Chapter 15 Shock and Resuscitation Copyright ©2010 by Pearson Education, Inc. All rights reserved. Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich • Keith J. Karren Objectives 1. Define key terms introduced in this chapter. 2. Explain the pathophysiology of shock (hypoperfusion), including the consequences of cellular hypoxia and death (slide 16 ). 3. Describe the physiology of maintaining adequate perfusion (slide 17 ). 4. Describe how inadequate vascular volume, inadequate heart function, and decreased peripheral vascular resistance can lead to shock (slide 18-22 ). 5. Give examples of conditions that can lead to (slides 18 - 22 , 25-47 ): a. Loss of vascular volume b. Inadequate heart function c. Decreased peripheral vascular resistance Objectives 6. Explain the mechanisms and pathophysiology of each of the following categories and types of shock (slides 23-50 ): a. Hypovolemic (hemorrhagic and nonhemorrhagic) b. Distributive (anaphylactic, septic, neurogenic) c. Cardiogenic d. Obstructive e. Metabolic or respiratory 7. Explain how compensatory mechanisms to shock are maintained through (slides 53-56 ): a. Direct nerve stimulation b. Release of hormones 8. Explain the body’s compensatory responses to hypoperfusion and how they manifest in the early signs and symptoms of shock (slides 51-56 ).

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Chapter 15
Shock and Resuscitation
Copyright ©2010 by Pearson Education, Inc.All rights reserved.
Prehospital Emergency Care, Ninth EditionJoseph J. Mistovich • Keith J. Karren
Objectives
1. Define key terms introduced in this chapter.2. Explain the pathophysiology of shock (hypoperfusion),
including the consequences of cellular hypoxia anddeath (slide 16).
3. Describe the physiology of maintaining adequateperfusion (slide 17).
4. Describe how inadequate vascular volume, inadequateheart function, and decreased peripheral vascularresistance can lead to shock (slide 18-22).
5. Give examples of conditions that can lead to (slides 18-22, 25-47):a. Loss of vascular volumeb. Inadequate heart functionc. Decreased peripheral vascular resistance
Objectives
6. Explain the mechanisms and pathophysiology of eachof the following categories and types of shock (slides23-50):a. Hypovolemic (hemorrhagic and nonhemorrhagic)b. Distributive (anaphylactic, septic, neurogenic)c. Cardiogenicd. Obstructivee. Metabolic or respiratory
7. Explain how compensatory mechanisms to shock aremaintained through (slides 53-56):a. Direct nerve stimulationb. Release of hormones
8. Explain the body’s compensatory responses tohypoperfusion and how they manifest in the early signsand symptoms of shock (slides 51-56).

Objectives
9. Differentiate between early (compensatory) and late(decompensatory/irreversible) signs of shock (slide 58).
10. Describe the progression of shock through thecompensatory, decompensatory (progressive), andirreversible stages (slide 58).
11. Explain how to identify the patient who is in a shockstate and demonstrate the assessment of patients toidentify shock (slides 59-64).
12. Explain the influence of age on the assessment andmanagement of patients with shock (slides 65-66).
13. Discuss the goals of prehospital management ofpatients with shock (slides 67-69).
Objectives
14. Describe the pathophysiology of cardiac arrest (slides70-73).
15. Differentiate between the electrical, circulatory, andmetabolic phases of cardiac arrest (slide 73).
16. Identify situations in which resuscitative attemptsshould be withheld (slides 76-77).
17. Explain each of the links in the Chain of Survival ofcardiac arrest (slides 78-79).
18. Explain the importance of early defibrillation in cardiacarrest (slides 80-81).
19. Explain the rationale for the “push hard and push fast”approach to cardiopulmonary resuscitation (CPR)(slides 82-83).
Objectives
20. Describe the features, functions, advantages,disadvantages, use, and precautions in the use ofautomated external defibrillators (AEDs) (slides 84-87).
21. Compare and contrast ventricular fibrillation, ventriculartachycardia, asystole, and pulseless electrical activity(slides 88-92).
22. Given a series of cardiac arrest scenarios involvinginfants, children, and adults, demonstrate appropriateassessment and resuscitative techniques, including theintegrated use of AEDs (automated andsemiautomated), ventilation, and CPR, and explain thepurpose and procedure for reassessment of thecardiac arrest patient (slides 94-101).

