MINISTRY OF HEALTH AND SOCIAL PROTECTION OF THE POPULATION REPUBLIC OF TAJIKISTAN

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Mobility and Function for all
MINISTRY OF HEALTH AND SOCIALPROTECTION OF THE POPULATION
REPUBLIC OF TAJIKISTAN
Disability and Rehabilitation Programme
- Breaking Barriers to Include All

SITUATIONAL ANALYSIS State of rehabilitation in Tajikistan
MINISTRY OF HEALTH AND SOCIAL PROTECTION OF THE POPULATION
REPUBLIC OF TAJIKISTAN
Disability and Rehabilitation Programme
Breaking Barriers to Include All

Situational Analysis: State of Rehabilitation in Tajikistan. 1. Persons with disabilities - statistics and numerical data. 2. Persons with disabilities –rehabilitation. 3. Delivery of health care. 4. Children with disabilities. 5. Education. 6. Employment. 7. Person with disabilities – Policy and services. I. World HealthOrganization.
Address requests about publications of the WHO Regional Office for Europe to: Publications WHO Regional Office for Europe UN City, Marmorvej 51 DK-2100 Copenhagen Ø, Denmark
Alternatively, complete an online request form for documentation, health information, or for permission to quote or translate, on the Regional Office website (http://www.euro.who.int/pubrequest).
© World Health Organization 2015 All rights reserved. The Regional Office for Europe of the World Health Organization welcomes requests for permission to reproduce or translate its publications, in part or in full. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either express or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. The views expressed by authors, editors, or expert groups do not necessarily represent the decisions or the stated policy of the World Health Organization.
AbstractThis publication summarizes the current gap, need and opportunities for intervention in the field rehabilitation for persons with disabilities in Tajikistan. The situational analysis process was conducted by an intersectoral working group consisting of members from different ministries under the leadership of the Ministry of Health and Social Protection, Republic of Tajikistan and with technical support from the WHO Country Office, Tajikistan. It was undertaken in collaboration with different disability and development related stakeholders and adopted a realist synthesis approach, being responsive to the unique social, cultural, economical and political circumstances in the country. The evaluation focuses on rehabilitation policy and governance, service provisions and its impact on persons with disabilities in development of an inclusive, rights-based society with equal opportunity for all in Tajikistan.
Illustrations provided by Aziza Khojaeva, Rustam Dustov and Satish Mishra
Keywords
ISBN 978 92 890 5075 3
Contents Contributors ...................................................................................................................... iv
Abbreviations .................................................................................................................... vi
Executive summary ........................................................................................................... vii
Introduction......................................................................................................................... 1 General information about Tajikistan.................................................................................... 1 Methodology ........................................................................................................................ 2 Concepts and definitions ..................................................................................................... 5 Data-gathering and limitations ............................................................................................. 7
Legislation and services relevant to persons with disabilities ..................................... 9 Legislative framework relating to disability .......................................................................... 9 Overview of health-care, education, labour and social protection systems ......................... 12 Health care .......................................................................................................................... 12 Education ............................................................................................................................ 16 Livelihoods ........................................................................................................................... 18 Social protection system ...................................................................................................... 20 Social assistance for persons with disabilities ..................................................................... 21
Rehabilitation ..................................................................................................................... 26 Prevalence of disability........................................................................................................ 26 Mapping of rehabilitation service providers ......................................................................... 30 Supply of and demand for rehabilitation services ............................................................... 36 Medical rehabilitation techniques and practices .................................................................. 39 Community-based rehabilitation .......................................................................................... 43
Human resources for rehabilitation ................................................................................ 44 Training and education of rehabilitation professionals ........................................................ 44 Availability of rehabilitation professionals ............................................................................ 47
The cost of exclusion ........................................................................................................ 48
Conclusions and recommendations ................................................................................ 49 Strengthening existing services ........................................................................................... 50 Improving human resource capacity .................................................................................... 51 Improving identification of disabilities .................................................................................. 52 Extending services to all....................................................................................................... 52 Disability-inclusive health .................................................................................................... 52 Improving the legislative framework relating to disability ..................................................... 53 Changing societal attitudes ................................................................................................. 53 Improving accessibility of facilities ...................................................................................... 54 Improving data collection .................................................................................................... 55
References ......................................................................................................................... 55
Annex 1. Terminology of rehabilitation……………………………………………………...... 59 Annex 2. Review and analysis of existing legislation……………………........................ 67 Annex 3. Structure of the Ministry of Health and Social Protection……………………… 71 Annex 4. Structure of the State Agency on Social Protection of the Population……… 72 Annex 5. Rehabilitation services for adults with disabilities in Tajikistan……………. 73 Annex 6. Rehabilitation services for children with disabilities in Tajikistan………….. 74 Annex 7. Service providers included in the mapping………………………………………. 75
iii

ContributorsEditors Satish Mishra and Sherali Rahmatulloev
AuthorsGoibov Amonullo, Lola Bobohojieva, Albert-Philip Burger D'Haem; Safo Kalandarov, Aziza Khojaeva, Zamira Kоmilova, Kudratullo Kurbonov, Satish Mishra, Hamza Navruzov, Sherali Rahmatulloev, Abdulkarim Shekhov
Peer contributors (individuals and organizations)Agency for Medical and Social Examination; Agency on Social Insurance and Pensions; Agency on Social Protection; Association for Aid and Relief, Japan; Association of Parents with Children with Disabilities, Dushanbe; Association of Parents with Children with Disabilities “Gamkhori”; Association of Parents with Children with Down Syndrome; Baby Home (Khujand, Istaravshan, Dushanbe); Blind Society Tajikistan; boarding schools for blind and visually impaired children (Khujand, Isfara, Hissor); boarding schools for intellectually impaired children (Dushanbe, Khujand, Kulob); Cardio-Rheumatology Sanatorium for Children (Dushanbe and Vakhdat); Caritas Germany; Children and Youth Centre of Dushanbe City; City Hospital No. 5, Dushanbe; complex of kindergarten and special school for blind and visually impaired children, Khujand; Dasti Yori; daycare centres (Dushanbe, Khujand, Yovon, Khorugh, Qurgonteppa, Kulob); daycare centre for children with disabilities “Kishti”; daycare centre of social services “Nur”; Doctors’ Consultative Commission (VKK) Department, Dushanbe polyclinic; Doctor’s Vocational Expert Commission centre (VTEK), Dushanbe; Handicap International; International Committe of the Red Cross Special Fund for the Disabled; League of Disabled Women “Ishtirok”; Manbai Mehr, Khujand; Mission East; National Health Centre, Dushanbe; National Rehabilitation Centre for Children and Adolescents “Chorbog”, Varzob; National Research Institute for Rehabilitation of Persons with Disabilities; National Orthopaedic Centre, Dushanbe; National Union of Deaf People; National Union of Disabled People of Tajikistan; Nuri Umed; Oblast Centre for Rehabilitation of Cardiovascular Diseases, Khujand; Oblast Mental Clinical Centre, Khujand; Operation Mercy; Parents with Children with Autism “Iroda”; Psychological, medical and pedagogical consultation centres (Dushanbe, Shokhmansur, Isfara, Khujand, Panjikent, Kulob, Khorog, Kugrontepa, Bobojon Gafurov); Public Organization of the Blind (Dushanbe, Konibodom); Public Organization “Chashmai Ehson”; Public Organization “Children’s World”, Kulob; Public Organization of Hearing-Impaired Children, Rudaki; Public Organization “Nuri Oftob”; Public Organization “Dilshod”; republican boarding school for children with poliomyelitis, Hissor; Republican Centre for Labour-related Diseases; Republican Centre for Medical Statistics and Information; Republican Clinical Centre for Mental Health of Children and Adolescents; Republican Clinical Centre for Ophthalmology; Republican Clinical Centre for Psychological Problems; Republican Clinical Centre for Orthopaedics and Traumatology; Republican Medical College (Dushanbe and Khujand); Republican Physiotherapy Hospital, Khujand; Republican Rehabilitation Centre for Children, Vakhdat (Macheton); residential care institutions for adults and persons with disabilities (Khujand, Yavan, Bokhtar, Jabbor Rasulov, Penjikent, Vakhdat, Karatag); residential care institutions for intellectually impaired people (Vose, Hissar); social assistance at home units (Dushanbe, Khujand, Bobojon Gafurov); Society of Disabled People in Dushanbe “Imkoniyat”; Boarding schools for deaf and hearing-impaired children (Bobojon Gafurov, Rudaki); Tajikistan Mine Action Centre; Tajik State Medical University; Territorial Centre for Social Services for Elderly and People with Disabilities, Ghonchi; Territorial Centre for Social Services at Home for Elderly and Disabled People, Dushanbe; Training and Practical Unit for Social Work and Innovations, Varzob; United Nations Development Programme (UNDP); United Nations Children's Fund (UNICEF); Union of Disabled of Chernobyl; United Nations Women.
iv

Financial supportThis situational assessment has been made possible by the support of the American people through the United States Agency for International Development (USAID). The contents do not necessarily reflect the views of USAID or the United States Government.
v
vi
Abbreviations ASIP DRS GDP ICF PWD
PMPC RCST
TJS UNICEF
UNDP USAID VKK VMKB
VTEK
Agency on Social Insurance and Pensions Districts of Republican Subordination gross domestic product International Classification of Functioning, Disability and Health persons with disabilities
psychological, medical and pedagogical consultation Red Crescent Society of Tajikistan
Tajik somoni (currency) United Nations Children’s Fund
United Nations Development Programme United States Agency for International Development Doctors’ Consultative Commission Gorno-Badakhshan Autonomous Region (Viloyati Mukhtori Kuhistoni Badakhshon) Doctor’s Vocational Expert Commission centre
Executive summary The availability of rehabilitation services for people with disabilities in Tajikistan has increased in recent years. Many of the current pilot rehabilitation programmes show great promise, despite the harsh geography of the country and the difficulty of extending services to everyone who needs them. However, current rehabilitation services remain inadequate to serve the needs of the population, both as regards the quantity of services available and their quality. The main challenges can be summarized as follows:
• lack of a strategy on disability and a limited legislative framework;
• lack of professional-level human resources in the field of rehabilitation;
• lack of rehabilitation services at all levels, especially in rural areas where mostpeople live;
• lack of quality standards and adequate monitoring of disability and rehabilitationservices;
• limited funding for disability and rehabilitation activities;
• poor coordination among the few stakeholders supporting disability and rehabilitationin Tajikistan;
• limited involvement of people with disabilities in decision-making;
• a general lack of information about the benefits and potential of rehabilitationservices to reduce impairment and disability and promote inclusion and participation.
The consolidation of disability issues under the new Ministry of Health and Social Protection is a potential asset. The Ministry needs to show leadership in coordinating a multisectoral and multidisciplinary response. This requires:
• development of an appropriate disability strategy and legislation and theirenforcement;
• human resource development for allied health professions in line with internationalstandards;
• identification and consensus on an appropriate service delivery model focusing onthe decentralization of rehabilitation services;
• action to address bottlenecks in rehabilitation service delivery;
• support for the development of a barrier-free, accessible and nondiscriminatoryenvironment;
• participation by persons with disabilities in decisions that directly affect their lives.Accession by Tajikistan to the Convention on the Rights of Persons with Disabilities would provide an overall framework for and create synergies in the disability and rehabilitation response. Tajikistan is currently moving from “side-stream” rehabilitation services to “mainstream” services. There is a growing awareness of the need for and benefits of rehabilitation services and their contribution to the empowerment of people with disabilities. This transition needs to be supported to ensure the provision of quality rehabilitation services that can contribute to the development of an inclusive, rights-based society with equal opportunities for all.
vii

Introduction Disability is a public-health, human-rights and development issue. The overall health of persons with disabilities is poorer than that of the general population, and their health and rehabilitation needs more often remain unmet. Disability is a human-rights issue because persons with disabilities experience inequality, are subject to multiple violations of their rights and are denied autonomy. Disability is a development issue because disability and poverty reinforce and perpetuate one another. Disability may lead to lower living standards and poverty owing to lack of access to education and employment and the increased expenditure related to disability. Rehabilitation services build human capacity and can be instrumental in enabling persons with disabilities to remain in or return to their home or community, live independently, and participate in education, the labour market and civic life. They can reduce the need for formal support services as well as reducing the time and physical burden on caregivers. Tajikistan has shown tremendous potential for rehabilitation following the outbreak of poliomyelitis in 2010. However, the rehabilitation services currently available remain inadequate to serve the needs of the population, in terms of both quantity and quality. The main challenges can be summarized as follows:
• lack of a strategy on disability and a limited legislative framework;
• lack of professional-level human resources in the field of rehabilitation;
• lack of rehabilitation services at all levels, especially in rural areas where mostpeople live;
• lack of quality standards and adequate monitoring of disability and rehabilitationservices;
• limited funding for disability and rehabilitation activities;
• poor coordination among the few stakeholders supporting disability and rehabilitationin Tajikistan;
• limited involvement of people with disabilities in decision-making;
• a general lack of information about the benefits and potential of rehabilitationservices to reduce impairment and disability and promote inclusion and participation.
These challenges contribute to the disadvantages experienced by persons with disabilities, many of which are avoidable.
General information about Tajikistan Tajikistan is located in the south-west of the Central Asia region, covering a territory of 142 600 km in total (Fig. 1). To the west and to the north, it borders Uzbekistan, to the east and north Kyrgyzstan, to the south Afghanistan and to the east China. Tajikistan is divided into four administrative divisions: two provinces (viloyatho – Khatlon in the south and Sughd in the north), one autonomous province (viloyat) in the east, Gorno-Badakhshan Autonomous Region (Viloyati Mukhtori Kuhistoni Badakhshon - VMKB) and the centrally located Districts of Republican Subordination, governed directly from Dushanbe city. Each region consists of smaller administrative zones, called districts (nohiyaho). There are 58 districts, 17 cities and 57 townships in Tajikistan (1). The population remains essentially rural. In January 2012, out of a total population of 7.807 million people, 2.064 million lived in urban areas and 5.742 million in rural areas; the rural population is thus 73.6% of the total. As the result of high birth-rates and
1

population growth, the population remains young: 35.2% of the population are aged 15 years or younger, whereas people of 65 years or over constitute only 4.7% of the total population (1). After independence, Tajikistan underwent a period of difficult economic transition compounded by the civil war that raged between 1992 and 1997. As a result, Tajikistan’s gross domestic product (GDP) contracted, from US$ 2.6 billion in 1990 to only US$ 860 million in 2002, and inflation soared, resulting in severe curtailments in health, education and social spending. Although the economy has been recovering since 2000, it was further hit by the financial crisis of 2008, and Tajikistan remains a low-income country. Tajikistan ranks 127th on the Human Development Scale (2): 41% of the population still lives below the poverty line and 17% below the extreme poverty line. Fig. 1. Map of Tajikistan
Source: based on United Nations Office for the Coordination of Humanitarian Affairs/ReliefWeb data.
Methodology The WHO Country Office, Tajikistan, in partnership with the Government, is implementing a three-year disability rehabilitation programme for development of a national rehabilitation policy, system and services focusing on community-based rehabilitation and human resource development in the field of rehabilitation. This situational analysis on the current gap, need and opportunities for intervention in the field of rehabilitation in Tajikistan was developed as part of this programme. The methodology for the situational analysis was formulated in November and December 2013. The goal is to assess the availability and quality of rehabilitation services in Tajikistan, including the following objectives.
2
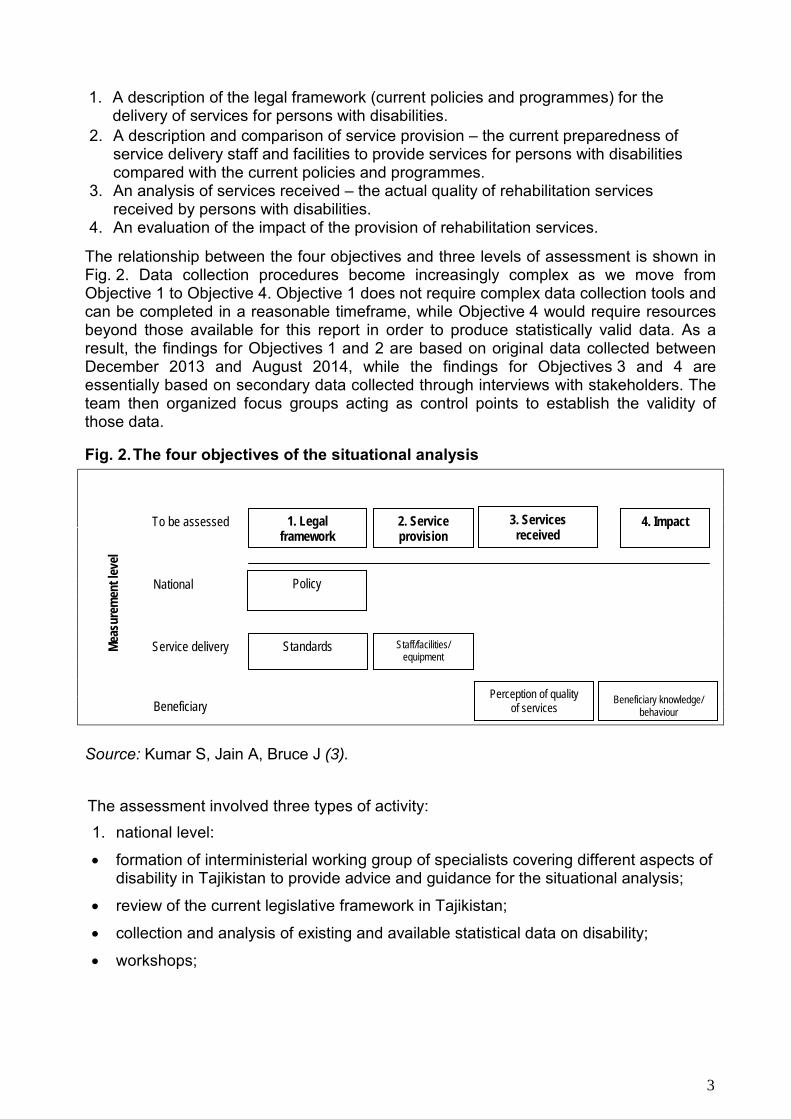
2. A description and comparison of service provision – the current preparedness ofservice delivery staff and facilities to provide services for persons with disabilitiescompared with the current policies and programmes.
3. An analysis of services received – the actual quality of rehabilitation servicesreceived by persons with disabilities.
4. An evaluation of the impact of the provision of rehabilitation services.
The relationship between the four objectives and three levels of assessment is shown in Fig. 2. Data collection procedures become increasingly complex as we move from Objective 1 to Objective 4. Objective 1 does not require complex data collection tools and can be completed in a reasonable timeframe, while Objective 4 would require resources beyond those available for this report in order to produce statistically valid data. As a result, the findings for Objectives 1 and 2 are based on original data collected between December 2013 and August 2014, while the findings for Objectives 3 and 4 are essentially based on secondary data collected through interviews with stakeholders. The team then organized focus groups acting as control points to establish the validity of those data.
Fig. 2. The four objectives of the situational analysis
Source: Kumar S, Jain A, Bruce J (3).
To be assessed
Standards
Policy
1. Legalframework
2. Serviceprovision
3. Servicesreceived
4. Impact
Staff/facilities/ equipment
Service delivery
Beneficiary Perception of quality
of services Beneficiary knowledge/
behaviour
Mea
sure
men
t lev
el
National
The assessment involved three types of activity: 1. national level:
• formation of interministerial working group of specialists covering different aspects ofdisability in Tajikistan to provide advice and guidance for the situational analysis;
• review of the current legislative framework in Tajikistan;
• collection and analysis of existing and available statistical data on disability;
• workshops;
1. A description of the legal framework (current policies and programmes) for thedelivery of services for persons with disabilities.
3

2. service-delivery level:
• visits to selected service providers throughout the country, including bothGovernmental and nongovernmental facilities, in major urban areas and in ruralareas;
• visits and interviews with stakeholders, including educational facilities, Stateagencies and local authorities; and
3. beneficiary level:
• interviews with members of civil society and international organizations involved indisability issues;
• focus groups of people with disabilities in urban and rural areas.The national workshop took place in December 2013, with the participation of a large number of stakeholders involved in disability and rehabilitation, including representatives of the Ministries of Health and Social Protection of the Population, Labour and Social Protection of the Population and Education and Science, United Nations agencies, national and international nongovernmental organizations and disabled people’s organizations, and representatives of various facilities linked with rehabilitation, including staff members of polyclinics and the prosthetic and orthotic centre. The workshop aimed to present the situational analysis to the various actors and gather information from them in order to focus the research more efficiently. It provided several subjects for preliminary reflection, the results of which were used when formulating the recommendations of this report. It should be noted that, during the course of the situational analysis, the social protection portfolio was transferred from the Ministry of Labour to the Ministry of Health, now called the Ministry of Health and Social Protection. Following the national workshop, visits, interviews and focus groups were organized between January and May 2014, and a zero draft of this report was then produced. This draft was presented to the Government of Tajikistan and the various stakeholders between July and September 2014. Following further recommendations and modifications, the final draft version was produced in October 2014. The final draft version was again presented to various stakeholders for review and feedbacks. Following further inputs and modification, the final version of the report was produced in December 2014. This situational analysis is relevant to all persons who experience disability. The analysis covers persons who have long-term impairments – those who are traditionally understood as disabled, e.g. persons with a physical disability or those who are blind or deaf – and also the wider group of persons who experience difficulties in functioning owing to a wide range of health conditions, e.g. chronic or noncommunicable diseases, neurological disorders and infectious diseases. The WHO World report on disability defines rehabilitation as “a set of measures that assist individuals who experience, or are likely to experience, disability to achieve and maintain optimal functioning in interaction with their environments” (4). Rehabilitation is, therefore, essentially a multisectoral discipline. However, this report focuses on the health aspects of rehabilitation, namely therapy (physiotherapy, occupational therapy, speech therapy, orientation and mobility training, etc.), assistive technology (prostheses, orthoses, wheelchairs, hearing aids, white canes, etc.) and rehabilitation medicine. But while the medical aspect of rehabilitation remains at the core of this situational analysis – and this is reflected in the data collected, in the findings and in the recommendations – the human-rights aspect of disability is too strongly intertwined with the medical condition to be ignored in any analysis of rehabilitation services. This analysis therefore summarizes the current situation in the fields of health, education, social assistance and support and enabling environment for people with disabilities in Tajikistan.
4
Preliminary preparations included a full mapping of rehabilitation service providers in Tajikistan in the sectors of health, social protection and education. Although the total number of service providers is not unreasonably high, it was clear from the onset that it would not be possible to visit and/or interview every stakeholder and service provider in the country. Nevertheless, the team was able, with the support of the Ministry of Health and Social Protection and the Government of Tajikistan, to gain full access to a large number of facilities and agencies throughout the country, in both urban and rural areas. These were mostly in the health sector, but included facilities from other sectors in order to provide a broader perspective. The validity of the findings has been further strengthened by the homogeneity of the situations observed. While this situational analysis describes the state of rehabilitation services only in broad terms, we believe that it gives an accurate picture at this point. The report goes into the details of rehabilitation (terminology, international reference standards, etc.) as it is envisaged that the content and findings of the report will also serve as a tool for awareness generation as well as advocacy. It is hoped that it will help to improve the quality of life of persons with disabilities in Tajikistan.
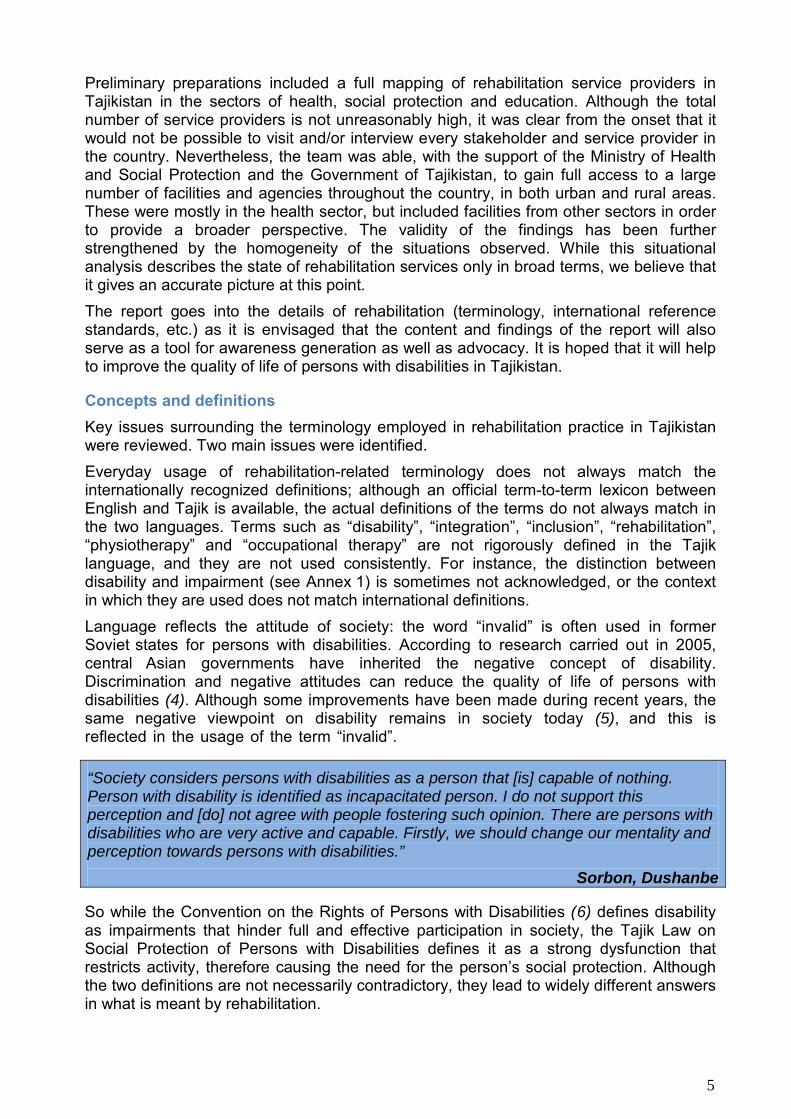
Concepts and definitions Key issues surrounding the terminology employed in rehabilitation practice in Tajikistan were reviewed. Two main issues were identified. Everyday usage of rehabilitation-related terminology does not always match the internationally recognized definitions; although an official term-to-term lexicon between English and Tajik is available, the actual definitions of the terms do not always match in the two languages. Terms such as “disability”, “integration”, “inclusion”, “rehabilitation”, “physiotherapy” and “occupational therapy” are not rigorously defined in the Tajik language, and they are not used consistently. For instance, the distinction between disability and impairment (see Annex 1) is sometimes not acknowledged, or the context in which they are used does not match international definitions. Language reflects the attitude of society: the word “invalid” is often used in former Soviet states for persons with disabilities. According to research carried out in 2005, central Asian governments have inherited the negative concept of disability. Discrimination and negative attitudes can reduce the quality of life of persons with disabilities (4). Although some improvements have been made during recent years, the same negative viewpoint on disability remains in society today (5), and this is reflected in the usage of the term “invalid”.
“Society considers persons with disabilities as a person that [is] capable of nothing. Person with disability is identified as incapacitated person. I do not support this perception and [do] not agree with people fostering such opinion. There are persons with disabilities who are very active and capable. Firstly, we should change our mentality and perception towards persons with disabilities.”
Sorbon, Dushanbe
So while the Convention on the Rights of Persons with Disabilities (6) defines disability as impairments that hinder full and effective participation in society, the Tajik Law on Social Protection of Persons with Disabilities defines it as a strong dysfunction that restricts activity, therefore causing the need for the person’s social protection. Although the two definitions are not necessarily contradictory, they lead to widely different answers in what is meant by rehabilitation.
5

