Monthly Webinar Tuesday 20 th February 2018, 16:00 “Vanishing Vanco Variation” Audio dial-in (phone): 01 526 0058

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Monthly WebinarTuesday 20th February 2018, 16:00
“Vanishing Vanco Variation”
Audio dial-in (phone): 01 526 0058

Instructions
• Interactive– Please use chat box function for
questions and comments• Select send to “All Participants”
• Sound– Better over phone
• 01 526 0058 (if attending withinIreland)
• Follow us on Twitter– @AMSInSight– @hpscireland

We’d like to ask you a few questions……

VanishingVanco
Variation
Gerry HughesResearch PharmacistSt. James’s Hospital Dublin

A brief history of vancomycin
• 1952 – discovery of the “vanquishing”antibiotic
• “Mississippi Mud”, poor purification
Levine DP. History of Vancomycin .Clin Inf Dis 2006:42 (Suppl 1) S5 Griffith RS. Vancomycin use - an historical review. JAC 1984: 14 Suppl D:1-5.
http://www.rosincerate.com/2015/04/the-unpleasant-muddiness-of-crudely.html

Levine DP. History of Vancomycin .Clin Inf Dis 2006:42 (Suppl 1) S5

@medsafetymin

A brief history of vancomycin
• 1952 – discovery of the “vanquishing”antibiotic
• “Mississippi Mud”, poor purification• Became valuable tool in fight against MRSA/CDI• Continued concerns about ability to maintain
safe, therapeutic levels
Levine DP. History of Vancomycin .Clin Inf Dis 2006:42 (Suppl 1) S5

J Antimicrob Chemother 2014; 69: 2274–2283


A PHARMACIST – DIRECTED QUALITYIMPROVEMENT OF VANCOMYCINDOSING AND MONITORING AT ST.JAMES’S HOSPITAL

Background• Antimicrobial Stewardship Committee: one of key priorities 2016
– Optimisation of therapeutic drug monitoring (TDM) includingvancomycin
• Previous internal audits– 2006 – small pilot study, pharmacist directed vancomycin therapy (1)– 2013 – observational audit, prescribing/monitoring continues to be
suboptimal
• Drivers of suboptimal vancomycin prescribing/monitoring– Prescribing guidelines not consulted before prescribing– Misinterpretation of guidelines if accessed– Overlooking renal impairment, using eGFR in place of Cockcroft & Gault
• Pharmacist-led interventions successful with other (TDM) drugs(2-4)

Methods
• Literature review conducted to informproposal
• Proposal reviewed and approved by– Antimicrobial Stewardship Committee– SJH/AMNCH Research and Ethics committee– SJH Research and Development Hub
• Six wards chosen to trial intervention

Medical
Surgical
Antimicrobial Pharmacist Consult Service Available
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24

Methods
• Project outlined and discussed with– Directorate leads– Teams who have majority of their patients on
chosen wards– Ward nurse managers– Staff nurses
• Flagged intervention on ward notice boardsand above key work areas– Example: above computer workstations


Methods
• Data collected and stored in Microsoft Excel ®• Study (intervention) data compared to 2013
(observation) data• Trough levels deemed in range if 10-20 mg/L• Statistical analysis using ‘R’ stats package
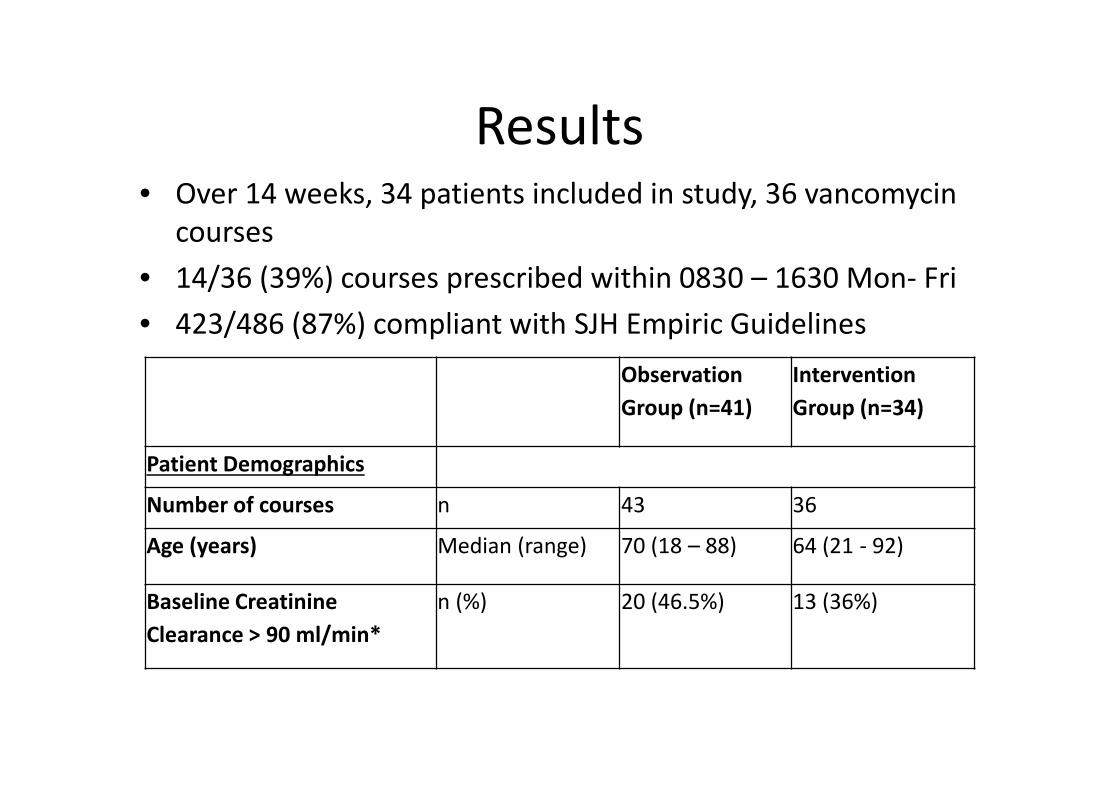
Results• Over 14 weeks, 34 patients included in study, 36 vancomycin
courses• 14/36 (39%) courses prescribed within 0830 – 1630 Mon- Fri• 423/486 (87%) compliant with SJH Empiric Guidelines
ObservationGroup (n=41)
InterventionGroup (n=34)
Patient Demographics
Number of courses n 43 36
Age (years) Median (range) 70 (18 – 88) 64 (21 - 92)
Baseline CreatinineClearance > 90 ml/min*
n (%) 20 (46.5%) 13 (36%)

