REVIEW AND PERSPECTIVE Mitochondria and cancer Valdemar Máximo & Jorge Lima & Paula Soares & Manuel Sobrinho-Simões Received: 15 January 2009 / Revised: 6 March 2009 / Accepted: 17 March 2009 / Published online: 3 April 2009 # Springer-Verlag 2009 Abstract The authors review the role played by mutations in mitochondrial DNA and in nuclear genes encoding mitochondrial proteins in cancer development, with an emphasis on the alterations of the oxidative phosphorylation system and glycolysis. Keywords Mitochondria . mtDNA . Tumourigenesis . Glycolysis . OXPHOS Introduction The last decades witnessed the intensive utilisation of genetics in the understanding of the etiopathogenesis of neoplastic processes. The identification of oncogenes and tumour-suppressor genes has allowed major advances in prevention of hereditary cancers and early and precise diagnosis of numerous tumour types. Cancer genetics has also provided valuable information for prognostic and therapy selection purposes. Despite such advances, the limitations of the molecular approaches, even reinforced by high throughput technologies with all their “omics” derivatives, to disentangle the complexity of cancer development, turned progressively obvious and have been leading to other approaches. Some of these approaches are leading to an increased complexity of cancer genetics models being grouped under the umbrella descriptive terms of systems or integrative biology, whereas others are based on the rediscovery of developmental and organismal biology models of cancer. Whatever the model used as a conceptual frame for addressing carcinogenesis, it has to incorporate a number of imposing observational data: pronounced genotypic hetero- geneity of most cancers, crucial role of host cells in every neoplastic growth, key function of angiogenesis (and vasculogenesis?) in cancer development, importance of 3D modelling for understanding cancer initiation and cancer progression. The aforementioned data support the concept that cancer is an extremely complex, chimeric new growth, a sort of highly regulated, successful, invasive clone of our own tissues. To address the dynamics of such “new tissue”, it is necessary to combine genetics and epigenetics with metabolic data. One of the most interesting (and consistent) characteristics of neoplastic tissues from a metabolic standpoint is the overproduction of lactic acid as a consequence of elevated glycolysis [1, 2]. As Warburg [1] claimed, more than 50 years ago “mutation and carcino- genic agent are not alternatives, but empty words unless metabolically specified”. He also pointed out that tumour cells obtained their energy by fermentation rather than by respiration [3] and that the damage to respiration should be irreversible since the respiration of cancer cells never returned to normal [1]. Elaborating on this, Warburg advanced that “in cancer, the inhibition of respiration continues through all the following divisions. This origi- nally mysterious phenomenon has been explained…the Virchows Arch (2009) 454:481–495 DOI 10.1007/s00428-009-0766-2 V. Máximo : J. Lima : P. Soares : M. Sobrinho-Simões Department of Pathology, Medical Faculty, University of Porto, Porto, Portugal V. Máximo : J. Lima : P. Soares : M. Sobrinho-Simões (*) Institute of Molecular Pathology and Immunology of the University of Porto (IPATIMUP), Rua Dr. Roberto Frias, S/N, 4200-465 Porto, Portugal e-mail: [email protected] M. Sobrinho-Simões Department of Pathology, Hospital S. João, Porto, Portugal

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
REVIEW AND PERSPECTIVE
Mitochondria and cancer
Valdemar Máximo & Jorge Lima & Paula Soares &
Manuel Sobrinho-Simões
Received: 15 January 2009 /Revised: 6 March 2009 /Accepted: 17 March 2009 /Published online: 3 April 2009# Springer-Verlag 2009
Abstract The authors review the role played by mutationsin mitochondrial DNA and in nuclear genes encodingmitochondrial proteins in cancer development, with anemphasis on the alterations of the oxidative phosphorylationsystem and glycolysis.
Keywords Mitochondria . mtDNA . Tumourigenesis .
Glycolysis . OXPHOS
Introduction
The last decades witnessed the intensive utilisation ofgenetics in the understanding of the etiopathogenesis ofneoplastic processes. The identification of oncogenes andtumour-suppressor genes has allowed major advances inprevention of hereditary cancers and early and precisediagnosis of numerous tumour types. Cancer genetics hasalso provided valuable information for prognostic andtherapy selection purposes.
Despite such advances, the limitations of the molecularapproaches, even reinforced by high throughput technologies
with all their “omics” derivatives, to disentangle thecomplexity of cancer development, turned progressivelyobvious and have been leading to other approaches. Someof these approaches are leading to an increased complexityof cancer genetics models being grouped under the umbrelladescriptive terms of systems or integrative biology, whereasothers are based on the rediscovery of developmental andorganismal biology models of cancer.
Whatever the model used as a conceptual frame foraddressing carcinogenesis, it has to incorporate a number ofimposing observational data: pronounced genotypic hetero-geneity of most cancers, crucial role of host cells in everyneoplastic growth, key function of angiogenesis (andvasculogenesis?) in cancer development, importance of 3Dmodelling for understanding cancer initiation and cancerprogression.
The aforementioned data support the concept that cancer isan extremely complex, chimeric new growth, a sort of highlyregulated, successful, invasive clone of our own tissues.
To address the dynamics of such “new tissue”, it isnecessary to combine genetics and epigenetics withmetabolic data. One of the most interesting (and consistent)characteristics of neoplastic tissues from a metabolicstandpoint is the overproduction of lactic acid as aconsequence of elevated glycolysis [1, 2]. As Warburg [1]claimed, more than 50 years ago “mutation and carcino-genic agent are not alternatives, but empty words unlessmetabolically specified”. He also pointed out that tumourcells obtained their energy by fermentation rather than byrespiration [3] and that the damage to respiration should beirreversible since the respiration of cancer cells neverreturned to normal [1]. Elaborating on this, Warburgadvanced that “in cancer, the inhibition of respirationcontinues through all the following divisions. This origi-nally mysterious phenomenon has been explained…the
Virchows Arch (2009) 454:481–495DOI 10.1007/s00428-009-0766-2
V. Máximo : J. Lima : P. Soares :M. Sobrinho-SimõesDepartment of Pathology, Medical Faculty, University of Porto,Porto, Portugal
V. Máximo : J. Lima : P. Soares :M. Sobrinho-Simões (*)Institute of Molecular Pathology and Immunology of theUniversity of Porto (IPATIMUP),Rua Dr. Roberto Frias, S/N,4200-465 Porto, Portugale-mail: [email protected]
M. Sobrinho-SimõesDepartment of Pathology, Hospital S. João,Porto, Portugal

respiratory grana are autonomous organisms… The respi-ration connected with the grana remains damaged; when ithas once been damaged, it is for the same reason thatproperties linked with genes remain damaged when geneshave been damaged” [1]. The grana are today’s mitochon-dria and Warburg’s insights, in 1956, are almost unbeliev-able taking into consideration the date of the double helixdiscovery by Watson and Crick.
A last point to refer that Warburg also anticipated that “theinjury to respiration must not be so great that the cells arekilled for then no cancer cells could result” [1]. It took almost50 years to demonstrate that germline mutations in subunitsB, C and D of succinate dehydrogenase account for the vastmajority of hereditary paragangliomas [4–6], whereas muta-tions in SDHA, the flavoprotein subunit that forms thecatalytic core of complex II of mitochondrial respiratorychain, leads to Leigh syndrome, a neurodegenerativecondition [7]. These findings support Warburg’s educatedguess and show that mitochondrial alterations may beinvolved in the two extremes of the disease spectrum:degenerative conditions caused by cell death and neoplasticconditions apparently caused by a blockage of cell death.
In the present review, we will try to highlight the linksbetween mitochondrial alterations and carcinogenesis usingthe available epidemiological and experimental data. Forthe sake of simplicity, the review will be divided into thefollowing sections:
(a) “Mitochondrial DNA (mtDNA) mutations and humantumours”
(b) “Mutations in nuclear genes encoding mitochondrialproteins and human tumours”
(c) “In vitro models (cybrids) and animal models”(d) “Mitochondrion-rich and oncocytic (Hürthle cell)
tumours”(e) “Genetic and biochemical alterations in oncocytic
tumours”(f) “Therapeutic hints”(g) “Summary and conclusions”
Mitochondrial DNA mutations and human tumours
Although the vast majority of human genes are located inthe nucleus and are inherited equally from both parents,there is one vital set of genes that resides in the cytoplasmand is inherited exclusively from the mother—the mito-chondrial DNA (mtDNA). mtDNA is located within themitochondria, which are double-membrane organelles, oncefree-living bacteria and are responsible for producing mostof the cellular ATP (adenosine-5′-triphosphate) via theoxidative phosphorylation (OXPHOS) in an oxygen-
dependent process [8, 9]. In the human species, there are37 genes which are encoded by the mtDNA: two ribosomalRNAs, 22 transfer RNAs, and 13 genes—ND1, ND2, ND3,ND4, ND4L, ND5, ND6, CytB, COI, COII, COIII, ATPase6and ATPase8—that encode proteins of the OXPHOSsystem (Fig. 1) [8, 9].
In addition to OXPHOS, cells can also produce ATPthrough glycolysis, which takes place in the cytosol anddoes not require O2. OXPHOS is more efficient ingenerating ATP than glycolysis; therefore, this is thepreferred cellular process, provided there is enough O2
available. Whenever there is a decrease in O2 levels, thereis a shift from OXPHOS to glycolysis and the ATP isgenerated mainly through glycolysis (Pasteur effect).
