Moderate Sedation In-Service Training Web Course Credits Developed by The Employee Education System in conjunction with the VHA National Anesthesia Service (Patient Care Services), Michael J Bishop, MD, Director LEAD AUTHOR: Vadim Vornik, MD, Department of Anesthesiology, North Texas VA MODERATE SEDATION WORKGROUP MEMBERS: • Beverly O’Connor-Griffin, CRNA, Bay Pines VA • Susan T Brooks, RN, Baltimore VA • Grace Chien, MD, Portland VAMC • Kent Yucel, MD, Boston VA Health Care System • Sean Kennedy, MD, (Anesthesiology Field Advisory Committee), Philadelphia VA • Susan Valley, MD, (Anesthesiology Field Advisory Committee), Northern California VA HCS • Jonathan Mark, MD, (Anesthesiology Field Advisory Committee)Durham VA • Douglas Rotte, (Central Office Anesthesiology Health Systems Specialist) EES PROJECT TEAM: Richard Lussier, DR. P. H. - Program Manager, Employee Education System Beau Chandler - Program Specialist, Employee Education System

Moderate Sedation In-Service Training Web Course Credits Developed by The Employee Education System in conjunction with the VHA National Anesthesia Service.
Dec 23, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Moderate Sedation In-Service Training Web Course Credits
Developed by The Employee Education System in conjunction with the VHA National Anesthesia Service(Patient Care Services), Michael J Bishop, MD, Director
LEAD AUTHOR:Vadim Vornik, MD, Department of Anesthesiology, North Texas VA
MODERATE SEDATION WORKGROUP MEMBERS: •Beverly O’Connor-Griffin, CRNA, Bay Pines VA •Susan T Brooks, RN, Baltimore VA •Grace Chien, MD, Portland VAMC •Kent Yucel, MD, Boston VA Health Care System •Sean Kennedy, MD, (Anesthesiology Field Advisory Committee), Philadelphia VA•Susan Valley, MD, (Anesthesiology Field Advisory Committee), Northern California VA HCS•Jonathan Mark, MD, (Anesthesiology Field Advisory Committee)Durham VA•Douglas Rotte, (Central Office Anesthesiology Health Systems Specialist)
EES PROJECT TEAM: Richard Lussier, DR. P. H. - Program Manager, Employee Education SystemBeau Chandler - Program Specialist, Employee Education SystemDarea Chappelle - Program Specialist, Employee Education SystemRussell Bennett, MBA - Media Producer, Employee Education System

General Information•Privileges may be granted to a licensed independent practitioner to perform procedures under moderate sedation. Such privileges are not required when monitored anesthesia care is provided by an anesthesia provider.
•Moderate sedation training or evidence of ongoing competency is required at the time of re-privileging.
•Evidence of mastery of the content of this course or equivalent training is required for nursing personnel who assist with administration of sedation and monitoring.

Course Summary•This course consists of eight parts:
–Definitions, Objectives, Standards, Guidelines –Pre-sedation Assessment –Sedation Pharmacology –Monitoring and Documentation –Airway Management –Complications of Sedation –Post-sedation Patient care –Sedation of the Geriatric Patient •Each part will require about 10-15 min to complete •At the end of the course the final exam will be conducted. You are required to have at least 75% correct answers in order to get full credit.
Good Luck!!

Part 1: Definitions, Objectives, Standards, Guidelines

JCAHO Standards Overview
•New JCAHO Sedation/Analgesia Standards became effective in January 2004.
•The JCAHO Standards for sedation and anesthesia apply when patients receive, in any setting for any purpose, by any route, moderate or deep sedation as well as general, spinal, or other major regional anesthesia.
•These standards DO NOT apply to patients receiving minimal sedation (anxiolysis).

The VA Moderate Sedation Directive
•Strict adherence to the JCAHO sedation standards
•Adequate training of all individuals administering, monitoring, and or supervising moderate sedation with mandatory supervisory CPR competence

The Goals of Moderate Sedation/Analgesia
•Providing a comfortable and cooperative patient
•Elevation of pain threshold
•Rapid recovery

Objectives of Moderate Sedation
•Maintain adequate sedation with minimal risk –The patient’s ability to communicate should be preserved. Monitoring must be employed. Emergency resuscitation must always be on hand. •Relieve anxiety and produce amnesia when desired
–These objectives are accomplished by means of good preoperative communication and instructions as well as administration of anxiolitic drugs. •Provide relief from pain and other noxious stimuli
–Opioids are given to supplement local or topical anesthetics as needed.

Levels of Sedation & Analgesia
Minimal Sedation (anxiolysis)
Moderate sedation/ analgesia (conscious sedation)
Deep Sedation/ Analgesia
General Anesthesia
Responsiveness
Normal Purposeful* response to verbal/tactile stimulation
Purposeful* response to tactile or painful stimulation
Unarousable even with painful stimulation
Airway Unaffected No intervention required
Intervention may be required
Intervention often required
Spontaneous ventilation
Unaffected Adequate May be inadequate
Frequently inadequate
Cardiovascular function
Unaffected Usually maintained
Usually maintained
May be impaired
Sedation and analgesia is a continuum and consist of the following states:
* Reflex withdrawal from a painful stimulus is NOT considered a purposeful response
Definitions •Because it is not always possible to predict how each patient will respond to sedative and/or analgesic medications, practitioners intending to produce a given level of sedation should be able to rescue patients whose level of sedation becomes deeper than initially intended!
e.g.: The practitioner who provides moderate sedation must be able to manage a compromised airway or hypoventilation in a patient who cannot be easily aroused, but responds purposefully following repeated or painful stimulation (deep sedation/ analgesia).

