Mood & Anxiety Disorders in Primary Care: A Review Arun V. Ravindran, MB, MSc, PhD, FRCPC, FRCPsych Professor and Director, Global Mental Health and Office of Fellowship Training, Department of Psychiatry; Graduate Faculty, Department of Psychology and Institute of Medical Sciences; University of Toronto Chief, Division of Mood and Anxiety Disorders, Centre for Addiction and Mental Health Toronto, Ontario, Canada 1

Mood & Anxiety Disorders in Primary Care: A Review Arun V. Ravindran, MB, MSc, PhD, FRCPC, FRCPsych Professor and Director, Global Mental Health and Office.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Mood & Anxiety Disorders in Primary Care: A ReviewArun V. Ravindran, MB, MSc, PhD, FRCPC, FRCPsych
Professor and Director, Global Mental Health and Office of Fellowship Training, Department of Psychiatry; Graduate Faculty, Department of Psychology and Institute of Medical Sciences; University of TorontoChief, Division of Mood and Anxiety Disorders, Centre for Addiction and Mental HealthToronto, Ontario, Canada
1

Anxiety Disorders
2
Anxiety
What is Anxiety?• Diffuse, unpleasant, vague sense of
apprehension often accompanied by autonomic symptoms
When do you treat Anxiety?• “Anxiety symptoms exist on a continuum and milder forms of
recent onset often remit without treatment.”• Need for treatment determined by:
• Severity and persistence of symptoms• Presence of co-morbidity• Disability + Impaired function• Impact on social function 3

Generalized anxiety disorder
Depression
Social anxiety disorder
Panic disorder
Obsessive-compulsive disorder
Posttraumatic stress disorder
The Spectrum of Anxiety Disorders
4

Co-morbidity in Anxiety Disorders
Anxiety Disorders
Mood Disorders
Substance Use
Disorders
Medical Conditions
Somatoform Disorders
5

Anxiety Disorders – DSM-IV – Fear vs. Distress Disorders
Panic DisorderAgoraphobia
Specific PhobiaSocial Phobia
PTSD
ASD
OCD
GAD AD / GMC / SU / NOS6

Key Fears in Anxiety Disorders
• PD/A – Dying, going crazy or losing control• SP – Harm from an external object or situation• SAD – Humiliation or embarrassment• GAD – Future events involving real life concerns• PTSD – Re-experiencing trauma in memories/dreams• OCD – Harm, uncertainty, uncontrollable actions
7