In the first half of the twentieth century, Otto Warburg[1, 2] made an outstanding discovery: Cancer cells prefer tometabolise glucose by glycolysis, not using OXPHOS,even in the presence of O2 (Warburg effect or aerobicglycolysis). He further hypothesised that this phenomenonwas attributable to irreversible damages in cancer cellsOXPHOS [1]. The Warburg effect has since been demon-strated in different types of tumours and the concomitantincrease in glucose uptake has been exploited clinically forthe detection of tumours by fluorodeoxyglucose positronemission tomography [10]. Although aerobic glycolysis hasnow been generally accepted as a metabolic hallmark ofcancer, its cause and its causal relationship with cancerprogression are still unclear.
This metabolic shift may be due to defects in OXPHOSthat force cancer cells towards glycolysis. Genetic evidencefor OXPHOS defects has been provided, during the past10 years, with the identification of mutations in mtDNA-encoded OXPHOS genes in most types of human cancers[11–32].
Although most of the studies on record report homo-plasmic mtDNA mutations in cancer cells, there is evidencethat mtDNA mutations do not need to reach homoplasmy inorder to influence tumour cell growth [19, 33]. Thedynamics of this process, i.e. the putative existence of atrend towards homoplasmy in most neoplastic settings [34],remains to be fully clarified.
The first comprehensive study on mtDNA alterations intumours was made by Polyak et al. in 1998 [16], whoscreened the entire mtDNA genome and detected mutationsin seven out of ten colon cancer cell lines, which were alsopresent in the corresponding primary tumours. Variousstudies followed the report of Polyak et al. [16] and itbecame clear that mtDNA mutations were frequent eventsin carcinomas of the breast, stomach, liver, prostate, kidney,bladder, head and neck and lung [35, 36].
The mtDNA is a hotspot for mutations because themutation rate of mtDNA is ten to 20 times higher than that of
482 Virchows Arch (2009) 454:481–495

nuclear DNA for a number of reasons: The mtDNApolymerase γ replicates mtDNA with poor fidelity; there isa high concentration of reactive oxygen species (ROS) in themitochondrial inner membrane (close to the mtDNAmolecule); there are no efficient mtDNA repair mechanismsand there are no mtDNA-coating proteins like the histones inthe nucleus [9]. The mutations seem to be present throughoutthe mtDNA molecule, even though the D-loop—a regulatorynon-coding region where transcription factors encoded bythe nuclear DNA bind to mtDNA—is where mutations aremore frequent. The carcinogenic significance of D-loopalterations is unknown and, although D-loop alterationscorrelate, in some studies, with clinical parameters [37], itremains to be confirmed their role in tumourigenesis.
Mutations in the 13 protein-encoding mtDNA genesmay, in turn, have a direct effect on the protein function,hence in the OXPHOS system. There appears not to exist aparticularly affected gene, even though the seven complex Igenes seem to accumulate more mutations. This is the casefor thyroid tumours, which are amongst the best studied interms of mtDNA mutations. Yeh et al. in 2000 [18] andMaximo et al. in 2002 [21] described somatic mutations in23% and 51.5% of thyroid tumours, respectively. In thestudy by Maximo et al. [21], a significant associationbetween mutations in complex I genes and malignancy wasobserved. Furthermore, Yeh et al. [18] found, in compar-ison with a control population, a significant association
between germline polymorphisms in complex I genes andthe occurrence of thyroid tumours, whereas Maximo et al.[21] observed that germline polymorphisms in complexes Iand IV were associated with the development of malignantthyroid tumours [18, 21].
The importance of complex I and its dysfunction inthyroid tumourigenesis advanced by Yeh et al. [18] andMaximo et al. [21] has been supported by more recentstudies. Abu-Amero et al. [22] identified seven somaticmutations in 19 thyroid tumours samples (36.8%), most ofthem being located in complex I genes, and four mutationsin four thyroid tumour-derived cell lines, all in complex Igenes. The authors also observed that in two thyroid cancercell lines, there was a severe defect in complex I activity[22], possibly due to the mutations in complex I genes.Another thyroid cancer cell line—the XTC.UC1, derivedfrom a Hürthle cell thyroid carcinoma—was found toharbour a frameshift mutation in ND1 gene (complex I)and a missense mutation in CytB gene (complex III) [23].These alterations were associated with a marked reductionin the enzymatic activity of complexes I and III inconjunction with a enhanced production of ROS [23].
The functional tumourigenic role played, in vivo, bymtDNA mutations has been demonstrated in 2005, usingprostate and cervical cancer models, by two groups [38,39]. The results obtained by Shidara et al. [39] support theconclusion that the cancer-promoting effect of mtDNA
Fig. 1 Schematic representationof the OXPHOS system and theKrebs cycle in the mitochondria.We have highlighted the genes/proteins addressed in the presentreview. MtDNA-encodedOXPHOS proteins are depictedin orange and nuclear-encodedmitochondrial proteins aredepicted in green
Virchows Arch (2009) 454:481–495 483

pathogenic mutations is achieved through blockage ofapoptosis, whereas Petros et al. [38] point to the influenceof mtDNA mutations in ROS overproduction, which, inturn, would stimulate cell proliferation.
It has also been shown that mitochondrial respirationdefects in cancer cells cause activation of the AKT survivalpathway through a redox-mediated mechanism [40].
Reviewing the evidence on record, Gottlieb and Tomlinson[41], advanced that mitochondrial dysfunction may lead tocarcinogenesis through several mechanisms: decrease inapoptosis, increase in the production of ROS and activationof a hypoxia-like pathway (pseudo-hypoxia; see below).
Mutations in nuclear genes encoding mitochondrialproteins and human tumours
Whilst the aforementioned studies focussed on mtDNAalterations, others have reported that nuclear-encoded mito-chondrial proteins of the OXPHOS system and Krebs cyclemight also be involved in mitochondrial dysfunction andtumourigenesis.
The most compelling evidence showing that defects innuclear-encoded mitochondrial proteins are involved intumourigenesis came out in 2000 when Baysal et al. [4]demonstrated that germline loss-of-function mutations inSDHD, a gene that encodes the homonym subunit of themitochondrial enzyme succinate dehydrogenase (SDH—also known as complex II of the OXPHOS) cause familialparagangliomas (PGL). Besides its role in the OXPHOS,SDH is also involved in the Krebs cycle (Fig. 1).Immediately after the publication of Baysal et al. [4], otherstudies showed that also SDHB and SDHC, which encodetwo other subunits of SDH, are mutated in familial PGLand phaeochromocytomas [5, 6]. Furthermore, SDH alter-ations may be involved in other types of tumours. Lima etal. [42] studied a case of familial C-cell hyperplasia[thought to be a pre-malignant lesion of medullary thyroidcarcinoma (MTC)] where the affected individuals presenteda germline alteration in SDHD. Subsequent studies foundthat individuals with MTC presented more frequentlySDHB or SDHD polymorphisms than a control population[43] and that MTC patients harbouring germline SDHDpolymorphisms had lower mean age at diagnosis than MTCpatients without germline SDHD polymorphisms [44].These results suggest that SDH alterations may act asmodulators of MTC tumourigenesis.
In a recent paper, Ricketts et al. [45] investigatedwhether germline mutations in SDHB, SDHC or SDHDwere associated with renal cell carcinoma (RCC) suscepti-bility in 68 patients with no clinical evidence of a RCCsusceptibility syndrome. No mutations in SDHC or SDHDwere identified, but three of the 68 (4.4%) probands had a
germline SDHB mutation. Patients with germline SDHBmutations presented with familial RCC (n=1) or bilateralRCC (n=2) without any personal or family history ofphaeochromocytoma or head and neck PGL [45]. Thisfinding suggests that SDHB may represent a susceptibilitygene for non-syndromic RCC [45]. Curiously, downregu-lation of GRIM-19, another nuclear-encoded OXPHOSgene, has been associated with RCC (see below).
SDHB, SDHC and SDHD (SDH genes) were the firstnuclear genes encoding mitochondrial proteins to be consid-ered as tumour-suppressor genes. Another nuclear-encodedmitochondrial enzyme—fumarate hydratase (FH)—was alsofound to fit into that category. Tomlinson et al. [46] reportedthat heterozygous FH mutations predispose to dominantlyinherited uterine fibroids, skin leiomyomata and type IIpapillary renal cell cancer, the so-called hereditary leiomyo-mas and renal cell carcinoma (HLRCC) syndrome. In contrastto this and partially mimicking the different outcome ofSDHA mutations, homozygous mutations of FH are associ-ated with fumarase deficiency, a degenerative condition [47].
In addition to the involvement in apparently opposeddiseases, such as cancer and degenerative disorders, SDHand FH share other important features. They are both partof the Krebs cycle, where they catalyse subsequent steps(Fig. 1) and although there is no clear overlap of thetumour spectrum associated with SDH and FH mutations(possibly with the exception of renal cell carcinoma), bothneoplastic syndromes give rise to tumours showingincreased microvessel density and activation of thehypoxia pathway [48]. It is thus possible that failure ofthe Krebs cycle in PGL and HLRCC tumours causesinappropriate signalling of a hypoxic state of the neoplas-tic cells, leading to angiogenesis and, perhaps, to clonalexpansion and tumour growth.
Maximo et al. [49] analysed a nuclear gene—GRIM-19—which encodes a mitochondrial complex I protein [50] inHürthle and non-Hürthle thyroid tumours and identifiedthree GRIM-19 missense somatic mutations in threeHürthle cell thyroid tumours, as well as a germlinemutation in a Hürthle cell papillary carcinoma arising ina thyroid with multiple Hürthle cell tumours and familialclustering [49]. No mutations were detected in any of the20 non-Hürthle cell carcinomas tested, nor in any of the 96blood donor samples. It was proposed that such mutationsmay be tumourigenic through the dual function of GRIM-19 in mitochondrial metabolism (as part of OXPHOScomplex I) and cell death (being involved in retinoic acidand interferon-β induced apoptosis) [49]. In the chapter ononcocytic tumours (below), the pathogenic meaning ofGRIM-19 mutations in thyroid oncology will be discussed.Herein, we just want to stress that the expression ofGRIM-19 is lost or severely downregulated in a number ofprimary RCC, regardless of the histotype of the tumours
484 Virchows Arch (2009) 454:481–495

[51]. We have confirmed these findings in two clear cellRCCs we have recently analysed (Portugal and Máximo,unpublished results).