The English language unfortunately suffers from similar issues. Not only is the vocabulary associated with disability often misused in common parlance, key terms have been redefined over the years as the conceptualization of disability evolved. It is therefore useful in the framework of this analysis to reiterate the terminology currently in use by the United Nations, so as to provide a common ground for all readers. Definitions of key terms used in this analysis are presented below, and a more comprehensive lexicon is provided in Annex 1. Various definitions of disability are used in Tajikistan, depending on the policy or purpose for which disability is being defined. WHO considers “disability” to be the umbrella term for impairments, activity limitations and participation restrictions, referring to the negative aspects of the interaction between an individual (with a health condition) and that individual’s contextual factors (environmental and personal factors) (4). Disability results from the interaction between persons with impairments and attitudinal and environmental barriers that hinder their full and effective participation in society (6). Intervention is required to remove environmental and social barriers. For this situation analysis, the authors bore in mind the wording of Article 1 of the Convention on the Rights of Persons with Disabilities: “Persons with disabilities include those who have long-term physical, mental, intellectual or sensory impairments which in interaction with various barriers may hinder their full and effective participation in society on an equal basis with others”. The concept of rehabilitation, as defined in the Convention on the Rights of Persons with Disabilities and the United Nations Standard Rules on the Equalization of Opportunities for Persons with Disabilities (7), is wide and addresses the areas of health, education, employment and social services. Rehabilitation is described in the Convention on the Rights of Persons with Disabilities as “… appropriate measures, including through peer support, to enable persons with disabilities to attain and maintain maximum independence, full physical, mental, social and vocational ability, and full inclusion and participation in all aspects of life” (6).The ultimate aim of rehabilitation is to provide the individual with opportunities for full and effective participation and inclusion in society, including studying, working and access to all services, that are equal to those of other citizens. Rehabilitation teams and specific disciplines may work across different categories of disability. Depending on the individual country context, additional disciplines may be added to the rehabilitation team. In general, the following specialists are closely involved in rehabilitation: • physiotherapist
• physiotherapy technician and/or assistant
• occupational therapist
• occupational therapy technician and/or assistant
• prosthetist and orthotist1
• speech therapist2
1 Prosthetists and orthotists provide care and aids/devices intended to improve functioning in people with physical impairments. Orthotic care involves the provision of external appliances designed to support, straighten or improve the functioning of a body part (e.g. calipers, braces). Prosthetic interventions involve the provision of an artificial external replacement for a missing body part (e.g. artificial limbs). 2 Speech therapists work to restore people’s capacity to communicate effectively and to swallow safely and efficiently.
6

Physiotherapy (physical therapy) comprises services which help individuals to maintain and maximize their movement and functional ability (for example through exercises or movement training or stretching). For more information, see Annex 1. Occupational therapy comprises services which help individuals to participate in the activities of everyday life (for example teaching people to feed themselves safely or adapting the home to their needs). For more information, see Annex 1. Prosthetics and orthotics comprise provision of an artificial external replacement for a body part (prosthetics) or external appliances designed to support, straighten or improve the functioning of a body part (orthotics), and of the related care (4). Assistive technology and assistive devices are terms that are often used interchangeably. An assistive device is “any item, piece of equipment or product […] that is used to increase, maintain or improve the functional capabilities of individuals with disabilities” (4) (e.g. eyeglasses, hearing aids, wheelchairs). Assistive technology is an umbrella term covering both assistive devices themselves and the provision of related services.
Data-gathering and limitations Primary data were collected during interviews, focus group exercises and direct visits to selected institutions and facilities. Secondary data were obtained by reviewing a wide range of published literature and reports, as well as data made available to us by the Government of Tajikistan. In order to complete the analysis in a reasonable timeframe, a limited subset of facilities was selected, located in the capital, Dushanbe, the surrounding Districts of Republican
Subordination and the northern Sughd region. These facilities reflect the highly centralized structure of medical services, while still providing an overview of the availability of these services in rural areas, and included a range of facilities run by civil society, with or without Government support. Although this methodology limits the comprehensiveness of the analysis, there was no indication at the review by the stakeholders that the conclusions drafted are inaccurate for other regions of Tajikistan. Secondary data, including statistics, were kindly provided by the Government of Tajikistan through its Statistical Agency and the Ministry of Health and Social Protection. The drafting of the situational analysis took place at the beginning of 2014, with the various agencies providing figures for 2013 as they became available. However, discrepancies were observed in the data provided, in particular:
• physical medicine and rehabilitation doctor1
• social worker2
• psychologist3
• rehabilitation nurse.
1 Rehabilitation doctors (physiatrists) diagnose health conditions, assess functioning and prescribe medical and technological interventions to treat the condition and optimize functional capacity. 2 Professional social workers restore or enhance the capacity of individuals or groups to function well in society, and help society to accommodate their needs. 3 Psychologists are professionals specializing in diagnosing and treating diseases of the brain, emotional disturbance and behaviour problems, more often through therapy than through medication.
7

• discrepancies between the figures provided by different agencies, and discrepanciesbetween data provided by an agency and the data provided by an individualinstitution under that agency (problem in the collation of individual reports at a higherlevel);
• discrepancies in the availability of data between geographical areas – district-leveldetailed data may be available for one region while only a summary of collatedregional data is available for another, limiting any attempts to compare figuresbetween geographical areas.
Although probably stemming from an underdeveloped system of monitoring and data collection, these inconsistencies are not indicative of fundamentally flawed figures, provided that the analysis is confined to the analysis of people with disabilities who are registered within the system. Of greater concern, and a more significant barrier to a correct assessment of the current situation of rehabilitation in Tajikistan, is the lack of data collection relating to the part of the population that is not officially recognized as having a disability. Although some of the ministries and agencies have their own figures relating to persons with disabilities, no consistent effort has been made to collect reliable data. For instance, all existing data concerning numbers of persons with disabilities and the prevalence of disabling conditions relate to individuals who have acquired a disability certificate through official means, thus excluding from the statistics all those who have not registered, whether through lack of knowledge or an unwillingness to register. And although civil society, notably nongovernmental organizations with a local presence in remote areas, may have collected their own figures, it is impossible to access these at a national level. Another major concern is the limited quantity of statistics concerning other disabling conditions, such as noncommunicable diseases (cardiovascular disease, diabetes, etc.), HIV/AIDS, etc. Noncommunicable diseases — including cancer, cardiovascular disease, chronic respiratory diseases, diabetes, mental health and neurological disorders (such as Alzheimer’s disease) — are the leading cause of disability and death worldwide, since many people with noncommunicable diseases are likely to develop disabilities as their disease progresses (8). According to the WHO health status report Highlights on health in Tajikistan 2005, noncommunicable diseases accounted for about 80% of all deaths in Tajikistan and cardiovascular disease alone is responsible for 57% of overall mortality (9). Tajikistan is one of the countries where HIV prevalence has increased by more than 25% over the last 10 years (10). Too often, individuals with a disability have not been included in HIV prevention and AIDS outreach efforts because it is assumed that they are not sexually active and therefore at low or no risk of HIV infection. In fact, people with physical, sensory and intellectual disabilities are among the most vulnerable to the impacts of AIDS (11). In addition, throughout history, Tajikistan has experienced many natural and man-madedisasters and adverse events, which further contribute to the prevalence of vulnerable populations and persons with disabilities.
While it is not within the scope of this report to assess the existing gaps in data, it should be noted that WHO generally recognizes that 15% of the population have a disability. With a current population of about 7.8 million inhabitants, Tajikistan can be expected to be home to about 1.17 million persons with a disability, while the official figure for 2012 for registered persons with disabilities is only 171 447.
8
Legislation and services relevant to persons with disabilities
Legislative framework relating to disability The function of policy in the disability sector is to remove the barriers to full inclusion faced by persons with disabilities and their families in all aspects of life. Policy at all levels of government should address the systematic dismantling of barriers that prevent persons with disabilities from being full and active citizens. In this situational analysis, the existing legislative framework in Tajikistan was reviewed in order to determine whether it adequately promotes the rights of persons with disabilities. A detailed analysis of Tajik legislation relating to rehabilitation appears in Annex 2. People with disabilities are granted specific rights under Tajik legislation. Some pieces of legislation are fully geared towards persons with disabilities, but the majority of these rights are defined in subsections and articles. The legislative texts often do not provide an implementation framework, with these details being published afterwards in additional decrees and strategy documents. In addition, several multiyear plans aimed at implementing services aimed specifically or in part at people with disabilities are currently in operation, including the National Development Strategy, which runs until 2015, and the Living Standards Improvement Strategy of Tajikistan for 2013−2015 (12). Although the Government of Tajikistan set up the Coordination Council on social protection for people with disabilities in 2011, there is neither a national strategic document with a holistic and consistent approach, nor a precise action plan for the sector defining roles and responsibilities. Despite a body of law that, taken as a whole, has the potential to define the rights of persons with disabilities adequately, this fragmentation constitutes a major barrier to the implementation of a coherent system of services. The Tajikistan Constitution (1994, amended in 2003) also protects the rights of persons with disabilities, describing their rights to medical services, education, social welfare services, housing and leisure facilities, as well as their equality in society. According to the Constitution, every individual, including people with disabilities, shall be treated equally and has the right to all services guaranteed by the Government.
Tajik legislation stipulates additional specific rights for persons with disabilities and their families in a range of laws, among them the Law on Social Protection of Persons with Disabilities (2010), the Law on Pensions (1993, 2012), the Family Code (1998, 2008), the Housing Code (1997), and the Law on Health Care (1997, 2013). A number of Government decrees set out the exact entitlements in more detail. Moreover, several pieces of legislation provide the general framework for rehabilitation of persons with disabilities. However, these laws do not focus specifically on rehabilitation, but are derived from the larger framework relating to disabilities (Law on Social Protection of Persons with Disabilities), injuries (National Programme on Preventing Trauma and Modernization of Medical Care in Case of Trauma and its Consequences in the Republic of Tajikistan for the Period 2010–2015 (2010)), and the provision of category-specific services (as in the Law on Social Services (2008) and Law on Medical and Social Protection of Persons with Diabetes (2012) and the Regulation on Providing Persons with Disabilities with Technical Assistive Devices for Rehabilitation (2011)). The Law on Social Protection of Persons with Disabilities, approved in December 2010, represents a significant advance on the 1991 law with the same title and lays the basic foundations for compliance with the Convention on the Rights of Persons with Disabilities.
9
The Law states that it “shall determine the legal, economic and organizational basis for ensuring the social protection of disabled persons and provide them with equal opportunities for vital activity and integration into society” (13). However, the Law needs to be strengthened and amended to cover all aspects of disability (both mainstream and disability-specific) with specific assignment of responsibilities and development of institutional and organizational capacity to promote, facilitate and support the design, implementation, monitoring and evaluation of the provisions of the Law.
A number of laws1 provide for social welfare services for persons with disabilities. The state guarantees monthly pensions for the elderly, those living with disabilities, survivors (i.e. families that have lost their breadwinner) and other special-merit individuals (e.g. Second World War veterans, persons affected by the Chernobyl nuclear accident, Olympic athletes, etc.). The amount of the assistance depends on the person’s disability group and individual situation. Finally, pursuant to a 2008 decree of the Government of Tajikistan, additional social assistance is provided through the transfer of compensation payments for gas and electricity for families with two or more children with disabilities and single parents with disabilities who care for a child with disabilities. In addition, a number of pieces of legislation2 relate to the realization of the right to health and rehabilitation in Tajikistan. The National Health Strategy of the Republic of Tajikistan for the Period 2010–2020, adopted in 2010, is the main policy governing the health-care sector. Although it recognizes that rehabilitation of chronically ill patients and disabled people is an important factor in reducing the burden of disease, the Strategy does not focus specifically on persons with disabilities or their rehabilitation. Improvement of the accessibility, quality and efficiency of health services is one of the stated priorities of the Strategy. Under access of the population to health care, the Strategy refers only to establishing new health-care facilities. Physical access by people with disabilities to existing health-care facilities, which is one of the main obstacles faced by people with disabilities, is not mentioned.
In 2011, the Government of Tajikistan adopted a programme on provision of a basic benefits package for medical services for 2012–2013 in pilot areas.3 The basic benefits package is designed to provide free access to primary health care for all and free hospital services for certain groups, while others make a nominal copayment.
1 Law on Social Services, Law on Pensions and Law on State Social Insurance (1997, 2008); Regulation on Providing Quotas for Employment for Specific Groups of the Population (2009, 2011), Regulation on Approval of the Scope and Procedures for Provision of Free Social Care Services (2012), Regulation on Providing People with Disabilities with Sanatorium Treatment (2011), Procedures on Provision of Pensions, Allowances and Other Types of Social Benefits for Citizens of the Republic of Tajikistan (1999), Procedures on Approving the List of Medical Indications Allowing Rights for Social Pensions and Benefits for Children with Disabilities up to 18 Years of Age (2013), Procedures on Approving the List of Specialized Products for Personal Use for the Disabled, the Supply and Import of Which are Exempt from Value Added Tax (2006, 2012). 2 National Programme on Preventing Trauma and Modernization of Medical Care in Case of Trauma and its Consequences in the Republic of Tajikistan for the Period 2010–2015, National Programme on Prevention, Diagnosis and Treatment of Diabetes in the Republic of Tajikistan for the Period 2012–2017, Regulation on Providing Persons with Disabilities with Technical Assistive Devices for Rehabilitation (2011), Procedures for Providing Medical Care for Victims of Road Accidents (2012). 3 These areas are: Sarband, Norak, Tursunzoda, Dangara, Spitamen, Rasht, Shahrinav and Varzob.
10

The categories exempted from payment include Second World War veterans, persons disabled from birth, children with disabilities aged up to 18 years, orphan children and children living in residential care institutions, persons affected by the Chernobyl nuclear accident and their families, persons disabled during military service, babies up to 1 year old, disabled people in groups I and II who were injured in the workplace, adults from the age of 80 years, adults living in residential institutions and individuals with particular medical conditions such as HIV/AIDS and diabetes. Patients who are not exempt but are referred by a primary health care worker pay 50% of the average cost of the required health service, while those without a referral pay 70%. As is the case with many other legislative and normative documents, in practice the majority of persons with disabilities are not aware of these provisions and have difficulty obtaining a referral to the services.
In 2005, Tajikistan signed the Mental Health Declaration (14) and Mental Health Action Plan for Europe (15), which called upon WHO Member States to establish mental health policies, programmes and legislation based on current knowledge and considerations regarding human rights, in consultation with all stakeholders in mental health. Tajikistan still lacks a comprehensive national plan addressing mental health. The Law on Psychiatric Care (2002), the primary law governing the provision of mental health services in Tajikistan, has not been fully implemented and many of its provisions are outdated (16). Recognizing the challenges of persons with disability and their family members, the Ministry of Health and Social Protection, in consultation with a wide range of stakeholders, developed a six-year (2014−2019) position paper entitled “Better Health for Persons with Disabilities for an Inclusive Society in Tajikistan”. The vision of the position paper is a country where persons with disabilities and their families enjoy the highest attainable standard of health: the overall goal is to contribute to achieving health, well-being and the enjoyment of human rights for persons with disabilities. Its objectives are as follows:
• to address barriers and improve access to health-care services and programmes;
• to strengthen and expand rehabilitation services;
• to support the collection of appropriate data on disability and promotemultidisciplinary research.
Tajikistan remains the only Central Asian country that has not signed the Convention on the Rights of Persons with Disabilities, although the country is party to over 60 international treaties that recognize the right to health (see Annex 2). In accordance with Article 10 of the Constitution of 1994, international legal instruments that are recognized by Tajikistan become a constituent part of its national legal system.
“I do not know exactly about rights and benefits that our Government is providing. I only know that [a] person with disability has some sort of benefits for communal services, but such benefit does not apply to other members of the family. If the person with disabilities is the head of the household and he is registered as an owner of the apartment, he will get 50% discounts for paying bills for the gas, electricity and water. There are public transport benefits but in our city this benefit not applicable as we are paying for travel [by] public transport. Although there is [a] one-time benefit for purchasing medicines, nobody in the medical institutions would tell us about [it] unless we reach for the head [of the institution].”
Zukhro, Dushanbe
11

Under these conventions,Tajikistan has obligations regarding children and women with disabilities and the vocational rehabilitation of persons with disabilities. Accession to the Convention on the Rights of Persons with Disabilities would help to coordinate the implementation of national laws and responsibilities under other international conventions. Although the Government of Tajikistan has several pieces of legislation that could be applied to persons with disabilities, the relevant legislation is still fragmented and lacks a comprehensive national document which could act as a reference point for disability services. The failure to implement existing laws is another obvious problem in Tajikistan. Although the national legislation provides for the rights and freedoms of persons with disabilities, these are not always transformed into reality. Thus, many persons with disabilities do not, in practice, have access to health care, education, social services, employment or justice. The medical view of disability as something which is the individual’s own fault dominates in the legislation, while international standards highlight the obstacles caused by the society that lead to the exclusion of persons with disabilities. Tajik legislation treats persons with disabilities as being in need of protection – as manifested in the Law on Social Protection of Persons with Disabilities. In order to improve access of persons with disabilities to all services guaranteed by the Government, a strategic national programme dealing specifically with the rights of persons with disabilities is required, which must be consistent with the Convention on the Rights of Persons with Disabilities and incorporate the various international treaties to which Tajikistan is party. Current legislation (i.e. the Law on Social Protection of Persons with Disabilities) needs to be updated to bring it into line with best international practices, particularly the Convention on the Rights of Persons with Disabilities, to make it consistent with other national legislation and to promote a rights-based approach to disability.
Overview of health-care, education, labour and social protection systems The health, education, labour and social protection sectors are major components in the rehabilitation of persons with disabilities. This overview presents the current state of these sectors and the mechanisms through which persons with disabilities can access disability-specific services.
Health care Tajikistan has inherited the Soviet model of health care, with limited structural changes so far. The Ministry of Health and Social Protection is responsible for national health policy, although it has limited control over the overall health budget, and directly manages most health facilities at the national level. Local authorities are responsible for local health services. See Annex 3 for the structure of the Ministry. The various structures range from dispensaries and primary health points at the district (rayon) level, to city and district hospitals and polyclinics. At the top of the referral pyramid, the national and republican centres (the latter obtaining that status by Presidential decree only) offer tertiary care (specialized services) in their respective disciplines within the public health system. The health system is highly centralized, with the vast majority of national and republican centres situated in Dushanbe or the surrounding Districts of Republican Subordination.
The quality of services and the infrastructure suffered greatly from a sharp decline in expenditure in the health sector following independence and the civil war that took place between 1992 and 1997. Public expenditure fell from 4.5% of GDP in 1991 to only 0.9% in 2002. As a result, and although the system remains nominally free to access, out-of-. pocket payments became a major part of total health spending, reaching 78.8% of total
12

spending in 2005 (17). Public health spending has increased significantly since 2002, reaching 2.8% of GDP in 2012, while Tajikistan’s GDP itself grew considerably, from US$ 1.5 billion in 2002 to almost US$ 7 billion in 2012 (18). However, the increased spending has been insufficient to slow down the ageing of the health facilities and equipment, and the Joint Annual Review for 2011/12 emphasizes the fact that the low level of funding by the state compared with out-of-pocket payments, which constitute a barrier to access to essential health services for the most vulnerable people, is a major challenge (19).
The Tajik health system is now undergoing a complex transition to a new health system with new mechanisms of management, financing and operation. There are plans for a fundamental reform of the system intended to increase the availability of medical services. Support will be provided for the implementation and monitoring of the Conceptual Plan for Health Care Reform and the Basic Programme for the Delivery of Medical Care and Public Health Services, which will help improve the quality and availability of medical care (12). There is a serious imbalance in the distribution of the material base and budget between primary health care and hospital services, as a result of which the bulk of the funding goes to secondary health care (hospitals), where the services provided are expensive and out of reach of the poor (20).
Fig. 3 shows the flow of financing in the disability and rehabilitation system. The exception is Dushanbe and the Districts of Republican Subordination, where funds are sent directly to the city/district finance administration.
Ministry of Finance
Ministry of Health and Social Protection
State Agency on Social Protection
Provincial (oblast) administrations
Republican facilities
Residential care institutions
Nongovernmental organizations
Provincial finance departments
District (rayon) finance
administrations
Provincial health administrations
District health administrations
Citizens Out-of-pocket payments
Fig. 3. Financial flows in the disability and rehabilitation system
Source: adapted from Law No. 395 on State Finances of the Republic of Tajikistan (18 June 2008).
13

Until recently, health services for people with disabilities were provided by structures belonging to two separate ministries, the Ministry of Health and the Ministry of Labour and Social Protection. The structure of the ministries was reviewed following the presidential election of 2013, and many of the services, units and structures under the supervision of the Ministry of Labour and Social Protection were transferred to the Ministry of Health, which was renamed Ministry of Health and Social Protection to reflect its new responsibilities. All Government structures providing specialized services for people with disabilities are now under the supervision of the Ministry of Health and Social Protection, with the exception of boarding schools, which remain the responsibility of the Ministry of Education, although medical staff working in these facilities also report to the Ministry of Health and Social Protection. Although the recent changes have raised fears among nongovernmental stakeholders that the newly formed Ministry will be less focused on the social aspect of rehabilitation and that the range of social services available may decrease, the change allows for a clearer structure and avoids pitfalls in interministerial cooperation. It is hoped that the newly formed Ministry will maintain a balanced approach to rehabilitation, in which all aspects of the field, both health-related and social-related,receive equal attention. In addition, the change opens the door to an eventual nomination of a focal point or service bringing together and fully dedicated to disability-related issues.
Access to service providers specializing in disabilities requires official recognition of the disabling condition and the acquisition of a “disability certificate”. Following a preliminary diagnosis by a general practitioner or local dispensary, the person is referred to higher-level facilities, where the disabling condition will be assessed. The person then presents this assessment to a medical commission, which determines whether the person qualifies for the status of a person with disabilities. For adults over 18 years of age, the commission in charge is the Agency for Medical and Social Examination (still colloquially known under its former Soviet name, VTEK – Doctor’s Vocational Expert Commission). Until 2008, these facilities were composed entirely of specialist commissions in charge of defining and categorizing disabilities in order for individuals to obtain disability-specific state allowances. After 2008, the responsibilities of the Agency for Medical and Social Examination were extended to include supervision and follow-up of individuals’ medical treatment and rehabilitation, as well as social programmes. The Agency employs 130 full-time doctors in various disability-related disciplines, and runs 32 facilities throughout the country. The Agency can also call upon additional specialists from any health facility when required. Commissions should be composed of at least five doctors, and additional medical tests can be required to support the original diagnosis. For children under 18 years of age, the commission in charge is the Doctor’s Consultative Commission (VKK). Every polyclinic that operates at city, regional or national level has a department of the Doctor’s Consultative Commission and the authority to set up an evaluation commission. Each commission is composed of one representative of the Doctor’s Consultative Commission, the family doctor who cares for the child, and one specialist in the relevant field from the polyclinic.1 The acquisition of a disability certificate is a key step in gaining access to specialized medical services, assistive devices, pensions and benefits, and to obtain a place in a boarding school or institution. In addition, the status of person with disabilities entitles the individual to free medical services, whether related to the disability or not.
1 It was announced at the time of writing that the two agencies in charge of providing disability certificates, the Agency for Medical and Social Examination and the Doctor’s Consultative Commission, will be merged in the near future.
14

Tajikistan does not use the International Classification of Functioning, Disability and Health,1 but instead employs its own categorization to determine the level of disability, and hence the range of services that can be accessed. Children with disabilities (two years and above) are placed in a single category, while adults are assigned to categories 1 to 3, with 1 representing the severest level of impairment. The category chosen depends on the individual’s motor function or mental ability, but does not place disability within any societal context or evaluate the environment as a positive or limiting factor. Because thecategories are not rigidly defined, borderline cases are common, which leads to a system that is open to manipulation. The lack of a universallyaccepted classification system is also a barrier to effective evaluation of the capacity and limitations of individuals and the formulation of suitable policies.
“I have acquired disability group III, which means that I am able to work. I was left-handed and lost my left hand. According to the Law of the Republic of Tajikistan on Pension Provision, if I would have lost my right hand, I would be considered as a disabled person of group II. In the meantime I am not working, I have got a family and three children. The disability pension I am entitled to is 90 TJS [Tajik somoni] per month, which is obviously not enough even for meeting very basic needs of myself and my family. I have referred to the Republican Agency for Medical and Social Examination in order to re-assess my case but nothing changed. Officials referred to the Law where indicated that the loss of left hand is to be considered as disability group III.”
Samad, Rasht district
Individuals who have acquired a disability certificate are required to revisit the evaluation commission every two years for reassessment. On such occasions, persons with disabilities can be moved from one category to another, or even lose their disability certificate altogether, depending on the development of their condition. The need for regular visits to maintain the status of the person with disabilities places a heavy burden on the most vulnerable people, especially those living in remote areas, because of both the cost and the difficulty of travelling through the country with a disabling condition. Official statistics on the prevalence of disability (171 447 persons in 2012) are based solely on the number of individuals that have officially gained the status of persons with disabilities. However, this figure excludes those people who would be recognized as having a disability under the Tajik classification, but who did not apply through the commissions for a variety of reasons. The rights of persons with disabilities and the services available to them are not well known to the general population, especially in rural areas. Also, the poorest people, especially persons with disabilities, do not always have the means to access the medical system in the first place. Cultural rejection of disability is another factor, and the more conservative groups of the population are unwilling to have themselves or their children officially classified in the disability system. Finally, among the more educated and wealthy groups of the population, some eschew the official system entirely, obtaining services through the private sector and abroad, mostly in the Russian Federation and the Islamic Republic of Iran.
1 The International Classification of Functioning, Disability and Health (ICF (http: www.who. int/ classifications/ icf/en) is a classification of health and health-related domains. As the functioning and disability of an individual occurs in a context, ICF also includes a list of environmental factors.
15

