Istituto Auxologico Italiano Istituto Auxologico Italiano 31 MARZO 1 APRILE 2017 COMO Aritmologia MONITORAGGIO REMOTO DEI DISPOSITIVI CARDIACI IMPIANTABILI G. B. Perego Istituto Auxologico Italiano Ospedale S. Luca - Milano

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Isti
tuto
Auxolo
gico
Ital
iano
Isti
tuto
Auxolo
gico
Ital
iano
31 MARZO 1 APRILE 2017 COMO
Aritmologia
MONITORAGGIO REMOTO
DEI DISPOSITIVI CARDIACI IMPIANTABILI
G. B. PeregoIstituto Auxologico Italiano
Ospedale S. Luca - Milano

Isti
tuto
Auxolo
gico
Ital
iano
Parthiban et. Al.. JACC 2015; 65: 2591-2560

Isti
tuto
Auxolo
gico
Ital
iano
Remote Patient Management
Results of Randomized Studies
Remote Control results in patient care that is non-inferior to classical FU with in-office visits
Remote Monitoring results:
➢earlier clinical decision-making
➢ less inappropriate shocks and improved device
longevity
➢“hard” endpoints
❖Reduction of health care utilization
❖Decrease of urgent hospital admissions
❖Reduction in the length of cardiovascular hospitalizations
❖Decrease of mortality in ICD patients with heart failure

Isti
tuto
Auxolo
gico
Ital
iano
Parthiban et. Al.. JACC 2015; 65: 2591-2560

Isti
tuto
Auxolo
gico
Ital
iano
(J Am Coll Cardiol 2011;57:1181–9)
Isti
tuto
Auxolo
gico
Ital
iano
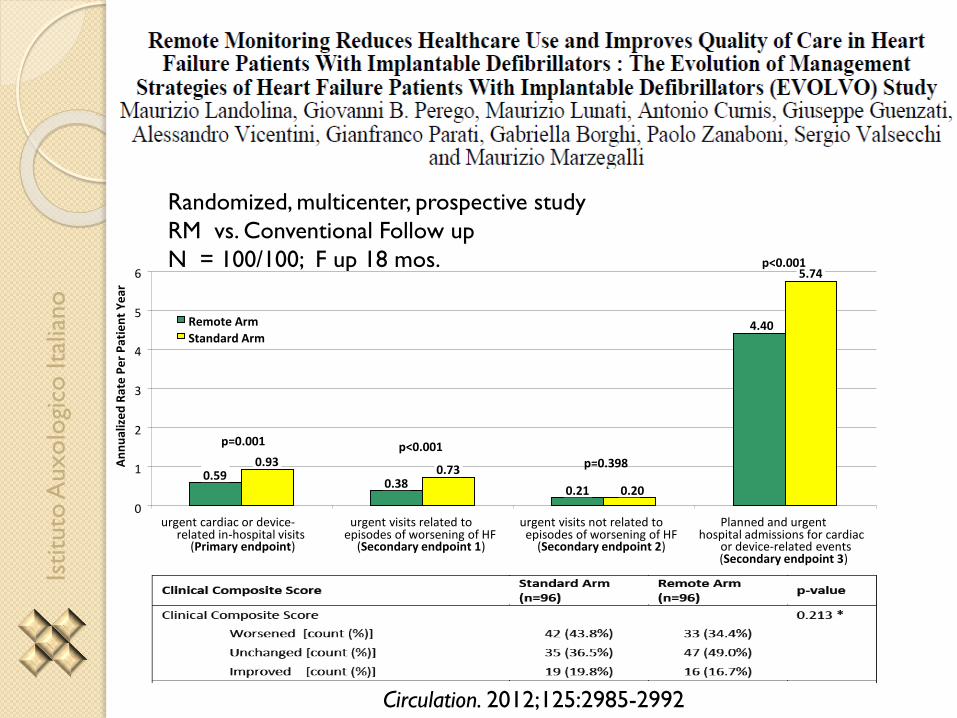
Circulation. 2012;125:2985-2992
Randomized, multicenter, prospective study
RM vs. Conventional Follow up
N = 100/100; F up 18 mos.
0.590.38
0.21
4.40
0.930.73
0.20
5.74
0
1
2
3
4
5
6
urgent cardiac or device-related in-hospital visits
(Primary endpoint)
urgent visits related toepisodes of worsening of HF
(Secondary endpoint 1)
urgent visits not related toepisodes of worsening of HF
(Secondary endpoint 2)
Planned and urgenthospital admissions for cardiac
or device-related events(Secondary endpoint 3)
An
nu
aliz
ed
Rat
e P
er
Pat
ien
t Y
ear
Remote Arm
Standard Arm
p=0.001 p<0.001p=0.398
p<0.001

