378 European Journal of Trauma 2004 · No. 6 © Urban & Vogel Original Article Minimally Invasive Management of Distal Metaphyseal Tibial Fractures and Pilon Fractures Technique and Early Results with the IP-XS Nail Jonas Gehr, Florian Hilsenbeck, Tim Arnold, WilhelmFriedl 1 European Journal of Trauma Abstract Background and Purpose: Pilon fractures and distal metaphyseal tibial fractures as high-energy injuries to the lower limb frequently lead to extensive soft-tissue damage, delayed union and nonunion, infections, and posttraumatic arthrosis. The operative treatment de- mands a stable fixation of the reconstructed joint and, at the same time, minimal irritation of the soft tissues by the fixation devices. The additional consideration of a minimal surgical approach especially in critical soft-tissue situations and the potential for soft-tissue irritation by the subcutaneously placed material has led the authors to look for alternative techniques of osteosynthesis. Material and Methods: Following an experimental study examining the stabilization of the fibula with an IP-XS nail in comparison to plate osteosynthesis and good results of the XS nail for ankle joint fractures, the nail is now used in percutaneous technique for con- comitant fractures of the fibula in distal metaphyseal fractures of the lower leg, pilon fractures and for fixa- tion of the tibia following joint reconstruction. The advantage here is the avoidance of a lateral incision. 18 distal tibial fractures, ten type C and eight type A fractures, five of which were open (II° and III°) fractures, were treated with the XS nail. The results after a 1-year follow-up were classified according to Ovadia’s objec- tive and subjective evaluation scale. Results: 15 of 18 patients could be followed up for 1 year (eight type C and seven type A fractures). According to the subjective section of the Ovadia score, four of 15 pa- tients had an excellent, seven a good, three a fair, and one patient a poor result. Using the objective Ovadia score, three of 15 patients had an excellent, six a good, four a fair, and two a poor result. Because of the short follow-up late osseous complications, such as osteo- myelitis or infected nonunion, after fresh pilon frac- tures could not be observed. Conclusion: The IP-XS nail presented here meets the re- quirements of maximum protection of soft tissue, se- cure fixation of the fracture and a minimally invasive approach, as set out for an internal fixation device. Key Words Pilon fracture · Soft-tissue damage · IP-XS nail · Minimally invasive Eur J Trauma 2004;30:378–86 DOI 10.1007/s00068-004-1414-9 Introduction The pilon fracture is one of the most serious fractures of the lower limb. It was first described in 1911, by the French radiologist Destot [7]. In 1951, Lorenz Böhler attempted a systematic analysis trying to relate trauma mechanism and fracture morphology for the first time [2]. The classification most frequently used was the clas- sification by Ruedi & Allgöwer, which was replaced by the AO-ASIF classification in 1991. Early experiments with surgical treatment produced poor results; thus, conservative treatment was initially favored. However, different authors were able to prove that even the slightest dislocation of the fracture, axis deviation and small joint graduations led to arthrotic destruction of the ankle joint [11, 14]. The results of con- servative treatment were correspondingly poor. 1 Klinikum Aschaffenburg, Teaching Hospital of the University of Wuerzburg, Aschaffenburg, Germany. Received: February 23, 2004; revision accepted: October 15, 2004.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
378 European Journal of Trauma 2004 · No. 6 © Urban & Vogel
Original Article
Minimally Invasive Management of Distal Metaphyseal Tibial Fractures and Pilon FracturesTechnique and Early Results with the IP-XS Nail
Jonas Gehr, Florian Hilsenbeck, Tim Arnold, WilhelmFriedl1
European Journal of Trauma
Ab stract Background and Purpose: Pilon fractures and distal metaphyseal tibial fractures as high-energy injuries to the lower limb frequently lead to extensive soft-tissue damage, delayed union and nonunion, infections, and posttraumatic arthrosis. The operative treatment de-mands a stable fixation of the reconstructed joint and, at the same time, minimal irritation of the soft tissues by the fixation devices. The additional consideration of a minimal surgical approach especially in critical soft-tissue situations and the potential for soft-tissue irritation by the subcutaneously placed material has led the authors to look for alternative techniques of osteosynthesis.Material and Methods: Following an experimental study examining the stabilization of the fibula with an IP-XS nail in comparison to plate osteosynthesis and good results of the XS nail for ankle joint fractures, the nail is now used in percutaneous technique for con-comitant fractures of the fibula in distal metaphyseal fractures of the lower leg, pilon fractures and for fixa-tion of the tibia following joint reconstruction. The advantage here is the avoidance of a lateral incision. 18 distal tibial fractures, ten type C and eight type A fractures, five of which were open (II° and III°) fractures, were treated with the XS nail. The results after a 1-year follow-up were classified according to Ovadia’s objec-tive and subjective evaluation scale.Results: 15 of 18 patients could be followed up for 1 year (eight type C and seven type A fractures). According to the subjective section of the Ovadia score, four of 15 pa-tients had an excellent, seven a good, three a fair, and one patient a poor result. Using the objective Ovadia score, three of 15 patients had an excellent, six a good,
four a fair, and two a poor result. Because of the short follow-up late osseous complications, such as osteo-myelitis or infected nonunion, after fresh pilon frac-tures could not be observed.Conclusion: The IP-XS nail presented here meets the re-quirements of maximum protection of soft tissue, se-cure fixation of the fracture and a minimally invasive approach, as set out for an internal fixation device.