“My daughter has autism. Most doctors even do not know about this disabling condition. My great desire is that my daughter would be accepted by the society. Mothers who have child[ren] with autism want that members of the society would treat our children as other children. Recently [the] nongovernmental organization Iroda organized combined summer camp for children with autism, Down’s syndrome and other nondisabled children. It was such a great event. There was not [any] difference among children and we could not identify which child has got impairment and which does not. Children were communicating with each other; problem arises when communicating with adults. My daughter sometimes becomes aggressive: if she does not like something, she can pinch me. When we are in the [public] transport, during these moments of aggression people usually turn around to see what is happening. I got used to such attitude and now I do not pay attention. She is my daughter and she is my everything! During moments of aggression, I hug her and quietly sing a song, thereby calming her. When my daughter goes out to [the] playground, she does not usually join other children, she avoid[s] communication with other children. I think this is the main characteristic of children with autism, they do not know how to interact with other children even though they want to. Usually they live in their own world, and it is okay for them [to] play on their own.”
Firuza, Dushanbe
Education Education is the gateway to full participation in society. It is particularly important for children with disabilities, who are often excluded from society. Taking part at school is an important way for children with disabilities to correct misconceptions that prevent inclusion. The inclusion of children and adults with disabilities in education is important, as education contributes to human capital formation and is thus a key determinant of personal well-being and welfare; excluding children with disabilities from educational and employment opportunities has a high social and economic cost; and the country cannot achieve Education for All or Millennium Development Goal 2 (universal completion of primary education) unless children with disabilities are included in the education system. The National Concept on Inclusive Education focuses on the inclusion of children with disabilities in the overall educational process. The right to equal opportunities in the field of education is implicitly defined, and includes provisions on inclusive education for children with disabilities in mainstream pre-schools and basic and vocational education in appropriately equipped establishments. For children in residential care institutions, the Concept stipulates that these institutions shall be responsible for the education and upbringing of the children under their responsibility. In addition, the Concept provides for home-based education for children with disabilities who do not have the opportunity to be educated in specialized or mainstream educational establishments. It also provides for additional social assistance for families with two or more children with disabilities and for single parents of children with disabilities. Since 1997 and the end of Tajikistan’s civil war, which devastated the country’s schools along with other national infrastructure, the Government has made attempts to improve the country’s fragile education system. The National Strategy for Education Development (2006–2015) focuses on improving management, quality of education, equitable access, community participation and physical infrastructure. In Tajikistan, children with disabilities are offered various types of education, depending on the situation and their individual needs. The Law on Education (2004), as revised in 2013, stipulates that all children with disabilities have a right to education. By law, children with disabilities have access to assistance and special technical equipment in accordance with their needs, whether they are in a mainstream or a special school. If a
16
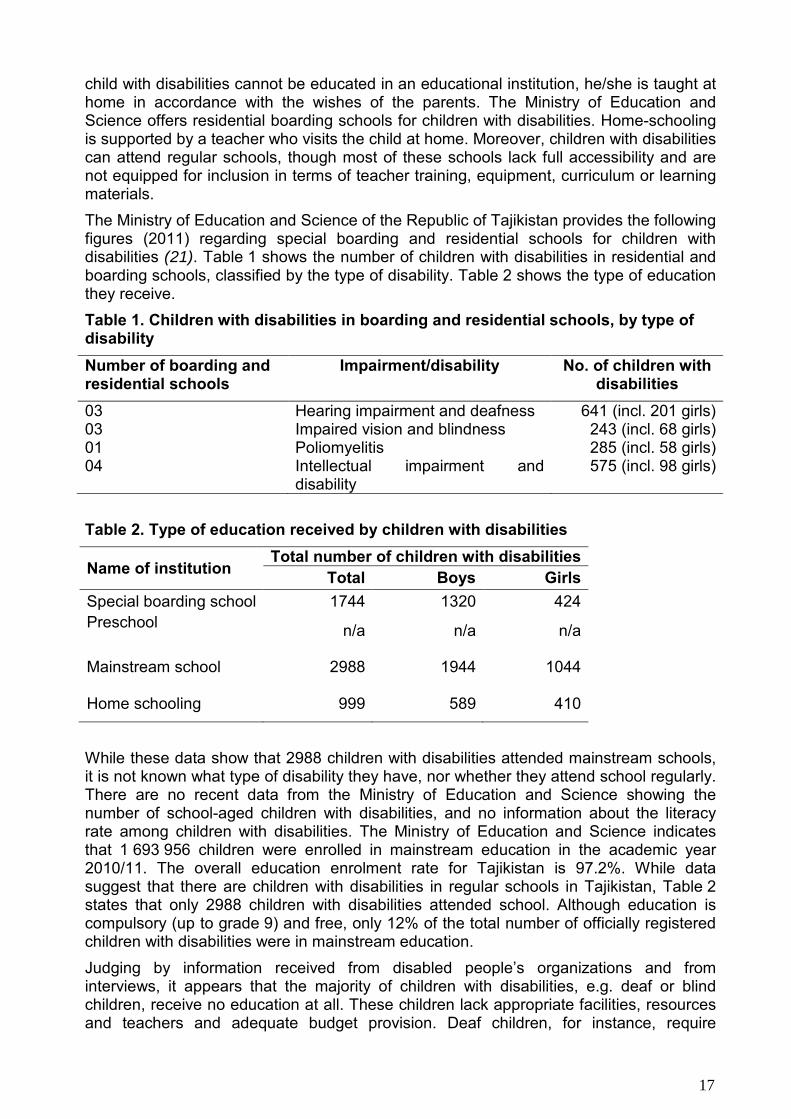
child with disabilities cannot be educated in an educational institution, he/she is taught at home in accordance with the wishes of the parents. The Ministry of Education and Science offers residential boarding schools for children with disabilities. Home-schooling is supported by a teacher who visits the child at home. Moreover, children with disabilities can attend regular schools, though most of these schools lack full accessibility and are not equipped for inclusion in terms of teacher training, equipment, curriculum or learning materials. The Ministry of Education and Science of the Republic of Tajikistan provides the following figures (2011) regarding special boarding and residential schools for children with disabilities (21). Table 1 shows the number of children with disabilities in residential and boarding schools, classified by the type of disability. Table 2 shows the type of education they receive. Table 1. Children with disabilities in boarding and residential schools, by type of disability Number of boarding and residential schools
Impairment/disability No. of children with disabilities
03 Hearing impairment and deafness 641 (incl. 201 girls) 03 Impaired vision and blindness 243 (incl. 68 girls) 01 Poliomyelitis 285 (incl. 58 girls) 04 Intellectual impairment and
disability 575 (incl. 98 girls)
Table 2. Type of education received by children with disabilities
Name of institution Total number of children with disabilities
Total Boys Girls Special boarding school 1744 1320 424 Preschool n/a n/a n/a
Mainstream school 2988 1944 1044
Home schooling 999 589 410
While these data show that 2988 children with disabilities attended mainstream schools, it is not known what type of disability they have, nor whether they attend school regularly. There are no recent data from the Ministry of Education and Science showing the number of school-aged children with disabilities, and no information about the literacy rate among children with disabilities. The Ministry of Education and Science indicates that 1 693 956 children were enrolled in mainstream education in the academic year 2010/11. The overall education enrolment rate for Tajikistan is 97.2%. While data suggest that there are children with disabilities in regular schools in Tajikistan, Table 2 states that only 2988 children with disabilities attended school. Although education is compulsory (up to grade 9) and free, only 12% of the total number of officially registered children with disabilities were in mainstream education. Judging by information received from disabled people’s organizations and from interviews, it appears that the majority of children with disabilities, e.g. deaf or blind children, receive no education at all. These children lack appropriate facilities, resources and teachers and adequate budget provision. Deaf children, for instance, require
17

teachers conversant in sign language, but schools have no such provisions. In the Law on Social Protection of Persons with Disabilities, sign language is recognized as a medium for interpersonal communication. However, the article does not list the situations in which a deaf person or person with a hearing impairment has the right to be provided with services in sign language.
“I am 23 years old and I am visually impaired. Recently I joined [the] Association of Blind People and learned that there is a special school for visually impaired and blind children. Until then neither my parents nor me knew about existence of such [a] school. I am illiterate and only at age 22, I start learning alphabet. If we knew before we could save a lot of time, and by now I could apply for a job.”
Safargul, Dushanbe
Despite education for all citizens being prescribed by law, many children with disabilities do not receive education. Access to education is limited because of inaccessible buildings, untrained teachers, lack of assistance, negative attitudes and limited educational material to meet the needs of the children with disabilities. This reduces opportunities for children with disabilities to access education, participate in social life and be included in society.
Livelihoods Participation in economic activity is necessary for every human being, not only for sustenance, basic survival and to supplement the family income, but also to contribute to one’s self-esteem and enhance self-fulfilment. WHO suggests that a secure livelihood1 can reduce poverty among persons with disabilities. The term “livelihood” not only refers to the ability to earn but also the opportunity to develop the person’s full potential with control over factors that shape his/her life and contribute to societal development. A sustainable livelihood approach emphasizes access to resources; market and economic services; removal of barriers to participation; reform of basic services; and improvements in infrastructure. Persons with disabilities in developing countries face a multitude of barriers to securing a decent livelihood. Globally, the International Labour Organization estimates that some 386 million people of working age are disabled, with unemployment among disabled people as high as 80% in many countries (22). There are serious factors that affect livelihoods of persons with disabilities, e.g. difficulty in identification of suitable jobs, accessibility, discrimination, negative attitudes and lack of education and skills. Despite improvements in living conditions, an estimated 42% of the total population of Tajikistan still lives in poverty (12). The exact number of persons with disabilities who live in poverty is not recorded. Empirical analysis suggests that most persons with disabilities in Tajikistan do not have opportunities for employment. Although it is assumed that unemployment rates among persons with disabilities are very high, no accurate data are available.
1 The term “livelihood” can be understood as the means of earning a living or accessing a source of income. Livelihoods may relate to a range of activities and services to promote self-reliance, including formal and informal education, vocational training, waged employment, self-employment, microfinance, agriculture programmes and social protection schemes.
18

Similarly, there is no information about self-employment among persons with disabilities. It is widely recognized that employment and income generation are key factors for empowering and promoting the inclusion of people with disabilities in society (23). A State institution, the Vocational Lyceum1 and Boarding School for Persons with Disabilities in Dushanbe city, with a branch in Rushon district2 is the only vocational school that provides vocational services (including accommodation, food and professional training) for young people with disabilities. Students can obtain vocational education in five disciplines: shoemaker, seamstress, radio mechanic, accounting technician and computer operator. According to the State Agency on Social Protection, Employment and Migration, 295 students with disabilities were studying and living at the lyceum in 2013. From 162 students who graduated in 2011, 49 continued their education at university level and 89 have been employed in the area of their specialization.
Employment opportunities in Tajikistan are limited to a number of disabled people’s organizations that provide job placements for their members. For example, the Association of Blind People employs about 640 people with various levels of visual impairment. Similarly, the National Union of Deaf People, among other activities, trains nondisabled sign-language teachers who, in their turn, teach children at boarding schools for deaf and hearing-impaired children.
“I have cerebral palsy, but it did not stop me to sell books on the street. After some years, I have been told to close my ‘business’. My social pension is 200 somoni. From [this sum] I am paying 160 somoni for electricity and water bills. I went to several banks and asked [for] credits to open [a] new business, but I was refused [by] all of them. Because of my disability, I am recognized as [an] incapacitated person and could not bear legal responsibility for any actions, and banks cannot confiscate my property.”
Ashraf, Dushanbe
Limited formal or informal employment opportunities, lack of income and lack of access to finances, savings and credit programmes are major challenges for disabled people’s livelihoods in Tajikistan. As a result of unemployment or low levels of employment, most persons with disabilities do not have any other option than to rely on Government social assistance programmes, whether they wish to or not. The pension received from the Government is usually not sufficient to create new income-generating projects.
Fig. 4 below, although not representative of the whole country, gives an indication of the income sources of persons with disabilities. There is little difference between rural and urban residents, with the only difference being the level of self-employment. One of the reasons behind the low number of self-employed persons with disabilities in rural areas may be that any feasible self-employment option in rural areas is hindered by unavailability of the necessary resources as well as lack of supportive environment for livelihood opportunity.
1 The lyceum is a category of educational institution offering a three-year educational programme majoring in a specific subject. 2 The branch in Rushon district does not offer accommodation.
19

Fig. 4. Sources of income of persons with disabilities, Tajikistan, 2014
Source: focus group data.
Women with disabilities often face greater challenges in finding employment than men because of negative attitudes towards disabled women. None of the female participants in the focus group discussions had any source of income other than disability pensions. The Labour Code of Tajikistan obliges employers to hire persons with disabilities according to a quota. More specific regulations on the quota are contained in the Law on Social Protection of Persons with Disabilities, which states that, if a company has more than 20 employees, disabled persons should make up no less than 5% of the workforce. Organizations that provide employment for persons with disabilities are granted preferential taxation conditions. While the legislation is a positive step in protecting the rights and ensuring the dignity of persons with disabilities, many problems still remain. For instance, although the Government has declared a 5% employment quota across all sectors, this has never been properly implemented. This can be partially explained by a lack of awareness among employers about the potential of persons with disabilities and/or the employers’ view that employment of disabled people is “charity”. The private sector needs to be motivated to see persons with disabilities as productive workers, by means of greater advocacy and information. Civil society organizations working in the areas of livelihood and income generation also need to make room for the disabled. The economic empowerment of persons with disabilities is key to independent living and sustainable livelihoods. Therefore, State policy and legislation in Tajikistan should be designed in a way that promotes improvement of the capacity of disabled men and women to earn an income by enhancing employable skills, improving training and enterprise development, increasing opportunities for job placements and reducing dependency on state benefits.
Social protection system The ongoing development of the social protection system is a strategic priority of Tajikistan’s social policy aimed at ensuring constitutional rights of people. As Tajikistan’s principal strategic document, the National Development Strategy for the Period to 2015 defines the priorities and general thrust of Government policy, which is focused on achieving sustainable economic growth, expanding the public’s access to basic social services and reducing poverty.
20

All of the state, sectoral and regional conceptual frameworks, strategies, programmes and plans for the country’s development currently in place and under development, as well as the activities of all Government agencies, are based on the National Development Strategy. The Living Standards Improvement Strategy of Tajikistan for 2013–2015 is developed within the framework of the National Development Strategy; it is a three-year, mid-term programme. It includes the implementation of strategic and priority areas for national economic and social development, harmonizes sectoral and regional strategies and programmes and guides the country’s development. The Living Standards Improvement Strategy also recognizes the following issues as challenges for the social protection sector: inadequate management and financial mechanisms in the social sector; lack of contemporary methodology and mechanisms for collection, processing and submission of sectoral statistical information; limited funding sources and incomplete normative legal framework for social protection; insufficient level of social allowances and services, and lack of social service standards; unfavourable conditions for the organization and development of alternative infrastructure for providing social services with state-of-the-art implementation mechanisms; lack of an effective policy to prevent social risks. Difficulties in transition and the protracted civil conflict in the 1990s caused GDP to contract and inflation to soar, resulting in severe cuts in health, education and social spending. Despite rapid economic growth in the first decade of the 21st century, spending has not returned to its pre-transition levels: in 2009, total state spending on health, education and social protection was just 3.3% of GDP, a long way from the average of 20.4% of GDP recorded in 1992–1994 (24). In 2012, the Government allocated TJS 4.064 billion (25) of the total state budget to the health, social protection and education sector. Of this sum, TJS 654 million were allocated to health care, which represents 7.5% of total state expenditure. Thus, in general terms, the Government spent an average of TJS 82.10 per capita on health care in 2012. The average nominal salary for health-care workers in 2012 was TJS 447.53 per month (26) while the average monthly salary in Tajikistan in 2012 was TJS 555.29 per month (27). However, the monthly salary varies between regions, with the lowest, TJS 350.46, recorded in Khatlon and the highest, TJS 1048.22 (28) in Dushanbe. The Government of Tajikistan allocated TJS 1.473 billion to the education sector in 2012, which constitutes 10.3% of GDP and 17% of total state expenditure. The average nominal salary for workers in education sector was TJS 425.82/month (27) in 2012. For the social sector (including social insurance and pensions), TJS 1.771 billion were allocated in 2012, which constitutes 8.3% of GDP and 21.3% of total state expenditure (28). For workers in the social sector, the average monthly salary in 2012 remained at TJS 440.83 (28). In recent years, despite the qualitative improvement in the country's financial situation and the increase in spending on the social sector in absolute terms, high population growth has not allowed any significant progress to be made in the social sector. Persons with disabilities, elderly people, households headed by women, unemployed people, orphans and large families are considered to be the most vulnerable groups.
Social assistance for persons with disabilities Social assistance programmes promote participation and inclusion in the life of society and the nation and contribute to the prevention and reduction of social marginalization and exclusion. The social assistance system in Tajikistan is dominated by:
• social insurance in the form of pensions;
21

• social assistance in the form of subsidies (transport, electricity, telephone);
• social assistance; and
• a small programme of family allowances for poor families with primary-school-agechildren.
The Law on Social Protection of Persons with Disabilities entitles persons with disabilities to receive social assistance, mainly pensions and social services, regardless of whether the person is working or not. The Law provides free social and personal services for persons with disabilities who are in need of constant care and entitled to receive assistance at home. In addition, persons with disabilities also receive benefits such as gas, water, energy, housing, utilities and telephone services. Furthermore, electricity, gas and drinking-water supplies are connected free of charge for persons with disabilities.
The main pension schemes are contributory labour pensions (which include old-age, disability and survivor benefits1) and noncontributory social pensions. For the contributory labour pension, the employee must pay contributions, while the employer often pays matching contributions to increase the value of the pension. In contrast, for the noncontributory pension, the employee (or pensioner) makes no contributions. Instead, the employer makes all contributions on the employee's behalf. The Poverty Assessment in the Republic of Tajikistan in 2009 conducted by the World Bank (29) shows that the number of households, including households with persons with disabilities, which are covered by any social programme in many domains is tending to decline (Table 3). According to the assessment, old-age-pension benefits made up the largest proportion (89%) of social protection benefit receipts, while disability benefits accounted for 10% of all benefits in 2007. These figures clearly indicate that the current mechanisms for pension distribution and the social protection scheme are not enough to cover all the needs of the population and persons with disabilities.
Table 3. Percentage of households receiving pensions and benefits 2003 (%) 2007 (%)
Covered by any social programme 38.7 34.4
Receiving old-age pension 27.2 33.3
Receiving disability pension 8.8 5.2
The Statistical Agency under the President of the Republic of Tajikistan indicates that the total amount of pensions and allowances paid out in the year 2013 was TJS 1.4 billion (30), even though the average monthly pension amounted to only TJS 181.82 per person (27). Fig. 5 shows the distribution of pension payments in 2013, by region. Table 4 shows the amount of pension paid to persons with disabilities in various categories.
Households
1 Survivor benefits are paid to families and children under 18 years who have lost the family breadwinner, families of Second World War veterans, liquidators from the Chernobyl nuclear accident, etc.
22

Fig. 5. Distribution of pension payments by region
Source: Tajikistan in figures 2013 (27).
According to the Agency on Social Insurance and Pensions,1 as at January 2013 there were 171 447 people (including 26 345 children) who received social assistance owing to disability, including children with congenital disabilities, those who acquired a disability later in life, those injured in the workplace, Second World War veterans, and liquidators of the Chernobyl nuclear accident. According to the data provided by the Agency on Social Insurance and Pensions, the following amounts of money were paid out in 2013 (Table 4).
Table 4. Amount of pension paid to persons with disabilities, Tajikistan, 2013
Pension receivers by
category
Average pension in TJS
Average monthly pension
(TJS)
Total pensions
paid in 2013 (billion TJS)
Total number of pensioners
(persons) StatisticalAgency
ASIPa
Disabled since childhoodb
n/a 129.68
181.82 1.4 171 447 Disability pension 251.78 310.03c
Survival 197.68 142.67 Social pension 99.37 88.57
Old age 176.54 227.04 a ASIP: Agency on Social Insurance and Pensions. b Including children with a congenital disability. c The exact amount of the pension depends on the pensioner’s disability category and ranges from TJS 63.00 to TJS 478.49 per month.
1 In December 2 13, the Agency on Social Insurance and Pensions was transferred from the Ministry of Labour and Social Protection of the Population to the direct control of the Government of Tajikistan.
23
Mishra Satish
Sticky Note
Marked set by Mishra Satish

As Table 4 shows, there are discrepancies between data provided by the Agency on Social Insurance and Pensions and the Statistical Agency about the average amount of pension paid to people with disabilities in 2013. Despite the fact that the Government of Tajikistan makes efforts to raise pensions regularly (hence the pension was raised from TJS 20.00 in 2007, to TJS 80.00 in 2010, to TJS 104.00 in September 2012), it is still insufficient to cover the basic needs of the population, particularly persons with disabilities who have greater needs. Tajikistan does not have an official “basket” of consumer goods and services1 or a consumer price index, which makes it difficult to calculate the amount of money needed per person per month. The poverty line was set at TJS 195 per person per month in 2009 (31). Today, the figure would be higher, taking into account inflation and the rising prices of food and other goods. According to the data provided by the Statistical Agency, the average monthly expenditure per capita per month in 2012 was TJS 251.59, which is much higher than most average pensions paid to any category of pensioner. Moreover, these figures by no means reflect the additional needs and expenditures of a person with disabilities as a result of his/her disability – such as costs associated with medical care or assistive devices, or the need for personal support and assistance – and they therefore often require more resources. The situation of disabled veterans of the Second World War and liquidators of the Chernobyl accident is better, amounting to an average pension of TJS 768.47 and TJS 602.28 per month respectively, which is higher than the average monthly salary (TJS 555.29).
“My neighbour is disabled as well as his two children. Children have mobility limitation problems whereas father has intellectual impairment. Both of them go to school, but often suffer from sicknesses. Since family does not have means to buy food and medicines, children are forced to skip classes. The family receives scanty pension of 130 somoni. The family consists of five members; three of them are in great need of medications and treatment. They have very difficult conditions and situation. More attention needs to be paid to those families.”
Mamadjon, Dushanbe
The State Agency on Social Protection of the Population (formerly the State Agency on Social Protection, Employment and Migration) was formed by decree of the Government of the Republic of Tajikistan in 2014 (Decree No. 168 of 4 March 2014). The Agency aims at the consolidation of efforts, coordination of activities and implementation of common policy related to social protection. In January 2014, social protection functions were transferred from the Ministry of Labour, Migration and Employment to the State Agency on Social Protection of the Population (see Annex 4 for its current structure). The Agency is the executive body that ensures the provision of state guaranteed services in the area of social protection. The Agency is responsible for a wide range of actions, including:
• implementation of measures for the implementation of state policy in the area of social protection, including measures for pensioners, persons with disabilities and other socially vulnerable people;
• implementation of actions for the social adaptation of persons with disabilities,including children, and for orphans and children from poor families;
1 The list of foods and other products to be included in the consumer basket has not yet been approved by the Government.
24