Epidemiology of Anxiety Disorders
Disorder Life Time Prevalence
Panic Disorder 2 – 5%Specific Phobias 1 – 19%Agoraphobia 0.2 – 5%Social Phobia 5 – 12%General Anxiety Disorder 1 – 6%Post Traumatic Stress Disorder 2 – 8%Obsessive-Compulsive Disorder 2 – 3%As a group 20-30%
8
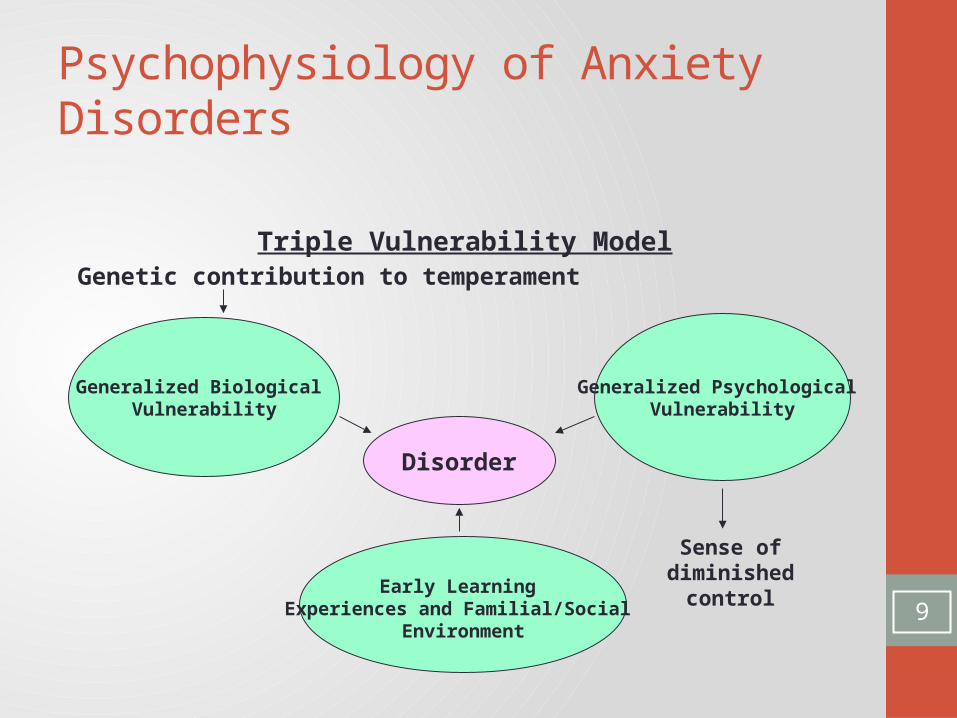
Psychophysiology of Anxiety Disorders
Triple Vulnerability ModelGenetic contribution to temperament
Sense of diminished control
Generalized Biological Vulnerability
Generalized Psychological Vulnerability
Early Learning Experiences and Familial/Social
Environment
Disorder
9
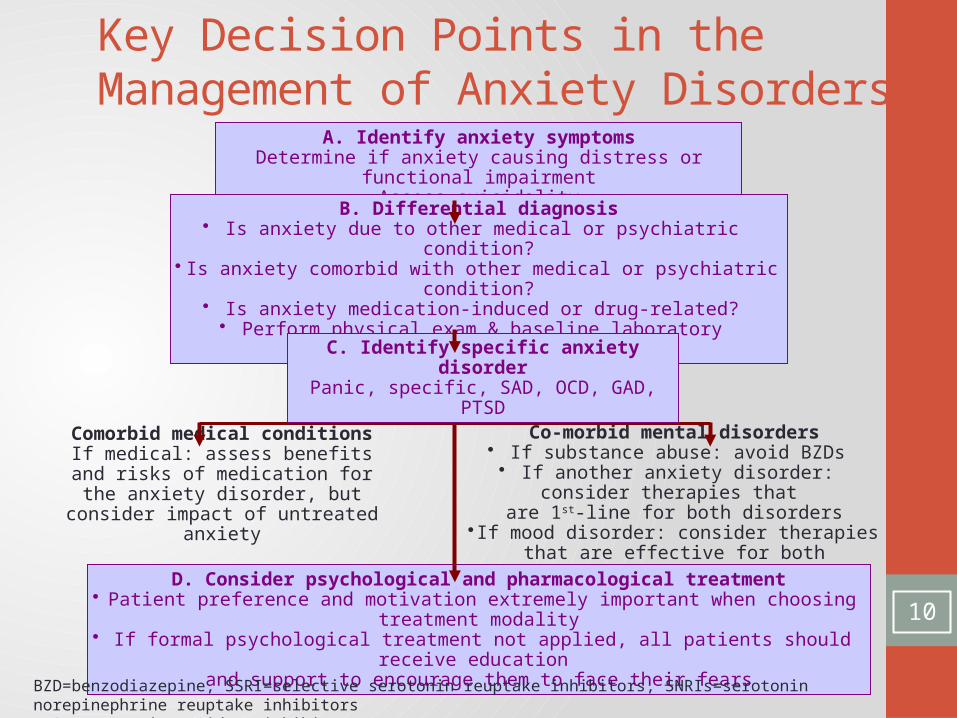
A. Identify anxiety symptomsDetermine if anxiety causing distress or functional impairment
Assess suicidality
Co-morbid mental disorders• If substance abuse: avoid BZDs
• If another anxiety disorder: consider therapies that are 1st-line for both disorders
• If mood disorder: consider therapies that are effective for both disorders, also refer to depression or
bipolar disorder guidelines
Comorbid medical conditionsIf medical: assess benefits and risks of
medication for the anxiety disorder, but consider impact of untreated anxiety
B. Differential diagnosis• Is anxiety due to other medical or psychiatric condition?
• Is anxiety comorbid with other medical or psychiatric condition?• Is anxiety medication-induced or drug-related?
• Perform physical exam & baseline laboratory assessment
D. Consider psychological and pharmacological treatment• Patient preference and motivation extremely important when choosing treatment modality
• If formal psychological treatment not applied, all patients should receive education and support to encourage them to face their fears
BZD=benzodiazepine, SSRI=selective serotonin reuptake inhibitors, SNRIs=serotonin norepinephrine reuptake inhibitorsMAOIs=monoamine oxidase inhibitors
C. Identify specific anxiety disorderPanic, specific, SAD, OCD, GAD, PTSD
Key Decision Points in the Management of Anxiety Disorders
10

