Multi-drug Multi-drug Resistant Resistant Tuberculosis Tuberculosis Hail M. Al-Abdely Hail M. Al-Abdely Consultant, Infectious Consultant, Infectious Diseases, KFSH&RC Diseases, KFSH&RC

Multi-drug Resistant Tuberculosis Hail M. Al-Abdely Consultant, Infectious Diseases, KFSH&RC.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Multi-drug Resistant Multi-drug Resistant TuberculosisTuberculosisHail M. Al-AbdelyHail M. Al-Abdely
Consultant, Infectious Consultant, Infectious Diseases, KFSH&RCDiseases, KFSH&RC

Presentation OutlinePresentation Outline
Definition of MDR TBDefinition of MDR TB Epidemiology of MDR TBEpidemiology of MDR TB Genesis of MDRGenesis of MDR Mechanism of resistanceMechanism of resistance TreatmentTreatment Chemoprophylaxis for MDR TB Chemoprophylaxis for MDR TB
exposureexposure

Definition of MDR TBDefinition of MDR TB
1950s-1970s: 1950s-1970s: – M. tb resistant to INH, streptomycin M. tb resistant to INH, streptomycin
and/or PASand/or PAS 1980s-current: 1980s-current:
– M. tb resistant to at least INH and M. tb resistant to at least INH and RifampinRifampin

Why INH and RifampinWhy INH and Rifampin Most potent and bacteriocidalMost potent and bacteriocidal Tb can be treated effectively with INH+Rif Tb can be treated effectively with INH+Rif
alonealone Mono-resistance to one of them can be Mono-resistance to one of them can be
treated effectively with a regimen treated effectively with a regimen containing the other agent with very low containing the other agent with very low failure rate (2.5-5%)failure rate (2.5-5%)
Failure rate when INH+Rif resistant is 44% Failure rate when INH+Rif resistant is 44% in non-HIV and 70% in HIV patientsin non-HIV and 70% in HIV patients
Duration required for cure doubles to Duration required for cure doubles to triples.triples.

Tuberculosis notification rates, 2000Tuberculosis notification rates, 2000
25 - 49
50 - 99100 or more
0 - 9
10 - 24
No report
Rate per 100 000
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
Global Tuberculosis Control. WHO Report 2002. WHO/CDS/TB/2002.295
25 - 49
50 - 99100 or more
0 - 9
10 - 24
No report
Rate per 100 000
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
Global Tuberculosis Control. WHO Report 2002. WHO/CDS/TB/2002.295

25 - 49
50 - 99
100 - 300
0 - 9
10 - 24
300 or more
No estimate
Rate per 100 000
Estimated TB incidence rates, 2000Estimated TB incidence rates, 2000
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
Global Tuberculosis Control. WHO Report 2002. WHO/CDS/TB/2002.295

Epidemiology of MDR TBEpidemiology of MDR TB
85,008 (4.5)Western Pacific
75,062 (2.5)Southeast Asia
45,964 (7.9)45,964 (7.9)Eastern Mediterranean
25,199 (1.8)Africa, high HIV
15,014 (1.9)Africa, low HIV
17,269 (5.5)Eastern Europe
8508 (2.2)Latin America
882 (0.7)Established market economies
272,906 (3.2)All countries (n = 136)
No. of MDR TB cases (% of all new cases)Geographic region
Dye et al. Global Burden of Multidrug-Resistant TB. JID 185(8), 2002Dye et al. Global Burden of Multidrug-Resistant TB. JID 185(8), 2002

