Monte Carlo based treatment planning systems Joanna E. Cygler, Ph.D., FCCPM, FAAPM, FCOMP The Ottawa Hospital Cancer Centre, Ottawa, Canada Carleton University, Dept. of Physics, Ottawa, Canada University of Ottawa, Dept. of Radiology, Ottawa, Canada

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Monte Carlo based treatment planning
systems
Joanna E. Cygler, Ph.D., FCCPM, FAAPM, FCOMP
The Ottawa Hospital Cancer Centre, Ottawa, Canada
Carleton University, Dept. of Physics, Ottawa, Canada
University of Ottawa, Dept. of Radiology, Ottawa, Canada

Rationale for Monte Carlo dose
calculation for electron beams
• Difficulties of commercial pencil beam based algorithms
– Monitor unit calculations for arbitrary SSD
values – large errors*
– Dose distributions
in heterogeneous media
have large errors for
complex geometries
*can be circumvented by entering separate virtual
machines for each SSD – labor consuming
Ding, G. X., et al, Int. J. Rad. Onc. Biol. Phys.
(2005) 63:622-6332

Rationale for MC dose calculations
for photon beams
Arnfield et al. (MCV), Med. Phys, 27 (6) 2000
water water
3

Commercial MC-based TPS:
electron beams
• MDS Nordion (NucletronElekta) 2001
– First commercial Monte Carlo treatment planning for electron beams
– Kawrakow’s VMC++ Monte Carlo dose calculation algorithm (2000)
– Handles electron beams from all clinical linacs
• Varian Eclipse eMC 2004
– Neuenschwander’s MMC dose calculation algorithm (1992)
– Handles electron beams from Varian linacs only (23EX)
– work in progress to include beam models for linacs from other vendors (M.K. Fix et al, Phys. Med.
Biol. 58 (2013) 2841–2859)
• Elekta-CMS XiO eMC for electron beams 2010
– Based on VMC (Kawrakow, Fippel, Friedrich, 1996)
– Handles electron beams from all clinical linacs
• Elekta – Monaco
– Kawrakow’s VMC++ Monte Carlo dose calculation algorithm (2000)
– Handles electron beams from all clinical linacs
4

• Elekta (CMS) - Monaco (IMRT)
• Brainlab - iPlan
Based on XVMC (Kawrakow, Fippel, Friedrich, 1996 and Fippel 1999)
Commercial MC-based TPS:
photon beams
• Accuray - Multiplan in CyberKnife TPS
Based on MCDOSE (Ma et al 2002 and 2008)
5

Components of Monte Carlo based dose
calculation system
There are two basic components of MC dose calculation, see
the next slide:
1. Particle transport through the accelerator head
– explicit transport (e.g. BEAM code)
– accelerator head model (parameterization of primary and
scattered beam components)
2. Dose calculation in the patient
6

Example of a beam model
Sub-sources
1 - the main diverging source
of electrons and photons;
2 - edge source of electrons;
3 - transmission source of
photons;
4 - line source of electrons
and photons.
M.K. Fix et al, Phys. Med. Biol. 58 (2013) 2841–28597

Clinical implementation of MC
treatment planning software
• Beam data acquisition and fitting
• Software commissioning tests*
– Beam model verification
– Dose profiles and MU calculations in a homogeneous water tank
– In-patient dose calculations
• Clinical implementation
– procedures for clinical use
– possible restrictions
– staff training
*should include tests specific to Monte Carlo
A physicist responsible for TPS implementation should have a thorough understanding of how the system works.
8

Issues to consider
• Statistical noise
• Voxel size (spatial resolution)
• Isodose smoothing
• Dose to water vs. dose to medium
• Differences between standard (water tank based)
and MC based MU calculations
• Potential clinical implications of MC calculated dose
distributions
– prescription change?
9
Guidance on how to proceed - AAPM Task Group Report No. 105: Issues
associated with clinical implementation of photon and electron beam
Monte Carlo-based treatment planning (Med. Phys. 34, 4818-53, 2007 )