Isti
tuto
Auxolo
gico
Ital
iano
Parthiban et. Al.. JACC 2015; 65: 2591-2560

Isti
tuto
Auxolo
gico
Ital
iano
European Heart Journal doi:10.1093/eurheartj/ehs425
«The proportion of patients whose battery was depleted at the end of the study
was .50% lower in the active than in the control group.»

Isti
tuto
Auxolo
gico
Ital
iano
• chronic heart failure lasting for at least 3 months
• New York Heart Association (NYHA) functional class II or III
• left ventricular ejection fraction 35% or less
• indication for dual-chamber ICD or CRT-D treatment according to European guidelines
Lancet 2014; 384: 583–90

Isti
tuto
Auxolo
gico
Ital
iano
Parthiban et. Al.. JACC 2015; 65: 2591-2560
Isti
tuto
Auxolo
gico
Ital
iano
Parthiban et. Al.. JACC 2015; 65: 2591-2560
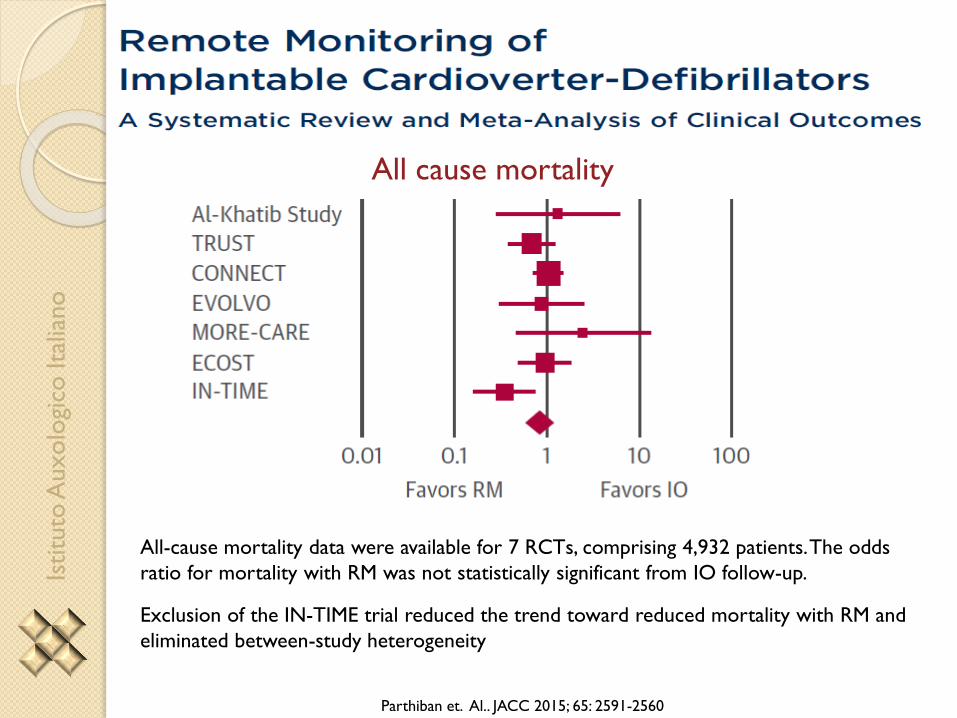
All cause mortality
All-cause mortality data were available for 7 RCTs, comprising 4,932 patients. The odds
ratio for mortality with RM was not statistically significant from IO follow-up.
Exclusion of the IN-TIME trial reduced the trend toward reduced mortality with RM and
eliminated between-study heterogeneity
Isti
tuto
Auxolo
gico
Ital
iano