Key WordsPilon fracture · Soft-tissue damage · IP-XS nail · Minimally invasive
Eur J Trau ma 2004;30:378–86
DOI 10.1007/s00068-004-1414-9
IntroductionThe pilon fracture is one of the most serious fractures of the lower limb. It was first described in 1911, by the French radiologist Destot [7]. In 1951, Lorenz Böhler attempted a systematic analysis trying to relate trauma mechanism and fracture morphology for the first time [2]. The classification most frequently used was the clas-sification by Ruedi & Allgöwer, which was replaced by the AO-ASIF classification in 1991.
Early experiments with surgical treatment produced poor results; thus, conservative treatment was initially favored. However, different authors were able to prove that even the slightest dislocation of the fracture, axis deviation and small joint graduations led to arthrotic destruction of the ankle joint [11, 14]. The results of con-servative treatment were correspondingly poor.
1 Klinikum Aschaffenburg, Teaching Hospital of the University of Wuerzburg, Aschaffenburg, Germany.
Received: February 23, 2004; revision accepted: October 15, 2004.

Gehr J, et al. Fracture Management with the IP-XS Nail
379European Journal of Trauma 2004 · No. 6 © Urban & Vogel
Good operative results were first published by Ruedi & Allgöwer [19, 20]. The important primary osteosynthe-sis of the fibula, sparing the soft tissue, was already indi-cated. Anatomic reduction of the fibula eases anatomic reconstruction of the tibial joint surface because of liga-mentotaxis. The medial support of the tibia by plate os-teosynthesis is the last operative measure, after cancel-lous bone grafting for metaphyseal defects. Ankle joints treated according to these principles produced satisfac-tory results for the first time. Soft-tissue management by a two-sided tactical procedure has been demanded by several authors, since significant soft-tissue damage is usually present due to the accident mechanism [3, 4, 15, 21, 22].
Up to now, implants such as T, L, 3.5-mm LCDC, LC (locking compression) or reconstruction plates and, as a newer concept, anatomic angle-stabilized plates have al-so been available to treat the fibula. They all share the same problems of additional traumatization of the soft tissue, due to the large surgical approach and the position of the plate between the bones and the generally thin soft tissue of the distal lower limb. A minimally invasive treat-ment is striven for. The use of intramedullary wires rep-resents a correct approach being much less invasive and, thus, having a lower access morbidity. However, simple wires are too weak and not stable in length or rotation, thus compromising the anatomic reduction of the fibula. For this reason, a new concept with IP-XS (L) nails (In-traplant® Company), small lockable nails, has been pur-sued in our clinic. The advantages of the new implant and the first clinical results of a follow-up investigation after 1 year are presented in this article.
Material and MethodsImplant and Operative Technique
The XS nail® (Intraplant®) for the treatment of malle-olar fractures has a round profile and a diameter of 4.5 mm (Figure 1), or 3.5 mm for the XXS(L) nail [9, 10]. Depending on the fracture to be treated, the XS nail is available with four to eleven locking holes with 9-mm spacing, with the two holes closest to the fixation having a longitudinal oval alignment. The smaller XXS nail is available with three, four, six, eight, and ten nail holes. The XSL long nails are available in lengths up to 272 mm, and the XXSL up to a length of 197 mm. The nail bearing is prepared after closed reduction in the case of pilon fractures. A central guide wire of 2 mm thick-ness (XXS 1.6 mm), and a hollow drill of 4.5 mm (XXS 3.5 mm) are deployed exactly in line with the medullary
space of the fibula. Using a radiolucent aiming device, the XS nail is introduced into the fibula or intraosse-ously into the medial malleolus over the fracture, and cross-locking takes place with threaded Kirschner wires (thickness 2 mm, or 1.6 mm XXS), at an angle of 90°. In the case of a very thin medullary space, the XXS nail is used. In transverse fractures, additional interfragmenta-ry compression can take place via a compression screw which is inserted after removal of the aiming device. In oblique fractures, the compression created by the re-duction forceps is fixed by means of the threaded wires which cross the fracture. Instead of the standard threa-ded K-wires, angle-stable locking with 2.4-mm threaded wires for the XS nail and 2.0-mm threaded wire for the XXS nail can be performed. We recommend that the XS nail be three holes (2.7 cm) longer than the fracture to ensure stability.
