MRI IN CARCINOMA CERVIX- A PICTORIAL ESSAY ABSTRACT ID : IRIA – 1167 ABSTRACT NO : 186

MRI IN CARCINOMA CERVIX- A PICTORIAL ESSAY ABSTRACT ID : IRIA – 1167 ABSTRACT NO : 186.
Dec 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

MRI IN CARCINOMA CERVIX- A PICTORIAL ESSAY
ABSTRACT ID : IRIA – 1167
ABSTRACT NO : 186

INTRODUCTION
• 3rd most common gynecologic malignancy.
• Typically seen in middle aged females between 45 and 55 years.
• The International Federation of Gynecology and Obstetrics (FIGO) staging system provides worldwide epidemiologic and treatment response statistics.
• However, there are significant inaccuracies in the FIGO staging system.

• MRI although not included in that system, is now widely accepted as optimal for evaluation of important prognostic factors such as tumour volume and nodal status.
• MRI obviates the use of invasive procedures such as cystoscopy and proctoscopy, especially when there is no evidence of local extension.
• Brachytherapy and external beam therapy are optimized with MR imaging evaluation of the shape and direction of lesion growth.
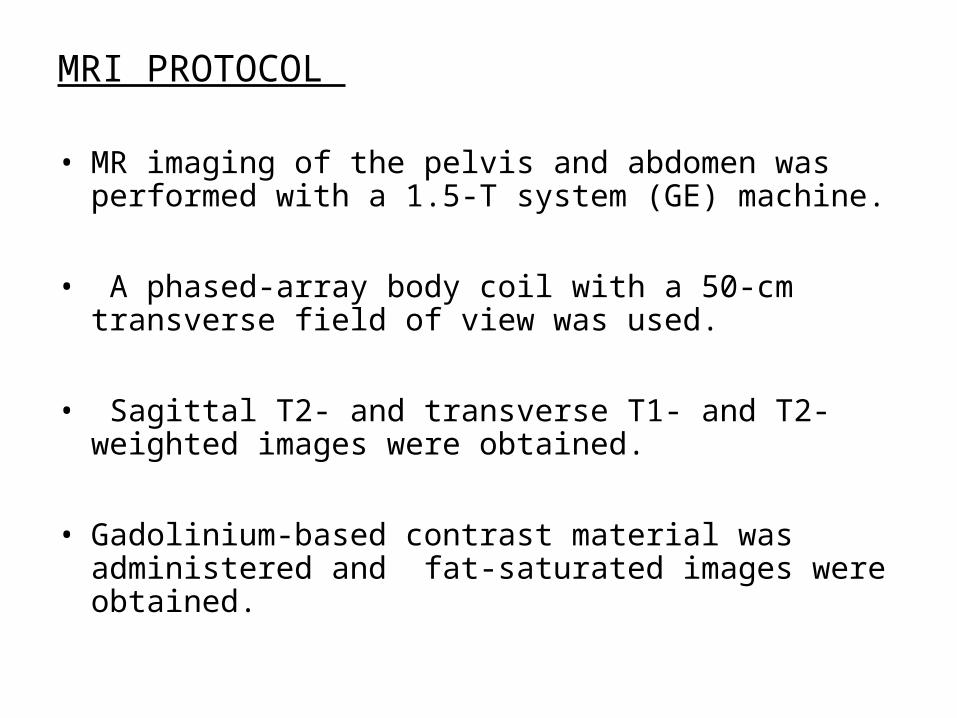
MRI PROTOCOL
• MR imaging of the pelvis and abdomen was performed with a 1.5-T system (GE) machine.
• A phased-array body coil with a 50-cm transverse field of view was used.
• Sagittal T2- and transverse T1- and T2-weighted images were obtained.
• Gadolinium-based contrast material was administered and fat-saturated images were obtained.
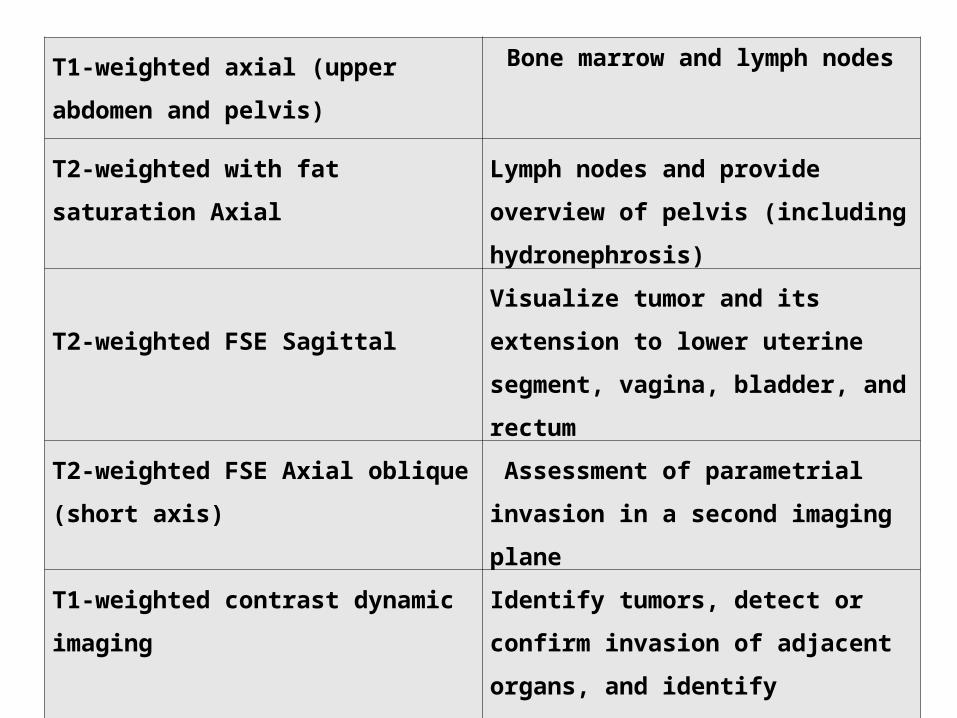
T1-weighted axial (upper abdomen
and pelvis)
Bone marrow and lymph nodes
T2-weighted with fat saturation Axial Lymph nodes and provide overview
of pelvis (including hydronephrosis)
T2-weighted FSE Sagittal
Visualize tumor and its extension to
lower uterine segment, vagina,
bladder, and rectum
T2-weighted FSE Axial oblique
(short axis)
Assessment of parametrial invasion
in a second imaging plane
T1-weighted contrast dynamic
imaging
Identify tumors, detect or confirm
