i The Role of Resistance Exercise in the Treatment of Co- morbid Insulin Resistance and Depressive Symptoms Alexander K. Bate, B.Ex&Sp.Sc, Grad. Dip. Ex Phys Thesis submitted in fulfilment of the requirements for the degree of Master of Applied Science (Research) Faculty of Medicine and Health The University of Sydney 2022

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
i
The Role of Resistance Exercise in the Treatment of Co-
morbid Insulin Resistance and Depressive Symptoms
Alexander K. Bate, B.Ex&Sp.Sc, Grad. Dip. Ex Phys
Thesis submitted in fulfilment of the requirements for the degree of
Master of Applied Science (Research)
Faculty of Medicine and Health
The University of Sydney
2022
ii
Supervisor statement
This is to certify that the thesis entitled “The Role of Resistance Exercise in the
Treatment of Co-morbid Insulin Resistance and Depressive Symptoms”
submitted by Alexander K. Bate in fulfilment of the requirements for the degree of
Master of Applied Science (Research) is in a form ready for examination.
_________________________________
Doctor Yorgi Mavros
Discipline of Exercise & Sport Science
Faculty of Medicine and Health
The University of Sydney
_________________________________
Professor Maria Fiatarone Singh
Discipline of Exercise & Sport Science
Faculty of Medicine and Health
The University of Sydney
________________________________
Doctor Trinidad Valenzuela
Discipline of Exercise & Sport Science
Faculty of Medicine and Health
The University of Sydney

iii
Student declaration
I, Alexander Bate, hereby declare that the work contained within this thesis is my
own and has not been submitted to any other university or institution as a part or a
whole requirement for any higher degree.
In addition, ethical approval from the University of Sydney Human Ethics Committee
was granted for the study presented in this thesis. Participants were required to read
a participant information document and informed consent was gained prior to data
collection.
Name_Alexander K. Bate_
Signed ________________
Date _ 27th April 2022

iv
Acknowledgements
I would like to extend my sincere thanks and appreciation to my supervisors, Dr.
Yorgi Mavros, Professor Maria Fiatarone Singh, and Dr. Trinidad Valenzuela for their
invaluable assistance and guidance. I’d like to thank my partner, Dr. Katharine Kott,
for inspiring me to accept this challenge and supporting me all the way through the
process. I’d also like to thank my parents who offered their financial support when
needed throughout all my university years.
Finally, I’d like to thank the participants of the PRT Medic study for volunteering so
much of their time and effort towards furthering our understanding of the role of
exercise in the treatment of chronic disease. The study could not have happened
without their generosity.

v
Table of contents
Title page _________________________________________________________________ i
Supervisor statement ________________________________________________________ ii
Student declaration ________________________________________________________ iii
Acknowledgements ________________________________________________________ iv
Table of contents ___________________________________________________________ v
Thesis abstract _____________________________________________________________ 1
CHAPTER 1: Introduction _____________________________________________________ 3
Type 2 diabetes and major depressive disorder in Australia _____________________________ 4
Insulin resistance and the pathophysiology of metabolic syndrome and type 2 diabetes ______ 5
Interaction between major depressive disorder and insulin resistance ____________________ 7
Management of individuals with insulin resistance and major depressive disorder _________ 11
Objectives ____________________________________________________________________ 15
References ___________________________________________________________________ 17
CHAPTER 2: The effect of resistance exercise on depressive symptoms in adults with insulin
resistance: A systematic review of randomised controlled trials _____________________ 32
Abstract _____________________________________________________________________ 33
Introduction __________________________________________________________________ 36
Methods _____________________________________________________________________ 41
Search Strategy _______________________________________________________________________ 41
vi
Deviations from Registered Protocol ______________________________________________________ 42
Eligibility Criteria ______________________________________________________________________ 42
Assessment of Exercise Reporting Standards ________________________________________________ 46
Risk of Bias Assessment _________________________________________________________________ 47
Data Extraction _______________________________________________________________________ 47
Data Synthesis and Analysis _____________________________________________________________ 48
Results ______________________________________________________________________ 51
Assessment of Exercise Reporting Standards ________________________________________________ 52
Risk of Bias Assessment _________________________________________________________________ 53
Cohort Characteristics __________________________________________________________________ 54
Intervention and Comparator Characteristics _______________________________________________ 56
Depressive Symptoms __________________________________________________________________ 60
Glucose Metabolism ___________________________________________________________________ 64
Other Cardiometabolic Variables _________________________________________________________ 66
Adverse Events _______________________________________________________________________ 68
Discussion ____________________________________________________________________ 70
References ___________________________________________________________________ 78
Tables ______________________________________________________________________ 101
Table 1: Search strategy _______________________________________________________________ 101
Table 2: Intervention and control characteristics of included studies ___________________________ 104
Table 3: Consensus on Exercise Reporting Template (CERT) scoring ____________________________ 105
Table 4: Cohort characteristics for included studies _________________________________________ 106
Table 5: Chronic disease and medication use status of included cohorts _________________________ 107
Table 6: Intervention exercise prescription ________________________________________________ 108
Table 7: Intervention, comparator, and co-intervention details ________________________________ 109
Table 8: Depression outcomes for included studies _________________________________________ 110
Table 9: HbA1c outcomes for included studies _____________________________________________ 111
vii
Table 10: Lipids outcomes where reported for included studies _______________________________ 112
Table 11: Reported adverse events for included studies ______________________________________ 113
Figures _____________________________________________________________________ 114
Figure 1: PRISMA flow diagram of study selection___________________________________________ 114
Figure 2. Consensus on Exercise Reporting total scoring _____________________________________ 115
Figure 3. Risk of Bias assessment using intention-to-treat analysis _____________________________ 116
Figure 4. Depression outcomes by study design and exercise intensity __________________________ 117
Figure 5. Depression outcomes by study design and exercise exposure _________________________ 118
Figure 6. HbA1c outcomes by study design and exercise intensity ______________________________ 119
Figure 7. HbA1c outcomes by study design and exercise exposure _____________________________ 120
CHAPTER 3: The Progressive Resistance Training in Metabolic syndrome and Depression
Integrative Care (PRT MEDIC) trial: A randomised controlled trial.__________________ 121
Abstract ____________________________________________________________________ 122
Introduction _________________________________________________________________ 124
Methods ____________________________________________________________________ 129
Trial Design _________________________________________________________________________ 129
Participants _________________________________________________________________________ 129
Pre-screening ________________________________________________________________________ 131
Participant flow through study __________________________________________________________ 132
Blinding ____________________________________________________________________________ 133
Primary outcome measures ____________________________________________________________ 134
Secondary Outcome Measures __________________________________________________________ 135
Randomisation _______________________________________________________________________ 143
Monitoring __________________________________________________________________________ 143
Data management ____________________________________________________________________ 144
Interventions ________________________________________________________________________ 144
Sample Size _________________________________________________________________________ 147
viii
Impact of COVID-19 ___________________________________________________________________ 147
Data analysis ________________________________________________________________________ 148
Results _____________________________________________________________________ 150
Adherence __________________________________________________________________________ 151
Psychological outcomes _______________________________________________________________ 151
Metabolic outcomes __________________________________________________________________ 153
Body composition ____________________________________________________________________ 153
Blood pressure _______________________________________________________________________ 153
Inflammation ________________________________________________________________________ 154
Regression analyses ___________________________________________________________________ 154
Adverse events ______________________________________________________________________ 155
Discussion ___________________________________________________________________ 156
References __________________________________________________________________ 161
Tables ______________________________________________________________________ 173
Table 1. Eligibility criteria ______________________________________________________________ 173
Table 2. Pilot data from GREAT2DO and Previous depression studies ___________________________ 174
Table 3. Baseline participant characteristics _______________________________________________ 175
Table 4. 12-week outcome data _________________________________________________________ 176
Table 5. Linear regression of primary outcomes ____________________________________________ 177
Figures _____________________________________________________________________ 178
Figure 1. Eligibility pre-screening flowchart ________________________________________________ 178
Figure 2: Assessment flowchart _________________________________________________________ 179
Figure 3. CONSORT flowchart of participant enrolment ______________________________________ 180
Figure 4. Hamilton Rating Scale for Depression before and after the 12-week intervention _________ 181
Figure 5. Homeostatic model of assessment before and after the 12-week intervention ____________ 182
Figure 6. Patient Health Questionnaire-9 before and after the 12-week intervention ______________ 183
Figure 7. CES-D scale before and after the 12-week intervention_______________________________ 184
ix
Figure 8. CES-D scale throughout intervention _____________________________________________ 185
Figure 9. Oxford happiness scale before and after the 12-week intervention _____________________ 186
Figure 10. Fasting glucose before and after the 12-week intervention __________________________ 187
Figure 11. 2-hour glucose before and after the 12-week intervention ___________________________ 188
Figure 12. Oral glucose tolerance test before and after the 12-week intervention _________________ 189
Figure 13. Glucose area under the curve before and after the 12-week intervention _______________ 190
Figure 14. Change in HOMA2-IR and change in HAM-D ______________________________________ 191
Figure 15. Change in HOMA2-IR and change in PHQ-9 _______________________________________ 192
Figure 16. Change in HOMA2-IR and change in CES-D ________________________________________ 193
Figure 17. Change in fasting glucose and change in HAM-D ___________________________________ 194
Figure 18. Change in fasting glucose and change in PHQ-9 ____________________________________ 195
Figure 19. Change in fasting glucose and change in CES-D ____________________________________ 196
Figure 20. Change in 2-hour glucose and change in HAM-D ___________________________________ 197
Figure 21. Change in 2-hour glucose and change in PHQ-9 ____________________________________ 198
Figure 22. Change in 2-hour glucose and change in CES-D ____________________________________ 199
Figure 23. Change in oral glucose tolerance test AUC and change in HAM-D _____________________ 200
Figure 24. Change in oral glucose tolerance test AUC and change in PHQ-9 ______________________ 201
Figure 25. Change in oral glucose tolerance test AUC and change in CES-D _______________________ 202
CHAPTER 4: Discussion and Conclusions _______________________________________ 203
Discussion ___________________________________________________________________ 204
Limitations __________________________________________________________________ 206
Future directions _____________________________________________________________ 209
Conclusion __________________________________________________________________ 211
References __________________________________________________________________ 213
Bibliography _____________________________________________________________ 216
Appendices ______________________________________________________________ 252

x
Appendix 1. Prospero registration for systematic review _____________________________ 252
Appendix 2. ANZCTR registration for PRT Medic study _______________________________ 263
Appendix 3. HREC approval for PRT Medic study ____________________________________ 268

1
Thesis abstract
Insulin resistance (IR) and major depressive disorder (MDD) share common
pathophysiology, and when clustered together, increase the risk of type-2 diabetes.
Exercise has been shown to effectively manage both IR and MDD separately.
However, it is unknown to what extent exercise can simultaneously improve IR and
depressive symptoms, with the specific role of resistance training (RT) requiring
further investigation. To address this gap, a systematic review of the literature and a
randomised controlled trial were performed.
First, seven electronic databases were searched, with search terms for IR combined
with search terms for exercise. Seven randomised controlled trials reporting the
effects of RT on depressive symptoms in individuals with IR were identified. The
limited data available suggests RT may be an effective standalone intervention to
simultaneously reduce depressive symptoms and glycated haemoglobin (HbA1c).
However, the studies were of low quality, with no studies performed in adults with
MDD or using a clinician-rated assessment of depression.
Next, a 12-week randomised controlled trial of progressive RT in adults with
metabolic syndrome and MDD was conducted. Eleven participants were randomised
to receive high intensity RT (n=4) or usual care (n=7). Data were analysed with a
repeated measures ANOVA. No group x time interaction was observed for the
Hamilton Depression Rating Scale. However, a significant (p<0.05) group x time
reduction on the Patient Health Questionnaire-9 was observed favouring RT. There
were no changes in IR or HbA1c.
Overall, the existing literature on the effects of RT on simultaneously improving IR
and depressive symptoms was small and of low quality. While our randomised
2
controlled trial attempted to address this gap in the literature, the small sample size
meant the study was underpowered. Nevertheless, a significant reduction in self-
rated symptoms was observed. Given the small sample size, future studies of RT are
warranted.

3
CHAPTER 1: Introduction
4
Type 2 diabetes and major depressive disorder in Australia
Type-2 diabetes (T2DM) and major depressive disorder (MDD) are amongst two of
the most common chronic diseases in Australia. The Australian Institute of Health
and Welfare reports a prevalence of T2DM in adults of 5.3%, with a peak prevalence
of 18.5% of males aged 75 years and over.1 In the most recent National Health
Survey, 4.1% of Australians reported having T2DM, with 10.4% of individuals
reporting depression or feelings of depression.2 Additionally, in 2018-19, 27.7 million
prescriptions were written for antidepressant medications, with average per person
spending on mental health related services increasing by 1.1% per year since 2013-
14.1 When considering burden of disease, MDD and T2DM are the 6th and 11th
leading cause of Disability-Adjusted Life Years (DALY), representing 2.9% and 2.3%
of all DALYs in Australia respectively.3 The economic costs associated with T2DM to
the healthcare system in Australia are considerable, with an estimated $10.6 billion
spent in both direct healthcare and government subsidies.4 Similarly, the economic
cost of depression, anxiety and substance use disorders was estimated at $12.8
billion, the majority of which ($11.8 billion) come from lost productivity.5 Thus, there
is an urgent need for therapeutic strategies for the prevention, management and
treatment of these two leading causes of morbidity in Australia.

5
Insulin resistance and the pathophysiology of metabolic syndrome
and type 2 diabetes
Insulin resistance is an impaired biological response to insulin, primarily in the liver,
skeletal muscle, and adipose tissue. Insulin resistance encompasses a spectrum of
chronic conditions, which in totality make up 4.7% of the total disease burden in the
Australian healthcare system.6 The primary characteristic of insulin resistance is a
dysregulation of glucose metabolism, with reduced suppression of glucose output
from the liver, combined with impaired glucose uptake in peripheral tissues such as
skeletal muscle. In the early stages of insulin resistance, compensatory
hyperinsulinaemia occurs to maintain glucose homoeostasis. When compensatory
hyperinsulinaemia is no longer sufficient, blood glucose may become chronically
elevated in both fasted (impaired fasting glucose) and/or post-prandial states
(impaired glucose tolerance), otherwise known as ‘pre-diabetes’, which is estimated
to affect nearly 1 in 6 adults, or over 2 million Australians.7
Risk of developing insulin resistance is determined by modifiable and non-modifiable
risk factors. Modifiable contributors to insulin resistance and risk factors for T2DM
include physical inactivity,8 dietary choices,9 alcohol consumption,10 and smoking.11
For non-modifiable factors, risk has been observed to vary by ethnic group, with
higher odds of having T2DM when compared with White populations observed in
Asian (odds ratio (OR) 2.36, 95% confidence intervals (CI) 2.26 to 2.47), Black (OR
1.65, 95% CI 1.56 to 1.73), and Mixed/Other ethnic groups (OR 1.17, 95% CI 1.08 to
1.27), after adjustment for age, sex, and social deprivation.12 Sex is another non-
6
modifiable risk factor, with greater visceral adipose tissue combined with lower
endogenous estrogen levels in males being proposed as an explanation for greater
insulin resistance when compared with premenopausal women.13 Finally, increasing
age is a commonly cited risk factor for T2DM,14-16 with a possible explanatory
mechanism being the association of insulin resistance with age-related loss of
muscle mass, known as sarcopenia.17 18
Chronic insulin resistance is associated with a number of risk factors for
cardiometabolic disease; primarily abdominal or visceral obesity, hypertension, and
dyslipidaemia, all of which are essential criteria for metabolic syndrome.19 20 If left
unmanaged, individuals with prediabetes or metabolic syndrome are four-to-twelve21
and four-to-five22 times more likely to develop T2DM than their healthy counterparts.
Thus, early identification and treatment of insulin resistance and metabolic syndrome
is essential in the prevention of T2DM. However, for individuals who do develop
T2DM, appropriate management of insulin resistance and blood glucose is essential
to minimise the risk of complications including cardiovascular disease,23 stroke,23
retinopathy,24 neuropathy,25 kidney disease,26 and peripheral vascular disease,27 as
well as cognitive decline and dementia.28 29 Therefore, early recognition and
appropriate management of insulin resistance is important to reduce the risk of future
complications and premature mortality. Additionally, slowing or preventing disease
progression requires not only management of insulin resistance itself, but also
identifying and managing risk factors that may be associated with the onset and
progression of insulin resistance, including obesity, insufficient physical activity,
hypertension, smoking, and excess alcohol, for example.
7
Interaction between major depressive disorder and insulin
resistance
In addition to the risk factors noted above, psychological conditions are known to be
associated with insulin resistance and T2DM, in particular depressive disorders and
schizophrenia (even in the absence of psychotropic medications), suggesting
underlying shared pathophysiology or genetic susceptibility. Depressive disorders
are of particular importance in this regard.
Major depressive disorder is a mood disorder that is characterised by persistent
feelings of sadness and a loss of interest or pleasure. To be diagnosed with MDD,
the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5 (R))30
outlines the following diagnostic criteria:
A. Five (or more) of the following symptoms have been present during the same
two-week period and represent a change from previous functioning: at least
one of the symptoms is either (1) depressed mood or (2) loss of interest or
pleasure.
Note: Do not include symptoms that are clearly attributable to another
medical condition.
1. Depressed mood most of the day, nearly every day, as indicated by
either subjective report (e.g., feels sad, empty, hopeless) or
observation made by others (e.g., appears tearful). (Note: In children
and adolescents, can be irritable mood).
8
2. Markedly diminished interest or pleasure in all, or almost all,
activities most of the day, nearly every day (as indicated by either
subjective account or observation).
3. Significant weight loss when not dieting or weight gain (e.g., a
change of more than 5% of body weight in a month), or decrease or
increase in appetite nearly every day. (Note: In children, consider
failure to make expected weight gain.)
4. Insomnia or hypersomnia nearly every day.
5. Psychomotor agitation or retardation nearly every day (observable
by others, not merely subjective feelings of restlessness or being
slowed down).
6. Fatigue or loss of energy nearly every day.
7. Feelings of worthlessness or excessive or inappropriate guilt (which
may be delusional) nearly every day (not merely self-reproach or guilt
about being sick).
8. Diminished ability to think or concentrate, or indecisiveness, nearly
every day (either by subjective account or as observed by others).
9. Recurrent thoughts of death (not just fear of dying), recurrent
suicidal ideation without a specific plan, or a suicide attempt or a
specific plan for committing suicide.
B. The symptoms cause clinically significant distress or impairment in social,
occupational, or other important areas of functioning.
9
C. The episode is not attributable to the physiological effects of a substance or to
another medical condition.
Note: Criteria A-C represent a major depressive episode.
Note: Responses to a significant loss (e.g., bereavement, financial ruin,
losses from a natural disaster, a serious medical illness or disability) may
include the feelings of intense sadness, rumination about the loss, insomnia,
poor appetite, and weight loss noted in Criterion A, which may resemble a
depressive episode. Although such symptoms may be understandable or
considered appropriate to the loss, the presence of a major depressive
episode in addition to the normal response to a significant loss should also be
carefully considered. This decision inevitably requires the exercise of clinical
judgment based on the individual’s history and the cultural norms for the
expression of distress in the context of loss.
D. The occurrence of the major depressive episode is not better explained by
schizoaffective disorder, schizophrenia, schizophreniform disorder, delusional
disorder, or other specified and unspecified schizophrenia spectrum and other
psychotic disorders.
E. There has never been a manic episode or a hypomanic episode.
Note: This exclusion does not apply if all of the manic-like or hypomanic-like
episodes are substance-induced or are attributable to the physiological effects
of another medical condition.
The World Health Organization estimated a global mean prevalence for depressive
disorders of 4.4% in 2015, ranking them as the single greatest contributor to non-

10
fatal health loss (7.5% of all Years Lived with Disability),31 and the third overall cause
of disease burden worldwide.32
Major depressive disorder and insulin resistance are often comorbid, with increasing
prevalence of MDD seen with worsening insulin resistance. The AusDiab study, for
example, reported a prevalence of depression 20% higher in individuals with
impaired glucose tolerance or impaired fasting glucose, 31% higher in individuals
with metabolic syndrome, and 65% higher in individuals with T2DM, as compared
with metabolically healthy individuals.33 Data suggest that insulin resistance
increases the risk of developing MDD, with individuals that have metabolic syndrome
being over two-times more likely to develop MDD over 10 years than healthy
individuals.34 Similarly, individuals with T2DM have been found to be 15%35 to 33%36
more likely to develop incident MDD, with some estimates projecting over 9 million
cases of depression worldwide being potentially attributable to T2DM.36 Conversely,
MDD is also independently associated with progression of insulin resistance, as
individuals with depressive symptoms or MDD are 52% more likely to develop
metabolic syndrome,37 and have a 37% increased risk of developing T2DM.38
Collectively, these data suggest a bi-directional relationship between depression and
insulin resistance, which may be explained by shared biological pathways, including
brain-derived neurotrophic factor (BDNF),39-41 hypothalamic-pituitary-adrenal (HPA)
axis,42 43 and systemic inflammation.44 45 These shared pathways may result in a
significantly increased risk of disease progression for dually-afflicted individuals. In a
prospective study, the co-existence of depressive symptoms and metabolic
11
syndrome increased the risk of developing T2DM 6.6-fold within 4.5 years compared
to healthy individuals.46 Interestingly, a synergistic effect was found between the
two, suggesting that the combined effect of metabolic syndrome and depressive
symptoms was greater than the sum of the simple effects. Thus, individuals with
insulin resistance (including metabolic syndrome and T2DM) and MDD represent a
high-risk cohort who require early and effective intervention to reduce the risk of
disease progression and the development of associated complications and co-
morbidities.
Management of individuals with insulin resistance and major
depressive disorder
Pharmacological management of insulin resistance and MDD simultaneously would
require multiple treatments. Insulin resistance may be managed with one or more
oral hypoglycaemics such as biguanides (Metformin), thiazolidinediones, and insulin
secretagogues, or the use of exogenous insulin.47 Common anti-depressant drugs
include selective serotonin reuptake inhibitors, serotonin–norepinephrine reuptake
inhibitors, and tricyclic antidepressants.48 In the case of metabolic syndrome where
hypertension and dyslipidaemia are present, drugs such as statins, angiotensin
converting enzyme (ACE)-inhibitors, calcium-channel blockers, or diuretics may also
be added to the pharmacological regimen.49 Considering this, it is not surprising that
individuals with T2DM have a much higher likelihood of polypharmacy compared
with those without diabetes, with one cross-sectional study of individuals aged over
50 years finding 51.6% of individuals with T2DM reporting polypharmacy, compared
12
to 21.4% of individuals without T2DM.50 Polypharmacy is similarly applicable to
cohorts with MDD, as patients in a cross-sectional study were nearly three times
more likely to be using five or more chronic prescription drugs simultaneously
compared to individuals without any mental illness, and this finding remained even
when antidepressant medications were excluded.51
In addition to increasing the financial cost, such polypharmacy also increases risk of
drug interactions and adverse effects. Some adverse effects commonly associated
with antidepressants include fatigue, dry mouth, gastrointestinal disturbance, sleep
disturbance, blood pressure dysregulation, sweating, and dizziness,52 53 while
metabolic medications have been associated with mild but typical side effects such
as myalgia,54 dizziness,55 headache,55 56 and gastrointestinal distress.56 Finally, there
also exists potential for unnecessary drug prescription if therapy is duplicated across
multiple specialists or adverse drug events are misinterpreted as new medical
conditions, e.g. sleep disturbance could be mischaracterised as its own condition
and treated with additional drugs, each with their own set of side effects, which for
some may potentially even include depression.57 These data highlight the need for
effective non-pharmacological approaches for concomitant management of insulin
resistance and depression, along with common co-existing comorbidities such as
hypertension and obesity.
Lifestyle interventions have been found to improve insulin resistance and glycaemic
control, with repeated exercise bouts improving glucose uptake into skeletal muscle
by increasing glucose transporter GLUT4 expression at the cell membrane in

13
response to insulin.58 59 This effect extends to patients with T2DM60 and has been
demonstrated using resistance training,61 high-intensity interval training,62 and
aerobic exercise.63 64 In large scale randomised controlled trials (RCT) such as the
Da Qing IGT and Diabetes Study, the US Diabetes Prevention Program, and the
Finnish Diabetes Prevention Study , exercise has been shown reduce the risk of
developing type 2 diabetes by 46% when used as a sole intervention65 and by 58%
when combined with a dietary intervention.66 67 Additionally, in the US Diabetes
Prevention Program the lifestyle intervention was even significantly superior to the
drug arm, with the risk of T2DM 27% lower when compared to metformin.67 These
large-scale trials clearly indicate the effectiveness of non-pharmaceutical
interventions in preventing T2DM in those at increased risk.
For those adults who have already developed T2DM, exercise interventions
including aerobic and resistance exercise in isolation or combination have similarly
been shown to improve insulin resistance and glucose homeostasis.68-70 The latest
recommendations from the American College of Sports Medicine for this cohort are
to engage aerobic exercise 3-7 days/week, for a total of 150-300 min/week of
moderate intensity (40-59% heart rate reserve) or 75-150 min/week of vigorous
intensity (60%-89% heart rate reserve) activity, or an equivalent combination
thereof.71 Additionally, it is recommended that resistance training (RT) be engaged in
2-3 days/week, at a moderate (50-69% of 1-repetition maximum [1RM]) or vigorous
(70-85% 1RM) intensity, for 10-15 repetitions per set of 1-3 sets per exercise.
Exercise programs following these guidelines have been shown to improve insulin
resistance and glucose homeostasis. There are many, complex mechanisms
underlying improvements in insulin resistance following exercise, however the

14
primary change that is observed is an improvement in intracellular signalling
following the binding of insulin to the receptor on the cell surface.63 64 Following
adaptation to chronic exercise, for a given insulin concentration, a greater number of
glucose transporter 4 (GLUT4) molecules are stimulated to translocate to the cell
membrane to facilitate the transfer of glucose from the bloodstream into the muscle
cell.58 Overall, these guidelines aim to maximise potential exercise effects for
individuals with T2DM such as improved fitness, improved insulin sensitivity,
reductions in HbA1c of 0.5%-0.7%, reduced frequency of hyperglycaemic episodes,
and improved body composition.71
The therapeutic benefits of exercise also extend to the many cardiovascular risk
factors that commonly cluster with insulin resistance such as visceral adiposity,72
dyslipidaemia73 and hypertension,74 75 with the metabolic effects of exercise on blood
pressure comparable to anti-hypertensive medication.76 Similar to the benefits of
aerobic and resistance exercise in insulin resistance syndromes noted above, these
exercise modalities have also been shown to have potent anti-depressant effects,77-
80 with results comparable to those achieved by anti-depressant medication.81 For
example, RCTs comparing 16 weeks of aerobic exercise to 50-200 mg of sertraline
observed that exercise and sertraline groups had similar rates of remission of
depression by the end of the intervention,82 or that the exercise group had
significantly higher rates of remission.83 In addition, exercise has also been shown
to reduce depressive symptoms in patients with undiagnosed or sub-syndromal
depression and a comorbid chronic illness, including chronic pain, obesity,
neurological disorders, and chronic obstructive pulmonary disease.78 Thus, when
considered together, these data suggest that exercise is a single, targeted

15
intervention that can assist in the management of insulin resistance, MDD and other
associated co-morbidities such as hypertension, obesity, and dyslipidaemia.
To date, the majority of the literature has focused on the effects of aerobic exercise,
with far fewer studies focusing on other modalities of exercise. Resistance training is
an anabolic form of exercise that may be more accessible for some individuals
where aerobic modalities such as walking or cycling may be painful or difficult in
individuals with underlying conditions such as obesity,84 osteoarthritis,85 86 peripheral
neuropathy,87 or peripheral arterial disease.88 While less well studied than aerobic
exercise, strong evidence exists that RT can improve insulin resistance89 90 and
depressive symptoms,79 91 with evidence of a dose-response effect of intensity,
favouring higher intensity training for depression92 as well as metabolic outcomes.93
94 Therefore, RT presents as a novel yet potentially potent intervention for the
simultaneous management of both insulin resistance and depressive symptoms in
dually-afflicted individuals.
Objectives
In order to reduce morbidity, mortality, and healthcare costs associated with
comorbid insulin resistance and major depressive disorder, early, robust, and
targeted interventions are necessary. While a considerable body of literature exists
on exercise interventions for insulin resistance and depressive disorders
independently, a greater understanding is needed on how exercise, and in particular
resistance-based of exercise, is able to simultaneously improve these conditions.
16
Therefore, to investigate this gap, two studies were performed:
1. A systematic review the literature for the effect of resistance training in
managing symptoms of depression in individuals with insulin resistance in
randomised controlled trials, with primary outcomes being any measure of:
i. depressive symptoms;
ii. insulin resistance; or
iii. glucose metabolism.
2. A RCT of progressive resistance training (PRT) in adults with metabolic
syndrome and MDD to test the hypotheses:
i. 12 weeks of high intensity PRT in addition to usual care will
significantly improve clinician-rated, blindly assessed depressive
symptoms measure via Hamilton Depression Rating Scale.
ii. 12 weeks of high-intensity PRT in addition to usual care will
significantly reduce insulin resistance, as measured via
Homeostatic Model of Assessment-2 compared to controls referred
for usual care.
17
References
1. Australian Institute of Health and Welfare. Australia's health 2020: in brief.
Canberra: AIHW, 2020.
2. Australian Bureau of Statistics. National health survey: First results 2018
[Available from: https://www.abs.gov.au/statistics/health/health-conditions-
and-risks/national-health-survey-first-results/latest-release#data-download
accessed 1st December 2021.
3. Australian Institute of Health and Welfare. Australian burden of disease study:
Impact and causes of illness and death in Australia 2018. . Canberra: AIHW,
2021.
4. Lee CM, Colagiuri R, Magliano DJ, et al. The cost of diabetes in adults in
Australia. Diabetes Research and Clinical Practice 2013;99(3):385-90. doi:
https://doi.org/10.1016/j.diabres.2012.12.002 [published Online First:
2013/01/10]
5. Lee Y-C, Chatterton ML, Magnus A, et al. Cost of high prevalence mental
disorders: Findings from the 2007 Australian national survey of mental health
and wellbeing. Australian & New Zealand Journal of Psychiatry
2017;51(12):1198-211. doi: https://doi.org/10.1177/0004867417710730
6. Australian Institute of Health Welfare. Diabetes Canberra: AIHW; 2020 [Available
from: https://www.aihw.gov.au/reports/diabetes/diabetes accessed
24/04/2022.
7. Shaw J, Tanamas S. Diabetes: The silent pandemic and its impact on Australia.
Melbourne: Baker Health & Diabetes Institute, 2012.

18
8. Yaribeygi H, Maleki M, Sathyapalan T, et al. Pathophysiology of physical
inactivity-dependent insulin resistance: A theoretical mechanistic review
emphasizing clinical evidence. Journal of Diabetes Research
2021;2021:7796727-27. doi: https://doi.org/10.1155/2021/7796727
9. Adeva-Andany MM, Rañal-Muíño E, Vila-Altesor M, et al. Dietary habits contribute
to define the risk of type 2 diabetes in humans. Clinical Nutrition ESPEN
2019;34:8-17. doi: https://doi.org/10.1016/j.clnesp.2019.08.002
10. Cullmann M, Hilding A, Östenson CG. Alcohol consumption and risk of pre-
diabetes and type 2 diabetes development in a Swedish population. Diabetic
Medicine 2012;29(4):441-52. doi: https://doi.org/10.1111/j.1464-
5491.2011.03450.x [published Online First: 2011/09/16]
11. Artese A, Stamford BA, Moffatt RJ. Cigarette smoking: An accessory to the
development of insulin resistance. American Journal of Lifestyle Medicine
2017;13(6):602-05. doi: https://doi.org/10.1177/1559827617726516
12. Pham TM, Carpenter JR, Morris TP, et al. Ethnic differences in the prevalence of
type 2 diabetes diagnoses in the UK: Cross-sectional analysis of the health
improvement network primary care database. Clinical Epidemiology
2019;11:1081-88. doi: 10.2147/clep.S227621 [published Online First:
2020/02/06]
13. Geer EB, Shen W. Gender differences in insulin resistance, body composition,
and energy balance. Gender Medicine 2009;6 Suppl 1(Suppl 1):60-75. doi:
https://doi.org/10.1016/j.genm.2009.02.002
14. Ismail L, Materwala H, Al Kaabi J. Association of risk factors with type 2
diabetes: A systematic review. Computational and Structural Biotechnology
Journal 2021;19:1759-85. doi: https://doi.org/10.1016/j.csbj.2021.03.003
19
15. Choi BC, Shi F. Risk factors for diabetes mellitus by age and sex: Results of the
National Population Health Survey. Diabetologia 2001;44(10):1221-31. doi:
https://doi.org/10.1007/s001250100648 [published Online First: 2001/11/03]
16. Zafar J, Bhatti F, Akhtar N, et al. Prevalence and risk factors for diabetes mellitus
in a selected urban population of a city in Punjab. Journal Of Pakistan Medical
Association 2011;61(1):40-7. [published Online First: 2012/03/01]
17. Srikanthan P, Hevener AL, Karlamangla AS. Sarcopenia exacerbates obesity-
associated insulin resistance and dysglycemia: Findings from the National
Health and Nutrition Examination Survey III. PLoS One 2010;5(5):e10805.
doi: https://doi.org/10.1371/journal.pone.0010805 [published Online First:
2010/05/26]
18. Cleasby ME, Jamieson PM, Atherton PJ. Insulin resistance and sarcopenia:
Mechanistic links between common co-morbidities. Journal of Endocrinology
2016;229(2):R67-81. doi: https://doi.org/10.1530/joe-15-0533 [published
Online First: 2016/03/05]
19. Alberti KGMM, Zimmet P, Shaw J. Metabolic syndrome—a new world-wide
definition. A consensus statement from the International Diabetes Federation.
Diabetic Medicine 2006;23(5):469-80. doi: https://doi.org/10.1111/j.1464-
5491.2006.01858.x
20. National Cholesterol Education Program (NCEP) Expert Panel on Detection
Evaluation and Treatment of High Blood Cholesterol in Adults (Adult
Treatment Panel III). Third report of the National Cholesterol Education
Program (NCEP) expert panel on detection, evaluation, and treatment of high
blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation
2002;106(25):3143-421. [published Online First: 2002/12/18]
20
21. Gerstein HC, Santaguida P, Raina P, et al. Annual incidence and relative risk of
diabetes in people with various categories of dysglycemia: A systematic
overview and meta-analysis of prospective studies. Diabetes Research and
Clinical Practice 2007;78(3):305-12. doi:
https://doi.org/10.1016/j.diabres.2007.05.004 [published Online First:
2007/07/03]
22. Ford ES, Li C, Sattar N. Metabolic syndrome and incident diabetes: Current state
of the evidence. Diabetes Care 2008;31(9):1898-904. doi:
https://doi.org/10.2337/dc08-0423 [published Online First: 2008/07/02]
23. Emerging Risk Factors Collaboration, Sarwar N, Gao P, et al. Diabetes mellitus,
fasting blood glucose concentration, and risk of vascular disease: a
collaborative meta-analysis of 102 prospective studies. Lancet
2010;375(9733):2215-22. doi: https://doi.org/10.1016/S0140-6736(10)60484-9
24. Wang W, Lo ACY. Diabetic retinopathy: Pathophysiology and treatments.
International Journal of Molecular Sciences 2018;19(6):1816. doi:
https://doi.org/10.3390/ijms19061816
25. Callaghan BC, Cheng HT, Stables CL, et al. Diabetic neuropathy: Clinical
manifestations and current treatments. The Lancet Neurology 2012;11(6):521-
34. doi: https://doi.org/10.1016/S1474-4422(12)70065-0 [published Online
First: 2012/05/16]
26. Stephens JW, Brown KE, Min T. Chronic kidney disease in type 2 diabetes:
Implications for managing glycaemic control, cardiovascular and renal risk.
Diabetes, Obesity and Metabolism 2020;22(S1):32-45. doi:
https://doi.org/10.1111/dom.13942
21
27. Thiruvoipati T, Kielhorn CE, Armstrong EJ. Peripheral artery disease in patients
with diabetes: Epidemiology, mechanisms, and outcomes. World Journal of
Diabetes 2015;6(7):961-69. doi: https://doi.org/10.4239/wjd.v6.i7.961
28. Ferreira LSS, Fernandes CS, Vieira MNN, et al. Insulin resistance in Alzheimer's
disease. Frontiers in Neuroscience 2018;12:830-30. doi:
https://doi.org/10.3389/fnins.2018.00830
29. Cholerton B, Baker LD, Montine TJ, et al. Type 2 diabetes, cognition, and
dementia in older adults: Toward a precision health approach. Diabetes
Spectrum :A Publication of the American Diabetes Association
2016;29(4):210-19. doi: https://doi.org/10.2337/ds16-0041
30. Diagnostic and statistical manual of mental disorders : DSM-5™. 5th edition. ed.
Washington, DC ;: American Psychiatric Publishing, a division of American
Psychiatric Association 2013.
31. World Health Organization. Depression and other common mental disorders:
global health estimates. Geneva: World Health Organization, 2017.
32. World Health Organization. The global burden of disease: 2004 update. 2008
33. Tanamas S, Magliano D, Lynch V, et al. AusDiab 2012: The Australian diabetes,
obesity and lifestyle study Baker IDI: Heart and Diabetes Institute 2013
34. Almeida OP, Calver J, Jamrozik K, et al. Obesity and metabolic syndrome
increase the risk of incident depression in older men: The health in men study.
The American Journal of Geriatric Psychiatry 2009;17(10):889-98. doi:
https://doi.org/10.1097/JGP.0b013e3181b047e3
35. Mezuk B, Eaton WW, Albrecht S, et al. Depression and type 2 diabetes over the
lifespan: A meta-analysis. Diabetes Care 2008;31(12):2383-90. doi:
https://doi.org/10.2337/dc08-0985

22
36. Chireh B, Li M, D'Arcy C. Diabetes increases the risk of depression: A systematic
review, meta-analysis and estimates of population attributable fractions based
on prospective studies. Preventive Medicine Reports 2019;14:100822-22. doi:
https://doi.org/10.1016/j.pmedr.2019.100822
37. Pan A, Keum N, Okereke OI, et al. Bidirectional association between depression
and metabolic syndrome: A systematic review and meta-analysis of
epidemiological studies. Diabetes Care 2012;35(5):1171-80. doi:
https://doi.org/10.2337/dc11-2055
38. Knol MJ, Twisk JWR, Beekman ATF, et al. Depression as a risk factor for the
onset of type 2 diabetes mellitus. A meta-analysis. Diabetologia
2006;49(5):837. doi: https://doi.org/10.1007/s00125-006-0159-x
39. Celik Guzel E, Bakkal E, Guzel S, et al. Can low brain-derived neurotrophic
factor levels be a marker of the presence of depression in obese women?
Neuropsychiatric Disease and Treatment 2014;10:2079-86. doi:
https://doi.org/10.2147/ndt.S72087 [published Online First: 2014/11/15]
40. Krabbe KS, Nielsen AR, Krogh-Madsen R, et al. Brain-derived neurotrophic
factor (BDNF) and type 2 diabetes. Diabetologia 2007;50(2):431-38. doi:
https://doi.org/10.1007/s00125-006-0537-4
41. Yu H, Chen Z-y. The role of BDNF in depression on the basis of its location in
the neural circuitry. Acta Pharmacologica Sinica 2011;32(1):3-11. doi:
https://doi.org/10.1038/aps.2010.184 [published Online First: 2010/12/06]
42. Yokoyama K, Yamada T, Mitani H, et al. Relationship between hypothalamic–
pituitary–adrenal axis dysregulation and insulin resistance in elderly patients
with depression. Psychiatry Research 2015;226(2):494-98. doi:
https://doi.org/10.1016/j.psychres.2015.01.026
23
43. Carroll BJ, Cassidy F, Naftolowitz D, et al. Pathophysiology of hypercortisolism in
depression. Acta Psychiatrica Scandinavica 2007;115(s433):90-103. doi:
https://doi.org/10.1111/j.1600-0447.2007.00967.x
44. Leonard BE. Inflammation and depression: A causal or coincidental link to the
pathophysiology? Acta Neuropsychiatrica 2018;30(1):1-16. doi:
https://doi.org/10.1017/neu.2016.69 [published Online First: 2017/06/23]
45. Ouakinin SRS, Barreira DP, Gois CJ. Depression and obesity: Integrating the
role of stress, neuroendocrine dysfunction and inflammatory pathways.
Frontiers in Endocrinology 2018;9:431-31. doi:
https://doi.org/10.3389/fendo.2018.00431
46. Schmitz N, Deschenes SS, Burns RJ, et al. Depression and risk of type 2
diabetes: The potential role of metabolic factors. Molecular Psychiatry
2016;21(12):1726-32. doi: https://doi.org/10.1038/mp.2016.7 [published
Online First: 2016/02/24]
47. Lebovitz HE. Thiazolidinediones: The forgotten diabetes medications. Current
Diabetes Reports 2019;19(12):151-51. doi: https://doi.org/10.1007/s11892-
019-1270-y
48. Duval F, Lebowitz BD, Macher J-P. Treatments in depression. Dialogues in
Clinical Neuroscience 2006;8(2):191-206. doi:
https://doi.org/10.31887/DCNS.2006.8.2/fduval
49. Nguyen Q, Dominguez J, Nguyen L, et al. Hypertension management: An
update. American Health & Drug Benefits 2010;3(1):47-56.
50. Huang YT, Wei L, Steptoe A, et al. OP48 The prevalence and risk factors of
polypharmacy among diabetic people: evidence from the english longitudinal
study of ageing (ELSA). Journal of Epidemiology and Community Health

24
2019;73(Suppl 1):A23. doi: https://doi.org/10.1136/jech-2019-
SSMabstracts.49
51. Holvast F, van Hattem BA, Sinnige J, et al. Late-life depression and the
association with multimorbidity and polypharmacy: A cross-sectional study.
Family Practice 2017;34(5):539-45. doi:
https://doi.org/10.1093/fampra/cmx018
52. Ferguson JM. SSRI antidepressant medications: Adverse effects and tolerability.
Primary Care Companion to the Journal of Clinical Psychiatry 2001;3(1):22-
27. doi: https://doi.org/10.4088/pcc.v03n0105
53. Ramic E, Prasko S, Gavran L, et al. Assessment of the antidepressant side
effects occurrence in patients treated in primary care. Materia Socio-mMdica
2020;32(2):131-34. doi: https://doi.org/10.5455/msm.2020.32.131-134
54. Ramkumar S, Raghunath A, Raghunath S. Statin therapy: Review of safety and
potential side effects. Acta Cardiologica Sinica 2016;32(6):631-39. doi:
https://doi.org/10.6515/acs20160611a
55. Gonçalves CB, Moreira LB, Gus M, et al. Adverse events of blood-pressure-
lowering drugs: Evidence of high incidence in a clinical setting. European
Journal of Clinical Pharmacology 2007;63(10):973-8. doi:
https://doi.org/10.1007/s00228-007-0352-y [published Online First:
2007/08/19]
56. Chaudhury A, Duvoor C, Reddy Dendi VS, et al. Clinical review of antidiabetic
drugs: Implications for type 2 diabetes mellitus management. Frontiers in
Endocrinology 2017;8:6-6. doi: https://doi.org/10.3389/fendo.2017.00006
57. Lie JD, Tu KN, Shen DD, et al. Pharmacological treatment of insomnia.
Pharmacy and Therapeutics 2015;40(11):759-71.
25
58. Richter EA, Hargreaves M. Exercise, GLUT4, and skeletal muscle glucose
uptake. Physiological Reviews 2013;93(3):993-1017. doi:
https://doi.org/10.1152/physrev.00038.2012
59. Roberts CK, Little JP, Thyfault JP. Modification of insulin sensitivity and glycemic
control by activity and exercise. Medicine & Science in Sports & Exercise
2013;45(10) doi: https://doi.org/10.1249/MSS.0b013e318295cdbb
60. Kennedy JW, Hirshman MF, Gervino EV, et al. Acute exercise induces GLUT4
translocation in skeletal muscle of normal human subjects and subjects with
type 2 diabetes. Diabetes 1999;48(5):1192. doi:
https://doi.org/10.2337/diabetes.48.5.1192
61. Holten MK, Zacho M, Gaster M, et al. Strength training increases insulin-
mediated glucose uptake, GLUT4 content, and insulin signaling in skeletal
muscle in patients with type 2 diabetes. Diabetes 2004;53(2):294. doi:
https://doi.org/10.2337/diabetes.53.2.294
62. Little JP, Gillen JB, Percival ME, et al. Low-volume high-intensity interval training
reduces hyperglycemia and increases muscle mitochondrial capacity in
patients with type 2 diabetes. Journal of Applied Physiology
2011;111(6):1554-60. doi: https://doi.org/10.1152/japplphysiol.00921.2011
63. Hussey SE, McGee SL, Garnham A, et al. Exercise training increases adipose
tissue GLUT4 expression in patients with type 2 diabetes. Diabetes, Obesity
and Metabolism 2011;13(10):959-62. doi: https://doi.org/10.1111/j.1463-
1326.2011.01426.x
64. Dela F, Ploug T, Handberg A, et al. Physical training increases muscle GLUT4
protein and mRNA in patients with NIDDM. Diabetes 1994;43(7):862. doi:
https://doi.org/10.2337/diab.43.7.862
26
65. Pan X-R, Li G-W, Hu Y-H, et al. Effects of diet and exercise in preventing NIDDM
in people with impaired glucose tolerance: The Da Qing IGT and diabetes
study. Diabetes Care 1997;20(4):537. doi:
https://doi.org/10.2337/diacare.20.4.537
66. Tuomilehto J, Lindström J, Eriksson JG, et al. Prevention of type 2 diabetes
mellitus by changes in lifestyle among subjects with impaired glucose
tolerance. New England Journal of Medicine 2001;344(18):1343-50. doi:
https://doi.org/10.1056/NEJM200105033441801
67. Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of
type 2 diabetes with lifestyle intervention or metformin. The New England
Journal of Medicine 2002;346(6):393-403. doi:
https://doi.org/10.1056/NEJMoa012512 [published Online First: 2002/02/08]
68. Umpierre D, Ribeiro PAB, Kramer CK, et al. Physical activity advice only or
structured exercise training and association with HbA1c levels in type 2
diabetes: A systematic review and meta-analysis. Journal of the American
Medical Association 2011;305(17):1790-99. doi:
https://doi.org/10.1001/jama.2011.576
69. Umpierre D, Ribeiro PAB, Schaan BD, et al. Volume of supervised exercise
training impacts glycaemic control in patients with type 2 diabetes: A
systematic review with meta-regression analysis. Diabetologia
2013;56(2):242-51. doi: https://doi.org/10.1007/s00125-012-2774-z
70. Boulé NG, Haddad E, Kenny GP, et al. Effects of exercise on glycemic control
and body mass in type 2 diabetes mellitus: a meta-analysis of controlled
clinical trials. The Journal of the American Medical Association

27
2001;286(10):1218-27. doi: https://doi.org/10.1001/jama.286.10.1218
[published Online First: 2001/09/18]
71. Kanaley JA, Colberg SR, Corcoran MH, et al. Exercise/physical activity in
individuals with type 2 diabetes: A consensus statement from the American
College of Sports Medicine. Medicine & Science in Sports & Exercise
2022;54(2) doi: https://doi.org/10.1249/mss.0000000000002800
72. Strasser B, Arvandi M, Siebert U. Resistance training, visceral obesity and
inflammatory response: A review of the evidence. Obes Rev 2012;13(7):578-
91. doi: https://doi.org/10.1111/j.1467-789X.2012.00988.x [published Online
First: 2012/03/06]
73. Gordon BA, Benson AC, Bird SR, et al. Resistance training improves metabolic
health in type 2 diabetes: A systematic review. Diabetes Research and
Clinical Practice 2009;83(2):157-75. doi:
https://doi.org/10.1016/j.diabres.2008.11.024 [published Online First:
2009/01/13]
74. Tarray R, Saleem S, Afroze D, et al. Role of insulin resistance in essential
hypertension. Cardiovascular Endocrinology & Metabolism 2014;3(4) doi:
https://doi.org/10.1097/XCE.0000000000000032
75. Salvetti A, Brogi G, Di Legge V, et al. The inter-relationship between insulin
resistance and hypertension. Drugs 1993;46(2):149-59. doi:
https://doi.org/10.2165/00003495-199300462-00024
76. Naci H, Salcher-Konrad M, Dias S, et al. How does exercise treatment compare
with antihypertensive medications? A network meta-analysis of 391
randomised controlled trials assessing exercise and medication effects on
28
systolic blood pressure. British Journal of Sports Medicine 2019;53(14):859.
doi: https://doi.org/10.1136/bjsports-2018-099921
77. Schuch FB, Vancampfort D, Richards J, et al. Exercise as a treatment for
depression: A meta-analysis adjusting for publication bias. Journal of
Psychiatric Research 2016;77:42-51. doi:
https://doi.org/10.1016/j.jpsychires.2016.02.023
78. Herring MP, Puetz TW, O’Connor PJ, et al. Effect of exercise training on
depressive symptoms among patients with a chronic illness: A systematic
review and meta-analysis of randomized controlled trials. Archives of Internal
Medicine 2012;172(2):101-11. doi:
https://doi.org/10.1001/archinternmed.2011.696
79. Gordon BR, McDowell CP, Hallgren M, et al. Association of efficacy of resistance
exercise training with depressive symptoms: Meta-analysis and meta-
regression analysis of randomized clinical trials. JAMA Psychiatry
2018;75(6):566-76. doi: https://doi.org/10.1001/jamapsychiatry.2018.0572
80. Morres ID, Hatzigeorgiadis A, Stathi A, et al. Aerobic exercise for adult patients
with major depressive disorder in mental health services: A systematic review
and meta-analysis. Depression and Anxiety 2019;36(1):39-53. doi:
https://doi.org/10.1002/da.22842 [published Online First: 2018/10/20]
81. Cooney GM, Dwan K, Greig CA, et al. Exercise for depression. Cochrane
Database of Systematic Reviews 2013(9):Cd004366. doi:
https://doi.org/10.1002/14651858.CD004366.pub6 [published Online First:
2013/09/13]
82. Blumenthal JA, Babyak MA, Doraiswamy PM, et al. Exercise and
pharmacotherapy in the treatment of major depressive disorder.
29
Psychosomatic Medicine 2007;69(7):587-96. doi:
https://doi.org/10.1097/PSY.0b013e318148c19a [published Online First:
2007/09/10]
83. Blumenthal JA, Sherwood A, Babyak MA, et al. Exercise and pharmacological
treatment of depressive symptoms in patients with coronary heart disease:
Results from the UPBEAT (Understanding the Prognostic Benefits of Exercise
and Antidepressant Therapy) study. Journal of the American College of
Cardiology 2012;60(12):1053-63. doi:
https://doi.org/10.1016/j.jacc.2012.04.040
84. Strasser B, Schobersberger W. Evidence for resistance training as a treatment
therapy in obesity. Journal of Obesity 2011;2011:482564. doi:
https://doi.org/10.1155/2011/482564 [published Online First: 2010/08/10]
85. Li Y, Su Y, Chen S, et al. The effects of resistance exercise in patients with knee
osteoarthritis: A systematic review and meta-analysis. Clinical Rehabilitation
2016;30(10):947-59. doi: https://doi.org/10.1177/0269215515610039
[published Online First: 2015/10/17]
86. Lange AK, Vanwanseele B, Fiatarone singh MA. Strength training for treatment
of osteoarthritis of the knee: A systematic review. Arthritis Care & Research
2008;59(10):1488-94. doi: https://doi.org/10.1002/art.24118
87. Tofthagen C, Visovsky C, Berry DL. Strength and balance training for adults with
peripheral neuropathy and high risk of fall: Current evidence and implications
for future research. Oncology Nursing Forum 2012;39(5):E416-24. doi:
https://doi.org/10.1188/12.Onf.E416-e424 [published Online First: 2012/09/04]
88. Parmenter BJ, Mavros Y, Ritti Dias R, et al. Resistance training as a treatment
for older persons with peripheral artery disease: A systematic review and

30
meta-analysis. British Journal of Sports Medicine 2020;54(8):452. doi:
https://doi.org/10.1136/bjsports-2018-100205
89. Qadir R, Sculthorpe NF, Todd T, et al. Effectiveness of resistance training and
associated program characteristics in patients at risk for type 2 diabetes: A
systematic review and meta-analysis. Sports Medicine - Open 2021;7(1):38.
doi: https://doi.org/10.1186/s40798-021-00321-x
90. Acosta-Manzano P, Rodriguez-Ayllon M, Acosta FM, et al. Beyond general
resistance training. Hypertrophy versus muscular endurance training as
therapeutic interventions in adults with type 2 diabetes mellitus: A systematic
review and meta-analysis. Obesity Reviews 2020;21(6):e13007. doi:
https://doi.org/10.1111/obr.13007 [published Online First: 2020/02/19]
91. Moraes HS, Silveira HS, Oliveira NA, et al. Is strength training as effective as
aerobic training for depression in older adults? A randomized controlled trial.
Neuropsychobiology 2020;79(2):141-49. doi:
https://doi.org/10.1159/000503750
92. Singh NA, Clements KM, Fiatarone MA. A randomized controlled trial of
progressive resistance training in depressed elders. Journals of Gerontology
Series a-Biological Sciences and Medical Sciences 1997;52(1):M27-M35. doi:
https://doi.org/10.1093/gerona/52A.1.M27
93. Black LE, Swan PD, Alvar BA. Effects of intensity and volume on insulin
sensitivity during acute bouts of resistance training. The Journal of Strength
and Conditioning Research 2010;24(4):1109-16. doi:
https://doi.org/10.1519/JSC.0b013e3181cbab6d [published Online First:
2010/01/23]

31
94. Liu Y, Ye W, Chen Q, et al. Resistance exercise intensity is correlated with
attenuation of HbA1c and insulin in patients with type 2 diabetes: A systematic
review and meta-Analysis. International Journal of Environmental Research
and Public Health 2019;16(1):140. doi: https://doi.org/10.3390/ijerph16010140

32
CHAPTER 2: The effect of resistance exercise on
depressive symptoms in adults with insulin resistance: A
systematic review of randomised controlled trials
Alexander Bate1, Maria Fiatarone Singh, MD, FRACP123, Yorgi Mavros, PhD1
1Faculty of Medicine and Health, University of Sydney, Australia
2Professor, Sydney Medical School
3John Sutton Chair of Exercise and Sport Science, Sydney School of Health Sciences
Corresponding author:
Alexander Bate, B.Ex&Sp.Sc, Grad. Dip. Ex Phys, ESSAM AEP
Mail: Level 6, Susan Wakil Health Building, D18 The University of Sydney NSW 2006 Australia
Tel: +61 432 588 554; Fax: +61 (2) 9351 9163; Email: [email protected]
33
Abstract
Background Insulin resistance and depressive disorders are chronic health
conditions that commonly co-exist, with evidence indicating possible shared
underlying pathophysiology. Non-pharmacological interventions to treat both
conditions are required to reduce the risk of polypharmacy and drug-to-drug
interaction. The benefits of resistance exercise interventions for insulin resistance
and depressive disorders have been well established, but to date a quantitative
analysis of resistance training (RT) effects on cohorts with both depressive
symptoms and insulin resistance has not been conducted.
Objectives To systematically review the evidence in randomised controlled trials
(RCT) for RT interventions in adults with insulin resistance where depressive
symptoms were also measured, with primary outcomes being any measure of
depressive symptoms, insulin resistance, or glucose metabolism.
Data sources MEDLINE, AMED (Allied and Complimentary Medicine) Embase,
PsycINFO, Sportdiscus, CINAHL, and PEDro (Physiotherapy Evidence Database)
were search for articles published before December 2019.
Study selection Randomised controlled trials that employed a RT intervention that
utilised any validated objective or subjective tool to measure symptoms of
depression, in any cohort that met accepted criteria for insulin resistance, including
metabolic syndrome, polycystic ovary syndrome or type-2 diabetes. No restrictions
were placed on comparison groups, and RT could be prescribed in isolation or in
combination with another active treatment.
34
Data extraction and synthesis Studies were analysed for intervention and
comparator characteristics, exercise frequency and intensity, duration of intervention,
and Hedges’ g effect sizes were calculated for all outcomes. Assessment of exercise
reporting was done using the Consensus on Exercise Reporting Template (CERT)
and risk of bias assessed using the Cochrane RoB-2 tool.
Results Seven RCTs providing 10 between-group comparisons met the inclusion
criteria. Study design and intervention characteristics were largely heterogenous,
precluding meta-analysis. All studies were performed in adults with type-2 diabetes.
No studies recruited participants with major depressive disorder, and all studies used
self-reported assessments of depressive symptoms. Significant reductions (p <. 05)
in depressive symptom severity favouring RT were reported in 2 studies that
prescribed resistance training in isolation against non-active comparator groups.
Significant reductions (p <. 05) in HbA1c levels favouring RT were reported in 3
studies: 1 prescribing RT in isolation against a non-active comparator; 1 prescribing
a combined RT and aerobic intervention against a non-active comparator; and 1
prescribing a combined RT and aerobic intervention against an active exercise
comparator group. Moderate-to-large effects for both depressive symptoms and
HbA1c were seen across studies of different intensities and volumes, though
similarly favoured studies that employed non-active comparator groups.
Conclusions The limited data available suggests that RT is an effective standalone
intervention to simultaneously reduce depressive symptoms and HbA1c in
individuals with depressive symptoms and insulin resistance. However, the literature
is small and of low quality, with no studies performed in adults with major depressive
disorder or using a clinical assessment of depression. Well-designed studies

