<< :,¢J,. a >> Home I TOC I [ndex Mucogingival Considerations in Orthodontic Treatment Jan L. Wennstrb'm Alterations in the mucogingival complex will occur during orthodontic tooth movement, but these are independent of the apico-coronal width (height) of the gingiva. The integrity of the periodontium can be maintained during orthodontic therapy also in areas that have only a minimal zone of gingiva. In terms of changes in the position of the soft tissue margin and in gingival dimensions, the important factors to consider are the direction of the tooth movement and the bucco-lingual thickness of the gingiva. Lingual tooth movement will result in an increased bucco-lingual thickness of the tissue at the facial aspect of the tooth which results in coronal migration of the soft tissue margin (decreased clinical crown height). Facial tooth movement, on the other hand, will result in a reduced bucco-lingual tissue thickness and thereby a reduced height of the free gingival portion and an increased clinical crown height. The risk for development of recession type defects in conjunc- tion with orthodontic tooth movement is present only if the tooth has been moved out of the alveolar bone housing, ie, when an alveolar bone dehiscence has been created. (Semin Orthod 1996;2:46-54.) Copyright© 1996 by W.B. Saunders Company A necdotal data, as well as results from clinical and experimental studies, have documented that most forms of orthodontic therapy are innocuous to the periodontium. Hence, appro- priately applied orthodontic forces do not result in permanent damage to a healthy periodon- tium, despite clearly defined structural changes during the active phase of tooth movement. However, an altered position of the tooth may bring about changes in the dimensions of the gingiva and in the position of the soft tissue margin (clinical crown height), and some pa- tients may respond to labial movement of inci- sors and lateral movement of posterior teeth with gingival recession and loss of attachment. 1-2 Since it has been claimed that recession type defects may develop during orthodontic therapy From the Department of Periodontology, Faculty of Odontolog 3, G6teborgUniversity, G6teborg,Sweden. Address correspondenceto Jan L. Wennstr6m, LDS, Odont Dr, Department of Periodontology, Faculty of Odontology, G6teborg University, Box 33070, S-413 90 G6teborg,Sweden. Copyright© 1996 by W.B. Saunders Company 1073-8746/96/0201-000755.00/0 involving teeth that have an inadequate zone of gingiva, ~5 it has been recommended that in areas where the width of gingiva is less than 2 ram, a grafting procedure to increase the gingival di- mension should precede the initiation of orth- odontic therapy. There are consequently two aspects to be discussed in relation to the effect of orthodontic tooth movement on the mucogingi- val complex, namely: 1. Alterations in gingival dimensions and the requirement of a certain gingival width for the maintenance of the integrity of the peri- odontium and 2. Changes in the position of the soft tissue margin and the development of soft tissue recessions. Gingival Dimensions The position in which a tooth erupts through the alveolar process and its eventual position in relation to the bucco-lingual dimension of the alveolar process have a profound influence on the amount of gingiva that will be established 46 Seminars in Orthodontics, Vol 2, No 1 (March), 1996: pp 46-54

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

<< :,¢J,. a >> H o m e I T O C I [ndex
Mucogingival Considerations in Orthodontic Treatment Jan L. Wennstrb'm
Alterations in the mucogingival complex will occur during orthodontic tooth movement, but these are independent of the apico-coronal width (height) of the gingiva. The integrity of the periodontium can be maintained during orthodontic therapy also in areas that have only a minimal zone of gingiva. In terms of changes in the position of the soft tissue margin and in gingival dimensions, the important factors to consider are the direction of the tooth movement and the bucco-lingual thickness of the gingiva. Lingual tooth movement will result in an increased bucco-lingual thickness of the tissue at the facial aspect of the tooth which results in coronal migration of the soft tissue margin (decreased clinical crown height). Facial tooth movement, on the other hand, will result in a reduced bucco-lingual tissue thickness and thereby a reduced height of the free gingival portion and an increased clinical crown height. The risk for development of recession type defects in conjunc- tion with orthodontic tooth movement is present only if the tooth has been moved out of the alveolar bone housing, ie, when an alveolar bone dehiscence has been created. (Semin Orthod 1996;2:46-54.) Copyright© 1996 by W.B. Saunders Company
A necdotal data, as well as results f rom clinical and experimental studies, have documented
that most forms of or thodont ic therapy are innocuous to the per iodont ium. Hence, appro- priately applied or thodont ic forces do not result in p e r m a n e n t damage to a healthy per iodon- tium, despite clearly defined structural changes dur ing the active phase of tooth movement . However, an altered position of the tooth may bring about changes in the dimensions of the gingiva and in the position of the soft tissue margin (clinical crown height) , and some pa- tients may respond to labial movemen t of inci- sors and lateral movemen t of posterior teeth with gingival recession and loss of at tachment. 1-2 Since it has been claimed that recession type defects may develop dur ing or thodont ic therapy
From the Department of Periodontology, Faculty of Odontolog 3, G6teborg University, G6teborg, Sweden.
Address correspondence to Jan L. Wennstr6m, LDS, Odont Dr, Department of Periodontology, Faculty of Odontology, G6teborg University, Box 33070, S-413 90 G6teborg, Sweden.
