluating vascular disease. How-ver, this has largely been supplanted by noninvasive im-ging methods, particularly since the introduction of sophis-icated diagnostic tools such as magnetic resonance andultidetector computed tomography (MDCT) angiography.his latter technique is capable of studying the entire chesturing a single breathhold, and it allows clinicians and
Conflict of interest: The authors report no conflicts of interest.* Corresponding author.E-mail address: [email protected]
wSubmitted January 21, 2008. Accepted for publication May 21, 2008.
934-5925/$ -see front matter © 2008 Society of Cardiovascular Computed Tomoi:10.1016/j.jcct.2008.05.147
adiologists to identify congenital thoracic vascular anom-lies noninvasively.2
ethods
We studied 2705 outpatients, 2103 adult subjects for aonvascular disorder and 602 adult subjects who wereuspected of having vascular or coronary artery disease;ll of them were adult (mean age, 58 years), 41% wereomen and 59% were men. They underwent chestDCT angiography in the period between December
003 and December 2007. MDCT scans were performedith the use of a 16-channel MDCT scanner (LightSpeed6; General Electric Company, Milwaukee, WI). Fortandard chest CT we used a craniocaudal acquisition,ollimation of 3.75 mm, table increase of 27.50 mm, tubeoltage of 120 kV, tube current of 250 mA; the data set
as then reconstructed with a slice thickness of 1.25 mm.ography. All rights reserved.
FscaM
246 Journal of Cardiovascular Computed Tomography, Vol 2, No 4, July/August 2008
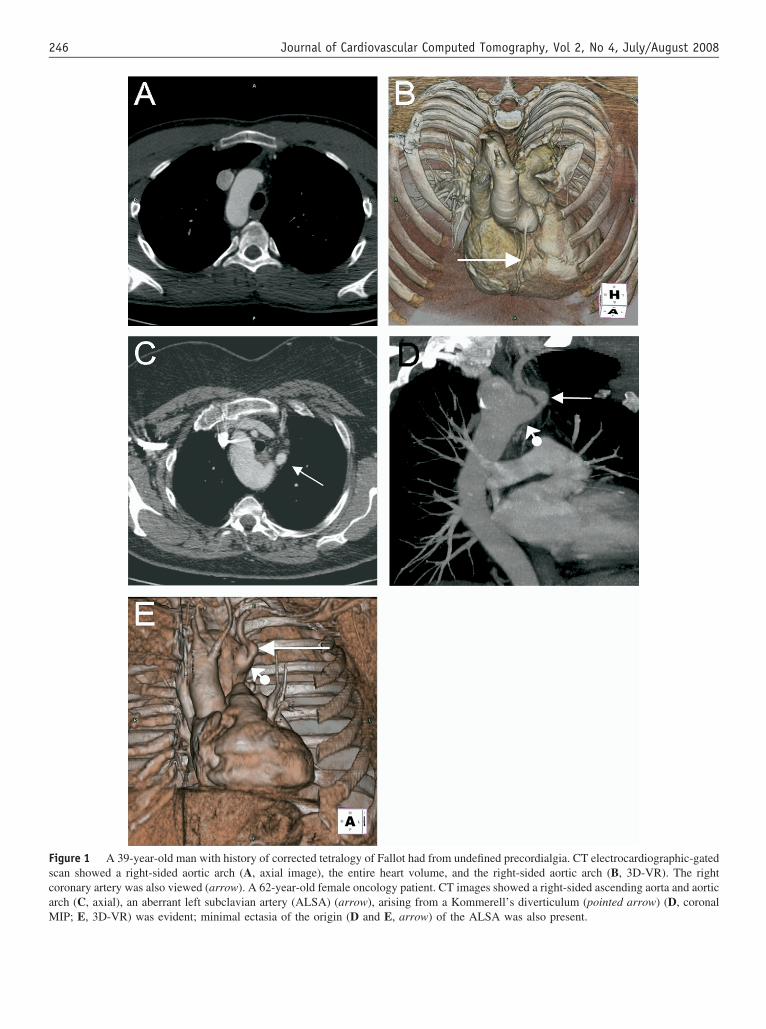
igure 1 A 39-year-old man with history of corrected tetralogy of Fallot had from undefined precordialgia. CT electrocardiographic-gatedcan showed a right-sided aortic arch (A, axial image), the entire heart volume, and the right-sided aortic arch (B, 3D-VR). The rightoronary artery was also viewed (arrow). A 62-year-old female oncology patient. CT images showed a right-sided ascending aorta and aorticrch (C, axial), an aberrant left subclavian artery (ALSA) (arrow), arising from a Kommerell’s diverticulum (pointed arrow) (D, coronal