Issues to consider
• Statistical noise
• Voxel size (spatial resolution)
• Isodose smoothing
• Dose to water vs. dose to medium
• Differences between standard and MC based MU
calculations
• Potential clinical implications of MC calculated dose
distributions
– prescription change?
10
Guidance on how to proceed - AAPM Task Group Report No. 105: Issues
associated with clinical implementation of photon and electron beam
Monte Carlo-based treatment planning (Med. Phys. 34, 4818-53, 2007 )

AAPM TG-105: Summary of Recommendations
Patient Simulation:
• Statistical Uncertainties:
Should be specified to doses within volumes
consisting of many voxels; single-voxel dose
uncertainty estimates should be avoided as should be
specification to the maximum or minimum dose voxels,
Rogers and Mohan, (2000)
11
2
5.05.0
2
maxmax
1
DD i
i
DD D
D
K

10 million50 million150 million1.5 billion
Effect of uncertainties on the 95% IDL
I.Chetty et al, Red Journal, (2006), 1249-5912

Issues to consider
• Statistical noise
• Voxel size (spatial resolution)
• Isodose smoothing
• Dose to water vs. dose to medium
• Differences between standard and MC based MU
calculations
• Potential clinical implications of MC calculated dose
distributions
– prescription change?
13
Guidance on how to proceed - AAPM Task Group Report No. 105: Issues
associated with clinical implementation of photon and electron beam
Monte Carlo-based treatment planning (Med. Phys. 34, 4818-53, 2007 )

Voxel size – required spatial
resolution
• Small voxel size when high spatial resolution required
• Smaller voxel – increased calculation time
14

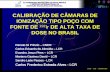
Monte-Carlo Settings: Effect on
computation time
Timing Results XiO TPS:
For 9 and 17 MeV beams, 10x10
cm2 applicator and the trachea
and spine phantom, timing tests
were performed for a clinical XiO
Linux workstation, which employs
8 processors, 3 GHz each, with
8.29 GB of RAM.
y = 3.4x-2.0
y = 6.4x-2.1
y = 0.7x-2.0
y = 0.4x-2.0
0
5
10
15
20
25
30
0 0.5 1 1.5 2 2.5
MRSU %
tim
e /
min
9 MeV 2.5 mm voxel
17 MeV 2.5 mm voxel
17 MeV 5 mm voxel
9MeV 5 mm voxel
Cygler, J.E., and Ding, G.X., in Monte Carlo Techniques in Radiation Therapy,
ISBN-10: 1466507926, Taylor & Francis (CRC Press INC ) Boca Raton 2013, p 155-16615

Issues to consider
• Statistical noise
• Voxel size (spatial resolution)
• Isodose smoothing
• Dose to water vs. dose to medium
• Differences between standard and MC based MU
calculations
• Potential clinical implications of MC calculated dose
distributions
– prescription change?
16
Guidance on how to proceed - AAPM Task Group Report No. 105: Issues
associated with clinical implementation of photon and electron beam
Monte Carlo-based treatment planning (Med. Phys. 34, 4818-53, 2007 )

Eclipse eMC
Effect of voxel size and smoothing
Ding, G X., et al (2006). Phys. Med. Biol. 51 (2006) 2781-2799. 17

Issues to consider
• Statistical noise
• Voxel size (spatial resolution)
• Isodose smoothing
• Dose to water vs. dose to medium
• Differences between standard and MC based MU
calculations
• Potential clinical implications of MC calculated dose
distributions
– prescription change?
18
Guidance on how to proceed - AAPM Task Group Report No. 105: Issues
associated with clinical implementation of photon and electron beam
Monte Carlo-based treatment planning (Med. Phys. 34, 4818-53, 2007 )

Dose-to-water vs. dose-to-medium
Ding, G X., et al Phys. Med. Biol. 51 (2006) 2781-2799.
Dm - energy absorbed
in a medium voxel
divided by the mass of
the medium element.
Dw - energy absorbed in
a small cavity of water
divided by the mass of
that cavity. Voxel of medium
w
mmw
SDD
Small volume
of water
Voxel of medium

Clinical Examples: 6MV Dw and Dm
DmDw
Dogan, et al, Phys Med Biol 51, (2006) 4967-4980 20