Copyright © 1996 by W.B. Saunders Company 1073-8746/96/0201-000755.00/0
involving teeth that have an inadequate zone of gingiva, ~5 it has been r e c o m m e n d e d that in areas where the width of gingiva is less than 2 ram, a grafting procedure to increase the gingival di- mension should precede the initiation of orth- odontic therapy. There are consequently two aspects to be discussed in relation to the effect of or thodont ic tooth movemen t on the mucogingi- val complex, namely:
1. Alterations in gingival dimensions and the requ i rement of a certain gingival width for the main tenance of the integrity of the peri- odont ium and
2. Changes in the position of the soft tissue margin and the deve lopment of soft tissue recessions.
Gingival Dimensions
The position in which a tooth erupts through the alveolar process and its eventual position in relation to the bucco-lingual dimension of the alveolar process have a p rofound influence on the amoun t of gingiva that will be established
46 Seminars in Orthodontics, Vol 2, No 1 (March), 1996: pp 46-54

< < ?J-'.l,- ?-- > >
Mucogingival Considerations
Home I TOC I Bndex
47
around the tooth. 6 Accordingly, if a tooth is erupt ing in a labial position in close relationship to the mucogingival line (Fig 1), only a minimal width, or complete lack of gingiva will be found on its facial aspect. Since the prevailing opinion has been that the nonkerat inized and loosely attached lining mucosa is incapable of serving as a defense barr ier for the underlying connective tissue a t tachment to the root, and that a certain apico-coronal width of gingiva (gingival height) is necessary for p roper protection, 5 it has been argued that the width of gingiva has to be increased by surgical means over teeth erupt ing in such a position. However, before a decision is made to surgically increase the gingival zone, one should carefully consider the biological events that take place during the deve lopment of the dentition. In the child the gingival dimen- sions will increase because of growth in the alveolar process and changed position of the teeth in the alveolar process. Longitudinally moni tor ing of the gingival dimensions at the facial aspect of anter ior teeth in the developing dentit ion has shown that a significant increase of the gingival height will take place. 7 Also, the spontaneous change of the tooth position in the bucco-lingual direction that often occurs dur ing the development , will affect the gingival height. 8 Hence, a more lingual posit ioning of the tooth results in an increase of the gingival height (decreased clinical crown height; Fig 2), whereas the opposite will be the case when a tooth moves to a more facial position in the alveolar process.
Figure 1. A mandibular canine erupting in a facial position which has resulted in a minimal width of gingiva. Poor plaque control and obvious signs of gingival inflammation are evident.
Tooth movemen t P
Figure 2. Schematic illustration of the dimensional alterations in the periodontal tissues on the facial aspect of a tooth moved lingually.
There are basically two factors that may ex- plain this alteration in gingival height: (1) a change in the height of the free gingival port ion caused by a change in bucco-lingual thickness of the gingiva and (2) a change in the distance between the genetically def ined position of the mucogingial junct ion and the tooth surface. Clinical and histological evaluations of the dimen- sions of the free gingiva indicate that there is a ratio of about 1:1.5 between its thickeness at the level of the most coronal fiber a t tachment to the root and its height. A tooth facially posit ioned often shows an alveolar bone dehiscence with a thin covering soft tissue, but when moved in a lingual direction into a more p roper position within the alveolar process, the tissue dimen- sions on its facial aspect will increase in thick- ness, 9-1° which in turn results in an increased height of the free gingiva and a decreased clinical crown height. Fur thermore , because the mucogingival line is a stable anatomical land- mark that cannot be permanent ly altered by apically posit ioned flap surgery, u and because the gingiva is anchored to the supracrestal por- tion of the root and therefore will follow the tooth during its movemen t in a lingual direction, the consequence is that the distance between the apical bo rde r of the gingiva, the mucogingival line, and the tooth surface will increase, ie, an increased gingival height.
Surgical wounding of the tooth border ing soft tissue may also influence the dimensions of the gingiva. 12 Heal ing of the per iodontal wound is characterized by the format ion of a granulation
<< ~,r'J,. a >> H o m e I T O C I Bndex
48 Jan L. Wennstr6m
tissue over which epithelial cells migrate from surrounding gingiva a n d / o r alveolar mucosa. Whether keratinization of the covering epithe- lium will occur is determined by the properties of the connective tissue from which the granula- tion tissue originates. 1-~ Granulation tissue de- rived not only from the remaining or adjacent gingiva, but also from the periodontal mem- brane, will form a tissue in the wounded area which in most respects, clinically as well as histologically, is similar to that of a normal gingiva, ie, a dense collagen-rich connective tissue lined by a parakeratinized epithelium.
