SCIENTIFIC ARTICLE MR findings in patients with disabling musculocutaneous chronic graft-versus-host disease M. Horger & A. Boss & W. Bethge & C. Faul & G. Fierlbeck & A. Bornemann & C. D. Claussen & W. Vogel Received: 16 April 2008 / Revised: 23 May 2008 / Accepted: 25 May 2008 / Published online: 12 July 2008 # ISS 2008 Abstract Objective To describe musculocutaneous MR-findings re- sponsible for disability in chronic graft-versus-host disease (cGVHD) after allogeneic hematopoietic cell transplantation (HCT). Material and methods Between June 2005 and February 2008, we performed whole-body musculoskeletal magnetic resonance imaging (MRI; n =12) or regional MRI (n =4) in 16 consecutive patients presenting with disabling sclerodermatous cGVHD (e.g., skin edema, fixed deep dermal sclerosis, joint contractures, painful muscular con- tractures, or myalgia). Results In all patients, MRI showed musculocutaneous abnormalities reflecting different degrees of inflammation and collagen tissue involvement of the skin (n =10), subcutaneous fat tissue (n =13), muscle fasciae (n =16), subfascial muscular septae (n =6), or findings compatible with myositis (n =3). The most frequently involved muscle fasciae comprised those of the vastus lateralis muscle (n = 12), biceps femoris muscle (n =11), gastrocnemius medialis muscle (n =8), serratus anterior muscle, and latissimus dorsi muscle (each, n =5). Increased signal of involved tissues on STIR-images and fat-saturated postgadolinium T1- weighted images represented the most frequent MR-signal abnormalities. Conclusion MR imaging of musculocutaneous cGVHD allows accurate evaluation including assessment of deep tissue infiltration and assists in the differential diagnosis. Keywords Disabling chronic musculocutaneous graft versus host disease . MR-imaging . Fascial thickening . Myositis . Subcutaneous fascial thickening . Impairment of motility Introduction Chronic graft-versus-host disease (cGVHD) is a disabling complication after allogeneic hematopoietic cell transplan- tation (HCT) with important cutaneous manifestations often resulting in joint contractures and fasciitis [1, 2]. Cutaneous cGVHD can be differentiated into an early lichenoid phase characterized by a band-like infiltrate of lymphocytes and a late sclerodermatoid type with thick- ening of dermal collagen bundles. The dermal fibrosis usually extends into subcutis, resulting in septal hyalini- zation. The sclerodermoid cGVHD can be classified into a morpheaformic stage with plaques of dermal sclerosis resembling morphea (localized scleroderma), and a gener- alized sclerodermic stage, the latter often resulting in disability with joint contractures, fasciitis, and musculo- Skeletal Radiol (2008) 37:885–894 DOI 10.1007/s00256-008-0535-3 M. Horger (*) : A. Boss : C. D. Claussen Department of Diagnostic Radiology, Eberhard-Karls-University, Hoppe-Seyler-Str.3, 72076 Tübingen, Germany e-mail: [email protected] W. Bethge : C. Faul : W. Vogel Department of Internal Medicine-Oncology, Eberhard-Karls-University, Ottfried-Müller-Str. 5, 72070 Tübingen, Germany G. Fierlbeck Department of Dermatology, Eberhard-Karls-University, Liebermeisterstraße 25, 72070 Tübingen, Germany A. Bornemann Insitute for Brain Research, Eberhard-Karls-University, Calwerstraße 3, 72076 Tübingen, Germany

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
SCIENTIFIC ARTICLE
MR findings in patients with disabling musculocutaneouschronic graft-versus-host disease
M. Horger & A. Boss & W. Bethge & C. Faul &G. Fierlbeck & A. Bornemann & C. D. Claussen & W. Vogel
Received: 16 April 2008 /Revised: 23 May 2008 /Accepted: 25 May 2008 / Published online: 12 July 2008# ISS 2008
AbstractObjective To describe musculocutaneous MR-findings re-sponsible for disability in chronic graft-versus-host disease(cGVHD) after allogeneic hematopoietic cell transplantation(HCT).Material and methods Between June 2005 and February2008, we performed whole-body musculoskeletal magneticresonance imaging (MRI; n=12) or regional MRI (n=4)in 16 consecutive patients presenting with disablingsclerodermatous cGVHD (e.g., skin edema, fixed deepdermal sclerosis, joint contractures, painful muscular con-tractures, or myalgia).Results In all patients, MRI showed musculocutaneousabnormalities reflecting different degrees of inflammationand collagen tissue involvement of the skin (n=10),
subcutaneous fat tissue (n=13), muscle fasciae (n=16),subfascial muscular septae (n=6), or findings compatiblewith myositis (n=3). The most frequently involved musclefasciae comprised those of the vastus lateralis muscle (n=12), biceps femoris muscle (n=11), gastrocnemius medialismuscle (n=8), serratus anterior muscle, and latissimus dorsimuscle (each, n=5). Increased signal of involved tissueson STIR-images and fat-saturated postgadolinium T1-weighted images represented the most frequent MR-signalabnormalities.Conclusion MR imaging of musculocutaneous cGVHDallows accurate evaluation including assessment of deeptissue infiltration and assists in the differential diagnosis.
Keywords Disabling chronicmusculocutaneous graft versushost disease .MR-imaging . Fascial thickening .Myositis .
Subcutaneous fascial thickening . Impairment of motility
Introduction
Chronic graft-versus-host disease (cGVHD) is a disablingcomplication after allogeneic hematopoietic cell transplan-tation (HCT) with important cutaneous manifestationsoften resulting in joint contractures and fasciitis [1, 2].Cutaneous cGVHD can be differentiated into an earlylichenoid phase characterized by a band-like infiltrate oflymphocytes and a late sclerodermatoid type with thick-ening of dermal collagen bundles. The dermal fibrosisusually extends into subcutis, resulting in septal hyalini-zation. The sclerodermoid cGVHD can be classified into amorpheaformic stage with plaques of dermal sclerosisresembling morphea (localized scleroderma), and a gener-alized sclerodermic stage, the latter often resulting indisability with joint contractures, fasciitis, and musculo-
Skeletal Radiol (2008) 37:885–894DOI 10.1007/s00256-008-0535-3
M. Horger (*) :A. Boss :C. D. ClaussenDepartment of Diagnostic Radiology, Eberhard-Karls-University,Hoppe-Seyler-Str.3,72076 Tübingen, Germanye-mail: [email protected]
W. Bethge : C. Faul :W. VogelDepartment of Internal Medicine-Oncology,Eberhard-Karls-University,Ottfried-Müller-Str. 5,72070 Tübingen, Germany
G. FierlbeckDepartment of Dermatology, Eberhard-Karls-University,Liebermeisterstraße 25,72070 Tübingen, Germany
A. BornemannInsitute for Brain Research, Eberhard-Karls-University,Calwerstraße 3,72076 Tübingen, Germany

skeletal system involvement in ca. 3.4% of patients [3–5].Fasciitis, resembling eosinophilic fasciitis is another raremanifestation of cGVHD and is limited to muscular fasciae.Compared to skin lesions, polymyositis is far less commonin cGVHD and usually occurs rather late after HCT [6–8].However, the extent and severity of these pathologic findingsis variable, and their clinical detection depending on theinvolved anatomical sites often proves to be difficult.