Part 2: Pre-sedation Assessment

The Goals of Pre-Sedation Patient Assessment
•Identify pre-sedation risk factors •Determine if any pre-sedation investigations or specialty consultations are required •Optimize the patient’s condition prior to the procedure •Review available documentation related to previous sedation/analgesia •Formulate a sedation plan •Obtain informed consent •Reduce patient’s anxiety through education and communication
Conducting the Pre-Procedure Assessment
•The assessment is best conducted by the provider who will participate in the administration of sedation. If it is not possible, a different qualified staff member can perform the pre-procedure evaluation. In any case, an LIP must either complete or sign off on the assessment prior to the start of the case and/or administration of sedation.•When possible, pre-sedation assessment should be conducted several days prior to the proposed procedure to allow sufficient time for the collection of consults and laboratory results. •The pre-sedation assessment must be completed before the administration of any sedative agent. A set of vital signs must be documented prior to giving any sedatives. On the basis of the collected information a sedation plan should be developed and clearly documented in the chart. •The patient must be reassessed again immediately prior to the procedure. Any interval changes must be documented in the chart and addressed if necessary.

Components of the Pre-Sedation Evaluation
•Documentation of relevant past medical history
•Focused physical examination
•Collecting relevant specialists’ consultations and tests

Collecting the Past Medical History (PMH)
•At least the following information should be collected:
–Height and weight (obesity, malnourishment)–Major organ systems abnormalities and evaluation of the airway –History of any previous adverse experiences with sedation/analgesia as well as regional and general anesthesia –Drug allergies and current medications –Tobacco, alcohol or substance use or abuse –Time and nature of last oral intake –An assessment of risk such as the American Society of Anesthesiologists Physical Status

Obesity and Moderate Sedation •Morbidly obese patients undergoing sedation are under significantly higher risk of complications than non-obese patients with otherwise similar medical problems •The negative effect on organs and systems is directly related to the degree of obesity with minimal changes in overweight patients (BMI=25-29kg/m2) and maximal impact on morbidly obese patients (BMI above 35kg/m2)* •Obese patients have a high prevalence of obstructive apnea and desaturate quickly. In general no sedative drugs should be administered before all the monitors have been applied and airway equipment is readily available •Obese patients are prone to pulmonary aspiration secondary to decreased gastric motility, increased gastric volume and intra-gastric pressure. Pre-medication with antacids, gastric stimulants and H2-blockers may be needed prior to administering sedation
*Body Mass Index (BMI) = Weight (kg) / Height2 (M)

Pharmacokinetics and Pharmacodynamics in Obesity •In obese patients lipophilic drugs (benzodiaiepines, opioids) may demonstrate longer elimination half-life. In addition the sensitivity to the sedative drugs is unpredictable in this population •To minimize the development of deep sedation states, dosage requirements for sedative medications should be based on ideal body weight and NOT the patient’s actual weight •If obstructive sleep apnea is suspected further decrease in dosage of sedative medications (as much as 50% to 70%) may be needed
In general when dealing with obese patients titration to clinical effect is the safest approach to avoid
oversedation

Sleep Apnea and Moderate Sedation
•Sleep apnea is cessation of air flow for longer than 10 sec during sleep leading to arterial hypoxemia and hypercarbia. •If sleep apnea is suspected, pre-sedation assessment should include questioning about associated signs and symptoms such as morning headaches, overwhelming somnolence during normal waking hours, loss of initiative, memory problems, etc. •Institution of CPAP immediately after the procedure results in significantly fewer desaturation episodes. Ask those patients who use CPAP at home to bring their personal CPAP machines when coming for the procedures. This approach helps to avoid delays with the delivery of CPAP machines to numerous sleep apnea patients coming to the hospital. •Since sleep apnea patients are at increased risk for developing hypoxemia after the procedure, they should receive written discharge instructions to avoid taking any CNS depressants or consuming alcohol in the immediate post-procedure period. In some cases 24-hrs in-house observation may be considered.

PMH: Malnourished Patients
•Patients with nutritional disorders, carcinoma, recent weight loss, advanced renal and liver diseases may experience an exaggerated effect from sedatives and analgesics as a result of the CNS hypersensitivity to drugs and decreased plasma protein binding ability.
•Titration of pharmacologic agents is advised in such situations by administration of small incremental doses slowly over several minutes while continuously assessing the patient’s condition.