Limits & pitfalls of RCTs
Single vendor:Are results technology-specific?
Strictly defined protocols:Active groups: are protocols applicable in real life ?
Control groups: do we unterestimate the benefit ?
Relatively small numbers
Impact of nurse counselling
Isti
tuto
Auxolo
gico
Ital
iano
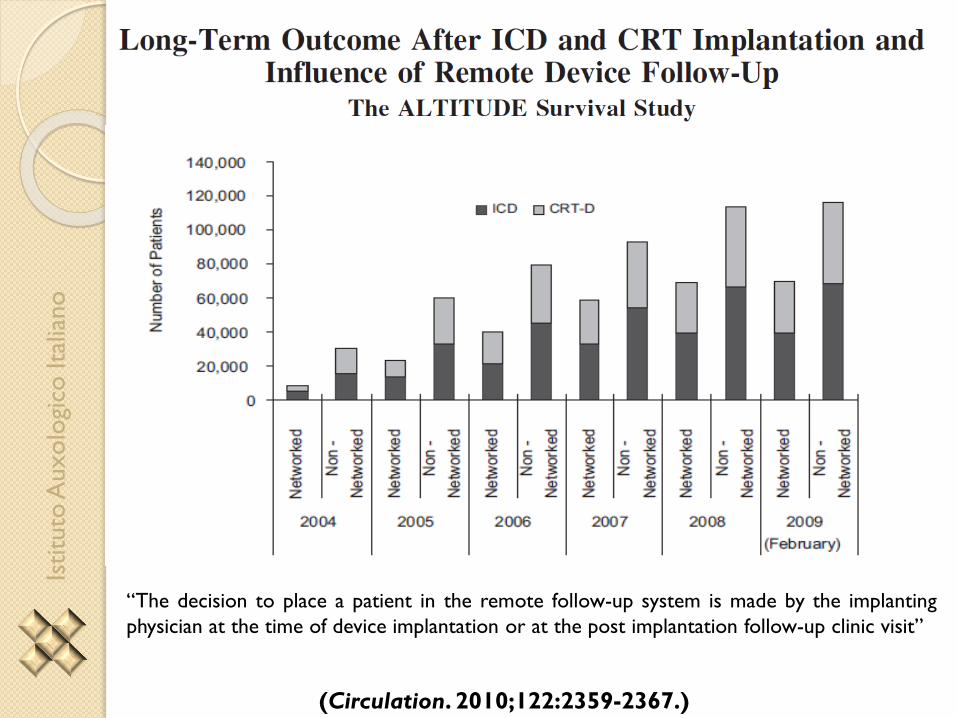
(Circulation. 2010;122:2359-2367.)
“The decision to place a patient in the remote follow-up system is made by the implanting
physician at the time of device implantation or at the post implantation follow-up clinic visit”

Isti
tuto
Auxolo
gico
Ital
iano
(Circulation. 2010;122:2359-2367.)
“To assess for possible physician referral bias that may influence the decision to refer a patient for
networked versus traditional device follow-up, patients followed on and off the network were further
compared by analysis of residential postal zip code. United States census data were then accessed to
determine and compare economic, racial, and educational status”
Networked vs. non networked
• White
• Rural
• Same age and sex
• Same educational level

Isti
tuto
Auxolo
gico
Ital
iano
(Circulation. 2010;122:2359-2367.)

