CLINICAL IMAGING 1994;18:173-178 173 MRI OF LUMBAR INTRADURAL DISC HERNIATION MIKA LIDOV, MD, ARYEH STOLLMAN, MD, ANDREW CASDEN, MD, PETER SOM, MD, AND JOSHUA BEDERSON, MD We present the magnetic resonance imaging [MRI) ap- pearance of a patient with an intradural lumbar disc herniation and discuss this entity. This case demon- strates the role of MRI in comparison to myelogra- phylpostmyelogram computed tomography with re- spect to the diagnosis of intradural disc herniation. KEY WORDS: Spine; Intervertebral discs; Magnetic resonance imaging INTRODUCTION Rupture of a lumbar intervertebral disc into the in- tradural space is an unusual occurrence, with only 50 reported cases since this entity was first described in 1942. A review of the literature suggests that an accurate preoperative diagnosis of this lesion is uncommon be- cause it typically produces a complete block on my- elography, with features suggesting an extrinsic lesion because of the presence of the extradural disc mate- rial. In the patient presented in this case report, mag- netic resonance imaging (MlU), which is not depen- dent on the flow of contrast past a high grade block, was able to delineate both the intradural and extradural components of this lesion, as well as the inflamma- tory response in the nerve roots adherent to the in- tradural fragment. From the Departments of Diagnostic Radiology (M.L., AS., P.S.), Orthopedics (A.C.), and Neurosurgery (J.B.), of the Mount Sinai School of Medicine, City University of New York, New York, NY. Address reprint requests to: Mika Lidov, MD, Department of Radi- ology, Box 1234, Mount Sinai Medical Center, One Gustave L. Levy Place, New York, NY 10029-6574. Received August 9, 1993; accepted October 4, 1993. 0 1994 Elsevier Science Inc. 655 Avenue of the Americas, New York, NY 10010 0899-707l/94/$7.00 CASE REPORT A 5%year-old woman with no significant past history presented for evaluation of left leg weakness and loss of sensation with respect to bladder and bowel func- tion. Six weeks prior to admission she awakened with back pain and left leg pain and weakness. She was evaluated at a local hospital and treated with a non- steroidal antiinflammatory medication and bed rest. This regimen produced some decrease in her pain, al- though her leg weakness persisted. Over the follow- ing 2 weeks she experienced loss of sensation with re- spect to bladder and bowel function. After 6 more weeks of conservative treatment, she presented at the orthopedic clinic for further evaluation. Physical ex- amination revealed 3/5 dorsa-flexion of the ankle, 3/5 EHL and 0.5 plantar flexion on the left side, with right side strength within normal limits. Sensation to light touch and pin was decreased in the left L-5 and S-l distributions. Reflexes were 2 + at the knees, 2 + on the right ankle, and absent in the left ankle. The ex- amination was otherwise unremarkable. The myelo- gram and postmyelogram computed tomography (CT) scan (Figures lA and B and ZA, B, and C) showed an almost complete block at L-4-L-5 with features of both an intradural mass and extrinsic compression. The post myelogram CT demonstrated a mild bulge of the intervertebral disc at the level of the myelographic block and a questionable parasagittal disc fragment below the disc space. MIU was performed on a .5T Gyrex S5OOO (Elscint, Boston) with Tl-weighted sagittal and axial images (SE 500/28,2 averages), both without con- trast and following intravenous injection of GD-DTPA (Figure 3A, B, C, and D). MRI not only showed a large inferiorly migrated disc fragment, but also clearly demonstrated both an irregularly marginated enhanc- ing intradural mass and enhancement within the ad- jacent nerve roots. The patient underwent L-4 and L-5 laminectomies that revealed an intrathecal mass ex- panding the dura. This mass arose anteriorly and dis-

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
CLINICAL IMAGING 1994;18:173-178 173
MRI OF LUMBAR INTRADURAL DISC HERNIATION
MIKA LIDOV, MD, ARYEH STOLLMAN, MD, ANDREW CASDEN, MD, PETER SOM, MD, AND JOSHUA BEDERSON, MD
We present the magnetic resonance imaging [MRI) ap- pearance of a patient with an intradural lumbar disc herniation and discuss this entity. This case demon- strates the role of MRI in comparison to myelogra- phylpostmyelogram computed tomography with re- spect to the diagnosis of intradural disc herniation.