In this article, we present the results of magneticresonance imaging (MRI) imaging in 16 consecutive patientsdiagnosed with disabling musculocutaneous cGVHD at ourinstitution. In order to explain the particular localization ofthese abnormalities throughout the musculocutaneous sys-tem, we describe additional clinical and hematologic dataand try to correlate proposed pathomechanisms with ourMR-imaging findings. Finally, we review possible differen-tial diagnoses of disabling musculocutaneous cGVHD.
Material and methods
Patient cohort
At our institution, additional MRI evaluation of patientspresenting with disabling cGVHD is part of a standardizedwork-up initiated to improve patient management. In thisstudy, we retrospectively evaluated the MRI findings,clinical symptoms, and laboratory data of 16 consecutivepatients diagnosed with disabling musculocutaneouscGVHD after allogeneic HCT between June, 2005 andFebruary, 2008. During this period, 106 (53%) of 199patients receiving allogeneic HCT at our center developedacute GVHD and 60 (30%) patients were diagnosed withcGVHD during follow-up. Among patients with cGVHD,12 (20%) patients presented with musculocutaneous symp-toms such as joint contractures, impaired mobility andmyalgia classifiable as disabling cGVHD (according to NIHConsensus Development Project on Criteria from ClinicalTrials in Chronic Graft-versus-Host Disease) and under-went musculoskeletal MRI for assessment of musculofas-cial and joint involvement by cGVHD [9]. Additionally,four patients were identified retrospectively by a PACSreview, searching for musculoskeletal MR investigationsperformed at our institution in patients after allogeneic HCTsince the year 2002. We performed whole-body MRI in 12patients and regional MRI in four patients.
Our institutional review board approved this retrospec-tive study and waived informed consent.
Clinical data
All 16 consecutive patients included in this retrospectivestudy revealed cutaneous, subcutaneous, fascial, or mus-
cular abnormalities that were related to their cGVHD.Nine patients were female, and seven were male, with amedian age of 44 years (range, 26–72 years). The patientshad received allogeneic HCT for treatment of acutemyelogenous leukemia (AML; n=9), chronic lymphocyticleukemia (CLL) with transformation into high-grade non-Hodgkin lymphoma (hg-NHL; n=2), hg-NHL (n=2),acute lymphoblastic leukemia (ALL; n=2), and follicularNHL (n=1).
HCT was performed from HLA-matched related (n=7)or unrelated (n=9) donors.
Clinical, laboratory, and biological features in our patientsincluding the type of underlying hematological disease,conditioning regimens, degree of acute skin GVHD, type ofGVHD-prophylaxis, and onset time of cGVHD wererecorded. At the occurrence of edematous skin lesions, acomplete blood cell count and chemistry including C-reactiveprotein levels was performed in all patients. Serum creatinekinase levels were determined in all patients with myalgia.
Clinical signs of sclerodermatous cGVHD such as skindiscoloration, skin induration, joint contractures, impairedmobility, and myalgia were documented together with theinvolved anatomical regions.
The diagnosis of chronic skin GVHD was established byclinical observation during follow-up and in associationwith other organ manifestations of cGVHD in nine patients[9]. A deep biopsy was performed in six patients withsclerotic skin lesions including subcutis, subcutaneous fat,intermediate septa, and muscular fascia either on arm,thigh, or trunk. In two patients, additional muscle biopsieswere taken. Specimens were fixed in formaldehyde andfurther embedded in paraffin.
MR imaging protocol
Whole-Body-MRI exams were conducted at a 1.5-Teslaclosed-bore whole-body MR scanner (Siemens Avanto,Erlangen, Germany) equipped with parallel-imaging tech-nology of up to 32 independent receiver channels [Siemenstotal imaging matrix (TIM) technique]. A signal wasrecorded with the complete matrix coil set with 76 pluggedarray elements. For whole-body MRI examinations, a state-of-the-art MR imaging from head to toe was performedusing high-performance gradients (max. amplitude: 45 mT/m;min. rise time 200 µs, max. slew rate 200 T/m/s), integratedparallel acquisition technique (iPAT) in three spatial directionsand a total scan range of 205 cm by combining the large field-of-view (500 mm) with automatic table move. We used fivesubsequent table positions in coronal direction (head/thorax;thorax/abdomen; pelvis; upper leg; lower leg) and in axialdirection (over the involved sites). The imaging protocolconsisted of gradient-echo localizers on each table positionfollowed by T1-weighted FSE sequences (TR/TE, 602/
886 Skeletal Radiol (2008) 37:885–894
13 ms), STIR images (TR/TE/TI, 6700/87/150 ms), andcontrast-enhanced fat-suppressed T1-weighted images, per-formed after unique intravenous application of Gd-DTPA(Magnevist, Schering, Berlin, Germany). The total examina-tion time was about 40 min. Stacks of fused whole bodyimages were generated using the standard workstationsoftware. Two regional MRI examinations were performedon a 1.5-T MR scanner (Sonata, Erlangen, Germany) usingthe same sequence protocol as above, limited to a soleanatomical region (e.g., lower limb).
In one patient, only coronal and axial STIR images couldbe performed before the patient declined further imagingdue to anxiety. In two patients, whole-body MRI wasperformed only nonenhanced because of severely restrictedrenal function.
MR image analysis
Two radiologists (M.H., C.D.C) with over 15 yearsexpertise in musculoskeletal diagnosis analyzed both imagesets independently. Studies were presented in random order,blinded to patient data, date, and time. All individual cross-sectional images and fused whole-body images (in patientsundergoing WB-MRI) were evaluated for: (a) evidence andanatomical distribution; (b) depth infiltration of inflamma-tory or fibrotic lesions (such as skin, subcutaneous fattytissue septae, muscle fasciae, intramuscular septal, andmusculature) and accompanying tenosynovial or enthesialchanges; (c) MR imaging characteristics of cGVHD-associated musculocutaneous abnormalities (signal charac-teristics on T1-weighted images, STIR images, and post-GdT1-weighted fat-suppressed images) as well as for (d)incidence of musculocutaneous cGVHD-related abnormal-ities throughout the body; (e) patterns of distribution(symmetrical vs. asymmetrical) of these abnormalities;and (f) clinical/radiological matching performed (consider-ing either the distribution of sclerodermatous skin changesor of skin induration).
Assessment differences were resolved by consensus
Definitions of musculocutaneous abnormalities associatedwith cGVHD
Skin thickening
Focal plaque-like or circular thickening of the skin,sometimes also accompanied by scar-like retraction, areeasily identified on MRI by comparison with unin-volved skin areas and in contrast to physiological signalof skin on T1-weighted-, STIR- and post-Gd-images(Fig. 1a). We classified skin thickening according to avisual score as follows: (− none), (+ mild to moderate) and(++ strong).
Subcutaneous septal thickening
Lattice-like thickening of subcutaneous fatty tissue septacontrasting to the otherwise homogenous MR signal ofadipose tissue (Fig. 1b and c). We classified subcutane-ous septal thickening similarly with cutaneous thickeningas follows: (−; none), (+; mild to moderate), and (++;strong).