Isti
tuto
Auxolo
gico
Ital
iano
(Circulation. 2010;122:2359-2367.)
Sensitivity analysis for ICDs cohort.
Scenarios of proportionate risk demonstrate that only if the risk factor burden in
the nonnetworked population were 5 times that of the networked patients would
imbalance in these baseline factors reproduce the mortality difference observed
(scenario 7; HR, 0.57).

Isti
tuto
Auxolo
gico
Ital
iano
Circ Arrhythm Electrophysiol. 2015;8:1173-1180
A limited data set constructed from Boston Scientific ALTITUDE Registry and National
Cardiovascular Data Registry ICD Registry between January 2006 and March 2010

Isti
tuto
Auxolo
gico
Ital
iano
Circ Arrhythm Electrophysiol. 2015;8:1173-1180
A limited data set constructed from Boston Scientific ALTITUDE Registry and National
Cardiovascular Data Registry ICD Registry between January 2006 and March 2010

Isti
tuto
Auxolo
gico
Ital
iano
Circ Arrhythm Electrophysiol. 2015;8:1173-1180
Effect of RPM Use on Survival and Rehospitalization at 3-Year Follow-Up
(Patients Without RPM Use Are the Reference)
Isti
tuto
Auxolo
gico
Ital
iano

Isti
tuto
Auxolo
gico
Ital
iano
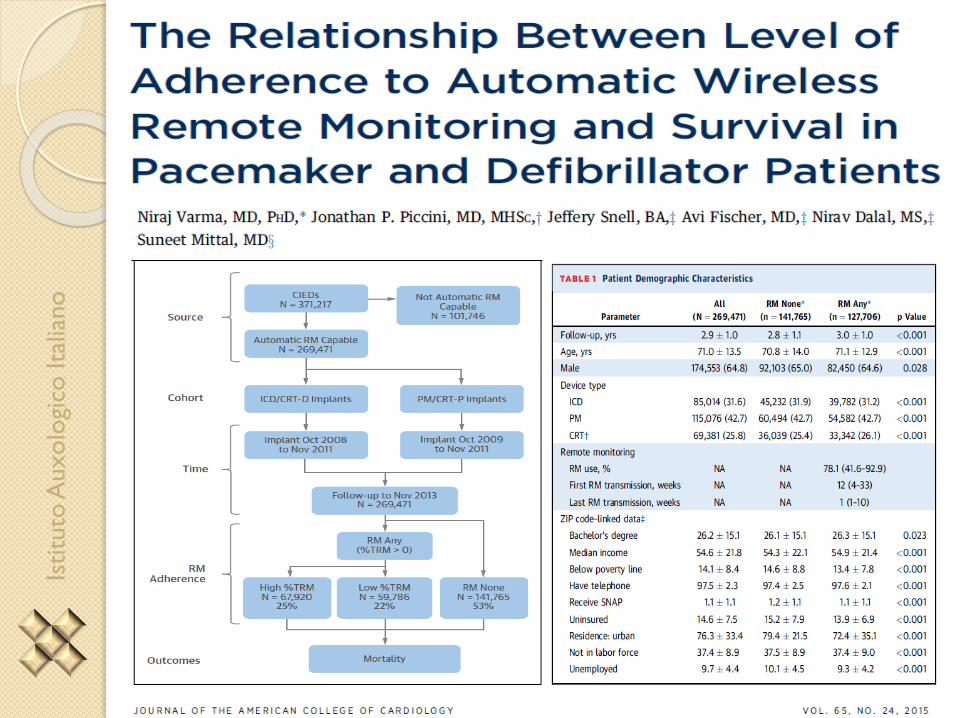
Aim:
To better understand the influence of RM on outcomes,
Hypothesis:
Survival would be better in patients with greater RM use and should apply to all
types of CIEDs: patients with pacemakers (PMs) who have less cardiovascular
risk as well as those with implantable cardioverter-defibrillators (ICDs) and
cardiac resynchronization therapy (CRT) with pacing/defibrillation capability
(CRT-P/CRT-D).
Method:
We tested this in a cohort of CIED patients, all receiving automatic RM devices,
by leveraging “big data” from a nationwide RM system generated proprietary
database, which collects comprehensive longitudinal follow-up data