35
specifically targeting individuals with insulin resistance and major depressive
disorder are warranted.
36
Introduction
Insulin resistance is a metabolic condition characterised by impaired insulin action in
metabolically active tissues and organs, and is associated with states of glucose
dysregulation such as impaired fasting glucose, impaired glucose tolerance,
metabolic syndrome, and type-2 diabetes mellitus (T2DM).1-3 Insulin resistance could
be defined briefly as ‘a clinical state in which a normal or elevated insulin level
produces an attenuated biologic response, specifically insulin-stimulated glucose
disposal’.4 This manifests in early clinical stages as either impaired fasting glucose,
impaired glucose tolerance, or both simultaneously.5 Longitudinal studies have
demonstrated that insulin resistance is central to the development of hypertension
and dyslipidaemia, resulting in progression to metabolic syndrome,2 6 and if left
unmanaged, to T2DM.7 Furthermore, T2DM is pathophysiologically associated with
cardiovascular disease,8-10 stroke,11 retinopathy,12 neuropathy,13 renal disease,14
peripheral vascular disease,15 and dementia.16 17 Therefore it is crucial to target
insulin resistance in order to not only prevent disease progression to T2DM, but also
reduce the risk of future complications, co-morbidities, and premature mortality.
Less well recognised, but increasingly important risk factors for the progression of
insulin resistance are mental health disorders, including major depressive disorder
(MDD).18-20 Prospectively, individuals with elevated depressive symptoms have a
37% increased risk of incident T2DM compared to individuals with mild or no
depressive symptoms.21 Conversely, the risk of incident depression has been
observed to be over two-fold higher (137%) over an eight-year period for individuals
37
with metabolic syndrome22 and 15% higher for those with T2DM compared to
metabolically healthy individuals.23 This apparent bi-directional relationship between
metabolic and affective illness increases the future risk of other co-morbidities and
poor health. For example, individuals with co-existing depressive symptoms and
metabolic syndrome have a six-fold higher risk of developing T2DM over 4.5 years
compared with healthy individuals,24 while individuals with co-existing MDD and
T2DM are at a 33% and 38% increased risk of micro- and macrovascular
complications, respectively,25 as well as higher rates of hospitalisation,26 cardiac,27
and all-cause mortality.26 Thus, for individuals with insulin resistance, identification
and management of depressive illness is important to delay progression to T2DM as
well as to reduce the risk of future complications and mortality.
Simultaneous pharmacological management of insulin resistance, depressive
symptoms and the associated cardiovascular risk factors of hypertension and
dyslipidaemia in metabolic syndrome would require multiple drug therapies.28 29 30
Such poly-pharmacological approaches to care include inherent risks. Not only does
each additive drug have its own risk profile, there is an increased risk of drug-drug
and drug-nutrient interactions,31 greater financial burden on the patient, reduced
medication adherence,32 and the potential for unnecessary drug prescription if
therapy is duplicated across multiple specialists or adverse drug events are
misinterpreted as new medical conditions (referred to as the ‘prescribing cascade’).33
34 Thus, there is a clear need for effective, non-pharmacological approaches to
manage existing or emergent depressive symptoms in the presence of insulin
resistant states such as metabolic syndrome and T2DM.
38
Structured exercise is one non-pharmacological approach that has been shown to be
effective at reducing both insulin resistance and depressive symptoms. Exercise has
been shown to improve insulin resistance in individuals with impaired fasting
glucose, impaired glucose tolerance, metabolic syndrome, and T2DM, with benefits
observed after continuous aerobic training, interval training and resistance training,
as well as combinations of these modalities.35-38 The therapeutic benefits of exercise
also extend to the many cardiovascular risk factors that commonly cluster with
insulin resistance such as visceral adiposity39 and hypertension, with the effects of
exercise on blood pressure comparable to anti-hypertensive medication.40
Similar to the benefits of exercise in insulin resistance syndromes noted above,
exercise has also been shown to have potent anti-depressant effects.41 42 For
example aerobic exercise had similar efficacy to sertraline for a reduction in
symptoms and remission of depressive episodes in a head-to-head comparison in
middle-aged to older adults with MDD.43 44 With respect to depression as a co-
morbidity, exercise interventions have been shown to improve depressive symptoms
in individuals who had pre-existing chronic diseases including cardiovascular
disease,45 chronic pain, fibromyalgia, obesity, neurological disorders, and chronic
obstructive pulmonary disease, including trials where participants had undiagnosed
or subsyndromal depression.42 Thus, there is compelling evidence that exercise is an
effective intervention for the treatment of both insulin resistance and depressive
symptoms.
39
However, despite the well documented effects of exercise in improving both insulin
resistance and depressive symptoms noted above, many questions remain. First, it
is unknown to what extent exercise can simultaneously improve insulin resistance
and depressive symptoms in individuals who present with both conditions.
Furthermore, with the majority of the literature to date focusing on aerobic exercise,
the specific role of resistance exercise requires further investigation.
Resistance training (RT) is an anabolic form of exercise that may be more accessible
for some individuals where aerobic modalities such as walking or cycling may be
painful or difficult in individuals with underlying conditions such as obesity,46
osteoarthritis,47 48 peripheral neuropathy,49 or peripheral arterial disease.50 While less
well studied than aerobic exercise, strong evidence exists that RT can improve
insulin resistance51 52 and depressive symptoms,41 53 with evidence of a dose-
response effect of intensity, favouring higher intensity training for depression54 as
well as metabolic outcomes.55 56 In addition, RT offers a unique advantage over other
modalities of exercise; namely the ability to increase muscle mass and strength. This
is particularly relevant in the context of T2DM, which may be complicated by a
diabetic myopathy, or treated with energy-restricted diets during which up to 40% of
weight loss may come from lean tissue.57 In older adults, such losses of muscle and
bone mass58 may predispose an individuals to, or worsen, pre-existing sarcopenia
and osteoporosis, thus leaving them at risk of future mobility impairment, falls, hip
fractures and/or disability.59-61 Resistance training is the only modality of exercise
shown to preserve lean tissue during severe caloric restriction in young to middle-
aged adults,62-66 and has been shown to increase lean tissue and improve glycaemic
control in older adults with T2DM undergoing moderate caloric restriction.67 68
40
Therefore, a strong rationale exists for the use of RT as a treatment for co-morbid
depressive and metabolic illness. This rationale is based on the fact that it can
improve both conditions simultaneously, potentially reduce hazardous polypharmacy,
and provides an economical exercise prescription that targets many of the other
comorbidities common in this cohort (e.g., sarcopenia, osteoporosis, peripheral
vascular disease, cardiovascular disease, osteoarthritis, among others), while being
potentially more feasible in some individuals than weight-bearing aerobic exercise.
However, to our knowledge, the literature addressing this topic has never been
systematically reviewed where all conditions of insulin resistance and all severity of
depressive illness were included. Thus, the purpose of this paper was to
systematically review all published randomised controlled trials (RCT) that
investigated the effects of RT on adults with insulin resistance, where depressive
symptoms were also measured, with primary outcomes being any measure of
depressive symptoms, insulin resistance, or glucose metabolism.
41
Methods
A systematic review of the literature was conducted. Details of the protocol for this
systematic review were prospectively registered on PROSPERO register of
systematic reviews,69 with PROSPERO ID CRD42020160903. The methods for this
review are detailed in accordance with the 2020 Preferred Reporting Items for
Systematic Reviews and Meta-analyses (PRISMA) statement guidelines,70 including
the extension for searches (PRIMSA-S).71
Search Strategy
An electronic database search was performed for studies published from date of
database inception through to 10 December 2019 using the following databases:
MEDLINE (Ovid), Sportdiscus (EBSCOhost), Allied and Complementary Medicine
(AMED, EBSCOhost), CINAHL (EBSCOhost), Physiotherapy Evidence Database
(PEDro), Embase (Ovid), and PsycINFO (Ovid). The complete search strategy can
be seen in Table 1. To improve specificity, the MEDLINE and CINAHL searches
were limited to human participants. For MEDLINE, this was further limited to RCTs,
multicentre studies or clinical trials. All languages were included in the search
results, with non-English results being removed during the screening process if
English titles and abstracts were not available. Duplicates were removed by
Covidence72 using its automatic duplicate removal process. AB reviewed the
resulting papers (title and abstract) using Covidence to identify potentially relevant
studies. The full text of each of the remaining papers was retrieved and reviewed by
AB. The reference lists of any journal articles meeting the inclusion criteria were also
42
searched to identify additional relevant articles for inclusion. Potentially eligible
articles remaining after full-text review by AB were reviewed by YM, and any
disputes adjudicated by MFS.
Deviations from Registered Protocol
In the pre-registered protocol, eligible interventions were defined as any form of
structured or multiple bouts of exercise prescription that could be differentiated from
acute exercise studies or incidental increases in physical activity. After conducting
the search, eligible full-text papers were separated by exercise modality (aerobic or
resistance). This review focuses on the RT modality, as defined below, as it most
closely aligns with the topic of this thesis.
Eligibility Criteria
Selected studies from the initial search met the following criteria:
i. Population: human individuals of any age or sex that had any of the following
criteria:
• Impaired glucose tolerance (<7.0 mmol/L or 126 mg/dL fasting blood glucose
and 2-hour OGTT level between 7.8 mmol/L and 11.0 mmol/L, or 140 mg/dL
and 198 mg/dL);
• Insulin resistance as captured by impaired fasting glucose (fasting glucose 6.1
mmol/L to 6.9 mmol/L, or 110 mg/dL and 124 mg/dL);73 74
43
• Meeting the criteria for metabolic syndrome set by the International Diabetes
Federation,75 the World Health Organization,76 the European Group for the
study of Insulin Resistance,73 or the National Cholesterol Education Program
– Third Adult Treatment Panel at the time of publication;77 or
• Type 2 diabetes, either by physician diagnosis, or blood test results of
glycated haemoglobin (HbA1c) ≥ 6.5%, fasting blood glucose ≥7.0 mmol/L or
126 mg/dL, or 2-hour oral glucose tolerance test result of ≥11.1 mmol/L or 200
mg/dL.
The review accepted individuals with and without a diagnosis of depression, and
with any severity of depressive symptoms, so long as depressive symptoms were
measured before and after the intervention.
ii. Intervention: Resistance training either in isolation or in combination with another
therapeutic intervention, including but not limited to alternate exercise modalities,
diet, diabetes or lifestyle education, or psychological interventions. For the
purposes of this review, RT was defined as any movement or exercise that
requires muscular contraction against either external resistance or gravity with
the expected outcome of hypertrophy, or increased strength, muscular
endurance, or power.78 Resistance may have been imposed by gravity (e.g.,
body weight exercises or calisthenics), a fixed object, free weights, exercise
bands, or weightlifting machines. No restrictions were applied to intensity or
loading. Resistance training modalities could include isotonic, isokinetic, or
isometric exercises, but hydrotherapy or programs focused on specialised
44
musculoskeletal rehabilitation programs were excluded. Yoga and Pilates were
included if the type of exercises performed were judged to satisfy the criteria of
resistance training. For example, meditative types of yoga (e.g., Kundalini yoga)
were excluded, whereas power yoga and ashtanga yoga were considered eligible
since these types of yoga closely resemble body weight and calisthenics-type
resistance training. An intervention was defined as repeated bouts of exercise ≥1
day/week, lasting at least two weeks (i.e., a minimum of two sessions over two
weeks). Exposures lower than this threshold (e.g., one bout only or two bouts
over more than two weeks) were defined as acute bout studies and not included
in the review. No restriction was placed on supervision of the intervention or level
of adherence.
iii. Comparator: No restrictions were placed on comparator interventions, with
comparisons stratified as active or non-active. Non-active comparators may have
included no contact, no treatment, usual care, waiting list, attention control,
advice, or placebo. Active comparator groups included alternative exercise
modalities (e.g., resistance vs. aerobic training), lower-intensity or sham RT, or
the use of other active treatments including, but not limited to, medication, diet,
diabetes or lifestyle education, or psychological interventions. Education
interventions were classified as active if they were described in sufficient detail
and were designed with the specific intent to improve health outcomes related to
insulin resistance and/or depression. Education interventions that did not provide
detail or were generic handouts detailing guidelines or recommendations for
lifestyle changes were classified as non-active interventions.

45
iv. Outcomes: any validated objective or subjective tool to assess symptoms of
depression. This may have included any reported changes to depression status
such as: remission of symptoms; change in treatments such as use of
antidepressant medication or other psychotropic medications; use of
psychological services such as counselling, cognitive behavioural therapy,
mindfulness training, or any other treatment used for its purported effects on
depressive symptoms; or occurrence of suicidal ideation, suicide, self-harm, or
depression-related hospitalisation. Depression outcomes using any validated
assessment tool or procedure at the trial’s baseline and pre-specified endpoint
were accepted, and in the case where only interim data were available, these
were used as the post-test endpoint. As previously stated, no minimum threshold
for depression symptom severity was set for review eligibility.
Other primary outcomes were any direct measure of insulin and glucose
metabolism including but not limited to insulin, fasting blood glucose, glycosylated
haemoglobin (HbA1c), 2-hour oral glucose tolerance test (OGTT), homeostatic
model assessment for insulin resistance (HOMA-IR), or hyperinsulinaemic-
euglycaemic clamp.
Secondary outcomes included measurements of metabolic syndrome criteria:
lipids, blood pressure, or waist circumference. Adverse events reporting was also
considered within the context of secondary study outcomes.

46
v. Study design: Only RCTs were accepted for this review. Observational,
uncontrolled, and non-randomised controlled trials were excluded.
vi. Publication type: peer-reviewed, published, full-length articles with full-text
available.
No restriction was placed on language. For non-English full-texts deemed potentially
eligible by title and abstract, translation was sought with the assistance of colleagues
where possible.
Assessment of Exercise Reporting Standards
Assessment of reporting on the exercise interventions was rated using the
Consensus on Exercise Reporting Template (CERT)79 tool. A CERT score is
calculated to a total of 16 criteria, three of which are subdivided into two items, giving
a total score out of 19. While inapplicable criteria for studies were recorded as N/A,
these did not add to the total score, and therefore counted as zero for scoring
purposes. For example, item 9, which concerned detailed descriptions of any home
program components, was inapplicable to four studies80-83 which did not contain a
home program component. For studies that included a home program component
that was not adequately described, this item was scored as zero. To avoid penalising
studies for not reporting inapplicable criteria, a score was also calculated of the total
percentage of applicable criteria met.

47
Risk of Bias Assessment
Risk of bias of eligible studies was assessed using the Revised Cochrane Risk-of-
Bias Tool for randomised trials (RoB) 2 tool (ver. 2, 22/08/2019).84 This was
implemented using the provided Cochrane excel macro tool.84 Studies were
analysed for the effect of group assignment (intention-to-treat) by AB. Studies are
analysed using the RoB 2 tool according to the following domains: randomisation
process; deviations from intended interventions; missing outcome data;
measurement of the outcome; and selection of the reported result. Signalling
questions are used to determine a judgement of high risk of bias, some concerns, or
low risk of bias within these domains, and an overall risk of bias for the study was
derived algorithmically from these domain results. Any ambiguous assessments
were determined by consensus of AB and YM, and any disputes adjudicated by
MFS.
Data Extraction
AB extracted data into pre-designed templates approved by consensus. Data
pertaining to participant characteristics, intervention and comparator characteristics,
study design, depressive outcomes, and related health outcomes were extracted. If a
trial included multiple publications, these were also retrieved to extract relevant data.
Intervention data were extracted with the modality of RT designated as the primary
intervention treatment, with any other treatments (exercise or other) designated as
co-interventions. Other active treatment groups that did not include RT were treated
as comparators. In trials with three arms, all study arms that did not include RT were
extracted as separate comparators. In trials that reported outcomes at multiple
timepoints, these were extracted and analysed separately in comparison to baseline

48
values. Study authors were emailed for any missing data or information that was
required for analysis purposes.
When assessing exercise interventions, exercise exposure was calculated as
individual session length (minutes) x frequency (number of sessions/week, excluding
unsupervised home exercise) x duration (intervention length in weeks). This
produced a measure of total exercise intervention exposure, rather than weekly
exercise volume. Session length was interpreted as the estimated minutes of
supervised exercise excluding non-RT components (where reported), with the higher
estimate used where a range was provided. Exercise intensity was defined
according to ACSM85 guidelines where:
• ≥85% of 1 repetition-maximum (1RM), rate of perceived exertion (RPE) ≥18,
or 1 - 6 repetition-maximum (RM) is very high, near maximal or maximal;
• 70%–84% of 1RM, RPE 14–17, or 6 – 8 RM is high;
• 50-69% 1RM, RPE 12-13, or 8 – 15 RM is moderate; and
• <50% 1RM, RPE <12, or ≥ 15RM is light.
Repetition-maximum guidelines have been adapted from the ACSM position stand
on progression models in resistance training86 and applied when 1RM and RPE were
not provided.
Data Synthesis and Analysis
Baseline and post-intervention outcome measures were extracted. Participant,
intervention, and outcome data were extracted from text and tables. In cases where
a follow-up period after the initial intervention yielded follow-up outcome data, these
49
were also extracted. For data that were presented in figures, Webplotdigitizer87 was
used to extract data. To allow for comparisons across studies, where blood lipid and
glucose values were reported in mmol/L, these were converted to mg/dL. Standard
errors (SE) were converted to standard deviations (SD) using the following formula:
𝑆𝐷 = 𝑆𝐸 × √𝑛. Where 95% confidence intervals (95% CI) were reported, these were
converted to SD using the formula 𝑆𝐷 = √𝑛 ×(𝑈𝑝𝑝𝑒𝑟 𝑙𝑖𝑚𝑖𝑡−𝑙𝑜𝑤𝑒𝑟 𝑙𝑖𝑚𝑖𝑡)
3.92 ×𝑡−𝑑𝑖𝑠𝑡𝑟𝑖𝑏𝑢𝑡𝑖𝑜𝑛 𝑠𝑡𝑎𝑡𝑖𝑠𝑡𝑖𝑐 as detailed by
the Cochrane manual.88 Cohen’s d effect sizes were calculated using the reported
means and pooled baseline SDs using the formula d =
(𝑚𝑒𝑎𝑛 𝑑𝑖𝑓𝑓𝑒𝑟𝑒𝑛𝑐𝑒𝑖𝑛𝑡𝑒𝑟𝑣𝑒𝑛𝑡𝑖𝑜𝑛 )− (𝑚𝑒𝑎𝑛 𝑑𝑖𝑓𝑓𝑒𝑟𝑒𝑛𝑐𝑒𝑐𝑜𝑚𝑝𝑎𝑟𝑖𝑠𝑜𝑛 )
𝑝𝑜𝑜𝑙𝑒𝑑 𝑏𝑎𝑠𝑒𝑙𝑖𝑛𝑒 𝑆𝐷 .89 90 Cohen’s d was then adjusted
for small sample bias (Hedges' g). For the primary outcome reported for all studies,
negative effect sizes indicate a reduction (improvement) in depression symptom
severity.
Due to heterogeneity across studies with respect to study design, including but not
limited to RT intensity, supervision, co-interventions and comparison conditions, a
meta-analysis was not appropriate. Rather, a narrative synthesis of the results is
presented, with results stratified by the following:
1) RT in isolation vs. non-active comparator;
2) RT in isolation vs. active comparator;
3) Combined intervention (RT plus co-intervention) vs. non-active
comparator; and
4) Combined intervention (RT plus co-intervention) vs. active comparator.
50
Co-interventions and active comparators included alternative modality or lower-
intensity exercise, sham RT, or the use of other active treatments including, but not
limited to, medication, diet modification, diabetes, exercise or lifestyle advice or
psychoeducation therapies. Non-active comparator groups included usual care,
inattention control, wait-list control, generic or non-specific education, placebo, or
any other arm where no therapy is applied.
51
Results
A flow chart of study selection is presented in Figure 1. The initial search yielded
28,237 papers, which were reduced to 22,247 after removal of duplicates. A further
19,932 studies were excluded by title and abstract screening, leaving 2,315 studies
that were assessed for full-text eligibility. Of these, 159 were unable to be retrieved,
2,146 were excluded during full-text screening, leaving 10 potentially eligible studies
remaining. Three of these studies were subsequently judged ineligible: one due to
being an aerobic-based yoga intervention;91 one being a hydrotherapy intervention
with minimal RT components;92 and one using the Profile of Mood States, a
psychometric tool which is not specific to depression.93 Seven studies enrolling 452
participants in total (median 38; range 29 – 209) ultimately met the eligibility criteria
for this review.80-83 94-96
Four of the studies took place in the USA,81 82 95 96 two in Turkey,80 94 and one in
Croatia.83 Five of the studies 81-83 94 96 were set in either university or outpatient
exercise clinics, one employed a telerehabilitation intervention,80 while one did not
report the trial setting.95 Three of the studies included an unsupervised home
intervention component, two of which were undefined home-based replications of the
interventions95 96 and one being a walking program.94
Three studies (providing four comparisons) used RT as a standalone intervention.80
81 96 All three studies used a usual care comparator group, with Putiri et al. (2012)96
also using Yi Ren Medical Qigong (YMRQ) as an alternative exercise intervention.

52
Duruturk & Özköslü (2019)80 used a usual care group that also received a single
education session. As this education session was not detailed, and it was not
reported whether it was also offered to the intervention group, the comparator group
was designated as non-active.
The remaining four studies (providing six comparisons) used a RT intervention in
combination with another active intervention.82 83 94 95 Of these, only one study95
allowed for the isolated effects of RT to be determined. Further details on
intervention and comparator conditions are provided below and in Table 2.
Assessment of Exercise Reporting Standards
Overall, exercise reporting standards according to CERT79 criteria were poor, with a
median of 53% (range 12-82%) of eligible items satisfactorily reported. Mueller et al.
(2013)82 and Aylin et al. (2009)94 produced the equal highest percentage score of
82%. Putiri et al. (2012)96 was assessed to have the lowest adherence to reporting
standards, with a percentage score of 12%. The most consistently reported criteria
were related to supervision and delivery of exercise (6/7 studies) and exercise
progression, adverse events, and exercise setting (5/7 studies). Study scores were
generally downgraded for lack of detailed reporting on components such fidelity and
adherence (0 studies), description of motivation strategies (2/7 studies) and clear
decision rules for determining exercise progression (2/7 studies). A summary of the
CERT scoring is shown in Table 3 with overall scoring in Figure 2.
53
Risk of Bias Assessment
Risk of bias assessments are presented in Figure 3. Six studies were judged to be at
high risk of overall bias,80 81 83 95 96 while one study was judged to have some
concerns of bias.82 In studies judged at high risk of bias, the direction of the bias was
regarded to favour the experimental group. Six out of the seven studies were judged
to have a high risk of bias for the domain concerning the measurement of the
outcome.80-83 94-96 As all studies used a patient-reported scale for the primary
outcome, participants were accordingly designated as outcome assessors. As
participants cannot remain blinded to their allocation of resistance training, subjective
measures of depressive symptoms cannot be assessed as a blinded outcome and
are therefore subject to assessor bias. The exception to this is Mueller et al. (2013)82
who had two similar exercise groups, and therefore any bias from self-reporting
depression symptoms was not deemed to favour either group. One study83 showed
high risk of bias in the randomisation process due to lack of assessor blinding and
concealment of allocation with randomisation occurring before the baseline
assessment. Two studies showed a high risk of bias in terms of missing outcome
data with 12%80 and 37.5%96 of participant data missing at follow-up. As
missingness is potentially associated with the outcome (i.e., individuals with greater
depressive symptoms or who do not respond to treatment are more likely to drop
out), then high amounts of missing data may bias the result to those with lower
depressive symptoms at follow-up. In all other criteria, studies were not judged to
have a high risk of bias.
54
Cohort Characteristics
Cohort characteristics are presented in Table 4. All studies enrolled participants of a
similar age (mean of all cohorts = 60.0 ± 4.8 years; range of means 52.9 ± 11.2 to
66.3 ± 8.1 years) and with diagnoses of T2DM. Across all studies, 61.2% of
participants were men, with one study95 recruiting men only. The mean body mass
index (BMI) of all participants across studies was 31.2 ± 4.8 kg.m-2 (range 29.9 ± 1.0
to 36.8 ± 4.5 kg.m-2). One study enrolled participants with co-morbid chronic kidney
disease,95 and another individuals with peripheral neuropathy.82 While one study
included individuals with subsyndromal depression, no studies intentionally enrolled
individuals with MDD as an inclusion criterion. Baseline depressive symptoms
ranged from minimal (BDI of 5 ± 3.5)96 to indicative of clinical depression (CES-D of
20 ± 8.7).83 Three studies had cohorts with depressive symptom severity in the
minimal or non-clinical range,82 95 96 two had cohorts with mild depressive
symptoms,80 81 and two had cohorts with symptoms severe enough to indicate
clinical depression.83 94
Reporting of medication for managing blood glucose was mixed. Four studies81 94-96
reported the use of oral hypoglycaemic medication (median 80.2%; range 47% to
100% of participants), while three studies did not report on oral hypoglycaemic
medication use.80 82 83 Four studies81 83 95 96 reported on insulin use (median 32%;
range 0 - 61% of participants using at baseline), with one further study specifically
excluding individuals using exogenous insulin94 and two studies not reporting on
insulin use.80 82 Only one study81 reported medications prescribed for affective
symptoms, with 17% of that study’s cohort using these medications. Reporting of
medication use for common co-morbidities was poor, with only two studies providing
55
information on cholesterol-lowering medication use (40.3% and 80.6%) as well as
antihypertensive medication use (75.8% and 91%).81 95 Reporting of chronic
diseases was also poor. Only three out of seven studies reported on the presence of
cardiovascular disease (median 58.6%; range 0 - 59.7%),81 82 94 with one of these
studies also reporting on hypertension (76% of participants).81 One study reported on
the presence of cancer (24.1%),82 and the presence of other chronic diseases, if
reported, was done only as a function as inclusion or exclusion criteria. See Table 5
for further details.

56
Intervention and Comparator Characteristics
Characteristics of intervention and comparator groups can be found in Table 2,
separated by the presence or absence of co-interventions with the RT prescriptions.
Exercise prescription parameters can be found in Table 6, and co-interventions are
described in detail in Table 7.
RT in isolation vs. non-active comparator
Three studies employed RT alone vs. a non-active comparator.80 81 96 One of these
studies used Keiser resistance training machines,81 one used calisthenics,80 and one
did not report on training equipment used.96 The median duration of interventions
was 12 weeks (range 6 to 16 weeks), with a median training frequency of 3
days/week (range 1 to 3 days/week). The median of total intervention exposure over
the trial duration (min per session x frequency x weeks) was 810 minutes (range 720
minutes96 to 2160 minutes).81 Only one 16-week study prescribed exercise according
to 1RM, setting the initial load at 60% 1RM (moderate intensity)78 and progressing to
70-80% re-tested 1RM (high intensity) by week 10.81 Duruturk & Özköslü (2019)80
used light-intensity bodyweight exercises, with progression only of repetition volume
(10-15 repetitions at start of intervention, progressed to 25-30 repetitions at end of
intervention). Exercise intensity or method of exercise progression were not reported
by Putiri et al. (2012),96 however following inspection of the clinical trial registration,
the study was classified as low intensity.97 Participants were also asked to practice
their exercise at home twice a week for 30 minutes.
57
RT in isolation vs. active comparator
The YMRQ arm of Putiri et al. (2012)96 was considered an active comparator group
and analysed separately to the usual care comparator. The YMRQ prescription was
comparable to the RT group, with low intensity, 720 minutes of total exercise, and 2
x 30 minute home exercise sessions per week.
Combined intervention vs. non-active comparator
Only one study was classified as using RT in combination with a co-intervention
compared to a non-active group.94 This study prescribed RT utilising body weight,
dumbbells, ankle weights and sandbags. The intervention had a duration of 8 weeks
with a supervised RT frequency of 2 days/week. Intensity was moderate and
prescribed at 50% of baseline 1RM, then progressed to 60% of baseline 1RM at the
fourth week of the intervention. This was supplemented with a home-based walking
program ≥2 times per week that progressively increased volume by 10 minutes per
fortnight, up to a maximum of 45 minutes per session. Intensity for the walking
component was prescribed at 60 – 79% of the participant’s age-predicated maximum
heart rate. The comparator group was instructed not to undertake any formal
exercise or change their physical activity levels. Total exposure for the RT
prescription was 720 minutes.
Combined intervention vs. active comparator
Three studies were classified as combination interventions with active comparator
groups.82 83 95 Only one study allowed for the isolated effect of RT to be determined.
In this study, participants were randomised to receive nutritional counselling and

58
lifestyle modification (consisting of instruction on weight loss and increasing physical
activity) with or without RT. The RT intervention was a 12-week high intensity
program using hand-held weights, resistance bands, and weight machines for lower-
body progressive RT, following the protocol reported in Dunstan et al. (2002).67 Total
exercise exposure for the 12-week intervention was 3240 minutes. At the end of the
12-week program, participants were transitioned to a home exercise program for 40
weeks. The home program consisted of 3 x 60 min (or 6 x 30 min) sessions per
week, however exercise selection, intensity and modality were not reported for the
home-based exercise. The RT group similarly received nutritional counselling and
referral for lifestyle modification. Outcomes at both 12-weeks and 52-weeks were
extracted and analysed separately in comparison to baseline values.
The remaining three studies did not allow for the isolated effects of RT to be
determined. Aylin et al. (2009)94 combined RT with a walking program and compared
this with an non-active comparator group. In Pibernik-Okanović et al. (2015),83 the
intervention group received six RT sessions, but did not report further details on RT
exercise with respect to equipment used or modality of RT.83 Total intervention
exposure was 480 minutes, with exercise intensity reported to be light-to-medium as
determined by heart rate, however the target heart rate range was not reported.
Each RT session was preceded with a group education class on exercise and
diabetes management. The intervention in Pibernik-Okanović et al. (2015)83 was
compared to two separate comparison groups. One group received 6 sessions of
psychoeducation, where participants were taught cognitive behavioural therapy
techniques to manage depressive symptoms. The second comparison group
received a single 90-minute education session on diabetes self-management plus

59
some written materials on self-management of mood. While education between the
RT intervention group and education only group covered similar topics, content of
the materials differed between groups. As a single education session could
potentially be effective for metabolic improvements,98 the education only group was
designated as an active comparator. Outcomes for both comparator groups were
extracted and analysed separately.
Finally, Mueller et al. (2013)82 compared combined modality (aerobic and resistance
training) weight bearing exercise training compared to combined modality non-weight
bearing exercise, with both groups matched for volume and intensity of exercise. The
intervention group performed weight-bearing RT utilising lower-limb bodyweight
exercises, accompanied by a walking program that progressed in volume by a 10%
increase in average daily step count every fortnight. The comparator group was
prescribed a non-weight-bearing RT program utilising resistance bands and exercise
balls, accompanied by a stationary cycling program that was progressed in volume
equivalent to the intervention group. Intensity was maintained between 60% and
70% of age-predicted maximum heart rate, and total exposure for the RT portion of
the intervention was 2160 minutes. For this study, weight bearing exercise was
considered as having greater difficulty and therefore designated as the active
intervention, with non-weight bearing exercise the comparison group. While this
allowed comparison between modalities, it did not allow for isolation of the RT effect.

60
Depressive Symptoms
Depressive symptoms are reported in Table 8. and presented graphically in Figure 4
and Figure 5. All studies used self-reported measures of depression. Three studies
used the Beck Depression Inventory (BDI), three used the Center for
Epidemiological Studies-Depression (CES-D) scale, and one used the Geriatric
Depression Scale (GDS). No studies used clinician assessment of depressive
symptoms. While none of the studies had a diagnosis of depression as an eligibility
requirement, two studies had baseline mean CES-D scores that indicated moderate
symptom severity.83 94 Effect sizes (Hedges’ g) for depressive symptoms across all
studies were heterogeneous, and ranged from -1.28 81 to 0.15.83 Overall, studies
using high intensity RT reported larger effect sizes. The largest effect sizes were
observed in studies of RT in isolation when compared to a non-active comparison
group. Small-to-negligible effect sizes were observed in studies with active
comparator groups, where the therapeutic effect of the active comparators may have
reduced between-group differences. One study reported a clinically meaningful
change from mild depression to normal in the intervention group.81 Results are
summarised by study design below.
RT in isolation vs. non-active comparator
Results for the three studies that compared RT in isolation to a non-active
comparator group were mixed, with larger effect sizes reported in studies that
prescribed high intensity RT. Specifically, a significant and very large effect size was
reported following 16 weeks of high-intensity RT compared to usual care (p < .0001;
Hedges’ g = -1.28; 95% CI -1.85 to -0.72),81 with the upper bound confidence interval
suggesting clear clinical benefit from the intervention. A large but not significant
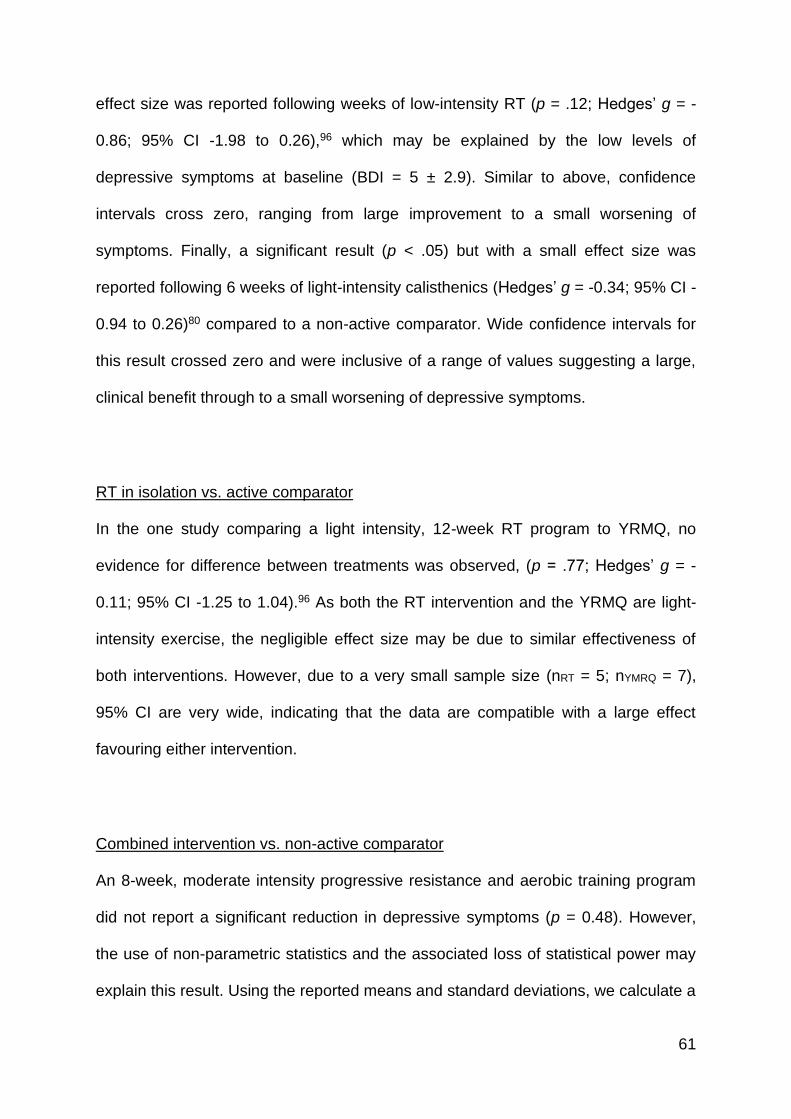
61
effect size was reported following weeks of low-intensity RT (p = .12; Hedges’ g = -
0.86; 95% CI -1.98 to 0.26),96 which may be explained by the low levels of
depressive symptoms at baseline (BDI = 5 ± 2.9). Similar to above, confidence
intervals cross zero, ranging from large improvement to a small worsening of
symptoms. Finally, a significant result (p < .05) but with a small effect size was
reported following 6 weeks of light-intensity calisthenics (Hedges’ g = -0.34; 95% CI -
0.94 to 0.26)80 compared to a non-active comparator. Wide confidence intervals for
this result crossed zero and were inclusive of a range of values suggesting a large,
clinical benefit through to a small worsening of depressive symptoms.
RT in isolation vs. active comparator
In the one study comparing a light intensity, 12-week RT program to YRMQ, no
evidence for difference between treatments was observed, (p = .77; Hedges’ g = -
0.11; 95% CI -1.25 to 1.04).96 As both the RT intervention and the YRMQ are light-
intensity exercise, the negligible effect size may be due to similar effectiveness of
both interventions. However, due to a very small sample size (nRT = 5; nYMRQ = 7),
95% CI are very wide, indicating that the data are compatible with a large effect
favouring either intervention.
Combined intervention vs. non-active comparator
An 8-week, moderate intensity progressive resistance and aerobic training program
did not report a significant reduction in depressive symptoms (p = 0.48). However,
the use of non-parametric statistics and the associated loss of statistical power may
explain this result. Using the reported means and standard deviations, we calculate a
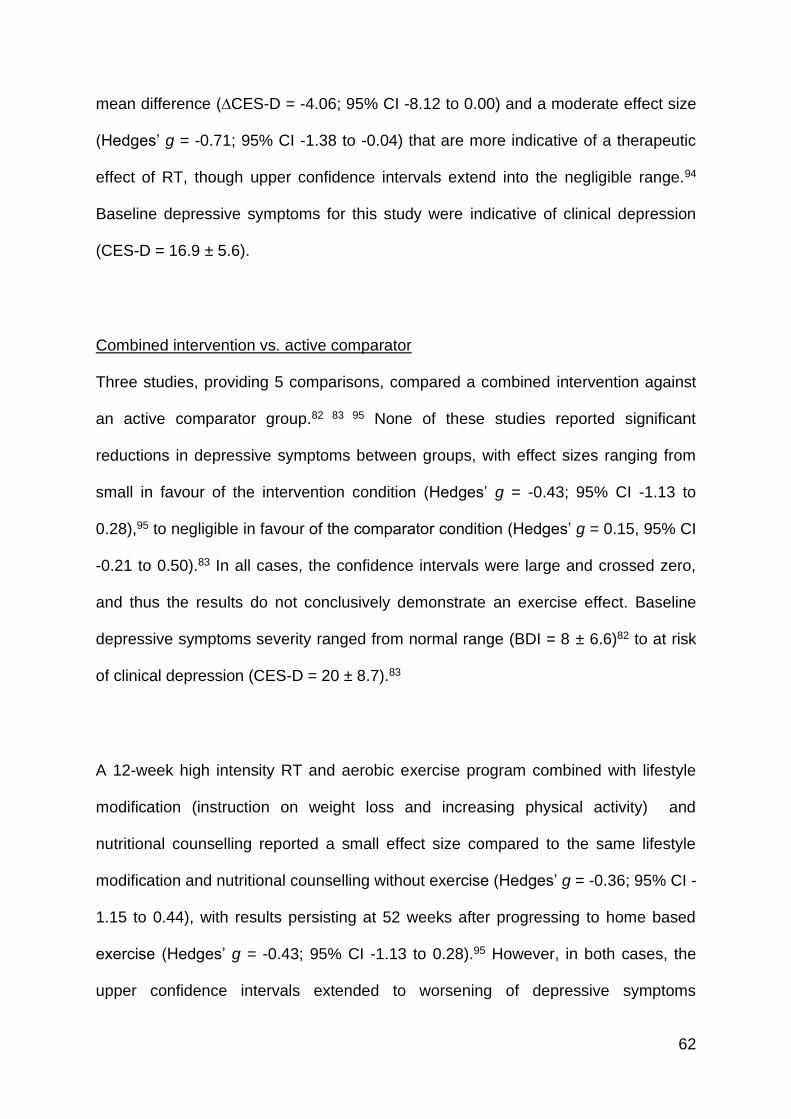
62
mean difference (∆CES-D = -4.06; 95% CI -8.12 to 0.00) and a moderate effect size
(Hedges’ g = -0.71; 95% CI -1.38 to -0.04) that are more indicative of a therapeutic
effect of RT, though upper confidence intervals extend into the negligible range.94
Baseline depressive symptoms for this study were indicative of clinical depression
(CES-D = 16.9 ± 5.6).
Combined intervention vs. active comparator
Three studies, providing 5 comparisons, compared a combined intervention against
an active comparator group.82 83 95 None of these studies reported significant
reductions in depressive symptoms between groups, with effect sizes ranging from
small in favour of the intervention condition (Hedges’ g = -0.43; 95% CI -1.13 to
0.28),95 to negligible in favour of the comparator condition (Hedges’ g = 0.15, 95% CI
-0.21 to 0.50).83 In all cases, the confidence intervals were large and crossed zero,
and thus the results do not conclusively demonstrate an exercise effect. Baseline
depressive symptoms severity ranged from normal range (BDI = 8 ± 6.6)82 to at risk
of clinical depression (CES-D = 20 ± 8.7).83
A 12-week high intensity RT and aerobic exercise program combined with lifestyle
modification (instruction on weight loss and increasing physical activity) and
nutritional counselling reported a small effect size compared to the same lifestyle
modification and nutritional counselling without exercise (Hedges’ g = -0.36; 95% CI -
1.15 to 0.44), with results persisting at 52 weeks after progressing to home based
exercise (Hedges’ g = -0.43; 95% CI -1.13 to 0.28).95 However, in both cases, the
upper confidence intervals extended to worsening of depressive symptoms

63
compared to controls, indicating uncertainty in the results. Baseline depressive
symptoms for this study were mild-to-moderate (CES-D = 14 ± 9.1).
One day/week of light-to-moderate intensity RT program combined with group
education for 6 weeks was not found to be different from a single, 90-min group
education session on diabetes self-care (Hedges’ g = -0.01; 95% CI -0.38 to 0.35) or
from psychoeducation (Hedges’ g = 0.15; 95% CI -0.21 to 0.50).83
In the final study, Mueller et al. (2013)82 compared a weight-bearing RT and aerobic
exercise program to a non-weight-bearing program of comparable intensity and
volume. No between group effect was reported (Hedges’ g = 0.11; 95% CI -0.62 to
0.83), likely due to the similarity of the exercise interventions.
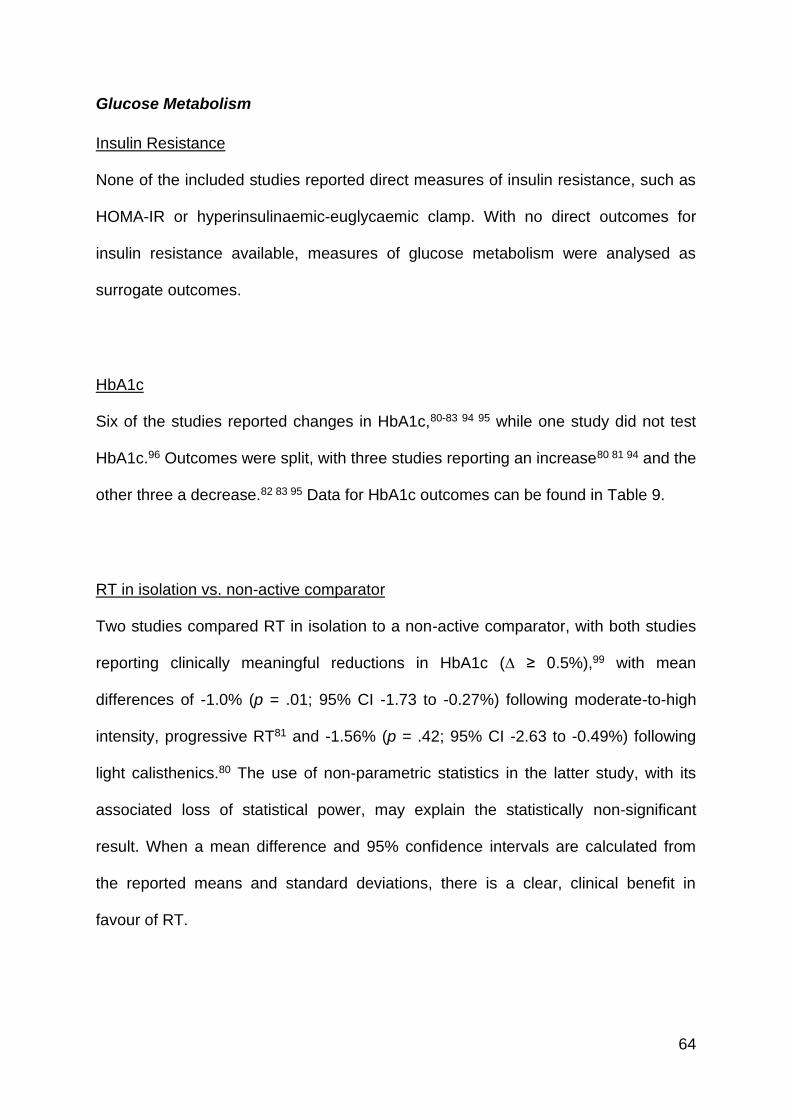
64
Glucose Metabolism
Insulin Resistance
None of the included studies reported direct measures of insulin resistance, such as
HOMA-IR or hyperinsulinaemic-euglycaemic clamp. With no direct outcomes for
insulin resistance available, measures of glucose metabolism were analysed as
surrogate outcomes.
HbA1c
Six of the studies reported changes in HbA1c,80-83 94 95 while one study did not test
HbA1c.96 Outcomes were split, with three studies reporting an increase80 81 94 and the
other three a decrease.82 83 95 Data for HbA1c outcomes can be found in Table 9.
RT in isolation vs. non-active comparator
Two studies compared RT in isolation to a non-active comparator, with both studies
reporting clinically meaningful reductions in HbA1c (∆ ≥ 0.5%),99 with mean
differences of -1.0% (p = .01; 95% CI -1.73 to -0.27%) following moderate-to-high
intensity, progressive RT81 and -1.56% (p = .42; 95% CI -2.63 to -0.49%) following
light calisthenics.80 The use of non-parametric statistics in the latter study, with its
associated loss of statistical power, may explain the statistically non-significant
result. When a mean difference and 95% confidence intervals are calculated from
the reported means and standard deviations, there is a clear, clinical benefit in
favour of RT.
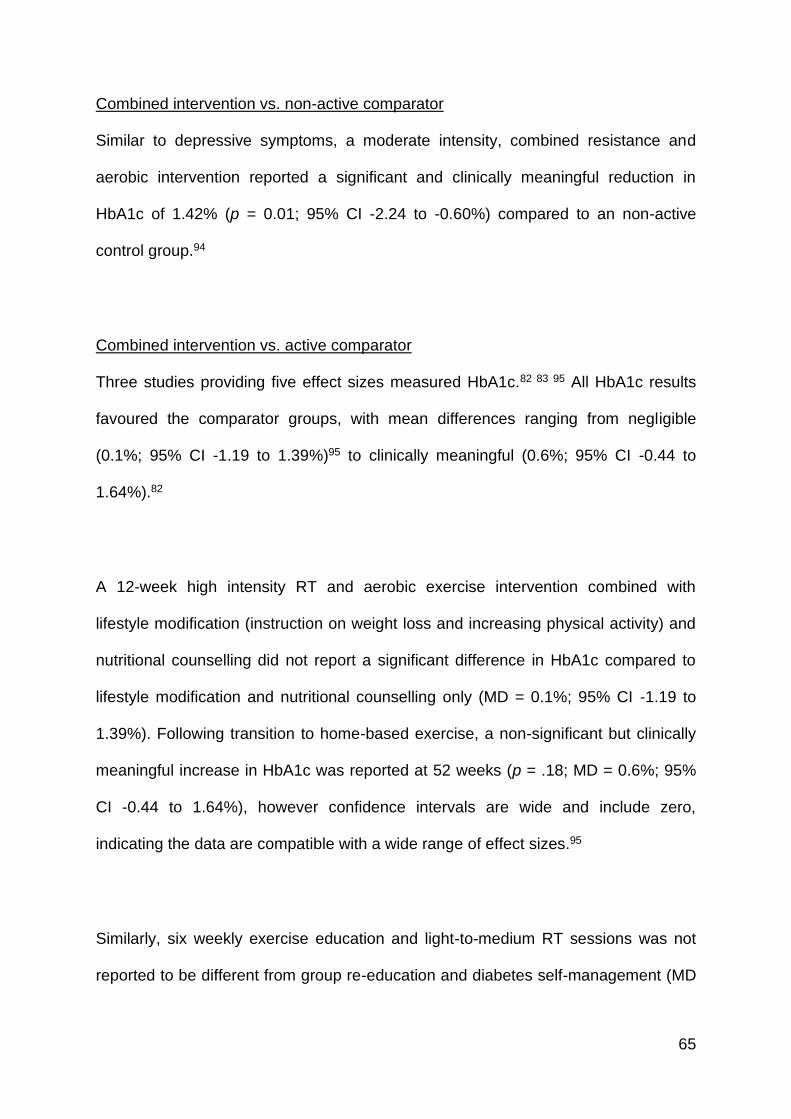
65
Combined intervention vs. non-active comparator
Similar to depressive symptoms, a moderate intensity, combined resistance and
aerobic intervention reported a significant and clinically meaningful reduction in
HbA1c of 1.42% (p = 0.01; 95% CI -2.24 to -0.60%) compared to an non-active
control group.94
Combined intervention vs. active comparator
Three studies providing five effect sizes measured HbA1c.82 83 95 All HbA1c results
favoured the comparator groups, with mean differences ranging from negligible
(0.1%; 95% CI -1.19 to 1.39%)95 to clinically meaningful (0.6%; 95% CI -0.44 to
1.64%).82
A 12-week high intensity RT and aerobic exercise intervention combined with
lifestyle modification (instruction on weight loss and increasing physical activity) and
nutritional counselling did not report a significant difference in HbA1c compared to
lifestyle modification and nutritional counselling only (MD = 0.1%; 95% CI -1.19 to
1.39%). Following transition to home-based exercise, a non-significant but clinically
meaningful increase in HbA1c was reported at 52 weeks (p = .18; MD = 0.6%; 95%
CI -0.44 to 1.64%), however confidence intervals are wide and include zero,
indicating the data are compatible with a wide range of effect sizes.95
Similarly, six weekly exercise education and light-to-medium RT sessions was not
reported to be different from group re-education and diabetes self-management (MD
66
= 0.2%; 95% CI -0.10 to 0.50%) or psychoeducation (MD = 0.2%; 95% CI -0.10 to
0.50%).83
In the final study, Mueller et al. (2013)82 compared a weight-bearing RT and aerobic
exercise program to a non-weight-bearing program of comparable intensity and
volume. A significant between group effect (p = 0.04) with a clinically meaningful
reduction in HbA1c (MD = 0.5%; 95% CI -0.48 to 1.48%) was reported favouring the
non-weight-bearing group.
Fasting glucose
For fasting plasma glucose, results were mixed. Moderate-to-high progressive RT
was not found to reduce fasting glucose compared to usual care (p = .34; MD = 1.8
mg/dL; 95% CI -21.6 to 25.2 mg/dL).81 Conversely, a moderate intensity, combined
resistance and aerobic program reported a large and significant reduction in fasting
plasma glucose compared to a non-active comparator (p = .01; MD = -21.1 mg/dL;
95% CI -35.5 to -6.6 mg/dL).94
Other Cardiometabolic Variables
Reporting on other cardiometabolic variables was largely absent, with one study
reporting blood pressure,81 and four studies reporting on blood lipid outcomes.81 83 94
95
67
Lipids
Data for the four studies reporting blood lipid outcomes81 83 94 95 are available in Table
10. In two studies, RT in isolation81 and in combination with aerobic training94
reported no statistically significant changes in any lipid outcomes. The remaining two
studies (four comparisons) were combined interventions with active comparator
groups.83 95
A high intensity RT and aerobic exercise intervention combined with lifestyle
modification (instruction on weight loss and increasing physical activity) and
nutritional counselling did not report significant difference in any lipid values
compared to lifestyle modification and nutritional counselling only at 12-weeks.
However, following transition of RT and aerobic exercise to home-based, significant
increases in total cholesterol (p = .05; MD = 26.0 mg/dL; 95% CI 5.7 to 46.3 mg/dL)
and LDL-C (p = .04; MD = 28.0 mg/dL; 95% CI 6.8 to 49.2 mg/dL) were reported in
the exercise group compared to the comparison (lifestyle modification and nutritional
counselling only) group. In the remaining study, six weekly exercise education and
light-to-medium RT sessions was not reported to be different from psychoeducation,
however a significant worsening in HDL cholesterol (p = 0.04; MD = -3.9 mg/dL; 95%
CI -7.6 to -0.1 mg/dL) was reported for the intervention group compared to one
session of re-education and diabetes self-management.83
Blood pressure
In the one study that reported blood pressure, moderate-to-high intensity RT using
machine exercises reported significant reductions in systolic BP (p = .05; MD = -17.4
68
mmHg; 95% CI -25.6 to -9.2 mmHg) but not diastolic BP (p = .52; MD = - 3.1 mmHg;
95% CI -6.6 to 0.4 mmHg) compared to a usual care control group.81 This reduction
in systolic BP exceeds what has been reported for expected reductions as a result of
common classes of antihypertensive medications,100 as well as overall mean systolic
BP reductions (-6.2 mmHg; 95% CI –8.27 to -4.04) reported in a recent meta-
analysis of RT interventions in pre-hypertensive and hypertensive cohorts.101
Adverse Events
Six out of the seven studies reported on adverse events (AE), however, many
studies did not provide sufficient detail as to whether AEs were attributable to the
study interventions. Two studies reported no AEs,94 95 while Putri et al. (2012)96
reported no AEs for both active treatment arms (RT and YMRQ) but did not report
AEs for the control arm. Pibernik-Okanović et al. (2015)83 reported serious adverse
events, with four instances of critical disease (intervention group = 2;
psychoeducation group = 1; education only group = 1) and three instances of death
(intervention group = 2; education only group = 1), but did not state whether these
were related to the trial. Lincoln et al. (2011)81 reported (as per Castaneda et al.
(2002)102) 5 post-exercise hypoglycaemic events in the intervention group and 3
episodes of chest pain during exercise in subjects with coronary artery disease.
Additionally, 7 hypoglycaemic events were reported in the control group.
Mueller et al. (2013),82 reported 41 AEs in their study of individuals with T2DM and
peripheral neuropathy. Twenty-nine AEs (1 calf strain, 7 foot lesions, 1 foot ulcer,
and 20 occasions of pain requiring exercise modification) occurred in the weight
69
bearing exercise group, while 12 AEs occurred in the non-weight bearing exercise
group (6 foot lesions, 3 foot ulcers, and 3 occasions of pain requiring exercise
modification). Adverse event causality was only directly assigned to exercise for the
calf strain during treadmill walking. Frequency of skin lesions and ulcers were similar
between weight bearing (7 lesions, 1 ulcer) and non-weight bearing (6 lesions, 3
ulcers) groups. By contrast, instances of exercise modification or deferral due to pain
were far more frequent in the weight-bearing group (weight bearing = 12
modification, 8 deferrals; non-weight-bearing = 3 modifications, 0 deferrals). All
instances of pain requiring exercise modification or deferral were associated with the
aerobic exercise component in both groups, and no instances to the resistance
training component. A summary of AE reporting can be found in Table 11.
70
Discussion
The purpose of this paper was to review the literature on the efficacy of resistance
exercise training on depressive symptoms in adults with insulin resistance, whilst
concurrently examining the effect on markers of glucose homeostasis and insulin
resistance. Overall, the literature base is small and confined to adults with T2DM,
with no direct measures of insulin resistance, and without diagnoses of major
depressive disorder. Studies were of low-to-moderate quality and a moderate-to-high
risk of bias. From the limited data available, RT may be effective in the simultaneous
reduction of self-reported depressive symptoms and HbA1c levels in adults with
T2DM. As expected, larger effect sizes for reductions in depression and HbA1c were
observed in studies that used RT in isolation or combined with walking compared to
non-active control groups. Where studies employed active comparator groups, it may
be expected that between-group effect sizes would be reduced where both studies
received a therapeutic intervention. Across all study designs, interventions utilising
higher intensities and volumes of RT exercise show larger reductions in depressive
symptoms (Figures 4 and 5), with no dose-response effect seen for HbA1c (Figure 6
and 7). Therefore, from the limited available data, individuals with insulin resistance
and depressive symptoms may receive dual benefit from the use RT interventions
when used as a standalone therapy, with higher intensities and volumes potentially
eliciting greater therapeutic benefit for depressive symptoms.
The reduction in depressive symptoms is consistent with previous findings. In a
recent meta-analysis, a moderate effect size following resistance training (Hedges’ g

71
= 0.66; 95% CI 0.48-0.83) was reported, with smaller effect sizes when analyses
were restricted to individuals with physical illness (mean ES = 0.34; 95% CI 0.17-
0.52) or chronic disease (mean ES = 0.30; 95% CI 0.25-0.36).41 By comparison,
effect sizes in the present study ranged from g = -1.28 (95% CI -1.85, -0.72) to g = -
0.36 (95% CI -1.15, 0.44) when compared to an non-active control group, indicating
that the presence of insulin resistance (specifically T2DM) or the absence of a MDD
diagnosis does not preclude a therapeutic benefit from this modality of exercise. This
finding is of clinical significance given that 11.8% of individuals with metabolic
syndrome and 16.2% of individuals with T2DM are estimated to have MDD as a co-
morbidity.103 Similarly, the risk of incident depression is significantly greater in those
with metabolic syndrome (137% over 10 years; 95% CI 60% - 251%)22 and T2DM
(pooled relative risk 1.24; 95% CI 1.09 – 1.40).104 Current guidelines for the
management of existing or new mood disorders recommend lifestyle changes such
as regular exercise,105-108 however utilisation in clinical practice remains low.109
Despite the small body of evidence available, the current data show that the RT
presents as a suitable alternative modality of exercise for the management of
depression in cohorts with insulin resistance. This is particularly important as it
provides patients with choice and a sense of autonomy about the type of exercise
they can do, which are known to improve adherence and uptake.110-112 Perhaps the
strongest indication for why this modality of exercise is a suitable alternative comes
from the adverse events reporting, particularly from that by Mueller et al. (2013).82 In
this study, both groups performed identical intensities and volumes of aerobic and
resistance exercise, with individuals randomised to either weight bearing or non-
weight bearing exercise. While no difference was observed between groups for
depressive symptoms or HbA1c, adverse events were far more common amongst
72
the weight bearing group (21 in total) compared to the non-weight bearing group
(12), with all pain, missed sessions and modifications to exercise in both groups
being attributed to the aerobic exercise co-intervention. While adverse event
reporting in other studies was not as complete, where adverse events were reported,
there was no evidence for any harm from this modality of exercise, including studies
of high intensity programs in older adults,81 102 and is consistent with the low risk of
adverse events reported in other reviews of RT, including older adults.113 Clinically,
RT is the only mode of exercise that has been shown to increase muscle mass and
strength, as well as bone density.114 115 This is particularly important in the context of
ageing where these body composition compartments are known to decline, but also
during weight loss, where 25-35% of mass lost can come from lean tissue.57 116
Resistance training is therefore recommended as a safe and effective alternative
modality to aerobic exercise for treatment of depressive symptoms, particularly in
older adults or those who may have difficulty with ambulatory or impact exercises.
Overall, larger effect sizes were reported by studies with higher training intensities
and volumes. While this contrasts with the meta-analysis by Gordon et al. (2018)41
where no moderating effect of exercise intensity or volume was reported,
randomised controlled trials designed to test the dose-response effect of exercise
have shown greater reductions in depressive symptoms following higher intensities
of aerobic and resistance exercise,117-120 with similar effects observed with greater
volumes of aerobic exercise.121 In the current review, light-intensity RT was not
found to be different from YMRQ (similarly classified as light),96 however caution in
interpretation of the results are required due to the very small sample size (RT = 5,
YRMQ = 7), with the effect size calculated for light intensity RT (g = -0.86; 95% CI -

73
1.98 to 0.26); which was not different to YRMQ, two-times higher than a meta-
analysis of Tai Chi (g = -0.36; 95% CI -0.53 to -0.19) and Qigong (g = -0.38; 95% CI
-0.51 to 0.25) exercise on depressive symptoms.122 Nonetheless, these data suggest
that different modalities of exercise that are matched for intensity may produce
similar therapeutic benefit, consistent with results from Mueller et al. (2013) where
combined weight-bearing exercise was not different to combined non-weight bearing
exercise.82 However, given the known dose-response effect of high intensity RT on
depressive symptoms,117 and the known benefits of higher intensities of resistance
exercise on muscle strength and performance, as well as muscular hypertrophy and
bone density, particularly in the context of weight loss,67 68 123 higher intensity
programs should be utilised where possible.
Glycaemic outcomes in the retrieved studies were mostly restricted to HbA1c, with
only two studies reporting on fasting glucose, and none reporting any direct
measures of insulin resistance. When compared to non-active comparison groups,
RT was associated with clinically meaningful reductions in HbA1c, consistent with
previous reviews of exercise.51 56 124 However, in contrast to the findings with
depressive symptoms, the addition of RT to education or lifestyle-based
interventions did not provide added benefit. While the minimal data available do not
suggest any moderating effect of intensity or volume, previous meta-analyses found
additional benefit of higher intensity RT,52 56 while one observed benefit from greater
volume (>150 min/week total exercise volume as compared to <150 min/week).124
More recently, a meta-analysis by Liu et al. (2019) of 24 trials enrolling 962
participants with T2DM56 reported that intensities ≥ 75% 1RM were sufficient to
significantly reduce fasting insulin (MD = −4.60; p = 0.002), while intensities lower

74
than this did not produce a significant effect (MD = 0.07; p = 0.97), suggesting that
improvement in insulin sensitivity may only occur following higher intensity programs.
When results for depressive symptoms and metabolic outcomes are taken together,
there is a strong suggestion that simultaneous improvement of both outcomes is
possible through RT. This finding has strong clinical implications. Head-to-head trials
of aerobic exercise and sertraline have not found evidence of a differential effect
between exercise and pharmacotherapy,43 44 with both interventions similarly
beneficial when compared to placebo.43 44 Of note however, despite similar efficacy
between exercise and sertraline, participants were 20-times more likely to
discontinue treatment due to adverse effects from pharmacotherapy. Similarly, the
reduction in HbA1c following RT programs in this review (ranging from -1.0% to -
1.56% vs non-active control) or other meta-analyses (-0.37% to -0.62% in cohorts
with diabetes;52 56 124-126 -0.29% in one analyses of studies on pre-diabetic cohorts)51
are comparable to the effects of oral hypoglycaemic medication on HbA1c, such as
metformin (-1.13%), gliclazide (-1.37%),127 or thiazolidinediones (-1% to -1.5%).128
This brings to the forefront the potential for exercise, and specifically RT, as a way to
simultaneously improve mental and metabolic health outcomes, and potentially
reduce the burden of polypharmacy and drug-to-drug interactions with dually-afflicted
individuals. There is a clear bi-directional association between insulin resistance and
depression which can be explained by shared biological pathways. Dysregulation of
the hypothalamic-pituitary-adrenal (HPA) axis, elevated cytokines and decreased
brain-derived neurotrophic factor (BDNF) are all present in both depression and
obesity,129-132 and are also associated with the development of insulin resistance85
133-136 and impaired glucose tolerance.130 Importantly, exercise, including RT, has

75
been shown to favourably modify these pathways.137-140 However, evidence that
improvements in these pathways translates directly to an improvement in depressive
symptoms is inconclusive,141 and so the role of these biological pathways, and
others, remains unclear and further research is warranted to better understand the
mechanisms by which exercise can improve depressive and metabolic outcomes.
There are numerous limitations to the current literature that should be addressed in
future studies. None of the included studies specifically recruited individuals with
MDD. Rather, participants across studies ranged from having minimal symptom
severity, with one study including individuals with subsyndromal depression, while
one study recruited participants with symptoms clinically indicative of MDD. It is well
documented that the effect of exercise is greater in individuals with higher
depressive symptoms,41 42 44 or where depression is the primary outcome.41 Perhaps
of greater concern is that all measures of depressive symptoms in the included
studies are self-reported measures, where participants themselves are considered
the assessor. Given the difficulties of blinding participants to an intervention, the use
of self-reported scales means blinding of participants (and therefore the assessor) is
not possible, and so findings from this review should be interpreted with appropriate
caution. Well-powered studies that intentionally recruit individuals with insulin
resistance and MDD that also use a clinical assessment of symptoms such as the
Hamilton Rating Scale for Depression are warranted. Furthermore, cohorts with
insulin resistance were confined to individuals with T2DM, with no direct measures of
insulin resistance such as HOMA-IR or hyperinsulinaemic-euglycaemic clamp, and
glycaemic outcomes mostly restricted to HbA1c. Given the association between
MDD and worsening insulin resistance prospectively, studies in cohorts with earlier

76
stages of disease such as impaired fasting glucose, impaired glucose tolerance and
metabolic syndrome are warranted, with the inclusion of more diverse measures of
insulin resistance and glucose homeostasis. Similarly, the assessment of other
cardiometabolic risk factors in the present studies is minimal with only two studies
reporting on fasting glucose, four studies reporting on lipid outcomes, one study on
blood pressure, and no studies providing data on waist circumference, all
components of the diagnostic criteria for metabolic syndrome from the International
Diabetes Federation75 or the Adult Treatment Panel III criteria.142 Finally, studies that
combined exercise modalities, or combined exercise with other therapeutic
interventions, do not allow us to isolate the effect of RT. With only 3 of the included
studies prescribing RT in isolation,80 81 96 this limits the certainty of our analysis.
There are a few limitations of this review that warrant consideration. The search was
restricted to articles in peer reviewed journals and did not include grey literature such
as preprints and student theses. Thus, the outcomes presented in this review may
subject to publication bias, particularly with the small number found to be eligible.
Title, abstract, and full-text screening were performed by one author, which
increases the possibility that relevant articles may have been excluded. Furthermore,
due to the low number of eligible studies, a decision was made to include studies
with co-interventions (including aerobic exercise) and active comparison groups.
Thus, interpreting the isolated effect of RT on depressive symptoms in individuals
with T2DM must be done with caution. However, in the few studies where studies
were done in isolation, the efficacy of RT appears consistent with meta-analyses of
effect of RT across all studies where depression was measured. Data were extracted
from figures in one study96 using Webplotdigitizer.87 While technique in using this
77
tool was agreed on between researchers, these data points were not independently
verified and therefore subject to greater error.
In conclusion, the limited data available suggests that RT is an effective standalone
intervention to simultaneously reduce depressive symptoms and HbA1c in
individuals with depressive symptoms and insulin resistance. However, the literature
is confined to a small number of low-quality studies which do not measure insulin
resistance directly, with cohorts of individuals with T2DM who do not have diagnosed
MDD. Therefore, future, well designed studies are required, and caution should be
taken in the interpretation of these findings.