The evidence obtained in the setting of tumourigenesisassociated with mutations in nuclear genes encodingOXPHOS proteins (e.g. SDH and GRIM-19) fits with theresults obtained with mtDNA mutations (see above). Itremains to be better clarified the functional role, from atumourigenic standpoint, of the mutations in Krebs cyclegenes (SDH and FH).
Conceptually, any alteration that disrupts either theOXPHOS system or the Krebs cycle will have a directeffect on the cell’s metabolism: If ATP production throughOXPHOS is no longer viable, glycolysis remains the onlyway to obtain energy. There are two consequences of thismetabolic shift that constitute important advantages totumour cells: overproduction of lactic acid and acidificationof the media with concomitant injury to “normal” cells, aswell as oxygen-independent growth and survival. Classicaloncogenes and tumour suppressor genes such as Ras, Myc,Akt and p53 can also drive metabolic changes and promoteglycolysis [52–55]. The altered metabolism of cancer cellsmay confer a selective advantage for survival and prolifer-ation in the unique tumour microenvironment, an adapta-tion in which the hypoxia-inducible factor (HIF) probablyplays a major role [52–55].
Summing up, aerobic (and anaerobic) glycolysis isconstitutively upregulated in cancer cells through bothgenetic and epigenetic changes caused by mitochondrialalterations [52, 56]. It represents an evolved solution tocommon environmental constraints (i.e. space) [56]. Upre-gulation of glycolysis leads to microenvironmental acidosisthus creating a powerful growth advantage for the acid-resistant neoplastic cells over “normal” cells (see Summaryand conclusions).
In vitro models (cybrids) and animal models
Cybrids
The means to assess the phenotypic effects of mtDNAmutations are not the standard cloning/transfection methodsused to study nuclear DNA genes because the mitochon-drial genome has its own genetic code and because it is notpossible to make stable transfections directed to mtDNA.Another major drawback is the existence of hundreds orthousands of mtDNA copies inside one cell. Instead, it ispossible to substitute the mtDNA content of one cell linewith foreign mtDNA that contains a mutation of interest,leading to the establishment of cybrid cell lines. Thesecybrid cell lines are obtained from the fusion of a recipientρ0 cell line that is devoid of mitochondrial DNA and adonor cell line (that has to be removed of the nucleus butmaintains mitochondria and mtDNA) that contains themtDNA of interest (Fig. 2). The major advantage of cybridcell lines is that they allow the distinction of the phenotypiceffects caused by mtDNA mutations from those caused bythe nuclear background of the donor cells, i.e. should themtDNA mutation confer a selective advantage in the donorcell line (independently of the nuclear background), thiseffect will be observed in the resulting cybrid cells lines.
This methodology has already been performed to studymtDNA mutations, namely those that are found in humantumours. Petros et al. [38] introduced a pathogenicATPase6 mutation (T8993G) in a prostate cancer cell lineand observed that the resulting cybrids induced theformation of tumours in nude mice that were seven timeslarger than those tumours induced by the same cell linewith wt mtDNA. Similarly, Shidara et al. [39] establishedcybrids derived from HeLa cells and mtDNA containingeither the T8993G or T9176C pathogenic ATPase6 muta-
Fig. 2 Schematic representationof the cybrid productionmethod. Starting from a cell linewithout mtDNA (but withmitochondria) and fromenucleated cells that contain themtDNA mutation of interest, itis possible to perform cell fusionresulting in a cybrid cell linethat harbours the mtDNAmutation in a varying degree ofheteroplasmy. After culturingthis cybrid cell line, it is possibleto obtain a homoplasmic wt orhomoplasmic mutant mtDNAcell line and a heteroplasmic cellline
Virchows Arch (2009) 454:481–495 485

tions and observed that mutant cybrids grew faster than thewt in culture and that the ATP6 mutations conferred anadvantage in the early stage of tumour growth when thecybrids were transplanted into nude mice. Interestingly,upon transfection of a wt nuclear version of the ATPase6gene in the mutant cybrids, these reverted the phenotype,thus reinforcing the functional effects of the mtDNAmutations [39]. Recently, the importance of mtDNAmutations in the metastatic process was disclosed byIshikawa et al. [57], who analysed two mouse tumour celllines, one highly metastatic and the other poorly metastatic,observing the results of interchanging their mtDNA; therecipient tumour cells acquired the metastatic potential ofthe transferred mtDNA, i.e. the poorly metastatic cell lineacquired metastatic potential when its mtDNAwas replacedby the mtDNA from the metastatic cell line and vice versa[57]. Additionally, the mtDNA conferring high metastaticpotential contained two ND6 mutations—G13997A and13885insC—that produced a deficiency in complex Iactivity and were associated with overproduction of ROS[57]. ROS appear to play a major role in the metastaticpotential, since pre-treatment with ROS scavengers abol-ished metastasis formation [57].
Animal models
The generation of animal models has provided some insightson the effects of OXPHOS inactivation. Piruat et al. [58]generated knockout mice for the SDHD gene and observedthat the homozygous null mice died at early embryonicstages (7.5 days post-conception) whereas heterozygousmice developed without morphological abnormalities ormajor physiological dysfunction. The authors looked indetail at the carotid body function, which is one of the mostaffected organs in PGL syndrome type 1, and detected anoveractivity of the carotid body cells due to a decrease of K+
conductance and persistent Ca2+ influx into glomus cells[58]. This overactivity was accompanied by a subtlehypertrophy and hyperplasia of the carotid body, meaningthat the inheritance of a heterozygous defect in SDHD leadsto a state of cellular “overactivation” and, therefore, to anincreased susceptibility to tumourigenesis upon subsequentgenetic alterations [58]. In this way, OXPHOS inactivationwould be an initial step in tumour development conferringtumourigenic potential to the cells. Piruat et al. [58] did notobserve the occurrence of tumours in this mouse model, butit is possible that tumours would only appear later on [58].
In addition to SDHD, the functional importance ofGRIM-19 has also been highlighted by knock-out experi-ments. Huang et al. [50] generated mice deficient in GRIM-19 by gene targeting and showed that homologous deletionof GRIM-19 causes embryonic lethality at embryonicday 9.5. Interestingly, GRIM-19−/− blastocysts display
abnormal mitochondrial structure, morphology and cellulardistribution [50].
Mitochondrion-rich and oncocytic (Hürthle cell)tumours
The accumulation of huge numbers of abnormal mitochon-dria as seen by electron microscopy and immunohisto-chemistry is the hallmark of oncocytic cells regardless ofthe organ of origin (thyroid, parathyroid, kidney, salivarygland,…) and of the benign or malignant nature of thelesions [25, 59–66]. Such accumulation may also reflect a“normal” process; for example, the parathyroid glandsnormally present a variable percentage of oncocytic cells,most probably related with cell ageing [67]. Besides therole played by increased proliferation of mitochondria inthe cytoplasm without cell division, it is not known whethera decreased turnover of the mitochondria may alsocontribute to their accumulation in oncocytic cells [21, 68].
Oncocyte is a descriptive term for a neoplastic or non-neoplastic cell stuffed with mitochondria that give agranular eosinophilic appearance to its large cytoplasm. Inmany instances, oxyphilic transformation is used as asynonym for oncocytic transformation, thus leading to theutilisation of oxyphilic tumour as a synonym for oncocytictumour or oncocytoma. In the thyroid, other terms are used:Hürthle cell transformation and Hürthle cell tumours [61,62, 69]. The question of who first described oncocytic cellsin the thyroid gland is still open, although most authorsacknowledge the 1907 Virchows Archiv article of TheodorLanghans as the first clear report of oxyphilic cells in athyroid tumour [70]. Finally, there are, in some organs,tumours composed by oncocytes that carry specific desig-nations (e.g. Warthin’s tumour of the salivary glands).
The prominence of oncocytic cells in endocrine organs,salivary glands, kidney and other parenchymatous organs (andin their respective tumours), in contrast to the rarity of oncocyticcells in the mucosa and respective tumours of the digestive andrespiratory tract, suggests that this alteration occurs in tissueswith low proliferative index and reduced turnover, i.e. in stablecells with a very long intermitotic interval.
Following this rationale, the accumulation of mitochon-dria in neoplastic lesions indicates a low proliferativeturnover and is thus associated, in most instances, to benignneoplasms or malignant tumours of low malignancy (as if thecells of the digestive and respiratory tract and of theirtumours divide too quickly or die/desquamate too soon toallow the accumulation of abnormal mitochondria) [21, 25].It takes many years before the accumulation of mitochon-dria reaches the “oncocytic” threshold (three or fourthousand mitochondria per cell) thus justifying the utilisa-tion, in some circumstances, of the term “oncocytoid”.
486 Virchows Arch (2009) 454:481–495

The great majority of oncocytic tumours are epithelial-derived tumours, but there are also on record examples ofoncocytomas occurring in non-epithelial settings. In arecent review, we have summarised the different sites,other than the thyroid, where oncocytomas have beenreported to occur in 499 papers published in English in thelast 55 years. During the same period, more than 600 paperson thyroid oncocytic tumours have been published [34].
