AJR:179, September 2002 641 MR Imaging of the Knee: Findings in Asymptomatic Collegiate Basketball Players OBJECTIVE. The purpose of our study was to evaluate the knees of asymptomatic high- level collegiate basketball players before the beginning of the basketball season to gain an un- derstanding of nonclinical findings in this patient population. SUBJECTS AND METHODS. Bilateral knee MR imaging examinations of 17 varsity basketball players (12 men and five women) were performed before basketball season began. All of the subjects were imaged on a 1.5-T magnet. The MR imaging studies were reviewed by two musculoskeletal radiologists. Structures analyzed were the menisci, ligaments, carti- lage, plicae, and bone marrow. The presence of a joint effusion was also noted. RESULTS. Fourteen (41%) of the 34 knees had bone marrow edema, eight (24%) showed signal in the patellar tendon, and 14 (41%) had abnormal cartilage signal or a focal abnormal- ity. Twelve (35%) of the 34 knees showed a joint effusion. Two knees (6%) showed abnormal signal along the infrapatellar plica. Four knees (12%) were noted to have a discoid meniscus. CONCLUSION. An MR examination of the knees of high-level collegiate basketball players may show changes unique to this population. The changes seen on MR imaging in these athletes may be asymptomatic abnormalities. For instance, changes suggestive of patel- lar tendinopathy were identified in these asymptomatic subjects. R imaging has proven useful for evaluating the knee for internal derangement. This imaging mo- dality is accurate for evaluating meniscal ab- normalities [1–3] as well as for assessing the integrity of the anterior cruciate ligament [4, 5], examining articular cartilage [6, 7], and diagnosing bone marrow edema [8]. This study was prompted by requests to evaluate several of our division I college bas- ketball players for knee problems before the rigorous college basketball season began. At the time of these MR imaging studies, abnor- malities were noted within the knee joint that did not prove to be symptomatic to the player. This finding prompted us to evaluate the knees of all the basketball players to assess changes that could be misinterpreted as abnormal if a player presented for imaging during the sea- son. Our study evaluates the spectrum of MR imaging findings in bilateral knees in asymp- tomatic high-level collegiate basketball players to provide a baseline for interpretation. Subjects and Methods Both knees of 17 varsity college basketball play- ers (12 men and five women) were imaged (n = 34 knees) during the course of their preseason physical examination. Internal review board approval for this study was obtained. The athletes were questioned about any relevant prior injury or surgery. All sub- jects were imaged on a 1.5-T magnet (Signa; Gen- eral Electric Medical Systems, Milwaukee, WI) using a send–receive knee coil. Our routine knee protocol was performed: fast spin-echo T2-weighted images (TR/TE eff , 3500/65) were obtained with fat suppression in the axial, coronal, and sagittal orien- tations and spin-echo proton density fat-suppressed images (TR/TE, 2000/20) were obtained in the sag- ittal plane to evaluate the menisci. A matrix of 256 × 192 with 2 excitations, a slice thickness of 4 mm with an interslice gap of 0.4 mm, and a field of view of 16 cm were used. The MR studies were reviewed independently by two musculoskeletal radiologists, forming a consensus opinion; the reviewers evalu- ated the appearance of patellar tendon, menisci, cru- ciate and collateral ligaments, cartilage, joint effusions, plicae, and bone contusion patterns. Criteria for characterizing a tendon as abnormal were an alteration in thickness compared with the remainder of the tendon and abnormal signal within the tendon. Because of the potential effect of the magic angle on the patellar tendon, changes suggestive of patellar tendinopathy included an al- teration in size as well as an abnormal signal. The meniscus was considered discoid if the ratio of body segments to the anterior and posterior horns Nancy M. Major 1 Clyde A. Helms Received October 8, 2001; accepted after revision March 4, 2002. 1 Both authors: Department of Radiology, Duke University Medical Center, Box 3808, Durham, NC 27710. Address correspondence to N. M. Major. AJR 2002;179:641–644 0361–803X/02/1793–641 © American Roentgen Ray Society M Downloaded from www.ajronline.org by 27.70.129.20 on 03/21/23 from IP address 27.70.129.20. Copyright ARRS. For personal use only; all rights reserved

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
MR Imaging of the Knee: Findings in Asymptomatic Collegiate Basketball PlayersFindings in Asymptomatic Collegiate Basketball Players
OBJECTIVE
.
The purpose of our study was to evaluate the knees of asymptomatic high- level collegiate basketball players before the beginning of the basketball season to gain an un- derstanding of nonclinical findings in this patient population.
SUBJECTS AND METHODS
.
Bilateral knee MR imaging examinations of 17 varsity basketball players (12 men and five women) were performed before basketball season began. All of the subjects were imaged on a 1.5-T magnet. The MR imaging studies were reviewed by two musculoskeletal radiologists. Structures analyzed were the menisci, ligaments, carti- lage, plicae, and bone marrow. The presence of a joint effusion was also noted.
RESULTS
.