78
References
1. Wilcox G. Insulin and insulin resistance. The Clinical Biochemist Reviews
2005;26(2):19-39.
2. Reaven GM. The insulin resistance syndrome: Definition and dietary approaches
to treatment. Annual Review of Nutrition 2005;25(1):391-406. doi:
https://doi.org/10.1146/annurev.nutr.24.012003.132155
3. Petersen MC, Shulman GI. Mechanisms of insulin action and insulin resistance.
Physiological Reviews 2018;98(4):2133-223. doi:
https://doi.org/10.1152/physrev.00063.2017
4. Cefalu WT. Insulin resistance: Cellular and clinical concepts. Experimental Biology
and Medicine 2001;226(1):13-26. doi:
https://doi.org/10.1177/153537020122600103 [published Online First:
2001/05/23]
5. Abdul-Ghani MA, Tripathy D, DeFronzo RA. Contributions of beta-cell dysfunction
and insulin resistance to the pathogenesis of impaired glucose tolerance and
impaired fasting glucose. Diabetes Care 2006;29(5):1130-9. doi:
https://doi.org/10.2337/dc05-2179 [published Online First: 2006/04/29]
6. Roberts CK, Hevener AL, Barnard RJ. Metabolic syndrome and insulin resistance:
Underlying causes and modification by exercise training. Comprehensive
Physiology 2013;3(1):1-58. doi: https://doi.org/10.1002/cphy.c110062
7. Banday MZ, Sameer AS, Nissar S. Pathophysiology of diabetes: An overview.
Avicenna Journal of Medicine 2020;10(4):174-88. doi:
https://doi.org/10.4103/ajm.ajm_53_20
79
8. Tenenbaum A, Adler Y, Boyko V, et al. Insulin resistance is associated with
increased risk of major cardiovascular events in patients with preexisting
coronary artery disease. American Heart Journal 2007;153(4):559-65. doi:
https://doi.org/10.1016/j.ahj.2007.01.008
9. Haffner SM, Miettinen H, Gaskill SP, et al. Metabolic precursors of hypertension:
The San Antonio heart study. Archives of Internal Medicine
1996;156(17):1994-2001. doi:
https://doi.org/10.1001/archinte.1996.00440160106013
10. Petrie JR, Guzik TJ, Touyz RM. Diabetes, hypertension, and cardiovascular
disease: Clinical insights and vascular mechanisms. The Canadian Journal of
Cardiology 2018;34(5):575-84. doi: https://doi.org/10.1016/j.cjca.2017.12.005
[published Online First: 2017/12/11]
11. Emerging Risk Factors Collaboration, Sarwar N, Gao P, et al. Diabetes mellitus,
fasting blood glucose concentration, and risk of vascular disease: a
collaborative meta-analysis of 102 prospective studies. Lancet
2010;375(9733):2215-22. doi: https://doi.org/10.1016/S0140-6736(10)60484-9
12. Wang W, Lo ACY. Diabetic retinopathy: Pathophysiology and treatments.
International Journal of Molecular Sciences 2018;19(6):1816. doi:
https://doi.org/10.3390/ijms19061816
13. Callaghan BC, Cheng HT, Stables CL, et al. Diabetic neuropathy: Clinical
manifestations and current treatments. The Lancet Neurology 2012;11(6):521-
34. doi: https://doi.org/10.1016/S1474-4422(12)70065-0 [published Online
First: 2012/05/16]
14. Stephens JW, Brown KE, Min T. Chronic kidney disease in type 2 diabetes:
Implications for managing glycaemic control, cardiovascular and renal risk.
80
Diabetes, Obesity and Metabolism 2020;22(S1):32-45. doi:
https://doi.org/10.1111/dom.13942
15. Thiruvoipati T, Kielhorn CE, Armstrong EJ. Peripheral artery disease in patients
with diabetes: Epidemiology, mechanisms, and outcomes. World Journal of
Diabetes 2015;6(7):961-69. doi: https://doi.org/10.4239/wjd.v6.i7.961
16. Ferreira LSS, Fernandes CS, Vieira MNN, et al. Insulin resistance in Alzheimer's
disease. Frontiers in Neuroscience 2018;12:830-30. doi:
https://doi.org/10.3389/fnins.2018.00830
17. Cholerton B, Baker LD, Montine TJ, et al. Type 2 diabetes, cognition, and
dementia in older adults: Toward a precision health approach. Diabetes
Spectrum :A Publication of the American Diabetes Association
2016;29(4):210-19. doi: https://doi.org/10.2337/ds16-0041
18. Tomasik J, Lago SG, Vázquez-Bourgon J, et al. Association of insulin resistance
with schizophrenia polygenic risk score and response to antipsychotic
treatment. JAMA Psychiatry 2019;76(8):864-67. doi:
https://doi.org/10.1001/jamapsychiatry.2019.0304
19. Andrade C. Cardiometabolic risks in schizophrenia and directions for
intervention, 1: Magnitude and moderators of the problem. Journal of Clinicial
Psychiatry 2016;77(7):e844-7. doi: https://doi.org/10.4088/JCP.16f10997
[published Online First: 2016/07/28]
20. Lyra E Silva NdM, Lam MP, Soares CN, et al. Insulin resistance as a shared
pathogenic mechanism between depression and type 2 diabetes. Frontiers in
Psychiatry 2019;10:57-57. doi: https://doi.org/10.3389/fpsyt.2019.00057
81
21. Golden SH, Lazo M, Carnethon M, et al. Examining a bidirectional association
between depressive symptoms and diabetes. Journal of the American Medical
Association 2008;299(23):2751-59. doi: https://10.1001/jama.299.23.2751
22. Almeida OP, Calver J, Jamrozik K, et al. Obesity and metabolic syndrome
increase the risk of incident depression in older men: The health in men study.
The American Journal of Geriatric Psychiatry 2009;17(10):889-98. doi:
https://doi.org/10.1097/JGP.0b013e3181b047e3
23. Mezuk B, Eaton WW, Albrecht S, et al. Depression and type 2 diabetes over the
lifespan: A meta-analysis. Diabetes Care 2008;31(12):2383-90. doi:
https://doi.org/10.2337/dc08-0985
24. Schmitz N, Deschenes SS, Burns RJ, et al. Depression and risk of type 2
diabetes: The potential role of metabolic factors. Molecular Psychiatry
2016;21(12):1726-32. doi: https://doi.org/10.1038/mp.2016.7 [published
Online First: 2016/02/24]
25. Nouwen A, Adriaanse MC, van Dam K, et al. Longitudinal associations between
depression and diabetes complications: a systematic review and meta-
analysis. Diabetic Medicine 2019;36(12):1562-72. doi:
https://doi.org/10.1111/dme.14054
26. Guerrero Fernández de Alba I, Gimeno-Miguel A, Poblador-Plou B, et al.
Association between mental health comorbidity and health outcomes in type 2
diabetes mellitus patients. Scientific Reports 2020;10(1):19583. doi:
https://doi.org/10.1038/s41598-020-76546-9
27. Farooqi A, Khunti K, Abner S, et al. Comorbid depression and risk of cardiac
events and cardiac mortality in people with diabetes: A systematic review and
82
meta-analysis. Diabetes Research and Clinical Practice 2019;156:107816.
doi: https://doi.org/10.1016/j.diabres.2019.107816
28. Lebovitz HE. Thiazolidinediones: The forgotten diabetes medications. Current
Diabetes Reports 2019;19(12):151-51. doi: https://doi.org/10.1007/s11892-
019-1270-y
29. Duval F, Lebowitz BD, Macher J-P. Treatments in depression. Dialogues in
Clinical Neuroscience 2006;8(2):191-206. doi:
https://doi.org/10.31887/DCNS.2006.8.2/fduval
30. Nguyen Q, Dominguez J, Nguyen L, et al. Hypertension management: An
update. American Health & Drug Benefits 2010;3(1):47-56.
31. Dobrică E-C, Găman M-A, Cozma M-A, et al. Polypharmacy in type 2 diabetes
mellitus: Insights from an internal medicine department. Medicina
2019;55(8):436. doi: https://doi.org/10.3390/medicina55080436
32. Ammassari A, Trotta MP, Murri R, et al. Correlates and predictors of adherence
to highly active antiretroviral therapy: Overview of published literature. Journal
of Acquired Immune Deficiency Syndromes 2002;31:s123-27. doi:
https://doi.org/10.1097/00126334-200212153-00007
33. Austin RP. Polypharmacy as a risk factor in the treatment of type 2 diabetes.
Diabetes Spectrum 2006;19(1):13. doi:
https://doi.org/10.2337/diaspect.19.1.13
34. Si T, Wang P. When is antidepressant polypharmacy appropriate in the
treatment of depression? Shanghai Archives of Psychiatry 2014;26(6):357-59.
doi: https://doi.org/10.11919/j.issn.1002-0829.214152
35. Holten MK, Zacho M, Gaster M, et al. Strength training increases insulin-
mediated glucose uptake, GLUT4 content, and insulin signaling in skeletal

83
muscle in patients with type 2 diabetes. Diabetes 2004;53(2):294. doi:
https://doi.org/10.2337/diabetes.53.2.294
36. Little JP, Gillen JB, Percival ME, et al. Low-volume high-intensity interval training
reduces hyperglycemia and increases muscle mitochondrial capacity in
patients with type 2 diabetes. Journal of Applied Physiology
2011;111(6):1554-60. doi: https://doi.org/10.1152/japplphysiol.00921.2011
37. Hussey SE, McGee SL, Garnham A, et al. Exercise training increases adipose
tissue GLUT4 expression in patients with type 2 diabetes. Diabetes, Obesity
and Metabolism 2011;13(10):959-62. doi: https://doi.org/10.1111/j.1463-
1326.2011.01426.x
38. Dela F, Ploug T, Handberg A, et al. Physical training increases muscle GLUT4
protein and mRNA in patients with NIDDM. Diabetes 1994;43(7):862. doi:
https://doi.org/10.2337/diab.43.7.862
39. Sabag A, Way KL, Keating SE, et al. Exercise and ectopic fat in type 2 diabetes:
A systematic review and meta-analysis. Diabetes & Metabolism
2017;43(3):195-210. doi: https://doi.org/10.1016/j.diabet.2016.12.006
40. Pan B, Ge L, Xun YQ, et al. Exercise training modalities in patients with type 2
diabetes mellitus: A systematic review and network meta-analysis.
International Journal of Behavioral Nutrition and Physical Activity
2018;15(1):72. doi: https://doi.org/10.1186/s12966-018-0703-3 [published
Online First: 2018/07/27]
41. Gordon BR, McDowell CP, Hallgren M, et al. Association of efficacy of resistance
exercise training with depressive symptoms: Meta-analysis and meta-
regression analysis of randomized clinical trials. JAMA Psychiatry
2018;75(6):566-76. doi: https://doi.org/10.1001/jamapsychiatry.2018.0572
84
42. Herring MP, Puetz TW, O’Connor PJ, et al. Effect of exercise training on
depressive symptoms among patients with a chronic illness: A systematic
review and meta-analysis of randomized controlled trials. Archives of Internal
Medicine 2012;172(2):101-11. doi:
https://doi.org/10.1001/archinternmed.2011.696
43. Blumenthal JA, Babyak MA, Doraiswamy PM, et al. Exercise and
pharmacotherapy in the treatment of major depressive disorder.
Psychosomatic Medicine 2007;69(7):587-96. doi:
https://doi.org/10.1097/PSY.0b013e318148c19a [published Online First:
2007/09/10]
44. Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older
patients with major depression. Archives of Internal Medicine
1999;159(19):2349-56. doi: https://doi.org/10.1001/archinte.159.19.2349
[published Online First: 1999/11/05]
45. Blumenthal JA, Babyak MA, O’Connor C, et al. Effects of exercise training on
depressive symptoms in patients with chronic heart failure: The HF-ACTION
randomized trial. Journal of the American Medical Association
2012;308(5):465-74. doi: https://doi.org/10.1001/jama.2012.8720
46. Strasser B, Schobersberger W. Evidence for resistance training as a treatment
therapy in obesity. Journal of Obesity 2011;2011:482564. doi:
https://doi.org/10.1155/2011/482564 [published Online First: 2010/08/10]
47. Li Y, Su Y, Chen S, et al. The effects of resistance exercise in patients with knee
osteoarthritis: A systematic review and meta-analysis. Clinical Rehabilitation
2016;30(10):947-59. doi: https://doi.org/10.1177/0269215515610039
[published Online First: 2015/10/17]
85
48. Lange AK, Vanwanseele B, Fiatarone singh MA. Strength training for treatment
of osteoarthritis of the knee: A systematic review. Arthritis Care & Research
2008;59(10):1488-94. doi: https://doi.org/10.1002/art.24118
49. Tofthagen C, Visovsky C, Berry DL. Strength and balance training for adults with
peripheral neuropathy and high risk of fall: Current evidence and implications
for future research. Oncology Nursing Forum 2012;39(5):E416-24. doi:
https://doi.org/10.1188/12.Onf.E416-e424 [published Online First: 2012/09/04]
50. Parmenter BJ, Mavros Y, Ritti Dias R, et al. Resistance training as a treatment
for older persons with peripheral artery disease: A systematic review and
meta-analysis. British Journal of Sports Medicine 2020;54(8):452. doi:
https://doi.org/10.1136/bjsports-2018-100205
51. Qadir R, Sculthorpe NF, Todd T, et al. Effectiveness of resistance training and
associated program characteristics in patients at risk for type 2 diabetes: A
systematic review and meta-analysis. Sports Medicine - Open 2021;7(1):38.
doi: https://doi.org/10.1186/s40798-021-00321-x
52. Acosta-Manzano P, Rodriguez-Ayllon M, Acosta FM, et al. Beyond general
resistance training. Hypertrophy versus muscular endurance training as
therapeutic interventions in adults with type 2 diabetes mellitus: A systematic
review and meta-analysis. Obesity Reviews 2020;21(6):e13007. doi:
https://doi.org/10.1111/obr.13007 [published Online First: 2020/02/19]
53. Moraes HS, Silveira HS, Oliveira NA, et al. Is strength training as effective as
aerobic training for depression in older adults? A randomized controlled trial.
Neuropsychobiology 2020;79(2):141-49. doi:
https://doi.org/10.1159/000503750
86
54. Singh NA, Clements KM, Fiatarone MA. A randomized controlled trial of
progressive resistance training in depressed elders. Journals of Gerontology
Series a-Biological Sciences and Medical Sciences 1997;52(1):M27-M35. doi:
https://doi.org/10.1093/gerona/52A.1.M27
55. Black LE, Swan PD, Alvar BA. Effects of intensity and volume on insulin
sensitivity during acute bouts of resistance training. The Journal of Strength
and Conditioning Research 2010;24(4):1109-16. doi:
https://doi.org/10.1519/JSC.0b013e3181cbab6d [published Online First:
2010/01/23]
56. Liu Y, Ye W, Chen Q, et al. Resistance exercise intensity is correlated with
attenuation of HbA1c and insulin in patients with type 2 diabetes: A systematic
review and meta-Analysis. International Journal of Environmental Research
and Public Health 2019;16(1):140. doi: https://doi.org/10.3390/ijerph16010140
57. Dixon JB, Lambert EA, Grima M, et al. Fat-free mass loss generated with weight
loss in overweight and obese adults: What may we expect? Diabetes, Obesity
and Metabolism 2015;17(1):91-93. doi: https://doi.org/10.1111/dom.12389
58. Seimon RV, Wild-Taylor AL, Keating SE, et al. Effect of weight loss via severe vs
moderate energy restriction on lean mass and body composition among
postmenopausal women with obesity: The TEMPO diet randomized clinical
trial. JAMA Network Open 2019;2(10):e1913733-e33. doi:
https://doi.org/10.1001/jamanetworkopen.2019.13733
59. Hirani V, Blyth F, Naganathan V, et al. Sarcopenia is associated with incident
disability, institutionalization, and mortality in community-dwelling older men:
The concord health and ageing in men project. Journal of the American
Medical Directors Association 2015;16(7):607-13. doi:
87
https://doi.org/10.1016/j.jamda.2015.02.006 [published Online First:
2015/03/31]
60. Yeung SSY, Reijnierse EM, Pham VK, et al. Sarcopenia and its association with
falls and fractures in older adults: A systematic review and meta-analysis.
Journal of Cachexia, Sarcopenia and Muscle 2019;10(3):485-500. doi:
https://doi.org/10.1002/jcsm.12411 [published Online First: 2019/04/16]
61. Greco EA, Pietschmann P, Migliaccio S. Osteoporosis and sarcopenia increase
frailty syndrome in the elderly. Frontiers in Endocrinology 2019;10:255-55.
doi: https://doi.org/10.3389/fendo.2019.00255
62. Bryner RW, Ullrich IH, Sauers J, et al. Effects of resistance vs. aerobic training
combined with an 800 calorie liquid diet on lean body mass and resting
metabolic rate. Journal of the American College of Nutrition 1999;18(2):115-
21. doi: https://doi.org/10.1080/07315724.1999.10718838
63. Hamilton KC, Fisher G, Roy JL, et al. The effects of weight loss on relative bone
mineral density in premenopausal women. Obesity 2013;21(3):441-48. doi:
https://doi.org/10.1002/oby.20052
64. Bouchard DR, Soucy L, Sénéchal M, et al. Impact of resistance training with or
without caloric restriction on physical capacity in obese older women.
Menopause 2009;16(1)
65. Armamento-Villareal R, Aguirre L, Napoli N, et al. Changes in thigh muscle
volume predict bone mineral density response to lifestyle therapy in frail,
obese older adults. Osteoporosis International 2014;25(2):551-58. doi:
https://doi.org/10.1007/s00198-013-2450-2 [published Online First:
2013/07/27]
88
66. Villareal DT, Chode S, Parimi N, et al. Weight loss, exercise, or both and
physical function in obese older adults. The New England Journal of Medicine
2011;364(13):1218-29. doi: https://doi.org/10.1056/NEJMoa1008234
67. Dunstan DW, Daly RM, Owen N, et al. High-intensity resistance training
improves glycemic control in older patients with type 2 diabetes. Diabetes
Care 2002;25(10):1729-36. doi: https://doi.org/10.2337/diacare.25.10.1729
68. Daly RM, Dunstan DW, Owen N, et al. Does high-intensity resistance training
maintain bone mass during moderate weight loss in older overweight adults
with type 2 diabetes? Osteoporosis International 2005;16(12):1703-12. doi:
https://doi.org/10.1007/s00198-005-1906-4
69. Prospero international prospective register of systematic reviews: University of
York; [Available from:
https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=160903.
70. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: An
updated guideline for reporting systematic reviews. BMJ (Clinical research ed)
2021;372:n71-n71. doi: https://doi.org/10.1136/bmj.n71
71. Rethlefsen ML, Kirtley S, Waffenschmidt S, et al. PRISMA-S: An extension to the
PRISMA statement for reporting literature searches in systematic reviews.
Systematic Reviews 2021;10(1):39. doi: https://doi.org/10.1186/s13643-020-
01542-z
72. Veritas Health Innovation. Covidence systematic review software. Melbourne,
Australia:www.covidence.org.
73. Balkau B, Charles MA. Comment on the provisional report from the WHO
consultation. European Group for the Study of Insulin Resistance (EGIR).
89
Diabetic Medicine 1999;16(5):442-3. doi: 10.1046/j.1464-5491.1999.00059.x
[published Online First: 1999/05/26]
74. Einhorn D, Reaven GM, Cobin RH, et al. American College of Endocrinology
position statement on the insulin resistance syndrome. Endocrine Practice
2003;9(3):237-52. [published Online First: 2003/08/20]
75. Alberti KGMM, Zimmet P, Shaw J. Metabolic syndrome—a new world-wide
definition. A consensus statement from the International Diabetes Federation.
Diabetic Medicine 2006;23(5):469-80. doi: https://doi.org/10.1111/j.1464-
5491.2006.01858.x
76. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes
mellitus and its complications. Part 1: diagnosis and classification of diabetes
mellitus provisional report of a WHO consultation. Diabetic Medicine
1998;15(7):539-53. doi: https://doi.org/10.1002/(sici)1096-
9136(199807)15:7<539::Aid-dia668>3.0.Co;2-s [published Online First:
1998/08/01]
77. Executive Summary of The Third Report of The National Cholesterol Education
Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of
High Blood Cholesterol In Adults (Adult Treatment Panel III). Journal of the
American Medical Association 2001;285(19):2486-97. doi:
https://doi.org/10.1001/jama.285.19.2486 [published Online First: 2001/05/23]
78. Garber CE, Blissmer B, Deschenes MR, et al. Quantity and quality of exercise for
developing and maintaining cardiorespiratory, musculoskeletal, and
neuromotor fitness in apparently healthy adults: Guidance for prescribing
exercise. Medicine & Science in Sports & Exercise 2011;43(7) doi:
https://doi.org/10.1249/MSS.0b013e318213fefb
90
79. Slade SC, Dionne CE, Underwood M, et al. Consensus on Exercise Reporting
Template (CERT): Explanation and elaboration statement. British Journal of
Sports Medicine 2016;50(23):1428-37. doi: https://doi.org/10.1136/bjsports-
2016-096651 [published Online First: 2016/10/07]
80. Duruturk N, Ozkoslu MA. Effect of tele-rehabilitation on glucose control, exercise
capacity, physical fitness, muscle strength and psychosocial status in patients
with type 2 diabetes: A double blind randomized controlled trial. Primary Care
Diabetes 2019;13(6):542-48. doi: https://doi.org/10.1016/j.pcd.2019.03.007
[published Online First: 2019/04/25]
81. Lincoln AK, Shepherd A, Johnson PL, et al. The impact of resistance exercise
training on the mental health of older Puerto Rican adults with type 2
diabetes. The Journals of Gerontology, Series B: Psychological Sciences and
Social Sciences 2011;66(5):567-70. doi:
https://doi.org//10.1093/geronb/gbr034 [published Online First: 2011/05/17]
82. Mueller MJ, Tuttle LJ, Lemaster JW, et al. Weight-bearing versus nonweight-
bearing exercise for persons with diabetes and peripheral neuropathy: A
randomized controlled trial. Archives of Physical Medicine and Rehabilitation
2013;94(5):829-38. doi: https://doi.org/10.1016/j.apmr.2012.12.015 [published
Online First: 2013/01/02]
83. Pibernik-Okanovic M, Hermanns N, Ajdukovic D, et al. Does treatment of
subsyndromal depression improve depression-related and diabetes-related
outcomes? A randomised controlled comparison of psychoeducation, physical
exercise and enhanced treatment as usual. Trials 2015;16:305. doi:
https://doi.org/10.1186/s13063-015-0833-8 [published Online First:
2015/07/16]

91
84. Sterne J, Savović J, Page M, et al. RoB 2: A revised tool for assessing risk of
bias in randomised trials. BMJ 2019;3666 doi:
https://doi.org/10.1136/bmj.l4898
85. Akash MSH, Rehman K, Liaqat A. Tumor necrosis factor-alpha: Role in
development of insulin resistance and pathogenesis of type 2 diabetes
mellitus. Journal of Cellular Biochemistry 2018;119(1):105-10. doi:
https://doi.org/10.1002/jcb.26174
86. American College of Sports Medicine. Progression models in resistance training
for healthy adults. Medicine & Science in Sports & Exercise 2009;41(3) doi:
https://doi.org/10.1249/MSS.0b013e3181915670
87. Rohatgi A. WebPlotDigitizer. Pacifica, California, USA, 2020.
88. Higgins J, Li T, Deeks J. Chapter 6: Choosing effect measures and computing
estimates of effect. In: Higgins J, Thomas J, Chandler J, et al., eds. Cochrane
Handbook for Systematic Reviews of Interventions: Cochrane 2021.
89. Morris SB. Estimating effect sizes from pretest-posttest-control group designs.
Organizational Research Methods 2007;11(2):364-86. doi:
https://doi.org/10.1177/1094428106291059
90. Morris SB, DeShon RP. Combining effect size estimates in meta-analysis with
repeated measures and independent-groups designs. Psychological Methods
2002;7(1):105-25. doi: https://doi.org/10.1037/1082-989X.7.1.105
91. Yucel H, Uysal Ö. Pilates-based mat exercises and parameters of quality of life
in women with type 2 diabetes. Iranian Red Crescent Medical Journal
2016;Inpress doi: https://doi.org/10.5812/ircmj.21919
92. Asa C, Maria S, Katharina SS, et al. Aquatic exercise is effective in improving
exercise performance in patients with heart failure and type 2 diabetes

92
mellitus. Evidence-Based Complementary Alternative Medicine
2012;2012:349209. doi: https://doi.org/10.1155/2012/349209 [published
Online First: 2012/05/18]
93. Nam S, Dobrosielski DA, Stewart KJ. Predictors of exercise intervention dropout
in sedentary individuals with type 2 diabetes. Journal of Cardiopulmonary
Rehabilitation and Prevention 2012;32(6):370-8. doi:
https://doi.org/10.1097/HCR.0b013e31826be485 [published Online First:
2012/09/27]
94. Aylin K, Arzu D, Sabri S, et al. The effect of combined resistance and home-
based walking exercise in type 2 diabetes patients. Internation Journal of
Diabetes in Developing Countries 2009;29(4):159-65. doi:
https://doi.org/10.4103/0973-3930.57347 [published Online First: 2010/03/26]
95. Leehey DJ, Collins E, Kramer HJ, et al. Structured exercise in obese diabetic
patients with chronic kidney disease: A randomized controlled trial. American
Journal of Nephrology 2016;44(1):54-62. doi:
https://doi.org/10.1159/000447703 [published Online First: 2016/07/08]
96. Putiri AL, Lovejoy JC, Gillham S, et al. Psychological effects of yi ren medical
qigong and progressive resistance training in adults with type 2 diabetes
mellitus: A randomized controlled pilot study. Alternative Therapies
2012;18(1):30-34.
97. Sun G-C, Lovejoy JC, Bradley R. Effects of qigong on type 2 diabetic patients
2008 [updated January. Available from:
https://ClinicalTrials.gov/show/NCT00885846.
98. Banerjee M, Macdougall M, Lakhdar AF. Impact of a single one-to-one education
session on glycemic control in patients with diabetes. Journal of Diabetes

93
2012;4(2):186-90. doi: https://doi.org/10.1111/j.1753-0407.2011.00178.x
[published Online First: 2011/12/20]
99. Little RR, Rohlfing CL, Sacks DB, et al. Status of hemoglobin A1c measurement
and goals for improvement: From chaos to order for improving diabetes care.
Clinical Chemistry 2011;57(2):205-14. doi:
https://doi.org/10.1373/clinchem.2010.148841
100. Wu J, Kraja AT, Oberman A, et al. A summary of the effects of antihypertensive
medications on measured blood pressure. American Journal of Hypertension
2005;18(7):935-42. doi: https://doi.org/10.1016/j.amjhyper.2005.01.011
101. Abrahin O, Moraes-Ferreira R, Cortinhas-Alves EA, et al. Is resistance training
alone an antihypertensive therapy? A meta-analysis. Journal of Human
Hypertension 2021;35(9):769-75. doi: https://doi.org/10.1038/s41371-021-
00582-9
102. Castaneda C, Layne JE, Munoz-Orians L, et al. A randomized controlled trial of
resistance exercise training to improve glycemic control in older adults with
type 2 diabetes. Diabetes Care 2002;25(12):2335-41. doi:
https://doi.org/10.2337/diacare.25.12.2335 [published Online First:
2002/11/28]
103. Tanamas S, Magliano D, Lynch V, et al. AusDiab 2012: The Australian
diabetes, obesity and lifestyle study Baker IDI: Heart and Diabetes Institute
2013
104. Nouwen A, Winkley K, Twisk J, et al. Type 2 diabetes mellitus as a risk factor
for the onset of depression: A systematic review and meta-analysis.
Diabetologia 2010;53(12):2480-86. doi: https://doi.org/10.1007/s00125-010-
1874-x [published Online First: 2010/08/14]
94
105. Gelenberg AJ, Freeman MP, Markowitz JC, et al. Practice guideline for the
treatment of patients with Major Depressive Disorder. American Psychiatric
Association
2010(3):17-38.
106. Malhi GS, Bell E, Singh AB, et al. The 2020 Royal Australian and New Zealand
College of Psychiatrists clinical practice guidelines for mood disorders: Major
depression summary. Bipolar Disorders 2020;22(8):788-804. doi:
https://doi.org/10.1111/bdi.13035
107. Ravindran AV, Balneaves LG, Faulkner G, et al. Canadian Network for Mood
and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the
management of adults with major depressive disorder: Section 5.
complementary and alternative medicine treatments. The Canadian Journal of
Psychiatry 2016;61(9):576-87. doi:
https://doi.org/10.1177/0706743716660290
108. Stubbs B, Vancampfort D, Hallgren M, et al. EPA guidance on physical activity
as a treatment for severe mental illness: a meta-review of the evidence and
Position Statement from the European Psychiatric Association (EPA),
supported by the International Organization of Physical Therapists in Mental
Health (IOPTMH). European Psychiatry 2018;54:124-44. doi:
https://doi.org/10.1016/j.eurpsy.2018.07.004 [published Online First:
2018/07/18]
109. Ekkekakis P. Why is exercise underutilized in clinical practice despite evidence
it is effective? Lessons in pragmatism from the inclusion of exercise in
guidelines for the treatment of depression in the British National Health
95
Service. Kinesiology Review 2021;10(1):29-50. doi:
https://doi.org/10.1123/kr.2020-0036
110. Silva MN, Vieira PN, Coutinho SR, et al. Using self-determination theory to
promote physical activity and weight control: A randomized controlled trial in
women. Journal of Behavioral Medicine 2010;33(2):110-22. doi:
https://doi.org/10.1007/s10865-009-9239-y
111. Silva MN, Markland D, CarraÇA EV, et al. Exercise autonomous motivation
predicts 3-yr weight loss in women. Medicine & Science in Sports & Exercise
2011;43(4)
112. Mata J, Silva MN, Vieira PN, et al. Motivational “spill-over” during weight
control: Increased self-determination and exercise intrinsic motivation predict
eating self-regulation. Health Psychology 2009;28(6):709-16. doi:
https://doi.org/10.1037/a0016764
113. Liu CJ, Latham N. Adverse events reported in progressive resistance strength
training trials in older adults: 2 sides of a coin. Archives of Physical Medicine
and Rehabilitation 2010;91(9):1471-3. doi:
https://doi.org/10.1016/j.apmr.2010.06.001 [published Online First:
2010/08/31]
114. Grgic J, McLlvenna LC, Fyfe JJ, et al. Does aerobic training promote the same
skeletal muscle hypertrophy as resistance training? A systematic review and
meta-analysis. Sports Medicine 2019;49(2):233-54. doi:
https://doi.org/10.1007/s40279-018-1008-z [published Online First:
2018/10/21]
115. Armamento-Villareal R, Aguirre L, Waters DL, et al. Effect of aerobic or
resistance exercise, or both, on bone mineral density and bone metabolism in

96
obese older adults while dieting: A randomized controlled trial. Journal of
Bone and Mineral Research 2020;35(3):430-39. doi:
https://doi.org/10.1002/jbmr.3905
116. Weinheimer EM, Sands LP, Campbell WW. A systematic review of the separate
and combined effects of energy restriction and exercise on fat-free mass in
middle-aged and older adults: implications for sarcopenic obesity. Nutrition
Reviews 2010;68(7):375-88. doi: https://doi.org/10.1111/j.1753-
4887.2010.00298.x [published Online First: 2010/07/02]
117. Singh NA, Stavrinos TM, Scarbek Y, et al. A randomized controlled trial of high
versus low intensity weight training Versus general practitioner care for clinical
depression in older adults. The Journals of Gerontology: Series A
2005;60(6):768-76. doi: https://doi.org/10.1093/gerona/60.6.768
118. Helgadóttir B, Forsell Y, Hallgren M, et al. Long-term effects of exercise at
different intensity levels on depression: A randomized controlled trial.
Preventive Medicine 2017;105:37-46. doi:
https://doi.org/10.1016/j.ypmed.2017.08.008 [published Online First:
2017/08/22]
119. Nebiker L, Lichtenstein E, Minghetti A, et al. Moderating effects of exercise
duration and intensity in neuromuscular vs. endurance exercise interventions
for the treatment of depression: A meta-analytical review. Frontiers in
Psychiatry 2018;9:305-05. doi: https://doi.org/10.3389/fpsyt.2018.00305
120. Schuch FB, Vancampfort D, Richards J, et al. Exercise as a treatment for
depression: A meta-analysis adjusting for publication bias. Journal of
Psychiatric Research 2016;77:42-51. doi:

97
https://doi.org/10.1016/j.jpsychires.2016.02.023 [published Online First:
2016/03/16]
121. Dunn AL, Trivedi MH, Kampert JB, et al. Exercise treatment for depression:
Efficacy and dose response. American Journal of Preventive Medicine
2005;28(1):1-8. doi: https://doi.org/10.1016/j.amepre.2004.09.003
122. Yin J, Dishman RK. The effect of Tai Chi and Qigong practice on depression
and anxiety symptoms: A systematic review and meta-regression analysis of
randomized controlled trials. Mental Health and Physical Activity
2014;7(3):135-46. doi: https://doi.org/10.1016/j.mhpa.2014.08.001
123. Dunstan DW, Daly RM, Owen N, et al. Home-based resistance training is not
sufficient to maintain improved glycemic control following supervised training
in older individuals with type 2 diabetes. Diabetes Care 2005;28(1):3-9. doi:
https://doi.org/10.2337/diacare.28.1.3 [published Online First: 2004/12/24]
124. Umpierre D, Ribeiro PAB, Kramer CK, et al. Physical activity advice only or
structured exercise training and association with HbA1c levels in type 2
diabetes: A systematic review and meta-analysis. Journal of the American
Medical Association 2011;305(17):1790-99. doi:
https://doi.org/10.1001/jama.2011.576
125. Lee J, Kim D, Kim C. Resistance training for glycemic control, muscular
strength, and lean body mass in old type 2 diabetic patients: A meta-analysis.
Diabetes Therapy 2017;8(3):459-73. doi: https://doi.org/10.1007/s13300-017-
0258-3
126. Umpierre D, Ribeiro PAB, Schaan BD, et al. Volume of supervised exercise
training impacts glycaemic control in patients with type 2 diabetes: A
98
systematic review with meta-regression analysis. Diabetologia
2013;56(2):242-51. doi: https://doi.org/10.1007/s00125-012-2774-z
127. Jia Y, Lao Y, Zhu H, et al. Is metformin still the most efficacious first-line oral
hypoglycaemic drug in treating type 2 diabetes? A network meta-analysis of
randomized controlled trials. Obesity Reviews 2019;20(1):1-12. doi:
https://doi.org/10.1111/obr.12753
128. Yki-Järvinen H. Thiazolidinediones. N Engl J Med 2004;351(11):1106-18. doi:
10.1056/NEJMra041001 [published Online First: 2004/09/10]
129. Naismith SL, Norrie LM, Mowszowski L, et al. The neurobiology of depression
in later-life: Clinical, neuropsychological, neuroimaging and pathophysiological
features. Progress in Neurobiology 2012;98(1):99-143. doi:
https://doi.org/10.1016/j.pneurobio.2012.05.009
130. Rustad JK, Musselman DL, Nemeroff CB. The relationship of depression and
diabetes: Pathophysiological and treatment implications.
Psychoneuroendocrinology 2011;36(9):1276-86. doi:
https://doi.org/10.1016/j.psyneuen.2011.03.005
131. Celik Guzel E, Bakkal E, Guzel S, et al. Can low brain-derived neurotrophic
factor levels be a marker of the presence of depression in obese women?
Neuropsychiatric Disease and Treatment 2014;10:2079-86. doi:
https://doi.org/10.2147/ndt.S72087 [published Online First: 2014/11/15]
132. Ouakinin SRS, Barreira DP, Gois CJ. Depression and obesity: Integrating the
role of stress, neuroendocrine dysfunction and inflammatory pathways.
Frontiers in Endocrinology 2018;9:431-31. doi:
https://doi.org/10.3389/fendo.2018.00431

99
133. Karczewska-Kupczewska M, Adamska A, Nikolajuk A, et al. Decreased serum
brain-derived neurotrophic factor concentration in young nonobese subjects
with low insulin sensitivity. Endocrine Abstracts 2010;22:345.
134. Plomgaard P, Bouzakri K, Krogh-Madsen R, et al. Tumor necrosis factor-α
induces skeletal muscle insulin resistance in healthy human subjects via
inhibition of akt substrate 160 phosphorylation. Diabetes 2005;54(10):2939.
doi: https://doi.org/10.2337/diabetes.54.10.2939
135. Chiodini I, Adda G, Scillitani A, et al. Cortisol secretion in patients with type 2
diabetes. Diabetes Care 2007;30(1):83. doi: https://doi.org/10.2337/dc06-
1267
136. Krabbe KS, Nielsen AR, Krogh-Madsen R, et al. Brain-derived neurotrophic
factor (BDNF) and type 2 diabetes. Diabetologia 2007;50(2):431-38. doi:
https://doi.org/10.1007/s00125-006-0537-4
137. Szuhany KL, Bugatti M, Otto MW. A meta-analytic review of the effects of
exercise on brain-derived neurotrophic factor. Journal of Psychiatric Research
2015;60:56-64. doi: https://doi.org/10.1016/j.jpsychires.2014.10.003
[published Online First: 2014/10/12]
138. Balducci S, Zanuso S, Nicolucci A, et al. Anti-inflammatory effect of exercise
training in subjects with type 2 diabetes and the metabolic syndrome is
dependent on exercise modalities and independent of weight loss. Nutrition,
Metabolism and Cardiovascular Diseases 2010;20(8):608-17. doi:
https://doi.org/10.1016/j.numecd.2009.04.015
139. Beserra AHN, Kameda P, Deslandes AC, et al. Can physical exercise modulate
cortisol level in subjects with depression? A systematic review and meta-
analysis. Trends in Psychiatry and Psychotherapy 2018;40(4):360-68. doi:
100
https://doi.org/10.1590/2237-6089-2017-0155 [published Online First:
2018/12/21]
140. Mavros Y, Kay S, Simpson KA, et al. Reductions in C-reactive protein in older
adults with type 2 diabetes are related to improvements in body composition
following a randomized controlled trial of resistance training. Journal of
Cachexia, Sarcopenia and Muscle 2014;5(2):111-20. doi:
https://doi.org/10.1007/s13539-014-0134-1 [published Online First:
2014/02/12]
141. Schuch FB, Deslandes AC, Stubbs B, et al. Neurobiological effects of exercise
on major depressive disorder: A systematic review. Neuroscience &
Biobehavioral Reviews 2016;61:1-11. doi:
https://doi.org/10.1016/j.neubiorev.2015.11.012
142. National Cholesterol Education Program (NCEP) Expert Panel on Detection
Evaluation and Treatment of High Blood Cholesterol in Adults (Adult
Treatment Panel III). Third report of the National Cholesterol Education
Program (NCEP) expert panel on detection, evaluation, and treatment of high
blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation
2002;106(25):3143-421. [published Online First: 2002/12/18]

101
Tables
Table 1: Search strategy
Database Terms Filters (Ovid) MEDLINE(R) ALL 1946 to December 10, 2019
1 "metabolic syndrome".mp. or Metabolic Syndrome/ (53193) 2 syndrome x.mp. (2029) 3 Insulin Resistance/ or "insulin resist*".mp. (93389) 4 Diabetes Mellitus, Type 2/ or "hyperglyc*".mp. (182371) 5 Hypoglycemia/ or "hypoglyc*".mp. (107974) 6 Glyce#mia 7 ogtt.mp. or Glucose Tolerance Test/ (36820) 8 Blood Glucose/ or glyc?emia.mp. (164843) 9 Insulin Resistance/ or homa*.mp. (63731) 10 diabetes.mp. or Diabetes Mellitus, Type 2/ (587121) 11 T2D?.mp. (26893) 12 NIDDM.mp. (6821) 13 homeo* model assessment.mp. (11724) 14 resistance training.mp. or Resistance Training/ (11933) 15 Exercise/ or exercise.mp. (332272) 16 bodyweight training.mp. (6) 17 machine training.mp. (31) 18 weight training.mp. (1002) 19 Weight Lifting/ or weightlifting.mp. (4762) 20 resistance activit*.mp. (173) 21 PRT.mp. (1581) 22 isometric training.mp. (160) 23 isometric exercise.mp. (1637) 24 circuit training.mp. or Circuit-Based Exercise/ (270) 25 free weights.mp. (139) 26 elastic band.mp. (678) 27 theraband.mp. (31) 28 universal machine.mp. (50) 29 nautilus.mp. (221) 30 power training.mp. (427) 31 walk*.mp. or Walking/ (119437) 32 jog*.mp. or Jogging/ or Running/ (20851) 33 Tai Ji/ (1006) 34 Yoga/px, th [Psychology, Therapy] (445) 35 Exercise Movement Techniques/ or pilates.mp. (884) 36 Qigong/ (145) 37 Bicycling/ or bicycle.mp. (20331) 38 balance training.mp. (1266) 39 boxing.mp. (1663) 40 aqua aerobics.mp. (12) 41 water aerobics.mp. (40) 42 Dancing/ or danc*.mp. (7622) 43 Swimming/ or swim*.mp. (42591)
Limits: humans and (adaptive clinical trial or clinical study or clinical trial, all or controlled clinical trial or multicenter study or randomized controlled trial)
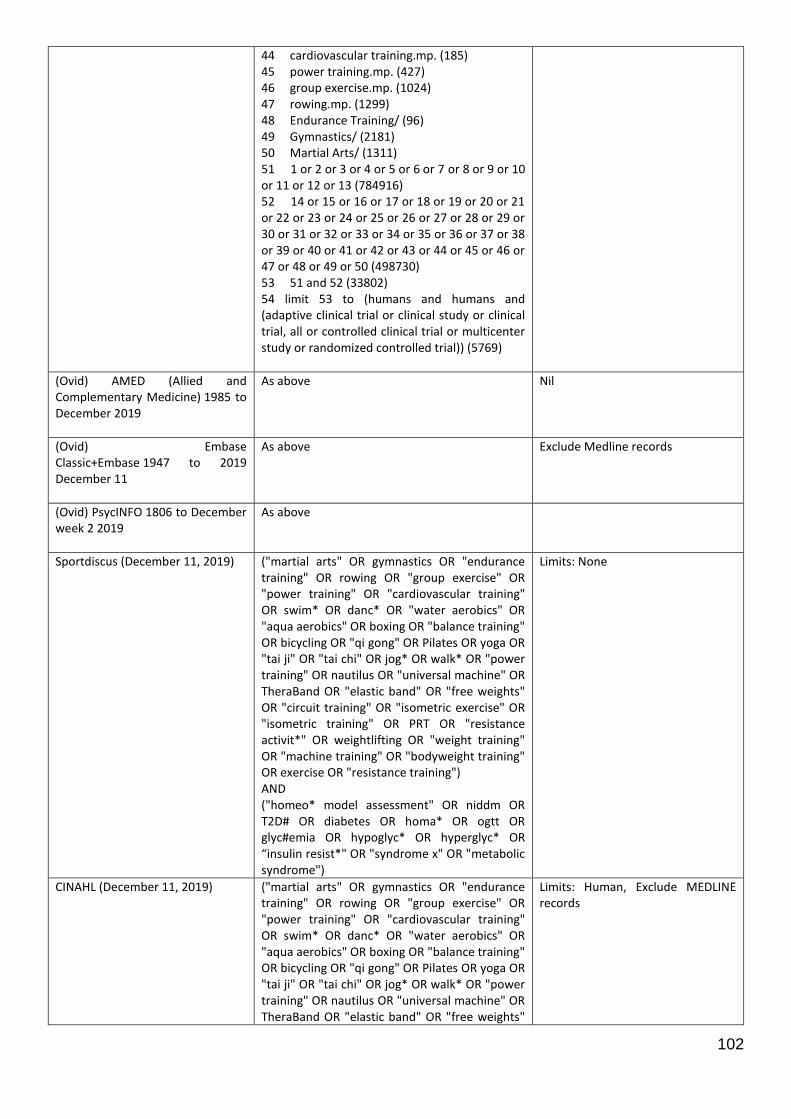
102
44 cardiovascular training.mp. (185) 45 power training.mp. (427) 46 group exercise.mp. (1024) 47 rowing.mp. (1299) 48 Endurance Training/ (96) 49 Gymnastics/ (2181) 50 Martial Arts/ (1311) 51 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 (784916) 52 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 (498730) 53 51 and 52 (33802) 54 limit 53 to (humans and humans and (adaptive clinical trial or clinical study or clinical trial, all or controlled clinical trial or multicenter study or randomized controlled trial)) (5769)
(Ovid) AMED (Allied and Complementary Medicine) 1985 to December 2019
As above Nil
(Ovid) Embase Classic+Embase 1947 to 2019 December 11
As above Exclude Medline records
(Ovid) PsycINFO 1806 to December week 2 2019
As above
Sportdiscus (December 11, 2019) ("martial arts" OR gymnastics OR "endurance training" OR rowing OR "group exercise" OR "power training" OR "cardiovascular training" OR swim* OR danc* OR "water aerobics" OR "aqua aerobics" OR boxing OR "balance training" OR bicycling OR "qi gong" OR Pilates OR yoga OR "tai ji" OR "tai chi" OR jog* OR walk* OR "power training" OR nautilus OR "universal machine" OR TheraBand OR "elastic band" OR "free weights" OR "circuit training" OR "isometric exercise" OR "isometric training" OR PRT OR "resistance activit*" OR weightlifting OR "weight training" OR "machine training" OR "bodyweight training" OR exercise OR "resistance training") AND ("homeo* model assessment" OR niddm OR T2D# OR diabetes OR homa* OR ogtt OR glyc#emia OR hypoglyc* OR hyperglyc* OR “insulin resist*" OR "syndrome x" OR "metabolic syndrome")
Limits: None
CINAHL (December 11, 2019) ("martial arts" OR gymnastics OR "endurance training" OR rowing OR "group exercise" OR "power training" OR "cardiovascular training" OR swim* OR danc* OR "water aerobics" OR "aqua aerobics" OR boxing OR "balance training" OR bicycling OR "qi gong" OR Pilates OR yoga OR "tai ji" OR "tai chi" OR jog* OR walk* OR "power training" OR nautilus OR "universal machine" OR TheraBand OR "elastic band" OR "free weights"
Limits: Human, Exclude MEDLINE records

103
OR "circuit training" OR "isometric exercise" OR "isometric training" OR PRT OR "resistance activit*" OR weightlifting OR "weight training" OR "machine training" OR "bodyweight training" OR exercise OR "resistance training") AND ("homeo* model assessment" OR niddm OR T2D# OR diabetes OR homa* OR ogtt OR glyc#emia OR hypoglyc* OR hyperglyc* OR “insulin resist*" OR "syndrome x" OR "metabolic syndrome")
Physiotherapy Evidence Database (December 11, 2019)
1) Metabolic AND syndrome AND exercise 2) Diabetes AND Exercise 3) Metabolic AND exercise AND depression 4) Depression AND diabetes 5) depression and metabolic

104
Table 2: Intervention and control characteristics of included studies
Citation Intervention modality (co-intervention) Comparator condition Setting Supervised Equipment used
Isolated RET
Lincoln et al., 2002 Resistance training (usual care) Usual care University research clinic Yes Keiser resistance training machines
Duruturk & Özköslü., 2019 Calisthenics (usual care) Education session + usual care Telerehabilitation Yes Bodyweight
Putiri et al., 2012 Resistance training (usual care + home practise) 1. Usual care University research clinic Yes NR
2. Qigong + usual care + home practise
RET with co-interventions
Aylin et al., 2009 Resistance training (home-based walking)
Inactive Outpatient exercise clinic for supervised resistance exercise, aerobic exercise performed in area around patients’ home
Resistance training only
Dumbbells + sandbag + ankle weights
Mueller et al., 2013 Weight-bearing resistance training (flexibility + walking)
Non-weight-bearing strengthening + cycling
University physical therapy research clinic Yes Chair + steps
Pibernik-Okanović et al., 2015
Resistance training (flexibility + group education)
1. Enhanced usual care Outpatient diabetes clinic Yes NR
2. Psychoeducation
Leehey et al., 2016 Resistance training (aerobic training + diet modification + lifestyle modification + usual care)
Diet modification + lifestyle modification + usual care NR
First 12 weeks only
Resistance bands + free weights + weight machines
NR: Not reported; SD: standard deviation; T2DM: Type-2 Diabetes Mellitus; CKD: Chronic Kidney Disease; BMI: Body Mass Index
a: Outcomes measured at 12 months
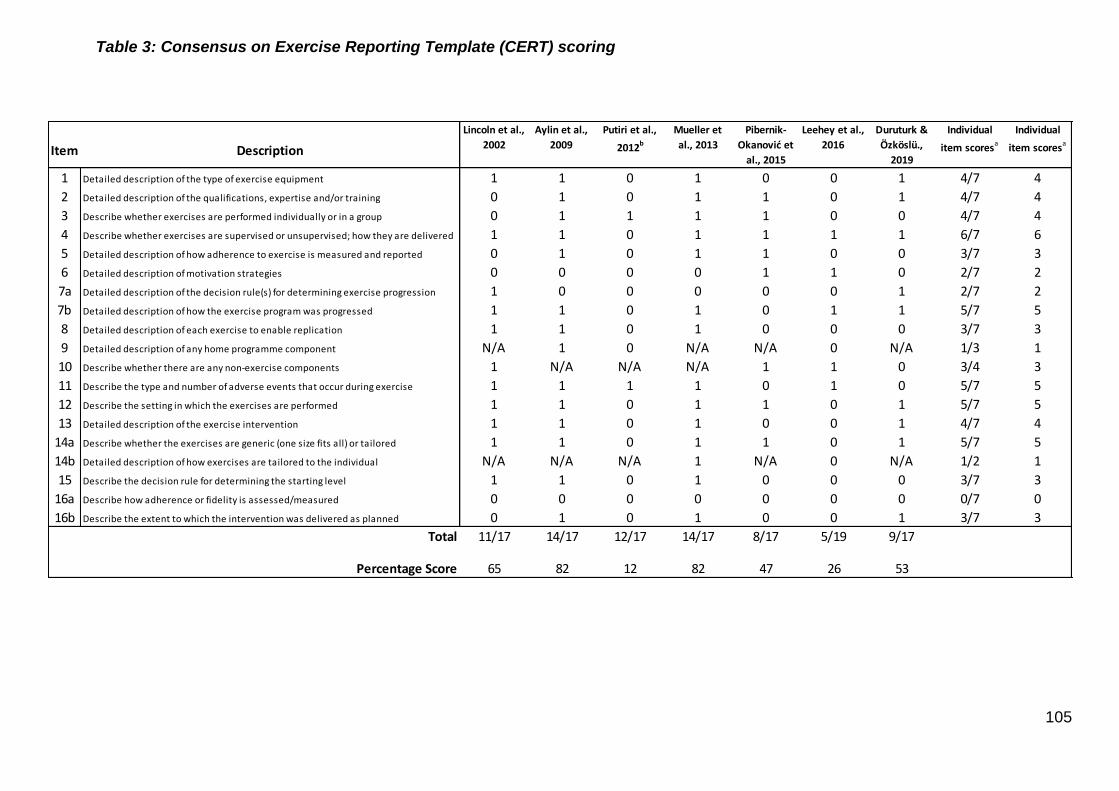
105
Table 3: Consensus on Exercise Reporting Template (CERT) scoring
Item
1 1 1 0 1 0 0 1 4/7 4
2 Detailed description of the qualifications, expertise and/or training 0 1 0 1 1 0 1 4/7 4
3 Describe whether exercises are performed individually or in a group 0 1 1 1 1 0 0 4/7 4
4 Describe whether exercises are supervised or unsupervised; how they are delivered 1 1 0 1 1 1 1 6/7 6
5 Detailed description of how adherence to exercise is measured and reported 0 1 0 1 1 0 0 3/7 3
6 Detailed description of motivation strategies 0 0 0 0 1 1 0 2/7 2
7a Detailed description of the decision rule(s) for determining exercise progression 1 0 0 0 0 0 1 2/7 2
7b Detailed description of how the exercise program was progressed 1 1 0 1 0 1 1 5/7 5
8 Detailed description of each exercise to enable replication 1 1 0 1 0 0 0 3/7 3
9 Detailed description of any home programme component N/A 1 0 N/A N/A 0 N/A 1/3 1
10 Describe whether there are any non-exercise components 1 N/A N/A N/A 1 1 0 3/4 3
11 Describe the type and number of adverse events that occur during exercise 1 1 1 1 0 1 0 5/7 5
12 Describe the setting in which the exercises are performed 1 1 0 1 1 0 1 5/7 5
13 Detailed description of the exercise intervention 1 1 0 1 0 0 1 4/7 4
14a Describe whether the exercises are generic (one size fits all) or tailored 1 1 0 1 1 0 1 5/7 5
14b Detailed description of how exercises are tailored to the individual N/A N/A N/A 1 N/A 0 N/A 1/2 1
15 Describe the decision rule for determining the starting level 1 1 0 1 0 0 0 3/7 3
16a Describe how adherence or fidelity is assessed/measured 0 0 0 0 0 0 0 0/7 0
16b Describe the extent to which the intervention was delivered as planned 0 1 0 1 0 0 1 3/7 3
Total 11/17 14/17 12/17 14/17 8/17 5/19 9/17
65 82 12 82 47 26 53
Lincoln et al.,
2002
Aylin et al.,
2009
Putiri et al.,
2012b
Mueller et
al., 2013
Pibernik-
Okanović et
al., 2015
Leehey et al.,
2016
Duruturk &
Özköslü.,
2019Description
Detailed description of the type of exercise equipment
Individual
item scoresa
Individual
item scoresa
Percentage Score