It has been noted from a number of case reports, however, that if a tooth is erupting in a facial position through the alveolar mucosa, no gingiva will form adjacent to the tooth surface. The fact that a zone of gingiva invariably regener- ates after surgical removal of the entire port ion of this tissue, 12 seems to be contradictory to the observation that no gingiva is formed when the tooth spontaneously erupts through the alveolar mucosa. A likely explanation of this contradic- tion regarding the establishment of a gingival zone may be that, when the tooth during the eruption penetrates into the oral cavity, the reduced enamel epithelium and the epithelium of the alveolar mucosa fuse at the edge of the tooth. This means that no wounding of the connective tissue occurs and, consequently, no granulation tissue formation can take place origi- nating from the periodontal membrane. The marginal soft tissue on the facial aspect of the erupting tooth will therefore be composed of the loose connective tissue of the alveolar mucosa and covered by a nonkeratinized epithelium. If, on the other hand, a wound is created that allows the formation of a granulation tissue derived from the periodontal membrane, a zone of gingiva will be formed during healing.14
The understanding of these biological con- cepts is of importance from a treatment point of view. If a tooth has an erupting position which may result in the positioning of its facial aspect within the alveolar mucosa, one should consider the possibility of surgically uncovering the tooth before it breaks through the mucosa. Such a treatment approach will establish a proper colla- gen-rich, keratinized border tissue around the tooth and will prevent the development of a potential mucogingival problem. Furthermore, taking into account the fact that the gingival
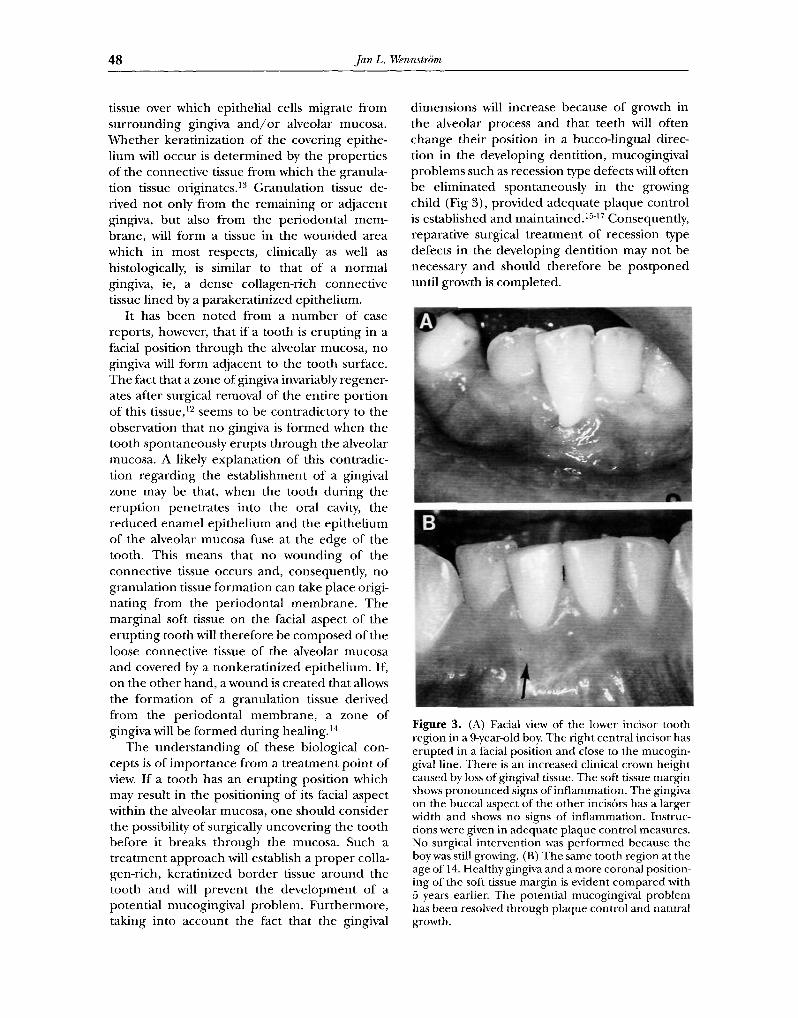
dimensions will increase because of growth in the alveolar process and that teeth will often change their position in a bucco-lingual direc- tion in the developing dentition, mucogingival problems such as recession type defects will often be eliminated spontaneously in the growing child (Fig 3), provided adequate plaque control is established and maintained. 1517 Consequently, reparative surgical treatment of recession type defects in the developing dentition may not be necessary and should therefore be postponed until growth is completed.
Figure 3. (A) Facial view of the lower incisor tooth region in a 9-year-old boy. The right central incisor has erupted in a facial position and close to the mucogin- gival line. There is an increased clinical crown height caused by loss of gingival tissue. The soft tissue margin shows pronounced signs of inflammation. The gingiva on the buccal aspect of the other incis6rs has a larger width and shows no signs of inflammation. Instruc- tions were given in adequate plaque control measures. No surgical intervention was performed because the boy was still growing. (B) The same tooth region at the age of 14. Healthy gingiva and a more coronal position- ing of the soft tissue margin is evident compared with 5 years earlier. The potential mucogingival problem has been resolved through plaque control and natural growth.
< < :"--I-'.1,- ~-- > >
Mucogingival Considerations
Home I TOC I Bndex
49
Requirement of a Certain Gingival Dimension
For many years the presence of an adequate zone of gingiva was considered critical for the mainte- nance of gingival health and for the prevention of continuous loss of connective tissue attach- ment? 8 A concept thus prevailed that a narrow zone of gingiva was insufficient to (1) protect the periodontium from injury caused by friction forces encountered during mastication and (2) dissipate the pull on the soft tissue margin created by the muscles of the adjacent alveolar mucosa. Moreover, it was believed that an inad- equate zone of gingiva would facilitate subgingi- val plaque formation as well as the apical spread of plaque-associated gingival lesions.