Isti
tuto
Auxolo
gico
Ital
iano

Isti
tuto
Auxolo
gico
Ital
iano
Isti
tuto
Auxolo
gico
Ital
iano

Isti
tuto
Auxolo
gico
Ital
iano
JACC 2015; 65 (24): 2611-2613
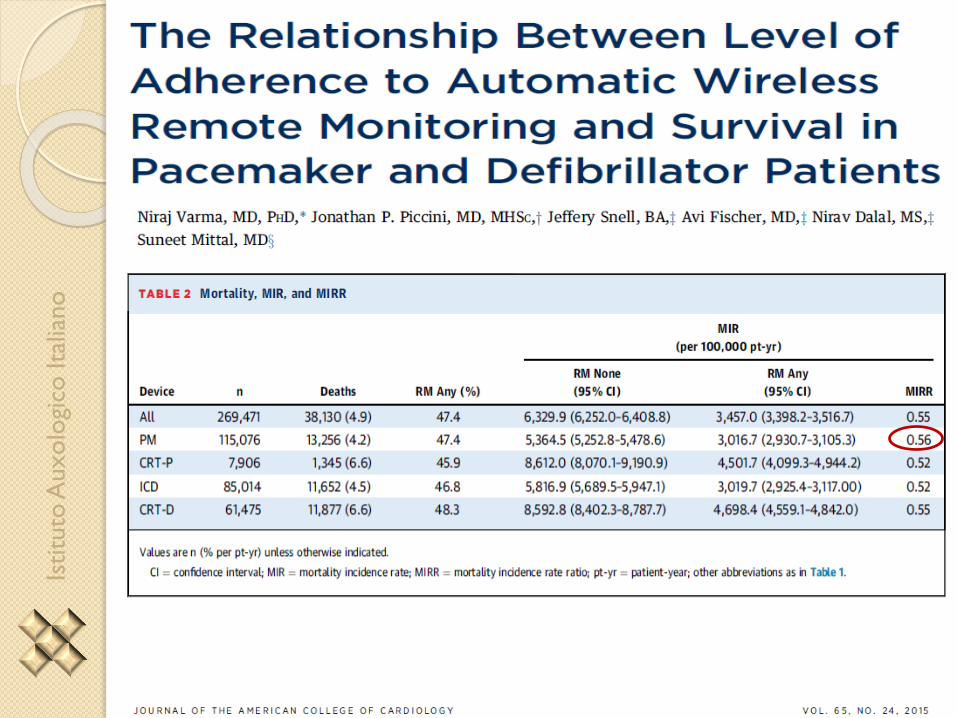
More than one-half (53%) of patients implanted with RM-capable devices never
used the RM functionality.
There was a survival advantage for those patients who used RM, and increased
use of RM with weekly transmissions more than 75% of the time was associated
with a greater survival advantage compared with those who used RM less
frequently. >>> Threshold effect ?
