Modified Grid Laser Photocoagulation Versus Pars Plana Vitrectomy With Internal Limiting Membrane Removal in Diabetic Macular Edema ATES YANYALI, MD, AHMET F. NOHUTCU, MD, FATIH HOROZOGLU, MD, AND ERKAN CELIK, MD ● PURPOSE: To compare the effectiveness of pars plana vitrectomy (PPV) and removal of the internal limiting membrane (ILM) with modified grid laser photocoagula- tion in diabetic macular edema. ● DESIGN: Randomized, comparative, interventional study. ● METHODS: In this prospective study, 24 eyes of 12 patients with bilateral diabetic macular edema were eval- uated. PPV with removal of the ILM was performed at random in one eye of 12 patients (ILM group), and a single session of modified grid laser photocoagulation was performed in the fellow eyes (grid group). Main outcome measures were the foveal thickness measured with opti- cal coherence tomography, preoperative, and postopera- tive visual acuities. Mann-Whitney U and Wilcoxon tests were used in statistical analysis. ● RESULTS: All patients were followed up for 6 months. In the ILM group, mean foveal thickness was 439.2 106.5 m preoperatively and 219.8 63.2 m postop- eratively (P .002). In the grid group, mean foveal thickness was 407 100.2 m preoperatively and 378.5 141.6 m postoperatively (P .433). A mean decrease in foveal thickness was found to be 219.4 127.6 m in the ILM group and 28.5 90.5 m in the grid group (P .001). In the ILM group, best-corrected logMAR visual acuity was 0.75 0.41 preoperatively and 0.53 0.41 postoperatively (P .006). In the grid group, best-corrected logMAR visual acuity was 0.59 0.27 preoperatively and 0.49 0.27 postoperatively (P .058). Visual acuity improved by 2 or more lines in six eyes (50%) in the ILM group and in three eyes (25%) in the grid group. Visual acuity remained stable in six eyes (50%) in the ILM group and in nine eyes (75%) in the grid group. ● CONCLUSIONS: PPV with ILM removal appears to be more effective than a single session of modified grid laser photocoagulation in the treatment of diabetic macular edema. Further studies with a large number of patients are required for a more reliable conclusion. (Am J Ophthalmol 2005;139:795– 801. © 2005 by Elsevier Inc. All rights reserved.) D IABETIC MACULAR EDEMA IS THE MAJOR CAUSE of visual loss in diabetic patients. 1 The Early Treatment Diabetic Retinopathy Study Research Group has shown that focal laser photocoagulation reduces the risk of moderate visual loss by 50% in eyes with clinically significant diabetic macular edema. 2 In diabetic macular edema, it has been reported that grid laser pho- tocoagulation stabilizes or improves best-corrected visual acuity in 75.4% of eyes, whereas 24.6% of eyes experience loss of vision after 3 years’ follow-up. 3 In recent studies, pars plana vitrectomy (PPV), with or without internal limiting membrane (ILM) removal, has been reported to decrease macular edema and to improve visual acuity in patients with diabetic macular edema 4–8 The purpose of this prospective study was to compare the effectiveness of modified grid laser photocoagulation and PPV with removal of the ILM in diabetic macular edema. PATIENTS AND METHODS IN THIS PROSPECTIVE STUDY, 24 EYES OF 12 PATIENTS WITH bilateral diabetic macular edema were evaluated between May 2002 and April 2004. Diabetic macular edema was defined as retinal thickening of two or more disk areas involving the foveal avascular zone with or without cystoid Accepted for publication Dec 3, 2004. From the Department of Ophthalmology, Haydarpasa Numune Edu- cation and Research Hospital, Istanbul, Turkey. This study was presented at the meeting of the European Vitreo Retinal Society, Istanbul, Turkey, September 2004. Inquiries to Ates Yanyali, MD, Topagac sok, Akarsu Apt. No. 3/13, Caddebostan, Turkey; fax: (90) 212 275 40 64; e-mail: ayanyali@hotmail. com © 2005 BY ELSEVIER INC.ALL RIGHTS RESERVED. 0002-9394/05/$30.00 795 doi:10.1016/j.ajo.2004.12.017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
●
vmt●
s●
purspmctw●
I1et�d1glag0�e
A
c
S
Cc
0d
Modified Grid Laser Photocoagulation VersusPars Plana Vitrectomy With Internal Limiting
Membrane Removal in DiabeticMacular Edema
ATES YANYALI, MD, AHMET F. NOHUTCU, MD, FATIH HOROZOGLU, MD,
AND ERKAN CELIK, MDt(g●
mpeaOI
DGtcmtal
wbvTeP
I
bMd
PURPOSE: To compare the effectiveness of pars planaitrectomy (PPV) and removal of the internal limitingembrane (ILM) with modified grid laser photocoagula-
ion in diabetic macular edema.DESIGN: Randomized, comparative, interventional
tudy.METHODS: In this prospective study, 24 eyes of 12
atients with bilateral diabetic macular edema were eval-ated. PPV with removal of the ILM was performed atandom in one eye of 12 patients (ILM group), and aingle session of modified grid laser photocoagulation waserformed in the fellow eyes (grid group). Main outcomeeasures were the foveal thickness measured with opti-
al coherence tomography, preoperative, and postopera-ive visual acuities. Mann-Whitney U and Wilcoxon testsere used in statistical analysis.RESULTS: All patients were followed up for 6 months.