IP; E, 3D-VR) was evident; minimal ectasia of the origin (D and E, arrow) of the ALSA was also present.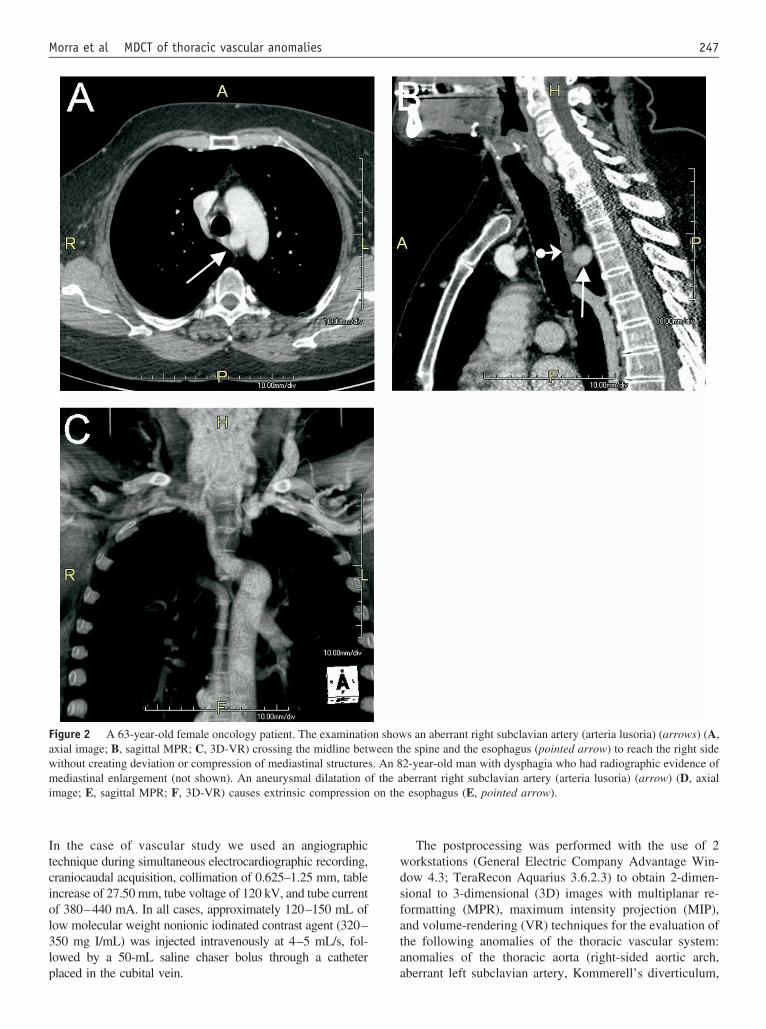
Itciol3lp
wdsfata
Fawmi
247Morra et al MDCT of thoracic vascular anomalies
n the case of vascular study we used an angiographicechnique during simultaneous electrocardiographic recording,raniocaudal acquisition, collimation of 0.625–1.25 mm, tablencrease of 27.50 mm, tube voltage of 120 kV, and tube currentf 380–440 mA. In all cases, approximately 120–150 mL ofow molecular weight nonionic iodinated contrast agent (320–50 mg I/mL) was injected intravenously at 4–5 mL/s, fol-owed by a 50-mL saline chaser bolus through a catheter
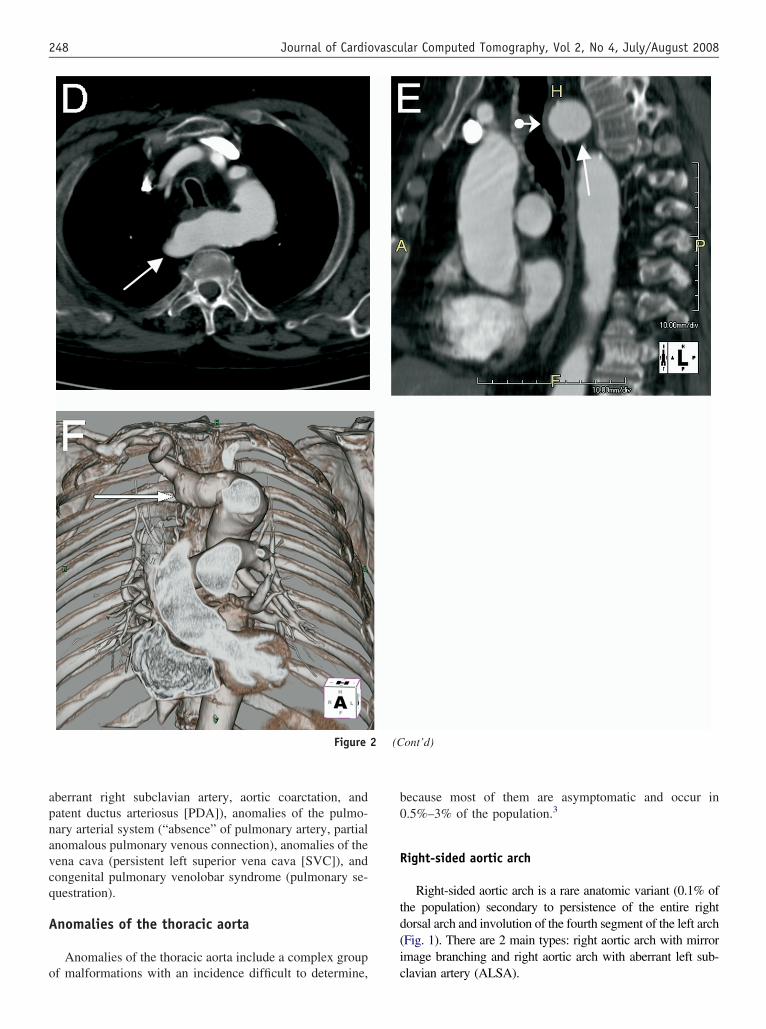
igure 2 A 63-year-old female oncology patient. The examinatioxial image; B, sagittal MPR; C, 3D-VR) crossing the midline betwithout creating deviation or compression of mediastinal structuresediastinal enlargement (not shown). An aneurysmal dilatation o
mage; E, sagittal MPR; F, 3D-VR) causes extrinsic compression
laced in the cubital vein. a
The postprocessing was performed with the use of 2orkstations (General Electric Company Advantage Win-ow 4.3; TeraRecon Aquarius 3.6.2.3) to obtain 2-dimen-ional to 3-dimensional (3D) images with multiplanar re-ormatting (MPR), maximum intensity projection (MIP),nd volume-rendering (VR) techniques for the evaluation ofhe following anomalies of the thoracic vascular system:nomalies of the thoracic aorta (right-sided aortic arch,
s an aberrant right subclavian artery (arteria lusoria) (arrows) (A,e spine and the esophagus (pointed arrow) to reach the right side
2-year-old man with dysphagia who had radiographic evidence ofberrant right subclavian artery (arteria lusoria) (arrow) (D, axialesophagus (E, pointed arrow).