Treatment of Anxiety Disorders in Primary Care: General Principles• Screening
• Beck Anxiety Inventory (BAI; 21 items) • Interventions
• Pharmacotherapy (mild to moderate)• CBT (mild to moderate)• Antidepressants + CBT (moderate to severe)
• Maintain antidepressants + CBT boosters – 1-2 years
11

The “CBT Package” – The Proven Intervention• Psychoeducation• Monitoring/early cue detection• Applied relaxation• Imaginal and in vivo exposure• Coping skills rehearsal• Cognitive restructuring
12

Case History
Jenny, 56-year-old accountant, married with three grown children
• Describes herself as a ‘worrier’• Has worried more “for the past 1 year” about her children’s
health, finances, marital relationship, the future
Jenny is likely suffering from: Clinical Depression Generalized Anxiety Disorder Adjustment Disorder Alcohol dependence
What further information is useful in her diagnosis?13
Generalized Anxiety Disorder (GAD): The Facts“Inappropriate and/or extreme worry with multiple somatic
anxiety”- Restlessness- Poor concentration- Fatigue- Irritability- Sleep difficulties- Tension
• 5% of the general population• Onset in adolescence, disability and chronic course• Comorbidity and vulnerability to MDD
14

Treatment of GAD
15
• Pharmacotherapy• Antidepressants• Beta blockers• Benzodiazepines• Anticonvulsants• Buspirone
• Psychotherapy• CBT
• Recent advances• Focus on “worries”• Mindfulness and acceptance
Case History
Sam, 24-year-old computer programmer, single and living on his own
• 1 year history of physical symptoms• Has seen several physicians – multiple investigations• Convinced that he has heart disease and believes that it is
being missed
Which of the following is most likely? Hypothyroidism Panic Disorder Schizophrenia Incompetent Physicians
16

Panic Disorder and Panic Disorder with Agoraphobia (PD/A)“Characterized by panic attacks and avoidance behaviour”• Prevalence
• Lifetime 3-5%• Specialty clinics 10-60%
• Impaired function• High rates of utilization• Early evidence of anxiety• Common medical/psychiatric co-morbidity
17

PD/A Diagnosis (DSM-IV)
Diagnostic criteria: recurrent panic attacks
18
Cognitive symptoms
Physical symptoms
4 or more of the following: Dyspnea or the sensation of being smothered Depersonalization or derealization Fear of going crazy or of losing self-control Fear of dying Palpitations or tachycardia Sweating Trembling or shaking Feeling of choking Chest pain or discomfort Nausea or abdominal upset Dizziness, feeling of unsteadiness or faintness Numbness or tingling sensation Flushes or chills

Billy Crystal and Robert De Niro in Analyze This – Panic Disorder
19

Treatment of PD/A• Pharmacotherapy
• Antidepressants• Benzodiazepines
• Psychotherapy• CBT plus
• Breathing retraining• Relaxation exercises
• Recent advances• Mindfulness based CBT (MBCT)/Mindfulness based stress
reduction (MBSR)• Sensation focused intensive treatment (SFIT)• Virtual reality exposure therapy
20

PD/A: Treatment Outcomes
• CBT vs. pharmacotherapy vs. combination• Similar benefit short-term• CBT better on long term• CBT useful• Sequential PT + CBT – new trend
• In General• Low remission rate – 20-50%• High rates of relapse – 25-85% on discontinuation
21Good initial response – less probability of relapse

Case HistoryBrian, 30-year-old graduate student, engaged to be
married in 6 months• Is very anxious and apprehensive about the event• “I don’t like being looked at”, “I think people will laugh at
how I look or what I say”• History of shyness, being ‘quiet’
What further information would be useful for diagnosis?What is the likely diagnoses?
22