Fourteen (41%) of the 34 knees had bone marrow edema, eight (24%) showed signal in the patellar tendon, and 14 (41%) had abnormal cartilage signal or a focal abnormal- ity. Twelve (35%) of the 34 knees showed a joint effusion. Two knees (6%)
showed abnormal signal along the infrapatellar plica. Four knees (12%) were noted to have a discoid meniscus.
CONCLUSION
.
An MR examination of the knees of high-level collegiate basketball players may show changes unique to this population. The changes seen on MR imaging in these athletes may be asymptomatic abnormalities. For instance, changes suggestive of patel- lar tendinopathy were identified in these asymptomatic subjects.
R imaging has proven useful for evaluating the knee for internal derangement. This imaging mo-
dality is accurate for evaluating meniscal ab- normalities [1–3] as well as for assessing the integrity of the anterior cruciate ligament [4, 5], examining articular cartilage [6, 7], and diagnosing bone marrow edema [8].
This study was prompted by requests to evaluate several of our division I college bas- ketball players for knee problems before the rigorous college basketball season began. At the time of these MR imaging studies, abnor- malities were noted within the knee joint that did not prove to be symptomatic to the player. This finding prompted us to evaluate the knees of all the basketball players to assess changes that could be misinterpreted as abnormal if a player presented for imaging during the sea- son. Our study evaluates the spectrum of MR imaging findings in bilateral knees in asymp- tomatic high-level collegiate basketball players to provide a baseline for interpretation.
Subjects and Methods
Both knees of 17 varsity college basketball play- ers (12 men and five women)
were imaged (
n
= 34
knees) during the course of their preseason physical examination. Internal review board approval for this study was obtained. The athletes were questioned about any relevant prior injury or surgery. All sub- jects were imaged on a 1.5-T magnet (Signa; Gen- eral Electric Medical Systems, Milwaukee, WI) using a send–receive knee coil. Our routine knee protocol was performed: fast spin-echo T2-weighted images (TR/TE
eff
×
192 with 2 excitations, a slice thickness of 4 mm with an interslice gap of 0.4 mm, and a field of view of 16 cm were used. The MR studies were reviewed independently by two musculoskeletal radiologists, forming a consensus opinion; the reviewers evalu- ated the appearance of patellar tendon, menisci, cru- ciate and collateral ligaments, cartilage, joint effusions, plicae, and bone contusion patterns.
Criteria for characterizing a tendon as abnormal were an alteration in thickness compared with the remainder of the tendon and abnormal signal within the tendon. Because of the potential effect of the magic angle on the patellar tendon, changes suggestive of patellar tendinopathy included an al- teration in size as well as an abnormal signal. The meniscus was considered discoid if the ratio of body segments to the anterior and posterior horns
Nancy M. Major
Received October 8, 2001; accepted after revision March 4, 2002.
1
Both authors: Department of Radiology, Duke University Medical Center, Box 3808, Durham, NC 27710. Address correspondence to N. M. Major.
AJR
AJR:179, September 2002
Major and Helms
was less than 1:2 on sagittal imaging and if the pro- tuberant meniscus extended deep within the joint, which was best seen on coronal imaging [9, 10]. If abnormal signal within the substance of the menis- cus interrupted the articular surface or if abnormal morphology was present on the proton density im- ages, a tear was diagnosed. Ligaments were as- sessed as abnormal if they were discontinuous, abnormal in size, or contained increased signal intensity on T2-weighted images. A plica was con- sidered abnormal if it had increased signal on T2-
weighted imaging or showed a subjective increase in thickness. Bone marrow was considered abnor- mal if high signal was identified on fat-suppressed fast spin-echo images. Cartilage was considered abnormal if it had high signal, focal or diffuse, or showed full-thickness defects on the fat-suppressed T2-weighted images in any imaging plane.
Results
≈
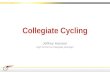
1:2); this finding was bilateral in two players (Fig. 2). Eight (24%) of the 34 knees had abnormal signal in the cartilage (trochlea,
n
n
= 4), and six (18%) had focal cartilage defects (Fig. 3). One player had un- dergone arthroscopic débridement of a lateral femoral condyle cartilage defect 18 months before the study. The cartilage defect was seen on MR imaging and corresponded to the area that had been débrided arthroscopically (Fig. 4). Twelve (35%) of the 34 knees had small joint effusions, and 14 (41%) had bone mar- row edema (Fig. 5). Bone marrow edema was seen in the medial femoral condyle in seven knees, the lateral femoral condyle in two, the lateral tibial plateau in two, and the patella in three. Bone marrow edema was identified bi- laterally, but not symmetrically. In most cases, the pattern of bone marrow edema was neither subarticular nor adjacent to ligament attach-
ments. None of the players had tears in the cru- ciate or collateral ligaments, although one player was found to have an anterior cruciate ligament cyst. The players with focal cartilage abnormalities (six knees [18%]) included the player with a history of débridement. No inter- val change was noted in the appearance of his cartilage (the prior examination was available for comparison). Three of the subjects with fo- cal cartilage abnormalities showed focal de- fects at the apex of the patella, and three showed signal change at the apex of the patella without a full-thickness defect. One player showed abnormal high signal in both knees along the infrapatellar plica (Fig. 6). None of the players showed meniscal abnormalities. Discoid meniscus was noted but is not neces- sarily considered pathologic. These menisci are prone to tears, but no tears in the discoid menisci were found in this series.
