This document is built on the Early Warning and Response System (EWARS), daily data received through MOHWF and WHO from the service providers in settlements of the Unregistered Myanmar Nationals (UMNs) and from health facilities in Cox’s Bazar. As such, it can only be considered a snapshot of conditions in those reporting facilities. The presented information may hardly be viewed as representative of the overall health situation in Cox’s Bazar; nonetheless we believe that it gives all actors in the field a stepping stone for building a true picture of morbidity and mortality in the UMNs. We thank all partners contributing to the EWARS. The EWARS itself and the resulting reports can only be a work in progress. We welcome all comments, feedback and further inputs that can help to improve the system and our joint understanding of the prevailing epidemiological situation, and ultimately - to avert spread of diseases. Contact Information Dr. Edwin Salvador, Deputy WHO Representative / Incident Manager, [email protected] Dr. Hammam El Sakka, Team Leader, Health Emergency Programms, [email protected] WHO Bangladesh: http://www.searo.who.int/bangladesh ) Mortality and Morbidity Weekly Bulletin (MMWB Cox’s Bazar Volume N o 1: 15 October 2017 Photo Credit: WHO Bangladesh, Dr. Syed Mahfuzul Huq

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

This document is built on the Early Warning and Response System (EWARS), daily data received through MOHWF and WHO from the service providers in settlements of the Unregistered Myanmar Nationals (UMNs) and from health facilities in Cox’s Bazar. As such, it can only be considered a snapshot of conditions in those reporting facilities. The presented information may hardly be viewed as representative of the overall health situation in Cox’s Bazar; nonetheless we believe that it gives all actors in the field a stepping stone for building a true picture of morbidity and mortality in the UMNs. We thank all partners contributing to the EWARS.
The EWARS itself and the resulting reports can only be a work in progress. We welcome all comments, feedback and further inputs that
can help to improve the system and our joint understanding of the prevailing epidemiological situation, and ultimately - to avert spread
of diseases.
Contact Information Dr. Edwin Salvador, Deputy WHO Representative / Incident Manager, [email protected] Dr. Hammam El Sakka, Team Leader, Health Emergency Programms, [email protected]
WHO Bangladesh: http://www.searo.who.int/bangladesh
)Mortality and Morbidity Weekly Bulletin (MMWB
Cox’s Bazar
Volume No 1: 15 October 2017
Photo Credit: WHO Bangladesh, Dr. Syed Mahfuzul Huq
WHBangladesh

MMWB Morbidity and Mortality Weekly Bulletin, Cox’s Bazar, Bangladesh 15 October 2017 / Vol. 1
2
1. Early Warning and Response System (EWARS)
The main goal of the Early Warning and Response System (EWARS) in Cox’s Bazar District is the early
detection of and timely response to public health threats. The main attributes of the system are
sensitivity and timeliness.
Sensitivity defines the capacity of the system to detect all occurring public health alerts. Since any
signal can be the starting point of an outbreak or a public health crisis, EWARS must have the capacity to
detect all of them. At the level of reporting, sensitivity refers to the proportion of cases of a given
disease detected by the surveillance system. At the level of data analysis and decision-making,
sensitivity refers to the ability to detect outbreaks, including the ability to detect new and emerging
pathogens.
Timeliness defines the capacity of the system to detect a public health alert early enough for control
measures to have the greatest possible impact on morbidity and mortality. EWARS is designed to
reduce delays in reporting and to detect public health emergencies even when affecting individual or
limited disease clusters. Data received through surveillance must be analysed correctly, synthesized
clearly, and disseminated effectively. Other attributes to be taken into consideration during the EWARS
development and implementation are acceptability, usefulness, simplicity, representation, and
sustainability.
The success of effective EWARS functions in a national surveillance system depends on strong
commitment of both national authorities and health partners working in the field.
1.1 EWARS data collection form
All new cases and deaths are reported through a standardized data collection form, which has been
developed for the ongoing emergency in Cox’s Bazar. The data collection form includes the following
information: identification number, date of reporting, GPS coordinates, district, upazila, union, name of
the camps or health facility, total population, population under 5. In addition, name of responsible
person filling the form has to be included together with the contact information. The reporting form in
English is attached as Annex 1.
1.2 Health events under surveillance and case definitions
The EWARS reporting form contains the list of priority diseases and syndromes compiled based on the
epidemiological profiles of both Bangladesh and Myanmar; standardized case definitions were
developed and distributed to health partners along with the reporting forms.