The opinions expressed regarding the require- ment of a sufficient width (height) of gingiva for the maintenance of the integrity of the periodon- tium, however, were based mainly on clinical experience and poorly substantiated by scientific evidence. Clinicians had the impression that sites with a narrow zone of gingiva were often in- flamed, whereas the wide zone of gingiva found at neighboring tooth surfaces remained healthy (Fig 4A). Additional support for this clinical impression was obtained from cross-sectional examinations showing that a correlation existed between the presence of recession defects and decreased width of the gingiva. 19 In this context it must be realized, however, that data derived from cross-sectional studies cannot prove or disprove a cause-effect relationship. Conse- quently, data reported from such studies may also be interpreted to show that the formation of a recession defect results in a reduction of the width of the gingiva.
The study by Lang and L6e 2° on the signifi- cance of gingiva for periodontal health conclud- ing that, "2 mm of keratinized gingiva (corre- sponding to 1 mm attached gingiva) is adequate to maintain gingival health," has been widely quoted as a definition as to what constitutes an adequate width of gingiva for the maintenance of periodontal health. However, results obtained from more recent experimental studies, as well as longitudinal studies, in patients showing areas with a minimal zone of gingiva is have all failed to generate support for this definition. In fact, the conclusion that can be drawn from these studies is that a certain quantity of gingiva does not seem
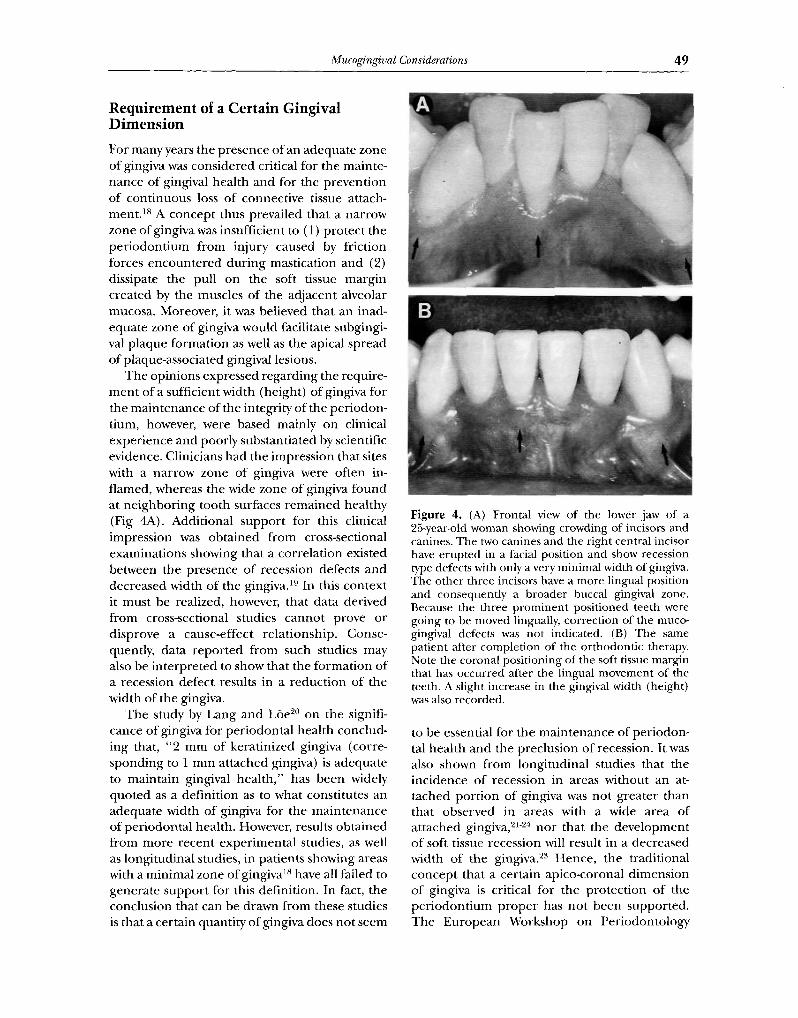
Figure 4. (A) Frontal view of the lower jaw of a 25-year-old woman showing crowding of incisors and canines, The two canines and the right central incisor have erupted in a facial position and show recession type defects with only a very minimal width of gingiva. The other three incisors have a more lingual position and consequently a broader buccal gingival zone. Because the three prominent positioned teeth were going to be moved lingually, correction of the muco- gingival defects was not indicated. (B) The same patient after completion of the orthodontic therapy. Note the coronal positioning of the soft tissue margin that has occurred after the lingual movement of the teeth. A slight increase in the gingival width (height) was also recorded.