• coordination of activities among all stakeholders, including the donor community anddepartments providing social assistance at home;
• implementation of comprehensive rehabilitation services, including prosthetic andorthopaedic devices, and social integration of persons with disabilities;
• provision of social care, medical care and cultural events;
• implementation of measures of targeted assistance to vulnerable families andpeople, including persons with disabilities;
• monitoring of activities related to social protection.The Agency has 35 staff and oversees the activities of residential care institutions for adults with disabilities, sanatoriums for war and labour veterans, territorial centres for adults with disabilities, departments providing social assistance at home and daycare rehabilitation centres. The Agency’s budget comes from the republican budget. In Tajikistan, the State and its structures are the main provider of rehabilitation services for persons with disabilities, including children, war veterans, retired persons and others who need services and support. Services are provided in eight residential care facilities; by outsourcing services for children and adults with disabilities to local nongovernmental organizations through social contracting mechanisms; and through community-based rehabilitation projects. Rehabilitation services are provided through psychological, medical and pedagogical consultation units, the Republican Rehabilitation Centre for Children with Disabilities and the republican physical therapy hospital. In addition, the National Orthopaedic Centre, the National Research Institute for Rehabilitation of Persons with Disabilities and the Republican Clinical Centre for Mental Health of Children and Adolescents were providing services for persons with disabilities at the time of the review. Please refer to Annex 5 and Annex 6 on the current process for accessing rehabilitation services for children and adults with disabilities. According to the State Agency on Social Protection, Employment and Migration, the total number of people living in these residential care institutions in 2013 was 1667 (of whom 672 were children and 689 were women), and 1802 persons with disabilities received daycare services. Whereas some information is available about the number of children and adults with disabilities who live and receive services in residential and daycare facilities, nothing is known about other persons with disabilities living at home, and their needs are not assessed or addressed. There is a need to increase coverage of rehabilitation and other services in all settings. Policy options should be designed to meet the demand for rehabilitation services for all. In 2013, two residential care institutions – the Chorbog National Rehabilitation Centre for Children and Adolescents and the Residential Institution for the Elderly and People with Disabilities of Tursunzade City – were selected as pilot institutions for restructuring. The purpose of restructuring was identified as piloting new categories of social services within the institutions and the introduction of physiotherapy and occupational therapy. The restructuring plans were informed by an assessment of service-users’ needs, undertaken in early 2012 by a consortium led by Oxford Policy Management. The assessment confirmed that children and elderly people in residential care usually need a variety of therapy services, rather than specialized medical care. Most of the children could be reintegrated into their families and society simply by providing rehabilitation services, e.g. occupational and physical therapy, speech therapy and assistive devices. The analysis also highlighted the importance of deinstitutionalization and community-based services for integration within the community. There is a growing recognition that, no matter how much money is spent on institutions, the characteristics of institutional care are bound to make it extremely difficult to provide an adequate quality of life for users, to ensure their enjoyment of human rights and accomplish the goal of social inclusion. In general, available studies
25

confirm that, if high-quality community services are provided, most formerly institutionalized users have a clear preference for living in the community and display higher levels of personal satisfaction and social inclusion, with fewer problems linked with insecurity or loneliness. These professional services should be extended and sustained on a national scale to overcome the persistent over-reliance on residential care for children with disabilities (32).
Rehabilitation Prevalence of disability Tajikistan is a young nation. According to official statistics, approximately half (48.7%) of the population is made up of children and adolescents (age 0-14 years – 36.4%, age 15-19 years – 12.3%). A total of 41% of the population still lives below the poverty line, with 17% below the extreme poverty line. Life expectancy in Tajikistan is the second lowest in the WHO European Region1 with noncommunicable diseases constituting the main causes of mortality. Globally, the number of people with disabilities is growing. This is because of the increase in chronic health conditions associated with disability, such as diabetes, cardiovascular disease and mental illness. Patterns of disability are also influenced by trends in environmental and other factors, such as road traffic injuries, natural disasters, conflicts, diet and substance abuse. Disability disproportionately affects vulnerable populations and is more common among women, older people and low-income households.
1The Region has 53 Member States (see http://www.euro.who.int/en/countries, accessed 12 September
2014).
Global prevalence rate estimates 15% of the population with disability, and the increase in prevalence of noncommunicable diseases is having a profound effect on disability trends; for example, these diseases are estimated to account for about two thirds of all years lived with disability in low-income and middle-income countries. Noncommunicable disease related disability (such as amputation, blindness or paralysis) places significant demands on social welfare and health systems, lowers productivity and impoverishes families (33). In case of Tajikistan, the World health statistics 2012 report shows that 57% of all deaths were due to cardiovascular diseases; 14% died from cancer, and 3% each from chronic respiratory conditions and from injuries (34).
Within the framework of the WHO countrywide integrated noncommunicable disease intervention (CINDI) and WHO studies from 2010, 22% of the adult population were diagnosed with hypertension and 15% of the adult population with an excessive level of total cholesterol (35). Cardiovascular disease mortality in the country is 206 per 100 000 population. Diabetes and iodine-deficiency disorders are the major metabolic and endocrine diseases in Tajikistan. According to the Republican Endocrinology Hospital, 5000 people with diabetes report to hospital every year, with 50% of them in need of rehabilitation interventions (therapy, assistive devices, etc.). According to data from the Republican Centre for Medical Statistics and Information, 3000 new cases of cancer are recorded every year, with cancer incidence in 2010 standing at 37.5 per 100 000 population. Respiratory diseases are also a serious issue, being the most frequent cause of primary morbidity. Over the last 10 years, recorded cases of respiratory disease in primary uptake has increased by a factor of almost two (up from 5200 to 11 672 per 100 000 population).
26

Injuries traditionally occupy a leading position in the structure of total morbidity, mortality and disability in Tajikistan (35). Trauma occupies fourth place in total incidence and death structure, second place for temporary disabilities and third place for permanent disability status. A particular concern today is the rise in numbers and the qualitative change in the injury structure. Nowadays, there is a noted increase in the proportion of multiple and associated injuries, open fractures and complicated injuries, as well as an increase in the proportion of injuries sustained in the home (31.8% in 2011) and in the street (29.6% in 2011), traffic injuries (22.9% in 2011), and gunshot injuries (2.6% in 2011). An increase in injuries is also noted among the child population. In general, in recent years injuries accounted for 5.6% of morbidity. In 65% of cases of injury, 43.8% of those injured report a temporary or permanent disability. As mentioned before, no data are available on the impact of noncommunicable diseases in terms of disability, but a significant number of people affected by noncommunicable diseases could lead a better quality of life with appropriate rehabilitation interventions. Rehabilitation can address risk factors (e.g. obesity and physical inactivity), as well as loss of function arising from noncommunicable diseases (e.g. amputation and blindness due to diabetes or stroke). Access to rehabilitation services can decrease the effects and consequences of disease, hasten discharge from hospital, slow or halt a deterioration in health and improve quality of life. According to the UNAIDS Report on the global AIDS epidemic 2012 (10), Tajikistan is one of the countries where HIV prevalence has increased by more than 25% over the last 10 years, although the epidemic is still at the concentrated stage (less than 1% among the general population). According to official statistics, by the end of 2013 a total of 5550 HIV cases were registered (36), of whom 32% were female and 69% were male. The relationship between HIV, AIDS and disability is a complex one. On the one hand, “HIV infection, and its treatment, can cause physical, psychological or social disabilities that prevent people living with HIV from full and equal participation in society”(37). On the other hand, there is evidence that persons with disabilities are “as likely, or even at greater risk, as their non-disabled peers to contract HIV” (37). The last decade has witnessed a growing recognition of the need to acknowledge the vulnerability of persons with disabilities to HIV and the need to find ways to increase their inclusion in HIV prevention and response
The residents of Tajikistan have historically experienced many natural disasters and adverse events, which have had a significant impact on health and security. The country is vulnerable to many hazards, including floods, landslides or mudslides, drought, earthquakes, avalanches, insect infestation and windstorms. According to the Global Seismic Hazard Map (38), the whole country is located in the high to very-high risk earthquake zone. In addition, it faces severe winter conditions, and this compound crisis also had a significant impact on health services (39). People with disabilities are more vulnerable to emergencies and disasters, and new disabilities may be created. People with visual, hearing and intellectual impairments and severe mental health conditions, and those who are socially excluded or living in institutions, may be unprepared for events that lead to emergencies, and may not know or understand what is happening. They may also have greater difficulty meeting their basic needs, including food, water, shelter, latrines and health services. In addition, emergencies lead to disability due to injuries, poor basic surgical and medical care, emergency-induced mental health and psychological problems, abandonment and breakdown in support structures and preventive health care. Untreated or inadequately treated injuries can lead to unnecessary deaths or severe and long-lasting impairments (40).
27

Official figures on the prevalence of disability are available through the Ministry of Health and Social Protection, albeit only for people who have registered and received a disability certificate. The accuracy of these official prevalence figures is affected by a variety of factors, including negative societal attitude towards disability. It remains a common practice in rural areas to hide children with disabilities and raise them at home to avoid the associated public shame. A large proportion of the population is still unaware of disability issues. Women are often blamed for giving birth to a child with disabilities, and doing so can be grounds for divorce, even though there is a law banning that practice. This makes it much more unlikely that mothers will make the effort to arrange travel and visit appropriate facilities. The procedure for registering a person with disabilities is still not well understood, and anecdotal evidence indicates that a large proportion of the population is not aware of its existence. The population of the more remote areas does not have easy access to the facilities that provide registration services (Agency for Medical and Social Examination). The wealthier groups of the population often bypass the registration process and seek disability services abroad. The definition of disability is still essentially dependent on context, and the Tajik system of classification does not recognize conditions that would be defined as disabling under the ICF. It can thus be inferred that a large proportion of the population with disabilities remains uncaptured by official statistics. The figures provided here represent only the situation of the registered population. See Fig. 6 for the number of registered persons with disabilities and the number of new registrations in the period 2000-2012.
Fig. 6. Number of persons with disabilities and new registrations, Tajikistan, 2000−2012
Source: Ministry of Health and Social Protection and Statistical Agency.
The number of persons with disabilities has risen steadily over the last few years. According to Government agencies, the main reason for the rise is not a higher prevalence of disability in Tajikistan. Although, as mentioned above, the current system of registration is still not well known and there is limited awareness of the links between noncommunicable diseases, injuries and other disabling conditions, on the one hand, and disability, on the other, awareness is increasing as a result of the various programmes being implemented in the country. At Government level, the newer outreach
28
Registered persons with disabilities
programmes run by health facilities, including psychological, medical and pedagogical consultation services and polyclinics, are bringing in new registrations from rural areas. In civil society, especially among disabled people’s organizations, supporting and disseminating knowledge about the registration process is a core activity. Recent improvements in the availability of rehabilitation services, such as the psychological, medical and pedagogical consultation services, are also conducive to new registrations. The rise in the official numbers of persons with disabilities indicates, above all, that a higher percentage of the population with disability is now going through the system. The drop in new registrations in 2012 (from 12 899 in 2010 to 8085 in 2012 – see Fig. 6) is due to a modification of the classification system: since that year, children under the age of two years have no longer been eligible for registration. This decision was taken because of the creation of early intervention services, which should, in theory, provide comprehensive treatment for a number of conditions before the child reaches the age of two. This is obviously not always the case, depending on the condition, and a paradoxical situation has been created in which the parents are unable to access services freely because their children are not registered, but these services are the ones deemed necessary by the state in order to avoid registration at a later date. It remains the official position of the Government of Tajikistan that the number of children with disabilities has decreased over the past few years, as reflected in official statistics, while civil society maintains that the number has actually risen sharply. As is often the case in low-income countries, men are more likely than women to practise occupations, especially higher-risk manual labour, which may lead to disability. Although this is a common explanation for the discrepancy in the prevalence of disability between men and women, anecdotal evidence from civil society also points to cultural bias, favouring boys among the rural population and the more traditional groups in society. Such families are more likely to seek rehabilitation services for their sons than for their daughters. This trend can be expected to continue unless strong action is taken at national level, as the country moves from its Soviet egalitarian past towards restoring its cultural roots. In the UNWomen report Implementation of the Rights of People with Disabilities in the Sughd Province, Republic of Tajikistan (41), UNWomen notes the following on gender inequality among persons with disabilities.
• It is well established that women with disabilities are subject to double and even triplediscrimination being women, disabled and, very often, indigent. […] Furthermore, awoman with disability as a rule possess[es] lower literacy levels than men, andconsequently a greater percentage are unemployed compared to men withdisabilities.
• National legislation and policies on gender equality and social protection of personswith disabilities lack a gender dimension. No analysis has been made of therequirements of men and women with disabilities.
• The legislation and safeguards for women reflect the stereotypes of women's roles inthe family and is not directed, as required by CEDAW [Convention on the Eliminationof All Forms of Discrimination against Women], for equality, for both men and womento care for the family and children with disabilities.
29
Mapping of rehabilitation service providers Preliminary preparations for the situational analysis included a full mapping of rehabilitation service providers in Tajikistan in the sectors of health, social protection and education (see Annex 7). Health and rehabilitation services dedicated to persons with disabilities have been heavily influenced by the concepts of Soviet “defectology”, which postulated limitations on the development of children with disabilities, and hence their need for a special educational and developmental environment. Defectology (Box 1) emphasized “special education” as the best remedial treatment for children with disabilities. While these strategies had some positive intentions and outcomes, their implementation – imbued as these strategies were with a profound stigma relating to persons with disabilities – resulted in many children with disabilities being shut away in institutions. It was not uncommon for infants and children with medium or severe disabilities to be placed in residential schools, only to “graduate” to an adult institution for the rest of their lives. The discipline limits and, in some instances, excludes the use of rehabilitation techniques such as physical medicine and rehabilitation, physiotherapy, occupational therapy, speech therapy or assistive devices.
Box 1. Defectology
Defectology – literally “the study of defects” – is a science unique to the former Soviet countries. Defectology was developed in the Soviet Union during the 1920s. The discipline holds that the loss or weakness of biological functions can best be compensated for through development of higher psychological functions. The theory posits that intellectual capacity has endless potential and, if helped by proper educative methods, personal contact and stimulation, it can correct or circumvent impairments in lesser bodily functions. Importantly, special education was supposed to compensate not only for “primary” defects (i.e. organic impairments in the body), but also to prevent, correct and remedy “secondary” effects (i.e. the disabling effects of social factors on higher functions) by psychological and pedagogical means. However, unlike the rights-based model, defectology focused primarily on changing disabled individuals themselves, rather than their social and physical environments. Defectology was taken up by the Soviet State, and special education was emphasized as the main remedial tool for children with disabilities. In practice, special education was carried out in residential schools and institutions, a practice that segregated children with disabilities and virtually cut them off from society, community and even family. Many children with disabilities were simply deemed “ineducable” and practically shut away from society. In this way, the practice of defectology has effectively contributed to high rates of institutionalization in the region (42).
As a result, institutionalization of children and adults with disabilities in national and regional centres remains common among those who seek access to state-based services, while mainstreaming is still mostly in the hands of civil society. However, the situation has been evolving in the past few years. Because of rising costs in the existing institutionalized system, the perceived need to develop long-term solutions and pressure from parents and civil society as a whole, facilities dedicated to children with disabilities are increasingly moving towards a model of inclusive rehabilitation, where people with a variety of disabilities can access a range of services. For adults, especially those with intellectual disability, institutionalization remains the only solution offered by the state. It should be noted that, despite the number of service providers in Tajikistan, and saying nothing about the quality of said services, all evidence tends to indicate that the majority of people with disabilities have no access to services, or only limited access.
30

At the regional level, nine psychological, medical and pedagogical consultation services were established in 2006 by presidential decree within existing polyclinics, to provide assessment, short-term rehabilitation services and psychological support for children withdisabilities and their families. The staff include doctors, social workers and on-the-job-trained therapists. International agencies have actively provided support for the psychological, medical and pedagogical consultation services in the form of equipment and training for their personnel. Because polyclinics are well-known facilities within the country, the psychological, medical and pedagogical consultation services are especially well located to service a large part of the population of children with disabilities. However, not all centres are fully functional, and access to equipment and trained rehabilitation professionals remains a concern. Access to services is also an issue for the rural population, although several centres have implemented limited ad-hoc outreach programmes either with international support or with funding from the local Department of Health. Two additional psychological, medical and pedagogical consultation units are not yet fully equipped, although this should be addressed in 2014. Also at the regional level, eight residential care centres provide institutionalized services for children and adults with disabilities. These residential centres were originally built after the Second World War to provide services for elderly war veterans, and now provide full-time services and housing. They are considered a solution of last resort for children with disabilities who require intensive rehabilitation services; however, they provide little in terms of rehabilitation and have limited access to rehabilitation professionals or equipment. National and republican centres provide the highest level of specialized health services available, and often constitute the sole provider of services countrywide in the speciality concerned. Most are situated either in Dushanbe or in the surrounding Districts of Republican Subordination, and distance and travel costs are a barrier to access for anyone living outside these areas. The following centres are some of the biggest and better-funded facilities dedicated to rehabilitation.
• The Republican Rehabilitation Centre for Children, Vakhdat district (also called theRehabilitation Centre for Children with Disabilities, Macheton) provides 15-dayresidential rehabilitation services for children with (especially physical) disabilities. Asa dependency of one of the major hospitals in the country, the Centre has receivedstrong international support, including training sessions, equipment and buildingreconstruction support from various international organizations. Nevertheless, thefacility does not have access to formally qualified rehabilitation professionals.
• The Chorbog National Rehabilitation Centre for Children and Adolescents, Varzobdistrict, has long been presented by the state as Tajikistan’s most successful facility,and has received considerable funding to ensure the most comfortable environmentpossible for the children institutionalized there, although the quality and availability ofrehabilitation services still remain extremely limited. Originally supposed to cater forchildren with different disabling conditions, the vast majority of the 200 full-time bedscater mainly for children with cerebral palsy. Recognizing the limits of the institutionmodel (the child must leave the facility at age 18, and no public adult residentialinstitution in the country has the means to provide a similarly pleasant environment,making the transition from Chorbog to any adult institution a potentially traumaticone), combined with the rising costs of disability services, Chorbog is modifying itsapproach: in 2013, a programme was introduced which aims to return children totheir families and put them back into mainstream education, and the centre hasbegun to provide short-term stays, treatment and training for children and theirparents.
31

• The Republican Physiotherapeutic Hospital, Khujand, Sughd region (also called theNational Physiotherapy Hospital, Khujand) has 330 beds and has been in operationfor 84 years, with separate children’s and adults’ sections. The Hospital provides 15-day residential stays for persons with different disabling conditions. The hospital staffincludes doctors, nurses and therapy personnel trained in the Soviet era, with noaccess to qualified rehabilitation professionals. The Hospital has also received inputsfrom international agencies, although these are limited in nature. The Hospitalreceives financial resources from the central and local authorities.
• The National Orthopaedic Centre/State Unitary Enterprise of Prosthetic-OrthopaedicPlants was founded in 1942, with the main workshop building constructed in 1963. In1999, the workshop was technically supported (materials, equipment, formal and on-the-job training) by the International Committee of the Red Cross, and the RedCrescent Society of Tajikistan (RCST). Currently, the Centre is in need of renovationand new equipment. The building has not been renovated since 1963 and is nowunder threat of collapse. The Centre also runs satellite workshops in Khujand (in thenorth), Kulob (in the centre of the country) and Khorog (in the south-east) for repairand maintenance, although these centres lack capacity and are in poor condition.The Centre also provides meals and accommodation paid for fromGovernmentfunds. It employs 88 workers – the majority have a disability – andincludes medical doctors, on-the-job trained physiotherapists, bench workers andshoemakers. Since January 2013, the Centre has been technically supported by theSpecial Fund for the Disabled of the International Committee of the Red Cross, whichhas provided on-the-job training, support for formal training of seven students inprosthetics and orthotics in Viet Nam and renovation of the satellite workshop inKhujand. The seven students (three students in category II1 multidiscipline and fourstudents in category II single-discipline) will return to Tajikistan by the beginning of2015. The profession of prosthetist and orthotist is still not included in the All-Republican Classifier of Occupations (the recognized list of professionals) inTajikistan. Ageing buildings, equipment, availability of appropriate fabricationmaterials and sustainability of support for returning trained staff are all issues for theNational Orthopaedic Centre.
• The National Research Institute for Rehabilitation of Persons with Disabilities/Scientific Research Institute for Examination and Rehabilitation of Persons withDisabilities in Dushanbe conducts research on disability issues and provides limitedrehabilitation services for children and adults with disabilities. The Institute, foundedin 1993, provides both inpatient (60 inpatient beds) and outpatient services.Historically, it provided surgical care, but at present surgical services are notavailable and a lot of the equipment in the institute is no longer operational. Its staff ismainly doctors and nurses, with limited access to qualified rehabilitationprofessionals. The Institute has developed a long-term action plan for the period2012–2015 which includes objectives to improve its infrastructure and access tohigh-quality services and build the capacities of the personnel. However, limitedfinancial resources are a barrier to the full achievement of the goals and objectives ofthe plan. In the past, the Institute has been supported by the European Union, WHO,UNICEF, the United Nations Development Programme, the United NationsPopulation Fund and the Japan International Cooperation Agency. The institute isphysically difficult to access and is having problems with retention and skill levels ofstaff. This has an impact on the quality, efficiency and effectiveness of services.
1 The International Society of Prosthetics and Orthotics has developed detailed education and training guidelines, in close collaboration with WHO, for the full professional prosthetist/orthotist (category I), the orthopaedic technologist (category II) and the orthopaedic technician/benchworker (category III). See http://www.ispoint.org/standards-guidelines (accessed 25 September 2014).
32
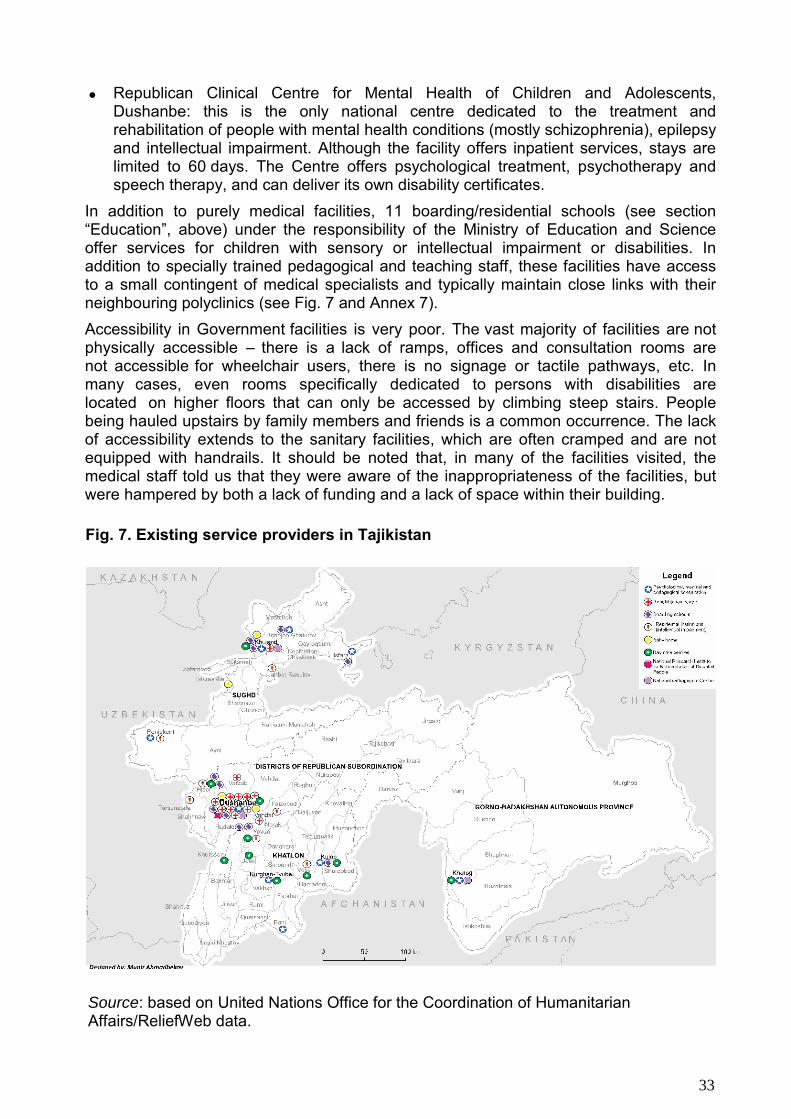
• Republican Clinical Centre for Mental Health of Children and Adolescents,Dushanbe: this is the only national centre dedicated to the treatment andrehabilitation of people with mental health conditions (mostly schizophrenia), epilepsyand intellectual impairment. Although the facility offers inpatient services, stays arelimited to 60 days. The Centre offers psychological treatment, psychotherapy andspeech therapy, and can deliver its own disability certificates.
In addition to purely medical facilities, 11 boarding/residential schools (see section “Education”, above) under the responsibility of the Ministry of Education and Science offer services for children with sensory or intellectual impairment or disabilities. In addition to specially trained pedagogical and teaching staff, these facilities have access to a small contingent of medical specialists and typically maintain close links with their neighbouring polyclinics (see Fig. 7 and Annex 7). Accessibility in Government facilities is very poor. The vast majority of facilities are not physically accessible – there is a lack of ramps, offices and consultation rooms are not accessible for wheelchair users, there is no signage or tactile pathways, etc. In many cases, even rooms specifically dedicated to persons with disabilities are located on higher floors that can only be accessed by climbing steep stairs. People being hauled upstairs by family members and friends is a common occurrence. The lack of accessibility extends to the sanitary facilities, which are often cramped and are not equipped with handrails. It should be noted that, in many of the facilities visited, the medical staff told us that they were aware of the inappropriateness of the facilities, but were hampered by both a lack of funding and a lack of space within their building.
Fig. 7. Existing service providers in Tajikistan
Source: based on United Nations Office for the Coordination of Humanitarian Affairs/ReliefWeb data.
33