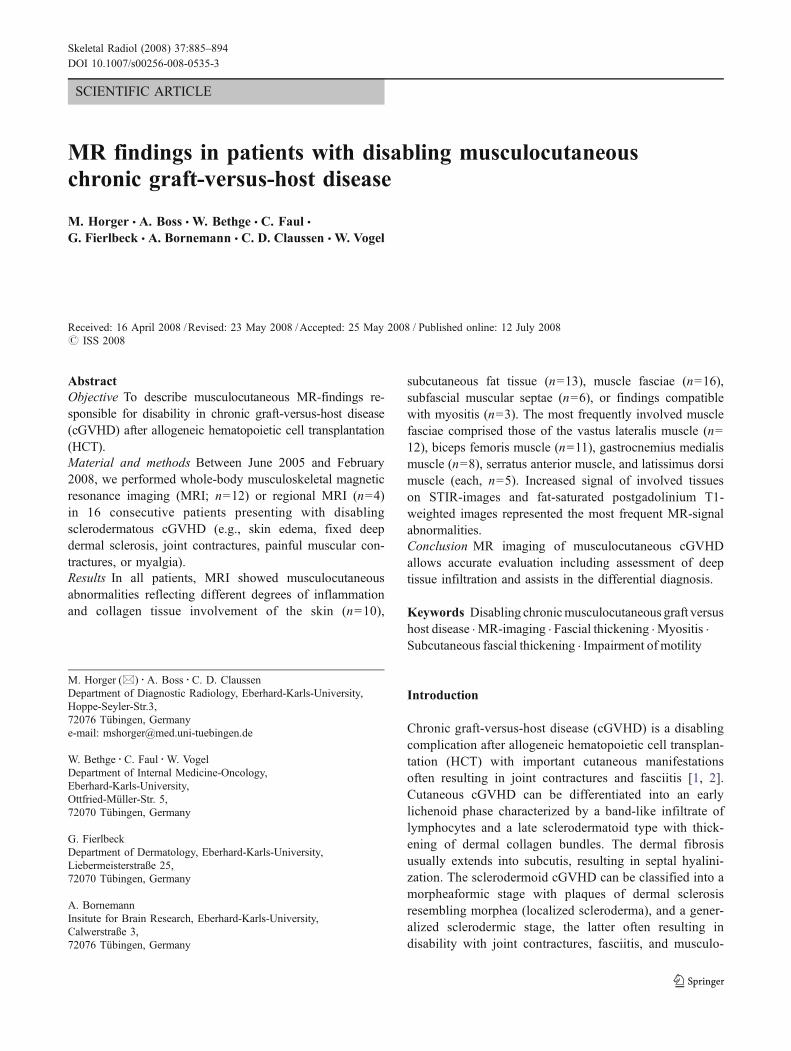
Fig. 1 a, b, and c A 44-year-old female patient with disablingcGVHD claiming about progressive impairment of mobility andstiffness, especially in the lower limbs. Axial fat-saturated T1-weighted postgadolinium TSE image through the femoral condylesshows focally thickened and retracted skin (long arrows) as well asthickening of subcutaneous fatty tissue septa (short arrows) bothaccompanied by intense Gd enhancement (a). Note that the subcuta-neous reticular abnormalities are asymmetrically distributed, nonde-pendent, and adjacent to involved muscle fasciae. Osteonecrosis isseen in both distal femoral bones. This represents another frequentmusculoskeletal complication after allogeneic HCT. Axial STIR image(b) through both mid-thighs and the corresponding axial fat-saturatedT1-weighted postgadolinium TSE image (c) shows thickening ofsubcutaneous fatty tissue septa with increased signal on water-selective STIR image (arrows) and lattice-like Gd-enhancement(arrows). Note also muscle fascial thickening (arrowhead)
Skeletal Radiol (2008) 37:885–894 887
Fascial thickening
Thickening and/or increased Gd-enhancement of muscularfascia was considered abnormal. Fascial thickening can befocal or generalized (Fig. 2). We considered fascial thickening<2 mm as moderate (+), and a thickness of the muscle fasciaexceeding 2 mm (range, 2–7 mm) as strong (++). Thereby,Gd-enhancement was considered moderate (isointense tomusculature) or marked (higher than muscular signal).
Involvement of perifascial intramuscular septa presentsat MRI as edema-like signal on fluid-sensitive sequences aswell as increase in signal on post-Gd T1-weighted fat-suppressed images due to collagen tissue septa (as stated byhistological analysis; Fig. 3).
Myositis
Abnormal, focal, or diffuse muscular signal abnormalitiesshowing hyperintensity on STIR images and Gd-enhancementwere considered suggestive of myositis (Fig. 4).
Clinical/radiological matching was categorized as positive(yes) if anatomical sites of clinically diagnosed disabilitycorresponded to involved musculoskeletal regions at MRI, onlyin part positive (partial matching) or negative (no matching).
Results
Clinical and laboratory findings
Patients presented at clinical inspection with either skindiscoloration (n=8), skin induration (n=12), myalgia (n=5), or impaired mobility (n=15). Disability was projectedby the patients on the following anatomical regions: thigh(n=10), calf (n=9), arms (n=8), torso (n=5), and face (n=2). None of the patients reclaimed disability of the pelvic orabdominal wall regions.
After allogeneic HCT, 12 patients developed acute skinGVHD, four did not. All patients received GVHDprophylaxis. Immunosuppression for GVHD was discon-tinued in nine patients after a mean time of 186 days (range,38–400 days). In seven patients, immunosuppressivetherapy was continuously administered until diagnosis ofcGVHD.
No significant influence of the conditioning regimensused was observed (data not shown). In 13 patients, totalbody irradiation (TBI) was part of the conditioning regimen,one patient received additional radioimmunotherapy.
At the clinical onset of disabling sclerodermatoidcGVHD, elevated counts of peripheral eosinophils (median1,132/µl, range 633–6630) were measured in all patients,but no eosinophilic infiltration was found in the biopsyspecimens.
MRI-findings
a) We found cGVHD-related musculocutaneous abnor-malities in following anatomical regions: pelvis (n=
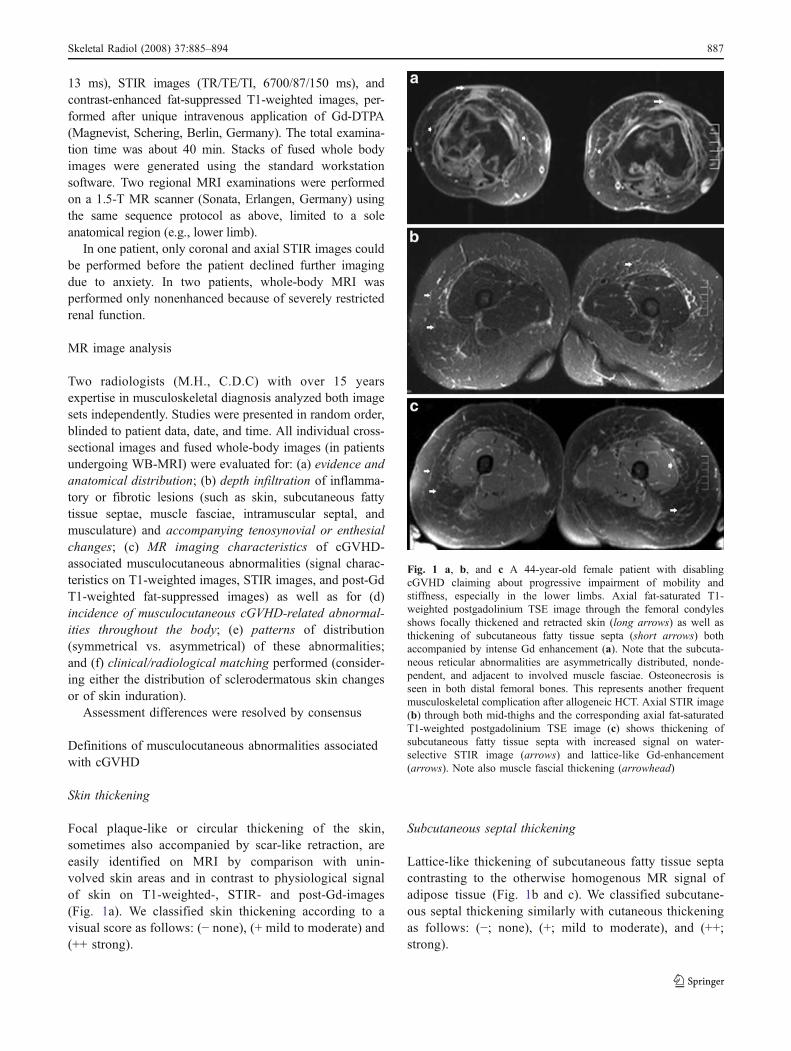
Fig. 2 Whole-body coronal STIR-image in a 44-year-old femalepatient with sclerodermatous disabling cGVHD. Note almost ubiqui-tous fascial thickening with increased MR-signal (arrows). Note alsoabnormal signal in the subcutaneous fatty tissue septa, but the leadingfinding in this case was the fasciitis
888 Skeletal Radiol (2008) 37:885–894
11), thigh (n=15), calf (n=13), arms (n=4), torso (n=7), and abdominal wall (n=7).