invasion of adjacent organs, and
identify fistulous tracts.
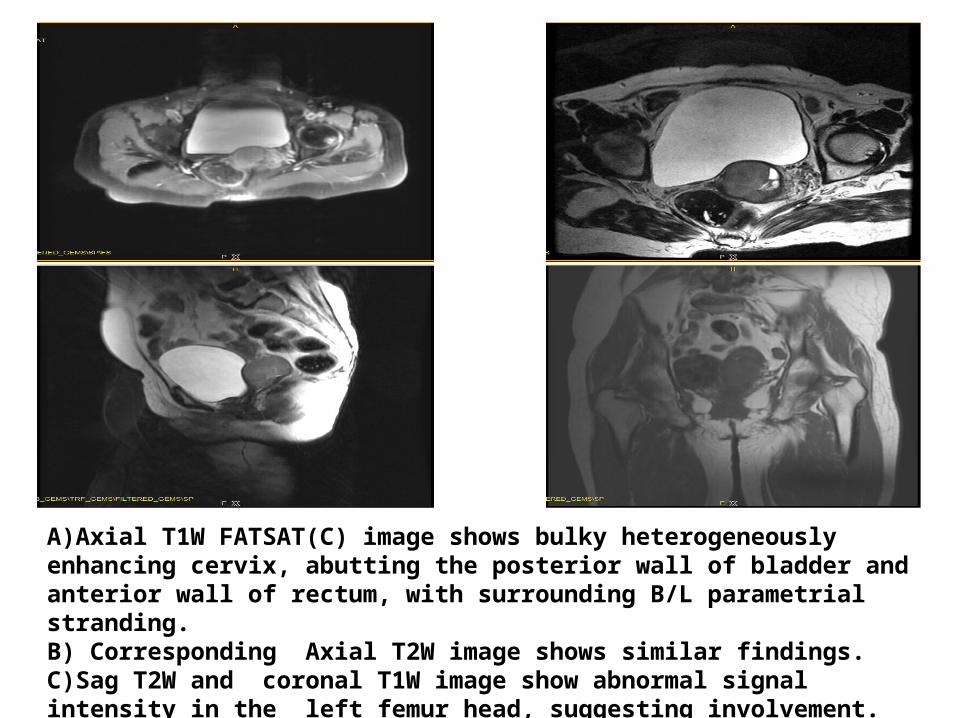
A)Axial T1W FATSAT(C) image shows bulky heterogeneously enhancing cervix, abutting the posterior wall of bladder and anterior wall of rectum, with surrounding B/L parametrial stranding. B) Corresponding Axial T2W image shows similar findings. C)Sag T2W and coronal T1W image show abnormal signal intensity in the left femur head, suggesting involvement.
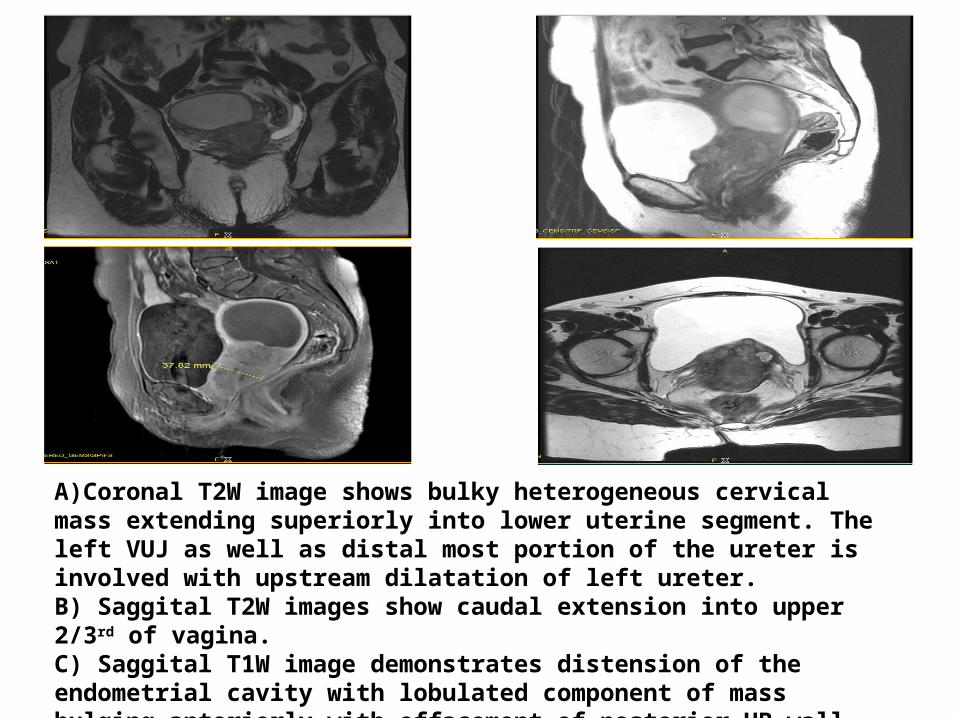
A)Coronal T2W image shows bulky heterogeneous cervical mass extending superiorly into lower uterine segment. The left VUJ as well as distal most portion of the ureter is involved with upstream dilatation of left ureter. B) Saggital T2W images show caudal extension into upper 2/3rd of vagina. C) Saggital T1W image demonstrates distension of the endometrial cavity with lobulated component of mass bulging anteriorly with effacement of posterior UB wall. D)Axial T2 FATSAT images shows bilateral parametrial involvement