PMH: Major Organ System Diseases
Evaluation should focus on the following: •Assessment for disease severity, stability and any recent changes in the patient’s condition •Assessment for prior and ongoing treatment and determining the time of the last dose of medication •Determining the variables that may affect the patient’s sensitivity to sedative drugs, predispose to airway compromise or/and cardio-pulmonary instability

PMH: Previous Complications with Anesthesia
Review any old anesthesia or sedation flow sheets focusing on:
•airway management •reaction to the medication •family history of complications related to anesthesia

PMH: Current medications
Review the patient’s list of current medications focusing on the drugs that might:
•affect pharmacokinetics or/and pharmacodynamics of the sedatives (e.g.: MAO inhibitors + meperidine hypertension, hyperpyrexia, coma)•cause hemodynamic or respiratory compromise in combination with sedatives (e.g.: ACE inhibitors + sedatives exaggerated hypotension)

PMH: Alcohol Abuse
•In addition to multisystem disease state, chronic alcohol consumption leads to cross-tolerance to sedatives/analgesics.
•Patients who seem to be acutely intoxicated are generally not good candidates for sedation because it suggests they are not NPO and also may not be able to follow post-procedure directives. In such patients, the urgency of the procedure should be weighed against the potentially increased risk.

PMH: Stimulant Abuse •Cocaine – is a potent vasoconstrictor and has direct negative effects on the heart as well as causing coronary vasospasm, dysrhythmia and seizures. Any elective procedures should be delayed if the patient appears acutely intoxicated. •Marijuana – produces mild to moderate sympathetic stimulation, increases heart rate and myocardial oxygen consumption, sometimes produces orthostatic hypotension. Severe tachycardia warrants cancellation of the case. •Amphetamines - Chronic abuse of amphetamines leads to tolerance and psychosis. Catecholamine stores may be depleted. Any elective procedure should be delayed if the patient appears acutely intoxicated. •Ecstasy – chemically resembles a combination of amphetamine and mescaline. Most common complications include hyperthermia, mental status changes, tachycardia, tachypnea, profuse sweating. No procedure should be performed till at least 6 hrs since last consumption.

Focused physical examination •At a minimum, focused physical examination should include the following:
–Baseline vital signs (BP, HR, RR, room air SpO2)–Mental status, level of awareness –Body habitus –Auscultation of heart & lungs –Airway assessment –Any pre-existing neurologic or motor deficits •If the collected information suggests presence of a new serious medical problem, further detailed evaluation will be necessary and elective procedure should be delayed.
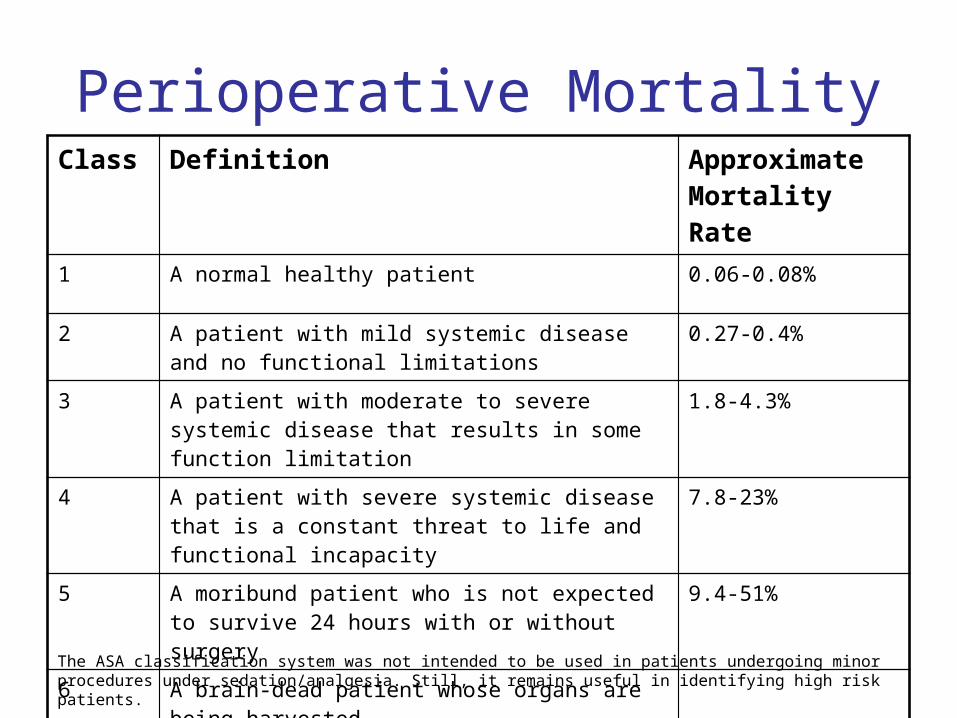
Perioperative Mortality Class Definition Approximate
Mortality Rate 1 A normal healthy patient 0.06-0.08%
2 A patient with mild systemic disease and no functional limitations
0.27-0.4%
3 A patient with moderate to severe systemic disease that results in some function limitation
1.8-4.3%
4 A patient with severe systemic disease that is a constant threat to life and functional incapacity
7.8-23%
5 A moribund patient who is not expected to survive 24 hours with or without surgery
9.4-51%
6 A brain-dead patient whose organs are being harvested
E The procedure is an emergency (for example, “2E”)
The ASA classification system was not intended to be used in patients undergoing minor procedures under sedation/analgesia. Still, it remains useful in identifying high risk patients.