The osteosynthesis is prepared by an angled inci-sion, 1–1.5 cm long, on the distal end of the fibula. Here, a 1.6 mm or 2.0 mm thick guide wire is introduced in line with the direction of the fibular medullary cavity, after securing the peroneal tendons with a retractor. After closed reduction the fracture level is crossed with the wire, the medullary channel reamed with the cannulated drills and the nail introduced. The nail is then fixed with threaded K-wires. The length of the nail can either be assessed previously on the initial X-ray image or follow-ing intraoperative X-ray examination. With the nail fixed to the aiming device it is possible to reduce the fibula and the tibia by pulling on the aiming device and using the nail as a joystick. Ante- and retroflexion and the reduction in the frontal plane will almost always have been effected by the intramedullary position of the nail. Using the standard XS nail, the reduced fracture is transfixed by cross-locking the nail using the aiming de-
Figure 1. Standard XS nail with aiming device. 1: X-ray-transparent car-bon aiming device; 2: XS standard (4.5 mm) nail, here twelve-hole nail; 3: adapter for the nail on the aiming device; 4: lateral drill steve for the locking wires; 5: cross-locking threaded K-wire.

Gehr J, et al. Fracture Management with the IP-XS Nail
380 European Journal of Trauma 2004 · No. 6 © Urban & Vogel
vice. With the long (X[X]SL) nails, proximal freehand locking is necessary. As the next step, the tibial fracture is reduced and temporarily fixed using an external fix-ator waiting for definitive treatment after soft-tissue consolidation. However, reconstruction of the tibial joint can also take place primarily with an XS nail and/or cannulated screws, within the framework of the pri-mary osteosynthesis.
In case of severe soft-tissue damage, a minimally in-vasive percutaneous XS nailing can be used as a tempo-rary osteosynthesis of the tibia. The XS nail can also be left as a definitive osteosynthesis, if a good formation of callus is perceptible after 6 weeks on a control X-ray and the anatomic reduction is still valid. We successfully use the covered treatment with the nail system for metaphyseal tibial frac-tures or for successfully reduced fractures of the tibial joint. In these cases an XS nail is always positioned from the medial ankle to the proxi-mal lateral cortical bone and, if nec-essary, a second nail is inserted from the distal lateral tibia aiming at the proximal medial cortical bone. This second nail can also be positioned from proximal medial to distal lat-eral. The entrance point on the bone surface should be opened with a 2.5- to 3.5-mm drill for the latter two pro-cedures.
Case MaterialThe XS nail has been implanted in case of distal metaphyseal tibial fractures and pilon fractures since 07/2002. The patient data has been recorded prospectively with a stan-dardized form since the first appli-cation. From 07/2002 to 12/2003, 32 patients with 33 pilon fractures were recorded and the early results were documented in the form of a 1-year follow-up, using the Ovadia score [16] (Table 1). After 1 year, 18 pati-ents were summoned for a follow-up investigation. 15 patients could be followed up, two had died and one patient had moved (83.3% follow-up rate). The average age was 52.0 ye-
ars (35–80 years); five female and ten male patients ca-me to the evaluation. There were eight type C (three C3, three C2, two C1) and seven type A (six A3, one A2) fractures, of which three were II° open, one was III° open, and ten were closed. Two patients had a reosteo-synthesis after treatment with plate osteosynthesis. In one case, an infected nonunion was present, the second patient presented with incorrect reduction in valgus and tibial and fibular nonunion. In nine cases, the fibula had been fixed primarily with an XS nail and retained with an external fixator until soft-tissue consolidation. In a second procedure the tibia was treated with an XS nail and/or screws or plate osteosynthesis after 5–8 days. In one case, after primary osteosynthesis of the fibula with
Table 1. Ovadia score [16].
