1 1 Mood and Cognition: Options for Treatment Professor Allan Young Director of the Centre for Affective Disorders Institute of Psychiatry, Psychology and Neuroscience KCL Date of Preparation: February 2015 UK/VOR/1501/0066a

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1 1
Mood and Cognition:
Options for Treatment
Professor Allan Young
Director of the Centre for Affective Disorders
Institute of Psychiatry, Psychology and
Neuroscience
KCL
Date of Preparation: February 2015 UK/VOR/1501/0066a

2
Disclosures
• Employed by King’s College London; Honorary Consultant
Maudsley and Bethlem Hospitals (NHS)
• Paid lectures and advisory boards for all major pharmaceutical companies with
drugs used in affective and related disorders
• No share holdings in pharmaceutical companies
• Lead Investigator for Embolden Study (AZ), BCI Neuroplasticity Study, and
Aripiprazole Mania Study
• Investigator-initiated studies from AZ, Eli Lilly and Company, Lundbeck, Wyeth
• Grant funding (past and present): NIMH (USA); CIHR (Canada); NARSAD (USA);
Stanley Medical Research Institute (USA); MRC (UK); Wellcome Trust (UK);
Royal College of Physicians (Edin); BMA (UK); UBC-VGH Foundation (Canada);
WEDC (Canada); CCS Depression Research Fund (Canada); MSFHR (Canada).
• Associate Director of the NIHR Clinical Research Network; EMCT Cluster Lead

3
Table of contents
The burden of depression
Cognitive symptoms are common
Cognitive symptoms are
debilitating
Cognitive symptoms are not well
treated

4
THE BURDEN OF
DEPRESSION
The burden of depression

5
MDD is among the Top 5 global causes
of DALYs
Murray CJ, Lopez AD. Science 1996;274:740-3
Disease / injury
1990 2020 baseline scenario
Rank Total DALYs (%) Rank Total DALYs (%)
Lower respiratory infections 1 8.2 6 3.1
Diarrheal diseases 2 7.2 9 2.7
Conditions arising during perinatal period 3 6.7 11 2.5
Unipolar major depression 4 3.7 2 5.7
Ischemic heart disease 5 3.4 1 5.9
Cerebrovascular disease 6 2.8 4 4.4
Tuberculosis 7 2.8 7 3.1
Measles 8 2.6 25 1.1
Road traffic accidents 9 2.5 3 5.1
Congenital anomalies 10 2.4 13 2.2
Malaria 11 2.3 24 1.1
Chronic obstructive pulmonary disease 12 2.1 5 4.1
Falls 13 1.9 19 1.5
Iron-deficiency anemia 14 1.8 39 0.5
Protein-energy malnutrition 15 1.5 37 0.6
War 16 1.5 8 3.0
Self-inflicted injuries 17 1.4 14 1.9
Violence 19 1.3 12 2.3
HIV 28 0.8 10 2.6
Trachea / bronchus / lung cancers 33 0.6 15 1.8
MDD, major depressive disorder; DALY, disability-adjusted life-year

6
Depression has more negative effects on health
100
80
60
40
20
0
Mea
n h
ealt
h s
co
re (
0–
100)
90.6
80.3 79.6 79.3 78.9
72.9 67.1
65.8 65.4
58.5
71.8
56.1
In terms of mean health score, depression exerts more of an impact than
asthma, angina, arthritis, or diabetes
Depression adds to the
burden of asthma, angina,
arthritis, or diabetes
Adapted from Moussavi S et al. Lancet 2007;370:851-8
7
Table of contents
The burden of depression
Cognitive symptoms are common

8
Cognitive deficits are common in depression

9
DSM-5 identifies cognitive symptoms as a criterion
item of an MDE
● “Diminished ability to think or concentrate,
nearly every day (either by subjective
account or observed by others)”
1 of the 9 diagnostic criteria for
depression
American Psychiatric Association. DSM-5.
American Psychiatric Publishing, 2013
DSM-5, Diagnostic and Statistical Manual of Mental Disorders, 5th Edition;
MDE, major depressive episode