106
Table 4: Cohort characteristics for included studies
Cohort characteristics for included studies
Citation Region/countries of recruitment Inclusion criteria
Total participants at randomisation (n)
Sex, % male
Age, y (SD) BMI, kg/m2 (SD)
Habitual physical activity level
Isolated RET
Lincoln et al., 2002a USA T2DM >3 years, >55years old, Latino 58 36.2 66.3 (7.7) 31.05 (5.8) Baseline mean PASE leisure score of 10.6
Duruturk & Özköslü., 2019 Ankara, Turkey T2DM >6 months, 18-65 years 50 59 52.9 (11.2) 31.1 (5.6) NR
Putiri et al., 2012 Washington, USA T2DM, HbA1c > 7.5%, FBG > 7.0mmol/L 32 40.6 58.2 (6.9) 31.1 (4.0) NR
RET with co-interventions
Aylin et al., 2009 Turkey T2DM, no resistance or aerobic exercise in previous 6 months 38 75 53.72 (7.5) 29.9 (1.0) NR
Mueller et al., 2013 Washington, USA T2DM, peripheral neuropathy (inability to sense the 5.07 Semmes-Weinstein monofilament on at least 1 spot on the plantar foot and inability to sense vibration at the plantar great toe from a biothesiometer at <25V), step count 2000-9000 steps/day, currently exercising <3 times/week and <20mins/session, approved to participate by primary physician
29 58.6 64.57 (12.7) 35.01 (6.8) <3 times/week, <20 minutes/session
Pibernik-Okanović et al., 2015
Croatia T2DM > 1 year, 18-65 years, at least one medical check-up in previous year, sub-syndromal depression with presence of at least one depressive symptom in last month and need for receiving professional help, without diagnosis of MDD or dysthymia
209 62.2 58.11 (5.6) 30.07 (4.5) 3.6 days/week adhering to exercise recommendations of the Diabetes Self-Care Activities
Leehey et al., 2016 NI T2DM, BMI > 30kg/m2, CKD stage 2-3 with urine protein/creatinine >200mg/g >3/12
36 100 66 (8.1) 36.8 (4.5) NR
NR: Not reported; SD: standard deviation; CKD: chronic kidney disease; T2DM: type-diabetes mellitus; CES-D: Center for Epidemiological Studies - Depression scale; PASE: Physical Activity Scale for the Elderly
a: Values taken from Casteneda et al., 2002
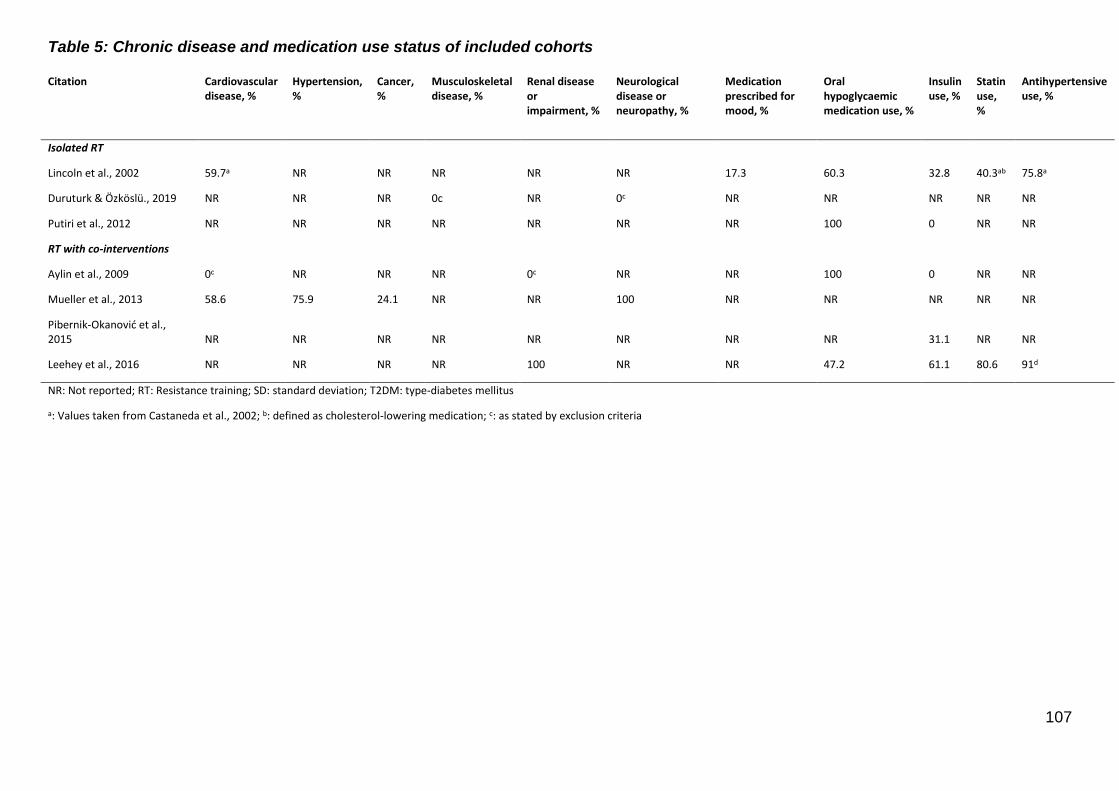
107
Table 5: Chronic disease and medication use status of included cohorts
Citation Cardiovascular disease, %
Hypertension, %
Cancer, %
Musculoskeletal disease, %
Renal disease or impairment, %
Neurological disease or neuropathy, %
Medication prescribed for mood, %
Oral hypoglycaemic medication use, %
Insulin use, %
Statin use, %
Antihypertensive use, %
Isolated RT
Lincoln et al., 2002 59.7a NR NR NR NR NR 17.3 60.3 32.8 40.3ab 75.8a
Duruturk & Özköslü., 2019 NR NR NR 0c NR 0c NR NR NR NR NR
Putiri et al., 2012 NR NR NR NR NR NR NR 100 0 NR NR
RT with co-interventions
Aylin et al., 2009 0c NR NR NR 0c NR NR 100 0 NR NR
Mueller et al., 2013 58.6 75.9 24.1 NR NR 100 NR NR NR NR NR
Pibernik-Okanović et al., 2015 NR NR NR NR NR NR NR NR 31.1 NR NR
Leehey et al., 2016 NR NR NR NR 100 NR NR 47.2 61.1 80.6 91d
NR: Not reported; RT: Resistance training; SD: standard deviation; T2DM: type-diabetes mellitus
a: Values taken from Castaneda et al., 2002; b: defined as cholesterol-lowering medication; c: as stated by exclusion criteria
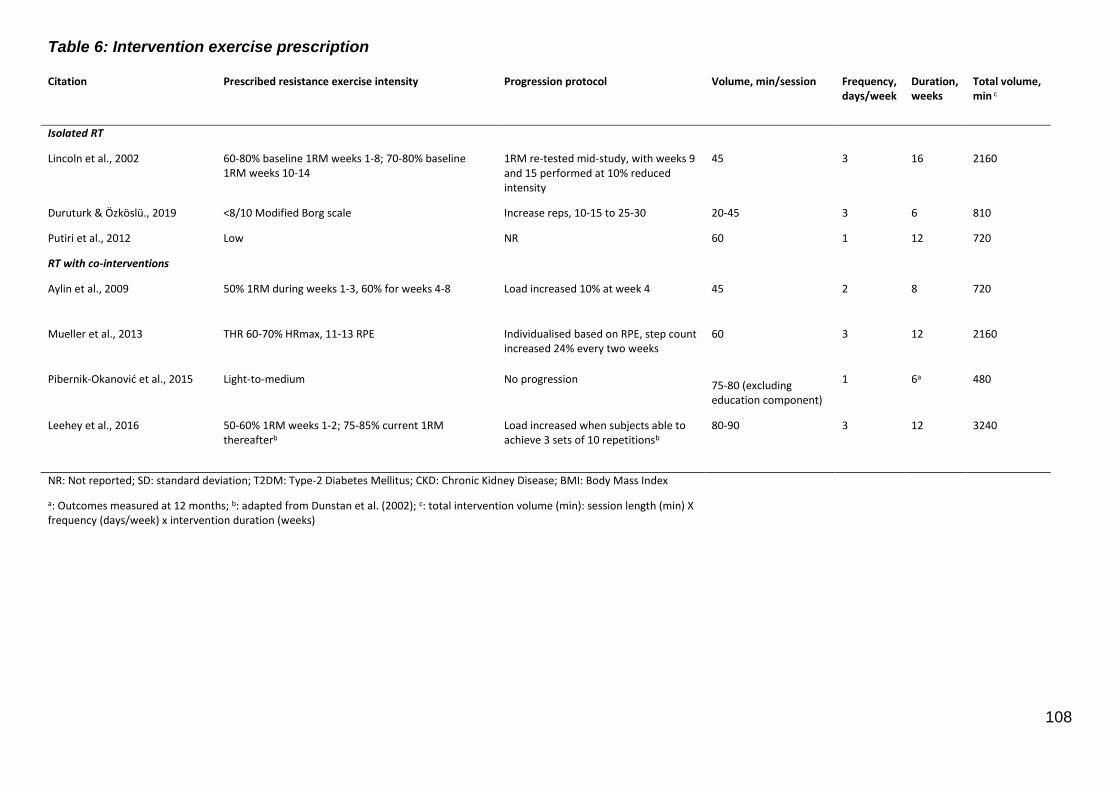
108
Table 6: Intervention exercise prescription
Citation Prescribed resistance exercise intensity Progression protocol Volume, min/session Frequency, days/week
Duration, weeks
Total volume, min c
Isolated RT
Lincoln et al., 2002 60-80% baseline 1RM weeks 1-8; 70-80% baseline 1RM weeks 10-14
1RM re-tested mid-study, with weeks 9 and 15 performed at 10% reduced intensity
45 3 16 2160
Duruturk & Özköslü., 2019 <8/10 Modified Borg scale Increase reps, 10-15 to 25-30 20-45 3 6 810
Putiri et al., 2012 Low NR 60 1 12 720
RT with co-interventions
Aylin et al., 2009 50% 1RM during weeks 1-3, 60% for weeks 4-8 Load increased 10% at week 4 45 2 8 720
Mueller et al., 2013 THR 60-70% HRmax, 11-13 RPE Individualised based on RPE, step count
increased 24% every two weeks 60 3 12 2160
Pibernik-Okanović et al., 2015 Light-to-medium No progression
75-80 (excluding education component)
1 6a 480
Leehey et al., 2016 50-60% 1RM weeks 1-2; 75-85% current 1RM
thereafterb Load increased when subjects able to achieve 3 sets of 10 repetitionsb
80-90 3 12 3240
NR: Not reported; SD: standard deviation; T2DM: Type-2 Diabetes Mellitus; CKD: Chronic Kidney Disease; BMI: Body Mass Index
a: Outcomes measured at 12 months; b: adapted from Dunstan et al. (2002); c: total intervention volume (min): session length (min) X frequency (days/week) x intervention duration (weeks)
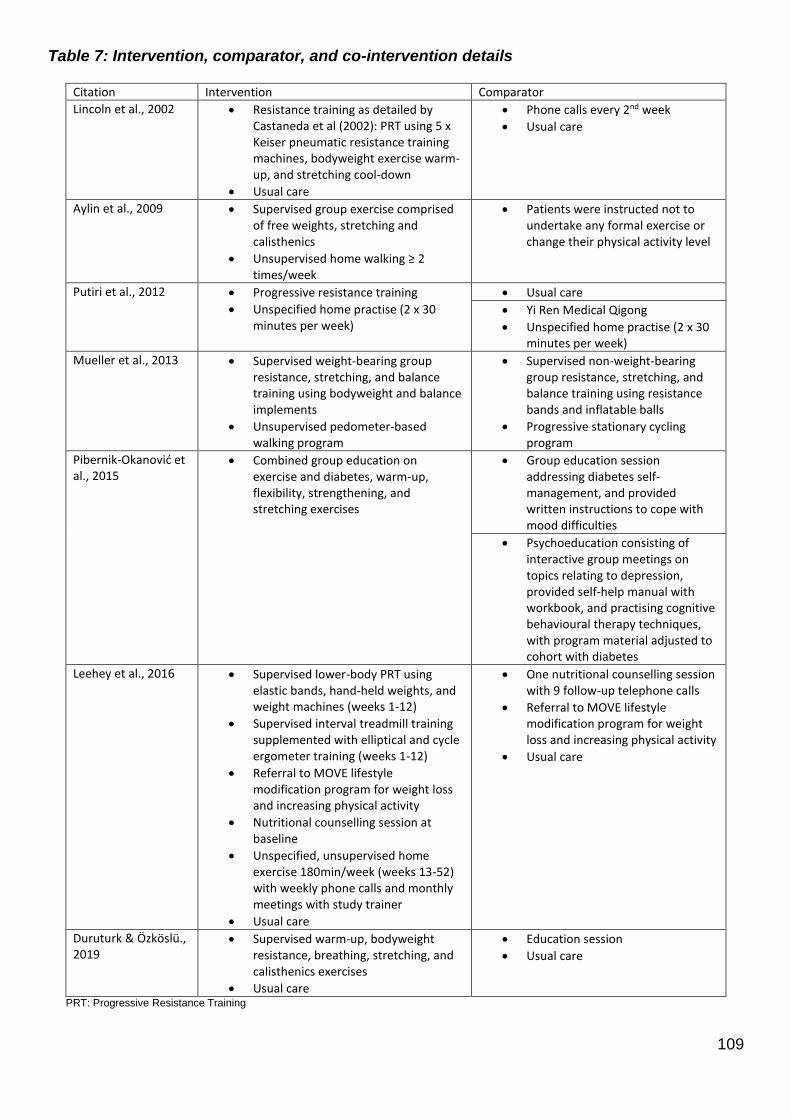
109
Table 7: Intervention, comparator, and co-intervention details
Citation Intervention Comparator
Lincoln et al., 2002 • Resistance training as detailed by Castaneda et al (2002): PRT using 5 x Keiser pneumatic resistance training machines, bodyweight exercise warm-up, and stretching cool-down
• Usual care
• Phone calls every 2nd week
• Usual care
Aylin et al., 2009 • Supervised group exercise comprised of free weights, stretching and calisthenics
• Unsupervised home walking ≥ 2 times/week
• Patients were instructed not to undertake any formal exercise or change their physical activity level
Putiri et al., 2012 • Progressive resistance training
• Unspecified home practise (2 x 30 minutes per week)
• Usual care
• Yi Ren Medical Qigong
• Unspecified home practise (2 x 30 minutes per week)
Mueller et al., 2013 • Supervised weight-bearing group resistance, stretching, and balance training using bodyweight and balance implements
• Unsupervised pedometer-based walking program
• Supervised non-weight-bearing group resistance, stretching, and balance training using resistance bands and inflatable balls
• Progressive stationary cycling program
Pibernik-Okanović et al., 2015
• Combined group education on exercise and diabetes, warm-up, flexibility, strengthening, and stretching exercises
• Group education session addressing diabetes self-management, and provided written instructions to cope with mood difficulties
• Psychoeducation consisting of interactive group meetings on topics relating to depression, provided self-help manual with workbook, and practising cognitive behavioural therapy techniques, with program material adjusted to cohort with diabetes
Leehey et al., 2016 • Supervised lower-body PRT using elastic bands, hand-held weights, and weight machines (weeks 1-12)
• Supervised interval treadmill training supplemented with elliptical and cycle ergometer training (weeks 1-12)
• Referral to MOVE lifestyle modification program for weight loss and increasing physical activity
• Nutritional counselling session at baseline
• Unspecified, unsupervised home exercise 180min/week (weeks 13-52) with weekly phone calls and monthly meetings with study trainer
• Usual care
• One nutritional counselling session with 9 follow-up telephone calls
• Referral to MOVE lifestyle modification program for weight loss and increasing physical activity
• Usual care
Duruturk & Özköslü., 2019
• Supervised warm-up, bodyweight resistance, breathing, stretching, and calisthenics exercises
• Usual care
• Education session
• Usual care
PRT: Progressive Resistance Training
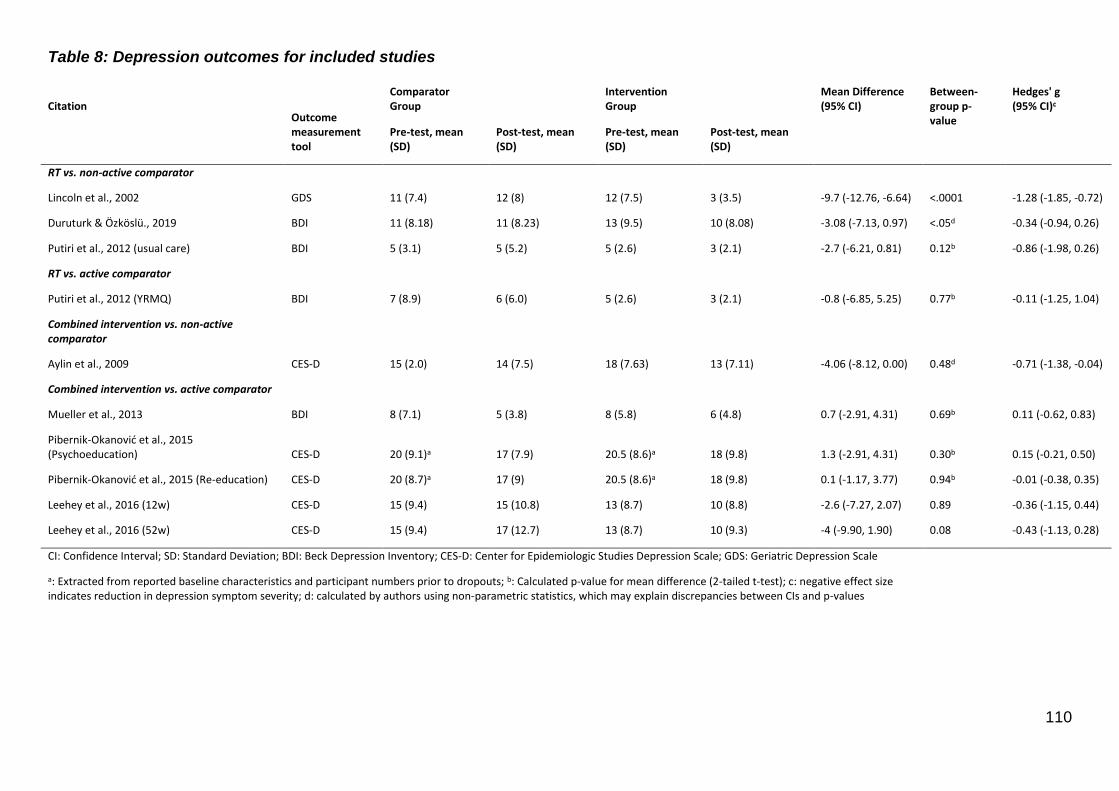
110
Table 8: Depression outcomes for included studies
Citation Outcome measurement tool
Comparator Group
Intervention Group
Mean Difference (95% CI)
Between-group p-value
Hedges' g (95% CI)c
Pre-test, mean (SD)
Post-test, mean (SD)
Pre-test, mean (SD)
Post-test, mean (SD)
RT vs. non-active comparator
Lincoln et al., 2002 GDS 11 (7.4) 12 (8) 12 (7.5) 3 (3.5) -9.7 (-12.76, -6.64) <.0001 -1.28 (-1.85, -0.72)
Duruturk & Özköslü., 2019 BDI 11 (8.18) 11 (8.23) 13 (9.5) 10 (8.08) -3.08 (-7.13, 0.97) <.05d -0.34 (-0.94, 0.26)
Putiri et al., 2012 (usual care) BDI 5 (3.1) 5 (5.2) 5 (2.6) 3 (2.1) -2.7 (-6.21, 0.81) 0.12b -0.86 (-1.98, 0.26)
RT vs. active comparator
Putiri et al., 2012 (YRMQ) BDI 7 (8.9) 6 (6.0) 5 (2.6) 3 (2.1) -0.8 (-6.85, 5.25) 0.77b -0.11 (-1.25, 1.04)
Combined intervention vs. non-active comparator
Aylin et al., 2009 CES-D 15 (2.0) 14 (7.5) 18 (7.63) 13 (7.11) -4.06 (-8.12, 0.00) 0.48d -0.71 (-1.38, -0.04)
Combined intervention vs. active comparator
Mueller et al., 2013 BDI 8 (7.1) 5 (3.8) 8 (5.8) 6 (4.8) 0.7 (-2.91, 4.31) 0.69b 0.11 (-0.62, 0.83)
Pibernik-Okanović et al., 2015 (Psychoeducation) CES-D 20 (9.1)a 17 (7.9) 20.5 (8.6)a 18 (9.8) 1.3 (-2.91, 4.31) 0.30b 0.15 (-0.21, 0.50)
Pibernik-Okanović et al., 2015 (Re-education) CES-D 20 (8.7)a 17 (9) 20.5 (8.6)a 18 (9.8) 0.1 (-1.17, 3.77) 0.94b -0.01 (-0.38, 0.35)
Leehey et al., 2016 (12w) CES-D 15 (9.4) 15 (10.8) 13 (8.7) 10 (8.8) -2.6 (-7.27, 2.07) 0.89 -0.36 (-1.15, 0.44)
Leehey et al., 2016 (52w) CES-D 15 (9.4) 17 (12.7) 13 (8.7) 10 (9.3) -4 (-9.90, 1.90) 0.08 -0.43 (-1.13, 0.28)
CI: Confidence Interval; SD: Standard Deviation; BDI: Beck Depression Inventory; CES-D: Center for Epidemiologic Studies Depression Scale; GDS: Geriatric Depression Scale
a: Extracted from reported baseline characteristics and participant numbers prior to dropouts; b: Calculated p-value for mean difference (2-tailed t-test); c: negative effect size indicates reduction in depression symptom severity; d: calculated by authors using non-parametric statistics, which may explain discrepancies between CIs and p-values
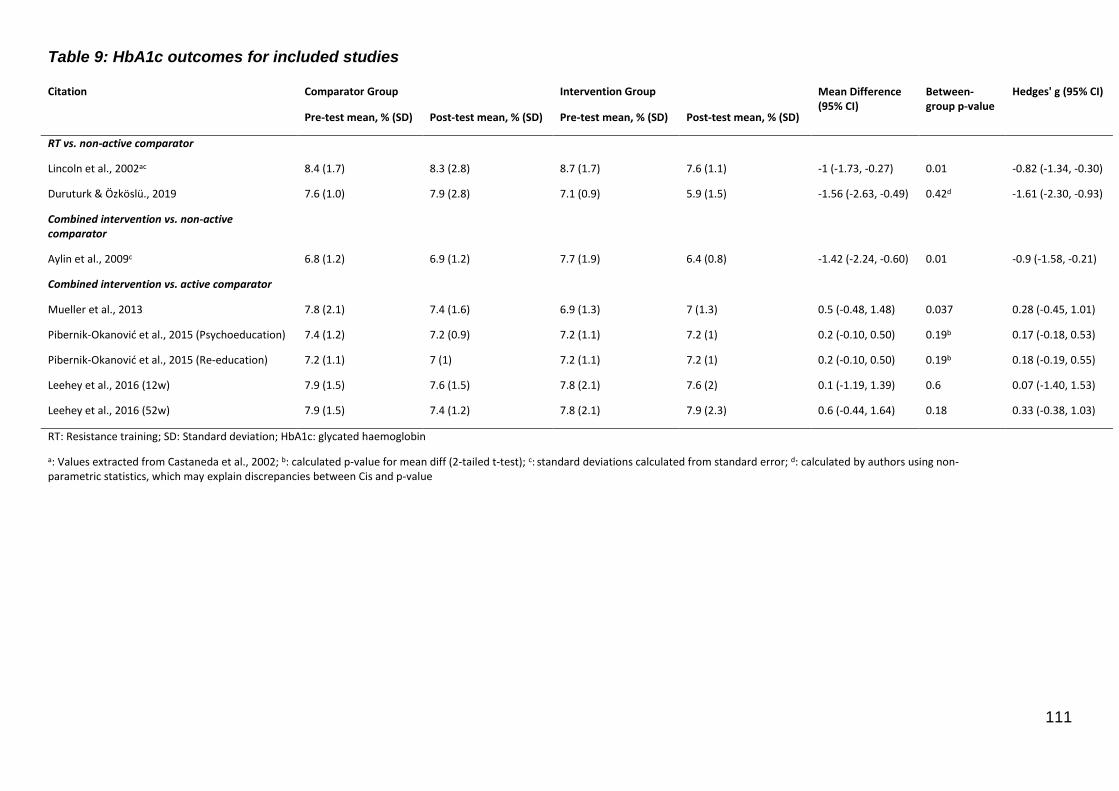
111
Table 9: HbA1c outcomes for included studies
Citation Comparator Group Intervention Group Mean Difference (95% CI)
Between-group p-value
Hedges' g (95% CI)
Pre-test mean, % (SD) Post-test mean, % (SD) Pre-test mean, % (SD) Post-test mean, % (SD)
RT vs. non-active comparator
Lincoln et al., 2002ac 8.4 (1.7) 8.3 (2.8) 8.7 (1.7) 7.6 (1.1) -1 (-1.73, -0.27) 0.01 -0.82 (-1.34, -0.30)
Duruturk & Özköslü., 2019 7.6 (1.0) 7.9 (2.8) 7.1 (0.9) 5.9 (1.5) -1.56 (-2.63, -0.49) 0.42d -1.61 (-2.30, -0.93)
Combined intervention vs. non-active comparator
Aylin et al., 2009c 6.8 (1.2) 6.9 (1.2) 7.7 (1.9) 6.4 (0.8) -1.42 (-2.24, -0.60) 0.01 -0.9 (-1.58, -0.21)
Combined intervention vs. active comparator
Mueller et al., 2013 7.8 (2.1) 7.4 (1.6) 6.9 (1.3) 7 (1.3) 0.5 (-0.48, 1.48) 0.037 0.28 (-0.45, 1.01)
Pibernik-Okanović et al., 2015 (Psychoeducation) 7.4 (1.2) 7.2 (0.9) 7.2 (1.1) 7.2 (1) 0.2 (-0.10, 0.50) 0.19b 0.17 (-0.18, 0.53)
Pibernik-Okanović et al., 2015 (Re-education) 7.2 (1.1) 7 (1) 7.2 (1.1) 7.2 (1) 0.2 (-0.10, 0.50) 0.19b 0.18 (-0.19, 0.55)
Leehey et al., 2016 (12w) 7.9 (1.5) 7.6 (1.5) 7.8 (2.1) 7.6 (2) 0.1 (-1.19, 1.39) 0.6 0.07 (-1.40, 1.53)
Leehey et al., 2016 (52w) 7.9 (1.5) 7.4 (1.2) 7.8 (2.1) 7.9 (2.3) 0.6 (-0.44, 1.64) 0.18 0.33 (-0.38, 1.03)
RT: Resistance training; SD: Standard deviation; HbA1c: glycated haemoglobin
a: Values extracted from Castaneda et al., 2002; b: calculated p-value for mean diff (2-tailed t-test); c: standard deviations calculated from standard error; d: calculated by authors using non-parametric statistics, which may explain discrepancies between Cis and p-value
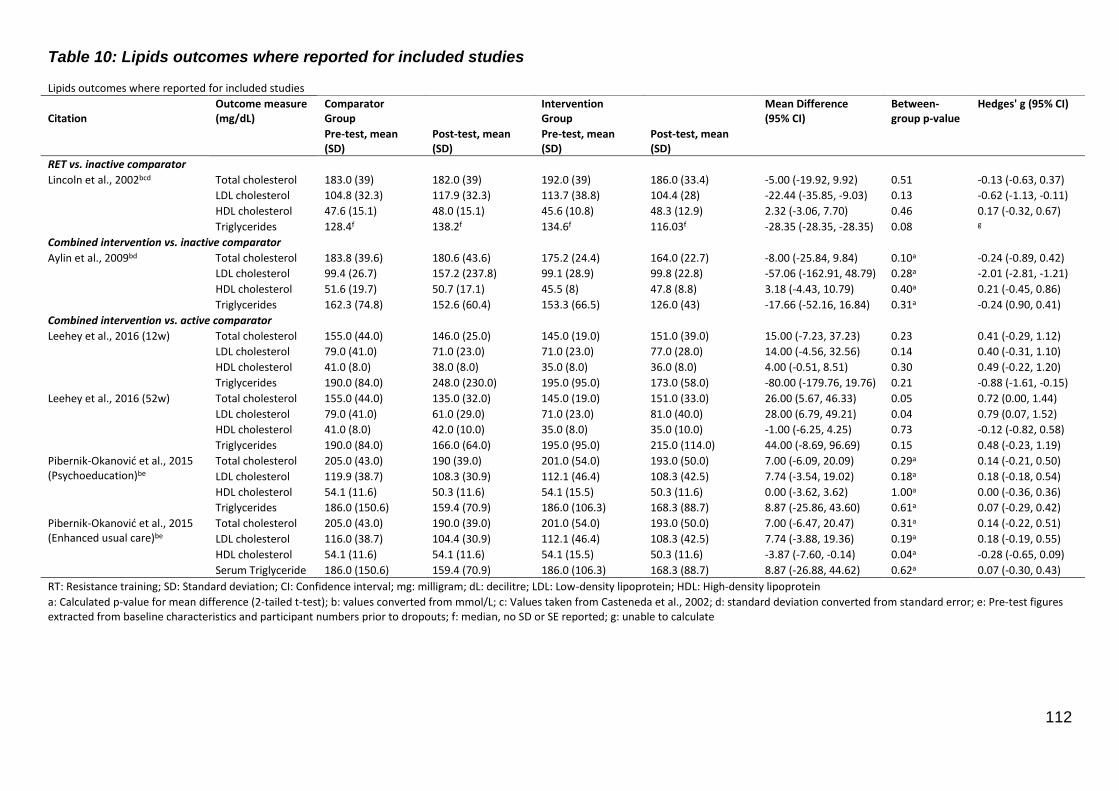
112
Table 10: Lipids outcomes where reported for included studies Lipids outcomes where reported for included studies
Citation Outcome measure (mg/dL)
Comparator Group
Intervention Group
Mean Difference (95% CI)
Between-group p-value
Hedges' g (95% CI)
Pre-test, mean (SD)
Post-test, mean (SD)
Pre-test, mean (SD)
Post-test, mean (SD)
RET vs. inactive comparator
Lincoln et al., 2002bcd Total cholesterol 183.0 (39) 182.0 (39) 192.0 (39) 186.0 (33.4) -5.00 (-19.92, 9.92) 0.51 -0.13 (-0.63, 0.37)
LDL cholesterol 104.8 (32.3) 117.9 (32.3) 113.7 (38.8) 104.4 (28) -22.44 (-35.85, -9.03) 0.13 -0.62 (-1.13, -0.11)
HDL cholesterol 47.6 (15.1) 48.0 (15.1) 45.6 (10.8) 48.3 (12.9) 2.32 (-3.06, 7.70) 0.46 0.17 (-0.32, 0.67)
Triglycerides 128.4f 138.2f 134.6f 116.03f -28.35 (-28.35, -28.35) 0.08 g
Combined intervention vs. inactive comparator
Aylin et al., 2009bd Total cholesterol 183.8 (39.6) 180.6 (43.6) 175.2 (24.4) 164.0 (22.7) -8.00 (-25.84, 9.84) 0.10a -0.24 (-0.89, 0.42)
LDL cholesterol 99.4 (26.7) 157.2 (237.8) 99.1 (28.9) 99.8 (22.8) -57.06 (-162.91, 48.79) 0.28a -2.01 (-2.81, -1.21)
HDL cholesterol 51.6 (19.7) 50.7 (17.1) 45.5 (8) 47.8 (8.8) 3.18 (-4.43, 10.79) 0.40a 0.21 (-0.45, 0.86)
Triglycerides 162.3 (74.8) 152.6 (60.4) 153.3 (66.5) 126.0 (43) -17.66 (-52.16, 16.84) 0.31a -0.24 (0.90, 0.41)
Combined intervention vs. active comparator
Leehey et al., 2016 (12w) Total cholesterol 155.0 (44.0) 146.0 (25.0) 145.0 (19.0) 151.0 (39.0) 15.00 (-7.23, 37.23) 0.23 0.41 (-0.29, 1.12)
LDL cholesterol 79.0 (41.0) 71.0 (23.0) 71.0 (23.0) 77.0 (28.0) 14.00 (-4.56, 32.56) 0.14 0.40 (-0.31, 1.10)
HDL cholesterol 41.0 (8.0) 38.0 (8.0) 35.0 (8.0) 36.0 (8.0) 4.00 (-0.51, 8.51) 0.30 0.49 (-0.22, 1.20)
Triglycerides 190.0 (84.0) 248.0 (230.0) 195.0 (95.0) 173.0 (58.0) -80.00 (-179.76, 19.76) 0.21 -0.88 (-1.61, -0.15)
Leehey et al., 2016 (52w) Total cholesterol 155.0 (44.0) 135.0 (32.0) 145.0 (19.0) 151.0 (33.0) 26.00 (5.67, 46.33) 0.05 0.72 (0.00, 1.44)
LDL cholesterol 79.0 (41.0) 61.0 (29.0) 71.0 (23.0) 81.0 (40.0) 28.00 (6.79, 49.21) 0.04 0.79 (0.07, 1.52)
HDL cholesterol 41.0 (8.0) 42.0 (10.0) 35.0 (8.0) 35.0 (10.0) -1.00 (-6.25, 4.25) 0.73 -0.12 (-0.82, 0.58)
Triglycerides 190.0 (84.0) 166.0 (64.0) 195.0 (95.0) 215.0 (114.0) 44.00 (-8.69, 96.69) 0.15 0.48 (-0.23, 1.19)
Pibernik-Okanović et al., 2015 (Psychoeducation)be
Total cholesterol 205.0 (43.0) 190 (39.0) 201.0 (54.0) 193.0 (50.0) 7.00 (-6.09, 20.09) 0.29a 0.14 (-0.21, 0.50)
LDL cholesterol 119.9 (38.7) 108.3 (30.9) 112.1 (46.4) 108.3 (42.5) 7.74 (-3.54, 19.02) 0.18a 0.18 (-0.18, 0.54)
HDL cholesterol 54.1 (11.6) 50.3 (11.6) 54.1 (15.5) 50.3 (11.6) 0.00 (-3.62, 3.62) 1.00a 0.00 (-0.36, 0.36)
Triglycerides 186.0 (150.6) 159.4 (70.9) 186.0 (106.3) 168.3 (88.7) 8.87 (-25.86, 43.60) 0.61a 0.07 (-0.29, 0.42)
Pibernik-Okanović et al., 2015 (Enhanced usual care)be
Total cholesterol 205.0 (43.0) 190.0 (39.0) 201.0 (54.0) 193.0 (50.0) 7.00 (-6.47, 20.47) 0.31a 0.14 (-0.22, 0.51)
LDL cholesterol 116.0 (38.7) 104.4 (30.9) 112.1 (46.4) 108.3 (42.5) 7.74 (-3.88, 19.36) 0.19a 0.18 (-0.19, 0.55)
HDL cholesterol 54.1 (11.6) 54.1 (11.6) 54.1 (15.5) 50.3 (11.6) -3.87 (-7.60, -0.14) 0.04a -0.28 (-0.65, 0.09)
Serum Triglyceride 186.0 (150.6) 159.4 (70.9) 186.0 (106.3) 168.3 (88.7) 8.87 (-26.88, 44.62) 0.62a 0.07 (-0.30, 0.43)
RT: Resistance training; SD: Standard deviation; CI: Confidence interval; mg: milligram; dL: decilitre; LDL: Low-density lipoprotein; HDL: High-density lipoprotein
a: Calculated p-value for mean difference (2-tailed t-test); b: values converted from mmol/L; c: Values taken from Casteneda et al., 2002; d: standard deviation converted from standard error; e: Pre-test figures extracted from baseline characteristics and participant numbers prior to dropouts; f: median, no SD or SE reported; g: unable to calculate
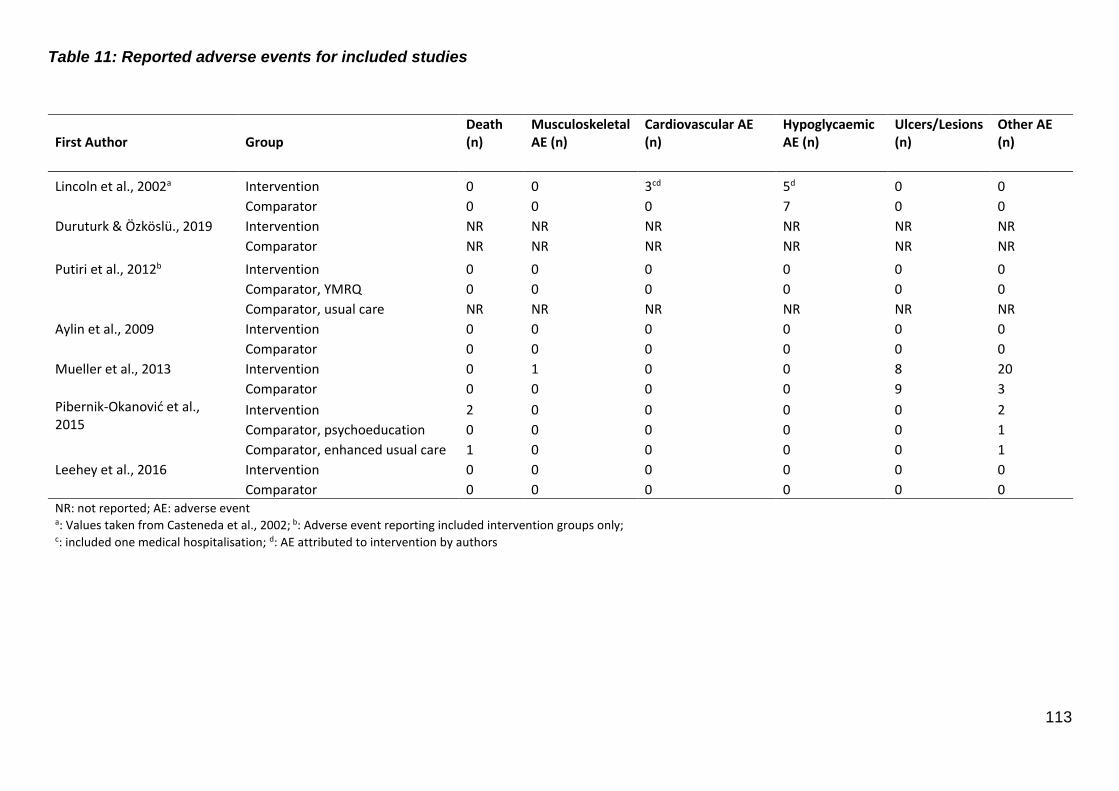
113
Table 11: Reported adverse events for included studies
First Author Group Death (n)
Musculoskeletal AE (n)
Cardiovascular AE (n)
Hypoglycaemic AE (n)
Ulcers/Lesions (n)
Other AE (n)
Lincoln et al., 2002a Intervention 0 0 3cd 5d 0 0
Comparator 0 0 0 7 0 0 Duruturk & Özköslü., 2019 Intervention NR NR NR NR NR NR
Comparator NR NR NR NR NR NR
Putiri et al., 2012b Intervention 0 0 0 0 0 0
Comparator, YMRQ 0 0 0 0 0 0
Comparator, usual care NR NR NR NR NR NR Aylin et al., 2009 Intervention 0 0 0 0 0 0
Comparator 0 0 0 0 0 0 Mueller et al., 2013 Intervention 0 1 0 0 8 20 Comparator 0 0 0 0 9 3 Pibernik-Okanović et al., 2015
Intervention 2 0 0 0 0 2 Comparator, psychoeducation 0 0 0 0 0 1
Comparator, enhanced usual care 1 0 0 0 0 1 Leehey et al., 2016 Intervention 0 0 0 0 0 0 Comparator 0 0 0 0 0 0 NR: not reported; AE: adverse event a: Values taken from Casteneda et al., 2002; b: Adverse event reporting included intervention groups only; c: included one medical hospitalisation; d: AE attributed to intervention by authors
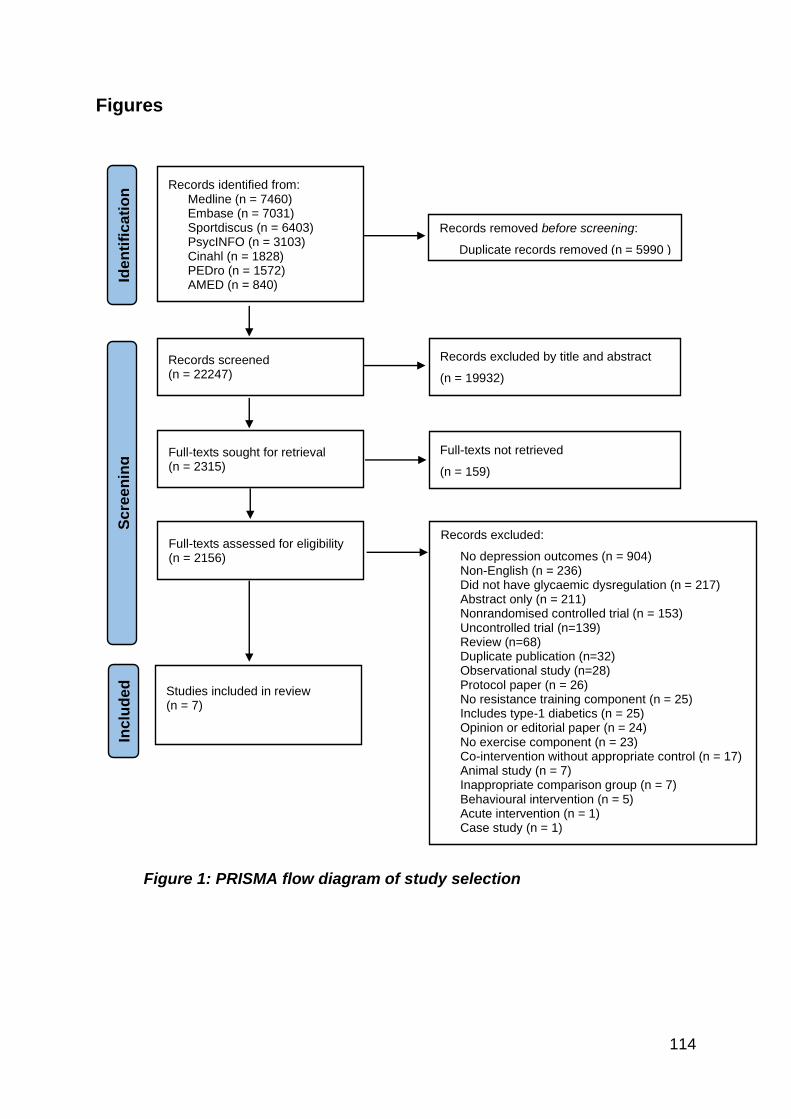
114
Figures
Figure 1: PRISMA flow diagram of study selection
Records identified from: Medline (n = 7460) Embase (n = 7031) Sportdiscus (n = 6403) PsycINFO (n = 3103) Cinahl (n = 1828) PEDro (n = 1572) AMED (n = 840)
Records removed before screening:
Duplicate records removed (n = 5990 )
Records screened (n = 22247)
Records excluded by title and abstract
(n = 19932)
Full-texts sought for retrieval (n = 2315)
Full-texts not retrieved
(n = 159)
Full-texts assessed for eligibility (n = 2156)
Records excluded:
No depression outcomes (n = 904) Non-English (n = 236) Did not have glycaemic dysregulation (n = 217) Abstract only (n = 211) Nonrandomised controlled trial (n = 153) Uncontrolled trial (n=139) Review (n=68) Duplicate publication (n=32) Observational study (n=28) Protocol paper (n = 26) No resistance training component (n = 25) Includes type-1 diabetics (n = 25) Opinion or editorial paper (n = 24) No exercise component (n = 23) Co-intervention without appropriate control (n = 17) Animal study (n = 7) Inappropriate comparison group (n = 7) Behavioural intervention (n = 5) Acute intervention (n = 1) Case study (n = 1)
Studies included in review (n = 7)
Iden
tifi
cati
on
S
cre
en
ing
Inclu
de
d
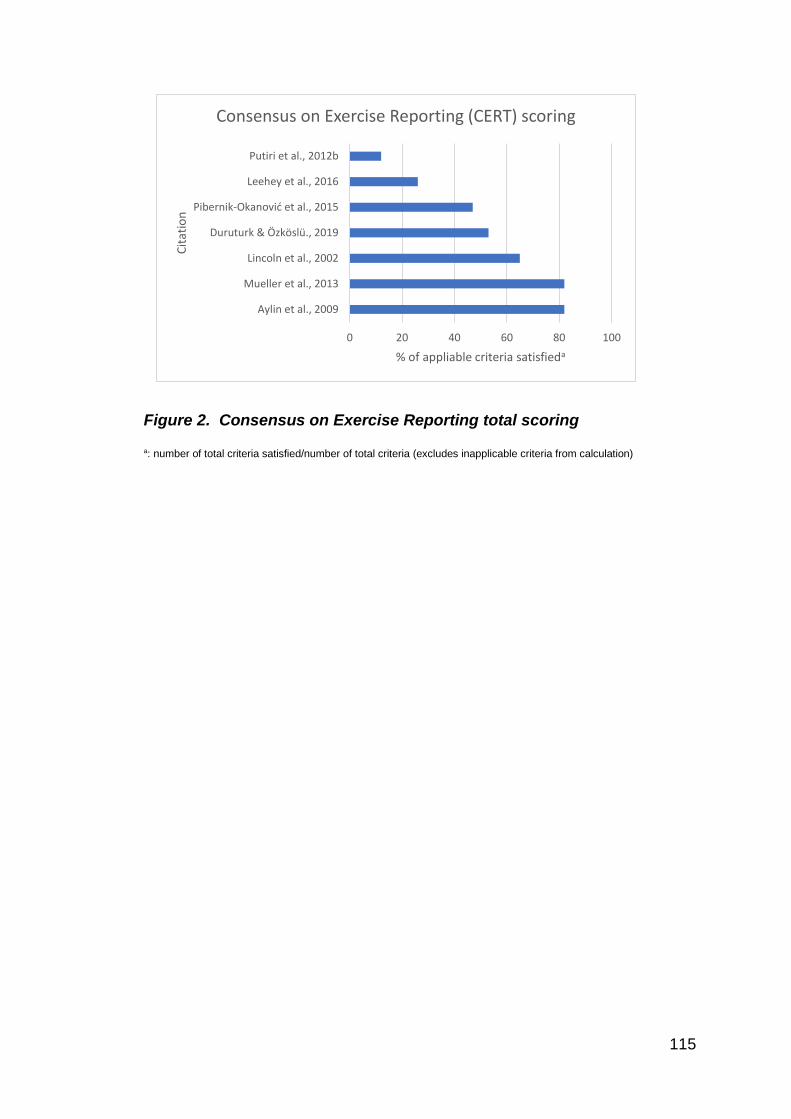
115
Figure 2. Consensus on Exercise Reporting total scoring
a: number of total criteria satisfied/number of total criteria (excludes inapplicable criteria from calculation)
0 20 40 60 80 100
Aylin et al., 2009
Mueller et al., 2013
Lincoln et al., 2002
Duruturk & Özköslü., 2019
Pibernik-Okanović et al., 2015
Leehey et al., 2016
Putiri et al., 2012b
% of appliable criteria satisfieda
Cit
atio
n
Consensus on Exercise Reporting (CERT) scoring

116
Figure 3. Risk of Bias assessment using intention-to-treat analysis
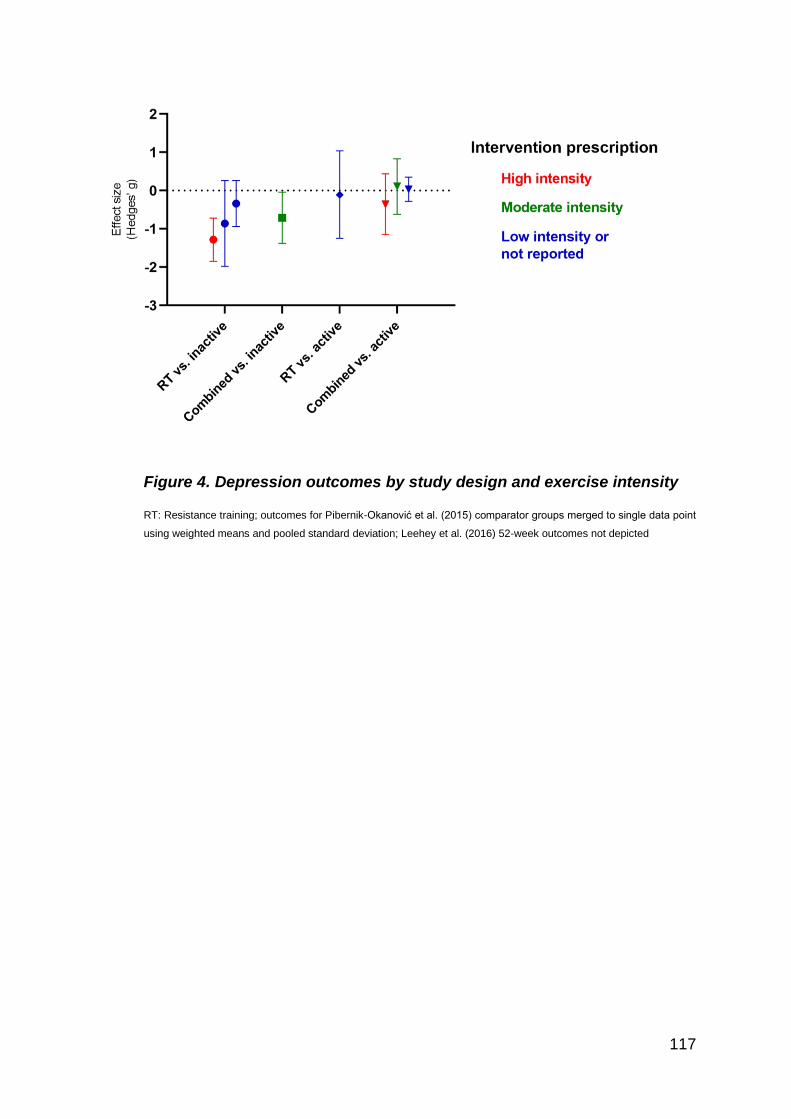
117
Figure 4. Depression outcomes by study design and exercise intensity
RT: Resistance training; outcomes for Pibernik-Okanović et al. (2015) comparator groups merged to single data point
using weighted means and pooled standard deviation; Leehey et al. (2016) 52-week outcomes not depicted

118
Figure 5. Depression outcomes by study design and exercise exposure
RT: Resistance training; total exercise exposure (min): session length (min) X frequency (days/week) x intervention
duration (weeks); outcomes for Pibernik-Okanović et al. (2015) comparator groups merged to single data point using
weighted means and pooled standard deviation; Leehey et al. (2016) 52-week outcomes not depicted
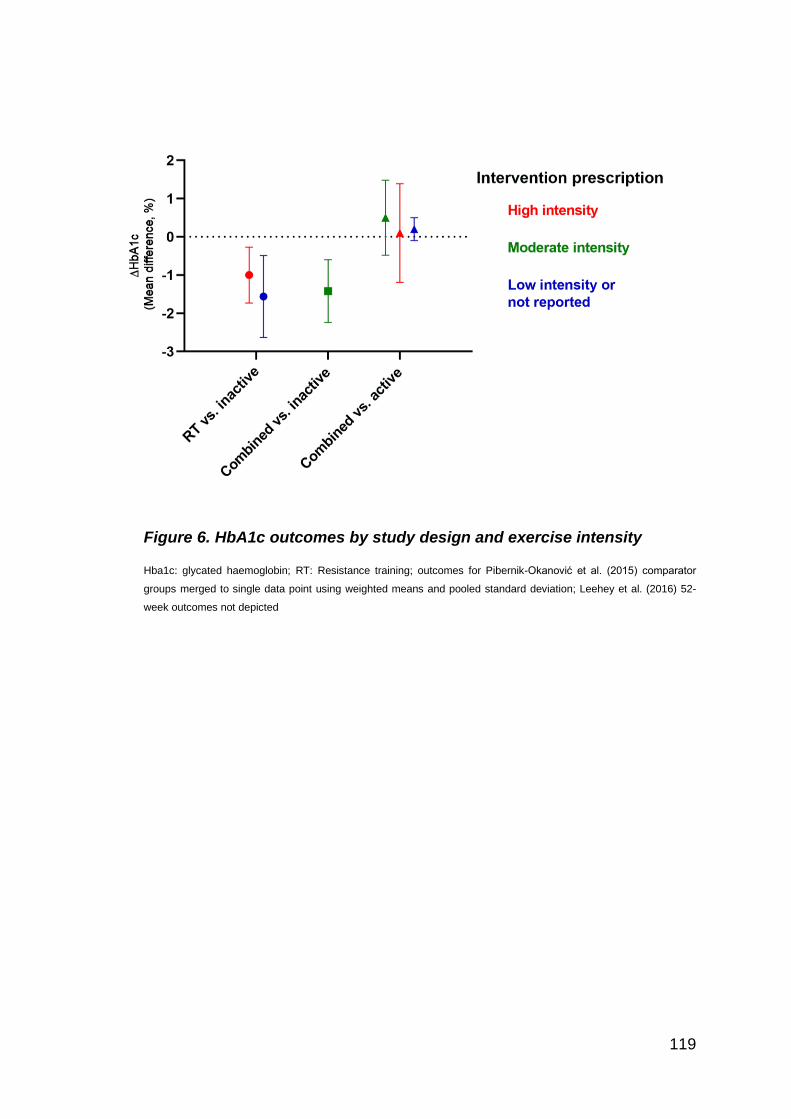
119
Figure 6. HbA1c outcomes by study design and exercise intensity
Hba1c: glycated haemoglobin; RT: Resistance training; outcomes for Pibernik-Okanović et al. (2015) comparator
groups merged to single data point using weighted means and pooled standard deviation; Leehey et al. (2016) 52-
week outcomes not depicted
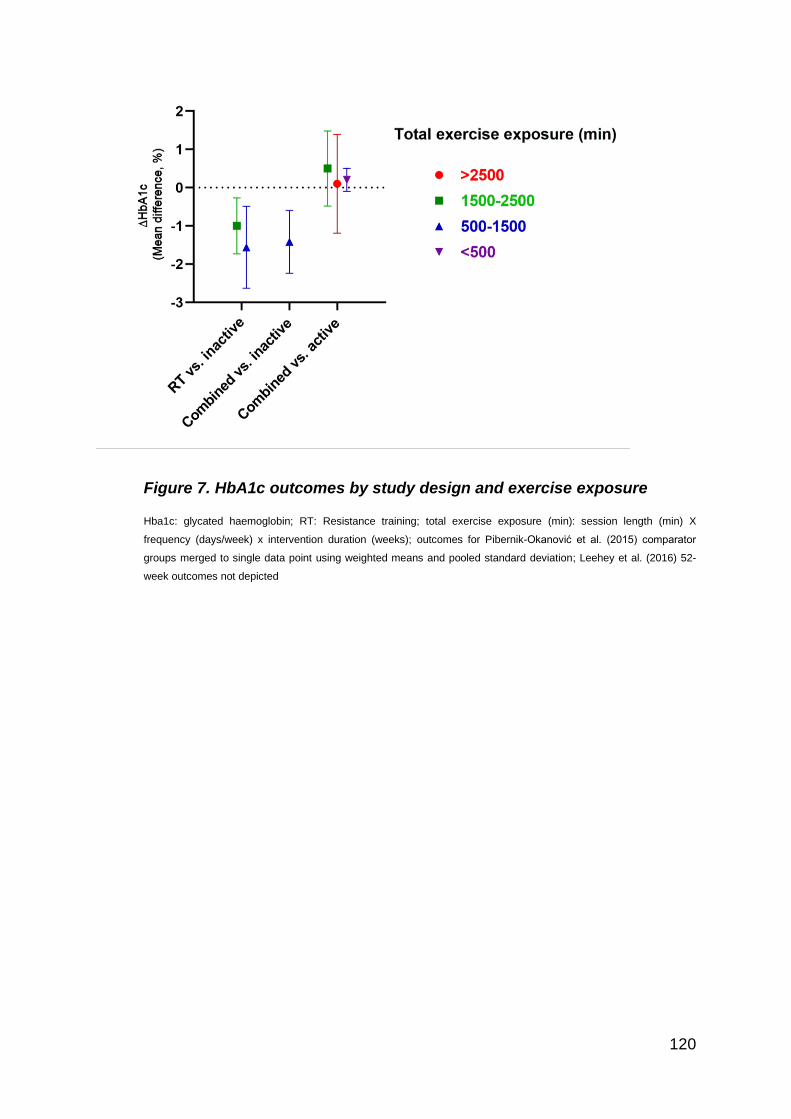
120
Figure 7. HbA1c outcomes by study design and exercise exposure
Hba1c: glycated haemoglobin; RT: Resistance training; total exercise exposure (min): session length (min) X
frequency (days/week) x intervention duration (weeks); outcomes for Pibernik-Okanović et al. (2015) comparator
groups merged to single data point using weighted means and pooled standard deviation; Leehey et al. (2016) 52-
week outcomes not depicted
121
CHAPTER 3: The Progressive Resistance Training in
Metabolic syndrome and Depression Integrative Care (PRT
MEDIC) trial: A randomised controlled trial.
Alexander Bate1, Maria Fiatarone Singh, MD, FRACP123, Yorgi Mavros, PhD1
1Faculty of Medicine and Health, University of Sydney, Australia
2Professor, Sydney Medical School
3John Sutton Chair of Exercise and Sport Science, Sydney School of Health Sciences
Corresponding author:
Alexander Bate, B.Ex&Sp.Sc, Grad. Dip. Ex Phys, ESSAM AEP
Mail: Level 6, Susan Wakil Health Building, D18 The University of Sydney NSW 2006 Australia
Tel: +61 432 588 554; Fax: +61 (2) 9351 9163; Email: [email protected]
122
Abstract
Background: Individuals with metabolic syndrome and major depressive disorder are
at a high risk of developing type 2 diabetes. Alternative treatments to pharmacological
management are required to address both metabolic syndrome components and
depressive symptoms in these individuals.
Aim: To determine the effectiveness of 12 weeks of high intensity progressive
resistance training (PRT) on insulin resistance and depressive symptoms in individuals
with metabolic syndrome and major depressive disorder.
Design: Single blind, randomised controlled trial.
Primary outcome: Homeostatic Model of Assessment 2 (HOMA2-IR) and depressive
symptoms as measured by the Hamilton Rating Scale for Depression (HAM-D).
Secondary outcomes: Depressive symptoms on the Patient Health Questionnaire-9
(PHQ-9), The Center for Epidemiological Studies-Depression (CES-D) and fasting
glucose, 2-hour glucose, and area under the curve on following a 75-g oral glucose
tolerance test.
Method: Eleven participants were randomised to receive high intensity PRT (n=4) or
usual care (n=7). Participants in the PRT group trained three times per week under
direct supervision at 80% of their maximum strength, for 12 weeks. Participants in the
usual care group were referred back to their general practitioner.
Results: One participant from the usual care was lost to follow-up due to COVID-19
restrictions preventing follow-up assessment. Of the remaining 10 participants, no
significant group x time interactions were observed for either primary outcome, however

123
a significant group x time interaction was observed for reductions in depressive
symptoms on the PHQ-9 and CES-D (p<0.05).
Conclusion: 12 weeks of high intensity PRT may be an effective strategy to improve
depressive symptoms in individuals with comorbid metabolic syndrome and major
depressive disorder, which may translate to a future reduction in risk of type 2 diabetes.
Given the small sample size, further research is warranted.
124
Introduction
Type-2 diabetes mellitus (T2DM) is a chronic condition that affects almost 1 million
Australians,1 costing $10.6 billion in both direct healthcare and government subsidies in
2005.2 Individuals with diabetes have up to five times the mortality risk as those with
normal glucose tolerance3 and twice the healthcare costs.2 The AusDiab study reported
the incidence of T2DM in 2011/2012 to be 0.7% amongst adults aged 25 years and
over, with approximately 275 adults developing T2DM every day.3 Projections estimate
that in 2030 there will be over 1.5 million adults in Australia with diabetes, 85-90% of
whom will have T2DM.3 Thus, early targeted interventions in individuals at risk of
developing type 2 diabetes is crucial to reducing diabetes-related morbidity and
mortality as well as the managing the increasing economic burden.
Two risk factors associated with the pathogenesis of T2DM are metabolic syndrome
and depression. Metabolic syndrome is recognised as a cluster of cardiac and
metabolic risk factors that are significantly associated with future risk of T2DM:
abdominal obesity; impaired fasting glucose; hypertension; and atherogenic
dyslipidaemia.4 A meta-analysis of 9 cohorts found that those with metabolic syndrome
according to International Diabetes Federation (IDF) criteria were 4.4 times more likely
to develop T2DM than those without metabolic syndrome over 5 years.5 Major
depressive disorder (MDD) is a widespread and serious unipolar affective disorder
characterised by a state of low mood and aversion to activity which negatively affects
125
the way a person feels and acts, causing a loss of enjoyment and feelings of sadness.6 7
Like metabolic syndrome, MDD is independently associated with incident T2DM, with
individuals with MDD or depressive symptoms 1.3-to-1.4 times more likely to develop
T2DM over 3-to-16 years.8 Both metabolic syndrome and MDD share common
pathophysiological pathways include hypothalamic-pituitary-adrenal axis hyperactivity,
stress-induced activation of the sympatho-medullary pathway, elevated cytokines and
decreased brain-derived neurotrophic factor (BDNF),9 10 which may explain why bi-
directional associations have been found in prospective studies.11 More recently,
individuals with ≥3 metabolic syndrome criteria (as defined by the IDF)12 and depressive
symptoms (Patient Health Questionnaire (PHQ)-9 ≥ 6) had over six times the odds of
developing T2DM over 4.5 years compared to healthy individuals.13 Additionally, a
synergistic effect was found between the two conditions, with the combined effect of
metabolic dysregulation and depressive symptoms being greater than the sum of the
individual effects. Thus, individuals with both metabolic syndrome and MDD represent a
high-risk cohort who require robust management in order to reduce their chance of
developing T2DM, and the subsequent increase in morbidity and mortality that is
associated with comorbid T2DM and mental health conditions.14
Drug therapy regimes for individuals with concurrent depression and metabolic
syndrome often require multiple medications targeting dyslipidaemia, hypertension, and
insulin resistance, as well as depressive symptoms.15 16 Polypharmacological
treatments increase the risk of adverse drug effects,17 as well as drug-drug
interactions,18 without always directly targeting the underlying pathophysiology. In

126
contrast, exercise has been shown to be an effective treatment for depressive
disorders19 20 and improving clinical outcomes in cohorts with metabolic syndrome.21 22
In the Diabetes Prevention Program, exercise in combination with diet modification was
found to be more effective at reducing incidence of T2DM (55% reduction) than
metformin (31% reduction) in populations at risk of T2DM, as compared with placebo.23
Similarly, when aerobic exercise has been compared to sertraline in head-to-head trials
in patients with MDD, both interventions were found to be similarly beneficial for
reduction of symptoms and remission of MDD when compared with placebo.24
Additionally, while efficacy was comparable between exercise and sertraline,
participants in the pharmacotherapy group were 20-times more likely to discontinue
treatment due to adverse effects of the intervention.25 26 Thus, exercise interventions
present a clear therapeutic alternative to drug therapies for MDD and metabolic
syndrome independently.
Progressive Resistance Training (PRT) is a modality of exercise in which the muscles
are worked against an external resistance that is increased in accordance with the
individual’s increases in strength.27 Meta-analyses have indicated the significant effect
resistance training has on both depressive symptoms28 and cardiometabolic risk
factors.29 Importantly, PRT has been shown to improve the underlying mechanistic
factors common to both metabolic syndrome and MDD, including levels depression-
linked sarcopenia,30 31 inflammatory pathways,32 and insulin resistance.33-35 By targeting
the pathophysiology of these conditions, and their potential bidirectional interaction,36
PRT may be used as an early and effective non-pharmaceutical treatment.
127
As stated in Chapter 2 of this thesis, our systematic review found only a small body of
low-quality evidence that was restricted to adults with T2DM, with no studies recruiting
individuals with a diagnosis of MDD. Moreover, the data that were found in cohorts with
T2DM largely examined depressive symptoms as secondary outcomes, and were
judged to be at a high risk of bias due to the use of self-rated assessments for
depression, as opposed to clinician-rated outcomes. Thus, the effectiveness of PRT in
the reduction of depressive symptoms and cardiometabolic risk factors in individuals
with MDD who are at high risk of developing T2DM (e.g., those with metabolic
syndrome) is unknown. To address these gaps in the literature, the PRT Medic
(Progressive Resistance Training for Metabolic syndrome and Depression Integrated
Care) study was designed to test for the first time the efficacy of a 12-week, high
intensity PRT program in addition to usual care in adults with co-morbid metabolic
syndrome and MDD. We hypothesised that:
1. 12 weeks of high intensity PRT in addition to usual care will significantly improve
clinician-rated, blindly assessed depressive symptoms measured via Hamilton
Depression Rating Scale (HAM-D).
2. 12 weeks of high-intensity PRT in addition to usual care will significantly reduce
insulin resistance, as measured via Homeostatic Model of Assessment-2
(HOMA2-IR) compared to controls referred for usual care.