Hürthle cells can be observed in all sorts of thyroiditis(and are prominent in Hashimoto’s thyroiditis of adult andelderly patients), nodular goitre, adenoma, follicular carci-noma, papillary carcinoma (PTC) and poorly differentiatedcarcinoma of the thyroid. Undifferentiated (anaplastic)carcinomas composed of Hürthle cells are extremely rareprobably because the neoplastic cells divide too rapidly toallow the accumulation of mitochondria. With the exceptionof undifferentiated carcinoma, every type of benign ormalignant thyroid tumour has its oncocytic counterpart.This concept has been incorporated in the third edition ofthe WHO Book on Endocrine Tumours in which the “old”Hürthle cell (oncocytic) carcinoma has been substituted bythe oncocytic variants of follicular carcinoma, PTC andpoorly differentiated carcinoma [71].
In the thyroid, Hürthle cells are not restricted to follicularcell-derived tumours. There are also some medullary carcino-mas composed of Hürthle cells that are morphologicallyindistinguishable from those derived from the follicular cells[72]. The occurrence of Hürthle cell transformation inmedullary thyroid carcinoma fits with its occurrence in otherneuroendocrine tumours throughout the body [73–75].
The presence of abundant mitochondria in the cytoplasmof the neoplastic cells may be seen throughout the entiretumour (“primary” oxyphilia, indicating that the carcino-genic hit has occurred in cells with pre-existing mitochon-drial abnormalities) or just in some parts of the tumour(“secondary” oxyphilia, indicating that the mitochondrialabnormalities have occurred after tumour development)[25].
The criteria used in the diagnosis of the oncocytic variant ofPTC and of follicular carcinoma are those used in thediagnosis of conventional tumours [76]. Although it is nowwidely accepted that most oncocytic tumours of the thyroidare benign, one should search actively for capsular andvascular invasion and for PTC nuclei, whenever dealing withany oncocytic tumour [76]. It has also been shown that thetypical molecular features of conventional PTC and follicularcarcinoma are also present in their oncocytic counterparts[77, 78]. This has been recently confirmed with regard to theBRAF V600E mutation, which is detected in about 50%cases of conventional PTC, as well as in about 50% of casesof the oncocytic variant of PTC [79]. This mutation is alsovery prevalent in Warthin’s like PTC which is characteris-tically composed by oncocytic cells [80].
The prognostic factors associated to Hürthle cell carci-nomas do not differ from those that were found to carrymeaningful information in non-Hürthle cell carcinomas[81–85]. It remains, however, controversial whether thecategory of Hürthle cell variant of follicular carcinomacarries per se a worse prognosis. Some authors claim thatthese carcinomas spread to the perithyroid soft tissues andgive rise to metastases more often than do conventionalfollicular carcinomas [85], but it remains to be seen whetheror not the higher prevalence of nodal metastases in thissetting reflects the inclusion, in the series, of cases ofHürthle cell variant of PTC erroneously classified asfollicular carcinoma. The overall mortality rate of patientswith Hürthle cell carcinoma [81] appears to be higher thanthose of patients with papillary or follicular carcinoma [86]without Hürthle cell features, as a consequence, partly atleast, of the poor responsiveness of Hürthle cells toradioiodine therapy [86, 87].
Parathyroid adenomas composed predominantly (morethan 90%) or exclusively of oxyphilic cells are uncommon.According toApel andAsa [88], they constitute 4.4% to 8.4%of all parathyroid adenomas and usually remain clinicallysilent, whereas Giorgadze et al. [89] advanced that oxyphilicparathyroid adenomas, although rare, tend to be large and areoften associated with minimal hyperparathyroidism.
Oxyphilic carcinomas of the parathyroid are frequentlyfunctional tumours, associated with high serum calcium,presenting higher Ki-67 and lower p27 than oxyphilicadenomas [90]. Oxyphilic carcinomas are associated withrecurrent disease and death in about 50% of the cases.These figures do not substantially differ from those ofpatients with chief cell carcinoma of the parathyroid [90].
Warthin’s tumour is the second most common salivarygland tumour, arising almost always in the parotid gland(accounts for about 15% of all epithelial tumours of theparotid gland), occasionally causing pain or facial nerveparalysis [91]. Warthin’s tumours are constituted by cysticspaces, lined by a double layer of oncocytic cells ofquestionable neoplastic nature that rest on a lymphoidstroma [92]. Some are multi-focal and about 10% arebilateral but malignant transformation is very rare [91].Smokers have approximately eight times higher risk fordeveloping these tumours than non-smokers [93]. Onco-cytic carcinoma of the salivary glands is a very rare high-grade carcinoma.
Renal oncocytomas, the most common benign solid renaltumour, are thought to originate from the intercalated cells ofthe renal collecting duct and account for about 3–7% of allrenal tumours [94]. About 2–12% of oncocytomas are multi-focal, and 4–14% are bilateral [95]. Almost all cases ofoncocytoma behave in a benign fashion with no recurrence,metastasis or mortality. Some atypical features, such asnuclear pleomorphism, perinephric fat involvement, focal
Virchows Arch (2009) 454:481–495 487

necrosis and even extension to branches of the renal vein, donot seem to worsen significantly the prognosis [95].
Genetic and biochemical alterations in oncocytictumours
The best studied oncocytic tumours in terms of mtDNA arethose of the thyroid. A large deletion encompassing 4,977 bpof mtDNA, known as the mtDNA common deletion (CD), isalmost always detected and was proposed as a hallmark ofoncocytic thyroid tumours [21, 25, 96, 97]. This deletionremoves seven OXPHOS genes (ATPase6, ATPase8, COIII,ND3, ND4L, ND4 and ND5) and five tRNAs (glycine,arginine, histidine, serine and leucine), thus resulting insevere impairment of the OXPHOS system.
The mtDNA CD was found in every thyroid tumour withoncocytic features, irrespectively of the histological sub-types; the mtDNA CD was also present in non-oncocyticthyroid tumours, but with significantly lower frequency andrelative lower amount [21].
Traditionally, the association between mtDNA CD andoncocytic phenotype has been explained through a positivefeedbackmechanism: The severe impairment of the OXPHOSsystem (as a consequence of the mtDNA CD) would engageand activate nuclear genes that control mitochondrial number,resulting in an increase in the mitochondrial mass [98, 99].
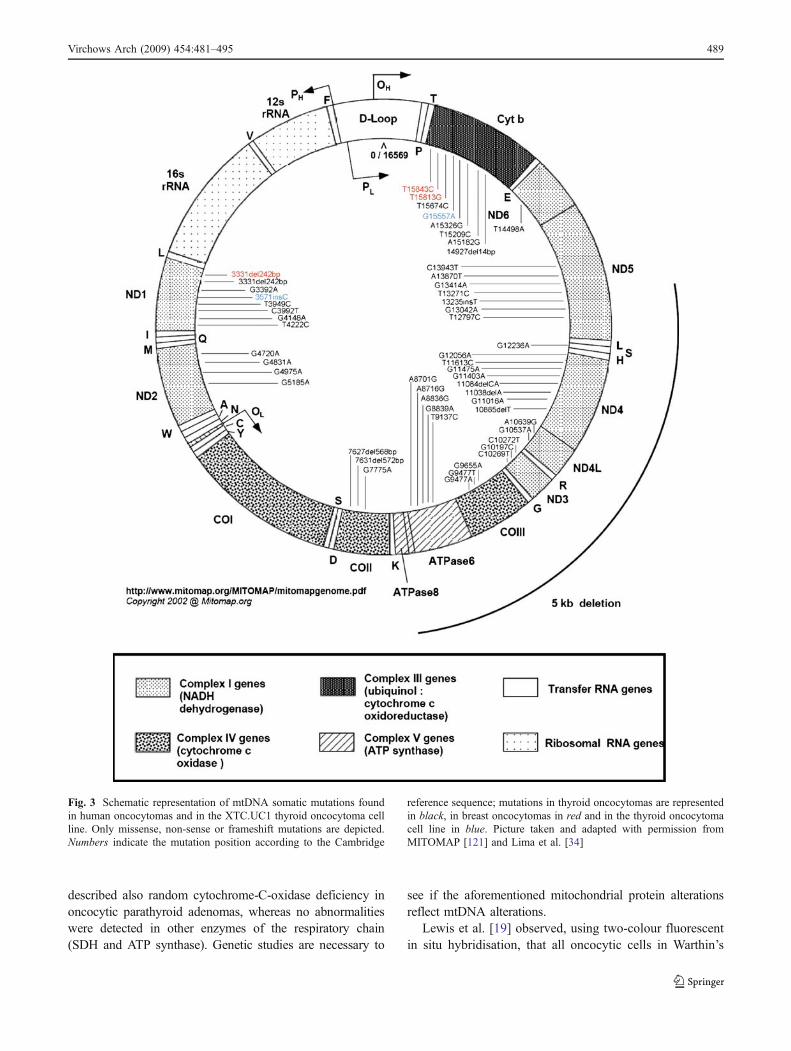
The analysis of the prevalence of mtDNA mutations hasshown that missense somatic mutations in complex I genes(without any apparent concentration in a single gene) weremore frequently detected in malignant tumours than inadenomas [21]. A significant association was also observedbetween D-loop somatic mutations and the occurrence ofsomatic mutations in other mtDNA genes [21]. We havesummarised in Fig. 3 all but silent mtDNA somaticmutations reported to date in oncocytic tumours. A largenumber (n=253) of mtDNA variants (alterations present bothin tumour and adjacent thyroid tissue) were disclosed in alltumour types. The variants affecting genes of complex I andIV were significantly more frequent in patients withmalignant tumours than in patients with benign tumours,whereas those affecting complex V genes—almost all inATPase6 (34/37) and most of them missense (27/34)—wereassociated with the presence of oncocytic features in thetumours of the patients [21]. For a thorough review onmitochondria and oncocytic tumours, see Lima et al. [34].