10
Cognitive dysfunction: common symptoms
in MDD
American Psychiatric Association. DSM-5.
American Psychiatric Publishing, 2013
DSM-5 criterion Additional information
Depressed mood Feeling sad or empty
Anhedonia Markedly diminished interest or pleasure in all or nearly all activities
Significant weight
change
Weight loss and / or increases or decreases in appetite
Sleep problems Insomnia or hypersomnia
Psychomotor problems Psychomotor agitation or retardation
Fatigue Evident as a loss of energy
Feeling worthless or
inappropriately guilty
Excessive feeling of worthlessness or inappropriate guilt, not merely
self-reproach or guilt about being sick
Cognitive problems Diminished ability to think or concentrate, or indecisiveness, either
documented by subjective account or as observed by others
Thoughts of death Recurrent thoughts of death or suicidal ideation; suicidal attempt or plan
DSM-5, Diagnostic and Statistical Manual of Mental Disorders, 5th Edition

11
Many patients with MDD have discernible
cognitive impairments
● Patients with depression performed significantly worse on working memory and
reaction time tests, while patients with schizophrenia were significantly worse on all
tests compared to controls
Neurocognitive test scores in patients with depression (mean HAM-D 22.4),
schizophrenia (mean PANSS 75.6), and control subjects
*p<0.05 depression vs control
HAM-D, Hamilton Depression Rating Scale;
PANSS, Positive and Negative Syndrome Scale Rund BR et al. Acta Psychiatr Scand 2006;113:350-9
Working
memory
0.5
0.0
-0.5
-1.0
-1.5
-2.0
-2.5 Executive
function
Visual
memory
Verbal
memory
Visual info.
processing
Reaction
time
Attention /
vigilance
z-s
core
s
Control (n=50)
Depression (n=45)
Schizophrenia (n=53)
* *
14
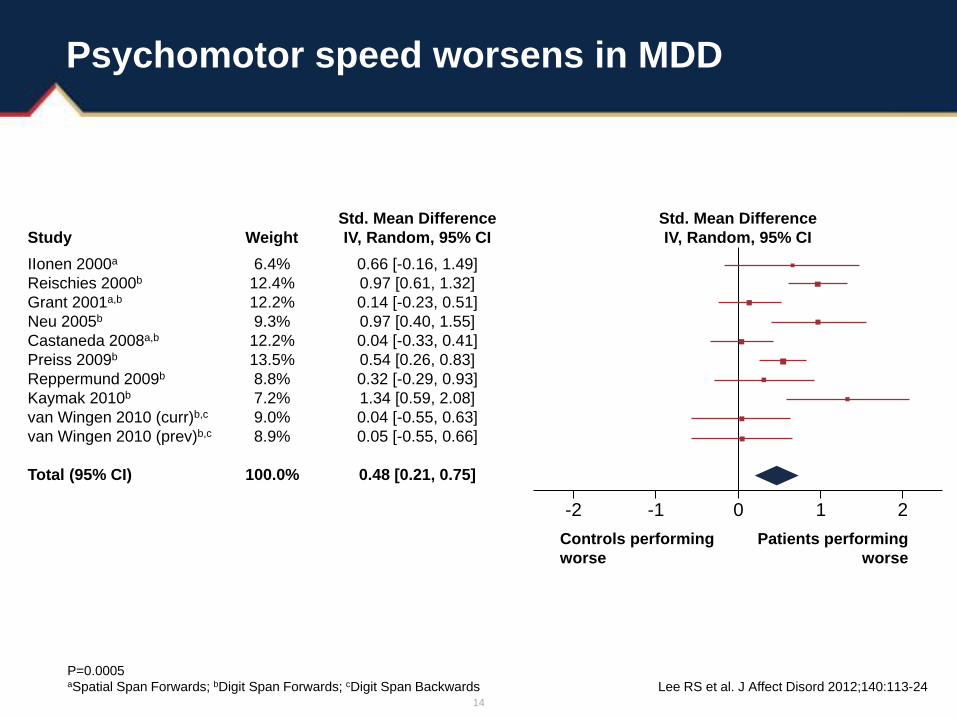
Psychomotor speed worsens in MDD
Lee RS et al. J Affect Disord 2012;140:113-24
Study Weight
Std. Mean Difference
IV, Random, 95% CI
Std. Mean Difference
IV, Random, 95% CI
IIonen 2000a
Reischies 2000b
Grant 2001a,b
Neu 2005b
Castaneda 2008a,b
Preiss 2009b
Reppermund 2009b
Kaymak 2010b
van Wingen 2010 (curr)b,c
van Wingen 2010 (prev)b,c
Total (95% CI)
6.4%
12.4%
12.2%
9.3%
12.2%
13.5%
8.8%
7.2%
9.0%
8.9%
100.0%
0.66 [-0.16, 1.49]
0.97 [0.61, 1.32]
0.14 [-0.23, 0.51]
0.97 [0.40, 1.55]
0.04 [-0.33, 0.41]
0.54 [0.26, 0.83]
0.32 [-0.29, 0.93]
1.34 [0.59, 2.08]
0.04 [-0.55, 0.63]
0.05 [-0.55, 0.66]
0.48 [0.21, 0.75]
Controls performing
worse
Patients performing
worse
-2 -1 0 1 2
P=0.0005 aSpatial Span Forwards; bDigit Span Forwards; cDigit Span Backwards