128
Key secondary objectives of the study were to determine the effect of PRT on self-rated
symptoms of depression on the PHQ-9, and Center for Epidemiologic Studies
Depression Scale (CES-D), remission of the depressive episode, improvements in
metabolic syndrome components, improvements in glucose tolerance, body
composition and central haemodynamics, as well as reductions in systemic
inflammation and cortisol.
129
Methods
Trial Design
The study was approved by the University of Sydney Human Research Ethics
Committee (HREC project no. 2017/066) and was registered on the Australia and New
Zealand Clinical Trials Registry (ACTRN12617000400369). This was a single-centre,
single-blind, randomised controlled trial (RCT) with a 1:1 allocation ratio to each group.
Between July 2017 and February 2020, 11 adults over 40 years of age were
randomised to receive usual care (n=7) or usual care and high intensity PRT (n=4). All
participants were assessed at baseline and at 12 weeks. Due to the nature of the
intervention, participants were unable to be blinded as to group allocation. The study
was conducted at the University of Sydney, Cumberland Campus, Lidcombe, NSW,
Australia. Assessments and training sessions were conducted in separate buildings to
maintain assessor blinding.
Participants
Eligible participants were community-dwelling adults aged 40 and above, with metabolic
syndrome criteria as defined by the IDF Consensus Statement,4 and major depressive
disorder according to the Diagnostic and Statistical Manual (DSM)-5(R)7 criteria.
Participants were eligible if they were currently experiencing symptoms of depression (a
PHQ-9 ≥ 5 for participants receiving antidepressant therapy and PHQ-9 ≥ 10 for
participants not currently receiving anti-depressant therapy or other treatment for
130
depression), were previously diagnosed with MDD by a general practitioner, psychiatrist
or psychologist, and did not have a change in anti-depressant medication within the
previous 3 months. For participants without a diagnosis of MDD but who were
experiencing symptoms of MDD (PHQ-9 ≥10), a current episode of MDD was confirmed
by the study physician at in-person screening according to DSM-5(R) diagnostic criteria.
Participants were required to be sedentary with no current participation in a resistance
training exercise program and agree to commit to 3 sessions of supervised training per
week for a continuous 12-week period.
Exclusion criteria were: diagnosis of T2DM; illnesses or musculoskeletal conditions that
contraindicated resistance training; use of insulin or other hypoglycaemic medication;
commencement or alteration of treatment for depression (pharmacological or
counselling) within the previous 3 months; commencement or alteration of treatment for
any components of metabolic syndrome within the previous 3 months; undertaking
active weight loss (e.g., through a diet); alcohol abuse or dependence defined as 3 or 4
on the Cut Annoyed Guilty Eye (CAGE) questionnaire;37 self-reported use of illicit drugs;
participation in a structured exercise regime or >150 min/week of moderate-to-vigorous
physical activity; presence of a terminal or rapidly progressing illness; and assessed as
currently suicidal or at risk of suicide or self-harm. Unintentional weight loss attributable
to depression did not preclude participation. Refer to Table 1. for full list of inclusion and
exclusion criteria.
131
Pre-screening
Initial eligibility pre-screening was conducted by telephone interview or by online
questionnaire. Figure 1. depicts the order of eligibility criteria assessed during pre-
screening.
Potential participants were first screened for basic eligibility criteria of age, diagnosis of
T2DM or use of hypoglycaemic medication, or potential alcohol dependency. Next,
history of depression and use of anti-depressant medication was collected, and
depressive symptoms were assessed using the PHQ-9 questionnaire. A PHQ-9 ≥ 5 for
those receiving antidepressant therapy and PHQ-9 ≥ 10 for those not receiving anti-
depressant therapy or other treatment for depression were considered to have sufficient
symptom severity to proceed to full telephone screening. Individuals who gave positive
responses to PHQ-9 items regarding thoughts of self-harm were followed-up for
potential active suicidal ideation, with referral to appropriate services if required. Those
who were still eligible following pre-screening proceeded to a full telephone screen
consisting of a 30-minute interview questionnaire designed to fully inform them about
the study procedures, and gather personal and demographic information, information on
medical history, medication use, current physical activity levels, and assess the
participant for inclusionary and exclusionary criteria. Individuals who were potentially
eligible were then asked to perform a blood test to assess glucose, glycated
haemoglobin (HbA1c) and blood lipids. To be eligible for baseline assessment,
individuals were required to satisfy IDF metabolic syndrome criteria (Table 1.), and not
be found to have T2DM (fasting blood glucose > 7mmol/L or HbA1c ≥ 6.5%). As the

132
minimum waist circumference was unable to be verified during telephone screening,
central obesity was assumed if the participant’s body mass index was >30 kg/m2, as per
IDF protocol. As required to confirm eligibility, waist circumference and resting blood
pressure were measured in clinic. Once the potential participant had been assessed as
meeting metabolic syndrome criteria and depressive symptom severity, they were then
invited to a baseline in person assessment.
Participant flow through study
Refer to Figure 2 for an overview of participant flow through the assessment battery. At
baseline and 12 weeks, participants were required to attend the clinic on three separate
days, spread over 2 weeks. Day 1 consisted of: informed consent; psychological
questionnaires (PHQ-9, HAM-D, CES-D, Oxford Happiness Scale, Beck Anxiety
Inventory, Positive and Negative Affect Schedule, Core Self Evaluation, demographics);
cognitive testing (National Institutes of Health (NIH) toolbox, Trail Making Test, delayed
word recall); physician screening with medical and psychiatric history and physical
examination, including confirmation of a current bout of MDD according to DSM-5 (R)
criteria,7 but without suicidal ideation/intent; a graded treadmill exercise test to volitional
fatigue with 12-lead electrocardiography; and one-repetition maximum (1RM) strength
testing. Cognitive testing and psychological questionnaires were undertaken prior to
exercise testing in order to avoid any acute antidepressant or cognitive effects of
exercise. Participants were then provided instructions on completing a 3-day food diary
prior to the next assessment, as well as fitted with Actigraphs (wGT3X-BT, Actigraph,
LLC, Pensacola, FL, USA). and given instructions to log wear times.
133
Day 2 of assessment was conducted at least 8 days after day 1 to allow for 7 full days
of Actigraph data collection. Participants attended day 2 in a fasted state, with
assessments consisting of: anthropometry (stretch stature, naked weight, waist
circumference); body composition analysis using dual-energy X-ray absorptiometry
(DXA); and haemodynamic testing - pulse wave analysis (PWA) and pulse wave
velocity (PWV). Participants’ 3-day food diary was also reviewed and completed with
the assistance of an investigator. At the conclusion of the assessment, participants were
fitted with an a 24-hour ambulatory BP monitor. Using their completed 3-day food diary
as a guide, participants were provided with instructions as to how to modify their diet to
achieve 300 g/day of CHO for the 3 days preceding the oral glucose tolerance test
(OGTT) on assessment day 3. Participants were also asked to record their food intake
on these three days to verify their CHO intake.
Day 3 of assessment was scheduled at least 4 days after assessment day 2 in order to
allow for 3 days of 300 g/day CHO intake. An OGTT was scheduled in the morning with
participants presenting in a fasted state. After OGTT testing was completed,
participants were provided with breakfast, and 1RM testing was repeated (at baseline
only).
Blinding
The study physician and all assessors were blind to group allocation. Assessment
sessions were conducted in a separate building to training sessions in order to maintain
134
assessor blinding. Participant monitoring throughout the intervention was performed by
trainers either face-to-face or by telephone.
Primary outcome measures
Depressive symptoms
Depressive symptoms were quantified with the clinician-rated HAM-D.38 The HAM-D
consists of 17 questions/observations probing the range of depressive symptoms/signs,
giving a total score from 0 (normal) to 52 (very severe depression). Measures of
depressive symptoms at baseline were conducted prior to exercise testing and
measures at 12 weeks were scheduled at least 72 hours following the final training
session for participants randomised to the intervention group. This was done to remove
any acute effect of exercise on depressive symptoms, ensuring the result reflected a
chronic improvement in symptoms.
Insulin resistance
Insulin resistance was determined using HOMA2-IR using fasting plasma glucose and
insulin at both baseline and 12 weeks. Measurement of insulin resistance at 12 weeks
for participants in the intervention group was scheduled 48 hours after their final training
session. Fasting blood samples were collected from the cubital vein at the clinic by a
team member trained in venepuncture using either a 21-gauge or 23-gauge butterfly
needle. These were immediately refrigerated, then transported the same day to a
commercial pathology laboratory (Douglass Hanly Moir) for analysis. Values for

135
HOMA2-IR were calculated using the HOMA2 calculator developed by the University of
Oxford Diabetes Trials Unit (version 2.2.3, University of Oxford, UK).39
Secondary Outcome Measures
Psychometric questionnaires
Self-reported symptoms of depression were assessed using the PHQ-9 and the CES-D.
For the PHQ-9, a score below 5 (the cut off for mild symptoms) was considered as
remission of depression. The Oxford Happiness Scale (OHS) was administered to
measure positive affect. Other psychometric questionnaires included the Positive And
Negative Affect Schedule (PANAS), the Beck Anxiety Inventory (BAI), and the Core
Self-Evaluations. Psychometric questionnaires at baseline were conducted prior to any
exercise testing and at 12 weeks were scheduled at least 72 hours after the last
exercise bout for participants randomised to the intervention group. As with the HAM-D,
this was done to remove any acute effect of exercise on depressive symptoms or
general affect, ensuring the result reflected a chronic change in psychological state.
Anthropometry and body composition
Morning fasted stretch stature (wall-mounted Holtain stadiometer; Holtain Limited,
Crymych Pembs, UK) and naked weight (weight in gown [kg] - weight of gown [kg])
were measured to the nearest 0.1 cm and 0.01 kg, respectively, taking the median of 3
measurements. Body composition was performed using Dual-energy X-ray
Absorptiometry (DXA) (Lunar Prodigy scanner and encore software; GE Medical
136
Systems, Madison, WI, USA) to determine whole body and regional muscle, fat, and
bone mass as well as bone mineral density using the lumbar spine (L2-L4) and total hip.
Waist circumference was performed using a Lufkin W606PM measuring tape (Apex
Tool Group LLC, Sparks, Maryland, USA) at the midpoint between the lower costal (10th
rib) and the superior border of the iliac crest, parallel to the ground, at the end of normal
expiration. Three measurements were taken, with the median recorded as the subject’s
waist circumference.
Cognitive assessment
Cognitive testing was performed using the NIH Toolbox cognitive battery,40 Trail Making
Test,41 and Rey Auditory Verbal Learning Test.42 The NIH toolbox testing was delivered
using an iPad and Bluetooth keyboard. The cognitive testing battery was comprised of
the following tests, in order:
• Picture Vocabulary Test
• Flanker Inhibitory Control and Attention Test
• List Sorting Working Memory Test
• Dimensional Change Card Sort Test
• Pattern Comparison Processing Speed Test
• Picture Sequence Memory Test
• Oral Reading Recognition Test
• Oral Symbol Digit Test
• Auditory Verbal Learning Test
137
After the NIH Toolbox was completed, the participant performed the Trail Making Test
(Test A and B) using pen-and-paper. A delayed word recall test was performed after a
20-minute period from finishing the Auditory Verbal Learning Test, using the same set of
15 words.
Cardiometabolic risk factors
Metabolic syndrome and other cardiometabolic risk factors were measured in a fasting
state, including the withholding of all usual medications taken on the morning of the
assessment.
Ambulatory blood pressure was recorded over 24 hours using AtCor Medical Oscar 2
(Oscar 2; AtCor Medical, Sydney, NSW, Australia) blood pressure monitoring device.
The device was placed on the non-dominant arm, and participants were instructed to
record events of unusual exertion, and sleep and waking times. This 24-hour blood
pressure monitoring was done at least 24 hours after any exercise testing or training so
as to avoid any effect of post-exercise hypotension and capture any chronic intervention
effects.43
Pulse Wave Analysis (PWA) and Pulse Wave Velocity (PWV) were performed using the
AtCor Medical SphygmoCor XCEL PWA/PWV system (CvMS; AtCor Medical, Sydney,
NSW, Australia). Participants were instructed to be fasted and to not take
138
antihypertensive medication on the day of testing. After 10 minutes of lying supine, the
SphygmoCor cuff was placed on the upper arm and the PWA measurement taken,
including central systolic and diastolic pressures. A second reading was taken after a
short rest. If the difference between systolic readings was < 5 mmHg, the mean was
taken as the PWA value. If the difference was ≥ 5 mmHg, a third reading was taken,
and the median recorded as the PWA measurement. Next, with the participants still
lying supine after PWA measurement, the carotid pulse point palpated and marked.
Participants flexed their hip and knee on the same side as the carotid marking and
placed their fingers on the inguinal crease. The thigh cuff was then applied as proximal
as possible, and the leg straightened back. The distance in millimetres between the
inguinal crease and the proximal edge of the thigh cuff was recorded into the
SphygomoCor Xcel software. Similarly, the straight-line distance between the carotid
marking and proximal edge of the cuff was also measured and recorded. The PWV
measurement was started, and the tonometer placed on the carotid marking as the cuff
inflated. This was maintained until a full set of waveforms were captured and the Xcel
software confirmed an acceptable measurement. The PWV process was repeated for a
second trial, followed by a third if the difference between trials 1 and 2 was ≥ 0.5 m/s.
The mean was taken as the PWV measurement if two trials were conducted, and the
median for 3 trials. The side of the participant used for readings was recorded for
replication at the 12-week assessment.
In addition to measurement of fasting plasma glucose and insulin, blood samples were
analysed for total cholesterol, high density lipoprotein (HDL) and low-density lipoprotein
139
(LDL), triglycerides, C-reactive protein and cortisol at a commercial laboratory
(Douglass Hanly Moir). To account for the diurnal pattern of cortisol, fasting blood
samples were taken between 9am and 10am in all participants.
Aerobic capacity
A graded exercise test on a treadmill was used to assess aerobic capacity. The
participant’s usual gait speed was measured prior to the test, using an Ultra timer
(DCPB electronics, Glasgow, Scotland). The participant was asked to walk 6 meters at
their habitual walking speed with the assessor recording the time taken to walk the
middle 2 meters, so as to exclude 2 meters of acceleration and 2 meters of
deceleration. The procedure is repeated until 2 measures are taken that are within 0.02
m.s-1 of each other. These measures are then averaged, converted to km/hr, and set as
the treadmill speed at 0% incline. The incline was increased by 2% every minute until
test termination due to volitional fatigue or physician decision due to abnormalities,
which included but were not limited to:
o abnormalities of pulse or ECG noted by physician/research assistant such
as:
▪ Change in resting ECG compared to old tracing suggesting new or
indeterminant age infarct such as q waves, t wave inversions);
▪ Angina or probable angina with exercise (with or without ECG
changes);
▪ Ventricular tachycardia (1 x 3-beat run or worse ventricular
arrhythmias;
▪ New onset atrial flutter or atrial fibrillation during exercise (not
known or intermittent or rate related atrial arrythmias);
▪ ST elevation of 2mm or more compared to rest;
140
▪ Third degree block or increased 2nd degree block;
▪ Lack of chronotropic response with increasing workload;
▪ Pacemaker failure;
▪ Drop of systolic BP greater than 20mmHg compared to standing BP
at rest;
o Failure of technical equipment,
o Signs of poor perfusion (light-headedness, confusion, pallor, nausea, cold
and clammy skin); or
o Other patient instability clinically: Cardiovascular, Pulmonary, Gait, CNS or
other.
The test also included indirect calorimetry for the assessment of maximal oxygen
uptake (VO2peak) using an Ultima PFX series (MGC Diagnostics, St. Paul, Minnesota,
U.S.A) pulmonary function/stress testing system. Throughout the test, participants were
monitored with 12-lead electrocardiogram (Quinton Q-stress system, Quinton 4500
Stress Test Monitor and Quinton Automatic BP monitor model 412, Bothell, WA, U.S.A).
Strength Testing
One-repetition maximum testing was performed on Keiser pneumatic sports strength
training equipment (Keiser Sports Health, Ltd, Fresno, CA, USA) machines for leg
press, seated chest press, triceps pushdown, seated knee extension, and seated knee
flexion. Resistances were increased in response to participant rating of perceived
exertion (Borg 6-20 RPE scale)44 until one repetition could not be performed with
satisfactory technique. The participant was then given a one-minute rest before being
allowed a second attempt at the same resistance. If the second attempt was judged a
failure, then the participant was considered to have reached his/her peak strength and
141
the highest successful resistance completed was taken as the 1RM. Participants were
given verbal encouragement during 1RM attempts. This 1RM testing was conducted
twice at baseline 8 days apart to minimise potential learning effects. For each machine,
the highest value from both attempts at baseline was used.
Physical activity and sleep
Subjective sleep duration and quality was measured using the Pittsburgh Sleep Quality
Index (PSQI)45 and the Insomnia Severity Index (ISI).46 Objective physical activity,
sedentary behaviour and sleep measures are recorded with Actigraph accelerometers.
The activity Actigraph was placed on the hip on the non-dominant side, taken off at
night and when bathing, and worn for 8 days. A matching Actigraph for recording sleep
was placed on the non-dominant wrist, also worn for 8 days, and only removed when
bathing. Participants were given a log in order to record times when the Actigraphs are
removed. The ActiLife software program (version 6.13.4, Actigraph, LLC, Pensacola,
FL, USA) was used to initialise, download, and analyse data from both monitors. Self-
reported physical activity levels were estimated using the Paffenbarger Physical Activity
Questionnaire,47 which was undertaken by the participant with assistance provided by
the examiner if necessary for distance and steps measurements.
Food Diary
Energy intake and macronutrients were quantified using a 3-day food diary. The
participant was asked to record 2 weekdays and 1 weekend day of usual food intake,

142
selecting consecutive days where possible. They were allowed the option of recording
food intake by either written template, or using an iPhone application (Research Food
Diary, Xyris Pty Ltd.), and were offered the use of a portable kitchen scale to assist with
accurate measurement. Once 3 days of food intake were recorded, data were
transferred to the FoodWorks 8 (FoodWorks, Xyris Pty Ltd.) program for analysis. Upon
attendance of their next assessment day, participants were asked to confirm food logs
and specify ingredients, brands and quantities if necessary.
The results of the 3-day food diary were then used to provide instructions and
suggestions to the participant as to how to achieve 300 g CHO/day for the 3 days
preceding the OGTT. Participants were then asked to repeat the food diary for the 3
days preceding the OGTT to confirm their adherence to the CHO requirements.
Oral Glucose Tolerance Test
Following the fasting blood sample, participants were given a 300 ml drink containing 75
g of carbohydrate (Carbotest) and instructed to consume the drink within 10 minutes.
Blood samples were drawn at 30-, 60-, 90- and 120-min post-ingestion and analysed for
plasma glucose and insulin at a commercial laboratory (Douglass Hanly Moir). Absolute
area under the curve was calculated using the trapezoidal rule: 𝐴𝑟𝑒𝑎 =
1
2∑ 𝑋𝑛
𝑖=1 i-1(yi-1 + y).48 Participants with a 2-hour glucose ≥ 11.1 mmol/L at baseline were
excluded from the study as they would be diagnosed with T2DM and referred back to
their physician.
143
Randomisation
At the completion of baseline assessment, participants were randomised to either the
intervention or usual care group. A concealed, computer-generated sequence of
randomly permuted variable blocks (block size = 2-6) were stratified by sex, age (40-59,
60+), and current drug treatment for depression (yes/no). This sequence was generated
(www.randomization.com) by an investigator not involved in the assessment or training
sections of the study, and then concealed in sealed, opaque envelopes. After
completing all baseline assessments, participants opened the next envelope in the
sequence of the appropriate stratum to learn their group allocation.
Monitoring
Participants were monitored for adverse events and changes in depressive symptoms
post-randomisation. Adverse event monitoring consisted of weekly questionnaires
administered automatically using Research Electronic Data Capture (REDCap).
Participants were asked to report acute illnesses, visits to healthcare professionals,
changes in medications or supplements, changes in management of depression or
metabolic syndrome, and changes in any physical or psychological symptoms.
Depression symptoms were assessed fortnightly also via REDCap using the CES-D. If
automatic surveys were not completed within 3 days, participants were called by a
trainer to have questionnaires completed over the phone.
144
Data management
Data from telephone screens, questionnaires and assessments were entered into a
secure REDCap server managed by University of Sydney. Where data were not entered
directly into REDCap, they were recorded in hardcopy and entered later. Hardcopies
were then scanned, with digitized copies stored on a secure server managed by
University of Sydney and hardcopies archived at a secure university storage facility.
Interventions
Usual care
Participants allocated to the usual care group were referred back to their general
practitioner for ongoing treatment of any medical conditions. The GP was sent a copy of
baseline assessment results with details on the participant’s metabolic syndrome and
depressive symptoms.
Progressive resistance training + usual care
In addition to usual care, participants allocated to the intervention group underwent PRT
3 days/week at the exercise clinic located at the University of Sydney, Faculty of Health
Sciences, Cumberland Campus. The exercise clinic was located in a separate building
to the assessment area so as to prevent un-blinding of assessors. All exercise sessions
were fully supervised by investigators not involved in assessments. All trainers had a
degree in exercise physiology or exercise and sport science. Participants performed 8
machine or free-weight exercises: leg press, knee extension, knee flexion, chest press,

145
seated row, seated triceps dip, machine hip abduction, and calf raises. The machines
used were pneumatic strength training equipment (Keiser Sports Health Ltd., Fresno,
CA USA), which allow for changes in resistance in increments of approximately 1
newton (N).
Resistance training sessions began with a warm-up set, followed by 3 sets of 8
repetitions at 80% of 1RM. Total session time was approximately 45 minutes, with a
ratio of no more than 1 trainer for 4 participants. Repeat 1RM testing was also
performed every 2 weeks to assess changes in strength, with the training intensity
adjusted to maintain relative intensity at the prescribed 80% 1RM. Between 1RM testing
sessions, training load was titrated based on the Borg RPE scale (6-20),44 with loads
adjusted continuously to maintain the RPE between 15-18, which is known to
approximate 80% of the 1RM.49
Participants were instructed to achieve a full range-of-motion for all exercises. This was
modified as necessary for participants with joint pain or range-of-motion restrictions by
adjusting seat and movement arm positions.
The protocol for PRT exercises was as follows:
• The participant was shown how each piece of strength training equipment works,
what muscle group it isolates and where this muscle group is located.
• Proper breathing technique was explained and demonstrated to participants
(exhaling on exertion, avoidance of Valsalva manoeuvre).
146
• The participant was placed on the piece of equipment and the settings recorded
to ensure proper biomechanics and to ensure replication for all training sessions
and follow-up assessments.
• The participant performed 3 sets of 8 repetitions on each machine. Each
repetition was slow for both the concentric and eccentric phase (3-4 seconds),
with a 2-3 second rest between repetitions and 60-90 seconds rest between sets.
In the case where musculoskeletal conditions preclude participation in some exercises,
alternative exercises that use the same muscle groups were substituted. If substitution
was not possible, a rehabilitation program was provided, or the joint/area in question
was not exercised. For example, should a participant be limited on chest press and
seated row exercises by rotator cuff pathology, motion on these exercises was limited
within the pain-free range. If a pain-free range of motion was unable to be performed,
these exercises were substituted with biceps curls, triceps extensions, and
internal/external rotation as tolerated.
The trainer discussed with the participant any problems that occurred before, during, or
after each training session regarding muscle or joint soreness, presyncope, or any other
kind of adverse reaction. Serious adverse during exercise sessions events were
reported immediately to the study physician. Upper limb and lower limb exercises were
alternated to manage fatigue, so that performance in subsequent exercises for major
muscle groups was not impaired.

147
Sample Size
We used results from our previous our high intensity PRT studies to estimate sample
sizes. In a previous study of PRT in older adults with T2DM, the Graded Resistance
Exercise And Type 2 Diabetes in Older adults (GREAT2DO) trial,50 a moderate effect
size of -0.78 was seen for reductions in HOMA2-IR after 6 months of the intervention in
individuals with depressive symptoms at baseline. In another study, 8 weeks of PRT
reduced depressive symptoms in older adults with MDD, with large effect sizes of -1.0
and -1.8 for the HAM-D and the Geriatric Depression Scale (GDS), respectively.51 Thus,
choosing the smaller effect size of -0.78 for HOMA2-IR, and assuming a beta of 0.8, we
estimated that a sample size of 22 participants per group (44 total) would be required to
detect a significant effect for both of our primary outcomes of insulin resistance and
symptoms of depression. Table 2. shows effect size and sample size calculations from
pilot data from the GREAT2DO study and previously published data.
Impact of COVID-19
Data collection and analysis were impacted by the spread of SARS-CoV-2 and
subsequent public health restrictions during the timeframe of the study. This resulted in
suspension of participant recruitment and data collection, preventing the study from
reaching the planned sample size. One participant allocated to the usual care group
was unable to attend 12-week outcome assessments due to public health restrictions
and is therefore not included in the outcomes analysis. Due to restrictions placed on
being able to attend the university campus, computers that contained the necessary
software to view, clean, analyse and export specific data were not accessible, and were

148
therefore not included in this chapter. These data include: cognitive testing (NIH
toolbox, trail making test, and delayed word recall); subjective and objective sleep
(Actigraph data; PSQI; ISI); exercise stress test; 1RM testing; PWA and PWV; heart-
rate variability; DXA; and some questionnaire data (Beck Anxiety Inventory; PANAS;
Core Self Evaluation; Paffenbarger physical activity questionnaire). Thus, the only data
available for this chapter were psychological outcomes, blood glucose including fasting
and OGTT outcomes, blood lipids, CRP and cortisol, ambulatory blood pressure and
waist circumference. No other deviations from the protocol occurred.
Data analysis
Data are presented as mean ± SE. Data were inspected for normality using frequency
histograms and skewness statistics, and any outliers inspected. No data were
subsequently removed. To test the primary hypothesis, a repeated measures ANOVA
was used to determine effects of time and group x time interaction. Data for 10
participants were available for depression outcomes. Data for one participant allocated
to PRT were unable to be collected at 12 weeks for all other outcomes and were
therefore not included (n=9 for all other models). A two-tailed, repeated measures
ANOVA was used to determine effects of time and group x time interaction on all
secondary outcome variables as well. For all continuous variables, scores pre- and
post-intervention were used. For CES-D, where additional unblinded measures were
collected fortnightly during the trial by trainers, an additional exploratory repeated
measures ANOVA model was performed using data from all assessments (n=8), with
post-hoc tests performed only after a significant group x time interaction to identify

149
significant differences between all pairwise comparisons. Due to the small sample size,
post-hoc tests were done without adjustment for multiple comparisons, and thus any
significant findings would be considered exploratory. No covariates were added to
repeated measures ANOVA models to prevent over-fitting. Mean difference and 95%
confidence intervals were calculated.52 Cohen’s d effect sizes (ES) were calculated
using the reported means and pooled baseline SDs using the formula: 𝑑 =
(𝑚𝑒𝑎𝑛 𝑑𝑖𝑓𝑓𝑒𝑟𝑒𝑛𝑐𝑒𝑖𝑛𝑡𝑒𝑟𝑣𝑒𝑛𝑡𝑖𝑜𝑛 )− (𝑚𝑒𝑎𝑛 𝑑𝑖𝑓𝑓𝑒𝑟𝑒𝑛𝑐𝑒𝑐𝑜𝑚𝑝𝑎𝑟𝑖𝑠𝑜𝑛 )
𝑝𝑜𝑜𝑙𝑒𝑑 𝑏𝑎𝑠𝑒𝑙𝑖𝑛𝑒 𝑆𝐷.53 54 Effect sizes were then adjusted
for small sample bias (Hedges' g) and 95% confidence intervals calculated. Effect sizes
were interpreted following the rule: “negligible”, (< 0.20); “small”,(≥ 0.20 < 0.50);
“moderate”,(≥ 0.50 < 0.80); and “large”,(≥ 0.80).55 For the primary outcomes, negative
effect sizes indicate a reduction (improvement) in depression symptom severity and
HOMA2-IR scores. To test if remission of depression was different between groups at
the end of the intervention, a chi-square (χ2) was performed. Next, a univariable linear
regression was performed to test if changes in depressive symptoms (independent
variables; HAM-D, PHQ-9 and CES-D) were associated with changes in HOMA2-IR,
fasting glucose, 2-hour glucose and area under the curve (dependent variables). Linear
regressions were then adjusted for group allocation with no meaningful effect on results,
and so unadjusted data are presented. All analyses were performed using IBM SPSS
Statistics for Windows, version 27 (IBM Corp., Armonk, N.Y., USA). A p-value <0.05
was considered statistically significant.
150
Results
Participant flow though the study is shown in the CONSORT flowchart in Figure 3.
Baseline participant characteristics are shown in Table 3. Two individuals were deemed
ineligible following baseline assessment: one due to a 2-hour glucose ≥ 11.1 mmol/L
indicating T2DM; and one deemed as not having MDD following physician screening.
Eleven participants completed baseline assessments and were randomised (4 PRT; 7
usual care). One participant in the usual care group was lost to follow-up due to COVID-
19 public health restrictions. Data were not collected for ambulatory BP for 2
participants (1 PRT; 1 usual care) due to insufficient measurements stemming from
equipment failure. Finally, one participant in the PRT group provided psychological
outcomes, BMI, and waist circumference at 12 weeks, but no other data were collected.
At baseline, 3 participants (1 PRT; 2 usual care) satisfied the IDF criterion for raised
fasting glucose on screening; 9 participants satisfied the IDF criterion for hypertension;
4 participants (2 PRT; 2 usual care) satisfied the IDF criterion for low HDL cholesterol;
all participants either satisfied the IDF criterion for raised triglycerides or were taking
lipid-lowering medication, while one participant (PRT) had impaired glucose tolerance.
Ten participants (4 PRT; 6 usual care) had a pre-existing diagnosis of depression, with
one participant having MDD confirmed during the physician screen, with four
participants reporting the current episode as their first (2 PRT; 2 usual care). Three
participants (1 PRT; 2 Usual care) did not report any current treatment for their
151
depressive episode, while six participants (2 PRT; 4 usual care) reported current
antidepressant medication and eight participants (3 PRT; 5 usual care) reported seeing
a psychiatrist or psychologist. Self-reported severity of depressive symptoms according
to the PHQ-9 at baseline was considered moderate-to-severe. with 2 participants (1
PRT; 1 usual care) classified as having mild depressive symptoms, 4 participants (1
PRT; 3 usual care) classified as having moderate severity depression; 1 participant
(usual care) moderately severe depressive symptoms and 4 participants (2 PRT; 2
usual care) having severe depressive symptoms.
Adherence
Median attendance for training sessions was 96% (range 39% to 100%). The most
common reason provided for missed sessions was being away or unavailable, followed
by minor illnesses unrelated to the intervention.
Psychological outcomes
Data are shown in Table 3. Significant effects of time were observed for the HAM-D (p =
0.002), PHQ-9 (p = 0.008), and the CES-D (p < 0.001), all indicating reduced
depressive symptom burden/severity. Effects of time were not significant for the OHS (p
= 0.101). Contrary to our primary hypothesis, a significant group x time interaction was
not observed for HAM-D (p = 0.166). By contrast, a significant reduction in PHQ-9 was
observed in the PRT group compared to usual care (mean difference = -7; 95% CI -
13.96, -0.54, p = 0.037). No significant group x time interaction was observed for OHS
152
(p = 0.057) or CES-D (p = 0.061). However, when the repeated measures ANOVA was
re-run for CES-D with all interim measures included, a significant group x time
interaction was observed (p=0.03), but post-hoc tests did not reveal any significant
differences between any 2 timepoints (p>0.05 for all), likely due to low statistical power.
For all psychological outcomes, Hedges’ g effect sizes ranged from moderate for the
HAM-D (-0.76; 95% CI -2.07, 0.54) to large for the PHQ-9 (-1.14; 95% CI -2.49, 0.22),
CES-D (-1.12; 95% CI -2.48, 0.23), and OHS (0.83; 95% CI -0.48, 2.15), all favouring
the PRT group. Due to the small sample size, confidence intervals for all effect sizes
were large and cross zero, indicating a significant degree of uncertainty in these results.
Seven participants (4/4 PRT, 3/6 usual care; χ2 = 2.9; p = 0.09) achieved remission of
depression by DSM-5(R) criteria as rated by the study physician. By contrast, only 3
people were categorised as achieving remission of depression when assessed by PHQ-
9, all in the PRT group (3/4 PRT and 0/6 Usual care; χ2 = 6.4, p = 0.01). Minimum
clinically important thresholds for change were exceeded for the mean differences of the
PHQ-9 (≥5 point change),56 and the HAM-D ( ≥27.1% change),57 although for the HAM-
D this difference was observed in both groups. For the CES-D, the mean scores for the
PRT group decreased to below the threshold for indication of clinical depression (CES-
D ≥ 16 indicative of clinical depression),58 while this did not occur in the usual care
group.

153
Metabolic outcomes
A significant time effect was observed for 2-hour glucose (p = 0.028), indicating worse
glucose tolerance, however there was no group x time interaction (p = 0.204). No
significant time or group x time interactions were observed for any other metabolic
outcomes (p > 0.05). Moderate effect sizes were observed indicating a worsening of
HOMA2-IR (g = 0.52; 95% CI -0.89, 1.93), a reduction of cortisol (g = -0.59; 95% CI -
2.00, 0.83), and an improvement in HDL-C (g = 0.60; 95% CI -0.81, 2.01) for the PRT
group compared to usual care, however due to the wide confidence intervals, a wide
range of possible effect sizes in either direction are compatible with these data, and
thus these data remain inconclusive.
Body composition
No main effect of time (p = 0.137) or group x time (0.160) were observed for BMI.
Similarly, no significant time (p = 0.638) or group x time (0.703) interactions were
observed for waist circumference. Effect sizes were negligible for both BMI (g = -0.15;
95% CI -1.42, 1.12) and waist circumference (g = -0.11; 95% CI -1.38, 1.15).
Blood pressure
Significant time effects were observed for sleeping systolic (p = 0.003) and diastolic (p =
0.021) pressures, consistent with reduced readings. No other significant time effects
were observed, and no significant group x time effects were observed for any blood
pressure outcomes (p > 0.05). Small effect sizes were observed for awake systolic
pressures (g = -0.33; 95% CI -1.77, 1.11) and asleep diastolic pressures (g = -0.38;
154
95% CI -1.83, 1.06), although due to wide confidence intervals, these data are
inconclusive. All other effect sizes for blood pressure outcomes were negligible.
Inflammation
No time (p = 0.139) or group x time (p = 0.160) interactions were observed for CRP.
The group x time interaction was consistent with a small effect size (g = -0.37; 95% CI -
1.42, 1.12), resulting from a lesser increase in the PRT group relative to usual care.
Confidence intervals for the effect size were wide and crossed zero and are therefore
inconclusive.
Regression analyses
Contrary to our hypothesis, a significant, inverse association was observed between
changes in PHQ-9 and changes in HOMA2-IR across the whole cohort (n=9; r = -0.718;
p = 0.045), indicating that a reduction (improvement) in depression symptoms was
associated with an increase (worsening) in insulin resistance. Similarly, a significant
inverse association was also observed between changes in HAM-D and changes in
OGTT area under the curve (n=9; r = -0.757; p = 0.030). No other significant
associations were observed, though small inverse associations were observed for CES-
D and HOMA2-IR (r = -0.463; p = 0.248), HAM-D and fasting glucose (r = -0.399; p =
0.328), PHQ-9 and OGTT area under the curve (r = -0.332; p = 0.422), and CES-D and
OGTT area under the curve (r = -0.359; p = 0.382), all suggesting a trend that

155
improvements in depressive symptoms were associated with worsening of metabolic
profile.
Adverse events
Two serious adverse events occurred that were not attributed to the study. One
participant in the PRT group was hospitalised for two days with pyelonephritis
secondary to a urinary tract infection. The event occurred after the invention during the
12-week assessment period, therefore no training sessions were missed, but the final
assessment day was postponed by several weeks. One participant in the usual care
group fell at home, causing an ankle sprain, but was still able to complete their 12-week
assessment.
Two minor adverse events were reported in the PRT group (1 visit to massage therapist
for muscle soreness, 1 report of soreness in knees) that were adjudicated as likely
related to the intervention. Neither of these events required exercise modification or
resulted in missed sessions. Four visits to healthcare professionals for pre-existing
musculoskeletal conditions occurred in the usual care group.
156
Discussion
The purpose of this trial was to determine if 12 weeks of high intensity PRT would
reduce depressive symptoms and improve insulin resistance in adults with MDD and
metabolic syndrome. While there was insufficient power to show a significant reduction
in the clinician assessment of depression (HAM-D), the PHQ-9 and CES-D (when all
interim timepoints were included) showed a significant reduction in depressive
symptoms in the PRT group compared to usual care. Importantly, all four participants in
the PRT group were judged to have achieved remission of depression by DSM-5(R)
criteria (compared to three out of six in usual care), and three out of four by PHQ-9
(compared to zero out of six in usual care, a significant difference). Effect sizes for
depressive outcomes were moderate (HAM-D) to very large (PHQ-9, CES-D) favouring
the PRT group, with a corresponding increase in positive affect as observed by a large
effect size for the OHS. Importantly, effect sizes observed in this study are comparable
to similar trials of PRT and depression.51 59-63 This is the first study of PRT in individuals
who had both metabolic syndrome and MDD, and thus we demonstrate that PRT
appears to remain effective as an antidepressant treatment in individuals where
metabolic syndrome is a co-morbidity. Importantly this antidepressant effect of PRT was
not impacted by existing treatment, with 2/4 individuals on drug treatment and 3/4
participants receiving professional counselling. Contrary to our hypotheses however, no
changes were observed in any metabolic syndrome components, including HOMA2-IR,
waist circumference, fasting glucose, blood lipids or ambulatory blood pressure
measurements.
157
Despite there being no improvement in metabolic syndrome components following the
intervention, it is possible that the reduction in depressive symptoms would translate to
a reduction in future risk of T2DM. Prospectively, individuals with metabolic syndrome
and symptoms of depression (PHQ-9 score ≥ 6) were 1.59 times more likely to develop
T2DM in 5 years, compared to individuals with metabolic syndrome only.64 Our PHQ-9
scores suggest complete resolution of the depressive episode in all participants in the
PRT group, compared to none in the usual care group. Thus, it is reasonable to suggest
that despite no improvement in HOMA2-IR scores or OGTT indices over 12 weeks, that
the improvements in depressive symptoms would still lead to a reduction in future risk of
T2DM. Further investigation however would be required in this cohort to determine if the
reduced risk of incident T2DM through remission of depression alone is significant.
The lack of improvement in any metabolic syndrome components is concordant with a
recent review of exercise in metabolic syndrome that included PRT which reported no
evidence of an improvement in any metabolic syndrome components.65 However, the
literature for PRT in individuals with metabolic syndrome remains small, with only three
previous studies. Progressive resistance training has been shown to improve glucose
metabolism,29 66 waist circumference and adiposity,29 67 and blood pressure,29 66 68 and
thus many more robust studies are required. In the review by Wewege et al. (2018),65
subgroup analyses for aerobic training revealed a potential dose response for studies of
higher intensity and longer duration (> 12 weeks), and thus longer-term studies of PRT
are warranted. Importantly, while we did recruit individuals with metabolic syndrome,
there was no requirement to specifically satisfy fasting glucose criteria, while use of
158
medication was also allowed to satisfy criteria for hypertension and dyslipidaemia. This
recruitment strategy may have also reduced the effectiveness of PRT. As can be seen
in Figure 6, only 1 person in the PRT group had an elevated fasting glucose at baseline,
compared to 2 individuals in usual care. Similarly, only one person in the PRT had
impaired glucose tolerance, while baseline HbA1c levels show well-controlled glucose
homeostasis. Thus, the relative lack of impaired glucose metabolism in this cohort may
have precluded any effect of PRT on these outcomes, as previous reviews have
reported that the effects of PRT are greater in those with worse clinical status.66
Similarly, 3/4 and 5/7 participants in the PRT and usual care groups were taking anti-
hypertensive medications at enrolment. Previous reviews of PRT in hypertension have
shown that the effect of PRT is attenuated in individuals who are prescribed anti-
hypertensive medication,69 again potentially precluding any benefit of PRT in this study.
Thus, in addition to studies of longer duration, studies targeting cohorts with worse
clinical status or who are not already treated with medication are required to determine
the effectiveness of PRT.
The results from linear regression were unexpected, in that reductions in depressive
symptoms on the PHQ-9 were associated with worsening of insulin resistance (HOMA2-
IR), and similarly reductions in HAM-D scores were associated with increased area
under the curve following the OGTT. One possible explanation is that participants in the
PRT group could have increased caloric intake in response to the anabolic intervention,
as has been observed in other studies of progressive resistance training in older men
with T2DM.70 While 3-day food records were collected in this study, these data remain
159
unavailable at the time of writing, and thus the reasons for this unexpected association
remain unknown.
There are a number of limitations in this study. Due to the impact of SARS-CoV-2, as
well as other possible impediments such as restrictive inclusion criteria, inadequate
participant incentive, or inadequate recruitment strategy, we were unable to achieve our
intended sample size, and thus we are underpowered to detect our primary outcome. It
is possible that with a larger sample size, more significant outcomes may have been
observed, though it cannot be predicted whether our hypotheses would have been
confirmed. This study is ongoing, and while data collection and participant recruitment
was impacted by SARS-CoV-2, these processes are scheduled to resume so as to
allow the study to meet its goals and intended sample size. It is also of importance to
consider that as a preliminary analysis, we have not accordingly adjusted our critical
alpha as would be done in a pre-specified interim analysis. Thus, the significant findings
in this study should be interpreted with caution. However, the reduction in depressive
symptoms is consistent with previous literature, and this is the first study in individuals
with any manifestation of insulin resistance as a co-morbidity to have a diagnosis of
depression, and the use of a clinician-rated assessment. Additionally, while we
specifically recruited individuals with metabolic syndrome only 3 of 11 participants
satisfied the criterion for elevated fasting glucose at baseline. Had a cohort with
elevated fasting glucose been specifically targeted, a more substantial change in
outcomes that are markers for glucose metabolism may have been seen in the PRT
group.

160
In conclusion, we present the results of the first study of PRT in adults with major
depressive disorder and metabolic syndrome. Despite not reaching our intended sample
size, we do show preliminary evidence that PRT can improve depressive symptoms and
achieve remission of the depressive episode in this cohort. Despite no concomitant
improvement in metabolic syndrome criteria was observed, the reduction in depressive
symptoms alone may be sufficient to reduce the risk of future T2DM in this high-risk
cohort.
161
References
1. Australian Bureau of Statistics. National Health Survey: First Results, 2017-18 2018
[Available from:
https://www.abs.gov.au/ausstats/[email protected]/PrimaryMainFeatures/4364.0.55.001?
OpenDocument.
2. Lee CM, Colagiuri R, Magliano DJ, et al. The cost of diabetes in adults in Australia.
Diabetes Research and Clinical Practice 2013;99(3):385-90. doi:
https://doi.org/10.1016/j.diabres.2012.12.002 [published Online First: 2013/01/10]
3. Tanamas S, Magliano D, Lynch V, et al. AusDiab 2012: The Australian diabetes,
obesity and lifestyle study Baker IDI: Heart and Diabetes Institute 2013
4. Alberti KGMM, Zimmet P, Shaw J. Metabolic syndrome—a new world-wide definition.
A consensus statement from the International Diabetes Federation. Diabetic
Medicine 2006;23(5):469-80. doi: https://doi.org/10.1111/j.1464-
5491.2006.01858.x
5. Ford ES, Li C, Sattar N. Metabolic syndrome and incident diabetes: current state of
the evidence. Diabetes care 2008;31(9):1898-904. doi: 10.2337/dc08-0423
6. Otte C, Gold SM, Penninx BW, et al. Major depressive disorder. Nature Reviews
Disease Primers 2016;2:16065. doi: https://doi.org/10.1038/nrdp.2016.65
[published Online First: 2016/09/16]
7. Diagnostic and statistical manual of mental disorders : DSM-5 (R). Arlington, VA:
American Psychiatric Association 2013.
162
8. Knol MJ, Twisk JWR, Beekman ATF, et al. Depression as a risk factor for the onset
of type 2 diabetes mellitus. A meta-analysis. Diabetologia 2006;49(5):837. doi:
https://doi.org/10.1007/s00125-006-0159-x
9. Naismith SL, Norrie LM, Mowszowski L, et al. The neurobiology of depression in
later-life: Clinical, neuropsychological, neuroimaging and pathophysiological
features. Progress in Neurobiology 2012;98(1):99-143. doi:
https://doi.org/10.1016/j.pneurobio.2012.05.009
10. Rustad JK, Musselman DL, Nemeroff CB. The relationship of depression and
diabetes: Pathophysiological and treatment implications.
Psychoneuroendocrinology 2011;36(9):1276-86. doi:
https://doi.org/10.1016/j.psyneuen.2011.03.005
11. Pan A, Keum N, Okereke OI, et al. Bidirectional association between depression
and metabolic syndrome: A systematic review and meta-analysis of
epidemiological studies. Diabetes Care 2012;35(5):1171-80. doi:
https://doi.org/10.2337/dc11-2055
12. Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a
joint interim statement of the International Diabetes Federation Task Force on
Epidemiology and Prevention; National Heart, Lung, and Blood Institute;
American Heart Association; World Heart Federation; International
Atherosclerosis Society; and International Association for the Study of Obesity.
Circulation 2009;120(16):1640-5. doi:
https://doi.org/10.1161/circulationaha.109.192644 [published Online First:
2009/10/07]
163
13. Schmitz N, Deschenes SS, Burns RJ, et al. Depression and risk of type 2 diabetes:
The potential role of metabolic factors. Molecular Psychiatry 2016;21(12):1726-
32. doi: https://doi.org/10.1038/mp.2016.7 [published Online First: 2016/02/24]
14. Guerrero Fernández de Alba I, Gimeno-Miguel A, Poblador-Plou B, et al.
Association between mental health comorbidity and health outcomes in type 2
diabetes mellitus patients. Scientific Reports 2020;10(1):19583. doi:
https://doi.org/10.1038/s41598-020-76546-9
15. Holvast F, van Hattem BA, Sinnige J, et al. Late-life depression and the association
with multimorbidity and polypharmacy: A cross-sectional study. Family Practice
2017;34(5):539-45. doi: https://doi.org/10.1093/fampra/cmx018
16. Grundy SM. Drug therapy of the metabolic syndrome: minimizing the emerging
crisis in polypharmacy. Nature Reviews Drug Discovery 2006;5(4):295-309. doi:
https://doi.org/10.1038/nrd2005 [published Online First: 2006/04/04]
17. Qato DM, Ozenberger K, Olfson M. Prevalence of Prescription Medications With
Depression as a Potential Adverse Effect Among Adults in the United States.
JAMA 2018;319(22):2289-98. doi: 10.1001/jama.2018.6741
18. Dumbreck S, Flynn A, Nairn M, et al. Drug-disease and drug-drug interactions:
Systematic examination of recommendations in 12 UK national clinical
guidelines. BMJ 2015;350:h949. doi: https://doi.org/10.1136/bmj.h949
19. Schuch FB, Vancampfort D, Richards J, et al. Exercise as a treatment for
depression: A meta-analysis adjusting for publication bias. Journal of Psychiatric
Research 2016;77:42-51. doi: https://doi.org/10.1016/j.jpsychires.2016.02.023
[published Online First: 2016/03/16]

164
20. Kvam S, Kleppe CL, Nordhus IH, et al. Exercise as a treatment for depression: A
meta-analysis. J Affect Disord 2016;202:67-86. doi: 10.1016/j.jad.2016.03.063
21. Joseph MS, Tincopa MA, Walden P, et al. The impact of structured exercise
programs on metabolic syndrome and its components: A systematic review.
Diabetes, Metabolic Syndrome and Obesity : Targets and Therapy
2019;12:2395-404. doi: https://doi.org/10.2147/DMSO.S211776
22. Strasser B, Siebert U, Schobersberger W. Resistance training in the treatment of
the metabolic syndrome: A systematic review and meta-analysis of the effect of
resistance training on metabolic clustering in patients with abnormal glucose
metabolism. Sports Medicine 2010;40(5):397-415. doi:
https://doi.org/10.2165/11531380-000000000-00000 [published Online First:
2010/05/04]
23. Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type
2 diabetes with lifestyle intervention or metformin. The New England Journal of
Medicine 2002;346(6):393-403. doi: https://doi.org/10.1056/NEJMoa012512
[published Online First: 2002/02/08]
24. Blumenthal JA, Babyak MA, Doraiswamy PM, et al. Exercise and pharmacotherapy
in the treatment of major depressive disorder. Psychosomatic Medicine
2007;69(7):587-96. doi: https://doi.org/10.1097/PSY.0b013e318148c19a
[published Online First: 2007/09/10]
25. Qaseem A, Barry MJ, Kansagara D. Nonpharmacologic versus pharmacologic
treatment of adult patients with major depressive disorder: A clinical practice

165
guideline from the american college of physicians. Annals of Internal Medicine
2016;164(5):350-59. doi: https://doi.org/10.7326/M15-2570
26. Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older
patients with major depression. Archives of Internal Medicine 1999;159(19):2349-
56. doi: https://doi.org/10.1001/archinte.159.19.2349 [published Online First:
1999/11/05]
27. Latham NK, Bennett DA, Stretton CM, et al. Systematic review of progressive
resistance strength training in older adults. Journal of Gerontology: Series A,
Biological Sciences and Medical Sciences 2004;59(1):48-61. doi:
https://doi.org/10.1093/gerona/59.1.m48 [published Online First: 2004/01/14]
28. Gordon BR, McDowell CP, Hallgren M, et al. Association of efficacy of resistance
exercise training with depressive symptoms: Meta-analysis and meta-regression
analysis of randomized clinical trials. JAMA Psychiatry 2018;75(6):566-76. doi:
https://doi.org/10.1001/jamapsychiatry.2018.0572
29. Strasser B, Siebert U, Schobersberger W. Resistance training in the treatment of
the metabolic syndrome. Sports Medicine 2010;40(5):397-415. doi:
https://doi.org/10.2165/11531380-000000000-00000
30. Fragala MS, Cadore EL, Dorgo S, et al. Resistance training for older adults: Position
statement from the National Strength and Conditioning Association. The Journal
of Strength & Conditioning Research 2019;33(8) doi:
https://doi.org/10.1519/JSC.0000000000003230
31. Pasco JA, Williams LJ, Jacka FN, et al. Sarcopenia and the common mental
disorders: A potential regulatory role of skeletal muscle on brain function?