Objective evaluation Subjective evaluation
Excellent resultMotion of the ankle and the subtalar joint > 75% of No pain that on the normal sideNormal tibiotalar alignment Return to the same jobNo tibial shortening or chronic swelling Persues normal recreational activitiesNormal pronation-supination of the midpart of No limit in walking the footNo equines or calcaneus deformation No medication for pain No limp Good resultMotion of the ankle and the subtalar joint between Mild pain after strenuous activity50% and 75% of that on the normal sideNormal tibiotalar alignment Return to the same jobNo tibial shortening or chronic swelling Mild modification of recreational activities Normal pronation-supination of the midpart of the foot No limit in walkingNo equines or calcaneus deformation No medication for pain No limpFair resultMotion of the ankle and the subtalar joint between Moderate pain with regular work25% and 50% of that on the normal side≤ 5° of varus or valgus angulation or Patient works but has changed jobrecurvation≤ 1.0 cm of tibial shortening Significant modification in recreational activitiesModerate swelling Limited walking Moderately decreased pronation-supination of the Nonnarcotic analgesics for painmidpart of the footNo equines or calcaneus deformation Limp occasionally
Poor resultMotion of the ankle and the subtalar joint < 25% of Pain with each stepthat on the normal side> 5° of varus or valgus angulation or Unable to workrecurvation> 1.0 cm of tibial shortening Pursues no recreational activitiesSevere swelling Severely limited with respect to walkingMarkedly decreased pronation-supination of the Narcotic analgesics for painmidpart of the footEquines or calcaneus deformation of the ankle present Limp

Gehr J, et al. Fracture Management with the IP-XS Nail
381European Journal of Trauma 2004 · No. 6 © Urban & Vogel
an XS nail and application of an external fixator (type A3 fracture, III° open), the tibia was fixed permanently with an intramedullary AO nail. In six cases, a primary osteosynthesis of the tibia also took place, with percu-taneous plate osteosynthesis in three patients and with XS nail and cannulated screws to form a joint block in three patients.
ResultsAmong 32 osteosyntheses carried out up to now, can-cellous bone grafting of the distal tibial metaphysis for delayed union of fracture had to be performed in six cases. Two of these bone graftings were done within the framework of reosteosynthesis for nonunion after plate osteosynthesis. In three cases, apart from bone grafting, a retrograde suralis flap had to be used to attain soft-tissue coverage following primary damage to the soft tissue. Additional soft-tissue complicati-ons such as infections or cases of osteomyelitis did not occur (Table 2). The patient with infected nonunion following osteosynthesis in another clinic, achieved consolidation through a change of procedure, with an XS nail in the fibula and crossed XS nails in the tibia, including cancellous bone grafting. However, this pa-tient has recently had a poor subjective and objective Ovadia score result, with a very restricted ability to work and take part in sports. He also suffers from poor mobility in the lower and upper ankle joint, compared to the contralateral side.
An additional poor objective result arose through an 18° varus malpositioning of the distal tibial axis af-ter consolidation. 1½ years later a correction of the axis was performed using bone grafting and a plate os-teosynthesis.
All in all, four of 15 patients had an excellent, seven a good, three a fair, and one patient a poor result ac-cording to the subjective section of the Ovadia score. In the objective Ovadia score, three of 15 patients had an excellent, six a good, four a fair, and two a poor result (Table 3).
DiscussionIn spite of improved operative techniques and modified management, the pilon fracture continues to be one of the most serious fractures of the lower leg. In 1959, Jer-gesen [13] still regarded it as impossible to anatomical-ly reduce the fracture and to stabilize it internally. The treatment of pilon fractures by operative means became accepted after the introduction of the operation guideli-
nes and the standardization of the operative therapy by Ruedi, Matter, Allgöwer, and Heim [1, 11, 12].
Only the exact anatomic reduction and osteosynthe-sis stable enough for early functional physiotherapy makes satisfactory long-term results possible [12, 18, 20]. However, the four treatment principles of the AO-ASIF (reconstruction of the fibula with plates, reconstruction of the joint, bone grafting, and medial support) do not take the frequently heavy damage to the soft tissue into account. These circumstances have led to a reworking of the operative strategy, setting out the primary manage-ment of the soft tissue as a priority [5, 6, 18].
In 1994, Rommens et al. were able to demonstrate that the primary consolidation of the soft tissue is di-rectly connected to acceptable long-term results [17]. As a consequence, the operative tactics was modified into a two-sided procedure [3, 4, 15, 21, 22]. The de-finitive fracture treatment allowing early mobilization exercise takes place after an interval following prima-ry stabilization with external fixation and soft-tissue consolidation. Another consequence of this study was that big implants requiring more space are accompa-nied by a higher rate of complications, because of the more extensive soft-tissue damage caused, and the disruption to the microcirculation associated with it. The implementation of pure screw osteosynthesis through minimally invasive approaches, particularly on the tibia, was one of the results. After this modifi-cation, Rommens et al. were able to achieve > 70%
Table 2. Complication rates of 15 patients reexamined 12 months after osteosynthesis.
Osteomyelitis 0/15 (0%) Arthrodesis 0/15 (0%) Amputation 0/15 (0%) Soft-tissue reconstruction 1/15 (8%) retrograde suralis flapBone graft after XS nail osteosynthesis 1/15 (8%) delayed metaphyseal tibial unionSecondary reosteosynthesis after XS 1/15 (8%)nail osteosynthesis of the tibia
Table 3. 15 patients reexamined using the Ovadia score [16] 12 months after osteosynthesis.