KEY WORDS:
Spine; Intervertebral discs; Magnetic resonance imaging
INTRODUCTION Rupture of a lumbar intervertebral disc into the in- tradural space is an unusual occurrence, with only 50 reported cases since this entity was first described in 1942. A review of the literature suggests that an accurate preoperative diagnosis of this lesion is uncommon be- cause it typically produces a complete block on my- elography, with features suggesting an extrinsic lesion because of the presence of the extradural disc mate- rial. In the patient presented in this case report, mag- netic resonance imaging (MlU), which is not depen- dent on the flow of contrast past a high grade block, was able to delineate both the intradural and extradural components of this lesion, as well as the inflamma- tory response in the nerve roots adherent to the in- tradural fragment.
From the Departments of Diagnostic Radiology (M.L., AS., P.S.), Orthopedics (A.C.), and Neurosurgery (J.B.), of the Mount Sinai School of Medicine, City University of New York, New York, NY.
Address reprint requests to: Mika Lidov, MD, Department of Radi- ology, Box 1234, Mount Sinai Medical Center, One Gustave L. Levy Place, New York, NY 10029-6574.
Received August 9, 1993; accepted October 4, 1993. 0 1994 Elsevier Science Inc. 655 Avenue of the Americas, New York, NY 10010 0899-707l/94/$7.00
CASE REPORT A 5%year-old woman with no significant past history presented for evaluation of left leg weakness and loss of sensation with respect to bladder and bowel func- tion. Six weeks prior to admission she awakened with back pain and left leg pain and weakness. She was evaluated at a local hospital and treated with a non- steroidal antiinflammatory medication and bed rest. This regimen produced some decrease in her pain, al- though her leg weakness persisted. Over the follow- ing 2 weeks she experienced loss of sensation with re- spect to bladder and bowel function. After 6 more weeks of conservative treatment, she presented at the orthopedic clinic for further evaluation. Physical ex- amination revealed 3/5 dorsa-flexion of the ankle, 3/5 EHL and 0.5 plantar flexion on the left side, with right side strength within normal limits. Sensation to light