Guidelines to identify "high risk" patients
1. Difficult airway 2. Age >70 years 3. Sleep apnea or airway obstruction 4. Morbid obesity 5. Severe major organ system disease resulting in ASA score greater than 3 6. Drug or alcohol abuse
Although the majority of “high risk” patients are safely managed by an experienced practitioner, consideration should be given to consult an anesthesiologist if significant difficulties are expected or invasive monitoring is required.

Laboratory testing
•Pre-procedure laboratory testing should be guided by the patient’s underlying medical condition and the likelihood that the results may affect the management.
•A “routine” comprehensive laboratory testing for asymptomatic patients is discouraged since it increases cost but does not improve safety.
Specialist Consults
•Whenever possible, appropriate medical specialists should be consulted before the administration of sedation to patients with significant underlying conditions. •Consideration should be given to consult an anesthesiologist if:
–the patient is severely compromised or medically unstable –the patient has difficult airways –the patient has a know history of complicated or unsuccessful moderate sedation/analgesia
NPO Status •NPO Guidelines for healthy patients:
•Clear liquids administered up to 2 hours before a scheduled procedure do not alter residual gastric volume when compared with the standard NPO overnight fasting •Solid food consumption warrants 6-8 hr delay of a procedure •The following factors slow down gastric emptying and increase the risk of pulmonary aspiration (strict 6-8 hrs NPO status is required for patients with these conditions - no solid or liquid food is allowed):
–pregnancy - recent opioid administration –diabetes with neuropathy - severe pain –esophageal dysmotility - trauma –extreme anxiety or fear - known GERD –Obesity - hiatal hernia
Documentation of the Preoperative Evaluation
•A standardized pre-sedation evaluation form should be completed prior to all sedation procedures.
•The pre-sedation evaluation must be signed by the attending physician in all cases.

Pre-procedure Patient Education •By the end of the pre-sedation assessment the patient should be given detailed instructions pertinent to the planned procedure. At least the following issues should be addressed:
–NPO –Time of arrival –Estimated procedure time –Medication instructions –Procedure-specific guidelines (e.g.: bowel preparation, dye preparations, etc) •Patients must be instructed to arrange for a competent adult to accompany them home. It is not acceptable to discharge a sedated patient from the hospital without an accompanying responsible adult. This designated person will assume post-sedation care and will follow the post-procedure instructions. If such person is not available, the procedure should be re-scheduled or the patient needs to be lodged or admitted overnight.
Last Preparations for the Procedure
•The site, procedure and patient are accurately identified and documented according to the JCHAO requirements. Informed consent is re-checked. •Presence of a responsible adult for post-procedure home transportation or arrangements for lodging or overnight admission are confirmed. •The patient’s health status is re-evaluated immediately before the sedation procedure, and any changes from the last visit are documented and addressed. •Pre-procedure vital signs are checked and documented.

Part 3: Sedation
Pharmacology
Titration to Clinical Effect
•Titration to clinical effect is considered to be the safest approach to administering sedation/analgesia
•Titration provides for slow, controlled rise in plasma level
•Titration allows to combine different groups of medications safely

General Recommendations •The drugs should be titrated using minimal nesessary doses with sufficient interval in between to allow enough time for the drug to demonstrate its full effect. •Dosage requirements for sedation generally decrease in elderly patients, in debilitated patients and in patients with a significant cardiac, pulmonary or CNS disease. •Total doses and/or frequency of administration may also need to be reduced in patients with renal and/or hepatic dysfunction. •Drugs that are anesthetic agents (e.g. propofol, thiopental, methohexital, ketamine, etomidate, etc.) must be administered by an anesthesiologist, nurse anesthetist or by a licensed independent practitioner with sufficient training and ability to rescue a patient from general anesthesia.

Benzodiazepines (BDZ)
The following effects on major systems are typically observed with the administration of BDZs: •Cardiovascular System: Systemic blood pressure is slightly decreased. •Respiratory System: This effect is usually insignificant unless the drugs are administered quickly or combined with other CNS depressants. •Central Nervous System: These drugs provide anti-seizures effect, produce anterograde amnesia, anxiolysis and centrally-mediated muscle relaxation.

Opioids• The following effects on major systems are typically observed with the administration of opioids:
•Cardiovascular System: Bradycardia (fentanyl, morphine) or tachycardia (meperedine). Hypovolemic patients may develop hypotension.
•Respiratory System: Respiratory depression or apnea. Extreme caution must be exercised when administering to patients with COPD or decreased respiratory reserve especially when combined with BDZ.
•Central Nervous System : Euphoria, sedation. Addition of other CNS depressant drugs produces a synergistic effect.
•A sudden increase in muscle tone ("stiff-chest" syndrome) causing difficulties with ventilation may occur if fentanyl is administered rapidly. The treatment consists of assisted ventilation and naloxone (IV). If hypertonus does not resolve within a minute, immediate consultation with an anesthesiologist should be requested.