n the ILM group, mean foveal thickness was 439.2 �06.5 �m preoperatively and 219.8 � 63.2 �m postop-ratively (P � .002). In the grid group, mean fovealhickness was 407 � 100.2 �m preoperatively and 378.5
141.6 �m postoperatively (P � .433). A meanecrease in foveal thickness was found to be 219.4 �27.6 �m in the ILM group and 28.5 � 90.5 �m in therid group (P � .001). In the ILM group, best-correctedogMAR visual acuity was 0.75 � 0.41 preoperativelynd 0.53 � 0.41 postoperatively (P � .006). In the gridroup, best-corrected logMAR visual acuity was 0.59 �.27 preoperatively and 0.49 � 0.27 postoperatively (P.058). Visual acuity improved by 2 or more lines in six
yes (50%) in the ILM group and in three eyes (25%) in
ccepted for publication Dec 3, 2004.From the Department of Ophthalmology, Haydarpasa Numune Edu-
ation and Research Hospital, Istanbul, Turkey.This study was presented at the meeting of the European Vitreo Retinal
ociety, Istanbul, Turkey, September 2004.Inquiries to Ates Yanyali, MD, Topagac sok, Akarsu Apt. No. 3/13,
iaddebostan, Turkey; fax: � (90) 212 275 40 64; e-mail: ayanyali@hotmail.
om
© 2005 BY ELSEVIER INC. A002-9394/05/$30.00oi:10.1016/j.ajo.2004.12.017
he grid group. Visual acuity remained stable in six eyes50%) in the ILM group and in nine eyes (75%) in therid group.CONCLUSIONS: PPV with ILM removal appears to beore effective than a single session of modified grid laserhotocoagulation in the treatment of diabetic maculardema. Further studies with a large number of patientsre required for a more reliable conclusion. (Am Jphthalmol 2005;139:795–801. © 2005 by Elsevier
nc. All rights reserved.)
IABETIC MACULAR EDEMA IS THE MAJOR CAUSE
of visual loss in diabetic patients.1 The EarlyTreatment Diabetic Retinopathy Study Research
roup has shown that focal laser photocoagulation reduceshe risk of moderate visual loss by 50% in eyes withlinically significant diabetic macular edema.2 In diabeticacular edema, it has been reported that grid laser pho-
ocoagulation stabilizes or improves best-corrected visualcuity in 75.4% of eyes, whereas 24.6% of eyes experienceoss of vision after 3 years’ follow-up.3
In recent studies, pars plana vitrectomy (PPV), with orithout internal limiting membrane (ILM) removal, haseen reported to decrease macular edema and to improveisual acuity in patients with diabetic macular edema4–8
he purpose of this prospective study was to compare theffectiveness of modified grid laser photocoagulation andPV with removal of the ILM in diabetic macular edema.
PATIENTS AND METHODS
N THIS PROSPECTIVE STUDY, 24 EYES OF 12 PATIENTS WITH
ilateral diabetic macular edema were evaluated betweenay 2002 and April 2004. Diabetic macular edema was
efined as retinal thickening of two or more disk areas
nvolving the foveal avascular zone with or without cystoidLL RIGHTS RESERVED. 795
ccishEwet(mutihogsvehtfpiraatIs
egmgr
v
(Tawawssaaot
dFcseddhNpc
�dscIM
(Aatwg
7
hanges attributable to diffuse leakage from dilated retinalapillaries, retinal pigment epithelium, and ischemic ret-na. Patients with bilateral diabetic macular edema, dia-tolic blood pressure less than 100 mm Hg, glycosylatedemoglobin equal to or less than 10 mg/dl were included.yes that met the following criteria were excluded: (1)ith unilateral macular edema; (2) with only focal maculardema attributable to focal leaks from microaneurysms; (3)reated previously with macular laser photocoagulation;4) treated with panretinal photocoagulation within 12onths; (5) that underwent vitreoretinal surgery; (6) that
nderwent cataract surgery within 12 months; (7) withraction retinal detachment; (8) with active neovascular-zation; (9) with media opacity such as cataract or vitreousemorrhage; (10) with angiographic evidence of wideningr irregularity of the foveal avascular zone; (11) withreater than 6 clock-hours of macular capillary nonperfu-ion in fluorescein angiography; and (12) with evidence ofitreomacular traction. None of the eyes showed anyvidence of epiretinal membrane, thickening of posterioryaloid, or incomplete posterior vitreous detachment withraction and detachment of the macula in preoperativeundus and optical coherence tomography (OCT, Hum-hrey Instruments, San Leandro, California, USA) exam-nations. Patients with chronic renal failure maintained onenal dialysis were excluded as well. The possible meritsnd risks of the treatment were explained to the patients,nd an informed consent was obtained in accordance withhe Helsinki Declaration before inclusion in the study. Nonstitutional Review Board approval was required for thistudy.
PPV with ILM removal was performed unilaterally in 12yes of 12 patients, and these eyes were defined as the ILMroup. The fellow eyes treated with a single session ofodified grid laser photocoagulation were defined as the
rid group. The eye to be treated with PPV and ILMemoval was selected at random.