Objectives
23. Demonstrate assessment and management of a postcardiac-arrest patient with return of spontaneouscirculation (slides 98-101).
24. Given a cardiac arrest scenario, make decisionsregarding obtaining advanced cardiac life support(ACLS) (slide 105).
25. Describe the safety precautions to be taken to protectyourself, other EMS providers, the patient, andbystanders in resuscitation situations (slides 93, 107-108).
Objectives
26. Explain the importance of AED maintenance, EMTtraining and skills maintenance, and medical directionin the Chain of Survival of cardiac arrest (slides 109-115).
27. Discuss special considerations in the use of an AED inpatients with cardiac pacemakers and automaticimplanted cardioverter-defibrillators (slides 118-121).
28. List the advantages and disadvantages of automatedchest compression devices, impedance thresholddevices, and other circulation-enhancing devices(slides 122-129).
Multimedia Directory
Slide 22 Etiology of Shock AnimationSlide 50 Types of Shock AnimationSlide 69 Bleeding Control/Shock Management Video

Topics
ShockResuscitation in Cardiac ArrestAutomated External Defibrillation and CardiopulmonaryResuscitationRecognizing and Treating Cardiac ArrestSpecial Considerations for the AED
CASE STUDYCASE STUDY
Dispatch
Respond to 46 Hillman Street. You have a 26-year-old male patient who has been stabbed in
the leg and is bleeding profusely. Lawenforcement is en route.
EMS Unit 102
Time out 2102

• A police officer leads you into the basement• Patient is supine on the floor with a large pool of
blood around his right thigh• Patient is not alert, does not respond to voice,
and appears extremely pale
Upon Arrival
How would you proceed with theassessment of this patient?
Back to Topics
Shock

Inadequate tissueperfusion
Back to Objectives
Review of Respiratory Pathophysiology
Back to Objectives
Etiologies of Shock
Back to Objectives

Inadequate Volume
Fig. 15-01
Don’t have artyet - WDS
Fig. 15-02
Inadequate Pump Function
Don’t have artyet - WDS
Fig. 15-03
Inadequate VesselTone
Don’t have artyet - WDS

Etiology of Shock
Return to Directory
Click here to view an animation on the etiology of shock
Categories of Shock
Back to Objectives
Fig. 15-04
Don’t have artyet - WDS

Categories of Shock
Hypovolemic Shock
Back to Objectives
Fig. 15-05
Don’t have artyet - WDS
Categories of Shock
Distributive Shock

Fig. 15-06
Don’t have artyet - WDS
Categories of Shock
Cardiogenic Shock
Fig. 15-07
Don’t have artyet - WDS

Categories of Shock
Obstructive Shock
Fig. 15-08
Don’t have artyet - WDS
Categories of Shock
Metabolic orRespiratory Shock

Inability of thebody to use,
transport, and/oroffload oxygen
Specific Types of Shock
Specific Types of Shock
HemorrhagicHypovolemic Shock

Fig. 15-05a only(trim outnonhemorrhagichypovolemicshock)Don’t have art
yet - WDS
Specific Types of Shock
NonhemorrhagicHypovolemic Shock
Fig. 15-05bonly (trim outhemorrhagichypovolemicshock)
Don’t haveart yet -WDS

Specific Types of Shock
Burn Shock
Fluid is pulled from thevascular space to the
interstitial space,causing hypovolemia.
Specific Types of Shock
Anaphylactic Shock

Vasodilation movesblood from the centralcore to the periphery,causing distributive
shock.
Specific Types of Shock
Septic Shock
Bacteria or toxinsthroughout the body
cause the bloodvessels to dilate and
to become permeable.