Administration and Doses of Sedative Drugs
Drug Single Dose
Titration Onset Peak Duration Antagonist Other
Midazolam (Versed)
0.5-2 mg IV
Small increments every 3-5 min
1-2.5 min
3-5 min
20-40 min Flumazenil No active metabolites
Fentanyl (Sublimaze)
25-50 mcg IV
Small increments every 3-5 min
1-5 min
3-5 min
30-60 min Naloxone May cause the “stiff-chest” syndrome
Meperidine (Demerol)
12.5-50 mg
Small increments every 10-15 min
1-5 min
5-7 min
60-120 min
Naloxone Causes less spasm of smooth muscles. Avoid in renal impairment, in patients on MAO inhibitors, in patients with severe CAD (risk of tachycardia)
Morphine 1-3 mg IV
Small increments every 5-15 min
1-5 min
20-30 min
20-180 min
Naloxone Lower the dose for renal impairment

Reversal Agents: General Consideration
•Reversal agents should be available whenever opioids/BDZ are administered.•Before or concomitantly with pharmacological reversal, patients who become hypoxic or apneic should:
–Continue to receive supplemental oxygen (should always (!) be available and administered to the sedated patient)–Be stimulated and encouraged to breath deeply–Receive mask ventilation if spontaneous ventilation becomes inadequate
•After pharmacological reversal, patients should be observed long enough to ensure that cardio-pulmonary depression does not recur once the effect of the antagonist dissipates.•Routine administration of the reversal agents at the end of the case is not recommended.

Administration and Doses of Reversal Agents
Drug Bolus Dose
Administration Onset Duration Other
Flumazenil (Romazicon)
0.2 mg IV
Administer the dose over 15 sec; may repeat every 1min up to max dose of 1 mg. No more than 3 mg is recommended in any 1-hour period
0.5-1 min
60 min May precipitate seizures in patients chronically treated with BDZ. May cause cutaneous vasodilatation, sweating, flushing, arrhythmias, HTN.
Naloxone (Narcan)
0.1-0.2 mg IV
Administer 0.02-0.04 mg IV every minute till the desired degree of reversal is achieved. The large bolus (0.2-0.4 mg IV) should be reserved for emergency reversal of profound respiratory depression.
1 min 15-30 min Caution must be utilized when administering to patients with preexisting cardiac disease or patients with known or suspected physical dependence to opioids.

Part 4: Monitoring and
Documentation

Monitoring: The Basics•The administration of moderate sedation/analgesia for each patient is documented in the medical records regardless of the duration of the case.•At a minimum, the procedure flow sheet should include vital signs:
1. Before giving the first dose of the drug 2. After the administration of the sedatives/analgesics 3. At regular intervals during the procedure (max interval is 5 min) 4. During the initial recovery 5. Just before discharge
•A designated individual ("monitoring person"), other thanpractitioner performing the procedure, must be present to provide monitoring:
–Throughout the procedure a monitoring person should have no other responsibilities apart from the continuous monitoring of the patient.–Under certain circumstances institutional sedation policy may allow the monitoring person to assist with minor tasks while maintaining adequate monitoring once the patient's level of sedation / vital signs have stabilized.

Monitors
•Minimal monitoring for moderate sedation procedures include:•Non-invasive blood pressure •Pulse oximetry•Respiration rate•Level of consciousness•Level of pain•ECG for patients with significant cardiac disease

Level of Consciousness•Evaluate the patient's behavior and response to stimuli on any available standardized sedation scale:•Observer's Assessment of Alertness / Sedation (OAA/S) •Sedation Visual Analogue Scale•Modified Ramsey Sedation Scale (RSS), e.g.:
Responsiveness ScorePatient paralyzed, unable to assess level of sedation 0
Patient anxious, agitated, or restless 1
Patient cooperative, oriented, and tranquil 2
Patient sedated but responds to commands 3
Patient asleep but responds to glabellar tap 4
Patient asleep but responds to nail bed pressure(no response to glabellar tap)
5
Patient asleep, no response to nail bed pressure 6
Monitor Alarms•All monitors have alarms activated when the patient's vital signs deviate from the preset thresholds. These alarms become activated by default whenever the monitors are turned on.
•The alarms must not be disabled during the procedure, and the volume of the alarm should be set high enough to be heard despite ambient noises of the procedure room.
•Alarm limits should not be set broadly since it may obscure a dangerous situation. Initial alarm limits should be set approximately 20% above/below the patient's pre-sedation baseline vital signs.

Moderate Sedation Flow Sheet•During any sedation/analgesia procedures vital signs, given medications, performed measures and other intra-procedure events must be documented. Most facilities will use a flow sheet for this documentation.
•Vital signs are recorded every 5 min, and any monitored artifacts should be documented to avoid confusion and misinterpretations during a later review of the record.
•The flow sheet should be signed by the attending physician.
Part 5: Airway
Management

Applicable Anatomy and Physiology of Airway
•The upper airway obstruction (problems with structures above the vocal cords) is the most common cause of ventilation difficulties in sedated patients, and is usually due to the reduction of the space between the posterior pharyngeal wall and the base of the tongue.
•The pharynx, epiglottis, and vocal cords play a role in protecting the lower airway from aspiration. The most important function is the glottic closure reflex in response to direct glottic or supraglottic stimulation, or as a reflex response to visceral stimulation. The physiologic exaggeration of this reflex, laryngospasm can compromise ventilation during a procedure.