These results were consistent across all device types including PMs, ICDs, and
CRT devices
Isti
tuto
Auxolo
gico
Ital
iano
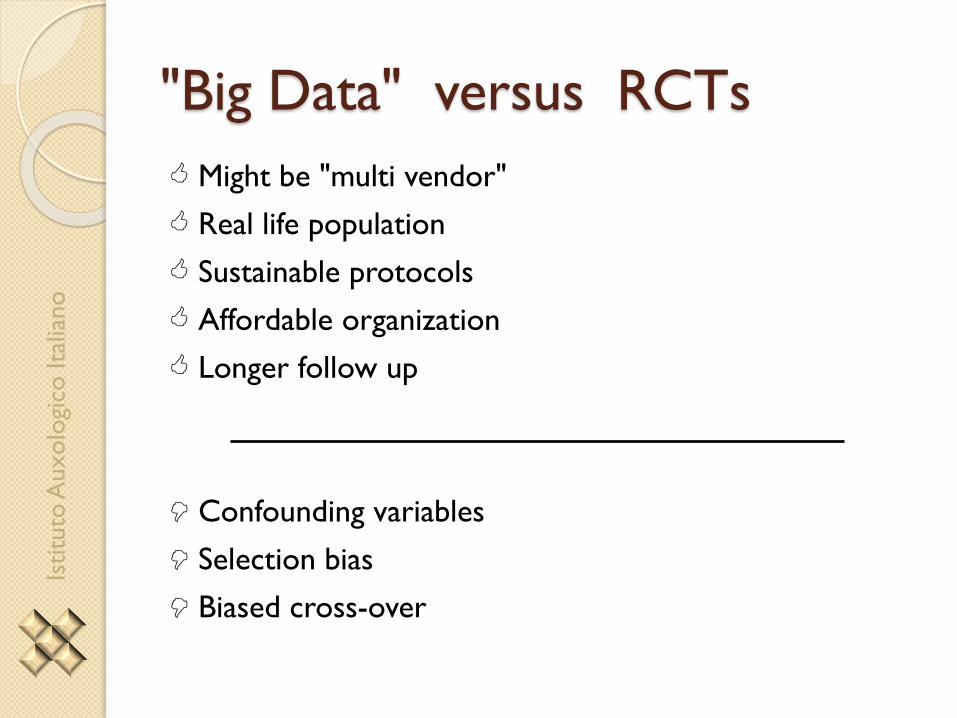
"Big Data" versus RCTs
Might be "multi vendor"
Real life population
Sustainable protocols
Affordable organization
Longer follow up
Confounding variables
Selection bias
Biased cross-over
Isti
tuto
Auxolo
gico
Ital
iano
Istituto Auxologico Italiano
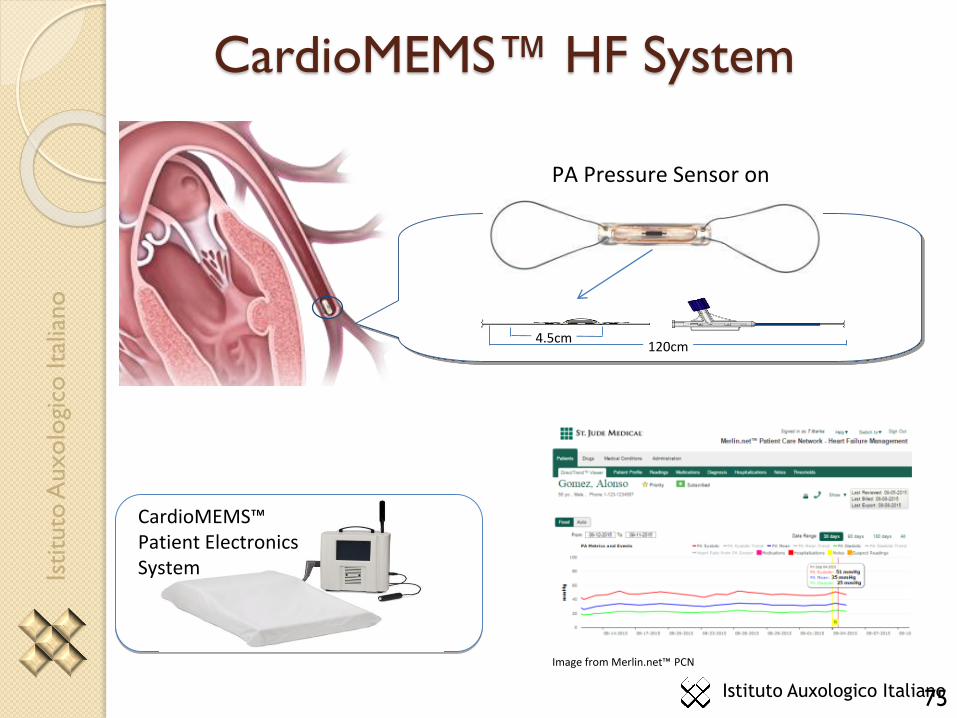
PA Pressure Sensor on Catheter Delivery System
CardioMEMS™ HF System
CardioMEMS™ Patient Electronics System
120cm4.5cm
Image from Merlin.net™ PCN
75