For parents’ associations, the focus is on supporting inclusion in mainstream schools and contributing to the children’s future autonomy. Further activities in the domains of training of parents and community-based rehabilitation aim at avoiding institutionalization and ensuring that children with disabilities receive appropriate home-based services. However, during the review, it was difficult to quantify the impact of services managed by civil society, as limited data or no data at all were available to substantiate the above-mentioned information.
In terms of provision of rehabilitation services, parents’ associations generally have access to their own on the-job-trained staff, especially as the activities run by these associations revolve around daycare centres and outreach programmes. While the formal level of education of the staff is generally low, mostly no higher than nursing diploma level, the majority of associations have also had access to short-term training provided by various organizations, United Nations agencies, international nongovernmental organizations and a number of international foundations and associations. As a result, the level of qualifications among staff of disabled people’s organizations and nongovernmental organizations tends to be highly contrasted: while formal qualifications may be lacking, the staff are also not influenced by the theories about the development of persons with disabilities which are current among the Tajik medical community, and thus they are much more open to internationally recognized rehabilitation techniques that are still largely spurned by state-based facilities. As a result, the rehabilitation services provided tend to be closer to international standards, but quality control and monitoring are issues in the absence of qualified professional staff and given the lack of national standards on rehabilitation.
Disaffection with the existing system has been growing among people with disabilities, especially among the more educated groups of the population. Awareness of an alternative, more inclusive model of rehabilitation has been spreading through access to the Internet and the presence of international organizations in Tajikistan. Faced with an official state-based system that is perceived as not adequately addressing people’s needs, civil society is increasingly taking matters into its own hands. Disabled people’s organizations and nongovernmental organizations have developed their own services, and now represent an important part of the rehabilitation service providers in Tajikistan. These organizations differentiate their services from those of the state in three fundamental ways: they provide services in geographical areas where the state does not have adapted health facilities; they provide services for those who are not entitled to state support under current regulations; and they focus strongly on mainstreaming, inclusion, support for parents and outreach. From a geographical point of view, nongovernmental organizations and disabled people’s organizations are the sole providers of adapted services in many remote areas. The full range of state services for people with disabilities is available only in Dushanbe, with a small number of facilities providing a narrower range of services in Khujand, Kulob and other urban centres. Nongovernmental organizations and disabled people’s organizations are also the only providers of rehabilitation services for children with autism or Down syndrome, which are not recognized by the state as disabling conditions and thus do not give access to either social assistance or rehabilitation services. Mainstreaming into the educational system and integration into health services are an important part of the activities of the nongovernmental organizations and disabled people’s organizations, and advocacy on these matters is often one of their core activities. For adults, this means inclusion in the workforce and access to equal opportunities on a par with their nondisabled peers.
34
The provision of daycare centres for children with disabilities is one of the major services run mostly by nongovernmental organizations (including parents’ associations), and has proven popular among parents and caregivers of children with disabilities. The centre also provides a break for parents and caregivers and allows them to do other activities. In addition to providing basic rehabilitation and educational care for the children, the daycare centres also constitute a meeting point for parents/caregivers to meet and share their experiences. Guidance for parents is also commonly provided by the centres, as well as sessions of psychosocial support. The Government has recognized the importance of these facilities and the ability of the nongovernmental organizations to run them efficiently. Most daycare centres are situated in facilities belonging to local authorities, and funding is available through annual central-Government tenders. The services managed by nongovernmental organizations are monitored twice a year by the Ministry of Health and Social Protection, although successful quality control would be dependent on Ministry staff being trained, preferably formally, in the same techniques that are employed in non-state facilities. Daycare centre monitoring is currently limited to food, finances and centre infrastructure. There is limited planning, monitoring and evaluation of technical and quality parameters. It is important for Government and civil society organizations to plan jointly and set standards for the daycare centres in an appropriate planning and monitoring plan (goal and indicator setting).
The services provided by civil society remains linked to the existing state-based network. Most nongovernmental-organization-run facilities stay in regular contact with neighbouring polyclinics and other specialized service providers, and persons with disabilities often regularly access both. Cooperation, where successful, leads to referral of people from state-run medical facilities to the most appropriate local daycare centre run by a nongovernmental organization. In return, many disabled people’s organizations and nongovernmental organizations feed back into the official system through “legal support” activities which aim at supporting access to existing state services and ensuring that that access is free, as guaranteed under Tajik law for people with disabilities. Psychological, medical and pedagogical consultation services have been observed as being particularly instrumental in developing strong relationships with nongovernmental organizations. As a result, they are central in linking the identification of disability with early intervention and referral to nongovernmental facilities. Despite the above-mentioned progress, coordination between stakeholders working in the disability sector has been identified as a challenge, and there is a need to strengthen these mechanisms. It would appear that there is limited coordination at the national level among nongovernmental organizations and State actors working in the disability sector. At the district level, coordination mechanisms have been established in some districts to bring together all relevant stakeholders. Some nongovernmental organizations are working with disabled people’s organizations to build their capacity and improve coordination and collaboration between the organizations, particularly at the national level. However, despite arguable successes, civil society also faces a number of barriers and limitations. In addition, funding, a perennial issue for nongovernmental organizations, can be particularly difficult to come by in Tajikistan, with the number of active international institutional donors constantly decreasing over the last few years. As a result, the long-term sustainability of even the most successful projects could be called into question in the near future.
35
The lack of qualified personnel, both in the field of rehabilitation (as will be discussed in the section on human resources below), but also in the field of finance and management, also constitutes a significant barrier to access to international funding, as organizations find it difficult to follow the standards for accounting and reporting set by the donors. And although civil society has an important role to play in filling gaps in services in remote rural areas, the total coverage by all organizations remains very limited to this day. As a result, the achievements of civil society remain fragile. This is particularly true for the introduction of modern rehabilitation techniques, the sustainability of which can only be achieved through adoption by mainstream Government services.
Although services for people with disabilities have improved in Tajikistan, the vast majority of the improvements have been aimed at children aged under 18 years; the availability of services drops drastically past that age. This concern was raised repeatedly during visits, by both governmental and nongovernmental staff, in short-term and outpatient facilities and within institutions. The current transition upon reaching adulthood, where services become scarcer or even absent, and facilities provide a much less friendly environment, is potentially deeply damaging, mitigating the benefits of improving health, rehabilitation and social services for children with disabilities. Moreover, access is entirely predicated on the actual age of the individual and not on the individual needs and abilities of the person with disabilities.
Box 2. Disability rehabilitation camps for children with poliomyelitis in Tajikistan In 2010, Tajikistan had the largest poliomyelitis outbreak in the world since 2005. In total, 457 people, mostly children, were confirmed as poliomyelitis victims. Many people affected by poliomyelitis have developed impairments over the last three years and need long-term rehabilitation. In March 2014, with the technical support of the WHO country office, rehabilitation camps were organized to assess current needs, develop an appropriate intervention plan for children with poliomyelitis and provide guidance to strengthen relevant service providers. These camps were organized in strategic locations covering 30 severely poliomyelitis-affected districts. Through these camps, 360 people with poliomyelitis were reached, representing the majority (80%) of the known proven poliomyelitis cases from the 2010 outbreak. On the basis of the camp findings, some 300 children were recommended for physiotherapy and/or orthoses and other assistive devices. In addition, 77 children were recommended for various surgical operations. The children’s main rehabilitation needs are for assistive devices and physiotherapy. However, in another few years, the need for surgery for this age group will increase if urgent rehabilitation interventions are not provided now.
Although the country had been certified as poliomyelitis-free since 2002, a major poliomyelitis outbreak took place in Tajikistan in 2010. With 712 cases reported, of which 457 received laboratory confirmation of wild poliovirus type 1, this was the largest poliomyelitis outbreak in the WHO European Region for more than a decade and the largest outbreak worldwide for that year. The international intervention described in Box 2 shed new light on poliomyelitis in particular and on rehabilitation for persons with disabilities in general, and significantly raised public awareness of disability and rehabilitation.
Supply of and demand for rehabilitation services
36
Institutionalization still remains a very popular option for parents with children with disabilities, as many still see institutions as the best way to provide proper care and the optimum long-term solution. Every facility visited reported operating at full capacity, and several mentioned subscription to long waiting lists as a prerequisite for gaining entry. Several facilities are trying to increase their capacity by constructing new buildings, although acquiring the necessary additional staff is an issue, and the increase in capacity will remain modest at best. For those families who do not have access or are not aware of alternative solutions to institutionalization, the situation is dire. During interviews with facilities operating at full capacity, it was reported that, until a place could be found, children and adults with disabilities are kept at home without any particular regular treatment, sometimes under heavy sedation in the case of intellectual impairment or mental health conditions. The demand for home-based services remains low but is growing, owing to strong advocacy and the activities of nongovernmental and disabled people’s organizations. At Government level, these services remain very limited, but are increasing. A total of 38 social assistance at home units, manned by social workers, are currently operating at regional and district level under the supervision of local authorities. However, the social workers have vocational (paraprofessional) education or on-the-job training only, and do not have either adequate recognized qualifications or relevant education acquired from a university. Social workers in these units provide home-based basic services for the elderly and people with disabilities and have been trained on the job in a few areas of personal care by international agencies. Where available, the units work in collaboration with polyclinics, psychological, medical and pedagogical consultation services and international nongovernmental organizations, which extends the geographical coverage of these facilities and organizations although the care is limited to children with disabilities. Evidence shows that these programmes have the potential for success, but actual results are heavily dependent on external support, the availability of services (psychological, medical and pedagogical consultation, polyclinics, etc.) and the goodwill of the local authorities. In addition, the staff’s limited knowledge of rehabilitation and the lack of qualified professionals is also a challenge for these units. Research conducted by the then Ministry of Labour and Social Protection of the Population, UNICEF and the nongovernmental organization Faroshturuk in 2012 (43) identified the following challenges: high personnel turnover due to low salaries; workers of retirement or post-retirement age; heavy work; lack of reimbursement of travel costs and lack of professional skills in service provision. The cost of transport and long travel times resulting from Tajikistan’s mountainous geography also limits the potential of these outreach programmes to cover the whole country in the near future.
Today, the demand for rehabilitation services clearly outstrips the available supply, although the specific services sought by the population vary according to a number of factors which include level of education, place of residence, degree of contact with nongovernmental and disabled people’s organizations, and understanding of the impact of proper rehabilitation services on the future potential of a person with disability.
As knowledge about alternatives to long-term institutionalization grows, mostly among the urban population, the demand for daycare centres or similar facilities is also growing. Again, the supply remains very limited: although civil society has made more daycare centres available over the past decade, access remains limited and future growth is limited by funding issues.
37
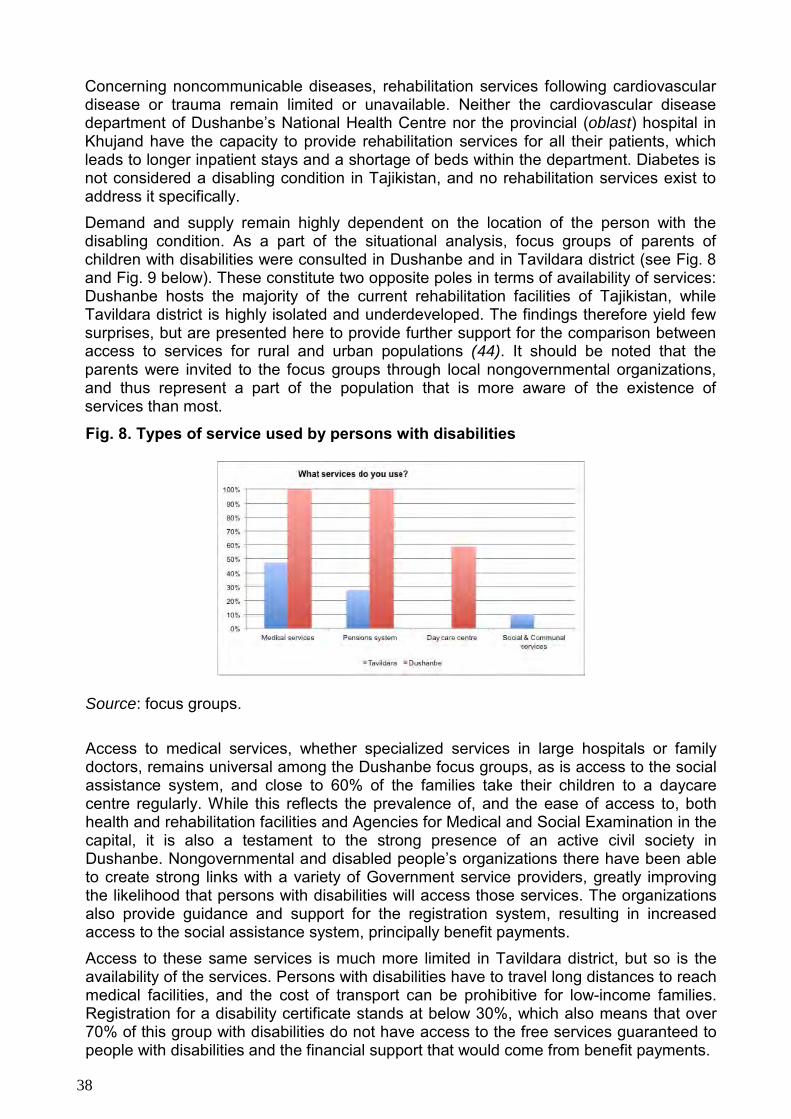
Concerning noncommunicable diseases, rehabilitation services following cardiovascular disease or trauma remain limited or unavailable. Neither the cardiovascular disease department of Dushanbe’s National Health Centre nor the provincial (oblast) hospital in Khujand have the capacity to provide rehabilitation services for all their patients, which leads to longer inpatient stays and a shortage of beds within the department. Diabetes is not considered a disabling condition in Tajikistan, and no rehabilitation services exist to address it specifically. Demand and supply remain highly dependent on the location of the person with the disabling condition. As a part of the situational analysis, focus groups of parents of children with disabilities were consulted in Dushanbe and in Tavildara district (see Fig. 8 and Fig. 9 below). These constitute two opposite poles in terms of availability of services: Dushanbe hosts the majority of the current rehabilitation facilities of Tajikistan, while Tavildara district is highly isolated and underdeveloped. The findings therefore yield few surprises, but are presented here to provide further support for the comparison between access to services for rural and urban populations (44). It should be noted that the parents were invited to the focus groups through local nongovernmental organizations, and thus represent a part of the population that is more aware of the existence of services than most.
Fig. 8. Types of service used by persons with disabilities
Source: focus groups.
Access to medical services, whether specialized services in large hospitals or family doctors, remains universal among the Dushanbe focus groups, as is access to the social assistance system, and close to 60% of the families take their children to a daycare centre regularly. While this reflects the prevalence of, and the ease of access to, both health and rehabilitation facilities and Agencies for Medical and Social Examination in the capital, it is also a testament to the strong presence of an active civil society in Dushanbe. Nongovernmental and disabled people’s organizations there have been able to create strong links with a variety of Government service providers, greatly improving the likelihood that persons with disabilities will access those services. The organizations also provide guidance and support for the registration system, resulting in increased access to the social assistance system, principally benefit payments. Access to these same services is much more limited in Tavildara district, but so is the availability of the services. Persons with disabilities have to travel long distances to reach medical facilities, and the cost of transport can be prohibitive for low-income families. Registration for a disability certificate stands at below 30%, which also means that over 70% of this group with disabilities do not have access to the free services guaranteed to people with disabilities and the financial support that would come from benefit payments.
38

Fig. 9. Barriers to obtaining services
Source: focus groups.
This situation creates a particularly vicious circle for the most vulnerable people in the rural population: because of a lack of financial means, they cannot access health or rehabilitation services that would provide them with the diagnosis required to go through registration; but without registration, they do not get the funding or subsidies that would enable them to obtain access to medical services. The system is even more heavily biased against the rural population with mental disorders, as the registration process for such conditions requires diagnostics and testing that cannot be obtained at the district level and require expensive travel to Dushanbe. One notable feature is the importance of social relations in overcoming barriers to access. Knowing the right people and using their influence remains the easiest way to gain access to services in Tajikistan. Once again, this is heavily biased against the most vulnerable groups of the population, as wealthier and better educated people are much more likely to be in a social relationship with service providers. The cost of medical services remains a major concern in both Tavildara and Dushanbe. Although this due to a variety of factors and varies depending on the disabling condition, it remains indicative of the importance of having to make out-of-pocket payments as a barrier to access, and this constitutes an important limitation on the supply of services in all areas of the country.
Medical rehabilitation techniques and practices Rehabilitation services in Tajikistan remain rooted in the techniques developed in the USSR. Although newer, internationally recognized techniques are slowly being introduced, either by civil society or through international organizations, they are seldom put to use in Government facilities. Senior staff at these facilities have graduated, in the vast majority, either from Soviet universities or from the Medical University of Dushanbe before independence, which explains in great part their reluctance to abandon the model that has defined their respective specialities for their entire careers. Access to information, including medical reviews, is also an issue, although the Internet is widely available in Tajikistan. Language could constitute a barrier to accessing foreign publications, although Russian translations are generally available and all senior personnel interviewed were fluent in that language. Rehabilitation services for people with disabilities, the majority of whom have chronic disabling conditions with permanent disabilities, are based on three services found in the majority of facilities: massage, electrical stimulation and paraffin heat therapy. These three techniques are described in Tajikistan as “physiotherapy”.
39

Massage is considered an integral part of physiotherapy treatment in Tajikistan, although the techniques observed were for the most part limited to relaxing and/or invigorating massage. As such, the contribution of these massages to actual rehabilitation is dubious. They remain, however, a useful adjunct to manual therapy when applied appropriately, either for preparatory relaxation or for pain management. Although specific and highly specialized massage techniques have also been developed in physiotherapy and have gained international recognition, such as tendon and hamstring massages or manipulative massages for club-foot correction, these techniques are generally not applied in Tajikistan. Currently massage, as applied in Tajik medical facilities, does not constitute treatment per se. Electrical stimulation is a fundamental element of physiotherapy in Tajikistan, and is applied widely in the treatment of a variety of disabling conditions (orthopaedic, neurological, cardiovascular, etc.) The treatment is provided using a variety of (generally outdated) electrical devices, most of which are not otherwise found outside the former Soviet Union. While electrical stimulation is used internationally, it remains limited at the clinical level to very specific cases, such as functional electrical stimulation for the rehabilitation of persons with paralysed lower limbs owing to spinal cord injury, or neuromuscular electrical stimulation for the treatment of disuse atrophy of the muscles. While the use of electrical stimulation in Tajik physiotherapy may yield some benefits for its patients, its usage is quite disproportionate to the benefits gained, owing to a lack of formal knowledge about electrical therapy. Paraffin heat therapy is the third element of rehabilitation. Paraffin brushing is practised in most medical facilities that provide rehabilitation services. Thermotherapy in general is known to increase nerve conduction velocity, arterial and capillary blood flow, tendon extensibility, and collagenase activity (45). Thermotherapy includes applications to decrease muscle spasms, decrease pain and reduce inflammation, joint stiffness and contractures. It can be an effective adjunct to manipulation and manual therapy, but does not constitute actual treatment in itself, and its use is once again disproportionate to its benefits. It should be noted that, while it is not within the framework of this report to analyse in depth the rehabilitation practices of the facilities visited, contraindicated uses of paraffin heat therapy have been observed during the visits and interviews, including application on paralysed limbs (impaired sensation may predispose to burns) and application on patients who may be unable to indicate properly that they are in pain. Internationally, rehabilitation therapy is defined as activities and interventions concerned with restoring and compensating for loss of function, and preventing or slowing deterioration in functioning in every area of a person’s life (4). All three techniques – massage, electrical stimulation and paraffin heat therapy – may in varying degrees constitute useful preparatory practices for manual therapy, but manual therapy itself, including passive and active mobilization with the objective of promoting functional independence (a vital and core technique of modern physiotherapy) is essentially absent from rehabilitation practices in Tajikistan. A variety of other techniques dedicated to the management of different disabling conditions can be found in individual facilities throughout the country, but their availability is variable. Therapeutic exercises are generally available in major facilities, although the absence of a specialist to provide the rehabilitation services, as well as limited knowledge of their importance and usage, are common issues. Acupuncture and reflexology were introduced in Tajikistan during the Soviet era and are used to treat a variety of conditions in rehabilitation, although the main recognized benefit of acupuncture remains pain management. Phytotherapy, based either on locally growing plants or on plants imported from the USSR, was also introduced during the Soviet era and remains in use, although the described benefits remain entirely separate from rehabilitation services, with the exception of pain management.
40

Psychosocial activities as practised in Tajikistan are more akin to counselling, and focus heavily on moral support, conflict management and improving dialogue within families. Occupational therapy remains completely lacking, however. While the position of occupational therapist was added to the list of officially recognized professions in 2013, there are no recognized practitioners in the country and no courses available. Prosthetics and orthotics services are an important component of rehabilitation. These services manufacture and supply assistive devices, which are often the first step to ensuring that people with disabilities can become equal members of society. Of the various types of assistive device, prostheses and orthoses are required by the majority of people with physical disabilities. Many people also require additional walking aids or mobility aids, such as wheelchairs, walking frames, crutches or assistive seating. To create a solid base for long-term sustainable services, the prosthetics and orthotics technologies used need to be appropriate.1 Currently, prosthetic and orthotic services are delivered through the National Orthopaedic Centre and are based on polypropylene technology which is affordable and easy to manufacture. Services are delivered free of charge, and the annual output is 1200 devices per year, including approximately 450 prostheses (mostly for adults) and 730 orthoses for children and adults. In addition, approximately 100 crutches are manufactured by the workshop every year. The core element of the prosthetic and orthotic service is the fitting of the orthopaedic device. This is partly clinical work – which requires considerable medical and technical knowledge – and partly practical manual work done in an industrial setting (with tools, machines and other equipment for working plastic, metal and plaster and manufacturing the product). The potential for producing certain components (sidebars, joints, etc.) within the country – using locally available or imported materials – should also be explored for efficiency.Prosthetics and orthotics services are hampered by the lack of trained prosthetists and orthotists, the lack of knowledge about the benefits of assistive devices, the ageing infrastructure and equipment and the dependence on international sources for the procurement of materials. There is currently one model for distribution of a Government-funded mobility device (wheelchair) (46).There appears to be no system for the provision of other assistive devices, with the exception of cases referred to the prosthetics and orthotics service and the provision of crutches by the National Orthopaedic Workshop. Wheelchair service provision is one of “distribution” rather than “service provision”. A referral from a polyclinic or psychological, medical and pedagogical consultation service is made to VTEK at the local level and, if appropriate, a referral will be made which puts the individual on a waiting list. This information on the need for wheelchairs is collected at the district level by regional branches of the State Agency on Social Protection, Employment and Migration and consolidated by the Ministry of Health and Social Protection for centralized procurement by the National Orthopaedic Workshop. Once procured, the wheelchairs are distributed by State Agency on Social Protection, Employment and Migration, following the waiting list. The only local production workshop additional to the above system is in Vakhsh, managed by the local organization Dilshod, although more investment would be required to improve the quality and quantity of products manufactured there. The two other methods by which wheelchairs are currently distributed are through donation or private purchase. Donor-funded wheelchairs are distributed to beneficiaries
1 Appropriate technology is a system providing good fit and alignment which suits the needs of the individual and can be sustained by the country at the most economical price. Proper fit and alignment should be based on sound biomechanical principles, as defined by the International Society for Prosthetics and Orthotics.
41

through nongovernmental organizations. In addition, a small number of imported wheelchairs are available for private purchase from a local pharmacy in Dushanbe. There is a lack of awareness of this service, and the current systems limit accessibility. The range and quality of appropriate and currently available products do not meet the recommendations set out in the WHO guidelines on the provision of manual wheelchairs in less-resourced settings (47). Action intended to meet the need for wheelchairs should focus on improving the quality of imported wheelchairs and utilizing the skills and experience of staff to assemble and modify them. This will maintain employment within the community and improve both the quality of products and the service provided. Local production, particularly of assistive devices (walkers, developmental aids, etc.), could work in parallel with this change. One key issue to be addressed as the Government is reassessing the structure for rehabilitation and social service provision is the cooperation and integration between social protection and rehabilitation. Traditionally, prosthetics and orthotics and the provision of mobility devices are linked with rehabilitation services and clinics rather than with social services. While a social model of disability is welcome, social service providers currently lack technical knowledge and have many and wide-ranging responsibilities; this will make it challenging for them to engage in the time-intensive process of person-focused service provision. In the light of this, it might be better to create a stronger link to the rehabilitation units (National Orthopaedic Centre, national rehabilitation centres, psychological, medical and pedagogical consultation services) and improve the understanding of social and medical rehabilitation there. Rehabilitation services for sensory, intellectual and mental health conditions receive much less attention in Tajikistan, and the number of facilities and dedicated personnel is considerably lower than for physical disabilities. Rehabilitation services for persons with speech and/or hearing impairments suffer greatly from a lack of adequate equipment. On the one hand, identification is poor owing to the lack of audiometric devices, and those few facilities that do have equipment do not have access to properly sound-insulated rooms; on the other hand, rehabilitation is hampered by a lack of hearing aids and other assistive devices. The capacity for surgical intervention is nonexistent, and people have to go abroad for treatment. Speech therapy techniques in Tajikistan concentrate on teaching verbal communication to persons with speech impairments, with a focus on producing particular sounds and syllables (articulation therapy), and on improving the motor function of facial and oral muscles (oral motor therapy), including the use of vigorous mouth massage. Language intervention and augmentative and alternative communication techniques are much less commonly used, although examples have been observed in a small number of facilities that provide services for children with cerebral palsy, intellectual impairment, etc. Equipment for the diagnosis, identification and treatment of visual impairments is much more readily available in Tajikistan. Basic ophthalmology services are available in the majority of urban centres. Surgical intervention, including laser corrective surgery, is said to be available in Dushanbe, although this could not be directly observed and the cost of such surgery could not be ascertained. However, access to specialized assistive devices beyond eyeglasses is a major issue. None are available at Government level, and although a small number of devices, such as magnifying glasses, can be found on the private market, they remain expensive and cannot be ordered to a certain specification. As well as dedicated services, persons with disabilities require the same health services as anyone else. However, interviews with civil society representatives indicated that medical staff in general lack training in and awareness of disability issues. In addition to the lack of accessibility described in the previous section, hospital visits can include long waiting times without available seating and trips between floors of the building without
42

support from the medical staff to facilitate the process. As a result, persons with disabilities cannot always consult medical professionals independently and often require the help of family members or friends. Medical specialists’ lack of knowledge of the causes of disability and its impact on health was also mentioned, as well as the propensity of these specialists to link – wrongly – all medical conditions suffered by the person with his/her disability.
Community-based rehabilitation Community-based rehabilitation was initiated by WHO to improve access to rehabilitation services for people with disabilities in low-income and middle-income countries, making optimum use of local resources (48). It aims to enable persons with disabilities to maximize their physical and mental abilities, to access regular services and opportunities and to achieve full social integration. Community-based rehabilitation projects call for inclusive development in five key areas: health (including rehabilitation and assistive devices), education, livelihood, social and empowerment. The model does not define new services, but rather defines a strategy for bringing these services to communities. Community-based rehabilitation projects are not intended to create services parallel to those provided by the state: indeed, more often, they constitute an extension of the state services. Community-based rehabilitation was officially introduced in Tajikistan in 2010 with active support of international agencies and organizations. Currently there are four international nongovernmental organizations engaged in community-based rehabilitation projects: Caritas Germany, Handicap International, Mission East and Operation Mercy. In addition, three Tajik nongovernmental organizations, Manbai Mehr in Khujand, Gamkhori in Vakhsh and Mahbuba in Kurgan-Tube city, have also developed community-based rehabilitation activities with international support. Although the exact health component (including rehabilitation and assistive devices) varies with each project, the following four subcomponents are implemented: prevention, through awareness building for members of the community, parents and community-level stakeholders; medical care, through early identification and referral to suitable facilities; rehabilitation, with home-based basic rehabilitation services provided by nurses and social workers; provision of assistive devices, either through referral to the state system, through the development of local production capacity, or through direct provision by the nongovernmental organization. The large-scale involvement of the international community in community-based rehabilitation activities has been a vector for the introduction of modern basic rehabilitation techniques and, on the social side, for strong components of inclusive education and empowerment of people with disabilities, the ability to interact directly with the communities being an integral factor in the success of inclusion and mainstreaming activities. Direct involvement of communities is a key component in community-based rehabilitation projects, but in this respect these projects in Tajikistan have met with varying degrees of success. In addition, the projects are still being implemented, and further involvement of the communities is expected in future. The vast majority of the services are provided by social workers and community nurses (health workers) delegated by the Government, whose wages are paid by the international organizations and who are only incidentally members of the communities. As such, most of the activities are run under an outreach rather than a community-based rehabilitation model, owing to the limited involvement of the community. However, families receive training so that they can provide basic rehabilitation services themselves. This is a major step forward for communities that would otherwise, at best, receive weekly visits from outreach programmes, and at worst would have no access whatsoever to rehabilitation services.
43