Discussion
MR imaging is sensitive and specific for identifying injuries to the meniscus, anterior cruciate ligament, collateral ligaments, and tendons [1–5]. MR imaging performed using a marrow-sensitive technique is both sensi- tive and specific for the detection of bone contusions and occult fractures [8].
Little has been reported about the MR im- aging findings in the asymptomatic knee of the dedicated athlete [11–16]. Krampla et al. [17] examined the knees of marathon runners and identified no abnormal marrow signal after the runners had completed a marathon. One possi- ble explanation for the lack of edema in the pa- tients in their series could be the selected population. Trained runners such as maratho- ners have appropriate shoes or orthotics that can properly distribute stress across the joint.
The knee absorbs a large amount of force during a game of basketball, especially at the competitive collegiate level. During the course of a basketball season, a player’s knees are subject to repetitive trauma. Consequently, a high percentage of athletes have areas of signal abnormality in the bones, cartilage, and ten- dons. It is probably more accurate to say that the athletes are presumably asymptomatic. The players in our study were fully functional because none missed practices or games as a result of knee complaints. However, our MR findings suggest that the players might be symptomatic. Whether these athletes are truly asymptomatic is impossible to determine given the tremendous incentive to deny symp- toms at this level of play. The abnormalities
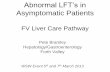
Fig. 1.—20-year-old male college basketball player with patellar tendon abnormality. Sagittal fast spin-echo T2- weighted MR image (TR/TEeff, 3500/65) obtained with fat suppression shows thickening of patellar tendon with fo- cus of high signal within substance of tendon (arrow). Findings resemble jumper’s knee, although patient was asymptomatic.
Fig. 2.—19-year-old male college basketball player with discoid me- niscus. Coronal fat-suppressed fast spin-echo MR image (TR/TEeff, 3500/ 65) reveals discoid meniscus. Ar- rows show meniscus extending more toward notch than expected for normal-sized meniscus. Finding was bilateral in this patient.
D ow
nl oa
de d
fr om
w w
w .a
jr on
lin e.
or g
by 2
7. 70
.1 29
.2 0
on 0
3/ 21
/2 3
fr om
I P
ad dr
es s
27 .7
0. 12
9. 20
. C op
yr ig
ht A
R R
S. F
or p
er so
AJR:179, September 2002
643
found in our study suggest that playing basket- ball at a high level for most of their lives might lead to some structural abnormalities within the knee. Possible expected abnormalities in- clude injuries to the meniscus, cartilage, liga- ments, and tendons, especially the patellar tendon. Bone contusions may also occur either in isolation or as a result of meniscal or liga- mentous abnormalities.
In our study, players denied having any pain in the knee, but 74% of the players had at least one abnormal finding that was pre- sumably asymptomatic. Although our sample of female basketball players was small, the im- aging findings were seen in both sexes.
No meniscal abnormality was identified in our study population. This finding differs from that of a prior study of football players, which reported meniscal abnormalities in 59% [12]. This difference is perhaps an effect of the type of movements a basketball player makes com- pared with the repetitive trauma sustained by football players including a higher incidence of twisting injuries. A discoid meniscus was identified in 12% of the knees in our series. This incidence of discoid meniscus is higher in our subjects than that seen in the ordinary pop- ulation and likely reflects the small number of subjects in our study.
Signal abnormalities were identified in the cartilage, but the players denied any symptoms referable to cartilage or the joint line.
As a pri- mary shock absorber in the knee, cartilage would be a likely area for developing abnor- malities. It would be interesting to note the changes in the cartilage after a subject has played a full season of competitive basketball.
Fig. 4.—21-year-old male college bas- ketball player with cartilage defect in knee. Sagittal fast spin-echo fat-sup- pressed MR image (TR/TEeff, 3500/65) shows focal cartilage abnormality (arrows) corresponding to known ar- throscopically débrided area.
Fig. 3.—20-year-old male college bas- ketball player with cartilage defect. Axial fast spin-echo T2-weighted MR image (TR/TEeff, 3500/65) obtained with fat suppression shows focal area of cartilage abnormality at apex of cartilage in patella (large arrow). Smaller defect (small arrow) can be seen along medial facet.
Fig. 5.—19-year-old male college basketball player with bone marrow edema. Ax- ial fast spin-echo T2-weighted MR image (TR/TEeff, 3500/65) shows area of high signal in medial portion of patella (arrows).
Fig. 6.—22-year-old male college basketball player with infrapatellar plica signal. Sagittal fast spin-echo fat-suppressed MR image (TR/TEeff, 3500/65) shows abnor- mal signal along infrapatellar plica (arrows).
D ow
nl oa
de d
fr om
w w
w .a
jr on
lin e.
or g
by 2
7. 70
.1 29
.2 0
on 0
3/ 21
/2 3
fr om
I P
ad dr
es s
27 .7
0. 12
9. 20
. C op
yr ig
ht A
R R
S. F
or p
er so
AJR:179, September 2002
Major and Helms
We plan to study these athletes immediately after the season as part of another project.