n shoween th
. An 8f the aon the
berrant left subclavian artery, Kommerell’s diverticulum,
apnavcq
A
o
b0
R
td(i
248 Journal of Cardiovascular Computed Tomography, Vol 2, No 4, July/August 2008
berrant right subclavian artery, aortic coarctation, andatent ductus arteriosus [PDA]), anomalies of the pulmo-ary arterial system (“absence” of pulmonary artery, partialnomalous pulmonary venous connection), anomalies of theena cava (persistent left superior vena cava [SVC]), andongenital pulmonary venolobar syndrome (pulmonary se-uestration).
nomalies of the thoracic aorta
Anomalies of the thoracic aorta include a complex group
Figure
f malformations with an incidence difficult to determine, c
ecause most of them are asymptomatic and occur in.5%–3% of the population.3
ight-sided aortic arch
Right-sided aortic arch is a rare anatomic variant (0.1% ofhe population) secondary to persistence of the entire rightorsal arch and involution of the fourth segment of the left archFig. 1). There are 2 main types: right aortic arch with mirrormage branching and right aortic arch with aberrant left sub-
ont’d)
2 (Clavian artery (ALSA).
A
aefr
K
oidccpaa
A
aoa0pfid
A
(oadiola(
P
a(t(cbtao
dtc
A
“
Ftcti
249Morra et al MDCT of thoracic vascular anomalies
berrant left subclavian artery
ALSA occurs in almost all cases of right-sided aorticrch4,5 (Fig. 1). It crosses the midline on the left behind thesophagus. The ALSA is the last of the 4 branches arisingrom the arch and occasionally from an aortic diverticulumepresenting a remnant of the distal primitive left arch.6
ommerell’s diverticulum
Kommerell’s diverticulum is the name of the broad-basedrigin of the root of the subclavian artery (Fig. 1). It can occurn a number of anomalies of the aortic arch system that can, buto not always, cause symptoms of tracheal or esophagealompression. The diverticulum is most frequently present inases of right aortic arch with an ALSA associated with theersistence of the right aortic arch.7 This diverticulum is a rarenomaly, occurring in �1% of the population; it is usuallyssociated to an aneurysm.8
berrant right subclavian artery
Aberrant right subclavian artery (arteria lusoria) (Fig. 2),lso called arteria lusoria (named after lusus naturae, freakf naturae), is an abnormal origin of the right subclavianrtery from the aortic arch. It affects approximately.4%–2% of the population.9 This anomaly is caused by theersistence of the posterior segment of the embryologicourth aortic arc. Usually, it is asymptomatic; very rarely its related to aneurysmal dilatation10,11 (Fig. 2) and causesysphagia (called dysphagia lusoria).
ortic coarctation
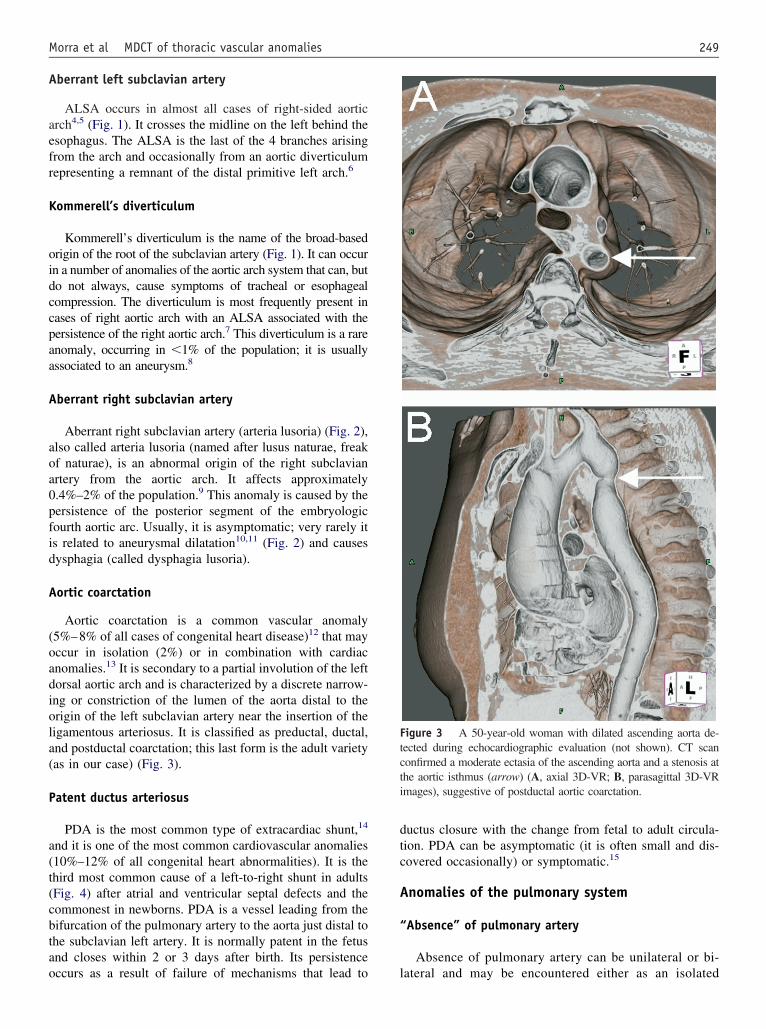
Aortic coarctation is a common vascular anomaly5%–8% of all cases of congenital heart disease)12 that mayccur in isolation (2%) or in combination with cardiacnomalies.13 It is secondary to a partial involution of the leftorsal aortic arch and is characterized by a discrete narrow-ng or constriction of the lumen of the aorta distal to therigin of the left subclavian artery near the insertion of theigamentous arteriosus. It is classified as preductal, ductal,nd postductal coarctation; this last form is the adult varietyas in our case) (Fig. 3).