As mentioned above, community-based rehabilitation projects can act as an extension of Government services, and this is certainly the case in Tajikistan. However, in their current form they have a tendency to suffer from the same constraints as outreach programmes in terms of transport costs and travel time. In 2010/11, 21 community-based rehabilitation support rooms were established in districts with locally made facilities to provide rehabilitation services, although only a few of them are currently operational. The nurses and social workers who provide the services are still employed by the state, and once funding stops, they will be able to provide these services only with the support of local authorities. Each project has also set up local rehabilitation committees, but these are unlikely to remain functional without the support of the current projects. A recent amendment to the Law on Social Protection of Persons with Disabilities calls for the creation of “coordination committees for the social protection of people with disabilities at oblast, city and district levels” (13), which might provide an opportunity to formalize the local rehabilitation committee structure within the Government.
All current community-based rehabilitation activities are heavily dependent on external, international funding, and their long-term sustainability is therefore not guaranteed unless Government agencies at national and local level are involved in planning, implementation, monitoring and evaluation of programmes. Government involvement in these projects needs to be improved: this remains a major issue in the long-term viability and sustainability of community-based rehabilitation projects. The lack of replication of these projects and/or development of original projects is also a concern for the future of community-based activities. This is characteristic of the fragmentation of responsibilities related to disability and the lack of a single body in charge, but also indicates a failure to present the positive results of these projects in a convincing manner. Considering that the national authorities recognize the limitations of the current model of centralized institutions, better cooperation between all parties involved (national and local authorities and international organizations) is needed to evaluate how community-based rehabilitation can be part of the national strategy on disability. The recent merging of social protection with health (in the new Ministry of Health and Social Protection) offers a window of opportunity for the Ministry to take the lead in this process and determine how this model can be integrated and implemented at the national level.
Human resources for rehabilitation Training and education of rehabilitation professionals While the majority of the specialists interviewed have been trained abroad, mostly during the Soviet era in what is now the Russian Federation, Tajikistan has increasingly had to rely on its own education system to train new medical staff. The Avicenna Tajik State Medical University is the sole provider of MD degrees in Tajikistan. The curriculum is set by the Ministry of Health and Social Protection, and although the university offers courses leading to six different postgraduate degrees, with 31 specializations, none is dedicated to rehabilitation professions. The core graduate curriculum also provides little training on disability and rehabilitation, with only 50 hours dedicated to massage and electrotherapy and no practical exposure to rehabilitation. While both the Ministry of Health and Social Protection and the university have expressed interest in developing a postgraduate degree in rehabilitation services in the future, it should be noted that international norms for developing human resources in the field of rehabilitation (physiotherapy and occupational therapy, prosthetics and orthotics, speech therapy, etc.), i.e. certificate/diploma, graduate level and postgraduate level, are not known in Tajikistan.
44

In addition, there are currently no specialists in the country capable of teaching such courses. Nurses are trained at the Medical College of Dushanbe and the Medical College of Khujand. Approximately 1400–2000 nurses graduate every year. Although they constitute the majority of health workers and contribute significantly to the provision of health services, nursing has so far failed to attract sufficient attention. Currently there are approximately 24 000 working nurses in Tajikistan. They work in preventive and curative health. Approximately 17 000 of them work as community nurses (health workers) in primary health care centres, and the remainder as nurses and trainers in hospitals (district, regional and national) and training institutes. There is one community nurse per 750 inhabitants, although there is a shortage of health workers in rural areas. In addition to the above, many nurses work in rehabilitation centres (national centres, psychological, medical and pedagogical consultation services, etc.) as rehabilitation personnel and have received extra on-the-job training in rehabilitation. There are some positive developments in the training of nurses. The Republican Institute of Nursing and Republican Institute of Family Medicine have been established to provide continuing professional education for working nurses. Both institutes have expressed their willingness to work on disability. Currently, nurses are involved in disability rehabilitation through the community-based rehabilitation programmes; however, a structured approach targeting the republican training institutes for nurses will help to mainstream disability in the primary health care system and develop disability-inclusive public health programmes. Although the original nursing diploma does not address rehabilitation, a new third-year optional specialization additional to the two-year nursing diploma has been developed by the Medical College of Dushanbe with the support of the Ministry of Health and Social Protection. The new course, aptly entitled Massage and Electrotherapy for Nurses, is currently taught at both facilities and focuses specifically on health care for people with disabilities. The first enrolled class will graduate from the Medical College of Dushanbe in June 2014. In some places, on-the-job trained social workers have become an important part of the provision of basic rehabilitation services. Social workers are trained in the social work department of the Tajik National University. The curriculum has been reviewed to prepare the workers to meet the needs of vulnerable groups (elderly or disabled people, orphans, etc.) more effectively. The first 40 students graduated with the new bachelor’s degree in June 2013. Among social-related courses, the current curriculum includes specific sections on social work with people with disabilities and art therapy. The Faculty of Pedagogy of the S. Ayni Tajik State Pedagogical University trains a variety of specialized educators, including educational psychologists and defectologists. It should be noted that the curriculums and details of the courses provided by the Pedagogical University were not made available for this report.
In the Soviet era, physiotherapy and occupational therapy were taught at postgraduate level. This two-year postgraduate training is available as a postgraduate specialization for graduate doctors and nurses and is available only in the Russian Federation (St Petersburg Medical and Social Institute, official communication, October 2013). At vocational level, in 2012, the Government of Tajikistan established an independent state institution, the Training and Practical Unit for Social Work and Innovations in Chorbog. In 2010/11, 20 staff members from selected institutions were trained in the basics of physiotherapy and occupational therapy at the institution. The training programme Basics of Physiotherapy and Occupational Therapy for Social Care Institutions focused on providing basic knowledge and skills for the safe movement of service-users, prevention of secondary complications, keeping
45

individuals physically active in everyday activities and adaptation to their surroundings (32). At the time of writing the report, most of the trained staff have left the country and/or changed their profession, and the centre has currently no plans to enrol new students. Indeed, as of June 2014, no new students have enrolled for the following year, making it unlikely that any classes will be taught in the 2014/15 academic year. Whether the centre will continue to operate in the future remains in question at the moment. In accordance with international norms on education in the physiotherapy and occupational therapy professions, these staff can only be classified as rehabilitation assistants, since there are no graduate physical or occupational therapy professionals to supervise them. However, the above initiative was an important development for Tajikistan, as it recognized the need for and importance of rehabilitation professionals.
Nevertheless, the introduction of modern rehabilitation practices remains slow and limited. Even newer diplomas, such as those provided by the medical colleges, have a curriculum based on a curriculum from Belarus and will thus do little to introduce internationally recognized techniques. In addition, modern practices are mostly introduced into the lower and mid-level diplomas on an ad-hoc basis, but no significant changes have been introduced at graduate or postgraduate level. This limits the adoption of modern practices, hampers proper supervision, and creates the potential for conflict between younger nurses and social workers and older medical specialists, who often were trained in the USSR. It is important to note that currently there is no professional human resource development in the fields of physiotherapy, occupational therapy, prosthetics and orthotics, speech therapy, physical medicine, rehabilitation, etc. The Convention on the Rights of Persons with Disabilities highlights the responsibilities of countries to promote the training of professionals and staff working with persons with disabilities, and investment is being supported in this area by the Ministry of Health and Social Protection, WHO and the Special Fund for the Disabled of the International Committee of the Red Cross. Four students from the Diploma in Nursing training and two doctors from national rehabilitation centres have been sent on bachelor’s courses in physiotherapy, occupational therapy and adapted courses in physical medicine and rehabilitation in India. In addition, the Special Fund for the Disabled anticipates the return of seven prosthetists and orthotists from training in Viet Nam in early 2015. In addition to state formal education, a number of short training courses have been provided by the international organizations involved in disability, including UNICEF, WHO and international nongovernmental organizations. Local nongovernmental and disabled people’s organizations have also been able to access external support to train their personnel. Although this training has had a very positive impact in modernizing the rehabilitation techniques and practices employed and addressing the current gaps in the State education system, sustainability remains an issue in the absence of formal supervision and continuing education. The hospital and clinical staff interviewed spoke highly of the training received and the positive results observed with the patients, but bemoaned the lack of formal Government-recognized certification and the absence of opportunities to refresh and upgrade their knowledge. Over the longer term, deterioration in the quality of practices can only be addressed by introducing these practices in the State education system and training internationally recognized graduate and postgraduate specialists capable of supervising rehabilitation facilities and staff.
46

Availability of rehabilitation professionals No statistics are available showing the number of posts currently vacant, but strong anecdotal evidence suggests that medical facilities struggle to recruit specialists in the field of rehabilitation. Physiotherapists and occupational therapists have only recently been added to the list of professions recognized by the state. As at the time of writing, there is no physiotherapist or occupational therapist currently practising in Tajikistan. The gap is not, however, recognized by these facilities, as management is not always aware of the existence of these professions, or does not feel the need to add them to the staff. It should be noted that, during the visits to facilities made as part of this situational analysis, a number of “physiotherapists” were interviewed. However, this title is a homonym partially transliterated from Russian,1 and does not refer to the profession of physiotherapist as the term is understood internationally. Physiotherapists in Tajikistan are medical practitioners who have received some training in physiotherapy in the USSR or the Russian Federation, with an emphasis on massage and electrostimulation. Because massage and electrostimulation are central elements of rehabilitation as practised in Tajikistan, these specialists are highly sought after by all suitably equipped facilities. As mentioned above, professions such as prosthetist and orthotist, physical medicine therapist, rehabilitation therapist, speech therapist, etc. are still not included in the All-Republican Classifier of Occupations in Tajikistan. Many facilities have reported that they have tried, and failed, to hire psychologists. There is an increasing awareness among medical professionals of the psychological aspect of disability and its importance in the rehabilitation process for all disabilities, as well as the need to provide both training and psychological support for parents and other relatives. While this is a welcome evolution in the management of persons with disabilities, there are simply not enough practising psychologists in Tajikistan to fill the new posts. Speech therapists and the various pedagogical specialities related to sensory disabilities also constitute a major gap in the supply of personnel. Senior positions are currently filled by staff trained abroad on short-term courses, and several facilities have reported that younger staff trained in Tajikistan might not able to replace them with the same level of competence. Besides the failings of the still-developing educational system, the main issue affecting personnel hiring and retention remains the shortcomings of human resource management, outdated medical equipment, the poor state of health facilities and low salaries. Not only are salaries not competitive with the private sector, medical staff can also find better working conditions abroad. One facility trying, and failing, to hire a psychologist reported that it could offer a salary of around US$ 200 per month for the position, but said the same professional could easily earn 10 times as much setting up a private practice in the Russian Federation. The current pay grades also affect the quality of the students who enter the Medical University and colleges, as the brightest students are more likely to pursue studies in economics or business rather than medicine. The quality of medical professionals is therefore likely to decrease in the coming years, as senior specialists trained in Moscow and other leading Soviet-era universities continue to retire.
1 The Russian word also translates as “physiotherapist”, but the profession has evolved considerably in the rest of the world. In Tajikistan, the word still has its original, Soviet-era meaning.
47
The cost of exclusion Countries most often view the cost of disability in terms of the services, structures and social assistance required, but ignore the cost in lost production of excluding people with disabilities from the workforce. Firstly, the relationship between poverty and disability should be emphasized. Poverty leads to disability through lack of access to services, lack of awareness and knowledge, and employment in manual and dangerous jobs. In turn, disability leads to poverty through lack of opportunities, loss of jobs, cultural barriers and exclusion from society. Any country looking to maximize the opportunities available to its population should attempt to break the cycle of disability and poverty.
The economic and social costs of disability are significant, but difficult to quantify. They include direct and indirect costs, some borne by people with disabilities themselves and their families, friends and employers, and some by society. Many of these costs arise because of inaccessible environments, and could be reduced in a more inclusive setting. Knowing the cost of disability is important not only for making a case for investment, but also for the design of public programmes. Estimates of the cost of disability are scarce and fragmented. The report Disability issues, trends and recommendations for the World Bank (49) attempts to measure the loss of GDP revenue due to unemployment resulting from disability by extrapolating from earlier research in Canada to the rest of the world. Because a number of assumptions have to be made, the report produces a low and high estimate rather than a unique figure. For 1997, GDP loss due to exclusion of people with disabilities is estimated to be between 1.16% and 1.35% of total GDP for Tajikistan. As employment among persons with disabilities has not changed measurably between 1997 and 2012, we can reasonably assume that these figures, albeit rough estimates, are still indicative, and represent losses of between US$ 80 million and US$ 94 million per year for Tajikistan. A further study published in 2009 by the International Labour Organization aimed to refine earlier figures on the macroeconomic losses incurred through exclusion of people with disabilities from the workforce through the analysis of three factors: labour productivity losses due to a disabling work or social environment, gaps between potential and actual productivity of people with disabilities, and differences in unemployment rates (50). The study included 10 middle-income countries from Asia and Africa, using country-level data and country-sensitive statistical information rather than extrapolation from previous studies. The study showed a net loss of GDP incurred of between 3% and 7%. Although this report does not include Tajikistan and does not argue that these figures are valid for that country, there remains a strong economic argument for strengthening rehabilitation services and inclusion in society in general and the workforce in particular: considering the current low level of expenditure by the state on the health system, any additional expenditure on health and rehabilitation services that result in people with disabilities returning to and/or performing fully in the workforce is greatly outweighed by the cost of not making that investment. Without access to health and rehabilitation, people are often confined to their homes – excluded from participating in society, and locked into poverty and isolation. The above analysis confirms that greater investment is required in the field of health and rehabilitation to ensure that all persons with disabilities enjoy functioning, independence and better quality of life.
48
Conclusions and recommendations Tajikistan has shown tremendous potential for rehabilitation following the outbreak of poliomyelitis in 2010. The availability of rehabilitation services for people with disabilities has increased in recent years. Many of the current pilot programmes show great promise, despite the harsh geography of the country and the difficulty of extending services to everyone who needs them. The increased health spending by the Government in the past five years is showing results, albeit still limited at this point. However, the main finding of this report is that the rehabilitation services currently available in Tajikistan remain inadequate to serve the needs of the population, in terms of both quantity and quality. In terms of quantity, the current services cannot provide proper geographical coverage for the whole population. The centralization of the system, in facilities mostly located in major urban centres, constitutes an essential barrier to access to services for the large majority of the population that lives in remote rural communities and does not have the means to travel.
The quality of the services is of great concern. Facilities commonly report difficulties in employing rehabilitation professionals, but even when staff are available, their work is hampered by ageing infrastructures and a lack of the necessary skills. Finally, the classification of disability and the status of persons with disabilities in Tajikistan also remain an issue, in the absence of a unified and serviceable model of identification. The different challenges identified that need to be addressed in a comprehensive manner can be summarized as follows:
• socioeconomic situation of persons with disabilities and their families, who are oftenliving in poverty;
• lack of a strategy on disability and a limited legislative framework;
• lack of professional-level human resources in the field of rehabilitation;
• lack of rehabilitation services at all levels, especially in rural areas where mostpeople live;
• lack of quality standards and adequate monitoring of disability and rehabilitationservices;
• limited coordination and mechanisms for referral between service providers;
• limited knowledge and understanding about the place of rehabilitation in the health-care system;
• limited funding for disability and rehabilitation activities;
• poor coordination among the few stakeholders supporting disability and rehabilitationin Tajikistan;
• limited involvement of people with disabilities in decision-making;
• environmental barriers facing persons with disabilities;
• limited availability of assistive devices;
• stigma and prejudice which hinder access to services;
• a general lack of information about the benefits and potential of rehabilitationservices to reduce impairment and disability and promote inclusion and participation.
The recommendations presented below propose practical solutions that both take into account the specificity of the country and are implementable within 10 years.
49

Strengthening existing services The scope and geographical coverage of rehabilitation services in Tajikistan need to be strengthened: most persons with disabilities are unlikely to have access to these services at present. Currently, the majority of services are based in cities and availability of rehabilitation services at community level is limited. It is recommended that rehabilitation services should be decentralized, integrated into the primary health care system and complemented with community-based rehabilitation and strengthening of psychological, medical and pedagogical consultation services, daycare centres and national rehabilitation centres. A robust referral and follow-up system should be developed. It is highly recommended that the national rehabilitation centres should introduce outpatient services, along with family training. This will help to prevent institutionalization of persons with disabilities. Support mechanisms to improve the continuum of care experienced by persons with disabilities need to be strengthened through referral pathways, follow-up mechanisms and multidisciplinary and multisectoral teamwork. The following scheme for the rehabilitation services (Fig. 10) is recommended, coming under the authority of the Ministry of Health and Social Protection.
Fig. 10. Recommended structure of rehabilitation services
Note. PMPC = psychological, medical and pedagogical consultation service.
Community Level (Health workers and workers in social assistance at home units)
Health promotion and disability prevention Early identification of disabling conditions and disability, referral to secondary levels
Basic interventions to avoid complications Follow-up
Referral to social protection services Disability awareness for family and community
Support formation and strengthening of disability network
District level (PMPC and daycare centre)
Rehabilitation services – physiotherapy, occupational therapy, speech therapy, psychosocial care, assistive devices Assess for social protection services
Referral for access to medical care at district hospital/ specialized rehabilitation services and follow-up
Support for access to education (including special education), employment and other services
Support initiation of community based rehabilitation programmes at community level Outreach and mobile services to support primary care
Strengthen disability network
Prim
ary
care
Seco
ndar
y ca
reTe
rtia
ry c
are
Regional and national level (national rehabilitation centres, specialized hospitals)
Rehabilitation services (inpatient and outpatient) – physiotherapy, occupational therapy, assistive devices, prosthetics and orthotics,
speech therapy, psychosocial care, etc. Referral to regional/national hospitals and follow-up
Outreach and mobile services to support secondary and primary care Support for access to education, employment and other mainstream
services
50

Improving human resource capacity Tajikistan needs to develop its own pool of specialists in the fields of physiotherapy and occupational therapy, prosthetics and orthotics, speech therapy and allied health professions, which are essential to the provision of effective rehabilitation services. It will also be important to upgrade the All-Republican Classifier of Occupations in Tajikistan to include important professions such as prosthetist and orthotist, physical medicine specialist, rehabilitation specialist, speech therapist, etc. The first step is to train a reasonable number of graduates in physiotherapy and occupational therapy in a country that provides internationally recognized degrees. Upon completing their education and returning to Tajikistan, at least some of these physiotherapists and occupational therapists must teach at the Medical University and/or medical colleges, to increase the number of specialists at the highest level. To ensure decentralization of services, it will be extremely important to address specific challenges to the quality of health care experienced by people with disabilities, including health workers’ knowledge, attitudes and practices. This requires training for existing health workers – doctors and health workers working in primary health care and existing public health-care service providers (polyclinics and hospitals) – in the importance of rehabilitation services for persons with disabilities. In addition, relevant graduate and postgraduate curriculums for doctors and nurses need to be strengthened in the areas of disability and rehabilitation. Despite the growth in health expenditure, there is currently limited funding to address the three major concerns observed in the existing facilities: the decay of the infrastructure, the lack of workspace, and the lack of modern rehabilitation equipment. Although this report recognizes Tajikistan’s current economic difficulties, and even with the potential for international support, increased health expenditure and strict monitoring of funding are necessary steps, not only to modernize and maintain the existing infrastructure, but also to extend and develop new facilities to cater for the growing number of persons with disabilities. While, generally speaking, all public facilities should be made accessible, it is vital that all facilities (existing and future) providing services for persons with disabilities should be made fully accessible if they are to fulfil their function. Personnel retention within the medical system is already an issue that will only be compounded by the introduction of new, internationally trained specialists. While wages have slowly been increasing, they currently cannot match those on offer in the Russian Federation or Tajikistan’s neighbours. Efforts to increase wages have to be pursued if specialists trained abroad are to be retained within the Tajik medical system in the long term. Both financial and nonfinancial incentives need to be offered, e.g. opportunities for continuing education and career development, professional association, improvements in working conditions and improved status of relevant professions would all contribute to better personnel retention. Existing protocols and rehabilitation guidelines for various disabling conditions should be updated and developed, as required. In addition, it is important for a glossary of commonly used terms in the field of disability and rehabilitation to be developed in Tajikistan. This process would be supported by the training of specialists abroad. All protocols should be evidence-based and consistent with international standards, and long-term regulatory mechanisms should be put in place to ensure that these standards are consistently applied.
51

Improving identification of disabilities This report strongly recommends the adoption of international standards for the identification and classification of disabilities in Tajikistan. The current system is open to interpretation, which leads to discrepancies and the potential for manipulation. Tajikistan already has a wide-ranging network of facilities and medical specialists dedicated to the identification and the classification of disabilities (Agencies for Medical and Social Examination and Doctor’s Consultative Commissions), and adoption of international standards (e.g. Washington Group on Disability Statistics, ICF, etc.) would provide a common, unified and rigorous model to support the diagnoses reached by the medical commissions. Adoption of international standards would not necessarily imply increased funding for disability care from the state, but would provide a useful guideline for improving the efficient allocation of resources dedicated to people with disabilities, both for the development of services and for the provision of social assistance and benefits.
Extending services to all The mountainous geography of Tajikistan constitutes a major barrier to access to services for the rural population. Not only does the most vulnerable population not have the means to pay transport costs, but many disabilities also hamper travel. Decentralization of services, and a greater flexibility for regional and district facilities to provide their services in a way that allows them to reach the largest possible number of the rural population, would be a useful step in extending the coverage of existing service providers. In addition, the community-based rehabilitation model has been developed specifically to reach populations that do not have access to mainstream services in low-income countries, and as such, it is particularly well adapted to Tajikistan. Regional and local governments have recently been developing outreach programmes, in which social workers and nurses provide home-based basic rehabilitation services. These programmes have the potential to be successful, and certainly deserve to be supported and replicated in the development of community-based rehabilitation. However, rehabilitation is a daily process, and for the more remote communities, daily services can only be achieved by involving the communities themselves. All projects currently active in the country are run by nongovernmental organizations, and it is vital that the Government, at both national and local level, is involved in all phases of programme development and acquires the knowledge required to run such projects successfully, so that these services are sustainable and available throughout the country. Every community-based rehabilitation project currently active in Tajikistan is run according to its own model. While it is not within the remit of this report to determine which of these models is optimally adapted for Tajikistan, appropriate models need to be agreed and/or developed at national level to serve as a basis for future Government-run programmes. That model should remain flexible, however, to allow for the variety of situations encountered in the field and to ensure that local authorities are able to implement the required activities with the local resources available.
Disability-inclusive health People with disabilities have the same rights as the general population to participate and be included in all aspects of their communities, which includes access to services such as health care. Disability-inclusive health refers to the process of including people with disabilities in the health-care services that are available to the general population. Many people presume that people with disabilities have specific health needs related to their disability and therefore require “specialist health services”. While this may be true for some people with disabilities, it should be recognized that all people with disabilities have
52
general health-care needs, for example immunization or screening for chronic health conditions, and therefore also require access to “mainstream” health services. To achieve universal coverage and in order for health-care services to become inclusive of people with disabilities, changes may be required at the level of the health system, health service or individual health provider. In Tajikistan, this may include changes in legislation and policies, implementation of reasonable accommodations and education of health workers to bring about changes in attitudes towards people with disabilities.
Improving the legislative framework relating to disability While Tajikistan has developed strong legislative frameworks, references to disability in strategy documents remain sporadic. Persons with and without disabilities need to enjoy equal rights. Several studies show that persons with disabilities are commonly excluded and denied their basic rights and entitlements. In addition, one of the major issues identified is the lack of an overall national disability strategy setting out a consolidated and comprehensive long-term vision for improving the well-being of persons with disabilities. It is recommended that a national disability strategy and action plan should be developed. The national disability strategy should be based on the principles and ethos of the Convention on the Rights of Persons with Disabilities and Tajikistan legislation. In addition, it is recommended that the Law of the Republic of Tajikistan on Social Protection of Disabled Persons (2010) should be reviewed and amended to produce a comprehensive law on the rights of persons with disabilities. This law should cover all sectors, specifying mechanisms of coordination, decision-making, regular monitoring and reporting, and control of resources. Participation by civil society, particularly disabled people’s organizations, in the preparation of strategic documents, a process that is already envisaged by the law, would ensure that the needs of people with disabilities are taken into account. Monitoring and enforcement of existing and new laws need to be strengthened. Bridging the divide between what is prescribed by the law and the actual application of the law in practice should not be the sole realm of civil society, as it is today. Monitoring would also benefit considerably from a strong national-level coordination body, so that all disability-related interventions are coherent and enforced. It will be extremely important for there to be one responsible agency or ministry for coordination, decision-making, implementation of the laws, monitoring and reporting. In the case of Tajikistan, this will be the Ministry of Health and Social Protection, and this will also ensure greater accountability. It is also recommended that in each relevant Government ministry – especially health and social protection, education, labour and transport – a focal point should be appointed for people in vulnerable situations, such as persons with disabilities, children or elderly people. This would also ensure that a single interlocutor is in charge of disability-related issues in each sector. It is recommended that the present coordination forum on disability, the Coordination Council, is strengthened by adopting a multisectoral approach. It will be important to identify its objectives, plans and deliverables. The Government of Tajikistan has been studying the feasibility of ratifying the Convention on the Rights of Persons with Disabilities, and this report strongly supports this process. Ratification of the Convention would provide an internationally recognized common basis for Tajikistan’s efforts to develop rehabilitation services.
Changing societal attitudes Despite the recognition of equal rights for all people in Tajikistan, persons with disabilities still struggle on the margins of recognition. They often face stigma, discrimination and misunderstanding from their families and society. Social and economic inclusion and
53
participation in social, cultural, economic and political life are hindered by a lack of understanding, based on stereotypes and misperceptions among the general population of the rights, needs and abilities of persons with disabilities. Persons with disabilities are still seen as objects of charity, not as rights-holders who are capable of making decisions and participating in society. Persons with disabilities, or their families, are often unaware of their rights and lack the capacity to advocate on their own behalf. Despite significant changes, there has been limited improvement in the situation of persons with disabilities, and one of the major contributing factors in this is societal attitudes towards persons with disabilities. A cultural change within Tajik society is required to facilitate reform in the disability sector. This may involve increasing awareness, educating on a large scale and shifting attitudes to move towards genuine community inclusion of persons with disabilities. It is essential to disseminate information about disabilities in order to change negative attitudes towards persons with disabilities in society at large. It is recommended that a behavioural communication and change strategy and plans for disability issues should be developed and implemented. These should target family and community members, service providers and authorities at all levels to promote an inclusive and rights-based society. In addition, persons with disabilities and community members should be trained on the need for and importance of high-quality rehabilitation services as well as on the rights of persons with disabilities.
Improving accessibility of facilities In Tajikistan, persons with disabilities face a multitude of obstacles in their physical environment. Built environments, transport systems and information are often inaccessible. Lack of physical access (e.g. to health centres) is a frequent reason for a person with a disability being discouraged from accessing services and subsequently remaining confined in residential hostels or at home. This is compounded by the mountainous terrain, ageing infrastructure and harsh winter conditions in Tajikistan. In addition, the communication needs of people with disabilities often remain unmet. Information is rarely available in accessible formats, and some people with disabilities are unable to access basic information. These barriers prevent persons with disabilities from participating in social, cultural or professional life on an equal basis with other citizens, and also prevent them from fully exercising their rights. A barrier-free, accessible environment improves their participation and mobility and is a prerequisite for a truly inclusive society. As well as persons with disabilities, the entire society, including the elderly, pregnant women, people in a temporary situation of reduced mobility, children, etc., benefits from improved accessibility.
It is recommended that legislation on accessibility should be strengthened, awareness-raising activities should be conducted and essential existing buildings and all new buildings should be made accessible and barrier-free to enable greater access to services for persons with disabilities. In addition, communication materials must be developed in appropriate and accessible formats, e.g. audio or braille for persons with a visual disability, written or pictorial presentation for hearing-impaired people and audiovisual materials. Government, donors, civil society organizations and communities need to work together systematically to facilitate barrier-free environments and access to services for everyone.
54
Improving data collection Understanding the numbers of people with disabilities and their circumstances can improve country efforts to remove disabling barriers and provide appropriate services for people with disabilities. Although some of the ministries and agencies have their own figures relating to persons with disabilities, no consistent effort has been made to collect reliable data. No single-source data are available from the Government for all schemes related to disabilities. For instance, the Agency on Social Insurance and Pensions is the main agency that collects data on persons with disabilities, but it only collects data related to allowances and pensions which are directly disbursed. The programmes implemented by civil society organizations have no consistent data on their beneficiaries. Establishment of a single centralized database for persons with disabilities is recommended, in order to use resources as effectively as possible and to formulate and implement appropriate policies, plans and programmes. Methodologies for collecting data on persons with disabilities need to be developed, tested and consistently applied. Data need to be standardized and internationally comparable for benchmarking and monitoring progress on disability issues. Nationally, disability data should be included in data collection. In the short term, it is recommended that national health and social surveys should include information on disability, disaggregated by population features such as age, sex, race, socioeconomic status, etc. This will also produce information on disability prevalence, health conditions associated with disability and use of and need for services, including rehabilitation. In the long term, it is recommended that national population census data should include details of persons with disabilities.
References 1. Statistical Agency under the President of the Republic of Tajikistan, 2013.2. United Nations Development Programme. Human development report 2009.
Basingstoke/New York: Palgrave Macmillan; 2009(http://hdr.undp.org/en/content/human-development-report-2009, accessed 27August 2014).
3. Kumar S, Jain A, Bruce J. Assessing the quality of family planning services indeveloping countries. New York: The Population Council; 1989 (Programs DivisionWorking Paper, No. 2; http://www.popline.org/node/369190, accessed 4 September2014).
4. World Health Organization, World Bank. World report on disability. Geneva: WorldHealth Organization; 2011 (http://www.who.int/disabilities/world_report/2011/en/,accessed 17 August 2014).
5. Katsui H. Towards equality. Creation of the disability movement in Central Asia.Helsinki: Helsinki University Department of Social Policy and Institute ofDevelopment Studies, Helsinki University; 2005(http://digitalcommons.ilr.cornell.edu/gladnetcollect/331/, accessed 27 August 2014).
6. United Nations General Assembly resolution A/RES/61/106 on a Convention on theRights of Persons with Disabilities. New York: 2007(http://www.refworld.org/docid/45f973632.html, accessed 27 August 2014).
7. United Nations General Assembly resolution A/RES/48/96 on the United NationsStandard Rules on the Equalization of Opportunities for Persons with Disabilities.New York: 1993 (http://www.un.org/esa/socdev/enable/dissre00.htm, accessed 27August 2014).
55