A)Saggital T2W image shows bulky, irregularly thickened cervical mass, extending into uterine myometrium along the entire fundus and body. B) Axial T2 W image shows enlarged external iliac lymph node. C) Axial T2w FATSAT image demonstrates indistinct fat plane between the cervical stroma and posterior wall of bladder. Minimal bilateral parametrial stranding is noted bilaterally .D) Coronal T2W image shows enlarged lymph node.

A)Saggital T2W image shows a large lobulated mass involving the cervix with extension into lower uterine body and upper ¾ rd of vagina. Posteriorly this mass is seen to extend along the meso-rectal fascia into rectum. B & C) Coronal and Axial T1 FATSAT images show lobulated cervical mass with hyperintensities in bilateral levator ani and obturator muscles. Adjacent portions of bilateral pelvic bones also appear involved D) Axial T2FATSAT image shows left parametrial involvement.
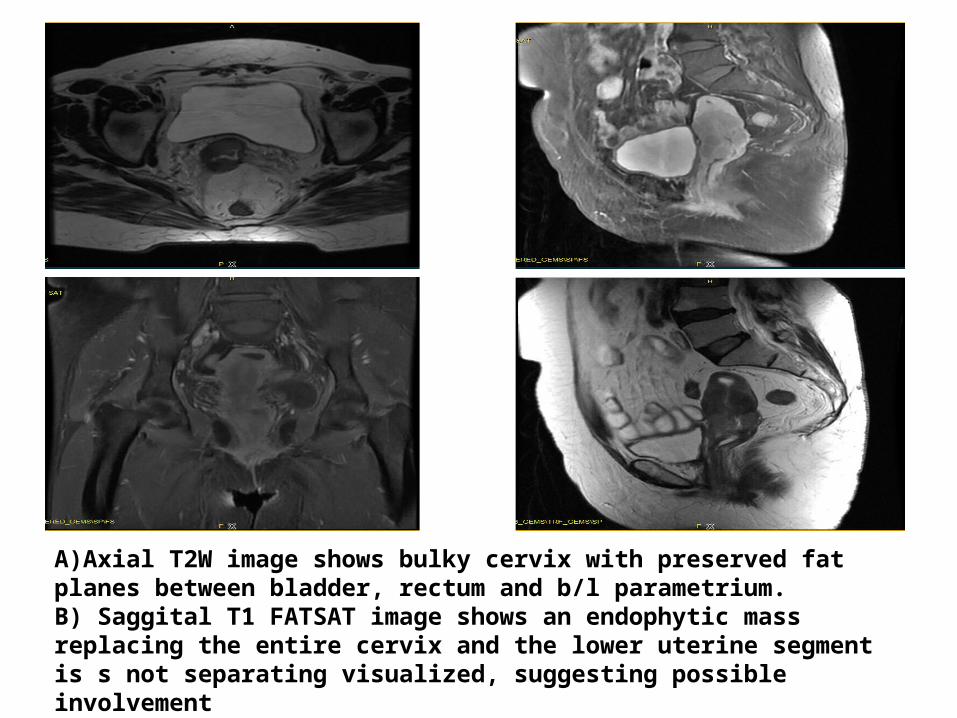
A)Axial T2W image shows bulky cervix with preserved fat planes between bladder, rectum and b/l parametrium. B) Saggital T1 FATSAT image shows an endophytic mass replacing the entire cervix and the lower uterine segment is s not separating visualized, suggesting possible involvement C& D)Coronal T1 FATSAT and Saggital T2w images show the cervical mass