atent ductus arteriosus
PDA is the most common type of extracardiac shunt,14
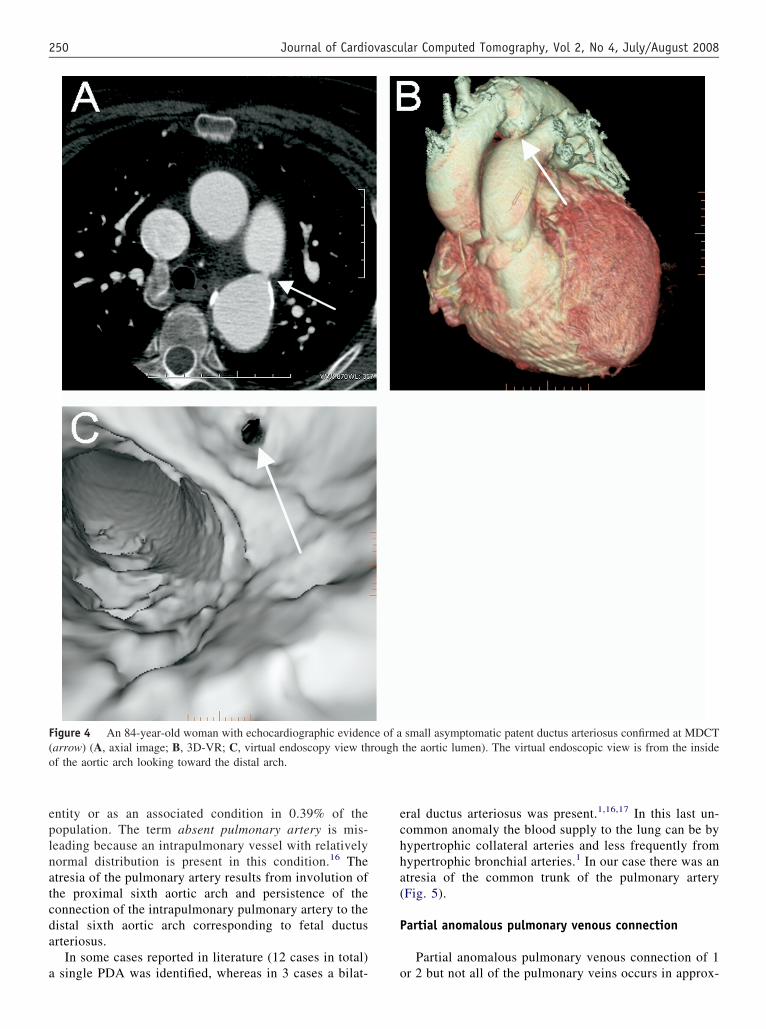
nd it is one of the most common cardiovascular anomalies10%–12% of all congenital heart abnormalities). It is thehird most common cause of a left-to-right shunt in adultsFig. 4) after atrial and ventricular septal defects and theommonest in newborns. PDA is a vessel leading from theifurcation of the pulmonary artery to the aorta just distal tohe subclavian left artery. It is normally patent in the fetusnd closes within 2 or 3 days after birth. Its persistence
ccurs as a result of failure of mechanisms that lead to luctus closure with the change from fetal to adult circula-ion. PDA can be asymptomatic (it is often small and dis-overed occasionally) or symptomatic.15
nomalies of the pulmonary system
Absence” of pulmonary artery
Absence of pulmonary artery can be unilateral or bi-
igure 3 A 50-year-old woman with dilated ascending aorta de-ected during echocardiographic evaluation (not shown). CT scanonfirmed a moderate ectasia of the ascending aorta and a stenosis athe aortic isthmus (arrow) (A, axial 3D-VR; B, parasagittal 3D-VRmages), suggestive of postductal aortic coarctation.
ateral and may be encountered either as an isolated
eplnatcda
a
echha(
P
F(o
250 Journal of Cardiovascular Computed Tomography, Vol 2, No 4, July/August 2008
ntity or as an associated condition in 0.39% of theopulation. The term absent pulmonary artery is mis-eading because an intrapulmonary vessel with relativelyormal distribution is present in this condition.16 Thetresia of the pulmonary artery results from involution ofhe proximal sixth aortic arch and persistence of theonnection of the intrapulmonary pulmonary artery to theistal sixth aortic arch corresponding to fetal ductusrteriosus.
In some cases reported in literature (12 cases in total)
igure 4 An 84-year-old woman with echocardiographic evidenarrow) (A, axial image; B, 3D-VR; C, virtual endoscopy view thf the aortic arch looking toward the distal arch.