Preoperative and postoperative best-corrected Snellen
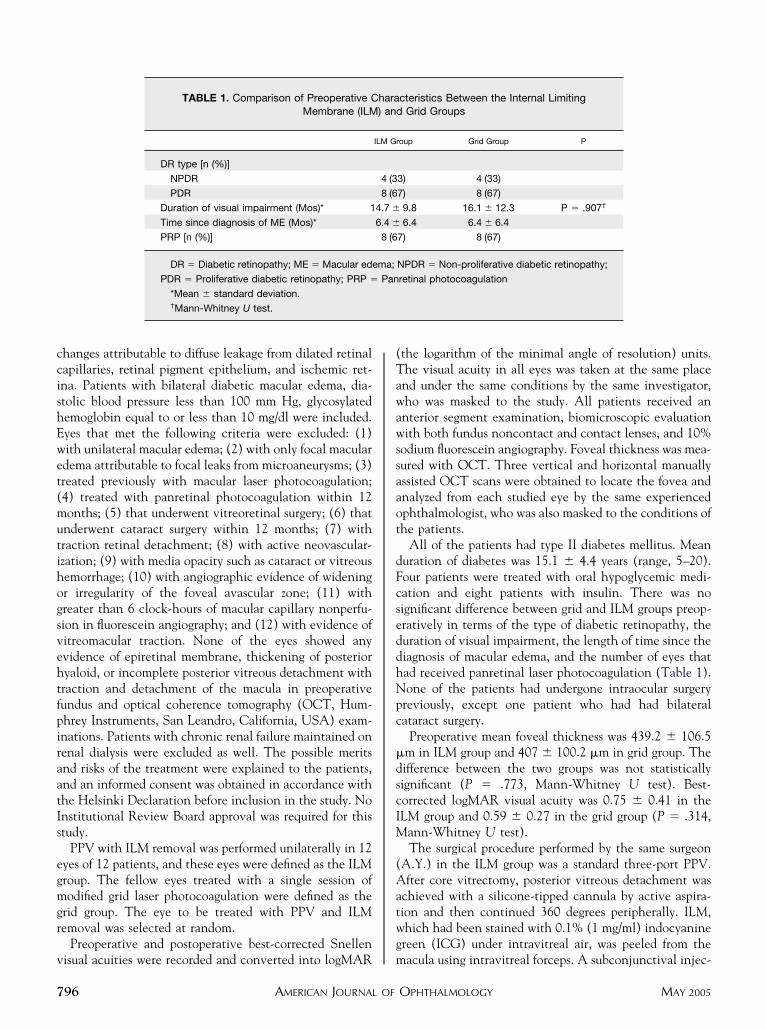
TABLE 1. Comparison of Preoperative CMembrane (ILM
DR type [n (%)]
NPDR
PDR
Duration of visual impairment (Mos)* 1
Time since diagnosis of ME (Mos)*
PRP [n (%)]
DR � Diabetic retinopathy; ME � Macular ed
PDR � Proliferative diabetic retinopathy; PRP �
*Mean � standard deviation.†Mann-Whitney U test.
isual acuities were recorded and converted into logMAR m
AMERICAN JOURNAL OF96
the logarithm of the minimal angle of resolution) units.he visual acuity in all eyes was taken at the same placend under the same conditions by the same investigator,ho was masked to the study. All patients received annterior segment examination, biomicroscopic evaluationith both fundus noncontact and contact lenses, and 10%
odium fluorescein angiography. Foveal thickness was mea-ured with OCT. Three vertical and horizontal manuallyssisted OCT scans were obtained to locate the fovea andnalyzed from each studied eye by the same experiencedphthalmologist, who was also masked to the conditions ofhe patients.
All of the patients had type II diabetes mellitus. Meanuration of diabetes was 15.1 � 4.4 years (range, 5–20).our patients were treated with oral hypoglycemic medi-ation and eight patients with insulin. There was noignificant difference between grid and ILM groups preop-ratively in terms of the type of diabetic retinopathy, theuration of visual impairment, the length of time since theiagnosis of macular edema, and the number of eyes thatad received panretinal laser photocoagulation (Table 1).one of the patients had undergone intraocular surgery
reviously, except one patient who had had bilateralataract surgery.