Dose-to-water vs. dose-to-medium
electron beams
DTM DTW
DTW-DTM
6 MeV beam, 15x15 cm2 applicator, both 602 MU
MRSU=2%, voxel size=4×4×4 mm3
21

AAPM TG-105: Summary of Recommendations
Patient Simulation:
• Dose to water and dose to medium:
Vendors
should state explicitly to which material dose is
reported;
allow for conversion between Dw and Dm
At this point only Elekta XiO fully complies
22

AAPM TG-105: Summary of Recommendations
Experimental Verification:
• In addition to standard dose algorithm commissioning
tests, verification should include testing in complex
situations to verify the expected improved accuracy
with the MC method;
• Detector perturbations need to be carefully assessed
particularly under conditions of electronic
disequilibrium;
• Measurement uncertainties should be understood and
estimated, where possible, in the verification process 23

Example of beam model verification
XiO eMC: cutout factors
Vandervoort et al, Med. Phys. 41, 2014; http://dx.doi.org/10.1118/1.4853375
Cutout Output Factors: 9 MeV
0.350
0.450
0.550
0.650
0.750
0.850
0.950
1.050
1 2 3 4 5 6 7 8 9
Square Cutout Length (cm)
Ou
tpu
t F
acto
r (c
Gy/M
U)
Experimental
XiO Calculated
Cutout Output Factors: 17 MeV
0.600
0.650
0.700
0.750
0.800
0.850
0.900
0.950
1.000
1.050
1 2 3 4 5 6 7 8 9
Square Cutout Length (cm)
Ou
tpu
t F
acto
r (c
Gy/M
U)
Experimental
XiO Calculated
SSD=100 cm
SSD=115 cm
0.800
0.850
0.900
0.950
1.000
1.050
1 3 5 7 9
Square Cutout Length (cm)
0.390
0.440
0.490
0.540
0.590
0.640
0.690
0.740
1 3 5 7 9
Square Cutout Length (cm)
SSD=100 cm
SSD=115 cm
24

More clinical issues to consider:
electron beams
25

MU - MC vs. hand calculations
Monte Carlo Hand calculations
Real physical dose
calculated on a patient
anatomy
Rectangular water tank
Heterogeneity correction
included
Contour irregularities
No heterogeneity
correction
Arbitrary beam anglePerpendicular beam
incidence only
26

9 MeV, full scatter phantom (water tank)
RDR=1 cGy/MU
100% isodose at the nominal (reference) dmax depth 27

Lateral scatter missing
Real contour / Water tank =
=234MU / 200MU=1.17
Reason for more MU: % isodose at the nominal (reference) dmax depth is
less than 100% 28

MU real patient vs. water tank
MC / Water tank= 292 / 256=1.14
29

30
More clinical issues to consider:
photon beams

DVH for the PTV
Pe
rce
nt
Vo
lum
e
Percent Dose
MC
EPL
DVH for the PTV
Pe
rce
nt
Vo
lum
e
Percent Dose
MC
EPL
DVH for the PTV
Pe
rce
nt
Vo
lum
e
Percent Dose
MC
EPL
Under-dosage of the PTV
Treatment Planning: The main
dosimetric issue
Solid = MC , 100%
Dashed = EPL, 100%
Blue = PTV
6 MV oblique fields
TG-105, courtesy of I.Chetty31

CyberKnife dose calculation issues
• Two dose calculation algorithms:
• Ray tracing or EPL (path length correction) algorithm
– no corrections for changes in electron transport or
lateral scatter disequilibrium that may develop in the
presence of low-density heterogeneities.
• Monte Carlo algorithm - based MCDOSE (Ma et al 2002
and 2008)
32

Recommendations Van der Voort van Zyp et al
Radiotherapy and Oncology 96 (2010) 55–60
• The EPL algorithm overestimates the actual delivered dose
• Dose reduction with MC depended on tumor size and
location
• Separate prescription dose according to tumor size
• Recommendation for peripheral tumors
– 3 x 16 Gy for tumors <3 cm,
– 3 x 17 Gy for tumors of 3–5 cm
– 3 x 18 Gy for tumors >5 cm
• Central tumors- no recommendation given yet - longer
follow-up needed
33