166
Current Osteoporosis Reports 2015;13(5):351-7. doi:
https://doi.org/10.1007/s11914-015-0279-7 [published Online First: 2015/08/01]
32. Miller EG, Sethi P, Nowson CA, et al. Effects of progressive resistance training and
weight loss versus weight loss alone on inflammatory and endothelial biomarkers
in older adults with type 2 diabetes. European Journal of Applied Physiolgy
2017;117(8):1669-78. doi: https://doi.org/10.1007/s00421-017-3657-2 [published
Online First: 2017/06/10]
33. Lyra E Silva NdM, Lam MP, Soares CN, et al. Insulin resistance as a shared
pathogenic mechanism between depression and type 2 diabetes. Frontiers in
Psychiatry 2019;10:57-57. doi: https://doi.org/10.3389/fpsyt.2019.00057
34. Holten MK, Zacho M, Gaster M, et al. Strength training increases insulin-mediated
glucose uptake, GLUT4 content, and insulin signaling in skeletal muscle in
patients with type 2 diabetes. Diabetes 2004;53(2):294. doi:
https://doi.org/10.2337/diabetes.53.2.294
35. Rasgon NL, McEwen BS. Insulin resistance—a missing link no more. Molecular
Psychiatry 2016;21(12):1648-52. doi: https://doi.org/10.1038/mp.2016.162
36. Renn BN, Feliciano L, Segal DL. The bidirectional relationship of depression and
diabetes: A systematic review. Clinical Psychology Review 2011;31(8):1239-46.
doi: https://doi.org/10.1016/j.cpr.2011.08.001 [published Online First: 2011/10/04]
37. Ewing JA. Detecting alcoholism: The CAGE questionnaire. The Journal of the
American Medical Association 1984;252(14):1905-07. doi:
https://doi.org/10.1001/jama.1984.03350140051025
167
38. Hamilton M. Development of a rating scale for primary depressive illness. British
Journal of Social and Clinical Psychology 1967;6(4):278-96. doi:
https://doi.org/10.1111/j.2044-8260.1967.tb00530.x [published Online First:
1967/12/01]
39. Holman R, Hines G, Kennedy I, et al. A calculator for HOMA. Diabetologia
2004;47(Suppl. 1: A222)
40. Weintraub S, Dikmen SS, Heaton RK, et al. Cognition assessment using the NIH
Toolbox. Neurology 2013;80(11 Suppl 3):S54-S64. doi:
https://doi.org/10.1212/WNL.0b013e3182872ded
41. Partington JE, Leiter RG. Partington's pathways test. Psychological Service Center
Journal 1949
42. Rey A. L'examen psychologique dans les cas d'encéphalopathie traumatique.(Les
problems.). Archives de Psychologie 1941
43. Kenney MJ, Seals DR. Postexercise hypotension. Key features, mechanisms, and
clinical significance1993.
44. Borg G. Perceived exertion as an indicator of somatic stress. Scandinavian Journal
of Rehabilitation Medicine 1970;2(2):92-98.
45. Buysse DJ, Reynolds CF, Monk TH, et al. The Pittsburgh sleep quality index: A new
instrument for psychiatric practice and research. Psychiatry Research
1989;28(2):193-213. doi: https://doi.org/10.1016/0165-1781(89)90047-4
46. Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an
outcome measure for insomnia research. Sleep Medicine 2001;2(4):297-307. doi:
https://doi.org/10.1016/S1389-9457(00)00065-4
168
47. Paffenbarger RSJ, Wing AL, Hyde RT. Physical activity as an index of heart attack
risk in college alumni. American Journal of Epidemiology 1978;108(3):161-75.
doi: https://doi.org/10.1093/oxfordjournals.aje.a112608
48. Tai MM. A mathematical model for the determination of total area under glucose
tolerance and other metabolic curves. Diabetes Care 1994;17(2):152. doi:
https://doi.org/10.2337/diacare.17.2.152
49. Garber CE, Blissmer B, Deschenes MR, et al. Quantity and quality of exercise for
developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor
fitness in apparently healthy adults: Guidance for prescribing exercise. Medicine
& Science in Sports & Exercise 2011;43(7) doi:
https://doi.org/10.1249/MSS.0b013e318213fefb
50. Simpson KA, Mavros Y, Kay S, et al. Graded Resistance Exercise And Type 2
Diabetes in Older adults (The GREAT2DO study): methods and baseline cohort
characteristics of a randomized controlled trial. Trials 2015;16:512-12. doi:
https://doi.org/10.1186/s13063-015-1037-y
51. Singh NA, Stavrinos TM, Scarbek Y, et al. A randomized controlled trial of high
versus low intensity weight training Versus general practitioner care for clinical
depression in older adults. The Journals of Gerontology: Series A
2005;60(6):768-76. doi: https://doi.org/10.1093/gerona/60.6.768
52. Higgins J, Thomas J, Chandler J, et al. Chapter 6: Choosing effect measures and
computing estimates of effect. In: Higgins J, Li T, Deeks J, eds. Cochrane
Handbook for Systematic Reviews of Interventions: Cochrane 2021.
169
53. Morris SB. Estimating effect sizes from pretest-posttest-control group designs.
Organizational Research Methods 2007;11(2):364-86. doi:
https://doi.org/10.1177/1094428106291059
54. Morris SB, DeShon RP. Combining effect size estimates in meta-analysis with
repeated measures and independent-groups designs. Psychological Methods
2002;7(1):105-25. doi: https://doi.org/10.1037/1082-989X.7.1.105
55. Cohen J. Statistical power analysis for the behavioral sciences. New York:
Academic press 1988.
56. Löwe B, Unützer J, Callahan CM, et al. Monitoring depression treatment outcomes
with the patient health questionnaire-9. Medical Care 2004;42(12):1194-201. doi:
https://doi.org/10.1097/00005650-200412000-00006 [published Online First:
2004/11/20]
57. Masson SC, Tejani AM. Minimum clinically important differences identified for
commonly used depression rating scales. Journal of Clinical Epidemiology
2013;66(7):805-07. doi: https://doi.org/10.1016/j.jclinepi.2013.01.010
58. Siddaway AP, Wood AM, Taylor PJ. The Center for Epidemiologic Studies-
Depression (CES-D) scale measures a continuum from well-being to depression:
Testing two key predictions of positive clinical psychology. Journal of Affective
Disorders 2017;213:180-86. doi: https://doi.org/10.1016/j.jad.2017.02.015
[published Online First: 2017/02/20]
59. Aylin K, Arzu D, Sabri S, et al. The effect of combined resistance and home-based
walking exercise in type 2 diabetes patients. Internation Journal of Diabetes in
170
Developing Countries 2009;29(4):159-65. doi: https://doi.org/10.4103/0973-
3930.57347 [published Online First: 2010/03/26]
60. Singh NA, Clements KM, Fiatarone MA. A randomized controlled trial of progressive
resistance training in depressed elders. Journals of Gerontology Series a-
Biological Sciences and Medical Sciences 1997;52(1):M27-M35. doi:
https://doi.org/10.1093/gerona/52A.1.M27
61. Levinger I, Selig S, Goodman C, et al. Resistance training improves depressive
symptoms in individuals at high risk for type 2 diabetes. The Journal of Strength
and Conditioning Research 2011;25(8):2328-33. doi:
https://doi.org/10.1519/JSC.0b013e3181f8fd4a [published Online First:
2011/06/11]
62. Norvell N, Belles D. Psychological and physical benefits of circuit weight training in
law enforcement personnel. Journal of Consulting and Clinical Psychology
1993;61(3):520-27. doi: https://doi.org/10.1037/0022-006X.61.3.520
63. Lincoln AK, Shepherd A, Johnson PL, et al. The impact of resistance exercise
training on the mental health of older Puerto Rican adults with type 2 diabetes.
The Journals of Gerontology, Series B: Psychological Sciences and Social
Sciences 2011;66(5):567-70. doi: https://doi.org//10.1093/geronb/gbr034
[published Online First: 2011/05/17]
64. Schmitz N, Deschênes SS, Burns RJ, et al. Depression and risk of type 2 diabetes:
The potential role of metabolic factors. Molecular Psychiatry 2016;21(12):1726-
32. doi: https://doi.org/10.1038/mp.2016.7 [published Online First: 2016/02/24]
171
65. Wewege MA, Thom JM, Rye KA, et al. Aerobic, resistance or combined training: A
systematic review and meta-analysis of exercise to reduce cardiovascular risk in
adults with metabolic syndrome. Atherosclerosis 2018;274:162-71. doi:
https://doi.org/10.1016/j.atherosclerosis.2018.05.002 [published Online First:
2018/05/22]
66. Ashton RE, Tew GA, Aning JJ, et al. Effects of short-term, medium-term and long-
term resistance exercise training on cardiometabolic health outcomes in adults:
systematic review with meta-analysis. British Journal of Sports Medicine
2020;54(6):341-48. doi: https://doi.org/10.1136/bjsports-2017-098970 [published
Online First: 2018/06/24]
67. Benson AC, Torode ME, Fiatarone Singh MA. The effect of high-intensity
progressive resistance training on adiposity in children: A randomized controlled
trial. International Journal of Obesity 2008;32(6):1016-27. doi:
https://doi.org/10.1038/ijo.2008.5 [published Online First: 2008/02/20]
68. Naci H, Salcher-Konrad M, Dias S, et al. How does exercise treatment compare with
antihypertensive medications? A network meta-analysis of 391 randomised
controlled trials assessing exercise and medication effects on systolic blood
pressure. British Journal of Sports Medicine 2019;53(14):859. doi:
https://doi.org/10.1136/bjsports-2018-099921
69. MacDonald HV, Johnson BT, Huedo-Medina TB, et al. Dynamic resistance training
as stand-alone antihypertensive lifestyle therapy: A meta-analysis. Journal of the
American Heart Association 2016;5(10):e003231. doi:
https://doi.org/10.1161/JAHA.116.003231
172
70. Ibañez J, Izquierdo M, Argüelles I, et al. Twice-weekly progressive resistance
training decreases abdominal fat and improves insulin sensitivity in older men
with type 2 diabetes. Diabetes Care 2005;28(3):662. doi:
https://doi.org/10.2337/diacare.28.3.662
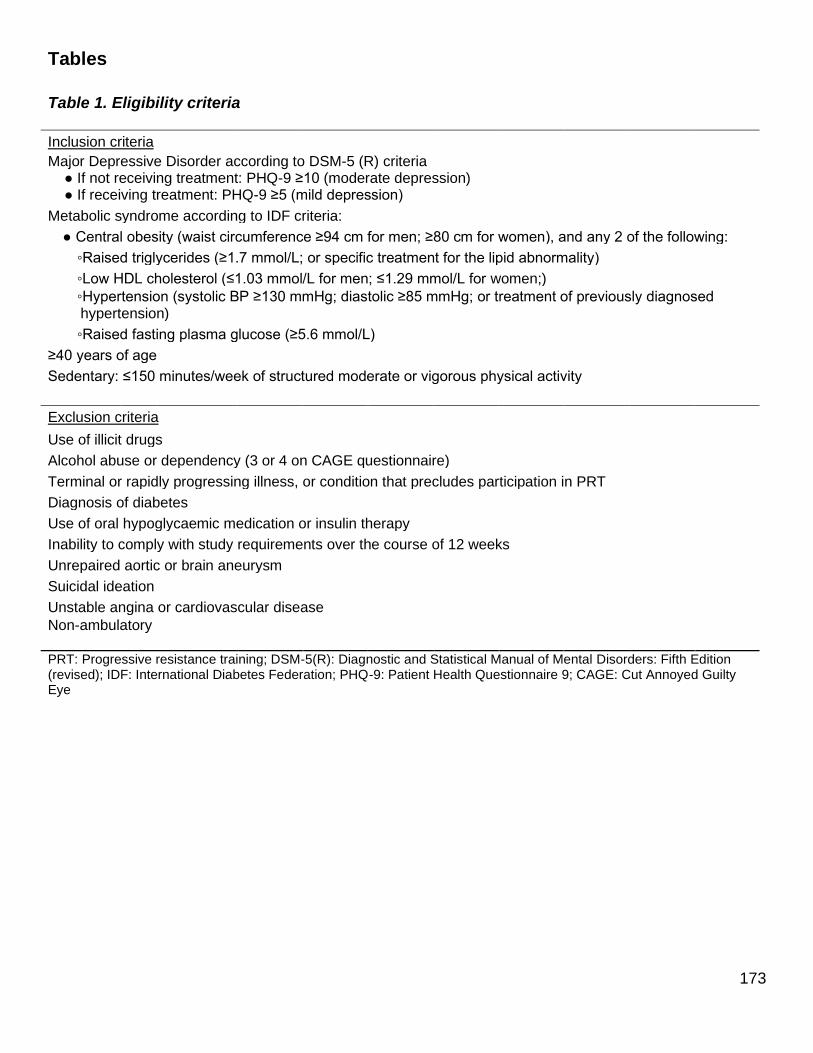
173
Tables
Table 1. Eligibility criteria
Inclusion criteria Major Depressive Disorder according to DSM-5 (R) criteria ● If not receiving treatment: PHQ-9 ≥10 (moderate depression) ● If receiving treatment: PHQ-9 ≥5 (mild depression)
Metabolic syndrome according to IDF criteria:
● Central obesity (waist circumference ≥94 cm for men; ≥80 cm for women), and any 2 of the following:
◦Raised triglycerides (≥1.7 mmol/L; or specific treatment for the lipid abnormality)
◦Low HDL cholesterol (≤1.03 mmol/L for men; ≤1.29 mmol/L for women;) ◦Hypertension (systolic BP ≥130 mmHg; diastolic ≥85 mmHg; or treatment of previously diagnosed
____hypertension)
◦Raised fasting plasma glucose (≥5.6 mmol/L)
≥40 years of age
Sedentary: ≤150 minutes/week of structured moderate or vigorous physical activity
Exclusion criteria
Use of illicit drugs
Alcohol abuse or dependency (3 or 4 on CAGE questionnaire)
Terminal or rapidly progressing illness, or condition that precludes participation in PRT
Diagnosis of diabetes
Use of oral hypoglycaemic medication or insulin therapy
Inability to comply with study requirements over the course of 12 weeks
Unrepaired aortic or brain aneurysm
Suicidal ideation
Unstable angina or cardiovascular disease Non-ambulatory PRT: Progressive resistance training; DSM-5(R): Diagnostic and Statistical Manual of Mental Disorders: Fifth Edition (revised); IDF: International Diabetes Federation; PHQ-9: Patient Health Questionnaire 9; CAGE: Cut Annoyed Guilty Eye
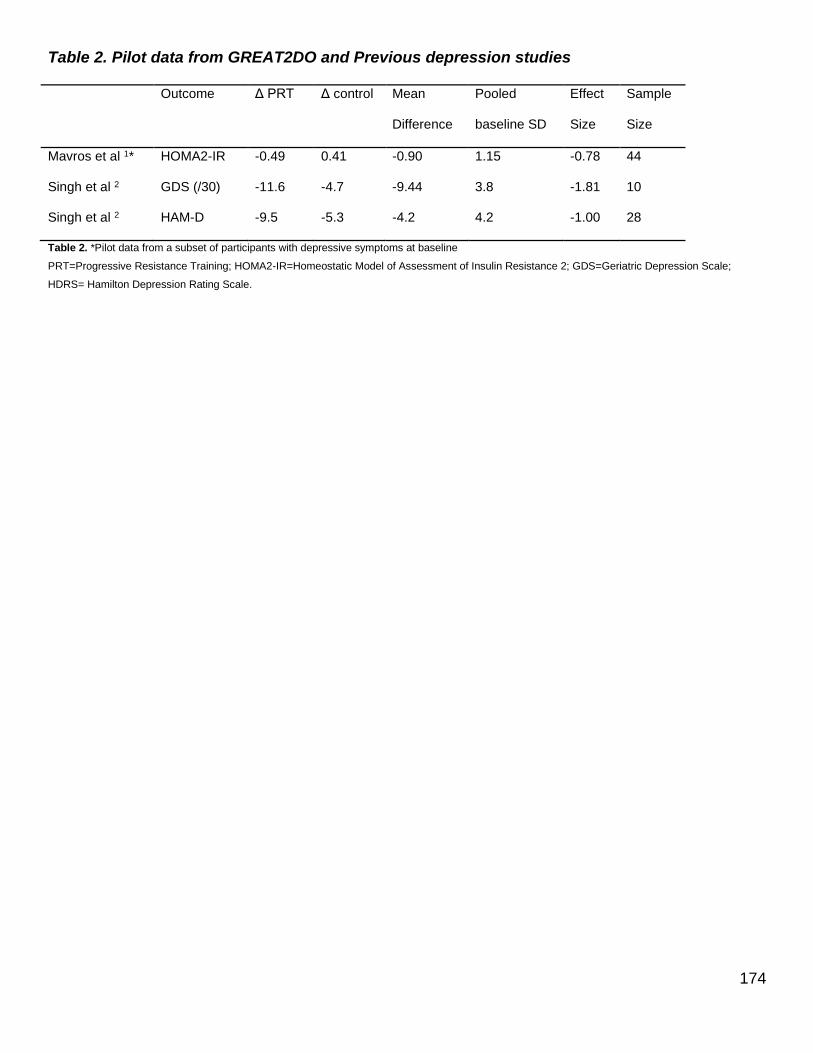
174
Table 2. Pilot data from GREAT2DO and Previous depression studies
Outcome Δ PRT Δ control Mean
Difference
Pooled
baseline SD
Effect
Size
Sample
Size
Mavros et al 1* HOMA2-IR -0.49 0.41 -0.90 1.15 -0.78 44
Singh et al 2 GDS (/30) -11.6 -4.7 -9.44 3.8 -1.81 10
Singh et al 2 HAM-D -9.5 -5.3 -4.2 4.2 -1.00 28
Table 2. *Pilot data from a subset of participants with depressive symptoms at baseline
PRT=Progressive Resistance Training; HOMA2-IR=Homeostatic Model of Assessment of Insulin Resistance 2; GDS=Geriatric Depression Scale;
HDRS= Hamilton Depression Rating Scale.

175
Table 3. Baseline participant characteristics PRT Usual Care
n 4 7
Age (years) 60.7 ±3.46 58.1 ±3.40
Sex (female/male) 3/1 6/1
BMI (kg/m2) 32.9 ±1.00 34.6 ±4.22
Waist Circumference (cm) 106.6 ±7.62 110.3 ±7.90
Cardiometabolic medication
Cholesterol lowering medication (n) 1 5
Antihypertensive medication (n) 3 5
Depression treatment
No current depression treatment (n) 1 2
Antidepressant medication (n) 2 4
Counselling - psychiatrist/psychologist (n) 3 5
Counselling - other (n) 1 1
Electroconvulsive therapy (n) 0 0
Nutritional/herbal supplements (n) 1 2
Meditation (n) 0 1
Depression history
Existing diagnosis of MDD (y/n) 4/0 6/1
Number of depressive episodes in past 5 years
First episode (n) 2 2
2-5 (n) 1 3
>5 1 2
Metabolic measures
HOMA2-IR 2.00 ±0.62 1.47 ±0.64
Glycosylated haemoglobin (%) 5.6 ±0.12 5.5 ±0.27
Fasting glucose 5.3 ±0.68 5.4 ±0.79
2-hour glucose 6.4 ±2.23 5.7 ±1.80
3 metabolic syndrome components (n) 1 5
4 metabolic syndrome components (n) 2 2
5 metabolic syndrome components (n) 1 0
Psychological measures
HAM-D (/52) 12 ±7.0 15 ±3.6
PHQ-9 (/27) 15 ±7.2 15 ±4.8
CES-D (/60) 31 ±7.9 27 ±11.5
OHS (/174) 77 ±19.5 91 ±20.9
24-hour blood pressure
Awake, systolic (mmHg) 128.3 ±14.57 129.6 ±10.61
Awake, diastolic (mmHg) 75.3 ±5.69 78.1 ±9.0
Asleep, systolic (mmHg) 118.0 ±15.0 116.4 ±8.9
Asleep, diastolic (mmHg) 69.3 ±10.0 64.7 ±7.9
24-hour, systolic (mmHg) 126.7 ±13.0 126.6 ±9.9
24-hour, diastolic (mmHg) 73.7 ±5.0 75.3 ±8.7
Lipids
Total cholesterol (mmol/L) 5.4 ±1.25 5.4 ±1.53
HDL-C (mmol/L) 1.2 ±0.19 1.4 ±0.18
LDL-C (mmol/L) 3.2 ±1.00 3.3 ±1.31
Triglycerides (mmol/L) 2.4 ±0.81 1.5 ±0.63
C-reactive protein (mg/L) 2.8 ±0.65 2.3 ±1.50
Cortisol (nmol/L) 286.8 ±125.05 275.9 ±77.86
Data are means ±SD PRT: Progressive resistance training; BMI: Body mass index; HOMA2-IR; Homeostatic model of assessment-2; HAM-D: Hamilton Rating Scale for Depression; PHQ-9: Patient Health Questionnaire-9; CES-D: Center for Epidemiological Studies Depression scale; OHS: Oxford Happiness Scale; HDL-C: high-density lipoprotein; LDL-C: low-density lipoprotein
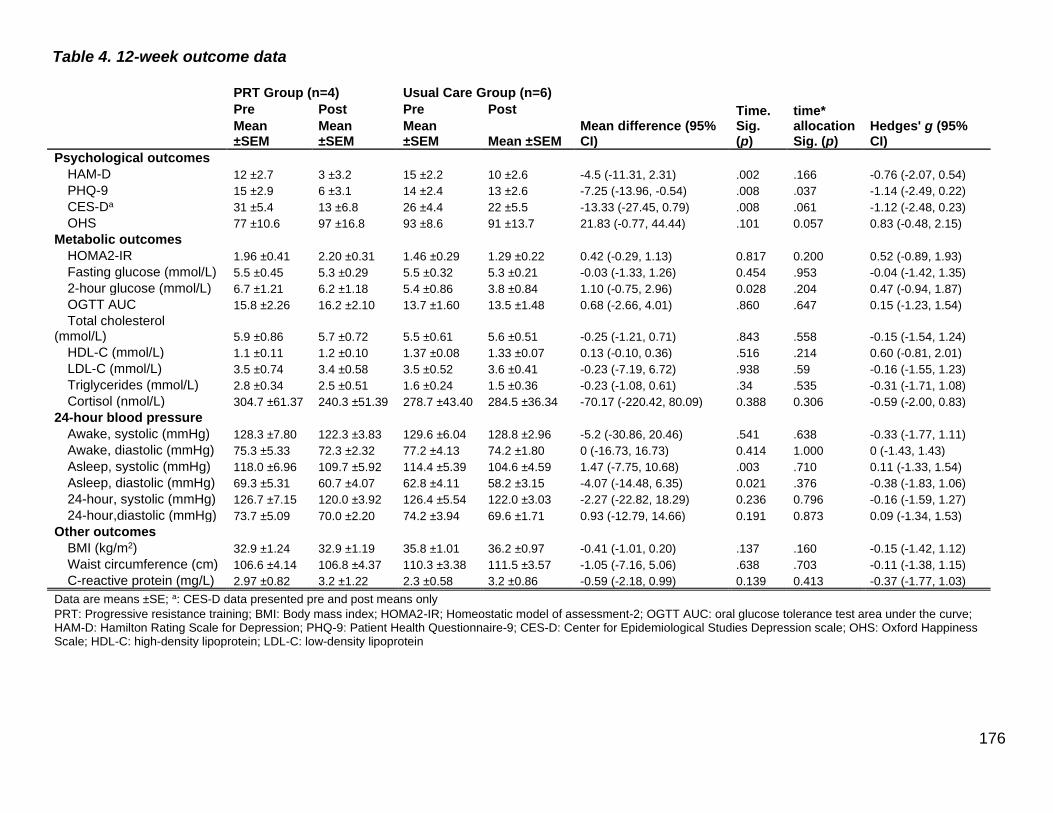
176
Table 4. 12-week outcome data
PRT Group (n=4) Usual Care Group (n=6)
Mean difference (95% CI)
time* allocation Sig. (p)
Hedges' g (95% CI)
Pre Post Pre Post Time. Sig. (p)
Mean ±SEM
Mean ±SEM
Mean ±SEM Mean ±SEM
Psychological outcomes HAM-D 12 ±2.7 3 ±3.2 15 ±2.2 10 ±2.6 -4.5 (-11.31, 2.31) .002 .166 -0.76 (-2.07, 0.54)
PHQ-9 15 ±2.9 6 ±3.1 14 ±2.4 13 ±2.6 -7.25 (-13.96, -0.54) .008 .037 -1.14 (-2.49, 0.22)
CES-Da 31 ±5.4 13 ±6.8 26 ±4.4 22 ±5.5 -13.33 (-27.45, 0.79) .008 .061 -1.12 (-2.48, 0.23)
OHS 77 ±10.6 97 ±16.8 93 ±8.6 91 ±13.7 21.83 (-0.77, 44.44) .101 0.057 0.83 (-0.48, 2.15)
Metabolic outcomes HOMA2-IR 1.96 ±0.41 2.20 ±0.31 1.46 ±0.29 1.29 ±0.22 0.42 (-0.29, 1.13) 0.817 0.200 0.52 (-0.89, 1.93)
Fasting glucose (mmol/L) 5.5 ±0.45 5.3 ±0.29 5.5 ±0.32 5.3 ±0.21 -0.03 (-1.33, 1.26) 0.454 .953 -0.04 (-1.42, 1.35)
2-hour glucose (mmol/L) 6.7 ±1.21 6.2 ±1.18 5.4 ±0.86 3.8 ±0.84 1.10 (-0.75, 2.96) 0.028 .204 0.47 (-0.94, 1.87)
OGTT AUC 15.8 ±2.26 16.2 ±2.10 13.7 ±1.60 13.5 ±1.48 0.68 (-2.66, 4.01) .860 .647 0.15 (-1.23, 1.54)
Total cholesterol (mmol/L) 5.9 ±0.86 5.7 ±0.72 5.5 ±0.61 5.6 ±0.51 -0.25 (-1.21, 0.71) .843 .558 -0.15 (-1.54, 1.24)
HDL-C (mmol/L) 1.1 ±0.11 1.2 ±0.10 1.37 ±0.08 1.33 ±0.07 0.13 (-0.10, 0.36) .516 .214 0.60 (-0.81, 2.01)
LDL-C (mmol/L) 3.5 ±0.74 3.4 ±0.58 3.5 ±0.52 3.6 ±0.41 -0.23 (-7.19, 6.72) .938 .59 -0.16 (-1.55, 1.23)
Triglycerides (mmol/L) 2.8 ±0.34 2.5 ±0.51 1.6 ±0.24 1.5 ±0.36 -0.23 (-1.08, 0.61) .34 .535 -0.31 (-1.71, 1.08)
Cortisol (nmol/L) 304.7 ±61.37 240.3 ±51.39 278.7 ±43.40 284.5 ±36.34 -70.17 (-220.42, 80.09) 0.388 0.306 -0.59 (-2.00, 0.83)
24-hour blood pressure Awake, systolic (mmHg) 128.3 ±7.80 122.3 ±3.83 129.6 ±6.04 128.8 ±2.96 -5.2 (-30.86, 20.46) .541 .638 -0.33 (-1.77, 1.11)
Awake, diastolic (mmHg) 75.3 ±5.33 72.3 ±2.32 77.2 ±4.13 74.2 ±1.80 0 (-16.73, 16.73) 0.414 1.000 0 (-1.43, 1.43)
Asleep, systolic (mmHg) 118.0 ±6.96 109.7 ±5.92 114.4 ±5.39 104.6 ±4.59 1.47 (-7.75, 10.68) .003 .710 0.11 (-1.33, 1.54)
Asleep, diastolic (mmHg) 69.3 ±5.31 60.7 ±4.07 62.8 ±4.11 58.2 ±3.15 -4.07 (-14.48, 6.35) 0.021 .376 -0.38 (-1.83, 1.06)
24-hour, systolic (mmHg) 126.7 ±7.15 120.0 ±3.92 126.4 ±5.54 122.0 ±3.03 -2.27 (-22.82, 18.29) 0.236 0.796 -0.16 (-1.59, 1.27)
24-hour,diastolic (mmHg) 73.7 ±5.09 70.0 ±2.20 74.2 ±3.94 69.6 ±1.71 0.93 (-12.79, 14.66) 0.191 0.873 0.09 (-1.34, 1.53)
Other outcomes BMI (kg/m2) 32.9 ±1.24 32.9 ±1.19 35.8 ±1.01 36.2 ±0.97 -0.41 (-1.01, 0.20) .137 .160 -0.15 (-1.42, 1.12)
Waist circumference (cm) 106.6 ±4.14 106.8 ±4.37 110.3 ±3.38 111.5 ±3.57 -1.05 (-7.16, 5.06) .638 .703 -0.11 (-1.38, 1.15)
C-reactive protein (mg/L) 2.97 ±0.82 3.2 ±1.22 2.3 ±0.58 3.2 ±0.86 -0.59 (-2.18, 0.99) 0.139 0.413 -0.37 (-1.77, 1.03)
Data are means ±SE; a: CES-D data presented pre and post means only PRT: Progressive resistance training; BMI: Body mass index; HOMA2-IR; Homeostatic model of assessment-2; OGTT AUC: oral glucose tolerance test area under the curve; HAM-D: Hamilton Rating Scale for Depression; PHQ-9: Patient Health Questionnaire-9; CES-D: Center for Epidemiological Studies Depression scale; OHS: Oxford Happiness Scale; HDL-C: high-density lipoprotein; LDL-C: low-density lipoprotein
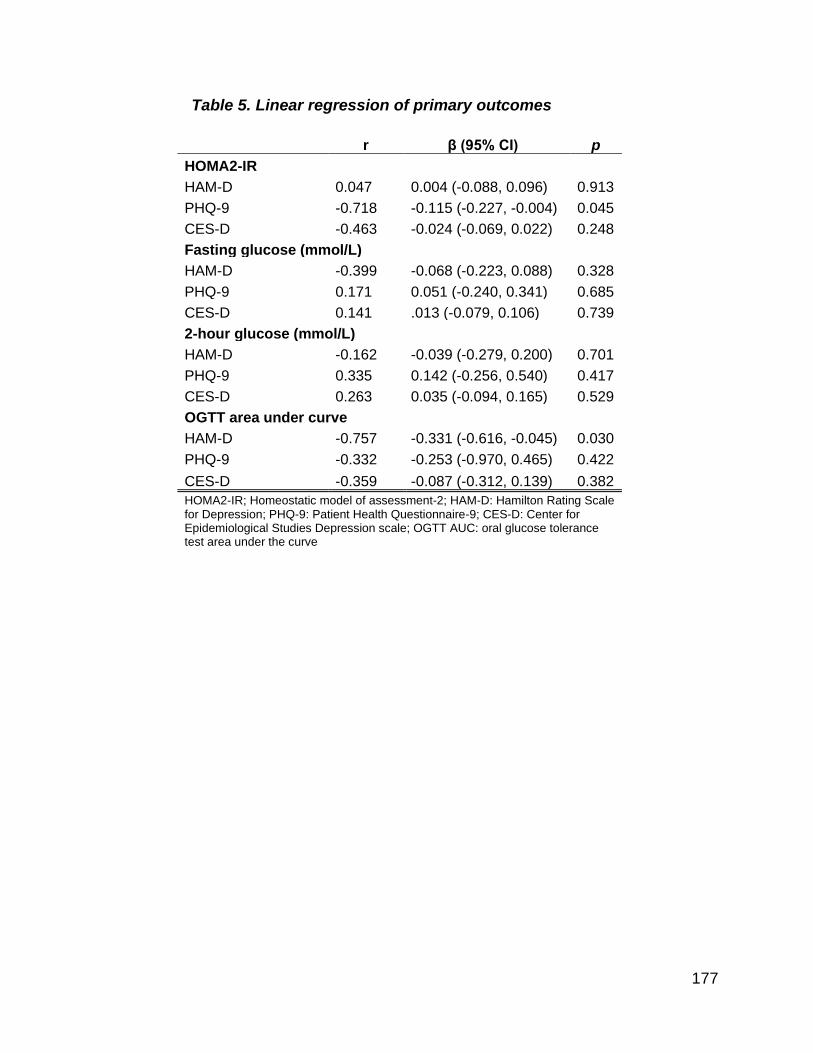
177
Table 5. Linear regression of primary outcomes
r β (95% CI) p
HOMA2-IR
HAM-D 0.047 0.004 (-0.088, 0.096) 0.913
PHQ-9 -0.718 -0.115 (-0.227, -0.004) 0.045
CES-D -0.463 -0.024 (-0.069, 0.022) 0.248
Fasting glucose (mmol/L)
HAM-D -0.399 -0.068 (-0.223, 0.088) 0.328
PHQ-9 0.171 0.051 (-0.240, 0.341) 0.685
CES-D 0.141 .013 (-0.079, 0.106) 0.739
2-hour glucose (mmol/L)
HAM-D -0.162 -0.039 (-0.279, 0.200) 0.701
PHQ-9 0.335 0.142 (-0.256, 0.540) 0.417
CES-D 0.263 0.035 (-0.094, 0.165) 0.529
OGTT area under curve
HAM-D -0.757 -0.331 (-0.616, -0.045) 0.030
PHQ-9 -0.332 -0.253 (-0.970, 0.465) 0.422
CES-D -0.359 -0.087 (-0.312, 0.139) 0.382 HOMA2-IR; Homeostatic model of assessment-2; HAM-D: Hamilton Rating Scale for Depression; PHQ-9: Patient Health Questionnaire-9; CES-D: Center for Epidemiological Studies Depression scale; OGTT AUC: oral glucose tolerance test area under the curve
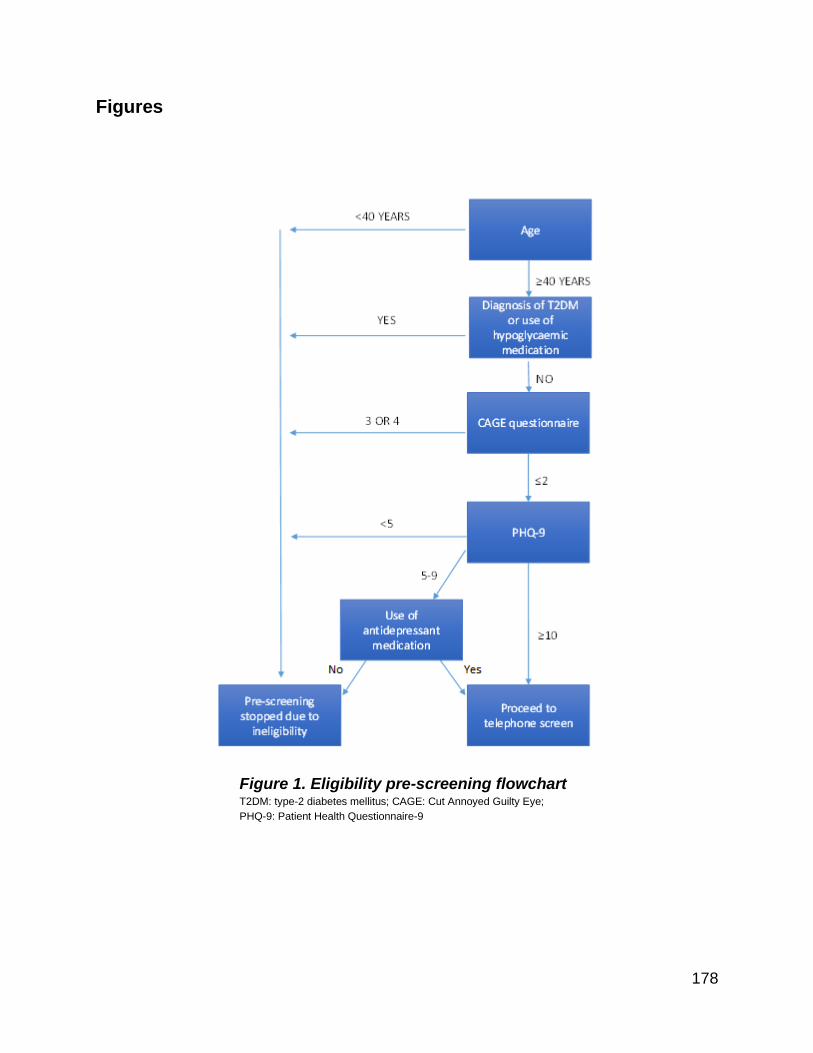
178
Figures
Figure 1. Eligibility pre-screening flowchart T2DM: type-2 diabetes mellitus; CAGE: Cut Annoyed Guilty Eye;
PHQ-9: Patient Health Questionnaire-9
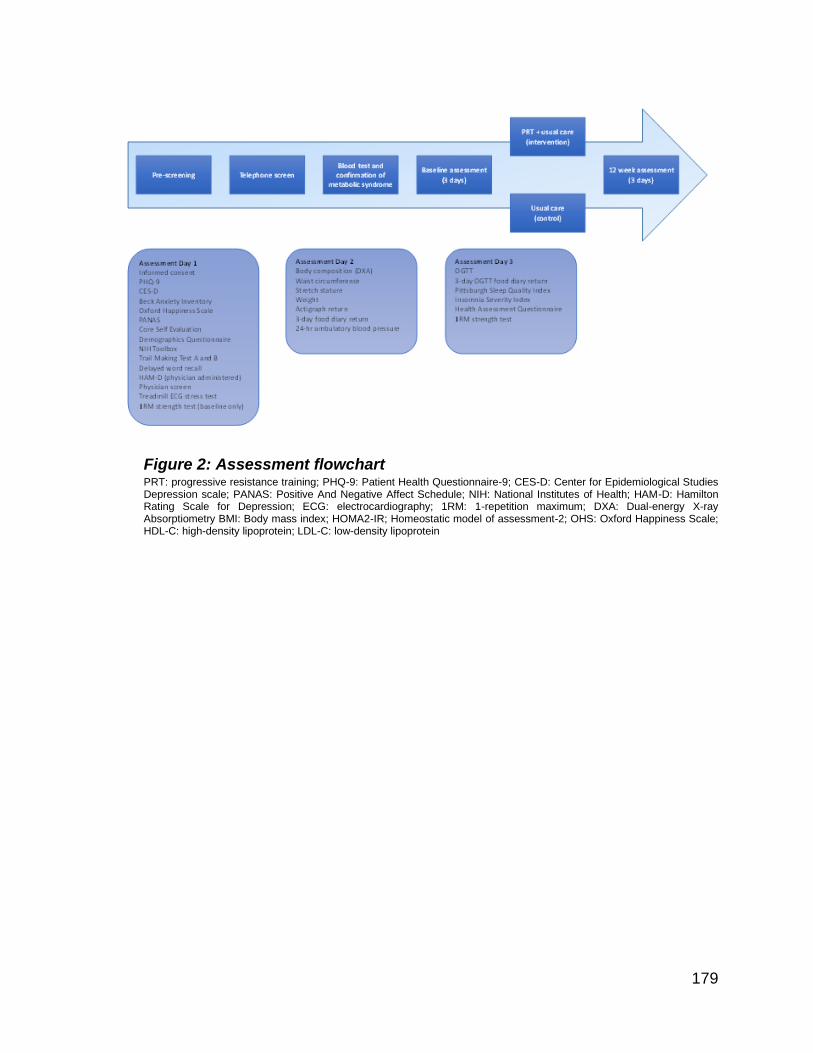
179
Figure 2: Assessment flowchart PRT: progressive resistance training; PHQ-9: Patient Health Questionnaire-9; CES-D: Center for Epidemiological Studies Depression scale; PANAS: Positive And Negative Affect Schedule; NIH: National Institutes of Health; HAM-D: Hamilton Rating Scale for Depression; ECG: electrocardiography; 1RM: 1-repetition maximum; DXA: Dual-energy X-ray Absorptiometry BMI: Body mass index; HOMA2-IR; Homeostatic model of assessment-2; OHS: Oxford Happiness Scale; HDL-C: high-density lipoprotein; LDL-C: low-density lipoprotein
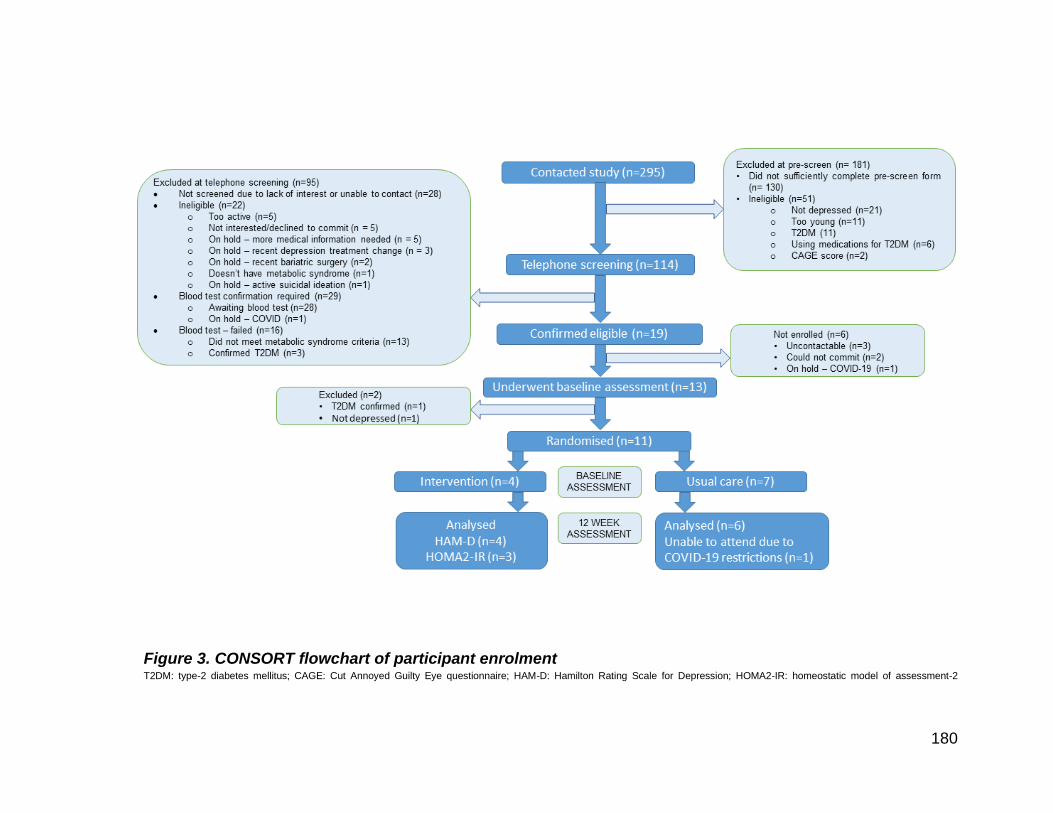
180
Figure 3. CONSORT flowchart of participant enrolment T2DM: type-2 diabetes mellitus; CAGE: Cut Annoyed Guilty Eye questionnaire; HAM-D: Hamilton Rating Scale for Depression; HOMA2-IR: homeostatic model of assessment-2
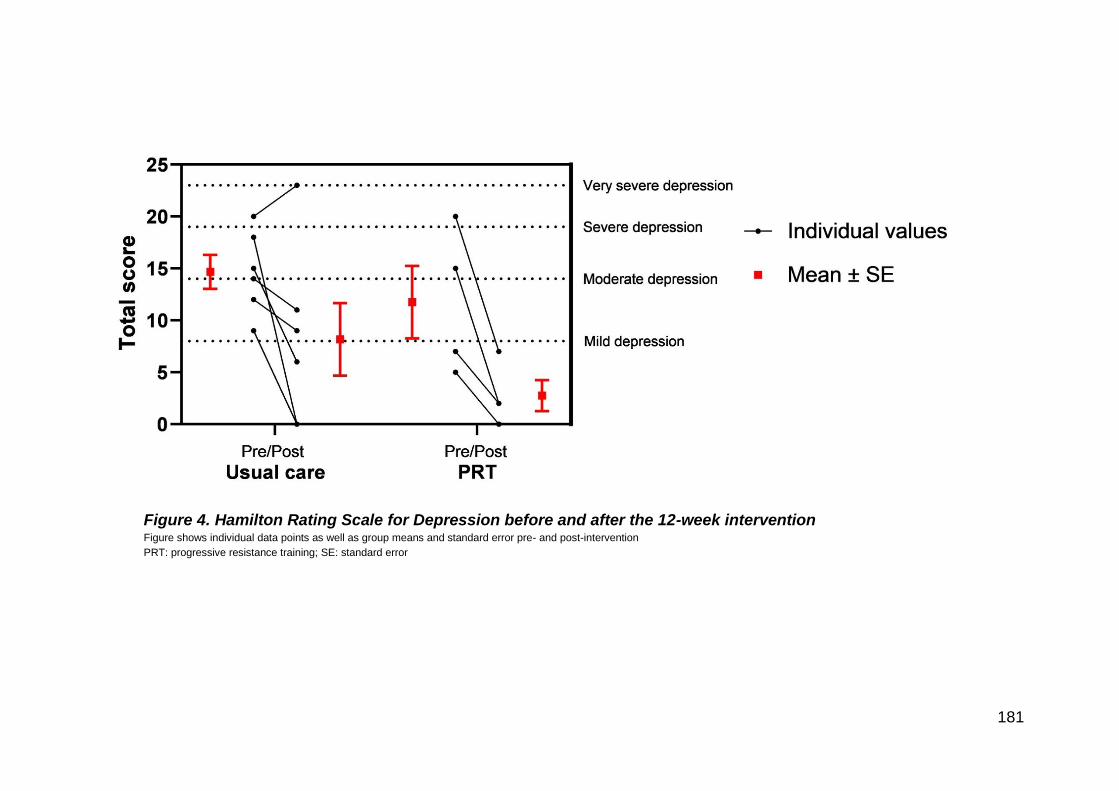
181
Figure 4. Hamilton Rating Scale for Depression before and after the 12-week intervention Figure shows individual data points as well as group means and standard error pre- and post-intervention
PRT: progressive resistance training; SE: standard error
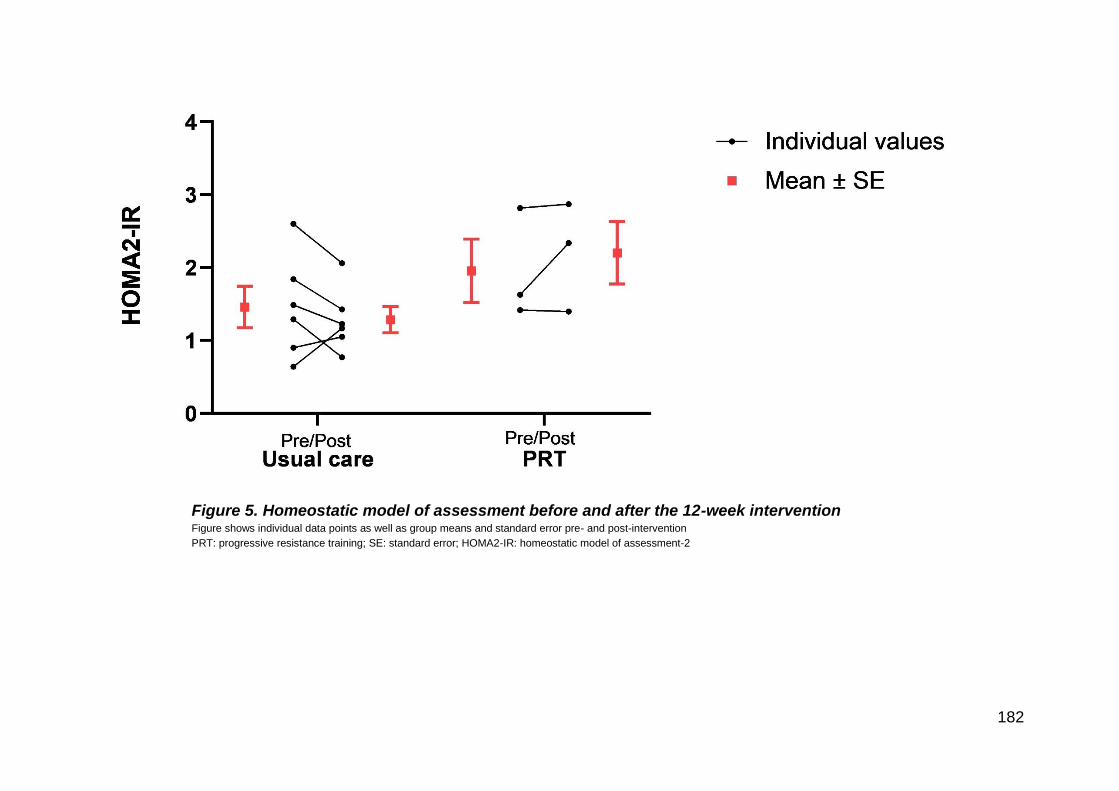
182
Figure 5. Homeostatic model of assessment before and after the 12-week intervention Figure shows individual data points as well as group means and standard error pre- and post-intervention
PRT: progressive resistance training; SE: standard error; HOMA2-IR: homeostatic model of assessment-2

183
Figure 6. Patient Health Questionnaire-9 before and after the 12-week intervention Figure shows individual data points as well as group means and standard error pre- and post-intervention
PRT: progressive resistance training; SE: standard error
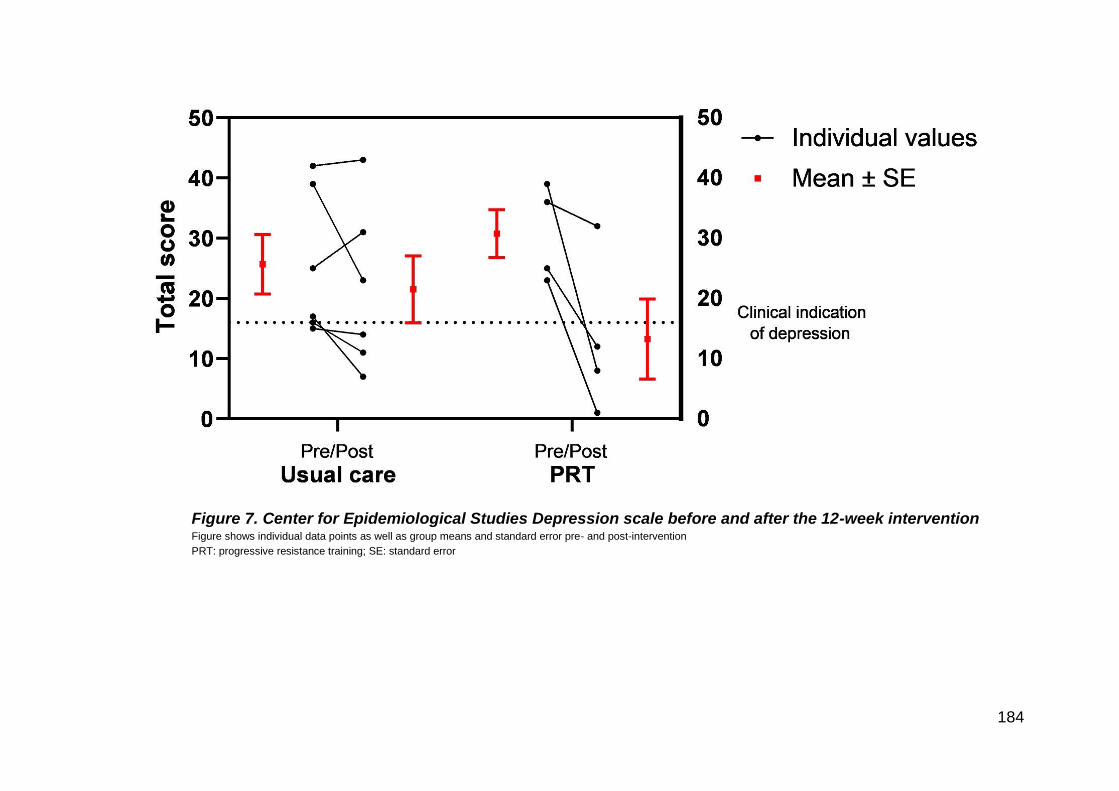
184
Figure 7. Center for Epidemiological Studies Depression scale before and after the 12-week intervention Figure shows individual data points as well as group means and standard error pre- and post-intervention
PRT: progressive resistance training; SE: standard error
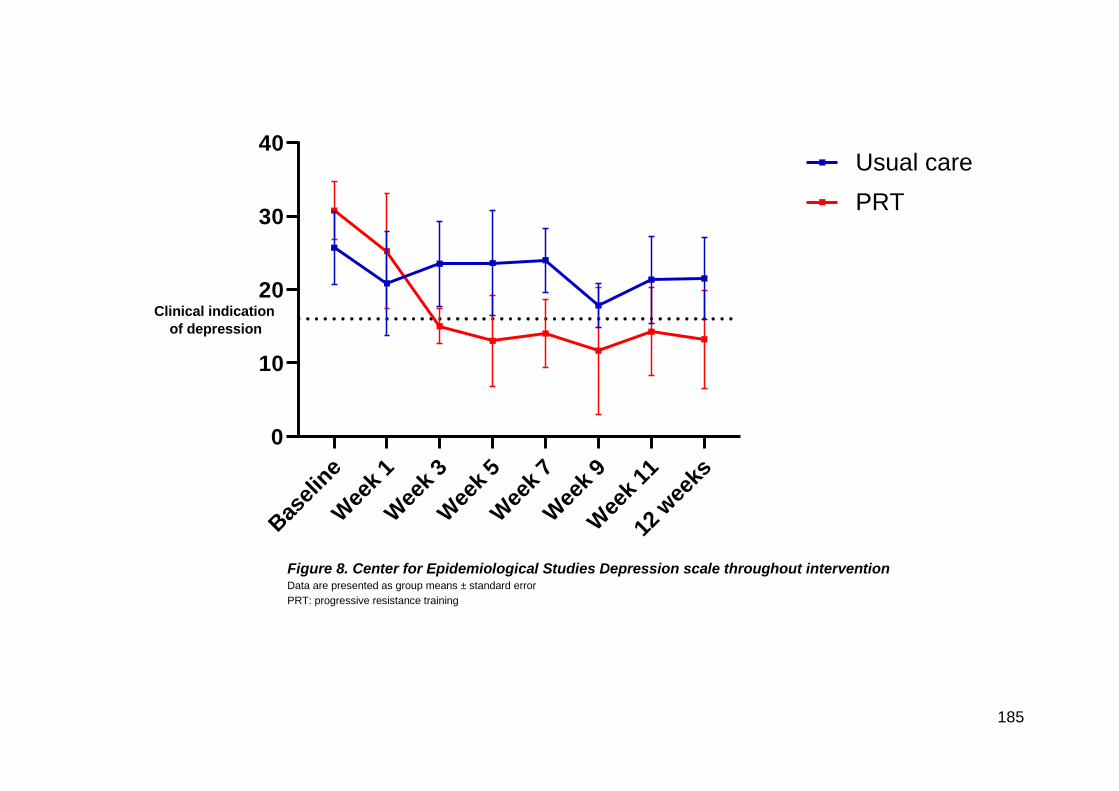
185
Figure 8. Center for Epidemiological Studies Depression scale throughout intervention Data are presented as group means ± standard error
PRT: progressive resistance training
Bas
elin
e
Wee
k 1
Wee
k 3
Wee
k 5
Wee
k 7
Wee
k 9
Wee
k 11
12 w
eeks
0
10
20
30
40
CES-D means throughout intervention
Usual care
PRT
Clinical indication
of depression

186
Figure 9. Oxford happiness scale before and after the 12-week intervention Figure shows individual data points as well as group means and standard error pre- and post-intervention
PRT: progressive resistance training; SE: standard error
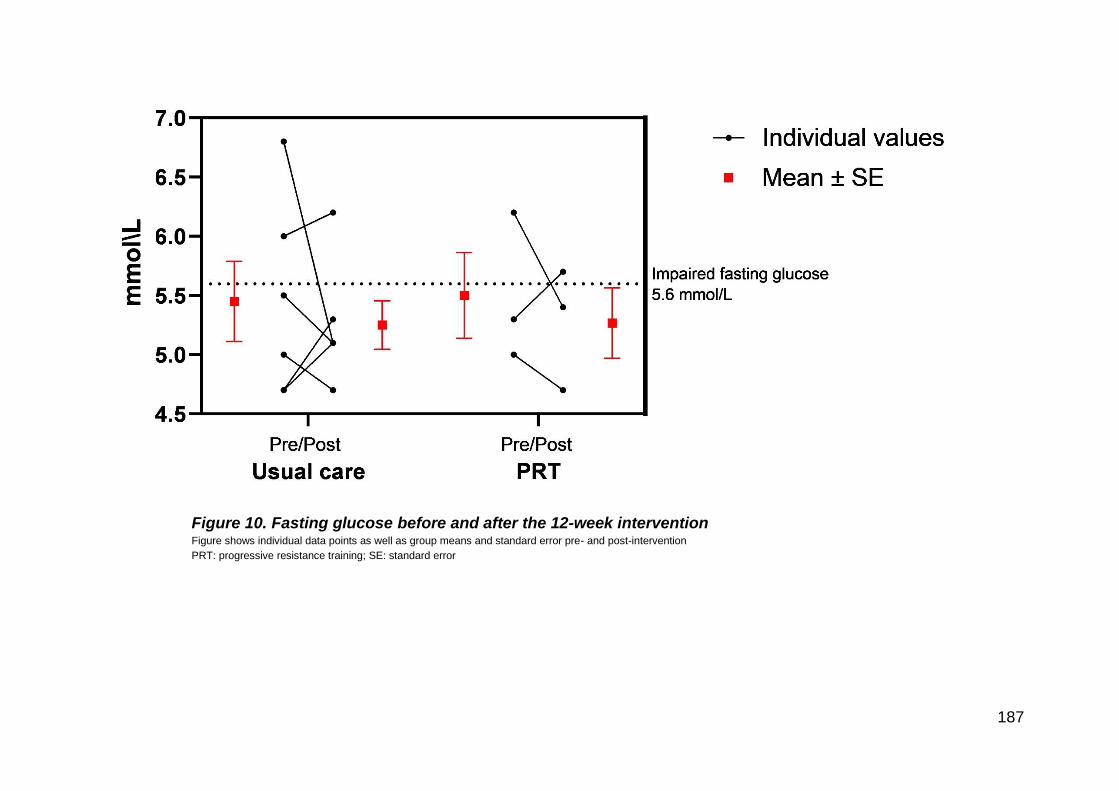
187
Figure 10. Fasting glucose before and after the 12-week intervention Figure shows individual data points as well as group means and standard error pre- and post-intervention
PRT: progressive resistance training; SE: standard error

188
Figure 11. 2-hour glucose before and after the 12-week intervention Figure shows individual data points as well as group means and standard error pre- and post-intervention
PRT: progressive resistance training; SE: standard error
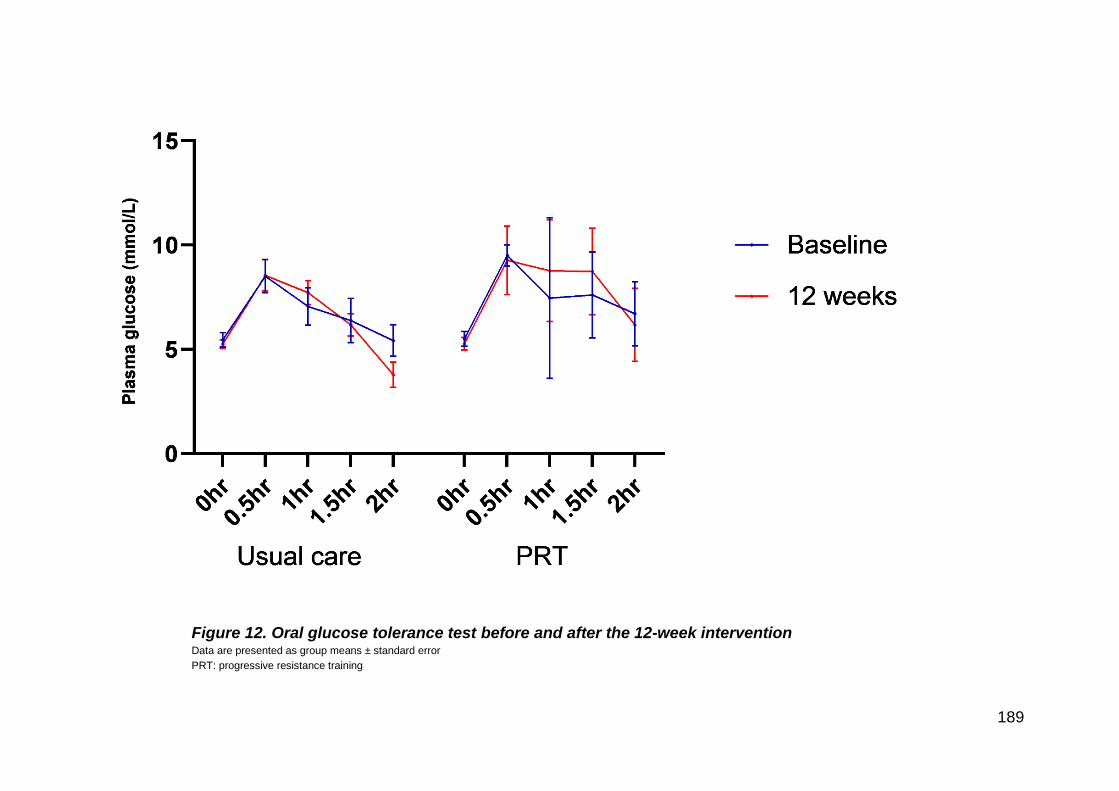
189
Figure 12. Oral glucose tolerance test before and after the 12-week intervention Data are presented as group means ± standard error
PRT: progressive resistance training

190
Figure 13. Glucose area under the curve before and after the 12-week intervention Figure shows individual data points as well as group means and standard error pre- and post-intervention
PRT: progressive resistance training; SE: standard error
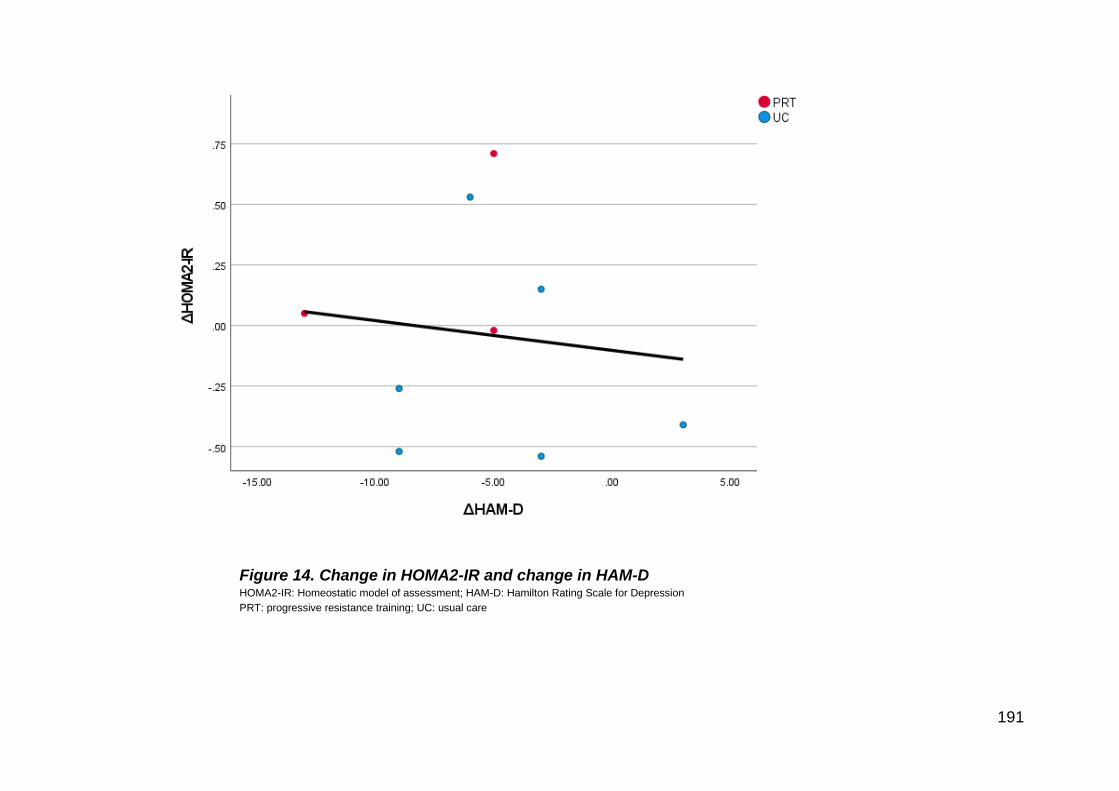
191
Figure 14. Change in HOMA2-IR and change in HAM-D HOMA2-IR: Homeostatic model of assessment; HAM-D: Hamilton Rating Scale for Depression
PRT: progressive resistance training; UC: usual care
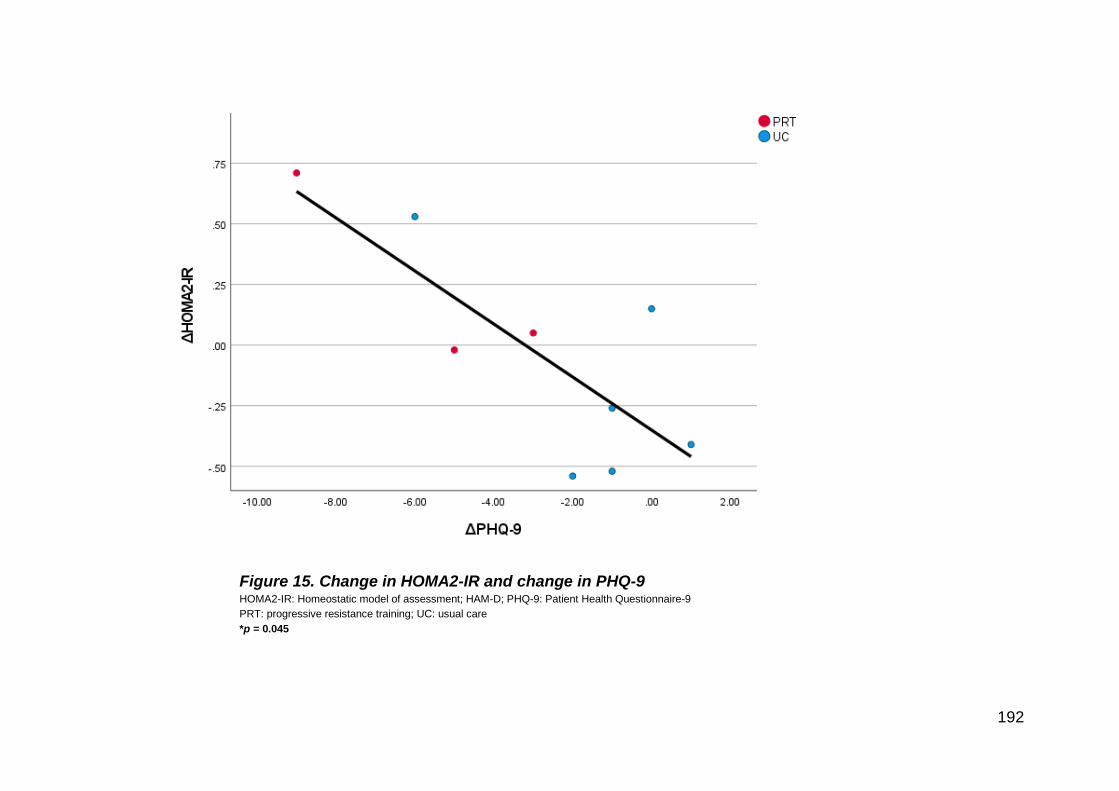
192
Figure 15. Change in HOMA2-IR and change in PHQ-9 HOMA2-IR: Homeostatic model of assessment; HAM-D; PHQ-9: Patient Health Questionnaire-9
PRT: progressive resistance training; UC: usual care
*p = 0.045
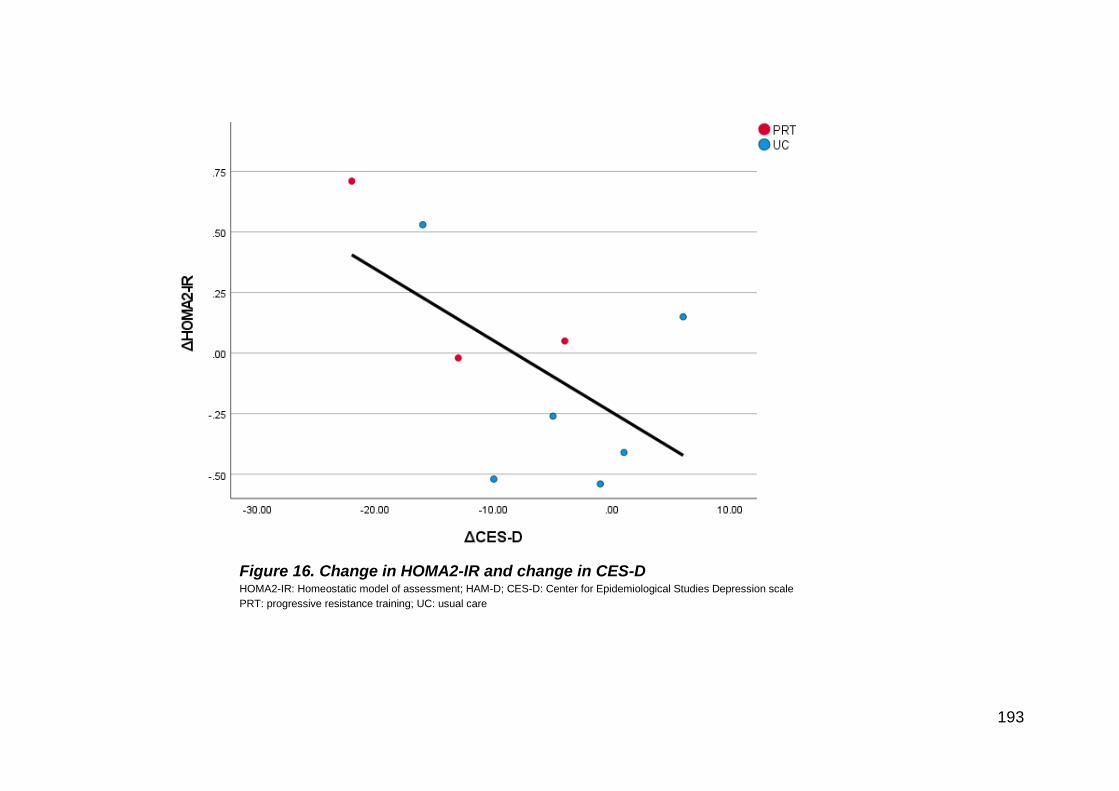
193
Figure 16. Change in HOMA2-IR and change in CES-D HOMA2-IR: Homeostatic model of assessment; HAM-D; CES-D: Center for Epidemiological Studies Depression scale
PRT: progressive resistance training; UC: usual care