touch and pin was decreased in the left L-5 and S-l distributions. Reflexes were 2 + at the knees, 2 + on the right ankle, and absent in the left ankle. The ex- amination was otherwise unremarkable. The myelo- gram and postmyelogram computed tomography (CT) scan (Figures lA and B and ZA, B, and C) showed an almost complete block at L-4-L-5 with features of both an intradural mass and extrinsic compression. The post myelogram CT demonstrated a mild bulge of the intervertebral disc at the level of the myelographic block and a questionable parasagittal disc fragment below the disc space. MIU was performed on a .5T Gyrex S5OOO (Elscint, Boston) with Tl-weighted sagittal and axial images (SE 500/28,2 averages), both without con- trast and following intravenous injection of GD-DTPA (Figure 3A, B, C, and D). MRI not only showed a large inferiorly migrated disc fragment, but also clearly demonstrated both an irregularly marginated enhanc- ing intradural mass and enhancement within the ad- jacent nerve roots. The patient underwent L-4 and L-5 laminectomies that revealed an intrathecal mass ex- panding the dura. This mass arose anteriorly and dis-
174 LIDOV ET AL. CLINICAL IMAGING VOL. 18, NO. 3
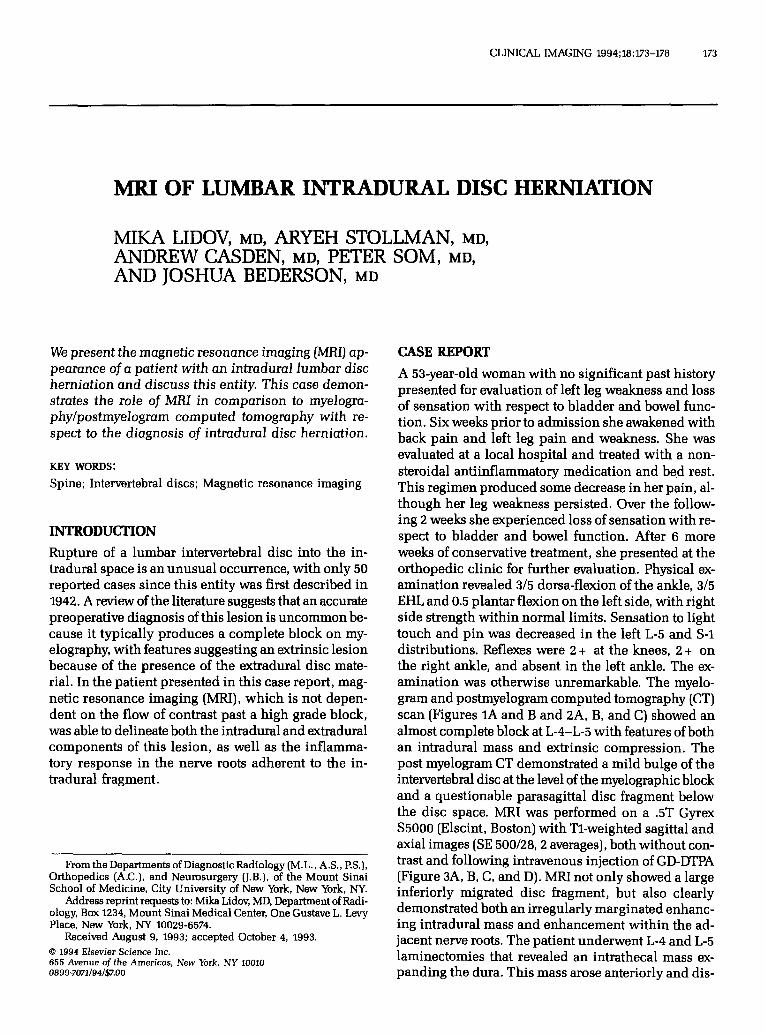
FIGURE 1. Lumbar myelogram. Lateral view (A) shows complete block at L-4-L-5 level with smooth ventral extrinsic com- pression most consistent with L-4-L-5 disc herniation @TOWS). Oblique view shows (B) an exquisitely defined lobulated mass suggesting an intradural lesion (arrows). Note slightly peripheralized nerve roots.
placed and compressed the nerve roots bilaterally, more severely on the left side. The mass was densely adher- ent to the dura anteriorly and to the anterior surface of the nerve roots of the cauda equina, which it dis- placed posteriorly. F’rozen section was consistent with disc material. The herniated fragment created a hole measuring 1 cm in diameter in the ventral dura. Removal of the extradural disc material was accom- plished through this dural defect. The patient had an uneventful postoperative course and was discharged
1 week later, at which time neurological function failed to improve and bowel and bladder function remained impaired.