MMWB Morbidity and Mortality Weekly Bulletin, Cox’s Bazar, Bangladesh 15 October 2017 / Vol. 1
3
The list of priority diseases/syndromes includes: acute watery diarrhoea (AWD), bloody diarrhoea (BD),
acute respiratory infections (ARI), suspected measles/rubella (SMR), acute flaccid paralysis (AFP),
suspected meningitis (MEN), acute jaundice syndrome (AJS), suspected haemorrhagic fever (HF),
neonatal Diseases (NNT), adult tetanus (AT), suspected malaria (SM), confirmed malaria (CM),
unexplained fever (UXF), severe malnutrition (SMN), skin diseases (SKN), eye infections (EIF), injuries
(INJ) and other consultations (OTH).
To facilitate data management, software has been developed by WHO and installed in the Control Room
of the Civil Surgeon Office in Cox’s Bazar. WHO Surveillance and Immunization Medical officers (SIMOs)
and MoHFW staff have been trained on standardized data collection tools. From daily collected and
processed data, trained data managers are able to generate reports down to the upazila level. On a daily
basis the data is shared with the MoHFW at central level. A global Information System (GIS) unit
established in the Control Room is actively mapping disease patterns in all settlements in Cox’s Bazar.
1.3 Population under surveillance and reporting units
The population under surveillance is the entire population of Unregistered Myanmar Nationals (UMNs)
living presently in different locations such as public places, established or informal camps, and within
host community in Cox’s Bazar. To calculate disease incidences, the denominator is calculated based on
IOM estimated population data as of 10 October 20171. New cases and deaths of health events under
surveillance are reported daily using the EWRAS standardized data collection tool form District Sadar
hospital Cox’s Bazar, health complexes in Ukhia and Teknaf, and humanitarian health partners providing
health services to UMNs through static or mobile units as shown in table 1.
Table1: Estimated Population and Health Service Providers by upazila, Cox’s Bazar, Bangladesh, 2017.
Ukhia Teknaf
Camp/Settlement Provider Population Camp/Settlement Provider Population
Hakimpara BDRCS 52,204 Ali Akbar Prara IOM 6,500
Jamtoli/ /Thangkhali IHA, MSF 27,459 Leda Make Shift IOM 26,015
Kutupalong Registered Camp
UNHCR, MSF, IOM
33,900 Rangikhali IOM 7,500
Kutupalong, Balukhali Expansion
IOM, MSF 300,460 Shamlapur Settlement IOM 35,756
Baggoha/Potibonia MSF 20,792 Nayapara Registered Camp
UNHCR 34,230
Ukhia Health Complex
IOM, MOHFW
39,559 Roikhong / Unchiprang MSF 28,494
TOTAL 474,374 Teknaf Health Complex MOHWF 71,607
TOTAL 210,102 IHA=Indonesia Humanitarian Alliance, BDRCS: Bangladesh Red Crescent Society, MOHWF: Ministry of Health and Family
Welfare.
1 https://reliefweb.int/report/bangladesh/bangladesh-situation-update-rohingya-refugee-crisis-cox-s-bazar-10-oct-2017;