Social Phobia/Social Anxiety Disorder (SAD)
23
Barbra Streisand Donny Osmond Carly Simon

SAD: Signs and Symptoms
Cognitive:• Fear of scrutiny, humiliation and
embarrassment, • Exposure promotes anxiety
Physical:• Blushing, sweating, tremor
Behavioural: • Avoidance and anticipatory anxiety in
social/performance situations• Good Insight
24

Nicholas Cage in Adaptation – Social Phobia
25
Treatment of SAD
Pharmacotherapy vs. CBT vs. combination
Goals:
• Improve cognitive and physical symptoms
• Reduce anticipatory anxiety and avoidance
• Treat comorbid conditions
• Improve functioning
Methods
• Psychoeducation
• CBT plus• Social skills training
• Exposure therapy
26
27

Performance-Specific Anxiety• SAD vs. shyness vs. performance anxiety• Proposed overlap with non-generalized SAD• Evidence for benefit with propranolol (RCTs)
• Surgical patients and surgeons• Dental patients• Medical students
• Benzodiazepines – decrease anticipatory anxiety but may impair performance
28

Specific Phobias
Specific phobia is excessive or irrational fear of object or situation, and is usually associated with avoidance of feared object• Lifetime prevalence: 12.5%• Median age of onset: 7 years
Common Phobias: animal and blood-injection, claustrophobia, heights
Treatment• Pharmacotherapy: Difficult to use and unproven• Psychotherapy: In vivo and virtual exposure
29

Case HistorySonya – 33 year old housewife brought against her wishes by her
husband• Vague complaints – 3-4 years• “I don’t understand what is wrong with her” – husband• Superstitious about leaving the house without knocking on the
door posts. “It’s bad luck if I don’t.”• Spends half an hour each night checking and double-checking
that the doors and windows are locked and all kitchen appliances are turned off
• Not able to cope with housework because she spends too much time on one task. “I’m a perfectionist.”
What would your diagnosis be? 30
Obsessive Compulsive Disorder (OCD)
• Obsessions and/or compulsions• Recurrent, persistent ideas, thoughts, impulses or images• Repetitive, purposeful and intentional behaviours that are performed
in response to an obsession
• Repetitive, unpleasant and ego dystonic + resisted• Excessive/unreasonable• Marked distress and impact on functioning • Affects 2-3 % of the population, with onset in teens
31

OCD: Common Obsessions and Compulsions
• Obsessions• Repetitive thoughts about
contamination• Repetitive doubts• Intense need for
orderliness and symmetry• Aggressive impulses• Repeated sexual imagery
• Compulsions• Behaviours
• Hand washing• Ordering• Checking• Demanding reassurance• Repeating actions
• Mental Acts• Counting• Repeating words silently
32

Jack Nicholson in As Good As It Gets - OCD
33

Treatment of OCD
• Pharmacotherapy• Serotonergic agents• AAPs• Combination
• Psychotherapy• CBT with focus on
• Exposure and response prevention• Cognitive interventions
• Poorer outcomes in• Males• Early onset• Delayed treatment
34

Case HistoryGoran, a 47-year-old parking attendant• Complains of feeling tired and ‘down’ for the past 5-6 months,
since being robbed and beaten up at work last year• Has difficulty sleeping due to nightmares, is ‘jumpy’ and
irritable• Feels distant from family and friends• Constant sense of inner and physical tension
Do you think Goran is suffering from: Fibromyalgia Fatigue Post traumatic stress Overwork
35

PTSD: Key Features
• Exposure to threat to life or physical integrity AND
• Emotional reaction of fear, helplessness or horror
36
+
Persistent intrusive reexperience of the event Avoidance of trauma-associated stimuli and numbing – emotional and behavioural withdrawal Persistent symptoms of increased arousal Duration 1 month to years Prevalence 3-4 % High risk of suicide

Damian Lewis in Band of Brothers - PTSD
37

PTSD - TreatmentBoth Pharmacotherapy and Psychotherapy are useful
Pharmacotherapy• Antidepressants and atypical antipsychotics
Psychotherapy• Trauma focused therapies best results• CBT, exposure therapy beneficial• Less effective - IPT, psychodynamic therapy, supportive
therapy• Different types of trauma may respond to different
psychotherapies, benefit across subtypes 38