b) Patients with disabling chronic musculocutaneousGVHD showed different degrees of depth infiltration.
Focal skin thickening on MR-imaging in our series wasclassified as strong (n=3), moderate (n=7) or absent (n=6).Thickening of fatty tissue septae was found in 13 patients;five of them were scored as strong, eight proved moderate.In six patients, pathological MR signal was found in themusculature, adjacent to the involved fasciae, probablycaused by infiltration of peripheral intramuscular septae byinflammation and collagen tissue. MR-signal abnormalitiessuggestive of myositis were observed in three patients. Oneof them presented with a riffled pattern involving moremuscle groups; the second patient presented with solelyinvolvement of the adductor muscles, while the third patientrevealed patchy distribution throughout almost all musclegroups.
Associated joint synovitis, tenosynovitis, and enthesitiswere diagnosed in six patients. Patients presented withthickening of the knee synovia and increased Gd-enhancementin the knee joint (n=5) and the ankle joint (n=4). One patientshowed signs of tenosynovitis of the tibialis anterior muscle.In one patient, thickening of the insertion of the gluteusmedium muscle was noted.
c) MR imaging characteristics. GVHD-related signalabnormalities of the cutaneous, subcutaneous, or
muscular fascial thickening appeared hypointense tosubcutaneous fat in all patients on T1-weighted images.On STIR images, MR signal proved always hyperin-tense to neighboring fat tissue and musculature. AfterIV Gd-application, subcutaneous thickened fatty septarevealed strong enhancement in seven patients, while insix patients, postgadolinium signal was isointense tothat of the adjacent musculature. Among the threepatients with myositis, signal abnormalities on T1-weighted-, STIR- and fat-saturated postgadolinium T1-weighted images differed, probably due to differentdegrees of rhabdomyolysis with release of protein richsecretion (Figs. 4 and 5a,b,c,d).
d) Incidence of musculocutaneous findings in cGVHD.The leading abnormality in this series was musclefascial thickening. Of all patients presenting withfascial thickening (n=16), only one had symmetrical,circular thickening of muscle fasciae with no prefer-ence for certain muscle compartments, while the otherspresented with focal or more extended but asymmetri-cal thickening of the muscle fasciae. Involvement ofthe thigh musculature was diagnosed in all patientsreceiving whole-body MRI (n=12) and in threepatients receiving only a regional MR investigationwas performed, based on the distribution of skinchanges. In the thigh, the vastus lateralis muscle was
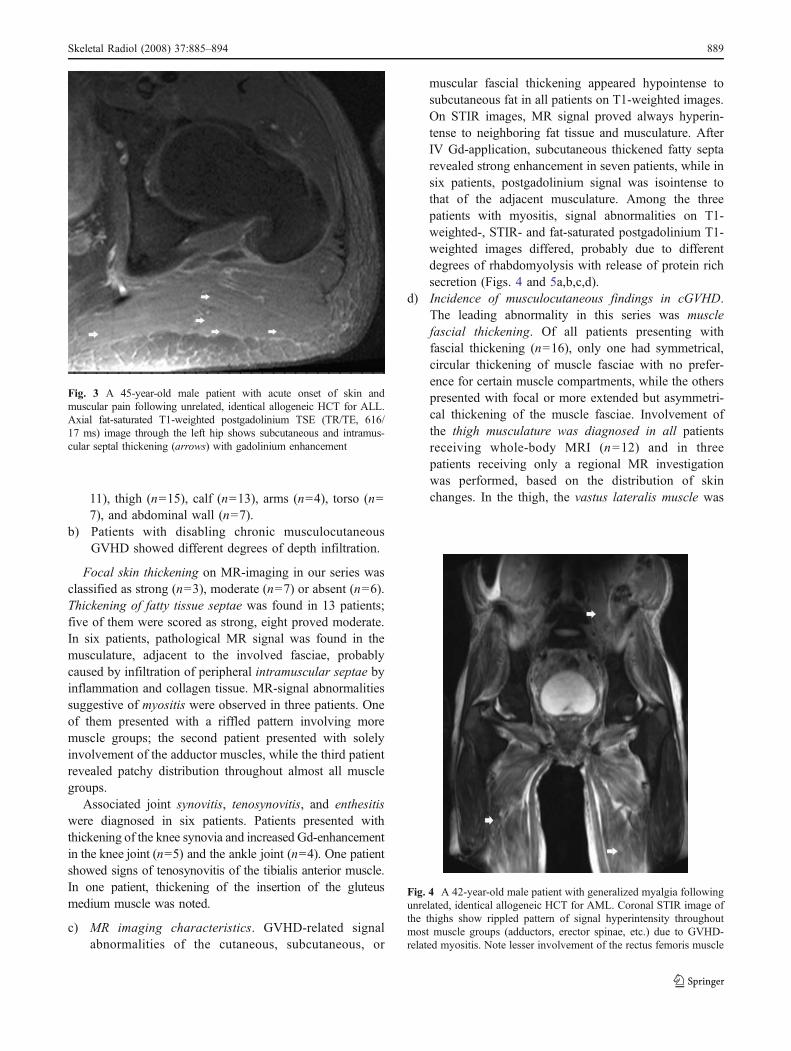
Fig. 4 A 42-year-old male patient with generalized myalgia followingunrelated, identical allogeneic HCT for AML. Coronal STIR image ofthe thighs show rippled pattern of signal hyperintensity throughoutmost muscle groups (adductors, erector spinae, etc.) due to GVHD-related myositis. Note lesser involvement of the rectus femoris muscle
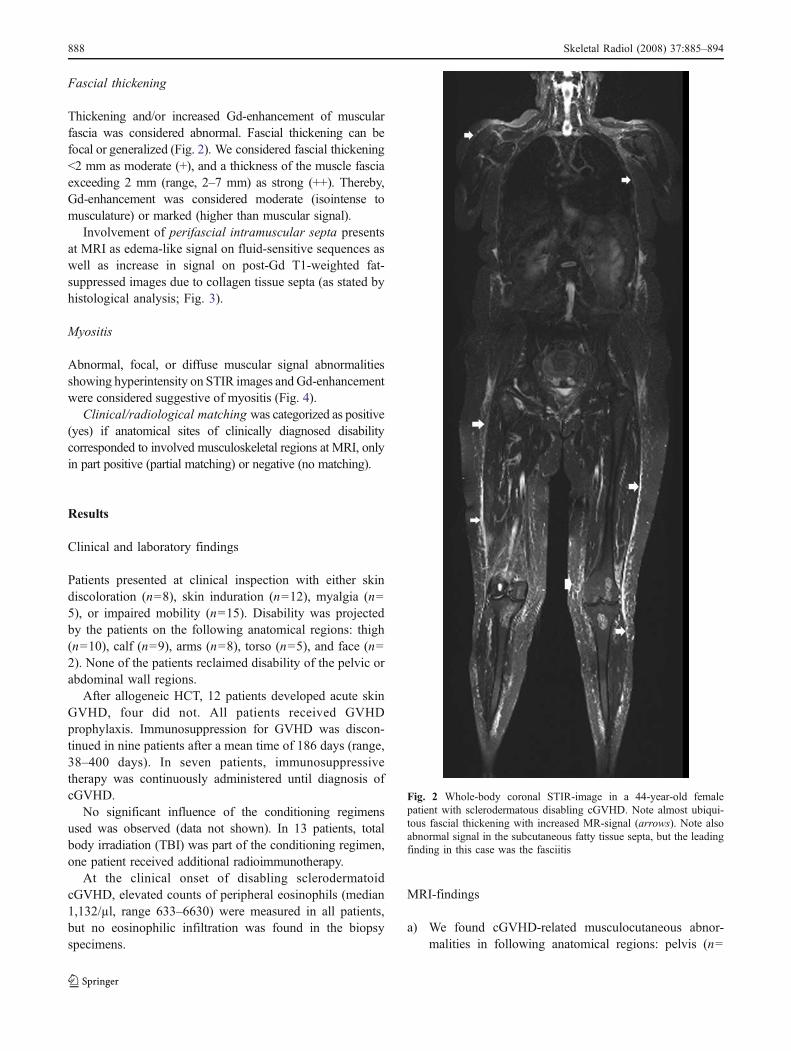
Fig. 3 A 45-year-old male patient with acute onset of skin andmuscular pain following unrelated, identical allogeneic HCT for ALL.Axial fat-saturated T1-weighted postgadolinium TSE (TR/TE, 616/17 ms) image through the left hip shows subcutaneous and intramus-cular septal thickening (arrows) with gadolinium enhancement
Skeletal Radiol (2008) 37:885–894 889