to be essential for the maintenance of periodon- tal health and the preclusion of recession. It was also shown from longitudinal studies that the incidence of recession in areas without an at- tached portion of gingiva was not greater than that observed in areas with a wide area of attached gingiva, 21-24 nor that the development of soft tissue recession will result in a decreased width of the gingiva. 23 Hence, the traditional concept that a certain apico-coronal dimension of gingiva is critical for the protection of the periodontium proper has not been supported. The European Workshop on Periodontology

<< :,v'J,. ~ >> H o m e [ T O C [ Bndex
50 Jan L. Wennstr6m
held in 1993 reached the consensus that, "surgi- cal treatment with the sole purpose of increasing the apico-coronal width of the gingiva to main- tain periodontal health and prevent the develop- ment of soft tissue recession cannot be consid- eredjustified."~5
Localized gingival recessions are often found at malaligned teeth that have a buccally deviated position of the root with an accompanying alveo- lar bone dehiscence. Such predisposing alveolar bone dehiscences may also be induced by orth- odontic tooth movement. 9,2~27 Although many etiologic factors have been proposed for local- ized gingival recessions (eg, trauma from occlu- sion, frenum attachments, impingement of restor- ative margins, orthodontic forces), trauma caused by toothbrushing and gingival lesions associated with bacterial plaque must be considered to be the dominating causative factors in orthodontic patients also (for review see~S).
position in the alveolar process, is also accompa- nied with bone formation (Fig 5).
Experimental studies in monkeys have noted that facial tipping, extrusion movements, and bodily movements of incisors will result in reces- sion of the labial gingival margin and loss of attachment. 26,2s However, similar studies per- formed in dogs 9,29 or humans 3° failed to show that labial tooth movement is accompanied with gingival recession and at tachment loss. This discrepancies in the response of the marginal soft tissue to orthodontic therapy in the studies
Orthodontic Tooth MovementnSof t Tissue Alterations
Similar alterations in the gingival dimensions and position of the soft tissue margin, as previ- ously discussed in relation to spontaneous tooth movement, will also occur following orthodonti- tally induced tooth movement. As ment ioned previously, it has been postulated that an alveolar bone dehiscence is a prerequisite for the develop- ment of a recession defect; ie, a root dehiscence may establish an environment which, for one reason or another, is conductive also for loss of gingival tissue. With respect to or thodont ic therapy, this would imply that as long as a tooth is moved exclusively within the alveolar bone, soft tissue recession cannot develop. On the other hand, because such predisposing alveolar bone dehiscences may be induced by uncontrol led facial expansion of teeth through the cortical plate, or thodontic treatment can create a situa- tion that renders the teeth liable to development of recession defects. In this context, experimen- tal studies have shown that labial bone will reform in the area of a dehiscence when the tooth is retracted toward a proper positioning of the root within the alveolar process. 9q° It is therefore likely that the reduction in recession seen at a previously prominent positioned tooth, which has been moved into a more proper
Figure 5. (A) Facial view of an upper right canine in a 22-year-old woman at which the recession increased in depth after the initiation of the orthodontic therapy. Note the healthy gingival condition despite only very narrow gingival height at the buccal aspect. An abra- sion defect is evident in the root surface. The tooth brushing technique was adjusted to minimize the trauma to the tissue. Because the tooth was planned to be moved in disto-lingual direction, surgical correc- tion of the recession defect was postponed until completion of the tooth movement. (B) The tooth after completion of the orthodontic therapy. Note the reduction in the recession and the increase of the gingiva zone that has taken place as a consequence of the changed position of the tooth.

<< :,¢J,. ~ >> H o m e I T O C I Bndex
Mucogingival Considerations 51