single PDA was identified, whereas in 3 cases a bilat- o
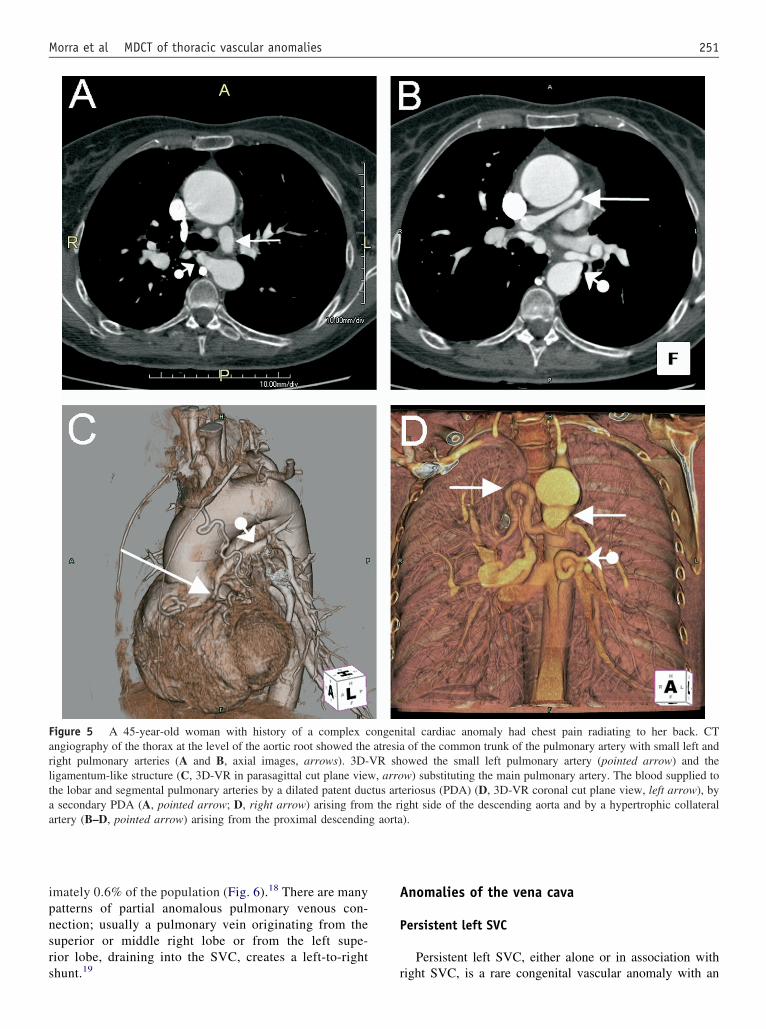
ral ductus arteriosus was present.1,16,17 In this last un-ommon anomaly the blood supply to the lung can be byypertrophic collateral arteries and less frequently fromypertrophic bronchial arteries.1 In our case there was antresia of the common trunk of the pulmonary arteryFig. 5).
artial anomalous pulmonary venous connection
Partial anomalous pulmonary venous connection of 1
small asymptomatic patent ductus arteriosus confirmed at MDCTthe aortic lumen). The virtual endoscopic view is from the inside
ce of arough
r 2 but not all of the pulmonary veins occurs in approx-
ipnsrs
A
P
Farltaa
251Morra et al MDCT of thoracic vascular anomalies
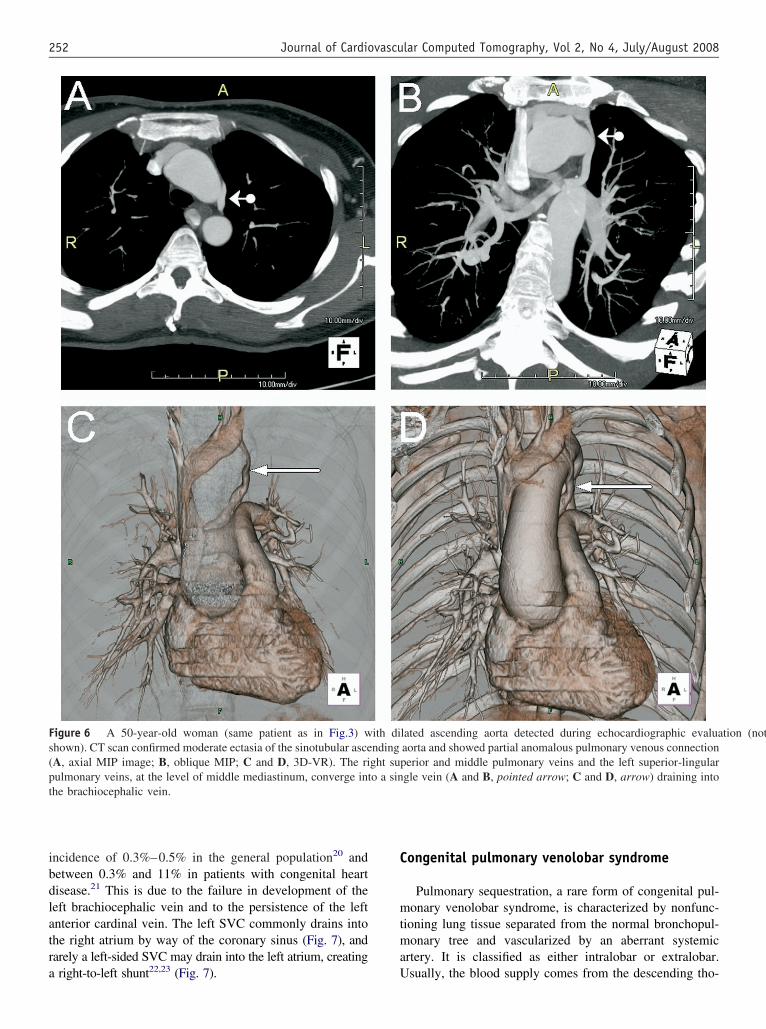
mately 0.6% of the population (Fig. 6).18 There are manyatterns of partial anomalous pulmonary venous con-ection; usually a pulmonary vein originating from theuperior or middle right lobe or from the left supe-ior lobe, draining into the SVC, creates a left-to-right
igure 5 A 45-year-old woman with history of a complex cngiography of the thorax at the level of the aortic root showed theight pulmonary arteries (A and B, axial images, arrows). 3D-igamentum-like structure (C, 3D-VR in parasagittal cut plane viewhe lobar and segmental pulmonary arteries by a dilated patent ducsecondary PDA (A, pointed arrow; D, right arrow) arising from
rtery (B–D, pointed arrow) arising from the proximal descendin
hunt.19 r
nomalies of the vena cava
ersistent left SVC
Persistent left SVC, either alone or in association with
tal cardiac anomaly had chest pain radiating to her back. CTof the common trunk of the pulmonary artery with small left and
owed the small left pulmonary artery (pointed arrow) and thew) substituting the main pulmonary artery. The blood supplied toeriosus (PDA) (D, 3D-VR coronal cut plane view, left arrow), byght side of the descending aorta and by a hypertrophic collateral).