involved (n=12), followed by the biceps femorismuscle (n=11) and the muscles of the medial musclecompartment (semimembranous muscle, semitendinousmuscle, gracilis muscle, and adductor muscles; Fig. 6).Interestingly, the vastus medialis and intermediusmuscles as well as the rectus femoris muscles wereinvolved in only one patient presenting a symmetricalpattern of involvement of all fascias.
The muscle fasciae of the calves were involved in 13patients (in two of them, only regional MRI wasperformed). In the calf, the muscle fascia of the medialgastrocnemius muscle (n=8) was most often involved,followed by the tibialis anterior muscle (n=7) andgastrocnemius lateralis muscle (n=2).
Pelvic fascial involvement was noted in 11 patients; inone of them, only regional MRI was performed. In thepelvis, the fascia of the gluteus medius muscle (n=7) wasmost frequently involved (Fig. 7). Thickening of othermuscular fasciae was also diagnosed in the gluteus
maximus muscle (n=5), obturator externus muscle (n=2),and the obturator internus muscle (n=2).
Torso involvement was diagnosed in seven patients,while four patients revealed fascial involvement of theabdominal wall muscles (Fig. 8a). The torso musculaturewas involved in six patients, all of them presenting withthickened fascia of the serratus muscle (n=5) and thelattissimus dorsi muscle (n=5).
Five patients revealed fascial and/or subcutaneous colla-gen tissue septal thickening in the abdominal wall, along thefasciae of the oblicus externus and internus muscles (n=3).
Fascial thickening along the musculature of the upperextremity was diagnosed in three patients, one of thempresenting also involvement of the palmar muscle fasciae.The musculature of the upper extremity was involved in twopatients. One patient revealed abnormal thickness and Gd-enhancement of the fascia of the deltoid (n=2) and bicepsbrachii muscle (n=1), while the other presented the sameabnormalities along the fasciae of the flexor digitorummuscle, interossei muscle, and lumbricales muscles (Fig. 8b).
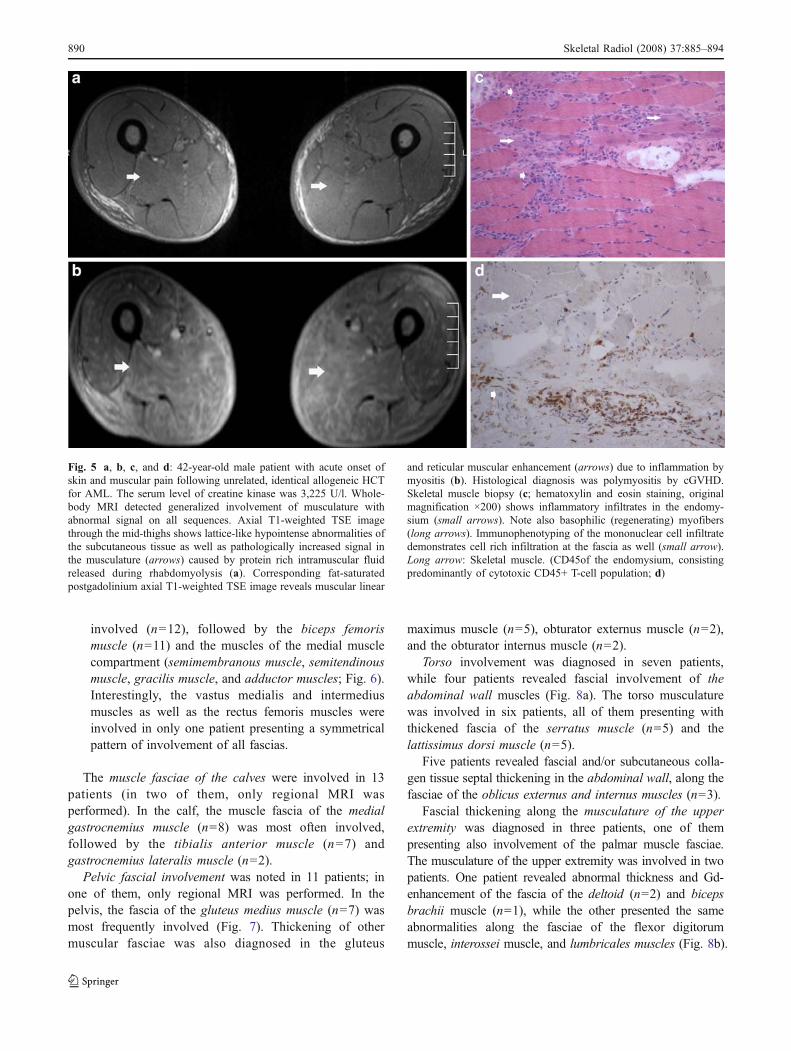
Fig. 5 a, b, c, and d: 42-year-old male patient with acute onset ofskin and muscular pain following unrelated, identical allogeneic HCTfor AML. The serum level of creatine kinase was 3,225 U/l. Whole-body MRI detected generalized involvement of musculature withabnormal signal on all sequences. Axial T1-weighted TSE imagethrough the mid-thighs shows lattice-like hypointense abnormalities ofthe subcutaneous tissue as well as pathologically increased signal inthe musculature (arrows) caused by protein rich intramuscular fluidreleased during rhabdomyolysis (a). Corresponding fat-saturatedpostgadolinium axial T1-weighted TSE image reveals muscular linear
and reticular muscular enhancement (arrows) due to inflammation bymyositis (b). Histological diagnosis was polymyositis by cGVHD.Skeletal muscle biopsy (c; hematoxylin and eosin staining, originalmagnification ×200) shows inflammatory infiltrates in the endomy-sium (small arrows). Note also basophilic (regenerating) myofibers(long arrows). Immunophenotyping of the mononuclear cell infiltratedemonstrates cell rich infiltration at the fascia as well (small arrow).Long arrow: Skeletal muscle. (CD45of the endomysium, consistingpredominantly of cytotoxic CD45+ T-cell population; d)
890 Skeletal Radiol (2008) 37:885–894
e) The pattern of distribution of cGVHD-related MRIabnormalities was asymmetrical in 15 patients andsymmetrical in one patient.