Gasparre et al. [29] analysed breast and thyroidoncocytic tumours and found that 26 of the 45 (57.8%)oncocytic thyroid samples harboured 30 somatic mtDNAmutations, 25 of which were located in complex I genes; in12 of the 45 cases (26.7%), the mutations were consideredas disruptive (either frameshift or non-sense), and they wereall located in complex I genes [29]. The association of
disruptive complex I mutations with the Hürthle cellphenotype was strengthened by the finding that the onlybreast tumour that presented a disruptive somatic mtDNAmutation (also located in a complex I gene) was amitochondrion-rich tumour [29].
To address the correlation between mtDNA mutationsand oncocytic phenotype, Gasparre et al. [29] establishedprimary cultures from two thyroid tumours, each with adisruptive mtDNA mutation. Intriguingly, none of theprimary cultures showed evidence of the disruptive mtDNAmutations found in the original biopsies and, moreover, theoncocytic phenotype was lost during culture [29]. It wassuggested that mtDNA mutations are negatively selectedunder the culture conditions [29], thus reinforcing theassumption that, in vivo, hypoxic conditions play a majorrole in the positive selection of the mtDNA mutations andthe oncocytic phenotype.
Few publications have analysed mtDNA alterations inrenal oncocytomas. Welter et al. [100] used restrictionendonucleases to search for mtDNA abnormalities in sixrenal oncocytomas and observed that every tumour dis-played an extra band, which was not noted in thecorresponding normal tissue; these findings were notreproduced by Brooks et al. [101], who did not observeany mtDNA alterations in five renal oncocytomas. Talliniet al. [20] did not find alterations in COXI and D-loopregion in ten renal oncocytomas. In addition, these authorsalso analysed the presence of the mtDNA CD, but failed todetect an increased frequency in comparison to controls[20]. Recently, we observed the mtDNA CD in 11 of 14renal oncocytomas (79%) and in seven of the 14 cases(50%) in the respective adjacent normal parenchyma(Portugal et al., unpublished observation).
Simonnet et al. [102] observed that renal oncocytomasdisplayed a normal or slightly elevated activity of complexesII–V of the OXPHOS system, whereas complex I was notdetectable in two-dimension electrophoresis; in addition,renal oncocytomas also showed a fivefold increase in citratesynthase (an indicator of mitochondrial proliferation) [102].The absence of complex I, together with an increase in theremaining complexes and citrate synthase, led to theconclusion that the mitochondrial proliferation in renaloncocytomas might be a compensatory mechanism for adecreased OXPHOS activity [102, 103]. Mayr et al. [104]confirmed the observations of Simonnet et al. [103], showingthat the enzymatic activity of complex I was undetectable orgreatly reduced in the tumour samples as well as lack ofassembled complex I. Furthermore, mtDNA mutation anal-ysis showed frameshift mutations either in ND1, ND4 orND5 in nine of 15 tumours [104].
Muller-Hocker et al. [67] showed that defects of therespiratory chain are present during cell ageing in theoncocytic cells of normal parathyroids. Muller-Hocker [59]
488 Virchows Arch (2009) 454:481–495
described also random cytochrome-C-oxidase deficiency inoncocytic parathyroid adenomas, whereas no abnormalitieswere detected in other enzymes of the respiratory chain(SDH and ATP synthase). Genetic studies are necessary to
see if the aforementioned mitochondrial protein alterationsreflect mtDNA alterations.
Lewis et al. [19] observed, using two-colour fluorescentin situ hybridisation, that all oncocytic cells in Warthin’s
Fig. 3 Schematic representation of mtDNA somatic mutations foundin human oncocytomas and in the XTC.UC1 thyroid oncocytoma cellline. Only missense, non-sense or frameshift mutations are depicted.Numbers indicate the mutation position according to the Cambridge
reference sequence; mutations in thyroid oncocytomas are representedin black, in breast oncocytomas in red and in the thyroid oncocytomacell line in blue. Picture taken and adapted with permission fromMITOMAP [121] and Lima et al. [34]
Virchows Arch (2009) 454:481–495 489

tumours contained mitochondria showing a reduction onnormal mtDNA signal and that oncocytic cells had mixedpopulations of normal and deleted mtDNA (heteroplasmy),but no cells had exclusively deleted mtDNA. Lewis et al.[19] also found the presence of a low level of mtDNAdeletions in normal parotid epithelial cells of smokerpatients, a finding that supports the assumption that thesedeletions may precede the oncocytic phenotype.
Biochemical analyses of oncocytic thyroid tumoursrevealed that the ATP synthesis in the tumour cells isimpaired, suggesting an inactivation of the OXPHOSsystem [28, 105]. Savagner et al. [28] studied seven freshoncocytic thyroid tumours and respective controls, havingfound that the ATP synthesis was lower in all the tumours,with a parallel overexpression of uncoupling protein 2,which is a protein that uncouples the electron flow in theOXPHOS system from the ATP production in complex V.Savagner et al. [28] also found that two mitochondrialgenes—ND2 and ND5—were overexpressed in relation tonormal thyroid tissue. Confirming these observations, twoother studies, using microarrays, have found that themajority of the peptide-encoding mtDNA genes wereoverexpressed in thyroid oncocytic tumours [106, 107].These results suggest that the defective ATP productionobserved in this setting may explain the characteristicmitochondrial proliferation of oncocytic cells.
Using differential display, it was disclosed, amongstother alterations, an overexpression of the gene encodingthe core I subunit of the complex III of the mitochondrialOXPHOS system in a follicular carcinoma composed ofHürthle cells [108]. However, in a large series of thyroidtumours, core I overexpression was found to be associatedwith benign and malignant tumours of the thyroid withmicrofollicular growth pattern, independently of the pres-ence of Hürthle cells [108].
A last point to refer is that the association betweenGRIM-19 mutations and Hürthle cell phenotype [49] hasnot been confirmed in renal oncocytomas, nor in Warthin’stumour of the salivary glands (Portugal, Guimarães et al.,unpublished results). In the thyroid, familial forms ofbenign and malignant Hürthle cell tumours may be due toa germline mutation in GRIM-19 (see above) [49].Downregulation of GRIM-19 has been shown to confer agrowth advantage on cells and to reduce the likelihoodthat they will enter apoptosis [51]. The detection of aRET/PTC1 re-arrangement in one case of the oncocyticvariant of PTC in which there was also a GRIM-19mutation [49] suggests that the latter mutation may serveas a predisposing alteration for the occurrence of tumourswith cell oxyphilia; other alterations such as RET/PTCrearrangement or BRAF mutation may be necessary for theacquisition of the malignant phenotype (for a thoroughreview, see [109]).
Therapeutic hints
Although the cause of the metabolic shift towards glycolysisof cancer tissues remains to be fully clarified, the glycolyticphenotype is such a common end product of diversemolecular abnormalities that the Warburg effect may turninto the Achilles’ heel of cancer cells from a therapeuticstandpoint [52, 56, 110, 111]. Since early carcinogenesis isthought to occur in a hypoxic microenvironment, Gatenbyand Gillies [56] proposed that the transformed cells initiallyhave to rely on glycolysis for energy production. Asdiscussed above, this early metabolic adaptation appears tooffer a proliferative advantage, suppressing apoptosis.Furthermore, the “byproducts” of glycolysis (i.e. lactate andacidosis) contribute to the breakdown of the extracellularmatrix, facilitate cell mobility and increase the metastaticpotential [56, 112]. In a recent study, Bonnet et al. [113]compared several cancer cell lines with normal cell lines andfound that cancer cells had more hyper-polarised mitochon-dria, having hypothesised that if this metabolic-electricalremodelling is an adaptive response, then its reversal mightincrease apoptosis and inhibit cancer growth [113]. Bonnetet al. [113] used dichloroacetate (DCA), a small moleculeand a well-characterised inhibitor of pyruvate dehydrogenasekinase (PDK). Inhibition of PDK by DCA in A549 cellsshifts pyruvate metabolism from glycolysis and lactateproduction to glucose oxidation in the mitochondria. Thismetabolic shift was associated with increased production ofROS, efflux of pro-apoptotic mediators from the mitochon-dria, induction of mitochondria-dependent apoptosis anddecreased tumour growth [113].
In 2001, Ko et al. [111] showed that a small moleculenamed 3-bromopyruvate (3BrPA) was a potent inhibitor ofthe glycolytic activity in tumour cells [111]. 3-BrPA is notonly an analogue of lactic acid but also highly reactive. Dueto its structural analogy to lactic acid, it is believed that 3-BrPA may take advantage of the Warburg effect byselectively entering cancer cells via the enhanced numberof lactic acid transporters that are present in such cells and,once inside, using its alkylating properties to block energyproduction. Ko et al. [111] showed that 3BrPA had little orno effect on normal hepatocytes used as control population,but destroyed almost all the hepatoma cells; it has beenshown, moreover, that 3-BrPAworks also in vivo [111, 112].
Summary and conclusions
Mitochondria are key organelles in cellular homeostasistaking part in vital processes, such as ATP production via theOXPHOS system, and programmed cell death (apoptosis)via cytochrome C release from the mitochondrial inter-membrane space. In 1956, Otto Warburg [114] showed that
490 Virchows Arch (2009) 454:481–495
human tumours displayed elevated glycolysis and reducedrate of OXPHOS, even in the presence of oxygen andsuggested that defects in OXPHOS could underlie manyforms of cancer. In the last decade, the finding of mtDNAmutations, as well as of mutations in nuclear genes encodingmitochondrial proteins in many types of sporadic andfamilial human tumours with and without oncocytic (Hürthlecell) features, has provided a genetic basis for the mitochon-drial dysfunction observed in human tumourigenesis.