DISCUSSION Rupture of a lumbar intervertebral disc into the in- tradural space is an infrequent occurrence with only 50 cases reported, predominantly within the orthope- dic and neurosurgical literature. Although this entity
JULY-SEPTEMBER 1994 MRI OF LUMBAR INTRADURAL DISC HERNIATION 175
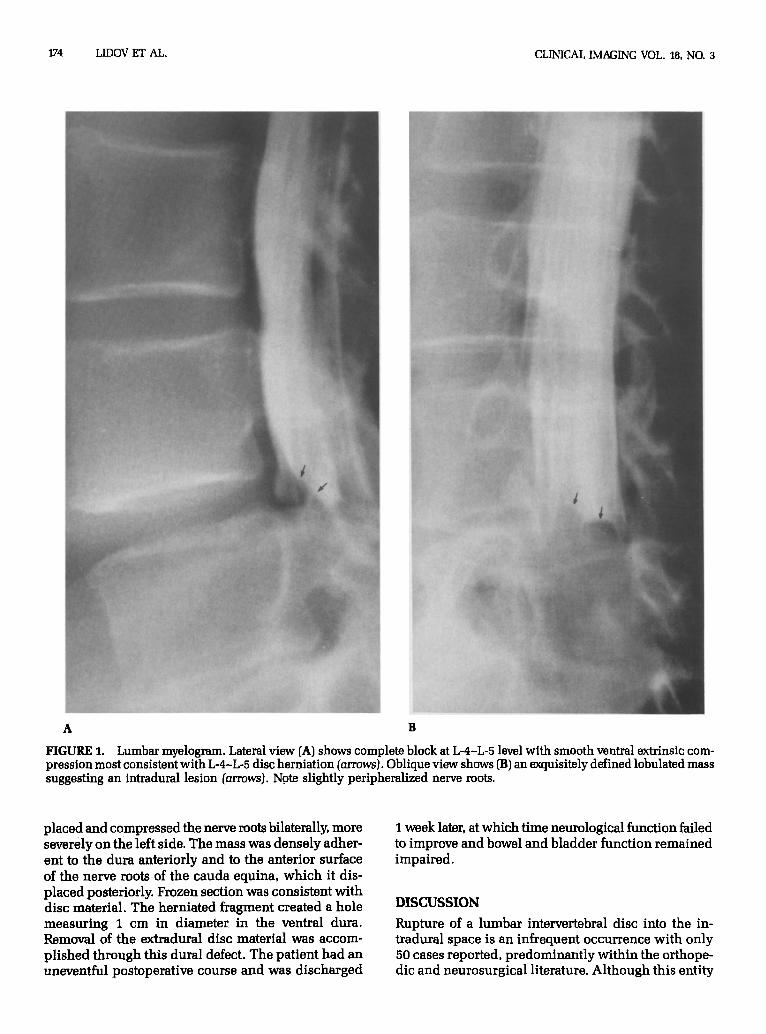
FIGURE 2. Postmyelogram CT. (A) 3 mm above the L-4-L- 5 disc, (B) at the level of L-4-L-5, and (C) 3 mm below the disc space. There is a mild bulge of the L-4-L-5 disc (B) and a questionable inferiorly marginated left parasagittal disc fragment (C, arrows). Again, there is peripheralization of nerve roots at and above the disc level (A, B, arrows). Note the very limited value of postmyelogram CT in the evaluat- ing this compressive lesion because of paucity of contrast .-.* +h.-. l.-...“l
was first reported in 1942 (I), the pathogenesis of this unusual lesion remains uncertain. Dense adhesions between the ventral dura and the posterior longitudi- nal ligament have been identified at surgery in a num- ber of these patients. These adhesions, presumably the result of prior surgery or trauma, prevent the more common lateral protrusion of the herniating disc. In such cases, the ventral dura, which is adherent to the posterior longitudinal ligament (PLL), may become the
path of relatively less resistance to the herniating disc (2,3). A cadaver study of the relationship between the PLL and the dura in the lumbar spine has shown that while at most levels only loose connections are found between the dura and the ligament, at the level of L-4- L-5 the ventral dura is more firmly attached to the PLL and annulus (4). This finding may explain why L-4-L-5 is the site of predilection for intradural herniation, with 52% of the reported cases occurring at this level as