referred to are difficult to explain but may be related to differences with respect to (1) the amount of labial tooth displacement, (2) the magnitude of force applied, a n d / o r (3) the presence/absence of plaque and gingival inflam- mation in the regions subjected to tooth move- ment. It was observed that gingival inflammation was consistently present at sites showing obvious signs of recession. 26 In addition, because several of the studies 9,29,3° did not include assessments describing the gingiva, differences in the width of gingiva at the experimental sites may also have accounted for the variability observed in the response of the marginal soft tissue to or thodon- tic tooth movement. The prevailing opinion has been that a narrow or " inadequate" gingival zone is the reason for observed soft tissue reces- sions in conjunction with orthodontic tooth movement. 4
Steiner et a126 speculated on mechanisms by which gingival tissue could be lost as a result of labial tooth movement and suggested that ten- sion in the marginal tissue created by the forces applied to the teeth could be an important factor. If this hypothesis is valid, obviously the volume (thickness) of the gingival tissue at the pressure side, rather than its apico-coronal width,
should determine whether or not soft tissue recession will develop dur ing or thodont ic therapy. To test this hypothesis, an experimental study was per formed in monkeys 27 in which teeth were orthodonticaUy moved into areas with vary- ing thickness and quality of the soft tissues. Following extensive bodily movement of incisors in a labial direction through the alveolar bone (Fig 6), most teeth showed clinically some apical displacement of the gingival margin as well as loss of probing attachment, but no loss of connec- tive tissue at tachment when evaluated histologi- cally (Fig 7). The apical displacement of the gingival margin was minute and the result of a reduced height of the free gingiva only. Histologi- cal evaluation showed that the size of the free gingival unit was considerably smaller at the labially moved incisors, not only in the apico- coronal but also in the bucco-lingual direction, than at the orthodontically untreated control teeth. It is most likely that these dimensional changes of the gingival tissue at the pressure side, in the presence of an alveolar bone dehis- cence, were related to tension, ie, stretching, developing in the soft tissues during the facial tooth movement. As a result of this reduction of the thickness and the height of the free gingiva,
Figure 6. (A) Occlusal view of the maxillary jaw in a monkey showing the position of the central incisors before (A) and after (B) the bodily movement in a labial direction. The canines and lateral incisors were joined in an individually fabricated silver splint and used as anchorage teeth. (B) The buccal aspect of the same incisors before (C), and after (D), the labial tooth movement. No change in the location of the gingival margin has occurred despite the pronounced labial displacement of the incisors. (Reprinted with permission from Wennstr6m et al, 1987, Munksgaard International Publishers Ltd, Copenhagen Denmark. 27)
<< :,FJ,. a >> H o m e I T O C I [ndex
52 Jan L. Wennstr6m
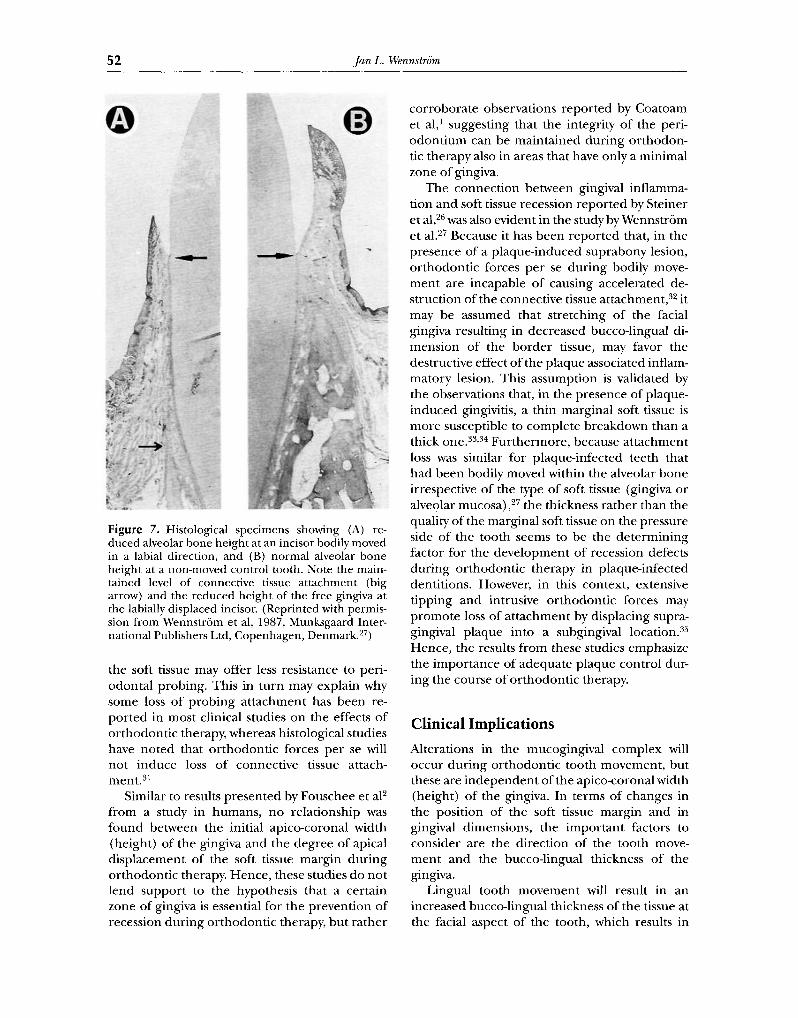
Figure 7. Histological specimens showing (A) re- duced alveolar bone height at an incisor bodily moved in a labial direction, and (B) normal alveolar bone height at a non-moved control tooth. Note the main- tained level of connective tissue attachment (big arrow) and the reduced height of the free gingiva at the labially displaced incisor. (Reprinted with permis- sion from Wennstr6m et al, 1987, Munksgaard Inter- national Publishers Ltd, Copenhagen, Denmark. 27)
the soft tissue may offer less resistance to peri- odontal probing. This in turn may explain why some loss of probing a t tachment has been re- por ted in most clinical studies on the effects of or thodont ic therapy, whereas histological studies have noted that or thodont ic forces per se will not induce loss of connective tissue attach- ment. 31
Similar to results presented by Fouschee et aF f rom a study in humans, no relationship was found between the initial apico-coronal width (height) of the gingiva and the degree of apical displacement of the soft tissue margin dur ing or thodont ic therapy. Hence, these studies do not lend suppor t to the hypothesis that a certain zone of gingiva is essential for the prevent ion of recession during or thodont ic therapy, but ra ther
corrobora te observations repor ted by Coatoam et a l l suggesting that the integrity of the peri- odont ium can be mainta ined during or thodon- tic therapy also in areas that have only a minimal zone of gingiva.