8. United Nations General Assembly resolution A/RES/66/2 on the Political Declarationof the High-level Meeting of the General Assembly on the Prevention and Control ofNon-communicable Diseases. New York: 2011(http://www.un.org/depts/dhl/resguide/r66_en.shtml, accessed 27 August 2014).
9. Highlights on health in Tajikistan 2005. Copenhagen: World Health Organization;2005 (http://www.euro.who.int/__data/assets/pdf_file/0010/103600/E88393.pdf?ua=1, accessed 27 August 2014).
10. Global report: UNAIDS report on the global AIDS epidemic 2012. Geneva: JointUnited Nations Programme on HIV/AIDS (UNAIDS); 2012(http://www.unaids.org/en/resources/publications/2012/name, accessed 27 August2014).
11. Groce N. Global survey on HIV/AIDS and disability. New Haven, CT: WorldBank/Yale University; 2004(http://siteresources.worldbank.org/DISABILITY/Resources/Health-and-Wellness/HIVAIDS.pdf, accessed 10 September 2014).
12. Living standards improvement strategy of Tajikistan for 2013−2015. Dushanbe:Republic of Tajikistan; 2012(http://www.tj.undp.org/content/dam/tajikistan/docs/legal_framework/UNDP_TJK_MidTermReview_eng.pdf, accessed 4 September 2014).
13. Law on Social Protection of Persons with Disabilities (No. 675 of 29 December2010)(in Russian) (http://www.ilo.org/dyn/natlex/country_profiles.nationalLaw?p_lang=en&p_country=T JK, accessed 10 September 2014).
14. Mental health declaration for Europe. Copenhagen: WHO Regional Office for Europe;2005 (EUR/04/5047810/6; http://www.euro.who.int/en/health topics/oncommunicable-diseases/mental-health/publications/2005/who-mental-health-declaration-for-europe,accessed 4 September 2014).
15. Mental health action plan for Europe. Copenhagen: WHO Regional Office for Europe;2005 (EUR/04/5047810/7; http://www.euro.who.int/en/health-topics/oncommunicable-diseases/mental-health/policy, accessed 4 September 2014)
16. Grover A. Report of the Special Rapporteur on the right of everyone to the enjoymentof the highest attainable standard of physical and mental health: Addendum: Missionto Tajikistan (24–31 May 2012). Geneva: United Nations Human Rights Council;2013 (http://www.refworld.org/docid/51a7406f4.html, accessed 16 October 2014).
17. World development indicators 2012. Washington, D.C.: International Bank forReconstruction and Development/World Bank; 2012 (http://data.worldbank.org/data-catalog/world-development-indicators/wdi-2012, accessed 4 September 2014).
18. Tajikistan: world development indicators [database]. Washington, D.C.: World Bank;2012 (http://data.worldbank.org/country/tajikistan, accessed 7 April 2014).
19. 2012-2013 Joint annual review report of implementation of the National HealthStrategy (2010-2020) of the Republic of Tajikistan. Dushanbe: Ministry of Health;2013.
20. Khodjamurodov G, Rechel B. Tajikistan: health system review. Health Systems inTransition. 2010;12(2):1–154 (http://www.euro.who.int/__data/assets/pdf_f ile/0009/119691/E94243.pdf, accessed 4 September 2014).
21. Statistical book of education sector of the Republic of Tajikistan for 2010-2011academic year. Dushanbe: Ministry of Education; 2011.
56

22. Facts on disability in the world of work. Geneva: International Labour Organization;2007 (http://www.ilo.org/asia/info/public/background/WCMS_098454/lang--en/index.htm, accessed 16 October 2014).
23. Disability, poverty and development (Issues Paper). London: United KingdomDepartment for International Development; 2000.
24. Son HH. Evaluating social protection programs in Tajikistan. Manila: AsianDevelopment Bank; 2011 (Asian Development Bank Economics Working PaperSeries No. 274; http://ssrn.com/abstract=1943271;http://dx.doi.org/10.2139/ssrn.1943271, accessed 4 September 2014).
25. Law of the Republic of Tajikistan on the State budget for 2012 (No. 766 of8 November 2011). Dushanbe: Republic of Tajikistan; 2011.
26. Healthcare in the Republic of Tajikistan. Dushanbe: Statistical Agency under thePresident of the Republic of Tajikistan; 2013.
27. Tadžikistan v cifrah 2013 [Tajikistan in figures 2013]. Dushanbe: Agency on Statisticsunder the President of the Republic of Tajikistan; 2013 (in Russian).
28. Social and economic status of the Republic of Tajikistan, January–December 2012.Dushanbe: Agency on Statistics under the President of the Republic of Tajikistan;2012.
29. Tajikistan: poverty assessment. Washington, D.C.: World Bank; 2009(http://documents.worldbank.org/curated/en/2009/12/11664677/tajikistan-poverty-assessment, accessed 16 October 2014).
30. Social and economic status of the Republic of Tajikistan, January–December 2013.Dushanbe: Agency on Statistics under the President of the Republic of Tajikistan;2014.
31. Certi bednosti v Tadjikistane net! [There are no signs of poverty in Tajikistan!]pressa.tj [website], 25 January [2011] (http://www.pressa.tj/news/cherty-bednosti-v-tadzhikistane-net, accessed 10 September 2014) (in Russian).
32. Technical assistance to sector policy support programme in the social protectionsector – service delivery component, Tajikistan (implemented by consortium led byOxford Policy Management Ltd., 2009-2013).
33. Global action plan for the prevention and control of noncommunicable diseases2013-2020. Geneva: World Health Organization; 2013(http://www.who.int/nmh/publications/ncd-action-plan/en/, accessed 12 September 2014)
34. World health statistics 2012. Geneva: World Health Organization; 2012(http://www.who.int/gho/publications/world_health_statistics/2012/en/, accessed 12September 2014).
35. Strategy for prevention and control of noncommunicable diseases and injuries in theRepublic of Tajikistan for 2013- 2023. Dushanbe: Ministry of Health and SocialProtection, 2013.
36. Tajik Republican AIDS Centre, Ministry of Health of Tajikistan, January 2014.37. Office of the United Nations High Commissioner for Refugees, World Health
Organization, Joint United Nations Programme on HIV/AIDS. Disability and HIVpolicy brief. Geneva: World Health Organization; 2009(http://www.who.int/disabilities/jc1632_policy_brief_disability_en.pdf, accessed 1 October 2014).
38. International Lithosphere Program. Global Seismic Hazard Map [website](http://www.seismo.ethz.ch/static/GSHAP/, accessed 1 October 2014).
57
39. WHO Regional Office for Europe, Ministry of Health of Tajikistan. Health Assessmentfor Tajikistan. Copenhagen: WHO Regional Office for Europe; 2008.
40. WHO, CBM, International Federation of Red Cross and Red Crescent Societies,International Organization for Migration, UNICEF, United Nations Office for DisasterRisk Reduction. Guidance note on disability and emergency risk management forhealth. Geneva: World Health Organization; 2013.
41. UNWomen, Bureau for Human Rights and Rule of Law, Ishtirok. Implementation ofthe rights of people with disabilities in Sughd Province, Republic of Tajikistan.Dushanbe: Bureau for Human Rights and Rule of Law; 2012.
42. Children and disability in transition in CEE/CIS and Baltic States. Florence: UnitedNations Children’s Fund, 2004 (http://www.unicef.org/ceecis/Disability-eng.pdf,accessed 20 September 2014).
43. Report on assessing social assistance at home departments in priority districts of theRepublic of Tajikistan. Dushanbe: Ministry of Labour and Social Protection of thePopulation, UNICEF, Faroshturuk; 2011.
44. Needs of persons with disabilities in the Republic of Tajikistan – analytical report.Dushanbe: Ministry of Health; 2013.
45. Cuccurullo S, editor. Physical Medicine and Rehabilitation Board review. New York:Demos; 2004.
46. Situational assessment report on mobility devices and wheelchairs in Tajikistan.Dushanbe: World Health Organization; 2014.
47. World Health Organization, International Society of Prosthetics and Orthotics, UnitedStates Agency for International Development. WHO guidelines on the provision ofmanual wheelchairs in less-resourced settings. Geneva, World Health Organization, 2008 (http://www.who.int/disabilities/publications/technology/wheelchairguidelines/en/, accessed 2 October 2014).
48. Community-based rehabilitation: CBR guidelines. Geneva: World HealthOrganization; 2010 (http://www.who.int/disabilities/cbr/guidelines/en/, accessed 2October 2014).
49. Metts RL. Disability issues, trends and recommendations for the World Bank.Washington, D.C.: World Bank; 2000 (http://siteresources.worldbank.org/DISABILITY/Resources/280658- 1172606907476/DisabilityIssuesMetts.pdf,accessed 2 October 2014).
50. Buckup S. The price of exclusion : the economic consequences of excluding peoplewith disabilities from the world of work. Geneva: International Labour Office; 2009(Employment Working Paper No. 43; http://www.ilo.org/wcmsp5/groups/public/---ed_emp/---ifp_skills/documents/publication/wcms_119305.pdf, accessed 2 October2014).
58
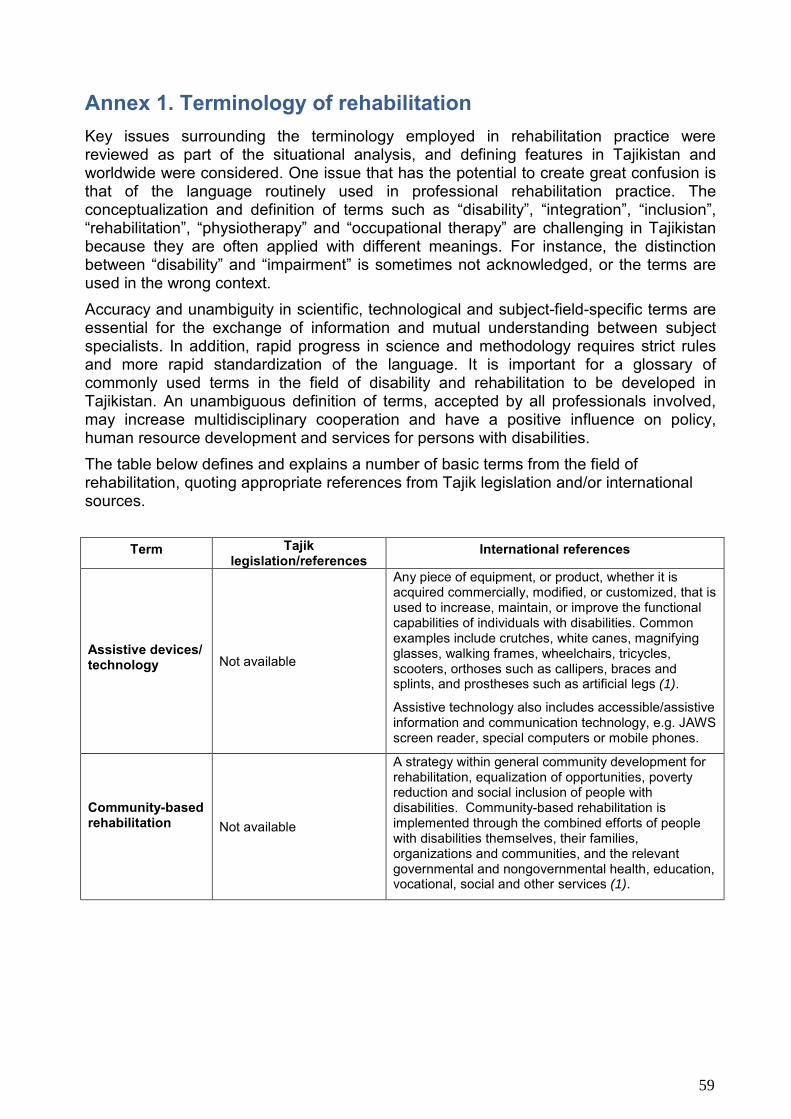
Annex 1. Terminology of rehabilitation Key issues surrounding the terminology employed in rehabilitation practice were reviewed as part of the situational analysis, and defining features in Tajikistan and worldwide were considered. One issue that has the potential to create great confusion is that of the language routinely used in professional rehabilitation practice. The conceptualization and definition of terms such as “disability”, “integration”, “inclusion”, “rehabilitation”, “physiotherapy” and “occupational therapy” are challenging in Tajikistan because they are often applied with different meanings. For instance, the distinction between “disability” and “impairment” is sometimes not acknowledged, or the terms are used in the wrong context. Accuracy and unambiguity in scientific, technological and subject-field-specific terms are essential for the exchange of information and mutual understanding between subject specialists. In addition, rapid progress in science and methodology requires strict rules and more rapid standardization of the language. It is important for a glossary of commonly used terms in the field of disability and rehabilitation to be developed in Tajikistan. An unambiguous definition of terms, accepted by all professionals involved, may increase multidisciplinary cooperation and have a positive influence on policy, human resource development and services for persons with disabilities. The table below defines and explains a number of basic terms from the field of rehabilitation, quoting appropriate references from Tajik legislation and/or international sources.
Term Tajik legislation/references
International references
Assistive devices/ technology Not available
Any piece of equipment, or product, whether it is acquired commercially, modified, or customized, that is used to increase, maintain, or improve the functional capabilities of individuals with disabilities. Common examples include crutches, white canes, magnifying glasses, walking frames, wheelchairs, tricycles, scooters, orthoses such as callipers, braces and splints, and prostheses such as artificial legs (1).
Assistive technology also includes accessible/assistive information and communication technology, e.g. JAWS screen reader, special computers or mobile phones.
Community-based rehabilitation Not available
A strategy within general community development for rehabilitation, equalization of opportunities, poverty reduction and social inclusion of people with disabilities. Community-based rehabilitation is implemented through the combined efforts of people with disabilities themselves, their families, organizations and communities, and the relevant governmental and nongovernmental health, education, vocational, social and other services (1).
59

Disability
Disability is a measure of restriction of vital activity of a person as a result of disability, with strong dysfunction of body functions (2).
Disability is a person’s full or partial loss of abilities or capabilities to: care for him or herself, move independently, orient him or herself, communicate, control his or her behaviour, learn and/or engage in employment.
There are two models of disability:
a) an individual model(medical approach), whereby the person with disabilities is considered as: a patient; sick; in severe need of medical care and not able to participate fully in society (this perception was common in the former Soviet Union). The main characteristic of this model is segregation: separation of persons with disabilities from mainstream society and creation of specialized residential care facilities for them.
b) a social model, whereby
WHO defines disability as a contextual variable, dynamic over time and in relation to circumstances. One is more or less disabled based on the interaction between the person and the individual, institutional and social environments. Disabilities is an umbrella term, covering impairments, activity limitations and participation restrictions. An impairment is a problem in body function or structure; an activity limitation is a difficulty encountered by an individual in executing a task or action; while a participation restriction is a problem experienced by an individual in involvement in life situations. Disability is thus not just a health problem. It is a complex phenomenon, reflecting the interaction between features of a person’s body and features of the society in which he or she lives. Overcoming the difficulties faced by people with disabilities requires interventions to remove environmental and social barriers (4). Disability can be described at three levels: body (impairment of body function or structure), person (activity limitations) and society (participation restrictions) (1).
the person with disabilities is perceived as: an ordinary person; operating in a working environment; studying equally alongside others; living a full life and receiving the same services as other members of society. The main feature of this model is integration – creation of equal opportunities for livelihood and development of persons with disabilities in society. This integrated approach also means the creation of [favourable] learning and employment conditions for people with disabilities. [Translated from (3)]
60
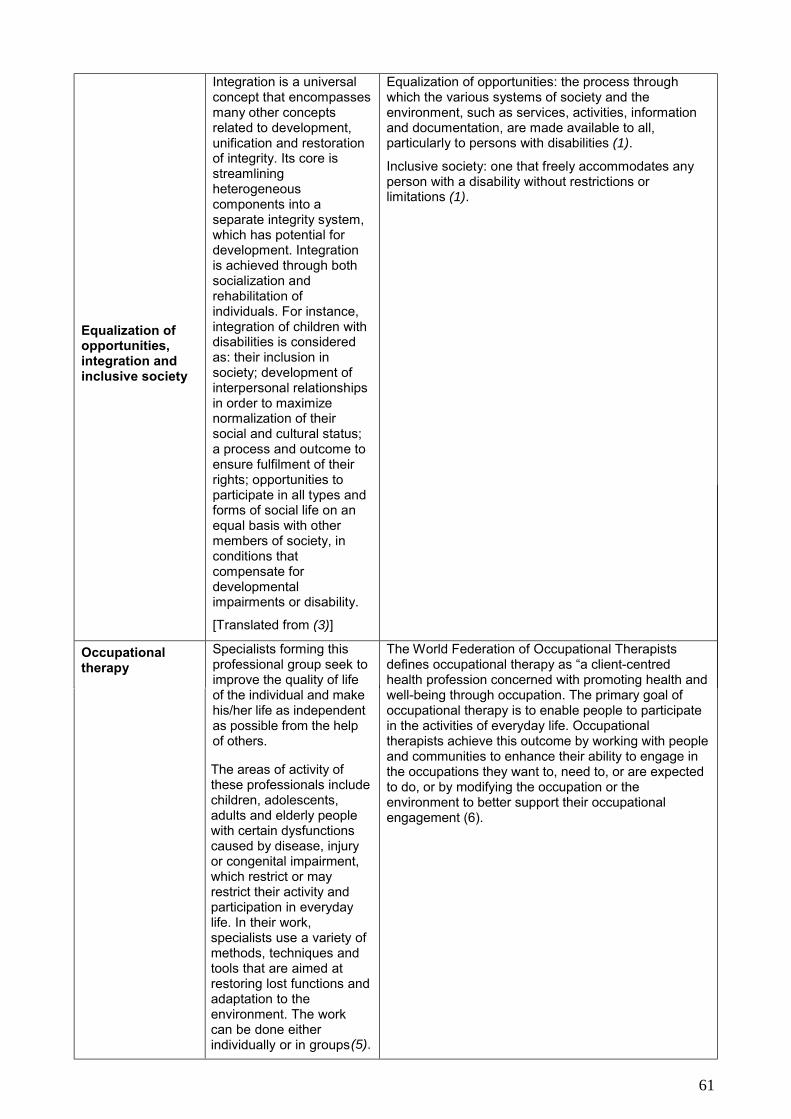
Equalization of opportunities, integration and inclusive society
Integration is a universal concept that encompasses many other concepts related to development, unification and restoration of integrity. Its core is streamlining heterogeneous components into a separate integrity system, which has potential for development. Integration is achieved through both socialization and rehabilitation of individuals. For instance, integration of children with disabilities is considered as: their inclusion in society; development of interpersonal relationships in order to maximize normalization of their social and cultural status; a process and outcome to ensure fulfilment of their rights; opportunities to participate in all types and forms of social life on an equal basis with other members of society, in conditions that compensate for developmental impairments or disability.
[Translated from (3)]
Equalization of opportunities: the process through which the various systems of society and the environment, such as services, activities, information and documentation, are made available to all, particularly to persons with disabilities (1).
Inclusive society: one that freely accommodates any person with a disability without restrictions or limitations (1).
Occupational therapy
Specialists forming this professional group seek to improve the quality of life of the individual and make his/her life as independent as possible from the help of others.
The World Federation of Occupational Therapists defines occupational therapy as “a client-centred health profession concerned with promoting health and well-being through occupation. The primary goal of occupational therapy is to enable people to participate in the activities of everyday life. Occupational therapists achieve this outcome by working with people and communities to enhance their ability to engage in the occupations they want to, need to, or are expected to do, or by modifying the occupation or the environment to better support their occupational engagement (6).
The areas of activity of these professionals include children, adolescents, adults and elderly people with certain dysfunctions caused by disease, injury or congenital impairment, which restrict or may restrict their activity and participation in everyday life. In their work, specialists use a variety of methods, techniques and tools that are aimed at restoring lost functions and adaptation to the environment. The work can be done either individually or in groups(5).
61