The findings in the patellar tendon are not sur- prising. Jumper’s knee is so named because of the frequency with which this entity, patellar ten- dinopathy, is seen in basketball players. Abnor- mal thickness and signal were identified in eight (24%) of the 34 knees. This finding is common in basketball players and could represent healed patellar tendinopathy. However, the appearance is also suggestive of symptomatic patellar tendi- nopathy. The findings of patellar tendinopathy in the players who are asymptomatic raise the question as to whether these findings should alert the trainer to treating the tendinopathy be- fore it becomes symptomatic to decrease poten- tially lost playing time if the player becomes symptomatic. Jumper’s knee can be a debilitat- ing injury. At a minimum, trainers and team physicians should monitor athletes with tendin- opathy more closely. Perhaps early identification can lead to early treatment.
The significance of the abnormal high sig- nal along the infrapatellar plica noted bilater- ally in one of the players is not clear. These findings might result from chronic stress or represent a variant of Hoffa’s disease. Ab- normal high signal along the infrapatellar plica was shown in one of our subjects.
One of the most surprising findings was the number of areas with bone marrow edema. Fourteen (41%) of the 34 knees showed bone marrow edema in at least one location. One possible explanation for this finding is that shock or microtrauma is being transmitted through the meniscus, dissipated by the carti- lage, and eventually absorbed into the bone, re- sulting in a microfracture or contusions. The continuous repetitive jumping and running in this sport may explain the presence of edema. No additional changes of osteoarthritis were as- sociated with the bone marrow edema; there- fore, this finding probably does not represent the changes described by Zanetti et al. [18].
One potential shortcoming in this study re- sults from the inherent problem in using dedi- cated athletes as subjects. The design of this study was to evaluate MR imaging findings in a small group of purportedly asymptomatic collegiate basketball players. Athletes are typi- cally stoic, and some players may fear losing playing time if they admit to having symp- toms. Nevertheless, this group of players rep- resents the typical cohort seen in sports
medicine and, thus, is the population needed to evaluate asymptomatic knees in athletes.
Another shortcoming is in the assumption of imaging the players “preseason.” The reality is that many of these athletes vigorously play basketball during the summer, and some are playing hard enough to make national or inter- national teams. Thus, the study was performed during the preseason only in relation to the col- lege basketball season. Regardless of summer league play, almost all players participate in basketball during the academic summer ses- sion. The findings in our study showed no dif- ference between the athletes known to have competed during the summer and those who did not compete during the summer.
In conclusion, 41% of the knees showed bone marrow edema. Abnormal cartilage sig- nal or a focal abnormality of cartilage was also seen in 41%. Signal along the infrapatellar plica was noted in two knees, and four knees (12%) were noted to have discoid meniscus. Joint effusions were identified in 35% of the knees imaged. Knowing what is “normal” for a competitive elite basketball player is impor- tant. Erroneously diagnosing bone contusions or cartilage abnormalities, for example, as ab- normal conditions could lead to decreased playing time or inappropriate therapy. Being uninformed about the significance of the find- ings of bone contusions or cartilage abnormal- ities, for example, could lead to aggressive therapies that may decrease the athlete’s play- ing time. This treatment strategy could be det- rimental to an athlete on scholarship with professional-level playing potential. The long- term effects of these findings are not known. The findings of patellar tendonitis might be potentially significant. Long-term evaluation and evaluation during the season might clarify the significance of our findings. A potential benefit of imaging players before the season is the detection of asymptomatic jumper’s knee. Early treatment of this entity may lead to a bet- ter long-term outcome for the player.
Acknowledgment
We thank Jeff Lamere for his help in coor- dinating this study.
References
1. Cheung L, Li K, Hollett M, Bergman A, Herfkens R. Meniscal tears of the knee: accuracy of detection with fast spin-echo MR imaging and arthroscopic correla-
tion in 293 patients.
Radiology
1997
;203:508–512 2. De Smet AA, Norris MA, Yandow DR, Quintana
FA, Graf BK, Keene JS. MR diagnosis of menis- cal tears of the knee: importance of high signal in the meniscus that extends to the surface.
AJR
1993
;161:101–107 3. Crues JI, Mink J, Levy T, Lotysch M, Stoller D.
Meniscal tears of the knee: accuracy of MR imag- ing.
Radiology
1987
;164:445–448 4. Mink J, Levy T, Crues JI. Tears of the anterior cru-
ciate ligament and menisci of the knee: MR imag- ing evaluation.
Radiology
1988
;167:769–774 5. Lee J, Yao L, Phelps C, Wirth C, Czajka J, Loz-
man J. Anterior cruciate ligament tears: MR im- aging compared with arthroscopy and clinical tests.
Radiology
1988
;166:861–864 6. Bohndorf K. Imaging of acute injuries of the articu-
lar surfaces (chondral, osteochondral and subchon- dral fractures).
Skeletal Radiol
1999
;28:545–560 7. Disler DG, Recht MP, McCauley TR. MR imaging of
articular cartilage.