WHO Surveillance and Incidence of WHO Surveillance and Incidence of MDR TBMDR TB
Country % MDR TB of all new cases
Estonia 14.1
Latvia 9.0
China (non-DOTS) 7.7
China (DOTS) 2.8
Russia 6.0
India 3.4
Iran 5.8
Dominican 6.6
Ivory Cost 5.3
Dye et al. Global Burden of Multidrug-Resistant TB. JID 185(8), 2002Dye et al. Global Burden of Multidrug-Resistant TB. JID 185(8), 2002
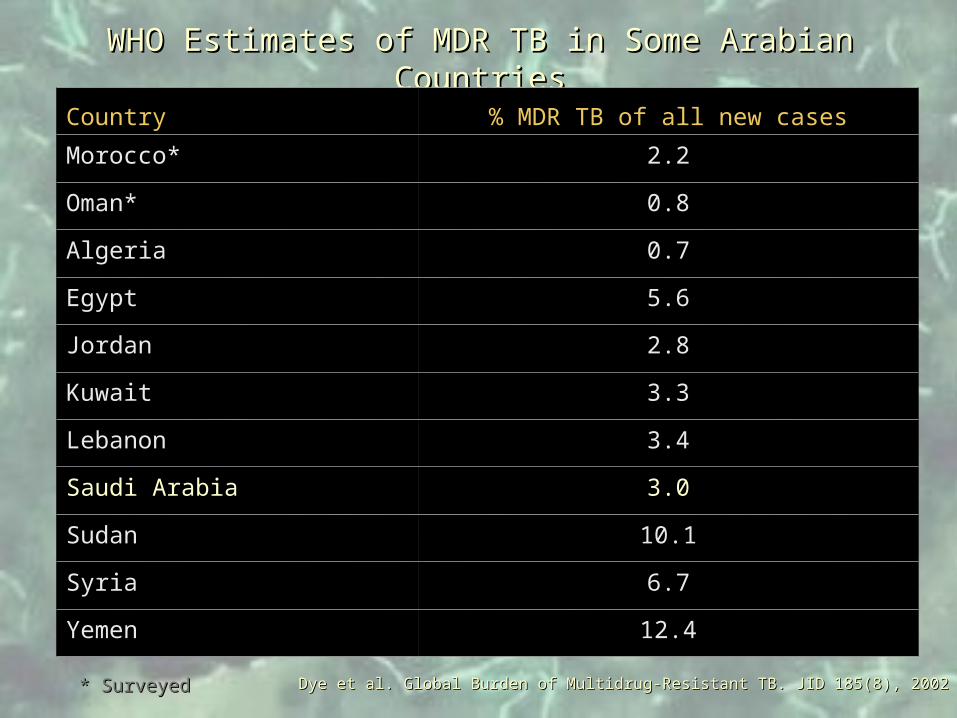
WHO Estimates of MDR TB in Some Arabian CountriesWHO Estimates of MDR TB in Some Arabian Countries
Country % MDR TB of all new cases
Morocco* 2.2
Oman* 0.8
Algeria 0.7
Egypt 5.6
Jordan 2.8
Kuwait 3.3
Lebanon 3.4
Saudi Arabia 3.0
Sudan 10.1
Syria 6.7
Yemen 12.4
Dye et al. Global Burden of Multidrug-Resistant TB. JID 185(8), 2002Dye et al. Global Burden of Multidrug-Resistant TB. JID 185(8), 2002* Surveyed* Surveyed

Genesis of MDR TBGenesis of MDR TB
Resistance is a man-made amplification of a Resistance is a man-made amplification of a natural phenomenon.natural phenomenon.
Inadequate drug delivery is main cause of Inadequate drug delivery is main cause of secondary drug resistance.secondary drug resistance.
Secondary drug resistance is the main cause of Secondary drug resistance is the main cause of primary drug resistance due to transmission of primary drug resistance due to transmission of resistant strains.resistant strains.
MDR due to spontaneous mutations is not MDR due to spontaneous mutations is not possible as the genes encoding resistance for anti possible as the genes encoding resistance for anti TB are unlinked.TB are unlinked.

Strains with genetic drug resistance
Wild M. TB strain
Acquired drug resistance
Primary drug resistance
Spontaneous mutationSpontaneous mutation
Selection: inadequate treatmentSelection: inadequate treatment
TransmissionTransmission
Development of anti-tuberculosis drug resistanceDevelopment of anti-tuberculosis drug resistance
Pablos-Mendez et al. WHO, 1997Pablos-Mendez et al. WHO, 1997

Clinical factors promoting resistanceClinical factors promoting resistance
Delayed diagnosis and isolationDelayed diagnosis and isolation Inappropriate drug regimen.Inappropriate drug regimen.
– Inadequate initial therapyInadequate initial therapy– Incomplete course of treatmentIncomplete course of treatment– Inappropriate treatment modificationsInappropriate treatment modifications– Adding single drug to a failing regimenAdding single drug to a failing regimen– Inappropriate use of chemoprophylaxisInappropriate use of chemoprophylaxis
Poor adherence and incomplete F/UPoor adherence and incomplete F/U Failure to isolate MDR TB patientsFailure to isolate MDR TB patients Failure to employ DOTFailure to employ DOT Over the counter anti TBOver the counter anti TB Faked drugsFaked drugs

Mechanism of ResistanceMechanism of Resistance
TB specific drugsTB specific drugs– INH, PZA, ETHINH, PZA, ETH
Antibiotics with activity against TBAntibiotics with activity against TB– RIFRIF– AminogycosidesAminogycosides– FlouroquinolonesFlouroquinolones
INHINH– Chromosomally mediatedChromosomally mediated– Loss of catalase/peroxidaseLoss of catalase/peroxidase– Mutation in mycolic acid synthesisMutation in mycolic acid synthesis– Regulators of peroxide responseRegulators of peroxide response
Mechanism of resistanceMechanism of resistance
RifampinRifampin– Reduced binding to RNA polymeraseReduced binding to RNA polymerase
Clusters of mutations at “Rifampin Clusters of mutations at “Rifampin Resistance Determining Region” (RRDR)Resistance Determining Region” (RRDR)
– Reduced Cell wall permeabilityReduced Cell wall permeability
Mechanism of resistanceMechanism of resistance