176 LIDOV ET AL. CLINICAL IMAGING VOL. 18. NO. 3
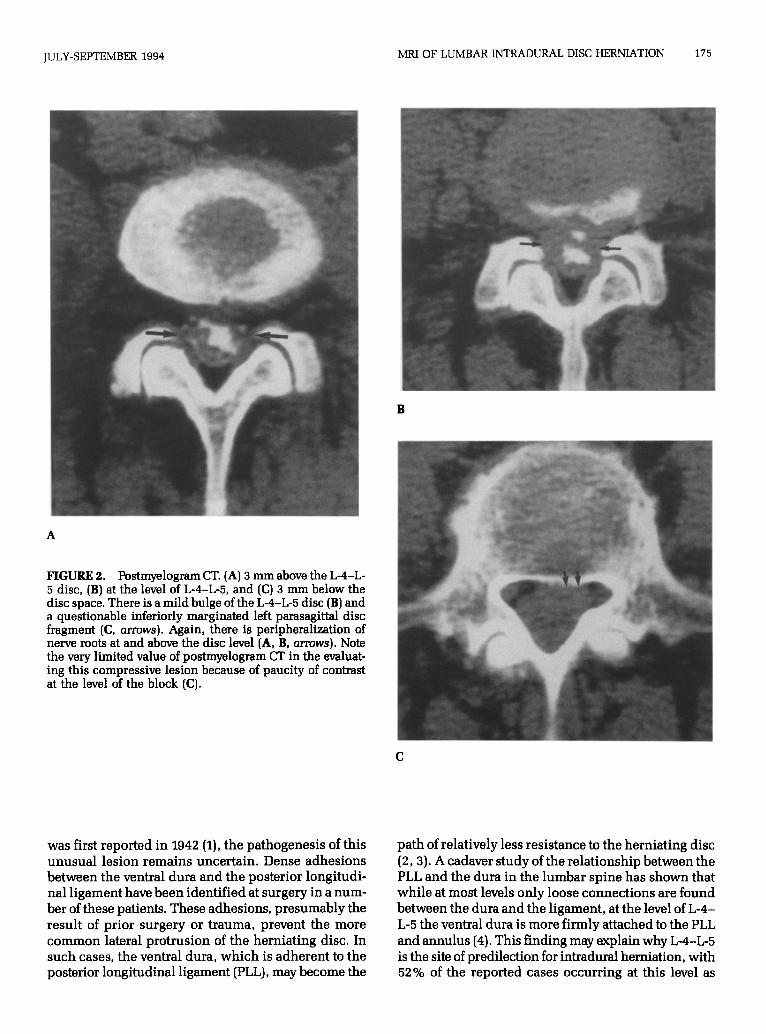
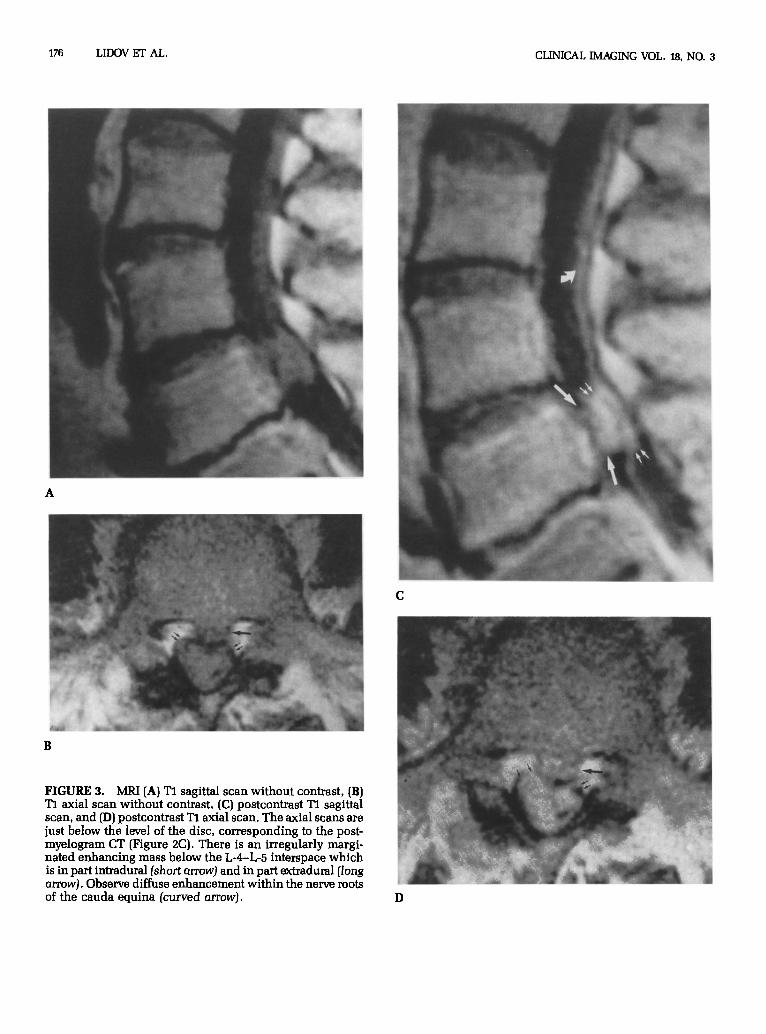
FIGURE 3. MRI [A) Tl sagittal scan without contrast, (B) Tl axial scan without contrast, (C) postcontrast Tl sagittal scan, and (D) postcontrast 7’1 axial scan. The axial scans are just below the level of the disc, corresponding to the post- myelogram CT (Figure 2C). There is an irregularly margi- nated enhancing mass below the L-4-L-5 interspace which is in part intradural (short arrow) and in part extmdural (long arrow). Observe diffuse enhancement within the nerve roots of the cauda equina [curved arrow). D

JULY-SEPTEMBER 1994 MRI OF LUMBAR INTRADURAL DISC HERNIATION 177
compared to 10% at L-l-L-2,14% at L-2-L-3 and 24% at L-3-L-4 (3). At L-5-S-1, where abundant epidural fat frequently separates the PLL from the ventral dura, intradural herniation is least common (5).
Review of case reports in the surgical literature sug- gests that the preoperative diagnosis of an intradural herniated disc is the exception rather than the rule. Many intradural disc fragments are detected intraoper- atively, without preoperative diagnosis. However, smaller intradural fragments may escape detection both on sectional imaging and at surgery, particularly in the presence of a dominant extradural lesion which ap- pears to account for the patient’s symptoms. It has been suggested that these small undetected intradural frag- ments may account for a number of “failed backs” (6) and that they may remain undetected on follow-up MRI examinations, where their presence may be obscured by postsurgical scar