Skeletal Radiol
2000
;29:367–377 8. Kapelov SR, Teresi LM, Bradley WG, et al. Bone
contusions of the knee: increased lesion detection with fast spin-echo MR imaging with spectroscopic fat saturation.
Radiology
1993
;189:901–904 9. Silverman JM, Mink JW, Deutsch AL. Discoid
menisci of the knee: MR imaging appearance.
Radiology
1989
;173:351–354 10. Rohren EM, Kosarek FS, Helms CA. Discoid lat-
eral meniscus and incidence of meniscal tears.
Skeletal Radiol
2001
;30:316–320 11. Quinn S, Brown T. Meniscal tears diagnosed with
MR imaging versus arthroscopy: how reliable a stan- dard is arthroscopy?
Radiology
1991
;181:843–847 12. Reinig J, McDevitt E, Ove P. Progression of
meniscal degenerative changes in college football players: evaluation with MR imaging.
Radiology
1991
;181:255–258 13. Brunner MC, Flower SP, Evancho AM, Allman
FL, Apple DF, Fajman WA. MRI of the athletic knee: findings in asymptomatic professional bas- ketball and collegiate football players.
Invest Ra- diol
;24:72–75 14. Ludman CN, Hough DO, Cooper TG, Gottschalk
A. Silent meniscal abnormalities in athletes: mag- netic resonance imaging of asymptomatic gym- nasts.
Br J Sports Med
1999
;33:414–416 15. Jerosch J, Hoffstetter I, Reer R, Assheuer J.
Strain-related long-term changes in the menisci in asymptomatic athletes.
Knee Surg Sports Trau- matol Arthrosc
1994
;2:8–13 16. Shellock FG, Deutsch AL, Mink JH, Kerr R. Do
asymptomatic marathon runners have an increased prevalence of meniscal abnormalities? an MR study of the knee in 23 volunteers.
AJR
1991
;157:1239–1241 17. Krampla W, Mayrhofer R, Malcher J, Kristen
KH, Urban M, Hruby W. MR imaging of the knee in marathon runners before and after competition.
Skeletal Radiol
2001
;30:72–76 18. Zanetti M, Bruder E, Romero J, Hodler J. Bone
marrow edema pattern in osteoarthritic knees: correlation between MR imaging and histologic findings.
Radiology
2000
OBJECTIVE
.
The purpose of our study was to evaluate the knees of asymptomatic high- level collegiate basketball players before the beginning of the basketball season to gain an un- derstanding of nonclinical findings in this patient population.
SUBJECTS AND METHODS
.
Bilateral knee MR imaging examinations of 17 varsity basketball players (12 men and five women) were performed before basketball season began. All of the subjects were imaged on a 1.5-T magnet. The MR imaging studies were reviewed by two musculoskeletal radiologists. Structures analyzed were the menisci, ligaments, carti- lage, plicae, and bone marrow. The presence of a joint effusion was also noted.
RESULTS
.
Fourteen (41%) of the 34 knees had bone marrow edema, eight (24%) showed signal in the patellar tendon, and 14 (41%) had abnormal cartilage signal or a focal abnormal- ity. Twelve (35%) of the 34 knees showed a joint effusion. Two knees (6%)
showed abnormal signal along the infrapatellar plica. Four knees (12%) were noted to have a discoid meniscus.
CONCLUSION
.
An MR examination of the knees of high-level collegiate basketball players may show changes unique to this population. The changes seen on MR imaging in these athletes may be asymptomatic abnormalities. For instance, changes suggestive of patel- lar tendinopathy were identified in these asymptomatic subjects.
R imaging has proven useful for evaluating the knee for internal derangement. This imaging mo-
dality is accurate for evaluating meniscal ab- normalities [1–3] as well as for assessing the integrity of the anterior cruciate ligament [4, 5], examining articular cartilage [6, 7], and diagnosing bone marrow edema [8].
This study was prompted by requests to evaluate several of our division I college bas- ketball players for knee problems before the rigorous college basketball season began. At the time of these MR imaging studies, abnor- malities were noted within the knee joint that did not prove to be symptomatic to the player. This finding prompted us to evaluate the knees of all the basketball players to assess changes that could be misinterpreted as abnormal if a player presented for imaging during the sea- son. Our study evaluates the spectrum of MR imaging findings in bilateral knees in asymp- tomatic high-level collegiate basketball players to provide a baseline for interpretation.
Subjects and Methods
Both knees of 17 varsity college basketball play- ers (12 men and five women)
were imaged (
n
= 34
knees) during the course of their preseason physical examination. Internal review board approval for this study was obtained. The athletes were questioned about any relevant prior injury or surgery. All sub- jects were imaged on a 1.5-T magnet (Signa; Gen- eral Electric Medical Systems, Milwaukee, WI) using a send–receive knee coil. Our routine knee protocol was performed: fast spin-echo T2-weighted images (TR/TE
eff
×
192 with 2 excitations, a slice thickness of 4 mm with an interslice gap of 0.4 mm, and a field of view of 16 cm were used. The MR studies were reviewed independently by two musculoskeletal radiologists, forming a consensus opinion; the reviewers evalu- ated the appearance of patellar tendon, menisci, cru- ciate and collateral ligaments, cartilage, joint effusions, plicae, and bone contusion patterns.