Treatment of MDR TBTreatment of MDR TB
Factors determining SuccessFactors determining Success– Culture of MDR TBCulture of MDR TB– Reliable susceptibilityReliable susceptibility– Reliable history of previous drug Reliable history of previous drug
regimensregimens– Program to assure delivery of prescribed Program to assure delivery of prescribed
drugs (DOT)drugs (DOT)– Correct choice of modified treatment Correct choice of modified treatment
regimenregimen– Reliable follow upReliable follow up
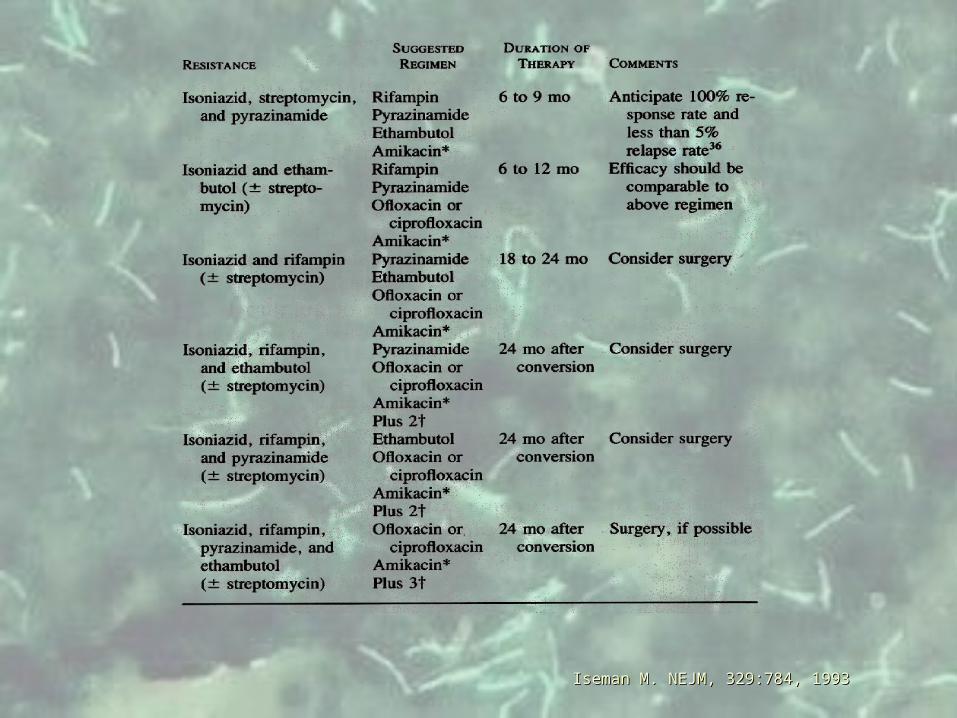
Iseman M. NEJM, 329:784, 1993Iseman M. NEJM, 329:784, 1993
New Chemotherapeutic AgentsNew Chemotherapeutic Agents Not many. Low interest from industryNot many. Low interest from industry Derivatives of RifamycinDerivatives of Rifamycin
– Rifabutin: Sensitive subset of Rifampin resistant strainsRifabutin: Sensitive subset of Rifampin resistant strains– Rifapentine: Extended half-life but more mono-Rifapentine: Extended half-life but more mono-
resistance to rifamycinsresistance to rifamycins– KRM-1648. benzoxazinorifamycin. In vitro and animal KRM-1648. benzoxazinorifamycin. In vitro and animal
models.models. New flouroquinolonesNew flouroquinolones
– Gatifloxacin, Moxifloxacin, levofloxacin, sparfloxacinGatifloxacin, Moxifloxacin, levofloxacin, sparfloxacin NitroimidazolesNitroimidazoles
– related to metronidazole. May work better against latent related to metronidazole. May work better against latent bacillibacilli
Avoiding pro-drug problemsAvoiding pro-drug problems

ChemoprophylaxisChemoprophylaxis
Determinants of interventionDeterminants of intervention– Likelihood of infection with MDR TBLikelihood of infection with MDR TB
LowLow IntermediateIntermediateHighHigh
– Likelihood of developing MDR TBLikelihood of developing MDR TB Immune suppressionImmune suppression

Likelihood of infection with MDR TB
Intermediate to highLow
High possibility for disease
YesNo
Consider Multidrug prophylaxis
Confirmed R to INH+RIF
Standard recommendation
For non-MDR TB contacts
Related Documents