Results: Prescribing and Administration
• Antimicrobial pharmacist involved in initial therapy strategyfor 13/36 (36%) courses
• Correct initial dose administered to 92% patients with pre-first dose pharmacist consultation vs 48% patients without(p=0.02)
• Correct initial vancomycin doses prescribed to 61% ofpatients in intervention vs 30% in the observation period(p<0.05).

Results: Trough Level Monitoring
In the intervention arm there were (non-significant) trends
towards:
• Increased accuracy of timing of first trough levels when
pharmacist guidance was given pre – first dose compared to
later in therapy : 77% vs 52%, respectively.
• Pre - first dose intervention by the pharmacist resulted in a
higher proportion of trough levels in the therapeutic range than
intervention which occurred later in the course: 63% vs. 55%,
respectively.

Proportion of correctly timed vancomycin levels in observation vs intervention study

Proportion of correctly timed trough levels with results in sub-therapeutic, therapeutic and potentially toxic ranges

Proportion of all trough levels taken by healthcare workers in the observation period and intervention period

Proportion of correctly timed trough levels taken by healthcare workers in the observation period and intervention period

Discussion
• Is a dedicated TDM/antimicrobial pharmacistbeneficial?– Patient more likely to receive correct initial dose– Patient more likely to have appropriately taken trough
level• Levels out of therapeutic range
– More likely to be sub therapeutic rather than toxic• Potentially toxic levels
– More likely to represent inaccurate trough measurement• Trend of improved accuracy for all operators with
pharmacist intervention

Conclusion
• Appropriate first dose and early antimicrobial pharmacist
intervention positively affected the quality of prescribing and TDM
• Significant improvement was observed in compliance with
– hospital guidelines in relation to dosing and
– trough level monitoring
• Results support the implementation of
– Pharmacist-directed TDM programme
– May incorporate pharmacist prescribing



References1. O' Reilly A, O' Connell B. To assess the impact of a pharmacist-led TDM
service on vancomycin and gentamicin levels at St. James’s Hospital(SJH). Microsoft PowerPoint Presentation. SJH Dublin 2006.
2. Murphy R CMaDL. Impact of a pharmacist-initiated therapeutic drugmonitoring drug consult service for children treated with gentamicin.The Canadian Journal of Hospital Pharmacy. 2007;60(3).
3. Mamdani MM, Racine E, McCreadie S, Zimmerman C, O'Sullivan TL,Jensen G, et al. Clinical and economic effectiveness of an inpatientanticoagulation service. Pharmacotherapy. 1999;19(9):1064-74.
4. Spence MM, Polzin JK, Weisberger CL, Martin JP, Rho JP, Willick GH.Evaluation of a pharmacist-managed amiodarone monitoring program.Journal of Managed Care Pharmacy. 2011;17(7):513-22.

Discussion

Next MonthTuesday 20th March 2018, 16:00
“Public Engagement in Antimicrobial Stewardship”Kirsten Schaffer, SVUH
Check www.hpsc.ie or follow @AMSInSight on Twitterfor registration details

Date for your diary:
Third Irish Antimicrobial Stewardship Conference11 June 2018
St. James’s Hospital Dublin 8Organised by the AMS InSight Team
Related Documents