and adhesive arachnoiditis. Fur- thermore, the literature suggests that the clinician will not be able to identify preoperatively those patients with an intradural disc herniation. While such patients generally have more severe and extensive neurologi- cal signs and symptoms, no clinical presentation is pathognomonic or even highly suggestive of the diag- nosis (3). Accurate radiographic identification of an in- tradural disc herniation is infrequent in the literature. This reflects in part the fact that these case reports, for the most part, predate the advent of water soluble con- trast and postmyelogram CT. It also reflects the limita- tion of postmyelogram CT in delineating a lesion at or below a block. Hodge et al. (3) in a review of 21 pa- tients with intradural disc herniations noted that a majority of the reported cases of intradural herniation have shown on myelogram only an irregularly margi- nated complete block, a myelographic appearance un- derstandably more commonly associated with an ex- tradural disc herniation. Less commonly, the herniated intradural fragment has been identified as a sharply defined, irregularly marginated intradural filling de- fect. The differential diagnosis of an intradural mass in the lumbar area includes neurofibroma, ependy- moma, lipoma, meningioma, epidennoid tumor, arach- noid cyst, metastasis, and an inflammatory mass such as may be seen with adhesive arachnoiditis. All of these possibilities except an inflammatory mass tend to be more smoothly contoured than the irregularly margi- nated disc fragment, although this finding may be poorly appreciated on myelography or postmyelogram CT due to a paucity of intrathecal contrast at the level of the block.