ongeniatresia
VR sh, arro
tus artthe ri
g aorta
ight SVC, is a rare congenital vascular anomaly with an
ibdlatra
C
mtma
Fs(pt
252 Journal of Cardiovascular Computed Tomography, Vol 2, No 4, July/August 2008
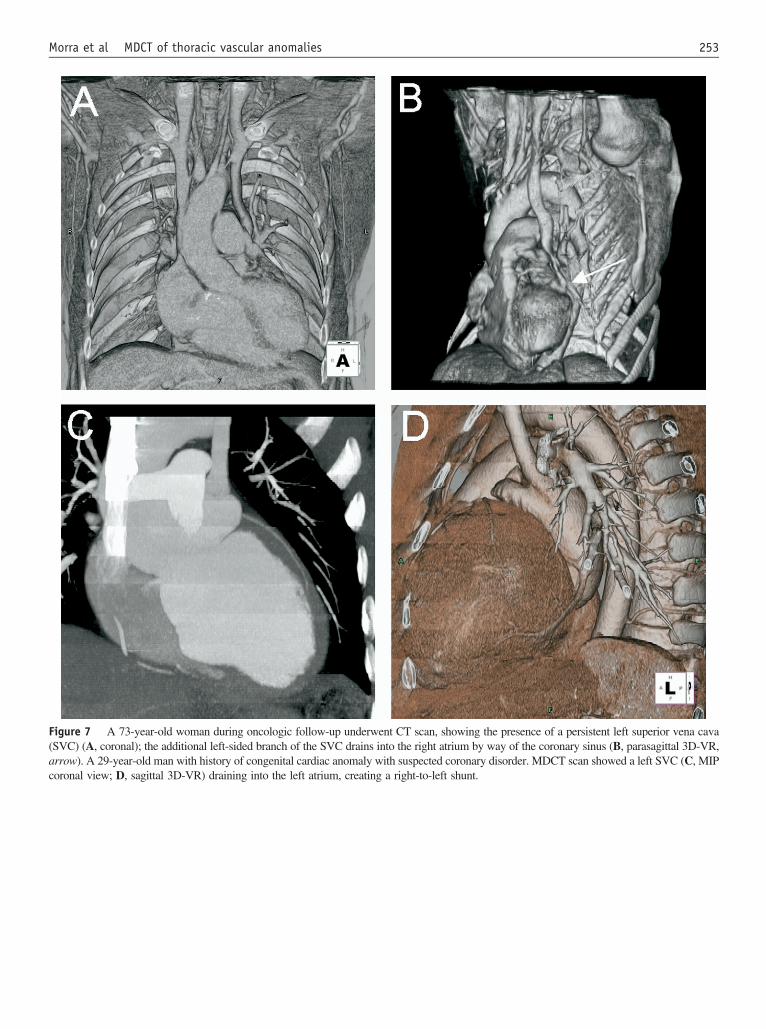
ncidence of 0.3%–0.5% in the general population20 andetween 0.3% and 11% in patients with congenital heartisease.21 This is due to the failure in development of theeft brachiocephalic vein and to the persistence of the leftnterior cardinal vein. The left SVC commonly drains intohe right atrium by way of the coronary sinus (Fig. 7), andarely a left-sided SVC may drain into the left atrium, creating
igure 6 A 50-year-old woman (same patient as in Fig.3) with dhown). CT scan confirmed moderate ectasia of the sinotubular asceA, axial MIP image; B, oblique MIP; C and D, 3D-VR). The riulmonary veins, at the level of middle mediastinum, converge inthe brachiocephalic vein.
right-to-left shunt22,23 (Fig. 7). U
ongenital pulmonary venolobar syndrome
Pulmonary sequestration, a rare form of congenital pul-onary venolobar syndrome, is characterized by nonfunc-
ioning lung tissue separated from the normal bronchopul-onary tree and vascularized by an aberrant systemic
rtery. It is classified as either intralobar or extralobar.
scending aorta detected during echocardiographic evaluation (notaorta and showed partial anomalous pulmonary venous connectionperior and middle pulmonary veins and the left superior-lingulargle vein (A and B, pointed arrow; C and D, arrow) draining into
ilated andingght suo a sin
sually, the blood supply comes from the descending tho-
F(ac
253Morra et al MDCT of thoracic vascular anomalies
igure 7 A 73-year-old woman during oncologic follow-up underwent CT scan, showing the presence of a persistent left superior vena cavaSVC) (A, coronal); the additional left-sided branch of the SVC drains into the right atrium by way of the coronary sinus (B, parasagittal 3D-VR,rrow). A 29-year-old man with history of congenital cardiac anomaly with suspected coronary disorder. MDCT scan showed a left SVC (C, MIPoronal view; D, sagittal 3D-VR) draining into the left atrium, creating a right-to-left shunt.