Preoperative mean foveal thickness was 439.2 � 106.5m in ILM group and 407 � 100.2 �m in grid group. Theifference between the two groups was not statisticallyignificant (P � .773, Mann-Whitney U test). Best-orrected logMAR visual acuity was 0.75 � 0.41 in theLM group and 0.59 � 0.27 in the grid group (P � .314,
ann-Whitney U test).The surgical procedure performed by the same surgeon
A.Y.) in the ILM group was a standard three-port PPV.fter core vitrectomy, posterior vitreous detachment was
chieved with a silicone-tipped cannula by active aspira-ion and then continued 360 degrees peripherally. ILM,hich had been stained with 0.1% (1 mg/ml) indocyaninereen (ICG) under intravitreal air, was peeled from the
cteristics Between the Internal LimitingGrid Groups
oup Grid Group P
3) 4 (33)
7) 8 (67)
9.8 16.1 � 12.3 P � .907†
6.4 6.4 � 6.4
7) 8 (67)
NPDR � Non-proliferative diabetic retinopathy;
retinal photocoagulation
hara) and
ILM Gr
4 (3
8 (6
4.7 �
6.4 �
8 (6
ema;
Pan
acula using intravitreal forceps. A subconjunctival injec-
OPHTHALMOLOGY MAY 2005
tNt
wsspf1afl22itfltwe
1Omnfictwt
eI
et
O
wApmiI1et3W
bpTmmo
1gdim
V
ion of gentamicin was performed at the end of the surgery.one of the eyes received periocular corticosteroid injec-
ion at the time of the surgery.In the grid group, modified grid laser photocoagulation
as performed under topical anesthesia by the sameurgeon (A.Y.), as described by Olk.9 One-hundred micronpots were applied for two to three rows around thearafoveal region up to and including the edge of theoveal avascular zone, placing the lesions approximately00 �m apart. Two-hundred micron spots were thenpplied throughout all areas of leakage seen on theuorescein angiogram, placing the lesions approximately00 �m apart. In areas of obvious focal leakage, additional00-�m spots were confluently applied. Average settingsncluded 50 to 100 100-�m spots at 75 to 100 mW and 200o 500 200-�m spots at 100 to 200 mW. A recentuorescein angiogram was used as a guide during thereatment session. All eyes in the grid group were treatedith argon green laser (514 nm, Ultima 2000 SE Coher-nt). None of them received supplemental treatment.
Patients were examined postoperatively at 1 day, 3 days,week, 1 month, 6 months, and every 6 months thereafter.CT measurements were recorded postoperatively at 1onth and 6 months. In the ILM group, topical pred-isolone acetate was administered six times a day in therst 2 weeks and then four times a day for 6 weeks,iprofloxacin six times a day for 2 weeks, and tropicamidehree times a day for 4 weeks. Topical prednisolone acetateas administered six times a day in the first 2 weeks and
hen four times a day for 6 weeks in the grid group.Main outcome measures were; preoperative and postop-
rative visual acuity and foveal thickness changes in the
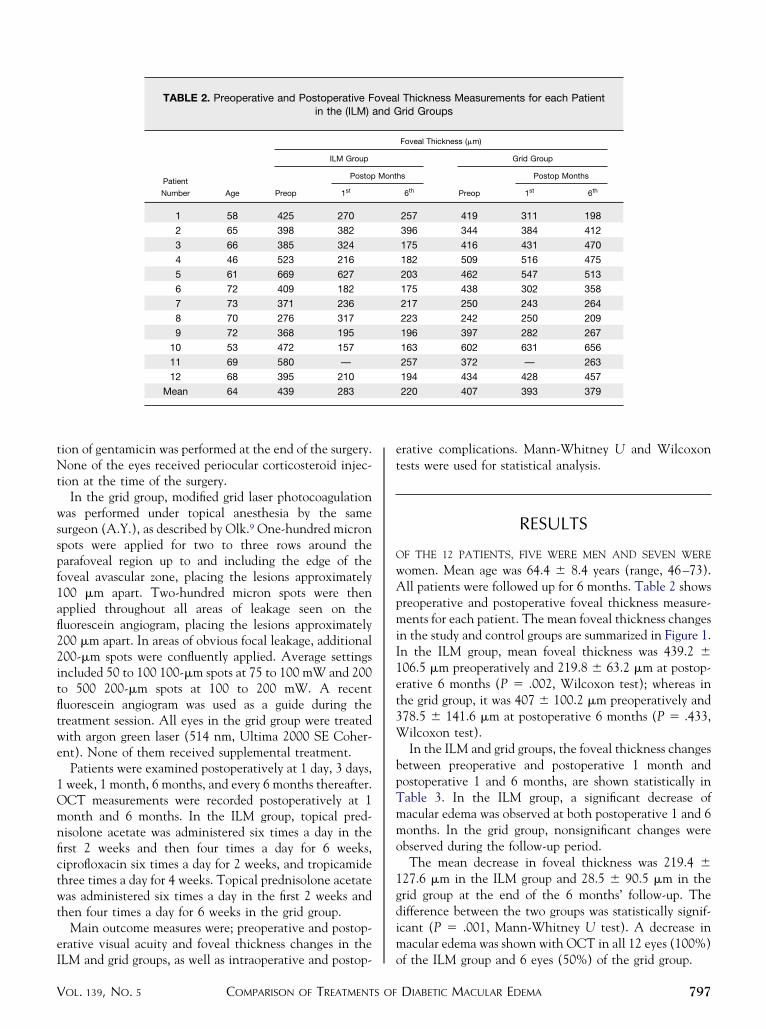
TABLE 2. Preoperative and Postoperative Fin the (ILM) a
Patient
Number Age
ILM Group
Preop
Postop
1st
1 58 425 270
2 65 398 382
3 66 385 324
4 46 523 216
5 61 669 627
6 72 409 182
7 73 371 236
8 70 276 317
9 72 368 195
10 53 472 157
11 69 580 —
12 68 395 210
Mean 64 439 283
LM and grid groups, as well as intraoperative and postop- o
COMPARISON OF TREATMENTS OFOL. 139, NO. 5
rative complications. Mann-Whitney U and Wilcoxonests were used for statistical analysis.