Acute Stress Disorder
Follows within 1 month acute exposure to threat and lasts few days to 4 weeks
Intervention: Brief and immediateFocus on high risk population
39
Components: • Information Education
• Psychological support
• Crisis intervention
• “Emotional first aid”
Does immediate intervention prevent PTSD?
Anxiety Disorders: Primary Care Perspectives• Often present with somatic symptoms or complaints related to
co-morbid conditions• High utilizers of primary care• May need to treat multiple anxiety disorders• Education and CBT-based brief interventions useful• Deal with barriers to care
40

Unipolar Depression
41

A Case History
Maria, a 47-year-old married lady, reports feeling ‘not her usual self’ for the past 6-8 months• She reports feeling both sad and anxious • She has difficulty sleeping and is always tired• Her appetite has decreased and she has lost 15
lbs. in the past 6 months• Her brother died in a car accident about 1 year
ago. She feels guilty about an argument they had just before, and thinks about it a lot.
What is your diagnosis?42

Mood/Affective Disorders
Definition: Mental illnesses presenting with altered mood/affect as the primary symptom
• Affect: External expression of an internal state (i.e. mood)
• Affect is more transient, mood is more sustained• Two broad syndromes of mood disorders
• Depression• Mania
43
How Common Are Mood Disorders and What is Their Disease Burden?• Life time prevalence
• Unipolar depression 8-20% • Bipolar disorder 1%
• WHO: Depression is the leading cause of disability• Impact on:
• Quality of life• Impaired function (occupational, social)• Suicide• Physical health
44

What Causes Mood Disorders?• Genetic vulnerability• Social and environmental factors
• Life stressors• Early childhood experiences• Social determinants
• Neurobiological factors• Neurotransmitter/neurohormonal challenges• Neural circuitry
Usually a multi-factorial etiology
45
Defining a Depressive Disorder (DSM)
• Clinically significant behavioural or psychological syndrome, associated with• Distress/disability• Increased risk of death/pain
• Not simply• Lowered mood• Response to loss• Maladaptive reaction to stress
• Two key forms• Major depressive disorder (MDD)• Dysthymic disorder (DD)/Persistent depressive disorder (DSM5)
46

Depression is Complex, Multidimensional
47
APA. DSM-IV-TR; 2000:352,356.
Physical Symptoms• Lack of energy• Decreased
concentration• Change in appetite• Change in sleep• Change in
psychomotor skills
Associated Symptoms• Brooding• Obsessive rumination• Irritability• Excessive worry over
physical health• Pain• Tearfulness• Anxiety or phobias
Emotional Symptoms• Feelings of guilt• Suicidal• Lack of interest• Sadness

Nicole Kidman in The Hours - Depression
48

What Are the Important Subtypes of MDD and DD?• Chronic depression• Melancholic depression• Atypical depression• Psychotic depression• Postpartum depression• Seasonal affective disorder
49

How Do Patients with Depression Present in Primary Care?• Less than 20% seek help from family physicians• Only 50% are recognized as depressed• 2/3 present in practice with somatic symptoms only• Common screening tools for primary care
• Brief Hamilton Depression Rating Scale (HDRS; 7 items)• Beck Depression Inventory (BDI-II; 21 items) • Patient Health Questionnaire (depression only) (PHQ-9; 9 items)
• Screening tools are specially useful in high risk populations
50

High Risk Groups and Symptomatic Presentation of MDDHigh Risk Clinical Groups High Risk Symptom Presentations
Past history of depression Unexplained physical symptoms
Family history of depression Pain
Psychosocial adversity Fatigue
High users of the medical system Insomnia
Chronic medical conditions Anxiety
Other psychiatric conditions Substance abuse
Times of hormonal challenge
51
Patten et al., 2009; J Affect Disord.
Managing Depression in Primary Care
• Assessment• Suicide risk• Physical health• Psychosocial issues• Psychiatric morbidity
• Management: “Stepped care approach”• Watchful waiting• Guided self-management• Brief psychological/pharmacological interventions• Referral to specialists
• Determine diagnosis and point in continuum of care52

