Martin B. Leon , MD Columbia University Medical Center Cardiovascular Research Foundation New York City Monday, October 31, 2016 9 mins

M.Leon, establishing the new standard_definitve treatment for bifurcation lesions_closing remarks
Jan 21, 2017
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Martin B. Leon, MD Columbia University Medical CenterCardiovascular Research Foundation
New York City
Monday, October 31, 2016
9 mins
Disclosure Statement of Financial InterestTCT 2016 Washington, DC; Oct 29 – Nov 2, 2016
Martin B. Leon, MD
Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below.
• Grant / Research Support Abbott, Boston Scientific, Edwards Lifescience, Medtronic, St. Jude Medical
• Consulting Fees / Honoraria Abbott, Boston Scientific
• Shareholder / Equity Claret, Cathworks, Elixir, GDS, Medinol,Mitralign, Valve Medical
Affiliation / Financial Relationship Company

Bifurcation Lesions are Still a Challenge!
• Require more time, anxiety, skill, and equipment (cost)
• Increased complicationsperi-‐procedural MIs,stent thrombosis, andrestenosis
• Suboptimal angiographic outcomes (esp. side branch ostium)

Tryton Concept: Treat Bifurcation Lesions with Ease, Confidence &
Consistent Efficacy
≈ 20% of PCIs Involve a Bifurcation Lesion
Bifurcation Lesions are Still a Challenge!

TCT 2005: Stent Technology InnovationUnfulfilled Promises?
Tryton:The SoleSurvivor!
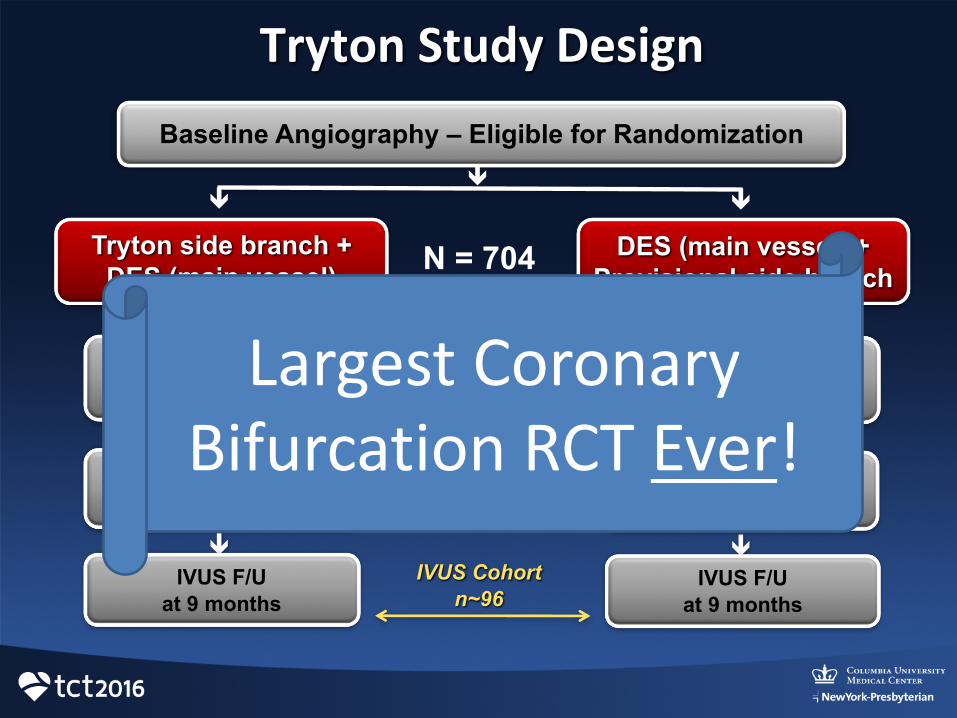
Tryton Study Design
DES (main vessel) + Provisional side branch
Baseline Angiography – Eligible for Randomization
Angiographic F/Uat 9 months
Clinical F/U at 9 months
ê
ê
ê
ê
ê
% DS side branchn~374
Tryton side branch + DES (main vessel)
êê
TVFPrimary Endpoint
ê
N = 704
IVUS F/Uat 9 months
ê
IVUS Cohort n~96
Clinical F/U at 9 months
Angiographic F/Uat 9 months
IVUS F/Uat 9 months
Largest Coronary Bifurcation RCT Ever!