The mechanisms by which mtDNA and nuclear DNAmutations and the resulting defective mitochondrial proteinsinvolved in OXPHOS and/or Krebs cycle can lead to orpromote tumourigenesis are not fully understood. It has beenadvanced that the outcome of such mechanisms would beenhanced glycolysis, with a concomitant survival advantagein hypoxic and acidic microenvironments, as well as an escapefrom the excessive ROS formation (which may lead toapoptosis) of a malfunctioning OXPHOS.
There is epidemiological and experimental evidenceshowing that some pathogenic mtDNA mutations, as wellas mutations in a few mitochondrial coding nuclear genes(GRIM-19, SDH, FH), create a favourable environment fortumour development by conferring growth advantage tocells. However, extra-hits, such as LOH and mutations inother oncogenes and/or tumour-suppressor genes, appear tobe required for tumour progression, including malignanttransformation.
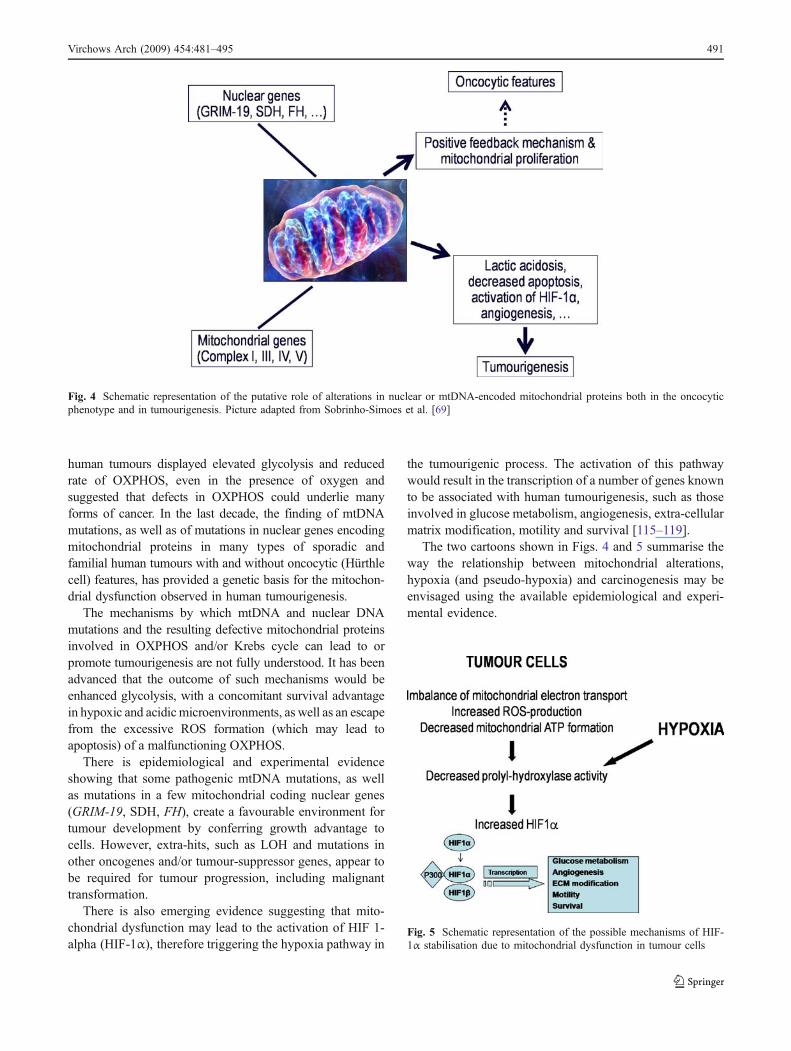
There is also emerging evidence suggesting that mito-chondrial dysfunction may lead to the activation of HIF 1-alpha (HIF-1α), therefore triggering the hypoxia pathway in
the tumourigenic process. The activation of this pathwaywould result in the transcription of a number of genes knownto be associated with human tumourigenesis, such as thoseinvolved in glucose metabolism, angiogenesis, extra-cellularmatrix modification, motility and survival [115–119].
The two cartoons shown in Figs. 4 and 5 summarise theway the relationship between mitochondrial alterations,hypoxia (and pseudo-hypoxia) and carcinogenesis may beenvisaged using the available epidemiological and experi-mental evidence.
Fig. 5 Schematic representation of the possible mechanisms of HIF-1α stabilisation due to mitochondrial dysfunction in tumour cells
Fig. 4 Schematic representation of the putative role of alterations in nuclear or mtDNA-encoded mitochondrial proteins both in the oncocyticphenotype and in tumourigenesis. Picture adapted from Sobrinho-Simoes et al. [69]
Virchows Arch (2009) 454:481–495 491
The role played by the increased activity of HIF-1α incancer development has been repeatedly aknowledged bothin connection with mitochondrial alterations [32, 57, 120]and in other settings [115–119]. The discussion of such rolerests beyond the scope of the present review.
Acknowledgments This work was supported by the PortugueseScience and Technology Foundation through the grant SFRH/BPD/29197/2006 (Jorge Lima) and by the Late David and Esther BernsteinHalpern Fund.
Conflict of interest statement We declare that we have no conflictof interest.
References
1. Warburg O (1956) On the origin of cancer cells. Science 123:309–314
2. Warburg O (1930) The metabolism of tumours. LondonConstable, London
3. Warburg O, Wind F, Negelein E (1927) The metabolism oftumors in the body. J Gen Physiol 8:519–530
4. Baysal BE, Ferrell RE, Willett-Brozick JE et al (2000) Mutationsin SDHD, a mitochondrial complex II gene, in hereditaryparaganglioma. Science 287:848–851
5. Astuti D, Latif F, Dallol A et al (2001) Gene mutations in thesuccinate dehydrogenase subunit SDHB cause susceptibility tofamilial pheochromocytoma and to familial paraganglioma. AmJ Hum Genet 69:49–54
6. Niemann S, Muller U (2000) Mutations in SDHC cause autosomaldominant paraganglioma, type 3. Nat Genet 26:268–270
7. Horvath R, Abicht A, Holinski-Feder E et al (2006) Leighsyndrome caused by mutations in the flavoprotein (Fp) subunitof succinate dehydrogenase (SDHA). J Neurol NeurosurgPsychiatry 77:74–76
8. Wallace DC (1999) Mitochondrial diseases in man and mouse.Science 283:1482–1488
9. Wallace DC (2005) A mitochondrial paradigm of metabolic anddegenerative diseases, aging, and cancer: a dawn for evolution-ary medicine. Annu Rev Genet 39:359–407
10. Rohren EM, Turkington TG, Coleman RE (2004) Clinicalapplications of PET in oncology. Radiology 231:305–332
11. Habano W, Sugai T, Nakamura SI et al (2000) Microsatelliteinstability and mutation of mitochondrial and nuclear DNA ingastric carcinoma. Gastroenterology 118:835–841
12. Richard SM, Bailliet G, Paez GL et al (2000) Nuclear andmitochondrial genome instability in human breast cancer. CancerRes 60:4231–4237
13. Maximo V, Soares P, Seruca R et al (2001) Microsatelliteinstability, mitochondrial DNA large deletions, and mitochon-drial DNA mutations in gastric carcinoma. Genes ChromosomesCancer 32:136–143
14. Burgart LJ, Zheng J, Shu Q et al (1995) Somatic mitochondrialmutation in gastric cancer. Am J Pathol 147:1105–1111
15. Habano W, Sugai T, Yoshida T et al (1999) Mitochondrial genemutation, but not large-scale deletion, is a feature of colorectalcarcinomas with mitochondrial microsatellite instability. Int JCancer 83:625–629
16. Polyak K, Li Y, Zhu H et al (1998) Somatic mutations of themitochondrial genome in human colorectal tumours. Nat Genet20:291–293
17. Fliss MS, Usadel H, Caballero OL et al (2000) Facile detectionof mitochondrial DNA mutations in tumors and bodily fluids.Science 287:2017–2019
18. Yeh JJ, Lunetta KL, Van Orsouw NJ et al (2000) Somaticmitochondrial DNA (mtDNA) mutations in papillary thyroidcarcinomas and differential mtDNA sequence variants in caseswith thyroid tumours. Oncogene 19:2060–2066
19. Lewis PD, Baxter P, Paul GA et al (2000) Detection of damageto the mitochondrial genome in the oncocytic cells of Warthin'stumour. J Pathol 191:274–281
20. Tallini G, Ladanyi M, Rosai J et al (1994) Analysis of nuclearand mitochondrial DNA alterations in thyroid and renaloncocytic tumors. Cytogenet Cell Genet 66:253–259
21. Maximo V, Soares P, Lima J et al (2002) Mitochondrial DNAsomatic mutations (point mutations and large deletions) andmitochondrial DNA variants in human thyroid pathology: a studywith emphasis on Hurthle cell tumors. Am J Pathol 160:1857–1865
22. Abu-Amero KK, Alzahrani AS, Zou M et al (2005) Highfrequency of somatic mitochondrial DNA mutations in humanthyroid carcinomas and complex I respiratory defect in thyroidcancer cell lines. Oncogene 24:1455–1460
23. Bonora E, Porcelli AM, Gasparre G et al (2006) Defectiveoxidative phosphorylation in thyroid oncocytic carcinoma isassociated with pathogenic mitochondrial DNA mutationsaffecting complexes I and III. Cancer Res 66:6087–6096
24. Lohrer HD, Hieber L, Zitzelsberger H (2002) Differentialmutation frequency in mitochondrial DNA from thyroidtumours. Carcinogenesis 23:1577–1582
25. Maximo V, Sobrinho-Simoes M (2000) Hurthle cell tumours ofthe thyroid. A review with emphasis on mitochondrial abnor-malities with clinical relevance. Virchows Arch 437:107–115
26. Maximo V, Lima J, Soares P et al (2005) Mitochondrial D-loopinstability in thyroid tumours is not a marker of malignancy.Mitochondrion 5:333–340
27. Rogounovitch T, Saenko V, Yamashita S (2004) MitochondrialDNA and human thyroid diseases. Endocr J 51:265–277
28. Savagner F, Franc B, Guyetant S et al (2001) Defectivemitochondrial ATP synthesis in oxyphilic thyroid tumors. J ClinEndocrinol Metab 86:4920–4925
29. Gasparre G, Porcelli AM, Bonora E et al (2007) Disruptivemitochondrial DNA mutations in complex I subunits are markersof oncocytic phenotype in thyroid tumors. Proc Natl Acad Sci US A 104:9001–9006
30. Gasparre G, Iommarini L, Porcelli AM et al (2008) An inheritedmitochondrial DNA disruptive mutation shifts to homoplasmy inoncocytic tumor cells. Hum Mutat 30:391–396
31. Jeronimo C, Nomoto S, Caballero OL et al (2001) Mitochondrialmutations in early stage prostate cancer and bodily fluids.Oncogene 20:5195–5198