RESULTS
F THE 12 PATIENTS, FIVE WERE MEN AND SEVEN WERE
omen. Mean age was 64.4 � 8.4 years (range, 46–73).ll patients were followed up for 6 months. Table 2 shows
reoperative and postoperative foveal thickness measure-ents for each patient. The mean foveal thickness changes
n the study and control groups are summarized in Figure 1.n the ILM group, mean foveal thickness was 439.2 �06.5 �m preoperatively and 219.8 � 63.2 �m at postop-rative 6 months (P � .002, Wilcoxon test); whereas inhe grid group, it was 407 � 100.2 �m preoperatively and78.5 � 141.6 �m at postoperative 6 months (P � .433,
ilcoxon test).In the ILM and grid groups, the foveal thickness changes
etween preoperative and postoperative 1 month andostoperative 1 and 6 months, are shown statistically inable 3. In the ILM group, a significant decrease ofacular edema was observed at both postoperative 1 and 6onths. In the grid group, nonsignificant changes were
bserved during the follow-up period.The mean decrease in foveal thickness was 219.4 �
27.6 �m in the ILM group and 28.5 � 90.5 �m in therid group at the end of the 6 months’ follow-up. Theifference between the two groups was statistically signif-cant (P � .001, Mann-Whitney U test). A decrease inacular edema was shown with OCT in all 12 eyes (100%)
l Thickness Measurements for each Patientrid Groups
Foveal Thickness (�m)
Grid Group
hs
Preop
Postop Months
6th 1st 6th
257 419 311 198
396 344 384 412
175 416 431 470
182 509 516 475
203 462 547 513
175 438 302 358
217 250 243 264
223 242 250 209
196 397 282 267
163 602 631 656
257 372 — 263
194 434 428 457
220 407 393 379
oveand G
Mont
f the ILM group and 6 eyes (50%) of the grid group.
DIABETIC MACULAR EDEMA 797
abp(.ca.mgva
gt
tsgttp
I
cwmbi
(a�etctsatroIrzewttm
mtweCdttfilmtms
Fam
7
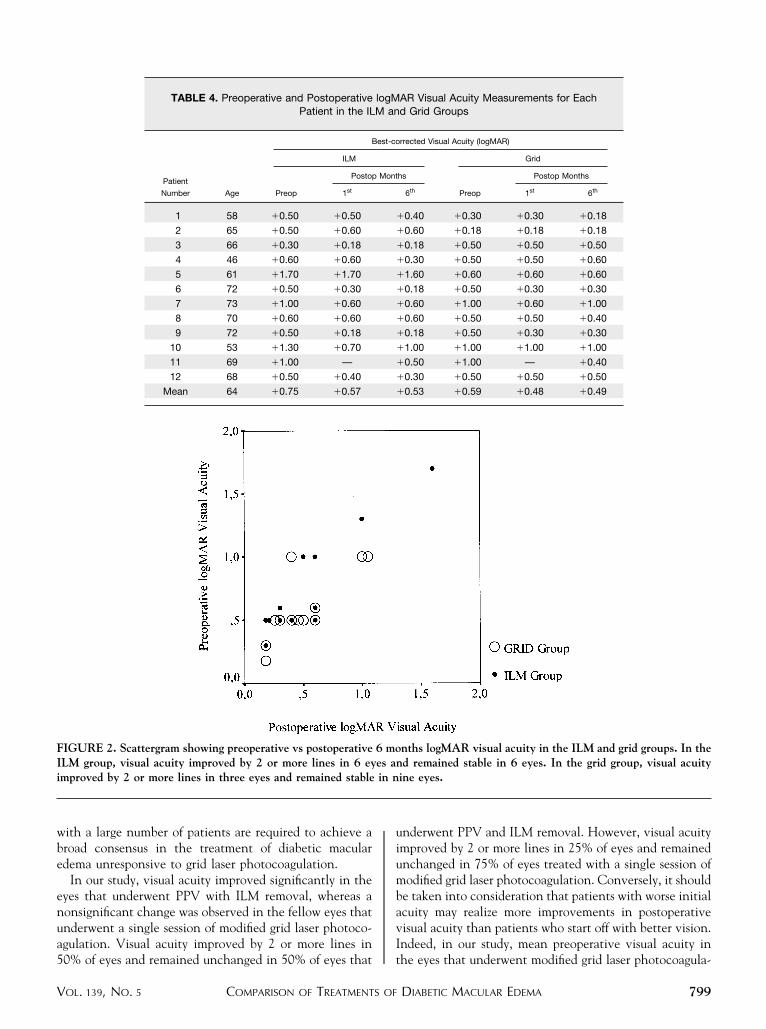
Table 4 shows the preoperative and postoperative visualcuity measurements for each patient. In the ILM group,est-corrected logMAR visual acuity was 0.75 � 0.41reoperatively and 0.53 � 0.41 at postoperative 6 monthsFigure 2). The difference was statistically significant (P �006, Wilcoxon test). However, in the grid group, best-orrected logMAR visual acuity was 0.59 � 0.27 preoper-tively and 0.49 � 0.27 at postoperative 6 months (P �058, Wilcoxon test). The statistical difference in improve-
ent of logMAR visual acuity between the ILM and gridroups was not significant (P � .061). In the ILM group,isual acuity improved by 2 or more lines in six eyes (50%)
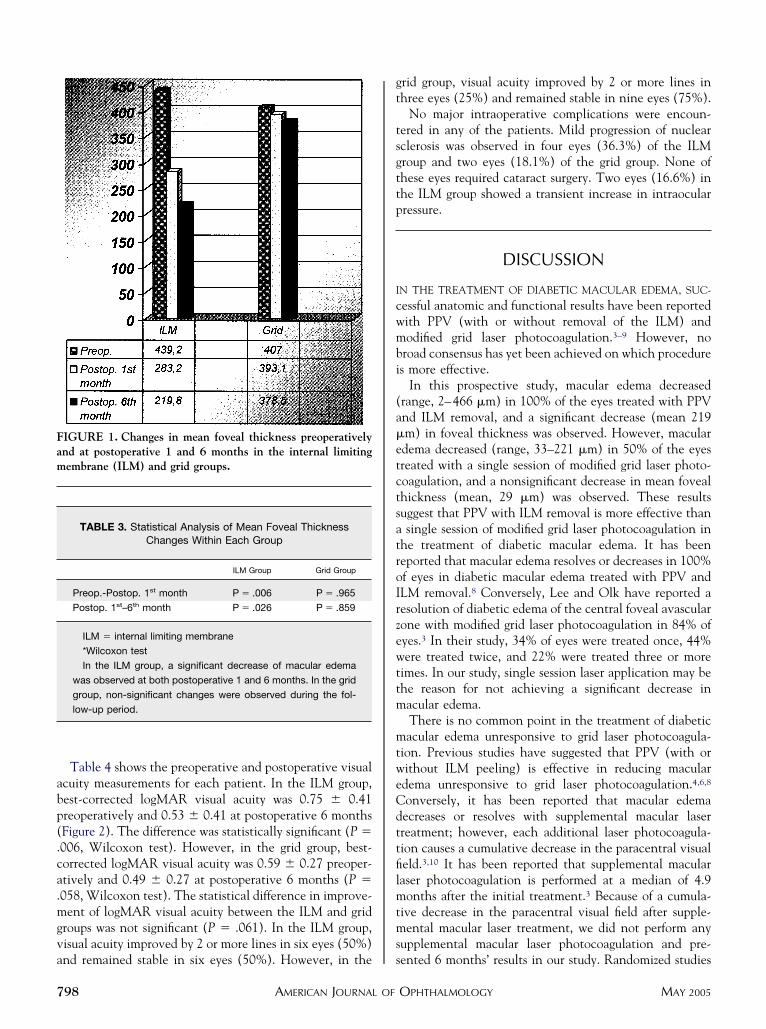
IGURE 1. Changes in mean foveal thickness preoperativelynd at postoperative 1 and 6 months in the internal limitingembrane (ILM) and grid groups.
TABLE 3. Statistical Analysis of Mean Foveal ThicknessChanges Within Each Group
ILM Group Grid Group
Preop.-Postop. 1st month P � .006 P � .965
Postop. 1st–6th month P � .026 P � .859
ILM � internal limiting membrane
*Wilcoxon test
In the ILM group, a significant decrease of macular edema
was observed at both postoperative 1 and 6 months. In the grid