194
Figure 17. Change in fasting glucose and change in HAM-D HAM-D: Hamilton Rating Scale for Depression; PRT: progressive resistance training; UC: usual care

195
Figure 18. Change in fasting glucose and change in PHQ-9 PHQ-9: Patient Health Questionnaire-9; PRT: progressive resistance training; UC: usual care
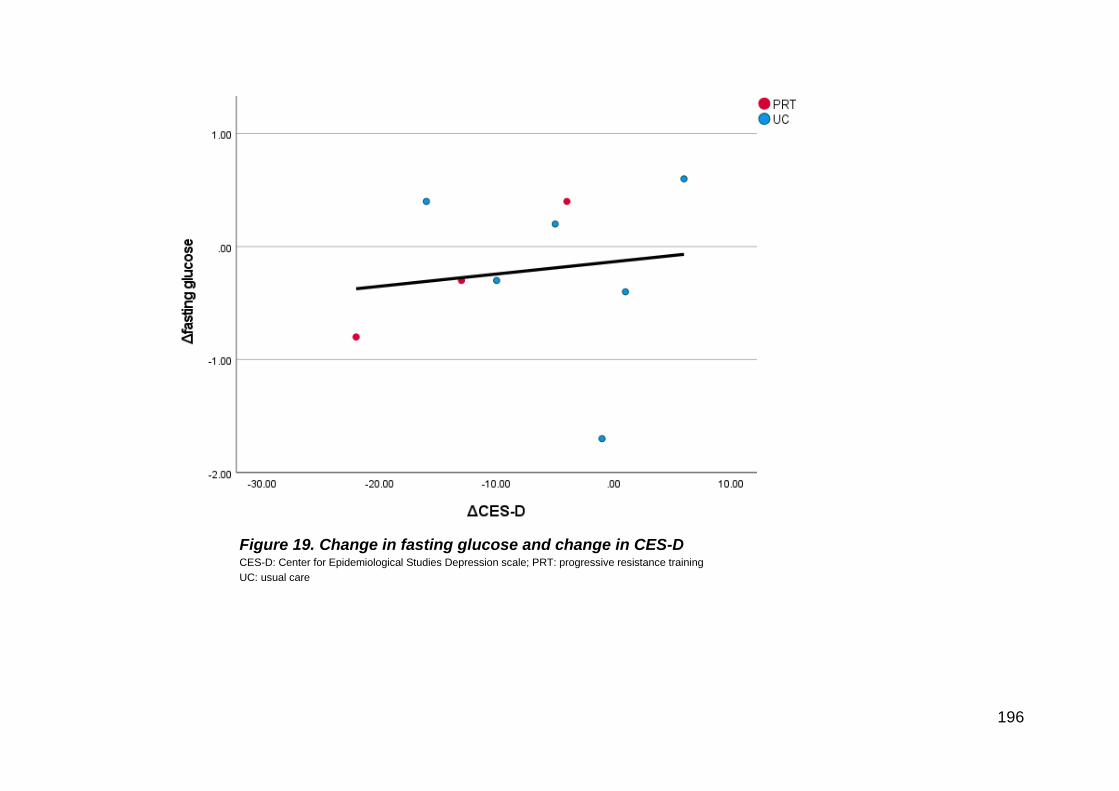
196
Figure 19. Change in fasting glucose and change in CES-D CES-D: Center for Epidemiological Studies Depression scale; PRT: progressive resistance training
UC: usual care

197
Figure 20. Change in 2-hour glucose and change in HAM-D HAM-D: Hamilton Rating Scale for Depression; PRT: progressive resistance training; UC: usual care

198
Figure 21. Change in 2-hour glucose and change in PHQ-9 PHQ-9: Patient Health Questionnaire-9; PRT: progressive resistance training; UC: usual care
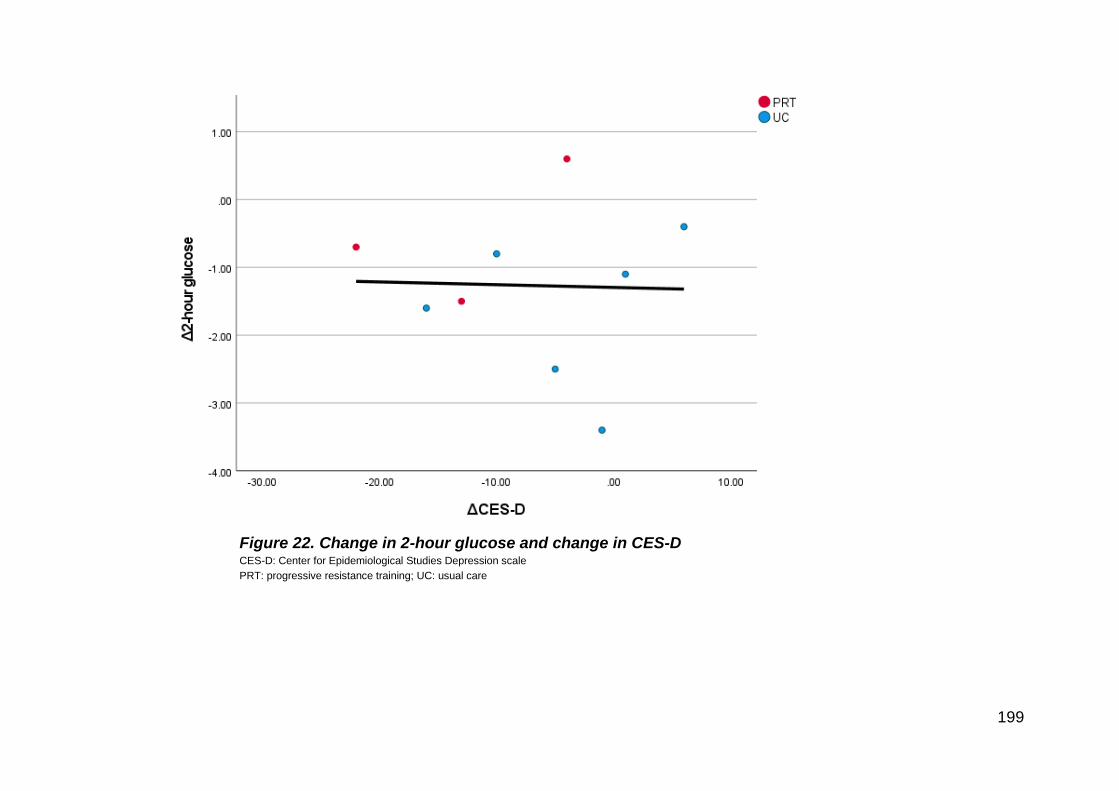
199
Figure 22. Change in 2-hour glucose and change in CES-D CES-D: Center for Epidemiological Studies Depression scale
PRT: progressive resistance training; UC: usual care
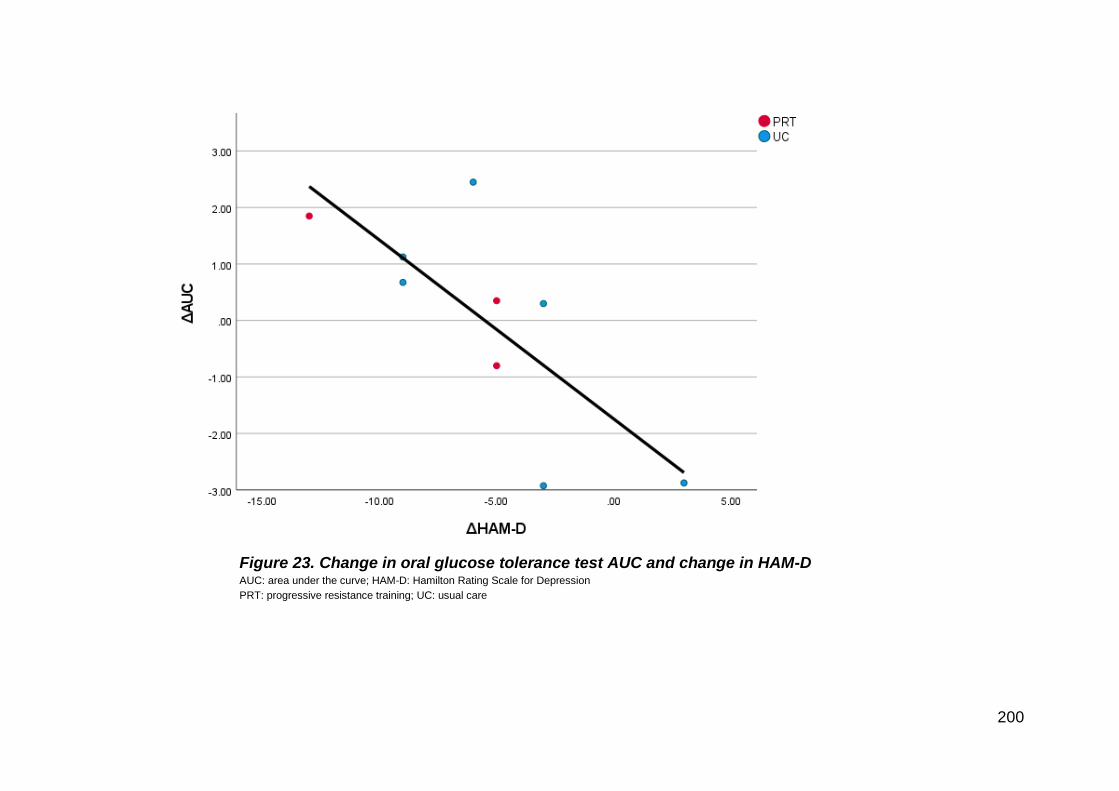
200
Figure 23. Change in oral glucose tolerance test AUC and change in HAM-D AUC: area under the curve; HAM-D: Hamilton Rating Scale for Depression
PRT: progressive resistance training; UC: usual care
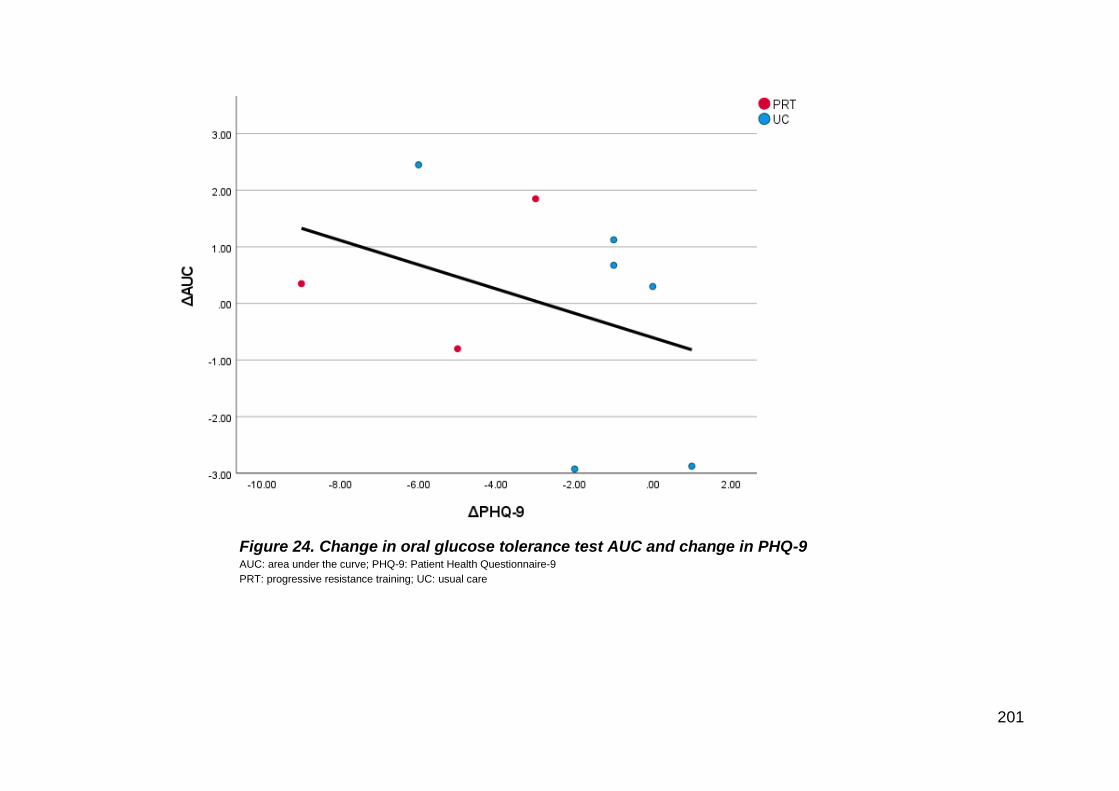
201
Figure 24. Change in oral glucose tolerance test AUC and change in PHQ-9 AUC: area under the curve; PHQ-9: Patient Health Questionnaire-9
PRT: progressive resistance training; UC: usual care
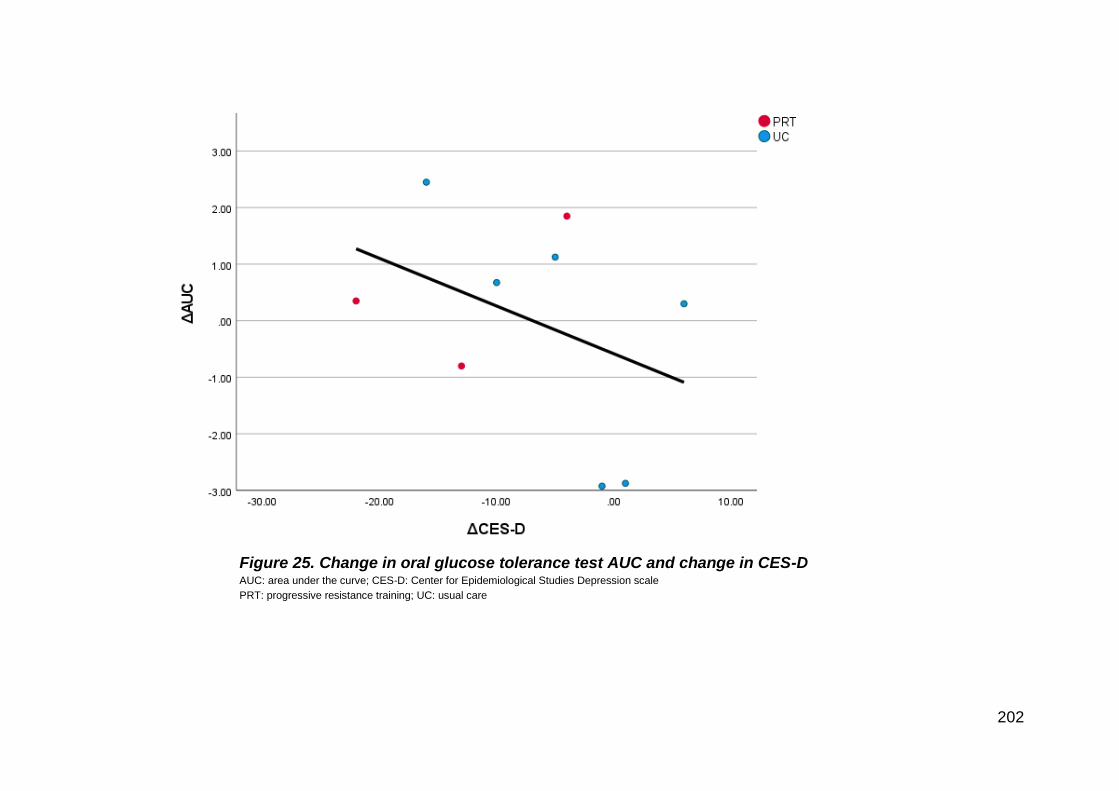
202
Figure 25. Change in oral glucose tolerance test AUC and change in CES-D AUC: area under the curve; CES-D: Center for Epidemiological Studies Depression scale
PRT: progressive resistance training; UC: usual care

203
CHAPTER 4: Discussion and Conclusions

204
Discussion
The primary purpose of this thesis was to investigate the effects of progressive
resistance training (PRT) on the simultaneous management of depressive symptoms
and markers of insulin resistance and glucose homeostasis.
Chapter 2 of this thesis was a systematic review of resistance training (RT) on
changes in depressive symptoms and cardiometabolic risk factors in individuals with
insulin resistance. Overall, the literature base was small, with only seven studies
included in the review.1-7 Across all seven studies, study quality was poor as
assessed by the Cochrane RoB 2 tool,8 was confined to individuals with type-2
diabetes (T2DM), and no studies recruited individuals with confirmed major
depressive disorder (MDD). While a meta-analysis had been originally planned, this
was ultimately deemed inappropriate due to the small number of eligible studies and
high heterogeneity in study designs. The main finding from the review was
interventions using RT were effective at reducing depressive symptoms, with the
effects of RT greater in studies where RT was used in isolation compared to a non-
active comparison group. Furthermore, across all study designs, studies of higher
intensity and volume appeared to show greater improvements, suggesting a dose
response effect, in line with previous studies of RT and depression in other cohorts.9
10 However, studies were limited by the use of self-rated assessment of depressive
symptoms, with no studies using a clinician-rated assessment such as the Hamilton
Rating of Depression (HAM-D).11 By contrast, results were not as consistent for
metabolic markers, with significant benefits on glycated haemoglobin (HbA1c) only
205
observed in studies where RT was compared to non-active comparison groups, with
no evidence of any dose-response effect. Despite all the studies recruiting
individuals with T2DM, reporting of cardiometabolic outcomes outside of HbA1c were
poor, with two studies reporting on fasting glucose, four studies on blood lipids, and
only one study reporting on blood pressure. No other measures of insulin resistance
such as HOMA2-IR or glucose metabolism such as an oral glucose tolerance test
(OGTT) were retrieved.
To address the many gaps identified in Chapter 2, a randomised controlled trial of
progressive resistance training in adults with major depressive disorder and
metabolic syndrome was conducted (Chapter 3). This group was selected as neither
condition had been investigated (Chapter 2), while individuals with both metabolic
syndrome and MDD have been previously shown to be at a high risk of developing
T2DM. We purposefully recruited individuals with symptoms of depression who also
satisfied at least two cardiometabolic risk factors, with confirmation of both MDD and
metabolic syndrome occurring during screening and baseline assessment. The
primary outcomes of the trial were depressive symptoms using the clinician-rated
HAM-D, as well as insulin resistance as measured using the Homeostatic Model of
Assessment (HOMA2-IR). In addition to these measurements, glucose metabolism
was measured using a 75g OGTT, while other metabolic syndrome components
such as blood lipids, 24-hour ambulatory blood pressure and waist-circumference
were also measured. Due to issues with participant recruitment and the impact of the
COVID-19 pandemic forcing a pause in the study, we were unable to reach the
target sample size, with only 11 participants eventually randomised into the study.
Consequently, Chapter 3 was therefore underpowered, and may explain why no
206
significant effect was observed for either primary outcome. However, a significant
reduction in self-rated symptoms of depression was observed for the Patient Health
Questionnaire-9 and Center for Epidemiological Studies-Depression scale (CES-D)
in the PRT group compared to usual care. Moderate-to-large effect sizes were also
seen across all depressive outcomes, consistent with the well-known anti-depressant
effect of PRT. Furthermore, all four participants in the PRT group achieved remission
of their depressive episode according to DSM-5 (R) criteria,12 compared to three out
of six in the usual care group. In contrast to depressive outcomes, there was no
evidence of an effect of PRT for any cardiometabolic outcomes. Despite the lack of
improvement in cardiometabolic outcomes, the remission of the depressive episode
alone may translate to a reduction in the risk of T2DM. The study presented in
Chapter 3 is still ongoing, with recruitment due to re-commence in January 2022.
Limitations
There were some limitations of this thesis that warrant consideration with how data
should be interpreted. In Chapter 2, the search and subsequent review of all titles,
abstracts, and full-texts were done by one author, although all final articles were
approved by consensus of all authors. In limiting the eligibility to those studies
utilising a resistance training intervention (RT), the number of included studies was
considerably reduced as the majority of exercise research on depression to date
uses aerobic interventions. Additionally, several of the studies2 4 6 7 that were
included employed comparator or co-intervention groups in such a way as to limit
analysis of the isolated effects of RT. However, in the few studies that were limited to

207
RT in isolation compared to a non-active comparison group, there is evidence that
RT can improve both symptoms of depression and HbA1c in individuals with T2DM.
Studies that were included in the review did not measure insulin resistance directly,
so surrogate measures of glucose homeostasis were analysed instead, where
available. Following this, standard techniques of measuring insulin resistance such
as hyperinsulinaemic-euglycaemic clamp and HOMA-IR were not discussed in this
chapter. Lastly, theses and other unpublished literature (e.g., preprints) were not
included in the review, as were publications in language other than English, and thus
it is possible that the review does not include all the available data on RT.
In addition to the small sample size in Chapter 3, other limitations warrant
consideration. While we consider the results of Chapter 3 generally applicable to
community-dwelling adults with metabolic syndrome and major depressive disorder,
we acknowledge that the cohort included in our RCT were self-selected. As MDD is
a psychological state that can comprise lower motivation and energy for daily
activities, individuals inclined to volunteer for a clinical trial may not be entirely
representative of the community population with MDD as a whole. It is possible that
a beneficial effect may have been experienced by the PRT group from regular
contact and socialisation with the intervention trainers. While we cannot be certain
that this occurred, use of an attention or sham-exercise control group would help
avoid this as a confounding variable. While we used scales with established
reliability in this study such as the HAM-D,13 14 CES-D,15 and PHQ-9,16 we do not
know if this reliability would have been the same in the assessment conditions in this
study. Reliability data for the scales used in this study were not re-established
208
however, due to the feasibility in such a small study with personnel limitations, and
therefore existing reliability data in the literature was utilised.
Furthermore, many outcomes collected in the study were unable to be presented in
this thesis due to limitations with access. Many of the computers that run the
necessary software were located on campus and could not be accessed during the
lockdown periods. Consequently, these data could not be retrieved and analysed in
time for this thesis. Access to 3-day food records, body composition using from dual-
energy Xray absorptiometry scans (DXA), and pulse wave analysis (PWA) and pulse
wave velocity (PWV) data would allow for a much more comprehensive analysis.
These data may help explain why no improvements were seen in some outcomes
(e.g., 3-day food records may help explain why HOMA2-IR and OGTT outcomes did
not improve), while other variables may be more sensitive to changes than the data
that was available (DXA vs. waist circumference and PWA/PWV vs. ambulatory BP).
Lastly, the design of the study may have precluded any potential benefit of PRT.
Despite intentionally recruiting individuals who satisfied metabolic syndrome
according to International Diabetes Federation criteria,17 participant’s clinical profile
may have precluded any potential benefit of PRT. This includes only three
individuals satisfying the criteria of impaired fasting glucose, while eight out of eleven
participants were taking anti-hypertensive medication. Furthermore, the study was
limited to 12 weeks. A recent meta-analysis of aerobic exercise in individuals with
metabolic syndrome observed a dose-response relationship with studies of longer
duration reporting greater improvements in metabolic syndrome components.18

209
Future directions
While the systematic review that forms Chapter 2 showed that RT may be effective
in improving both depressive symptoms and glucose metabolism simultaneously, the
literature base was small with a generally high risk of bias. There are some
implications in the review that may be addressed by future research:
• More trials are needed involving not just cohorts with T2DM, but also those at
heightened risk of developing T2DM, with conditions such as impaired fasting
glucose/impaired glucose tolerance, metabolic syndrome, and polycystic
ovary disease. These trials should also intentionally recruit individuals with a
confirmed diagnosis of MDD.
• To reduce the risk of bias inherent with utilising self-rated depression scales in
exercises studies where it’s not feasible to blind participants to group
allocation, efforts should be made to utilise clinician-rated scales where
possible.
• Future randomised controlled exercise trials involving cohorts with depression
may benefit from employing an attention or sham-exercise comparator group,
rather than usual care, so that both study groups receive equal exposure to
trial researchers.
• A thorough analysis of cardiometabolic risk factors such as body composition,
insulin resistance (HOMA2-IR), glucose tolerance (OGTT), and blood
pressures including ambulatory blood pressure and central haemodynamics
assists in patient risk stratification and examination of underlying physiological
changes.

210
• Possible common pathways between insulin resistance and depression such
as cortisol, C-reactive protein, brain-derived neurotrophic factor, and
inflammatory pathways show potential but require further examination.
While the randomised controlled trial that forms Chapter 3. attempted to address
some of the gaps identified above, many still remain:
• Whether PRT can simultaneously improve depressive symptoms and insulin
resistance in individuals. Data from the systematic review (Chapter 2) suggest
that PRT can simultaneously improve symptoms of depression and glycated
haemoglobin, however this was not seen in Chapter 3.
• Whether improvements in depressive symptoms are associated with
improvements in insulin resistance. Results in chapter 3 show an inverse
association, whereby a reduction in depressive symptoms was associated
with a worsening of insulin resistance. This finding is contrary to our a priori
hypothesis, and with data only in 10 individuals, warrants further investigation.
• Whether a dose-response relationship exists, whereby higher intensities
and/or volumes of PRT, or greater exposure from longer interventions or
higher frequency training, result in greater improvements in insulin resistance
and depressive symptoms than lower intensity exercise. Following this,
determining the minimum exercise dosage required to produce clinically
meaningful benefits.
• How long these benefits are sustained after training is ceased, through the
use of follow-up, and determining whether benefits are sustained similarly
across metabolic and psychological outcomes.

211
• Whether a dose-response relationship exists between PRT and metabolic
improvements as well as PRT and reductions in depressive symptoms.
• Studies in individuals with varying clinical status are required. Participants
recruited in chapter 3 did not have significant levels of insulin resistance, while
many were on anti-hypertensive medication, both of which may have
precluded any benefit of PRT.
• Trials are needed to compare the effectiveness of PRT to other therapeutic
interventions such as aerobic exercise, pharmacotherapy, lifestyle
interventions or psychological and educational interventions.
Conclusion
The investigations in this thesis examined the effectiveness of resistance exercise
training interventions in cohorts that had both insulin resistance and depressive
symptoms. A systematic review was conducted to examine the evidence base, which
was small and heterogenous, but indicated the potential for RT to improve
depressive symptoms and markers of glucose metabolism simultaneously, with 2
studies reporting significant reductions in depressive symptom severity favouring RT
and 3 studies reporting significant reductions in HbA1c levels favouring RT. Several
gaps in the existing literature were identified, which included a lack of direct
measurements of insulin resistance and no trial performed in individuals with MDD.
To address these gaps, we conducted a randomised controlled trial of PRT in adults
with metabolic syndrome and MDD. While no significant reductions in clinician
clinician-rated depressive symptoms and insulin resistance were observed owing to

212
a lack of statistical power, we observed significant reductions in self-rated depressive
symptoms in the PRT group compared to usual care.

213
References
1. Amy L. Putiri JCL, Sara Gillham, Masa Sasagawa, Ryan Bradley, Guan-Cheng
Sun. Psychological Effects of Yi Ren Medical Qigong and Progressive
Resistance Training in Adults With Type 2 Diabetes Mellitus: A Randomized
Controlled Pilot Study. Alternative Therapies 2012;18(1):30-34.
2. Aylin K, Arzu D, Sabri S, et al. The effect of combined resistance and home-based
walking exercise in type 2 diabetes patients. Int J Diabetes Dev Ctries
2009;29(4):159-65. doi: 10.4103/0973-3930.57347 [published Online First:
2010/03/26]
3. Duruturk N, Ozkoslu MA. Effect of tele-rehabilitation on glucose control, exercise
capacity, physical fitness, muscle strength and psychosocial status in patients
with type 2 diabetes: A double blind randomized controlled trial. Prim Care
Diabetes 2019;13(6):542-48. doi: 10.1016/j.pcd.2019.03.007 [published
Online First: 2019/04/25]
4. Leehey DJ, Collins E, Kramer HJ, et al. Structured Exercise in Obese Diabetic
Patients with Chronic Kidney Disease: A Randomized Controlled Trial. Am J
Nephrol 2016;44(1):54-62. doi: 10.1159/000447703 [published Online First:
2016/07/08]
5. Lincoln AK, Shepherd A, Johnson PL, et al. The impact of resistance exercise
training on the mental health of older Puerto Rican adults with type 2
diabetes. J Gerontol B Psychol Sci Soc Sci 2011;66(5):567-70. doi:
10.1093/geronb/gbr034 [published Online First: 2011/05/17]
6. Mueller MJ, Tuttle LJ, Lemaster JW, et al. Weight-bearing versus nonweight-
bearing exercise for persons with diabetes and peripheral neuropathy: a
214
randomized controlled trial. Arch Phys Med Rehabil 2013;94(5):829-38. doi:
10.1016/j.apmr.2012.12.015 [published Online First: 2013/01/02]
7. Pibernik-Okanovic M, Hermanns N, Ajdukovic D, et al. Does treatment of
subsyndromal depression improve depression-related and diabetes-related
outcomes? A randomised controlled comparison of psychoeducation, physical
exercise and enhanced treatment as usual. Trials 2015;16:305. doi:
10.1186/s13063-015-0833-8 [published Online First: 2015/07/16]
8. Sterne JAC SJ, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng
H-Y, Corbett MS, Eldridge SM, Hernán MA, Hopewell S, Hróbjartsson A,
Junqueira DR, Jüni P, Kirkham JJ, Lasserson T, Li T, McAleenan A, Reeves
BC, Shepperd S, Shrier I, Stewart LA, Tilling K, White IR, Whiting PF, Higgins
JPT. RoB 2: a revised tool for assessing risk of bias in randomised trials.
2019; 366.
9. Singh NA, Stavrinos TM, Scarbek Y, et al. A Randomized Controlled Trial of High
Versus Low Intensity Weight Training Versus General Practitioner Care for
Clinical Depression in Older Adults. The Journals of Gerontology: Series A
2005;60(6):768-76. doi: 10.1093/gerona/60.6.768
10. Singh NA, Clements KM, Fiatarone MA. A Randomized Controlled Trial of
Progressive Resistance Training in Depressed Elders. The Journals of
Gerontology: Series A 1997;52A(1):M27-M35. doi:
10.1093/gerona/52A.1.M27
11. Hamilton M. Development of a rating scale for primary depressive illness. Br J
Soc Clin Psychol 1967;6(4):278-96. doi: 10.1111/j.2044-8260.1967.tb00530.x
[published Online First: 1967/12/01]
215
12. Diagnostic and statistical manual of mental disorders : DSM-5 (R). Arlington, VA:
American Psychiatric Association 2013.
13. Wewege MA, Thom JM, Rye KA, et al. Aerobic, resistance or combined training:
A systematic review and meta-analysis of exercise to reduce cardiovascular
risk in adults with metabolic syndrome. Atherosclerosis 2018;274:162-71. doi:
10.1016/j.atherosclerosis.2018.05.002 [published Online First: 2018/05/22]

216
Bibliography
(2001). "Executive Summary of The Third Report of The National Cholesterol
Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment
of High Blood Cholesterol In Adults (Adult Treatment Panel III)." Journal of the
American Medical Association 285(19): 2486-2497.
(2013). Diagnostic and statistical manual of mental disorders : DSM-5 (R). Arlington,
VA, American Psychiatric Association.
(2013). Diagnostic and statistical manual of mental disorders : DSM-5™.
Washington, DC ;, American Psychiatric Publishing, a division of American
Psychiatric Association.
Abdul-Ghani, M. A., Tripathy, D. and DeFronzo, R. A. (2006). "Contributions of beta-
cell dysfunction and insulin resistance to the pathogenesis of impaired glucose
tolerance and impaired fasting glucose." Diabetes Care 29(5): 1130-1139.
Abrahin, O., Moraes-Ferreira, R., Cortinhas-Alves, E. A. and Guerreiro, J. F. (2021).
"Is resistance training alone an antihypertensive therapy? A meta-analysis." Journal
of Human Hypertension 35(9): 769-775.
Acosta-Manzano, P., Rodriguez-Ayllon, M., Acosta, F. M., Niederseer, D. and
Niebauer, J. (2020). "Beyond general resistance training. Hypertrophy versus
muscular endurance training as therapeutic interventions in adults with type 2
diabetes mellitus: A systematic review and meta-analysis." Obesity Reviews 21(6):
e13007.
Adeva-Andany, M. M., Rañal-Muíño, E., Vila-Altesor, M., Fernández-Fernández, C.,
Funcasta-Calderón, R. and Castro-Quintela, E. (2019). "Dietary habits contribute to
define the risk of type 2 diabetes in humans." Clinical Nutrition ESPEN 34: 8-17.

217
Akash, M. S. H., Rehman, K. and Liaqat, A. (2018). "Tumor necrosis factor-alpha:
Role in development of insulin resistance and pathogenesis of type 2 diabetes
mellitus." Journal of Cellular Biochemistry 119(1): 105-110.
Alberti, K. G., Eckel, R. H., Grundy, S. M., Zimmet, P. Z., Cleeman, J. I., Donato, K.
A., Fruchart, J. C., James, W. P., Loria, C. M. and Smith, S. C., Jr. (2009).
"Harmonizing the metabolic syndrome: a joint interim statement of the International
Diabetes Federation Task Force on Epidemiology and Prevention; National Heart,
Lung, and Blood Institute; American Heart Association; World Heart Federation;
International Atherosclerosis Society; and International Association for the Study of
Obesity." Circulation 120(16): 1640-1645.
Alberti, K. G. and Zimmet, P. Z. (1998). "Definition, diagnosis and classification of
diabetes mellitus and its complications. Part 1: diagnosis and classification of
diabetes mellitus provisional report of a WHO consultation." Diabetic Medicine 15(7):
539-553.
Alberti, K. G. M. M., Zimmet, P. and Shaw, J. (2006). "Metabolic syndrome—a new
world-wide definition. A consensus statement from the International Diabetes
Federation." Diabetic Medicine 23(5): 469-480.
Almeida, O. P., Calver, J., Jamrozik, K., Hankey, G. J. and Flicker, L. (2009).
"Obesity and metabolic syndrome increase the risk of incident depression in older
men: The health in men study." The American Journal of Geriatric Psychiatry 17(10):
889-898.
American College of Sports Medicine (2009). "Progression models in resistance
training for healthy adults." Medicine & Science in Sports & Exercise 41(3).
Ammassari, A., Trotta, M. P., Murri, R., Castelli, F., Narciso, P., Noto, P., Vecchiet,
J., Monforte, A. D. A., Wu, A. W., Antinori, A. and for the Ad, I. S. G. (2002).
218
"Correlates and predictors of adherence to highly active antiretroviral therapy:
Overview of published literature." Journal of Acquired Immune Deficiency
Syndromes 31: s123-127.
Andrade, C. (2016). "Cardiometabolic risks in schizophrenia and directions for
intervention, 1: Magnitude and moderators of the problem." Journal of Clinicial
Psychiatry 77(7): e844-847.
Armamento-Villareal, R., Aguirre, L., Napoli, N., Shah, K., Hilton, T., Sinacore, D. R.,
Qualls, C. and Villareal, D. T. (2014). "Changes in thigh muscle volume predict bone
mineral density response to lifestyle therapy in frail, obese older adults."
Osteoporosis International 25(2): 551-558.
Armamento-Villareal, R., Aguirre, L., Waters, D. L., Napoli, N., Qualls, C. and
Villareal, D. T. (2020). "Effect of aerobic or resistance exercise, or both, on bone
mineral density and bone metabolism in obese older adults while dieting: A
randomized controlled trial." Journal of Bone and Mineral Research 35(3): 430-439.
Artese, A., Stamford, B. A. and Moffatt, R. J. (2017). "Cigarette smoking: An
accessory to the development of insulin resistance." American Journal of Lifestyle
Medicine 13(6): 602-605.
Asa, C., Maria, S., Katharina, S. S. and Bert, A. (2012). "Aquatic exercise is effective
in improving exercise performance in patients with heart failure and type 2 diabetes
mellitus." Evidence-Based Complementary Alternative Medicine 2012: 349209.
Ashton, R. E., Tew, G. A., Aning, J. J., Gilbert, S. E., Lewis, L. and Saxton, J. M.
(2020). "Effects of short-term, medium-term and long-term resistance exercise
training on cardiometabolic health outcomes in adults: systematic review with meta-
analysis." British Journal of Sports Medicine 54(6): 341-348.
219
Austin, R. P. (2006). "Polypharmacy as a risk factor in the treatment of type 2
diabetes." Diabetes Spectrum 19(1): 13.
Australian Bureau of Statistics. (2018). "National health survey: First results."
Retrieved 1st December 2021, from https://www.abs.gov.au/statistics/health/health-
conditions-and-risks/national-health-survey-first-results/latest-release#data-
download.
Australian Institute of Health and Welfare (2020). Australia's health 2020: in brief.
Canberra, AIHW.
Australian Institute of Health and Welfare (2021). Australian burden of disease study:
Impact and causes of illness and death in Australia 2018. . Canberra, AIHW. 23.
Australian Institute of Health Welfare. (2020). "Diabetes." Retrieved 24/04/2022,
from https://www.aihw.gov.au/reports/diabetes/diabetes.
Aylin, K., Arzu, D., Sabri, S., Handan, T. E. and Ridvan, A. (2009). "The effect of
combined resistance and home-based walking exercise in type 2 diabetes patients."
Internation Journal of Diabetes in Developing Countries 29(4): 159-165.
Balducci, S., Zanuso, S., Nicolucci, A., Fernando, F., Cavallo, S., Cardelli, P.,
Fallucca, S., Alessi, E., Letizia, C., Jimenez, A., Fallucca, F. and Pugliese, G. (2010).
"Anti-inflammatory effect of exercise training in subjects with type 2 diabetes and the
metabolic syndrome is dependent on exercise modalities and independent of weight
loss." Nutrition, Metabolism and Cardiovascular Diseases 20(8): 608-617.
Balkau, B. and Charles, M. A. (1999). "Comment on the provisional report from the
WHO consultation. European Group for the Study of Insulin Resistance (EGIR)."
Diabetic Medicine 16(5): 442-443.
Banday, M. Z., Sameer, A. S. and Nissar, S. (2020). "Pathophysiology of diabetes:
An overview." Avicenna Journal of Medicine 10(4): 174-188.

220
Banerjee, M., Macdougall, M. and Lakhdar, A. F. (2012). "Impact of a single one-to-
one education session on glycemic control in patients with diabetes." Journal of
Diabetes 4(2): 186-190.
Bastien, C. H., Vallières, A. and Morin, C. M. (2001). "Validation of the Insomnia
Severity Index as an outcome measure for insomnia research." Sleep Medicine 2(4):
297-307.
Benson, A. C., Torode, M. E. and Fiatarone Singh, M. A. (2008). "The effect of high-
intensity progressive resistance training on adiposity in children: A randomized
controlled trial." International Journal of Obesity 32(6): 1016-1027.
Beserra, A. H. N., Kameda, P., Deslandes, A. C., Schuch, F. B., Laks, J. and
Moraes, H. S. (2018). "Can physical exercise modulate cortisol level in subjects with
depression? A systematic review and meta-analysis." Trends in Psychiatry and
Psychotherapy 40(4): 360-368.
Black, L. E., Swan, P. D. and Alvar, B. A. (2010). "Effects of intensity and volume on
insulin sensitivity during acute bouts of resistance training." The Journal of Strength
and Conditioning Research 24(4): 1109-1116.
Blumenthal, J. A., Babyak, M. A., Doraiswamy, P. M., Watkins, L., Hoffman, B. M.,
Barbour, K. A., Herman, S., Craighead, W. E., Brosse, A. L., Waugh, R., Hinderliter,
A. and Sherwood, A. (2007). "Exercise and pharmacotherapy in the treatment of
major depressive disorder." Psychosomatic Medicine 69(7): 587-596.
Blumenthal, J. A., Babyak, M. A., Moore, K. A., Craighead, W. E., Herman, S.,
Khatri, P., Waugh, R., Napolitano, M. A., Forman, L. M., Appelbaum, M.,
Doraiswamy, P. M. and Krishnan, K. R. (1999). "Effects of exercise training on older
patients with major depression." Archives of Internal Medicine 159(19): 2349-2356.

221
Blumenthal, J. A., Babyak, M. A., O’Connor, C., Keteyian, S., Landzberg, J., Howlett,
J., Kraus, W., Gottlieb, S., Blackburn, G., Swank, A. and Whellan, D. J. (2012).
"Effects of exercise training on depressive symptoms in patients with chronic heart
failure: The HF-ACTION randomized trial." Journal of the American Medical
Association 308(5): 465-474.
Blumenthal, J. A., Sherwood, A., Babyak, M. A., Watkins, L. L., Smith, P. J.,
Hoffman, B. M., O'Hayer, C. V. F., Mabe, S., Johnson, J., Doraiswamy, P. M., Jiang,
W., Schocken, D. D. and Hinderliter, A. L. (2012). "Exercise and pharmacological
treatment of depressive symptoms in patients with coronary heart disease: Results
from the UPBEAT (Understanding the Prognostic Benefits of Exercise and
Antidepressant Therapy) study." Journal of the American College of Cardiology
60(12): 1053-1063.
Borg, G. (1970). "Perceived exertion as an indicator of somatic stress." Scandinavian
Journal of Rehabilitation Medicine 2(2): 92-98.
Bouchard, D. R., Soucy, L., Sénéchal, M., Dionne, I. J. and Brochu, M. (2009).
"Impact of resistance training with or without caloric restriction on physical capacity in
obese older women." Menopause 16(1).
Boulé, N. G., Haddad, E., Kenny, G. P., Wells, G. A. and Sigal, R. J. (2001). "Effects
of exercise on glycemic control and body mass in type 2 diabetes mellitus: a meta-
analysis of controlled clinical trials." The Journal of the American Medical Association
286(10): 1218-1227.
Bryner, R. W., Ullrich, I. H., Sauers, J., Donley, D., Hornsby, G., Kolar, M. and
Yeater, R. (1999). "Effects of resistance vs. aerobic training combined with an 800
calorie liquid diet on lean body mass and resting metabolic rate." Journal of the
American College of Nutrition 18(2): 115-121.

222
Buysse, D. J., Reynolds, C. F., Monk, T. H., Berman, S. R. and Kupfer, D. J. (1989).
"The Pittsburgh sleep quality index: A new instrument for psychiatric practice and
research." Psychiatry Research 28(2): 193-213.
Callaghan, B. C., Cheng, H. T., Stables, C. L., Smith, A. L. and Feldman, E. L.
(2012). "Diabetic neuropathy: Clinical manifestations and current treatments." The
Lancet. Neurology 11(6): 521-534.
Carroll, B. J., Cassidy, F., Naftolowitz, D., Tatham, N. E., Wilson, W. H., Iranmanesh,
A., Liu, P. Y. and Veldhuis, J. D. (2007). "Pathophysiology of hypercortisolism in
depression." Acta Psychiatrica Scandinavica 115(s433): 90-103.
Carrozzino, D., Patierno, C., Fava, G. A. and Guidi, J. (2020). "The Hamilton Rating
Scales for Depression: A Critical Review of Clinimetric Properties of Different
Versions." Psychotherapy and Psychosomatics 89(3): 133-150.
Castaneda, C., Layne, J. E., Munoz-Orians, L., Gordon, P. L., Walsmith, J., Foldvari,
M., Roubenoff, R., Tucker, K. L. and Nelson, M. E. (2002). "A randomized controlled
trial of resistance exercise training to improve glycemic control in older adults with
type 2 diabetes." Diabetes Care 25(12): 2335-2341.
Cefalu, W. T. (2001). "Insulin resistance: Cellular and clinical concepts."
Experimental Biology and Medicine 226(1): 13-26.
Celik Guzel, E., Bakkal, E., Guzel, S., Eroglu, H. E., Acar, A., Kuçukyalcin, V. and
Topcu, B. (2014). "Can low brain-derived neurotrophic factor levels be a marker of
the presence of depression in obese women?" Neuropsychiatric Disease and
Treatment 10: 2079-2086.
Chaudhury, A., Duvoor, C., Reddy Dendi, V. S., Kraleti, S., Chada, A., Ravilla, R.,
Marco, A., Shekhawat, N. S., Montales, M. T., Kuriakose, K., Sasapu, A., Beebe, A.,
Patil, N., Musham, C. K., Lohani, G. P. and Mirza, W. (2017). "Clinical review of

223
antidiabetic drugs: Implications for type 2 diabetes mellitus management." Frontiers
in Endocrinology 8: 6-6.
Chen, I. P., Liu, S.-I., Huang, H.-C., Sun, F.-J., Huang, C.-R., Sung, M.-R. and
Huang, Y.-P. (2016). "Validation of the Patient Health Questionnaire for Depression
Screening Among the Elderly Patients in Taiwan." International Journal of
Gerontology 10(4): 193-197.
Chiodini, I., Adda, G., Scillitani, A., Coletti, F., Morelli, V., Di Lembo, S., Epaminonda,
P., Masserini, B., Beck-Peccoz, P., Orsi, E., Ambrosi, B. and Arosio, M. (2007).
"Cortisol secretion in patients with type 2 diabetes." Diabetes Care 30(1): 83.
Chireh, B., Li, M. and D'Arcy, C. (2019). "Diabetes increases the risk of depression:
A systematic review, meta-analysis and estimates of population attributable fractions
based on prospective studies." Preventive Medicine Reports 14: 100822-100822.
Choi, B. C. and Shi, F. (2001). "Risk factors for diabetes mellitus by age and sex:
Results of the National Population Health Survey." Diabetologia 44(10): 1221-1231.
Cholerton, B., Baker, L. D., Montine, T. J. and Craft, S. (2016). "Type 2 diabetes,
cognition, and dementia in older adults: Toward a precision health approach."
Diabetes Spectrum :A Publication of the American Diabetes Association 29(4): 210-
219.
Cleasby, M. E., Jamieson, P. M. and Atherton, P. J. (2016). "Insulin resistance and
sarcopenia: Mechanistic links between common co-morbidities." Journal of
Endocrinology 229(2): R67-81.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. New York,
Academic press.

224
Cooney, G. M., Dwan, K., Greig, C. A., Lawlor, D. A., Rimer, J., Waugh, F. R.,
McMurdo, M. and Mead, G. E. (2013). "Exercise for depression." Cochrane
Database of Systematic Reviews(9): Cd004366.
Cullmann, M., Hilding, A. and Östenson, C. G. (2012). "Alcohol consumption and risk
of pre-diabetes and type 2 diabetes development in a Swedish population." Diabetic
Medicine 29(4): 441-452.
Daly, R. M., Dunstan, D. W., Owen, N., Jolley, D., Shaw, J. E. and Zimmet, P. Z.
(2005). "Does high-intensity resistance training maintain bone mass during moderate
weight loss in older overweight adults with type 2 diabetes?" Osteoporosis
International 16(12): 1703-1712.
Dela, F., Ploug, T., Handberg, A., Petersen, L. N., Larsen, J. J., Mikines, K. J. and
Galbo, H. (1994). "Physical training increases muscle GLUT4 protein and mRNA in
patients with NIDDM." Diabetes 43(7): 862.
Dixon, J. B., Lambert, E. A., Grima, M., Rice, T., Lambert, G. W. and Straznicky, N.
E. (2015). "Fat-free mass loss generated with weight loss in overweight and obese
adults: What may we expect?" Diabetes, Obesity and Metabolism 17(1): 91-93.
Dobrică, E.-C., Găman, M.-A., Cozma, M.-A., Bratu, O. G., Pantea Stoian, A. and
Diaconu, C. C. (2019). "Polypharmacy in type 2 diabetes mellitus: Insights from an
internal medicine department." Medicina 55(8): 436.
Dumbreck, S., Flynn, A., Nairn, M., Wilson, M., Treweek, S., Mercer, S., Alderson,
P., Thompson, A., Payne, K. and Guthrie, B. (2015). "Drug-disease and drug-drug
interactions: Systematic examination of recommendations in 12 UK national clinical
guidelines." BMJ 350: h949.
225
Dunn, A. L., Trivedi, M. H., Kampert, J. B., Clark, C. G. and Chambliss, H. O. (2005).
"Exercise treatment for depression: Efficacy and dose response." American Journal
of Preventive Medicine 28(1): 1-8.
Dunstan, D. W., Daly, R. M., Owen, N., Jolley, D., Courten, M. d., Shaw, J. and
Zimmet, P. (2002). "High-intensity resistance training improves glycemic control in
older patients with type 2 diabetes." Diabetes Care 25(10): 1729-1736.
Dunstan, D. W., Daly, R. M., Owen, N., Jolley, D., Vulikh, E., Shaw, J. and Zimmet,
P. (2005). "Home-based resistance training is not sufficient to maintain improved
glycemic control following supervised training in older individuals with type 2
diabetes." Diabetes Care 28(1): 3-9.
Duruturk, N. and Ozkoslu, M. A. (2019). "Effect of tele-rehabilitation on glucose
control, exercise capacity, physical fitness, muscle strength and psychosocial status
in patients with type 2 diabetes: A double blind randomized controlled trial." Primary
Care Diabetes 13(6): 542-548.
Duval, F., Lebowitz, B. D. and Macher, J.-P. (2006). "Treatments in depression."
Dialogues in Clinical Neuroscience 8(2): 191-206.
Einhorn, D., Reaven, G. M., Cobin, R. H., Ford, E., Ganda, O. P., Handelsman, Y.,
Hellman, R., Jellinger, P. S., Kendall, D., Krauss, R. M., Neufeld, N. D., Petak, S. M.,
Rodbard, H. W., Seibel, J. A., Smith, D. A. and Wilson, P. W. (2003). "American
College of Endocrinology position statement on the insulin resistance syndrome."
Endocrine Practice 9(3): 237-252.
Ekkekakis, P. (2021). "Why is exercise underutilized in clinical practice despite
evidence it is effective? Lessons in pragmatism from the inclusion of exercise in
guidelines for the treatment of depression in the British National Health Service."
Kinesiology Review 10(1): 29-50.