Evaluation in the Airway
•The primary goal of airway examination is to predict possible difficulties with spontaneous ventilation of sedated patients as well as with positive pressure ventilation / intubation, if it becomes necessary.
•Every airway examination should include: –Oral cavity evaluation–Temporo-mandibular joint evaluation –Thyromental distance evaluation–Atlanto-occipital movement evaluation–Evaluation of the relationship between the tongue and other structures of the oral cavity (Mallampati classification)

Evaluation of the Airway: Part 1•Oral cavity evaluation: check the mouth opening (should be at least 2 fingerbreadth to allow intubation in case of emergency), presence of loose, chipped, broken, capped teeth, dentures, tumors, gross deformities.
•Temporo-mandibular joint evaluation: assess mobility by asking the patient to open the mouth as wide as possible while palpating the temporo-mandibular joints in an attempt to identify a limited range of motion or joint "locking".
•Thyromental distance evaluation: represents the straight distance from the notch of the thyroid cartilage to the tip of the mentum; if this distance is less than 6 cm or three fingerbreadths (receding mandible, short muscular neck), the larynx will be positioned anteriorly making intubation difficult.

Evaluation of the Airway: Part 2
•Atlanto-occipital movement evaluation: may be performed by having the patient sit facing the examiner, then tilt the head back as far as possible extending the atlanto-occipital joint (normally at least 35 degree). Failure to adequately extend the neck will make visualization of the glottis difficult or impossible.
•Mallampati classification: based on the size of the tongue and pharyngeal structures visible on mouth opening. The bigger the tongue (higher MP class), the more difficult to get a glottic view during laryngoscopy and the higher the chances of airway obstruction with sedation.

Mallampati classification
• Class I = visualization of the soft palate, uvula, and pillars • Class II = visualization of the soft palate and uvula • Class III = visualization of the soft palate and the base of the uvula • Class IV = soft palate is not visible at all

Equipment for Airway Management
Prior to any sedation procedure, necessary airway equipment should be prepared and its condition checked. At least the following equipment should be available:
•Oxygen administration devices (nasal cannula, simple face mask, Ambu bag)•Nasal/Oral airways of different sizes •Water-soluble lubricating gel •Tongue blade•Adequate oropharyngeal suction

Nasal and Oral Airway•Nasal Airway
–displaces the tongue from the posterior pharyngeal wall–the size of the nasal airway indicates the internal diameter in millimeters–needed length is determined by measuring the distance from the tip of the nares to the lobe of the ear–usually better tolerated than oral airway–not recommended in the presence of anticoagulants, cerebrospinal fluid rhinorrhea, septal deformity, nasal polyps–should always be lubricated prior to insertion and should never be forced if resistance is felt–long nasal airway may cause cough and laryngospasm •Oral Airway
–displaces the tongue from the posterior pharyngeal wall–may be the only possible solutions when the nasal airways are contraindicated or impossible to place–may stimulate the gag reflex or/and cause retching resulting in HTN and tachycardia, bradycardia (vagal response), laryngospasm, dental damage, pharyngeal or lip laceration

Effects of Sedatives/Analgesics on the Airway
•Decrease hypoxic and hypercarbic respiratory drive
•Cause loss of the upper airway muscle tone with subsequent narrowing of the upper airway lumen
•Cause obstruction of the airway by the soft tissues as the muscles supporting the soft tissue of the pharynx (tongue, epiglottis) lose their normal tone
•Decrease activity of the brain cortex allowing disinhibition of the protective reflexes in response to airway stimulation by saliva / foreign materials and leading to laryngospasm

Airway Management in Sedated Patients
The following action sequence is recommended to restore adequate ventilation and oxygenation in case of upper airway obstruction during sedation/analgesia:
1. Auditory/tactile stimulation of the patient.2. Lateral head tilt (results in tongue displacement to the side, away from
the posterior pharynx).3. Chin lift (permits anterior movement of the mandible with elevation of
the airway soft tissue anteriorly).4. Jaw thrust (provides significant anterior displacement of the mandible,
stretches the neck, moves supra-epiglottic soft tissue anteriorly.
Airway obstruction not relieved by above mentioned measures signifies oversedation and may require immediate consultation by an anesthesiologist!
5. Nasal/oral airway insertion6. Pharmacological reversal of sedative/analgesics

Dealing with Laryngospasm•This is uncontrolled spasm (glottic closure) of the vocal cords.•May be provoked by mucus, blood, saliva, locally instilled drugs, acrid smell, manipulation of airway, pain, or visceral distention.•May be incomplete (some air movement is present, inspiratory stridor, accessory respiratory muscles use) or complete (complete airway obstruction, no respiratory sounds; chest & diaphragm movement may be present, but not effective - "paradoxical breathing")•Treatment (procedures and sequence):
1.Stop the procedure to avoid any additional stimulation2. Suction oropharynx if the local irritants are suspected to be the cause of laryngospasm.3. Call Anesthesiologist or in house airway management resource stat while attempting a jaw thrust and mask ventilation with 100% 02 4. Consider Lidocaine IV bolus 0.5-0.8 mg/kg