32. Zhou S, Kachhap S, Sun W et al (2007) Frequency andphenotypic implications of mitochondrial DNA mutations inhuman squamous cell cancers of the head and neck. Proc NatlAcad Sci U S A 104:7540–7545
33. Park JS, Sharma LK, Li HZ et al. (2009) A heteroplasmic, nothomoplasmic, mitochondrial DNA mutation promotes tumori-genesis via alteration in reactive oxygen species generation andapoptosis. Hum Mol Genet (in press)
34. Lima J, Maximo V, Soares P et al (2009) Mitochondria andoncocytomas. In: Singh KK, Costello LC (eds) Mitochondriaand cancer. Springer, New York, pp 193–209
35. Copeland WC, Wachsman JT, Johnson FM et al (2002) Mitochon-drial DNA alterations in cancer. Cancer Invest 20:557–569
492 Virchows Arch (2009) 454:481–495
36. Czarnecka AM, Golik P, Bartnik E (2006) Mitochondrial DNAmutations in human neoplasia. J Appl Genet 47:67–78
37. Tamori A, Nishiguchi S, Nishikawa M et al (2004) Correlationbetween clinical characteristics and mitochondrial D-loop DNAmutations in hepatocellular carcinoma. J Gastroenterol 39:1063–1068
38. Petros JA, Baumann AK, Ruiz-Pesini E et al (2005) mtDNAmutations increase tumorigenicity in prostate cancer. Proc NatlAcad Sci U S A 102:719–724
39. Shidara Y, Yamagata K, Kanamori T et al (2005) Positivecontribution of pathogenic mutations in the mitochondrialgenome to the promotion of cancer by prevention fromapoptosis. Cancer Res 65:1655–1663
40. Pelicano H, Xu RH, Du M et al (2006) Mitochondrialrespiration defects in cancer cells cause activation of Aktsurvival pathway through a redox-mediated mechanism. J CellBiol 175:913–923
41. Gottlieb E, Tomlinson IP (2005)Mitochondrial tumour suppressors:a genetic and biochemical update. Nat Rev Cancer 5:857–866
42. Lima J, Teixeira-Gomes J, Soares P et al (2003) Germlinesuccinate dehydrogenase subunit D mutation segregating withfamilial non-RET C cell hyperplasia. J Clin Endocrinol Metab88:4932–4937
43. Montani M, Schmitt AM, Schmid S et al (2005) No mutationsbut an increased frequency of SDHx polymorphisms in patientswith sporadic and familial medullary thyroid carcinoma. EndocrRelat Cancer 12:1011–1016
44. Cascon A, Cebrian A, Pollan M et al (2005) Succinatedehydrogenase D variants do not constitute a risk factor fordeveloping C cell hyperplasia or sporadic medullary thyroidcarcinoma. J Clin Endocrinol Metab 90:2127–2130
45. Ricketts C, Woodward ER, Killick P et al (2008) GermlineSDHB mutations and familial renal cell carcinoma. J Natl CancerInst 100:1260–1262
46. Tomlinson IP, Alam NA, Rowan AJ et al (2002) Germlinemutations in FH predispose to dominantly inherited uterinefibroids, skin leiomyomata and papillary renal cell cancer. NatGenet 30:406–410
47. Eng C, Kiuru M, Fernandez MJ et al (2003) A role formitochondrial enzymes in inherited neoplasia and beyond. NatRev Cancer 3:193–202
48. Pollard PJ, Briere JJ, Alam NA et al (2005) Accumulation ofKrebs cycle intermediates and over-expression of HIF1alpha intumours which result from germline FH and SDH mutations.Hum Mol Genet 14:2231–2239
49. Maximo V, Botelho T, Capela J et al (2005) Somatic andgermline mutation in GRIM-19, a dual function gene involved inmitochondrial metabolism and cell death, is linked tomitochondrion-rich (Hurthle cell) tumours of the thyroid. Br JCancer 92:1892–1898
50. Huang G, Lu H, Hao A et al (2004) GRIM-19, a cell deathregulatory protein, is essential for assembly and function ofmitochondrial complex I. Mol Cell Biol 24:8447–8456
51. Alchanati I, Nallar SC, Sun P et al (2006) A proteomic analysisreveals the loss of expression of the cell death regulatory geneGRIM-19 in human renal cell carcinomas. Oncogene 25:7138–7147
52. Hsu PP, Sabatini DM (2008) Cancer cell metabolism: Warburgand beyond. Cell 134:703–707
53. Ramanathan A, Wang C, Schreiber SL (2005) Perturbationalprofiling of a cell-line model of tumorigenesis by usingmetabolic measurements. Proc Natl Acad Sci U S A 102:5992–5997
54. Matoba S, Kang JG, Patino WD et al (2006) p53 regulatesmitochondrial respiration. Science 312:1650–1653
55. Kaelin WG Jr, Ratcliffe PJ (2008) Oxygen sensing by meta-zoans: the central role of the HIF hydroxylase pathway. Mol Cell30:393–402
56. Gatenby RA, Gillies RJ (2004) Why do cancers have highaerobic glycolysis? Nat Rev Cancer 4:891–899
57. Ishikawa K, Takenaga K, Akimoto M et al (2008) ROS-generating mitochondrial DNA mutations can regulate tumorcell metastasis. Science 320:661–664
58. Piruat JI, Pintado CO, Ortega-Saenz P et al (2004) Themitochondrial SDHD gene is required for early embryogenesis,and its partial deficiency results in persistent carotid bodyglomus cell activation with full responsiveness to hypoxia. MolCell Biol 24:10933–10940
59. Muller-Hocker J (1992) Random cytochrome-C-oxidase defi-ciency of oxyphil cell nodules in the parathyroid gland. Amitochondrial cytopathy related to cell ageing? Pathol Res Pract188:701–706
60. Rosai J, CarcangiuML, DeLellis RA (1992) Tumours of the thyroidgland. Armed Force Institute of Pathology, Washington, DC
61. Sobrinho-Simoes MA, Nesland JM, Holm R et al (1985) Hurthlecell and mitochondrion-rich papillary carcinomas of the thyroidgland: an ultrastructural and immunocytochemical study. Ultra-struct Pathol 8:131–142
62. Nesland JM, Sobrinho-Simoes MA, Holm R et al (1985)Hurthle-cell lesions of the thyroid: a combined study usingtransmission electron microscopy, scanning electron microscopy,and immunocytochemistry. Ultrastruct Pathol 8:269–290
63. Ebner D, Rodel G, Pavenstaedt I et al (1991) Functional andmolecular analysis of mitochondria in thyroid oncocytoma.Virchows Arch B Cell Pathol Incl Mol Pathol 60:139–144
64. Muller-Hocker J, Jacob U, Seibel P (1998) Hashimoto thyroiditisis associated with defects of cytochrome-c oxidase in oxyphilAskanazy cells and with the common deletion (4, 977) ofmitochondrial DNA. Ultrastruct Pathol 22:91–100
65. Ortmann M, Vierbuchen M, Koller G et al (1988) Renaloncocytoma. I. Cytochrome c oxidase in normal and neoplasticrenal tissue as detected by immunohistochemistry—a valuableaid to distinguish oncocytomas from renal cell carcinomas.Virchows Arch B Cell Pathol Incl Mol Pathol 56:165–173
66. Muller-Hocker J (2000) Expression of bcl-2, Bax and Fas in oxyphilcells of Hashimoto thyroiditis. Virchows Arch 436:602–607
67. Muller-Hocker J, Aust D, Napiwotzky J et al (1996) Defects ofthe respiratory chain in oxyphil and chief cells of the normalparathyroid and in hyperfunction. Hum Pathol 27:532–541
68. Cheung CC, Ezzat S, Ramyar L et al (2000) Molecular basis offHurthle cell papillary thyroid carcinoma. J Clin EndocrinolMetab 85:878–882
69. Sobrinho-Simoes M, Maximo V, Castro IV et al (2005) Hurthle(oncocytic) cell tumors of thyroid: etiopathogenesis, diagnosisand clinical significance. Int J Surg Pathol 13:29–35
70. Langhans T (1907) Über die epithelialen Formen der malignenStruma. Virchows Arch 189:69–153
71. DeLellis RA LR, Heitz PU, Eng C (eds) (2004) World HealthOrganization classification of tumours. Pathology and genetics oftumours of endocrine glands. IARC, Lyon
72. Dominguez-Malagon H, Delgado-Chavez R, Torres-Najera M et al(1989) Oxyphil and squamous variants of medullary thyroidcarcinoma. Cancer 63:1183–1188
73. Volante M, La Rosa S, Castellano I et al (2006) Clinico-pathological features of a series of 11 oncocytic endocrinetumours of the pancreas. Virchows Arch 448:545–551
74. Moran CA, Suster S (2000) Primary neuroendocrine carcinoma(thymic carcinoid) of the thymus with prominent oncocyticfeatures: a clinicopathologic study of 22 cases. Mod Pathol13:489–494
Virchows Arch (2009) 454:481–495 493