Objective evaluation Subjective evaluation
3/15 (20.0%) excellent 4/15 (26.6%) excellent 6/15 (40.0%) good 7/15 (46.7%) good 4/15 (26.7%) fair 3/15 (20.0%) fair 2/15 (13.3%) poor 1/15 (6.6%) poor
Gehr J, et al. Fracture Management with the IP-XS Nail
382 European Journal of Trauma 2004 · No. 6 © Urban & Vogel
good final results in the subjective and > 60% good final results in the objective section, according to the Ovadia score. Bastian et al. could consolidate these results. Their patient group achieved a very good func-tional outcome at 54%; 80% of the patients were able to continue to work in their original profession and 59% were able to pursue their sports activities without any changes [1]. Up to now, the results of our study with the XS nail have not revealed greater problems regarding the soft tissue. Furthermore, we have not yet observed late osseous complications, such as os-teomyelitis or infected pseudarthrosis after fresh pi-lon fractures. It was only possible to achieve union of an already existent infected pseudarthrosis in one case, with a change of procedure, through XS nail os-teosynthesis and bone grafting. By contrast, osseous complications of 5.9–25% are given in the literature
[1, 8]. The 15 osteosyntheses (eight pilon fractures and seven distal metaphyseal lower leg fractures) already carried out with the new implant and the initial results of the follow-up investigation, at 73.3% subjective and 60% objective outstanding, excellent or good results in the Ovadia score, are hopeful. The presented per-cutaneous technique to treat concomitant fibular frac-tures in the case of pilon fractures enabled us to relin-quish a second open lateral access. Thus, no further stress to the posttraumatic soft-tissue situation arises. This minimally invasive osteosynthesis of the fibula meets the demands of many authors giving maximum consideration to the soft-tissue situation. At the same time, it represents an optimal preparation for the treatment of the tibia considering axis alignment, ro-tation and length. If plate osteosynthesis of the tibia is not possible because of stressed soft tissue, the tibia
c
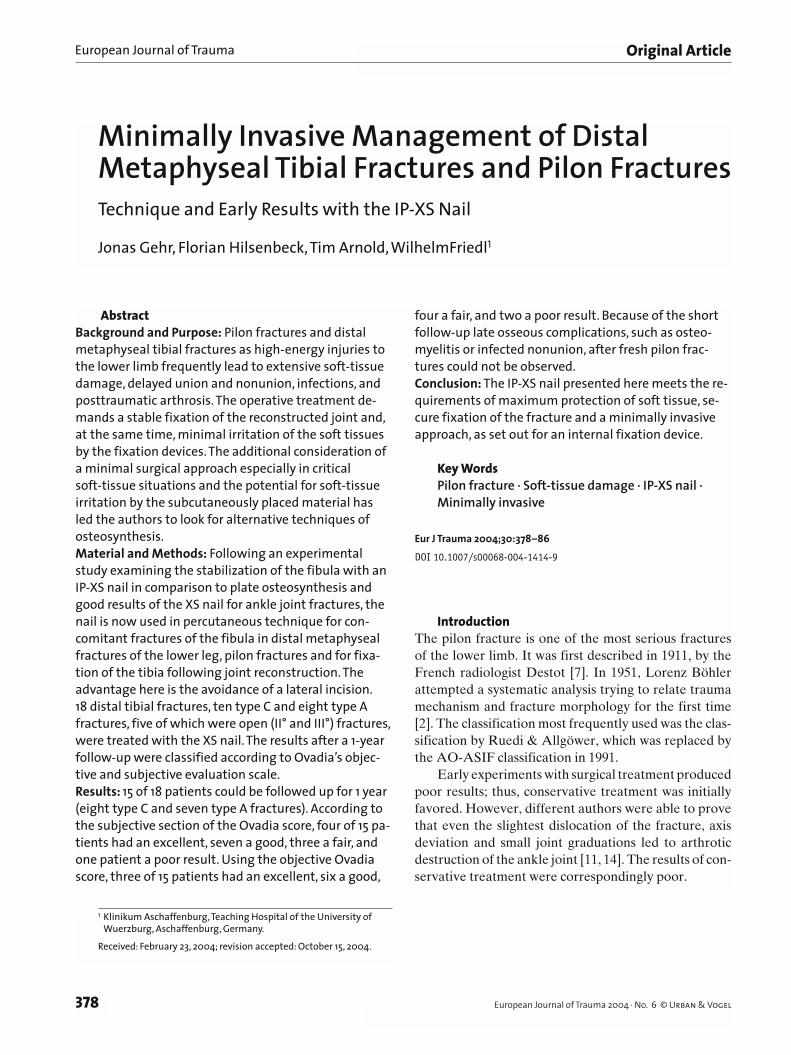
Figures 2a to 2g. 69-year-old patient after a fall from a 2-m ladder. a, b) II° open C1 pilon fracture with severe varicosis.c, d) Primary temporary external fixation and closed standard XS nail osteosynthesis of the fibula.e) After subsidence of swelling a combination of percutaneous standard XS nail osteosyn-thesis of the tibia was performed. No further soft-tissue problems occurred.f) Full weight bearing at 10 weeks.g) Removal of hardware after 1 year according to the patient’s wish.