Specific Types of Shock
Neurogenic Shock
Spinal cord traumacauses a loss of bloodvessel tone and results
in widespreadvasodilation.
Specific Types of Shock
Cardiogenic Shock

Depressed pump function reduces the force ofthe left ventricular contraction, stroke volume,cardiac output, systolic blood pressure, and
perfusion.
Types of Shock
Return to Directory
Click here to view an animation on types of shock.
The Body’s Response toShock
Back to Objectives

The Body’s Response to Shock
Direct NerveStimulation
Back to Objectives
• Increased heartrate
• Increasedcontractile force
• Vasoconstriction• Release of
epinephrine andnorepinephrine

The Body’s Response to Shock
Release of Hormones
Hormonesreleased
stimulate alphareceptors inperipheral
blood vessels,returning bloodto the central
core.
Stages of Shock

Back to Objectives
Shock Assessment
Back to Objectives
Shock Assessment
History

• Pay particularattention tochief complaintand SAMPLE
• Somemedicationsmay preventcompensation
Shock Assessment
Physical Exam
• Altered mental status• Pale, cool, and
clammy skin• Delayed capillary
refill• Decreased urine
output• Weak or absent
peripheral pulses

• Skin color,temperature, andcondition
• Pulse oximeterreading
• Blood pressure (bothsystolic and diastolic)
• Heart rate• Pulse character• Respiratory rate and
tidal volume
Age Considerations inShock
Back to Objectives
Childrencompensate well
and then suddenlydecompensate.
Medications andadvanced age
decreasecompensation
ability.

General Goals ofPrehospital Management of
Shock
Back to Objectives
• Secure and maintain an airway• Assure adequate ventilation• Provide high-flow, high-concentration oxygen• Avoid hyperventilation• Stop any external bleeding• Splint fractures to reduce bleeding• Leave impaled objects in place• Keep the patient warm• Apply PASG if indicated and local protocol
allows• Provide rapid transport and perform other
interventions en route• Consider an ALS intercept
Bleeding Control/Shock Management
Return to Directory
Click here to view a video on the topic of bleeding control and shockmanagement.

Resuscitation inCardiac Arrest
Back to Topics
Sudden Death:the patient dieswithin one hourof the onset of
symptoms
Cardiac Arrest:cardiac output is
completelyineffective and nopulse can be felt
Resuscitation:bringing the
patient back froma potential or
apparent death
Back to Objectives
Pathophysiology ofCardiac Arrest

Electrical PhaseLess than four minutes following arrest, the cardiac
muscle uses its sugar/oxygen stores.
Circulatory PhaseFrom four to ten minutes following arrest, the cardiac
muscle switches to anaerobic metabolism.
Metabolic PhaseGreater than ten minutes following arrest, cardiac cells
swell, rupture, and die.Back to Objectives
Terms Related toResuscitation
SurvivalA patient who survives tobe discharged from the
hospital
Return ofSpontaneous
Circulation (ROSC)The patient regains aspontaneous pulse
during the resuscitationeffort.
Total DowntimeThe total time from when
the patient goes intocardiac arrest until you
deliver the patient to theemergency department
DowntimeThe time the patient goes
into cardiac arrest untilCPR is effectively being
performed

Withholding a ResuscitationAttempt
Back to Objectives
You may also withholdresuscitation in cases ofobvious death, such as
decapitation.
The Chain of Survival
Back to Objectives

Early Access:The quicker someone can recognize a
patient in cardiac compromise, the betterthe chance of patient survival
Early CPR:Immediate CPR can double or even triplethe arrested patient’s chance of survival
from ventricular fibrillation
Early Defibrillation:Survival rates of patients in VF SCA
decrease approximately 7–10 percent forevery minute that defibrillation is delayed
Early Advanced Care:Advanced life support (ALS) is delivered
most often by paramedics who can provideadvanced cardiac life support (ACLS).
Automated ExternalDefibrillation andCardiopulmonary
Resuscitation
Back to Topics
AHA Rationale for EarlyDefibrillation
• The most frequent initial rhythm in suddencardiac arrest is ventricular fibrillation
• The most effective treatment for terminatingventricular fibrillation is electrical defibrillation
• The probability of successful defibrillation isdirectly related to the time from fibrillation todefibrillation
• Ventricular fibrillation will, without prompt orappropriate treatment, degenerate into asystole
Back to Objectives