Ftpae
254 Journal of Cardiovascular Computed Tomography, Vol 2, No 4, July/August 2008
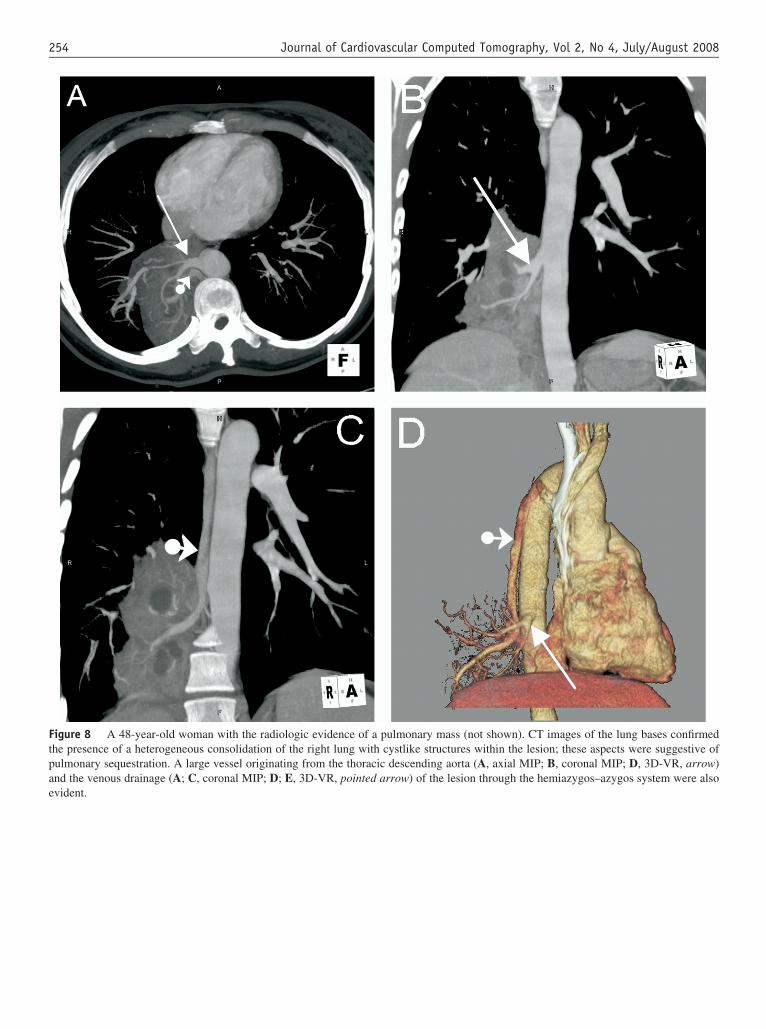
igure 8 A 48-year-old woman with the radiologic evidence of a pulmonary mass (not shown). CT images of the lung bases confirmedhe presence of a heterogeneous consolidation of the right lung with cystlike structures within the lesion; these aspects were suggestive ofulmonary sequestration. A large vessel originating from the thoracic descending aorta (A, axial MIP; B, coronal MIP; D, 3D-VR, arrow)nd the venous drainage (A; C, coronal MIP; D; E, 3D-VR, pointed arrow) of the lesion through the hemiazygos–azygos system were also
vident.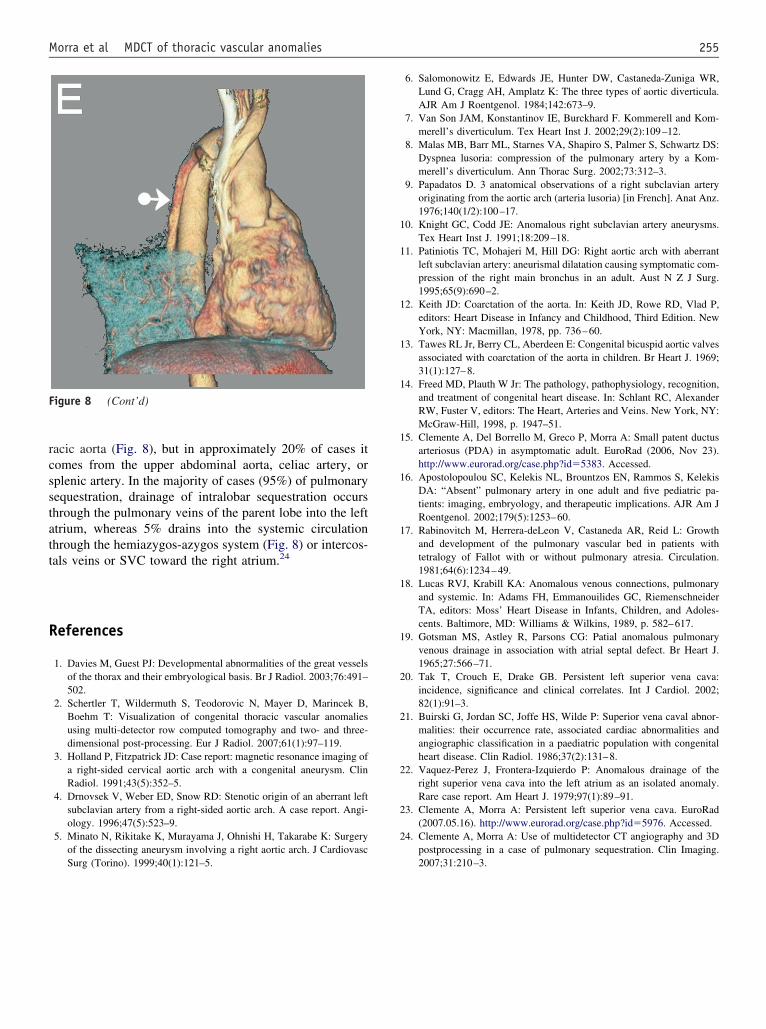
rcsstatt
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
F
255Morra et al MDCT of thoracic vascular anomalies
acic aorta (Fig. 8), but in approximately 20% of cases itomes from the upper abdominal aorta, celiac artery, orplenic artery. In the majority of cases (95%) of pulmonaryequestration, drainage of intralobar sequestration occurshrough the pulmonary veins of the parent lobe into the lefttrium, whereas 5% drains into the systemic circulationhrough the hemiazygos-azygos system (Fig. 8) or intercos-als veins or SVC toward the right atrium.24
eferences
1. Davies M, Guest PJ: Developmental abnormalities of the great vesselsof the thorax and their embryological basis. Br J Radiol. 2003;76:491–502.