a b
d e f
g

Gehr J, et al. Fracture Management with the IP-XS Nail
383European Journal of Trauma 2004 · No. 6 © Urban & Vogel
Figures 3a to 3c. 41-year-old man after a fall from 2 m. a) Closed type C3 pilon fracture.b) Primary percutaneous XSL nail osteosynthesis of the fibula and external fixation.c) 5 days later minimally invasive reconstruction of the tibia and ankle joint with percutaneous screws and plate fixation.
a b c
Figures 4a to 4d. 27-year-old man after a motorcycle accident. a) Closed type C3 pilon fracture.b) Primary percutaneous XSL nail osteosynthesis of the fibula for correction of length, rotation, and axis of the tibia.c, d) 6 days later removal of the external fixator, open reduction of the tibial joint, and fixation of tibia with a standard XS nail and threaded K-wires.
a b c d
can also be fixed definitively, or at least temporarily, through percutaneous initial XS nailing (Figures 2 to 4). However, this is only sensible in slightly dislocated joint fractures, purely metaphyseal (type A) fractures or joint fractures that can be repositioned and retained percutaneously with the elevator and joystick wires (Figures 5).
As it could be shown in this study, the presented XS nail meets the requirements of maximum consider-ation of the soft tissue with reliable stabilization as made on an implant. The intramedullary positioning of the XS nail avoids an additional traumatization of the soft tissue through the mortise, particularly in the case of high-risk patients with poor blood circulation or dia-betes and in case of extended posttraumatic contu-sions. Improved strength is also created in the case of osteoporotic fractures, because of the high intrinsic
stability and the intramedullary position of the im-plant. The aim is covered treatment of the fibula, with-in the framework of the primary minimal osteosynthe-sis, in the case of concomitant fibular fractures of a pilon fracture. The tibia can usually be treated without problems after a soft-tissue consolidation phase of 5–6 days. In some cases, it has already become evident that a one-timed procedure seems sensible, independently of the soft-tissue situation, because fixing the tibia with the XS nail does not represent a greater trauma than the application of an external fixator (Figure 6). How-ever, if no metaphyseal callus formation is present af-ter 6 weeks, an additional plate osteosynthesis must take place, which we also perform as a percutaneous plate osteosynthesis (Figure 7).
A change in pilon management away from primary temporary and secondary definitive treatment, toward
Gehr J, et al. Fracture Management with the IP-XS Nail
384 European Journal of Trauma 2004 · No. 6 © Urban & Vogel
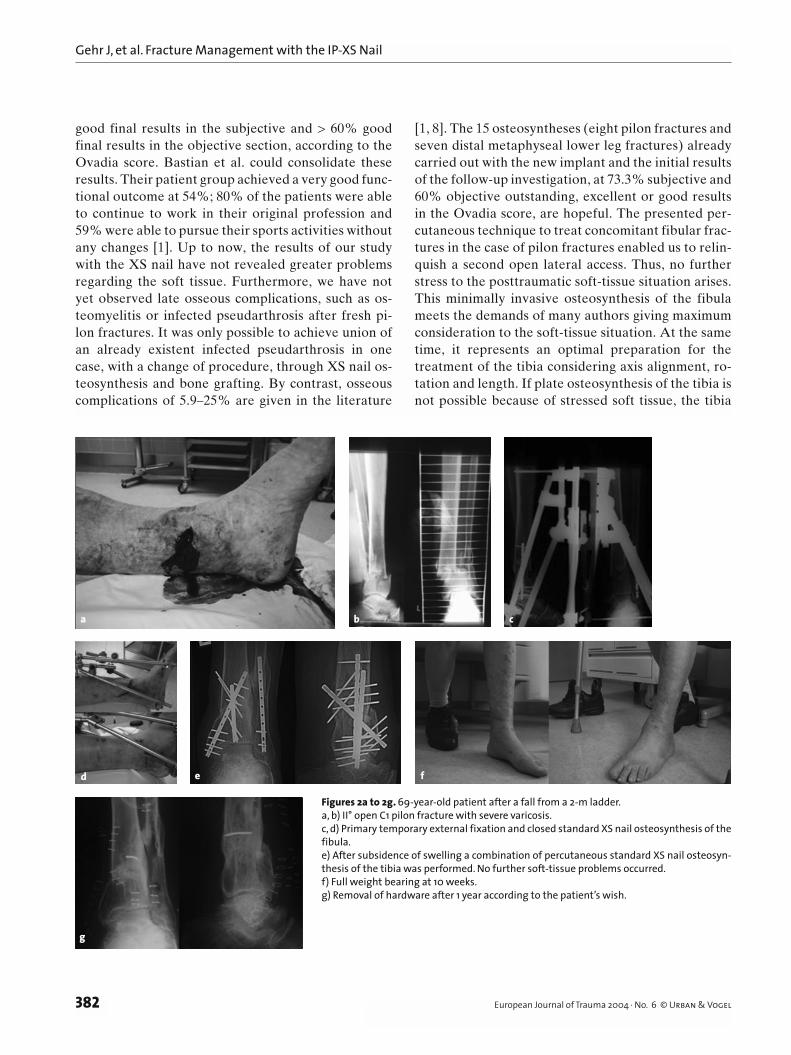
Figures 6a to 6d. 79-year-old woman with an axial trauma after a suicide attempt; fall from 4 m. a) Severe pilon fracture type C3.b) Primary closed osteosynthesis of the fibula with an XSL nail and percutaneus osteosyn-thesis of the tibia with XS nail and cannulated screws.c) After 1 year.d) After metal removal.