The connect ion between gingival inflamma- tion and soft tissue recession repor ted by Steiner e t al, 26 was also evident in the study by Wennstr6m et al. 27 Because it has been repor ted that, in the presence of a plaque-induced suprabony lesion, or thodont ic forces per se during bodily move- men t are incapable of causing accelerated de- struction of the connective tissue a t t achmen t ) 2 it may be assumed that stretching of the facial gingiva resulting in decreased bucco-lingual di- mension of the borde r tissue, may favor the destructive effect of the plaque associated inflam- matory lesion. This assumption is validated by the observations that, in the presence of plaque- induced gingivitis, a thin marginal soft tissue is more susceptible to complete breakdown than a thick one. 33,34 Fur thermore , because a t tachment loss was similar for plaque-infected teeth that had been bodily moved within the alveolar bone irrespective of the type of soft tissue (gingiva or alveolar mucosa),27 the thickness ra ther than the quality of the marginal soft tissue on the pressure side of the tooth seems to be the de termining factor for the development of recession defects dur ing or thodont ic therapy in plaque-infected dentitions. However, in this context, extensive t ipping and intrusive or thodont ic forces may p romote loss of a t tachment by displacing supra- gingival plaque into a subgingival loca t ion) 5 Hence, the results f rom these studies emphasize the impor tance of adequate plaque control dur- ing the course of or thodont ic therapy.
Clinical Implications
Alterations in the mucogingival complex will occur dur ing or thodont ic tooth movement , but these are independen t of the apico-coronal width (height) of the gingiva. In terms of changes in the position of the soft tissue margin and in gingival dimensions, the impor tan t factors to consider are the direction of the tooth move- men t and the bucco-lingual thickness of the gingiva.
Lingual tooth movemen t will result in an increased bucco-lingual thickness of the tissue at the facial aspect of the tooth, which results in

<< :"d- 'J,- ?:- >>
Mucogingival Considerations
Home I TOC I Bndex
53
coronal migration of the soft tissue margin (decreased clinical crown height). Consequently, in cases with a thin (delicate) gingiva caused by prominent position of the teeth (Fig 4), there is no need for a gingival augmentation procedure in advance of the orthodontic tooth movement. Neither, in the case of a recession type defect should a nmcogingival surgical procedure, aimed at root coverage, be per formed before the orth- odontic therapy (Fig 5). The recession, as well as the dehiscence, will decrease as a consequence of the lingual movement of the tooth into a more proper position within the alveolar bone, and if still indicated at that time, the surgical proce- dure will have a higher predictability of success than if it was per formed before the tooth move- ment.
Facial tooth movement, on the other hand, will result in a reduced bucco-lingual tissue thickness and thereby a reduced height of the free gingival portion, and an increased clinical crown height. However, recession type defects will not develop as long as the tooth is moved within the envelope of the alveolar process. If the tooth movement is expected to result in the establishment of an alveolar bone dehiscence, the volume (thickness) of the covering soft tissue must be considered as a factor that may influ- ence the development of soft tissue recessions during, as well as after, the phase of active o r t h o d o n t i c the rapy . O r t h o d o n t i c t o o t h m o v e -
m e n t p e r se will n o t c ause sof t t issue r eces s ion ,
b u t t h e t h i n g ing iva t h a t will be t h e c o n s e q u e n c e
o f t h e facia l t o o t h m o v e m e n t m a y s e r v e as a l ocus
m i n o r u s res i s t en t i a to d e v e l o p i n g sof t t issue
defec ts in t he p r e s e n c e o f bac t e r i a l p l a q u e a n d / o r
t r a u m a c a u s e d by i m p r o p e r t o o t h b r u s h i n g t ech -
n iques . B e f o r e t h e o r t h o d o n t i c t h e r a p y is ini t i -
a ted , o n e s h o u l d t h e r e f o r e ca re fu l ly c o n s i d e r i f
t h e b u c c o - l i n g u a l t h i cknes s o f t h e sof t t issue o n
t h e p r e s s u r e s ide o f t h e t o o t h s h o u l d be in-
c r eased . F u r t h e r m o r e , i n s t r u c t i o n s in a d e q u a t e
p l a q u e c o n t r o l m e a s u r e s s h o u l d be g iven a n d
c o n t r o l l e d b e f o r e , d u r i n g as wel l as a f t e r t h e
c o m p l e t i o n o f t h e o r t h o d o n t i c t h e r a p y to a v o i d u n n e c e s s a r y t r a u m a to t h e t issue m a r g i n .
References
1. Coatoam GW, Behrents RG, Bissada NE The width of keratinized gingiva during orthodontic treatment: Its significance and impact on periodontal status.J Periodon- tol 1981;52:307-313.
2. Foushee DG, Moriarty JD, Simpson DM. Effects of mandibular orthognatic treatment on mucogingival tis- sue.J Periodontol 1985;56:727-733.
3. Vanarsdall RL, Corn H. Soft tissue management of labially positioned unerupted teeth. AmJ Orthod 1977; 72:53-64.
4. Maynard JG. The rationale for mucogingival therapy in the child and adolescent. Int J Periodont Rest Dent 1987;7:37-51.
5. Hall WB. The current status of mucogingival problems and their therapy.J Periodontol 1981;52:569-575.
6. Maynard JG, Ochsenbein D. Mucogingival problems, prevalence and therapy in children. J Periodontol 1975; 46:543-552.
7. Andlin-Sobocki A. Changes of facial gingival dimensions in children. A 2-year longitudinal study. J Clin Periodon- tol 1993;20:212-218.