226
Emerging Risk Factors Collaboration, Sarwar, N., Gao, P., Seshasai, S. R. K.,
Gobin, R., Kaptoge, S., Di Angelantonio, E., Ingelsson, E., Lawlor, D. A., Selvin, E.,
Stampfer, M., Stehouwer, C. D. A., Lewington, S., Pennells, L., Thompson, A.,
Sattar, N., White, I. R., Ray, K. K. and Danesh, J. (2010). "Diabetes mellitus, fasting
blood glucose concentration, and risk of vascular disease: a collaborative meta-
analysis of 102 prospective studies." Lancet 375(9733): 2215-2222.
Ewing, J. A. (1984). "Detecting alcoholism: The CAGE questionnaire." The Journal of
the American Medical Association 252(14): 1905-1907.
Farooqi, A., Khunti, K., Abner, S., Gillies, C., Morriss, R. and Seidu, S. (2019).
"Comorbid depression and risk of cardiac events and cardiac mortality in people with
diabetes: A systematic review and meta-analysis." Diabetes Research and Clinical
Practice 156: 107816.
Ferguson, J. M. (2001). "SSRI antidepressant medications: Adverse effects and
tolerability." Primary Care Companion to the Journal of Clinical Psychiatry 3(1): 22-
27.
Ferreira, L. S. S., Fernandes, C. S., Vieira, M. N. N. and De Felice, F. G. (2018).
"Insulin resistance in Alzheimer's disease." Frontiers in Neuroscience 12: 830-830.
Ford, E. S., Li, C. and Sattar, N. (2008). "Metabolic syndrome and incident diabetes:
current state of the evidence." Diabetes care 31(9): 1898-1904.
Ford, E. S., Li, C. and Sattar, N. (2008). "Metabolic syndrome and incident diabetes:
Current state of the evidence." Diabetes Care 31(9): 1898-1904.
Fragala, M. S., Cadore, E. L., Dorgo, S., Izquierdo, M., Kraemer, W. J., Peterson, M.
D. and Ryan, E. D. (2019). "Resistance training for older adults: Position statement
from the National Strength and Conditioning Association." The Journal of Strength &
Conditioning Research 33(8).
227
Garber, C. E., Blissmer, B., Deschenes, M. R., Franklin, B. A., Lamonte, M. J., Lee,
I. M., Nieman, D. C. and Swain, D. P. (2011). "Quantity and quality of exercise for
developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor
fitness in apparently healthy adults: Guidance for prescribing exercise." Medicine &
Science in Sports & Exercise 43(7).
Geer, E. B. and Shen, W. (2009). "Gender differences in insulin resistance, body
composition, and energy balance." Gender Medicine 6 Suppl 1(Suppl 1): 60-75.
Gelenberg, A. J., Freeman, M. P., Markowitz, J. C., Rosenbaum, J. F., Thase, M. E.,
Trivedi, M. H. and Rhoads, R. S. V. (2010). "Practice guideline for the treatment of
patients with Major Depressive Disorder." American Psychiatric Association
(3): 17-38.
Gerstein, H. C., Santaguida, P., Raina, P., Morrison, K. M., Balion, C., Hunt, D.,
Yazdi, H. and Booker, L. (2007). "Annual incidence and relative risk of diabetes in
people with various categories of dysglycemia: A systematic overview and meta-
analysis of prospective studies." Diabetes Research and Clinical Practice 78(3): 305-
312.
Golden, S. H., Lazo, M., Carnethon, M., Bertoni, A. G., Schreiner, P. J., Roux, A. V.
D., Lee, H. B. and Lyketsos, C. (2008). "Examining a bidirectional association
between depressive symptoms and diabetes." Journal of the American Medical
Association 299(23): 2751-2759.
Gonçalves, C. B., Moreira, L. B., Gus, M. and Fuchs, F. D. (2007). "Adverse events
of blood-pressure-lowering drugs: Evidence of high incidence in a clinical setting."
European Journal of Clinical Pharmacology 63(10): 973-978.
228
Gordon, B. A., Benson, A. C., Bird, S. R. and Fraser, S. F. (2009). "Resistance
training improves metabolic health in type 2 diabetes: A systematic review." Diabetes
Research and Clinical Practice 83(2): 157-175.
Gordon, B. R., McDowell, C. P., Hallgren, M., Meyer, J. D., Lyons, M. and Herring,
M. P. (2018). "Association of efficacy of resistance exercise training with depressive
symptoms: Meta-analysis and meta-regression analysis of randomized clinical trials."
JAMA Psychiatry 75(6): 566-576.
Greco, E. A., Pietschmann, P. and Migliaccio, S. (2019). "Osteoporosis and
sarcopenia increase frailty syndrome in the elderly." Frontiers in Endocrinology 10:
255-255.
Grgic, J., McLlvenna, L. C., Fyfe, J. J., Sabol, F., Bishop, D. J., Schoenfeld, B. J. and
Pedisic, Z. (2019). "Does aerobic training promote the same skeletal muscle
hypertrophy as resistance training? A systematic review and meta-analysis." Sports
Medicine 49(2): 233-254.
Grundy, S. M. (2006). "Drug therapy of the metabolic syndrome: minimizing the
emerging crisis in polypharmacy." Nature Reviews Drug Discovery 5(4): 295-309.
Guerrero Fernández de Alba, I., Gimeno-Miguel, A., Poblador-Plou, B., Gimeno-
Feliu, L. A., Ioakeim-Skoufa, I., Rojo-Martínez, G., Forjaz, M. J. and Prados-Torres,
A. (2020). "Association between mental health comorbidity and health outcomes in
type 2 diabetes mellitus patients." Scientific Reports 10(1): 19583.
Haffner, S. M., Miettinen, H., Gaskill, S. P. and Stern, M. P. (1996). "Metabolic
precursors of hypertension: The San Antonio heart study." Archives of Internal
Medicine 156(17): 1994-2001.
229
Hamilton, K. C., Fisher, G., Roy, J. L., Gower, B. A. and Hunter, G. R. (2013). "The
effects of weight loss on relative bone mineral density in premenopausal women."
Obesity 21(3): 441-448.
Hamilton, M. (1967). "Development of a rating scale for primary depressive illness."
British Journal of Social and Clinical Psychology 6(4): 278-296.
Helgadóttir, B., Forsell, Y., Hallgren, M., Möller, J. and Ekblom, Ö. (2017). "Long-
term effects of exercise at different intensity levels on depression: A randomized
controlled trial." Preventive Medicine 105: 37-46.
Herring, M. P., Puetz, T. W., O’Connor, P. J. and Dishman, R. K. (2012). "Effect of
exercise training on depressive symptoms among patients with a chronic illness: A
systematic review and meta-analysis of randomized controlled trials." Archives of
Internal Medicine 172(2): 101-111.
Higgins, J., Li, T. and Deeks, J. (2021). Chapter 6: Choosing effect measures and
computing estimates of effect. Cochrane Handbook for Systematic Reviews of
Interventions. J. Higgins, J. Thomas, J. Chandler et al., Cochrane.
Higgins, J., Thomas, J., Chandler, J., M, M. C., Li, T., Page, M. and Welch, V.
(2021). Chapter 6: Choosing effect measures and computing estimates of effect.
Cochrane Handbook for Systematic Reviews of Interventions. J. Higgins, T. Li and J.
Deeks, Cochrane.
Hirani, V., Blyth, F., Naganathan, V., Le Couteur, D. G., Seibel, M. J., Waite, L. M.,
Handelsman, D. J. and Cumming, R. G. (2015). "Sarcopenia is associated with
incident disability, institutionalization, and mortality in community-dwelling older men:
The concord health and ageing in men project." Journal of the American Medical
Directors Association 16(7): 607-613.
230
Holman, R., Hines, G., Kennedy, I., Stevens, R., Matthews, D. and Levy, J. (2004).
"A calculator for HOMA." Diabetologia 47(Suppl. 1: A222).
Holten, M. K., Zacho, M., Gaster, M., Juel, C., Wojtaszewski, J. F. P. and Dela, F.
(2004). "Strength training increases insulin-mediated glucose uptake, GLUT4
content, and insulin signaling in skeletal muscle in patients with type 2 diabetes."
Diabetes 53(2): 294.
Holvast, F., van Hattem, B. A., Sinnige, J., Schellevis, F., Taxis, K., Burger, H. and
Verhaak, P. F. M. (2017). "Late-life depression and the association with
multimorbidity and polypharmacy: A cross-sectional study." Family Practice 34(5):
539-545.
Huang, Y. T., Wei, L., Steptoe, A. and Zaninotto, P. (2019). "OP48 The prevalence
and risk factors of polypharmacy among diabetic people: evidence from the english
longitudinal study of ageing (ELSA)." Journal of Epidemiology and Community
Health 73(Suppl 1): A23.
Hussey, S. E., McGee, S. L., Garnham, A., Wentworth, J. M., Jeukendrup, A. E. and
Hargreaves, M. (2011). "Exercise training increases adipose tissue GLUT4
expression in patients with type 2 diabetes." Diabetes, Obesity and Metabolism
13(10): 959-962.
Ibañez, J., Izquierdo, M., Argüelles, I., Forga, L., Larrión, J. L., García-Unciti, M.,
Idoate, F. and Gorostiaga, E. M. (2005). "Twice-weekly progressive resistance
training decreases abdominal fat and improves insulin sensitivity in older men with
type 2 diabetes." Diabetes Care 28(3): 662.
Ismail, L., Materwala, H. and Al Kaabi, J. (2021). "Association of risk factors with
type 2 diabetes: A systematic review." Computational and Structural Biotechnology
Journal 19: 1759-1785.
231
Jia, Y., Lao, Y., Zhu, H., Li, N. and Leung, S. W. (2019). "Is metformin still the most
efficacious first-line oral hypoglycaemic drug in treating type 2 diabetes? A network
meta-analysis of randomized controlled trials." Obesity Reviews 20(1): 1-12.
Joseph, M. S., Tincopa, M. A., Walden, P., Jackson, E., Conte, M. L. and Rubenfire,
M. (2019). "The impact of structured exercise programs on metabolic syndrome and
its components: A systematic review." Diabetes, Metabolic Syndrome and Obesity :
Targets and Therapy 12: 2395-2404.
Kanaley, J. A., Colberg, S. R., Corcoran, M. H., Malin, S. K., Rodriguez, N. R.,
Crespo, C. J., Kirwan, J. P. and Zierath, J. R. (2022). "Exercise/physical activity in
individuals with type 2 diabetes: A consensus statement from the American College
of Sports Medicine." Medicine & Science in Sports & Exercise 54(2).
Karczewska-Kupczewska, M., Adamska, A., Nikolajuk, A., Otziomek, E., Gorska, M.,
Straczkowski, M. and Kowalska, I. (2010). "Decreased serum brain-derived
neurotrophic factor concentration in young nonobese subjects with low insulin
sensitivity." Endocrine Abstracts 22: 345.
Kennedy, J. W., Hirshman, M. F., Gervino, E. V., Ocel, J. V., Forse, R. A., Hoenig, S.
J., Aronson, D., Goodyear, L. J. and Horton, E. S. (1999). "Acute exercise induces
GLUT4 translocation in skeletal muscle of normal human subjects and subjects with
type 2 diabetes." Diabetes 48(5): 1192.
Kenney, M. J. and Seals, D. R. (1993). Postexercise hypotension. Key features,
mechanisms, and clinical significance.
Knol, M. J., Twisk, J. W. R., Beekman, A. T. F., Heine, R. J., Snoek, F. J. and
Pouwer, F. (2006). "Depression as a risk factor for the onset of type 2 diabetes
mellitus. A meta-analysis." Diabetologia 49(5): 837.
232
Knowler, W. C., Barrett-Connor, E., Fowler, S. E., Hamman, R. F., Lachin, J. M.,
Walker, E. A. and Nathan, D. M. (2002). "Reduction in the incidence of type 2
diabetes with lifestyle intervention or metformin." The New England Journal of
Medicine 346(6): 393-403.
Krabbe, K. S., Nielsen, A. R., Krogh-Madsen, R., Plomgaard, P., Rasmussen, P.,
Erikstrup, C., Fischer, C. P., Lindegaard, B., Petersen, A. M. W., Taudorf, S.,
Secher, N. H., Pilegaard, H., Bruunsgaard, H. and Pedersen, B. K. (2007). "Brain-
derived neurotrophic factor (BDNF) and type 2 diabetes." Diabetologia 50(2): 431-
438.
Kvam, S., Kleppe, C. L., Nordhus, I. H. and Hovland, A. (2016). "Exercise as a
treatment for depression: A meta-analysis." J Affect Disord 202: 67-86.
Lange, A. K., Vanwanseele, B. and Fiatarone singh, M. A. (2008). "Strength training
for treatment of osteoarthritis of the knee: A systematic review." Arthritis Care &
Research 59(10): 1488-1494.
Latham, N. K., Bennett, D. A., Stretton, C. M. and Anderson, C. S. (2004).
"Systematic review of progressive resistance strength training in older adults."
Journal of Gerontology: Series A, Biological Sciences and Medical Sciences 59(1):
48-61.
Lebovitz, H. E. (2019). "Thiazolidinediones: The forgotten diabetes medications."
Current Diabetes Reports 19(12): 151-151.
Lee, C. M., Colagiuri, R., Magliano, D. J., Cameron, A. J., Shaw, J., Zimmet, P. and
Colagiuri, S. (2013). "The cost of diabetes in adults in Australia." Diabetes Research
and Clinical Practice 99(3): 385-390.
233
Lee, J., Kim, D. and Kim, C. (2017). "Resistance training for glycemic control,
muscular strength, and lean body mass in old type 2 diabetic patients: A meta-
analysis." Diabetes Therapy 8(3): 459-473.
Lee, Y.-C., Chatterton, M. L., Magnus, A., Mohebbi, M., Le, L. K.-D. and
Mihalopoulos, C. (2017). "Cost of high prevalence mental disorders: Findings from
the 2007 Australian national survey of mental health and wellbeing." Australian &
New Zealand Journal of Psychiatry 51(12): 1198-1211.
Leehey, D. J., Collins, E., Kramer, H. J., Cooper, C., Butler, J., McBurney, C.,
Jelinek, C., Reda, D., Edwards, L., Garabedian, A. and O''Connell, S. (2016).
"Structured exercise in obese diabetic patients with chronic kidney disease: A
randomized controlled trial." American Journal of Nephrology 44(1): 54-62.
Leonard, B. E. (2018). "Inflammation and depression: A causal or coincidental link to
the pathophysiology?" Acta Neuropsychiatrica 30(1): 1-16.
Levinger, I., Selig, S., Goodman, C., Jerums, G., Stewart, A. and Hare, D. L. (2011).
"Resistance training improves depressive symptoms in individuals at high risk for
type 2 diabetes." The Journal of Strength and Conditioning Research 25(8): 2328-
2333.
Li, Y., Su, Y., Chen, S., Zhang, Y., Zhang, Z., Liu, C., Lu, M., Liu, F., Li, S., He, Z.,
Wang, Y., Sheng, L., Wang, W., Zhan, Z., Wang, X. and Zheng, N. (2016). "The
effects of resistance exercise in patients with knee osteoarthritis: A systematic
review and meta-analysis." Clinical Rehabilitation 30(10): 947-959.
Lie, J. D., Tu, K. N., Shen, D. D. and Wong, B. M. (2015). "Pharmacological
treatment of insomnia." Pharmacy and Therapeutics 40(11): 759-771.
Lincoln, A. K., Shepherd, A., Johnson, P. L. and Castaneda-Sceppa, C. (2011). "The
impact of resistance exercise training on the mental health of older Puerto Rican
234
adults with type 2 diabetes." The Journals of Gerontology, Series B: Psychological
Sciences and Social Sciences 66(5): 567-570.
Little, J. P., Gillen, J. B., Percival, M. E., Safdar, A., Tarnopolsky, M. A., Punthakee,
Z., Jung, M. E. and Gibala, M. J. (2011). "Low-volume high-intensity interval training
reduces hyperglycemia and increases muscle mitochondrial capacity in patients with
type 2 diabetes." Journal of Applied Physiology 111(6): 1554-1560.
Little, R. R., Rohlfing, C. L., Sacks, D. B. and for the National Glycohemoglobin
Standardization Program Steering, C. (2011). "Status of hemoglobin A1c
measurement and goals for improvement: From chaos to order for improving
diabetes care." Clinical Chemistry 57(2): 205-214.
Liu, C. J. and Latham, N. (2010). "Adverse events reported in progressive resistance
strength training trials in older adults: 2 sides of a coin." Archives of Physical
Medicine and Rehabilitation 91(9): 1471-1473.
Liu, Y., Ye, W., Chen, Q., Zhang, Y., Kuo, C.-H. and Korivi, M. (2019). "Resistance
exercise intensity is correlated with attenuation of HbA1c and insulin in patients with
type 2 diabetes: A systematic review and meta-Analysis." International Journal of
Environmental Research and Public Health 16(1): 140.
López-Pina, J. A., Sánchez-Meca, J. and Rosa-Alcázar, A. I. (2009). "The Hamilton
Rating Scale for Depression: A meta-analytic reliability generalization study."
International Journal of Clinical and Health Psychology 9(1): 143-159.
Löwe, B., Unützer, J., Callahan, C. M., Perkins, A. J. and Kroenke, K. (2004).
"Monitoring depression treatment outcomes with the patient health questionnaire-9."
Medical Care 42(12): 1194-1201.
235
Lyra E Silva, N. d. M., Lam, M. P., Soares, C. N., Munoz, D. P., Milev, R. and De
Felice, F. G. (2019). "Insulin resistance as a shared pathogenic mechanism between
depression and type 2 diabetes." Frontiers in Psychiatry 10: 57-57.
MacDonald, H. V., Johnson, B. T., Huedo-Medina, T. B., Livingston, J., Forsyth, K.
C., Kraemer, W. J., Farinatti, P. T. V. and Pescatello, L. S. (2016). "Dynamic
resistance training as stand-alone antihypertensive lifestyle therapy: A meta-
analysis." Journal of the American Heart Association 5(10): e003231.
Malhi, G. S., Bell, E., Singh, A. B., Bassett, D., Berk, M., Boyce, P., Bryant, R., Gitlin,
M., Hamilton, A., Hazell, P., Hopwood, M., Lyndon, B., McIntyre, R. S., Morris, G.,
Mulder, R., Porter, R., Yatham, L. N., Young, A. and Murray, G. (2020). "The 2020
Royal Australian and New Zealand College of Psychiatrists clinical practice
guidelines for mood disorders: Major depression summary." Bipolar Disorders 22(8):
788-804.
Masson, S. C. and Tejani, A. M. (2013). "Minimum clinically important differences
identified for commonly used depression rating scales." Journal of Clinical
Epidemiology 66(7): 805-807.
Mata, J., Silva, M. N., Vieira, P. N., Carraça, E. V., Andrade, A. M., Coutinho, S. R.,
Sardinha, L. B. and Teixeira, P. J. (2009). "Motivational “spill-over” during weight
control: Increased self-determination and exercise intrinsic motivation predict eating
self-regulation." Health Psychology 28(6): 709-716.
Mavros, Y., Kay, S., Anderberg, K. A., Baker, M. K., Wang, Y., Zhao, R., Meiklejohn,
J., Climstein, M., O’Sullivan, A., de Vos, N., Baune, B. T., Blair, S. N., Simar, D.,
Rooney, K., Singh, N. and Fiatarone Singh, M. A. (2013). "Changes in Insulin
Resistance and HbA1c Are Related to Exercise-Mediated Changes in Body

236
Composition in Older Adults With Type 2 Diabetes: Interim outcomes from the
GREAT2DO trial." Diabetes Care 36(8): 2372-2379.
Mavros, Y., Kay, S., Simpson, K. A., Baker, M. K., Wang, Y., Zhao, R. R.,
Meiklejohn, J., Climstein, M., O'Sullivan, A. J., de Vos, N., Baune, B. T., Blair, S. N.,
Simar, D., Rooney, K., Singh, N. A. and Fiatarone Singh, M. A. (2014). "Reductions
in C-reactive protein in older adults with type 2 diabetes are related to improvements
in body composition following a randomized controlled trial of resistance training."
Journal of Cachexia, Sarcopenia and Muscle 5(2): 111-120.
Mezuk, B., Eaton, W. W., Albrecht, S. and Golden, S. H. (2008). "Depression and
type 2 diabetes over the lifespan: A meta-analysis." Diabetes Care 31(12): 2383-
2390.
Miller, E. G., Sethi, P., Nowson, C. A., Dunstan, D. W. and Daly, R. M. (2017).
"Effects of progressive resistance training and weight loss versus weight loss alone
on inflammatory and endothelial biomarkers in older adults with type 2 diabetes."
European Journal of Applied Physiolgy 117(8): 1669-1678.
Miller, W. C., Anton, H. A. and Townson, A. F. (2008). "Measurement properties of
the CESD scale among individuals with spinal cord injury." Spinal Cord 46(4): 287-
292.
Moraes, H. S., Silveira, H. S., Oliveira, N. A., Matta Mello Portugal, E., Araújo, N. B.,
Vasques, P. E., Bergland, A., Santos, T. M., Engedal, K., Coutinho, E. S., Schuch, F.
B., Laks, J. and Deslandes, A. C. (2020). "Is strength training as effective as aerobic
training for depression in older adults? A randomized controlled trial."
Neuropsychobiology 79(2): 141-149.
Morres, I. D., Hatzigeorgiadis, A., Stathi, A., Comoutos, N., Arpin-Cribbie, C.,
Krommidas, C. and Theodorakis, Y. (2019). "Aerobic exercise for adult patients with

237
major depressive disorder in mental health services: A systematic review and meta-
analysis." Depression and Anxiety 36(1): 39-53.
Morris, S. B. (2007). "Estimating effect sizes from pretest-posttest-control group
designs." Organizational Research Methods 11(2): 364-386.
Morris, S. B. and DeShon, R. P. (2002). "Combining effect size estimates in meta-
analysis with repeated measures and independent-groups designs." Psychological
Methods 7(1): 105-125.
Mueller, M. J., Tuttle, L. J., Lemaster, J. W., Strube, M. J., McGill, J. B., Hastings, M.
K. and Sinacore, D. R. (2013). "Weight-bearing versus nonweight-bearing exercise
for persons with diabetes and peripheral neuropathy: A randomized controlled trial."
Archives of Physical Medicine and Rehabilitation 94(5): 829-838.
Naci, H., Salcher-Konrad, M., Dias, S., Blum, M. R., Sahoo, S. A., Nunan, D. and
Ioannidis, J. P. A. (2019). "How does exercise treatment compare with
antihypertensive medications? A network meta-analysis of 391 randomised
controlled trials assessing exercise and medication effects on systolic blood
pressure." British Journal of Sports Medicine 53(14): 859.
Naismith, S. L., Norrie, L. M., Mowszowski, L. and Hickie, I. B. (2012). "The
neurobiology of depression in later-life: Clinical, neuropsychological, neuroimaging
and pathophysiological features." Progress in Neurobiology 98(1): 99-143.
Nam, S., Dobrosielski, D. A. and Stewart, K. J. (2012). "Predictors of exercise
intervention dropout in sedentary individuals with type 2 diabetes." Journal of
Cardiopulmonary Rehabilitation and Prevention 32(6): 370-378.
National Cholesterol Education Program (NCEP) Expert Panel on Detection
Evaluation and Treatment of High Blood Cholesterol in Adults (Adult Treatment
Panel III) (2002). "Third report of the National Cholesterol Education Program

238
(NCEP) expert panel on detection, evaluation, and treatment of high blood
cholesterol in adults (Adult Treatment Panel III) final report." Circulation 106(25):
3143-3421.
Nebiker, L., Lichtenstein, E., Minghetti, A., Zahner, L., Gerber, M., Faude, O. and
Donath, L. (2018). "Moderating effects of exercise duration and intensity in
neuromuscular vs. endurance exercise interventions for the treatment of depression:
A meta-analytical review." Frontiers in Psychiatry 9: 305-305.
Nguyen, Q., Dominguez, J., Nguyen, L. and Gullapalli, N. (2010). "Hypertension
management: An update." American Health & Drug Benefits 3(1): 47-56.
Norvell, N. and Belles, D. (1993). "Psychological and physical benefits of circuit
weight training in law enforcement personnel." Journal of Consulting and Clinical
Psychology 61(3): 520-527.
Nouwen, A., Adriaanse, M. C., van Dam, K., Iversen, M. M., Viechtbauer, W., Peyrot,
M., Caramlau, I., Kokoszka, A., Kanc, K., de Groot, M., Nefs, G., Pouwer, F. and the
European Depression in Diabetes Research, C. (2019). "Longitudinal associations
between depression and diabetes complications: a systematic review and meta-
analysis." Diabetic Medicine 36(12): 1562-1572.
Nouwen, A., Winkley, K., Twisk, J., Lloyd, C. E., Peyrot, M., Ismail, K., Pouwer, F.
and European Depression in Diabetes Research, C. (2010). "Type 2 diabetes
mellitus as a risk factor for the onset of depression: A systematic review and meta-
analysis." Diabetologia 53(12): 2480-2486.
Otte, C., Gold, S. M., Penninx, B. W., Pariante, C. M., Etkin, A., Fava, M., Mohr, D.
C. and Schatzberg, A. F. (2016). "Major depressive disorder." Nature Reviews
Disease Primers 2: 16065.

239
Ouakinin, S. R. S., Barreira, D. P. and Gois, C. J. (2018). "Depression and obesity:
Integrating the role of stress, neuroendocrine dysfunction and inflammatory
pathways." Frontiers in Endocrinology 9: 431-431.
Paffenbarger, R. S. J., Wing, A. L. and Hyde, R. T. (1978). "Physical activity as an
index of heart attack risk in college alumni." American Journal of Epidemiology
108(3): 161-175.
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow,
C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J.,
Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E.,
McDonald, S., McGuinness, L. A., Stewart, L. A., Thomas, J., Tricco, A. C., Welch,
V. A., Whiting, P. and Moher, D. (2021). "The PRISMA 2020 statement: An updated
guideline for reporting systematic reviews." BMJ (Clinical research ed.) 372: n71-
n71.
Pan, A., Keum, N., Okereke, O. I., Sun, Q., Kivimaki, M., Rubin, R. R. and Hu, F. B.
(2012). "Bidirectional association between depression and metabolic syndrome: A
systematic review and meta-analysis of epidemiological studies." Diabetes Care
35(5): 1171-1180.
Pan, B., Ge, L., Xun, Y. Q., Chen, Y. J., Gao, C. Y., Han, X., Zuo, L. Q., Shan, H. Q.,
Yang, K. H., Ding, G. W. and Tian, J. H. (2018). "Exercise training modalities in
patients with type 2 diabetes mellitus: A systematic review and network meta-
analysis." International Journal of Behavioral Nutrition and Physical Activity 15(1):
72.
Pan, X.-R., Li, G.-W., Hu, Y.-H., Wang, J.-X., Yang, W.-Y., An, Z.-X., Hu, Z.-X., Juan,
L., Xiao, J.-Z., Cao, H.-B., Liu, P.-A., Jiang, X.-G., Jiang, Y.-Y., Wang, J.-P., Zheng,
H., Zhang, H., Bennett, P. H. and Howard, B. V. (1997). "Effects of diet and exercise
240
in preventing NIDDM in people with impaired glucose tolerance: The Da Qing IGT
and diabetes study." Diabetes Care 20(4): 537.
Parmenter, B. J., Mavros, Y., Ritti Dias, R., King, S. and Fiatarone Singh, M. (2020).
"Resistance training as a treatment for older persons with peripheral artery disease:
A systematic review and meta-analysis." British Journal of Sports Medicine 54(8):
452.
Partington, J. E. and Leiter, R. G. (1949). "Partington's pathways test." Psychological
Service Center Journal.
Pasco, J. A., Williams, L. J., Jacka, F. N., Stupka, N., Brennan-Olsen, S. L.,
Holloway, K. L. and Berk, M. (2015). "Sarcopenia and the common mental disorders:
A potential regulatory role of skeletal muscle on brain function?" Current
Osteoporosis Reports 13(5): 351-357.
Petersen, M. C. and Shulman, G. I. (2018). "Mechanisms of insulin action and insulin
resistance." Physiological Reviews 98(4): 2133-2223.
Petrie, J. R., Guzik, T. J. and Touyz, R. M. (2018). "Diabetes, hypertension, and
cardiovascular disease: Clinical insights and vascular mechanisms." The Canadian
Journal of Cardiology 34(5): 575-584.
Pham, T. M., Carpenter, J. R., Morris, T. P., Sharma, M. and Petersen, I. (2019).
"Ethnic differences in the prevalence of type 2 diabetes diagnoses in the UK: Cross-
sectional analysis of the health improvement network primary care database."
Clinical Epidemiology 11: 1081-1088.
Pibernik-Okanovic, M., Hermanns, N., Ajdukovic, D., Kos, J., Prasek, M., Sekerija,
M. and Lovrencic, M. V. (2015). "Does treatment of subsyndromal depression
improve depression-related and diabetes-related outcomes? A randomised
241
controlled comparison of psychoeducation, physical exercise and enhanced
treatment as usual." Trials 16: 305.
Plomgaard, P., Bouzakri, K., Krogh-Madsen, R., Mittendorfer, B., Zierath, J. R. and
Pedersen, B. K. (2005). "Tumor necrosis factor-α induces skeletal muscle insulin
resistance in healthy human subjects via inhibition of akt substrate 160
phosphorylation." Diabetes 54(10): 2939.
Putiri, A. L., Lovejoy, J. C., Gillham, S., Sasagawa, M., Bradley, R. and Sun, G.-C.
(2012). "Psychological effects of yi ren medical qigong and progressive resistance
training in adults with type 2 diabetes mellitus: A randomized controlled pilot study."
Alternative Therapies 18(1): 30-34.
Qadir, R., Sculthorpe, N. F., Todd, T. and Brown, E. C. (2021). "Effectiveness of
resistance training and associated program characteristics in patients at risk for type
2 diabetes: A systematic review and meta-analysis." Sports Medicine - Open 7(1):
38.
Qaseem, A., Barry, M. J. and Kansagara, D. (2016). "Nonpharmacologic versus
pharmacologic treatment of adult patients with major depressive disorder: A clinical
practice guideline from the american college of physicians." Annals of Internal
Medicine 164(5): 350-359.
Qato, D. M., Ozenberger, K. and Olfson, M. (2018). "Prevalence of Prescription
Medications With Depression as a Potential Adverse Effect Among Adults in the
United States." JAMA 319(22): 2289-2298.
Ramic, E., Prasko, S., Gavran, L. and Spahic, E. (2020). "Assessment of the
antidepressant side effects occurrence in patients treated in primary care." Materia
Socio-mMdica 32(2): 131-134.

242
Ramkumar, S., Raghunath, A. and Raghunath, S. (2016). "Statin therapy: Review of
safety and potential side effects." Acta Cardiologica Sinica 32(6): 631-639.
Rasgon, N. L. and McEwen, B. S. (2016). "Insulin resistance—a missing link no
more." Molecular Psychiatry 21(12): 1648-1652.
Ravindran, A. V., Balneaves, L. G., Faulkner, G., Ortiz, A., McIntosh, D., Morehouse,
R. L., Ravindran, L., Yatham, L. N., Kennedy, S. H., Lam, R. W., MacQueen, G. M.,
Milev, R. V. and Parikh, S. V. (2016). "Canadian Network for Mood and Anxiety
Treatments (CANMAT) 2016 clinical guidelines for the management of adults with
major depressive disorder: Section 5. complementary and alternative medicine
treatments." The Canadian Journal of Psychiatry 61(9): 576-587.
Reaven, G. M. (2005). "The insulin resistance syndrome: Definition and dietary
approaches to treatment." Annual Review of Nutrition 25(1): 391-406.
Renn, B. N., Feliciano, L. and Segal, D. L. (2011). "The bidirectional relationship of
depression and diabetes: A systematic review." Clinical Psychology Review 31(8):
1239-1246.
Rethlefsen, M. L., Kirtley, S., Waffenschmidt, S., Ayala, A. P., Moher, D., Page, M.
J., Koffel, J. B., Blunt, H., Brigham, T., Chang, S., Clark, J., Conway, A., Couban, R.,
de Kock, S., Farrah, K., Fehrmann, P., Foster, M., Fowler, S. A., Glanville, J., Harris,
E., Hoffecker, L., Isojarvi, J., Kaunelis, D., Ket, H., Levay, P., Lyon, J., McGowan, J.,
Murad, M. H., Nicholson, J., Pannabecker, V., Paynter, R., Pinotti, R., Ross-White,
A., Sampson, M., Shields, T., Stevens, A., Sutton, A., Weinfurter, E., Wright, K.,
Young, S. and Group, P.-S. (2021). "PRISMA-S: An extension to the PRISMA
statement for reporting literature searches in systematic reviews." Systematic
Reviews 10(1): 39.
243
Rey, A. (1941). "L'examen psychologique dans les cas d'encéphalopathie
traumatique.(Les problems.)." Archives de Psychologie.
Richter, E. A. and Hargreaves, M. (2013). "Exercise, GLUT4, and skeletal muscle
glucose uptake." Physiological Reviews 93(3): 993-1017.
Roberts, C. K., Hevener, A. L. and Barnard, R. J. (2013). "Metabolic syndrome and
insulin resistance: Underlying causes and modification by exercise training."
Comprehensive Physiology 3(1): 1-58.
Roberts, C. K., Little, J. P. and Thyfault, J. P. (2013). "Modification of insulin
sensitivity and glycemic control by activity and exercise." Medicine & Science in
Sports & Exercise 45(10).
Rohatgi, A. (2020). WebPlotDigitizer. V. Ver. 4.4.
https://automeris.io/WebPlotDigitizer.
Rustad, J. K., Musselman, D. L. and Nemeroff, C. B. (2011). "The relationship of
depression and diabetes: Pathophysiological and treatment implications."
Psychoneuroendocrinology 36(9): 1276-1286.
Sabag, A., Way, K. L., Keating, S. E., Sultana, R. N., O’Connor, H. T., Baker, M. K.,
Chuter, V. H., George, J. and Johnson, N. A. (2017). "Exercise and ectopic fat in
type 2 diabetes: A systematic review and meta-analysis." Diabetes & Metabolism
43(3): 195-210.
Salvetti, A., Brogi, G., Di Legge, V. and Bernini, G. P. (1993). "The inter-relationship
between insulin resistance and hypertension." Drugs 46(2): 149-159.
Schmitz, N., Deschenes, S. S., Burns, R. J., Smith, K. J., Lesage, A., Strychar, I.,
Rabasa-Lhoret, R., Freitas, C., Graham, E., Awadalla, P. and Wang, J. L. (2016).
"Depression and risk of type 2 diabetes: The potential role of metabolic factors."
Molecular Psychiatry 21(12): 1726-1732.

244
Schmitz, N., Deschênes, S. S., Burns, R. J., Smith, K. J., Lesage, A., Strychar, I.,
Rabasa-Lhoret, R., Freitas, C., Graham, E., Awadalla, P. and Wang, J. L. (2016).
"Depression and risk of type 2 diabetes: The potential role of metabolic factors."
Molecular Psychiatry 21(12): 1726-1732.
Schuch, F. B., Deslandes, A. C., Stubbs, B., Gosmann, N. P., Silva, C. T. B. d. and
Fleck, M. P. d. A. (2016). "Neurobiological effects of exercise on major depressive
disorder: A systematic review." Neuroscience & Biobehavioral Reviews 61: 1-11.
Schuch, F. B., Vancampfort, D., Richards, J., Rosenbaum, S., Ward, P. B. and
Stubbs, B. (2016). "Exercise as a treatment for depression: A meta-analysis
adjusting for publication bias." Journal of Psychiatric Research 77: 42-51.
Seimon, R. V., Wild-Taylor, A. L., Keating, S. E., McClintock, S., Harper, C., Gibson,
A. A., Johnson, N. A., Fernando, H. A., Markovic, T. P., Center, J. R., Franklin, J.,
Liu, P. Y., Grieve, S. M., Lagopoulos, J., Caterson, I. D., Byrne, N. M. and Sainsbury,
A. (2019). "Effect of weight loss via severe vs moderate energy restriction on lean
mass and body composition among postmenopausal women with obesity: The
TEMPO diet randomized clinical trial." JAMA Network Open 2(10): e1913733-
e1913733.
Shaw, J. and Tanamas, S. (2012). Diabetes: The silent pandemic and its impact on
Australia. Melbourne, Baker Health & Diabetes Institute.
Si, T. and Wang, P. (2014). "When is antidepressant polypharmacy appropriate in
the treatment of depression?" Shanghai Archives of Psychiatry 26(6): 357-359.
Siddaway, A. P., Wood, A. M. and Taylor, P. J. (2017). "The Center for
Epidemiologic Studies-Depression (CES-D) scale measures a continuum from well-
being to depression: Testing two key predictions of positive clinical psychology."
Journal of Affective Disorders 213: 180-186.
245
Silva, M. N., Markland, D., CarraÇA, E. V., Vieira, P. N., Coutinho, S. R., Minderico,
C. S., Matos, M. G., Sardinha, L. B. and Teixeira, P. J. (2011). "Exercise
autonomous motivation predicts 3-yr weight loss in women." Medicine & Science in
Sports & Exercise 43(4).
Silva, M. N., Vieira, P. N., Coutinho, S. R., Minderico, C. S., Matos, M. G., Sardinha,
L. B. and Teixeira, P. J. (2010). "Using self-determination theory to promote physical
activity and weight control: A randomized controlled trial in women." Journal of
Behavioral Medicine 33(2): 110-122.
Simpson, K. A., Mavros, Y., Kay, S., Meiklejohn, J., de Vos, N., Wang, Y., Guo, Q.,
Zhao, R., Climstein, M., Baune, B. T., Blair, S., O'Sullivan, A. J., Simar, D., Singh, N.
and Singh, M. A. F. (2015). "Graded Resistance Exercise And Type 2 Diabetes in
Older adults (The GREAT2DO study): methods and baseline cohort characteristics
of a randomized controlled trial." Trials 16: 512-512.
Singh, N. A., Clements, K. M. and Fiatarone, M. A. (1997). "A randomized controlled
trial of progressive resistance training in depressed elders." Journals of Gerontology
Series a-Biological Sciences and Medical Sciences 52(1): M27-M35.
Singh, N. A., Clements, K. M. and Fiatarone, M. A. (1997). "A randomized controlled
trial of progressive resistance training in depressed elders." The Journals of
Gerontology: Series A 52A(1): M27-M35.
Singh, N. A., Stavrinos, T. M., Scarbek, Y., Galambos, G., Liber, C. and Fiatarone
Singh, M. A. (2005). "A Randomized Controlled Trial of High Versus Low Intensity
Weight Training Versus General Practitioner Care for Clinical Depression in Older
Adults." The Journals of Gerontology Series A: Biological Sciences and Medical
Sciences 60(6): 768-776.

246
Singh, N. A., Stavrinos, T. M., Scarbek, Y., Galambos, G., Liber, C., Fiatarone Singh,
M. A. and Morley, J. E. (2005). "A randomized controlled trial of high versus low
intensity weight training Versus general practitioner care for clinical depression in
older adults." The Journals of Gerontology: Series A 60(6): 768-776.
Slade, S. C., Dionne, C. E., Underwood, M. and Buchbinder, R. (2016). "Consensus
on Exercise Reporting Template (CERT): Explanation and elaboration statement."
British Journal of Sports Medicine 50(23): 1428-1437.
Srikanthan, P., Hevener, A. L. and Karlamangla, A. S. (2010). "Sarcopenia
exacerbates obesity-associated insulin resistance and dysglycemia: Findings from
the National Health and Nutrition Examination Survey III." PLoS One 5(5): e10805.
Stephens, J. W., Brown, K. E. and Min, T. (2020). "Chronic kidney disease in type 2
diabetes: Implications for managing glycaemic control, cardiovascular and renal
risk." Diabetes, Obesity and Metabolism 22(S1): 32-45.
Sterne, J., Savović, J., Page, M., Elbers, R., Blencowe, N., Boutron, I., Cates, C.,
Cheng, H., Corbett, M., Eldridge, S., Hernán, M., Hopewell, S., Hróbjartsson, A.,
Junqueira, D., Jüni, P., Kirkham, J., Lasserson, T., Li, T., McAleenan, A., Reeves, B.,
Shepperd, S., Shrier, I., Stewart, L., Tilling, K., White, I., Whiting, P. and Higgins, J.
(2019). "RoB 2: A revised tool for assessing risk of bias in randomised trials." BMJ
3666.
Sterne JAC, S. J., Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng
H-Y, Corbett MS, Eldridge SM, Hernán MA, Hopewell S, Hróbjartsson A, Junqueira
DR, Jüni P, Kirkham JJ, Lasserson T, Li T, McAleenan A, Reeves BC, Shepperd S,
Shrier I, Stewart LA, Tilling K, White IR, Whiting PF, Higgins JPT (2019) "RoB 2: A
revised tool for assessing risk of bias in randomised trials." 366 DOI:
https://doi.org/10.1136/bmj.l4898.
247
Strasser, B., Arvandi, M. and Siebert, U. (2012). "Resistance training, visceral
obesity and inflammatory response: A review of the evidence." Obes Rev 13(7): 578-
591.
Strasser, B. and Schobersberger, W. (2011). "Evidence for resistance training as a
treatment therapy in obesity." Journal of Obesity 2011: 482564.
Strasser, B., Siebert, U. and Schobersberger, W. (2010). "Resistance training in the
treatment of the metabolic syndrome." Sports Medicine 40(5): 397-415.
Strasser, B., Siebert, U. and Schobersberger, W. (2010). "Resistance training in the
treatment of the metabolic syndrome: A systematic review and meta-analysis of the
effect of resistance training on metabolic clustering in patients with abnormal glucose
metabolism." Sports Medicine 40(5): 397-415.
Stubbs, B., Vancampfort, D., Hallgren, M., Firth, J., Veronese, N., Solmi, M., Brand,
S., Cordes, J., Malchow, B., Gerber, M., Schmitt, A., Correll, C. U., De Hert, M.,
Gaughran, F., Schneider, F., Kinnafick, F., Falkai, P., Möller, H.-J. and Kahl, K. G.
(2018). "EPA guidance on physical activity as a treatment for severe mental illness: a
meta-review of the evidence and Position Statement from the European Psychiatric
Association (EPA), supported by the International Organization of Physical
Therapists in Mental Health (IOPTMH)." European Psychiatry 54: 124-144.
Sun, G.-C., Lovejoy, J. C. and Bradley, R. (2008, January). "Effects of qigong on
type 2 diabetic patients." from https://ClinicalTrials.gov/show/NCT00885846.
Szuhany, K. L., Bugatti, M. and Otto, M. W. (2015). "A meta-analytic review of the
effects of exercise on brain-derived neurotrophic factor." Journal of Psychiatric
Research 60: 56-64.
Tai, M. M. (1994). "A mathematical model for the determination of total area under
glucose tolerance and other metabolic curves." Diabetes Care 17(2): 152.
248
Tanamas, S., Magliano, D., Lynch, V., Sethi, P., Willenberg, L., Polkinghorne, K.,
Chadban, S., Dunstan, D. and Shaw, J. (2013). " AusDiab 2012: The Australian
diabetes, obesity and lifestyle study " Baker IDI: Heart and Diabetes Institute.
Tarray, R., Saleem, S., Afroze, D., Yousuf, I., Gulnar, A., Laway, B. and Verma, S.
(2014). "Role of insulin resistance in essential hypertension." Cardiovascular
Endocrinology & Metabolism 3(4).
Tenenbaum, A., Adler, Y., Boyko, V., Tenenbaum, H., Fisman, E. Z., Tanne, D.,
Lapidot, M., Schwammenthal, E., Feinberg, M. S., Matas, Z., Motro, M. and Behar,
S. (2007). "Insulin resistance is associated with increased risk of major
cardiovascular events in patients with preexisting coronary artery disease." American
Heart Journal 153(4): 559-565.
Thiruvoipati, T., Kielhorn, C. E. and Armstrong, E. J. (2015). "Peripheral artery
disease in patients with diabetes: Epidemiology, mechanisms, and outcomes." World
Journal of Diabetes 6(7): 961-969.
Tofthagen, C., Visovsky, C. and Berry, D. L. (2012). "Strength and balance training
for adults with peripheral neuropathy and high risk of fall: Current evidence and
implications for future research." Oncology Nursing Forum 39(5): E416-424.
Tomasik, J., Lago, S. G., Vázquez-Bourgon, J., Papiol, S., Suárez-Pinilla, P.,
Crespo-Facorro, B. and Bahn, S. (2019). "Association of insulin resistance with
schizophrenia polygenic risk score and response to antipsychotic treatment." JAMA
Psychiatry 76(8): 864-867.
Tuomilehto, J., Lindström, J., Eriksson, J. G., Valle, T. T., Hämäläinen, H., Ilanne-
Parikka, P., Keinänen-Kiukaanniemi, S., Laakso, M., Louheranta, A., Rastas, M.,
Salminen, V., Aunola, S., Cepaitis, Z., Moltchanov, V., Hakumäki, M., Mannelin, M.,
Martikkala, V., Sundvall, J. and Uusitupa, M. (2001). "Prevention of type 2 diabetes
249
mellitus by changes in lifestyle among subjects with impaired glucose tolerance."
New England Journal of Medicine 344(18): 1343-1350.
Umpierre, D., Ribeiro, P. A. B., Kramer, C. K., Leitão, C. B., Zucatti, A. T. N.,
Azevedo, M. J., Gross, J. L., Ribeiro, J. P. and Schaan, B. D. (2011). "Physical
activity advice only or structured exercise training and association with HbA1c levels
in type 2 diabetes: A systematic review and meta-analysis." Journal of the American
Medical Association 305(17): 1790-1799.
Umpierre, D., Ribeiro, P. A. B., Schaan, B. D. and Ribeiro, J. P. (2013). "Volume of
supervised exercise training impacts glycaemic control in patients with type 2
diabetes: A systematic review with meta-regression analysis." Diabetologia 56(2):
242-251.
Veritas Health Innovation Covidence systematic review software. Melbourne,
Australia: www.covidence.org.
Villareal, D. T., Chode, S., Parimi, N., Sinacore, D. R., Hilton, T., Armamento-
Villareal, R., Napoli, N., Qualls, C. and Shah, K. (2011). "Weight loss, exercise, or
both and physical function in obese older adults." The New England Journal of
Medicine 364(13): 1218-1229.
Wang, W. and Lo, A. C. Y. (2018). "Diabetic retinopathy: Pathophysiology and
treatments." International Journal of Molecular Sciences 19(6): 1816.
Weinheimer, E. M., Sands, L. P. and Campbell, W. W. (2010). "A systematic review
of the separate and combined effects of energy restriction and exercise on fat-free
mass in middle-aged and older adults: implications for sarcopenic obesity." Nutrition
Reviews 68(7): 375-388.
Weintraub, S., Dikmen, S. S., Heaton, R. K., Tulsky, D. S., Zelazo, P. D., Bauer, P.
J., Carlozzi, N. E., Slotkin, J., Blitz, D., Wallner-Allen, K., Fox, N. A., Beaumont, J. L.,

250
Mungas, D., Nowinski, C. J., Richler, J., Deocampo, J. A., Anderson, J. E., Manly, J.
J., Borosh, B., Havlik, R., Conway, K., Edwards, E., Freund, L., King, J. W., Moy, C.,
Witt, E. and Gershon, R. C. (2013). "Cognition assessment using the NIH Toolbox."
Neurology 80(11 Suppl 3): S54-S64.
Wewege, M. A., Thom, J. M., Rye, K. A. and Parmenter, B. J. (2018). "Aerobic,
resistance or combined training: A systematic review and meta-analysis of exercise
to reduce cardiovascular risk in adults with metabolic syndrome." Atherosclerosis
274: 162-171.
Wilcox, G. (2005). "Insulin and insulin resistance." The Clinical Biochemist Reviews
26(2): 19-39.
World Health Organization (2008). "The global burden of disease: 2004 update."
World Health Organization (2017). Depression and other common mental disorders:
global health estimates. Geneva, World Health Organization.
Wu, J., Kraja, A. T., Oberman, A., Lewis, C. E., Ellison, R. C., Arnett, D. K., Heiss,
G., Lalouel, J.-M., Turner, S. T., Hunt, S. C., Province, M. A. and Rao, D. C. (2005).
"A summary of the effects of antihypertensive medications on measured blood
pressure." American Journal of Hypertension 18(7): 935-942.
Yaribeygi, H., Maleki, M., Sathyapalan, T., Jamialahmadi, T. and Sahebkar, A.
(2021). "Pathophysiology of physical inactivity-dependent insulin resistance: A
theoretical mechanistic review emphasizing clinical evidence." Journal of Diabetes
Research 2021: 7796727-7796727.
Yeung, S. S. Y., Reijnierse, E. M., Pham, V. K., Trappenburg, M. C., Lim, W. K.,
Meskers, C. G. M. and Maier, A. B. (2019). "Sarcopenia and its association with falls
and fractures in older adults: A systematic review and meta-analysis." Journal of
Cachexia, Sarcopenia and Muscle 10(3): 485-500.

251
Yin, J. and Dishman, R. K. (2014). "The effect of Tai Chi and Qigong practice on
depression and anxiety symptoms: A systematic review and meta-regression
analysis of randomized controlled trials." Mental Health and Physical Activity 7(3):
135-146.
Yki-Järvinen, H. (2004). "Thiazolidinediones." N Engl J Med 351(11): 1106-1118.
Yokoyama, K., Yamada, T., Mitani, H., Yamada, S., Pu, S., Yamanashi, T.,
Matsumura, H., Nakagome, K. and Kaneko, K. (2015). "Relationship between
hypothalamic–pituitary–adrenal axis dysregulation and insulin resistance in elderly
patients with depression." Psychiatry Research 226(2): 494-498.
Yu, H. and Chen, Z.-y. (2011). "The role of BDNF in depression on the basis of its
location in the neural circuitry." Acta Pharmacologica Sinica 32(1): 3-11.
Yucel, H. and Uysal, Ö. (2016). "Pilates-based mat exercises and parameters of
quality of life in women with type 2 diabetes." Iranian Red Crescent Medical Journal
Inpress.
Zafar, J., Bhatti, F., Akhtar, N., Rasheed, U., Bashir, R., Humayun, S., Waheed, A.,
Younus, F., Nazar, M. and Umaimato (2011). "Prevalence and risk factors for
diabetes mellitus in a selected urban population of a city in Punjab." Journal Of
Pakistan Medical Association 61(1): 40-47.

252
Appendices
Appendix 1. Prospero registration for systematic review
Citation
Alexander Bate, Maria Fiatarone Singh, Hulya Sinmaz, Yorgi Mavros. The effect of
exercise interventions on depressive symptoms in individuals with insulin resistance,
metabolic syndrome and type-2 diabetes: a systematic review and meta-analysis of
randomised controlled trials. PROSPERO 2020 CRD42020160903 Available from:
https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020160903
Review question
To examine the effect of exercise interventions in randomised controlled trials on
depressive symptoms in any cohort with insulin resistance, metabolic syndrome or
type-2 diabetes.
Searches
The search strategy will include ‘intervention’ terms and ‘population’ terms, but not
‘outcome terms, so as to acquire papers that may include depression measures as
secondary outcomes.
‘’Population’ terms include: ‘homeo* model assessment’ OR ‘niddm’ OR
‘T2D#’ OR ‘diabetes’ OR ‘homa*’ OR ‘ogtt’ OR ‘glyc#emia’ OR ‘hypoglyc*’ OR
‘hyperglyc*’ OR ‘insulin resist*’ OR ‘syndrome x’ OR ‘metabolic syndrome’
253
Intervention terms will include: ‘martial arts’ OR ‘gymnastics’ OR ‘endurance
training’ OR ‘rowing’ OR ‘group exercise’ OR ‘power training’ OR
‘cardiovascular training’ OR ‘swim*’ OR ‘danc*’ OR ‘water aerobics’ OR ‘aqua
aerobics’ OR ‘boxing’ OR ‘balance training’ OR ‘bicycling’ OR ‘qi gong’ OR
‘pilates’ OR ‘yoga’ OR ‘tai ji’ OR ‘tai chi’ OR ‘jog*’ OR ‘walk*’ OR ‘power
training’ OR ‘nautilus’ OR ‘universal machine’ OR ‘theraband’ OR ‘elastic band’
OR ‘free weights’ OR ‘circuit training’ OR ‘isometric exercise’ OR ‘isometric
training’ OR ‘PRT’ OR ‘resistance activit*’ OR ‘weightlifting’ OR ‘weight training’
OR ‘machine training’ OR ‘bodyweight training’ OR ‘exercise’ OR ‘resistance
training’
Population and intervention searches will be combined with ‘AND’.
The search will include the following databases: MEDLINE, SPORTDiscus, AMED,
CINAHL, PEDro, Embase, and PsycINFO. RSS feeds and email alerts will be
established on these databases, and the updated results will be sorted weekly. In
addition to database searching, the first and last authors on the articles that meet the
inclusion criteria will be author-searched to identify any relevant articles not found by
the database searching. The reference lists of any journal articles meeting the
inclusion criteria, as well as existing reviews of exercise and depression, will also be
searched to identify additional relevant articles for inclusion. No date restrictions will
be applied. Languages to be included are English, Spanish, Portuguese, and
French.
254
Types of study to be included
The review will include randomised controlled trials of human participants
Condition or domain being studied
Depression is a common and serious affective disorder characterized by a state of
low mood and loss of interest in leisure and social activities. It negatively affects the
way a person feels and acts, causing a loss of enjoyment and feelings of sadness. It
may be diagnosed as persistent depressive disorder, dysthymia, or major depressive
disorder (MDD), depending on the number of symptoms experienced and the
persistence of those symptoms. In the case of MDD, a depressive episode is a
period of at least 2 weeks during which there is either a depressed mood or loss of
interest of pleasure in nearly all activities. In addition, four of the seven other
possible depressive symptoms from the diagnostic criteria Diagnostic and Statistical
Manual of Mental Disorders must be present, and must be accompanied by clinically
significant distress or impairment in social, occupational, or other important areas of
functioning. The presence and severity of these symptoms may be assessed using a
number of self-administered and clinician-rated psychometric tools. In this review,
results from such instruments will be used to assess symptom change, but no formal
diagnosis of a depressive order will be required.
Participants/population
Participants to be included may be of any age or sex and are not required to have a
diagnosis of MDD. No restrictions will be placed on whether participants are
receiving current treatment for depression. The diagnosis or rating of depressive

255
symptom severity may be made by a clinician, or by self-report through
questionnaires, as long as a quantified pre- and post-invention assessment is
performed. Studies that include participants with depressive symptoms secondary to
traumatic brain injury, stroke, dementia, or other chronic neurological or medical
diseases will be included and may be subject to separate analysis within the review
if sufficient numbers are retrieved.
Participants must have a diagnosis of insulin resistance, impaired glucose tolerance
(<7.0 mmol/L FBG and 2-hour OGTT level between 7.8 mmol/L and 11.0 mmol/L),
metabolic syndrome or type-2 diabetes, or meet criteria for metabolic syndrome set
by either the International Diabetes Federation,17 World Health Organization,19 the
European Group for the study of Insulin Resistance,20 or the NCEP – III ATP21 at the
time of publication. Participants with type-2 diabetes may have a formal diagnosis, or
blood test results of HbA1c ≥ 6.5%, fasting blood glucose ≥ 7.0 mmol/L, or 2-hour
OGTT result of ≥ 11.1 mmol/L.
Intervention(s), exposure(s)
The intervention must be a delivered in a form of structured and repeated exercise,
so that it may be differentiated from incidental increases in physical activity, or single
bouts of exercise. The intervention or exposure may be fully or partially supervised
or unsupervised. An intervention is defined as repeated bouts of exercise ?1
days/week, lasting at least two weeks. Exposures shorter than this (i.e., less than 2
sessions) will be defined as acute bout studies and not included in the review.

256
Comparator(s)/control
Comparison groups may include no contact, no treatment, usual care, waiting list,
attention control, advice, placebo, or alternative exercise modality (e.g., aerobic vs.
resistance training), lower-intensity or sham exercise, or the use of other active
treatments including by not limited to medication or cognitive behavioural therapy, for
example.
Context
No other limitations – may include inpatient or outpatient, lab-based, home-based,
community-based, and university trials.
Type of publication: Studies will be peer-reviewed full-length articles with a full-text
available and may include published or unpublished thesis chapters. For abstracts,
authors will be contacted to see if the abstract has progressed to full-text publication,
if it has not, these will not be included.
Main outcome(s)
1. Any validated objective or subjective tool to assess symptoms of depression.
2. Remission of depression as defined by DSM criteria at the time of publication.
3. Treatments utilised including use of antidepressants and other psychotropic
medications such as anxiolytics, anti-psychotics, mood stabilisers,
insomniacs, supplement/herbal or nutritional product used for depression
symptoms, use of psychological services or interventions, other counselling,
cognitive behavioural therapy, mindfulness training, meditation, acupuncture,
257
hypnosis, or any other treatment used for its purported effects on depressive
symptoms.
4. Occurrence of suicidal ideation, suicide, self-harm and depression-related
hospitalisation.
Measures of effect
Objective or subjective assessment of depressive symptoms at baseline and the pre-
specified endpoint. In the case where only interim data are available, then this would
be used as the primary outcome. Authors of the paper will be contacted to confirm
no other outcome data exist.
Additional outcome(s)
Secondary outcomes will include but not be limited to: Objective or subjective
symptoms of depression, or rates of remission/recovery or relapse/recurrence that
are measured beyond the primary endpoint of the study. Other secondary outcomes
include exercise program adherence and adverse events; muscle strength; aerobic
fitness; exercise volume and duration; metabolic profile encompassing glucose
homeostasis, lipids, blood pressure, waist circumference, and body composition; co-
morbidities and medications; smoking, alcohol and recreational drug consumption;
sleep quality and quantity (objective or subjective, cognition; and psychological well-
being or positive mood state.
Measures of effect
Objective or subjective assessment of secondary outcomes at baseline and the pre-
specified endpoint. In the case where only interim data are available, then this would
258
be used as the primary outcome. Authors of the paper will be contacted to confirm
no other outcome data exist.
Data extraction (selection and coding)
AB will review the resulting papers (title and abstract) to identify potentially relevant
studies. The remaining papers will be retrieved and assessed by two reviewers: AB
and HS. Disagreements will be resolved by consensus with other reviewers YM and
MFS to determine final eligibility.
AB will extract data into pre-designed templates approved by consensus based on
aforementioned outcomes, including: exercise frequency, intensity (as defined by
current ACSM guidelines), time, and modality; equipment utilised, level of
supervision, behavioural tools or theories used, if training was progressed; what was
prescribed vs. what was achieved (e.g. , actual intensity); program duration; age;
sex; diagnosis of MDD or other psychiatric disorder and how it was made;
comorbidities; health status; medication usage; and other treatments.
Risk of bias (quality) assessment
Quality assessment of eligible trials will be independently rated on the 15-item
quality rating TESTEX scale. The scale will assess study design quality from criteria
1-5, and study reporting from criteria 6-12. This will allow a maximum score out of
15, as some criteria award multiple points. Since supervision is an important
component of exercise, an additional quality item (“Exercise supervised: yes/no”) will
be included, but not used to calculate the final TESTEX score. Interventions will be
259
considered supervised if at least 50% of the exercise sessions were supervised in
person.
Strategy for data synthesis
Baseline and post-intervention outcome measures will be extracted. Participant,
intervention, and outcome data will be extracted from text and tables, or figures if
required. Standard error (SE) and 95% confidence intervals (CI) will be converted to
standard deviation (SD) as described by the Cochrane Handbook. Effect sizes (ESs)
will be extracted from text where available or otherwise calculated using the reported
means and pooled baseline SDs and adjusted for small sample bias (Hedges' g ES).
If studies report median and range or inter-quartile range due to non-parametric
data, then the median will be substituted for the mean when the sample size
exceeds 25, and their measures of variability were converted to standard deviation
as per Hozo et al. (2005). Meta-analyses may be conducted if the data are suitable.
All meta-analyses will use a random effects model and 95% CI and will compare
exercise with against a comparison at the end of intervention. As depression is
commonly measured using multiple tools in the same trial, it is expected that we find
a considerable number of dependent effect sizes (correlated dependency). If this is
the case, then meta-analysis and meta-regression using robust variance estimation
of effect sizes may be performed. Sources of heterogeneity will be explored by
stratifying cohorts based on diagnosis (metabolic syndrome or type 2 diabetes), or
other characteristics such age, sex, exercise intensity and frequency etc. Meta-
regression will be performed between changes in depressive symptoms and
changes in metabolic parameters such as blood glucose and HbA1c. Effect sizes
(ESs) will be interpreted according to Cohen’s scale where 0.2 represents a 'small'
260
effect size, 0.5 represents a 'medium' effect size, and 0.8 represents a 'large' effect
size.
Analysis of subgroups or subsets
Moderator analyses will be conducted using meta-analytic analogues of ANOVA and
regression, to assess the potential influence of key cohort or intervention
characteristics such as age, sex, and MDD diagnosis, baseline depression severity,
use of anti-depressant medication or frequency, intensity, duration or supervision of
the exercise program.
Contact details for further information
Alexander Bate
Organisational affiliation of the review
The University of Sydney
https://sydney.edu.au/
Review team members and their organisational affiliations
Mr Alexander Bate. The University of Sydney
Professor Maria Fiatarone Singh. The University of Sydney
Dr Yorgi Mavros. The University of Sydney
Type and method of review
Meta-analysis, Systematic review

261
Anticipated or actual start date
01 November 2019
Anticipated completion date
01 May 2020
Funding sources/sponsors
None
Conflicts of interest
None
Language
English
Country
Australia
Stage of review
Review Ongoing
Subject index terms status
Subject indexing assigned by CRD
Subject index terms
MeSH headings have not been applied to this record
Date of registration in PROSPERO
28 April 2020
Date of first submission
13 February 2020
Details of any existing review of the same topic by the same authors
Changed topic to include all exercise types from previous unpublished review of only resistance training interventions.
Stage of review at time of this submission Preliminary searches Yes Yes
Piloting of the study selection process Yes No
Formal screening of search results against eligibility criteria Yes No
262
Data extraction No No
Risk of bias (quality) assessment No No
Data analysis No No
The record owner confirms that the information they have supplied for this
submission is accurate and complete and they understand that deliberate provision
of inaccurate information or omission of data may be construed as scientific
misconduct.
The record owner confirms that they will update the status of the review when it is
completed and will add publication details in due course.
Versions
28 April 2020
263
Appendix 2. ANZCTR registration for PRT Medic study
Trial ID
ACTRN12617000400369
Date registered
17 March 2017
Health condition
Major Depressive Disorder, Metabolic Syndrome, Type 2 Diabetes
Recruitment countries
Australia
Recruitment site location(s) (State)
New South Wales
Recruitment status
Recruiting
Anticipated date of first participant enrolment
01 July 2017
264
Ethics application status
Approved
Brief summary
Individuals with depression and metabolic syndrome are 6.6 times more likely to develop
type 2 diabetes within 5 years compared to individuals without either condition. Thus, early,
robust and targeted interventions are warranted to alleviate symptoms of depression and
improve the metabolic health of these at-risk individuals.
The primary aims of this project are to determine the effects of progressive resistance training
on insulin resistance (measured using the Homeostatic Model of Assessment-2) and
depressive symptoms [assessor-rated Hamilton Depression Rating Scale (HDRS), Patient
Health Questionnaire (PHQ-9) and Center for Epidemiologic Studies Depression Scale (CES-
D) in adults with co-existing metabolic syndrome and major depressive disorder. Participants
will be randomized to receive either progressive resistance training (PRT), 3 days per week
for 12 weeks in addition to usual care from their GP, or referred to their GP for usual care.
Participants randomised to the control intervention will be referred to their GP for
management of their depression and metabolic syndrome. Blinded assessments will occur
pre, and post intervention.
This will be the first trial of PRT for individuals with co-existing major depressive disorder,
metabolic syndrome and impaired glucose tolerance, and only the 5th trial of PRT in clinical
depression.
265
Primary Hypotheses
1. 12 weeks of PRT will significantly reduce insulin resistance, measured via Homeostatic
Model of Assessment-2 (HOMA2-IR) compared to controls referred for General
Practitioner (GP) care.
2. 12 weeks of PRT will significantly improve therapist-rated depressive symptoms
[Hamilton Depression Rating Scale (HDRS)] as well as self-rated symptoms [Patient
Health Questionnaire (PHQ-9)] and Center for Epidemiologic Studies Depression Scale
(CES-D) compared to controls referred for GP care.
Secondary Hypotheses
1. 12 weeks of PRT will significantly reduce glucose and insulin area under the curve during
an oral glucose tolerance test (OGTT) compared to controls referred for GP care.
2. 12 weeks of PRT will significantly reduce glycated haemoglobin (HbA1c) compared to
controls referred for GP care.
3. 12 weeks of PRT will significantly increase lean body mass (LBM) and decrease central
adiposity compared to controls referred for GP care.
4. 12 weeks of PRT sill significantly improve central haemodynamics compared to controls
referred for GP care.
5. Reductions in depressive symptoms will be associated with reductions in HOMA2-IR.
6. Improvements in body composition (increases in lean tissue and reductions in central
adiposity), and reductions in systemic inflammation and serum cortisol will be
independently associated with improvements in metabolic profile and depressive
symptoms.
Eligibility
Key inclusion criteria
1. Major Depressive Disorder according to DSM 5 criteria
266
• If not receiving any treatment; PHQ-9 of 10 or higher (moderate depression)
• If receiving treatment, PHQ-9 of 5 or higher (mild depression)
2. Metabolic syndrome according to IDF criteria
• Central obesity (Waist circumference Men; greater than or equal to 94 cm men.
Women; greater than or equal to 80 cm) and any 2 of the following:
- Raised triglycerides (150 mg/dL (1.7 mmol/L) or higher, or specific treatment
for this lipid abnormality)
- Low HDL cholesterol (Less than 40 mg/dL (1.03 mmol/L) in men and less
than 50 mg/dL (1.29 mmol/L) in women or specific treatment for this lipid
abnormality
- Hypertension (systolic BP of 130 or higher, or diastolic BP of 85 mm Hg or
higher, or treatment of previously diagnosed hypertension)
- High fasting plasma glucose ((FPG) of 100 mg/dL (5.6 mmol/L) or higher.
3. At least 40 years of age
4. Not on oral hypoglycaemics or insulin therapy
5. No diagnosis of type 2 diabetes, or not found to have type 2 diabetes during the
screening process
6. Sedentary - less than 150 minutes per week of structured moderate or vigorous
physical activity.
7. No terminal or rapidly progressing illness, or condition that precludes participation in
progressive resistance training
Minimum age
40 Years
267
Maximum age
No limit
Gender
Both males and females
Key exclusion criteria
Type 2 diabetes or use of oral hypoglycaemic medication or insulin
Suicide ideation
Illegal drug use
Alcohol dependence/abuse (3 or 4 on CAGE questionnaire)
Substance abuse disorder
Contact details and further information
Primary Sponsor
Type: Individual
Name: Dr Yorgi Mavros
Address: K214
University of Sydney, Cumberland Campus
75 East Street,
Lidcombe NSW 2141
Country: Australia
Contact person for information and recruitment
Dr Yorgi Mavros
University of Sydney, Cumberland Campus
K214, 75 East Street
Lidcombe NSW 2141
Australia
+61 02 9351 9279
268
Appendix 3. HREC approval for PRT Medic study
269
270
Related Documents