a b
c d
Figures 5a to 5d. 80-year-old adipose patient with an axial trauma. a) Closed distal osteoporotic lower leg fractu-re.b) Primary osteosynthesis of the fibula with XSL nail and closed osteosynthesis of the tibia with standard XS nails.c, d) X-ray and soft tissue 1 year after treat-ment.
a b
c d
Gehr J, et al. Fracture Management with the IP-XS Nail
385European Journal of Trauma 2004 · No. 6 © Urban & Vogel
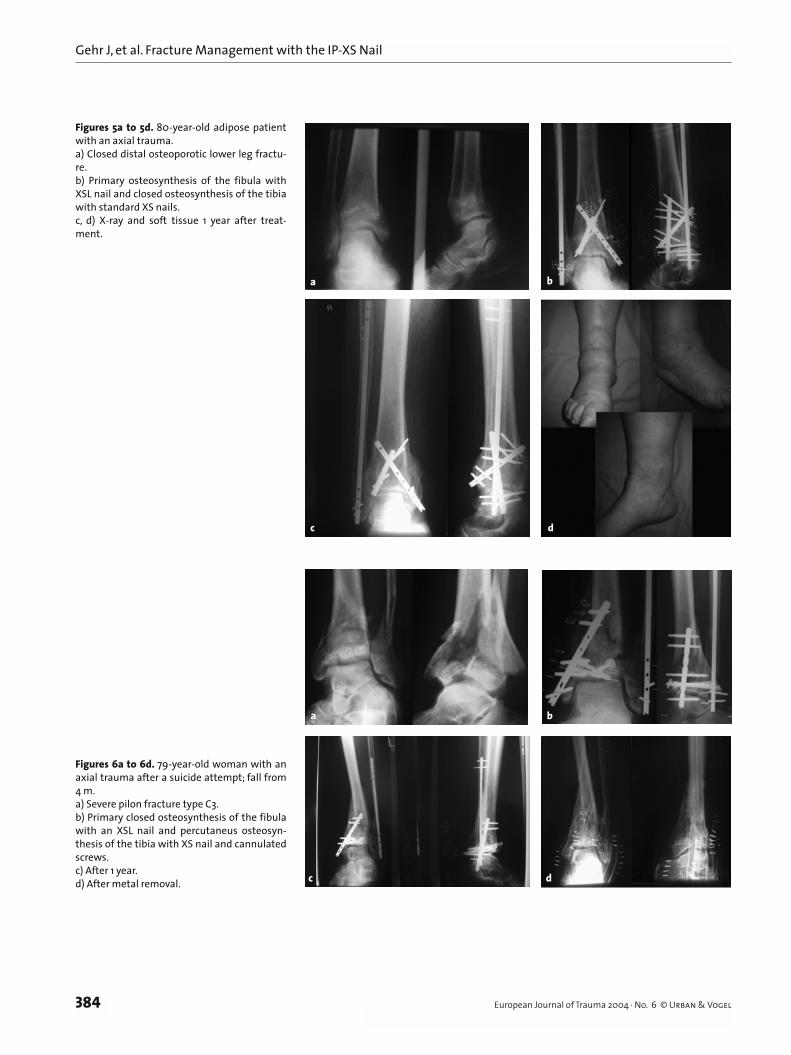
Figures 7a to 7e. 26-year-old woman after a car accident. a) III° open pilon fracture with severe medial soft-tissue and bone defect.b) Primary debridement and closed XSL nail osteosynthesis of the fibula, temporary external fixation, and reconstruction of the joint using K-wires and a screw.c) After subsidence of swelling and consolidation of the soft tissue using a vacuseal system and suralis flap, fixation of the tibia with a bone block and a standard XS nail.d, e) After 10 weeks, no callus formation in the distal tibial metaphysis. Indication for bone grafting and additional angle-stable plate fixation.
a b
c ed
primary definitive treatment, has been discussed be-cause of the new forms of osteosynthesis available such as the LCP, the LISS or the XS nail. It remains to be seen whether the early results, which have been good up to now, will also be confirmed after long-term fol-low-up investigations in larger series.