Occupational therapy is a multidisciplinary profession that uses knowledge from different scientific subjects, namely medicine, pedagogy, psychology, social pedagogy, social work, biomechanics and physiotherapy. Occupational therapy deals with the various activities that accompany each person throughout life (daily activities, work activities, productivity, activities during games, leisure and hobbies). The primary aim is the maximum possible restoring of human capacities for independent living, regardless of impairment, disability and/or limited participation in social life.
[Translated from (3)]
Physical medicine and rehabilitation
Not available
Physical medicine and rehabilitation, also called physiatry, is the branch of medicine emphasizing the prevention, diagnosis and treatment of disorders – particularly related to the nerves, muscles, bones and brain – that may produce temporary or permanent impairment (7).
Physical and rehabilitation medicine doctors carry out services to diagnose health conditions, assess functioning and prescribe medical and technological interventions that treat health conditions and optimize functional capacity (1).
Specialists forming this professional group seek as much as possible to develop, maintain and recover activity, mobility and functionalities of an individual or group of people.
The areas of activity of these professionals include children, adolescents, adults and elderly people with body dysfunctions caused by disease, injury or congenital diseases, which restrict or may restrict their activity and participation in every day life.
Physical therapy provides services to individuals and populations to develop, maintain and restore maximum movement and functional ability throughout the lifespan. This includes providing services in circumstances where movement and function are threatened by ageing, injury, pain, diseases, disorders, conditions or environmental factors. Functional movement is central to what it means to be healthy. Physical therapy is concerned with identifying and maximizing quality of life and movement potential within the spheres of promotion, prevention, treatment/intervention, habilitation and rehabilitation. This encompasses physical, psychological, emotional and social well-being. Physical therapy involves the interaction between the physical therapist, patients/clients, other health professionals, families, caregivers and communities in a process where movement potential is assessed and goals are agreed upon, using knowledge and skills unique to physical therapists (8).
Physiotherapy
62
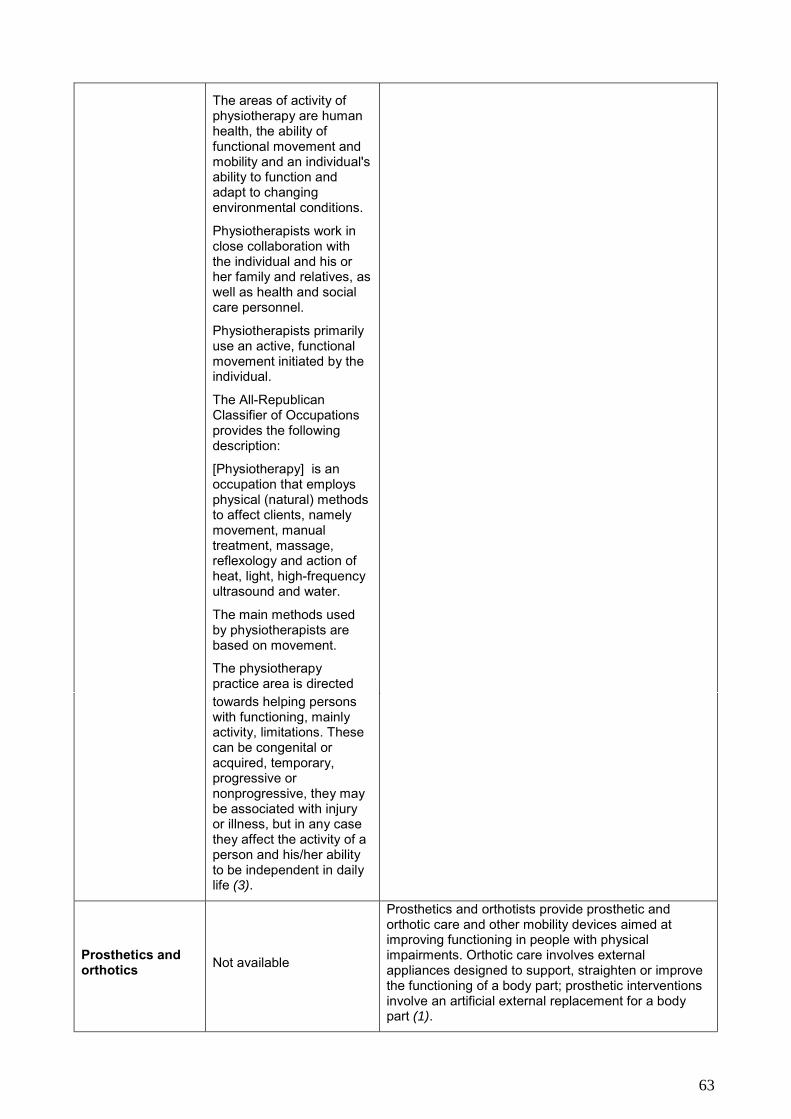
The areas of activity of physiotherapy are human health, the ability of functional movement and mobility and an individual's ability to function and adapt to changing environmental conditions.
Physiotherapists work in close collaboration with the individual and his or her family and relatives, as well as health and social care personnel.
Physiotherapists primarily use an active, functional movement initiated by the individual.
The All-Republican Classifier of Occupations provides the following description:
[Physiotherapy] is an occupation that employs physical (natural) methods to affect clients, namely movement, manual treatment, massage, reflexology and action of heat, light, high-frequency ultrasound and water.
The main methods used by physiotherapists are based on movement.
The physiotherapy practice area is directed towards helping persons with functioning, mainly activity, limitations. These can be congenital or acquired, temporary, progressive or nonprogressive, they may be associated with injury or illness, but in any case they affect the activity of a person and his/her ability to be independent in daily life (3).
Prosthetics and orthotics Not available
Prosthetics and orthotists provide prosthetic and orthotic care and other mobility devices aimed at improving functioning in people with physical impairments. Orthotic care involves external appliances designed to support, straighten or improve the functioning of a body part; prosthetic interventions involve an artificial external replacement for a body part (1).
63

Rehabilitation
Rehabilitation of people with disabilities is a system and process of full or partial restoration of a person with disabilities to consumer, social and professional activities for the purpose of their social adaptation; achievement of financial independence and integration into society (2).
[Rehabilitation is] a complex of medical, psychological, pedagogical, social, professional, juridical activities aimed at restoring or compensating for broken or lost social linkages and relations by a person as a result of changes in: health condition; social status; loss of loved ones; loss of particular professional skills; social misadaptation, etc., that is accompanied by long-term breakdown of body functions (disability), sickness, drug or/and alcohol addiction; loss of social status, job, housing, etc.
Rehabilitation [aims at the] quick and full restoration of the functions of the individual.
Almost all professional organizations refer to the description of rehabilitation in the Convention on the Rights of Persons with Disabilities:
[States Parties shall take effective and appropriate measures] to enable persons with disabilities to attain and maintain maximum independence, full physical, mental, social and vocational ability and full inclusion and participation in all aspects of life … [to] organize, strengthen and extend comprehensive habilitation and rehabilitation services and programmes, particularly in the areas of health, employment, education and social services, in such a way that these services and programmes:
a. Begin at the earliest possible stage, and are basedon the multidisciplinary assessment of individual needs and strengths;
b. Support participation and inclusion in the communityand all aspects of society, are voluntary and are available to persons with disabilities as close as possible to their own communities, including in rural areas (Art. 26, Habilitation and rehabilitation) (9).
A set of measures that assists individuals who experience, or are likely to experience, disability to achieve and maintain optimal functioning in interaction with their environments (1).
The European Board of Physical and Rehabilitation Medicine defines rehabilitation as “an independent medical speciality whose goal is to promote intellectual and physical functioning activities (including behaviour) and social participation (which includes quality of life). This can be achieved through various interventions, including modification of personal and environmental factors […] Rehabilitation includes prevention, diagnosis and treatment, as well as provision of assistive devices and mobility aids” (10).
Medical rehabilitation activities that are directed towards treating, diagnosing and restoring (particularly after trauma, heart attacks, strokes, surgeries or treatment of alcohol and drug addiction).
Psychological rehabilitation aimed at the restoration of the mental condition destroyed by traumatic events of various kinds.
64

Social rehabilitation aims at the recovery of social experience and links, behavioural norms, communication skills, emotional stability, active social life, renewal of social status.
Pedagogical rehabilitation is directed primarily towards renewal of learning skills, training, self-care and self-improvement.
Vocational rehabilitation is oriented towards recovery of professional skills and competencies that are necessary for returning to the labour market and employment (3).
Social worker Not available
The social work profession promotes social change, problem-solving in human relationships and the empowerment and liberation of people to enhance well-being. Utilizing theories of human behaviour and social systems, social work intervenes at the points where people interact with their environments (11). Professional social workers restore or enhance the capacity of individuals or groups to function well in society, and help society accommodate their needs (1).
Speech and language therapy Not available
Speech and language therapy is an allied health profession that assesses and treats speech, language and communication problems in people of all ages to help them better communicate (12). [Speech and language therapy is] aimed at restoring people’s capacity to communicate effectively and to swallow safely and efficiently (1).
References 1. World Health Organization, World Bank. World report on disability. Geneva: World
Health Organization; 2011 (http://www.who.int/disabilities/world_report/2011/en/,accessed 17 August 2014).
2. Law on Social Protection of Persons with Disabilities (No. 675 of 29 December 2010)(in Russian)(http://www.ilo.org/dyn/natlex/country_profiles.nationalLaw?p_lang=en&p_country=TJK, accessed 10 September 2014).
3. Bakhrombekov VA et al. Tajik-Russian Encyclopaedic Dictionary of Terms in SocialWork, 2nd ed. Dushanbe: LLC Contrast; 2013.
4. Disabilities. In: World Health Organization [website]. Geneva: World HealthOrganization; 2014 (http://www.who.int/topics/disabilities/en/, accessed 12 October2014).
65
5. Scientific Institute of Labour and Social Protection of the Population. All-RepublicanClassifier of Occupations, 2nd ed. Dushanbe: LLC Contrast; 2013.
6. Definition of occupational therapy. Forrestfield, Australia: World Federation ofOccupational Therapists, 2010(http://www.wfot.org/AboutUs/AboutOccupationalTherapy/DefinitionofOccupationalTherapy.aspx, accessed 12 October 2014).
7. About physical medicine and rehabilitation (PM&R). In: American Academy ofPhysical Medicine and Rehabilitation [website]. Rosemont, IL: American Academy ofPhysical Medicine and Rehabilitation; 2014(http://www.aapmr.org/patients/aboutpmr/Pages/default.aspx, accessed 12 October2014).
8. Policy statement: description of physical therapy. London: World Confederation forPhysical Therapy; 2013 (http://www.wcpt.org/policy/ps-descriptionPT, accessed 12October 2014).
9. United Nations General Assembly resolution A/RES/61/106 on a Convention on theRights of Persons with Disabilities. New York: 2007(http://www.refworld.org/docid/45f973632.html, accessed 27 August 2014).
10. UEMS-PRM-Section. Definition of physical and rehabilitation medicine (availablefrom: www.euro-prm.org, accessed 16 October 2014).
11. Definition of social work. Basel: International Federation of Social Workers; 2012(http://ifsw.org/policies/definition-of-social-work/, accessed 14 October 2014).
12. Definition of speech and language therapy. London: Royal College of Speech andLanguage Therapists; 2014 (adapted from http://www.nhscareers.nhs.uk/explore-by-career/allied-health-professions/careers-in-the-allied-health-professions/speech-and-language-therapist/, accessed 16 October 2014).
66

Annex 2. Review and analysis of existing legislation Scope and objective of the analysis The objective of the analysis of legislation and practice (where available and identified) is to provide an outline of the current situation of rehabilitation services. Legislation on rehabilitation services in Tajikistan includes three categories of legal documents: the overarching legislative framework, laws and secondary legislation in the area of rehabilitation services.
Tajikistan is party to over 60 international treaties that recognize the right to health. These include the International Covenant on Economic, Social and Cultural Rights, the International Covenant on Civil and Political Rights and its first Optional Protocol, the International Convention on the Elimination of All Forms of Racial Discrimination, the Convention on the Elimination of All Forms of Discrimination against Women, the Convention on the Rights of the Child and its first two Optional Protocols, the Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment, the International Convention on the Protection of the Rights of All Migrant Workers and Members of Their Families and the Convention on the Prohibition of the Use, Stockpiling, Production and Transfer of Anti-Personnel Mines and on their Destruction (Mine Ban Treaty). The main laws and secondary legislation which are key to the health-care and education sectors and social welfare services are listed below and their content briefly described. Legislative framework The country’s long-term development vision statement declares: “to strengthen social and political stability and to achieve the economic prosperity and social well-being of the people of Tajikistan in an environment shaped by the supremacy of the principles of a market economy, freedom, human dignity and equal opportunities for each person to realise his or her potential”. National goals and priorities are developed and implemented on the basis of this vision statement.
The National Development Strategy of the Republic of Tajikistan for the Period to 2015, as Tajikistan’s principal strategic document, defines the priorities and general thrust of Government policy, which is focused on achieving sustainable economic growth, expanding the public’s access to basic social services and reducing poverty. It comprises the following sectors: development of the health-care system; development of the education system and science; expansion of access to water supply, sanitation and housing and municipal services; improvement of social welfare; promotion of gender equality; and environmental sustainability. The National Development Strategy acknowledges that the “organization of essential support services for disabled adults, the elderly and children with disabilities ... is not in line with generally accepted standards”. The Strategy further notes that the “impact of the existing social welfare methods on reducing poverty among vulnerable segments of the population is negligible”. The Strategy specifically mentions the importance of reaching vulnerable groups, but without going into details.
67
The Constitution of the Republic of Tajikistan protects the rights of persons with disabilities, outlining their rights to medical services, education, social welfare services, housing and leisure facilities, as well as their equality in society. According to the Constitution of 1994, every individual, including people with disabilities, is treated equally and has rights to all services guaranteed by the Government.

The National Health Strategy of the Republic of Tajikistan for the Period 2010–2020 (Law No. 368, 2 August 2010) guarantees equal access to health-care facilities and management of people’s health, with maximum incorporation of individual needs and health risks. However, it does not address issues related to rehabilitation or disability. The National Programme on Preventing Trauma and Modernization of Medical Care in Case of Trauma and its Consequences in the Republic of Tajikistan for the Period 2010–2015 (Law No. 224, 3 May 2010) indicates that trauma holds a leading position in the structure of morbidity, mortality and disability, and its prevalence is increasing. The Programme also emphasizes that all patients with injuries, without exception, should undergo rehabilitation.
The National Programme on Prevention, Diagnosis and Treatment of Diabetes for the Period 2012–2017 (Law No. 310, 3 April 2012) is directed towards qualitative change in the provision of medical services, including emergency care for patients with diabetes, provision of specialized care and accessible treatment; and prevention, diagnosis and treatment of diabetic patients. It also aims to promote the overall health of the population, reduce the risk of acquiring a disability and reduce mortality rates among this population group. However, the programme does not cover the rehabilitation needs of people with diabetes. Legislative instruments – education The National Concept of Inclusive Education for Children with Disabilities for the Period 2011–2015 (Law No. 228, 30 April 2011) guarantees equal opportunities for all students (at all levels) and high-quality education irrespective of sex, social or economic status, ethnicity, race, geographical location, need for special education, age or religion. The basis for inclusive education is the right to education from early childhood until adulthood. However, the Concept does not have an action plan or monitoring and evaluation plan. Legislative instruments – social welfare The Concept of Social Protection of the Population of the Republic of Tajikistan (Law No. 783, 29 December 2006) guarantees realization of the right of citizens to work and social protection, as guaranteed by the Constitution, as well as rationalization and optimization of the terms of provision of social benefits and pensions. The Concept specifies that the basic social guarantees of the citizens should be preserved and implemented, such as the right to a state pension in case of disability, reaching retirement age, loss of breadwinner and other cases, as determined by law. The Concept document refers to labour and migration, social benefits and pensions, employment, unemployment and wage issues, and thereby limits coverage and provision of reforms overall. Social services and social care (either from the service-provider or the service-user point of view), human resource development, deinstitutionalization, improvement of service provision, etc. are not addressed. In addition, the Concept is silent on intrasectoral and intersectoral cooperation and lacks monitoring and evaluation plans.
68
Legislative instruments – health care
The Law of the Republic of Tajikistan on Social Services (Law No. 359, 5 January 2008) specifies that children and young people, pregnant women, elderly persons and disabled persons finding themselves in a difficult life situation have priority in the provision of social welfare services. It guarantees the right to these services, access to information about them, consent to or refusal of them, and confidentiality of information.

The Law of the Republic of Tajikistan on the Provision of Pensions for Citizens of the Republic of Tajikistan (Law No. 853, 3 July 2012) guarantees the right to maintenance in old age and in other cases by providing labour and social pensions. The Law guarantees the social security of pensioners by providing pensions at the minimum subsistence level. Disability pensions are assigned in the event of disability resulting in full or partial loss of functional ability due to occupational injury or disease; general illness (including injury not related to work and congenital disability); and diseases contracted during military service. Other laws and regulations relevant to persons with disabilities include: • Government Decree No. 221 of 2 July 2005 on Social Protection of Disabled
Persons, the Prevalence of Disability and Ways to Reduce;• Government Decree No. 463 of 3 October 2006 on Approving the List of Specialized
Products for Personal Use for the Disabled, the Supply and Import of Which areExempt from Value Added Tax (as amended by Decree of the Government of theRepublic of Tajikistan No. 346 of 1 July 2010).
The 2010 Law on Complaints by Citizens of the Republic of Tajikistan provides access for persons with disabilities to a formal statutory complaints mechanism to address their concerns and protect their rights.The 2009 Regulation of Social Assistance at Home Units allows staff to offer services to children with disabilities in their homes. However, the staff do not yet have the skills required to work with adults or children with disabilities. In addition, the allocation of resources to the social assistance at home units is insufficient to cover the existing needs. As a result, these units cannot reach all persons with disabilities who require assistance.
69
It also specifies the rights of persons including children and young people with disabilities) in (residential-care institutions of the social services. Although the Law refers to educational and health-care services, there is no mention of a specific mechanism for collaboration between social services and education or health-care facilities. In addition, the Law does not specify the agency responsible for overall coordination and implementation of the Law, lacks an implementation and monitoring plan and does not cite the responsible ministries. The Law of the Republic of Tajikistan on Social Protection of Persons with Disabilities (Law No. 675, 29 December 2010) is the main piece of legislation dealing with disability in Tajikistan. It specifies actions related to medical and social assessment; social benefits for persons with disabilities; aids and appliances; sanatorium and health-resort treatment for disabled persons; accessibility in the built environment; access to education (including home-based education) and vocational training; training and education in residential-care institutions; sign language; access to employment; transport-related benefits for persons with disabilities; premises, utility and ta-related ̀ benefits granted to disabled persons ̀ he ̀ aw ̀ proides ̀ a basis to enable people with disabilities to enjoy a variety of services; however, it lacks mechanis. s and procedures for realization of the rights in question. This uncertainty leads to misinterpretation and nonfulfilment of the provisions of the Law. In addition, the Law stipulates cooperation between ministries, but does not appoint a ministry with overall responsibility for coordination, implementation and monitoring of the Law and control over resources.

•
Funding of rehabilitation services is based on existing service-providing institutionsand the size of their premises and staff, instead of the needs (service users andspecific services needed) existing in a given territory, which makes the allocation offunds inefficient and limits coverage of rehabilitation services.
It is not clear which agency or ministry is responsible for coordination, decision-making, implementation of laws or monitoring and reporting mechanisms.
In the light of recent changes in Government ministries and the merger of social protection into the Ministry of Health, it is imperative to develop a national disability strategy with an action plan. The strategy should establish priorities, targets, actions and timelines for implementation, assigning responsibility to appropriate ministries or agencies and specifying the required resources. The national disability strategy should be based on the principles and ethos of the Convention on the Rights of Persons with Disabilities and major laws of Tajikistan. In addition, it is recommended that the Law of the Republic of Tajikistan on Social Protection of Persons with Disabilities (2010) should be reviewed and amended into a comprehensive law on the rights of persons with disabilities. This law should cover all relevant sectors – health, rehabilitation, social protection, education and labour – and specify mechanisms for coordination, decision-making, regular monitoring and reporting and control of resources.
•
70
Overall conclusions The review of policy documents and legislation in force with regard to rehabilitation of persons with disabilities has identified gaps, contradictions and other problems within the system in Tajikistan. While there is legislation for the social protection of persons with disabilities, there is no national disability policy or plan, and the disability sector still lacks the capacity effectively to promote inclusion and address the rights and needs of persons with disabilities. The main problems with implementation of the policy and legislative framework in the rehabilitation sector are the following.
• There is no overall national disability strategy setting out a consolidated andcomprehensive long-term vision for improving the well-being of persons withdisabilities.
• Most legislative frameworks lack implementation and monitoring plans andtimeframes.
• Secondary legislation (i.e. implementing laws) is only developed if expressly mentioned and assigned to a specific Government body; otherwise the law remains merely a declaration, as it is not supported by implementing mechanisms. There is no legal basis for individual needs assessment with the participation of persons with disabilities and no individual care plans on the basis of which the specific individual package of rehabilitation services should be provided.

71
Annex 3. Structure of the Ministry of Health and
Social Protection
Note. The dotted line box represents the departments and agency responsible for disability and rehabilitation issues at national level within the Ministry of Health and Social Protection of the Population, Republic of Tajikistan.
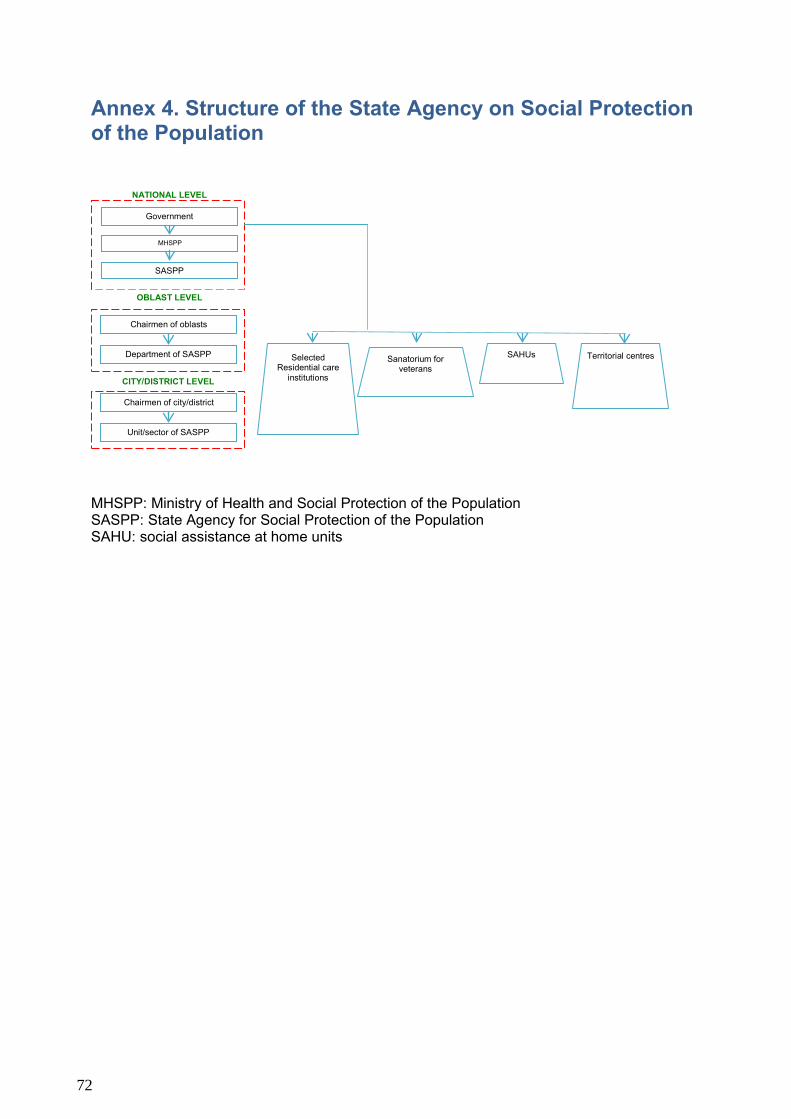
Annex 4. Structure of the State Agency on Social Protection of the Population
MHSPP: Ministry of Health and Social Protection of the Population SASPP: State Agency for Social Protection of the Population SAHU: social assistance at home units
NATIONAL LEVEL
MHSPP
SASPP
Government
OBLAST LEVEL
Chairmen of oblasts
Department of SASPP
CITY/DISTRICT LEVEL
Chairmen of city/district
Unit/sector of SASPP
Selected Residential care
institutions
SAHUs Sanatorium for veterans
Territorial centres
72

Annex 5. Rehabilitation services for adults with disabilities in Tajikistan
PMPC = psychological, medical and pedagogical consultation service. LA = local authority
Hospital (close to place of residence)
Polyclinic (close to place of residence)
Department of social protection under LA
Medical and Social Expertise Commission
(VTEK)
Decision on disability
Rehabilitation services
District hospital/ daycare centres
Provincial hospital/
specialized medical care institutions
National rehabilitation
centres/ specialized
medical-care institutions
Adult with disabilities
After five years of re-
examinations, disability
status may be granted
permanently
For groups II and III, re-
examinations every year, for group I, every
two years
73

Annex 6. Rehabilitation services for children with disabilities in Tajikistan
* One month before the child’s 18th birthday, he/she attends the adult service, theMedical and Social Expertise Commission, for examination. PMPC = psychological, medical and pedagogical consultation service. MCC = Medical Consultation Centre. LA = local authority
Health centres (district/city)
Department of social protection under LA
Rehabilitation services
District hospital/ day care centres
Decision on disability (PMPC, MCC, district/city
health centre)
Provincial hospital/
specialized medical care institutions
National rehabilitation
centres/ specialized
medical care
Child with disability
Child undergoes re-examination
approx. every two years, depending
on disability
Child with disability receives
benefits until 18 years of age
Specialized republican centres
Medical and Social Expertise Commission
(VTEK)*
74

Annex 7. Service providers included in the mapping
No. Name of organization Logo Number of
establishments Location
City District 1. Psychological,
medical andpedagogicalconsultation1
9 Dushanbe Qurgonteppa Kulob Khujand Isfara Panjikent Khorug
Bobojon Gafurov Panj
2. Rehabilitationcentre
1 (diagnostic centre) Dushanbe
1 (republican clinical centre for psychological problems)
Dushanbe
1 (republican centre for mental health of children and adolescents)
Dushanbe
1 (republican clinical hospital on mental issues)
Dushanbe
1 (republican clinical centre on eyes)
Dushanbe
1 (republican clinical cardio centre)
Dushanbe
1 (republican clinical centre on spine problems)
Dushanbe
1 (republican medical and social rehabilitation centre)
Dushanbe
1 (republican physiotherapy hospital)
Khujand
1 (republican rehabilitation centre for children)
Vahdat (Macheton)
1(national rehabilitation centre for children and adolescents)
Varzob (Chorbog)
1 Decree of Ministry of Health of the Republic of Tajikistan on establishing psychological, medical and pedagogical consultation (Ref. No. 286, 15.0.2012).
75

3. BoardingSchools1
3 (deaf and hearing-impaired children)
Bobojon Gafurov (1) Rudaki (2)
3 blind and visually impaired children
Khujand (1) Isfara (1)
Hisor (1)
1 poliomyelitis-affected children
Hisor
4 mentally impaired children
Dushanbe (2) Khujand (1) Kulob (1)
4. Baby home2 4 Khujand (1) Istaravshan (1) Dushanbe (2)
5. Residentialinstitutions(intellectuallyimpaired)3
7 Tursunzoda Panjikent Yovon
Jabbor Rasulov Hisor Vahdat Vose
6. Daycarecentres4
10 Dushanbe (1) Khujand (1) Yovon (1) Khorug (1) Qurgonteppa (1) Kulob (1)
Khuroson (1) Jomi (1) Hisor (1) Vose (1)
7. NationalOrthopaedicCentre
3 Dushanbe (1) Khujand (1) Kulob (1)
8. NationalResearchInstitute forRehabilitationof PersonswithDisabilities
1 Dushanbe
1 Statistical book in education sector of the Republic of Tajikistan for 2010-2011 academic year. Dushanbe: Ministry of Education; 2011. 2http://mapping.sdc-eu.info/5031.htm, Oxford Policy Management, European Union project, 2011.
3 http://mapping.sdc-eu.info/5051.htm, Oxford Policy Management, European Union project, 2011. 4 State Agency on Social Protection, Employment and Migration, 2013.
76


MINISTRY OF HEALTH AND SOCIALPROTECTION OF THE POPULATION
REPUBLIC OF TAJIKISTAN
Disability and Rehabilitation Programme
Breaking Barriers to Include All
World Health OrganizationRegional Office for Europe
UN City, Marmorvej 51, DK-2100 Copenhagen Ø, DenmarkTel.: +45 45 33 70 00 Fax: +45 45 33 70 01 Email: [email protected]
Website: www.euro.who.int
Related Documents