This case report not only adds to the body of litera- ture on intradural disc herniations, but points out sev- eral radiographic features that can suggest the correct diagnosis. The diagnosis in our case was suggested by the presence of imaging features of both an intradural
and an extradural lesion on the lumbar myelogram (Fig- ure 1A). The lateral view of the lumbar myelogram demonstrated a smooth posterior displacement of the thecal sac at the level of the complete block, strongly suggesting an extradural lesion while the oblique view (Figure 1B) demonstrated a sharply marginated lobu- lated mass, suggesting the possible presence of an ad- ditional intradural component. The postmyelogram CT, only slightly more helpful than a noncontrast CT because of the paucity of intrathecal dye at the level of the block, showed only a mild diffuse bulge of the L-4-L-5 (Figure 2) and barely hinted at the presence of an inferiorly migrated disc fragment (Figure 2C). In retrospect, peripheralization of the nerve roots above the level of the block suggested the presence of either an intradural mass splaying the roots or of adhesive arachnoiditis (Figure 2A). Sagittal MFU, without and with GD-DPTA (Figure 3), which is not dependent on intrathecal dye, demonstrated an irregularly margi- nated enhancing intradural lesion that was associated with abnormal enhancement of the nerve roots of the cauda equina. The axial scans (Figure 3D) confirmed the intradural location of the enhancing mass and also demonstrated a large inferiorly migrated left parasagit- tal extradural disc fragment. Both the intradural com- ponent and the downwardly migrated disc fragment were much better visualized on MRI (Figure 3D) as compared with postmyelogram CT (Figure 2C).
Arachnoiditis may occur as a result of the intradural rupture (7) and typically, as in this case, will cause the intradural disc fragment to be adherent to the dura and nerve roots. The enhancement of the roots of the cauda equina, as observed in this case, presumably represents the presence of arachnoiditis. However, enhancement of the lumbosacral nerve roots has been identified in association with the more common place extradural disc herniation (8) and is not itself an indication of in- tradural pathology. The MRI findings of an irregularly marginated enhancing intradural mass associated with nerve root enhancement may be found not only with an intradural disc herniation, but also with adhesive arachnoiditis secondary to infection, intrathecal hemor- rhage, surgery, trauma, intrathecal steroid, or anes- thetic administration or pantopaque myelography (9). The history of an appropriate clinical setting for the development of arachnoiditis should allow accurate differentiation of these entities.
Intradural disc fragments have been previously de- scribed on MRI as showing enhancement that is thought to represent granulation tissue (10). However, our case showed homogeneous enhancement of the disc fragment. The exact mechanism for this remains unclear. This case suggests that MRI may be the most reliable modality for detecting this uncommon com- plication of disc herniation.

178 LIDOV ET AL. CLINICAL IMAGING VOL. 18, NO. 3
REFERENCES 7. Hodge CJ. Lumbar Intradural Disc Rupture in Neurosurgery. In W&ins RI-I, Rengachary (eds): New York: McGraw-Hill, 1985: 2264-2265. 1.
2.
3.
4.
5.
6.
Dandy WE. Serious complications of ruptured intravertebral discs. JAMA 1942;119:474-477. Ciappetta P, Delfini R, Cantore GI? Intradural lumbar disc her- nia: Description of 3 cases. Neurosurgery 1981;8:104-197. Hodge CJ, Binet EF, Kieffer SA. Intradural herniation of lumbar intervertebral discs. Spine 1978;3:346-350. Blikera G. Intradural herniated disc. J Neurosurg 1969;31:676-679. Lesoin F, Duquennoy B, Rousseaux M, Servato R, Jomin M. In- tradural rupture of lumbar intervertebral disc: Report of three cases with review of the literature. Neurosurgery 1984;14:728-731. Sypert GW. Comment to intradural rupture of lumbar interver- tebral disc: Report of three cases with review of the literature. Neurosurgery 14:731.
8.
9.
10.
11.
Jinkins JR. MR of enhancing nerve roots in the unopen&d lum- bosacral spine. AJNR 1993;14:193-202. Ross JS. Inflammatory disease. In Modik MT, Masaryk TJ, Ross JS (eds): Magnetic Resonance Imaging of the Spine. Chicago: Yearbook Medical Publishing, 1989:167-172. Wasserman R, Mamourian AC, Black JF, Lehman RA. Intradural lumbar disc fragment with ring enhancement on MR. AJNR 1993;14:401-404. Bundschuh CV, Stein L, Slusser JH, Schinco FP, Ladaga LE, Dillon JD. Distinguishing between scar and recurrent herniated disc in postoperative patients: Value of contrast enhanced CT and MR imaging. AJNR 1990;11:949-958.
Related Documents