Criteria for characterizing a tendon as abnormal were an alteration in thickness compared with the remainder of the tendon and abnormal signal within the tendon. Because of the potential effect of the magic angle on the patellar tendon, changes suggestive of patellar tendinopathy included an al- teration in size as well as an abnormal signal. The meniscus was considered discoid if the ratio of body segments to the anterior and posterior horns
Nancy M. Major
Received October 8, 2001; accepted after revision March 4, 2002.
1
Both authors: Department of Radiology, Duke University Medical Center, Box 3808, Durham, NC 27710. Address correspondence to N. M. Major.
AJR
AJR:179, September 2002
Major and Helms
was less than 1:2 on sagittal imaging and if the pro- tuberant meniscus extended deep within the joint, which was best seen on coronal imaging [9, 10]. If abnormal signal within the substance of the menis- cus interrupted the articular surface or if abnormal morphology was present on the proton density im- ages, a tear was diagnosed. Ligaments were as- sessed as abnormal if they were discontinuous, abnormal in size, or contained increased signal intensity on T2-weighted images. A plica was con- sidered abnormal if it had increased signal on T2-
weighted imaging or showed a subjective increase in thickness. Bone marrow was considered abnor- mal if high signal was identified on fat-suppressed fast spin-echo images. Cartilage was considered abnormal if it had high signal, focal or diffuse, or showed full-thickness defects on the fat-suppressed T2-weighted images in any imaging plane.
Results
≈
1:2); this finding was bilateral in two players (Fig. 2). Eight (24%) of the 34 knees had abnormal signal in the cartilage (trochlea,
n
n
= 4), and six (18%) had focal cartilage defects (Fig. 3). One player had un- dergone arthroscopic débridement of a lateral femoral condyle cartilage defect 18 months before the study. The cartilage defect was seen on MR imaging and corresponded to the area that had been débrided arthroscopically (Fig. 4). Twelve (35%) of the 34 knees had small joint effusions, and 14 (41%) had bone mar- row edema (Fig. 5). Bone marrow edema was seen in the medial femoral condyle in seven knees, the lateral femoral condyle in two, the lateral tibial plateau in two, and the patella in three. Bone marrow edema was identified bi- laterally, but not symmetrically. In most cases, the pattern of bone marrow edema was neither subarticular nor adjacent to ligament attach-
ments. None of the players had tears in the cru- ciate or collateral ligaments, although one player was found to have an anterior cruciate ligament cyst. The players with focal cartilage abnormalities (six knees [18%]) included the player with a history of débridement. No inter- val change was noted in the appearance of his cartilage (the prior examination was available for comparison). Three of the subjects with fo- cal cartilage abnormalities showed focal de- fects at the apex of the patella, and three showed signal change at the apex of the patella without a full-thickness defect. One player showed abnormal high signal in both knees along the infrapatellar plica (Fig. 6). None of the players showed meniscal abnormalities. Discoid meniscus was noted but is not neces- sarily considered pathologic. These menisci are prone to tears, but no tears in the discoid menisci were found in this series.
Discussion
MR imaging is sensitive and specific for identifying injuries to the meniscus, anterior cruciate ligament, collateral ligaments, and tendons [1–5]. MR imaging performed using a marrow-sensitive technique is both sensi- tive and specific for the detection of bone contusions and occult fractures [8].
Little has been reported about the MR im- aging findings in the asymptomatic knee of the dedicated athlete [11–16]. Krampla et al. [17] examined the knees of marathon runners and identified no abnormal marrow signal after the runners had completed a marathon. One possi- ble explanation for the lack of edema in the pa- tients in their series could be the selected population. Trained runners such as maratho- ners have appropriate shoes or orthotics that can properly distribute stress across the joint.
The knee absorbs a large amount of force during a game of basketball, especially at the competitive collegiate level. During the course of a basketball season, a player’s knees are subject to repetitive trauma. Consequently, a high percentage of athletes have areas of signal abnormality in the bones, cartilage, and ten- dons. It is probably more accurate to say that the athletes are presumably asymptomatic. The players in our study were fully functional because none missed practices or games as a result of knee complaints. However, our MR findings suggest that the players might be symptomatic. Whether these athletes are truly asymptomatic is impossible to determine given the tremendous incentive to deny symp- toms at this level of play. The abnormalities
Fig. 1.—20-year-old male college basketball player with patellar tendon abnormality. Sagittal fast spin-echo T2- weighted MR image (TR/TEeff, 3500/65) obtained with fat suppression shows thickening of patellar tendon with fo- cus of high signal within substance of tendon (arrow). Findings resemble jumper’s knee, although patient was asymptomatic.
Fig. 2.—19-year-old male college basketball player with discoid me- niscus. Coronal fat-suppressed fast spin-echo MR image (TR/TEeff, 3500/ 65) reveals discoid meniscus. Ar- rows show meniscus extending more toward notch than expected for normal-sized meniscus. Finding was bilateral in this patient.