TUMOUR• Cervical carcinoma has intermediate signal intensity at
T2-weighted imaging and is seen disrupting the low-signal-intensity fibrous stroma.
• A wide variety of morphologic features - Exophytic ,
infiltrating, or endocervical with a barrel shape.
• Bulk of the lesion - centered at the level of the cervix, with either protrusion into the vagina or invasion of the lower myometrium.
MR IMAGING FINDINGS

• A visible tumor indicates stage IB or higher. The size of the tumor (ie, whether greater or less than 4 cm in diameter) has a great impact on the choice of therapy, and there is good correlation between MR imaging findings and macroscopic measurements .
VAGINA
Disruption of the hypointense vaginal wall with hyperintense thickening at T2-weighted imaging and contrast enhancement at T1- weighted imaging are signs of vaginal invasion.

PELVIC WALL
Tumor extending to involve the internal obturator, piriform, or levator ani muscles, with or without a dilated ureter, indicates pelvic wall invasion . Ureteral obstruction at the level of the tumor is considered to be an indication of wall invasion.
PARAMETRIA
• Preservation of a hypointense fibrous stromal ring at T2-weighted MR imaging has a high negative predictive value for parametrial invasion .
• Complete disruption of the ring with nodular or irregular tumor signal intensity extending into the parametrium are reliable signs of invasion.
• Unilateral or bilateral parametrial invasion is a definite contraindication to surgery.
• With disruption of the stromal ring, but no definite parametrial mass, there may be microscopic invasion (false-negative findings).
• Linear stranding around the cervical mass is suggestive of parametrial invasion but may be due to peritumoral inflammatory tissue (false-positive findings).
BLADDER & RECTUM
• Bladder or rectal invasion is present when disruption of their normal hypointense walls is seen at T2-weighted imaging, with or without a mass protruding into the lumen.
• Dynamic gadolinium-enhanced T1-weighted sequences are helpful for confirming invasion and identifying fistulous tracts .
• Hyperintense thickening of the bladder mucosa at T2-weighted imaging indicates edema and is not a direct sign of invasion.
• However, this “bullous edema sign” of the posterior wall mucosa should be analyzed carefully for any associated nodulation suggestive of tumor .