f) Clinical (disability)/radiological matching
Impaired mobility and MRI findings matched entirely ineight patients, only partially in seven patients, and none inone patient. In one patient presenting with muscular andfascial abnormalities in the thigh at MRI, the clinicalexamination proved inconspicuous. However, the patientcomplained about impaired mobility of the ankles causedby peritendinitis of the Achilles tendon which wasdocumented by ultrasound. In seven patients, MRI dis-closed involvement of additional anatomical sites (pelvis,thigh, or calf regions) that were clinically inconspicuous.Myalgia was the leading symptom in four patients. Onlytwo of them presented elevated serum creatine kinase levelsat the time of MRI examination, while only three showedmyositis-related MRI-signal abnormalities (Fig. 9).
Skin induration was also a frequent symptom, but it didnot correlate well with impaired mobility and related MRIabnormalities. Skin discoloration was not further evaluatedstatistically, as it does not represent a typical sign fordisabling cGVHD.
Discussion
Chronic GVHD includes inflammatory and/or fibrosingmanifestations that may arise at various times aftertransplantation of any organ containing lymphoid cells.Thereby, mucocutaneous manifestations are the mostfrequent, followed by involvement of the gastrointestinaltract, liver, and lung. The incidence of chronic GVHD isreported to be 25–60% in patients undergoing allogeneicHCT. The skin is involved in 90% of cGVHD [8, 10]. Maintypes of cutaneous manifestations in cGVHD are lichenoid
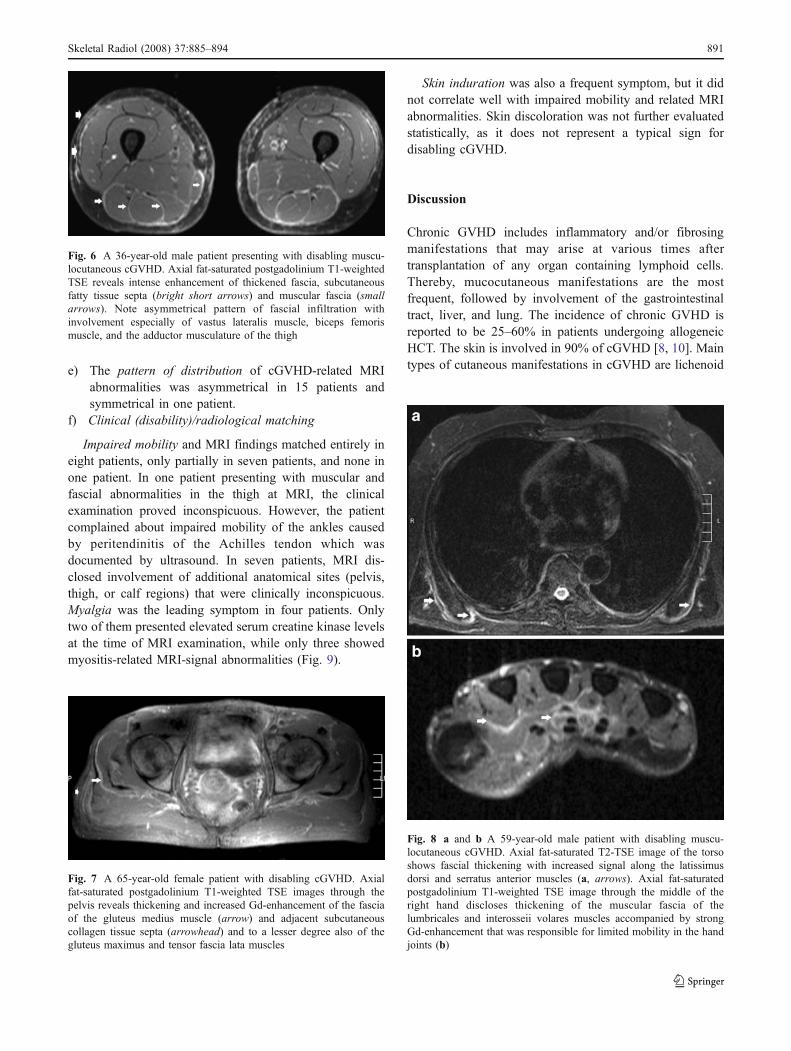
Fig. 6 A 36-year-old male patient presenting with disabling muscu-locutaneous cGVHD. Axial fat-saturated postgadolinium T1-weightedTSE reveals intense enhancement of thickened fascia, subcutaneousfatty tissue septa (bright short arrows) and muscular fascia (smallarrows). Note asymmetrical pattern of fascial infiltration withinvolvement especially of vastus lateralis muscle, biceps femorismuscle, and the adductor musculature of the thigh
Fig. 7 A 65-year-old female patient with disabling cGVHD. Axialfat-saturated postgadolinium T1-weighted TSE images through thepelvis reveals thickening and increased Gd-enhancement of the fasciaof the gluteus medius muscle (arrow) and adjacent subcutaneouscollagen tissue septa (arrowhead) and to a lesser degree also of thegluteus maximus and tensor fascia lata muscles
Fig. 8 a and b A 59-year-old male patient with disabling muscu-locutaneous cGVHD. Axial fat-saturated T2-TSE image of the torsoshows fascial thickening with increased signal along the latissimusdorsi and serratus anterior muscles (a, arrows). Axial fat-saturatedpostgadolinium T1-weighted TSE image through the middle of theright hand discloses thickening of the muscular fascia of thelumbricales and interosseii volares muscles accompanied by strongGd-enhancement that was responsible for limited mobility in the handjoints (b)
Skeletal Radiol (2008) 37:885–894 891
or sclerodermatoid. Disabling cGVHD is often a latemanifestation of cGVHD.