15
Cognitive impairment of functional domains
Std. Mean Difference
IV, Random, 95% CI P value
Cognitive flexibility 0.53 [0.23, 0.83] 0.0007
Attention 0.36 [0.13, 0.59] 0.002
Verbal fluency 0.59 [0.10, 1.07] 0.02
Attentional switching 0.22 [0.00, 0.44] 0.05
Visual 0.53 [-0.05, 1.11] 0.07
Working memory 0.16 [-0.20, 0.51] 0.38
Verbal 0.13 [-0.18, 0.45] 0.4
Lee RS et al. J Affect Disord 2012;140:113-24

16
Age (many studies in
elderly patients)
Age at onset
Educational attainment
Baseline depression severity
MDD subtype
Psychiatric co-morbidity
Symptomatic status
(remission vs non-remission)
Medical co-morbidity
Illness duration
Episode frequency
Treatment
Childhood adversity
Methodological
factors that may
affect the
interpretation of
study outcomes
Limitations of study methodology as they pertain to
cognitive symptoms in MDD
Adapted from: McIntyre RS et al. Depress Anxiety 2013;30:515-27

18
● ‘Hot’ cognition
– Emotional processing; response to negative feedback
– Changes in the ‘hot’ system are more likely to be associated with
antidepressant response
● ‘Cold’ cognition
– Emotion-independent; logical thinking and executive control
(executive, attention, perception, and psychomotor functions)
‘Hot’ and ‘cold’ cognition
Schaefer A et al. Neuroimage 2003;18:938-49

19
DLPFC, dorsolateral prefrontal cortex;
PFC, prefrontal cortex; vmPFC, ventromedial prefrontal cortex
‘Hot’ cognition
Ventromedial prefrontal cortex is
associated with emotion-based
cognition, with associations to emotional
processing areas (eg amygdala)
Connectivity between PFC and
other brain regions
‘Cold’ cognition
Dorsolateral prefrontal cortex is
associated with non-emotional cognition, sensory,
and motor areas (eg basal ganglia and parietal cortex)
‘Hot’ and ‘cold’ cognition have different brain pathways
and connectivity
Wood JN, Grafman J. Nat Rev Neurosci 2003;4:139-47
Image provided by Roger McIntyre
Cingulate Hippocampal
formation
Parietal / occipital
visual-association
areas
Motor structures Dorsolateral
prefrontal cortex
Posterior parietal
heteromodal area
Amygdala
complex Ventromedial
prefrontal
cortex
Inferior temporal
visual association
areas
20
Table of contents
The burden of depression
Cognitive symptoms are common
Cognitive symptoms are
debilitating