Tryton Pivotal RCT
Genereux P. J Am Coll Cardiol 2015; 65:533-‐43Genereux P. Cath Cardiovasc Interv 2015; epub

%
15.6
0
12.1
4.3
11.3
0
9.2
3.50
2
4
6
8
10
12
14
16
18
TVF Cardiac Death Target Vessel MI Clinically Driven TVR
P= 0.383
P = 0.563
P =0.769
ProvisionalTryton
Target Vessel Failure (TVF)Side Branch ≥ 2.25 mm
Provisional N=143 Tryton N=146
TVF Diff (95% CI) = -4.3%(-12.9,4.4%)
Non Hierarchical
(22/141) (16/141) (17/141) (13/141) (6/139) (5/141)

40.6
32.130.4
22.2
0
5
10
15
20
25
30
35
40
45
SB % Diameter Stenosis SB Binary Restenosis
ProvisionalTryton
P = 0.004
P = 0.260
Provisional N=81, Tryton =64
%
Angiographic Outcomes (QCA)Side Branch ≥ 2.25 mm 9 Months
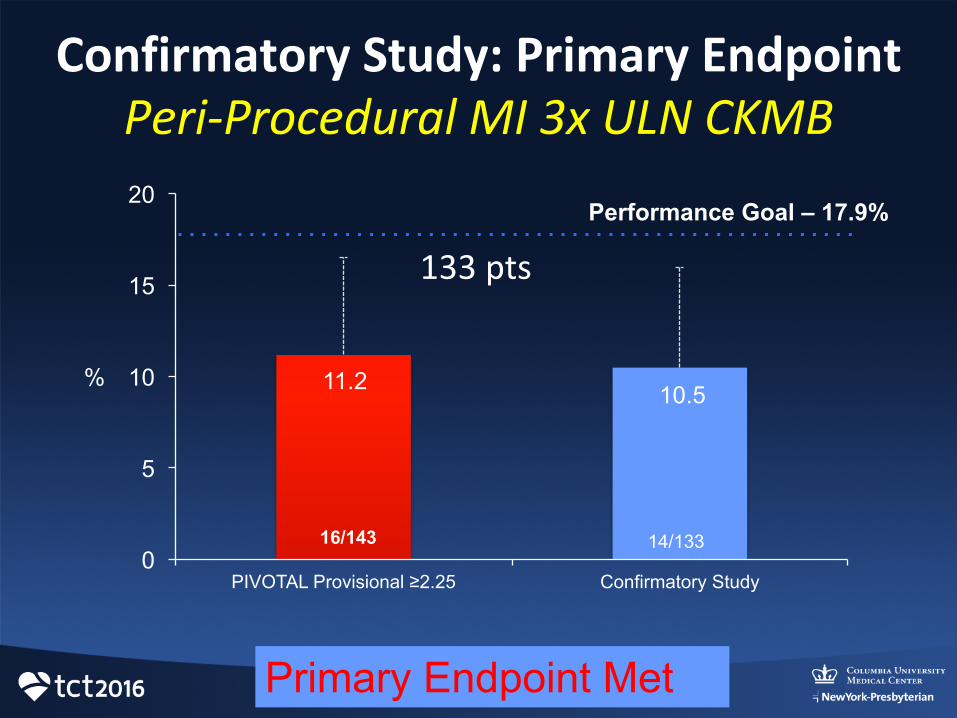
Confirmatory Study: Primary Endpoint Peri-‐Procedural MI 3x ULN CKMB
11.2 10.5
0
5
10
15
20
PIVOTAL Provisional ≥2.25 Confirmatory Study
16/143 14/133
%
Performance Goal – 17.9%
Primary Endpoint Met
133 pts