• “Push hard and pushfast”
• 100 compressions perminute
• 30:2 compression tobreath ratio
• Start with CPR if thedowntime is unknownor greater than four tofive minutes
• If the downtime is lessthan four to fiveminutes, use the AED
Pulse checks shouldNOT follow a
defibrillation attempt.Always resume CPR
after shocking a patientwith an AED.
Back to Objectives
AHA Rationale for Current AEDand CPR Standards
• “Push hard and push fast” will help avoidcompressions that are delivered either too slowor too shallow
• The ratio of 30:2 minimizes interruptions tocompressions for pulse checks and ventilations
• Compressions prior to defibrillation inunwitnessed arrests will make defibrillation moresuccessful
• Rarely will a perfusing rhythm be evident by apulse check immediately after defibrillation
• CPR as just described can double or triple thechance of survival
Types of Defibrillators
Back to Objectives
Manualdefibrillators
require extensivetraining prior to
use
An automatedexternal
defibrillator (AED)is much simpler to
operate.
Advantages of AEDs:•Speed of operation•Safer, more effectivedelivery•More efficient monitoring
Types of AEDs:•Fully automated AED•Semiautomated AED
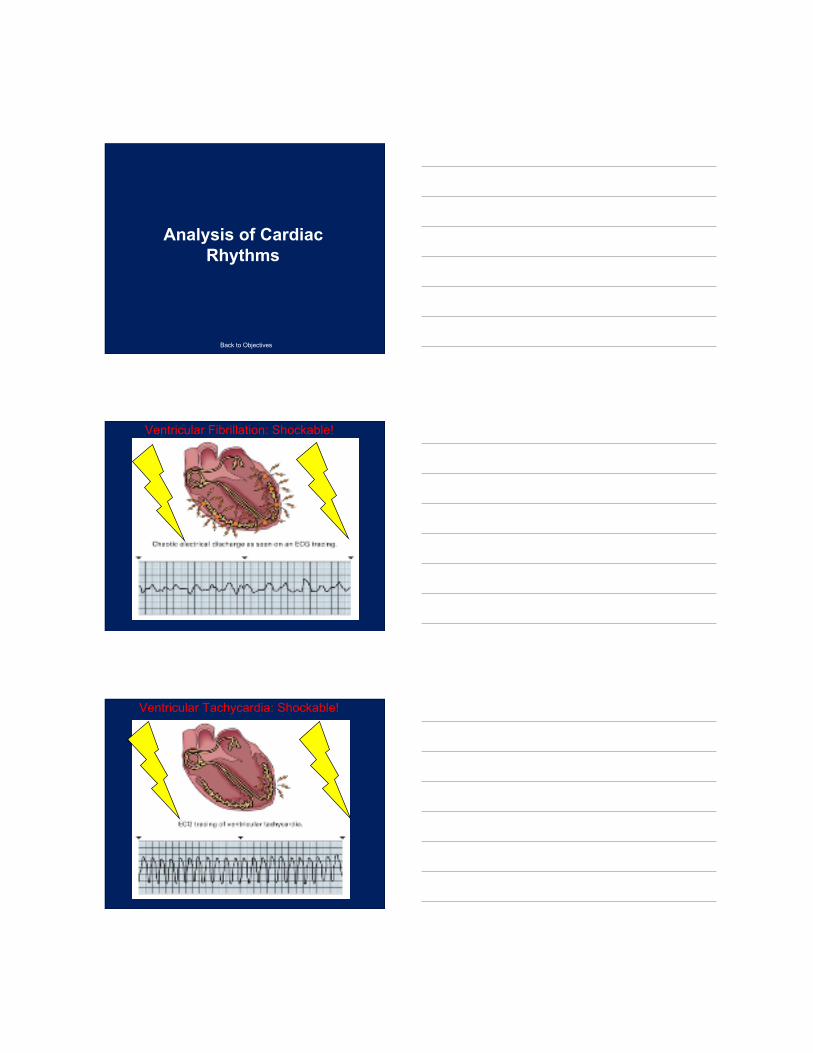
Biphasic versus Monophasic
Biphasic: moreeffective with less
energy
Monophasic: lesseffective with more
energy
150 to 200 J 200, 300, 360 J
Analysis of CardiacRhythms
Back to Objectives
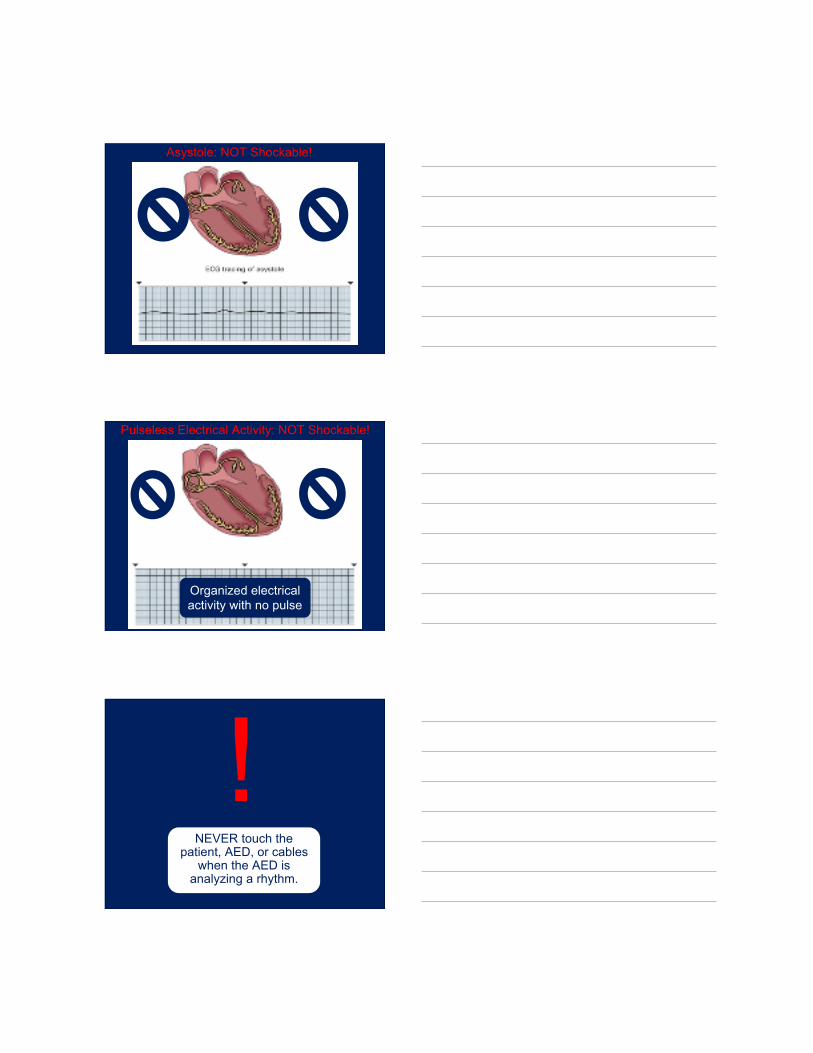
Ventricular Fibrillation: Shockable!
Ventricular Tachycardia: Shockable!
Asystole: NOT Shockable!
Pulseless Electrical Activity: NOT Shockable!
Organized electricalactivity with no pulse
NEVER touch thepatient, AED, or cables
when the AED isanalyzing a rhythm.
!