21
Cognitive deficits are debilitating

22
Cognitive impairment is associated with
life-functioning disability
Life-function disability
Attention
Working memory
Ideation fluency / executive function
Verbal knowledge
Non-verbal
function
Learning
Motor
Jaeger J et al. Psychiatry Res 2006;145:39-48
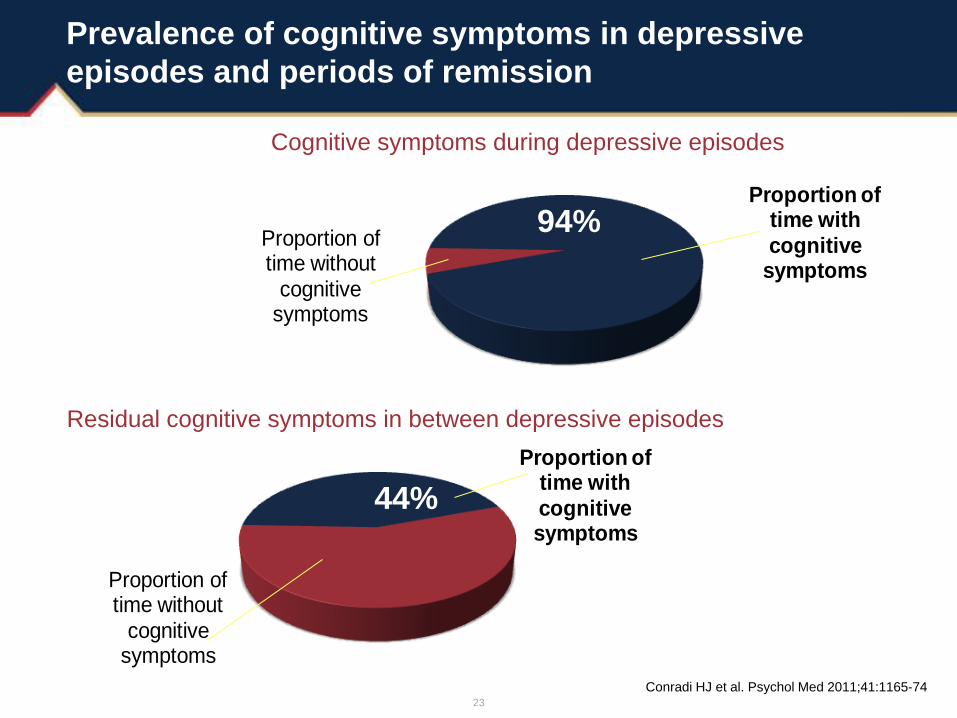
23
Prevalence of cognitive symptoms in depressive
episodes and periods of remission
Conradi HJ et al. Psychol Med 2011;41:1165-74
Proportion of time with cognitive symptoms
Proportion of time without
cognitive symptoms
44%
Residual cognitive symptoms in between depressive episodes
Proportion of time with cognitive
symptoms
Proportion of time without
cognitive symptoms
94%
Cognitive symptoms during depressive episodes

24
Functional impairment in the last 30 days in patients who had an MDE in the
past 30 days, past 12 months, >12 months ago, and healthy controls
Cognitive impairment is a common problem
in MDD patients in the short and long term
Groups standardized for age, sex, and ethnicity; all scales were transformed to a scale of 0
(no impairment at any time) to 1.0 (completely impaired for the entire time)
*p<0.05 vs subjects with no history of MDD
CI, confidence interval; WHO-DAS, World Health Organization-Disability Assessment Scale Kessler RC et al. JAMA 2003;289:3095-105
Recency of MDD, mean score (95% CI)
WHO-DAS
domains
Past 30 days
(n=222)
Past 12 months
(n=399)
>12 months ago
(n=889)
No lifetime MDD
(n=4044)
Out of role 0.25 (0.17, 0.33)* 0.06 (0.02, 0.09)* 0.01 (0, 0.02) -0.01 (-0.02, 0)
Self-care 0.10 (0.04, 0.16)* 0.02 (0, 0.04) 0.01 (0, 0.02) 0 (-0.01, 0)
Mobility 0.17 (0.09, 0.25)* 0.02 (0, 0.05) 0.02 (0, 0.04) -0.01 (-0.02, 0)
Cognition 0.29 (0.22, 0.36)* 0.11 (0.07, 0.15)* 0.01 (0, 0.03) -0.01 (-0.002, -0.01)
Productivity 0.21 (0.15, 0.28)* 0.08 (0.04, 0.12)* 0.02 (0, 0.04) -0.01 (-0.02, 0)
Social 0.27 (0.20, 0.33)* 0.06 (0.02, 0.10)* 0.01 (0, 0.02) -0.01 (-0.02, 0)