D ow
nl oa
de d
fr om
w w
w .a
jr on
lin e.
or g
by 2
7. 70
.1 29
.2 0
on 0
3/ 21
/2 3
fr om
I P
ad dr
es s
27 .7
0. 12
9. 20
. C op
yr ig
ht A
R R
S. F
or p
er so
AJR:179, September 2002
643
found in our study suggest that playing basket- ball at a high level for most of their lives might lead to some structural abnormalities within the knee. Possible expected abnormalities in- clude injuries to the meniscus, cartilage, liga- ments, and tendons, especially the patellar tendon. Bone contusions may also occur either in isolation or as a result of meniscal or liga- mentous abnormalities.
In our study, players denied having any pain in the knee, but 74% of the players had at least one abnormal finding that was pre- sumably asymptomatic. Although our sample of female basketball players was small, the im- aging findings were seen in both sexes.
No meniscal abnormality was identified in our study population. This finding differs from that of a prior study of football players, which reported meniscal abnormalities in 59% [12]. This difference is perhaps an effect of the type of movements a basketball player makes com- pared with the repetitive trauma sustained by football players including a higher incidence of twisting injuries. A discoid meniscus was identified in 12% of the knees in our series. This incidence of discoid meniscus is higher in our subjects than that seen in the ordinary pop- ulation and likely reflects the small number of subjects in our study.
Signal abnormalities were identified in the cartilage, but the players denied any symptoms referable to cartilage or the joint line.
As a pri- mary shock absorber in the knee, cartilage would be a likely area for developing abnor- malities. It would be interesting to note the changes in the cartilage after a subject has played a full season of competitive basketball.
Fig. 4.—21-year-old male college bas- ketball player with cartilage defect in knee. Sagittal fast spin-echo fat-sup- pressed MR image (TR/TEeff, 3500/65) shows focal cartilage abnormality (arrows) corresponding to known ar- throscopically débrided area.
Fig. 3.—20-year-old male college bas- ketball player with cartilage defect. Axial fast spin-echo T2-weighted MR image (TR/TEeff, 3500/65) obtained with fat suppression shows focal area of cartilage abnormality at apex of cartilage in patella (large arrow). Smaller defect (small arrow) can be seen along medial facet.
Fig. 5.—19-year-old male college basketball player with bone marrow edema. Ax- ial fast spin-echo T2-weighted MR image (TR/TEeff, 3500/65) shows area of high signal in medial portion of patella (arrows).
Fig. 6.—22-year-old male college basketball player with infrapatellar plica signal. Sagittal fast spin-echo fat-suppressed MR image (TR/TEeff, 3500/65) shows abnor- mal signal along infrapatellar plica (arrows).
D ow
nl oa
de d
fr om
w w
w .a
jr on
lin e.
or g
by 2
7. 70
.1 29
.2 0
on 0
3/ 21
/2 3
fr om
I P
ad dr
es s
27 .7
0. 12
9. 20
. C op
yr ig
ht A
R R
S. F
or p
er so
AJR:179, September 2002
Major and Helms
We plan to study these athletes immediately after the season as part of another project.
The findings in the patellar tendon are not sur- prising. Jumper’s knee is so named because of the frequency with which this entity, patellar ten- dinopathy, is seen in basketball players. Abnor- mal thickness and signal were identified in eight (24%) of the 34 knees. This finding is common in basketball players and could represent healed patellar tendinopathy. However, the appearance is also suggestive of symptomatic patellar tendi- nopathy. The findings of patellar tendinopathy in the players who are asymptomatic raise the question as to whether these findings should alert the trainer to treating the tendinopathy be- fore it becomes symptomatic to decrease poten- tially lost playing time if the player becomes symptomatic. Jumper’s knee can be a debilitat- ing injury. At a minimum, trainers and team physicians should monitor athletes with tendin- opathy more closely. Perhaps early identification can lead to early treatment.
The significance of the abnormal high sig- nal along the infrapatellar plica noted bilater- ally in one of the players is not clear. These findings might result from chronic stress or represent a variant of Hoffa’s disease. Ab- normal high signal along the infrapatellar plica was shown in one of our subjects.
One of the most surprising findings was the number of areas with bone marrow edema. Fourteen (41%) of the 34 knees showed bone marrow edema in at least one location. One possible explanation for this finding is that shock or microtrauma is being transmitted through the meniscus, dissipated by the carti- lage, and eventually absorbed into the bone, re- sulting in a microfracture or contusions. The continuous repetitive jumping and running in this sport may explain the presence of edema. No additional changes of osteoarthritis were as- sociated with the bone marrow edema; there- fore, this finding probably does not represent the changes described by Zanetti et al. [18].
One potential shortcoming in this study re- sults from the inherent problem in using dedi- cated athletes as subjects. The design of this study was to evaluate MR imaging findings in a small group of purportedly asymptomatic collegiate basketball players. Athletes are typi- cally stoic, and some players may fear losing playing time if they admit to having symp- toms. Nevertheless, this group of players rep- resents the typical cohort seen in sports
medicine and, thus, is the population needed to evaluate asymptomatic knees in athletes.