group, non-significant changes were observed during the fol-
low-up period.
nd remained stable in six eyes (50%). However, in the s
AMERICAN JOURNAL OF98
rid group, visual acuity improved by 2 or more lines inhree eyes (25%) and remained stable in nine eyes (75%).
No major intraoperative complications were encoun-ered in any of the patients. Mild progression of nuclearclerosis was observed in four eyes (36.3%) of the ILMroup and two eyes (18.1%) of the grid group. None ofhese eyes required cataract surgery. Two eyes (16.6%) inhe ILM group showed a transient increase in intraocularressure.
DISCUSSION
N THE TREATMENT OF DIABETIC MACULAR EDEMA, SUC-
essful anatomic and functional results have been reportedith PPV (with or without removal of the ILM) andodified grid laser photocoagulation.3–9 However, no
road consensus has yet been achieved on which procedures more effective.
In this prospective study, macular edema decreasedrange, 2–466 �m) in 100% of the eyes treated with PPVnd ILM removal, and a significant decrease (mean 219m) in foveal thickness was observed. However, maculardema decreased (range, 33–221 �m) in 50% of the eyesreated with a single session of modified grid laser photo-oagulation, and a nonsignificant decrease in mean fovealhickness (mean, 29 �m) was observed. These resultsuggest that PPV with ILM removal is more effective thansingle session of modified grid laser photocoagulation in
he treatment of diabetic macular edema. It has beeneported that macular edema resolves or decreases in 100%f eyes in diabetic macular edema treated with PPV andLM removal.8 Conversely, Lee and Olk have reported aesolution of diabetic edema of the central foveal avascularone with modified grid laser photocoagulation in 84% ofyes.3 In their study, 34% of eyes were treated once, 44%ere treated twice, and 22% were treated three or more
imes. In our study, single session laser application may behe reason for not achieving a significant decrease inacular edema.There is no common point in the treatment of diabeticacular edema unresponsive to grid laser photocoagula-
ion. Previous studies have suggested that PPV (with orithout ILM peeling) is effective in reducing maculardema unresponsive to grid laser photocoagulation.4,6,8
onversely, it has been reported that macular edemaecreases or resolves with supplemental macular laserreatment; however, each additional laser photocoagula-ion causes a cumulative decrease in the paracentral visualeld.3,10 It has been reported that supplemental macularaser photocoagulation is performed at a median of 4.9onths after the initial treatment.3 Because of a cumula-
ive decrease in the paracentral visual field after supple-ental macular laser treatment, we did not perform any
upplemental macular laser photocoagulation and pre-
ented 6 months’ results in our study. Randomized studiesOPHTHALMOLOGY MAY 2005
wbe
enua5
uiumbavI
�
FIi
V
ith a large number of patients are required to achieve aroad consensus in the treatment of diabetic maculardema unresponsive to grid laser photocoagulation.