25
Presence of residual cognitive symptoms during
depressive episodes and periods of remission
Mean proportion of time symptoms are present during
3-year follow-up period (n=267)
Conradi HJ et al. Psychol Med 2011;41:1165-74
1.00
0.80
0.60
0.40
0.20
Mea
n p
rop
ort
ion
of
tim
e D
SM
-IV
sym
pto
m c
luste
r is
pre
se
nt
0.00
Weeks of follow-up
Core symptoms: depressed mood / diminished interest
Cognitive problems
Lack of energy
Sleeping problems
Worthlessness / guilt
Eating problems
Psychomotor problems
Death ideations
DSM-IV, Diagnostic and Statistical Manual of
Mental Disorders, 4th edition
26
Cognitive deficits affect outcomes
Cognitive deficits in MDD are consistent, replicable, and
clinically significant
– Deficits in executive function occur in ~2030% of individuals
– Abnormalities are evident in working memory, attention, and
psychomotor processing speed
Cognitive deficits are a principal mediator of psychosocial
impairment (particularly workforce performance)
Pharmacological, behavioral, and neuromodulatory interventions
hold promise to reduce, reverse, and prevent cognitive deficits
McIntyre RS et al. Depress Anxiety 2013;30:515-27

27
Cognitive symptoms of MDD: impact on patient
Cognitive symptoms negatively affected all aspects of
the patient’s life, especially in the workplace
Work / school life
● Miss / forget deadlines
● Struggle to answer even simple questions
● Struggle to complete even simple tasks
● Loss of ability to focus on conversations and in meetings
● Often miss the point of what is being said to them
● Fear of under-performing
● Lose confidence in their abilities to function, second-guessing their
decisions and instincts at every turn
● Lose the ability to clearly communicate their thoughts and ideas
Social life
● Participation in conversations becomes challenging, causing them to withdraw
from social situations
● Forget important dates, memories, and plans
Family / personal life
● Unable to cope with daily household tasks
● Unable to fulfill their role in the family as spouse and / or parent
● Become frustrated and angry quickly, at times lashing out at others
McIntyre RS et al. Depress Anxiety 2013;30:515-27

28
MSIF, Multidimensional Scale of Independent Functioning
MDD patients 6 months post-hospital discharge1
Cognitive
impairments
were strongly
associated
with impaired
life functioning
at 6 months1-3
1. Jaeger J et al. Psychiatry Res 2006;145:39-48;
2. Greer TL et al. CNS Drugs 2010;24:267-84;
3. McIntyre RS et al. Depress Anxiety 2013;30:515-27
Cognitive symptoms can adversely affect life functioning
independent of improvement in depressive symptoms
12
10
8
6
4
2
0 0 2 3 4 5 6 7
No. part
icip
ants
MSIF score (1=normal functioning; 7=totally disabled)

29
Embarrassment
Mobility
Self-care
Cognition
Social Interaction
Discrimination
MDE
Participation
restriction
Cognition and
embarrassment were
the only determinants
significantly associated
with both MDEs and
work functioning
(participation restriction)
Arrows represent the associations between MDE and activity limitations (a1–a6) and the associations between
activity limitations and participation restrictions (b1–b6)
Mobility
Discrimination
Social
interaction
Self-care
MDE
Buist-Bouwman MA et al. Acta Psychiatr Scand 2008;118:451-8
Survey representative of the adult population in Belgium, France,
Germany, Italy, Netherlands, and Spain (n=21,425)
Cognition
Embarrassment
Cognitive symptoms in MDD mediate psychosocial
impairment in depression