MMWB Morbidity and Mortality Weekly Bulletin, Cox’s Bazar, Bangladesh 15 October 2017 / Vol. 1
4
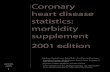
2. Proportion of primary causes for cases and deaths
During the period of 25 August-10 October 2017, a total of 38,209 consultations under surveillance were
reported through the EWARS system of which 32% (12,165) were due to ARI, 10% (3,876) due to AWD,
7% (2,585) due to SKN, 6% (2,272) due to unexplained fever (UNFEV), 4% (1,460) INJ, 2% BD, the rest
40% from other disease including severe malnutrition, eye infection, suspected measles/rubella,
jaundice, and malaria.
During the same period, there were 71 reported deaths, 41% due to ARI, 8% injury, 7% AWD, 7%
neonatal tetanus, 4% cardio vascular disease, 3% suspected malaria, 3% meningitis like disease, and 7%
unknown causes. The rest of the deaths were due to other causes and reported under the category
“Others”. The proportion of primary causes for the reported cases and related deaths is shown in
Figure2.
Figure 2: Proportion of primary causes for all reported cases and deaths, Cox’s Bazaar, Bangladesh, 25 August -10 October 2017.
(ARI: Acute Respiratory Tract Infection, AWD: Acute Water Diarrhoea, BD: Bloody Diarrohea, CVD: Cardio Vascular Disease, INJ:
Injuries, MEN: Meningitis like Disease, MAL: Malaria, NNT: Neonatal Diseases, OTH: Other diseases, SKN: Skin Disease, UNFEV:
Fever of unexplained origin and UNK: Unknown Causes).
For under-5 year age group, a total number of 14,015 cases of health events were reported through
EWARS constituting 37% of the total consultations. 39% (5,461) of these cases were attributed to ARI
while 16% (2,190) were due to AWD. There were 29 reported deaths in the children under-5
representing 41% of total deaths reported from Cox’s Bazar. Of these figures, 59% (17 deaths) were ARI-
related, 17% (5 deaths) were due to neonatal diseases and 10% (3 deaths) due to AWD. The proportion
of primary causes for the reported cases and deaths for the children under-5 year is shown in Figure 3.
Cases (n=38,209) Deaths (n=71)

MMWB Morbidity and Mortality Weekly Bulletin, Cox’s Bazar, Bangladesh 15 October 2017 / Vol. 1
5
Figure 3: Proportion of primary causes for the reported cases and deaths in the under-5 year age group, Cox;s Bazar, Bangladesh, 25 August -10 October 2017.
For the over-5 year age group, a total number of 24,194 cases of health events were reported through
EWARS constituting 63% of the total number of consultations. 28% (6,704) of these cases were
attributed to ARI and 7% (1,686) to AWD. There were 42 reported deaths in this age group, representing
59% of total deaths reported from Cox’s Bazar. Of these, 29% (12 deaths) were due to ARI, 4% to injury,
10% to AWD and 5% to CVD. The proportion of primary causes for the reported cases and deaths for the
children under-5 year is shown in Figure 4.
Figure 4: Proportion of primary causes for the reported cases and deaths in the Over 5 year age group, Cox;s Bazar, Bangladesh,
25 August -10 October 2017.
3. Measles cases
Between 10 and 25 September 2017, a total of 22 suspected measles cases were reported from Cox’s
Bazar district: 55% (12/22) from Ukhia, 41% (9/12) from Teknaf and 4% (1/22) from Ramu upazila. No
cases were reported from Bandarban district. Case investigations were conducted for all suspected
cases and samples collected for laboratory confirmation. Laboratory results showed that 64% (14/22)
were positive for measles specific IgM, 18% (4/22) were negative for measles specific IgM and 18%
(4/22) are still pending the laboratory results. From all confirmed cases, 93% (13/14) were among UMNs
while one confirmed case was reported from the host community in Teknaf upazila.
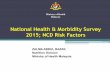
3.1 Measles vaccination campaign in Cox’s Bazar
Measles vaccination is one of the most recommended priority health interventions during emergencies.
In 2016, a total of 945 confirmed measles cases were reported from Bangladesh, and Cox’s Bazar
reported the highest attack rate in the country (>120/100,000 population). Measles incidence rate by
district in Bangladesh (2016) is shown in the Figure 5.