In our study, visual acuity improved significantly in theyes that underwent PPV with ILM removal, whereas aonsignificant change was observed in the fellow eyes thatnderwent a single session of modified grid laser photoco-gulation. Visual acuity improved by 2 or more lines in
TABLE 4. Preoperative and PostoperativePatient in the IL
Patient
Number Age
B
ILM
Preop
Postop
1st
1 58 �0.50 �0.50
2 65 �0.50 �0.60
3 66 �0.30 �0.18
4 46 �0.60 �0.60
5 61 �1.70 �1.70
6 72 �0.50 �0.30
7 73 �1.00 �0.60
8 70 �0.60 �0.60
9 72 �0.50 �0.18
10 53 �1.30 �0.70
11 69 �1.00 —
12 68 �0.50 �0.40
Mean 64 �0.75 �0.57
IGURE 2. Scattergram showing preoperative vs postoperativeLM group, visual acuity improved by 2 or more lines in 6 eymproved by 2 or more lines in three eyes and remained stable
0% of eyes and remained unchanged in 50% of eyes that t
COMPARISON OF TREATMENTS OFOL. 139, NO. 5
nderwent PPV and ILM removal. However, visual acuitymproved by 2 or more lines in 25% of eyes and remainednchanged in 75% of eyes treated with a single session ofodified grid laser photocoagulation. Conversely, it should
e taken into consideration that patients with worse initialcuity may realize more improvements in postoperativeisual acuity than patients who start off with better vision.ndeed, in our study, mean preoperative visual acuity in
AR Visual Acuity Measurements for Eachd Grid Groups
rrected Visual Acuity (logMAR)
Grid
hs
Preop
Postop Months
6th 1st 6th
0.40 �0.30 �0.30 �0.18
0.60 �0.18 �0.18 �0.18
0.18 �0.50 �0.50 �0.50
0.30 �0.50 �0.50 �0.60
1.60 �0.60 �0.60 �0.60
0.18 �0.50 �0.30 �0.30
0.60 �1.00 �0.60 �1.00
0.60 �0.50 �0.50 �0.40
0.18 �0.50 �0.30 �0.30
1.00 �1.00 �1.00 �1.00
0.50 �1.00 — �0.40
0.30 �0.50 �0.50 �0.50
0.53 �0.59 �0.48 �0.49
nths logMAR visual acuity in the ILM and grid groups. In thed remained stable in 6 eyes. In the grid group, visual acuity
ine eyes.
logMM an
est-co
Mont
�
�
�
�
�
�
�
�
�
�
�
�
6 moes anin n
he eyes that underwent modified grid laser photocoagula-
DIABETIC MACULAR EDEMA 799
tIesralImsoe
stStptcupDmtieaAtvomnuPc
owwBamwo(ePrpldrbp
PlrutbgvaP
blla
1
1
8
ion was better than in the eyes that underwent PPV withLM removal, and mean postoperative visual acuity in theyes treated with modified grid laser photocoagulation wastill better than the eyes treated with PPV and ILMemoval, although the improvement was not significant. In
recent study, visual acuity improvement by 2 or moreines has been reported in 91.6% of eyes with PPV andLM removal in diabetic macular edema.8 In diabeticacular edema, it has been reported that visual acuity
tabilizes with modified grid laser photocoagulation in 77%f eyes and improves in 13.7% of eyes, whereas 9.3% ofyes experiences loss of vision after 1 year of follow-up.3
The primary limitations of this study are the use of aingle session of grid laser photocoagulation, the rela-ively small number of patients, and the use of thenellen chart for visual acuity measurements. It is nothe standard of care to treat only once with laserhotocoagulation if the retina is still thickened. Fur-hermore, there is a selection bias that may, in someases, favor patients with more severe disease, becausenilateral macular edema was excluded and most of theatients (66.6%) had proliferative diabetic retinopathy.espite these limitations, because PPV with ILM re-oval in one eye and modified grid laser photocoagula-
ion in the fellow eye were performed at random,ndividual systemic conditions that may affect maculardema, such as type and glycemic control of diabetes,ge, blood pressure, and nephropathy, were eliminated.dditionally, there was no significant difference be-
ween the eyes in terms of preoperative foveal thickness,isual acuity, type of diabetic retinopathy, the durationf visual impairment, the length of time since theacular edema was diagnosed, and presence of panreti-al laser photocoagulation. This allowed us to make annbiased comparison between the eyes that underwentPV with ILM removal and modified grid laser photo-oagulation.