• MC-calculated doses can in some instances be significantly
different (10-20%) from conventional algorithms, such as
radiological path length, and convolution-based methods
• In light of these differences:
- should dose prescriptions change with MC-based
calculations ?
- How?
Dose prescription issues - summary
34

Dose prescription - AAPM TG-105
perspective
• MC method is just a more accurate dose algorithm
• Dose prescription issues are not specific to MC-based
dose calculation
• As with other changes to the therapy treatment process,
users should correlate doses and prescriptions with respect to
previous clinical experience
35

Conclusions
• Clinical implementation of MC-based systems must be performed
thoughtfully and users, especially physicists, must understand the
differences between MC-based and conventional dose algorithms
• Successful implementation of clinical MC algorithms requires strong
support from the clinical team and an understanding of the paradigm
shift with MC algorithms
• A properly commissioned MC-based dose algorithm will improve dose
calculation accuracy for electron and photon beams
• More accurate dose calculations
may improve dose-biological effect correlations
Lead to prescription changes in some cases

Acknowledgements
George X. Ding Indrin Chetty and other co-authors of TG-105
George Daskalov Margarida Fragoso
Charlie Ma Neelam Tyagi
Eric Vandervoort Ekaterina Tchistiakova
Junior Akunzi David W.O. Rogers
In the past I have received research support from Nucletron, Varian and Elekta.
TOHCC has a research agreement with Elekta.

Thank You
38

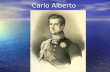
Monte-Carlo Settings: Effect on
computation time
Timing Results XiO TPS:
For 9 and 17 MeV beams, 10x10
cm2 applicator and the trachea
and spine phantom, timing tests
were performed for a clinical XiO
Linux workstation, which employs
8 processors, 3 GHz each, with
8.29 GB of RAM.
y = 3.4x-2.0
y = 6.4x-2.1
y = 0.7x-2.0
y = 0.4x-2.0
0
5
10
15
20
25
30
0 0.5 1 1.5 2 2.5
MRSU %
tim
e /
min
9 MeV 2.5 mm voxel
17 MeV 2.5 mm voxel
17 MeV 5 mm voxel
9MeV 5 mm voxel
Cygler, J.E., and Ding, G.X., in Monte Carlo Techniques in Radiation Therapy,
ISBN-10: 1466507926, Taylor & Francis (CRC Press INC ) Boca Raton 2013, p 155-16639

Timing – Nucletron TPS
Oncentra 4.0
4 MeV Timer Results:
Init = 0.321443 seconds
Calc = 42.188 seconds
Fini = 0.00158201 seconds
Sum = 42.5111 seconds
20 MeV Timer Results:
Init = 0.311014 seconds
Calc = 110.492 seconds
Fini = 0.00122603 seconds
Sum = 110.805 seconds
Anatomy - 201 CT slices
Voxels 3 mm3
10x10 cm2 applicator
50k histories/cm2
Faster than pencil beam!40

Timing – Varian Eclipse
Eclipse MMC, Varian single CPU Pentium IV
XEON, 2.4 GHz
10x10 cm2, applicator, water phantom,
cubic voxels of 5.0 mm sides
6, 12, 18 MeV electrons,
3, 4, 4 minutes, respectively
Chetty et al.: AAPM Task Group Report No. 105: Monte Carlo-based
treatment planning, Med. Phys. 34, 4818-4853, 200741

Selected references
1. Kawrakow, I., M. Fippel, and K. Friedrich. (1996), 3D electron dose
calculation using a Voxel based Monte Carlo algorithm (VMC). Med Phys
23 (4):445-57.
2. Kawrakow, I. “VMC++ electron and photon Monte Carlo calculations
optimized for radiation treatment planning”, Proceedings of the Monte
Carlo 2000 Meeting, (Springer, Berlin, 2001) pp229-236.
3. Neuenschwander H and Born E J 1992 A Macro Monte Carlo method for
electron beam dose calculations Phys. Med. Biol. 37 107 – 125.
4. Neuenschwander H, Mackie T R and Reckwerdt P J 1995 MMC—a high-
performance Monte Carlo code for electron
beam treatment planning Phys. Med. Biol. 40 543–74.
5. Janssen, J. J., E. W. Korevaar, L. J. van Battum, P. R. Storchi, and H.
Huizenga. (2001). “A model to determine the initial phase-space of a
clinical electron beam from measured beam data.” Phys Med Biol
46:269–286.