Tryton EU Experience Left Main Intervention
Baseline Final
ESC/EACTS Guidelines. CABG = PCI for low risk patients
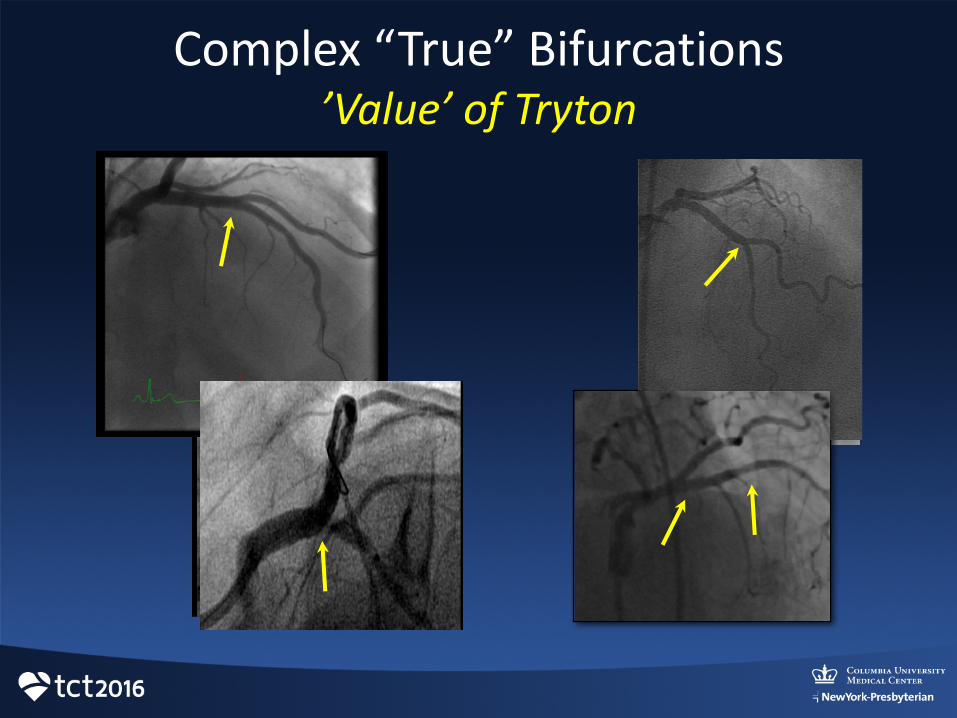
Complex “True” Bifurcations’Value’ of Tryton
Take-‐Home MessagesTryton in Bifurcations
• The TRYTON two-‐stent strategy in “true” and other complex bifurcations with large side branches, compared to a conventional provisional stent strategy…– Provides better coverage of the bifurcation (IVUS)– Reduces the need for bail-‐out stenting– Results in better acute angiographic results– Has a similar low frequency of complications (MIs and stent thrombosis)
Take Home MessagesTryton in Bifurcations
• The main advantage of the TRYTON two-‐stent strategy to the practicing interventionalist is the ability to achieve predictable (“low stress”) excellent angiographic and clinical outcomes in the most complex bifurcation lesions (esp. distal LM bifurcations)!
Take Home MessagesTryton in Bifurcations
• Stay tuned for…– Imminent FDA approval for commercial use in the U.S.
– Continued access bifurcation registry in the U.S. (75 centers)
– Announcement of marketing agreement in the U.S. for Tryton distribution
– Announcement of drug-‐eluting version of Trytonfor LM bifurcations

Cardinal Health signed a strategic agreement with Tryton Medical and is committed to a
long-‐term relationship in the U.S.
&
U.S. Strategic Alliance
Related Documents










![Nonlinear bifurcation analysis of stiffener profiles via ...especially for imperfection-sensitive shells where multiple bifurcation paths are possible [1], makes the bifurcation analysis](https://static.cupdf.com/doc/110x72/60e0b8694695dc175a47d4ad/nonlinear-bifurcation-analysis-of-stiffener-profiles-via-especially-for-imperfection-sensitive.jpg)