References 1. Bastian L, Blauth M, Thermann H, et al. Verschiedene Thera-
piekonzepte bei schweren Frakturen des Pilon. Unfallchirurg 1995;11:551–8.
2. Böhler L. Die Technik der Knochenbruchbehandlung 12–13 cdn. Wien: Maudrich, 1951 (reprint 1977).
3. Borrelli J, Catalano L. Current controversies in orthopaedic trauma: open reduction and internal fixation of pilon fractures. J Orthop Trauma 1999;13:573–82.
4. Borrelli J, Ellis E. Pilon fractures: assessment and treatment. Orthop Clin North Am 2002;33:231–45.
5. Bourne RB, Rorabec CH, Macnab J. Intra-articular fractures of the distal tibia: the pilon fracture. J Trauma 1983;23:591–5.
6. Burwell HN, Charnley AD. The treatment of displaced fractures
of the ankle by rigid internal fixation and early joint movement. J Bone Joint Surg Br 1965;47:634.
7. Destot E. Traumatismes du pied et rayons: X malléoles, astragale, calcanéum, avantpied. Paris: Masson, 1911:1–10.
8. Gay R, Evrard J. Les fractures récentes du pilon tibial chez l’adulte. Rev Chir Orthop 1963;49:397–411.
9. Gehr J, Friedl W. Neues Konzept in der Therapie der distalen Tibiametaphysenfrakturen und wenig dislozierten Pilonfrakturen mit schwerem Weichteilschaden. Unfallchirurg 2002;105:643–6.
10. Gehr J, Neber W, Hilsenbeck F, et al. New concepts in the treat-ment of ankle joint fractures. Arch Orthop T rauma Surg 2004;124:96–103.
11. Heim U. Die Pilon-tibial-Fraktur. Klassifikation, Operationstech-nik, Ergebnisse. Berlin–Heidelberg–New York: Springer, 1991.
12. Heim U, Naser M. Die operative Behandlung der Pilon-tibial-Frak-tur. Technik der Osteosynthese und Resultate bei 128 Patienten. Arch Orthop Unfallchir 1976;86:341–56.
13. Jergesen F. Fractures of the ankle. Am J Surg 1959;98:136–45.14. Kett K, Aichner R, Wesseley E. Der Einfluss der Reposition des mal-
leolus lateralis bei der Behandlung bimalleolarer Knochenbrüche. Monatsschr Unfallheilkd Invalidenw 1965;68:82.
15. Kilian O, Buundner MS, Horas U, et al. Langzeitergebnisse nach operativer Versorgung von Pilon-tibial-Frakturen. Eine retrospek-tive Untersuchung. Chirurg 2002;73:65–72.

Gehr J, et al. Fracture Management with the IP-XS Nail
386 European Journal of Trauma 2004 · No. 6 © Urban & Vogel
16. Ovadia DN, Beals RK. Fractures of the tibial plafond. J Bone Joint Surg Am 1986;68:543–51.
17. Rommens M, Claes P, De Boodt P, et al. Therapeutisches Vorgehen und Langzeitergebnisse bei der Pilonfraktur in Abhängigkeit vom primären Weichteilschaden. Unfallchirurg 1994;97:39–46.
18. Ruedi T. Pilon tibiale Frakturen: Whats new? Klassifikation, Opera-tionstechnik, Ergebnisse. Berlin–Heidelberg–New York: Springer, 1991:204–8.
19. Ruedi T, Allgöwer M. Fractures of the lower end of the tibia into the ankle joint. Injury 1969;1:92–9.
20. Ruedi T, Allgöwer M. Spätresultate nach operativer Behandlung der Gelenkbrüche am distalen Tibiaende (sog. Pilon-Frakturen). Unfallheilkunde 1978;81:319–23.
21. Sirkin M, Sanders R, DiPasquale T, et al. A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma 1999;13:78–84.
22. Watson JT, Moed BR, Karges DE, et al. Pilon fractures: treatment protocol based on severity of soft tissue injury. Clin Orthop 2000;375:78–90.
Address for CorrespondenceJonas Gehr, MDDepartment of Trauma and Reconstructive SurgeryTeaching Hospital AschaffenburgAm Hasenkopf 163739 AschaffenburgGermanyPhone (+49/6021) 32-0, Fax -4202e-mail: [email protected]
Related Documents