What Are the Phases of Treatment for Depression and Their Goals?• Acute
• Target goals• Remission• Restoration of function
• Outcome measures• Maintenance
• Resolve residual symptoms• Treat co-morbidities• Prevent recurrence
Use chronic disease management model53

What Are the Effective Interventions for Depression?• Pharmacotherapy
• Antidepressant agents• Older agents – TCAs, MAOIs• Newer agents – SSRIs, SNRIs, atypical antipsychotics, novel agents
• Psychological therapies• Cognitive Behaviour Therapy (CBT)• Interpersonal Therapy (IPT)• Other modalities, supportive therapy
• Combination: Medication + psychotherapy• Psychosocial interventions• Neurostimulation
• Electroconvulsive Therapy (ECT)• Rapid transcranial magnetic therapy (rTMS)• Investigational modalities
• Chronic disease management model
54
Psychotherapy: Best Modalities• Cognitive behaviour therapy (CBT)
• Basis: Thoughts, emotions and behaviours are inter-related• Focus on dispelling cognitive misperceptions of self, others and
surroundings and modifying maladaptive emotional and behavioural responses
• Interpersonal therapy (IPT)• Basis: Problematic interpersonal relationships may contribute to
depressive onset and maintenance• Focus on at least 1 key area: Role transitions, Interpersonal role
disputes, Grief, Interpersonal deficits• Pick the most appropriate form based on the need• Both forms effective in acute and maintenance treatment
55

Psychotherapy: Other ModalitiesPsychodynamic psychotherapy Behavioural activationBasis: Psychological dysfunction results from conscious or unconscious conflicts and defense mechanisms
Focus on recognizing the conflict and understanding sources/influences to promote psychological healing
Basis: “Depression is a consequence of compromised environmental sources of positive reinforcement”
Focus on increasing patient activity and rewarding experiences, and de-emphasizing particular cognitions/ mood states
Motivational interviewing Computer/internet/telephone psychotherapy
Basis: Individuals with dysfunctional behaviours wish to change but lack initiative/commitment
Focus on resolving ambivalence, building motivation, and working towards specific, realistic goals to achieve the desired change
CBT, IPT, supportive therapy, etc. in distance delivery formats
Advantages: Immediate help, anonymity, low cost, flexible schedule, ease of access for remote communities
56

Neurostimulation Therapies
ECT rTMS
Induction of a convulsion (seizure) by the application of electrical current to the brain
Application of a magnetic field (1.5-2.5T), delivered through the skull
Indications: Treatment resistance, intolerant of antidepressants, psychotic depression
Indication: Treatment resistance, severe depression
Physical and cognitive side effects Short term side effects: Headache and scalp pain.
Investigational therapies
VNS, DBS and MST
57

How does Depression Affect Physical Health?• Increase the effect of risk factors
• Obesity• Smoking• Cardiovascular• Immune
• Increase the risk of chronicity• Worsen pain disorders• Reduce treatment adherence• Reduce participation in prevention
58

What is the Long-term Outcome of Depressive Disorders?• MDD
• Variable duration• Spontaneous recovery in many• Longer illness poor outcome• Often recurrent• 20% non-recovery and chronic course
• Dysthymia/Persistent depressive disorder• Chronic fluctuating course• Superimposed MDD double depression• Poor function
59

Bipolar Disorder
60

Case History
Susan, a 20-year-old university student, presents with symptom of 2 months’ duration (worsening in last 2 weeks)• Has started many projects, but is easily distracted and does
not complete them – has affected her grades • Is sleeping less (but does not feel tired)• Has been buying unneeded things impulsively from the
internet• Her friends say her mood is unpredictable, and that she gets
overly excited or angry about even little things.
What is your assessment of this patient?61

Symptom Overlap: The Complexity of Mood Disorders
62
Unipolar Depression
Bipolar Mania Bipolar Depression
Treatment Resistant
Depression
Agitated Depression
Mixed State
Psychosis
*All have potential for psychotic presentation/escalation