In this study, mild progression of nuclear sclerosis wasbserved in 36.3% of phakic eyes that underwent PPVith ILM removal and in 18.1% of phakic eyes thatere treated with modified grid laser photocoagulation.ecause the progression of nuclear sclerosis was mildnd did not cause best-corrected visual acuity impair-ent, we did not feel that the removal of these cataractsould have resulted in even better visual acuity. Previ-usly, the incidence of cataract formation after PPVwith or without ILM removal) for diabetic maculardema has been reported as 10.3% to 63.2%.4,8,11,12
eripheral retinal tears (1.7%–20.7%), postoperativehegmatogenous retinal detachment (1.7%–16.6%),ostoperative epiretinal membrane (10.2%–13.8%) andamellar macular hole formation (1.5%), hard exudateeposits in the center of the macula (4.6%), andecurrent vitreous hemorrhage (1.5%–10%) have alsoeen reported in recent studies, in which PPV was
erformed in eyes with diabetic macular edema.4,8,11–13AMERICAN JOURNAL OF00
rogressive enlargement of laser scars (5.4%), premacu-ar fibroplasia (0.6%), and subretinal fibrosis have beeneported in eyes with diabetic macular edema thatnderwent grid laser photocoagulation.9,14,15 None ofhese complications were observed in our series. Nota-ly, despite the use of the two substances ICG dye andentamicin, which are potentially toxic to the retina,isual acuity improved by 2 or more lines in 50% of eyesnd remained unchanged in 50% of eyes that underwentPV and ILM removal.In conclusion, PPV with ILM removal was observed to
e more effective than a single session of modified gridaser photocoagulation in the treatment of diabetic macu-ar edema. Further studies with a large number of patientsre required for a more reliable conclusion.
REFERENCES
1. Klein R, Klein BEK, Moss SE. The epidemiology of ocularproblems in diabetes mellitus. In: Feman SS, editor. Ocularproblems in diabetes mellitus. Boston: Blackwell ScientificPublications, 1991:1–51.
2. Early Treatment Diabetic Retinopathy Study ResearchGroup. Photocoagulation for diabetic macular edema. EarlyTreatment Diabetic Retinopathy Study Report Number 1.Arch Ophthalmol 1985;103:1796–1806.
3. Lee CM, Olk RJ. Modified grid laser photocoagulation fordiffuse diabetic macular edema: long-term visual results.Ophthalmology 1991;98:1594–1602.
4. Lewis H, Abrams GW, Blumekranz MS, Campo RV. Vitrec-tomy for diabetic macular traction and edema associated withposterior hyaloidal traction. Ophthalmology 1992;99:753–759.
5. Ikeda T, Sato K, Katano T, Hayashi Y. Improved visualacuity following pars plana vitrectomy for diabetic cystoidmacular edema and detached posterior hyaloid. Retina 2000;20:220–222.
6. Heij ECL, Hendrikse F, Kessels AGH, Derhaag PJFM.Vitrectomy results in diabetic macular edema without evi-dent vitreomacular traction. Graefes Arch Clin Exp Oph-thalmol 2001;239:264–270.
7. Otani T, Kishi S. A controlled study of vitrectomy for diabeticmacular edema. Am J Ophthalmol 2002;134:214–219.
8. Gandorfer A, Messmer EM, Ulbig MW, Kampik A. Resolu-tion of diabetic macular edema after surgical removal of theposterior hyaloid and the inner limiting membrane. Retina2000;20:126–133.
9. Olk RJ. Modified grid argon (blue-green) laser photocoagu-lation for diffuse diabetic macular edema. Ophthalmology1986;93:938–950.
0. Striph GG, Hart WM Jr, Olk RJ. Modified grid laserphotocoagulation for diabetic macular edema: the effect onthe central visual field. Ophthalmology 1988;95:1673–1679.
1. Pendergast SD, Hassan TD, Williams GA, et al. Vitrectomyfor diffuse diabetic macular edema associated with a tautpremacular posterior hyaloid. Am J Ophthalmol 2000;130:
178–186.OPHTHALMOLOGY MAY 2005

1
1
1
1
V
2. Tachi N, Ogino N. Vitrectomy for diffuse macular edema incases of diabetic retinopathy. Am J Ophthalmol 1996;122:258–260.
3. Yamamoto T, Hitani K, Tsukahara I, et al. Early postopera-tive retinal thickness changes and complications after vit-rectomy for diabetic macular edema. Am J Ophthalmol
2003;135:14–19.COMPARISON OF TREATMENTS OFOL. 139, NO. 5
4. Schatz H, Madeira D, McDonald HR, Johnson RN. Progres-sive enlargement of laser scars following grid laser photoco-agulation for diffuse diabetic macular edema. ArchOphthalmol 1991;109:1549–1551.
5. Guyer DR, D’amico DJ, Smith CW. Subretinal fibrosis afterlaser photocoagulation for diabetic macular edema. Am J
Ophthalmol 1992;113:652–656.DIABETIC MACULAR EDEMA 801
Aiop
8
Biosketch
tes Yanyali graduated from the School of Medicine of Istanbul University, Turkey in 1990. He completed his residencyn Claude Bernard University in Lyon, France in 1994. He is currently working as an assistant professor in the Retina Unitf the Ophthalmology Department at Haydarpasa Numune Education and Research Hospital in Istanbul, Turkey. Hisrimary research interests are vitreoretinal diseases, especially macular surgery.
AMERICAN JOURNAL OF OPHTHALMOLOGY01.e1 MAY 2005
Related Documents