MMWB Morbidity and Mortality Weekly Bulletin, Cox’s Bazar, Bangladesh 15 October 2017 / Vol. 1
6
A recent (2017) needs assessment carried out by
WHO showed that measles vaccination coverage in
Cox’s Bazar was below 90%, which may explain
several reported outbreaks over the last few years.
On 16 September 2017, a mass measles vaccination
campaign was carried out in Cox’s Bazar for 14 days.
Activities included vaccination using a combination
of fixed posts and outreach immunization teams,
the use of checklists to monitor vaccination
sessions, social mobilization activities, and
surveillance for adverse events following
immunization. The campaign targeted 122,580
children <15 years old in the 2 upazilas of Cox’s
Bazar (Tekaf, Ukhia) and Naikhongchhari upazila in
Bandarban district. The total number of vaccinated
children is shown in table 2.
The Civil Surgeon’s Office in Cox’s Bazar was
responsible for planning, monitoring, coordinating
and implementing the campaign activities. The role
of the staff in the Control Room was to monitor
preparedness on a day-to-day basis, especially
mobilization of human and other resources like transport, inter-sectoral coordination and full utilization
of resources. In addition, the Control Room staff was providing regular updates on progress and
obstacles in implementing the campaign to the central level. The campaign faced several challenges,
including difficulty to correctly estimate the target population due to the continuing influx of UMNs into
the camps; heavy rains rendered most of the settlements inaccessible, forcing the vaccination teams to
turn around and return to the sites later.
Table2: Number of vaccinated children, Special Vaccination Campaign, 16 September –to 3 October 2017.
District Upazila Estimated Target Total Vaccinated/Vaccine Type
0-59 M 6M to <15 Y bOPV
(0-59 M) MR
(6 M to <15 Y) VIT A
Cox's Bazar Teknaf 14,450 29,410 20,826 36,116 21,265
Cox's Bazar Ukhia 28,800 84,000 48,713 93,634 47,676
Bandarban Naikhongchhari 3,915 9,170 2,795 5,769 3,123
TOTAL 47,165 122,580 72,334 135,519 72,064
Figure 5: Measles attack rate per district, Bangladesh, 2016

MMWB Morbidity and Mortality Weekly Bulletin, Cox’s Bazar, Bangladesh 15 October 2017 / Vol. 1
7
4. Acute respiratory infection
Between 25 August and 10 October 2017 (epidemiological weeks 34-41) , a total of 12,165 ARI cases
including 29 related deaths (CFR 0.24%) were reported from Cox’s Bazar district: of these 45%
(5,461/12,165) were under 5 years old. The peak in epidemiological week 39 was due to the increase in
the number of reporting units participating in EWRAS. The weekly distribution of ARI cases is shown in
Figure 5.
Figure 5: Weekly distribution of reported ARI cases by age groups, Cox’s Bazar, Bangladesh, 25 August –to 10 October 2017.
Teknaf reported 76% (9,278/12,165) of the total reported ARI cases followed by Ukhia and Cox’s Bazar
with 23% and 1% respectively. The weekly distribution of ARI cases by district is shown in Figure 6.
Figure 6: Weekly distribution of reported ARI cases by district, Cox’s Bazar, Bangladesh, 25 August –to 10 October 2017.

MMWB Morbidity and Mortality Weekly Bulletin, Cox’s Bazar, Bangladesh 15 October 2017 / Vol. 1
8
5. Acute watery diarrhoea
Between 25 August and 10 October 2017 (epidemiological weeks 34-41), a total of 3,876 AWD cases
including 10 related deaths (CFR 0.25%) were reported from Cox’s Bazar district: of these 57%
(2,190/3,876) were under 5 years old. The weekly distribution of AWD cases by age group is shown in
Figure 7.
Figure 7: Weekly distribution of reported AWD Cases by age groups, Cox’s Bazar, Bangladesh, 25 August -10 October 2017.
Ukhia reported 71% (2,736/3,876) of total reported AWD cases followed by Teknaf and Cox’s Bazar with
27% and 1% respectively. The weekly distribution of AWD cases by district is shown in Figure 8.
Figure 8: Weekly distribution of reported ARI cases by district, Cox’s Bazar, Bangladesh, 25 August –to 10 October 2017.