When and When Not to Usethe AED
Back to Objectives
Apply an AED if:
• The patient is in nontraumatic cardiacarrest
• For children one to eight years of age, anadult AED may be used, preferably with apediatric dose attenuating system
• The downtime is less than four to fiveminutes, or two minutes of CPR has beenperformed
Do not apply an AED if:
• The patient is less than one year of age• The patient is in cardiac arrest as a result
of trauma• The downtime is greater than four to five
minutes, and two minutes of CPR has notbeen performed

Recognizing andTreating Cardiac
Arrest
Back to Topics
Assessment-BasedApproach: Cardiac Arrest
Back to Objectives
Fig 15-16aAssessmentSummary Cardiac
Don’t have art yet -WDS
Performing Defibrillation
Fig 15-16b and/or15-17 I cannotdetermine withoutseeing content
Don’t have art yet -WDS
Transporting the CardiacArrest Patient

• When to transport• Transporting a patient with a pulse• Transporting a patient without a pulse
Providing for AdvancedCardiac Life Support
Request advance life support (ALS)providers as soon as possible.
Back to Objectives

SpecialConsiderations for
the AED
Back to Topics
Safety Considerations
Back to Objectives
Remember the following safetyguidelines:
• Clear the patient beforeshocking
• Water and metalconduct electricity verywell
• Never place anelectrode over amedication patch orimplanted pacemaker
If the patient has anextremely hairy chest andfirmly pressing the pad onthe chest does not work,
then consider shaving thearea with an electric
clippers or disposablerazor.