Isti
tuto
Auxolo
gico
Ital
iano
CardioMEMS Wireless Heart Failure Sensor
Regression Plot of Sensor vs. SG Mean
Pressure Measurements for All Patients
R2 = 0.9788
0
10
20
30
40
50
60
70
0 20 40 60 80
SG reading (mm Hg)
Sen
sor
read
ing
(m
m H
g)
Clinical evaluation has demonstrated safety, stability and excellent correlation to swan-ganz catheter

Isti
tuto
Auxolo
gico
Ital
iano
COMPASS –HF:
Acute decompensation prediction and ePAD
Zile ML et al.. J Cardiac Fail 2011;17:282e291
The product of small increases in pressure that occur over an extended period of time (PT) is the pressure-based hemodynamic factor most closely associated with the transition to acute decompensated heart failure.

Isti
tuto
Auxolo
gico
Ital
iano
COMPASS –HF: average ePAD
Stevenson LW et al.. Circ Heart Fail 2010;3;580-587
(…)many patients with advanced HF live on a plateau of high filling pressuresfrom which later events occur. This risk is progressively higher with higherchronic ambulatory pressures. It is not known whether more targetedintervention could maintain lower chronic ambulatory pressures and betteroutcomes.

Isti
tuto
Auxolo
gico
Ital
iano
CHAMPION Trial: By Targeting Pressure Ranges and Titrating Medications, Overall PAPs Can Be Reduced
Compared to the control group, patients managed with PAP had persistently lower mean PA pressures over the treatment period
CHAMPION Trial: PAP Mean Change from Baseline
Abraham WT, et al. Lancet, 2011.
PA
Me
an
Pre
as
ure
AU
C (
mm
Hg
-Da
ys
)
-220
-200
-180
-160
-140
-120
-100
-80
-60
-40
-20
0
20
40
60
80
100
Days from Implant
0 30 60 90 120 150 180
p = 0.0077
Treatment (-155.7 mmHg-Days)Control (33.1 mmHg-Days)
Isti
tuto
Auxolo
gico
Ital
iano
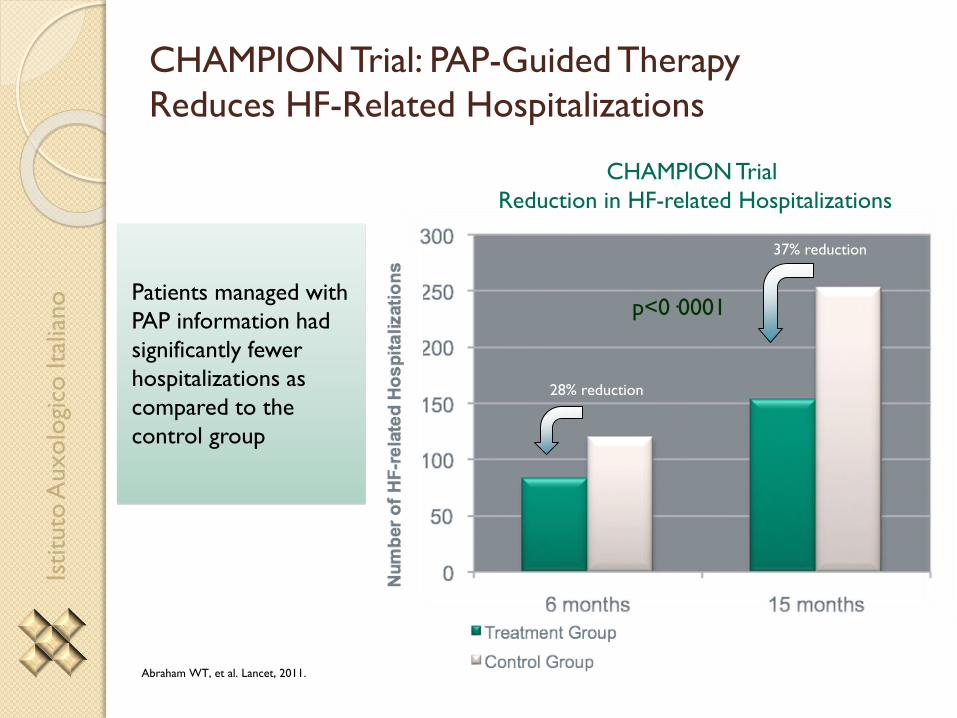
28% reduction
37% reduction
CHAMPION Trial: PAP-Guided Therapy
Reduces HF-Related Hospitalizations
CHAMPION Trial
Reduction in HF-related Hospitalizations
p<0·0001
Abraham WT, et al. Lancet, 2011.
Patients managed with
PAP information had
significantly fewer
hospitalizations as
compared to the
control group
Isti
tuto
Auxolo
gico
Ital
iano
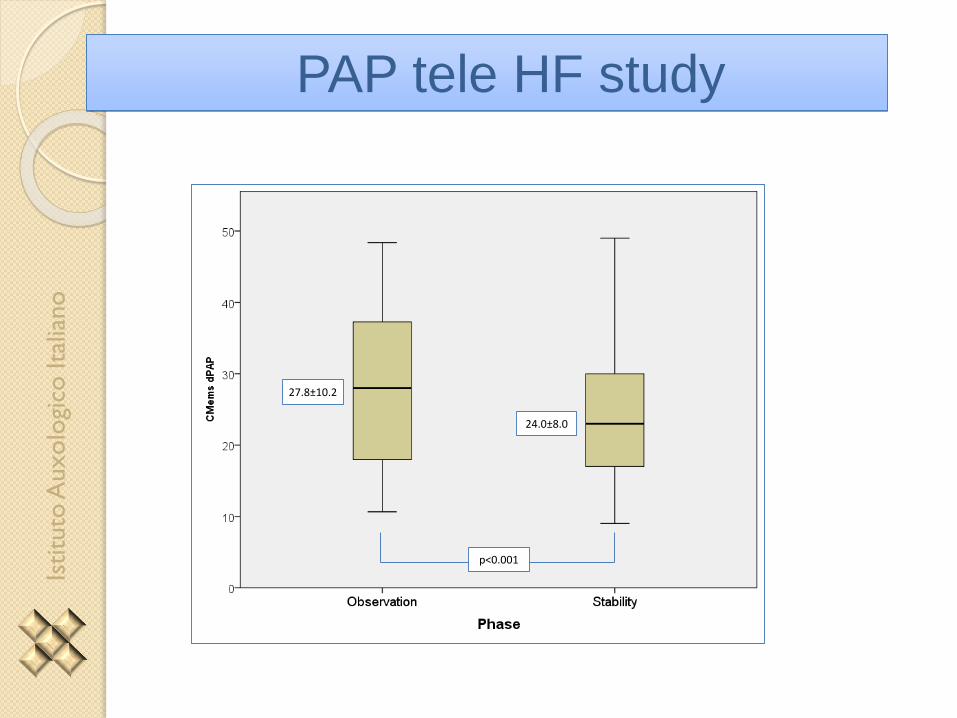
PAP tele HF study
27.8±10.2
24.0±8.0
p<0.001

Isti
tuto
Auxolo
gico
Ital
iano
Conclusioni
Related Documents