Additional to cutaneous manifestations, deep extensionof sclerosis in the subcutaneous fat involving intermediatesepta separating the fat lobules as well as muscle fasciaeand much rarer even the muscles themselves belong to therecognized manifestations of cGVHD. Among these,fasciitis constitutes a rare form of cGVHD that leads withtime to impaired mobility of the involved extremities. Theproximal part of the limbs and the trunk of the body areconsidered the preferentially affected sites. Fasciitis incGVHD might be a late, deep extension of a superficialsclerosis; however, there have been described cases offasciitis that were not always associated with sclerodermi-formic cutaneous lesions [6, 11, 12]. This knowledgecorrelates, in part, also with the results of our observationthat the presence of subcutaneous fibrotic changes includ-ing fasciitis was not always accompanied by sclerodermi-formic cutaneous lesions. Our results prove that fascialthickening, contrary to existing data, is a much morecommon finding in patients with sclerodermatoid disablingcGVHD (100% in our series). However, related signalabnormalities on MRI differ with respect to their intensity.Thus, while cutaneous, subcutaneous, and muscular fascialthickening always showed hypointensity on T1-weightedand hyperintensity on T2-weighted images, Gd-enhancementvaried consistently. This might be explained by differentdegrees of inflammatory activity and secondary collageniza-tion [6].
Unexpectedly, multifocality was diagnosed in all patientsreceiving WB-MRI. Most affected sites in our study werethe thighs, followed by the calves, pelvic, torso, and theabdominal regions, and finally the arms. Depth infiltrationof the arms proved rarer in our series, contrary to theincidence of superficial sclerodermiformic abnormalities.The pattern of involvement of muscular fascia in cGVHDseemed almost predictable (e.g., m. biceps femoris, m.vastus lateralis at the thighs; m. gastrocnemius medialis inthe calves, and the latissimus dorsi and serratus muscles atthe torso). This predilection for certain muscle groups mayprove beneficial for differential diagnosis. Generally, theclinical examination underestimated both degree of depthinfiltration and extent of cGVHD-related abnormalities(especially fasciitis) as the latter often occurred also inanatomical locations were the overlaying skin provedinconspicuous. We found discrepancies between patient’sdisability (joint contraction, impaired mobility) and local-
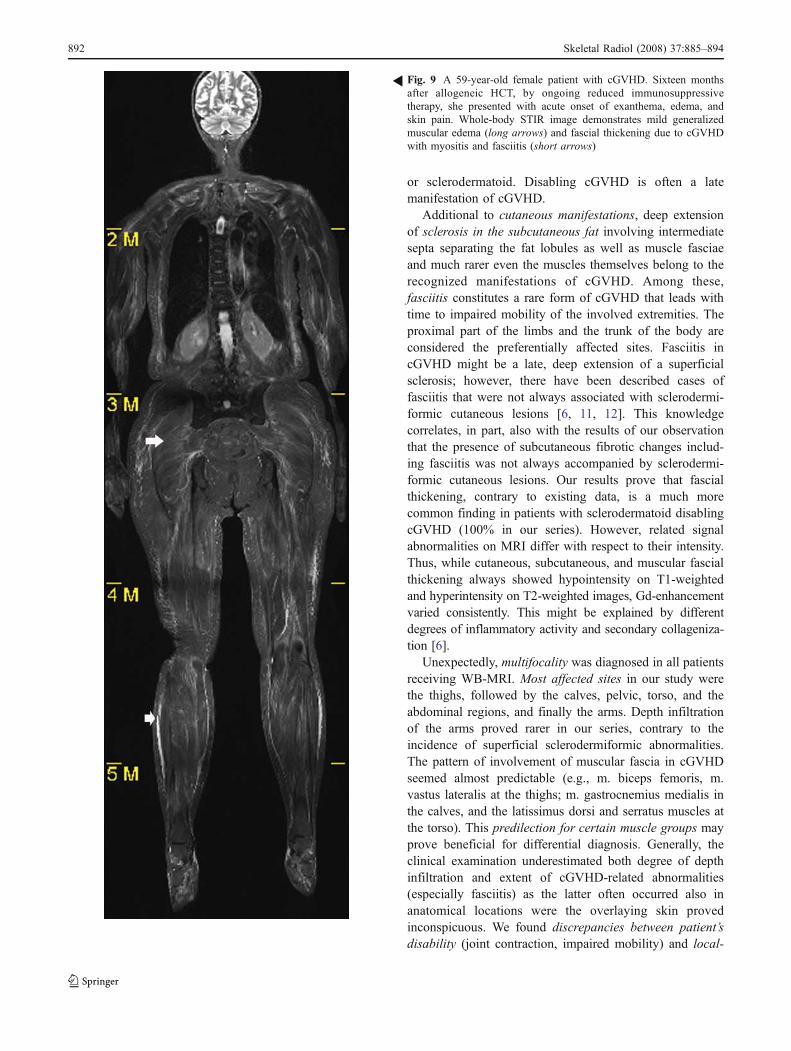
Fig. 9 A 59-year-old female patient with cGVHD. Sixteen monthsafter allogeneic HCT, by ongoing reduced immunosuppressivetherapy, she presented with acute onset of exanthema, edema, andskin pain. Whole-body STIR image demonstrates mild generalizedmuscular edema (long arrows) and fascial thickening due to cGVHDwith myositis and fasciitis (short arrows)
R
892 Skeletal Radiol (2008) 37:885–894

ization of responsible MR-imaging findings. Some of theaffected anatomical regions (abdominal wall, pelvis) docu-mented by MRI proved clinically asymptomatic, whileothers (e.g., face) proved discomfortable despite minimalsubcutaneous infiltration. Locations most often associatedwith disability were knees, ankles, hands, and shoulders,probably caused by limitation of motion in the adjacentjoints. Polymyositis that has been described as an infrequentneuromuscular complication after allogeneic HCT wasfound in three of our patients. The manifestations of post-transplant myositis are indistinguishable from thosereported for idiopathic myositis including muscle weakness,pain, and elevated CK. However, involvement of lowerextremities seems to be more common after HCT [13, 14].In our series, riffled or patchy multifocal muscularinvolvement predominated; however, one patient presentedwith isolated signal abnormalities in the adductor muscleloge but normal serum CK levels quickly resolved onsteroid therapy. Different MR-signal intensities on non-enhanced T1-weighted images in our series are likely torepresent different concentrations of extracellular proteinscaused by protein rich intramuscular fluid due to rhabdo-myolysis. Correlation between myalgia, serum level ofcreatine kinase, and expected MR findings matched onlypartially. Polymyositis may occur with other manifestations,but might also be the only manifestation of cGVHD [15]. Inour cohort, all patients presented mild accompanyingfasciitis. In contrast to fasciitis, polymyositis is usuallyresponsive to immunosuppressive therapy with steroids,tacrolimus, or cyclosporine and does not affect the overallprognosis. Reports about the association of cutaneouscGVHD with extracutaneous manifestations like articularsynovitis or tenosynovitis are rare [16]. Nevertheless, someof our patients presented also signs of tenosynovitis orenthesitis.
Immediate implications for patient’s management canbe derived from our findings. Therapies that addressexclusively the cutaneous form of sclerodermatouscGVHD (e.g., phototherapy) may have too little impacton deeper tissues and should be at least combined withsystemic immunosuppression.
Concerning the pathomechanisms of fasciitis in cGVHD,it has been postulated that the inflammatory reaction mightbe directly triggered in the fascia by a local microlesioninduced by microtrauma in the muscular fascia withsubsequent wound-healing fibrosis [6]. The role of totalbody irradiation (TBI) for induction of microtraumata withsecondary wound healing and sclerosis has also beenconsidered along the time as a promoter of fibrosis.Interestingly, 13 out of 16 patients in our series weretreated with a standard TBI-containing protocol. However,the pattern of fibrotic changes could not be explained byregional differences of radiotherapy intensity alone. Prob-
ably, the high degree of mobility and the friction betweenthe arms and the torso and the repeated microtrauma in thegluteal region and the thighs related to sitting areresponsible for the differences in the distribution patternof cGVHD manifestations.