MMWB Morbidity and Mortality Weekly Bulletin, Cox’s Bazar, Bangladesh 15 October 2017 / Vol. 1
9
5.1 Drinking water testing results
Between 18 September and 5 October 2017, a total of 112 water samples from different water sources
were collected from the Cox’s Bazar UMNs settlements. Using membrane filtration technique, only 23%
(37/112) of the samples were found negative for E. Coli, meeting the Bangladesh Standard and WHO
guideline value (0 cfu/100ml). The remaining 77% (86/112) tested positive for faecal contamination (E.
Coli); 40% (34/86) of all the positive samples were very highly contaminated (>100 cfu/100ml), 17%
(15/86) highly contaminated (>50 and <100 cfu/100ml) and intermediate contamination (<50
cfu/100ml) was found in 43% (37/86).
Out of all contaminated samples, 59% (51/86) were collected from water stored at household level, and
35% (30/86) from tube-wells, the remaining 5% were collected from other sources. . No contamination
was found in any of the tested supply reservoirs. Location-wise, the highest contamination level was
detected in Kutupalong settlement (33/86).
In addition to contamination at a source, the reasons for such high level of water contamination at
household level seem to be poor hygiene practices. Only 2% of surveyed households reported using
soap for handwashing after defecation and for washing water containers between refills. Often
containers are not covered, and other safe water handling practices not maintained.
Table 3: Contaminated Samples by Settlement and Water Source, Cox’s Bazar, Bangladesh, 2017 Camp/Settlement
Name Household
Supply Reservoir
Surface Water
Water Tank
Tube Well Other Total
Balukhali 4 0 1 0 6 0 11
Hakim Para 9 0 0 0 5 0 14
Jamtali 4 0 0 0 1 0 5
Kutupalong 23 0 0 0 10 0 33
Kutupalong Hindu 4 0 0 0 2 0 6
Moinnerghona 1 0 0 0 2 0 3
Sapmarajhuri 5 0 0 0 0 0 5
Shamlapur 0 0 0 0 2 0 2
Tajanirmarkhola 0 0 0 0 1 0 1
Unchiprang 1 0 1 1 0 0 3
Other 0 0 0 1 1 1 3
TOTAL 51 0 2 2 30 1 86
To reduce the high level of microbiological contamination of water at household level and associated
public health risk the following measures should be considered: installation of tube-wells at deep
aquifer; treatment and chlorination of surface water; removal of latrines installed adjacent (within 10
meter) to the water points; boiling water or disinfecting drinking water by aluminium or halogen tablets;
elimination of open defecation practice and ensuring improved sanitation facilities; hygiene awareness
campaign for preventing water contamination and recontamination; ensuring proper excreta
management including disposal of sludge; and constant surveillance of the water supply systems,
including regular water testing to monitor the risks and plan appropriate measures.

More partners will be added upon
participation
Morbidity (disease) and Mortality (death) Daily Reporting Surveillance Form (V-2.0)
Date: / / 2017 Latitude: Longitude:
District: Upazila: Union:
Health Facility/Camp:
Estimated Population: Population <5 years:
Agency/NGOs:
Name of contact person:
Phone: Email:
Events Under Surveillance Cases < 5 yrs Cases >=5 yrs Deaths < 5 yrs Deaths >=5 yrs
M F M F M F M F
Acute Water Diarrhoea
Bloody Diarrhoea
Other Diarrhoea
Acute Respiratory Infection
Suspected Measles/Rubella
Acute Flaccid Paralysis (AFP)
Suspected Meningitis
Acute Jaundice Syndrome
Suspected Hemorrhagic Fever
Neonatal Tetanus
Adult Tetanus
Suspected Malaria
Confirmed Malaria
Unexplained Fever > 101F/38.5C
Severe Malnutrition
Skin Diseases
Eye Infection
Injuries/Wounds
Others
- Please indicate ONLY those cases examined/admitted during the reporting week. Each case should be counted once only.
- Write Zero if you have no cases or death of one of the health events listed in the form.
- Deaths should be included in the mortality section, please fill the following table for each reported death:
No Name Age Sex Cause Location
1
2
3
4
5 A
Related Documents