30
Table of contents
The burden of depression
Cognitive symptoms are common
Cognitive symptoms are
debilitating
Cognitive symptoms are not well
treated
31
Cognitive symptoms are not well treated

32
1. Harvey PD. Psychiatry (Edgmont) 2009;6:23-5
Cognitive assessment
● Cognitive symptoms of depression can be assessed subjectively
and objectively by
– Self-report: complaints of cognitive deficits are common
– Clinician rating by interview or behavioral observation
– Wide variety of objective neuropsychological tests
● Subjectively reported symptoms and objectively measured
cognitive deficits are not consistent in MDD1

33
Assessing cognitive function using bedside tests
Common bedside tests to assess cognitive impairment
Not very sensitive for milder cognitive dysfunction seen in depression
Mini-mental state examination Montreal Cognitive Assessment
McIntyre RS et al. Depress. Anxiety 2013;30:515-27

34
Attention and processing speed:
Digit Symbol Substitution Test
● Asks you to match symbols with their corresponding digit as fast as possible
● There is also a speed of processing component, since you have a very small
amount of time to enter the correct symbol
● The score is the number of correct symbols drawn within 90 seconds for
a maximum score of 93
Hasselbalch BJ et al. J Affect Disord 2011;134:20-31

35
● Designed to assess immediate and delayed recall1
1. Lezak MD. Neuropsychological Assessment, 4th Edition, Chapter 11. Oxford University Press.
2. Hasselbalch BJ et al. J Affect Disord 2011;134:20-31
List Trial 1 Trial 2 Trial 3 Trial 4 Trial 5 20-minute
delay
Yacht
Irony
Dummy
Shriek
Reflex
Bandit
Homicide
Hope
Stone
Event
Child
Speech
Moment
Friend
Property
“I am going to read you a list
of words. I want you to listen
carefully and, when I finish,
repeat back as many
words as you can”
Patients with
depression do
more poorly on
this test than
age-matched
comparisons2
Memory: RAVLT

36
Executive function: Trail-Making Test Part B
● The patient draws lines to
connect the circles in an
ascending pattern, but with the
added task of alternating
between the numbers and
letters (ie 1-A-2-B-3-C etc)
● Results are reported as the
number of seconds required to
complete the task; therefore,
higher scores reveal greater
impairment (executive
dysfunction)
Average: 75 seconds
Deficient: >273 seconds
Rule of thumb: most in 3 minutes
8
9
B
H
I
4
3
1 7
C
12 C
2 L
F K
5
J
A
6 E
11
10
D

37
Examples of self-rated cognitive questionnaires
● British Columbia Cognitive Complaints Inventory (BC-CCI)
● Cognitive and Physical Functioning Questionnaire (CPFQ)
● Perceived Deficits Questionnaire (PDQ)
● Medical Outcomes Study Cognitive Functioning
(MOS-Cog) scale
● Cognitive Dysfunction Questionnaire (CDQ)
● Cognitive Failures Questionnaire (CFQ)
● Prospective and Retrospective Memory
Questionnaire (PRMQ)

38
Perceived Deficits Questionnaire (PDQ)
● 20-item self-report assessing self-perceived cognitive difficulties
(5-item version also available)1
● 4 subscales and total score1
– Attention / concentration
– Retrospective memory
– Prospective memory
– Planning / organization
● Originally developed for multiple sclerosis1
● Qualitative testing (focus groups) in depression2
– Items considered understandable, appropriate, and comprehensive
– Preferred PDQ to other cognitive questionnaires
– Minor modifications suggested for PDQ-D
● Validated in an online study of depressed and non-depressed individuals3
1. Sullivan MJ et al. Pain Res Manage 2002;7:120-6;
2. Forsyth B et al. Eur Neuropsychopharmacol 2012;22(Suppl 2):S229-30;
3. Lam RW et al. Unpublished data
PDQ-D, Perceived Deficits Questionnaire – Depression