Part 6: Common Complications
of Sedation

Hypoxia•Definition: Sp02 <90%•Diagnosis of hypoxia (auscultation, palpation, visualization):
–Continuously monitor the patient's respiration (mask fogging, chest movement, etc.)–Go with pulse oximetry, NOT color of the skin since cyanosis is a late sign of hypoxia and develops only at Sp02<70%–Never disable monitor alarms! Keep pulse oximeter signal loud!–Have all the rescue airway devices checked and ready •Treatment:
–Abort the procedure if possible and administer supplemental 02
–Proceed with airway manipulation to maintain its patency Institute mask ventilation if needed–Administration of pharmacologic reversal agents may be needed

Hypotension•Definition: decrease of the BP below 30% of the patient's baseline (know the patients' "usual" blood pressure!)
•Diagnosis:•Monitor NIBP every 3-5 min and use the correct size cuff •Check pulse if the BP reading is questionable•Check pulse oximeter plethysmogram - it reflects peripheral tissue perfusion•Treat sudden mental status change or nausea as a sign of low BP until proven otherwise!
•Treatment:•Abort the procedure if possible•Address the most probable cause first (hypoxia, hypovolemia, peritoneal stretching, etc.)•Administer IV fluid bolus•If the problem persists despite abovementioned measures request immediate anesthesiologist consult or in-house airway management resource stat

Aspiration•Definition: Inhalation of the gastric contents into the tracheo-bronchial tree•Diagnosis: Presence of stomach content in the mouth, coughing, laryngospasm, sudden hypoxia, bronchospasm, dyspnea•Treatment:
–Stop the procedure immediately, turn the patient's head to the side and suction the oropharynx–Consider placing the patient in the Trendelenburg position to prevent flooding of the airway with the stomach content–Once airway is cleared, apply 100% 02 by face mask and check for bilateral breathing sounds–If the patient remains hypoxic, proceed with hospital admitting for 24 hrs observation–If (and only if) particular matter aspiration is suspected, the patient will need intubation and bronchoscopy to remove the aspirated material from the trachea and large bronchi–Empirical antibiotic treatment is recommended only in immunocompromised patients, or if the patient aspirated feculent materials–No benefit from empirical steroids administration after aspiration has been demonstrated
•Prevention:–Identify the at risk patients and premedicate with antacid, H2 blocker, metoclopramide; delay non-emergent cases if patients are not NPO–In emergency situations, consider lighter plan of sedation or consult an anesthesiologist for securing the airway in a controlled fashion.

Documenting Complications•The Moderate Sedation Tracking form should be completed for every moderate sedation/analgesia procedure and submitted to the Clinical Quality Management. These forms are utilized for statistical purposes as well as for determining a provider specific / department-specific complication rate in order to improve the quality of care.•The cases in which any of the following events occur will be reported as complications to the service/section chief and to the Quality Management:
•All cases in which naloxone or flumazenil is administered •All cases requiring assisted ventilation•All unanticipated hospital admissions secondary to moderate sedation•All cases in which Sp02 was 10% below baseline for more than 5 minutes, including the recovery period•All cases of unanticipated hemodynamic instability, such as deviation of the blood pressure >30% from the patient's baseline, onset of new dysrhythmias, a pulse rate of 120 or higher for 5 minutes or more unless this is the patient's baseline (e.g.: a patient arriving to the EP lab for cardioversion / ablation)
•Every reported complication will be reviewed by the VAMC Moderate Sedation Committee to determine the nature and severity of the complication. If the Committee determines that there is a relationship between the reported event and sedation administration, a meeting with the sedation providers will be arranged to discuss the case in detail and to develop a strategy to avoid similar problems in the future.

Part 7: Post-sedation
Patient Care

Recovery: Phase 1Phase I represents initial recovery immediately after completing the procedure.
• Phase I should be completed in a designated area, or if such area is not available, in the post-anesthesia care unit (PACU).•Depending on the patient's status and procedure, this period can be as short as 15 minutes.•The Post-Anesthesia Recovery Score (PARS) of _> 9 or return to baseline status are used as criteria to determine that the patient has completed Phase I.•If transportation to the remote recovery area is needed, the patient must be accompanied by qualified personnel and adequately monitored during the transportation.