8. Andlin-Sobocki A, Bodin L Dimensional alterations of the gingiva related to changes of facial/lingual tooth position in permanent anterior teeth of children. A 2-year longitudinal study.J Clin Periodontol 1993;20:219- 224.
9. Karring T, Nyman S, Thilander B, et al. Bone regenera- tion in orthodontically produced alveolar bone dehis- cences.J Periodont Res 1982;17:309-315.
10. Engelking G, Zachrisson BU. Effects of incisor reposition- ing on monkey periodontium after expansion through the cortical plate, kanJ Orthod 1982;82:23-32.
11. Ainamo A, Bergenholtz A, Hugoson A, et al. Location of the mucogingival junction 18 years after apically reposi- tioned flap surgery.J Clin Periodontol 1992;19:49-52.
12. Wennstr6m JL. Regeneration of gingiva following surgi- cal excision. A clinical study. J Clin Periodontol 1983;10: 287-297.
13. Karring T, Cumming BR, Oliver RC, et al. The origin of granulation tissue and its impact on postoperative results of mucogingival surgery. J Periodontol 1975;46:577-585.
14. Lundberg M, Wennstr6m JL. Development of gingiva following surgical exposure of a facially positioned un- erupted incisor. J Periodontol 1988;59:652-655.
15. Powell RN, McEnlery TM. A longitudinal study of iso- lated gingival recession in the mandibular central incisor region of children aged 6-8 years. J Clin Periodontol 1982;9:357-364.
16. Persson M, Lennartsson B. Improvement potential of isolated gingival recession in children. Swed Dent J 1986; 10:45-51.
17. Andlin-Sobocki A, Marcusson A, Persson M. Three-year observation on gingival recession in mandibular incisors in children.J Clin Periodontol 1991;18:155-159.
18. Wennstr6m JL. Mucogingival surgery, In: Lang NP, Karring T, editors. Proceedings of the 1st European Workshop on Clinical Periodontology, Berlin, Quintes- sence, 1994:193-209.
19. Stoner j , Mazdyasna S. Gingival recession in the lower incisor region of 15-year-old subjects. J Periodontol 1980;51:74-76.
20. Lang NP, L6e H. The relationship between the width of keratinized gingiva and gingival health. J Periodontol 1972;43:623-627.
21. Schoo WH, van der Velden U. Marginal soft tissue
<< Ar'J~ e >> Home I TOC I Bndex
54 Jan L. Wennstr6m
recessions with and without attached gingiva.J Periodont Res 1985;20:209-211.
22. Kisch J, Badersten A, Egelberg J. Longitudinal observa- tion of "unattached," mobile gingival areas. J Clin Periodonto11986;13:131-134.
23. Wennstr6m JL. Lack of association between width of attached gingiva and development of gingival recessions. A 5-year longitudinal study. J Clin Periodontol 1987;14: 181-184.
24. Freedman A, Salkin LM, Stein MD, et al. A 10-year longitudinal study of untreated mucogingival defects. J Periodonto11992;63:71-72.
25. LindheJ, EcheverriaJ. Consensus report of session II, In: Lang NE Karring T, editors. Proceedings of the 1st European Workshop on Clinical Periodontology, Berlin, Quintessence, 1994:210-214.
26. Steiner GG, Pearson JK, Ainamo J. Changes of the marginal periodontium as a result of labial tooth move- ment in monkeys.J Periodonto11981;52:314-320.
27. Wennstr6mJL, LindheJ, Sinclair F, et al. Some periodon- tal tissue reactions to orthodontic tooth movement in monkeys.J Clin Periodontol 1987;14:121-129.
28. Batenhorst KF, Bowers GM, WilliamsJE. Tissue changes resulting from facial tipping and extrusion of incisors in monkeys. J Periodontol 1974;45:660-668.
29. Nyman S, Karring T, Bergenholtz G. Bone regeneration in alveolar bone dediscences produced by jiggling forces. J Periodont Res 1982;17:316-322.
30. Rateitschak KH, Herzog-Specht F, Hotz R. Reaktion und Regeneration des Parodonts auf Behandlung mit festsit- zenden Apparaten und abnehmbaren Platten. Fortschritte der Kieferorthopfidie 1968;29:415-435.
31. Zachrisson BU. Clinical implications of recent ortho- perio research findings, In: H6sl E, Zachrisson BU, Baldauf A, editors. Orthodontics and Periodontics, Chi- cago, IL: Quintessence, 1985:169-186.
32. Ericsson I, Thilander B, LindheJ. Periodontal condition after orthodontic tooth movement in the dog. Angle Orthod 1978;48:210-218.
33. Baker DL, Seymour GJ. The possible pathogenesis of gingival recession. A histological study of induced reces- sion in the rat. J Clin Periodon tol 1976;3:208-219.
34. Ericsson I, Lindhe J. Recession in sites with inadequate width of the keratinized gingiva, kal experimental study in the dog. J Clin Periodontol 1984; 11:95-103.
35. Ericsson I, Thilander B, Lindhe J, et al. The effect of orthodontic tilting movements on the periodontal tis- sues of infected and non-infected dentitions in dogs. J Clin Periodonto11977;4:278-293.
Related Documents