39
Perceived Deficits Questionnaire – Depression
5-item version (PDQ-D-5)
The following questions describe problems people may have with their memory,
attention, or concentration. Please select the best response based on your
experiences during the past 7 days
During the past 7 days, how often
did you…
Never in the
past
7 days
Rarely
(once or
twice)
Sometimes
(3 to 5 times)
Often
(about once
a day)
Very often
(more than
once a day)
Have trouble getting things
organized? 0 1 2 3 4
Have trouble concentrating on
what you were reading? 0 1 2 3 4
Forget the date unless you looked
it up? 0 1 2 3 4
Forget what you talked about after
a telephone conversation? 0 1 2 3 4
Feel like your mind went totally
blank? 0 1 2 3 4
Add up score in each column:
TOTAL SCORE: _________
40
Current treatments do not address cognitive
dysfunction
There is emerging evidence that, in some patients, the degree of cognitive deficit goes beyond that which can be accounted for by the severity of depressive symptoms
Current treatments (including SSRIs and SNRIs) have a partial or no effect on cognitive dysfunction in patients with MDD
In those with partial or full resolution of depressive symptoms, cognitive impairment may persist
Evidence is accumulating to support the view that, in subgroups of patients, cognitive deficits constitute a dimension of MDD that is independent of, and dissociable from, depressive symptomatology
Airaksinen E et al. Acta Psychiatr Scand 2007;115:458-65;
Behnken A et al. J Affect Disord 2010;122:144-8; Harvey P et al. J Psychiatr Res 2004;38:567-76;
Iverson GL et al. J Affect Disord 2011;132:360-7; Lee RS et al. J Affect Disord 2012;140:113-24;
McClintock SM et al. Neuropsychology 2010;24:9-34;
McDermott LM, Ebmeier KP. J Affect Disord 2009;119:1-8;
Reppermund S et al. Psychol Med 2009;39:603-14;
Naismith SL et al. J Clin Exp Neuropsychol 2003;25:866-77;
Weiland-Fiedler P et al. J Affect Disord 2004;82:253-8
SSRI, selective serotonin reuptake inhibitor;
SNRI, serotonin–noradrenaline reuptake inhibitor

41
Persistent symptoms in STAR*D responders
0
20
40
60
80
100
Mid-nocturnal
insomnia
Concentration /
decision-making
Suicidal ideation Negative self-view
Pa
tie
nts
(%
)
Baseline
Post-citalopram response
1. McClintock SM et al. J Clin Psychopharmacol 2011;31:180-6
Symptoms present in patients with MDD
who responded but did not remit (n=428)1

42
Cognitive dysfunction in depression
Clinically important1
Poor concentration (often described as poor memory) is a core symptom:
“mind going blank” and inability to make decisions
Often patients think they have attention-deficit disorder or, if older, Alzheimer’s disease
Deficits in almost every domain of cognitive functioning2
Processing speed
Attention
Executive function
Working memory
Episodic memory
1. Marazziti D et al. Eur J Pharmacol 2010;626:83-6;
2. Hasselbalch BJ et al. J Affect Disord 2011;134:20-31

43
Summary
• Cognitive deficit is an independent core symptom for the
diagnosis of MDD
• Present treatments have partial or no effect on cognitive
dysfunction in patients with MDD
• Residual cognitive dysfunction may be predictive for a
high risk of relapse and poor outcome for patients with
MDD
• There is the potential to greatly improve treatment to
target cognitive deficits in MDD

44
Take-home messages
● Cognitive dysfunction in MDD is prevalent, persistent, and identified
in symptomatic as well as ‘remitted’ patients
● Cognitive dysfunction can be defined according to domain affected
as well as ‘hot’ vs ‘cold’
● Cognitive dysfunction in MDD may predispose recurrence of illness
● In sub-populations, it is a principal mediator of functional impairment
● Clinicians are encouraged to “THINC” about cognitive impairment in
depression by evaluating patients for subjective complaint as well as
objective measurement
Related Documents