LYMPH NODES
• Lymph node disease detection is based only on a size criterion, the most widely accepted being a transverse diameter exceeding 10 mm .
• Within the pelvis, cervical cancer spreads first to the parametrial nodes, then to the obturator and iliac nodes.
• Lymph nodes best detected with T2-weighted imaging , at which they demonstrate intermediate signal intensity and are well differentiated from the hypointense muscles and blood vessels.
• A slightly hyperintense ring flow artifact - often found in the iliac veins and not to be confused with adenopathy .
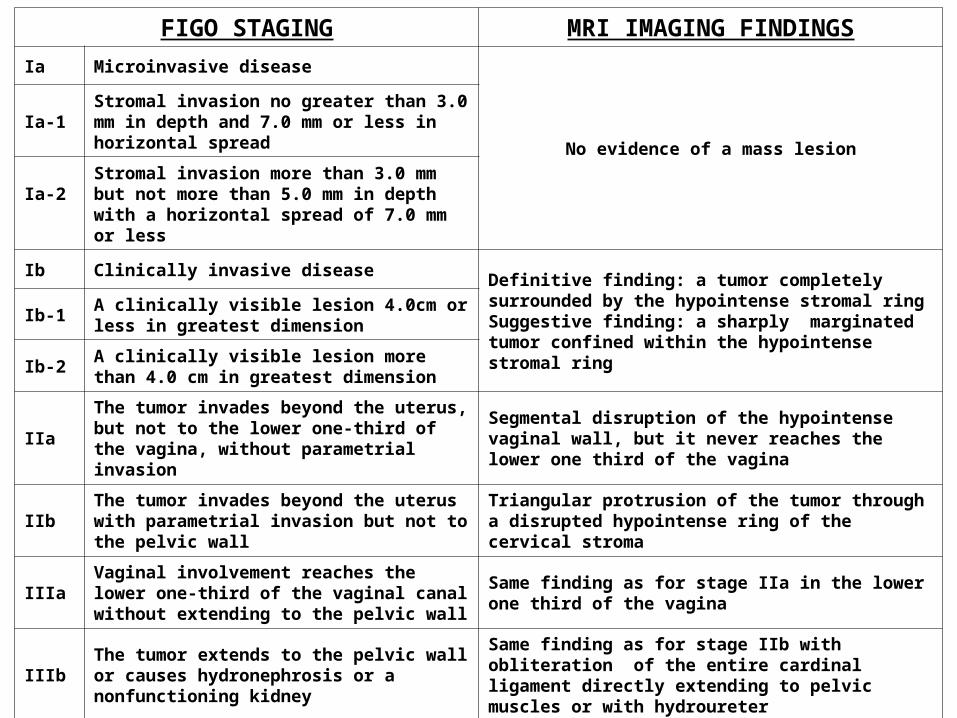
FIGO STAGING MRI IMAGING FINDINGSIa Microinvasive disease
No evidence of a mass lesionIa-1 Stromal invasion no greater than 3.0 mm in depth
and 7.0 mm or less in horizontal spread
Ia-2 Stromal invasion more than 3.0 mm but not more than 5.0 mm in depth with a horizontal spread of 7.0 mm or less
Ib Clinically invasive diseaseDefinitive finding: a tumor completely surrounded by the hypointense stromal ringSuggestive finding: a sharply marginated tumor confined within the hypointense stromal ring
Ib-1 A clinically visible lesion 4.0cm or less in greatest dimension
Ib-2 A clinically visible lesion more than 4.0 cm in greatest dimension
IIaThe tumor invades beyond the uterus, but not to the lower one-third of the vagina, without parametrial invasion
Segmental disruption of the hypointense vaginal wall, but it never reaches the lower one third of the vagina
IIb The tumor invades beyond the uterus with parametrial invasion but not to the pelvic wall
Triangular protrusion of the tumor through a disrupted hypointense ring of the cervical stroma
IIIaVaginal involvement reaches the lower one-third of the vaginal canal without extending to the pelvic wall
Same finding as for stage IIa in the lower one third of the vagina
IIIb The tumor extends to the pelvic wall or causes hydronephrosis or a nonfunctioning kidney
Same finding as for stage IIb with obliteration of the entire cardinal ligament directly extending to pelvic muscles or with hydroureter
IVa The tumor invades the mucosa of the bladder or rectum or extends beyond the true pelvis
Segmental disruption of the hypointense bladder or rectal wall or a segmental thickened rectal wall
IVb Distant metastasis Evidence of mass lesions in distant organs

CONCLUSION
MRI is very useful in local staging of the disease and therefore in concurrence with FIGO staging is now widely accepted as optimal for evaluation of the main prognostic factors and selection of therapeutic strategy.

REFERENCES
• Nicolate V, Carignan L, Bourdon F, Prosmanne O. MR imaging of cervical carcinoma: A practical staging approach. RadioGraphics 2000;20:1539-49.
• Mahajan M, Kuber R, Chaudhari KR, Chaudhari P,Ghadage P, Naik R. MR imaging of carcinoma cervix. Indian J Radiol Imaging 2013;23:247-52.
• FIGO Committee on Gynecologic Oncology. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynecol Obstet 2009;105:103-4.
• Okamoto Y, Tanaka YO, Nishida M, Tsunoda H, Yoshikawa H,Itai Y. MR Imaging of the uterine cervix: Imaging-pathologic correlation. RadioGraphics 2003;23:425-45.
Related Documents