Post-Anesthesia Recovery Scoring SystemAfter patients completed Phase I of recovery they are eligible for discharge to a less intensive setting if the total score from the following categories equals 9 or 10:ACTIVITY (able to move voluntarily or on command) RESPIRATION
4 extremities 2 Able to breathe deeply and cough freely 2
2 extremities 1 Dyspnea, shallow , or limited breathing 1
0 extremities 0 Apneic 0
CIRCULATION CONSCIOUSNESS
BP +1- 20 mmHg pre-sedation level 2 Fully awake 2
BP +/- 20 - 50 mmHg pre-sedation level 1 Arousable on calling, mostly sleeping 1
BP +/- 50 mmHg pre-sedation level 0 Not responding or only responds to painful stimuli
0
OXYGEN SATURATION
Able to maintain Oxygen saturation > 92% on room air
2
Needs supplementary Oxygen to maintain Oxygen saturation > 90%
1
Oxygen saturation < 90% even with supplementary Oxygen
0
Some patients will be unable to score 9 or 10 due to a pre-anesthetic deficit. These patients must return to their baseline prior to discharge
A score of 0 in any category excludes eligibility for discharge unless approved by a physician.

Recovery: Phase 2•Phase II represents the time after the patient completed Phase I until the patient is ready to be safely discharged home from Same Day Procedure Unit ("Home Readiness"). For inpatients, Phase II is completed at their assigned hospital areas (hospital wards).
•All outpatients will be discharged home by a qualified licensed independent practitioner who is familiar with the patient or by using established discharge criteria.
•Outpatients will always be discharged to the care of a competent adult. It is the responsibility of the physician to ensure that this is accomplished. The availability of a designated driver or assistant documented prior to starting the procedure.
•No moderate or deep sedation/analgesia procedures should be performed if a driver's or assistant's availability is not confirmed and not documented on the day of the expected procedure.
•Under certain circumstances, when the patient does not have a responsible adult to assist with home transportation, overnight lodging or 23-hrs observation admission should be arranged by the supervising physician.

Post- Anesthesia Discharge Scoring System
(PADS) for Determining Home Readiness A patient has completed Phase II of recovery when total score from the following categories equals 9 or 10.
VITAL SIGNS ( Vital signs must be stable for 1 hour and consistent with age and preoperative baseline)
NAUSEA AND VOMITING (The patient should have minimal nausea and vomiting before discharge)
BP and pulse within 20% of preoperative baseline 2 Minimal: successfully treated with PO medication
2
BP and pulse 20 - 40% of preoperative baseline 1 Moderate: successfully treated with IM 1
BP and pulse > 40% of preoperative baseline 0 Severe: continues after repeated treatment 0
SURGICAL BLEEDING ( Postoperative bleeding should be consistent with expected blood loss for the procedure) ACTIVITY LEVEL
Minimal: does not require dressing change 2 Steady gait (no dizziness for 15 min or meets preoperative level)
2
Moderate: up to 2 dressing changes required 1 Requires Assistance 1
Severe: more than 3 dressing 0 Unable to Ambulate 0
PAIN (The patient should have minimal or no pain before discharge. The level of pain that the patient has should be acceptable to the patient. Pain should be controllable by oral analgesics. The location, type and intensity of pain should be consistent with the anticipated postoperative discomfort)
Minimal 2
Moderate 1
Severe 0
Some patients will be unable to score 9 or 10 due to a pre-anesthetic deficit. These patients must return to their baseline prior to discharge
A score of 0 in any category excludes eligibility for discharge unless approved by a physician.

Part 8: Sedation of
the Geriatric Patient
Effect of Aging on Sedation/Analgesia Pharmacology
•Delayed response (up to 6-8 min) to the drugs, but increased magnitude of the response due to increased CNS sensitivity to drugs•BDZ:
–Effect is enhanced by increased sensitivity and decreased hepatic enzymes activity. –Generally a dose reduction of 30-50% is recommended
•Opioids:–Increased sensitivity and decreased clearance leading to prolonged action and enhanced effect. –There is a higher risk of sudden hypotension and bradycardia with the administration of opioids
•The risk of post-procedure delirium is high in this age group secondary to physical limitations of the patients (hearing and visual loss), unfamiliar environment, and prolonged drug effect. Maintaining voice contact and careful drug titration may help to decrease the frequency of confusion
•Overall, the anatomic and physiologic changes associated with aging predispose geriatric patients to pharmacologic hypersensitivity that can easily lead to cardio-pulmonary collapse. Dose reduction and longer intervals between administrations are needed to avoid oversedation.

End Of Course!•You have completed the course content. You must take the exam to receive credit for this course.•Version 1, June 2006•Sources of Information:
–Joint Commission: Standards for Operative or Other High-Risk Procedures and/or the Administration of Moderate or Deep Sedation or Anesthesia, January, 2004 –Dallas VA Hospital Policy for the administration of Moderate Sedation / Analgesia (Conscious Sedation) –Scammon FL, Klein SL, Choi WW: Conscious sedation for procedures under local or topical anesthesia. Ann Otol Rhinol Laryngol. 1985;94:21 –Michael Kost: Moderate sedation/analgesia core competencies for practice, 2nd ed. 2004 –American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non-Anesthesiologists. Practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology. 2002;96(4):1006, 1013 –Barash PG, Cullen BF, Stoelting RK: Clinical Anesthesia, 4th edition 2000, –Hurford WE et al: Clinical Anesthesia Procedure of the Massachusetts General Hospital, 5th edition, 1997 –Morgan GE, MikhailmSM: Clinical Anesthesiology, 2rd edition, 1996.




Related Documents