Another shortcoming is in the assumption of imaging the players “preseason.” The reality is that many of these athletes vigorously play basketball during the summer, and some are playing hard enough to make national or inter- national teams. Thus, the study was performed during the preseason only in relation to the col- lege basketball season. Regardless of summer league play, almost all players participate in basketball during the academic summer ses- sion. The findings in our study showed no dif- ference between the athletes known to have competed during the summer and those who did not compete during the summer.
In conclusion, 41% of the knees showed bone marrow edema. Abnormal cartilage sig- nal or a focal abnormality of cartilage was also seen in 41%. Signal along the infrapatellar plica was noted in two knees, and four knees (12%) were noted to have discoid meniscus. Joint effusions were identified in 35% of the knees imaged. Knowing what is “normal” for a competitive elite basketball player is impor- tant. Erroneously diagnosing bone contusions or cartilage abnormalities, for example, as ab- normal conditions could lead to decreased playing time or inappropriate therapy. Being uninformed about the significance of the find- ings of bone contusions or cartilage abnormal- ities, for example, could lead to aggressive therapies that may decrease the athlete’s play- ing time. This treatment strategy could be det- rimental to an athlete on scholarship with professional-level playing potential. The long- term effects of these findings are not known. The findings of patellar tendonitis might be potentially significant. Long-term evaluation and evaluation during the season might clarify the significance of our findings. A potential benefit of imaging players before the season is the detection of asymptomatic jumper’s knee. Early treatment of this entity may lead to a bet- ter long-term outcome for the player.
Acknowledgment
We thank Jeff Lamere for his help in coor- dinating this study.
References
1. Cheung L, Li K, Hollett M, Bergman A, Herfkens R. Meniscal tears of the knee: accuracy of detection with fast spin-echo MR imaging and arthroscopic correla-
tion in 293 patients.
Radiology
1997
;203:508–512 2. De Smet AA, Norris MA, Yandow DR, Quintana
FA, Graf BK, Keene JS. MR diagnosis of menis- cal tears of the knee: importance of high signal in the meniscus that extends to the surface.
AJR
1993
;161:101–107 3. Crues JI, Mink J, Levy T, Lotysch M, Stoller D.
Meniscal tears of the knee: accuracy of MR imag- ing.
Radiology
1987
;164:445–448 4. Mink J, Levy T, Crues JI. Tears of the anterior cru-
ciate ligament and menisci of the knee: MR imag- ing evaluation.
Radiology
1988
;167:769–774 5. Lee J, Yao L, Phelps C, Wirth C, Czajka J, Loz-
man J. Anterior cruciate ligament tears: MR im- aging compared with arthroscopy and clinical tests.
Radiology
1988
;166:861–864 6. Bohndorf K. Imaging of acute injuries of the articu-
lar surfaces (chondral, osteochondral and subchon- dral fractures).
Skeletal Radiol
1999
;28:545–560 7. Disler DG, Recht MP, McCauley TR. MR imaging of
articular cartilage.
Skeletal Radiol
2000
;29:367–377 8. Kapelov SR, Teresi LM, Bradley WG, et al. Bone
contusions of the knee: increased lesion detection with fast spin-echo MR imaging with spectroscopic fat saturation.
Radiology
1993
;189:901–904 9. Silverman JM, Mink JW, Deutsch AL. Discoid
menisci of the knee: MR imaging appearance.
Radiology
1989
;173:351–354 10. Rohren EM, Kosarek FS, Helms CA. Discoid lat-
eral meniscus and incidence of meniscal tears.
Skeletal Radiol
2001
;30:316–320 11. Quinn S, Brown T. Meniscal tears diagnosed with
MR imaging versus arthroscopy: how reliable a stan- dard is arthroscopy?
Radiology
1991
;181:843–847 12. Reinig J, McDevitt E, Ove P. Progression of
meniscal degenerative changes in college football players: evaluation with MR imaging.
Radiology
1991
;181:255–258 13. Brunner MC, Flower SP, Evancho AM, Allman
FL, Apple DF, Fajman WA. MRI of the athletic knee: findings in asymptomatic professional bas- ketball and collegiate football players.
Invest Ra- diol
;24:72–75 14. Ludman CN, Hough DO, Cooper TG, Gottschalk
A. Silent meniscal abnormalities in athletes: mag- netic resonance imaging of asymptomatic gym- nasts.
Br J Sports Med
1999
;33:414–416 15. Jerosch J, Hoffstetter I, Reer R, Assheuer J.
Strain-related long-term changes in the menisci in asymptomatic athletes.
Knee Surg Sports Trau- matol Arthrosc
1994
;2:8–13 16. Shellock FG, Deutsch AL, Mink JH, Kerr R. Do
asymptomatic marathon runners have an increased prevalence of meniscal abnormalities? an MR study of the knee in 23 volunteers.
AJR
1991
;157:1239–1241 17. Krampla W, Mayrhofer R, Malcher J, Kristen
KH, Urban M, Hruby W. MR imaging of the knee in marathon runners before and after competition.
Skeletal Radiol
2001
;30:72–76 18. Zanetti M, Bruder E, Romero J, Hodler J. Bone
marrow edema pattern in osteoarthritic knees: correlation between MR imaging and histologic findings.
Radiology
2000
Related Documents