AED Maintenance
Back to Objectives
Alwaysinspect your
AED forfunction andproper stock.
The mostcommon
cause of AEDfailure is
battery failure.
Training and SkillsMaintenance

• Be prepared to use the AED at any time
• Practice your skills with the AED at leastevery 90 days
• Review incidents for quality improvement
• Keep up to date on new research on AEDprocedures
Medical Direction and theAED
Responsible for the following:
• Making sure that the EMS system has allnecessary links in the AHA Chain ofSurvival
• Overseeing all levels of EMTs• Reviewing the continual competency skill
review program• Engaging in an audit and/or quality
improvement program

Incident review may beaccomplished by:
• Written reports• Review of the voice and/or ECG tapes if
the system’s AED is equipped with thatfeature
• Review of solid-state memory modulesand magnetic tapes if the system’s AED isso equipped
Energy Levels ofDefibrillators
Typical Energy Levels
• Manual defibrillators typically range fromfive joules to 360 joules
• Most AEDs have two preset values of 200joules and 360 joules

Cardiac Pacemakers
Back to Objectives
Some patientsrequire a
pacemaker tomaintain an
adequate heartrate. They areusually placed
under a clavicle.
Automatic ImplantableCardioverter Defibrillators

Automatic ImplantableCardioverter Defibrillators (AICD)
• Implanted device that monitors the heart’sactivity
• Capable of delivering shocks directly tothe heart to correct lethal dysrhythmias
• A conscious patient can tell you when ashock is delivered
• The shock from an AICD does not pose arisk to EMS providers
Automated Chest CompressionDevices
Mechanical PistonDevice
Back to Objectives
A mechanicalpiston device in
place on a patient

Automated Chest CompressionDevices
Load-Distributing-Band CPR or Vest CPR
A load-distributing-bandCPR device
Automated Chest CompressionDevices
Impedance ThresholdDevice

An impedancethreshold device
Automated Chest CompressionDevices
Other CirculationEnhancing Devices
Other devices, likethe LUCAS, may
also activelydecompress the
chest.

CASE STUDYCASE STUDY
Follow-Up
Primary Assessment• Patient not alert and doesn’t respond
when name is called• Pale color; apply in-line stabilization• Patient moans to painful stimuli• Respirations are adequate; place
nonrebreather mask at 15 lpm• Find blood coming from right leg wound;
expose leg and apply direct pressure
CASE STUDYCASE STUDY
Secondary Assessment• You expose the patient’s body to look for
other injuries while rolling onto backboard• No other injuries found• BP: 72/58mmHg; HR: 132; RR: 26; skin
pale, cool, and clammy• Patient still responsive only to pain• No history or medical information
obtainable
CASE STUDYCASE STUDY
Reassessment• Monitor mental status, ABCs, and
bleeding en route• No change en route• Upon arrival, trauma surgeon meets you
and brings the patient to the trauma bay• Prepare written report and return to
service
CASE STUDYCASE STUDY
• Dispatch advises you are responding to aman down; CPR in progress
• You arrive four minutes after the call camein and within moments of fire and PD
• You see a small crowd gathered around amale patient; two people are in factperforming CPR
Critical Thinking Scenario
• You’ve already donned gloves and eyeprotection while en route
• You grab your AED as you exit theambulance
• Your primary assessment reveals anunresponsive man, mid-50s, supine on theground with effective bystander CPR inprogress
Critical Thinking Scenario

• Bystanders state that they began CPRimmediately upon his collapse and thencalled 911
• The patient’s skin is slightly cyanotic• You request that CPR be stopped
temporarily while you assess pulse andbreathing
• Your partner is setting up the AED
Critical Thinking Scenario
• You find no carotid pulse and detect nobreathing
• This is a priority patient for whomdefibrillation is appropriate
• You direct a firefighter to resumecompressions while you ventilate with abag-valve mask and high-flow, high-concentration oxygen
Critical Thinking Scenario
1. What assessment findings indicate that thispatient is indeed in cardiac arrest?
2. Which components of the Chain of Survivalhave already been met?
3. Why is this patient a candidate for immediateversus delayed AED use?
4. What cardiac rhythm is this patient most likelygoing to show?
Critical Thinking Questions

5. What is the compression to ventilation ratiogoing to be for this patient?
6. If the AED indicates that no shock iswarranted, what should your next action be?
Critical Thinking Questions
Reinforce and Review
Please visitwww.bradybooks.com
and follow the myBradykit linksto access content for the text.
Related Documents