75. Baloch ZW, LiVolsi VA (1999) Oncocytic lesions of theneuroendocrine system. Semin Diagn Pathol 16:190–199
76. DeLellis RA (2006) Pathology and genetics of thyroid carcinoma.J Surg Oncol 94:662–669
77. Soares P, Trovisco V, Rocha AS et al (2003) BRAF mutationsand RET/PTC rearrangements are alternative events in theetiopathogenesis of PTC. Oncogene 22:4578–4580
78. Castro P, Rebocho AP, Soares RJ et al (2006) PAX8-PPARgammarearrangement is frequently detected in the follicular variant ofpapillary thyroid carcinoma. J Clin Endocrinol Metab 91:213–220
79. Trovisco V, Vieira DCI, Soares P et al (2004) BRAF mutationsare associated with some histological types of papillary thyroidcarcinoma. J Pathol 202:247–251
80. Trovisco V, Soares P, Preto A et al (2005) Type and prevalenceof BRAF mutations are closely associated with papillary thyroidcarcinoma histotype and patients' age but not with tumouraggressiveness. Virchows Arch 446:589–595
81. Carcangiu ML, Bianchi S, Savino D et al (1991) FollicularHurthle cell tumors of the thyroid gland. Cancer 68:1944–1953
82. Evans HL, Vassilopoulou-Sellin R (1998) Follicular and Hurthlecell carcinomas of the thyroid: a comparative study. Am J SurgPathol 22:1512–1520
83. McDonald MP, Sanders LE, Silverman ML et al (1996) Hurthlecell carcinoma of the thyroid gland: prognostic factors andresults of surgical treatment. Surgery 120:1000–1004
84. Papotti M, Botto Micca F, Favero A et al (1993) Poorlydifferentiated thyroid carcinomas with primordial cell compo-nent. A group of aggressive lesions sharing insular, trabecular,and solid patterns. Am J Surg Pathol 17:291–301
85. Watson RG, Brennan MD, Goellner JR et al (1984) InvasiveHurthle cell carcinoma of the thyroid: natural history andmanagement. Mayo Clin Proc 59:851–855
86. Lang W, Choritz H, Hundeshagen H (1986) Risk factors infollicular thyroid carcinomas. A retrospective follow-up studycovering a 14-year period with emphasis on morphologicalfindings. Am J Surg Pathol 10:246–255
87. Valenta LJ, Michel-Bechet M, Warshaw JB et al (1974) Humanthyroid tumors composed of mitochondrion-rich cells: electronmicroscopic and biochemical findings. J Clin Endocrinol Metab39:719–733
88. Apel RL, Asa SL (2002) The parathyroid glands. In: LiVolsi V,Asa SL (eds) Endocrine pathology. Churchill Livingstone,Philadelphia, pp 103–137
89. Giorgadze T, Stratton B, Baloch ZW et al (2004) Oncocyticparathyroid adenoma: problem in cytological diagnosis. DiagnCytopathol 31:276–280
90. Erickson LA, Jin L, Papotti M et al (2002) Oxyphil parathyroidcarcinomas: a clinicopathologic and immunohistochemical studyof 10 cases. Am J Surg Pathol 26:344–349
91. Yoo GH, Eisele DW, Askin FB et al (1994) Warthin's tumor: a40-year experience at The Johns Hopkins Hospital. Laryngo-scope 104:799–803
92. Honda K, Kashima K, Daa T et al (2000) Clonal analysis of theepithelial component of Warthin's tumor. Hum Pathol 31:1377–1380
93. Kotwall CA (1992) Smoking as an etiologic factor in thedevelopment of Warthin's tumor of the parotid gland. Am J Surg164:646–647
94. Zambrano NR, Lubensky IA, Merino MJ et al (1999) Histopa-thology and molecular genetics of renal tumors toward unifica-tion of a classification system. J Urol 162:1246–1258
95. Kuroda N, Toi M, Hiroi M et al (2003) Review of renaloncocytoma with focus on clinical and pathobiological aspects.Histol Histopathol 18:935–942
96. Maximo V, Soares P, Rocha AS et al (1998) The commondeletion of mitochondrial DNA is found in goiters and thyroidtumors with and without oxyphil cell change. Ultrastruct Pathol22:271–273
97. Maximo V, Sobrinho-Simoes M (2000) Mitochondrial DNA‘common’ deletion in Hurthle cell lesions of the thyroid. J Pathol192:561–562
98. Attardi G, Yoneda M, Chomyn A (1995) Complementation andsegregation behavior of disease-causing mitochondrial DNAmutations in cellular model systems. Biochim Biophys Acta1271:241–248
99. Heddi A, Faure-Vigny H, Wallace DC et al (1996) Coordinateexpression of nuclear and mitochondrial genes involved inenergy production in carcinoma and oncocytoma. BiochimBiophys Acta 1316:203–209
100. Welter C, Kovacs G, Seitz G et al (1989) Alteration ofmitochondrial DNA in human oncocytomas. Genes Chromo-somes Cancer 1:79–82
101. Brooks JD, Marshall FF, Isaacs WB et al (1999) Absence ofHinfI restriction abnormalities in renal oncocytoma mitochon-drial DNA. Mol Urol 3:1–3
102. Simonnet H, Alazard N, Pfeiffer K et al (2002) Lowmitochondrial respiratory chain content correlates with tumoraggressiveness in renal cell carcinoma. Carcinogenesis23:759–768
103. Simonnet H, Demont J, Pfeiffer K et al (2003) Mitochondrialcomplex I is deficient in renal oncocytomas. Carcinogenesis24:1461–1466
104. Mayr JA, Meierhofer D, Zimmermann F et al (2008) Loss ofcomplex I due to mitochondrial DNA mutations in renaloncocytoma. Clin Cancer Res 14:2270–2275
105. Savagner F, Chevrollier A, Loiseau D et al (2001) Mitochondrialactivity in XTC.UC1 cells derived from thyroid oncocytoma.Thyroid 11:327–333
106. Baris O, Savagner F, Nasser V et al (2004) Transcriptionalprofiling reveals coordinated up-regulation of oxidative metab-olism genes in thyroid oncocytic tumors. J Clin EndocrinolMetab 89:994–1005
107. Jacques C, Baris O, Prunier-Mirebeau D et al (2005) Two-stepdifferential expression analysis reveals a new set of genesinvolved in thyroid oncocytic tumors. J Clin Endocrinol Metab90:2314–2320
108. Maximo V, Preto A, Crespo A et al (2004) Core I gene isoverexpressed in Hurthle and non-Hurthle cell microfollicularadenomas and follicular carcinomas of the thyroid. BMC Cancer4:12
109. Sobrinho-Simoes M, Preto A, Rocha AS et al (2005) Molecularpathology of well-differentiated thyroid carcinomas. VirchowsArch 447:787–793
110. Pedersen PL (2007) Warburg, me and Hexokinase 2: multiplediscoveries of key molecular events underlying one of cancers'most common phenotypes, the “Warburg effect”, i.e., elevatedglycolysis in the presence of oxygen. J Bioenerg Biomembr39:211–222
111. Ko YH, Pedersen PL, Geschwind JF (2001) Glucose catabolismin the rabbit VX2 tumor model for liver cancer: characterizationand targeting hexokinase. Cancer Lett 173:83–91
112. Geschwind JF, Ko YH, Torbenson MS et al (2002) Noveltherapy for liver cancer: direct intraarterial injection of a potentinhibitor of ATP production. Cancer Res 62:3909–3913
113. Bonnet S, Archer SL, Allalunis-Turner J et al (2007) Amitochondria-K+ channel axis is suppressed in cancer and itsnormalization promotes apoptosis and inhibits cancer growth.Cancer Cell 11:37–51
494 Virchows Arch (2009) 454:481–495
114. Warburg O (1956) On respiratory impairment in cancer cells.Science 124:269–270
115. Pouyssegur J, Dayan F, Mazure NM (2006) Hypoxia signallingin cancer and approaches to enforce tumour regression. Nature441:437–443
116. Bristow RG, Hill RP (2008) Hypoxia and metabolism. Hypoxia,DNA repair and genetic instability. Nat Rev Cancer 8:180–192
117. Higgins DF, Kimura K, Bernhardt WM et al (2007) Hypoxiapromotes fibrogenesis in vivo via HIF-1 stimulation of epithelial-to-mesenchymal transition. J Clin Invest 117:3810–3820
118. Yang MH, Wu MZ, Chiou SH et al (2008) Direct regulation ofTWIST by HIF-1alpha promotes metastasis. Nat Cell Biol 10:295–305
119. Chiang AC, Massague J (2008) Molecular basis of metastasis. NEngl J Med 359:2814–2823
120. Selak MA, Armour SM, MacKenzie ED et al (2005) Succinatelinks TCA cycle dysfunction to oncogenesis by inhibiting HIF-alpha prolyl hydroxylase. Cancer Cell 7:77–85
121. MITOMAP (2007) A human mitochondrial genome databasewww.mitomap.org.
Virchows Arch (2009) 454:481–495 495
Related Documents