Bipolar Disorder and Bipolar Spectrum Disorders• BP I: Mania with/without depression• BP II: Depression with hypomania - Recurrent MDE with
clear-cut hypomanic episodes (lasting at least 4 days)• BP Spectrum/ Complex Subtypes
• Mixed states: Mania and depression
• Rapid cycling, Ultra-rapid cycling, Ultradian
• Cyclothymia
• Substance/Antidepressant-induced hypomania
• Prevalence:• Bipolar I Disorder: 1.2-1.6%
• Bipolar II Disorder: 2-6%
• Bipolar Spectrum Disorders: 6.4%
63
Bipolar Disorder: Burden of Disease
• High degree of psychiatric/physical co-morbidity and psychosocial consequences:• Suicidality• Substance abuse• Medical illnesses• Employment and family problems
• Increased mortality than those without bipolar disorder:• 2.5 times more likely to die in 12 months, if untreated
• One of the world’s 10 most disabling conditions• DALYs highest in 14-44 year olds
64
Diagnosing Mania
Mood: Abnormally and persistently elevated, expansive or irritable
Duration: At least one week or requiring admissionPLUS
Three (four if irritable mood) or more of the following:• Grandiosity • More talkative• Flight of ideas• Distractibility• Less need for sleep• More goal-directed activity • Excessive involvement in pleasurable activities
65

Hypomania: PresentationA distinct period of persistently elevated, expansive
or irritable mood, lasting at least 4 days PLUS
Three (four if irritable mood) or more of the following:
• Grandiosity • More talkative• Flight of ideas• Distractibility• Less need for sleep• More goal-directed activity • Excessive involvement in pleasurable activities
More commonly seen in primary care than mania
66

Bradley Cooper in Silver Linings Playbook - Hypomania
67

What are the common presentations of Bipolar I and II Disorder to the Family Physician?Psychological Physical
Depression Alcohol/substance use
Anxiety Sexually transmitted diseases
Sleep difficulties
Fatigue
Poor concentration
Social Other
Marital/relationship problems Episodic impulsivity/risk taking
Financial Suicide attempts
Occupational
68
The Complex Bipolar Patient
69
• Mixed episodes• Both manic and depressive symptoms• comorbid substance use disorders• risk of suicide and psychosis
• Rapid cycling• 4 or more cycles/year with > 8 weeks of well periods• Occurs in Bipolar I and II

The Complex Bipolar Patient: Co-morbidities/Complications
• Anxiety disorders• High co-morbidity (up to 92%)• Risk factor for bipolar disorder• May elevate risk of suicide
• Substance abuse• High rates of co-morbidity vs.
the general population• Higher prevalence of complex
subtypes
• ADHD• Bi-directional relationship• Overlap of symptoms• ADHD as a prodrome
• Personality disorders (cluster B)
• Medical conditions• Obesity• Cardiovascular• Endocrine • Cerebral pathology
• Suicide• 15% suicide rate• 25-50% attempt suicide
in lifetime 70

Bipolar Disorders: Management
Chronic disease management model: Long term, interdisciplinary, education focused and integrated• Bipolar I Disorder
• Emergency management• Acute care/short-term• Mixed/rapid cycling states• Bipolar mania• Bipolar depression
• Bipolar II Disorder• Mainly depression
• Maintenance treatment and prophylaxis71

Issues Specific to Primary Care
• Diagnostic difficulties – screening tools• Patient Health Questionnaire (depression only) (PHQ-9; 9 items)• Mood Disorder Questionnaire (mania only; 17 items)
• Check for “destabilization”/non response to antidepressants • Use antidepressants with caution• Referral for consultation/shared care• Treatment adherence• Risk of suicide /financial difficulties• Medical issues, e.g. obesity, cardiovascular disease• Psychoeducation and support through life transition for patient and
family• Relapse prevention
72

What Interventions are Useful for Bipolar Disorders?• Pharmacotherapy
• Antipsychotics• Mood stabilizers
• Lithium carbonate• Anticonvulsants
• Psychotherapy• Psychoeducation• CBT, IPT• Family interventions• Benefits: Improve adherence and function, early identification of
relapse and suicidal ideation, prevent suicide• Neurostimulation
• ECT73
Bipolar Patients: Baseline Investigations and Monitoring• CBC electrolytes• Fasting lipids and glucose• Liver function levels• TSH + ECG• Urine analysis
Regular monitoring:• The above +• Weight, smoking status and alcohol use• Medication serum levels• Cognitive function 74

75

On a Lighter Note…
76

END
77
Related Documents