Selected references cont.
6. Traneus, E., A. Ahnesjö, M. Åsell.(2001) “Application and Verification
of a Coupled Multi-Source Electron Beam Model for Monte Carlo
Based Treatment Planning,” Radiotherapy and Oncology, 61, Suppl.1,
S102.
7 Cygler, J. E., G. M. Daskalov, and G. H. Chan, G.X. Ding. (2004).
“Evaluation of the first commercial Monte Carlo dose calculation
engine for electron beam treatment planning.” Med Phys 31:142-153.
8 Ding, G. X., D. M. Duggan, C. W. Coffey, P. Shokrani, and J. E.
Cygler. (2006). “First Macro Monte Carlo based commercial dose
calculation module for electron beam treatment planning-new issues
for clinical consideration.” Phys. Med. Biol. 51 (2006) 2781-2799.
9. Popple, RA., Weinberg, R., Antolak, J., (2006) “Comprehensive
evaluation of a commercial macro Monte Carlo electron dose
calculation implementation using a standard verification data set”. Med Phys 33:1540-1551.

Selected references cont.
10. B.A. Faddegon, J.E. Cygler: “Use of Monte Carlo Method in Accelerator
Head Simulation and Modelling for Electron Beams”, Integrating New
Technologies into Clinic: Monte Carlo and Image-Guided Radiation Therapy,
AAPM Monograph No. 32, edited by B.H. Curran, J.M. Balter, I.J. Chetty,
Medical Physics Publishing (Madison, WI, 2006) P.51-69.
11. J.E. Cygler, E. Heath, G.X. Ding, J.P. Seuntjens: “Monte Carlo Systems in
Preclinical and Clinical Treatment Planning: Pitfalls and Triumphs”, Integrating New Technologies into Clinic: Monte Carlo and Image-Guided
Radiation Therapy Monograph No. 32, edited by B.H. Curran, J.M. Balter,
I.J. Chetty, Medical Physics Publishing (Madison WI, 2006) p.199-232.
12. I. Chetty, B. Curran, J.E. Cygler et al.,(2007) Report of the AAPM Task
Group No. 105: Issues associated with clinical implementation of Monte
Carlo-based photon and electron external beam treatment planning. Med
Phys 34, 4818-4853.

Selected references cont.
13. Reynaert, N., S. C. van der Marck, D. R. Schaart, et al. 2007. Monte Carlo
treatment planning for photon and electron beams . Radiat Phys Chem 76:
643–86.. Radiat Phys Chem 76: 643–86.
14. Fragoso, M., Pillai, S., Solberg, T.D., Chetty, I., (2008) “Experimental verification
and clinical implementation of a commercial Monte Carlo electron beam dose
calculation algorithm”. Med Phys 35:1028-1038.
15. Edimo, P., et al., (2009) Evaluation of a commercial VMC++ Monte Carlo based
treatment planning system for electron beams using EGSnrc/BEAMnrc
simulations and measurements. Phys Med, 25(3): 111-21.
16. J.E. Cygler and G.X. Ding, “Electrons: Clinical Considerations and Applications
“ in Monte Carlo Techniques in Radiation Therapy, ISBN-10: 1466507926,
Taylor & Francis (CRC Press INC ) Boca Raton 2013, p 155-166
17. M. K. Fix, J. E. Cygler, D. Frei,W. Volken, H. Neuenschwander, E.J. Born and P.
Manser, (2013), Generalized eMC implementation for Monte Carlo dose
calculation of electron beams from different machine types, Phys. Med. Biol.
58, 2841–2859,
18. 4. E.J. Vandervoort, E. Tchistiakova, D.J. La Russa, J.E. Cygler. Evaluation of a
new commercial Monte Carlo dose calculation algorithm for electron beams,
Med. Phys. 41 (2), http://dx.doi.org/10.1118/1.4853375 (8 pages), 2014
Related Documents