2. Schertler T, Wildermuth S, Teodorovic N, Mayer D, Marincek B,Boehm T: Visualization of congenital thoracic vascular anomaliesusing multi-detector row computed tomography and two- and three-dimensional post-processing. Eur J Radiol. 2007;61(1):97–119.
3. Holland P, Fitzpatrick JD: Case report: magnetic resonance imaging ofa right-sided cervical aortic arch with a congenital aneurysm. ClinRadiol. 1991;43(5):352–5.
4. Drnovsek V, Weber ED, Snow RD: Stenotic origin of an aberrant leftsubclavian artery from a right-sided aortic arch. A case report. Angi-ology. 1996;47(5):523–9.
5. Minato N, Rikitake K, Murayama J, Ohnishi H, Takarabe K: Surgeryof the dissecting aneurysm involving a right aortic arch. J Cardiovasc
igure 8 (Cont’d)
Surg (Torino). 1999;40(1):121–5.
6. Salomonowitz E, Edwards JE, Hunter DW, Castaneda-Zuniga WR,Lund G, Cragg AH, Amplatz K: The three types of aortic diverticula.AJR Am J Roentgenol. 1984;142:673–9.
7. Van Son JAM, Konstantinov IE, Burckhard F. Kommerell and Kom-merell’s diverticulum. Tex Heart Inst J. 2002;29(2):109–12.
8. Malas MB, Barr ML, Starnes VA, Shapiro S, Palmer S, Schwartz DS:Dyspnea lusoria: compression of the pulmonary artery by a Kom-merell’s diverticulum. Ann Thorac Surg. 2002;73:312–3.
9. Papadatos D. 3 anatomical observations of a right subclavian arteryoriginating from the aortic arch (arteria lusoria) [in French]. Anat Anz.1976;140(1/2):100–17.
0. Knight GC, Codd JE: Anomalous right subclavian artery aneurysms.Tex Heart Inst J. 1991;18:209–18.
1. Patiniotis TC, Mohajeri M, Hill DG: Right aortic arch with aberrantleft subclavian artery: aneurismal dilatation causing symptomatic com-pression of the right main bronchus in an adult. Aust N Z J Surg.1995;65(9):690–2.
2. Keith JD: Coarctation of the aorta. In: Keith JD, Rowe RD, Vlad P,editors: Heart Disease in Infancy and Childhood, Third Edition. NewYork, NY: Macmillan, 1978, pp. 736–60.
3. Tawes RL Jr, Berry CL, Aberdeen E: Congenital bicuspid aortic valvesassociated with coarctation of the aorta in children. Br Heart J. 1969;31(1):127–8.
4. Freed MD, Plauth W Jr: The pathology, pathophysiology, recognition,and treatment of congenital heart disease. In: Schlant RC, AlexanderRW, Fuster V, editors: The Heart, Arteries and Veins. New York, NY:McGraw-Hill, 1998, p. 1947–51.
5. Clemente A, Del Borrello M, Greco P, Morra A: Small patent ductusarteriosus (PDA) in asymptomatic adult. EuroRad (2006, Nov 23).http://www.eurorad.org/case.php?id�5383. Accessed.
6. Apostolopoulou SC, Kelekis NL, Brountzos EN, Rammos S, KelekisDA: “Absent” pulmonary artery in one adult and five pediatric pa-tients: imaging, embryology, and therapeutic implications. AJR Am JRoentgenol. 2002;179(5):1253–60.
7. Rabinovitch M, Herrera-deLeon V, Castaneda AR, Reid L: Growthand development of the pulmonary vascular bed in patients withtetralogy of Fallot with or without pulmonary atresia. Circulation.1981;64(6):1234–49.
8. Lucas RVJ, Krabill KA: Anomalous venous connections, pulmonaryand systemic. In: Adams FH, Emmanouilides GC, RiemenschneiderTA, editors: Moss’ Heart Disease in Infants, Children, and Adoles-cents. Baltimore, MD: Williams & Wilkins, 1989, p. 582–617.
9. Gotsman MS, Astley R, Parsons CG: Patial anomalous pulmonaryvenous drainage in association with atrial septal defect. Br Heart J.1965;27:566–71.
0. Tak T, Crouch E, Drake GB. Persistent left superior vena cava:incidence, significance and clinical correlates. Int J Cardiol. 2002;82(1):91–3.
1. Buirski G, Jordan SC, Joffe HS, Wilde P: Superior vena caval abnor-malities: their occurrence rate, associated cardiac abnormalities andangiographic classification in a paediatric population with congenitalheart disease. Clin Radiol. 1986;37(2):131–8.
2. Vaquez-Perez J, Frontera-Izquierdo P: Anomalous drainage of theright superior vena cava into the left atrium as an isolated anomaly.Rare case report. Am Heart J. 1979;97(1):89–91.
3. Clemente A, Morra A: Persistent left superior vena cava. EuroRad(2007.05.16). http://www.eurorad.org/case.php?id�5976. Accessed.
4. Clemente A, Morra A: Use of multidetector CT angiography and 3Dpostprocessing in a case of pulmonary sequestration. Clin Imaging.
2007;31:210–3.
Related Documents