A striking feature common in all our patients was bloodeosinophilia at the onset of the disease. The literaturesuggests that cGVHD and eosinophilic fasciitis may havesome common clinical and histological findings thatoverlap each other [17–19]. Janin et al. considered thatintense eosinophil activation often leads to cell lysis, andtherefore, subsequent detection of eosinophils in biopsyspecimens of older lesions proves difficult [20, 21]. In linewith this data, although elevated counts of peripheraleosinophils were present in all our patients at the clinicalonset of disabling sclerodermatous cGVHD, there were noeosinophils detected on biopsy.
From a differential diagnostic point of view, thickeningof subcutaneous collagen tissue septa and muscular fasciaeas reported in this cohort resemble, in part, findings thathave been reported in patients with other disorders such aseosinophilic fasciitis (EF) or scleroderma. EF can bedifferentiated from cGVHD due to the absence of skinchanges. Furthermore, in cGVHD, involvement of musclefascia seems to show preference for particular musclegroups. A difficult differential diagnosis to cGVHD islocalized scleroderma (morphea) which shares similarhistological and radiological findings and also the samepattern of fascial involvement as cGVHD. In a differentclinical setting, other types of fasciitis would deserveattention for differentiation, such as the macrophagicmyofasciitis, radiation-induced myofasciitis, TNF receptor-associated periodic syndrome, or even palmar fasciitis [22,23]. Particularly, the nephrogenic systemic fibrosis (NSF)shows clinically and histologically great resemblance tocGVHD [24]. However, fascial thickening and subcutane-ous collagenization in NSF usually show no preferentialdistribution throughout the muscle groups of the limbs.Other potential differential diagnoses such as eosinophilia–myalgia syndrome that is linked to the ingestion of a di-L-tryptophan aminal of acetaldehyde, or the even moreseldom so called Spanish toxic oil syndrome, should beexcluded anamnestically. Furthermore, in the latter, sclerosisis located only in the dermis and not in the fascia as in all ourpatients [25].
Limited by its small size, the current study encouragesthe use of MRI for accurate diagnosis of depth infiltrationand degree of musculocutaneous abnormalities in patientswith disabling cGVHD, as they are not always assessableby the clinical examination. MRI could also be imple-mented as a therapy monitoring tool of this disorder thatmight deliver information with respect to the degree ofactivity of cGVHD.
Skeletal Radiol (2008) 37:885–894 893

Conclusion
MR imaging of musculocutaneous cGVHD allows accurateevaluation including assessment of deep tissue infiltrationand assists in the differential diagnosis.
References
1. Graze PR, Gale RP. Chronic graft versus host disease: a syndromeof disordered immunity. Am J Med 1979; 66: 611–620.
2. Deeg HS, Storb R, Thomas ED. Bone marrow transplantation: areview of delayed complications. Br J Haematol 1984; 57: 185–208.
3. Penas PF, Jones-Cabllero M, Aragues M, et al. Sclerodermatousgraft-vs-host disease. Clinical and pathological study of 17patients. Arch Dermatol 2002; 138: 924–934.
4. Shulman HM, Sale GE, Lerner KG, et al. Chronic cutaneousgraft-versus-host disease in man. Am J Pathol 1978; 92: 545–570.
5. Janin-Mercier A, Saurat JH, Bourges M, et al. The lichen planus-like and sclerotic phases of the graft versus host disease in man:an ultrastructural study of six cases. Acta Derm Venereol (Stockh)1981; 61: 187–193.
6. Janin A, Socie G, Devergie A, et al. Fasciitis in chronic graft-versus-host disease: a clinicopathologic study of 14 cases. AnnIntern Med 1994; 120(12): 993–998.
7. Anderson BA, Young PV, Kean WF, et al. Polymyositis in chronicgraft-versus-host disease. A case report. Arch Neurol 1982; 39:188–190.
8. Pier N, Dubowitz V. Chronic graft versus host disease presentingwith polymyositis. Br Med J (Clin Res Ed) 1983; 286: 2024.
9. Pavletic SZ, Martin P, Lee SJ, et al. Measuring therapeuticresponse in chronic graft-versus-host disease: National Institutesof Health Consensus Development Project on Criteria for ClinicalTrials in Chronic Graft-versus-Host Disease: IV. Response CriteriaWorking Group report. Biol Blood Marrow Transplant 2006;12(3): 252–266, Mar.
10. Aractingi S, Chosidow O. Cutaneous graft-versus-host disease.Arch Dermatol 1998; 134: 602–612.
11. Vazquez Botet MV, Sanchez JL. The fascia in systemic scleroderma.J Am Acad Dermatol 1980; 2: 36–42.
12. Krieg T, Meurer M. Systemic scleroderma. Clinical and patho-physiologic aspects. J Am Acad Dermatol 1988; 18: 457–481.
13. Sato N, Okamoto S, Mori T, et al. Recurrent acute myositis afterallogeneic bone marrow transplantation for myelodysplasia.Hematology 2002; 7(2): 109–112.
14. Biju G, Debashis D, Mammen C, et al. Polymyositis—an unusualmanifestation of chronic GVHD. Rheumatol Int 2001; 20: 169–170.
15. Parker P, Chao NJ, Be-Ezra J, et al. Polymyositis as amanifestation of chronic graft versus host disease. Medicine(Baltimore) 1996; 75(5): 279–285.
16. Parker P, Chao NJ, Be-Ezra J, et al. Polymyositis as amanifestation of chronic graft versus host disease. Medicine(Baltimore) 1996; 75(5): 279–285.
17. Pincus SH, Ramesh KS, Wyler DJ. Eosinophils stimulatefibroblast DNA synthesis. Blood 1987; 70: 572–574.
18. Ustun C, Ho G Jr. Eosinophilic fasciitis after allogeneic stem celltransplantation: a case and review of the literature. LeukLymphoma 2004; 45(8): 1707–1709.
19. Caperton EM, Hataway DE, Dehner LP. Morphea, fasciitis andscleroderma with eosinophilia. A broad spectrum of disease.Arthritis Rheum 1976; 19: 792–793.
20. Markusse HM, Dijkmans BA, Fibbe WE. Eosinophilic fasciitisafter allogeneic bone marrow transplantation. J Rheumatol 1990;17: 692–694.
21. Janin A, Torpier G, Courtin P, et al. Segregation of eosinophilproteins in alveolar macrophage compartments in chronic eosin-ophilic pneumonia. Thorax 1993; 48: 57–62.
22. Desruelles F, Lacour J-P, Chevallier P, et al. Radiation myo-fasciitis. Acta Derm Venerol 2000; 80: 310–311.
23. McDermott MF, Aksentijevich I, Galon J, et al. Germlinemutations in the extracellular domains of the 55 kDa TNF-receptor, TNFR1, define a family of dominantly inherited auto-inflammatory syndromes. Cell 1999; 97: 133–140.
24. Broome DR, Girguis MS, Baron PW, et al. Gadodiamide-associated nephrogenis systemic fibrosis: why radiologists shouldbe concerned. AJR 2007; 188: 586–592.
25. Phelps RG, Fleischmajer R. Clinical, pathologic, and immuno-pathologic manifestations of the toxic oil syndrome. Analysis offourteen cases. J Am Acad Dermatol 1988; 18: 313–324.
894 Skeletal Radiol (2008) 37:885–894
Related Documents











